
Submitted:
25 October 2025
Posted:
28 October 2025
You are already at the latest version
Abstract
Safinamide is a reversible monoamine oxidase-B inhibitor approved as add-on to levodopa for the management of motor fluctuations in Parkinson’s disease (PD). Beyond dopaminergic modulation, it also inhibits abnormal glutamate release, a mechanism implicated in the pathophysiology of levodopa-induced dyskinesias (LID). Clinical evidence of this potential, however, remains scarce.A 65-year-old woman with a 7-year history of PD complicated by truncal LID and end-of-dose motor fluctuations underwent comprehensive baseline assessment. Hourly MDS-UPDRS-III and UDysRS-III–IV scores were collected over a 12-hour observation period during stable levodopa/benserazide (200/50 mg q4h) therapy. Safinamide was subsequently initiated at 100 mg/day, and the same protocol was repeated after three months. At baseline, motor scores improved two hours post-dose during each interval (mean MDS-UPDRS-III: 24.3) but were consistently accompanied by troublesome trunk dyskinesias (mean UDysRS-III: 16.3; UDysRS-IV: 13.5). At four hours post-dose, dyskinesias lessened (mean UDysRS-III: 7; UDysRS-IV: 8) while parkinsonism worsened (mean MDS-UPDRS-III: 33.6). After three months of safinamide, two-hour post-dose motor scores were maintained (mean: 21.6), four-hour scores improved (mean: 24), and dyskinesias resolved across all intervals (mean UDysRS-III: 2.3; UDysRS-IV: 0). These findings support safinamide’s role in motor fluctuation control and suggest that glutamatergic modulation may underlie a clinically relevant antidyskinetic effect.
Keywords:
Parkinson’s desease
; Wearing-off
; Dyskinesias
; Safinamide
; Glutamatergic-modulation
; Cortico-striatal-plasticity
1. Introduction
Safinamide 50 and 100 mg/day was recently approved for the treatment of mid- to late-stage fluctuating Parkinson’s disease (PD) as add-on therapy to a stable dose of levodopa alone or in combination with other PD medications [1]. Safinamide is an orally active aminoamide derivative that shows multiple dopaminergic and non-dopaminergic actions: reversible and highly selective monoamine oxidase B inhibition, glutamate release inhibition by blocks of voltage-dependent sodium channels and modulation of N-type calcium channels [2]. Safinamide significantly increases daily ON time without increasing the risk of developing troublesome levodopa-induced dyskinesias (LID) and significantly improves the activities of daily living and the quality of life [1]. Safinamide 100 mg demonstrates also a capacity to attenuate LID [3], likely through modulation of glutamatergic transmission; however, this effect remains still insufficiently explored and has not been adequately acknowledged. Herein, we report the effect of safinamide add-on to levodopa therapy on LID affecting the trunk in a mid-stage PD patient. Beyond clinical effects, contemporary reviews underscore safinamide’s dual mechanism—highly selective, reversible MAO-B inhibition plus suppression of presynaptic glutamate release via voltage-gated Na⁺ blockade and N-type Ca²⁺ channel modulation—providing a biologically plausible anti-LID rationale [4].
2. Case Report
A 65-year-old woman had a seven-year history of mild-stage PD complicated by LID and end-of-dose motor fluctuations. Family history was negative for neurological and psychiatric illness, and she was not taking neuroleptic drugs. The patient did not report previous medical history except from olfactory deficits. The onset of PD was dated to the age of 58, when the patient complained of rest tremor and loss of dexterity in the left upper limb. These symptoms improved in a clear and dramatic way following the initiation of levodopa treatment. Two years after PD onset the patient underwent neuropsychological assessment and routine serologic tests showed no abnormalities. Olfactory tests confirmed smell impairment. Brain 3T MRI was normal. Dopamine Transporter SPECT showed abnormal striatal uptake predominant in the right caudate and putamen; myocardial scintigraphy revealed no ¹²³metaiodobenzylguanidine (MIBG) uptake. After four years, the patient reported an end-of-dose deterioration of levodopa effect, characterized by the re-emergence of symptoms shortly before the next scheduled dose, which consistently resolved following medication intake (wearing-off) [5]. A few months later, the patient also developed involuntary and troublesome movements to the trunk more evident concomitantly with the period of maximal therapeutic benefit perceived by the patient. Based on the clinical features outlined above, and given the absence of red flags, the diagnosis of clinically established Parkinson's disease (PD) could be formulated [6]. Written informed consent was obtained from the patient for the publication of the case and videos in this article and all procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments, and approved by the local ethics committee. The effect of safinamide on LID control was evaluated through a comprehensive assessment performed at baseline and after three months of safinamide in add-on to levodopa treatment. One week before the baseline evaluation, the patient self-completed the WOQ-19 questionnaire [7] to evaluate the presence of motor and/or non-motor symptoms experienced during the day, and whether these symptoms improved after the next scheduled dose of levodopa (Table 1). On the baseline evaluation day, the patient arrived at 8 am in ‘practically defined’-OFF state, obtained by withholding all anti-parkinsonian medication after midnight the night before. Subsequently, she underwent baseline assessment using the Movement Disorder Society Unified Parkinson’s Disease Rating Scale part III and part IV (MDS-UPDRS-III–IV) and Unified Dyskinesia Rating Scale part III and part IV (UDysRS-III–IV) [8] prior to the first morning dose, corresponding to the initial administration of 200/50 mg levodopa/benserazide, administered every four hours, for a total of four daily doses. The scales were then repeated hourly until 20:00. Figure 1a depicts the 12-hour evolution of the evaluated scores. Before the initial morning dose, the patient demonstrated severe motor impairment in the absence of dyskinesias. After the first hour, a partial improvement in motor capabilities was observed, with no involuntary movements present. Two hours after the first morning levodopa dose, the patient showed further improvements in motor abilities, with evidence of non-rhythmic, choreiform, involuntary movements involving the trunk (Video—Part I). These observations are consistent with the hypothesis that peak-dose dyskinesias reflect excessive glutamatergic drive within cortico-striatal circuits. Pharmacological evidence supports the view that maladaptive plasticity and abnormal excitatory neurotransmission underlie truncal as well as appendicular LID, providing a plausible mechanistic substrate for therapeutic interventions targeting glutamate release [10,14,15]. After the fourth hour, a reduction in involuntary movements and a substantial decline in motor abilities were noted, which subsequently resolved following the administration of the next dose of levodopa. Throughout the remaining assessment period, scores remained generally stable, although a slight increase in motor blockade and a corresponding reduction in involuntary movements were noted during the afternoon hours. At the end of the baseline assessment, safinamide was prescribed at a dose of 50 mg/day for the first two weeks, followed by an increase to 100 mg/day starting from the beginning of the third week. All assessments were conducted by the same specialist in movement disorders. The patient also repeated the same evaluation the following day, and the results were superimposable. After the third month of 100 mg safinamide therapy, a week prior to the follow-up assessment, the patient re-self-completed the WOQ-19 scale which indicated improvements across multiple domains (Table 1). The same movement disorders specialist reassessed the patient following the initial pathway. Following the initial two hours of the follow-up evaluation, for each inter-dose period, MDS-UPDRS-III scores were comparable to baseline (MDS-UPDRS-III before the first morning dose: 40; mean two hours post-dose: 21.6), indicating motor improvement. In contrast, the scores recorded at the fourth hour of each inter-dose interval were lower than those observed at baseline (mean MDS-UPDRS-III: 24), establishing the complete resolution of wearing-off phenomenon (MDS-UPDRS-IV=0). It is also noteworthy that no dyskinesias were observed throughout the entire assessment (UDysRS-III=7; UDysRS-IV=0) (Video—Part I). Importantly, the disappearance of dyskinesias across all inter-dose intervals following safinamide introduction suggests not only symptomatic improvement but also a pharmacological effect coherent with its non-dopaminergic profile. Preclinical microdialysis studies have shown that safinamide suppresses abnormal glutamate outflow from hyperactive terminals [15], while clinical neurophysiology indicates normalization of cortical plasticity [13]. These converging findings reinforce the interpretation that the antidyskinetic benefit observed in our patient stems from modulation of glutamatergic neurotransmission in addition to MAO-B inhibition.
3. Discussion
Long-term treatment with levodopa is often complicated by the development of various types of motor response oscillations over the day, as well as LID [9]. Approximately 50% of patients with PD experience LID roughly after four-five years of levodopa treatment, with significant worsening of the quality of life [9]. Although LID typically appear in the extremities, trunk and head can also be involved [9]. The mechanisms responsible for the LID are still incompletely understood. However, LID are associated with changes in several neurochemical systems, including excessive glutamatergic transmission in the striatum [10]. This evidence is confirmed by the sustained antidyskinetic effect of amantadine, a drug with antagonist activity on NMDA glutamate receptors [11]. Recently, some authors have shown that safinamide induced an improvement of dyskinesia and prolonged levodopa antiparkinsonian effect in an animal model [12]. A post hoc analysis [3] of an 18-month extension of a randomized trial of safinamide add-on levodopa in PD with motor fluctuations demonstrated that safinamide significantly improved LID score in the subgroup of patients who maintained their levodopa dosage, suggesting that the antidyskinetic effect of safinamide was independent of the levodopa dose reduction. More recently [13], some authors demonstrated that both SICF (Short-interval intracortical facilitation) and M1 plasticity improved after long-term treatment with safinamide. The abnormality in SICF-related glutamatergic circuits plays a role in LID pathophysiology, and its long-term modulation may prevent LID worsening over time. Safinamide, when used as an adjunct to levodopa therapy, plays a pivotal role in the management of LID, likely through its modulatory effects on glutamatergic transmission, a mechanism that, despite its clinical relevance and the observed improvements in patients' quality of life, remains underexplored. This study seeks to further substantiate the established therapeutic effect of safinamide in mitigating end-of-dose motor fluctuations, while also providing preliminary evidence supporting its potential role in the modulation of dyskinesias. Further investigations in larger patient cohorts are necessary to establish a broader scientific consensus. Current pathophysiological syntheses highlight a glutamate-centered model of LID—maladaptive corticostriatal plasticity and abnormal firing within basal ganglia–motor cortex loops—which aligns with safinamide’s glutamatergic modulation [14,15].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Video—Part I. Before the introduction of 100 mg of safinamide. Evidence of levodopa-induced dyskinesias of the trunk in PD patient two hours after 200/50 mg of levodopa/ benserazide administration. Video—Part II. Three months after the introduction of 100 mg of safinamide in add-on to levodopa. Disappearance of levodopa-induced dykinesias of the trunk in PD patient s after 200/50 mg of levodopa/ benserazide administration.
Author Contributions
Conceptualization, G.P., M.M.; methodology, G.P., A.G.; M.M.; software, B.V.; validation, M.M.; A.Q.; A.G.; formal analysis, G.P.; A.G.; M.M.; investigation, G.P.; resources : G.P.; B.V.; data curation, G.P.; B.V.; A.Q.; A.G.; M.M.; writing—original draft preparation, G.P.; M.M. ; writing—review and editing, G.P.; B.V.; A.Q.; A.G.; M.M.; visualization, G.P.; B.V.; M.M.; supervision, G.P.; B.V.; A.Q.; A.G.; M.M.; project administration, A.G.; M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29:229-237. [CrossRef]
- Schapira AH. Safinamide in the treatment of Parkinson’s disease. Expert Opin Pharmacother. 2010;11:2261-2268. [CrossRef]
- Cattaneo C, La Ferla R, Bonizzoni E, Sardina M. Long-term effects of safinamide on dyskinesia in mid- to late-stage Parkinson’s disease: a post-hoc analysis. J Parkinsons Dis. 2015;5:475-481. [CrossRef]
- Bette S, Mollenhauer B, Trenkwalder C. Safinamide in the management of patients with Parkinson’s disease. Ther Adv Neurol Disord. 2018;11:1756286418789431. [CrossRef]
- Antonini A, Martinez-Martin P, Chaudhuri RK, et al. Wearing-off scales in Parkinson’s disease: critique and recommendations. Mov Disord. 2011;26(12):2169-2175. [CrossRef]
- Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30:1591-1601. [CrossRef]
- Abbruzzese G, Antonini A, Barone P, et al. Linguistic, psychometric validation and diagnostic ability assessment of an Italian version of a 19-item wearing-off questionnaire for wearing-off detection in Parkinson’s disease. Neurol Sci. 2012;33:1319-1327. [CrossRef]
- Christopher G, Glenn T, Theeuwes A, et al. Temporal stability of the Unified Dyskinesia Rating Scale. Mov Disord. 2011;26:—. [CrossRef]
- Schrag A, Quinn N. Dyskinesias and motor fluctuations in Parkinson's disease: a community-based study. Brain. 2000;123(Pt 11):2297-2305. [CrossRef]
- Calon F, Rajput AH, Hornykiewicz O, Bédard PJ, Di Paolo T. Levodopa-induced motor complications are associated with alterations of glutamate receptors in Parkinson’s disease. Neurobiol Dis. 2003;14:404-416. [CrossRef]
- Luginger E, Wenning GK, Bösch S, Poewe W. Beneficial effects of amantadine on L-dopa-induced dyskinesias in Parkinson’s disease. Mov Disord. 2000;15:873-878. [CrossRef]
- Grégoire L, Jourdain VA, Townsend M, Roach A, Di Paolo T. Safinamide reduces dyskinesias and prolongs L-DOPA antiparkinsonian effect in parkinsonian monkeys. Parkinsonism Relat Disord. 2013;19:508-514. [CrossRef]
- Guerra A, Asci F, Zampogna A, D’Onofrio V, Suppa A, Fabbrini G, Berardelli A. Long-term changes in short-interval intracortical facilitation modulate motor cortex plasticity and L-dopa-induced dyskinesia in Parkinson’s disease. Brain Stimul. 2022;15:99-108. [CrossRef]
- Kwon DK, Kim A, et al. Levodopa-Induced Dyskinesia in Parkinson’s Disease: mechanisms and management. Cells. 2022;11(23):3736. [CrossRef]
- Yang K, et al. Circuit mechanisms of L-DOPA-induced dyskinesia. Front Neurosci. 2021;15:614412. [CrossRef]
- Bhidayasiri R, et al. Sustained response in early responders to safinamide (post-hoc SETTLE). Front Neurol. 2023;14:1147008. [CrossRef]
- Nishikawa N, et al. Safinamide as adjunctive therapy to levodopa in older patients: motor, non-motor and quality-of-life outcomes. J Neurol Sci. 2024;451:123726. [CrossRef]
Figure 1.
The figure illustrates the trend of reference scale scores recorded during the 12-hour assessment at both baseline (1a) and follow-up (1b) evaluations; Abbreviations: MDS-UPDRS-III: Movement-disorder-society Unified Parkinson’s Disease Rating Scale-part III; UDysRS-III: Movement-disorder-society Unified Dyskinesia Rating Scale- part III; UDysRS-IV: Movement-disorder-society Unified Dyskinesia Rating Scale- part IV.
Figure 1.
The figure illustrates the trend of reference scale scores recorded during the 12-hour assessment at both baseline (1a) and follow-up (1b) evaluations; Abbreviations: MDS-UPDRS-III: Movement-disorder-society Unified Parkinson’s Disease Rating Scale-part III; UDysRS-III: Movement-disorder-society Unified Dyskinesia Rating Scale- part III; UDysRS-IV: Movement-disorder-society Unified Dyskinesia Rating Scale- part IV.
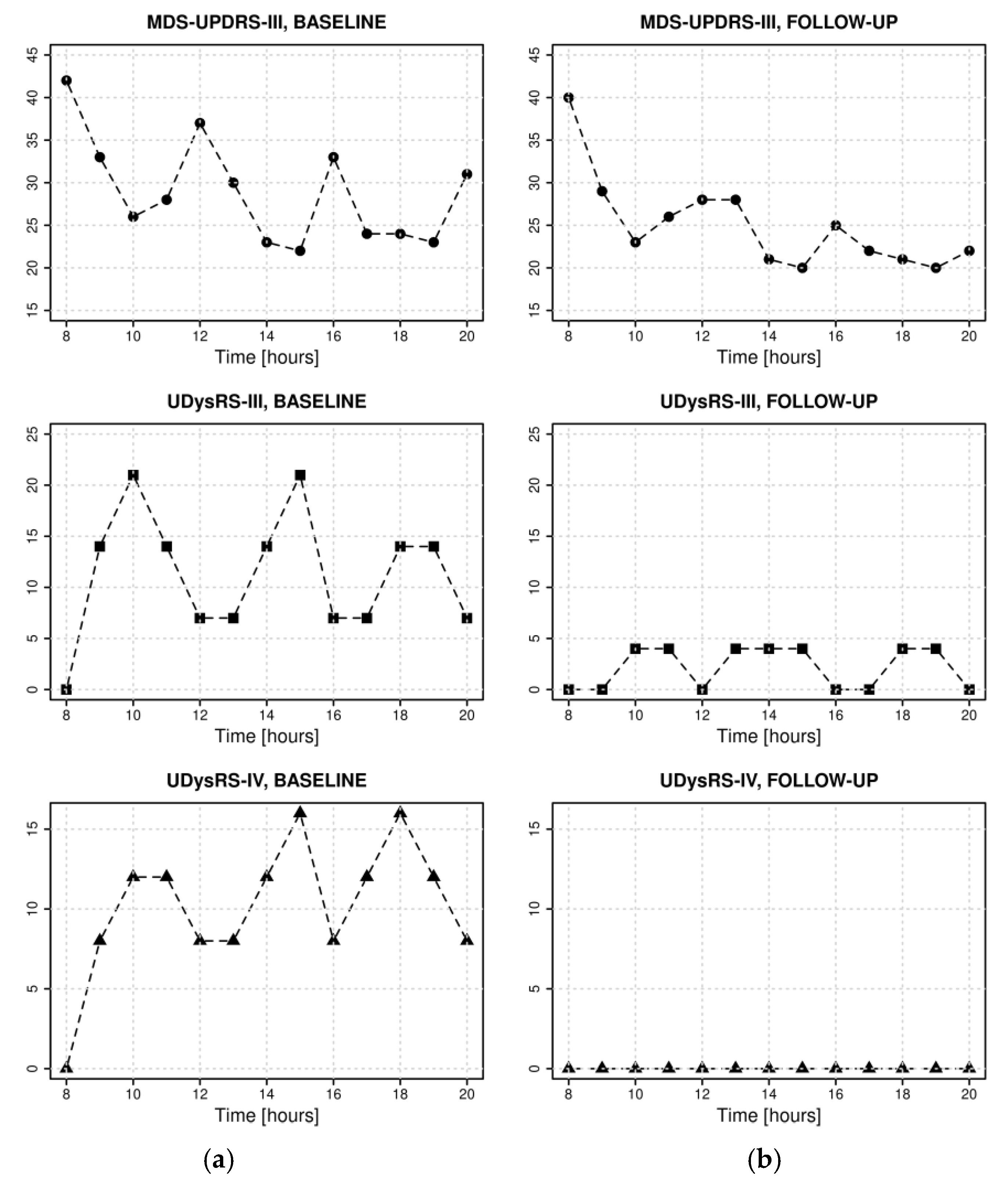

Table 1.
Wearing-off Questionnaire 19 (WOQ-19) domains experienced by the patient before and after 3 months of Safinamide treatment.
Table 1.
Wearing-off Questionnaire 19 (WOQ-19) domains experienced by the patient before and after 3 months of Safinamide treatment.
| Experience symptoms | Symptoms that improve after the next dose |
|||||
| WOQ-19 | Total score | Non-motor symptoms |
Motor symptoms | Total score | Non-motor symptoms |
Motor symptoms |
| Baseline | 11 | 6 | 5 | 8 | 5 | 3 |
| Follow-up | 6 | 3 | 3 | 3 | 2 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



