Submitted:
17 October 2025
Posted:
20 October 2025
You are already at the latest version
Abstract
Numerous ingredients in trichological shampoos are advertised as “active against hair loss”, however, the body of evidence behind such claims seems very limited or, in many cases, nonexistent. The aim of this study was to compile an inventory of substances advertised by shampoo manufacturers as “active” against hair loss, and systematically review available evidence from clinical trials that would corroborate such claims. We screened declared compositions of trichological shampoos for ingredients advertised as active against hair loss or promoting hair growth. The second step was a systematic review of clinical trials of these substances used topically in the treatment of hair loss. A query in PubMed, Scopus, and Web of Science followed PRISMA and PICO guidelines with the strength of evidence assessed according to GRADE guidelines. We identified 43 trichological shampoos in which 112 individual ingredients were advertised as “active”. Of these, 36 ingredients were indicated as “active” in at least two shampoos and were subject to further study. In the search for evidence, 103,639 articles were screened for relevant information. Ultimately, we identified 29 clinical trials which tested 16 of the 36 ingredients for efficacy against hair loss. Only 4 ingredients were tested individually: caffeine (9 trials; highest strength of evidence: moderate), adenosine (6; moderate); placental protein (3; moderate), and melatonin (1; moderate). Another 12 ingredients of interest were only tested as parts of complex preparations: Achillea millefolium extract, arginine, biotin, hydrolyzed wheat protein, hydrolyzed soy protein, Panax ginseng, panthenol, piroctone olamine, Prunus amygdalus dulcis, Rosmarinus officinalis, Serenoa serrulata, and Urtica dioica. Such study design made it impossible to attribute the observed effects to any specific ingredient. No clinical trials of efficacy could be found for the remaining 20 (55.6%) substances repeatedly cited as “active”. At present stage, scientific evidence for the efficacy against hair loss is available only for caffeine, adenosine, placental proteins and melatonin, but the overall strength of evidence is very low. Moreover, a substantial majority of topical ingredients promoted as “active against hair loss” were actually never tested in clinical trials to verify such claims. While unsubstantiated claims of supposed beneficial properties often refer to alleged scientific evidence, there are major gaps to be filled in the field of non-prescription treatments of hair loss.
Keywords:
trichological shampoos
; hair loss
; alopecia
; baldness
; ingredients
; efficacy
; scoping review
1. Introduction
Hair loss is a physiological phenomenon, but excessive hair loss can lead to visible thinning and even baldness, causing serious psychological distress and reduced quality of life [1]. It may be a sequela of nutritional deficiency, serious diseases or a side effect of pharmacotherapy, including cancer treatment [1–6]. To date, the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) have only approved topical minoxidil and oral finasteride for the treatment of baldness [7]. Due to its adverse hormonal effects, finasteride is approved for treatment only in men [8]. This is in spite of the fact that emerging evidence suggests efficacy of both oral minoxidil and topical finasteride, as well as of oral finasteride in female pattern hair loss (FPHL) [9–11]. Another pharmacological off-label modalities with emerging evidence of efficacy in hair loss is spironolactone and dutasteride [12,13]. Numerous other treatment modalities are discussed, including topical ketoconazole, isotretinoin, botulinum toxin type A, melatonin, pirfenidone, prostaglandin PGE2 and PGF2ɑ analogues bimatoprost and latanoprost, cetirizine, JAK inhibitors, adenosine, caffeine, veratric acid, nutritional supplements, botulinum toxin, platelet-rich plasma, RF electric currents, low-level laser therapy, autologous stem cells, exosomes and combination therapies [14–23]. Next to legal considerations with regard to off-label treatments, concerns about drug safety and possible adverse effects of pharmacotherapy seem to be factors discouraging patients and some doctors from initiating hair loss therapy with pharmacologic agents [24–26]. The fear of “chemical” therapies voiced by many patients has sparked a renaissance of natural ingredients in drugs and cosmetics, because products of “natural origin” are in high demand [27]. Herbal remedies have been used for centuries and they are still sought for due to the general reception of “natural” as “safe” [28]. In response to this demand, the industry searches for complementary and alternative therapies with better effectiveness and less adverse effects than therapies approved nowadays [29]. This trend is also reflected in the realm of topical products against hair loss, referred to as “trichological products” – a term supposed to underscore their intended superiority over common hair care products. According to Trüeb et al., the term “trichology” emerged around 1902 referring to the knowledge taught to people pursuing the practice of hair care and treatment of the human hair and scalp in health and disease, who otherwise were not medically qualified or licensed [30]. In the indexed medical literature, the adjective “trichological” was first used by Camacho et al. in 1978 (in French) and Plewig et al. in 1979 (in German) in reference to clinical investigation of hair [31,32]. By 2000, the term appeared altogether in only 10 PubMed-indexed articles (also in Czech, English and Polish) including 4 articles in which it featured in titles [32–35]. With the advent of the “International Journal of Trichology (IJT)”in 2009, the term “trichology” eventually entered the mainstream medical vocabulary [36]. As of 30 July 2025, PubMed listed 1061 articles featuring the terms “trichology” or “trichological” in any indexed field, including 36 article titles. On the other hand, the presence of these terms in scientific literature seems to have boosted their use in marketing which contributed to a dilution of its meaning and amplifying the unscientific and mercantile aspects to it [37,38]. This is also the impression when looking at “trichological” products, i.e., shampoos, lotions and serums presented by producers and resellers as allegedly more “specialist”, “professional” and “science-based” [39].
In our preliminary study [40], we observed that virtually all producers of trichological shampoos boasted about a range of ingredients supposed to be “active” against hair loss. The majority of these ingredients were of organic origin, ranging from well-defined biomolecules like adenosine and caffeine to complex and less standardized plant and animal organ extracts. A critical look at the ingredients’ lists led us to a suspicion that many of them have not actually undergone clinical trials that would confirm their alleged activity. This notion was seminal for a series of systematic reviews in order to collate and critically asses the evidence behind claims of the ingredients’ beneficial effects on the hair. Recently, we published systematic reviews of topical agents with most numerous (albeit still relatively few) clinical trials in hair loss: placenta derivatives, caffeine and adenosine [14,18,41]. The aim of the present scoping review was to conclude this cycle by collating the evidence with regard to remaining topical ingredients advertised as active against hair loss, and to map the knowledge gaps in this area.
2. Materials and Methods
2.1. Compilation of an Inventory of Ingredients Declared as Active in Trichological Shampoos
Trichological shampoos offered online in Poland between January and December 2024 were identified using the Google search engine by combining phrases like “trichological shampoo(s)”, “trichological preparation(s)”, “against hair loss”, “against baldness”, “stimulating hair regrowth”, “trichological company” or “trichology company” in Polish language. Products were included in further analysis if 1) they were distributed exclusively through trichologist offices, 2) the manufacturer unequivocally declared that the shampoo was effective against hair loss or promoted hair growth, by using phrases like “against hair loss”, “against alopecia”, “against effluvium”, “preventing hair loss”, “strengthening hair”, “inhibiting hair loss”, “stimulating hair growth” in Polish or English, and 3) a complete INCI list of ingredients was available from the manufacturer’s website. Next, a list was compiled of ingredients that were indicated as “active” by at least one producer. Based on experience from our previous research, we predicted that there will be a multitude of various ingredients indicated as active in individual products [39]. Therefore, further analyses were limited to ingredients declared as active in at least 2 shampoos.
2.2. Evidence Acquisition from Published Clinical Trials
A scoping review was conducted according to PRISMA and PICO protocols from January 2025 to July 2025. The protocol of the scoping review was registered and made public in the Open Science Framework (OSF) database [42]. Scientific publications indexed in PubMed, Web of Science and Scopus were searched using the query “X AND (hair OR alopecia OR effluvium OR bald OR baldness OR pilo* OR pili)”, where “X” was substituted with the names of substances from the list described above. For each substance, INCI name was used in the query, as well as synonyms retrieved from PubChem chemistry database (National Institutes of Health, Bethesda, MD). In all queries, the “all fields” option was enabled. No additional filters were used, such as language or publication date. After removing duplicates, the retrieved articles underwent an initial screening by title and abstract. Articles selected in this step underwent a second, full-text review done independently by both authors to select articles that met the inclusion criteria. For articles selected by only one co-author, consensus was reached through discussion. In case of trial reports selected in the described way, reference lists and “similar articles” listed in PubMed were additionally screened for relevant articles. Only original articles presenting results from clinical trials testing efficacy of the substances of interest applied topically in people with hair loss were included in the analysis. Review articles and studies published only as abstracts, posters or meeting reports were excluded. In order to ensure the scientific integrity in this rather commercially-biased area, only trials reported in peer-reviewed journals were included. Therefore, gray literature was not taken into consideration in the present study. The GRADE classification system was used to assess the strength of evidence in the included studies on a scale ranging from very low, through low, moderate to high [43]. Data relevant to this review were extracted into pre-designed tables reflecting the PICO criteria (Table 1).
When assessing the strength of evidence, special attention was paid to the study design, information on the concentration of tested substance, route of administration and formulation, as well as outcome measures selected. The entire search and selection process is presented in Figure 1.
3. Results
3.1. Ingredients Advertised as “Active” in Trichological Shampoos
Forty three trichological shampoos of 17 brands from 6 countries fulfilled the inclusion criteria. Italian products predominated with 16 trichological shampoos offered on the Polish market in the observation period, followed by 12 from Spain, 6 from Poland, 4 from Taiwan, 4 from the USA and 1 from the Netherlands. In those 43 shampoos, a total of 112 unique ingredients declared by at least one manufacturer as “active” were identified, 76 of which were indicated each in only one product. To ensure the feasibility of the project, the subsequent search for evidence was limited to 36 (32.1%) ingredients that were declared as “active against hair loss” in two or more trichological shampoos (Table 2).
3.2. Published Evidence Behind the “Active” Ingredients in Trichological Shampoos
The bibliographic query returned altogether 103,639 articles mentioning one or more of the 36 ingredients compiled in the first step, of which 19,928 duplicates were excluded. After reading the abstracts, further 83711 articles were excluded as not fulfilling the inclusion criteria. The remaining 609 articles were read in full text, which ultimately resulted in the selection of 29 articles meeting the inclusion criteria. These were clinical trial reports of substances listed in Table 2 studied in participants with various types of hair loss defined as androgenetic alopecia (AGA, 22 studies, 3695 participants in total), telogen effluvium (TE, 3 studies, 154 participants), unspecified hair loss (3 study, 107 participants), female pattern hair loss (FPHL, 2 studies, 46 participants), thinning hair (1 study, 84 participants), diffuse alopecia (DA, 1 study, 28 participants), and postpartum hair loss (1 study, 25 participants). Details on the hair problems in the study populations are presented in Table 3.
Eleven studies were identified that focused on single substances of interest: adenosine, caffeine, placental proteins, and melatonin. With regard to testing efficacy of individual substances against hair loss, scientific evidence of varying strength according to the GRADE scale was available only for four ingredients: caffeine (4 studies; highest strength of evidence: moderate), adenosine (4; moderate); placental proteins (2, moderate); and melatonin (1; moderate). Ingredients tested individually in more than one clinical trial were presented in separate systematic reviews devoted to placental proteins [41], caffeine [14], and adenosine [18]. Topical melatonin was the only remaining ingredient studied individually in a devoted clinical trial. The main conclusions from the previously published systematic reviews are summarized in Table 4, while the results from the clinical trial of topical melatonin in hair loss are presented in Table 5.
Beyond adenosine, caffeine, placental proteins and melatonin, another 12 substances out of 36 listed in Table 2 were tested in trials only as ingredients of complex preparations containing other substances considered “active”. This renders it impossible to attribute any observed effects to specific ingredients. This was the case of Achillea millefolium extract which was tested in a complex mixture of 6 substances in 1 trial (strength of evidence: medium), arginine – 5 to 23 substances (2 trials; highest strength of evidence: very low), biotin – 3 to 7 substances (7 trials; low), hydrolyzed wheat protein – 23 substances (1 trial; very low), hydrolyzed soy protein – 23 substances (1 trial; very low), Panax ginseng – 4 substances (1 trial; moderate), panthenol – 3 to 4 substances (2 trials; low), piroctone olamine – 3 to 5 substances (3 trials; very low), Prunus amygdalus dulcis – 23 substances (1 trial; very low), Rosmarinus officinalis – 4 to 23 substances (2 trials; moderate), Serenoa serrulata – 4 to 27 substances (3 trials; moderate), and Urtica dioica – 6 substances (1 trial; low). Some of the complex products included also adenosine, caffeine, placental proteins or melatonin. Key features of these studies of complex products are collated in Table 6.
Looking at the formulations of topical products tested in all 41 included trials of topical anti-hair loss preparations (as listed in Table 4, Table 5 and Table 6), there were 27 “leave-on” preparations (lotions, solutions, extracts, serums, or fluids; 79.4%) and 7 “rinse-off” (shampoos; 20.6%). Two studies tested more formulations [46,54]. The shortest study lasted 1 month [73], and the longest 18 months [52]. The total number of subjects participating in the analyzed studies was 4065, of which 1802 (44.3%) were men, 1546 (38.0%) women, and 717 (17.6%) were mixed groups with undisclosed sex ratio. The age range in the studies was 18 to 75 years. The strength of evidence according to the GRADE methodology was assessed as very low in 20 studies (51,2%), as low in 10 (24,4%), and moderate in the remaining 10 (24,4%). The use or absence of an appropriate comparator had a significant impact on the assessment of the strength of evidence provided in the analyzed trials. Further factors that reduced the assessment were the lack of blinding, error-prone outcome measurements, lack of information on the concentration of the tested substance, testing a mixture of substances considered to be active, small sample size, and short follow-up period. For the remaining 20 (55.6%) substances advertised in trichological shampoos as “active” (Table 1), no clinical trials of efficacy were retrieved in the above-described literature query.
4. Discussion
In cosmetic industry and marketing, advertisers draw on common assumptions about science to present skin-care products as “scientific” or “science-based” [74]. The use of scientific terms associated with objective knowledge and the impartiality of science is used to overcome the common consumers’ skepticism towards advertising by creating a sense of credibility and “transparency” on product ingredients and their benefits [75–77]. The scientific jargon used in marketing lacks explanation, but at the same time science is employed to explain phenomena beyond its explanatory powers, such as beauty standards [78]. This practice is referred to as “science-washing”, defined as the use of science beyond what evidence shows, without appropriate credentials or in instances where science cannot give the answer [79]. This term, which accurately indicates the dependence of marketing disinformation on scientific authority, is currently encountered in public discourse, rather than peer-reviewed scientific literature [80,81]. Science-washing effectively distorts understanding of scientific terms and reduces the role of science to a menial, commercial function. This tendency manifests in the marketing use of terms like “cosmeceuticals”, “dermocosmetics” or “hypoallergenic” products which were initially coined by scientists in an attempt to elaborate better or safer cosmetics, but were later effectively incorporated into marketing vocabulary [82–86]. Recommendations of cosmetic products by medical associations or scientific institutions may be perceived as another form of “science-washing” [87,88]. Another related and partly overlapping term “scienceploitation” is used mainly in reference to unethical practices of offering seemingly science-based but not validated and not approved therapy methods like stem cell treatments [89–91]. In contrast to these “scientific-turned-marketing” terms, the words “trichology” and “trichological” seem to have gone the reverse, “marketing-turned-scientific” path: As already discussed in the introduction, these terms were coined in the commercial context and only later entered the mainstream scientific terminology, without actually ever leaving the realm of marketing.
The overall impression from the present study is that the majority of substances added as “active ingredients” to anti-hair loss topical products have actually no scientific backing. Until presently, only four (adenosine, caffeine, placental proteins and melatonin) have been individually studied in dedicated clinical trials, though the resulting evidence is mostly of low strength due to flaws in study design and size. Moreover, for two advertised “active ingredients” of hair-loss shampoos in Table 1 (niacinamide and Zingiber officinale) there is evidence speaking against their beneficial effects which will be discussed in detail below. Twelve ingredients were only tested in clinical trials as components in complex products combining various substances presumed to be beneficial to hair (Table 6). This was the case for Achillea millefolium, arginine, biotin, hydrolyzed wheat protein, hydrolyzed soy protein, Panax ginseng extract, panthenol, piroctone olamine, Prunus amygdalus dulcis oil, Rosmarinus officinalis, Serenoa serrulata, and Urtica dioica. Regardless of the questionable strength of scientific evidence in most of these studies, such a study design in no way authorizes drawing any conclusions about individual effects of these ingredients on hair. To illustrate this, let’s imagine a hypothetical shampoo “XYZ” with ingredients X, Y, Z, of which component X will have an unfavorable effect on hair, component Y will have a beneficial effect much stronger than the untoward effect of X, and component Z will be neutral. In a clinical trial, the overall effect of the imaginary product “XYZ” would prove beneficial, owing to the strong effect of only one component Y, while X would lessen the net effect and Z would constitute an unnecessary ballast. Therefore, an assumption that the efficacy of the shampoo “XYZ” be a proof of effectiveness of each ingredients X, Y and Z will amount to faulty reasoning referred to as the fallacy of division, also known as the “whole-to-part fallacy” [92]. The fallacy of division occurs when from an observed property of an entire item (here: a complex anti-hair loss product), one infers that the same property is attributable to each of its parts (here: ingredients) [93]. Arguably, some ingredients must be active if beneficial effects of a complex product are confirmed in well-designed, controlled trials. However, the actual effect of each ingredient, whether beneficial, neutral or detrimental, will remain obscure until separately tested in a randomized, controlled trial against a suitable placebo. It must be stressed, therefore, that the information collated in Table 6 should by no means be regarded as a proof of efficacy of any of the ingredients listed. The table was created merely in order to document the search process, as well as map the gaps in current state of knowledge.
For the remaining 20 (55.6%) ingredients declared as “active” in analyzed anti-hair loss shampoos, their activity was not studied in any published clinical trials, not even as part in complex products. This observation largely confirms our concerns stemming from the study of 92 anti-hair loss products – shampoos, mesotherapy solutions, lotions, serums and conditioners of predominantly international brands, available in Poland between 2018 and 2019. In that study, we found that among 448 unique ingredients listed in the products, 207 were advertised as “active” against hair loss in at least one of them [39]. At that time, scientific evidence of varying (predominantly very low) quality could be found in medical literature for just 8 (3.9%) of these ingredients. Only 38.0% of the products contained at least one ingredient with confirmed beneficial effects on hair, including 8.7% containing two such ingredients. The majority of the anti-hair loss products (62.0%) analyzed in that study would not contain any ingredient with confirmed influence on hair growth, either beneficial or detrimental. Interestingly, ingredients supported with available evidence were not at all the most widespread ones in the preparations analyzed. We also found that according to evidence available at the time of the study, some ingredients advertised as “active” could actually worsen hair condition [39]. For example, 6-gingerol – the major active constituent of ginger (Zingiber officinale) was demonstrated to cause a dose-dependent inhibition of hair growth in ex vivo cultures of human hair units [94], as well as in an in vivo mouse model [95]. In spite of this evidence, Zingiber officinale was present on ingredients lists of 4 out of 92 anti-hair loss products (4,3%), including 3 scalp mesotherapy solutions and one lotion – in all of them, ginger was promoted as “beneficial for hair” [39]. Fortunately, we did not find Zingiber officinale in the ingredients lists of any of the shampoos analyzed in neither in the first study and in our follow-up evaluation of trichological shampoos available on the market from February 2022 to May 2023 [40], nor in the present analysis.
A closer look at niacinamide in anti-hair loss products offers an interesting, multi-dimensional insight into the interaction between published scientific evidence and the composition of anti-hair loss products. The period 2015–2020 may be arguably considered as formative for the perception of niacinamide. A literature query combining terms “hair” with “niacinamide”, “nicotinamide” or “vitamin B3” revealed that all relevant original research on the influence of topical niacinamide on hair appeared in the indexed literature between 2015-2020: During that period, the first three original studies were published of the effect of niacinamide on hair growth [63,96,97]. Other than that, by the time of completing the present review, only one further experimental paper was published with indirect relevance to the topic, and 4 clinical trials of complex products with niacinamide, where it was impossible to single out its individual influence on hair. The first of the three relevant studies was a double-blind, randomized clinical trial of Japanese men with AGA, in which participants were treated with lotions containing either adenosine 0.75% or niacinamide 0.1%. The authors stated explicitly that they did not consider niacinamide to be a hair growth promoter and used it as a “placebo-like lotion” because they did not receive a clearance for placebo-controlled study. The authors reported significant improvements in both compared groups after 6 months of treatment with regard to an increase of thick hair ratio and a decrease of vellus (thin) hair ratio. Nevertheless, the increase in objectively measured hair diameter, as well as percentage of patients who noticed increased thickness of hair were significantly higher in adenosine group. No significant change in hair density was observed in either groups, with a tendency toward an increase seen in the adenosine group (p=0.097), but not in niacinamide group (p=0.554) [63]. Altogether these results seem to speak in favor of adenosine, rather than niacinamide as the hair growth promoting agent. Unfortunately, lack of placebo in this study did not allow to compensate for bias, including seasonal changes in hair growth and loss [14]. The second study relevant to the topic, published in 2018, demonstrated inhibitory effects of niacinamide in ex-vivo human hair follicles [96]. Two years later, Oblong et. al. thoroughly compiled existing evidence to conclude that niacinamide actually has a net neutral effect on human hair growth [97]. This led us to consider niacinamide as equivalent with placebo in our previous paper [18]. The last, study so far of niacinamide was conducted in cultured human dermal papilla cells - specialized mesenchymal cells at the base of a hair follicle that are crucial for hair growth and pigmentation but are not hair cells themselves [98]. Moreover, the authors measured markers of oxidative stress, rather than proliferation or growth, and only speculatively suggested that “niacinamide could enhance hair growth by preventing oxidative stress-induced cell senescence and premature catagen entry of hair follicles”. Beyond that, four trials were published: two randomized, double blind and two open label studies of complex products that consisted of 3–6 presumably “active” ingredients – a design rendering it impossible to single out and assess the actual effect of niacinamide [65,99–101]. Collectively, the above research seemed to indicate that niacinamide has either neutral or unfavorable effect on hair growth.
Expectedly, published research results questioning the supposed beneficial effects of this ingredient on hair should be noticed and addressed accordingly by manufacturers of products that are promoted as “science-based”. Taking into account the lag between shampoo design and emergence on the market, we propose to consider the data from previous study of 2018-2019 as representative of the “before evidence” period with regard to niacinamide effects on hair [39], and the study of 2024 – as representative of the “after evidence” period [40]. Comparison of the data from these studies suggests that there was indeed a change in the usage of niacinamide in the period between them: In the analysis of products available between October 2018 and August 2019 [39], niacinamide was present in 9 out of 31 (29.0%) anti-hair loss shampoos, including 5 (16.1%) in which it was declared as “active ingredient”. In the latter analysis, niacinamide was listed in only one of 43 (2.3%) of trichology shampoos available in 2024 [41]. This single shampoo, in which niacinamide was both present and pronounced as “active ingredient”, was launched after completion of the first study, i.e., after August 2019, apparently in spite of the already published report suggesting unfavorable effects of niacinamide on hair growth [96]. Nevertheless, within the 5-year span between both studies, the overall presence of niacinamide in trichological shampoos on the market decreased significantly from 29.0% to 2.3% (chi2 test, Yates’ p = 0.02). Altogether, this might be cautiously interpreted as a sign that most manufacturers of trichology shampoos follow medical literature and abandon ingredients when the evidence speaks against them. Unfortunately, another observation from the current scoping review is that the lack of positive evidence does not discourage them from using untested ingredients and presenting them as “active”. This was true in case of the majority (20 out of 36) ingredients included into present analysis.
Another problem with alleged science-based composition of trichological shampoos is illustrated by the case of Curcuma (turmeric): As of May 2025, the “Plants of the World Online” database listed 237 entries for the genus Curcuma, including 183 accepted species [102]. The species arguably best known to the general public is Curcuma longa which is the source of yellow turmeric – a spice with a myriad of health benefits ascribed to it, many confirmed scientifically [103–109]. Notably, no study of influence of Curcuma longa on hair was published to date. Another species from the genus – Curcuma aeruginosa was demonstrated to inhibit testosterone 5α-reductase in experimental settings and proved effective against androgenetic alopecia in a randomized, double-blind clinical trial [110–112]. This picture is not entirely clear as another randomized, double blind trial showed that Curcuma aeruginosa effectively inhibits the growth of axillary hair [113]. It remains unclear whether this difference is due to different hair type (scalp versus axillary), different fractions of the plant material used (root aqueous extract versus root oil) or other factors. Nevertheless, among anti-hair loss products analyzed in the previous study, three (mesotherapy solutions and a topical lotion) included yet another Curcuma species - the white turmeric (Curcuma zedoaria) which was declared as “active” in two of these [39]. For this particular species, there is no evidence published until present that would support alleged beneficial influence on the hair, beyond an anecdotal mention of traditional use of Curcuma zedoaria in hair oils [114]. Even in case of the “right” Curcuma species, there is still a question about originality, quality, purity and safety of the raw material used [115]. Nevertheless, for the average consumer who usually only knows that “turmeric is good for health”, information about turmeric in a product would probably be an incentive to purchase, without realizing the multitude and diversity of plant species hidden under the names “Curcuma” or “turmeric” and the problem of raw material quality. This may be viewed either as another example of division fallacy in the science of hair loss products, as well as another example of “science-washing”.
As mentioned above, the overall strength of evidence in the trials included in the present review was very low. Many of these trials showed flaws in study design, including selection bias, lack of adequate controls and lack of compensation for seasonal hair loss stood in the foreground as discussed in detail in our previous two papers [14,18]. Guyatt et al. suggested that publication bias should especially be suspected when available evidence comes from a number of small studies, most of which have been commercially funded [116]. When looking at the trials on topical hair loss products, this might indeed be the case. Out of 11 trials of individual ingredients:
- Only in 2 studies, the authors explicitly declared the absence of conflict of interest (COI) both with regard to funding of the study and financial relations between authors with potentially commercial beneficiaries, of which a non-proprietary, in-house preparation was used in one study [73] and a commercial brand of product was named in the other [55].
- Six trials were disclosed (sometimes vaguely or indirectly) as industry-funded or -sponsored [45,56–58,62,63]. Except the above-mentioned two, in remaining 3 trials there was no statement with this regard.
- In 5 trials at least some co-authors were disclosed as employees of manufacturers of products tested, or received other financial gratifications from them for performing the study [45,56,62,63,69]. In 2 trials, the authors declared the absence of any link to manufacturers [55,73], while there was no statement with this regard in remaining four [57,58,61,67].
- Tested products were identified by brand or tradename in 5 trials [55–58,67], non-proprietary, in-house preparations were described in 3 trials [45,61,73] with no statement in the remaining three [63,69].
- Possible bias or study limitations were addressed in only 2 of the 11 trials [55,56].
Industry involvement in research does not automatically imply bad science. Collaboration between academia and industry is fundamental to technological progress [117,118]. On the other hand, the overlapping area of clinical research, industry and marketing seems to open door to specific type of bias, referred to as “sponsorship bias”. Steel defines sponsorship bias as a situation when the financial interests of funders of scientific research influence claims made by scientists, especially in peer-reviewed publications. He pointed out that such claims are not necessarily false but may encourage recipients to infer false conclusions [119]. Sponsorship bias seems instrumental to science washing. This phenomenon is not limited to hair care products, as it also affects regulated products, such as medicines, dietary supplements, or food for special medical purposes [120–123].
Next to research reports published in peer-reviewed journals, evidence can be found in other sources, e.g., academic theses and dissertations, research and committee reports, government reports, conference papers, and reports from ongoing research – information sources referred to collectively as “gray literature” [124,125]. Gray literature may reveal important details about topics that would otherwise be missed [126]. With a steady increase in information posted online, traditional systematic literature reviews could be combined with reviews of gray literature into “multivocal literature reviews” [127]. We abstained from relying on gray literature it in our research, as the realm of anti-hair loss seems especially prone to various kind of bias with commercial claims oftentimes disguised as “scientific evidence”. This problem seems confirmed by the overall low quality of peer-reviewed publications. We reasoned that gray literature in this area might be even less trustworthy and would add to the uncertainty of the results. Therefore, we decided to confine our sources of data to full trial reports published in peer-reviewed journals, considering the peer-review process by independent referees as a means of providing a minimum of scientific quality and integrity. Moreover, a more detailed reporting of trial design enabled us to assess the strength of evidence provided by the trial reports. Assessing the strength of evidence according to GRADE is typical of systematic, rather than scoping reviews. In fact, the present article was initially intended as a systematic review, closing a four-piece series of systematic reviews. In the process of writing, however, we have realized that the multitude of supposedly active substances covered, the heterogeneity in trial design and reported outcomes, as well as numerous knowledge gaps would not allow to register and complete this study as a systematic review. Instead, it seemed more reasonable and appropriate to register and finalize the present paper as scoping review. Due to the sheer volume of retrieved information, three active ingredient with sufficient data for systematic review – adenosine, caffeine and placental proteins were presented in separate systematic reviews [14,18,41]. The present article concludes the series and offers an inventory of the many unknowns in the field of topical prescription-free treatments for hair loss.
5. Conclusions
In the plethora of topical agents allegedly active against hair loss, only four were actually tested in dedicated clinical trials: caffeine (9 trials), adenosine (6 trials), placenta derivatives (3 trials) and melatonin (1 trial). The majority of these trials seem flawed in design and susceptible to bias and the strength of evidence delivered by them is predominantly very low or low. Furthermore, a dozen ingredients with alleged efficacy against hair loss were only tested clinically as part of complex products which renders impossible to make any conclusion about each such ingredient individually. Even more worryingly, a substantial majority of topical ingredients promoted as active against hair loss were actually never tested clinically with this regard. We conclude, therefore, that there are major gaps to be filled in the field of non-prescription treatments of hair loss, while unsubstantiated claims of supposed beneficial properties often refer to alleged scientific evidence.
Supplementary Materials
The following supporting information can be downloaded at website of this paper posted on Preprints.org, Table S1: An overview of clinical trials on the efficacy of the substances of interest to the present article tested individually in topical preparations against hair loss; Table S2: An overview of clinical trials on the efficacy of the substances of interest to the present paper tested in complex topical preparations against hair loss.
Author Contributions
Conceptualization, R.S.; methodology, R.S. and E.S.; bibliographic query, E.S.; data extraction, E.S.; data curation, E.S. and R.S.; writing—original draft preparation, R.S. and E.S.; writing—review and editing, R.S. and E.S.; visualization, E.S.; supervision, R.S.; project administration, R.S.; funding acquisition, R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Jagiellonian University Medical College, Krakow, Poland, grant number N42/DBS/000445.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author..
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Owecka, B.; Tomaszewska, A.; Dobrzeniecki, K.; Owecki, M. The Hormonal Background of Hair Loss in Non-Scarring. Alopecias Biomedicines. 2024, 12, 513. [CrossRef]
- Rallis, E.; Lotsaris, K.; Grech, V.S.; Tertipi, N.; Sfyri, E.; Kefala, V. The Nutrient-Skin Connection: Diagnosing Eating Disorders Through Dermatologic Signs. Nutrients 2024, 16, 4354. [CrossRef]
- Smolarczyk, K.; Meczekalski, B.; Rudnicka, E.; Suchta, K.; Szeliga, A. Association of Obesity and Bariatric Surgery on Hair Health. Medicina (Kaunas) 2024, 60, 325. [CrossRef]
- Brnic, S.; Spiljak, B.; Zanze, L.; Barac, E.; Likic, R.; Lugovic-Mihic, L. Treatment Strategies for Cutaneous and Oral Mucosal Side Effects of Oncological Treatment in Breast Cancer: A Comprehensive Review. Biomedicines 2025, 13, 1901. [CrossRef]
- Haagsma, A.B.; Otto, F.G.; de Sa Vianna, M.L.G.; Maingue, P.M.; Muller, A.P.; de Oliveira, N.; Abbott, L.A.; da Silva, F.P.G.; Klein, C.K.; Herzog, D.M.; et al. Clinical Evaluation of COVID-19 Survivors at a Public Multidisciplinary Health Clinic. Biomedicines 2025, 13, 1888. [CrossRef]
- Pan, L.; Moog, P.; Li, C.; Steinbacher, L.; Knoedler, S.; Kukrek, H.; Dornseifer, U.; Machens, H.G.; Jiang, J. Exploring the Association Between Multidimensional Dietary Patterns and Non-Scarring Hair Loss Using Mendelian Randomization. Nutrients 2025, 17, 2569. [CrossRef]
- Rosenthal, A.; Conde, G.; Greco, J.F.; Gharavi, N.M. Management of androgenic alopecia: a systematic review of the literature. J. Cosmet. Laser Ther. 2024, 26, 1-16. [CrossRef]
- Nobari, N.N.; Roohaninasab, M.; Sadeghzadeh-Bazargan, A.; Goodarzi, A.; Behrangi, E.; Nikkhah, F.; Ghassemi, M. A Systematic Review of Clinical Trials Using Single or Combination Therapy of Oral or Topical Finasteride for Women in Reproductive Age and Postmenopausal Women with Hormonal and Nonhormonal Androgenetic Alopecia. Adv. Clin. Exp. Med. 2023, 32, 813–823.
- Desai, D.D.; Nohria, A.; Sikora, M.; Anyanwu, N.; Shapiro, J.; Lo Sicco, K.I. Comparative analysis of low-dose oral minoxidil with spironolactone versus finasteride or dutasteride in female androgenetic alopecia management. Arch. Dermatol. Res. 2024, 316, 622. [CrossRef]
- Keerti, A.; Madke, B.; Keerti, A.; Lopez, M.J.C.; Lirio, F.S. Topical Finasteride: A Comprehensive Review of Androgenetic Alopecia Management for Men and Women. Cureus 2023, 15, e44949. [CrossRef]
- Starace, M.V.R.; Gupta, A.K.; Bamimore, M.A.; Talukder, M.; Quadrelli, F.; Piraccini, B.M. The Comparative Effects of Monotherapy with Topical Minoxidil, Oral Finasteride, and Topical Finasteride in Postmenopausal Women with Pattern Hair Loss: A Retrospective Cohort Study. Skin Appendage Disord. 2024, 10, 293-300. [CrossRef]
- Jimenez-Cauhe, J.; Lo Sicco, K.I.; Shapiro, J.; Hermosa-Gelbard, A.; Burgos-Blasco, P.; Melian-Olivera, A.; Ortega-Quijano, D.; Pindado-Ortega, C.; Buendia-Castano, D.; Asz-Sigall, D.; et al. Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review. J. Clin. Med. 2025, 14, 1805. [CrossRef]
- Kim, J.; Song, S.Y.; Sung, J.H. Recent Advances in Drug Development for Hair Loss. Int. J. Mol. Sci. 2025, 26, 3461. [CrossRef]
- Szendzielorz, E.; Spiewak, R. Caffeine as an Active Ingredient in Cosmetic Preparations Against Hair Loss: A Systematic Review of Available Clinical Evidence. Healthcare. 2025, 13, 395. [CrossRef]
- Krefft-Trzciniecka, K.; Pietowska, Z.; Pakiet, A.; Nowicka, D.; Szepietowski, J.C. Short-Term Clinical Assessment of Treating Female Androgenetic Alopecia with Autologous Stem Cells Derived from Human Hair Follicles. Biomedicines 2024, 12, 53. [CrossRef]
- Martinez-Pascual, M.A.; Sacristan, S.; Toledano-Macias, E.; Naranjo, P.; Hernandez-Bule, M.L. Effects of RF Electric Currents on Hair Follicle Growth and Differentiation: A Possible Treatment for Alopecia. Int. J. Mol. Sci. 2024, 25, 7865. [CrossRef]
- Lama, S.B.C.; Perez-Gonzalez, L.A.; Kosoglu, M.A.; Dennis, R.; Ortega-Quijano, D. Physical Treatments and Therapies for Androgenetic Alopecia. J. Clin. Med. 2024, 13, 4534. [CrossRef]
- Szendzielorz, E.; Spiewak, R. Adenosine as an Active Ingredient in Topical Preparations Against Hair Loss: A Systematic Review and Meta-Analysis of Published Clinical Trials. Biomolecules 2025, 15, 1093. [CrossRef]
- Perez, S.M.; AlSalman, S.A.; Nguyen, B.; Tosti, A. Botulinum Toxin in the Treatment of Hair and Scalp Disorders: Current Evidence and Clinical Applications. Toxins (Basel) 2025, 17. [CrossRef]
- Bento, E.B.; Matos, C.; Ribeiro Junior, H.L. Successful Treatment of Hair Loss and Restoration of Natural Hair Color in Patient with Alopecia Areata Due to Psychological Disorder Using Exosomes: Case Report with 6-Month Follow-Up. Cosmetics 2025, 12, 97. [CrossRef]
- Chen, S.; Li, L.; Ding, W.; Zhu, Y.; Zhou, N. Androgenetic Alopecia: An Update on Pathogenesis and Pharmacological Treatment. Drug. Des. Devel. Ther. 2025, 19, 7349-7363. [CrossRef]
- Vrapcea, A.; Pisoschi, C.G.; Ciupeanu-Calugaru, E.D.; Trasca, E.T.; Tutunaru, C.V.; Radulescu, P.M.; Radulescu, D. Inflammatory Signatures and Biological Markers in Platelet-Rich Plasma Therapy for Hair Regrowth: A Comprehensive Narrative Analysis. Diagnostics (Basel) 2025, 15, 1123. [CrossRef]
- You, J.; Jang, Y.; Sim, J.; Ryu, D.; Cho, E.; Park, D.; Jung, E. Anti-Hair Loss Effect of Veratric Acid on Dermal Papilla Cells. Int. J. Mol. Sci. 2025, 26, 2240. [CrossRef]
- Irwig, M.S. Safety concerns regarding 5alpha reductase inhibitors for the treatment of androgenetic alopecia. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 248-253. [CrossRef]
- Almohanna, H.M.; Perper, M.; Tosti, A. Safety concerns when using novel medications to treat alopecia. Expert Opin. Drug Saf. 2018, 17, 1115-1128. [CrossRef]
- Ho, R.S. Ongoing Concerns Regarding Finasteride for the Treatment of Male-Pattern Androgenetic Alopecia. JAMA Dermatol 2021, 157, 25-26. [CrossRef]
- Amberg, N.; Fogarassy, C. Green Consumer Behavior in the Cosmetics Market. Resources 2019, 8, 137. [CrossRef]
- Chaachouay, N.; Zidane, L. Plant-Derived Natural Products: A Source for Drug Discovery and Development. Drugs Drug Candidates 2024, 3, 184-207. [CrossRef]
- Wang, H.; Chen, Y.; Wang, L.; Liu, Q.; Yang, S.; Wang, C. Advancing herbal medicine: enhancing product quality and safety through robust quality control practices. Front. Pharmacol. 2023, 14, 1265178. [CrossRef]
- Trueb, R.M.; Rezende, H.D.; Dias, M.F.R.G.; Uribe, N.C. Trichology and Trichiatry; Etymological and Terminological Considerations. Int. J. Trichology 2022, 14, 117-119. [CrossRef]
- Camacho, F.; Armijo, M.; Naranjo, R.; Dulanto, F. Le syndrome tricho-rhino-phalangien (Giedion). Ann. Dermatol. Venereol. 1978, 105, 17-21.
- Plewig, G.; Schill, W.B.; Hofmann, C. [Oral treatment with tretinoin: andrological, trichological, ophthalmological findings and effects on acne (author’s transl)]. Arch. Dermatol. Res. 1979, 265, 37-47. [CrossRef]
- Bartosova, L.; Werkmannova, A.; Smolan, S.; Fingerova, H. Trichological alterations in women during pregnancy and after delivery. Acta Univ. Palacki Olomuc Fac. Med. 1987, 117, 225-246.
- Rushton, D.H.; Ramsay, I.D.; James, K.C.; Norris, M.J.; Gilkes, J.J. Biochemical and trichological characterization of diffuse alopecia in women. Br. J. Dermatol. 1990, 123, 187-197. [CrossRef]
- Brzezinska-Wcislo, L.; Bogdanowski, T.; Koslacz, E.; Hawrot, A. [Trichological examinations in women suffering from diabetes mellitus]. Wiad. Lek. 2000, 53, 30-34.
- Yesudian, P. Why Another journal? Int. J. Trichology 2009, 1, 1. [CrossRef]
- Trueb, R.M. A Comment on Mercantilism in the Trichological Sciences. Int. J. Trichology 2023, 15, 85-87. [CrossRef]
- Trueb, R.M.; Gadzhigoroeva, A.; Kopera, D.; Luu, N.C.; Dmitriev, A. The Problem with Capitalism in the Trichological Sciences. Int. J. Trichology 2023, 15, 79-84. [CrossRef]
- Pyzik, M.; Plichta, D.; Spiewak, R. Analiza występowania składników deklarowanych jako aktywne w preparatach przeciw wypadaniu włosów oraz przegląd systematyczny badań nad ich skutecznością. [An occurrence analysis of ingredients declared as active in anti-hair loss products and systematic review of studies on their effectiveness] (in Polish). Estetol. Med. Kosmetol. 2020. [CrossRef]
- Szendzielorz, E.; Śpiewak, R. An analysis of the presence of ingredients that were declared by the producers as “active” in trichological shampoos for hair loss. Estetol. Med. Kosmetol. 2024, 14, 001.en. [CrossRef]
- Szendzielorz, E.; Spiewak, R. Placental Extracts, Proteins, and Hydrolyzed Proteins as Active Ingredients in Cosmetic Preparations for Hair Loss: A Systematic Review of Available Clinical Evidence. Appl. Sci. 2024, 14, 10301. [CrossRef]
- Spiewak, R.; Szendzielorz, E. Topical ingredients considered as active against hair loss: a scoping review. Available online: https://osf.io/2kmhd (accessed on 30 July 2025).
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, 452 S.; Guyatt, G.H. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401-406. [CrossRef]
- Fischer, T.W.; Trüeb, R.M.; Hänggi, G.; Innocenti, M.; Elsner, P. Topical melatonin for treatment of androgenetic alopecia. Int. J. Trichology. 2012, 4, 236-245. http://doi:10.4103/0974-7753.111199.
- Fischer, T.W.; Burmeister, G.; Schmidt, H.W.; Elsner, P. Melatonin increases anagen hair rate in women with androgenetic alopecia or diffuse alopecia: results of a pilot randomized controlled trial. Br. J. Dermatol. 2004, 150, 341–345. [CrossRef]
- Pekmezci, E.; Dündar, C.; Türkoğlu, M. A proprietary herbal extract against hair loss in androgenetic alopecia and telogen effluvium: a placebo-controlled, single-blind, clinical-instrumental study. Acta Dermatovenerol. Alp. Pannonica Adriat. 2018, 27, 51-57.
- Reygagne, P.; Mandel, V.D.; Delva, C.; et al. An anti-hair loss treatment in the management of mild androgenetic alopecia: Results from a large, international observational study. Dermatol. Ther. 2021, 34, 15134. [CrossRef]
- Turlier, V.; Darde, M.S.; Loustau, J.; Mengeaud, V. Assessment of the effects of a hair lotion in women with acute telogen effluvium: a randomized controlled study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 12-20. [CrossRef]
- Pelfini, C.; Fideli, D.; Speziali, A.; Vignini, M. Effects of a topical preparation on some hair growth parameters, evaluated utilizing a morphometric computerized analysis. Int. J. Cosmet. Sci. 1987, 9, 1-11. [CrossRef]
- Marotta, J.C.; Patel, G.; Carvalho, M.; Blakeney, S. Clinical Efficacy of a Topical Compounded Formulation in Male Androgenetic Alopecia: Minoxidil 10%, Finasteride 0.1%, Biotin 0.2%, and Caffeine Citrate 0.05% Hydroalcoholic Solution. Int. J. Pharm. Compd. 2020, 24, 69-76.
- Lueangarun, S.; Panchaprateep, R. An Herbal Extract Combination (Biochanin A, Acetyl tetrapeptide-3, and Ginseng Extracts) versus 3% Minoxidil Solution for the Treatment of Androgenetic Alopecia: A 24-week, Prospective, Randomized, Triple-blind, Controlled Trial. J. Clin. Aesthet. Dermatol. 2020,13, 32-37.
- Piérard, G.; Piérard-Franchimont, C.; Nikkels-Tassoudji, N.; Nikkels, A.; Léger, D. S. Improvement in the inflammatory aspect of androgenetic alopecia. A pilot study with an antimicrobial lotion. J. Dermatol. Treatment. 1996, 7 , 153–157. [CrossRef]
- Masoud, F.; Alamdari, H.A.; Asnaashari, S.; Shokri, J.; Javadzadeh, Y. Efficacy and safety of a novel herbal solution for the treatment of androgenetic alopecia and comparison with 5% minoxidil: A double-blind, randomized controlled trial study. Dermatol. Ther. 2020, 33, 14467. [CrossRef]
- Wessagowit, V.; Tangjaturonrusamee, C.; Kootiratrakarn, T.; et al. Treatment of male androgenetic alopecia with topical products containing Serenoa repens extract. Australas J. Dermatol. 2016, 57, 76-82. [CrossRef]
- Barat, T.; Abdollahimajd, F.; Dadkhahfar, S.; Moravvej, H. Evaluation of the efficacy and safety of cow placenta extract lotion versus minoxidil 2% in the treatment of female pattern androgenetic alopecia. Int. J. Womens Dermatol. 2020, 6, 318–321. [CrossRef]
- Dhurat, R.; Chitallia, J.; May, T.W.;Ammani, M.; Madhukara, J.J.; Anandan, S.; Vaidya, P.; Klenk, A. An Open-Label Randomized Multicenter Study Assessing the Noninferiority of a Caffeine-Based Topical Liquid 0.2% versus Minoxidil 5% Solution in Male Androgenetic Alopecia. Skin Pharmacol. Physiol. 2017, 30, 298-305. [CrossRef]
- Sisto, T.; Bussoletti, C.; Celleno, L. Efficacy of a Cosmetic Caffeine Shampoo in Androgenetic Alopecia management. II Note. J. Appl. Cosmetol. 2013, 31, 57-66.
- Bussoletti, C; Mastropietro, F.; Tolaini, M.V; Celleno, L. Use of a Caffeine Shampoo for the Treatment of Male Androgenetic Alopecia. J. Appl. Cosmetol. 2010, 28, 153-162.
- Rapaport, J.; Sadgrove, N.J.; Arruda, S.; Swearingen, A.; Abidi, Z.; Sadick, N. Real World, Open-Label Study of the Efficacy and Safety of a Nowel Serum in Androgenetic Alopecia. J. Drugs Dermatol. 2023, 22, 559-564.
- Samadi, A.; Rokhsat, E.; Saffarian, Z.; Goudarzi, M.M.; Kardeh, S.; Nasrollahi, S.A.; Firooz, A. Assessment of the efficacy and tolerability of a topical formulation containing caffeine and Procapil 3% for improvement of male pattern hair loss. J. Cosmet. Dermatol. 2024, 23, 1492-1494. [CrossRef]
- Faghihi, G.; Iraji, F.; Harandi, M.; Nilforoushzadeh, M.A.; Askari, G. Comparison of the efficacy of topical minoxidil 5% and adenosine 0.75% solutions on male androgenetic alopecia and measuring patient satisfaction rate. Acta Dermatovenerol. Croat. 2013, 21, 155-159.
- Iwabuchi, T.; Ideta, R.; Ehama, R. et al. Topical adenosine increases the proportion of thick hair in Caucasian men with androgenetic alopecia. J. Dermatol. 2016, 43, 567-570. [CrossRef]
- Watanabe, Y.; Nagashima, T.; Hanzawa, N.; et al. Topical adenosine increases thick hair ratio in Japanese men with androgenetic alopecia. Int. J. Cosmet. Sci. 2015, 37, 579-587. [CrossRef]
- Garre, A.; et al. Efficacy and Safety of a New Topical Hair Loss-Lotion Containing Oleanolic Acid, Apigenin, Biotinyl Tripeptide-1, Diaminopyrimidine Oxide, Adenosine, Biotin and Ginkgo biloba in Patients with Androgenetic Alopecia and Telogen effluvium: A Six-month Open-Label Prospective Clinical Study. J. Cosmo. Trichol. 2018, 4. [CrossRef]
- Kim, J.; Shin, J.Y.; Choi, Y.H.; Joo, J.H.; Kwack, M.H.; Sung, Y.K.; Kang, N.G. Hair Thickness Growth Effect of Adenosine Complex in Male/Female-Patterned Hair Loss via Inhibition of Androgen Receptor Signaling. Int. J. Mol. Sci. 2024, 25, 6534. [CrossRef]
- Welzel, J.; Wolff, H.H; Gehring, W. Reduction of telogen rate and increase of hair density in androgenetic alopecia by a cosmetic product: Results of a randomized, prospective, vehicle-controlled double-blind study in men. J. Cosmet. Dermatol. 2022, 21, 1057-1064. [CrossRef]
- Sisto, T.; Bussoletti, C.; Celleno, L. Role of a Caffeine Shampoo in Cosmetic Management of Telogen Effluvium. J. Appl. Cosmetol. 2013, 31, 139-145.
- Merja, A.; Patel, N.; Patel, M.; Patnaik, S.; Ahmed, A.; Maulekhi, S. Safety and efficacy of REGENDIL™ infused hair growth promoting product in adult human subject having hair fall complaints (alopecia). J. Cosmet. Dermatol. 2023, 23, 938-948. [CrossRef]
- Oura, H.; Iino, M.; Nakazawa, Y.; et al. Adenosine increases anagen hair growth and thick hairs in Japanese women with female pattern hair loss: a pilot, double-blind, randomized, placebo-controlled trial. J. Dermatol. 2008, 35, 763-767. [CrossRef]
- Chen, D.; Yu, F.; Wang, C.; Chen, H.; Tan, J.; Shi, Q.; He, X.; Liu, X.; Wang, F.; Zhao, H. Anti-hair loss effect of a shampoo containing caffeine and adenosine. J. Cosmet. Dermatol. 2024, 00, 1-7. [CrossRef]
- Byeon, J.Y.; Choi, H.J.; Park, E.S.; Kim, J.Y.; Effectiveness of Hair Care Products Containing Placental Growth Factor for the Treatment of Postpartum Telogen Effluvium. Arch. Aesthetic Plast. Surg. 2017, 23, 73-78.
- Sawaya, M.E.; Shapiro, J. Alopecia: unapproved treatments or indications. Clin. Dermatol. 2000, 18, 177-186. [CrossRef]
- Tansathien, K.; Ngawhirunpat, T.; Rangsimawong, W.; Patrojanasophon, P.; Opanasopit, P.; Nuntharatanapong, N. In Vitro Biological Activity and In Vivo Human Study of Porcine-Placenta-Extract-Loaded Nanovesicle Formulations for Skin and Hair Rejuvenation. Pharmaceutics. 2022, 14, 1846. [CrossRef]
- Ringrow, H. Peptides, proteins and peeling active ingredients: exploring ‘scientific’ language in English and French cosmetics advertising. Études de Stylistique Anglaise 2017, 7, 183-210.
- Arroyo, M.D. Scientific language in skin-care advertising: Persuading through opacity. Revista Española de Lingüística Aplicada 2013, 26, 197-214.
- Fowler, J.G.; Reisenwitz, T.H.; Carlson, L. Deception in cosmetics advertising: Examining cosmetics advertising claims in fashion magazine ads. Journal of Global Fashion Marketing 2015, 6, 194–206. [CrossRef]
- Brown, R. What Is Science-Washing, And Can The Beauty Industry Do Anything About It? Beauty Independent , 18 Apr. 2022. https://www.beautyindependent.com/what-science-washing-can-the-beauty-industry-do-anything/.
- Mehtonen, R. Science-washing in Skincare Marketing. University of Helsinki, 2024.
- Wong M. Scientism or “Science-Washing” in Beauty. Lab Muffin Beauty Science. April 14, 2019. Accessed September 5, 2025. https://labmuffin.com/scientism-or-science-washing-in-beauty/.
- Siegel, S.T.; Terdenge, J. The Fine art of Detecting Sciencewashing: Definition, Consequences, Forms & Prevention. . Journal Trends und Themen aus der Wissenschaftskommunikation 2023, 1-4.
- Crowther, T. Science-washing: The flawed ways beauty brands are marketing products Cosmetics Business 2024.
- Murphy, L.A.; White, I.R.; Rastogi, S.C. Is hypoallergenic a credible term? Clin. Exp. Dermatol. 2004, 29, 325-327. [CrossRef]
- Boozalis, E.; Patel, S. Clinical utility of marketing terms used for over-the-counter dermatologic products. J. Dermatolog. Treat. 2018, 29, 841-845. [CrossRef]
- Draelos, Z.D. Cosmeceuticals. In Evidence-Based Procedural Dermatology, Alam, M., Ed.; Springer: Cham, 2019; pp. 479–497.
- Malinowska, P. Dermocosmetic packaging as an instrument of marketing communication. Zeszyty Naukowe Politechniki Poznańskiej. Organizacja i Zarządzanie 2020, 82, 159-171. [CrossRef]
- Hiranput, S.; McAllister, L.; Hill, G.; Yesudian, P.D. Do hypoallergenic skincare products contain fewer potential contact allergens? Clin. Exp. Dermatol. 2024, 49, 386-387. [CrossRef]
- Pokorska, P.; Śpiewak, R. Analiza składu kosmetyków rekomendowanych przez Polskie Towarzystwo Dermatologiczne oraz Polskie Towarzystwo Alergologiczne pod kątem występowania substancji o znanym potencjale uczulającym. Alergol. Immunol. 2012, 9, 227-232.
- Nurzyńska, M.; Śpiewak, R. The assessment of declared compositions of skin care products recommended by the Children’s Health Center and the Institute of Mother and Child with regard to the presence of ingredients with known sensitizing potential. Estetol. Med. Kosmetol. 2013, 3, 004.en. [CrossRef]
- Mosahebi, A. Commentary on: The Fountain of Stem Cell-Based Youth? Online Portrayals of Anti-Aging Stem Cell Technologies. Aesthet. Surg. J. 2015, 35, 737-738. [CrossRef]
- Kashihara, H.; Nakayama, T.; Hatta, T.; Takahashi, N.; Fujita, M. Evaluating the Quality of Website Information of Private-Practice Clinics Offering Cell Therapies in Japan. Interact. J. Med. Res. 2016, 5, e15. [CrossRef]
- Murdoch, B.; Zarzeczny, A.; Caulfield, T. Exploiting science? A systematic analysis of complementary and alternative medicine clinic websites’ marketing of stem cell therapies. BMJ Open 2018, 8, e019414. [CrossRef]
- Kent, D.M. Overall average treatment effects from clinical trials, one-variable-at-a-time subgroup analyses and predictive approaches to heterogeneous treatment effects: Toward a more patient-centered evidence-based medicine. Clin. Trials 2023, 20, 328-337. [CrossRef]
- Finocchiaro, M.A. The fallacy of composition: Guiding concepts, historical cases, and research problems. J. Appl. Logic. 2015, 13, 24-43. [CrossRef]
- Miao, Y.; Sun, Y.; Wang, W.; Du, B.; Xiao, S.E.; Hu, Y.; Hu, Z. 6-Gingerol inhibits hair shaft growth in cultured human hair follicles and modulates hair growth in mice. PLoS One 2013, 8, e57226. [CrossRef]
- Hou, C.; Miao, Y.; Ji, H.; Wang, S.; Liang, G.; Zhang, Z.; Hong, W. 6-Gingerol inhibits hair cycle via induction of MMP2 and MMP9 expression. An Acad. Bras. Cienc. 2017, 89, 2707-2717. [CrossRef]
- Haslam, I.S.; Hardman, J.A.; Paus, R. Topically Applied Nicotinamide Inhibits Human Hair Follicle Growth Ex Vivo. J. Invest. Dermatol. 2018, 138, 1420-1422. [CrossRef]
- Oblong, J.E.; Peplow, A.W.; Hartman, S.M.; Davis, M.G. Topical niacinamide does not stimulate hair growth based on the existing body of evidence. Int. J. Cosmet. Sci. 2020, 42, 217-219. [CrossRef]
- Choi, Y.H.; Shin, J.Y.; Kim, J.; Kang, N.G.; Lee, S. Niacinamide Down-Regulates the Expression of DKK-1 and Protects Cells from Oxidative Stress in Cultured Human Dermal Papilla Cells. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1519-1528. [CrossRef]
- Davis, M.G.; Piliang, M.P.; Bergfeld, W.F.; Caterino, T.L.; Fisher, B.K.; Sacha, J.P.; Carr, G.J.; Moulton, L.T.; Whittenbarger, D.J.; Schwartz, J.R. Scalp application of antioxidants improves scalp condition and reduces hair shedding in a 24-week randomized, double-blind, placebo-controlled clinical trial. Int. J. Cosmet. Sci. 2021, 43 Suppl 1, S14-S25. [CrossRef]
- Khare, S. Efficacy of Dr. SKS Hair Booster Serum in the Treatment of Female Pattern Alopecia in Patients With PCOS: An Open-Label, Non-randomized, Prospective Study. Cureus 2023, 15, e44941. [CrossRef]
- Khare, S. The Efficacy and Safety of Dr. SKS Hair Booster Serum (a Cocktail of Micronutrients and Multivitamins) in Adult Males and Females With Androgenetic Alopecia: An Open-Label, Non-randomized, Prospective Study. Cureus 2023, 15, e37424. [CrossRef]
- Royal Botanic Gardens, Kew: Plants of the World Online. https://powo.science.kew.org/results?q=Curcuma (electronic document, accessed on 26 July 2025).
- Vaughn, A.R.; Branum, A.; Sivamani, R.K. Effects of Turmeric (Curcuma longa) on Skin Health: A Systematic Review of the Clinical Evidence. Phytother. Res. 2016, 30, 1243-1264. [CrossRef]
- Alam, M.S.; Anwar, M.J.; Maity, M.K.; Azam, F.; Jaremko, M.; Emwas, A.H. The Dynamic Role of Curcumin in Mitigating Human Illnesses: Recent Advances in Therapeutic Applications. Pharmaceuticals (Basel) 2024, 17, 1674. [CrossRef]
- Alam, S.; Lee, J.; Sahebkar, A. Curcumin in Cancer Prevention: Insights from Clinical Trials and Strategies to Enhance Bioavailability. Curr. Pharm. Des. 2024, 30, 1838-1851.
- Dipalma, G.; Inchingolo, A.M.; Latini, G.; Ferrante, L.; Nardelli, P.; Malcangi, G.; Trilli, I.; Inchingolo, F.; Palermo, A.; Inchingolo, A.D. The Effectiveness of Curcumin in Treating Oral Mucositis Related to Radiation and Chemotherapy: A Systematic Review. Antioxidants (Basel) 2024, 13. [CrossRef]
- Jafari, A.; Abbastabar, M.; Alaghi, A.; Heshmati, J.; Crowe, F.L.; Sepidarkish, M. Curcumin on Human Health: A Comprehensive Systematic Review and Meta-Analysis of 103 Randomized Controlled Trials. Phytother. Res. 2024, 38, 6048-6061. [CrossRef]
- Ayub, H.; Islam, M.; Saeed, M.; Ahmad, H.; Al-Asmari, F.; Ramadan, M.F.; Alissa, M.; Arif, M.A.; Rana, M.U.J.; Subtain, M.; et al. On the health effects of curcumin and its derivatives. Food Sci. Nutr. 2024, 12, 8623-8650. [CrossRef]
- Das, G.; Kameswaran, S.; Ramesh, B.; Bangeppagari, M.; Nath, R.; Das Talukdar, A.; Shin, H.S.; Patra, J.K. Anti-Aging Effect of Traditional Plant-Based Food: An Overview. Foods 2024, 13. [CrossRef]
- Pumthong, G.; Asawanonda, P.; Varothai, S.; Jariyasethavong, V.; Triwongwaranat, D.; Suthipinittharm, P.; Ingkaninan, K.; Leelapornpisit, P.; Waranuch, N. Curcuma aeruginosa, a novel botanically derived 5alpha-reductase inhibitor in the treatment of male-pattern baldness: a multicenter, randomized, double-blind, placebo-controlled study. J. Dermatolog. Treat. 2012, 23, 385-392. [CrossRef]
- Suphrom, N.; Pumthong, G.; Khorana, N.; Waranuch, N.; Limpeanchob, N.; Ingkaninan, K. Anti-androgenic effect of sesquiterpenes isolated from the rhizomes of Curcuma aeruginosa Roxb. Fitoterapia 2012, 83, 864-871. [CrossRef]
- Suphrom, N.; Srivilai, J.; Pumthong, G.; Khorana, N.; Waranuch, N.; Limpeanchob, N.; Ingkaninan, K. Stability studies of antiandrogenic compounds in Curcuma aeruginosa Roxb. extract. J. Pharm. Pharmacol. 2014, 66, 1282-1293. [CrossRef]
- Srivilai, J.; Phimnuan, P.; Jaisabai, J.; Luangtoomma, N.; Waranuch, N.; Khorana, N.; Wisuitiprot, W.; Scholfield, C.N.; Champachaisri, K.; Ingkaninan, K. Curcuma aeruginosa Roxb. essential oil slows hair-growth and lightens skin in axillae; a randomised, double blinded trial. Phytomedicine 2017, 25, 29-38. [CrossRef]
- Kanase, V.; Khan, F. An overview of medicinal value of curcuma species. Asian J. Pharm. Clin. Res. 2018, 11, 40-45. [CrossRef]
- Abia, W.A.; Haughey, S.A.; Radhika, R.; Taty, B.P.; Russell, H.; Carey, M.; Maestroni, B.M.; Petchkongkaew, A.; Elliott, C.T.; Williams, P.N. Africa, an Emerging Exporter of Turmeric: Combating Fraud with Rapid Detection Systems. Foods 2025, 14, 1590. [CrossRef]
- Guyatt, G.; Wang, Y.; Eachempati, P.; Iorio, A.; Murad, M.H.; Hultcrantz, M.; Chu, D.K.; Florez, I.D.; Hemkens, L.G.; Agoritsas, T.; et al. Core GRADE 4: rating certainty of evidence-risk of bias, publication bias, and reasons for rating up certainty. BMJ 2025, 389, e083864. [CrossRef]
- Terán-Bustamante, A.; Martínez-Velasco, A.; López-Fernández, A.M. University–Industry Collaboration: A Sustainable Technology Transfer Model. Adm. Sci. 2021, 11, 142. [CrossRef]
- Pujotomo, D.; Syed Hassan, S.A.H.; Ma’aram, A.; Sutopo, W. University–industry collaboration in the technology development and technology commercialization stage: a systematic literature review. J. Appl. Res. Higher Educ. 2023, 15, 1276-1306. [CrossRef]
- Steel, D. If the Facts Were Not Untruths, Their Implications Were: Sponsorship Bias and Misleading Communication. Kennedy Inst. Ethics J 2018, 28, 119-144. [CrossRef]
- Marx, R.E. The deception and fallacies of sponsored randomized prospective double-blinded clinical trials: the bisphosphonate research example. Int. J. Oral Maxillofac. Implants 2014, 29, e37-44. [CrossRef]
- Rollins, N.; Piwoz, E.; Baker, P.; Kingston, G.; Mabaso, K.M.; McCoy, D.; Ribeiro Neves, P.A.; Perez-Escamilla, R.; Richter, L.; Russ, K.; et al. Marketing of commercial milk formula: a system to capture parents, communities, science, and policy. Lancet 2023, 401, 486-502. [CrossRef]
- Antonio, J.; Antonio, B.; Aragon, A.; Bustillo, E.; Candow, D.; Collins, R.; Davila, E.; Durkin, B.; Kalman, D.; Lockwood, C.; et al. “Common questions and misconceptions about dietary supplements and the industry - What does science and the law really say?”. J. Int. Soc. Sports Nutr. 2025, 22, 2534128. [CrossRef]
- Vojvodic, S.; Kobiljski, D.; Srdenovic Conic, B.; Torovic, L. Landscape of Herbal Food Supplements: Where Do We Stand with Health Claims? Nutrients 2025, 17, 1571. [CrossRef]
- Pappas, C.; Williams, I. Grey Literature: Its Emerging Importance. J. Hosp. Librarianship 2011, 11, 228-234. [CrossRef]
- Paez, A. Grey literature: An important resource in systematic reviews. J Evid Based Med 2017. [CrossRef]
- Kolaski, K.; Logan, L.R.; Ioannidis, J.P.A. Guidance to best tools and practices for systematic reviews. BMC Infect Dis. 2023, 23, 383. [CrossRef]
- Zhang, H.; Mao, R.; Huang, H.; Dai, Q.; Zhou, X.; Shen, H.; Rong, G. Processes, challenges and recommendations of Gray Literature Review: An experience report. Information Software Technol. 2021, 137, 106607. [CrossRef]
Figure 1.
PRISMA protocol for data acquisition.
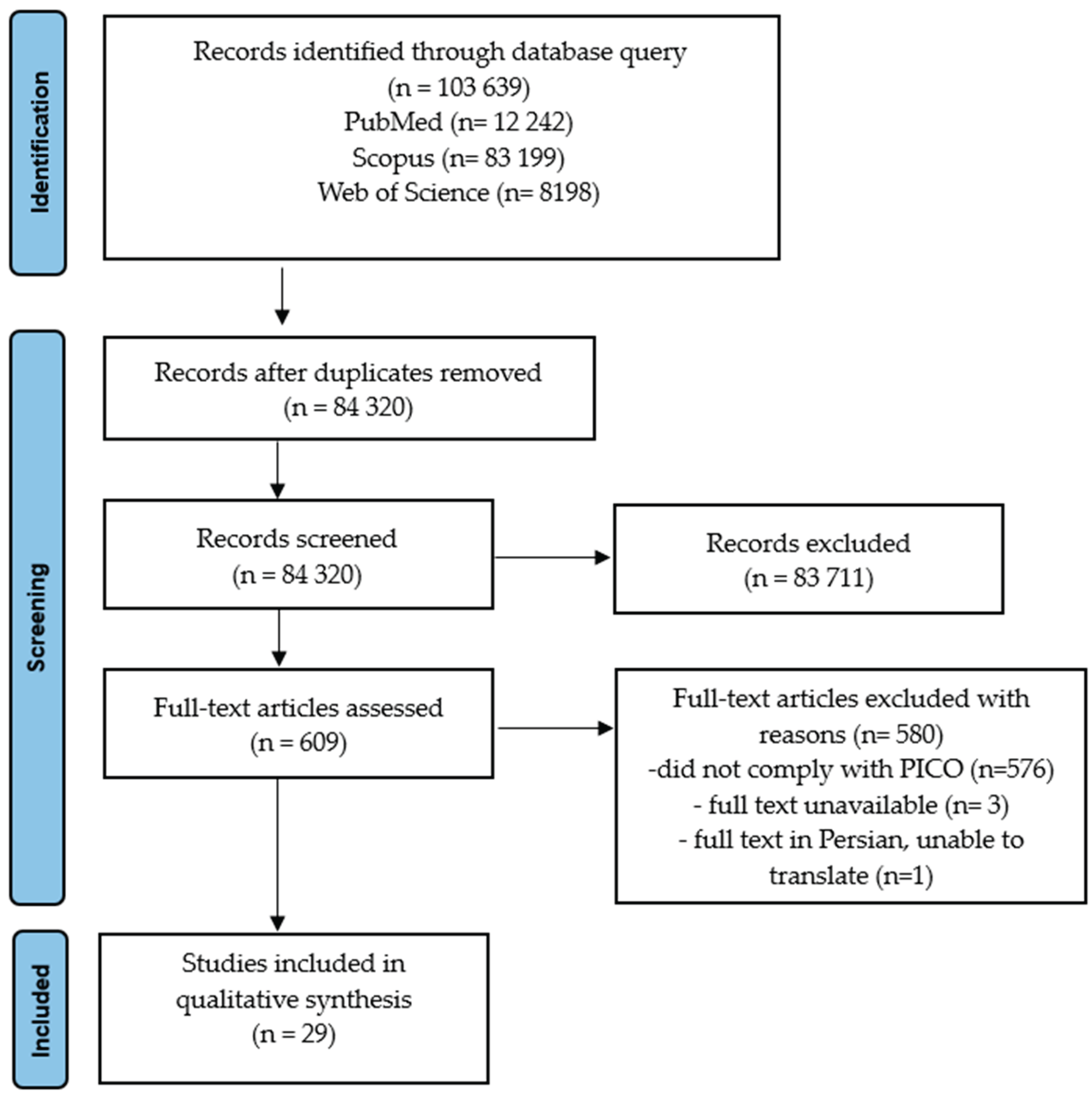

Table 1.
Inclusion criteria for the human studies covered in this systematic review.
| PICO criterion | Description |
|---|---|
| Patients/Participants | People suffering from baldness, hair loss, effluvium or alopecia |
| Intervention | Ingredients of interest tested in topical anti-hair loss preparations |
| Comparator/Control | Placebo or other topical anti-hair loss preparations, no comparator |
| Outcomes | Phototrichogram, trichoscopy, investigator assessment (IA), participant assessment (PA) |
Table 2.
Ingredients declared by the manufacturer as “active against hair loss” which were present in at least two of the 43 analyzed trichological shampoos.
Table 2.
Ingredients declared by the manufacturer as “active against hair loss” which were present in at least two of the 43 analyzed trichological shampoos.
| Ingredient | CAS number | Origin | N | A |
|---|---|---|---|---|
| Achillea millefolium extract | 84082-83-7 | Plant | 5 | 4 |
| Adenosine | 58-61-7 | Animal, various | 3 | 3 |
| Aloe barbadensis | 85507-69-3 | Plant | 6 | 2 |
| Arginine | 74-79-3 | Synthetic, plant, animal | 4 | 4 |
| Biotin | 58-85-5 | Synthetic, plant | 10 | 2 |
| Caffeine | 58-08-2 | Synthetic, plant | 7 | 6 |
| Calcium pantothenate | 137-08-6 | Synthetic, natural | 5 | 2 |
| Capsicum | 85940-30-3 | Plant | 9 | 7 |
| Cinchona succirubra bark extract | 84776-28-3 | Plant | 3 | 3 |
| Citrus paradisi extract | 90045-43-5 | Plant | 2 | 2 |
| Gardenia jasminoides meristem cell culture | - | Plant | 2 | 2 |
| Glycine soja germ extract | - | Plant | 2 | 2 |
| Humulus lupulus extract | 8060-28-4 | Plant | 5 | 2 |
| Hydrolyzed collagen | 92113-31-0 | Animal | 5 | 4 |
| Hydrolyzed keratin | 69430-36-0 | Animal, plant | 6 | 2 |
| Hydrolyzed soy protein | 68607-88-5 | Plant | 5 | 2 |
| Hydrolyzed wheat protein | 94350-06-8 | Plant | 6 | 2 |
| Lavandula Angustifolia oil | 8000-28-0 | Plant | 2 | 2 |
| Melaleuca Ericifolia Oil | 85085-48-9 | Plant | 2 | 2 |
| Malus domestica fruit cell culture | - | Plant | 5 | 3 |
| Medicago sativa extract | 84082-36-0 | Plant | 2 | 2 |
| Melatonin | 73-31-4 | Synthetic | 4 | 3 |
| Menthol | 1490-04-6 | Plant | 11 | 3 |
| Panax ginseng root extract | 84650-12-4 | Plant | 6 | 2 |
| Panicum milialecum | 90082-36-3 | Plant | 2 | 2 |
| Panthenol | 81-13-0 | Synthetic | 23 | 2 |
| Piroctone olamine | 68890-66-4 | Synthetic | 2 | 2 |
| Placental protein | 84195-59-5 | Animal | 5 | 3 |
| Prunus amygdalus dulcis oil | 8007-69-0 | Plant | 4 | 4 |
| Rosmarinus officinalis leaf extract | 84604-14-8 | Plant | 9 | 6 |
| Royal jelly | 8031-67-2 | Animal | 2 | 2 |
| Serenoa serrulata fruit extract | 84604-15-9 | Plant | 11 | 8 |
| Tocopherol | 1406-66-2 | Plant, synthetic | 7 | 2 |
| Tocopheryl acetate | 7695-91-2 | Plant, synthetic | 11 | 2 |
| Tussilago farfara extract | 84625-50-3 | Plant | 3 | 3 |
| Urtica dioica extract | 84012-40-8 | Plant | 9 | 3 |
Abbreviations: CAS – Chemical Abstracts Service; N – number of shampoos that according to the manufacturer’s declaration contained the given ingredient of interest; A – number of shampoos in which the given ingredient was advertised as “active”.
Table 3.
Types of hair loss included in the clinical trials of ingredients of interest.
| Hair problem |
Main features | Diagnostic methods used | Ref. |
|---|---|---|---|
| Androgenetic alopecia |
Miniaturization of hair follicles in androgen-dependent areas | Dermatoscopy, trichoscopy | [44–47,49–66] |
| Telogen effluvium |
It occurs about three months after the triggering factor, e.g., infection, drug use, hormonal disorders, metabolic diseases, nutritional deficiencies, or stress | Positive pull test, trichogram, laboratory tests for underlying conditions | [48,64,67] |
| Hair loss (unspecified) |
Losing more hair than usual for longer than three months | Positive pull test, trichogram, laboratory tests for underlying conditions | [44,49,68] |
| Female pattern hair loss | Miniaturization of hair follicles in androgen-dependent areas | Dermatoscopy, trichoscopy | [51,69] |
| Thinning hair | A noticeable reduction in hair density | Dermatoscopy, trichoscopy | [70] |
| Diffuse alopecia |
A large number of hairs prematurely entering the telogen phase, resulting in diffuse hair loss | Dermatoscopy, trichoscopy | [45] |
| Postpartum hair loss | Typically occurs about three months after childbirth | Positive pull test, trichogram, laboratory tests for underlying conditions | [71] |
Table 4.
Topical ingredients tested individually in clinical trials which were subject to previous systematic reviews in the series. More details are presented in Table S1 in the Supplementary material.
Table 4.
Topical ingredients tested individually in clinical trials which were subject to previous systematic reviews in the series. More details are presented in Table S1 in the Supplementary material.
| Ingredient | Total participants |
GRADE | Overall conclusions | Ref. |
|---|---|---|---|---|
| Adenosine | 466 | Tested individually: - moderate: 2 trials [63,69] - low: 2 trials [61,62] Tested in complex products: - low: 2 trials [65,70] - very low: 1 trial [64] |
Published trials seem to support the effectiveness of topical adenosine products against hair loss | [18] |
| Caffeine | 684 | Tested individually: - moderate: 1 trial [56] - low: 1 trial [57] - very low: 2 trials [58,67] Tested in complex products: - moderate: 2 trials [66,70] - very low: 3 trials [59,60,68] |
Published trials seem to support the effectiveness of topical caffeine products against hair loss | [14] |
| Placenta derivatives | 127 | Tested individually: - low: 2 trials [55,73] Tested in complex products: - very low: 1 trial [71] |
Published trials seem to support the effectiveness of topical placenta products in both stopping hair loss and stimulating hair growth | [41] |
GRADE - strength of evidence expressed in the GRADE scale [43].
Table 5.
An overview of the double-blind, randomized, placebo-controlled study of the efficacy of topical melatonin in hair loss [44]. More details are presented in Table S1 in the Supplementary material.
Table 5.
An overview of the double-blind, randomized, placebo-controlled study of the efficacy of topical melatonin in hair loss [44]. More details are presented in Table S1 in the Supplementary material.
| Patients | Intervention | Comparator | Outcome (reviewers’ summary) | GRADE |
|---|---|---|---|---|
| 12 F with AGA |
Melatonin 0.1% alcoholic solution (leave-on) | Alcohol | After 6 months of treatment, significantly higher anagen rate (85.0%) in mean occipital hair of melatonin-treated group than placebo (82.1%, p=0.012). A reverse tendency in frontal hair (80.4% versus 84.9%; ns). | moderate |
| 28 F with DA |
Melatonin 0.1% alcoholic solution (leave-on) | Alcohol | After 6 months of treatment, significantly higher anagen rate (83.8%) in mean frontal hair of melatonin-treated group than placebo (81.1%, p=0.046). A reverse tendency in occipital hair (83.7% versus 84.9%; ns). | moderate |
Abbreviations: AGA – androgenic alopecia; DA – diffuse alopecia; ns – non significant, GRADE - strength of evidence expressed in the GRADE scale [43].
Table 6.
An overview of clinical trials of complex products containing substances of interest (marked in italics). More details are presented in Table S2 in the Supplementary material.
Table 6.
An overview of clinical trials of complex products containing substances of interest (marked in italics). More details are presented in Table S2 in the Supplementary material.
| Study design | Patients | Intervention | Comparator | Major outcomes | GRADE | Ref. |
|---|---|---|---|---|---|---|
| Single-center, uncontrolled | 18 P with AGA, hair loss and thinning hair | Marketed hair lotion (leave-on) with biotin, thioglycoran, HUCP1, thurfyl nicotinate, sodium pantothenate (undiscl. conc.) | None | After 60 d: incr. anagen hair ratio (p<0.001), incr. growth rate (p<0.001). | very low | [49] |
| Single-center, open-label, uncontrolled |
20 M with AGA | Lotion (leave-on) with piroctone olamine (0.25%), triclosan (0.3%) | None | HCD index sign. decr. after 6 m. of treatment (-22.2%, p<0.05) and further on. Negative logarithmic correlation (r=-0.64, p<0.01) between time of treatment and HCD index. | very low | [52] |
| Single-center, open-label, uncontrolled |
30 M and F with AGA |
Lotion (leave-on) with melatonin 0.0033%, Ginkgo biloba (undiscl. conc.), biotin (undiscl. conc.) | None | Investigator assessment of alopecia severity decr. after 30 d. (-34.1%, p<0.001) and 60 d. (-39.0, p<0.001). P assessment of alopecia severity decr. after 30 d. (-68.3%, p<0.001) and 60 d. (-75.1%, p<0.001). |
very low | [44]2 |
| Single-center, open-label, uncontrolled | 35 M with AGA | Incr. hair density after 3 m. (+29.1%, p<0.001) and 6 m. (+40.9%, p<0.001). Rate of P satisfied (mostly satisfied) with the shampoo 93.2% after 3 m.: and after 6 m. |
very low | |||
| Multi-center, open-label, uncontrolled | 60 M and F hair loss or thinning hair | Hair stylist assessment after 90 d.: impr. of hair texture score by 18.5% (p<0.001), impr. hair loss score by 11.8% (p<0.001). | very low | |||
| Multi-center, open-label, uncontrolled | 1800 M and F with AGA | Investigator assessment: proportion of P with severe and moderate hair loss decr. from 61.6% at the beginning to 33.7% after 30 d. (p<0.001) and to 7.8% after 90 d. (p<0.001). Proportion of P with no hair loss incr. from 12.2% to 25.5% after 30 d. (p<0.001) and 61.5% after 90 d. (p<0.001). | very low | |||
| Single-center, open-label, uncontrolled |
50 M with AGA |
Marketed serum (leave-on) and shampoo (rinse-off) with Serenoa serrulata, green tea extract, peony root extract, piroctone olamine, oligopeptides (undiscl. conc.) | None | Sign. incr. in hair density after 6 w (+21.5%, p<0.001) and 12 w (+74.1%, p<0.001). | very low | [54] |
| Single-center, open-label, uncontrolled |
25 F with postpartum hair loss |
Shampoo (rinse-off) and tonic (leave-on) with equine placental growth factor (PIGF), pumpkin extract, panthenol, and niacinamide (undiscl. conc.) | None | After 3 m.: increased vertex hair thickness (+5.6%, p=0.028), increased occipital hair density (+8.1%, p<0.001) | very low | [71] |
| Single-center, open-label, prospective uncontrolled |
56 M and F with AGA (36 P) and TE (24 P) |
Lotion (leave-on) with oleanolic acid, apigenin, biotinyl tripeptide-1, 2-4-diamino pyrimidine-3-oxide, adenosine, Ginkgo biloba, biotin (undiscl. conc.) | None | After 6 mo, 79% P reported reduced hair loss, 86% P were satisfied with the results | very low | [64] |
| Single center, randomized, placebo-controlled, single-blind |
120 M and F with AGA | Shampoo (rinse-off) and solution (leave-on) with Urtica urens leaf extract, Urtica dioica root extract, Matricaria chamomilla flower extract, Achillea millefolium aerial part extract, Ceratonia siliqua fruit extract, Equisetum arvense leaf extract (undiscl. conc.) | Placebo shampoo and solution | After 6 mo, impr. anagen/telogen rate for both shampoo (sh) and solution (so, p<0.001). Efficacy ranking: sh+so> so > sh > placebo |
moderate | [46] |
| Single-center, open-label, uncontrolled |
5 M with AGA |
Solution (leave-on) with MNX (10%), finasteride (0.1%), biotin (0.2%), caffeine citrate (0.05%) | None | After 6 mo, assessment by a non-blinded expert: clinical improvements “visually noticeable” in all 5 patients. A blinded physician rated the overall effect as +0.75 in 1 P, +1.00 in 2 P, and +1.25 in further 2 P on a scale where 0 means “no change”, +1 – “slightly incr.” and +2 “moderately incr.”. 100% P satisfied after 180 d of the treatment. |
very low | [50] |
| Randomized, double-blind, controlled |
16 M and 16 F with AGA | Marketed hair tonic (leave-on) with acetyl tetrapeptide-3, biochanin A (red clover extracts), Panax ginseng extract, Salvia officinalis oil (undiscl. conc.) | 3% MNX solution | Blinded experts’ assessment after 24 w: in the vertex area, hair status improved (from slightly to greatly) in 100% participants both in I and C groups, “excellent improvement” in 12.5% of the I group and 21.0% in C group (ns). In frontal area, hair status improved in 87.5% of I group and 85.0% in C group (ns). Incr. of terminal hair count in both I group (8.3%, p=0.009) and C group (8.7%, p=0.002), no significant differences between groups. Increased HMI in both groups: I (13.8%, p=0.008) and C (31.5%, p=0.026) at after 24 w, no difference between the two groups (p=0.158). |
moderate | [51] |
| Single-center, randomized, double-blind, controlled |
24 M with AGA |
Morning: 5% MNX lotion (leave-on) Evening: Lotion (leave-on) with Rosmarinus officinalis, Olea europaea, lipidosterolic extract of Serenoa serrulata (undiscl. conc.) |
5% MNX lotion (morning and evening) | Hair diameter bigger in I group than C group after 24 w (+19.0%, p=0.005) and 36 w. (23.9%, p=0.001). No significant changes in hair density. PA score significantly lower (better outcome) in I group than C group (for various questions decrease by 45.4% to 59.1%, p from 0.001 to 0.007). |
moderate | [53] |
| Multi-center, open-label, observational |
527 M and F with AGA |
Marketed cosmetic solution (leave-on) with DPNO, arginine, 6-O glucose linoleate (SP94), piroctone olamine, Vichy mineralizing water (undiscl. conc.) | None | After 3 mo, 89.0% P and 96.7% treating dermatologists satisfied with the product. | very low | [47] |
| Two-center, open, randomized, controlled |
100 F with positive pull test (TE) |
Marketed hair lotion (leave-on) with acetyl tetrapeptite-2, biotin, creatine, panthenol, pyridoxine HCl (undiscl. conc.); + marketed neutral shampoo (rinse-off) |
Marketed neutral shampoo only | After 8 w. decr. in density of telogen hairs higher in intervention group than controls (p=0.0465). Reduction in total number of hairs shed in 60 s larger in I group than in C group after 8 w. (-31.8% vs. -13.5%, p= 0.0392), and 16 w. (-43.6% vs. -33.1%, p=0.0584). No significant difference in Anagen/Telogen Ratio between I group and C group (p=0.320). | low | [48] |
| Randomized, controlled, double-blind |
62 M with AGA | Foam (leave-on) with polyphenols (DHQG and EGCG2), NHE, zinc salt (anion unspecified), glycine, caffeine (undiscl. conc.) | Vehicle | After 3 and 6 mo: stronger decrease in telogen rate in I group than C group (p=0.02). Increase in hair density observed in both I group (p=0.001) and C group (p=0.04). No significant differences between I and C. |
moderate | [66] |
| Single-center, open-label, uncontrolled |
150 P with AGA (60 M and 90 W) | Marketed serum (leave-on) in a roller with caffeine, Serenoa serrulata, and 25 other ingredients (undiscl. conc.) | None | After 8 w, incr. thickness and density of crown and vertex hair (p<0.05), no significant changes in frontal hair. P satisfaction rates in various aspects of hair growth between 80-100%, except hair length (40%). |
very low | [59] |
| Single-center, open-label, uncontrolled |
32 M and F with hair loss or alopecia |
Marketed hair serum (leave-on) with hydrolyzed wheat protein, hydrolyzed soy protein, caffeine, arginine, Rosmarinus officinalis leaf oil and 18 other ingredients (undiscl. conc.) | none | Incr. hair growth rate after 30 d. (+10.5%, p<0.01) and 60 d. (+31.6%, p<0.01). Incr. hair thickness after 30 d. (+24%, p<0.01) and 60 d. (+34%, p<0.01). Incr. hair density after 30 d. (+25%, p<0.01) and 60 d. (+40%, p<0.01). |
very low | [68] |
| Single-center, open-label, uncontrolled |
20 M with AGA | Liquid (leave-on) with Procapil™ 3%3, caffeine (undiscl. conc.), zinc PCA4 (undiscl. conc.) | None | After 12 wk.: a 26.9% decrease in hair loss (p=0.026), 53% increase in terminal/vellus hair ratio (p=0.028), no significant changes in anagen rate and density. Investigator assessment: improvement (slight to much) in 68.4% P. | very low | [60] |
| Single center, randomized, placebo-controlled, double-blind |
46 P with AGA (27 M and 19 W) | Solution “APN” (leave-on) with adenosine (0.75%), panthenol (1%), niacinamide (2%) | Solution with MNX 5% | After 4 mo, incr. in hair density (I group: +6.2%, p<0.001; C group: +5.0%, p<0.01) and hair thickness (I: +10.3%, p<0.001; C: +5.1%, p<0.001). No direct comparisons I vs C. | low | [65] |
| Single center, randomized, placebo-controlled, single-blind |
84 M and F with self-perceived “thinning hair” |
Shampoo (rinse-off) with caffeine (0.4%) and adenosine (0.2%) | Placebo shampoo | After 3 mo, hair density incr.by 10.2%, hair loss decr. by 35.5% (each p<0.001 as compared with baseline and C group) | low | [70] |
Abbreviations: AGA – androgenic alopecia; C – comparator/control (placebo, sham treatment); d – days; DHQG - dihydroquercetin-glycoside; DPNO – 2,4-diamino-pyrimidine-N-oxide, EGCG2 - epigallocatechingallate-glucoside 2; F – female(s); I – intervention (verum, test treatment); ; IA – investigator’s assessment; incr. – increase(d); decr. – decrease(d); HCD index - hair cycle disturbance index; HMI - hair mass index; impr. – improved/improvement; M – male(s); MNX – minoxidil; mo – month(s); NHE - nicotinic acid hexyl ester; ns – non significant; P – participant(s); PA – participant’s assessment; sign. – significant(ly); TE – telogen effluvium; undiscl. conc. – undisclosed concentration(s); w – week(s). 1 The ingredient hidden under the acronym HUCP was not disclosed by authors of the source paper. In the context of hair loss products, Sawaya and Shapiro used it for hyaluronic acid [72], no other uses or explanation could be found in indexed literature or PubChem. 2 Article [44] presents data from 4 separate trials. 3 Procapil™ - a proprietary complex of oleanolic acid, apigenin and biotinoyl tripeptide-1. 4 Zinc PCA - a complex of one zinc anion and two molecules of pyrrolidone carboxylic acid (PCA).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



