
Submitted:
15 October 2025
Posted:
20 October 2025
You are already at the latest version
Abstract
In an aging society, solving problems associated with the diagnosis and treatment of dementia-related diseases represents a serious challenge. The aim of the study was to evaluate the possibility of applying molecular biology methods to test polymorphisms recognized in global literature as potentially useful in assessing the risk of developing dementia in a group of patients with hyperlipidemia. A sample of 203 patients- 109 diagnosed with both dementia and hyperlipidemia and 94 with hyperlipidemia were genotyped. Additional data about cognitive decline and neuropsychological assessment were collected. Among all the studied polymorphisms, the frequency of the ABCA1 rs2230806 polymorphism differed between the analyzed groups. The GG genotype (p=0.0002, RR=3.22, CI=1.63÷ 6.37) and the G allele (p=0.0007, RR=1.53, CI=1.19÷1.97) were more frequent in patients diagnosed with dementia, specifically in those with Alzheimer's disease. Furthermore, the GG genotype was more common in individuals with a shorter disease duration and lower scores on the MoCA scale, and consequently, with greater cognitive function deficits during early stages of the diagnostic process. ABCA1 rs2230806 genotyping is a potential marker for the early identification of dementia risk in patients with hyperlipidemia, which supports the validity of exploring options for incorporating diagnostics based on molecular biology methods.
Keywords:
ABCA1
; ABCB1
; APOE
; CYP46A1
; LRP
; dementia
; hyperlipidemia
; polymorphism
; markers
1. Introduction
The World Health Organization (WHO) defines dementia as a set of symptoms of a progressive or chronic nature, in the course of which cognitive functions deteriorate to a greater extent than in the case of the biological aging process. Nearly 10 million new cases were diagnosed every year [1]. In 2021 cardiovascular disease- ischemic heart disease and stroke were respectively first and third cause of death worldwide [2]. It is reviewed in existing literature that shared risk factors such as BMI, hypertension, diabetes, dyslipidemia can be affected by genetics. Numerous convergent genes are involved in disease progress of both morbid conditions [3]. Growing importance of molecular diagnostics in clinical practice might be a useful tool to understand pathogenesis and simultaneously a chance to modify lifestyle before prodromal phases. According to the latest report based on analysis nearly half million cases hyperlipidemia diagnosed in younger age results in higher risk in all-cause dementia (HR 1.46 in diagnosis <50 years) [4]. Moreover, lifestyle modification after CVD diagnosis reduces the risk of developing dementia [5]. Conclusions from observational studies and genotyping trials provide evidence that genetic markers are needed in public health policy for prevention.
Table 1 presents the genes selected for analysis based on their alignment in lipid metabolism processes and the development of dementia.
To follow this line, we conduct ABCA1, ABCB7, ABCB1, APOE, CYP46A1 and LRP1 genotyping to compare allele frequency in three groups of patients diagnosed in 1) dementia with coexisting hyperlipidemia, 2) hyperlipidemia, 3) healthy controls, to clarify their role in dementia development and assess their potential for use as early markers of dementia among patients with dyslipidemia.
2. Results
2.1. Baseline Characteristics
A total of 285 participants, 90 with dementia and hyperlipidemia patients, 94 with hypercholesterolemia and 101 individuals as allele frequency control group were included in the study. No significant difference was observed in sex distribution. Patients with both dementia and hyperlipidemia were older than with hyperlipidemia (70.8 (±11.5) vs. 64.1 (±12.9). Dementia & hyperlipidemia participants had a lower burden of comorbidities. Both diabetes and hypertension were more frequently observed in the hyperlipidemia group (p<0.05). The mean age of dementia diagnosis was 65.8 (±9.8), duration is average 7.8 (±2.4). MMSE and MoCA scores were respectively 18.1 (±4.0) and 19.0 (±4.1). In hyperlipidemia & dementia group laboratory workup shows significantly increased cholesterol, HDL, LDL and triglycerides levels (p<0.05 in all parameters).

Table 2.
Attributes of the sample.
| Parameter | Dementia & hyperlipidemia (n=109) | Hyperlipidemia (n=94) | p-value |
|---|---|---|---|
| Male / Female, sex | 47/62 (43.1%/56.9%) | 37/57 (39.4%/60,6%) | p=0.588 |
| Age, y | 70.8 (±11.5) | 64.1 (±12.9) | p <0.05 |
| Weight, kg | 78.0 (70.0÷86.5) | 79.5 (68.0÷95.5) | p=0.420 |
| Diabetes | 13 (11.9%) | 27 (28.7%) | p <0.05 |
| Hypertension | 20 (18.4%) | 68 (72.3%) | p <0.05 |
| Age of dementia diagnosis, y | 65.8 (±9.8) | - | |
| Dementia duration, y | 7.8 (±2.4) | - | |
| MMSE score | 18.1 (±4.0) | - | |
| MoCA score | 19.0 (±4.1) | - | |
| Total cholesterol, mg/dl | 231.0 (220.0÷244.0) | 146.0 (118.0÷168.0) | p <0.05 |
| HDL cholesterol, mg/dl | 55.0 (49.0÷64.0) | 43.0 (32.0÷56.0) | p <0.05 |
| LDL cholesterol, mg/dl | 140.7 (±21.3) | 77.3 (±34.6) | p <0.05 |
| Triglicerydes, mg/dl | 195.2 (±53.1) | 130.7 (±75.5) | p <0.05 |
Data expressed as n (%) mean (SD) or median (first÷third quartile). SI conversion: cholesterol to mmol/l, multiplied by 0.0259; triglycerides to mmol/l, by 0.0113.
2.2. Polymorphisms
First, we assessed differences in genotype frequency in all experiment groups: dementia& hyperlipidemia, non-demented with hyperlipidemia and controls (Table 3). The distribution of ABCA1 (rs2422493), ABCA7, ABCB1, APOE, CYP46A1 and LRP1 genotypes were not significantly different. The ABCA1 (rs2230806) genotypes were not evenly distributed between groups (p=0,004). Further analysis confirmed the existence of differences in the distribution of genotypes between dementia & hyperlipidemia versus hyperlipidemia, with a more frequent prevalence of the GG genotype (p=0.0002, RR=3.22, CI=1.63÷ 6.37) and G allele (p=0.0007, RR=1.53, CI=1.19÷1.97) in patients with dementia. This genotype was also related to an increased risk of Alzheimer disease diagnosis (p=0.006). We also compared the occurrence of genotypes in males and females, but no differences were observed.
Next, we conducted an analysis to evaluate the influence of investigated genotypes on age of dementia diagnosis and duration of disease. Patients with ABCA1 (rs2230806) GG variant presented shorter dementia duration compared to AA and GA genotypes (p=0.0001 and p=0.0004 respectively). Moreover, individuals with ABCA1 (rs2230806) GG genotype achieved lower scores on MoCA scale during first examination (p=0.01) (Figure 1).
An analysis of the impact of the polymorphisms studied on total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides levels was not conducted due to the long-term use of statins by patients in the hyperlipidemia group.
3. Discussion
The aim of this study was to assess the usefulness of ABCA1, ABCB7, ABCB1, APOE, CYP46A1 and LRP1 genotyping as promising dementia risk factors among a wide group of patients with hyperlipidemia diagnosed first. Our findings indicate that ABCA1 (rs2230806) is a suitable candidate. Analysis of other investigated polymorphisms did not reveal differences between the compared groups.
ABCA1 transporter is ATP binding cassette family protein involved in cholesterol efflux and metabolism. Its expression is regulated by several factors, including cholesterol itself, which provides ligands for liver X receptors that stimulate ABCA1 transcription [15]. This transporter plays a crucial role in various diseases including dyslipidemia, coronary heart disease, type 2 diabetes, and potential implications for neurological disorders [16].
Apart from critical role in HDL formation and lipid distribution at the plasma membranes, dysregulation of apolipoprotein lipidation associated with the occurrence of genetic polymorphism increases the risk of dementia developing by promoting the formation of Aβ through the activation of secretase action on the transmembrane amyloid precursor protein [17,18]. At the neurovascular unit without deficits, ABCA1 works alongside ABCB1 to facilitate Aβ clearance from the brain. While ABCB1 directly transports Aβ into the blood circulation, ABCA1 neutralizes Aβ aggregation capacity in an ApoE-dependent manner [19].
The most common context for rs2030806 polymorphism analysis is the risk of coronary artery disease (CAD). Studies have shown that the G allele of rs2230806 is significantly more frequent in coronary artery disease patients, potentially increasing CAD risk [20]. Moreover a meta-analysis revealed that rs2230806 A allele carriers had higher HDL-C levels and lower LDL-C and triglyceride levels compared to non-carriers [21]. Recent research highlights a strong association between cardiovascular disease (CVD) and Alzheimer’s disease (AD). Individuals with subclinical CVD are at higher risk for dementia and AD. Common risk factors for both conditions include hypertension, high LDL cholesterol, low HDL cholesterol, and diabetes [22]. In light of these evidence analysis in relation of neurodegeneration is required. Studies using mice lacking brain ABCA1 have shown increased neuroinflammation, astrogliosis, and cortical neuronal death [23]. Other survey on mouse models confirmed that ABCA1 haplodeficency results in increased Aβ levels and cognitive deficits, but the scale is significantly greater in individuals with the ApoE4 variant [24]. It is worth to be noted that ABCA1 is transcriptionally regulated by Liver X Receptors (LXR) and Retinoic X Receptors (RXR), presenting potential therapeutic targets for neurodegenerative disorders [25,26,27].
Contrary to the presented results of studies on mice findings from published genetic association studies between ABCA1 and Alzheimer’s disease are inconclusive. In Hungarian report the minor A allele of rs2230806 has been linked to a modest protective effect against Alzheimer’s disease [28]. Similarly, in the Chinese Han population, individuals with the A allele achieved better scores on the MMSE cognitive impairment assessment scale and have significantly higher concentration of HDL fraction than non-carriers [29]. According to Wavrant-De Vrièze et al. AG and GG genotypes are associated with the onset of Alzheimer disease, however coincidence with ApoE variant is noteworthy [30]. Sundar et al. indicate a gender-specific association between the ABCA1 rs2230806 polymorphism and late-onset Alzheimer’s disease (LOAD), because women with A allele exhibited 1,75- fold higher risk of the disease [31].
We found significant difference in ABCA1 (rs2230806) genotype distribution between the involved groups hyperlipidemia & dementia and hyperlipidemia. Moreover, GG genotype is related to AD incidence. Patients with GG genotype in comparison to other variants had shorter dementia duration and lower scores on MoCA test during the first examination. Until now, many publications have confirmed that the best risk marker for dementia is the APOE E4 variant; however, the vast majority have relied on comparative studies of healthy individuals and those with dementia. In our study, both groups of participants included patients with hyperlipidemia as an underlying condition, and the differentiating criterion was the presence or absence of dementia. Considering the essential role of APOE as a primary lipid transporter, this enhanced the credibility of the conducted experiment.
Currently, neuropathological examination of brain, neuroimaging and biomarkers widely accepted for the diagnosis of dementia, including the measurement of tau protein, phosphorylated tau protein, and Aβ 1-42 which requires the performance of an invasive procedure to collect cerebrospinal fluid, can provide high diagnostic accuracy in diagnosis of dementia [32]. Some promising plasma phosphorylated tau protein and Aβ42/Aβ40 ratio biomarkers were also reported recently [33,34].
However, molecular testing lately has become a basic diagnostic tool in primary care and has a promising potential to be used in different clinical cases. It is significant to consider the usefulness of genetic markers as screening factors in the targeted group of patients.
Limitations
The conducted study is characterized by several limitations, primarily related to the sample size and the polymorphisms selected based on a review of global literature, which have been reported as involved in both lipid metabolism disorders and dementia-related diseases. However, the study was intended as a preliminary analysis of the potential for identifying gene polymorphisms that should be considered as markers for dementia development in a dedicated patient group. Increasing the number of cases, conducting the analysis across different populations, and significantly expanding the number of polymorphisms tested, for example, through panel tests, would substantially enhance the reliability of the obtained data. In our study, we also did not take into account laboratory test results, particularly those related to lipid metabolism, due to differences in statin use between the two study groups. Cautious planning and implementation of extended lipid parameter diagnostics would undoubtedly add value by narrowing the patient group in which molecular test results could directly influence clinical decisions.
4. Materials and Methods
4.1. Study Population
The study protocol included 203 patients: 109 diagnosed with both dementia and hyperlipidemia hospitalized in Department of Psychiatry Wrocław Medical University and 94 with hyperlipidemia from 4 Military Hospital with Polyclinic in Wrocław. Moreover 101 healthy volunteers as genotype frequency control group were enrolled. Dementia was diagnosed in line with Alzheimer’s Association criteria while hypercholesterolemia according to defined LDL-C levels and risk of cardiovascular disease. Exclusion criteria were: 1) brain injuries 2) acquired causes of dementia 3) liver or kidney disease 4) secondary causes of dyslipidemia 5) long-term fat-elimination diet. Patients were informed about the details of the study and signed fixed consent forms for participation in molecular tests and clinical data processing without personalities. Questionnaires completed by authorized representatives in each department include demographic data (sex, age), anthropometric data (weight), laboratory results (cholesterol, LDL, HDL, triglycerides), comorbidities (diabetes, hypertension) age of diagnosis, duration of dementia, neuropsychological assessment including MMSE (Mini-Mental State Examination and MoCA (Montreal Cognitive Assessment) results collected at the early stage of diagnosing cognitive impairment, which subsequently progressed to dementia.. The study protocol was approved by the Local Ethics Committee of the Wrocław Medical University(141/2019).
4.2. Genotyping
One blood EDTA sampling was completed to extract DNA in the commercial kit (Omega Bio-tek, Georgia) for the genetic survey. The participants were genotyped for the ABCA1 (rs2230806, rs2422493), ABCA7 (rs4147929, rs3752246 rs3764650), ABCB1 (rs1045642, rs1128503, rs2032582) APOE, (rs429358, rs7412), CYP46A1 (rs754203), LRP1 (rs1799986) using AmpliSNiP Dementia Screening Panel (qPCR) (Amplicon, Poland) on Biometra TOptical 96 system (Analytic Jena, Germany).
4.3. Laboratory Markers
Total cholesterol, triglycerides, HDL cholesterol were measured during standard diczasagnostic process in hospital using the enzymatic colorimetric method on a biochemical analyzer using commercially available kits (Roche Diagnostics, Germany). LDL-C concentrations were calculated using the Friedewald formula (in case of triglycerides >= 400 mg/dl measured directly).
4.4. Statistical Analysis
The statistical analysis was performed using the Statistica Ver. 13.3. (TIBCO Software Inc.). The normality of the distribution was evaluated using the Shapiro-Wilk test. The homogeneity of variance was assessed with Levene’s test. Variables with a normal distribution were presented as the mean ± standard deviation, while different distribution as the median along with the first (Q1) and third (Q3) quartile. Qualitative data were expressed as an average percentage. Chi square or the Fisher exact test were performed to compare categorical data. ANOVA, Kruskal-Wallis or Mann-Whitney test were settled to compare continuous variables. P value below 0.05 was considered as significant.
5. Conclusions
The results of our research confirm the impact of the ABCA1 gene polymorphism rs2230806 on an increased risk of developing dementia among patients with hyperlipidemia. This polymorphism is also associated with the duration of the disease and MoCA scale results in the early stages of diagnosing mild cognitive impairment, which over time progressed to dementia. The ABCA1 gene is involved in the regulation of cholesterol transport and phospholipid balance in cells, while rs2230806 polymorphism leading to downregulation of gene activity play a significant role in the development of atherosclerosis and other age-related diseases, it may suggest that changes also occur within the central nervous system, promoting the onset of dementia. However, due to the relatively small sample size in this experiment, it is necessary to expand the study group in order to confirm the utility of ABCA1 rs2230806 genotyping as a predictive marker for the onset of dementia in individuals with hyperlipidemia.
Author Contributions
Conceptualization, M.M., J.L., J.P.; methodology, J.P., M.M.; software, M.R.; validation, A.W-H, B.T. and M.H.; formal analysis, A.W-H.; investigation, M.M., J.P, K.G., M.R; resources, M.M, K.G., M.R.K.; data curation, M.M., J.L., M.R.K, B.T., M.H.; writing—original draft preparation, M.M.; writing—review and editing, A.W-H., J.L.; visualization, M.M.; supervision, A.W-H, J.P.; project administration, M.M.; A.W-H; funding acquisition, A.W-H, J.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded under the Regional Operational Programme of the Lower Silesian Voivodeship 2014-2020, co-financed by the European Union, European Regional Development Fund. Project: „Opracowanie i walidacja panelowego testu diagnostycznego do oceny ryzyka zapadnięcia na chorobę otępienną i wdrożenie spersonalizowanej metody terapii farmakologicznej oraz algorytmu do interpretacji wyników” RPDS.01.02.01-02-0002/20.
Institutional Review Board Statement
The study was performed in accordance with the Declaration of Helsinki and received approval from the Ethics Committee at Wrocław Medical University (141/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
Author Janusz Piechota was employed by the company Amplicon Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 24S-OHC | 24(S)-Hydroxycholesterol |
| AD | Alzheimer disease |
| ApoE | Apolipoprotein E |
| APP | Amyloid precursor protein |
| Aβ | Amyloid β |
| BMI | Body mass index |
| CAD | Coronary artery disease |
| CNS | Central nervous system |
| CVD | Cardiovascular disease |
| HDL | High density lipoprotein |
| LDL | Low density lipoprotein |
| MMSE | Mini–Mental State Examination |
| MoCA | Montreal Cognitive Assessment |
| WHO | World Health Organization |
References
- WHO. Dementia. March 15, 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed in September 2024).
- WHO. The top 10 causes of death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed September 2024).
- Nordestgaard, L.T.; Christoffersen, M.; Frikke-Schmidt, R. Shared Risk Factors between Dementia and Atherosclerotic Cardiovascular Disease. Int J Mol Sci. 2022, 29, 9777. [CrossRef]
- Pan, Y.; Liang, J.; Zhang, W.; Gao, D.; Li, C.; Xie, W.; Zheng, F. Association between Age at Diagnosis of Hyperlipidemia and Subsequent Risk of Dementia. J Am Med Dir Assoc. 2024, 25, 104960. [CrossRef]
- van Gennip, A.C.E.; van Sloten, T.T.; Fayosse, A.; Sabia, S.; Singh-Manoux, A. Age at cardiovascular disease onset, dementia risk, and the role of lifestyle factors. Alzheimer’s Dement. 2024, 20, 1693-1702. [CrossRef]
- Behl, T.; Kaur, I.; Sehgal, A.; Kumar, A.; Uddin, M.S.; Bungau, S. The Interplay of ABC Transporters in Aβ Translocation and Cholesterol Metabolism: Implicating Their Roles in Alzheimer’s Disease. Mol Neurobiol. 2021, 58, 1564-1582. [CrossRef]
- De Roeck, A.; Van Broeckhoven, C.; Sleegers, K. The role of ABCA7 in Alzheimer’s disease: evidence from genomics, transcriptomics and methylomics. Acta Neuropathol. 2019, 138, 201-220. [CrossRef]
- Aikawa, T.; Holm, M.L.; Kanekiyo, T. ABCA7 and pathogenic pathways of Alzheimer’s disease. Brain Sci. 2018, 8, 27. [CrossRef]
- Giau, V. V.; Bagyinszky, E.; An, S. S.; Kim, S. Y. Role of apolipoprotein E in neurodegenerative diseases. Neuropsychiatric disease and treatment, 2015, 11, 1723–1737. [CrossRef]
- Passero, M.; Zhai, T.; Huang, Z. Investigation of Potential Drug Targets for Cholesterol Regulation to Treat Alzheimer’s Disease. Int J Environ Res Public Health. 2023, 20, 6217. [CrossRef]
- Petrov, A.M.; Pikuleva, I.A. Cholesterol 24-Hydroxylation by CYP46A1: Benefits of Modulation for Brain Diseases. Neurotherapeutics. 2019, 16, 635-648. [CrossRef]
- Haider, A.; Zhao, C.; Wang, L.; Xiao, Z.; Rong, J.; Xia, X.; Chen, Z.; Pfister, S.K.; Mast, N.; Yutuc, E.; Chen, J.; Li, Y.; Shao,T.; Warnock, G.I.; Dawoud, A.; Connors, T.R.; Oakley, D.H.; Wei, H.; Wang, J.; Zheng, Z.; Xu, H.; Davenport, A.T.; Daunais, J.B.; Van, R.S.; Shao, Y.; Wang, Y.; Zhang, M.R.; Gebhard, C.; Pikuleva, I.; Levey, A.I.; Griffiths, W.J.; Liang, S.H. Assessment of cholesterol homeostasis in the living human brain. Sci Transl Med. 2022, 14, 9967. [CrossRef]
- Shinohara, M.; Tachibana, M.; Kanekiyo, T.; Bu, G. Role of LRP1 in the pathogenesis of Alzheimer’s disease: evidence from clinical and preclinical studies. J Lipid Res. 2017, 58, 1267-1281. [CrossRef]
- Rauch, J. N.; Luna, G; Guzman, E.; Audouard, M.; Challis, C.; Sibih, Y. E.; Leshuk, C.; Hernandez, I.; Wegmann, S.; Hyman, B. T.; Gradinaru, V.; Kampmann, M.; Kosik, K. S. LRP1 is a master regulator of tau uptake and spread. Nature, 2020, 580, 381–385. [CrossRef]
- Knight, B.L. ATP-binding cassette transporter A1: regulation of cholesterol efflux. Biochem Soc Trans. 2004, 32, 124-127. [CrossRef]
- Jacobo-Albavera, L.; Domínguez-Pérez, M.; Medina-Leyte, D. J.; González-Garrido, A.; Villarreal-Molina, T. The Role of the ATP-Binding Cassette A1 (ABCA1) in Human Disease. International journal of molecular sciences, 2021, 22, 1593. [CrossRef]
- Akram, A; Schmeidler, J.; Katsel, P.; Hof, P.R.; Haroutunian, V. Increased expression of cholesterol transporter ABCA1 is highly correlated with severity of dementia in AD hippocampus. Brain Res. 2010, 1318, 167-177. [CrossRef]
- Reynolds, C.A.; Hong, M.G.; Eriksson, U.K.; Blennow, K.; Bennet, A.M.; Johansson, B.; Malmberg, B,; Berg, S.; Wiklund, F.; Gatz, M.; Pedersen, N.L.; Prince, J.A. A survey of ABCA1 sequence variation confirms association with dementia. Hum Mutat. 2009, 30, 1348-54. [CrossRef]
- Elali, A.; Rivest, S. The role of ABCB1 and ABCA1 in beta-amyloid clearance at the neurovascular unit in Alzheimer’s disease. Frontiers in physiology, 2013, 4, 45. [CrossRef]
- Zargar, S.; Wakil, S.M.; Mobeirek, A.F.; Al-Jafari, A.A. Involvement of ATP-binding cassette, subfamily A polymorphism with susceptibility to coronary artery disease. Biomedical reports, 2013, 16, 883-888 . [CrossRef]
- Lu, Z.; Luo, Z.; Jia, A.; Yu, L.; Muhammad, I.; Zeng, W.; Song, Y. Associations of the ABCA1 gene polymorphisms with plasma lipid levels. Medicine, 2018, 97. [CrossRef]
- Leszek, J.; Mikhaylenko, E.V.; Belousov, D.M.; Koutsouraki, E.; Szczechowiak, K.; Kobusiak-Prokopowicz, M.; Mysiak, A.; Diniz, B.; Somasundaram, S.G.; Kirkland, C.E.; Aliev, G. The Links between Cardiovascular Diseases and Alzheimer’s Disease. Current Neuropharmacology, 2020, 19, 152 – 169. [CrossRef]
- Karasinska, J.M.; Haan, W.D.; Franciosi, S.; Ruddle, P.; Fan, J.; Kruit, J.K.; Stukas, S.; Lütjohann, D.; Gutmann, D.H.; Wellington, C.L.; Hayden, M.R. ABCA1 influences neuroinflammation and neuronal death. Neurobiology of Disease, 2013, 54, 445-455. [CrossRef]
- Fitz, N. F.; Cronican, A. A.; Saleem, M.; Fauq, A. H.; Chapman, R.; Lefterov, I.; Koldamova, R. Abca1 deficiency affects Alzheimer’s disease-like phenotype in human ApoE4 but not in ApoE3-targeted replacement mice. The Journal of neuroscience : the official journal of the Society for Neuroscience, 2012, 32, 13125–13136. [CrossRef]
- Koldamova, R.; Fitz, N. F.; Lefterov, I. The role of ATP-binding cassette transporter A1 in Alzheimer’s disease and neurodegeneration. Biochimica et biophysica acta, 2010, 1801, 824–830. [CrossRef]
- Koldamova, R.; Fitz, N. F.; Lefterov, I. ATP-binding cassette transporter A1: from metabolism to neurodegeneration. Neurobiology of disease, 2014, 72, 13–21. [CrossRef]
- Donkin, J. J.; Stukas, S.; Hirsch-Reinshagen, V.; Namjoshi, D.; Wilkinson, A.; May, S.; Chan, J.; Fan, J.; Collins, J.; Wellington, C. L. ATP-binding cassette transporter A1 mediates the beneficial effects of the liver X receptor agonist GW3965 on object recognition memory and amyloid burden in amyloid precursor protein/presenilin 1 mice. The Journal of biological chemistry, 2010, 285, 34144–34154. [CrossRef]
- Fehér, Á.; Giricz, Z.; Juhász, A.; Pákáski, M.; Janka, Z.; Kálmán, J. ABCA1 rs2230805 and rs2230806 common gene variants are associated with Alzheimer’s disease. Neuroscience letters, 2018, 664, 79–83. [CrossRef]
- Xiao, Z.; Wang, J.; Chen, W.; Wang, P.; Zeng, H.; Chen, W. Association studies of several cholesterol-related genes (ABCA1, CETP and LIPC) with serum lipids and risk of Alzheimer’s disease. Lipids in health and disease, 2012, 11, 163. [CrossRef]
- Wavrant-De Vrièze, F.; Compton, D.; Womick, M.; Arepalli, S.; Adighibe, O.; Li, L.; Pérez-Tur, J.; Hardy, J. ABCA1 polymorphisms and Alzheimer’s disease. Neuroscience letters, 2007, 416, 180–183. [CrossRef]
- Sundar, P. D.; Feingold, E.; Minster, R. L.; DeKosky, S. T.; Kamboh, M. I. Gender-specific association of ATP-binding cassette transporter 1 (ABCA1) polymorphisms with the risk of late-onset Alzheimer’s disease. Neurobiology of aging, 2007, 28, 856–862. [CrossRef]
- Bogdanovic, N. The Challenges of Diagnosis in Alzheimer’s Disease. US neurology. 2018, 14, 15. [CrossRef]
- Ashton, N. J.; Puig-Pijoan, A.; Milà-Alomà, M.; Fernández-Lebrero, A.; García-Escobar, G.; González-Ortiz, F.; Kac, P. R.; Brum, W. S.; Benedet, A. L.; Lantero-Rodriguez, J.; Day, T. A.; Vanbrabant, J.; Stoops, E.; Vanmechelen, E.; Triana-Baltzer, G.; Moughadam, S.; Kolb, H.; Ortiz-Romero, P.; Karikari, T. K.; Minguillon, C.; Suárez-Calvet, M. Plasma and CSF biomarkers in a memory clinic: Head-to-head comparison of phosphorylated tau immunoassays. Alzheimer’s & dementia : the journal of the Alzheimer’s Association, 2023, 19, 1913–1924. [CrossRef]
- Pascual-Lucas, M.; Allué, J. A.; Sarasa, L.; Fandos, N.; Castillo, S.; Terencio, J.; Sarasa, M.; Tartari, J. P.; Sanabria, Á.; Tárraga, L.; Ruíz, A.; Marquié, M.; Seo, S. W.; Jang, H.; Boada, M.; & FACEHBI study group. Clinical performance of an antibody-free assay for plasma Aβ42/Aβ40 to detect early alterations of Alzheimer’s disease in individuals with subjective cognitive decline. Alzheimer’s research & therapy, 2023, 15, 2. [CrossRef]
Figure 1.
(a) Box-plot illustrates the distribution of individual ABCA1 (rs2230806) genotypes and the duration of the disease; (b) Box plot illustrates the relationship between the distribution of ABCA1 (rs2230806) genotypes and MoCa scores.
Figure 1.
(a) Box-plot illustrates the distribution of individual ABCA1 (rs2230806) genotypes and the duration of the disease; (b) Box plot illustrates the relationship between the distribution of ABCA1 (rs2230806) genotypes and MoCa scores.
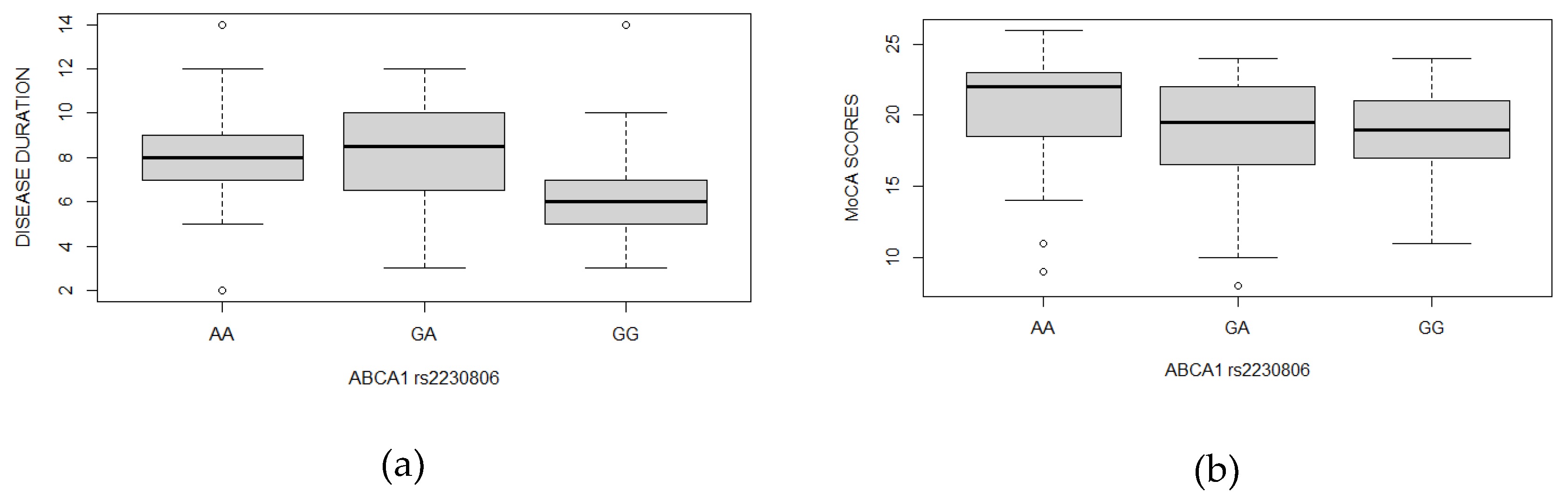
Table 1.
Genes under investigation, role in lipid metabolism and dementia.
| Gene | Role in lipid metabolism | Involvement in dementia | References |
|---|---|---|---|
| ABCA1 | Regulation of cholesterol, support ApoE lipidation | Influence for ApoE lipidation affect APP processing and Aβ cumulation | [6,8] |
| ABCA7 | Regulation of lipid metabolism, apolipoproteins lipidation | Phagocytic elimination of Aβ, suppression of AβPP proteolysis | [6,7,8] |
| ABCB1 | Efflux transporter, pharmacoresistance, detoxification, homeostasis maintaince in CNS | Transport of Aβ from neural processes to blood circulation | [6] |
| APOE | Lipid transporter protein | APOE E4 variant accelerate the accumulation, aggregation, and deposition of Aβ in the brain | [9] |
| CYP46A1 | Conversion cholesterol into form 24S-OHC capable of crossing blood-brain barrier | Decreased function leads to an increased production of Aβ and tau proteins | [10,11,12] |
| LRP1 | Internalization of lipoproteins into neurons, apoE receptor | Aβ deposition, tau regulation, brain homeostasis | [13,14] |
Table 3.
Genotype frequency.
| Gene | rs code | Participants | Genotype frequency | p-value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ABCA1 | rs2230806 | AA | GA | GG | 0.004 | ||||||
| Dementia & hyperlipidemia | 39 (35.8%) | 36 (33.0%) | 34 (31.2%) | ||||||||
| Hyperlipidemia | 45 (47.8%) | 40 (42.6%) | 9 (9.6%) | ||||||||
| Controls | 37 (36.6%) | 44 (43.6%) | 20 (19.8%) | ||||||||
| ABCA1 | rs2422493 | CC | CT | TT | 0.066 | ||||||
| Dementia & hyperlipidemia | 34 (31.2%) | 51 (46.8%) | 24 (22.0%) | ||||||||
| Hyperlipidemia | 20 (21.3%) | 56 (59.6%) | 18 (19.1%) | ||||||||
| Controls | 20 (19.8%) | 49 (48.5%) | 32 (31.7%) | ||||||||
| ABCA7 | rs4147929 | AA | AG | GG | 0.561 | ||||||
| Dementia & hyperlipidemia | 3 (2.8%) | 35 (32.1%) | 71 (65.1%) | ||||||||
| Hyperlipidemia | 2 (2.1%) | 30 (31.9%) | 62 (66.0%) | ||||||||
| Controls | 3 (3.0%) | 23 (22.8%) | 75 (74.2%) | ||||||||
| ABCA7 | rs3752246 | CC | CG | GG | 0.493 | ||||||
| Dementia & hyperlipidemia | 71 (65.1%) | 36 (33.0%) | 2 (1.9%) | ||||||||
| Hyperlipidemia | 64 (68.1%) | 29 (30.8%) | 1 (1.1%) | ||||||||
| Controls | 77 (76.2%) | 23 (22.8%) | 1 (1.0%) | ||||||||
| ABCA7 | rs3764650 | GG | GT | TT | 0.446 | ||||||
| Dementia & hyperlipidemia | 1 (0.9%) | 17 (15.6%) | 91 (83.5%) | ||||||||
| Hyperlipidemia | 1 (1.1%) | 11 (11.7%) | 82 (87.2%) | ||||||||
| Controls | - | 10 (9.9%) | 91 (90.1%) | ||||||||
| ABCB1 | rs1045642 | CC | CT | TT | 0.478 | ||||||
| Dementia & hyperlipidemia | 27 (24.8%) | 55 (50.4%) | 27 (24.8%) | ||||||||
| Hyperlipidemia | 28 (29.8%) | 44 (46.8%) | 22 (23.4%) | ||||||||
| Controls | 19 (18.8%) | 52 (51.5%) | 30 (29.7%) | ||||||||
| ABCB1 | rs1128503 | CC | CT | TT | 0.512 | ||||||
| Dementia & hyperlipidemia | 38 (34.9%) | 48 (44.0%) | 23 (21.1%) | ||||||||
| Hyperlipidemia | 38 (40.4%) | 48 (43.6%) | 15 (16.0%) | ||||||||
| Controls | 30 (29.7%) | 47 (46.5%) | 24 (23.8%) | ||||||||
| ABCB1 | rs2032582 | GG | GT | TT | 0.353 | ||||||
| Dementia & hyperlipidemia | 36 (33.6%) | 51 (47.7%) | 20 (18.7%) | ||||||||
| Hyperlipidemia | 44 (46.8%) | 37 (39.4%) | 13 (13.8%) | ||||||||
| Controls | 34 (33.7%) | 49 (48.5%) | 18 (17.8%) | ||||||||
| APOE | rs429358 rs7412 |
E2/E2 | E2/E3 | E2/E4 | E3/E3 | E3/E4 | E4/E4 | 0.224 | |||
| Dementia & hyperlipidemia | - | 16 (14.7%) | 5 (4.6%) | 77 (70.6%) | 7 (6.4%) | 4 (3.7%) | |||||
| Hyperlipidemia | 1 (1.1%) | 6 (6.3%) | 1 (1.1%) | 67 (71.3%) | 19 (20.2%) | - | |||||
| Controls | 1 (1.0%) | 7 (6.9%) | 1 (1.0%) | 86 (85.2%) | 6 (5.9%) | - | |||||
| CYP46A1 | rs754203 | AA | AG | GG | 0.148 | ||||||
| Dementia & hyperlipidemia | 51 (46.8%) | 52 (47.7%) | 6 (5.5%) | ||||||||
| Hyperlipidemia | 44 (46.8%) | 35 (37.2%) | 15 (16.0%) | ||||||||
| Controls | 48 (47.5%) | 40 (39.6%) | 13 (12.9%) | ||||||||
| LRP1 | rs1799986 | CC | CT | TT | 0.224 | ||||||
| Dementia & hyperlipidemia | 75 (68.8%) | 31 (28.4%) | 3 (2.8%) | ||||||||
| Hyperlipidemia | 73 (77.6%) | 17 (18.1%) | 4 (4.3%) | ||||||||
| Controls | 65 (64.4%) | 32 (31.6%) | 4 (4.0%) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



