Submitted:
20 November 2025
Posted:
24 November 2025
Read the latest preprint version here
Abstract
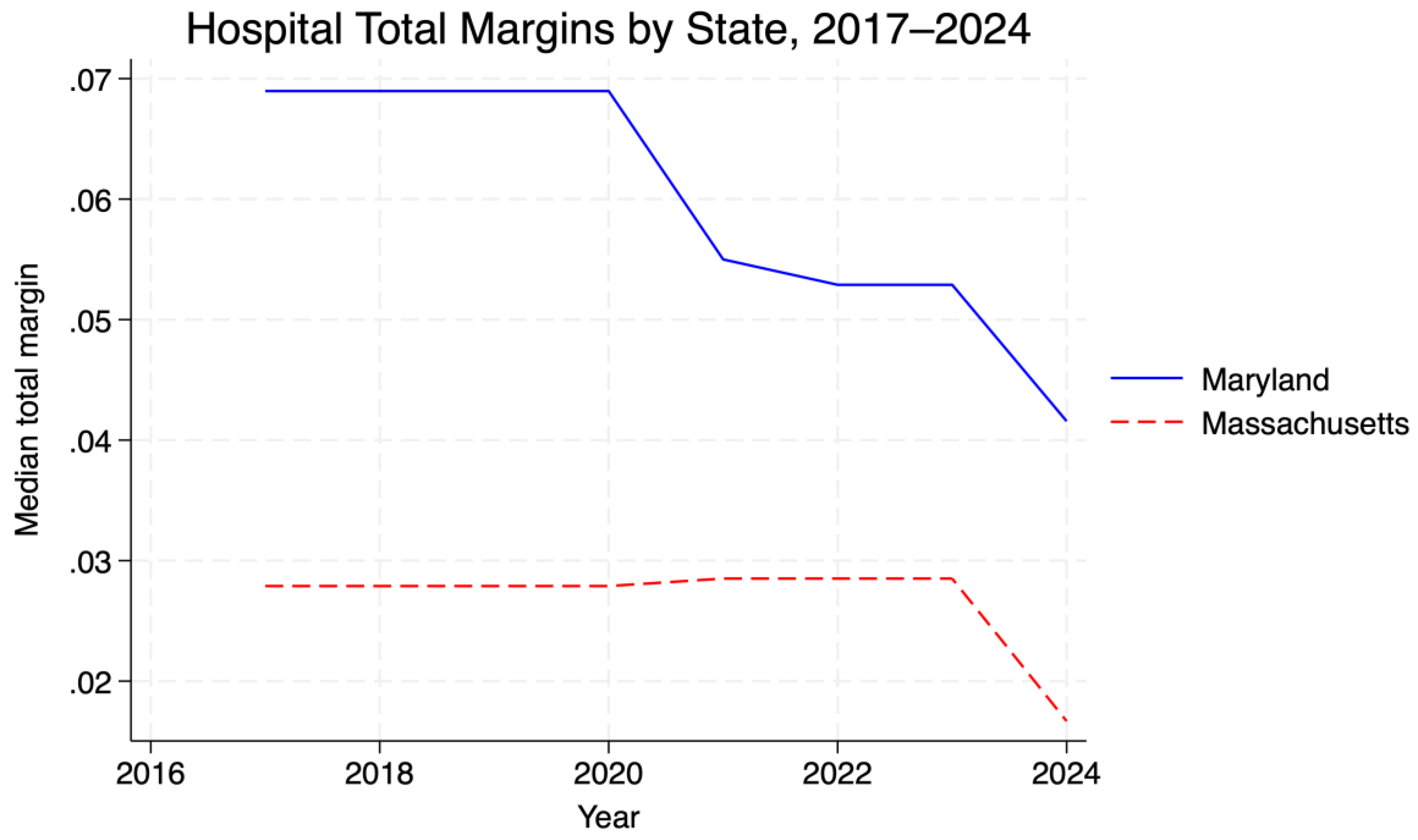
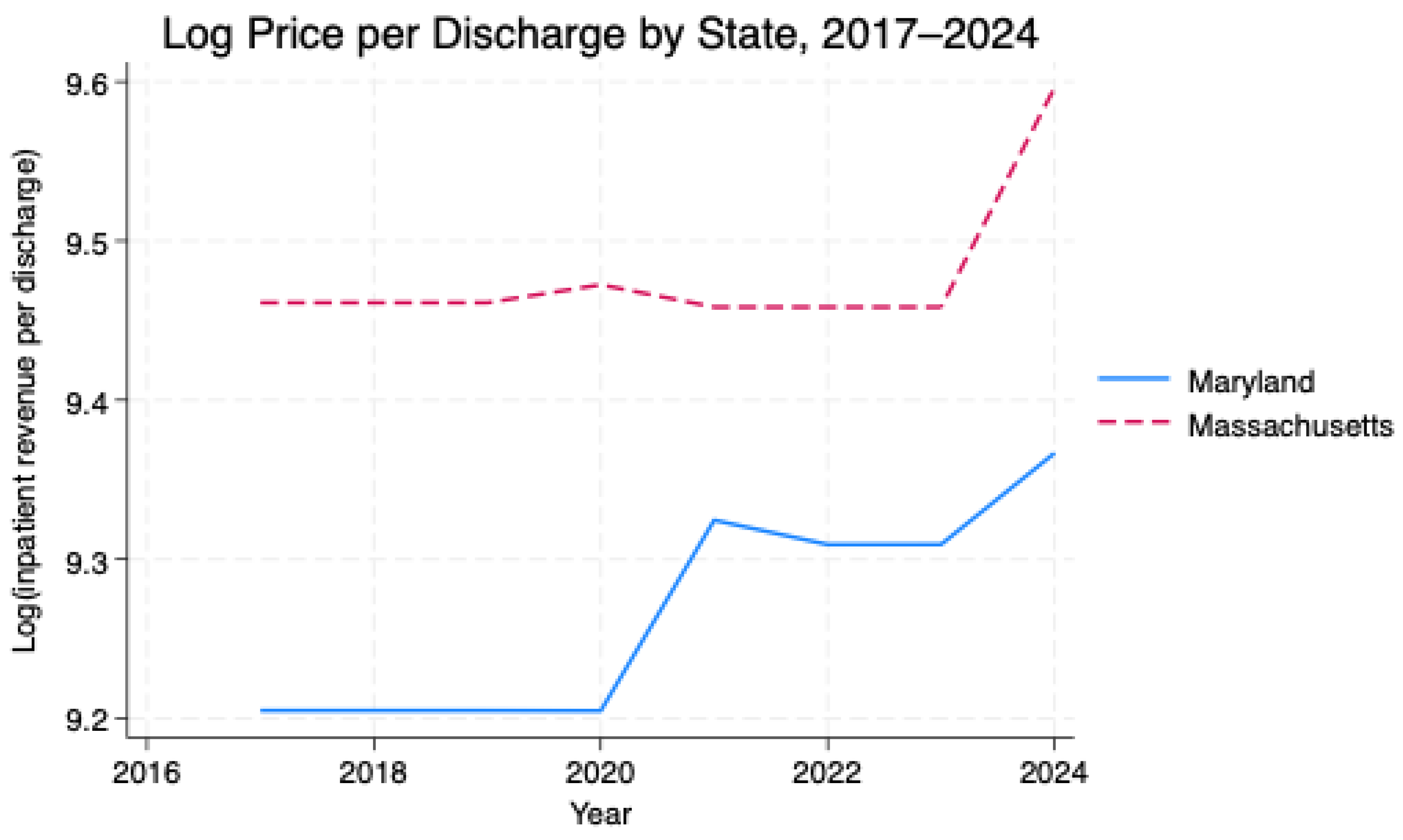
Background: Maryland's all-payment model (APM) replaces fee-for-service hospital payments with regulated global budgets to stabilize finances and restrain costs. Evidence of how this model affects hospital margins and prices relative to similar fee-for-service states remains limited. Objective: To compare trends in hospital financial margins and inpatient prices in Maryland and Massachusetts from 2017 to 2024. We hypothesized that Maryland hospitals would exhibit more stable margins and lower overall price levels than Massachusetts hospitals, under regulated global budgets. Methods: We used hospital-level panel data from the RAND Hospital Cost Report Information System for fiscal years 2017–2024, restricted to acute-care hospitals in Maryland and Massachusetts. The outcomes were total margin and log inpatient revenue per discharge (proxy for price per discharge). A difference-in-differences fixed-effects model with hospital and year fixed effects and standard errors clustered at the hospital level compared changes before and after 2019, when Maryland's Total Cost of Care phase began (md×post2019). Results: At baseline, Maryland hospitals had slightly higher margins and lower prices than Massachusetts hospitals (mean total margin 0.019 vs –0.073; mean log price per discharge 9.27 vs 9.49). After 2019, there was no statistically significant difference in the total margins between Maryland and Massachusetts (β = –0.001, SE = 0.003, p = 0.76). In contrast, log inpatient revenue per discharge grew modestly faster in Maryland, from a lower starting level (β = 0.072, SE = 0.025, p = 0.004), although Maryland prices remained below Massachusetts levels by 2024. Conclusions: Maryland's all-payer global budget system appears compatible with stable hospital margins and a loweroverall price level relative to a benchmark fee-for-service state, but it was not associated with slower post-2019 price growth. Global budgets may support financial stability and moderate price levels, yet they should not be assumed to produce stronger price restraints than well-regulated fee-for-service benchmarks.
Keywords:
Plain Language Summary
1. Introduction
2. Research Questions
3. Literature Review
4. Methods
4.1. Study Design and Analytic Framework
4.2. Data Source and Sample
4.3. Measures
4.3.1. Dependent Variables
4.3.2. Key Independent Variables
4.4. Statistical Analysis
4.5. Sensitivity Analyses and Diagnostics
5. Results
5.1. Sample Characteristics
5.2. Descriptive Comparisons
5.3. Difference-in-Differences Regression
5.4. Interpretation
5.5. Robustness
6. Discussion
6.1. Policy Implications
6.2. Future Research
7. Conclusions
Author Contributions
Funding
Data Citation
Data Availability Statement
Ethical Compliance
Ethical approval
Competing Interests
References
- Rajkumar R, Patel A, Murphy K, et al. Maryland's all-payer approach to delivery-system reform. N Engl J Med. 2014;370(6):493-495. doi: 10.1056/NEJMp1314868.
- Sharfstein JM, Gerovich S, Moriarty E, Chin D. An Emerging Approach to Payment Reform: All-Payer Global Budgets for Large Safety-Net Hospital Systems. New York, NY: The Commonwealth Fund; August 2017. Accessed November 19, 2025. Available at: https://www.chhs.ca.gov/wp-content/uploads/2021/10/An-Emerging-Approach-to-Payment-Reform_-All-Payer-Global-Budgets-for-Large-Safety-Net-Hospital-Systems.pdf.
- Beil H, Haber SG, Giuriceo K, et al. Maryland's global hospital budgets: impacts on Medicare cost and utilization for the first 3 years. Med Care. 2019;57(6):417-424. [CrossRef]
- Kilaru AS, Crider CR, Chiang J, Fassas E, Sapra KJ. Health care leaders' perspectives on the Maryland All-Payer Model. JAMA Health Forum. 2022;3(2):e214920. [CrossRef]
- Commonwealth Fund. Hospital Global Budgeting: Lessons From Maryland and Selected Nations. New York: The Commonwealth Fund, June 2024. Accessed November 19, 2025. Available at: https://www.commonwealthfund.org/publications/fund-reports/2024/jun/hospital-global-budgeting-lessons-maryland-selected-nations.
- RAND Corporation. Hospital Cost Report Information System (HCRIS) Data Files. Santa Monica, CA: RAND Corporation; 2025. Accessed November 19, 2025. Available at: https://www.rand.org/pubs/tools/TL303.html.
- Centers for Medicare & Medicaid Services. Maryland All-Payer Model. Accessed October 31, 2025. Available at: https://www.cms.gov/priorities/innovation/innovation-models/maryland-all-payer-model.
- StatsAmerica. State Per Capita Personal Income, 2024. Accessed October 31, 2025. Available at: https://www.statsamerica.org/sip/rank_list.aspx?rank_label=pcpi1.
- California Health Care Foundation. Commissioning Change: Four States' Advisory Boards for Health Care Cost Containment. Oakland, CA: California Health Care Foundation; 2020. Accessed November 19, 2025. Available at: https://www.chcf.org/publications/commissioning-change-four-states-advisory-boards-health-care-cost-containment.
- Song Z, Rose S, Safran DG, Landon BE, Day MP, Chernew ME. Changes in health care spending and quality 4 years into global payment. N Engl J Med. 2014;371(18):1704-1714. [CrossRef]
- Orlando AW, Field RI. Measuring the COVID-19 financial threat to hospital markets. Inquiry. 2021;58: doi:10.1177/00469580211059985.
- Neupane M, Warner S, Mancera A, et al. Association between hospital type and resilience during COVID-19 caseload stress. Ann Intern Med. 2024. [CrossRef]
- Sun L, Abraham S. Estimating dynamic treatment effects in event studies with heterogeneous treatment effects. J Econometrics. 2021;225(2):175–99. [CrossRef]
- Wing C, Simon K, Bello-Gomez RA. Designing difference-in-difference studies: best practices for public health policy research. Annu Rev Public Health. 2018;39:453–469. [CrossRef]
- Zeldow B, Hatfield LA. Confounding and regression adjustment in difference-in-differences studies. Health Serv Res. 2021;56(5):932–41. [CrossRef]
- Health Services Cost Review Commission. Total Cost of Care (TCOC) Model. Accessed November 19, 2025. Available at: https://hscrc.maryland.gov/Pages/tcocmodel.aspx.
- Health Services Cost Review Commission. AHEAD Model. Accessed November 19, 2025. Available at: https://hscrc.maryland.gov/Pages/ahead-model.aspx.

| State | Total margin | Log price per discharge |
|---|---|---|
| MA | –0.0727 | 9.4866 |
| MD | 0.0189 | 9.2713 |
| (1) Total margin | (2) Log price per discharge | |
|---|---|---|
| Maryland × post-2019 | –0.005 | –0.006 |
| (0.004) | (0.006) | |
| For-profit | 0.003 | 0.543*** |
| (0.005) | (0.025) | |
| Government | –0.001 | –0.327** |
| (0.006) | (0.129) | |
| Constant | –0.093*** | 9.448*** |
| (0.004) | (0.004) | |
| Observations | 649 | 662 |
| R² (within) | 0.007 | 0.0068 |
| Fixed effects | Hospital, year | Hospital, year |
| SEs | Clustered by hospital | Clustered by hospital |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



