Submitted:
20 October 2025
Posted:
21 October 2025
You are already at the latest version
Abstract
Securing electronic health records (EHRs) is critical in the modern healthcare landscape, where digital transformation enhances connectivity and data-driven decision-making. This paper introduces a secure framework that integrates voice-based authentication, blockchain technology, and machine learning to protect EHRs, particularly in IoT-enabled, high-frequency wireless communication environments. The new distributed system utilizes blockchain technology to improve the security and integrity of medical records. User verification is achieved through voice authentication, which adds a biometric element as well. A working model was designed to show the system’s feasibility along with a case study on heart health monitoring. Simulated results demonstrated better block creation time, transaction latency, and validation accuracy.
Keywords:
Voice authentication
; Blockchain
; Electronic Health Records
; Wireless Communication
; Data Security
1. Introduction
Extensive electronic health or medical records (EH/MRs) facilitate the retrieval and management of patient documentation by healthcare providers. This modification is associated with the increased utilization of EHRs which require the safeguarding of sensitive medical information. With greater dependence on computers to store sensitive medical information, an increase in information breaches, unauthorized access, identity theft and the erosion of patient privacy becomes a concern. Advanced Protection mechanisms are vital to secure EHRs in the contemporary face of danger to patients’ privacy and trust in the healthcare system. In the past decade, standard username-password combination authentication systems impeded access to EHRs. These methods, however, do have some gaps which include phishing, poor password choices, and the sharing of passwords. Eliminating the requirement of a physical token with a device that can capture biometric features such as fingerprints can improve the security of electronic health records while making it easier for the patients.
Voice verification, a form of biometric authentication, could be invaluable in the medical field. In healthcare, specialists and patients may be identified using voice authentication, which utilizes different speaking characteristics and patterns.
Also, create and construct a decentralized blockchain technology for the management of private health records in the healthcare field.
This study outlines a method for securing electronic healthcare records within the healthcare industry that relies on voice authentication, blockchain and high frequency wireless transmission. The work aims to accomplish several things, but its primary goals are to investigate the viability and efficacy of voice authentication as an extra safeguard for EHRs, to evaluate its influence on user processes and acceptability, and to handle any obstacles and legal concerns. Also used here is AI-powered speech recognition via the Internet of Things. From the two options shown, choose one kind of voice authentication that best suits your needs.
Our discussion of the voice enrolment process, authentication techniques, and security measures used to safeguard the voice biometric data and related EHRs will take us into the technical parts of voice authentication in the sections that follow. We will also provide the results of a thorough usability test that looked at how healthcare providers and patients felt about using the voice authentication system. Finally, the article analyzes the implications of using the fusion of voice identification and blockchain technology in healthcare and outlines the advantages of the proposed approach. With this research we intend to advance work underway to improve the protection and privacy of health data by explaining more about this new framework of security. Under “Evaluation and Execution” we analyze how well and how securely the prototype of our proposed approach was executed, then we assess and execute it.
2. Related Works
The increasing adoption of electronic health and medical records (EHRS/EMRS) has revolutionized the way health service providers access and manage patient data. With this shift, protections have become sensitive medical information considering the risk of unauthorized access, data leaks and identity theft. Traditional security measures such as passwords have proven susceptible to threats such as phishing and weak registration management [1].
To correct these defects, the biometric method pays attention to its reliability and user-friendly. Among them is language authentication as a user - a friendly and secure way to check your identity using your own vocal features [2]. At the same time, blockchain technology provides a decentralized and operational framework that improves data exchange and simultaneously maintains trust and security. It examines the practicality of integrating language authentication into medical work processes, examines user acceptance, and highlights potential regulatory considerations [3]. This approach also includes AI-driven speech recognition, which allows for flexible adaptation of authentication strategies. Usability analysis of health occupation members and patients assesses the effectiveness of the system [4]. Ultimately, we hope to contribute to further development of secure infrastructure for digital health by presenting the possibilities of this integrated approach. These studies provide valuable insight into the benefits and challenges of blockchain implementation in healthcare systems [5].
A recurring problem is the fragmentation of patient files. This is because people are often sourced from multiple providers. This leads to distributed data storage and restricts access to patient history information [6]. As a rule, patients do not continue to control these records due to legal orders of certain jurisdictions or procedural standards. According to HIPAA Health Insurance and Accountability (HIPAA), health service providers have a 60-day window to respond to patient inquiries regarding changes or deletion of records but are not obligated to comply with [7]. Establishing safe and consistent communication between agencies is complicated by including several stakeholders, such as hospitals, doctors, and insurance companies. Decentralization provides improved security and trust in data exchange, but can be ignored if malicious insiders are using access.
Memory limits also provide practical challenges. Medical files such as test results, images, and documents use critical storage space that makes efficient and scalable solutions essential. Despite growing global interest in blockchain, standardization is not sufficient [9]. Many health groups are reluctant to share patient files due to competition concerns, data protection risks, or economic motivations. To facilitate data exchange, trust must be cultivated among all parties. This is extremely important to providing effective care. Without robust protection measures, these systems are susceptible to cyber threats [10]. Extended hacking tools can bypass traditional security protocols and put sensitive health data at risk. Therefore, reliable infrastructure and effective measures are essential [11].
There is also the technical acceptance of human factors in patients and members of health occupations. Some agencies continue to rely on paper-based records, while others strive to protect encryption and access protocols. Resistance is often based on uncertainty or complaints about digital systems. Ethical concerns, particularly concerns about data confidentiality, remain fundamental to patient provider relationships [12]. Ensuring secure access through encryption, user authentication and regular data backups is important to maintaining trust. Nevertheless, concerns regarding data ownership, access control and network scalability should be considered [13]. The integration of asymmetric encryption methods and AI-based monitoring can help improve security and at the same time help to maintain system transparency [14].
3. System Architecture for Electronics Healthcare System
The proposed device is designed up-to-date provide a cozy and decentralized framework for dealing with electronic health information (EHRs) through a blockchain-enabled infrastructure. This structure helps a distributed ledger environment in which a couple of legal entities—along with hospitals, clinics, sufferers, and researchers—can take part in statistics management with defined get right of entry updated privileges.
relying on privacy requirements and operational goals, the device can be carried out as a non-public, public, or consortium blockchain community. every model defines precise regulations for get admission updated control, information sharing, and governance among participating nodes.
The centre additives of the gadget are as follows:
i. consumer Registration and Authentication:
This module manages consumer onboarding and identification verification. It creates and continues virtual identities for patients, scientific staff, and up-to-date. every user undergoes a comfy registration method up-to-date make certain that simplest legal members can get admission updated and interact with the system.
ii. Healthcare provider control
This phase governs the registration and verification of service companies inclusive of updated hospitals, laborious to dataries, and clinics. handiest tested entities can deliver services or up-to-date fitness records. This guarantees the integrity and trustworthiness of companies in the community.
iii. Profile control machine
This face updated handles the advent, update, and tracking of user profiles. patients can manage non-public data and set possibilities, whilst healthcare providers can list qualifications, specializations, and different credentials.
iv. Smart Contracts
Those contracts outline the terms of interplay between specific stakeholders—sufferers, companies, and establishments. They include permissions, information-sharing sees eye up updated, treatment propanediols, and economic agreements. smart contracts make sure that everyone interactions comply with agreed-upon regulations and that execution is automatic and verifiable.
v. Patient data up-to-date manage
This module enforces strict control over who can get entry updated up-to-date patient information. up to dated is granted based on the consent recorded in clever contracts and affected person-defined settings. All transactions are logged on the blockchain for traceability and duty.
vi. Continuous Enhancement and remarks Loop
The architecture supports modular improvements, allowing up to date development based on user remarks, rising threats, and advances in generation. regular updates ensure the device stays comfy and efficient.
vii. Integration and Interoperability Layer
To facilitate collaboration among various additives, this residue guarantees seamless conversation and facts trade. It lets in exceptional system modules updated feature cohesively, bridging gaps among special technologies or structures.
viii. Consumer-Cantered Interfaces
The device emphasizes intuitive and responsive interfaces for both sufferers and healthcare providers. those interfaces help a extensive variety of obligations, up to date having access updated clinical information, managing permissions, and interacting with providers, at the same time as administrative up to dated simplify operations for backend cuspidated.
ix. Scalability and performance Optimization
Up-to-date expanding consumer bases and huge volumes of clinical data, the device is built for scalability. Load balancing, records caching, and optimized algorithms make certain that performance stays high as the network grows.
4. Voice Authentication-Based Identity Management Integrated with Blockchain
Voice authentication, also referred to as voice biometrics, uses unique characteristics of an individual's speech to confirm their identity. Unlike traditional credentials such as passwords or PINs—which are prone to theft, sharing, or forgetting—voice authentication provides a more natural and secure verification method. This approach is especially relevant in scenarios where users need hands-free, secure access, such as in healthcare or high-risk environments.
Advancements in artificial intelligence (AI) and signal processing have significantly improved the accuracy of speech recognition systems. These technologies can now detect, process, and verify voice patterns with high reliability. Within the proposed framework, two types of voice authentication mechanisms are considered:
- High-frequency wireless voice authentication—which uses advanced transmission techniques but may be costlier and slower to deploy.
- AI-powered voice recognition—which integrates directly with IoT and blockchain systems, offering scalability and real-time analysis, though it requires robust integration efforts for secure deployment.
4.1. Benefits and Integration with Blockchain
Integrating voice authentication with blockchain enhances security and trust. While voice serves as the biometric layer, blockchain ensures data immutability, decentralized access control, and auditability. This combination addresses many
The Parameters of Figure 3:
SC – Summary Contact, RC – Registered Contact Administration, PPR – Patient Service Provider Administration challenges in healthcare security, such as unauthorized access, identity fraud, and data tampering. AI-enhanced voice systems are increasingly being used in secure infrastructures. When paired with blockchain, these systems not only verify identity but also maintain a tamper-proof record of authentication events. For example, sensitive health data can be accessed only after a successful voice match, with all access attempts being logged immutably. Moreover, blockchain’s decentralized structure allows the system to operate without a single point of failure, significantly reducing the risk of insider threats or external attacks.
4.2. Key Components of the Integrated System
The requirements of the system are met successfully according to a particular workflow:
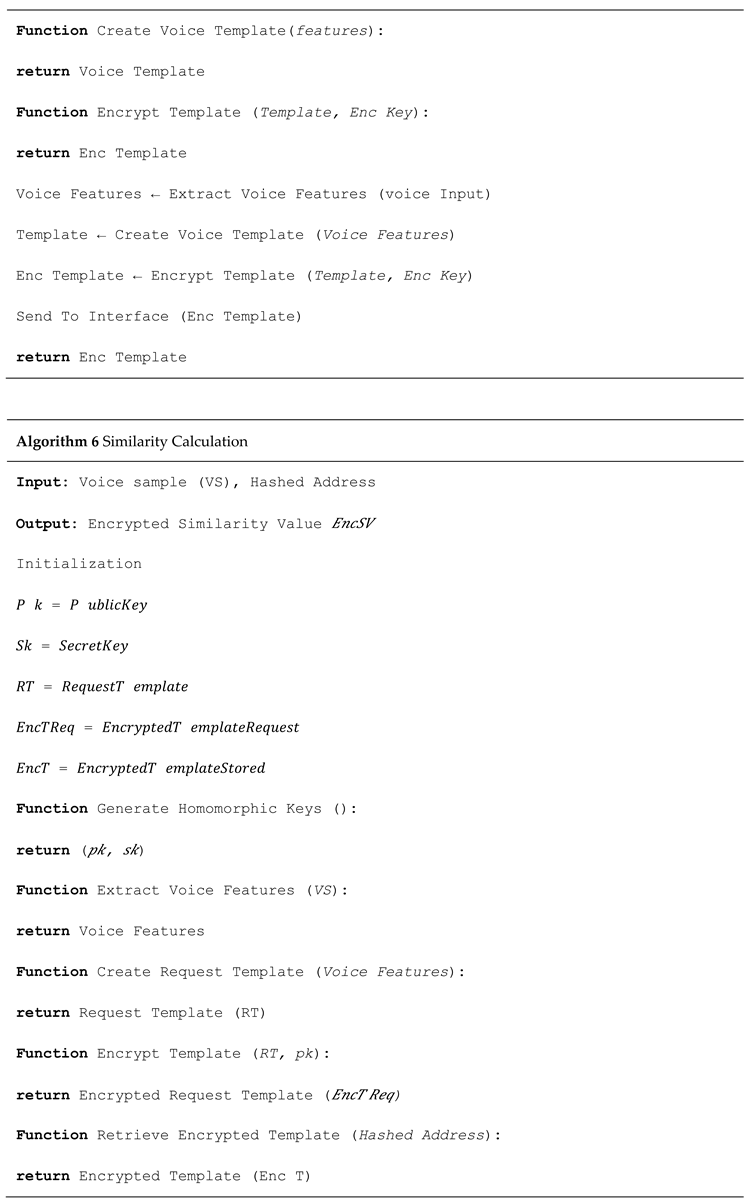
i. The voice enrolment stage deals with capturing voice samples reception and producing the necessary biometric templates, voiceprints. These templates are generated and safeguarded either on the blockchain or through secure off-chain storage that is encrypted and associated with the blockchain.
ii. Voice samples authentication. Standard authentication procedures check whether users utter a certain phrase. Incoming samples are matched against the voiceprint and the system outputs an authentication confirmation event on the blockchain.
iii. Trustless endorsement of systems. Each performed voice authentication process output is stored as a transaction on the blockchain within a bounded verifiable audit trail needed to ensure accountability and traceability.
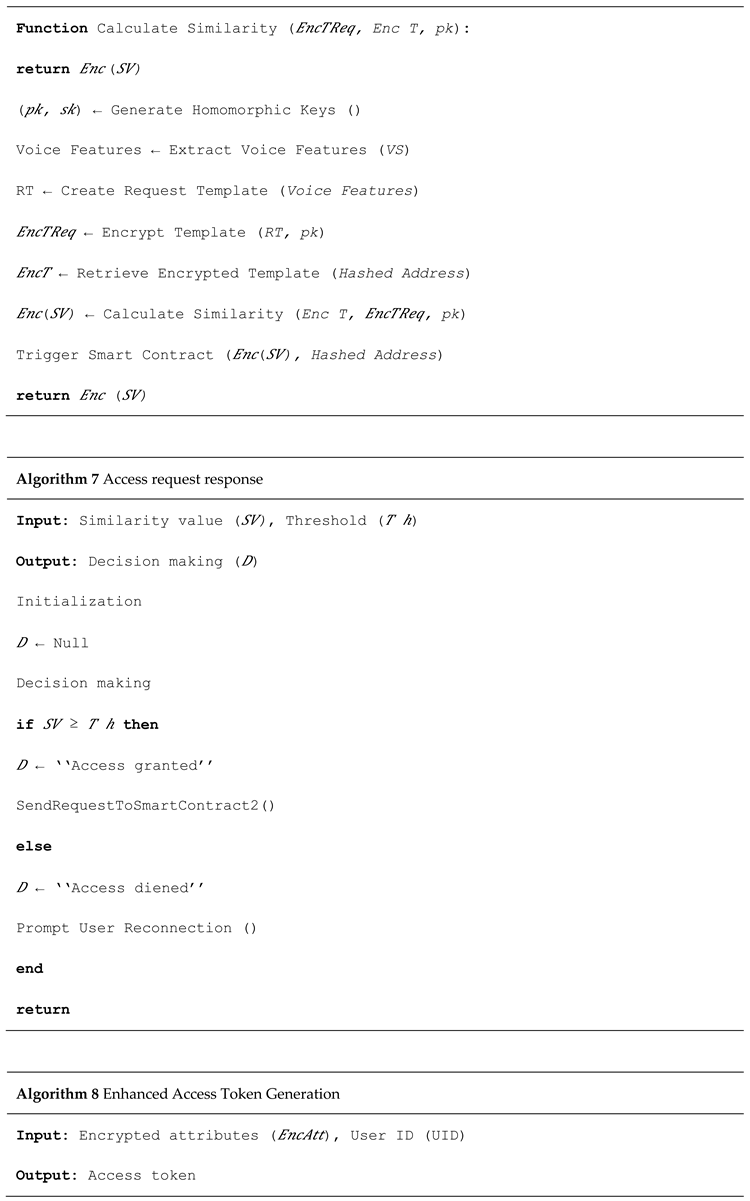
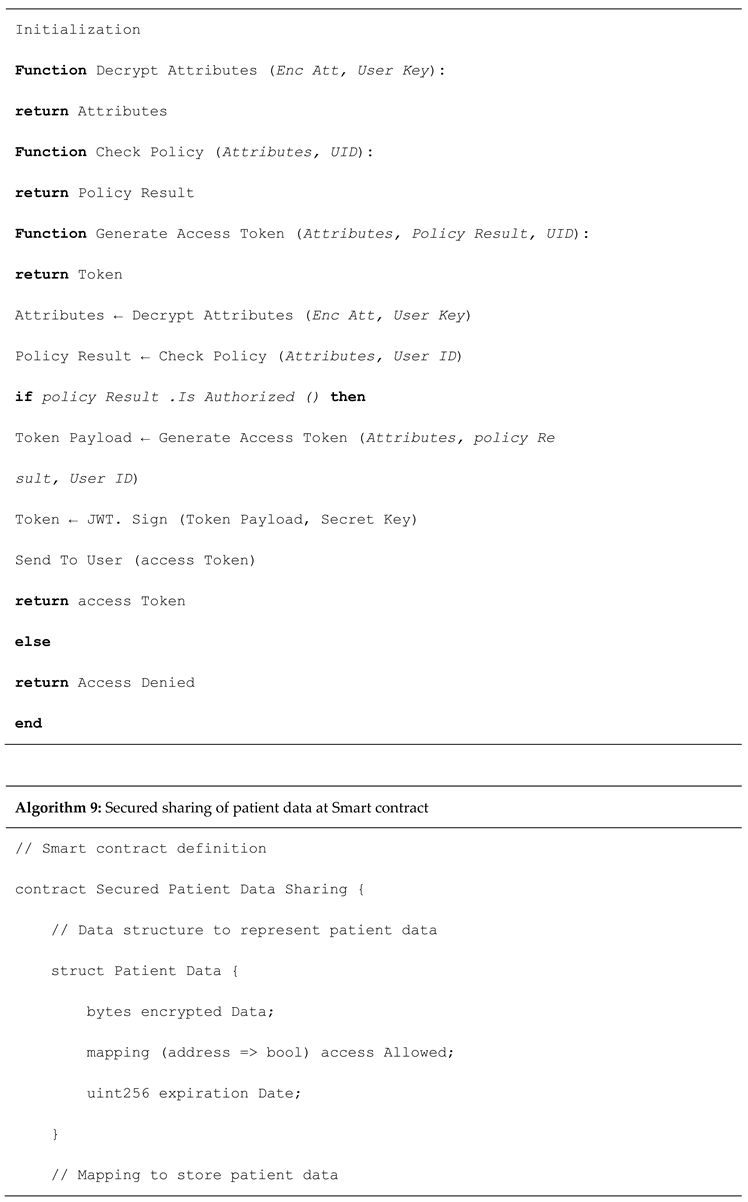
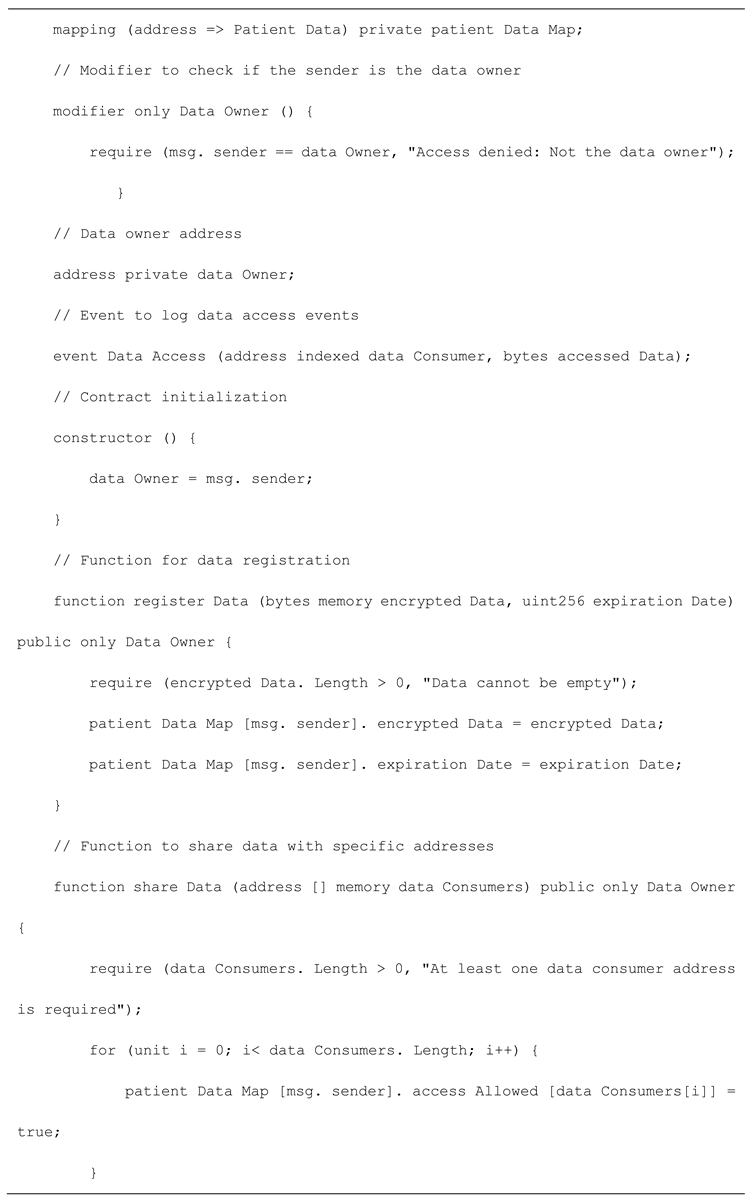
iv. Restriction access via smart contracts: Access Management policies are implemented by way of smart contracts. They setup the rules including who and under which authentication are allowed to access certain data. Voice recognition system can be used to trigger specific operations and authorize certain information da estrelas exchanges.
v. The immutable audit trail is enhanced regardless whether the authentication is successful or not. In addition serves compliance to scrutinize regulations for forensic investigation (actor disputes).
4.3. Security Implications and Use Cases
In healthcare environments, especially those transitioning into smart city infrastructures, digital access points must be rigorously protected. Voice authentication, combined with blockchain, allows for secure gateways to systems such as patient portals, diagnostic data, and remote monitoring tools.
Potential use cases include:
- Hospital record access control
- Secure transmission of sensitive diagnostics
- Voice-activated emergency alert systems
- Access control for wearable or mobile health devices
With the ability to detect anomalies (e.g., voice spoofing attempts or abnormal access patterns), AI-enhanced voice systems can further fortify system integrity. This approach also reduces reliance on vulnerable systems like passwords or smart cards. Phonation of vowels, noises, breathing noises, and counting numbers quickly and slowly are all examples of the voice samples that are collected. Further details included in the metadata include the following: gender, age, location, present health state, and comorbidities if any.
The Figure 4: demonstrates that the epoch loss of the test data is less than that of the training data. The model is successfully generalizing to the testing data when the test and train lines converge toward the end of the graph [20]. The model's ability to adapt to new, unknown data and produce correct predictions is shown by this convergence. The fact that the test and train lines are in perfect alignment shows how reliable the model is and how useful it may be in the real world. We evaluated the speech recognition system's performance using a specific test dataset of one hundred audio files. In this dataset, there were ten audio files total, one for each of the ten speakers included in the training set. We evaluated the system's performance on this test dataset and found it to be 87% accurate. The system correctly identified 100 out of 103 audio files.
4.4. Performance Evaluation and Experimental Findings
4.4.1. Accuracy in testing
Testing specificity, accuracy, and sensitivity are the three metrics used to assess the performance of the developed voice authentication model. They are employs optimization algorithm by Jaya honey badger for the training process of deep neural networks and reasoning aptitude from fuzzy inference systems (DNFN). The DNFN is trained by introduced optimization technique, named hybrid Honey Badger Optimization (JHBO) model for improving the detection performance shortly JHBO-based DNFN [21,22].
The true positive and negative fractions of all audio samples, which are denoted as
ii) Sensitivity: The accurate categorization of voice authentication is assessed by sensitivity, which is defined by
iii) Specificity: The formula for predicting the exact categorization of voice authentication, indicated as
we have ρt is represent as a true positive, ρf is true negative, σf stans for false negative and σt is false positive.
Ac =(ρt+ρf )/(ρt+ρf+σt+σf )
Se = ρf / ( ρf + σt )
Sp=ρt/(ρt+σf)
4.4.2. Machine Learning Optimization and Accuracy
The voice authentication system was enhanced using a hybrid optimization method—Jaya Honey Badger Optimization (JHBO)—applied to a Deep Neuro-Fuzzy Network (DNFN). The JHBO algorithm improves the learning performance by fine-tuning the network's parameters for more accurate predictions.
Test results using a dataset of 100 audio files (10 per speaker) showed that the system achieved an accuracy rate of 87%, correctly identifying 100 out of 103 audio samples.
4.4.3. Evaluation of Performance
The performance study of proposed method with help of JHBO based DNFN is detailed in Table 1 and Figure 5, using a variety of performance indicators and different training data.[23] Figure shows the results of analysing the accuracy of the JHBO-based DNFN that was developed using different iterations [24]. The creation JHBO based DNFN technique is achieved testing accuracy of 0.9757, 0.9763, 0.9851, 1.014, and 1.0276 with iterations 25, 45, 65, 85, and 115, respectively, compared to 85% training data. Figure 5: also shows the results of an investigation of the sensitivity of many iterations of a JHBO-based DNFN that was developed. With iterations 25, 45, 65, 85, and 115, the sensitivity of the proposed method is introduced by JHBO-based DNFN. The values are 0.975, 0.9873, 1.0105, 1.0207, and 1.0215, respectively. Figure 5, shows the results of an investigation to developed JHBO based DNFN method across several iterations with respect to specificity. For iterations 25, 45, 65, 85, and 110, the specificity of the developed JHBO-based DNFN is 0.974, 0.985, 0.998, 1.067, and 1.020, respectively, when the training data is 85%.
4.4.4. Comparative Analysis with Existing Techniques
To assessing the proposed approach's performance, the current voice authentication approaches are taken into consideration, including MFCC or Mel-frequency cepstral coefficients [25], HMM (Hidden Markov mode) [26], Gaussian Mixture Model (GMM) [27].
In this part, we can see how different performance metrics were used to compare the designed JHBO driven DNFN with data (training) and k-fold values shown in table 2 and 3. Predicted from other method, a proposed method using DCNN kernel A DNFN K-fold fusion protein based on JHBO Verifying precision 0.9176, 0.9005, 0.8806, 0.8894. A sensitivity of 0.8982, 0.8816, 0.8938, an alpha of 0.9307 Findings with a high degree of certainty (0.9125, 0.8926, 0.9014, 0.9219) Information used for training Accuracy of testing: 0.8959, 0.8910, 0.8901, 0.9151 In terms of specificity, we have 0.902 0.8896 0.8932 0.9182 and a sensitivity of 0.9123 0.8868 0.9001 0.9218.
The performance measures and the designed proposed method using JHBO-based DNFN are compared in table 2. The results of a comparison study of JHBO-driven DNFN that were introduced for assessing accuracy with different values of k-fold. In terms of k-fold value, MFCC, HMM, and GMM all achieve testing accuracy of 0.8925, with MFCC coming in at 0.887, and the proposed JHBO-based DNFN reaching 0.9054.
A comparison of the sensitivity of JHBO-based DNFN with different k-fold values for k-fold value, MFCC, HMM, and GMM have sensitivity values of 0.8912, 0.878, and 0.8816, respectively; in contrast, created proposed method using JHBO-based DNFN has a sensitivity of 0.9085.

Table 2.
Comparative Performance with Other Methods.
| Metric | MFCC | HMM | GMM | Proposed (JHBO-DNFN) |
|---|---|---|---|---|
| Accuracy | 0.8956 | 0.8910 | 0.8910 | 0.8979 |
| Sensitivity | 0.885 | 0.8831 | 0.8813 | 0.9107 |
| Specificity | 0.9164 | 0.8963 | 0.9031 | 0.9221 |
In a k-fold analysis, the proposed method continued to show superior performance:
| Metric | MFCC | HMM | GMM | Proposed |
| Accuracy | 0.9176 | 0.9005 | 0.8806 | 0.9394 |
| Sensitivity | 0.8982 | 0.8816 | 0.8938 | 0.9307 |
| Specificity | 0.9125 | 0.8926 | 0.9014 | 0.9312 |
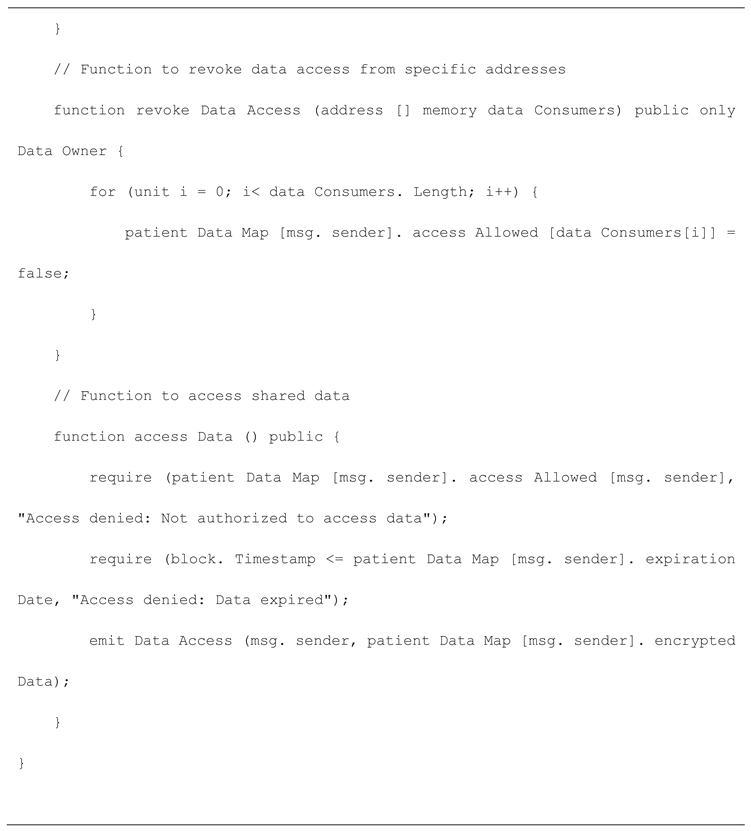
5. New Patient's Record Is Added by the Provider via System Administration Using Proposed Method
It makes sure that the system nodes can connect to pre - existing EMR systems. It interprets it as meaning that many nodes, mainly healthcare providers, already reliably operate databases on servers connected to the internet. Backend Library, Database Gatekeeper, Ethereum Client, and EMR Manager are the four components that our architecture presents.
It can run these components on servers and combine them to form a distributed type of system that functions. An online user interface and integration with use of SQLite database are the hallmarks of prototype implementation of these components. The modular protocol, defined by proposed blockchain contracts to allows any provider's backend. The user interface is implemented to participate in the system.
In this system, both providers and patient nodes contain the same fundamental components. Any desktop, laptop, or even a cell phone can run these components. They may use their local database, which is only one of several small database implementations. All the databases need to do is act as a temporary repository for the patients' medical records. If follow the steps in the node's summary contract, you can get missing data back from the network whenever you need it. The first is the backend library, which build to help the system run. It's a collection of tools that put together. The library hides the details of blockchain interactions by exposing a functional API. So, the record management apps and their user interfaces won't have to deal with the blockchain's complexities. Making sure the network confidently accepts every transaction is one such challenge. When it comes to mining and discarding transactions, the library takes care of the uncertainty automatically. When using an Ethereum client, the backend library may practice the protocol's low-level formatting and parsing. Details discuss how a new patents records added explain in [28].
The proposed architecture integrates voiceprint-based access control and blockchain technology to manage Electronic Health Records (EHRs) securely and transparently. The system utilizes provider nodes, Ethereum smart contracts (via the MedRec framework), and a distributed ledger to facilitate secure interactions. The end-to-end process is outlined as follows:
- 1.
- Record Initialization:
A new patient record is created and updated within the local database by the EHR Manager at the provider node. This event triggers the initialization of a blockchain transaction.
- 2.
- Smart Contract Association:
The system resolves the appropriate blockchain address and identifies the corresponding smart contract (SC). A new Patient-Provider Relationship (PPR) is posted to the blockchain. The smart contract is then linked to the newly created PPR.
- 3.
- Mining and Validation:
The transaction is broadcast to the blockchain network, where it is processed and validated by a miner. Upon successful mining, the miner receives an incentive or bounty for contributing to the consensus mechanism.
- 4.
- Smart Contract Update:
post-validation, the smart contract is updated to reflect the new record association and access permissions, as specified in the PPR metadata.
- 5.
- Notification Dispatch:
A notification is sent to relevant stakeholders or subsystems indicating the successful update of the EHR and its associated permissions on the blockchain.
- 6.
- PPR Status Synchronization:
The status of the PPR is updated within the smart contract to reflect its current state (e.g., pending, approved, or completed), ensuring consistent access control enforcement.
- 7.
- Query Processing:
When a provider node requires access to a patient’s health record, it initiates a query request. This request is sent to the blockchain network for verification.
- 8.
- Permission Verification:
The MedRec service within the Ethereum client evaluates the query by verifying access permissions embedded in the smart contract. If access is authorized, the requested EHR data is retrieved and returned to the provider node.
- 9.
- Database Update and Acknowledgment:
Based on the query response, the EHR Manager updates the local database accordingly. The system then provides a final acknowledgment or rejection, depending on the outcome of the access verification and data retrieval process.
This process ensures a decentralized, auditable, and secure mechanism for managing EHR access using blockchain technology while incorporating biometric voiceprint authentication for enhanced identity assurance and privacy control.
6. Assessment and Development
We shift to the use case scenario of patient support management in a smart city to describe the suggested architecture more clearly, as well as its integration with blockchain technology, and assess its viability and shown in Figure 4. Say there are three service providers engaged in a joint initiative for patient support management within the framework of our system. The to supervise the whole process and control the trash can sensors; Different groups are responsible for the sensors and equipment that capture related data. Individual information may have more than one profile since it can engage in different services. They are each regarded as their information within the system. Because the services' intelligent judgments are dependent on the huge amounts of data that are continuously gathered from the network resources, reliability and availability are crucial in this size of IoT application.
 |
 |
 |
 |
 |
 |
 |
 |
 |
6.1. System Prototype Implementation with Blockchain and Voice Authentication
To demonstrate the practical viability of the proposed model, a prototype was implemented and evaluated using a case study focused on heart health monitoring. The implementation integrates voice-based user authentication, high-frequency wireless data transmission, and blockchain-backed data integrity.
The developed system architecture comprises several essential components:
- Backend Library – Provides abstraction over blockchain interactions.
- Database Gateway – Manages temporary patient data storage.
- Ethereum Client – Facilitates blockchain transactions.
- EMR Manager – Connects the system with existing Electronic Medical Record (EMR) databases.
Each node—whether a healthcare provider or a patient—hosts a local version of these components. They can run on lightweight devices like laptops or smartphones, using SQLite or similar embedded databases to temporarily store records. The blockchain acts as the central ledger to verify and synchronize data across all nodes. Smart contracts are employed to enforce access policies and automate permissions. The system interface is web-based, developed using Flask and JWT (JSON Web Token) libraries for secure user authentication and session control. This modular design allows seamless integration with any healthcare provider’s digital infrastructure.
6.2. Environment for Experiments
We evaluated our approach by simulating the use case scenario for waste management from the prior section. As an example, each business in the simulated group of three companies collaborating on distinct services was able to register genuine hardware as assets and create JSON Tokens that complied with the access control specifications. The results of our study are based on two distinct types of locally stored (offline) data; for the second, we use the huge chain-DB online test node stores, and for the initial, Docker technology is used. The experiment's multiple components use RESTful APIs to communicate data. We created our prototype employing the programming language Python, the FLASK micro-online structure, plus the JWT Crypto Libraries to evaluate the performance of our proposed access control strategy. The execution environment is a virtual computer operating Ubuntu with 8 GB of Memory and a single Intel Core i5-4510U 2.00 GHz CPU. Additionally, parallel registration and authentication requests were modelled using Apache JMeter.
6. Results and Discussion
To evaluate the practical performance of the proposed voice-authenticated blockchain healthcare system, a simulation environment was developed using Network Simulator 3 (NS-3). This platform was chosen due to its flexibility and the availability of libraries tailored for blockchain-based network configurations. The simulation replicated a vehicular communication network context, adapted for healthcare data transmission scenarios.
The rate at which new transactions are uploaded to a blockchain is known as throughput. The calculation below may be used to calculate the average throughput.
Ai: is the total amount of operations for the ith trial, Bci: is the transaction dedicated time, and n is the total amount of trials conducted.
The processing time, also known as latency, is the interval between when a transaction is submitted and when it is carried out. These steps are used to compute the latency (L).
where: Bsi: When is the transaction deadline for the first trial,
Throughput and latency data for the two blockchain systems (existing system and suggested technique) are compared. The estimated throughput for the existing and suggested systems were (17.6756 and 16.4736, respectively), based on Equation (4). These two findings demonstrated that the suggested system increased overhead by 3.806%. The latency values of the two systems—the proposed system and the existing system—were (0.00191 and 0.00471, respectively) based on Equation (5). The latency of the baseline and suggested systems was too low for comparison.
- i.
- Throughput Analysis: As illustrated in the simulation (Figure 6.14), the proposed system achieved higher throughput compared to PoW, DTC, and VBCA. This performance gain is attributed to the optimized consensus selection process and the use of stationary "leader" nodes that minimize wait times for block confirmation. While PBFT demonstrated competitive throughput due to its private network nature, it lacks the scalability and flexibility offered by the proposed hybrid system.
- ii.
- Transaction Delay Analysis:Figure 6.15 shows that the proposed model also significantly reduces transaction latency compared to PoW and DTC. This is because, unlike traditional blockchain approaches that require network-wide agreement for every transaction, the system uses smart contracts and delegated verification to expedite processing. PBFT recorded the lowest delay among the comparison set, as expected from a permissioned network. However, our model balances lower latency with a broader, more scalable architecture.
Figure 7.
Throughput Analysis of Proposed EHR.
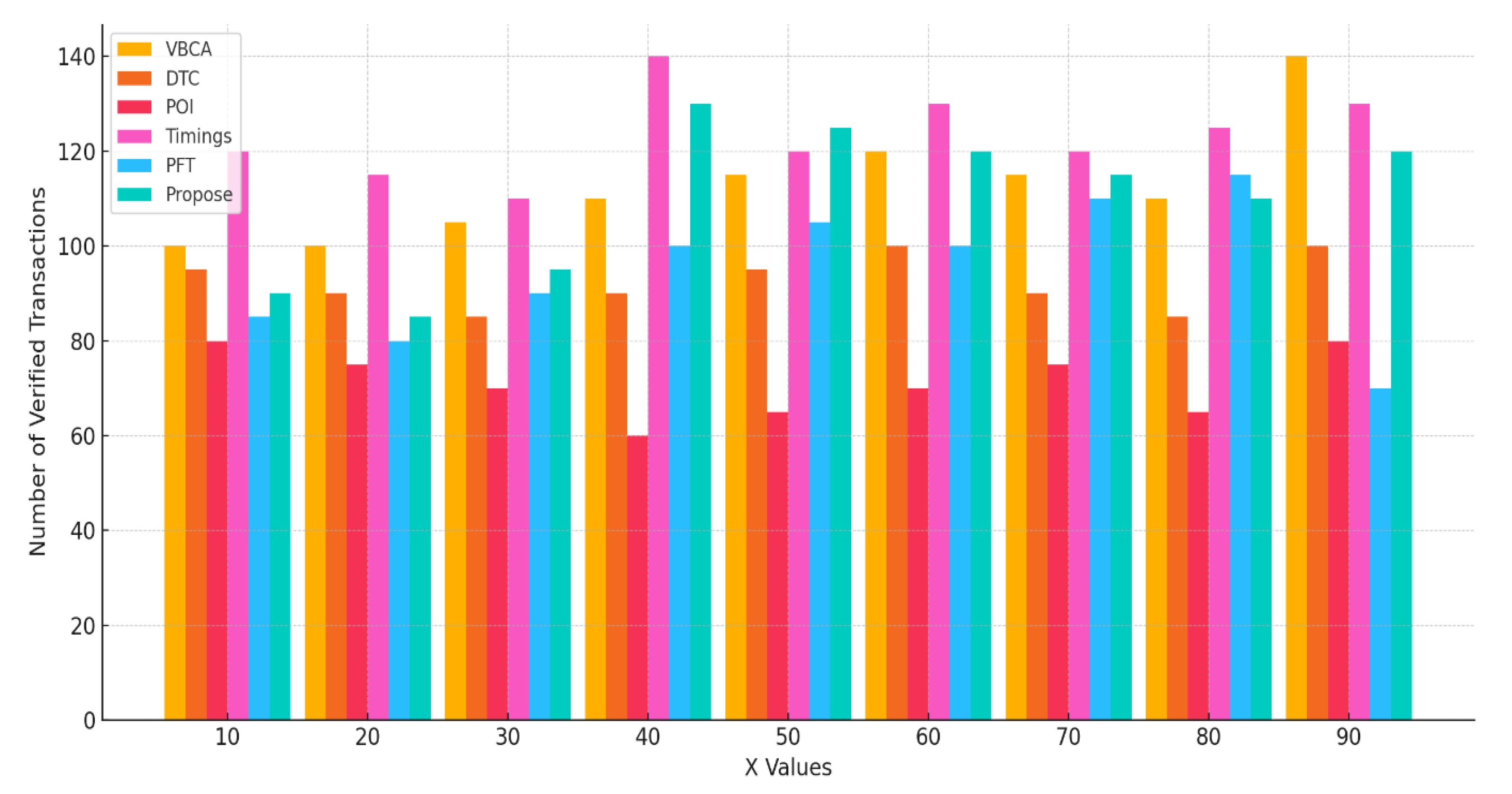
Figure 8.
Delay in transactions (transaction delay) proposed EHR.
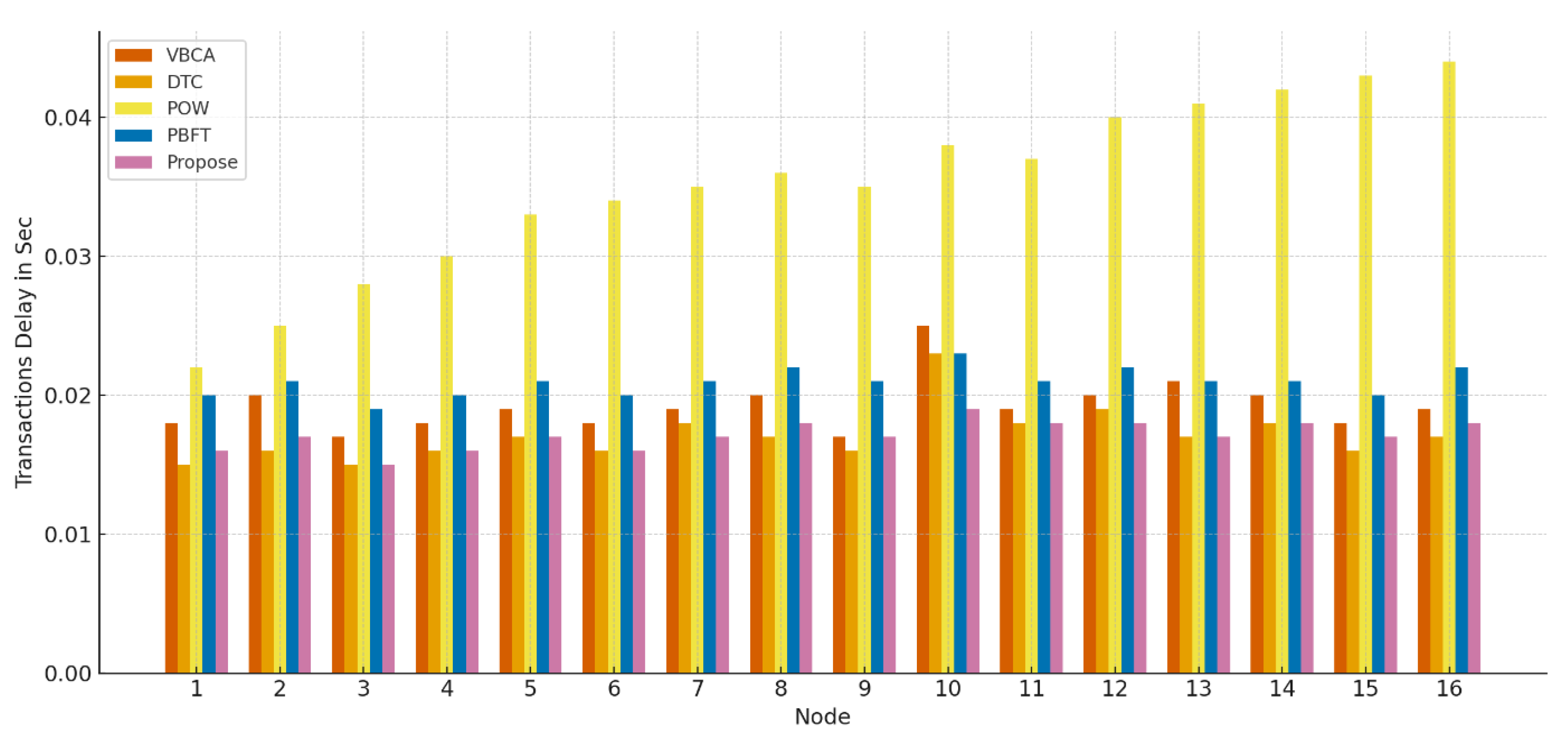
Table 3.
Confusion matrix results for proposed method.
| Test | Positive | Negative | Total |
|---|---|---|---|
| Positive | TP = 44 | FP = 1 | TP+ FP = 45 |
| Negative | FN = 0 | TN = 0 | FN+ TN = 0 |
| Total TP+ FN = 44 FP+ TN = 1 N = 45 | Total TP+ FN = 44 FP+ TN = 1 N = 45 | Total TP+ FN = 44 FP+ TN = 1 N = 45 | Total TP+ FN = 44 FP+ TN = 1 N = 45 |
Table 4.
Performance metrics results: Sensitivity, Specificity, FPR, FNR, FAR, FRR, and Accuracy.
| Metric | Formula | Value |
|---|---|---|
| Sensitivity or True Positive Rate | TPR = TP / (TP + FN) | 0.97 |
| Specificity or True Negative Rate | TNR = TN / (TN +FP) | 0 |
| False Positive Rate | FPR = FP /(FP +TN ) | 1 |
| False Negative rate | FNR = FN /(FN+TP ) | 0 |
| False Acceptance Rate | FAR = FP /Number of Attempts | 0.022 |
| False Rejection | Rate FRR = TN /Number of Attempts | 0 |
| Accuracy | (TP +TN) /N | 97.78% |
8. System Implementation and Case Study: Heart Monitoring with Blockchain and Voice Authentication
To display the practical feasibility of the proposed model, a prototype was applied and evaluated using a case study cantered on cardiac health monitoring. The implementation integrates voice-based user authentication, high-existing wireless data transmission and blockchain-supported data integrity.
8.1. Prototype Implementation
The developed system architecture comprises several essential components:
- Backend Library – Provides abstraction over blockchain interactions.
- Database Gateway – Manages temporary patient data storage.
- Ethereum Client – Facilitates blockchain transactions.
- EMR Manager – Connects the system with existing Electronic Medical Record (EMR) databases.
Each node—whether a healthcare provider or a patient—hosts a local version of these components. They can run on lightweight devices like laptops or smartphones, using SQLite or similar embedded databases to temporarily store records. The blockchain acts as the central ledger to verify and synchronize data across all nodes. Smart contracts are employed to enforce access policies and automate permissions. The system interface is web-based, developed using Flask and JWT (JSON Web Token) libraries for secure user authentication and session control. This modular design allows seamless integration with any healthcare provider’s digital infrastructure.
8.2. Case Study: Secure Heart Monitoring System in a Smart City Framework
In case study scenarios, the system is used to develop a secure real- time cardiac monitoring solution. The goal is to continuously collect and transmit cardiac data, while simultaneously using voice recognition to ensure data protection and patient authentication. To prevent unauthorized access, check your identity regularly.
Key System Components:
- o
- High-Frequency Wireless Communication: Supports rapid, encrypted transmission of sensor data over IoT networks.
- o
- Heart Monitoring Device: A wearable sensor collects real-time metrics such as heart rate and rhythm.
- o
- Voice Authentication Module: Verifies the identity of the user periodically or at login to prevent unauthorized access.
- o
- Blockchain Network: Stores encrypted health data in a decentralized manner, ensuring tamper resistance.
- o
- Data Analysis Engine: Detects abnormalities and triggers alerts for critical conditions.
- o
- User Interface (UI): Provides access to health records for patients and medical professionals with role-based controls.
8.3. System Workflow
The operational flow of the heart monitoring system is as follows:
- o
- User Enrolments: A user registers via a mobile app and provides a voice sample, which is encrypted and stored on the blockchain.
- o
- Device Pairing: The wearable heart monitoring device is connected to a user’s smartphone using wireless protocols like Bluetooth.
- o
- Data Collection: The device gathers and transmits vital signs at defined intervals.
- o
- Voice Authentication Checkpoint: At predefined intervals or during sensitive operations, users must authenticate through voice input.
- o
- Secure Data Logging: Authenticated health data is encrypted and appended to the blockchain ledger, maintaining an immutable audit trail.
- o
- Health Data Analysis: AI-driven analysis tools evaluate the collected data to identify irregularities and suggest interventions if necessary.
- o
- User Interaction: Patients and clinicians access historical data, live metrics, and alerts through the application dashboard.
8.4. Benefits of the Proposed System
- Security: Combines voice biometrics and blockchain for dual-layered protection.
- Data Integrity: Blockchain ensures that data remains tamper-proof and traceable.
- Privacy Control: Patients retain ownership and control over who accesses their medical information.
- Real-Time Monitoring: Continuous data collection allows early detection of cardiovascular issues.
- Scalability: The system is built to handle a growing number of users and data without performance degradation.
- User Experience: Intuitive interfaces and automated authentication simplify daily use for patients and providers.
This case study validates the effectiveness of integrating modern technologies such as blockchain and voice authentication in a healthcare setting. It highlights not only the feasibility of real-time health monitoring but also the importance of maintaining trust, security, and usability in sensitive digital health ecosystems.
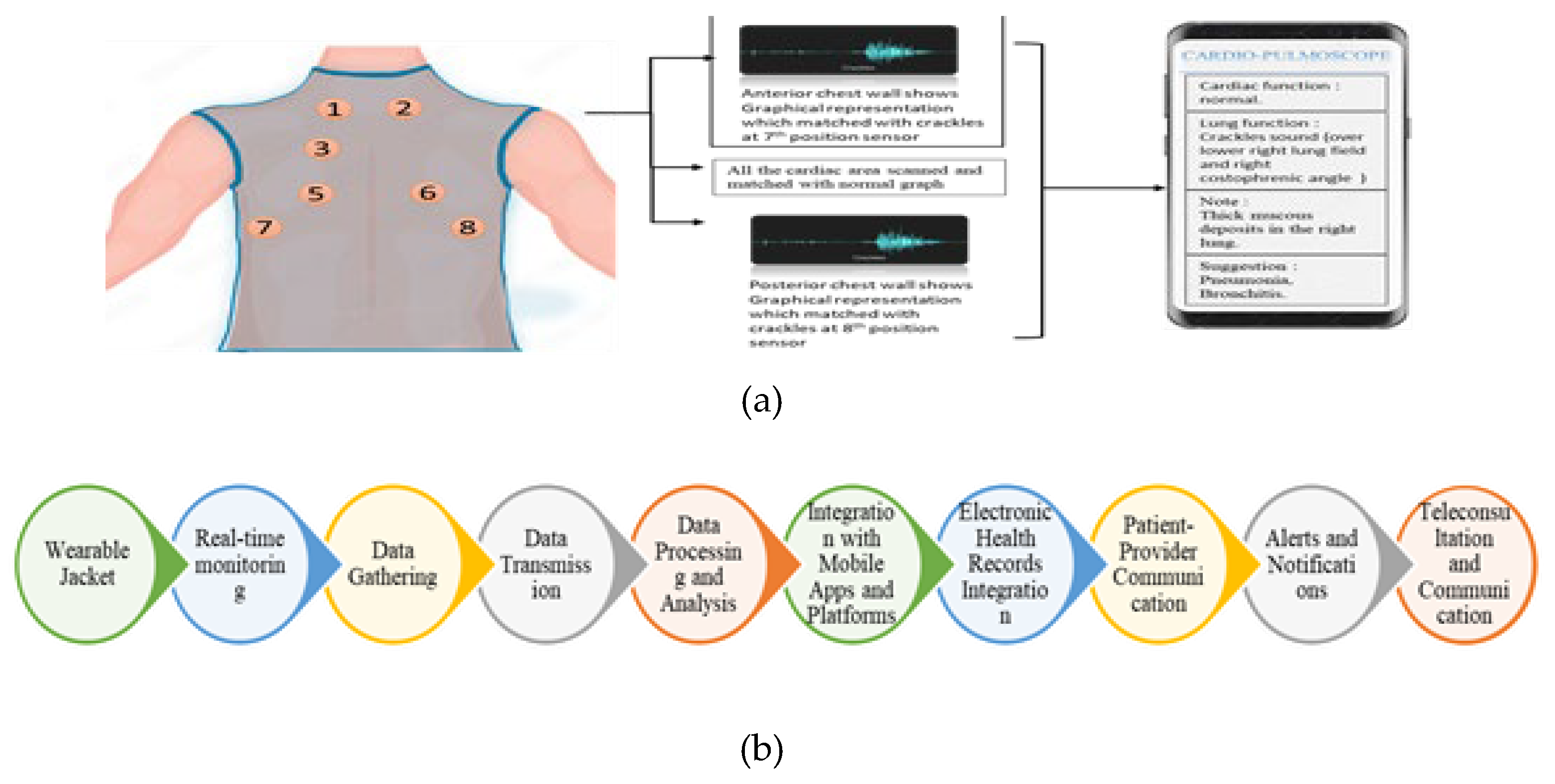
Figure 5.
(a) Proposed model and working principle of Heart monitoring system (a lightweight jacket with attached sensor). (b) Block representation of Heart monitoring system
Figure 5.
(a) Proposed model and working principle of Heart monitoring system (a lightweight jacket with attached sensor). (b) Block representation of Heart monitoring system
10. Conclusion
In this article, a voice authentication-based patient health information system linked with blockchain based secured healthcare system has been proposed. Voice authentication has several benefits over conventional forms of authentication like passwords or biometrics, It Enhances Security, User-Friendly Experience, Non-Intrusiveness, and Strong authentication are some of the main advantages of using voice authentication to secure electronic health records. Finally, the voice authentication-based blockchain network shows enormous potential to secure and efficiently handle the healthcare ecosystem. The proposed combination provides robust security, user-friendliness, and regulatory compliance. Expanded use of high frequency wireless communication-based voice authentication of the healthcare records will be possible with continued investment in health care sector and continuous advancements in blockchain technology. In the ever-changing healthcare business, voice authentication with blockchain has great potential to be an essential tool for protecting patient information and maintaining the trust and privacy that are fundamental to contemporary healthcare system.
References
- Ratta, P.; Kaur, A.; Sharma, S.; Shabaz, M.; Dhiman, G. (2021) “Application of blockchain and internet of things in healthcare and medical sector: Applications, challenges, and future perspectives.” In Journal of Food Qual. 2021(7608296). [CrossRef]
- Reegu, F.A.; Al-Khateeb, M.O.; Zogaan, W.A.; Al-Mousa, M.R.; Alam, S.; Al-Shourbaji, I. (2021) “Blockchain-based framework for interoperable electronic health record.” Ann. Rom. Soc. Cell Biol. 30: 6486–6495.
- Nazir, S.; Ali, Y.; Ullah, N.; García-Magariño, I. (2019) “Internet of things for healthcare using effects of mobile computing: A systematic literature review”. Wirel. Commun. Mob. Comput. 1315.
- Bamakan, S.M.H.; Moghaddam, S.G.; Manshadi, S.D. (2021) “Blockchain-enabled pharmaceutical cold chain: Applications, key challenges, and future trends.” J. Clean. Prod. 302 (127021).
- Makridakis, S.; Polemitis, A.; Giaglis, G.; Louca, S. (2018) “Blockchain: The next breakthrough in the rapid progress of AI. Artif. Intell.-Emerg.” Trends Appl. 27(10).
- Abunadi, I.; Kumar, R.L. (2021) “Blockchain and business process management in health care, especially for COVID-19 cases.”Secur. Commun. Netw: 2021(2245808).
- Bindlish, S.; Chhabra, S.; Mehta, K.; Sapra, P. (2022) “Blockchain in Health Care: A Review.” Cyber Security. Digit. Forensics. 122: 423–430.
- Attaran, M. (2022) “Blockchain technology in healthcare: Challenges and opportunities.” International Journal of Health care Management :15: 70–83.
- Mackey TK, Kuo T, Gummadi B, et al. (2019) “Fit-for-purpose? ’ - challenges and opportunities for applications of blockchain technology in the future of healthcare.” BMC Med. Mar 27;17(1):68.
- Hoy, MB. (2017) “An introduction to the blockchain and its implications for libraries and medicine. Med Ref Serv Q. ;36(3):273–279.
- Yaeger K, Martini M, Rasouli J, et al. (2019) “Emerging blockchain technology solutions for modern healthcare infrastructure.” J Sci Innov Med. 9(9):2–7.
- Roehrs A, da Costa CA, da Rosa Righi R. (2017) “OmniPHR: a distributed architecture model to integrate personal health records.” J Biomed Inform.; 71:70–81.
- Peterson K, Deeduvanu R, Kanjamala P, et al. (2020)“A blockchain-based approach to health information exchange networks.” Mayo Clinic.
- Ichikawa D, Kashiyama M, Ueno T. (2023) “Tamper-resistant mobile health using blockchain technology.” JMIR MhealthUhealth. ;5(7):134–144.
- [11] Zheng, Y. and Zhao, S. (2016) A Usable Authentication System Based on Personal Voice Challenge. 2016 International Conference on Advanced Cloud and Big Data (CBD), IEEE, Chengdu, 3-16 August 2016, 194-199.
- Aizat, K. , Mohamed, O., Orken, M., Ainur, A. and Zhumazhanov, B. (2020) Identification and Authentication of User Voice Using DNN Features and i-Vector. Co- gent Engineering, 7, Article ID, 1751557. [Google Scholar]
- Pal, P. , Sahana, B.C., Ghosh, S., Poray, J., Mallick, A.K. (2021). Voice Password-Based Secured Communication Using RSA and ElGamal Algorithm. In: Panigrahi, C.R., Pati, B., Pattanayak, B.K., Amic, S., Li, KC. (eds) Progress in Advanced Computing and Intelligent Engineering. Advances in Intelligent Systems and Computing, vol 1299. Springer, Singapore. [CrossRef]
- Lv, Z. , Qiao, L., Kumar Singh, A. and Wang, Q. (2021) AI-Empowered IoT Security for Smart Cities. ACM Transactions on Internet Technology, 21, 1-21. [CrossRef]
- Rashid, J. , Teh, Y.W., Memon, N.A., Mujtaba, G., Zareei, M., Ishtiaq, U., Akhtar, M.Z. and Ali, I. (2020) Text-Independent Speaker Identification through Feature Fusion and Deep Neural Network. IEEE Access, 8, 32187-32202.
- Dibaei, M. , Xia, Y., Xu, X., Jolfaei, A., Bashir, A.K., Tariq, U., Yu, D. and Vasilakos, A.V. (2022) Investigating the Prospect of Leveraging Blockchain and Machine Learning to Secure Vehicular Networks: A Survey. IEEE Transactions on Intelligent Transportation Systems, 23, 683-700. [CrossRef]
- Jawad Ahmad Dar, Kamal Kr. Srivastava, Sajaad Ahmed Lone, Spectral features and optimal Hierarchical attention networks for pulmonary abnormality detection from the respiratory sound signals, Biomedical Signal Processing and Control, Volume 78, 2022, 103905, ISSN 1746-8094. [CrossRef]
- Jawad Ahmad Dar, Kamal Kr Srivastava, Sajaad Ahmed Lone, Design and development of hybrid optimization enabled deep learning model for COVID-19 detection with comparative analysis with DCNN, BIAT-GRU, XGBoost, Computers in Biology and Medicine, Volume 150, 2022, 106123, ISSN 0010-4825. [CrossRef]
- Dar, J.A. , Srivastava, K.K. & Lone, S.A. Fr-WCSO- DRN: Fractional Water Cycle Swarm Optimizer-Based Deep Residual Network for Pulmonary Abnormality Detection from Respiratory Sound Signals. SN COMPUT. SCI. 3, 378 (2022). [CrossRef]
- Ponnupilla Omana S, Dar JA, Rajesh Kumar T, Sampath AK, Sharma S. Henry gas bird swarm optimization algorithm-based deep learning for brain tumor classification using magnetic resonance imaging. Concurrency Computat Pract Exper, 2023; 35(4):e7541. [CrossRef]
- Song, Z. , Ma, L. (2024). Speech Command Recognition Algorithm Based on Improved MFCC Features. In: Wang, W., Liu, X., Na, Z., Zhang, B. (eds) Communications, Signal Processing, and Systems. CSPS 2023. Lecture Notes in Electrical Engineering, vol 1032. Springer, Singapore. [CrossRef]
- Chen, Yinchun. "A hidden Markov optimization model for processing and recognition of English speech feature signals" Journal of Intelligent Systems, vol. 31, no. 1, 2022, pp. 716-725. [CrossRef]
- Ankur Maurya, Divya Kumar, R.K. Agarwal, Speaker Recognition for Hindi Speech Signal using MFCCGMM Approach, Procedia Computer Science, Volume 125, 2018, Pages 880-887, ISSN 1877-0509. [CrossRef]
- Pal P,Sahana B C and Poray J (2023) “Secured Information Transfer Power by Modified and Optimized RSA Cryptosystem”, Easy Chair Preprint no. 1 0318.
- Sehar, N.u. , Khalid, O., Khan, I.A. et al. (2023) “Blockchain enabled data security in vehicular networks”. Sci Rep 13(4412). [CrossRef]
- Shrestha, R. , Bajracharya, R. & Shrestha, A. P. (2020) “A new type of blockchain for secure message exchange in VANET”. Digit. Commun. Netw. 6(2), 177–186.
- [Chai, H. , Leng, S., Zeng, M. & Liang, H. (2019) “A Hierarchical blockchain aided proactive caching scheme for internet of vehicles”. In IEEE International Conf. on Communications (ICC).
- Dorri, A. , Kanhere, S. S., Jurdak, R. & Gaurava, P. (2019) “LSB: A lightweight scalable blockchain for IoT security and anonymity.” Journal of Parallel Distributing Computer. 134(7), 180–197.
- F.A. Hashim, E.H. F.A. Hashim, E.H. Houssein, K. Hussain, M.S. Mabrouk, W. Al-Atabany, Honey Badger Algorithm: new metaheuristic algorithm for solving optimization problems, Math. Comput. Simulat. 192 (2022) 84–110.
- S. Javaid, M. S. Javaid, M. Abdullah, N. Javaid, T. Sultana, J. Ahmed, N.A. Sattar, towards buildings energy management: using seasonal schedules under time of use pricing tariff via deep neuro-fuzzy optimizer, in: Proceedings of IEEE 15th International Wireless Communications & Mobile Computing Conference, IWCMC), June 2019, pp. 1594–1599.
Figure 1.
System architecture Electronic Health Records System Based on Voice Authentication Management.
Figure 1.
System architecture Electronic Health Records System Based on Voice Authentication Management.
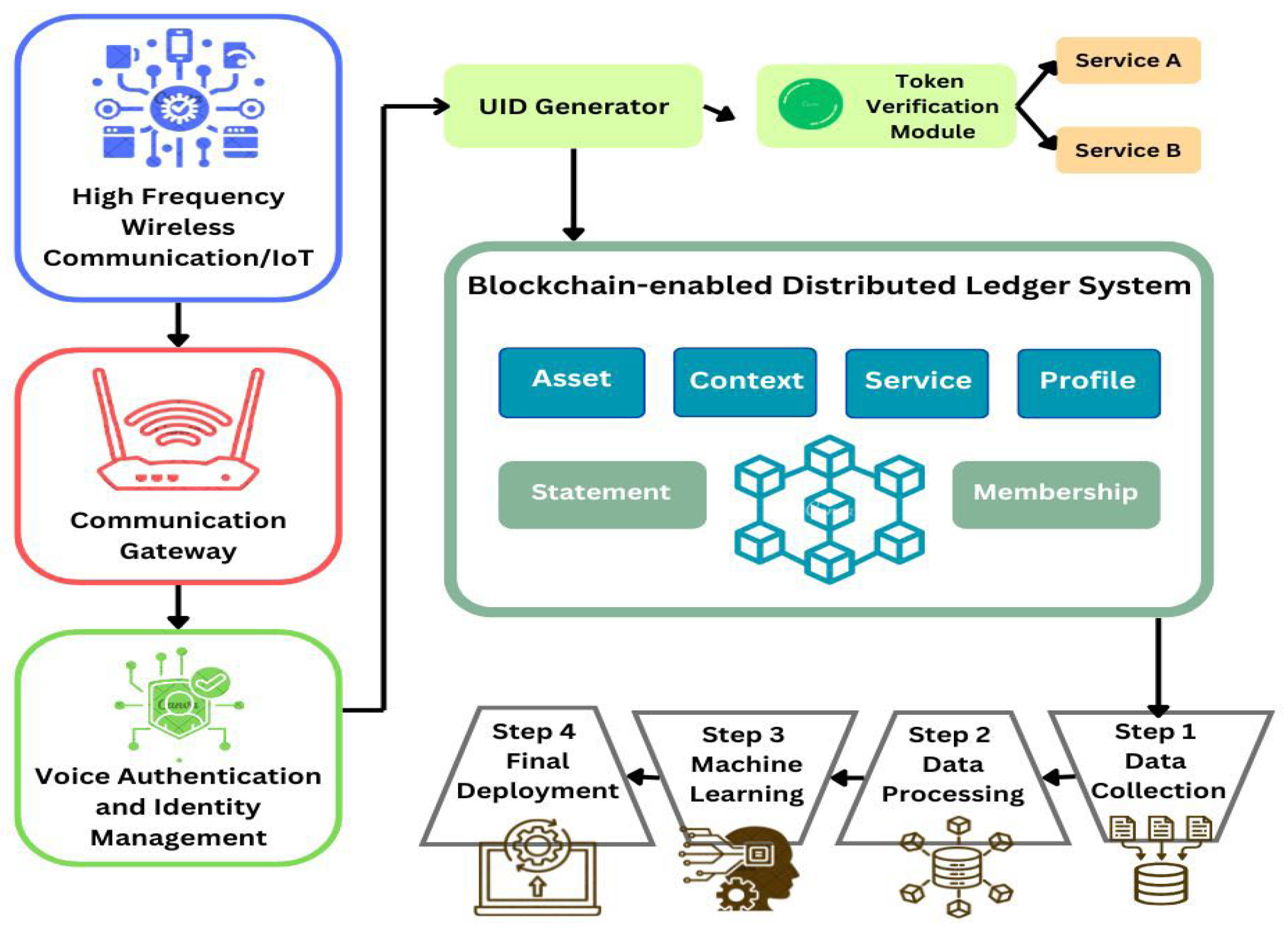
Figure 2.
Modelling how Blockchain work as a Structure for EHR.
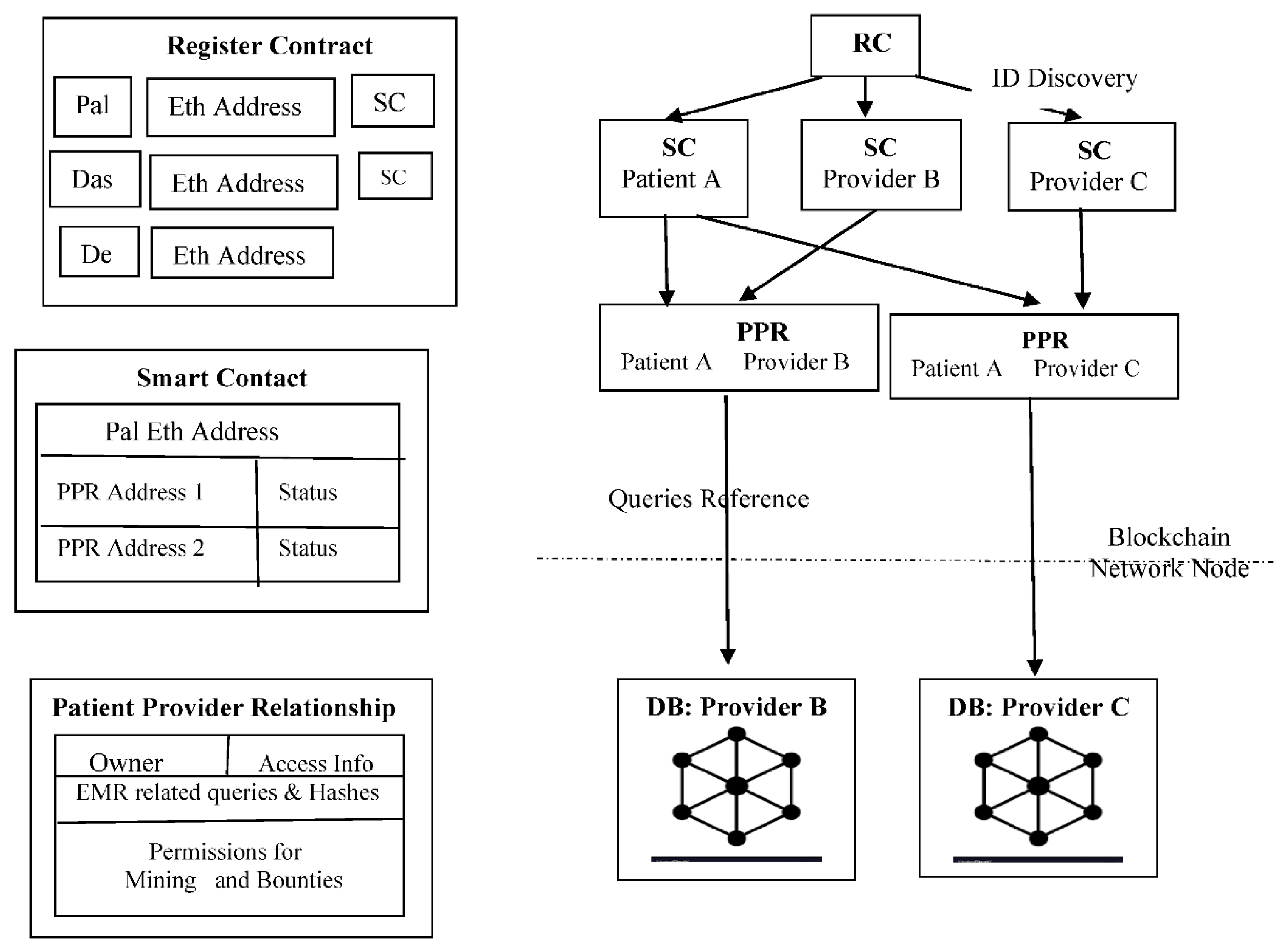
Figure 3.
Block Diagram of identity management system utilizing voice authentication.

Figure 4.
Epoch losses between train data and test data.
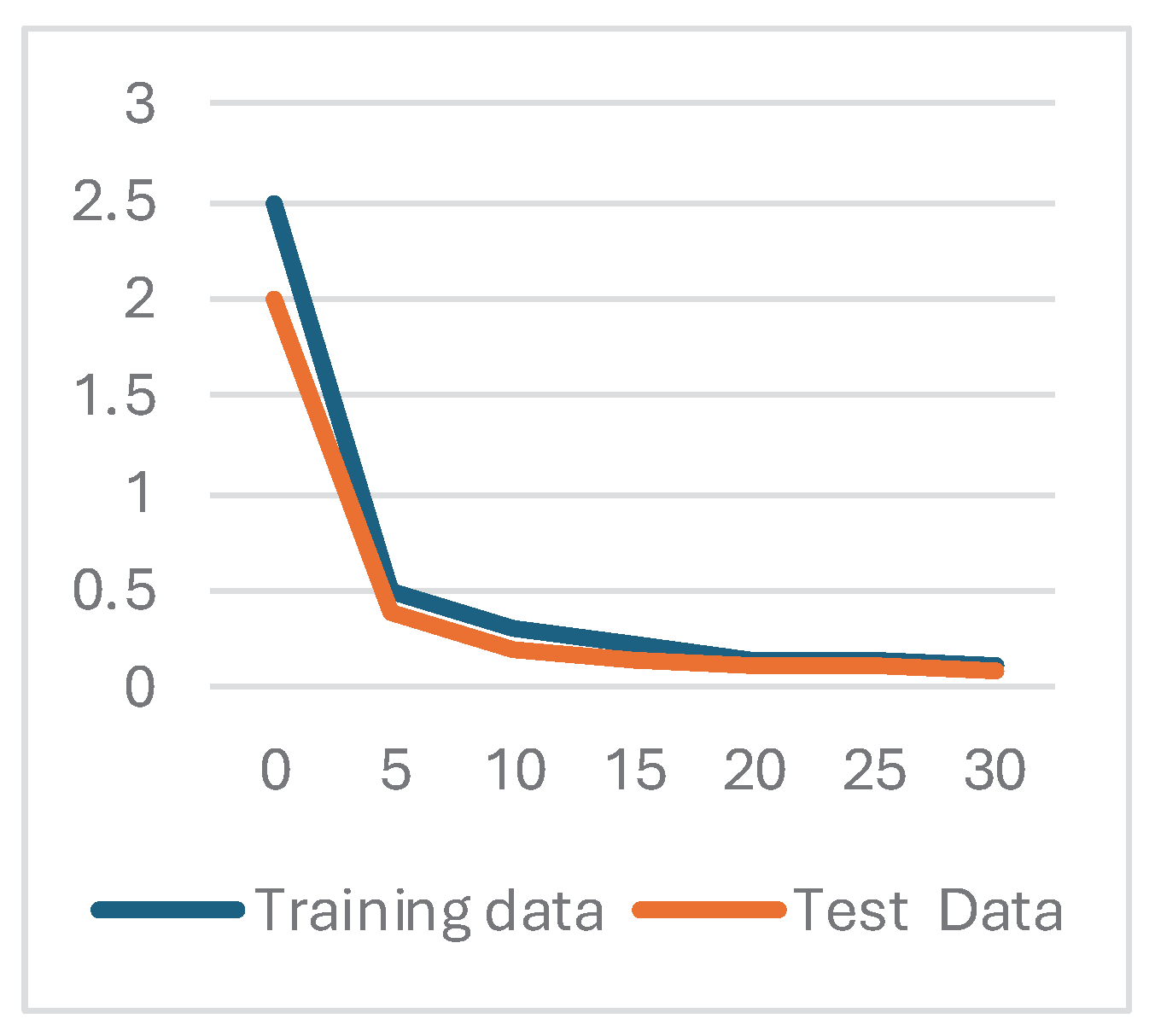
Figure 5.
Analysis of performance for proposed method using JHBO based DNFN accuracy, Specificity, and Sensitivity.
Figure 5.
Analysis of performance for proposed method using JHBO based DNFN accuracy, Specificity, and Sensitivity.
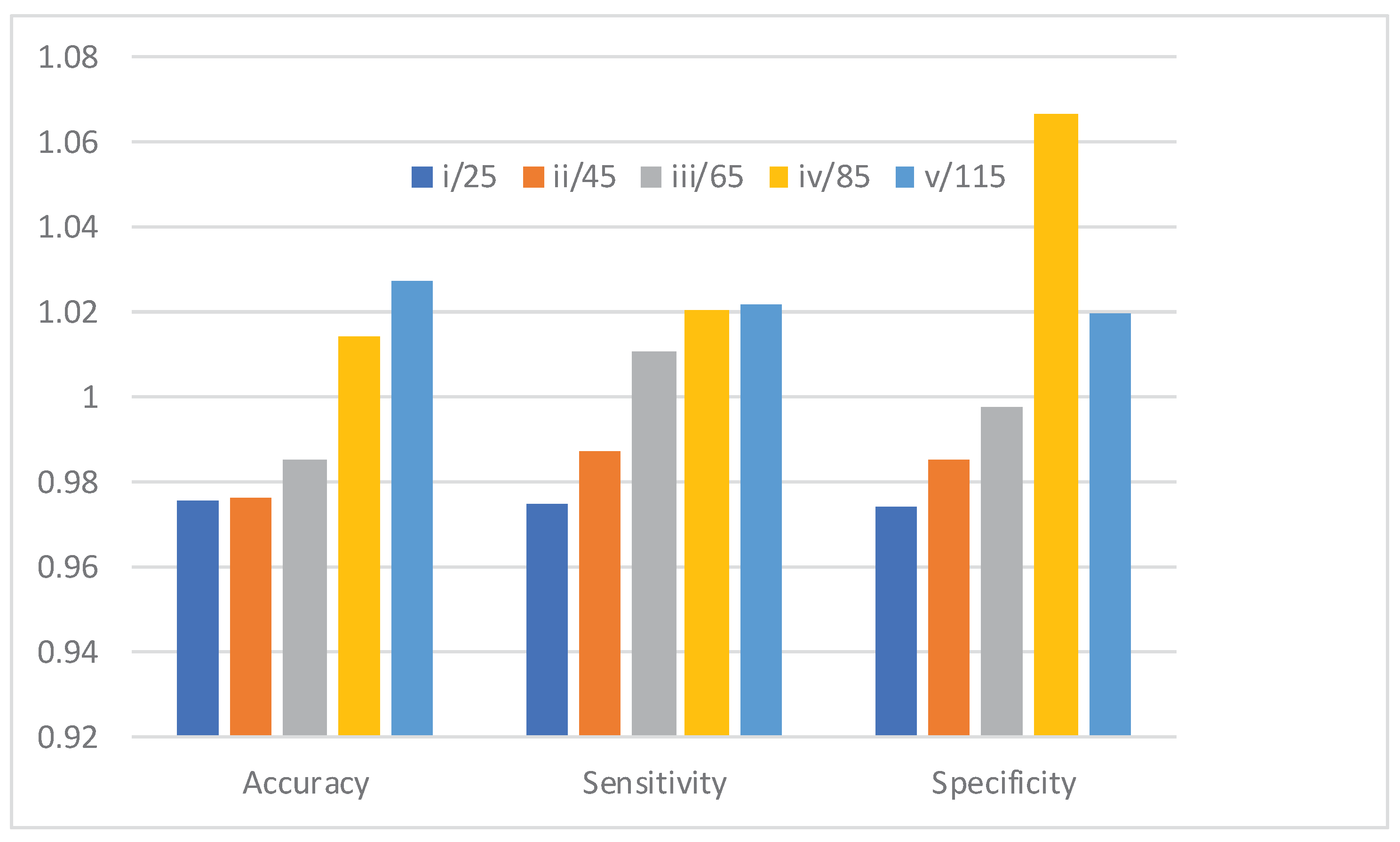
Figure 6.
Blockchain-Enabled EHR Management Process Flow.
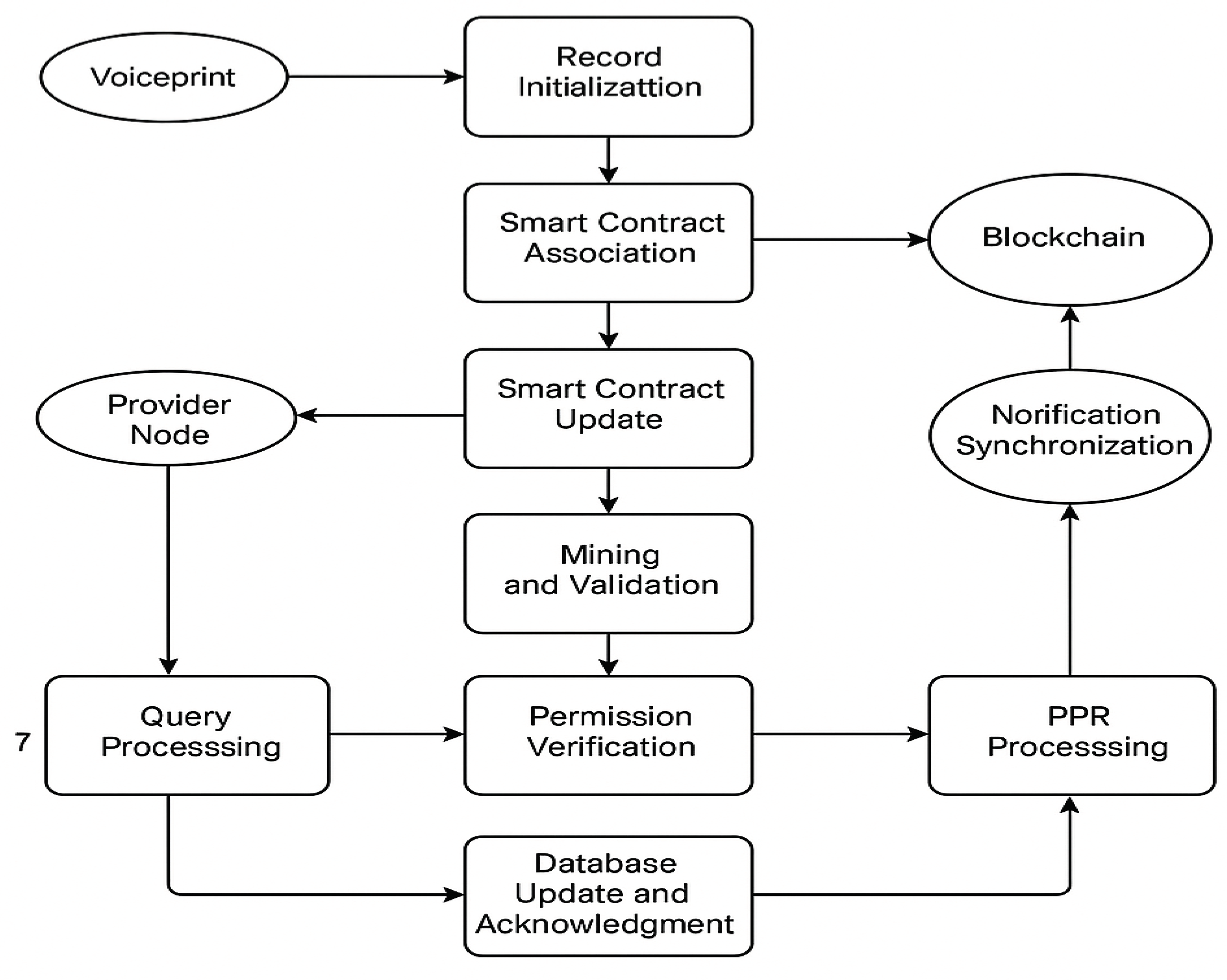
Table 1.
Performance across Iterations (JHBO-based DNFN).
| Iteration | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| 25 | 0.9757 | 0.975 | 0.974 |
| 45 | 0.9763 | 0.9873 | 0.985 |
| 65 | 0.9851 | 1.0105 | 0.998 |
| 85 | 1.014 | 1.0207 | 1.067 |
| 115 | 1.0276 | 1.0215 | 1.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



