1. Introduction
Aortic valve replacement (AVR), whether surgical or transcatheter, serves as the primary therapeutic option for symptomatic severe aortic stenosis (AS) or regurgitation (AR). It’s vital to conduct structural and functional assessments of the replacement valve in these patients. Transthoracic echocardiography is a key tool for evaluating valvular function and structural integrity, primarily because of its non-invasive nature, wide availability, and absence of ionizing radiation exposure. Various echocardiographic parameters, including mean and peak transvalvular gradients (TVG), the dimensionless index (the ratio of left ventricular outflow tract (LVOT) to aortic valve time velocity integrals (TVIs)), effective orifice area (EOA) calculated using the continuity equation, and geometric orifice area determined by planimetry, can be used to assess valvular function. Nevertheless, numerous studies have highlighted significant discrepancies between echocardiographic and cardiac catheterization measurements, often referred to as “discordance.” This may be due to various factors, including but not limited to flow jet eccentricity, the pressure recovery phenomenon, limitations of the Bernoulli equation, flow rates, and prosthetic valve design (1-3).
Another critical factor influencing TVG is prosthesis-patient mismatch (PPM), which occurs when the EOA of a normally functioning prosthetic valve is too small in relation to the patient’s body size (4). In surgically implanted aortic prostheses, PPM can result in elevated TVG, increased left ventricular afterload, and potential adverse outcomes. Its presence may also complicate echocardiographic assessments, making it challenging to differentiate true structural valve deterioration from flow-related TVG elevation (5). Elevated TVG often indicates biomechanical stress and valve deterioration, making their reliability essential for clinical decision-making. Due to the limitations of echocardiography, alternative imaging methods or invasive assessments may be required to confirm elevated echocardiographic TVGs (6,7).
This study assessed whether elevated TVG identified during routine echocardiographic follow-up in patients with surgically implanted aortic valve prostheses reflected actual elevations by comparing these findings with invasive transseptal catheterization measurements.
2. Methods
2.1. Study Population
This retrospective cohort study included 14 patients with a history of surgical AVR between August 2018 and November 2024 [metallic (n=12) and bioprosthetic (n=2)]. Patients with increased mean and/or peak aortic TVG on routine echocardiographic follow-up or presented with symptoms suggestive of prosthetic valve dysfunction underwent invasive gradient measurements. Baseline demographic and clinical data were retrieved from patient files and the hospital’s electronic database. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Hacettepe University Health Sciences Research Ethics Committee (Approval Date: 04.03.2025, Approval Number: 2025/06-19).
2.2. Echocardiographic Assessment
All patients underwent a comprehensive transthoracic echocardiographic evaluation using a Vivid E9 ultrasound system (manufactured by GE Vingmed Ultrasound). The same cardiologist analyzed all echocardiographic measurements without being aware of the patient’s clinical status. Standard 2D-based images and Doppler measurements, including parasternal and apical views, were obtained following the current expert consensus document (8,9).
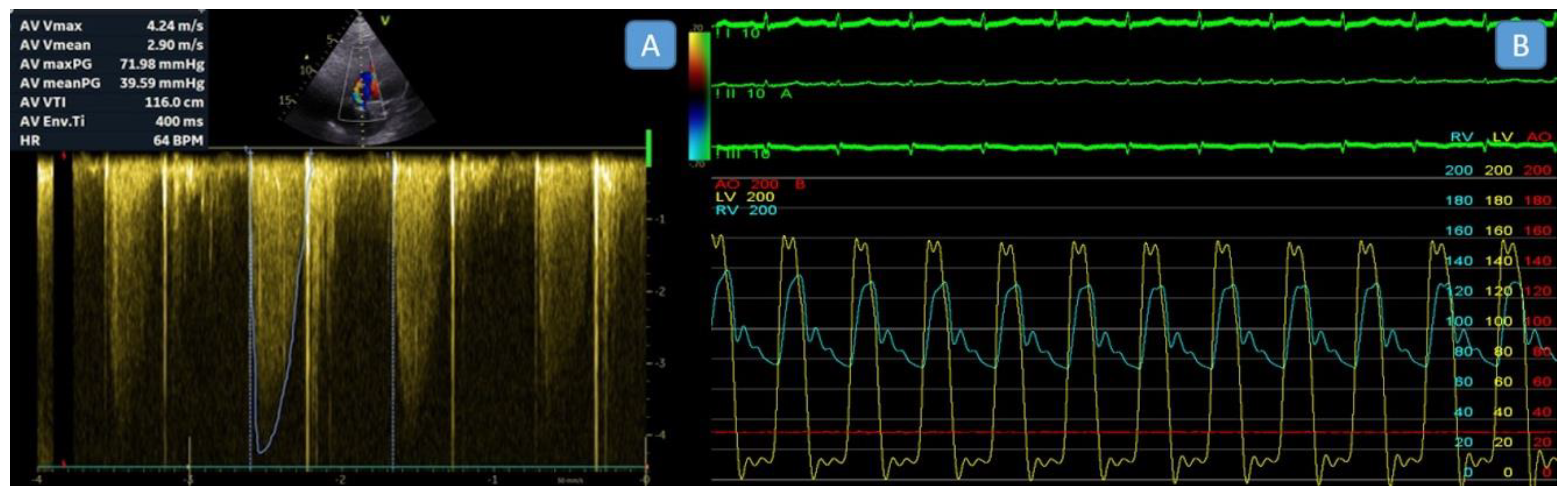
The peak velocity, mean gradient, velocity time integral (VTI), Doppler velocity index (DVI), and effective orifice area (EOA) of the aortic prosthetic valve were measured and recorded. The simplified Bernoulli equation was employed to calculate pressure gradients across aortic prosthetic valves noninvasively. Peak aortic velocity and mean aortic gradients were derived from the flow envelope, using the highest velocity recorded from multiple imaging views. The mean gradient was obtained by tracing the Doppler envelope (
Figure 1A).
The EOA of an aortic prosthesis was calculated as follows:
where the VTI
prosthetic valve is the velocity-time integral through the prosthesis determined by CW Doppler. Stroke volume was derived as the cross-sectional area just proximal to the prosthesis multiplied by the VTI of flow by PW Doppler at that site.
In cases where the replacement valve is functioning normally but is too small for the size of the recipient, patient–prosthesis mismatch in the aortic position is defined by an EOA indexed to body surface area (EOAI) of less than 0.85 cm2/m2 and severe mismatch is indicated by an EOAI of less than 0.65 cm2/m2, with normal valvular appearance and normal echocardiographic findings parameters.
2.3. Invasive Transseptal Left Heart Catheterization
The procedures were performed under conscious or deep sedation, ensuring patient comfort and procedural safety. For all patients, invasive hemodynamic measurements were obtained using a dual-catheter technique that allows for simultaneous recording of left ventricular (LV) and aortic pressures to assess TVG accurately. Two venous sheaths were placed in the femoral vein, and one arterial sheath was inserted into the femoral artery. A pigtail catheter was then positioned in the aortic root via the arterial sheath, and a diagnostic coronary sinus (CS) catheter was advanced into the CS through one of the venous sheaths to serve as markers for transseptal puncture. Using these markers as guidance, a transseptal puncture was performed employing the modified Brockenbrough technique under fluoroscopy visualization. After a successful puncture, a pigtail catheter was advanced into the left atrium and then across the mitral valve into the left ventricle (LV) (Video 1). This setup allowed for the simultaneous recording of left ventricular and aortic pressures, enabling accurate calculation of “peak-to-peak” transvalvular pressure gradients (Figure 1B). During the procedure, fluoroscopy was used to guide catheter placement and evaluate the motion and function of the prosthetic aortic valve leaflets, ensuring their proper operation during hemodynamic assessment. The dual-catheter approach is especially beneficial for patients with mechanical aortic valves, as it avoids crossing the valve apparatus, reducing the complication risk. Numerous studies have validated this method for its accuracy and reliability in measuring transvalvular pressure gradients, establishing it as a standard practice in invasive hemodynamic assessments (10,11).
2.4. Statistical Analysis
Statistical analyses were conducted using SPSS software (version 30.0). Descriptive variables were summarized as counts and percentages for categorical data. The normality of continuous variables was assessed using the Shapiro-Wilk test. Continuous variables following a normal distribution were expressed as mean ± standard deviation, while non-normally distributed data were presented as median and interquartile range. Group comparisons were performed using the independent Student’s t-test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables as appropriate. A two-tailed p-value of <0.05 was considered statistically significant.
3. Results
The baseline demographic and clinical characteristics of the 14 patients included in the study are outlined in
Table 1, and a detailed comparison of echocardiographic and catheter-derived gradients is provided in
Table 2. The mean age of the patients was 49.2 ± 16 years (range: 24 – 75 years), with the majority (71.4%) being female. Before an index valve surgery, all patients had primary severe AS, and one had an additional moderate AR. Among the cohort, 12 patients (85.7%) had mechanical bileaflet aortic valve prostheses, while the remaining two patients (14.3%) had bioprosthetic valves. Furthermore, 19mm size was implanted in 3 patients (21.4%) and 21mm size was preferred in the remaining 11 patients (78.6%). Although 9 patients (64.3%) were symptomatic on admission, the remaining 5 patients (35.7%) were asymptomatic. The median interval between aortic valve surgery and cardiac catheterization was 6.7 years, and between echocardiographic examination and cardiac catheterization was 7.2 days. The mean LVEF was 61.5 ± 4.5%, and the mean ascending aortic diameter was 33.4 ± 3.4 mm. Catheter-based measurements revealed a mean peak-to-peak transvalvular pressure gradient of 47.5 ± 21.74 mmHg, while the Doppler-derived peak gradient (77.0 ± 13.1 mmHg) was significantly higher (p<0.05). Doppler-derived mean aortic gradient was 44.2 ± 8.9 mmHg. Correlation analysis revealed no correlation between echocardiography-based mean or peak aortic gradient and catheter-based peak-to-peak aortic gradient (p=0.111, p=0.705). However, there was a significant negative correlation between the echocardiography-based aortic valve area and catheter-based peak-to-peak aortic gradient (r=-0.64, p=0.014). The EOAI also showed a significant negative correlation with catheter-based peak-to-peak aortic gradient (r=-0.63, p=0.015). Six patients (42,9%) who revealed severe catheter-based peak-to-peak aortic gradient underwent redo aortic valve surgeries. The cut-off value of EOAI of <0.50 cm
2/m
2 was found as the predictor of severe catheter-based peak-to-peak aortic gradient.
4. Discussion
There are several scenarios regarding replacement valves in clinical practice, including normal functioning, obstructed due to pannus formation, thrombosis or vegetation, and PPM. In our study, we hypothesized a fourth scenario regarding the high-pressure gradient across aortic replacement valves, which could be defined as a discrepancy between echocardiography and catheter-based measurements caused by several factors.
Long-term follow-up of prosthetic valve function requires an accurate evaluation of valve hemodynamics, as it plays a crucial role in predicting the need for future interventions. While Doppler echocardiography is well-established in assessing native valve functions, its accuracy in determining prosthetic valve function remains controversial. Numerous studies have explored the concordance between transthoracic echocardiography and invasive catheter-based TVG measurements across various patient groups. Early research demonstrated strong correlations between these modalities in cases of native aortic valve stenosis (12,13). However, subsequent investigations into prosthetic valves, including SAVR, TAVR, and ViV-TAVR, revealed notable discrepancies. While small-scale studies have provided limited data on Doppler-catheter concordance in prosthetic valves (14,15), more recent research consistently reports significant differences, with Doppler echocardiography frequently overestimating TVG. Our findings align with these previous observations, further emphasizing the limitations of Doppler methods in this context. A large multicenter study by Abbas et al. involving 808 TAVR patients demonstrated this phenomenon clearly: while good correlation existed between echocardiographic and invasive gradients in native aortic stenosis (r=0.614), this correlation became weak to absent post-TAVR (r=0.138), regardless of valve type or size (16). Similarly, DeSa et al. demonstrated that only 26 patients (7.2%) had abnormal Doppler gradients immediately post-TAVR, but this increased to 109 patients (30.1%) at discharge, emphasizing the temporal evolution of this discordance phenomenon (17).
The discrepancy between echocardiographic and invasive measurements is multifactorial. Firstly, the time sequences of pressures in LVOT and aortic valves are not simultaneous. While the gradient between LVOT and aortic valve would be the “peak instantaneous gradient” in Doppler measurement, that would be the “peak to peak gradient” during invasive measurement. The latter is a more accurate value reflecting the pressure gradient across replacement valves. Secondly, the “pressure recovery phenomenon” may result in differences in peak instantaneous pressure readings across the aortic valve when measured using continuous wave-doppler echocardiography and cardiac catheterization. In this phenomenon, where kinetic energy gained across a narrowed orifice is partially converted back into pressure energy downstream. This phenomenon is particularly pronounced in patients with smaller aortic root diameters, leading to an underestimation of catheter-based gradients compared to Doppler-derived values (6,18,19). Thirdly, Doppler-based methods have inherent technical limitations, including the assumptions of the simplified Bernoulli equation, which may not fully account for flow dynamics in prosthetic valves (3). The Continuous-wave Doppler technique measures the maximal instantaneous blood flow velocity along the LVOT-aortic valve axis. This velocity is then converted into an estimated pressure gradient using the modified Bernoulli equation (2,6).
In contrast, catheterization directly measures the transvalvular pressure gradient (ΔP) distal to the aortic valve after pressure recovery has occurred between the left ventricle and the aorta. Additionally, Doppler echocardiography relies heavily on operator expertise, image quality, and accurate LVOT diameter measurements, while hemodynamic changes can influence catheter-based measurements during sedation or anesthesia (2). The design of replacement valves, especially bileaflet mechanical valves, may contribute to incorrect Doppler-derived gradients. Studies have shown that bileaflet valves are particularly susceptible to localized high velocities and significant pressure recovery, which can lead to an underestimation of effective orifice areas and exaggerated Doppler gradients (20). For instance, the Medtronic-Hall tilting disc (Medtronic, Minneapolis, USA) and Hancock bioprosthetic valves (Medtronic, Minneapolis, USA) showed acceptable agreement between Doppler and catheter gradients. In contrast, St. Jude bileaflet (Abbott, Chicago, USA) and Starr-Edwards caged-ball (Edwards Lifesciences, Irvine, USA) valves exhibited significantly higher Doppler gradients than simultaneous catheter measurements (2). However, another in vitro study suggested that the Doppler-catheter gradient relationship might be independent of specific leaflet designs (20). Furthermore, the degree of discordance may be influenced by the mechanism of valve dysfunction and the severity of stenosis, with evidence suggesting that this discordance increases as prosthetic stenosis becomes less severe (1). Last but not least, suboptimal catheterization techniques, such as relying on catheter pullback instead of simultaneous left ventricular and aortic pressure measurements or using estimated Fick-derived cardiac output instead of direct measurement, may also contribute to the observed discrepancies (21). Additionally, most catheterization measurements are performed under general anesthesia or conscious sedation, which can induce significant hemodynamic changes. These include reduced systemic vascular resistance, diminished myocardial contractility and stroke volume, and decreased oxygen demand, all of which can impact transvalvular pressure gradient measurements (19).
Another well-recognized phenomenon contributing to elevated Doppler-derived gradients is prosthesis–patient mismatch (PPM), which occurs when a normally functioning prosthetic valve is disproportionately small relative to the patient’s body size. This results in abnormally high transvalvular gradients and reduced EOA, ultimately increasing left ventricular afterload and affecting long-term outcomes (7) (22). The assessment of PPM, however, is often complicated by technical limitations, flow dependency, and variability in EOA measurement (23). Herrmann et al. recently emphasized that the diagnostic accuracy of the indexed EOA (EOAi) may be compromised by measurement errors—particularly LVOT underestimation—and low-flow states, leading to “pseudo-PPM” and discordant findings between Doppler and invasive modalities (24). In contrast to these concerns, our findings suggest that EOAi may, in fact, serve as a reliable surrogate for true hemodynamic obstruction in the setting of suspected prosthetic valve dysfunction. Notably, all patients in our cohort with an EOAi <0.50 cm2/m2 exhibited significantly elevated transvalvular gradients confirmed by transseptal catheterization. Furthermore, we observed a strong inverse correlation between EOAi and peak-to-peak invasive gradients (r = –0.63, p = 0.015). These results support the clinical utility of EOAi in stratifying patients for further invasive testing and suggest that a lower EOAi threshold (e.g., <0.50 cm2/m2) may be more predictive of clinically significant obstruction than conventional PPM cutoffs. Accordingly, in patients with high Doppler-derived gradients and low EOAi, early invasive assessment may be considered to guide appropriate management.
Our study has several limitations. First, it is a retrospective single-center analysis with a small sample size, which may limit the generalizability of our findings to larger and more diverse populations. The limited number of patients also precluded a robust subgroup analysis, such as comparisons based on gender, comorbidities, or differing clinical presentations. Additionally, the cohort primarily consisted of patients with bileaflet prosthetic valves, and the absence of other valve types restricted our ability to evaluate variability in Doppler-catheter relationships across different designs. Another limitation is the lack of simultaneous Doppler and catheter-based measurements, as these were performed on different days. This temporal separation could introduce variability due to hemodynamic changes such as fluctuations in heart rate, blood pressure, or fluid status.
Furthermore, the influence of sedation or anesthesia during catheterization on hemodynamic parameters was not systematically assessed, potentially impacting the observed gradients. Finally, while our study provides valuable insights into the discordance between echocardiographic and invasive measurements, the findings should be interpreted cautiously, given both techniques’ inherent technical and methodological limitations. Future studies with larger cohorts and standardized protocols for simultaneous measurements are needed to validate and expand upon these results.
In conclusion, our findings confirm that echocardiography-derived TVG is often higher than catheter-based measurements in patients with aortic valve prostheses. Multiple factors influence this discrepancy. While echocardiography remains an essential tool for the noninvasive evaluation of prosthetic valve function, invasive catheterization should be considered in cases where Doppler findings are inconclusive or when precise hemodynamic data are needed to guide clinical decisions. A comprehensive multimodal approach is critical to optimizing patient outcomes and ensuring accurate diagnosis.
Ethics Approval
The study was performed following the Declaration of Helsinki and was approved by the Hacettepe University Health Sciences Research Ethics Committee (Approval Date: 04.03.2025, Approval Number: 2025/06-19).
Availability of Data and Material
The data supporting this study’s findings are available on request from the corresponding author [U.C.].
Central Message
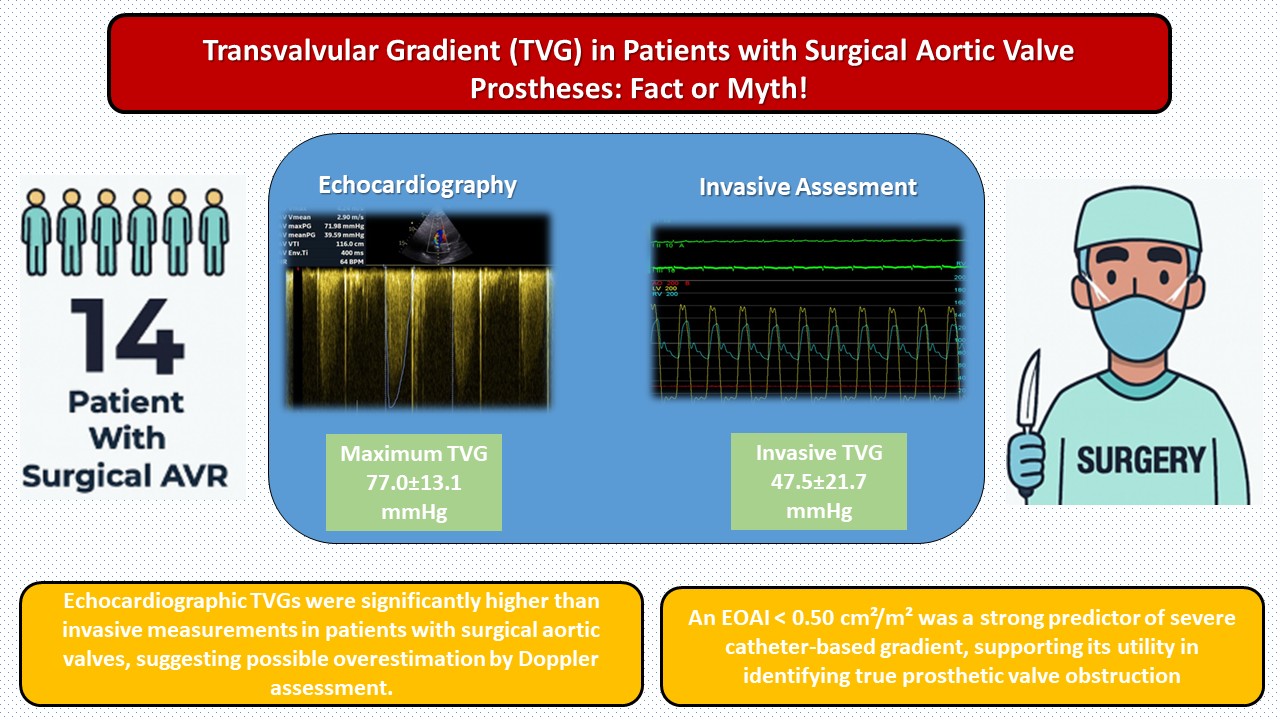
Echocardiography significantly overestimated transvalvular gradients compared to invasive catheterization. EOAI <0.50 cm2/m2 predicted severe hemodynamic obstruction.
Perspective Statement
This study demonstrates that echocardiographic evaluation tends to overestimate transvalvular gradients in patients with surgical AVR. It highlights the diagnostic utility of EOAI <0.50 cm2/m2 as a marker of true hemodynamic obstruction, emphasizing the value of invasive transseptal catheterization for confirmation in patients with discordant imaging findings.
Abbreviated Legend for Central Picture
Echo overestimates TVG; EOAI <0.50 cm2/m2 predicts severe catheter-based gradient.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Video S1. Simultaneous aortic valve gradient measurement is performed using a pigtail catheter placed into the left ventricle via transseptal puncture and another pigtail catheter placed transaortically.
Funding
The authors declared that this study has received no financial support.
Acknowledgments
This study was conducted without external funding or specific institutional support.
Conflicts of Interest
The authors declare they have no conflicts of interest.
References
- Kadri AN, Hanzel G, Elmariah S et al. Invasive versus echocardiographic gradients in degenerated surgical aortic valve prostheses: a multicenter study. JTCVS open 2021;7:51-60.
- Baumgartner H, Khan S, DeRobertis M, Czer L, Maurer G. Effect of prosthetic aortic valve design on the Doppler-catheter gradient correlation: an in vitro study of normal St. Jude, Medtronic-Hall, Starr-Edwards and Hancock valves. Elsevier, 1992:324-332.
- Abbas AE, Mando R, Hanzel G et al. Invasive versus echocardiographic evaluation of transvalvular gradients immediately post-transcatheter aortic valve replacement: demonstration of significant echocardiography-catheterization discordance. Circulation: Cardiovascular Interventions 2019;12:e007973.
- Pibarot P, Dumesnil JG. Prosthesis-patient mismatch: definition, clinical impact, and prevention. Heart 2006;92:1022-1029.
- Hahn RT, Pibarot P. Prosthesis-patient mismatch in transcatheter and surgical aortic valve replacement. Annals of Cardiothoracic Surgery 2024;13:211.
- Biersmith M, Alston M, Makki N et al. Comparison of Catheterization Versus Echocardiographic-Based Gradients in Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Implantation. The Journal of invasive cardiology 2022;34:E442-E447.
- Abbas AE, Mando R, Hanzel G, Goldstein J, Shannon F, Pibarot P. Hemodynamic principles of prosthetic aortic valve evaluation in the transcatheter aortic valve replacement era. Echocardiography 2020;37:738-757.
- Zoghbi WA, Jone PN, Chamsi-Pasha MA et al. Guidelines for the Evaluation of Prosthetic Valve Function With Cardiovascular Imaging: A Report From the American Society of Echocardiography Developed in Collaboration With the Society for Cardiovascular Magnetic Resonance and the Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr 2024;37:2-63.
- Lancellotti P, Pibarot P, Chambers J et al. Recommendations for the imaging assessment of prosthetic heart valves: a report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2016;17:589-90.
- Abbas AE, Mando R, Kadri A et al. Comparison of transvalvular aortic mean gradients obtained by intraprocedural echocardiography and invasive measurement in balloon and self-expanding transcatheter valves. Journal of the American Heart Association 2021;10:e021014.
- Pfenniger A, Stolte T, Reichl JJ et al. Comparison of invasive and non-invasive gradients before and after TAVI and their implications on clinical outcomes. Cardiovascular Intervention and Therapeutics 2024:1-16.
- Oh JK, Taliercio CP, Holmes Jr DR et al. Prediction of the severity of aortic stenosis by Doppler aortic valve area determination: prospective Doppler-catheterization correlation in 100 patients. Journal of the American College of Cardiology 1988;11:1227-1234.
- Hegrenaes L, Hatle L. Aortic stenosis in adults. Non-invasive estimation of pressure differences by continuous wave Doppler echocardiography. Heart 1985;54:396-404.
- Burstow DJ, Nishimura R, Bailey K et al. Continuous wave Doppler echocardiographic measurement of prosthetic valve gradients. A simultaneous Doppler-catheter correlative study. Circulation 1989;80:504-514.
- Simpson I, Fisher J, Reece I, Houston A, Hutton I, Wheatley D. Comparison of Doppler ultrasound velocity measurements with pressure differences across bioprosthetic valves in a pulsatile flow model. Cardiovascular research 1986;20:317-321.
- Abbas AE, Mando R, Kadri A et al. Comparison of Transvalvular Aortic Mean Gradients Obtained by Intraprocedural Echocardiography and Invasive Measurement in Balloon and Self-Expanding Transcatheter Valves. J Am Heart Assoc 2021;10:e021014.
- DeSa TB, Tecson KM, Lander SR et al. Comparison of Echocardiographic and Catheter Mean Gradient to Assess Stenosis After Transcatheter Aortic Valve Implantation. Am J Cardiol 2023;191:110-118.
- Abbas AE, Khalili H, Madanat L et al. Echocardiographic versus invasive aortic valve gradients in different clinical scenarios. Journal of the American Society of Echocardiography 2023;36:1302-1314.
- Bauer BS, Zachariah S, Levi D, Rothman A, Galindo A, Aboulhosn JA. Evaluation of peak pressure gradients in patients after melody valve implantation: a comparison of cardiac catheterization and doppler echocardiography. Echocardiography 2015;32:1073-1079.
- Baumgartner H, Schima H, Kühn P. Discrepancies between Doppler and catheter gradients across bileaflet aortic valve prostheses. The American journal of cardiology 1993;71:1241-1243.
- Yang CS, Marshall ES, Fanari Z et al. Discrepancies between direct catheter and echocardiography-based values in aortic stenosis. Catheterization and Cardiovascular Interventions 2016;87:488-497.
- Pibarot P, Magne J, Leipsic J et al. Imaging for predicting and assessing prosthesis-patient mismatch after aortic valve replacement. JACC: Cardiovascular Imaging 2019;12:149-162.
- Vriesendorp MD, De Lind Van Wijngaarden RA, Head SJ et al. The fallacy of indexed effective orifice area charts to predict prosthesis–patient mismatch after prosthesis implantation. European Heart Journal-Cardiovascular Imaging 2020;21:1116-1122.
- Herrmann Howard C, Pibarot P, Wu C et al. Bioprosthetic Aortic Valve Hemodynamics: Definitions, Outcomes, and Evidence Gaps. JACC 2022;80:527-544.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).