
Submitted:
24 October 2025
Posted:
27 October 2025
You are already at the latest version
Abstract
Patients with systemic lupus erythematosus (SLE) face a daunting journey accompanied by severe morbidity, a poor quality of life and potential damage to major organs including the kidneys, eyes, cardiovascular and cerebrovascular systems. Disease prevalence is highly skewed towards females of childbearing age - polarizing statistics pointing to a role for estrogen in disease origin and/or progression. Female patients of certain races/ethnicities are more predisposed to SLE while also presenting with more severe and aggressive disease. Unfortunately, this cohort also experiences the most delays in disease diagnosis. Herein we discuss SLE and its outcomes in the backdrop of estrogen and delays in diagnosis.
Keywords:
systemic lupus erythematosus
; estrogen
; females
; minorities
; diagnosis
; delays
; outcomes
1. Introduction
Affecting ~3.41million people worldwide, and more than 200,000 persons in the United States alone, systematic lupus erythematosus (SLE) is a debilitating autoimmune disease [1,2,3]. Patients experience diffuse symptoms including malar rash, malaise, fever, polyarthralgia and swelling with potential progression to organ damage. The eyes, kidneys, lungs, cardiovascular and the central nervous system (CNS) can each be compromised irreversibly by SLE [4,5]. Approximately 90% of those diagnosed with SLE are female and between 15 and 45 years of age [3] - polarizing statistics that suggest a role for estrogen in disease origin and/or progression. This disease can therefore effectively take a toll on a women’s professionally productive and childbearing years. Data from the National Lupus Patient Registry [3] at the Centers for Disease Control and Prevention indicate an increased prevalence, incidence, morbidity and mortality in Black/African Americans, Hispanic/Latinos, Native American/Alaska Native and Asian American/Pacific Islanders. Minority patients with SLE accrue more disease-related damage over time and at a faster pace than their White counterparts [6].
The diffuse and vague symptoms associated with SLE is associated with a door-to-diagnosis time that can exceed 6 years in SLE [7]. To make matters worse, historical experience suggests that compared with White males, females, especially minority females, experience disease-agnostic delays in diagnosis [8,9]. Herein we discuss SLE and its outcomes in the setting of estrogen and delays in diagnosis.
2. Methods
This study does include interaction with or intervention in human subjects; nor did it obtain any identifiable private information. Prevalence of SLE as a function of geography, age, sex and race/ethnicity was computed from the available literature and databases including AllofUs [10]. Figures were (re)drawn based on data from published literature. Door-to-diagnosis time and/or time-to-intervention were computed for several diseases based on the available literature.
3. Results and Discussion
3.1. Demographics and SLE
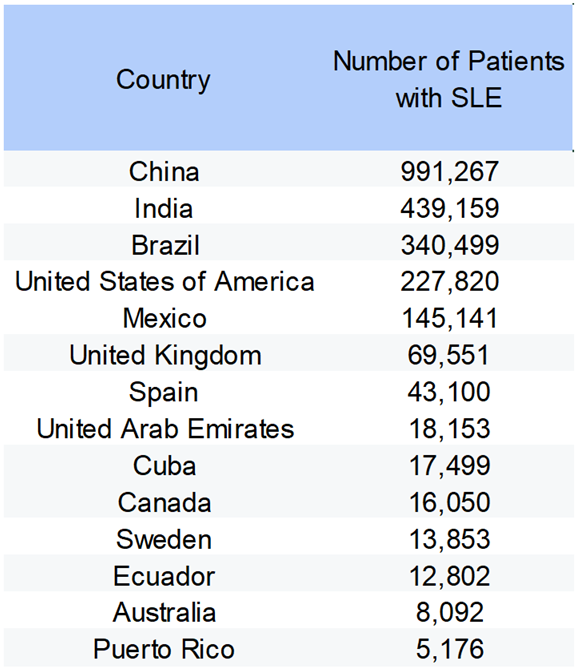
Table 1 shows the prevalence of SLE across a number of countries with China, India, Brazil, United States and Mexico each exceeding >100,000 patients with this disease [11,12]. Demographic data indicate that this disease predominantly affects one sex. Female:male ratios of 10:1 to 12:1 in China [13], 19:1 in India [14], 11:1 to 15:1 in Brazil [15] and 11:1 in Mexico [16] have been reported for patients with SLE (Figure 1A). Within the United States AllofUs registry [10], the prevalence of SLE is also skewed towards females (Figure 1B). Furthermore, female patients with SLE are typically of child- bearing years, the caveat being that these data are derived from patients consenting to participate in the registry. Needless to say, the sheer difference in prevalence translates to increased prevalence of lupus-related organ issues in females (Figure 1C).

Table 1.
Prevalence of SLE in various countries.
3.2. Estrogen and SLE
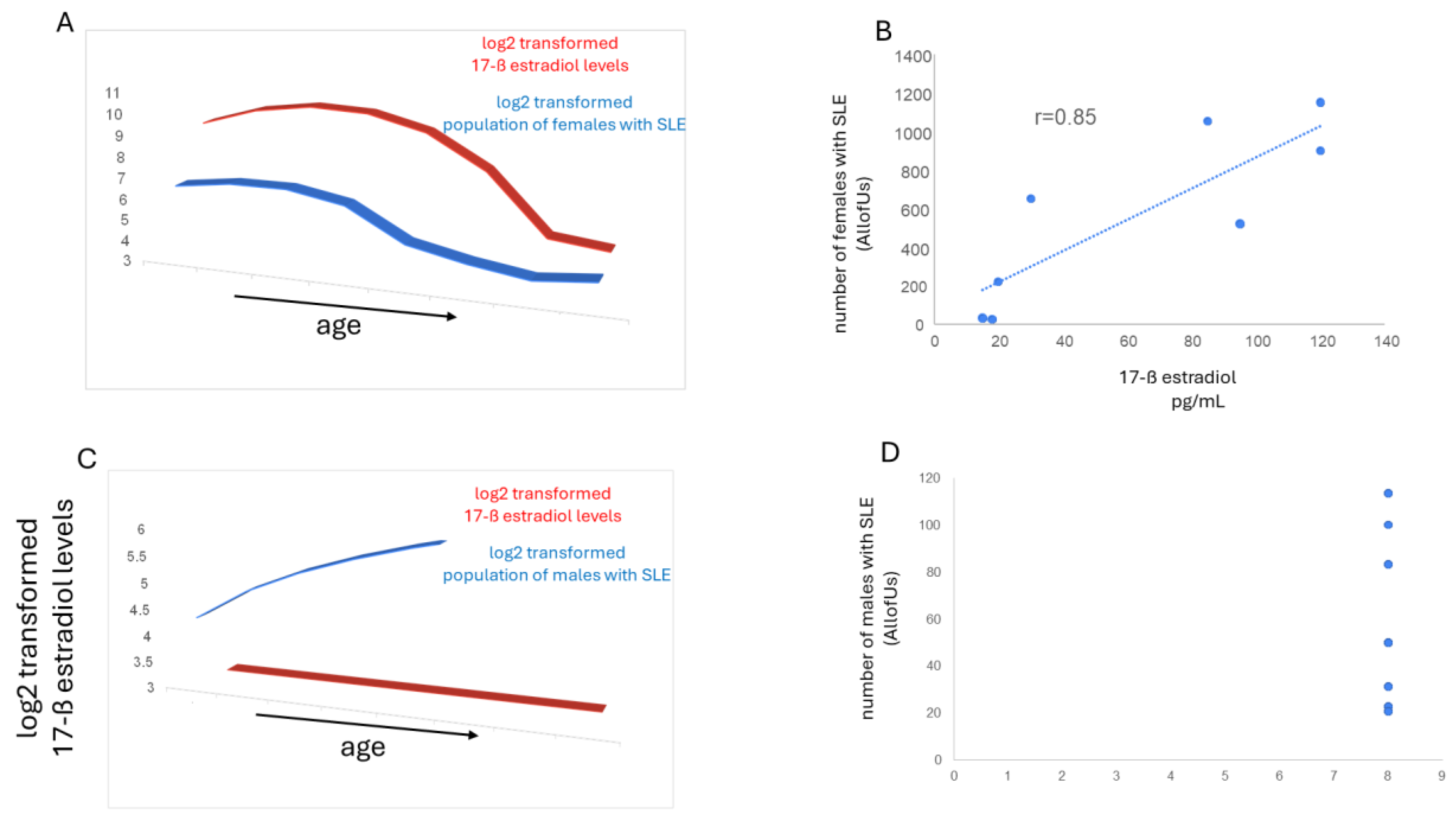
Considering that patients with SLE are predominantly female and of child-bearing age raises the question of estrogen involvement in disease origin and/or progression. Levels of 17-ß estradiol [17], the most potent form of estrogen, are similar in males and females between birth and puberty, higher in females vs. males between the ages of 10 and 55 and tend to converge between the ages of 55 and 85 (Figure 2). In females the prevalence of SLE tracks with their levels of 17-ß estradiol (Figure 3A). A robust correlation is observed between prevalence of SLE and 17-ß estradiol levels (Figure 3B). Such a relation is not observed in males given that their 17-ß estradiol level remain somewhat constant across their lifespan (Figure 3 C and D). These data suggest that estrogen may be a risk factor for SLE. Data from a cohort study comprising females with SLE suggests that the ratio of [estrogen+estrogen receptor/testosterone+androgen receptor] correlates with disease severity [18]. Indeed, lupus flares can be triggered by fluctuations in estrogen levels, which is why patients may experience flares during periods of high estrogen, such as during a menstrual cycle or pregnancy [19]. High estrogen levels can increase immune system activity [18], potentially leading to flares, while fluctuations from menopause can also trigger them. Thus, lupus flares can be considered an estrogenopathy. Curiously, a study [20] has reported that Black females have higher levels of estrogen, specifically estradiol, across the menstrual cycle compared to white women. That SLE is more prevalent in Blacks is well-known [3]. Nevertheless, these data notwithstanding, a causative relation between estrogen and SLE in females remains to be documented. Use of selective estrogen receptor modulators in patients with SLE is often contraindicated given the complex systemic role of estrogen including its regulation of the immune system and its beneficial effects including supporting bone health, cardiovascular health, and brain function [19].
3.3. Diagnosis Delays and Demographics
Historically, females experience greater delays in disease diagnosis vs. their male counterparts. Examination of longitudinal records from ~208 million Americans showed that among 112 acute and chronic diseases, women experience longer lengths of time between symptom onset and disease diagnosis than men for most diseases regardless of metric used, even when only symptoms common to both genders are considered [8]. The study of health data from 6.9 million Danish people found that across hundreds of diseases, women on average were diagnosed when they were about four years older than the age at which the conditions were recognized in men [9]. In so far as SLE is concerned, one study reported that the median delay in diagnosis was 14.09 months in men and 29.55 months in women [21]. A UK-wide survey [22] of individuals living with SLE found a significant period of time, 6.4 years, between initial symptoms and reaching the diagnosis of SLE. Almost one-half of the individuals who responded had also been given a different initial diagnosis prior to their final diagnosis. A trend towards a shorter time to diagnosis in men, 4.8 years, was observed. Interestingly, in this study, Blacks had the shortest time to diagnosis which was attributed to the severity of their symptoms at presentation. In a Polish cohort comprising White patients with SLE, the period between the onset and diagnosis of with late-onset disease was longer in females (38.7 months) vs. males. men (4 months) [23]. The delays in diagnosis appear to be due to a variety of factors and their combinations. Symptoms may present differently in males vs. female and some conditions are still considered the “male version” of a disease, leading to misdiagnosis or delays in females. In fact, even though SLE should be suspected in young symptomatic females, many times the diagnosis is finally made via exclusion. Females may face domestic barriers to seeking care such as having to care for children, the spouse and/or elderly family members, and/or not being financially dependent, which can lead to further delays. Provider bias is another factor influencing time to diagnosis with women’s symptoms may be dismissed as “normal” or psychosomatic. Finally, with much of biomedical research having been geared toward treatment of male White patients, there is limited understanding of X vs Y chromosomes and even differences between the two X chromosomes [24] and disease biology and outcomes.
Minority women face additional delays in diagnosis compared to their White counterparts. The delay in diagnosis appears agnostic to disease. Black women waited 1.75 times as long as White women to obtain a tissue diagnosis after an abnormal breast screening [25]. In another study, time to breast cancer diagnosis in Black patients was 53.6 months compared to 36 months for White patients [26]. Patients with endometriosis experienced a diagnosis time of 40.3 months if White vs. 43.7 months if Black [27]. In patients with multiple sclerosis, regardless of sex, average time from symptom onset to diagnosis was 69.8 months in Black, 21.5 months in Asian, 19.7 months in Hispanic and 18.2 months in White [28]. In so far as diagnosis time in SLE is concerned one study reported that residence in the southern United States and identification as American Indian/Alaska Native were associated with prolonged time to SLE diagnosis [29]. In another study, 22.4% of African American females but only 14.3% of white females experienced clinical delays > 3 months in their treatment of SLE. The California Lupus Survey reported that White patients with SLE were more likely to have > 16 years follow up after diagnosis compared to non-White patients (p<0.001) [31].
3.4. Diagnosis Delays and Outcomes in SLE
As with most any other disease, in SLE, longer time to diagnosis is associated with worse outcome. Analysis of the LulA cohort showed that the longer the time to diagnosis, the higher the SLE disease activity, disease-related damage and fatigue and the lower the health-related quality of life [32]. Patients in the GLADEL cohort with a time to diagnosis ≥ 24 months experienced a higher frequency of thrombocytopenia, associated comorbidities, antiphospholipid syndrome (APS), anti-beta-2-glycoprotein-I (B2GPI) positivity and cumulative damage with lower frequency of low complement at cohort entry [33]. Delayed diagnosis and misdiagnosis of SLE have far-reaching consequences for patients and healthcare providers. From irreversible organ damage and increased morbidity and mortality to emotional distress and financial strain, the toll of delayed diagnosis and misdiagnosis extends beyond physical symptoms to encompass psychological, social, and economic dimensions [34].
4. Conclusion
For patients with SLE, especially minority females, estrogen and a longer time to diagnosis can have an adverse effect on outcomes. Concepts in care with the intention to at the very least shorten the time to diagnosis are needed to improve the long-term outcome of the disease.
References
- European Lupus Society. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. SLEuro. Last accessed April 4, 2025.
- The US Centers for Disease Control and Prevention. People with Lupus. May 15, 2024. Last accessed April 4, 2025.
- Lupus Foundation of America; last accessed April 4, 2025.
- Lao C, et al. Mortality and causes of death in systemic lupus erythematosus in New Zealand: a population-based study. Rheumatology 63:1560-1567, 2024.
- Zen M, et al. Mortality and causes of death in systemic lupus erythematosus over the last decade: Data from a large population-based study. Eur J Intern Med 112:45-5, 2023.
- Buie J, et al. Disparities in Lupus and the Role of Social Determinants of Health: Current State of Knowledge and Directions for Future Research. ACR Open Rheumatol 5:454–464, 2023.
- Nikolopoulos D, et al. Evolving phenotype of systemic lupus erythematosus in Caucasians: low incidence of lupus nephritis, high burden of neuropsychiatric disease and increased rates of late-onset lupus in the ‘Attikon’ cohort. Lupus 29:514–52, 2020.
- Sun TY, et al. Large-scale characterization of gender differences in diagnosis prevalence and time to diagnosis. MedRxiv [Preprint]. 2023.10.12.23296976, 2023.
- Westergaard D, et al. Population-wide analysis of differences in disease progression patterns in men and women. Nat Commun 10, 666, 2019.
- AllofUs; last accessed October 23, 2025.
- Population by Country (2025) - Worldometer; last accessed, October 23, 2025.
- Tian J, et al. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheum Dis 82:351–356, 2023.
- Mok CC, et al. Clinical characteristics and outcome of southern Chinese males with systemic lupus erythematosus. Lupus 8:188-96, 1999.
- Mathur R, et al. Systemic Lupus Erythematosus in India: A Clinico-Serological Correlation. Cureus 14:e25763, 2022.
- Martyres A, et al. Mapping the spatial and temporal frequency of systemic lupus erythematosus in Brazil Rev Bras Epidemiol 28:e250030, 2025.
- Fajardo Hermosillo LD. AB0588 Systemic Lupus Erythematosus in Men from a Mexican Cohort. Annals of the Rheumatic Diseases 74, Supplement 2, 1096-1097, 2015.
- Veser CA, et al. Embracing Sex-specific Differences in Engineered Kidney Models for Enhanced Biological Understanding. 10.48550/arXiv.2308.15264; 2023.
- Abdolahpur S, et al. The Effect of Estradiol and Testosterone Levels Alone or in Combination with Their Receptors in Predicting the Severity of Systemic Lupus Erythematosus: A Cohort Study. Iran J Med Sci 50:69-76, 2025.
- Constatin AM, Bicus C. Estradiol in Systemic Lupus Erythematosus. Acta Endocrinol (Buchar) 19:274–276, 2023.
- Marsh EE, et al. Estrogen Levels Are Higher across the Menstrual Cycle in African-American Women Compared with Caucasian Women. The Journal of Clinical Endocrinology & Metabolism 96:1, 2011.
- Ramirez-Flores MF, et al. Factors associated with delay in the diagnosis and treatment of systemic lupus erythematosus in adult patients: a systematic review. Rheumatology (Oxford), keaf384, 2025.
- Morgan C, et al. Individuals living with lupus: findings from the LUPUS UK Members Survey 2014. Lupus 27:681–687, 2018.
- Jeleniewicz R, et al. Clinical picture of late-onset systemic lupus erythematosus in a group of Polish patients. POLSKIE ARCHIWUM MEDYCYNY WEWNĘTRZNEJ 125 (7-8), 2015.
- Not so inactive X chromosome | Whitehead Institute; last accessed, October 23, 2025.
- Manik R, et al. Racial Disparities and Strategies for Improving Equity in Diagnostic Follow-Up for Abnormal Screening Mammograms. JCO Oncol Pract 20:1367-1375, 2024.
- George P, et al. Diagnosis and Surgical Delays in African American and White Women with Early-Stage Breast Cancer. MMWR Morb Mortal Wkly Rep 68:419–422, 2019.
- Zhang, W.; et al. Time to Diagnosis for Endometriosis by Race. Journal of Minimally Invasive Gynecology 28, Supplement, Page S150, 2021.
- Akinsanya J, et al. The Impact of Race and Ethnicity on Time to Diagnosis of Multiple Sclerosis: Preliminary Results Neurology 98:756, 2022.
- Buie, J. Factors Influencing Time to Diagnosis in U.S. Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol 75 (suppl 9), 2023.
- African-American Ethnicity Associated with Longer Time to Lupus Low Disease Activity State • Johns Hopkins Rheumatology; last accessed, 10/24/2025.
- Maningding E, et al. Racial and Ethnic Differences in the Prevalence and Time to Onset of Manifestations of Systemic Lupus Erythematosus: The California Lupus Surveillance Project. Arthritis Care Res (Hoboken) 72:622-629, 2020.
- Kernder A, et al. Delayed diagnosis adversely affects outcome in systemic lupus erythematosus: Cross sectional analysis of the LuLa cohort. Lupus 30:431–438, 2021.
- Nieto, R; et al. DELAYED DIAGNOSIS IN SYSTEMIC LUPUS ERYTHEMATOSUS. The Journal of Rheumatology 52 (Suppl 1) 14-15, 2025.
- Mitchell, JL. Understanding the impact of delayed diagnosis and misdiagnosis of systemic lupus erythematosus (SLE). J Family Med Prim Care 13:4819–4823, 2024.
Figure 1.
SLE and its Demographics. A) Ratio of female: male patients with SLE in various countries. The actual numbers are presented within the text of the article. B) Increased prevalence of SLE in female patients of child-bearing age. Source AllofUs [10]. C) Increased prevalence of glomerulonephritis in female patients with SLE. Source AllofUs [10].
Figure 1.
SLE and its Demographics. A) Ratio of female: male patients with SLE in various countries. The actual numbers are presented within the text of the article. B) Increased prevalence of SLE in female patients of child-bearing age. Source AllofUs [10]. C) Increased prevalence of glomerulonephritis in female patients with SLE. Source AllofUs [10].
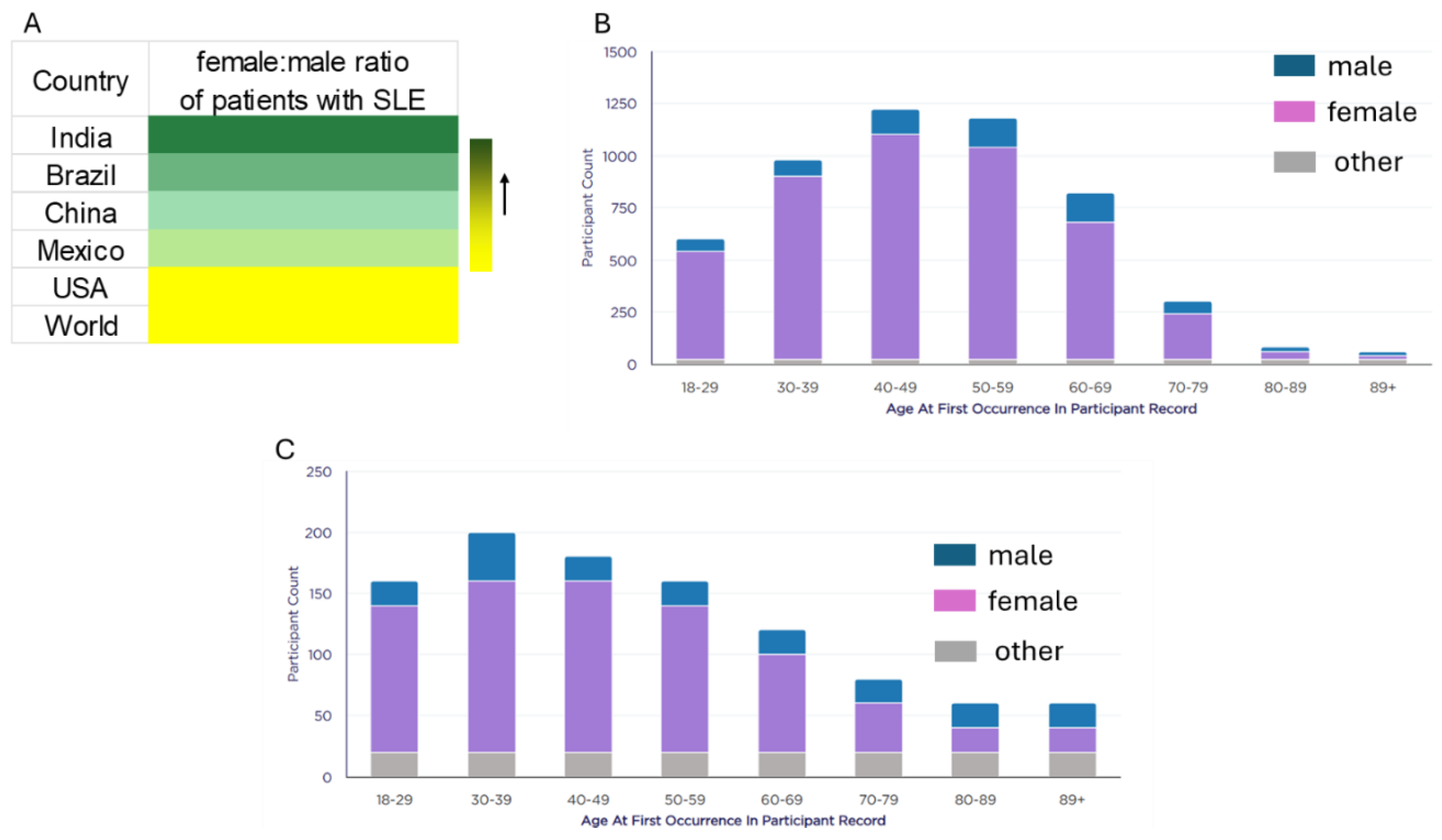
Figure 2.
Estrogen and its Demographics. 17-ß estradiol levels as a function of sex and age.
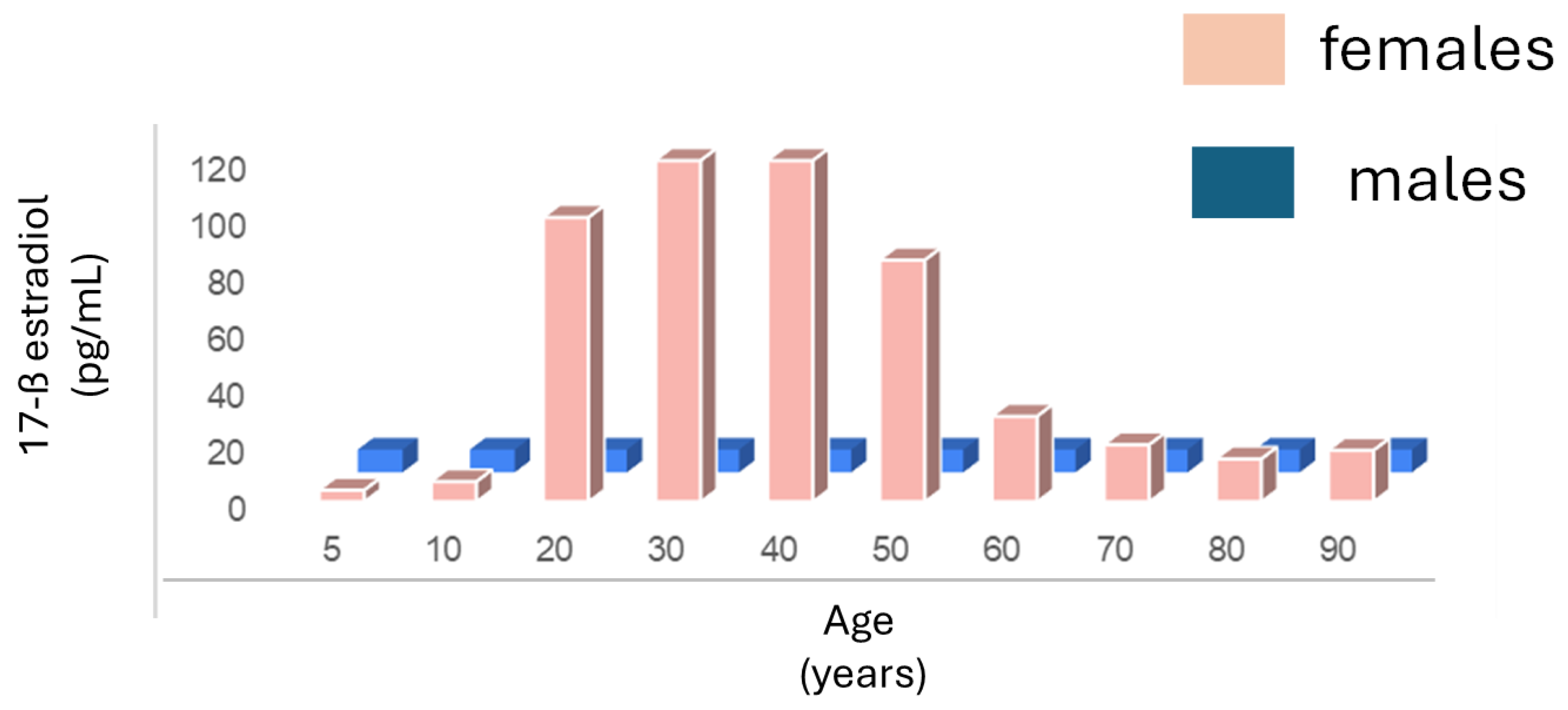
Figure 3.
Estrogen and SLE. A) In females, the prevalence of SLE tracks with their levels of 17-ß estradiol. B) A robust correlation is observed between prevalence of SLE and 17-ß estradiol levels in females. C) and D) In males, there is no relation between their 17-ß estradiol levels and prevalence of SLE.
Figure 3.
Estrogen and SLE. A) In females, the prevalence of SLE tracks with their levels of 17-ß estradiol. B) A robust correlation is observed between prevalence of SLE and 17-ß estradiol levels in females. C) and D) In males, there is no relation between their 17-ß estradiol levels and prevalence of SLE.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



