
Submitted:
27 October 2025
Posted:
28 October 2025
You are already at the latest version
Abstract
Primary biliary cholangitis (PBC) is a chronic autoimmune liver disease characterized by progressive destruction of intrahepatic bile ducts. Autoantibodies, particularly anti-mitochondrial antibodies (AMA) and antinuclear antibodies (ANA), are central to diagnosis, prognosis, and pathogenesis. This review provides a comprehensive overview of classical and emerging autoantibodies associated with PBC, including AMA-M2, anti-gp210, anti-sp100, anti-KLHL12, and anti-RPL30. We discuss their diagnostic significance, pathogenic implications, and potential utility in patient stratification and therapeutic monitoring. Furthermore, we explore the role of microbial factors and environmental triggers in autoantibody generation, highlighting molecular mimicry and gut–liver axis interactions. Advances in autoantibody profiling may pave the way for personalized medicine and improved outcomes in PBC.
Keywords:
primary biliary cholangitis (PBC)
; autoantibodies
; anti-mitochondrial antibody (AMA)
; antinuclear antibody (ANA)
; molecular mimicry
1. Introduction
In autoimmune liver diseases (AILD), the immune system aberrantly reacts against specific components of the liver, leading to the production of circulating autoantibodies. These autoantibodies play a crucial role in disease diagnosis, differentiation of clinical subtypes, and even prognostic assessment. Primary biliary cholangitis (PBC) is a prototypical form of AILD and is a chronic, progressive cholestatic liver disease that predominantly affects middle-aged and older women. Globally, it is estimated that approximately one in 1,000 women over 40 years of age is affected [1]. In North America and Europe, the incidence increased until around 2000 and then plateaued, whereas in the Asia–Pacific region a gradual rise has continued since 2000[2]. With advances in diagnostic technologies and improved understanding of the disease, prevalence rates have steadily increased across many regions [3,4]. In PBC, autoimmune mechanisms target the small intrahepatic bile ducts, resulting in progressive inflammation and destruction that lead to cholestasis, fibrosis, and ultimately cirrhosis. For diagnosis, not only clinical features and biochemical abnormalities of cholestasis (such as elevated alkaline phosphatase) but also the detection of serum autoantibodies are of paramount importance [5]. Indeed, current international diagnostic criteria—EASL 2017 [1] and AASLD 2018 [6]—define three key requirements: (i) evidence of cholestasis, typically alkaline phosphatase elevation; (ii) seropositivity for autoantibodies, mainly AMA-M2 or PBC-specific ANA; and (iii) histological findings of chronic nonsuppurative destructive cholangitis (CNSDC) and/or loss of interlobular bile ducts. Thus, autoantibodies are positioned as central biomarkers for PBC diagnosis. Beyond diagnosis, autoantibodies contribute to elucidating disease mechanisms, stratifying patients, predicting prognosis, and informing therapeutic strategies. The aim of this review is to provide a comprehensive and up-to-date overview of autoantibodies associated with PBC, integrating the latest findings into an overall understanding of their diagnostic and clinical relevance.
2.1. Anti-Mitochondrial Antibodies (AMA)
2.1.1. Historical Background and Diagnostic Significance
The association between PBC and autoantibodies was first suggested in 1958, when Mackay reported high titers of complement-fixing antibodies directed against tissue antigens in the liver and kidney [7]. In 1965, Walker and colleagues used indirect immunofluorescence (IIFL) to identify AMA in the sera of PBC patients, thereby establishing AMA as a serological marker for PBC diagnosis [8]. AMA are detected in approximately 90–95% of patients with PBC [1,9,10], whereas their prevalence in the general population is extremely low, at about 0.1–0.2% [11]. Importantly, AMA can often be detected in serum several years before the onset of clinical symptoms or biochemical abnormalities [12]. Among asymptomatic individuals with normal biochemical profiles but detectable AMA, histological features of PBC are already present in about 40% of cases, and clinical disease may subsequently develop over the following years [13]. Nevertheless, only about one in six AMA-positive individuals develop clinically apparent PBC within five years [14].
2.1.2. Target Antigens of AMA
The major target antigen of AMA is the E2 subunit of the pyruvate dehydrogenase complex (PDC-E2). AMA also react with other members of the 2-oxoacid dehydrogenase complex family, including the branched-chain 2-oxoacid dehydrogenase E2 (BCOADC-E2) and the α-ketoglutarate dehydrogenase E2 (OGDC-E2) [15,16]. All of these antigens are localized to the inner mitochondrial membrane, share a lipoic acid moiety, and participate in oxidative phosphorylation [17].
AMA can be subdivided into M1–M9 patterns based on antigenic specificity, with anti-M2, anti-M4, anti-M8, and anti-M9 most strongly associated with PBC [15,16]. Among these, anti-M2 antibodies have the highest diagnostic relevance and can be detected not only in serum but also in bile and saliva [18]. The M2 antigen corresponds to several molecular bands of 70, 56, 51, 45, and 36 kDa, all of which are derived from enzymatic components such as PDC-E2 and BCOADC-E2 [18]. Approximately 90–95% of PBC sera react with PDC-E2, establishing this antigen as the central autoantigen in the disease [16].
2.1.3. Evolution of AMA Detection Methods
Since its discovery, IIFL has been regarded as the “gold standard” for AMA detection, with titers above 1:40 considered positive [21]. In the triple-substrate method, which uses distal renal tubules, gastric mucosa, and liver tissue, AMA produce a characteristic fluorescence pattern [22]. AMA are not restricted to a single IgG subclass, but IgG3 predominance has been reported [23].
The introduction of solid-phase assays has significantly changed the diagnostic approach to PBC. Following the identification of AMA molecular targets, new molecular-based tests using recombinant or purified antigens have been developed. Representative methods include enzyme-linked immunosorbent assays (ELISA) on microtiter plates, chemiluminescence assays, and bead-based fluorescent assays [24,25,26]. Among these, commercially available ELISA kits have become widely adopted over time, offering high levels of standardization and automation, and eliminating the need for highly skilled personnel to perform and interpret the tests [27].
A major advance was achieved with the development of MIT3 by Gershwin and colleagues, a recombinant antigen that fuses immunodominant epitopes of PDC-E2, BCOADC-E2, and OGDC-E2. ELISA assays employing MIT3 identified AMA positivity in 30–50% of cases previously classified as negative by conventional methods, thereby markedly improving sensitivity [28,29]. More recently, enhanced bead-based techniques coupling three recombinant mitochondrial autoantigens (PDC-E2, BCOADC-E2, and OGDC-E2) have detected AMA in 20% of patients who were negative by IIFL; all of these newly identified AMA-positive patients were also ANA-positive [30]. The novel anti-M2-3E ELISA, which includes MIT3 and purified PDC, allows detection of mitochondrial antigens with lower immunodominance, such as PDC-E1a and E1b, and has shown further improvement in diagnostic accuracy compared with IIFL, traditional anti-PDC ELISA, and anti-MIT3 ELISA [24].
3. Antinuclear Antibodies (ANA) in Primary Biliary Cholangitis
3.1. Basis of ANA Testing
ANA are among the most representative autoantibodies detected in various autoimmune diseases such as systemic lupus erythematosus and systemic sclerosis, and they have long been used as clinical indicators of autoimmune reactivity [31]. The standard substrate for ANA testing is the HEp-2 cell line, which has served as the international reference since the 1970s [32]. HEp-2 cells have large nuclei and abundant mitotic figures, which make observation of fluorescence patterns easier and allow classification of diverse patterns reflecting antibody localization [22].
In the diagnosis of PBC, AMA have traditionally been used as a highly specific serological marker. However, a subset of PBC patients are AMA-negative, and in this group the presence of ANA is an indispensable adjunct to diagnosis [33].
3.2. Frequency and Characteristic ANA Patterns in PBC
ANA are detected in up to 70% of patients with PBC [34]. Several immunofluorescence patterns have been described as characteristic of PBC [35]. Figure 1. is an illustration of the ANA patterns.
・Multiple Nuclear Dots (MND) pattern:
This consists of 3–20 discrete dots scattered throughout the nucleus, sparing nucleoli. It is generated by reactivity to the 100-kDa sp100 protein and promyelocytic leukemia (PML) protein; more recently, sp140 and small ubiquitin-related modifier (SUMO) proteins have been reported as additional antigenic targets [36].
・Rim-like/Membranous (RL/M) pattern:
This produces a distinctive punctuation pattern on the nuclear envelope, reflecting reactivity to the nuclear pore complex (NPC), a multiprotein structure mediating nucleocytoplasmic transport. Sp210 is a major antigenic target in PBC and is currently used for diagnostic purposes. Other antigens with lower immunodominance but potential diagnostic relevance include nucleoporin p62 and the lamin B receptor (LBR) [37].
・Anti-centromere antibody (ACA) pattern:
This shows a punctate fluorescence aligned with centromeres. Although reported prevalence varies, ACA is generally present in 10–30% of PBC patients and is not specific for PBC [38]. ACA-positive cases often exhibit Raynaud’s phenomenon, telangiectasia, and sicca symptoms resembling connective tissue diseases, and overlap with systemic sclerosis (SSc) is a clinical concern. Indeed, the reported frequency of PBC–SSc overlap ranges from 1.4% to 17%, underscoring ACA’s importance as a serological marker linking these two diseases [39].
3.3. Additional High-Specificity Antibodies
Although anti-p62 antibodies are detected infrequently, their presence is highly specific for PBC. Therefore, even in patients negative for AMA, anti-gp210, and anti-sp100, detection of anti-p62 carries significant diagnostic weight as an important supplementary serological marker [41]. Anti-LBR antibodies also show high specificity for PBC and were detected in 15% of PBC patients including AMA-M2-negative cases, but not in other diseases or healthy controls [41,42].
4. Emerging Autoantibodies
4.1. Anti-Kelch-like 12(KLHL12) Antibody
Unlike conventional AMA or ANA, anti-KLHL12 antibodies are detected in a substantial proportion of marker-negative cases. They are present in ~40% of all PBC patients (42% AMA-positive, 35% AMA-negative) and exhibit 96.1% specificity compared with non-PBC diseases [43]. The Kelch-like (KLHL) protein family, comprising 66 genes, has been implicated in diverse cellular processes, including cytoskeletal organization, intercellular communication, transcriptional regulation, collagen export, and protein ubiquitination through interactions with cullin–RING E3 ligases. [44,45,46]. KLHL12, a nuclear member of this evolutionarily conserved superfamily, plays a pivotal role in collagen export [46]. The KLHL12 antigen has been identified by microarray, proteomic, and modified ELISA analyses [47].
4.2. Anti-RPL30 Antibody
Diagnosis is particularly challenging when all major autoantibodies (AMA, AMA-M2, anti-gp210, anti-sp100) are negative. Zeng et al. identified anti-RPL30 as showing the most prominent change in PBC, with high positivity even in antibody-negative cases [48]. ROC analysis yielded an AUC of 0.853, specificity 100%, and sensitivity 75%, and combined testing improved diagnostic yield from 61.3% to 79.0% [48].
4.3. Anti-HK1 Antibody
Hexokinase-1 (HK1), located on the outer mitochondrial membrane, catalyzes the phosphorylation of glucose to glucose-6-phosphate [49]. Beyond glucose metabolism, HK1 maintains mitochondrial homeostasis and regulates apoptotic susceptibility [50]. Anti-HK1 antibodies are significantly more frequent in PBC than in non-PBC controls (p<0.001) with 96.9% specificity [43]. The mechanisms underlying anti-KLHL12 and anti-HK1 production remain unclear [43].
5. Microbial Factors in the Pathogenesis of PBC
5.1. Molecular Mimicry as a Central Hypothesis
In PBC, AMA and ANA are the principal serological indicators of an ongoing autoimmune response; however, conclusive evidence demonstrating that these antibodies directly mediate bile duct injury remains limited [51]. Among the major hypotheses explaining the autoimmune pathogenesis of PBC, molecular mimicry is considered central [52]. In this model, exogenous antigens structurally resemble self-antigens and thereby induce cross-reactive immune responses. The principal autoantigen of PBC, the E2 subunit of the PDC-E2, is highly conserved across diverse microbial species, particularly within the Enterobacteriaceae family, creating opportunities for cross-reactivity and loss of immune tolerance [53].
5.2. Gut Microbiota and Autoimmune Activation
The interaction between the gut microbiota and the liver—the so-called gut–liver axis—has emerged as a key area of interest in PBC pathogenesis [54]. Alterations in gut microbial composition appear to modulate systemic immune responses and may promote the breakdown of tolerance to biliary epithelial cells. Several uncommon bacterial taxa have been reported to increase in PBC patients compared with healthy controls, suggesting their involvement in autoimmune activation [55]. Notably, unidentified genera within the Enterobacteriaceae show a strong association with PBC; rough mutants or other antigenic variants within this family may trigger AMA production via molecular mimicry mechanisms [53]. Klebsiella species—also Enterobacteriaceae members—correlate with serum bilirubin concentrations in PBC and are already implicated in other autoimmune diseases such as ankylosing spondylitis and Crohn’s disease, suggesting a shared immunopathogenic pathway [53]. Conversely, beneficial commensals with anti-inflammatory properties—including Faecalibacterium, Bacteroides, Sutterella, and Oscillospira—are reduced in PBC, particularly in gp210-positive patients [56]. Faecalibacterium prausnitzii, a major butyrate producer essential for maintaining mucosal immune homeostasis, may thus be protective; its depletion has been proposed to contribute to disease onset or perpetuation [56].
5.3. Specific Bacterial Antigens and Autoantibody Generation
A representative example of a potential molecular mimic is Escherichia coli (E. coli). Due to the high sequence homology between human PDC-E2 and E. coli PDC-E2, the bacterium has been proposed as a potential inducer of AMA production [57]. Specific antibodies directed against E. coli-derived PDC-E2 can cross-react with the lipoyl domain of human PDC-E2 through epitope spreading, leading to the generation of classical AMA [58]. Anti-gp210 antibodies may similarly arise following infection or shifts in the hepatic–intestinal microbial balance. The gp210 epitopes share homology with the protein products of the mutY gene in E. coli and the mutB gene in Salmonella typhimurium, with an exact identity of six consecutive amino acids [59]. This finding supports the notion that anti-gp210 antibodies may develop through molecular mimicry of bacterial antigenic determinants [60]. Moreover, antibody titers to E. coli antigens are more pronounced in advanced PBC, suggesting a link between unsanitary environments and later-age onset [61], and the recent increase in male patients may similarly reflect evolving environmental exposures [62]. Another noteworthy environmental microorganism is Novosphingobium aromaticivorans, which exhibits high homology with human mitochondrial autoantigens. In PBC patients, antibody titers to this bacterium are reported to be up to 1,000-fold higher than those to E. coli and detectable even in early or asymptomatic cases [63]. The proposed mechanism of autoantibody production leading to autoimmune activation in PBC is shown in Figure 2.
6. Environmental and Epidemiological Risk Factors
6.1. Exogenous Chemical Modifications of Autoantigens
The liver is specialized to metabolize complex food-derived substances. Recent findings show that chemical compounds can mimic PDC epitopes and are recognized by circulating antibodies in PBC sera. These chemical-specific antibodies often display higher affinity than those to native mitochondrial autoantigens [64]. Halogenated compounds or haloethyl agents can modify the inner lipoyl domain of E2 and enhance AMA reactivity in PBC patients [64]. This suggests that exogenous chemicals may “antigenize” intracellular components, although whether such modifications directly trigger disease onset remains unresolved [61].
6.2. Epidemiological Evidence for Environmental and Genetic Susceptibility
Various exogenous factors—including bacteria, viruses, and environmental chemicals—have been implicated as potential triggers [61]. Epidemiological investigations have revealed significant associations between PBC onset and exposures such as smoking, urinary tract infections, manicure products, and hair dyes [17,65,66]. Moreover, the prevalence of AMA among first-degree relatives of PBC probands is 13.1%, compared with only 1% in matched controls [67], strongly suggesting that both environmental risks and genetic determinants contribute to disease etiology.
7. Autoantigen-Specific Immune Responses in Primary Biliary Cholangitis
7.1. Breakdown of Immune Tolerance and T-Cell Responses
The pathogenesis of PBC begins with the breakdown of immune tolerance to self-antigens. PDC-E2 has been identified as the principal target antigen in PBC [68]. Proinflammatory cytokines can induce overexpression of PDC-E2 epitopes in biliary epithelial cells (BECs), which, through antigen presentation by dendritic cells, activate autoreactive T cells [69]. CD4+ and CD8+ T cells accumulate within the portal tracts and induce BEC apoptosis via Fas ligand (FasL), perforin, and granzyme B [70]. Chemokines such as CXCL10 and CXCL9 further recruit T cells to the local microenvironment and perpetuate inflammation [71] . Recently, a PDC-E2-specific CD8+ T-cell epitope (amino acids 159–167) was identified, providing direct evidence for cytotoxic T-cell responses against self-antigens in PBC [72]. These findings indicate that self-antigen presentation represents an essential pathogenic step preceding autoantibody production.
7.2. Link Between Innate Immunity and Autoantibody Induction
Innate immune mechanisms act in concert with adaptive immunity to amplify the antibody response. In PBC livers, CD1d-dependent natural killer T (NKT) cells and NK cells are increased and convert CD4+ T cells into cytotoxic phenotypes through IFN-γ [73]. Moreover, dysregulation of the Th17/Treg balance is closely associated with sustained inflammation and fibrotic progression [73]. These innate and adaptive immune interactions activate dendritic cells, which in turn stimulate B cells, leading to plasma cell production of diverse autoantibodies [74].
7.3. Apoptosis, Antigen Supply, and Disease Progression
BEC apoptosis plays a critical role in amplifying the autoimmune response. During apoptosis, PDC-E2 remains structurally intact without glutathionylation [77] and is retained within apoptotic bodies in an immunogenic form [78]. These apoptotic bodies can trigger inflammatory cytokine responses in mononuclear cells, thereby intensifying local inflammation. Impaired clearance of apoptotic cells (defective efferocytosis) has also been reported, resulting in secondary necrosis and persistent exposure of self-antigens to the immune system [79,80]. This process reinforces autoantibody production and sustains chronic immune responses [81].
Even in AMA-negative PBC, PDC-E2-specific T-cell responses have been demonstrated, underscoring that T-cell immunity, not solely autoantibody production, constitutes a central pathogenic mechanism [82]. Furthermore, increased expression of gp210 and mitochondrial antigens in small bile duct BECs has been reported [83,84]. These molecules become targets for anti-gp210 and other nuclear antibodies, potentially explaining selective damage to specific cholangiocyte populations.
8. Diagnostic and Prognostic Significance of Autoantibodies
Beyond their diagnostic utility, PBC-associated autoantibodies offer insights into prognosis and disease stratification. Among these, anti-gp210 antibody has become one of the most powerful predictors of adverse outcomes [85]. Multiple studies have shown that PBC patients who are anti-gp210–positive have significantly poorer outcomes than those who are negative [58]. Anti-gp210 antibodies are strongly associated with cirrhosis, hepatic functional decline, and severe cholestasis [86]. Patients who are anti-gp210–positive at diagnosis exhibit markedly higher rates of hepatic failure (RR = 5.77, 95% CI: 2.9–11.48) and mortality (RR = 2.38, 95% CI: 1.62–3.51) [87]. In a large U.K. cohort, anti-gp210 positivity was also linked to higher liver enzyme levels, bilirubin, and liver stiffness, as well as increased risk of all-cause death or liver transplantation (HR 3.22, 95% CI: 1.49–6.96; P = .003) [88]. Furthermore, sustained seropositivity for gp210 [83] and high gp210 expression in small bile ducts [89] have been reported to predict progression to end-stage liver failure.
The reported prevalence of anti-sp100 in PBC patients ranges from 8.7% to 40.0%[90,91,92]. However, no significant difference in the frequency of anti-sp100 was observed between AMA-positive and AMA-negative PBC patients, indicating that anti-sp100 is unlikely to serve as a complementary serological marker for PBC in AMA-negative patients [93].
AMA remains the most sensitive and specific serologic marker for the diagnosis of PBC. AMA is often detectable before the onset of clinical symptoms or biochemical cholestasis, making it particularly useful for early identification of asymptomatic PBC [12]. However, the relationship between AMA titers and disease severity or progression is less clear. Although AMA titers can vary more than 200-fold between patients, they tend to remain stable within an individual over many years and have not been shown to predict prognosis [94]. Therefore, the presence of AMA, rather than its titer, is critical for diagnosis [95]. While the classical view holds that AMA titer does not correlate with disease severity [96], some studies suggest otherwise [25]. In particular, the IgG3 subclass of AMA has been strongly associated with adverse prognosis; patients with IgG3 AMA positivity display more advanced histologic disease and higher rates of cirrhosis [97]. IgG3 AMA titers also show a positive correlation with the Mayo risk score, suggesting that this isotype may mediate immune injury more specifically [97].
AMA-negative PBC accounts for approximately 5–10% of all cases [25]. Although the clinical presentation and treatment response are generally similar to AMA-positive cases [98], delayed diagnosis may contribute to poorer outcomes [99].
Other autoantibodies have also been linked to disease progression and prognosis. ACA is associated with more rapid development of portal hypertension and earlier occurrence of esophagogastric varices [38]. Anti-RPL30 antibody correlates with the international normalized ratio (INR) and MELD score, suggesting potential utility in severity assessment [33]. Anti-KLHL12 antibody has been associated with bilirubin elevation, fibrosis, and poorer outcomes, supporting its role as a risk factor [42]. By contrast, anti-LBR antibody has not been linked to survival but has been reported to correlate with2 hepatic fibrosis [42]. The characteristics of the autoantibodies are summarized in Table 1.
9. Autoantibodies and Therapeutic Response in Primary Biliary Cholangitis
The effect of ursodeoxycholic acid (UDCA) therapy on AMA titers in patients with PBC remains unresolved. Several studies have reported that responders to UDCA exhibit a decrease in AMA titers—particularly IgG-AMA—that can persist over long periods [100]. A Chinese cohort study demonstrated that reductions in serum IgG-AMA correlated with biochemical improvement [101], and Japanese data also showed decreases in IgG-AMA and anti-pyruvate dehydrogenase antibodies following UDCA therapy [101]. These findings suggest that changes in AMA titers could serve as surrogate markers of treatment response.
Conversely, other investigations have yielded conflicting results. A Japanese study with a mean follow-up of 13.5 years found no significant changes in AMA titers over time regardless of UDCA administration [102]. It has also been reported that UDCA decreases IgM-AMA but does not affect IgG-AMA [103], and a long-term U.S. follow-up study similarly found no significant changes in IgG-AMA titers [104]. Thus, the impact of UDCA on AMA titers appears to vary by region and population, possibly reflecting genetic factors, ethnic differences, or heterogeneity in AMA subclasses.
Beyond direct effects on autoantibodies, UDCA therapy has been shown to partially correct specific abnormalities in the gut microbiota, modulating microbial composition [54]. Anti-gp210–positive patients tend to show slightly lower microbial species richness compared with negative cases, although not statistically significant [54]. This observation supports the notion that anti-gp210 antibody positivity may be associated with disease severity and progression [25]. Approximately 20% of anti-gp210–positive patients lose their seroreactivity under UDCA therapy [56,60,105]. Moreover, a reduction in anti-sp100 antibody titers, but not in anti-gp210 titers, was correlated with improvement of the Mayo risk score (p = 0.025) and with a favorable response to UDCA (p = 0.016) [106].
10. Conclusions
PBC is a chronic, progressive cholestatic liver disease characterized by autoimmune-mediated injury to the intrahepatic bile ducts. Without treatment, patients progress from cholestasis to fibrosis, ultimately developing cirrhosis and liver failure; however, the introduction of UDCA has markedly improved disease management and outcomes. Large-scale longitudinal data from Japan (2,579 cases since 1980) show that the mean age at diagnosis increased from 56.5 years before 2010 to 61.4 years after 2021, with the proportion of male patients rising from 12.4% to 20.6% [107]. These findings suggest shifting epidemiological features and raise concerns about delayed or missed early diagnosis, underscoring the need to reassess current diagnostic pathways.
Autoantibodies have been central to the diagnosis and management of PBC. AMA remains the most sensitive and specific serological marker, detectable years before clinical manifestations and therefore invaluable for early diagnosis [12]. Conversely, AMA-negative cases (5–10%) are at higher risk of delayed diagnosis and poorer outcomes [99]. Among ANA, anti-gp210 and anti-sp100 have emerged as highly specific and prognostically relevant biomarkers, with anti-gp210 strongly associated with cirrhosis, hepatic failure, and increased mortality [86]. Additional antibodies—including ACA, anti-RPL30, and anti-KLHL12—show associations with disease severity and complications, suggesting potential roles in patient stratification and precision medicine.
Despite these advances, several challenges remain. The heterogeneity of ANA patterns and the overlap with other autoimmune conditions (e.g., systemic sclerosis) complicate their interpretation and limit their specificity in clinical practice. Furthermore, the pathogenic versus marker role of ANA, including anti-gp210, remains unresolved, and their integration into routine prognostic algorithms has not yet been standardized across populations or laboratories. Subclass-specific AMA (such as IgG3-AMA) and ANA subtypes are beginning to show links with disease progression and treatment response [97], but their clinical utility as predictive biomarkers requires validation in large, prospective cohorts.
Future research should prioritize the development of standardized, high-throughput assays for PBC-specific ANA, systematic evaluation of antibody subclasses, and multi-marker panels that combine serology with genetic and microbiome data. Such approaches could refine prognostic stratification, improve therapeutic decision-making (including evaluation of UDCA and second-line agents), and accelerate the discovery of new immunological targets for therapy. Autoantibody-based strategies—particularly the next generation of ANA profiling—hold promise as pivotal tools for advancing personalized medicine, enabling earlier intervention, and ultimately improving long-term outcomes for patients with PBC.
Author Contributions
All the authors contributed to the accomplishment of the work. In particular, conceptualization, S.M. and A.M.; data curation, S.M.; writing—original draft preparation, S.M.; writing—review and editing K.O., R.Y., M.N., T.T., K.F., J.T. and M.T; supervision, A.M. and T.H.; project administration, H.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.:
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hirschfield, G.M.; Beuers, U.; Corpechot, C.; Invernizzi, P.; Jones, D.; Marzioni, M.; Schramm, C. EASL Clinical Practice Guidelines: The Diagnosis and Management of Patients with Primary Biliary Cholangitis. J Hepatol 2017, 67, 145–172. [Google Scholar] [CrossRef]
- Lv, T.; Chen, S.; Li, M.; Zhang, D.; Kong, Y.; Jia, J. Regional Variation and Temporal Trend of Primary Biliary Cholangitis Epidemiology: A Systematic Review and Meta-Analysis. Journal of Gastroenterology and Hepatology (Australia) 2021, 36, 1423–1434. [Google Scholar] [CrossRef]
- Lu, M.; Zhou, Y.; Haller, I. V.; Romanelli, R.J.; VanWormer, J.J.; Rodriguez, C. V.; Anderson, H.; Boscarino, J.A.; Schmidt, M.A.; Daida, Y.G.; et al. Increasing Prevalence of Primary Biliary Cholangitis and Reduced Mortality With Treatment. Clinical Gastroenterology and Hepatology 2018, 16, 1342–1350.e1. [Google Scholar] [CrossRef] [PubMed]
- Murillo Perez, C.F.; Goet, J.C.; Lammers, W.J.; Gulamhusein, A.; van Buuren, H.R.; Ponsioen, C.Y.; Carbone, M.; Mason, A.; Corpechot, C.; Invernizzi, P.; et al. Milder Disease Stage in Patients with Primary Biliary Cholangitis over a 44-Year Period: A Changing Natural History. Hepatology 2018, 67, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver EASL Clinical Practice Guidelines: Management of Cholestatic Liver Diseases. J Hepatol 2009, 51, 237–267. [CrossRef]
- Lindor, K.D.; Bowlus, C.L.; Boyer, J.; Levy, C.; Mayo, M. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2019, 69, 394–419. [Google Scholar] [CrossRef]
- Mackay, I.R. Primary Biliary Cirrhosis Showing a High Titer of Autoantibody; Report of a Case. N Engl J Med 1958, 258, 185–188. [Google Scholar] [CrossRef]
- Walker, J.G.; Doniach, D.; Roitt, I.M.; Sherlock, S. SEROLOGICAL TESTS IN DIAGNOSIS OF PRIMARY BILIARY CIRRHOSIS. The Lancet 1965, 285, 827–831. [Google Scholar] [CrossRef]
- Whyte, J.; Hough, D.; Maddison, P.J.; McHugh, N.J. The Association of Primary Biliary Cirrhosis and Systemic Sclerosis Is Not Accounted for by Cross Reactivity Between Mitochondrial and Centromere Antigens. J Autoimmun 1994, 7, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Vergani, D.; Alvarez, F.; Bianchi, F.B.; Cançado, E.L.R.; MacKay, I.R.; Manns, M.P.; Nishioka, M.; Penner, E. Liver Autoimmune Serology: A Consensus Statement from the Committee for Autoimmune Serology of the International Autoimmune Hepatitis Group. J Hepatol 2004, 41, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Liang, E.Y.; Liu, M.; Ke, P.F.; Han, G.; Zhang, C.; Deng, L.; Wang, Y.X.; Huang, H.; Huang, W.J.; Liu, R.P.; et al. A Population-Based Characterization Study of Anti-Mitochondrial M2 Antibodies and Its Consistency with Anti-Mitochondrial Antibodies. Lab Med 2023, 54, 618–625. [Google Scholar] [CrossRef]
- Abe, M.; Onji, M. Natural History of Primary Biliary Cirrhosis. Hepatology Research 2008, 38, 639–645. [Google Scholar] [CrossRef]
- Mitchison, H.C.; Bassendine, M.F.; Hendrick, A.; Bennett, M.K.; Bird, G.; Watson, A.J.; James, O.F.W. Positive Antimitochondrial Antibody but Normal Alkaline Phosphatase: Is This Primary Biliary Cirrhosis? Hepatology 1986, 6, 1279–1284. [Google Scholar] [CrossRef]
- Duan, W.; Chen, S.; Li, S.; Lv, T.; Li, B.; Wang, X.; Wang, Y.; Zhao, X.; Ma, H.; Ou, X.; et al. The Future Risk of Primary Biliary Cholangitis (PBC) Is Low among Patients with Incidental Anti-mitochondrial Antibodies but without Baseline PBC. Hepatol Commun 2022, 6, 3112. [Google Scholar] [CrossRef]
- Berg, P.A.; Klein, R. Mitochondrial Antigens and Autoantibodies: From Anti-M1 to Anti-M9. Klin Wochenschr 1986, 64, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.J.; Zhang, F.C.; Li, Y.Z.; Zhang, X. Primary Biliary Cirrhosis: What Do Autoantibodies Tell Us? World Journal of Gastroenterology : WJG 2010, 16, 3616. [Google Scholar] [CrossRef] [PubMed]
- Gershwin, M.E.; Ansari, A.A.; Mackay, I.R.; Nakanuma, Y.; Nishio, A.; Rowley, M.J.; Coppel, R.L. Primary Biliary Cirrhosis: An Orchestrated Immune Response against Epithelial Cells. Immunol Rev 2000, 174, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Reynoso-Paz, S.; Leung, P.S.C.; Van De Water, J.; Tanaka, A.; Munoz, S.; Bass, N.; Lindor, K.; Donald, P.J.; Coppel, R.L.; Ansari, A.A.; et al. Evidence for a Locally Driven Mucosal Response and the Presence of Mitochondrial Antigens in Saliva in Primary Biliary Cirrhosis. Hepatology 2000, 31, 24–29. [Google Scholar] [CrossRef]
- Lleo, A.; Maroni, L.; Glaser, S.; Alpini, G.; Marzioni, M. Role of Cholangiocytes in Primary Biliary Cirrhosis. Semin Liver Dis 2014, 34, 273. [Google Scholar] [CrossRef]
- Tanaka, A.; Leung, P.S.C.; Gershwin, M.E. Evolution of Our Understanding of PBC. Best Pract Res Clin Gastroenterol, 35. [CrossRef]
- Hirschfield, G.M.; Dyson, J.K.; Alexander, G.J.M.; Chapman, M.H.; Collier, J.; Hübscher, S.; Patanwala, I.; Pereira, S.P.; Thain, C.; Thorburn, D.; et al. The British Society of Gastroenterology/UK-PBC Primary Biliary Cholangitis Treatment and Management Guidelines. Gut 2018, 67, 1568. [Google Scholar] [CrossRef]
- Bogdanos, D.P.; Invernizzi, P.; Mackay, I.R.; Vergani, D. Autoimmune Liver Serology: Current Diagnostic and Clinical Challenges. World J Gastroenterol 2008, 14, 3374–3387. [Google Scholar] [CrossRef] [PubMed]
- ZHANG, L.; WEETMAN, A.P.; JAYNE, D.R.W.; TURNER, I.; YEAMAN, S.J.; BASSENDINE, M.F.; OLIVEIRA, D.B.G. Anti-mitochondrial Antibody IgG Subclass Distribution and Affinity in Primary Biliary Cirrhosis. Clin Exp Immunol 1992, 88, 56–61. [Google Scholar] [CrossRef]
- Dähnrich, C.; Pares, A.; Caballeria, L.; Rosemann, A.; Schlumberger, W.; Probst, C.; Mytilinaiou, M.; Bogdanos, D.; Vergani, D.; Stöcker, W.; et al. New ELISA for Detecting Primary Biliary Cirrhosis-Specific Antimitochondrial Antibodies. Clin Chem 2009, 55, 978–985. [Google Scholar] [CrossRef]
- Gabeta, S.; Norman, G.L.; Liaskos, C.; Papamichalis, P.A.; Zografos, T.; Garagounis, A.; Rigopoulou, E.I.; Dalekos, G.N. Diagnostic Relevance and Clinical Significance of the New Enhanced Performance M2 (MIT3) ELISA for the Detection of IgA and IgG Antimitochondrial Antibodies in Primary Biliary Cirrhosis. J Clin Immunol 2007, 27, 378–387. [Google Scholar] [CrossRef]
- Kadokawa, Y.; Omagari, K.; Hazama, H.; Ohba, K.; Masuda, J.I.; Kinoshita, H.; Hayashida, K.; Isomoto, H.; Mizuta, Y.; Murase, K.; et al. Evaluation of Newly Developed ELISA Using “MESACUP-2 Test Mitochondrial M2” Kit for the Diagnosis of Primary Biliary Cirrhosis. Clin Biochem 2003, 36, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Bogdanos, D.P.; Komorowski, L. Disease-Specific Autoantibodies in Primary Biliary Cirrhosis. Clinica Chimica Acta 2011, 412, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Moteki, S.; Leung, P.S.C.; Coppel, R.L.; Dickson, E.R.; Kaplan, M.M.; Munoz, S.; Gershwin, M.E. Use of a Designer Triple Expression Hybrid Clone for Three Different Lipoyl Domains for the Detection of Antimitochondrial Autoantibodies. Hepatology 1996, 24, 97–103. [Google Scholar] [CrossRef]
- Muratori, P.; Muratori, L.; Gershwin, M.E.; Czaja, A.J.; Pappas, G.; Maccariello, S.; Granito, A.; Cassani, F.; Loria, P.; Lenzi, M.; et al. “True” Antimitochondrial Antibody-Negative Primary Biliary Cirrhosis, Low Sensitivity of the Routine Assays, or Both? Clin Exp Immunol 2004, 135, 154–158. [Google Scholar] [CrossRef]
- Oertelt, S.; Rieger, R.; Selmi, C.; Invernizzi, P.; Ansari, A.A.; Coppel, R.L.; Podda, M.; Leung, P.S.C.; Gershwin, M.E. A Sensitive Bead Assay for Antimitochondrial Antibodies: Chipping Away at AMA-Negative Primary Biliary Cirrhosis. Hepatology 2007, 45, 659–665. [Google Scholar] [CrossRef]
- Satoh, M.; Chan, E.K.L.; Sobel, E.S.; Kimpel, D.L.; Yamasaki, Y.; Narain, S.; Mansoor, R.; Reeves, W.H. Clinical Implication of Autoantibodies in Patients with Systemic Rheumatic Diseases. Expert Rev Clin Immunol 2007, 3, 721–738. [Google Scholar] [CrossRef]
- Chan, E.K.L.; Damoiseaux, J.; Carballo, O.G.; Conrad, K.; de Melo Cruvinel, W.; Francescantonio, P.L.C.; Fritzler, M.J.; Garcia-De La Torre, I.; Herold, M.; Mimori, T.; et al. Report of the First International Consensus on Standardized Nomenclature of Antinuclear Antibody HEp-2 Cell Patterns (ICAP) 2014-2015. Front Immunol 2015, 6. [Google Scholar] [CrossRef]
- Zeng, X.; Lv, T.; Li, S.; Chen, S.; Li, B.; Lu, Z.; Wang, Y.; Ou, X.; Zhao, X.; You, H.; et al. Patients with AMA/Anti-Sp100/Anti-Gp210 Positivity and Cholestasis Can Manifest Conditions Beyond Primary Biliary Cholangitis. J Clin Transl Hepatol 2025, 13, 200. [Google Scholar] [CrossRef]
- Rigopoulou, E.I.; Dalekos, G.N. Molecular Diagnostics of Primary Billary Cirrhosis. Expert Opin Med Diagn 2008, 2, 621–634. [Google Scholar] [CrossRef]
- Granito, A.; Muratori, P.; Quarneti, C.; Pappas, G.; Cicola, R.; Muratori, L. Antinuclear Antibodies as Ancillary Markers in Primary Biliary Cirrhosis. Expert Rev Mol Diagn 2012, 12, 65–74. [Google Scholar] [CrossRef]
- Invernizzi, P.; Selmi, C.; Ranftler, C.; Podda, M.; Wesierska-Gadek, J. Antinuclear Antibodies in Primary Biliary Cirrhosis. Semin Liver Dis 2005, 25, 298–310. [Google Scholar] [CrossRef]
- Rigopoulou, E.I.; Bogdanos, D.P. Role of Autoantibodies in the Clinical Management of Primary Biliary Cholangitis. World J Gastroenterol 2023, 29, 1795. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Wang, Q.; Liu, H.; Xu, B.; Liu, Y.; Zhao, J.; Sun, L.; Chen, D.; Huang, C.; Jin, R. Gastroesophageal Varices in Primary Biliary Cholangitis with Anti-Centromere Antibody Positivity: Early Onset? Open Life Sci 2024, 19, 20220979. [Google Scholar] [CrossRef] [PubMed]
- Favoino, E.; Grapsi, E.; Barbuti, G.; Liakouli, V.; Ruscitti, P.; Foti, C.; Giacomelli, R.; Perosa, F. Systemic Sclerosis and Primary Biliary Cholangitis Share an Antibody Population with Identical Specificity. Clin Exp Immunol 2023, 212, 32. [Google Scholar] [CrossRef]
- Hirschfield, G.M.; Heathcote, E.J. Antimitochondrial Antibody-Negative Primary Biliary Cirrhosis. Clin Liver Dis 2008, 12, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.; Habior, A. Detection of Autoantibodies Against Nucleoporin P62 in Sera of Patients With Primary Biliary Cholangitis. Ann Lab Med 2019, 39, 291. [Google Scholar] [CrossRef]
- Bauer, A.; Habior, A.; Gawel, D. Diagnostic and Clinical Value of Specific Autoantibodies against Kelch-like 12 Peptide and Nuclear Envelope Proteins in Patients with Primary Biliary Cholangitis. Biomedicines 2022, 10, 801. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.L.; Yang, C.Y.; Ostendorff, H.P.; Shums, Z.; Lim, M.J.; Wang, J.; Awad, A.; Hirschfield, G.M.; Milkiewicz, P.; Bloch, D.B.; et al. Anti-Kelch-like 12 and Anti-Hexokinase 1: Novel Autoantibodies in Primary Biliary Cirrhosis. Liver Int 2014, 35, 642. [Google Scholar] [CrossRef]
- Jin, L.; Pahuja, K.B.; Wickliffe, K.E.; Gorur, A.; Baumgärtel, C.; Schekman, R.; Rape, M. Ubiquitin-Dependent Regulation of COPII Coat Size and Function. Nature 2012, 482, 495–500. [Google Scholar] [CrossRef]
- Rondou, P.; Haegeman, G.; Vanhoenacker, P.; Van Craenenbroeck, K. BTB Protein KLHL12 Targets the Dopamine D4 Receptor for Ubiquitination by a Cul3-Based E3 Ligase. Journal of Biological Chemistry 2008, 283, 11083–11096. [Google Scholar] [CrossRef]
- Gupta, V.A.; Beggs, A.H. Kelch Proteins: Emerging Roles in Skeletal Muscle Development and Diseases. Skelet Muscle 2014, 4. [Google Scholar] [CrossRef]
- Hu, C.J.; Song, G.; Huang, W.; Liu, G.Z.; Deng, C.W.; Zeng, H.P.; Wang, L.; Zhang, F.C.; Zhang, X.; Jeong, J.S.; et al. Identification of New Autoantigens for Primary Biliary Cirrhosis Using Human Proteome Microarrays. Molecular and Cellular Proteomics 2012, 11, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.Y.; Huang, Z.X.; Wang, Y.R.; Xie, L.K.; Lin, Y.P.; Liang, Y.; Liu, Z.Y.; Li, D.L.; Zhang, X.Y. Anti-RPL30 as a Novel Biomarker for Enhanced Diagnosis of Autoantibody-Negative Primary Biliary Cholangitis. World J Gastroenterol 2025, 31. [Google Scholar] [CrossRef]
- Saraiva, L.M.; Seixas da Silva, G.S.; Galina, A.; da-Silva, W.S.; Klein, W.L.; Ferreira, S.T.; de Felice, F.G. Amyloid-β Triggers the Release of Neuronal Hexokinase 1 from Mitochondria. PLoS One 2010, 5. [Google Scholar] [CrossRef]
- Robey, R.B.; Hay, N. Mitochondrial Hexokinases: Guardians of the Mitochondria. Cell Cycle 2005, 4, 654–658. [Google Scholar] [CrossRef]
- Syed, H.; Penner, T.; Mason, A.L. Linking Human Betaretrovirus with Autoimmunity and Liver Disease in Patients with Primary Biliary Cholangitis. Viruses 2022, 14, 1941. [Google Scholar] [CrossRef] [PubMed]
- Selmi, C.; Gershwin, M.E. Bacteria and Human Autoimmunity: The Case of Primary Biliary Cirrhosis. Curr Opin Rheumatol 2004, 16, 406–410. [Google Scholar] [CrossRef]
- Rashid, T.; Ebringer, A. Autoimmunity in Rheumatic Diseases Is Induced by Microbial Infections via Crossreactivity or Molecular Mimicry. Autoimmune Dis 2012, 1. [Google Scholar] [CrossRef]
- Tang, R.; Wei, Y.; Li, Y.; Chen, W.; Chen, H.; Wang, Q.; Yang, F.; Miao, Q.; Xiao, X.; Zhang, H.; et al. Gut Microbial Profile Is Altered in Primary Biliary Cholangitis and Partially Restored after UDCA Therapy. Gut 2018, 67, 534–541. [Google Scholar] [CrossRef]
- Stemerowicz, R.; Möller, B.; Rodloff, A.; Freudenberg, M.; Hopf, U.; Wittenbrink, C.; Reinhardt, R.; Galanos, C. ARE ANTIMITOCHONDRIAL ANTIBODIES IN PRIMARY BILIARY CIRRHOSIS INDUCED BY R(ROUGH)-MUTANTS OF ENTEROBACTERIACEAE? The Lancet 1988, 332, 1166–1170. [Google Scholar] [CrossRef]
- Nakamura, M.; Kondo, H.; Mori, T.; Komori, A.; Matsuyama, M.; Ito, M.; Takii, Y.; Koyabu, M.; Yokoyama, T.; Migita, K.; et al. Anti-Gp210 and Anti-Centromere Antibodies Are Different Risk Factors for the Progression of Primary Biliary Cirrhosis. Hepatology 2007, 45, 118–127. [Google Scholar] [CrossRef]
- Wang, J.J.; Yang, G.X.; Zhang, W.C.; Lu, L.; Tsuneyama, K.; Kronenberg, M.; Véla, J.L.; Lopez-Hoyos, M.; He, X.S.; Ridgway, W.M.; et al. Escherichia Coli Infection Induces Autoimmune Cholangitis and Anti-Mitochondrial Antibodies in Non-Obese Diabetic (NOD).B6 (Idd10/Idd18) Mice. Clin Exp Immunol 2014, 175, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Yang, Y.; Wang, Q.; Wang, Z.; Miao, Q.; Xiao, X.; Wei, Y.; Bian, Z.; Sheng, L.; Chen, X.; et al. The Risk Predictive Values of UK-PBC and GLOBE Scoring System in Chinese Patients with Primary Biliary Cholangitis: The Additional Effect of Anti-Gp210. Aliment Pharmacol Ther 2017, 45, 733–743. [Google Scholar] [CrossRef]
- Nickowitz, R.E.; Worman, H.J. Autoantibodies from Patients with Primary Biliary Cirrhosis Recognize a Restricted Region within the Cytoplasmic Tail of Nuclear Pore Membrane Glycoprotein Gp210. J Exp Med 1993, 178, 2237–2242. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Qin, Z.; Zhang, M.; Dai, Y.; Zhang, L.; Tian, W.; Gong, Y.; Chen, S.; Yang, C.; Xu, P.; et al. Autoantibodes to GP210 Are a Metric for UDCA Responses in Primary Biliary Cholangitis. J Transl Autoimmun 2024, 8, 100239. [Google Scholar] [CrossRef]
- Kaplan, M.M.; Gershwin, M.E. Primary Biliary Cirrhosis. N Engl J Med 2005, 353, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Ohfuji, S.; Abe, M.; Komori, A.; Takahashi, A.; Fujii, H.; Kawata, K.; Noritake, H.; Tadokoro, T.; Honda, A.; et al. Environmental Factors, Medical and Family History, and Comorbidities Associated with Primary Biliary Cholangitis in Japan: A Multicenter Case–Control Study. J Gastroenterol 2022, 57, 19–29. [Google Scholar] [CrossRef]
- Selmi, C.; Balkwill, D.L.; Invernizzi, P.; Ansari, A.A.; Coppel, R.L.; Podda, M.; Leung, P.S.; Kenny, T.P.; Van De Water, J.; Nantz, M.H.; et al. Patients With Primary Biliary Cirrhosis React Against a Ubiquitous Xenobiotic-Metabolizing Bacterium. Hepatology 2003, 38, 1250–1257. [Google Scholar] [CrossRef]
- Long, S.A.; Quan, C.; Van de Water, J.; Nantz, M.H.; Kurth, M.J.; Barsky, D.; Colvin, M.E.; Lam, K.S.; Coppel, R.L.; Ansari, A.; et al. Immunoreactivity of Organic Mimeotopes of the E2 Component of Pyruvate Dehydrogenase: Connecting Xenobiotics with Primary Biliary Cirrhosis. The Journal of Immunology 2001, 167, 2956–2963. [Google Scholar] [CrossRef] [PubMed]
- Howel, D.; Fischbacher, C.M.; Bhopal, R.S.; Gray, J.; Metcalf, J. V.; James, O.F.W. An Exploratory Population-Based Case-Control Study of Primary Biliary Cirrhosis. Hepatology 2000, 31, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.I.; Ducker, S.J.; James, O.F.W. Case-Control Studies of Risk Factors for Primary Biliary Cirrhosis in Two United Kingdom Populations. Gut 2010, 59, 508–512. [Google Scholar] [CrossRef]
- Lazaridis, K.N.; Juran, B.D.; Boe, G.M.; Slusser, J.P.; De Andrade, M.; Homburger, H.A.; Ghosh, K.; Dickson, E.R.; Lindor, K.D.; Petersen, G.M. Increased Prevalence of Antimitochondrial Antibodies in First-Degree Relatives of Patients with Primary Biliary Cirrhosis. Hepatology 2007, 46, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.M.; Nelson, J.L. Microchimerism: An Investigative Frontier in Autoimmunity and Transplantation. JAMA 2004, 291, 1127–1131. [Google Scholar] [CrossRef]
- Zhao, Y.; Wei, S.; Chen, L.; Zhou, X.; Ma, X. Primary Biliary Cholangitis: Molecular Pathogenesis Perspectives and Therapeutic Potential of Natural Products. Front Immunol 2023, 14. [Google Scholar] [CrossRef]
- Assassi, S.; Fritzler, M.J.; Arnett, F.C.; Norman, G.L.; Shah, K.R.; Gourh, P.; Manek, N.; Perry, M.; Ganesh, D.; Rahbar, M.H.; et al. Primary Biliary Cirrhosis (PBC), PBC Autoantibodies, and Hepatic Parameter Abnormalities in a Large Population of Systemic Sclerosis Patients. J Rheumatol 2009, 36, 2250. [Google Scholar] [CrossRef]
- Akimoto, S.; Ishikawa, O.; Muro, Y.; Takagi, H.; Tamura, T.; Miyachi, Y. Clinical and Immunological Characterization of Patients with Systemic Sclerosis Overlapping Primary Biliary Cirrhosis: A Comparison with Patients with Systemic Sclerosis Alone. Journal of Dermatology 1999, 26, 18–22. [Google Scholar] [CrossRef]
- Kita, H.; Matsumura, S.; He, X.S.; Ansari, A.A.; Lian, Z.X.; Van de Water, J.; Coppel, R.L.; Kaplan, M.M.; Gershwin, M.E. Analysis of TCR Antagonism and Molecular Mimicry of an HLA-A*0201-Restricted CTL Epitope in Primary Biliary Cirrhosis. Hepatology 2002, 36, 918–926. [Google Scholar] [CrossRef]
- Cavazzana, I.; Ceribelli, A.; Taraborelli, M.; Fredi, M.; Norman, G.; Tincani, A.; Satoh, M.; Franceschini, F. Primary Biliary Cirrhosis-Related Autoantibodies in a Large Cohort of Italian Patients with Systemic Sclerosis. Journal of Rheumatology 2011, 38, 2180–2185. [Google Scholar] [CrossRef]
- Kumagi, T.; Heathcote, E.J. Primary Biliary Cirrhosis. Orphanet J Rare Dis 2008, 3. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Nezu, S.; Uegaki, S.; Mikami, M.; Okuyama, S.; Kawamura, N.; Aiso, M.; Gershwin, M.E.; Takahashi, S.I.; Selmi, C.; et al. The Clinical Significance of IgA Antimitochondrial Antibodies in Sera and Saliva in Primary Biliary Cirrhosis. Ann N Y Acad Sci 2007, 1107, 259–270. [Google Scholar] [CrossRef]
- Matsumura, S.; Van De Water, J.; Leung, P.; Odin, J.A.; Yamamoto, K.; Gores, G.J.; Mostov, K.; Ansari, A.A.; Coppel, R.L.; Shiratori, Y.; et al. Caspase Induction by IgA Antimitochondrial Antibody: IgA-Mediated Biliary Injury in Primary Biliary Cirrhosis. Hepatology 2004, 39, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Joplin, R.; Wallace, L.L.; Johnson, G.D.; Lindsay, J.G.; Yeaman, S.J.; Palmer, J.M.; Strain, A.J.; Neuberger, J.M. Subcellular Localization of Pyruvate Dehydrogenase Dihydrolipoamide Acetyltransferase in Human Intrahepatic Biliary Epithelial Cells. J Pathol 1995, 176, 381–390. [Google Scholar] [CrossRef]
- Rong, G.; Zhong, R.; Lleo, A.; Leung, P.S.C.; Bowlus, C.L.; Yang, G.-X.; Yang, C.-Y.; Coppel, R.L.; Ansari, A.A.; Cuebas, D.A.; et al. AUTOIMMUNE, CHOLESTATIC AND BILIARY DISEASE Epithelial Cell Specificity and Apotope Recognition by Serum Autoantibodies in Primary Biliary Cirrhosis. 2011. [Google Scholar] [CrossRef]
- Odin, J.A.; Huebert, R.C.; Casciola-Rosen, L.; LaRusso, N.F.; Rosen, A. Bcl-2-Dependent Oxidation of Pyruvate Dehydrogenase-E2, a Primary Biliary Cirrhosis Autoantigen, during Apoptosis. J Clin Invest 2001, 108, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Allina, J.; Stanca, C.M.; Garber, J.; Hu, B.; Sautes-Fridman, C.; Bach, N.; Odin, J.A. Anti-CD16 Autoantibodies and Delayed Phagocytosis of Apoptotic Cells in Primary Biliary Cirrhosis. J Autoimmun 2008, 30, 238–245. [Google Scholar] [CrossRef]
- Berg, C.P.; Stein, G.M.; Keppeler, H.; Gregor, M.; Wesselborg, S.; Lauber, K. Apoptosis-Associated Antigens Recognized by Autoantibodies in Patients with the Autoimmune Liver Disease Primary Biliary Cirrhosis. Apoptosis 2008, 13, 63–75. [Google Scholar] [CrossRef]
- Shimoda, S.; Miyakawa, H.; Nakamura, M.; Ishibashi, H.; Kikuchi, K.; Kita, H.; Niiro, H.; Arinobu, Y.; Ono, N.; Mackay, I.R.; et al. CD4 T-Cell Autoreactivity to the Mitochondrial Autoantigen PDC-E2 in AMA-Negative Primary Biliary Cirrhosis. J Autoimmun 2008, 31, 110–115. [Google Scholar] [CrossRef]
- Nakamura, M.; Takii, Y.; Ito, M.; Komori, A.; Yokoyama, T.; Shimizu-Yoshida, Y.; Koyabu, M.; Matsuyama, M.; Mori, T.; Kamihira, T.; et al. Increased Expression of Nuclear Envelope Gp210 Antigen in Small Bile Ducts in Primary Biliary Cirrhosis. J Autoimmun 2006, 26, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Miyakoshi, M.; Sato, Y.; Nakanuma, Y. Increased Expression of Mitochondrial Proteins Associated with Autophagy in Biliary Epithelial Lesions in Primary Biliary Cirrhosis. Liver International 2013, 33, 312–320. [Google Scholar] [CrossRef]
- Wesierska-Gadek, J.; Penner, E.; Battezzati, P.M.; Selmi, C.; Zuin, M.; Hitchman, E.; Worman, H.J.; Gershwin, M.E.; Podda, M.; Invernizzi, P. Correlation of Initial Autoantibody Profile and Clinical Outcome in Primary Biliary Cirrhosis. Hepatology 2006, 43, 1135–1144. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; Ren, L.; Li, Y.; Xu, T.; Li, W.; Gao, W.; Sun, G.; Liu, M. Clinical Performance of AMA-M2, Anti-gp210 and Anti-sp100 Antibody Levels in Primary Biliary Cholangitis: When Detected by Multiplex Bead-based Flow Fluorescent Immunoassay. Immun Inflamm Dis 2024, 12, e1161. [Google Scholar] [CrossRef]
- Huang, C.; Han, W.; Wang, C.; Liu, Y.; Chen, Y.; Duan, Z. Early Prognostic Utility of Gp210 Antibody-Positive Rate in Primary Biliary Cholangitis: A Meta-Analysis. Dis Markers 2019, 2019. [Google Scholar] [CrossRef]
- Haldar, D.; Janmohamed, A.; Plant, T.; Davidson, M.; Norman, H.; Russell, E.; Serevina, O.; Chung, K.; Qamar, K.; Gunson, B.; et al. Antibodies to Gp210 and Understanding Risk in Patients with Primary Biliary Cholangitis. Liver International 2021, 41, 535–544. [Google Scholar] [CrossRef]
- Nakamura, M.; Shimizu-Yoshida, Y.; Takii, Y.; Komori, A.; Yokoyama, T.; Ueki, T.; Daikoku, M.; Yano, K.; Matsumoto, T.; Migita, K.; et al. Antibody Titer to Gp210-C Terminal Peptide as a Clinical Parameter for Monitoring Primary Biliary Cirrhosis. J Hepatol 2005, 42, 386–392. [Google Scholar] [CrossRef]
- Muratori, P.; Muratori, L.; Ferrari, R.; Cassani, F.; Bianchi, G.; Lenzi, M.; Rodrigo, L.; Linares, A.; Fuentes, D.; Bianchi, F.B. Characterization and Clinical Impact of Antinuclear Antibodies in Primary Biliary Cirrhosis. Am J Gastroenterol 2003, 98, 431–437. [Google Scholar] [CrossRef]
- Muratori, P.; Muratori, L.; Cassani, F.; Terlizzi, P.; Lenzi, M.; Rodrigo, L.; Bianchi, F.B. Anti-Multiple Nuclear Dots (Anti-MND) and Anti-SP100 Antibodies in Hepatic and Rheumatological Disorders. Clin Exp Immunol 2002, 127, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Züchner, D.; Sternsdorf, T.; Szostecki, C.; Heathcote, E.J.; Cauch-Dudek, K.; Will, H. Prevalence, Kinetics, and Therapeutic Modulation of Autoantibodies against Sp100 and Promyelocytic Leukemia Protein in a Large Cohort of Patients with Primary Biliary Cirrhosis. Hepatology 1997, 26, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Himoto, T.; Yamamoto, S.; Morimoto, K.; Tada, S.; Mimura, S.; Fujita, K.; Tani, J.; Morishita, A.; Masaki, T. Clinical Impact of Antibodies to Sp100 on a Bacterial Infection in Patients with Primary Biliary Cholangitis. J Clin Lab Anal 2021, 35, e24040. [Google Scholar] [CrossRef]
- Van Norstrand, M.D.; Malinchoc, M.; Lindor, K.D.; Therneau, T.M.; Gershwin, M.E.; Leung, P.S.C.; Dickson, E.R.; Homburger, H.A. Quantitative Measurement of Autoantibodies to Recombinant Mitochondrial Antigens in Patients with Primary Biliary Cirrhosis: Relationship of Levels of Autoantibodies to Disease Progression. Hepatology 1997, 25, 6–11. [Google Scholar] [CrossRef]
- Kim, K.A.; Jeong, S.H. The Diagnosis and Treatment of Primary Biliary Cirrhosis. Korean J Hepatol 2011, 17, 173. [Google Scholar] [CrossRef]
- Leuschner, U. Primary Biliary Cirrhosis—Presentation and Diagnosis. Clin Liver Dis 2003, 7, 741–758. [Google Scholar] [CrossRef]
- Rigopoulou, E.I.; Davies, E.T.; Bogdanos, D.P.; Liaskos, C.; Mytilinaiou, M.; Koukoulis, G.K.; Dalekos, G.N.; Vergani, D. Antimitochondrial Antibodies of Immunoglobulin G3 Subclass Are Associated with a More Severe Disease Course in Primary Biliary Cirrhosis. Liver International 2007, 27, 1226–1231. [Google Scholar] [CrossRef]
- Invernizzi, P.; Crosignani, A.; Battezzati, P.M.; Covini, G.; De Valle, G.; Larchi, A.; Zuin, M.; Podda, M. Comparison of the Clinical Features and Clinical Course of Antimitochondrial Antibody-Positive and -Negative Primary Biliary Cirrhosis. Hepatology 1997, 25, 1090–1095. [Google Scholar] [CrossRef]
- Juliusson, G.; Imam, M.; Björnsson, E.S.; Talwalkar, J.A.; Lindor, K.D. Long-Term Outcomes in Antimitochondrial Antibody Negative Primary Biliary Cirrhosis. Scand J Gastroenterol 2016, 51, 745–752. [Google Scholar] [CrossRef]
- Tang, L.; Zhong, R.; He, X.; Wang, W.; Liu, J.; Zhu, Y.; Li, Y.; Hou, J. Evidence for the Association between IgG-Antimitochondrial Antibody and Biochemical Response to Ursodeoxycholic Acid Treatment in Primary Biliary Cholangitis. J Gastroenterol Hepatol 2017, 32, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Kisand, K.E.; Karvonen, A.L.; Vuoristo, M.; Färkkilä, M.; Lehtola, J.; Inkovaara, J.; Miettinen, T.; Krohn, K.; Uibo, R. Ursodeoxycholic Acid Treatment Lowers the Serum Level of Antibodies against Pyruvate Dehydrogenase and Influences Their Inhibitory Capacity for the Enzyme Complex in Patients with Primary Biliary Cirrhosis. J Mol Med 1996, 74, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Benson, G.D.; Kikuchi, K.; Miyakawa, H.; Tanaka, A.; Watnik, M.R.; Gershwin, M.E. Serial Analysis of Antimitochondrial Antibody in Patients with Primary Biliary Cirrhosis. Clin Dev Immunol 2004, 11, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Hsu, W.; Hosoya, N.; Moritoki, Y.; Kajiyama, Y.; Kawai, T.; Takai, A.; Hayami, E.; Selmi, C.; Gershwin, M.E.; et al. Ursodeoxycholic Acid Reduces CpG-Induced IgM Production in Patients with Primary Biliary Cirrhosis. Hepatology Research 2009, 39, 448–454. [Google Scholar] [CrossRef]
- Tana, M.M.; Shums, Z.; Milo, J.; Norman, G.L.; Leung, P.S.; Gershwin, M.E.; Noureddin, M.; Kleiner, D.E.; Zhao, X.; Heller, T.; et al. The Significance of Autoantibody Changes Over Time in Primary Biliary Cirrhosis. Am J Clin Pathol 2015, 144, 601–606. [Google Scholar] [CrossRef]
- Nakamura, M.; Kondo, H.; Tanaka, A.; Komori, A.; Ito, M.; Yamamoto, K.; Ohira, H.; Zeniya, M.; Hashimoto, E.; Honda, M.; et al. Autoantibody Status and Histological Variables Influence Biochemical Response to Treatment and Long-Term Outcomes in Japanese Patients with Primary Biliary Cirrhosis. Hepatol Res 2015, 45, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Gatselis, N.K.; Zachou, K.; Norman, G.L.; Gabeta, S.; Papamichalis, P.; Koukoulis, G.K.; Dalekos, G.N. Clinical Significance of the Fluctuation of Primary Biliary Cirrhosis-Related Autoantibodies during the Course of the Disease. Autoimmunity 2013, 46, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Kugiyama, Y.; Abe, M.; Namisaki, T.; Yoshiji, H.; Abe, K.; Ohira, H.; Shirahashi, R.; Yokoyama, K.; Fukunaga, A.; Kawata, K.; et al. Clinical Characteristics and Long-Term Prognosis of Primary Biliary Cholangitis in Japan: Results of the 2nd-Generation Nationwide Survey. Hepatol Res 2025. [CrossRef] [PubMed]
Figure 1.
Characteristic ANA Patterns in PBC.
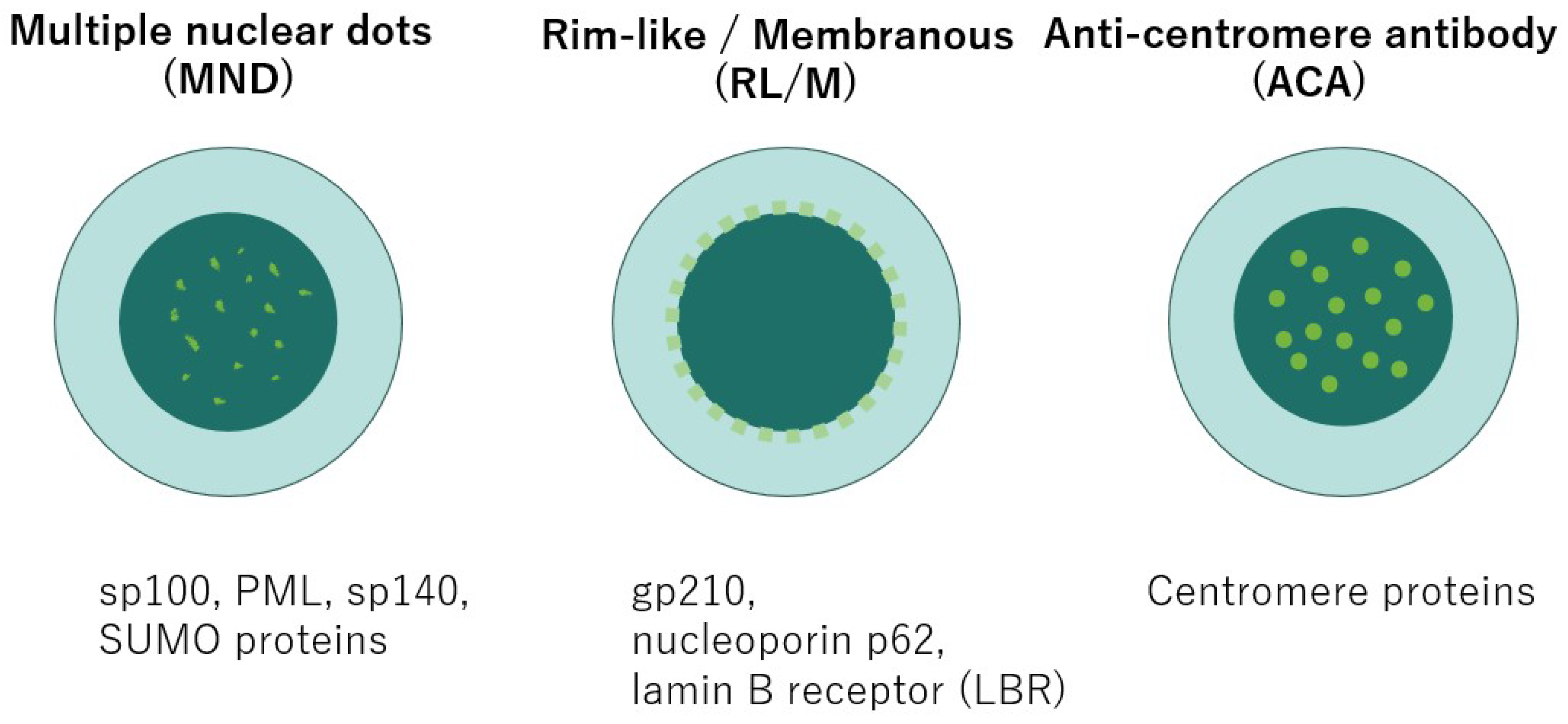
Figure 2.
Autoantibody Production and Autoimmune Activation in PBC.
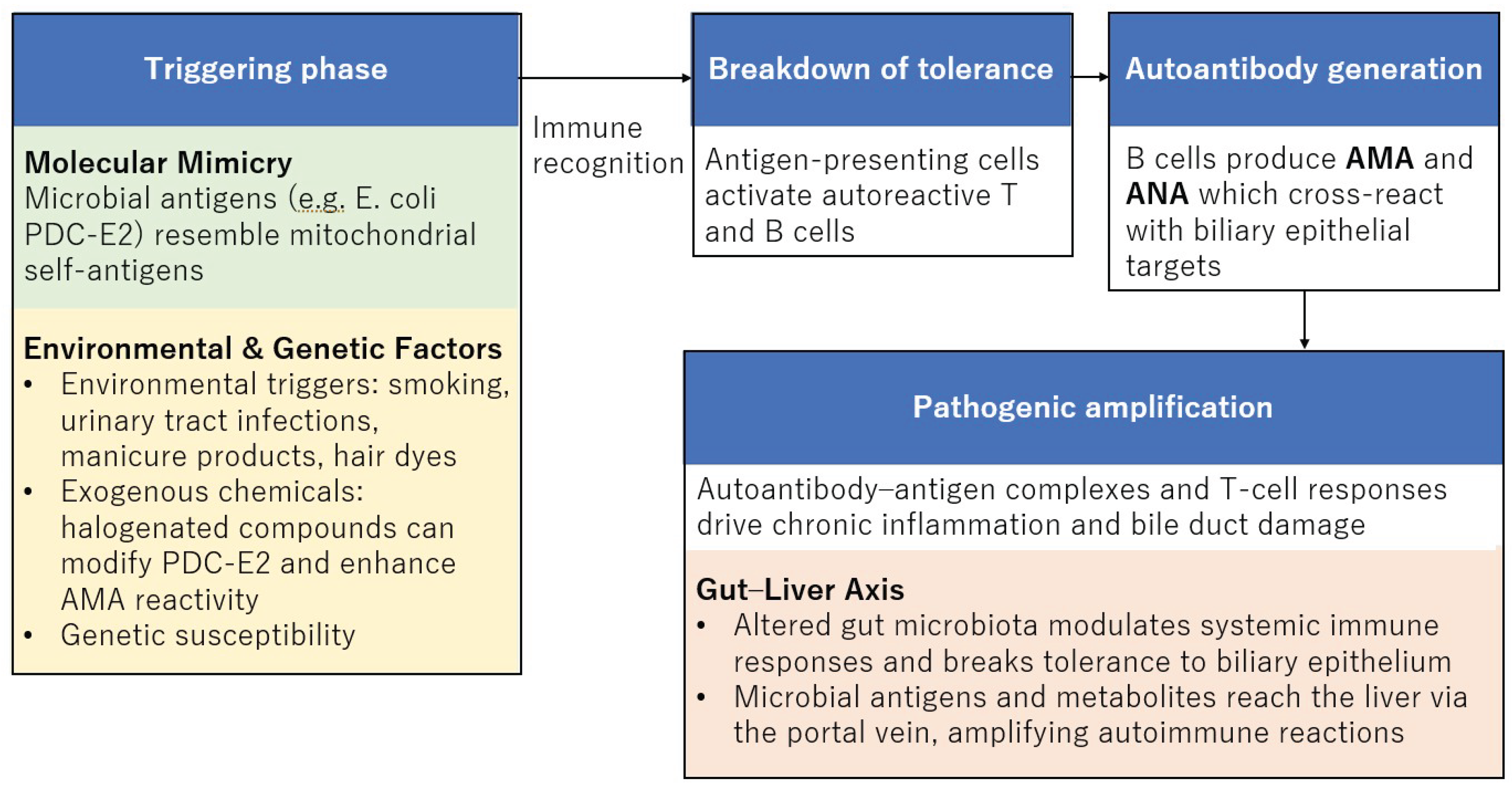

Table 1.
Autoantibodies in PBC and their associations with prognosis and disease progression.
| Autoantibody | Prevalence in PBC | Key prognostic / disease progression associations | References |
| AMA | 90-95% [1,9,10] | Diagnostic hallmark | [8] |
| Present years before symptoms/biochemical abnormalities | [12] | ||
| Titer not clearly predictive of prognosis | [94] | ||
| IgG3 AMA associated with advanced histology and higher cirrhosis frequency; correlates with Mayo risk score | [97] | ||
| Anti-gp210 (ANA, RL/M pattern) | 30-50% [28,29] | Strong predictor of poor prognosis: higher risk of cirrhosis, severe cholestasis, hepatic failure, and mortality | [85,86,87,88] |
| 20% of anti-gp210–positive patients lose their seroreactivity under UDCA therapy | [56,60,105] | ||
| Persistence of anti-gp210 or high gp210 expression in bile ducts associated with end-stage liver failure | [83,89] | ||
| Anti-sp100 (ANA, MND pattern) | 8.7-40.0% [90,91,92] |
No significant difference in the frequency of anti-sp100 was observed between AMA-positive and AMA-negative PBC patients | [90,91,92,93] |
| Anti-centromere antibody (ACA) | 10–30% [38] | Not PBC-specific; associated with Raynaud’s phenomenon, sicca symptoms, and overlap with systemic sclerosis | [38,39] |
| Correlated with improvement of the Mayo risk score (p = 0.025) and with a favorable response to UDCA | [106] | ||
| Anti-p62 (ANA, RL/M subtype) | detected infrequently [41] | Highly specific; useful in AMA-negative PBC; diagnostic adjunct; prognostic role not yet fully established | [41] |
| Anti-LBR (ANA) | 15% [41,42] | Highly specific for PBC; associated with liver fibrosis but not with overall survival | [41] |
| Anti-KLHL12 | 40% [43] | Associated with higher bilirubin, fibrosis; suggested as a risk factor for poor prognosis | [42,43] |
| Anti-RPL30 | Correlates with INR and MELD score; potential marker of disease severity | [33,48] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



