
Submitted:
28 May 2025
Posted:
28 May 2025
You are already at the latest version
Abstract
Background and objective: Safinamide improved non-motor symptoms (NMS) and quality of life
(QoL) in 50 PD patients who participated in the SAFINOMOTOR study. In this post hoc analysis we
analyzed the effect of safinamide on NMS and QoL according to sex, age, disease duration (DD)
and levodopa equivalent daily dose (LEDD).
Patients and Methods: The change from baseline to the end of the observational period (6 months)
in the Non-Motor Symptoms Scale (NMSS) and the 39-item Parkinson’s Disease Quality of Life
Questionnaire (PDQ-39) was analyzed in subgroups according to sex (male vs. female), age (> 75
vs. ≤ 75 years old), DD (> 10 years vs. ≤ 10 years) and LEDD (> 1000 vs. ≤ 1000 mg). Nonparametric
tests and general linear model (GLM) repeated measures were applied.
Results: Forty-four PD patients completed the V6M visit and were valid for the analysis. A significant
reduction in the NMSS was observed in all groups. Regarding QoL, a significant reduction in the
PDQ-39 was observed in females (p< 0.0001) and in patients with a DD > 10 years (p=0.011) but not
in males or those > 75 years old or receiving a LEDD > 1.000 mg. In the GLM, only LEDD at baseline
influenced the degree of change in the NMSS total score (p=0.026; F=5.23). The decrease in the
NMSS total scale was 43.8% for the group with a LEDD > 1.000 mg/day vs 33.7% for those ≤ 1.000
mg. None of the variables influenced the change in the PDQ39.
Conclusion: Safinamide improved NMS independently of sex, age, DD and LEDD.
Keywords:
Effectiveness
; Non-Motor Symptoms
; Post hoc analysis
; Parkinson´s disease
; Quality of life
; Safinamide
1. Introduction
Parkinson's disease (PD) is the second most common neurodegenerative disorder, following Alzheimer's disease [1], and is characterized by the degenerative loss of dopaminergic neurons in the substantia nigra [2]. While it is primarily distinguished by motor symptoms, PD patients may also present a wide range of non-motor symptoms (NMS) such as depression, cognitive impairment, anxiety, sleep disorders, and pain [3,4], all of which can significantly reduce their quality of life (QoL) [5,6]. The primary treatment for PD is dopamine replacement therapy, with levodopa as the gold standard for managing motor symptoms [7]. However, prolonged use is associated with motor complications such as the "wearing-off" phenomenon and the development of dyskinesia. For this reason, as the disease progresses, the use of adjuvant therapies and other antiparkinsonian drugs becomes necessary to complement levodopa [8]. Although current therapies have successfully addressed the majority of motor features, NMS do not improve always with dopamine replacement, making their treatment a challenge. This therapeutic need has driven research into drugs that modulate the activity of neurotransmitter systems other than dopamine, with the goal of alleviating these symptoms in PD [9,10].
In this context, safinamide, an oral α-aminoamide derivative [11], has been shown to be an effective adjunct therapy option to levodopa [12]. It has been approved in various regions, including Europe, the United States, Asia, and Japan, for the treatment of motor fluctuations in PD [13,14]. Specifically, safinamide has demonstrated benefits for motor symptoms such as tremor, bradykinesia, rigidity, and gait [15,16]. The distinctive mechanism of action of safinamide affects dopaminergic pathways through selective and reversible inhibition of monoamine oxidase type B (MAO-B), and glutamatergic pathways through the blocking of sodium channels and modulation of calcium channels [17]. Beyond its effects on motor function, recent studies, have shown that safinamide also has a positive impact on NMS and QoL [18,19,20]. Specifically, we observed in the SAFINONMOTOR study a positive impact of safinamide on NMS and QoL in 50 PD patients who had a severe or very severe NMS burden after 6-month follow-up [21]. Moreover, Benefits were observed in mood, sleep, daytime sleepiness, as well as pain in other analysis from this study [22,23,24]. Despite these advances, important questions remain about the extent and mechanisms of safinamide´s action, particularly concerning its role in alleviating NMS [18]. Factors such as sex, age, disease duration (DD), and daily levodopa dose could influence its effectiveness, making it crucial to understand these interactions in order to optimize personalized treatment for the disease. However, to date, no specific studies have addressed the effect regarding all these variables.
Therefore, the objective of this post hoc analysis of the SAFINONMOTOR study was to evaluate the effect of safinamide on NMS burden and QoL with respect to sex, age, DD, and daily levodopa equivalent dose (LEDD) in PD patients, in order to provide further evidence of its clinical impact and potential applications in personalized treatment for PD.
2. Materials and Methods
SAFINONMOTOR (an open-label study of the effectiveness of SAFInamide on NON-MOTOR symptoms in Parkinson’s disease patients) is a prospective, observational (Phase IV), open-label, multicenter, single-nation (Spain), and follow-up study conducted in 5 centers from Spain [21]. Patients with PD according to the United Kingdom Parkinson's Disease Society Brain Bank criteria [25] without dementia [26] who were considered for treating with safinamide by the neurologist having a NMSS total score ≥ 40 were included. Methods about SAFINONMOTOR are available in: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7999475/ [21].
The study included 4 scheduled visits: V0 (baseline; before starting safinamide); V1M (1 month ± 7 days); V3M (3 months ± 15 days); V6M (6 months ± 15 days, end of the observation period). With the aim to assess NMS and PD-related QoL, patients completed the Non-Motor Symptoms Scale (NMSS) [27] and the 39-item Parkinson’s disease Questionnaire (PDQ-39) [28], respectively, in all visits. The NMSS includes 30 items, each with a different non-motor symptom. The symptoms refer to the 4 weeks prior to assessment. The total score for each item is the result of multiplying the frequency (0, never; 1, rarely; 2, often; 3, frequent; 4, very often) x severity (1, mild; 2, moderate; 3, severe) and will vary from 0 to 12 points. The scale score ranges from 0 to 360 points (NMSS total score). The items are grouped into 9 different domains: 1) Cardiovascular (items 1 and 2; score, 0 to 24); 2) Sleep/fatigue (items 3, 4, 5 and 6; score, 0 to 48); 3) Depression/apathy (items 7, 8, 9, 10, 11 and 12; score, 0 to 72); 4) Perceptual problems/hallucinations (items 13, 14 and 15; score, 0 to 36); 5) Attention/memory (items 16, 17 and 18; score, 0 to 36); 6) Gastrointestinal tract (items 19, 20 and 21; score 0 to 36); 7) Urinary symptoms (items 22, 23 and 24; score, 0 to 36); 8) Sexual dysfunction (items 25 and 26; score 0 to 24); 9) Miscellaneous (items 27, 28, 29 and 30; score, 0 to 48). The PDQ-39 is a PD-specific questionnaire that assesses the patients’ QoL. There are 39 items grouped into 8 domains: (1) Mobility (items 1 to 10); (2) Activities of daily living (items 11 to 16); (3) Emotional well-being (items 17 to 22); (4) Stigma (items 23 to 26); (5) Social support (items 27 to 29); (6) Cognition (items 30 to 33); (7) Communication (items 34 to 36); (8) Pain and discomfort (items 37 to 39). For each item, the score may range from 0 (never) to 4 (always). The symptoms refer to the 4 weeks prior to assessment. Sociodemographic data, PD-related factors, comorbidities, and treatments were also collected. Moreover, other scales were administered by protocol in different visits of the study.
In relation to the purpose of this analysis, subgroups were defined according to sex (male vs. female), age (>75 vs. ≤75 years), disease duration (DD) (>10 vs. ≤10 years), and LEDD (>1000 vs. ≤1000 mg). The cut-off points established for the 3 groups with numerical variable were based on the literature and the possible implications from the point of view of daily clinical practice [29,30,31].
Safinamide was administered as a 50 mg tablet once daily for one month and increased to 100 mg/day at V2. In some cases (e.g., dyskinesia), the 100 mg dose could be introduced earlier, or the dose could be maintained at 50 mg/day based on the neurologist's judgment. No medication other than safinamide could be modified (schedule, dosage, etc.) during the follow-up unless deemed absolutely necessary by the neurologist. All changes were recorded, including medications related to Parkinson’s disease and non-related medications, as well as the LEDD [32].
The safety dataset included all subjects who initiated the study device. Safety analyses were assessed by adverse events (AEs). All AEs were coded using the current version of the Medical Dictionary for Regulatory Activities (MedDRA). The number and percentage of subjects with treatment-emergent AEs were provided according to the MedDRA system organ class and preferred term, classified by severity and relationship to the study treatment as evaluated by the investigator for all subjects.
Data Analysis
Data were analyzed using SPSS version 20.0 for Windows. Continuous variables were expressed as mean ± standard deviation (SD) or median and quartiles, depending on data distribution. Normality was checked using the Kolmogorov-Smirnov test for a single sample.
Only patients who completed the final visit at 6 months (V6M) were valid for this post hoc analysis. Each domain of the NMSS and PDQ-39 was expressed as a percentage: (score/total score) × 100. A Wilcoxon rank-sum test was performed to assess the change in the total score and in each domain score of the NMSS and PDQ-39 from baseline visit (V0) to the end of the observation period at six months (V6M) in each previously defined subgroup: males; females; ≤ 75 years old; > 75 years old; ≤ 10 years of DD; > 10 years of DD; ≤ 1000 mg of LEDD; > 1000 mg of LEDD. Cohen’s d formula was applied for measuring the effect size, which was considered to be absent, <0.2; small, 0.2–<0.5; moderate, 0.5–<0.8; large, 0.8–1.3; or very large, ≥1.3. Additionally, a general linear model for repeated measures (GLM) was used to analyze the impact of the variable under study (i.e., sex, age, DD, and LEDD) on the change experimented by the patients in the total score of the NMSS and PDQ-39 from V0 to V6M. Differences in the score of the NMSS and PDQ-39 between patients from a different subgroup according to the same variable (i.e., male vs. female, etc.) at V0 and V6M were analyzed using the Mann–Whitney U test. The frequency of patients with any adverse event was compared between subgroups using the Chi-squared test (all sample). Values of p < 0.05 were considered statistically significant.
Standard Protocol Approvals, Registrations, and Patient Consents
This study received approval from the Clinical Research Ethics Committee of Galicia (2018-052; 28/FEB/2019). Written informed consent was obtained from all participants prior to study initiation. SAFINONMOTOR was classified by the AEMPS (Spanish Agency for Medicines and Health Products) as a post-authorization prospective follow-up study with the code DSG-SAF-2018-01.
3. Results
Fifty PD patients were included in the SAFINONMOTOR study between May/2019 and February/2020 (age 68.5 ± 9.1 years; 58% females). Data about sociodemographic aspects, comorbidities, antiparkinsonian drugs, and other therapies have been previously published [21]. Forty-four PD patients (88%; age 69.1 ± 9.3 years; 54.5% females) completed the final visit (V6M) and were valid for this post hoc analysis.
A significant reduction in the NMSS total score was observed in all subgroups, including specifically patients > 75 years old (p=0.040), with a DD > 10 years (p=0.015), and those receiving a LEDD > 1000 mg (p=0.002) (Table 1 and Figure 1). By domains, a significant decrease in the score from V0 to V6M was detected in “Mood/apathy” and “Miscellaneous” in all subgroups (Table 2). At the other extreme, no significant change was found in “Cardiovascular”, “Perceptual symptoms” or “Sexual dysfunction” in any of the subgroups (Table 2). “Sleep/fatigue”, “Attention/memory”, and “Gastrointestinal symptoms” improved in males whereas “Urinary symptoms” in females (Table 2). Moreover, “Urinary symptoms” improved independently of age and LEDD (i.e., in both subgroups defined of the variable) (Table 2). Regarding QoL, a significant reduction in the PDQ-39 score was observed in females (p<0.0001) and in patients with a DD > 10 years (p=0.011) but not in males or those > 75 years old or receiving a LEDD > 1000 mg (Table 3 and Figure 2). By domains, “Emotional well-being” score decreased significantly in all defined subgroups except patients older than 75 years old (Table 4). Improvement in other domains was not detected in patients older than 75 years old, with a DD longer than years, or a LEDD higher than 1000 mg (Table 4). In the GLM, only LEDD at baseline influenced the degree of change in the NMSS total score from V0 to V6M (p=0.026; F=5.23), but the result was not significant (p>0.05) after adjustment to covariates (sex; age; disease duration). The decrease in the NMSS total score was 43.8% for the group with a LEDD > 1.000 mg/day vs 33.7% for those ≤ 1.000 mg. None of the variables influenced the change in the PDQ39.
As it has been previously published [21], a total of 21 adverse events in 16 patients (32%) were reported, 5 of which were severe (not related to safinamide). Dyskinesias and nausea were the most frequent (6%). The reasons for withdrawing from the study of the 6 patients were: 1 withdrawal of consent; 1 discontinuation of safinamide after deep brain stimulation procedure (it was recorded as SAE due to hospitalization process); 1 personal decision due to no effect and 3 due to an adverse event (2 dizziness; 1 respiratory infection). Only one patient discontinued due to an adverse event related to safinamide (dizziness). By groups, no differences were detected in the frequency of developing at least 1 AE: males 30% vs. females 20.8% (p=0.362); ≤ 75 years old 24.2% vs. > 75 years old 27.3% (p=0.565); DD ≤ 10 years 20.6% vs. DD > 10 years 40% (p=0.200); LEDD ≤ 1000 mg 16.7% vs. LEDD > 1000 mg 43.9% (p=0.070).
4. Discussion
In the previously published SAFINONMOTOR study [21], we observed improvement in NMS and QoL among patients with PD after six months of treatment with safinamide. In this post hoc analysis, we found that the significant improvement detected in the NMS burden was present across all groups, including in those patients with more clinically complex profiles, such as patients over 75 years old, those with a disease exceeding 10 years, and patients receiving a high LEDD (>1000 mg/day). As for QoL, gains were noted across the board but reached statistical significance particularly in women, patients no older than 75 years old, and those receiving a LEDD no higher than 1000 mg, regardless of disease duration (≤ 10 years or >10 years).
These findings align with previous research supporting the efficacy and/or effectiveness of safinamide in reducing the overall NMS burden [20,33,34,35]. Importantly, this is the first study to demonstrate a significant NMS improvement across diverse clinical profiles, regardless of sex, age, DD, or LEDD. These results highlight the potential of safinamide as an adjunct therapy for NMS across various patient subgroups and stages of progression. The observed benefit is particularly striking in individuals with more advanced conditions —those over 75 years old, with more than 10 years of disease progression, or requiring higher doses of levodopa— who experience a higher symptoms burden and poorer QoL. This subgroup is becoming increasingly common in routine clinical practice, further underscoring the clinical value of these results. In Japan, for instance, two-thirds of patients with PD treated with safinamide from the J-SILVER study [36] were over 75 years old, emphasizing the importance of having effective and well-tolerated treatments for this population. Safinamide improved motor and NMS and QoL in older patients with PD in the early stages of wearing-off in the mentioned J-SILVER study [36]. Data from other studies demonstrated the effectiveness of safinamide on motor and NMS in elderly and/or more advanced PD patients as well [12,37,38,39].
More specifically, a significant improvement has been consistently reported in domains such as mood, sleep, urinary symptoms, and pain [40,41,42]. Here, the strongest effect of safinamide was observed on mood and miscellaneous, which includes pain, that was detected in all groups independently of the sex, age, DD and LEDD. Previous studies have reported the differences in PD patients in their clinical profile according to sex [43], suggesting our findings that a different response to safinamide in some NMS could be expected. For example, we found a better response on urinary symptoms in females, something important but not analyzed in previous reports showing improvement in urinary symptoms as a whole [44,45]. Results from pivotal studies showed that safinamide has positive effects on both motor and non-motor functions [15,16,17] in patients with PD, with the same efficacy in both genders [46]. Regarding pain, one of the most common and limiting NMS in PD [47], the results of this study are particularly relevant. A significant improvement was observed in pain-related symptoms collected with the NMSS across all subgroups analyzed, independent of demographic or clinical characteristics such as sex, age, levodopa dose or disease duration, further underscoring the therapeutic potential of safinamide in this area. With prevalence estimates ranging from 30–50%—and up to 85% when accounting for all pain types [48] —its effective management remains a pressing clinical need. Alarmingly, despite its high prevalence and impact on QoL, nearly half of patients suffering from pain do not receive any analgesic intervention, a number that could rise to 3.7 million globally by 2030 [48]. This treatment gap stands in stark contrast with the growing evidence supporting the use of safinamide as an adjunctive strategy. Indeed, prior investigations, such as those by Geroin et al. [42], have reported significant improvements in the KPPS, BPI, and NRS scales after three months of treatment, while post hoc analyses [49] and systematic reviews with meta-analyses [50] have consistently supported its efficacy in relieving pain within the PD population. In this context, since majority of the patients of the SAFINONMOTOR study were receiving the dose of 100 mg per day at the end of the study, a influence of the safinamide on the glutamatergic pathways cannot be ruled out, as other authors have previously suggested [51,52].
Regarding QoL, safinamide has demonstrated beneficial effects on patients´ QoL [19,21,53,54]. Here, although the improvement was widespread, it was only significant in women, patients ≤75 years old, and those receiving ≤1000 mg of levodopa, regardless of how long patients had been living with the disease (≤10 years or >10 years). Notably, the improvement in QoL observed among women is especially meaningful, given their increased vulnerability and higher likelihood of experiencing depressive symptoms [23,55,56]. This subgroup exhibited a significant reduction in emotional well-being scores on the PDQ-39 scale. Pellecchia et al. [57] observed in a post hoc analysis of the XINDI study, greater improvements in females compared to males in socio-emotional domains like daily living, emotional well-being, and bodily discomfort in females. In contrast, we didn´t find significant reductions in men or in patients over 75 years old. This may reflect group-based differences in therapeutic response or QoL perception, though it could also stem from limited statistical power due to small sample sizes. A similar pattern was seen in patients receiving more than 1000 mg of LEDD, where improvements did not reach statistical significance. Nonetheless, previous studies, including that by Peña et al. [40], have highlighted safinamide’s positive effect on mood, with consistent gains in the PDQ-39 emotional well-being domain in both short- and long-term analyses [19], reinforcing its role as a valuable adjunctive treatment for NMS in PD.
The present study has some important limitations. First, the open-label design, which lacked a placebo group, introduces a potential risk of bias due to treatment expectancy. However, the observed improvements and their stability over time support the clinical relevance of the results. Second, the sample size was relatively small, particularly in certain subgroups, which may have limited the statistical power to detect significant differences. Third, the inclusion of patients with a severe or very severe NMS burden may reduce the generalizability of the results to all patients with PD. Fourth, the presence of antidepressant treatment in some participants, which could have influenced the interpretation of safinamide’s effects on mood. However, the favorable pharmacological profile of safinamide minimizes the risk of significant drug interactions. Finally, the COVID-19 pandemic impacted data collection, with 4 follow-up visits conducted via telephone. This shift in assessment method may have influenced subjective evaluations of mood and QoL.
Overall, our results demonstrate that safinamide treatment over six months significantly improved NMS in PD patients across all analyzed subgroups, irrespective of sex, age, disease duration, or levodopa dose, reinforcing its clinical utility as an adjunctive therapy in PD. Concerning QoL, an overall improvement was also observed after six months of treatment, with significant gains particularly in women, patients aged ≤75 years old, and those receiving a LEDD ≤1000 mg. These findings emphasize the importance of considering a patient's individual clinical profile when making therapeutic decisions and highlight safinamide’s value as an effective tool for enhancing the comprehensive management of PD. Further studies with larger sample sizes are needed to validate these results and explore more thoroughly how treatment response varies across demographic and clinical factors in order to optimize safinamide’s clinical use and maximize its therapeutic benefits for non-motor symptoms in PD patients.
Author Contributions
Solleiro Vidal A: statistical analysis; writing of the first draft of the manuscript; Yáñez Baña R: review and critique; recruitment and/or evaluation of participants; Labandeira Guerra C: review and critique; recruitment and/or evaluation of participants; Cimas Hernando MI: review and critique; recruitment and/or evaluation of participants; Cabo López I: review and critique; recruitment and/or evaluation of participants; Paz González JM: review and critique; recruitment and/or evaluation of participants; Alonso Losada MG: review and critique; recruitment and/or evaluation of participants; Santos García D: conception, organization, and execution of the project; statistical analysis; writing of the first draft of the manuscript; recruitment and/or evaluation of participants.
Funding
The present study is a study promoted by an independent clinical researcher (Diego Santos García). Zambon Spain has financed its expenses.
Institutional Review Board Statement
This study received approval from the Clinical Research Ethics Committee of Galicia (2018-052; 28/FEB/2019). Written informed consent was obtained from all participants prior to study initiation. SAFINONMOTOR was classified by the AEMPS (Spanish Agency for Medicines and Health Products) as a post-authorization prospective follow-up study with the code DSG-SAF-2018-01.
Informed Consent Statement
Written informed consent was obtained from all participants prior to study initiation.
Data Availability Statement
The protocol and statistical analysis plan are available upon request.
Acknowledgments
We would like to thank all Parkinson´s disease patients and their caregivers who collaborated in this study. Many thanks also to Zambon España and Fundación Degen.
Conflicts of Interest
The authors declare no conflict of interest.
Financial Disclosures
Solleiro Vidal A. has received payments for travel and accommodation for a training course by Stada. Yáñez Baña R. has received honoraria for educational presentations by Teva, Bial, and Zambon. Labandeira Guerra C. has received honoraria for educational presentations and advice service by Abbvie, Italfarmaco, Zambon, and Bial. Cimas Hernndo MI. has received honoraria for educational presentations and advice service by KRKA, Italfarmaco, Teva, Zambon, and Bial. Cabo López I. has received honoraria for educational presentations and advice service by Abbvie and Zambon and Bial. Paz González JM. has received honoraria for educational presentations and/or advice service by UCB Pharma, Lundbeck, KRKA, and Zambon. Alonso Losada MG. has received honoraria for educational presentations and advice service by Zambon and Bial. Santos-García D. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, Italfarmaco, Teva, Archímedes, Esteve, Stada, Merz, and grants from the “Fundación Professor Novoa Santos” as a result of the "CONVOCATORIA DE AYUDAS PARA LA REALIZACIÓN DE PROYECTOS DE INVESTIGACIÓN PARA GRUPOS EMERGENTES Y ASOCIADOS DEL INIBIC (2023/2024)".
Abbreviations
| AEs | adverse events |
| H&Y | Hoenh & Yahr |
| DD | disease duration |
| LEDD | levodopa equivalent daily dose |
| NMS | non-motor symptoms |
| NMSS | Non-Motor Symptoms Scale |
| PD | Parkinson´s disease |
| PDQ-39SI | 39-item Parkinson’s Disease Quality of Life Questionnaire Summary Index |
| QoL | quality of life |
References
- Willis AW, Roberts E, Beck JC, Fiske B, Ross W, Savica R, Van Den Eeden SK, Tanner CM, Marras C; Parkinson’s Foundation P4 Group. Incidence of Parkinson disease in North America. NPJ Parkinsons Dis 2022;8:170.
- Armstrong MJ, Okun MS. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA. 2020;323:548-60.
- Barone P, Antonini A, Colosimo C, et al.; PRIAMO study group. The PRIAMO study: A multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson's disease. Mov Disord 2009;24:1641-9.
- Martinez-Martin P, Rodriguez-Blazquez C, Kurtis MM, Chaudhuri KR; NMSS Validation Group. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson's disease. Mov Disord 2011;26:399-406.
- Santos García D, de Deus Fonticoba T, Suárez Castro E, et al.; Coppadis Study Group. Non-motor symptoms burden, mood, and gait problems are the most significant factors contributing to a poor quality of life in non-demented Parkinson's disease patients: Results from the COPPADIS Study Cohort. Parkinsonism Relat Disord 019;66:151-57.
- Santos-García D, de la Fuente-Fernández R. Impact of non-motor symptoms on health-related and perceived quality of life in Parkinson's disease. J Neurol Sci 2013;332:136-40.
- Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet 2021;397:2284-303.
- Fox SH, Katzenschlager R, Lim SY, et al.; Movement Disorder Society Evidence-Based Medicine Committee. International Parkinson and movement disorder society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson's disease. Mov Disord 2018;33:1248-66.
- Simuni T, Okun MS. Adjunctive Therapies in Parkinson Disease-Have We Made Meaningful Progress? JAMA Neurol 2022;79:119-20.
- Stocchi F, Vacca L, Radicati FG. How to optimize the treatment of early stage Parkinson's disease. Transl Neurodegener 2015;4:4.
- Fabbri M, Rosa MM, Abreu D, Ferreira JJ. Clinical pharmacology review of safinamide for the treatment of Parkinson's disease. Neurodegener Dis Manag 2015;5:481-96.
- Abbruzzese G, Kulisevsky J, Bergmans B, et al.; SYNAPSES Study Investigators Group. A European Observational Study to Evaluate the Safety and the Effectiveness of Safinamide in Routine Clinical Practice: The SYNAPSES Trial. J Parkinsons Dis 2022;12:473.
- Borgohain R, Szasz J, Stanzione P, et al.; Study 016 Investigators. Randomized trial of safinamide add-on to levodopa in Parkinson's disease with motor fluctuations. Mov Disord 2014;29:229-37.
- Borgohain R, Szasz J, Stanzione P, et al.; Study 018 Investigators. Two-year, randomized, controlled study of safinamide as add-on to levodopa in mid to late Parkinson's disease. Mov Disord 2014;29:1273-80.
- Stocchi F, Torti M. Adjuvant therapies for Parkinson's disease: critical evaluation of safinamide. Drug Des Devel Ther 2016;10:609-18.
- Espinoza-Vinces C, Villino-Rodríguez R, Atorrasagasti-Villar A, Martí-Andrés G, Luquin MR. Impact of Safinamide on Patient-Reported Outcomes in Parkinson's Disease. Patient Relat Outcome Meas 2023;14:285-95.
- Stocchi F, Antonini A, Berg D, et al. Safinamide in the treatment pathway of Parkinson's Disease: a European Delphi Consensus. NPJ Parkinsons Dis 2022;8:17.
- Blair HA, Dhillon S. Safinamide: A Review in Parkinson's Disease. CNS Drugs 2017;31:169-76.
- Cattaneo C, Jost WH, Bonizzoni E. Long-Term Efficacy of Safinamide on Symptoms Severity and Quality of Life in Fluctuating Parkinson's Disease Patients. J Parkinsons Dis 2020;10:89-97.
- Bianchi MLE, Riboldazzi G, Mauri M, Versino M. Efficacy of safinamide on non-motor symptoms in a cohort of patients affected by idiopathic Parkinson's disease. Neurol Sci 2019;40:275-9.
- Santos García D, Labandeira Guerra C, Yáñez Baña R, et al. Safinamide Improves Non-Motor Symptoms Burden in Parkinson's Disease: An Open-Label Prospective Study. Brain Sci 2021;11:316.
- Santos García D, Yáñez Baña R, Labandeira Guerra C, et al. Pain Improvement in Parkinson's Disease Patients Treated with Safinamide: Results from the SAFINONMOTOR Study. J Pers Med 2021;11:798.
- Labandeira CM, Alonso Losada MG, Yáñez Baña R, et al. Effectiveness of Safinamide over Mood in Parkinson's Disease Patients: Secondary Analysis of the Open-label Study SAFINONMOTOR. Adv Ther 2021;38(10):5398-5411.
- Santos García D, Cabo López I, Labandeira Guerra C, et al. Safinamide improves sleep and daytime sleepiness in Parkinson's disease: results from the SAFINONMOTOR study. Neurol Sci 2022;43:2537-2544.
- Daniel SE, Lees AJ. Parkinson's Disease Society Brain Bank, London: overview and research. J Neural Transm Suppl. 1993;39:165-72.
- Dubois B, Burn D, Goetz C, et al. Diagnostic procedures for Parkinson's disease dementia: recommendations from the movement disorder society task force. Mov Disord 2007;22:2314-24.
- Chaudhuri KR, Martinez-Martin P, Brown RG, et al. The metric properties of a novel non-motor symptoms scale for Parkinson's disease: Results from an international pilot study. Mov Disord 2007;22(13):1901-11.
- Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson's Disease Questionnaire (PDQ-39): development and validation of a Parkinson's disease summary index score. Age Ageing 1997;26(5):353-7.
- Virameteekul S, Phokaewvarangkul O, Bhidayasiri R. Profiling the most elderly parkinson's disease patients: Does age or disease duration matter? PLoS One 2021;22;16:e0261302.
- Peretz C, Chillag-Talmor O, Linn S, et al. Parkinson's disease patients first treated at age 75 years or older: a comparative study. Parkinsonism Relat Disord 2014;20:69-74.
- Dahodwala N, Pettit AR, Jahnke J, et al. Use of a medication-based algorithm to identify advanced Parkinson's disease in administrative claims data: Associations with claims-based indicators of disease severity. Clin Park Relat Disord 2020;3:100046.
- Schade S, Mollenhauer B, Trenkwalder C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov Disord Clin Pract 2020;7:343-5.
- Sharaf J, Williams KD, Tariq M, Acharekar MV, Guerrero Saldivia SE, Unnikrishnan S, Chavarria YY, Akindele AO, Jalkh AP, Eastmond AK, Shetty C, Rizvi SMHA, Mohammed L. The Efficacy of Safinamide in the Management of Parkinson's Disease: A Systematic Review. Cureus 2022;14:e29118.
- Plastino M, Gorgone G, Fava A, et al. Effects of safinamide on REM sleep behavior disorder in Parkinson disease: A randomized, longitudinal, cross-over pilot study. J Clin Neurosci 2021;91:306-12.
- Qureshi AR, Rana AQ, Malik SH, et al. Comprehensive Examination of Therapies for Pain in Parkinson's Disease: A Systematic Review and Meta-Analysis. Neuroepidemiology. 2018;51:190-206.
- Nishikawa N, Hatano T, Nishioka K, et al.; J-SILVER study group. Safinamide as adjunctive therapy to levodopa monotherapy for patients with Parkinson's disease with wearing-off: The Japanese observational J-SILVER study. J Neurol Sci 2024;461:123051.
- Rinaldi D, Bianchini E, Sforza M, et al. The tolerability, safety and efficacy of safinamide in elderly Parkinson's disease patients: a retrospective study. Aging Clin Exp Res 2021;33:1689-92.
- Lo Monaco MR, Petracca M, Vetrano DL, et al. Safinamide as an adjunct therapy in older patients with Parkinson's disease: a retrospective study. Aging Clin Exp Res 2020;32:1369-73.
- Kulisevsky J, Esquivel A, Freire-Álvarez E, et al. SYNAPSES. A European observational study to evaluate the safety and the effectiveness of safinamide in routine clinical practice: post-hoc analysis of the Spanish study population. Rev Neurol 2023;77:1-12.
- Peña E, Borrué C, Mata M, et al. Impact of SAfinamide on Depressive Symptoms in Parkinson's Disease Patients (SADness-PD Study): A Multicenter Retrospective Study. Brain Sci. 2021;11:232.
- Liguori C, Stefani A, Ruffini R, Mercuri NB, Pierantozzi M. Safinamide effect on sleep disturbances and daytime sleepiness in motor fluctuating Parkinson's disease patients: A validated questionnaires-controlled study. Parkinsonism Relat Disord 2018;57:80-81.
- Geroin C, Di Vico IA, Squintani G, Segatti A, Bovi T, Tinazzi M. Effects of safinamide on pain in Parkinson's disease with motor fluctuations: an exploratory study. J Neural Transm (Vienna) 2020;127:1143-52.
- Santos-García D, Laguna A, Hernández-Vara J, et al. On Behalf Of The Coppadis Study Group. Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson's Disease. J Clin Med 2023;12:1329.
- Gómez-López A, Sánchez-Sánchez A, Natera-Villalba E, et al. SURINPARK: Safinamide for Urinary Symptoms in Parkinson's Disease. Brain Sci 2021;11:57.
- De Micco R, Satolli S, Siciliano M, et al. Effects of safinamide on non-motor, cognitive, and behavioral symptoms in fluctuating Parkinson's disease patients: a prospective longitudinal study. Neurol Sci 2022;43:357-64.
- Pellecchia MT, Picillo M, Russillo MC, et al. Efficacy of Safinamide and Gender Differences During Routine Clinical Practice. Front Neurol 2021;12:756304.
- Cattaneo C, Jost WH. Pain in Parkinson's Disease: Pathophysiology, Classification and Treatment. J Integr Neurosci 2023;22:132.
- Beiske AG, Loge JH, Rønningen A, Svensson E. Pain in Parkinson's disease: Prevalence and characteristics. Pain 2009;141:173-7.
- Cattaneo C, Kulisevsky J, Tubazio V, Castellani P. Long-term Efficacy of Safinamide on Parkinson's Disease Chronic Pain. Adv Ther 2018;35:515-522.
- Qureshi AR, Rana AQ, Malik SH, et al. Comprehensive Examination of Therapies for Pain in Parkinson's Disease: A Systematic Review and Meta-Analysis. Neuroepidemiology 2018;5:190-206.
- Stocchi F, Borgohain R, Onofrj M, et al.; Study 015 Investigators. A randomized, double-blind, placebo-controlled trial of safinamide as add-on therapy in early Parkinson's disease patients. Mov Disord 2012;27:106-12.
- Cattaneo C, Barone P, Bonizzoni E, Sardina M. Effects of Safinamide on Pain in Fluctuating Parkinson's Disease Patients: A Post-Hoc Analysis. J Parkinsons Dis 2017;7:95-101.
- Cattaneo C, Sardina M, Bonizzoni E. Safinamide as Add-On Therapy to Levodopa in Mid- to Late-Stage Parkinson's Disease Fluctuating Patients: Post hoc Analyses of Studies 016 and SETTLE. J Parkinsons Dis 2016;6:165-73.
- Tsuboi Y, Hattori N, Yamamoto A, Sasagawa Y, Nomoto M; ME2125-4 Study Group. Long-term safety and efficacy of safinamide as add-on therapy in levodopa-treated Japanese patients with Parkinson's disease with wearing-off: Results of an open-label study. J Neurol Sci 2020.;416:117012.
- Hayes, MT. Parkinson's Disease and Parkinsonism. Am J Med 2019;132:802-07.
- Martinez-Martin P, Falup Pecurariu C, Odin P, et al. Gender-related differences in the burden of non-motor symptoms in Parkinson's disease. J Neurol. 2012 Aug;259(8):1639-47.
- Pellecchia MT, Picillo M, Russillo MC, Andreozzi V, Oliveros C, Cattaneo C. The effects of safinamide according to gender in Chinese parkinsonian patients. Sci Rep 2023;13:20632.
Figure 1.
Change in the NMSS total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD. Data are presented as box plots, with the box representing the median and the two middle quartiles (25-75%). Mild outliers (O) are data points that are more extreme than Q1 - 1.5 (case number shown). LEDD, levodopa equivalent daily dose; NMSS, Non-motor Symptoms Scale.
Figure 1.
Change in the NMSS total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD. Data are presented as box plots, with the box representing the median and the two middle quartiles (25-75%). Mild outliers (O) are data points that are more extreme than Q1 - 1.5 (case number shown). LEDD, levodopa equivalent daily dose; NMSS, Non-motor Symptoms Scale.
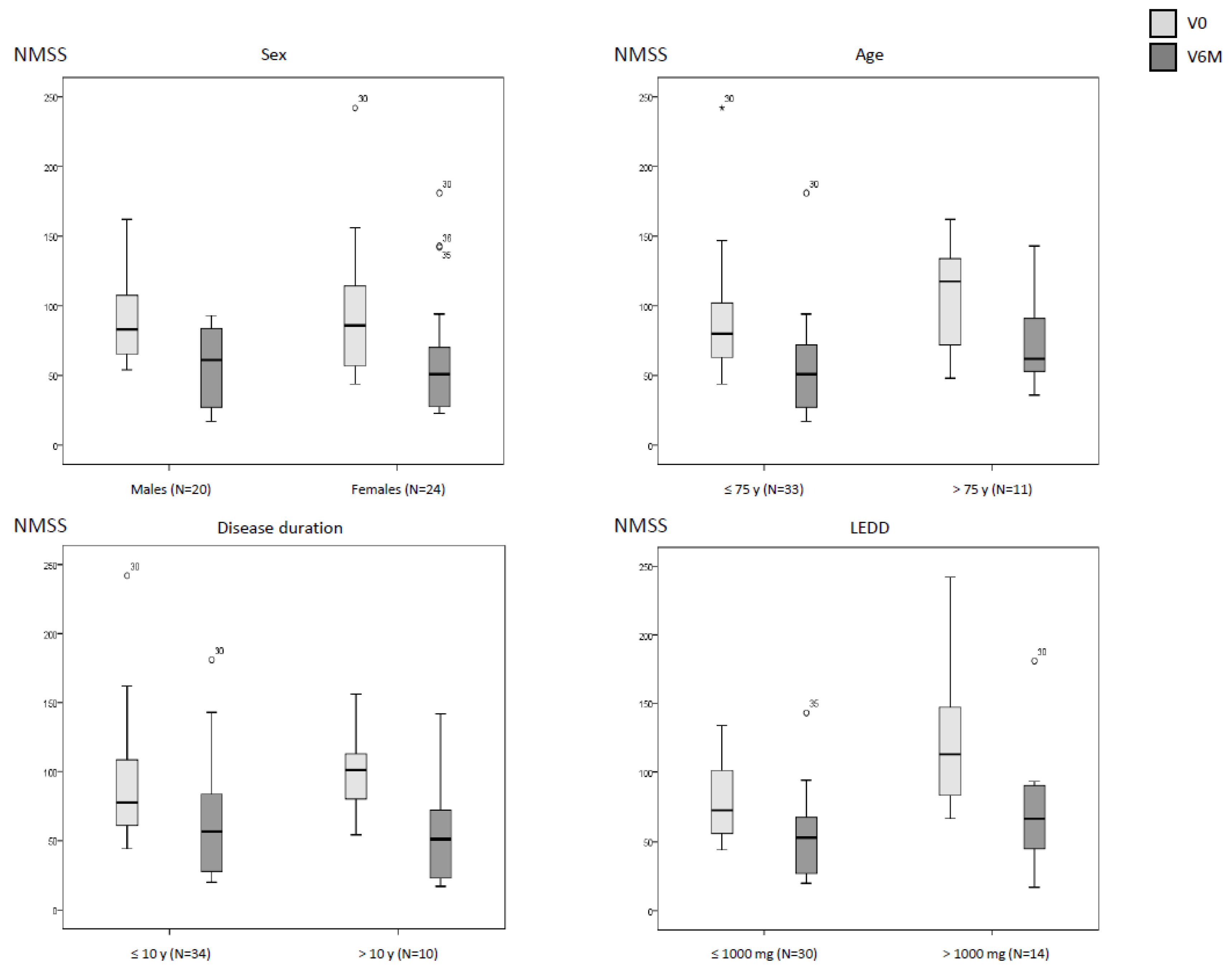
Figure 2.
Change in the PDQ39 total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD. Data are presented as box plots, with the box representing the median and the two middle quartiles (25-75%). Mild outliers (O) are data points that are more extreme than Q1 - 1.5 (case number shown). LEDD, levodopa equivalent daily dose; NMSS, PDQ-39, 39-item Parkinson’s Disease Quality of Life Questionnaire.
Figure 2.
Change in the PDQ39 total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD. Data are presented as box plots, with the box representing the median and the two middle quartiles (25-75%). Mild outliers (O) are data points that are more extreme than Q1 - 1.5 (case number shown). LEDD, levodopa equivalent daily dose; NMSS, PDQ-39, 39-item Parkinson’s Disease Quality of Life Questionnaire.
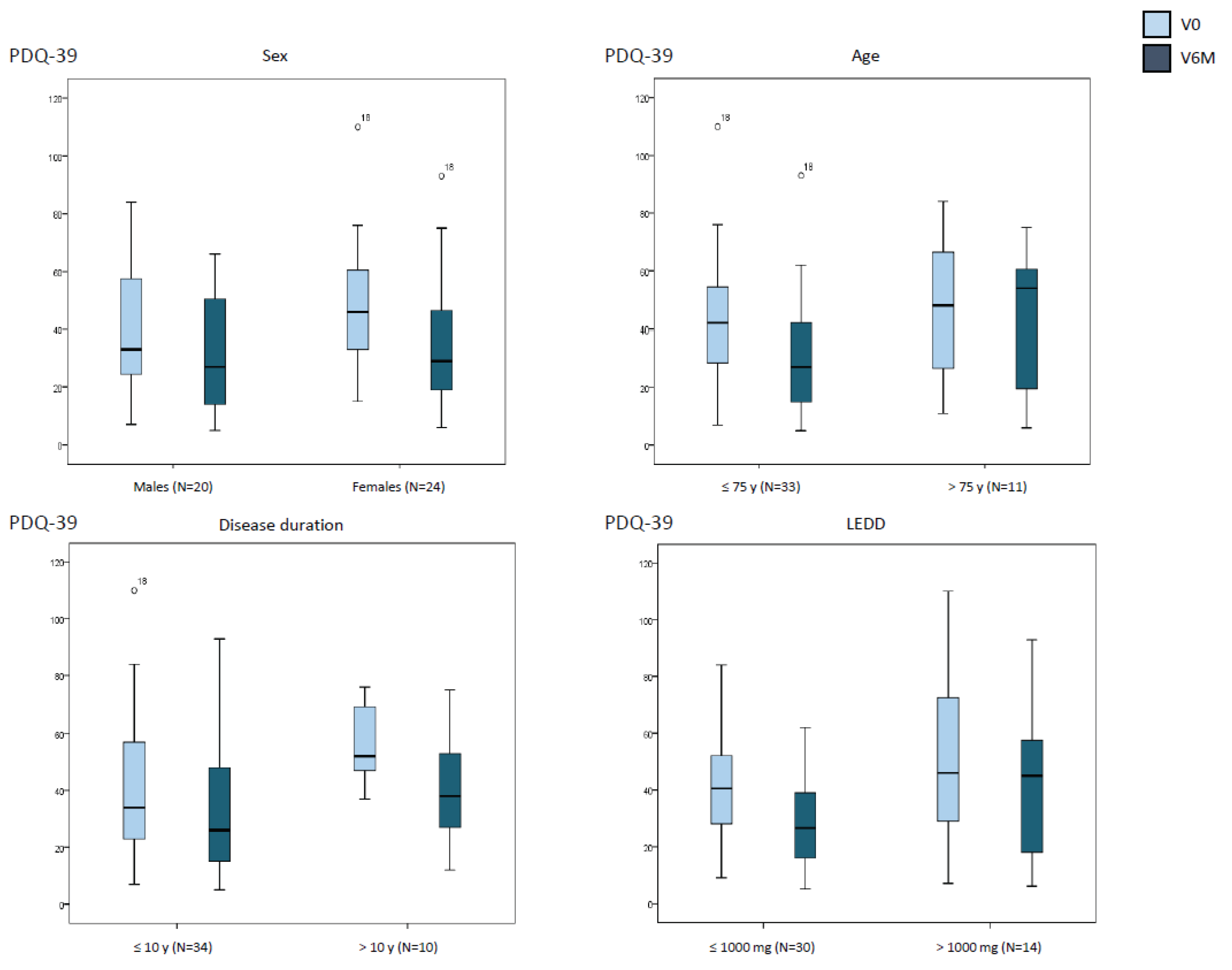

Table 1.
Change in the NMSS total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
Table 1.
Change in the NMSS total score from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
| At V0 | At V6M | Cohen´s d | pa | pb | pc | |
|---|---|---|---|---|---|---|
|
Sex Males (N=20) Females (N=24) |
93.6 ± 32.4 93.6 ± 45.2 |
59.4 ± 27.7 60.4 ± 41.5 |
-1.8 -1.3 |
<0.0001 0.001 |
0.629 | 0.494 |
|
Age ≤ 75 y (N=33) > 75 y (N=11) |
88.6 ± 38.9 108.7 ± 38.6 |
54.2 ± 34 77.2 ± 35.6 |
-1.9 -1.0 |
<0.0001 0.040 |
0.069 | 0.050 |
|
Disease duration ≤ 10 y (N=34) > 10 y (N=10) |
90.7 ± 41.1 102 ± 35.1 |
61.6 ± 35.5 55.2 ± 38.7 |
-1.4 -1.9 |
<0.0001 0.015 |
0.353 | 0.268 |
|
LEDD ≤ 1000 mg (N=30) > 1000 mg (N=14) |
80.9 ± 28.1 121.3 ± 49 |
53.6 ± 28.2 68.2 ± 43.1 |
-1.4 -1.7 |
<0.0001 0.002 |
0.004 | 0.425 |
a, comparison between the score at V0 and at V6 for each group individually (Wilcoxon’s rank sum test). b, comparison between patients of different group for each variable (i.e., males vs females, etc.) in the score at V0 (Mann–Whitney–Wilcoxon test). c, comparison between patients of different group for each variable (i.e., males vs females, etc.) in the score at V6M (Mann–Whitney–Wilcoxon test). LEDD, levodopa equivalent daily dose; NMSS, Non-motor Symptoms Scale.
Table 2.
Change in the score of each domain of the NMSS from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
Table 2.
Change in the score of each domain of the NMSS from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
| Males (N=20) |
Females (N=24) |
≤ 75 y old (N=33) |
> 75 y old (N=11) |
≤ 10 y DD (N=34) |
> 10 y DD (N=10) |
≤ 1000mg LEDD (N=30) |
> 1000 mg LEDD (N=14) | |
|---|---|---|---|---|---|---|---|---|
| Cardiovascular At V0 At V6M Cohen´s d p value |
8.8 ± 12.1 8.8 ± 12.3 0.0 0.838 |
8.7 ± 11.4 5 ± 9.7 -0.4 0.244 |
7.5 ± 11.1 3.8 ± 7.5 -0.4 0.077 |
12.5 ± 12.9 15.5 ± 14.9 0.3 0.552 |
9.3 ± 11.1 7.3 ± 11.1 -0.2 0.298 |
6.7 ± 13.4 4.6 ± 10.5 -0.2 0.785 |
8.9 ± 11.3 7.1 ± 11.4 -0.2 0.385 |
8.3 ± 12.6 5.9 ± 10.2 -0.3 0.483 |
| Sleep / fatigue At V0 At V6M Cohen´s d p value |
34.9 ± 16 19.2 ± 15.2 -1.6 <0.0001 |
34 ± 23.7 26.5 ± 19.9 -0.4 0.253 |
35.3 ± 20.4 21.3 ± 16.4 -1.0 0.001 |
31.8 ± 21 28.6 ± 22.4 -0.2 0.755 |
34.9 ± 19.7 23.8 ± 19.4 -0.7 0.008 |
32.7 ± 23.6 21 ± 13.4 -0.6 0.126 |
31.3 ± 16.8 23.9 ± 19.5 -0.5 0.045 |
41.2 ± 25.9 21.6 ± 15.3 -1.0 0.023 |
| Mood / apathy At V0 At V6M Cohen´s d p value |
26.3 ± 11.5 11.5 ± 12.9 -1.5 0.001 |
36.3 ± 30 17 ± 23.8 -1.2 <0.0001 |
30.5 ± 27.8 12.7 ± 19.6 -1.4 <0.0001 |
35.3 ± 24.6 19.9 ± 19.6 -1.1 0.040 |
27.2 ± 26.5 14.2 ± 20.6 -1.2 <0.0001 |
47.3 ± 22.4 15.4 ± 16.9 -2.2 0.005 |
25 ± 22.7 11.3 ± 13.6 -1.2 <0.0001 |
46 ± 30.1 21.3 ± 28.1 -1.6 0.004 |
| Perceptual symptoms At V0 At V6M Cohen´s d p value |
3.9 ± 7.8 4.6 ± 7.9 0.1 0.866 |
3.4 ± 7.3 1.4 ± 2.7 -0.4 0.301 |
3.7 ± 6.5 2.8 ± 6.1 -0.1 0.336 |
3.2 ± 9.9 2.8 ± 5.4 -0.1 0.989 |
4.3 ± 8.3 2.9 ± 5.6 -0.2 0.432 |
1.4 ± 2.6 2.5 ± 6.9 0.19 0.891 |
2.7 ± 6.6 2.3 ± 4.9 -0.1 0.759 |
5.6 ± 8.8 3.9 ± 7.7 -0.2 0.475 |
| Attention / memory At V0 At V6M Cohen´s d p value |
20.6 ± 17.6 14 ± 17.1 -0.9 0.010 |
14 ± 17.4 12.7 ± 19.4 -0.1 0.482 |
16.4 ± 15.9 11.1 ± 12.3 -0.7 0.006 |
18.7 ± 22.7 19.9 ± 29.5 0.1 0.858 |
15.2 ± 17.4 11.5 ± 17.3 -0.6 0.020 |
23.1 ± 17.9 19.4 ± 20.6 -0.3 0.553 |
13.2 ± 15.4 9.6 ± 15.2 -0.5 0.032 |
25 ± 19.9 21.2 ± 21.9 -0.3 0.373 |
| Gastrointestinal symptoms At V0 At V6M Cohen´s d p value |
19.9 ± 17.6 11.9 ± 11.4 -1.0 0.019 |
17.4 ± 16.6 14.1 ± 14.7 -0.3 0.148 |
16.1 ± 15.8 10.5 ± 11.7 -0.6 0.027 |
25.8 ± 18.8 20.9 ± 14.9 -0.4 0.090 |
19.3 ± 17.5 14.6 ± 12.9 -0.5 0.042 |
15.6 ± 15.2 8.1 ± 13.3 -0.5 0.108 |
17.9 ± 16.1 11.8 ± 12 -0.7 0.014 |
19.6 ± 19.2 16.1 ± 15.5 -0.3 0.278 |
| Urinary symptoms At V0 At V6M Cohen´s d p value |
45 ± 29.3 37.2 ± 25.4 -0.4 0.251 |
42.7 ± 30.7 25.1 ± 21.6 -1.1 <0.0001 |
40.3 ± 26.3 29.9 ± 25.7 -0.6 0.034 |
54 ± 37.9 32.5 18.6 -1.2 0.021 |
44.8 ± 29.6 33.6 ± 25.2 -0.7 0.012 |
40 ± 31.8 20.6 ± 16.6 -0.8 0.086 |
37.5 ± 26.4 28.3 ± 20.9 -0.6 0.031 |
57.1 ± 33.1 35.5 ± 29.8 -1.1 0.039 |
| Sexual dysfunction At V0 At V6M Cohen´s d p value |
40.2 ± 36.4 32.1 ± 33.9 -0.3 0.672 |
19.4 ± 33.8 17.2 ± 32.9 -0.2 0.812 |
23.4 ± 31.8 20.4 ± 32.3 -0.1 0.823 |
45.4 ± 44.3 39.8 ± 34.4 -0.2 0.888 |
31.5 ± 37.7 27.6 ± 34.7 -0.1 0.875 |
20 ± 30.1 17.5 ± 29.8 -0.3 0.565 |
24 ± 31.1 18.6 ± 26.7 -0.2 0.639 |
39.3 ± 44.7 39.6 ± 42.5 0.0 0.799 |
| Miscellaneous At V0 At V6M Cohen´s d p value |
29.2 ± 21 16 ± 12.1 -1.2 0.002 |
34.5 ± 21.1 21.4 ± 15.3 -1.1 0.002 |
30.6 ± 21.1 19.5 ± 14.7 -1.1 <0.0001 |
36.3 ± 21 17.4 ± 12.3 -1.4 0.013 |
30.2 ± 18 18.7 ± 11.6 -1.0 <0.0001 |
38.3 ± 29.4 19.8 ± 21.1 -1.6 0.012 |
29.9 ± 19 18.9 ± 11.4 -1.0 0.001 |
36.8 ± 24.1 19.1 ± 19 -1.6 0.003 |
Comparison between the score at V0 and at V6 for each group individually was assessed with the Wilcoxon’s rank sum test). DD, disease duration; LEDD, levodopa equivalent daily dose; NMSS, Non-motor Symptoms Scale. The score of each domain is expressed as a percentage of the corresponding maximum possible score (e.g., 36 points in Mood / apathy is expressed as 0.5).
Table 3.
Change in the PDQ-39 from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
Table 3.
Change in the PDQ-39 from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
| At V0 | At V6M | Cohen´s d | pa | pb | Pc | |
|---|---|---|---|---|---|---|
|
Sex Males (N=20) Females (N=24) |
39.1 ± 23.3 48.3 ± 22.1 |
32.4 ± 20.2 34.5 ± 22.7 |
-0.5 -1.4 |
0.080 <0.0001 |
0.202 | 0.741 |
|
Age ≤ 75 y (N=33) > 75 y (N=11) |
43.2 ± 22.2 46.7 ± 25.6 |
30.4 ± 19.8 42.4 ± 24 |
-1.4 -0.3 |
<0.0001 0.306 |
0.632 | 0.124 |
|
Disease duration ≤ 10 y (N=34) > 10 y (N=10) |
40.3 ± 23.5 57.9 ± 14.2 |
31.2 ± 21.5 42.1 ± 19.9 |
-0.8 -2.1 |
0.0020.011 |
0.009 | 0.105 |
|
LEDD ≤ 1000 mg (N=30) > 1000 mg (N=14) |
40.9.9 ± 18.5 50.6 ± 31.8 |
29.1 ± 17.1 41.9 ± 26.8 |
-1.1 -0.6 |
<0.0001 0.119 |
0.391 | 0.265 |
a, comparison between the score at V0 and at V6 for each group individually (Wilcoxon’s rank sum test). b, comparison between patients of different group for each variable (i.e., males vs females, etc.) in the score at V0 (Mann–Whitney–Wilcoxon test). c, comparison between patients of different group for each variable (i.e., males vs females, etc.) in the score at V6M (Mann–Whitney–Wilcoxon test). LEDD, levodopa equivalent daily dose; PDQ-39, 39-item Parkinson’s Disease Quality of Life Questionnaire.
Table 4.
Change in the score of each domain of the PDQ-39 from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
Table 4.
Change in the score of each domain of the PDQ-39 from baseline (V0) to the final visit at 6 months (V6M) in PD patients from the SAFINOMOTOR study according to sex, age, disease duration and LEDD.
| Males (N=20) |
Females (N=24) |
≤ 75 y old (N=33) |
> 75 y old (N=11) |
≤ 10 y DD (N=34) |
> 10 y DD (N=10) |
≤ 1000mg LEDD (N=30) |
> 1000 mg LEDD (N=14) | |
|---|---|---|---|---|---|---|---|---|
| Mobility At V0 At V6M Cohen´s d p value |
22.3 ± 30.3 23.5 ± 22.8 0.1 0.584 |
42.5 ± 27.6 33.8 ± 29.4 -0.6 0.017 |
31.4 ± 25.9 23.5 ± 22.7 -0.7 0.004 |
38.9 ± 28.2 45.9 ± 32.1 0.5 0.592 |
28.3 ± 25.7 25.9 ± 25.6 -0.2 0.184 |
50.3 ± 21.9 40 ± 29.5 -0.9 0.074 |
30.5 ± 20.7 24.3 ± 20.4 -0.5 0.021 |
39.3 ± 35.7 39.2 ± 35.9 0.0 0.574 |
| Activities of daily living At V0 At V6M Cohen´s d p value |
24.6 ± 23.4 18.3 ± 18.1 -0.5 0.244 |
27.6 ± 22.1 17.4 ± 18.2 -0.8 0.019 |
25.3 ± 21.9 14.9 ± 15.6 -0.9 0.002 |
29.2 ± 24.9 26.5 ± 22.2 -0.2 0.964 |
22.4 ± 20.2 14.8 ± 15.4 -0.6 0.047 |
39.2 ± 25.9 27.9 ± 22.9 -0.8 0.114 |
23.1 ± 21.8 15.2 ± 15.3 -0.6 0.119 |
33 ± 23.2 23.2 ± 22.3 -0.8 0.073 |
| Emotional well-being At V0 At V6M Cohen´s d p value |
31.4 ± 23.4 22.1 ± 20.9 -0.8 0.040 |
48.4 ± 27 29.8 ± 24.4 -1.3 <0.0001 |
40.4 ± 26.9 24.6 ± 24.1 -1.1 <0.0001 |
42.4 ± 27.1 31.4 ± 19.6 -1.0 0.052 |
38.6 ± 26.6 26.6 ± 23.3 -0.9 0.002 |
48.3 ± 26.7 25.4 ± 23 -1.9 0.008 |
39.4 ± 24.2 23.1 ± 20.2 -1.1 <0.0001 |
44.2 ± 32.3 33.3 ± 27.7 -1.1 0.022 |
| Stigmatization At V0 At V6M Cohen´s d p value |
21.7 ± 25.4 11.9 ± 16.1 -0.6 0.070 |
9.1 ± 10.9 4.2 ± 8.9 -0.5 0.107 |
13.9 ± 18.8 6.8 ± 12 -0.5 0.057 |
17 ± 22.4 10.2 ± 16.3 -0.9 0.063 |
14.4 ± 18.9 6.4 ± 12.3 -0.6 0.011 |
15.6 ± 22.4 11.8 ± 15.4 -0.3 0.492 |
15.4 ± 18.7 9.6 ± 14.4 -0.6 0.024 |
12.9 ± 21.9 3.6 ± 8.7 -0.5 0.207 |
| Social support At V0 At V6M Cohen´s d p value |
7.5 ± 8.7 3.3 ± 11.3 -0.4 0.121 |
4.5 ± 10.7 3.8 ± 193.9 -0.1 0.752 |
5.2 ± 9.1 4.3 ± 14.4 -0.1 0.651 |
7.6 ± 12 1.5 ± 3.8 -0.7 0.131 |
4.5 ± 8.9 2.2 ± 8.8 -0.3 0.181 |
10 ± 12.3 8.3 ± 21.1 -0.2 0.750 |
5 ± 9.7 4.4 ± 14.9 -0.1 0.643 |
7.7 ± 10.5 1.8 ± 4.8 -0.7 0.111 |
| Cognition At V0 At V6M Cohen´s d p value |
27.9 ± 20.9 28.4 ± 25.3 0.0 0.909 |
22.1 ± 16.9 19.8 ± 19.5 -0.2 0.158 |
26.2 ± 19.7 24.4 ± 22 -0.1 0.165 |
20.4 ± 16.1 21.6 ± 24.9 0.1 0.893 |
25.4 ± 20.5 22.9 ± 21.6 -0.2 0.295 |
22.5 ± 12.6 26.2 ± 26.3 0.2 0.918 |
23.1 ± 15.1 19.4 ± 19 -0.3 0.193 |
28.4 ± 25.9 33 ± 27.1 0.3 0.929 |
| Communication At V0 At V6M Cohen´s d p value |
25.9 ± 27.1 18.2 ± 17.5 -0.3 0.278 |
7.6 ± 10.9 6.3 ± 9.9 -0.2 0.497 |
15.6 ± 22.4 12.4 ± 15 -0.2 0.399 |
15.9 ± 19.9 11.4 16.3 -0.3 0.344 |
15.9 ± 21.7 12.7 ± 15.8 -0.2 0.367 |
15 ± 25.4 10 ± 13.9 -0.5 0.380 |
14.7 ± 21.5 9.2 ± 11.8 -0.4 0.090 |
17.9 ± 22.3 18.4 ± 19.6 0.1 0.980 |
| Pain and discomfort At V0 At V6M Cohen´s d p value |
37.2 ± 26.6 27.9 ± 20.9 -0.6 0.070 |
48.3 ± 27.7 37.8 ± 18.2 -0.5 0.080 |
43.5 ± 27.2 34.8 ± 19.4 -0.5 0.076 |
43.2 ± 29.3 28.8 ± 21.5 -1.0 0.043 |
44.2 ± 26.9 33.3 ± 19.8 -0.6 0.019 |
40.8 ± 30.3 33.3 ± 21.1 -0.3 0.362 |
42.8 ± 22.8 32.5 ± 19.6 -0.7 0.016 |
44.8 ± 37 35.1 ± 21.2 -0.4 0.307 |
Comparison between the score at V0 and at V6 for each group individually was assessed with the Wilcoxon’s rank sum test). DD, disease duration; LEDD, levodopa equivalent daily dose; NMSS, Non-motor Symptoms Scale. The score of each domain is expressed as a percentage of the corresponding maximum possible score (e.g., 20 points in Mobility is expressed as 0.5).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



