
Submitted:
15 October 2025
Posted:
16 October 2025
You are already at the latest version
Abstract
Mental health challenges are on the rise among young people in South Africa. These conditions are driven by widespread poverty, social stigma, and limited access to adequate healthcare services. A scoping review was conducted in accordance with the PRISMA-ScR framework. Three electronic databases (PubMed, CINAHL, and Google Scholar) were systematically searched for studies published between 2014 and 2025. Eligible studies included those involving youth (14-35 years) in rural South Africa, focusing on physical activity interventions that target mental health outcomes. A total of 42,384 records were identified, of which 12 studies met the inclusion criteria. Findings consistently demonstrated that physical activity was associated with reduced depression, anxiety, and behavioural problems, and improved prosocial behaviours and resilience. Context-specific initiatives, such as the Nyakaza–Move-for-Health program, have demonstrated that culturally tailored, school- and community-based interventions can enhance engagement and acceptability. Physical activity holds substantial potential as a scalable, accessible strategy to address the rural youth mental health burden in South Africa. Strengthening evidence through rigorous intervention trials, community-driven models, and integration into schools and health services is urgently needed. National policy alignment across the health, education, and sports sectors will be critical to ensuring sustainability and equity.
Keywords:
exercise
; mental health
; physical activity
1. Introduction
Mental health disorders are a leading contributor to the global burden of disease, increasingly affecting adolescents and young adults. Conditions such as depression, anxiety, post-traumatic stress disorder (PTSD), and substance use disorders compromise not only individuals’ well-being but also educational attainment, employability, and long-term health outcomes [1]. The World Health Organisation estimates that up to 20% of youth worldwide experience mental health problems, yet the majority remain untreated, particularly in low- and middle-income countries (LMICs) where health systems face severe resource constraints [2].
In South Africa, mental health disorders are similarly widespread across the country. National surveys estimate that approximately 16.5% of South Africans experience mental issues such as stress, depression and anxiety in their lifetime, with adolescents and youth being disproportionately affected [3]. More recent provincial studies suggest that depression prevalence among youth ranges between 15-20%, while anxiety symptoms are reported in up to one-third of school-going youth, particularly in under-resourced rural provinces [4]. These figures underscore a substantial treatment gap, as fewer than 25% of the affected individuals receive appropriate care [5].
Given these challenges, interest in accessible, cost-effective interventions that can support youth mental health outside traditional clinical settings has increased. Research promotes physical activity (PA) as a promising non-pharmacological strategy for preventing and managing mental health conditions. Global evidence shows that regular participation in PA effectively reduces symptoms of depression and anxiety, improves mood and cognitive functioning, and enhances social connectedness and self-esteem [6]. Interventions such as sport, dance, aerobic routines, and recreational play not only promote psychological well-being but also strengthen resilience and prosocial behaviours [7,8,9]. Although these benefits are well-documented, significant gaps remain in the literature.
Much of the literature is concentrated in high-income and urban settings, where infrastructure, school systems, and health services support the delivery of programs [10]. Evidence in these areas highlights the value of physical activity for adolescent health and psychosocial development [11]. Rural youth remain largely overlooked in both research and policy [12]. Research in rural areas, which faces substantial barriers, remains scarce [13]. Multiple structural and socio-cultural barriers contribute to this neglect. These often lack safe recreational facilities, trained facilitators, and supportive infrastructure, while poverty and gendered norms further constrain participation in physical activity [14]. Simultaneously, stigma surrounding mental illness, combined with limited access to formal healthcare, encourages delays in help-seeking, leaving many adolescents undiagnosed and untreated [15]. Alarmingly, recent studies estimate that the treatment gap for adolescent mental health in rural South Africa exceeds 70%, highlighting a pressing public health crisis [16].
Addressing these inequities requires evidence that reflects the realities of rural areas. Interventions developed in urban or clinical contexts may have limited relevance in settings where resources are scarce and where cultural norms strongly shape both physical activity practices and perceptions of mental illness [17]. A context-specific evidence base is therefore crucial for designing sustainable, community-driven interventions that align with the needs of rural communities.
This scoping review addresses these gaps by systematically reviewing existing evidence on physical activity interventions for youth mental health in rural South Africa. Unlike systematic reviews that narrowly assess the effectiveness of interventions, a scoping review approach captures the breadth of available research, identifies key concepts and intervention models, and highlights evidence gaps [18]. By synthesising this knowledge, the review aims to guide researchers, practitioners, and policymakers in developing culturally relevant and scalable strategies to reduce rural–urban disparities in youth mental health and to advance physical activity as a tool for equitable health promotion.
Research Objective
This scoping review aims to explore and map existing physical activity interventions designed to improve mental health outcomes among youth in South Africa.
2. Materials and Methods
2.1. Study Design
This study adopts a scoping review design, guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist. The review follows the methodological framework proposed by Arksey and O’Malley [19], further refined by Levac [20], to systematically map existing literature and identify key concepts, types of interventions, evidence gaps, and research trends relevant to physical activity and mental health among rural youth in South Africa.
2.2. Protocol and Registration
The protocol for this scoping review was prospectively registered on the Open Science Framework (OSF) to enhance transparency and methodological rigour [21]. The protocol outlines the review objectives, eligibility criteria, and planned methods, ensuring alignment with best practices for scoping reviews as recommended by PRISMA-ScR guidelines.
2.3. Eligibility Criteria
This review applies the Population Concept Context (PCC) framework to guide the selection of studies.
- Population: The review will include studies focusing on youth aged 14 to 35 living in rural areas of South Africa. This age range aligns with national definitions of youth and reflects the transitional life stage during which mental health vulnerabilities commonly emerge.
- Concept: Eligible studies must involve physical activity or exercise-based interventions designed to improve mental health. These may include structured or unstructured forms of physical activity such as aerobic exercise, sports, recreational play, dance, or community movement programs.
- Context: The review will focus on mental health promotion, prevention, or treatment interventions in South Africa.

Table 1.
Inclusion and Exclusion
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Timeframe | Studies published between 2014 and 2025 | Studies published before 2014 |
| Study Design | All empirical study designs: quantitative, qualitative, or mixed methods | Editorials, commentaries, and non-peer-reviewed literature |
| Population | Youth (14–35 years) in South Africa | Studies focused only on older people/children’s |
| Intervention | Any physical activity or exercise intervention | Interventions focused only on elite or professional athletes |
| Outcomes | Studies that report on mental health outcomes. | Studies that do not assess mental health outcomes |
| Language | Articles published in English | Articles published in other languages without an English translation |
2.4. Search Strategy
A comprehensive and systematic search was conducted in multiple electronic databases to identify relevant studies examining physical activity interventions for mental health among rural youth in South Africa. The databases searched included PubMed, CINAHL and Google Scholar. The search covered the period January 2014 to September 2025 to capture the most recent and relevant evidence
The population guided the search strategy using the Concept-Context framework (PCC), where the population was youth in rural South Africa and the concept was physical activity or exercise interventions. The context was mental health and well-being. The search terms combined key concepts related to physical activity, mental health, youth populations, and rural settings in South Africa.
The search string:
(“physical activity” OR exercise OR “sport-based intervention” OR “recreational activity”) AND (“mental health” OR depression OR anxiety OR stress OR “psychological well-being”) AND (youth OR adolescent OR “young people” OR “young adult” OR teenager) AND (“rural South Africa” OR “rural communities”)
In addition to peer-reviewed journal articles, gray literature was included where relevant and methodologically sound. These sources were identified through a hand-search of reference lists.
2.5. Study Selection
All articles retrieved from the database searches will be imported into Zotero, a reference management software, to manage citations and remove duplicates efficiently [22]. Two independent reviewers (M.O.L. and V.R.) will initially screen titles and abstracts to assess relevance based on the predefined eligibility criteria [23]. Following this, the full texts of potentially eligible articles will be retrieved and thoroughly screened against the inclusion and exclusion criteria to determine final eligibility. Any disagreements between reviewers during screening will be resolved through discussion. If consensus is not reached, a third reviewer (T.L.) will be consulted to adjudicate, ensuring transparency and minimising selection bias [18]. The study selection process will be documented and reported using a PRISMA-ScR flow diagram [18].
2.6. Data Extraction
Data from included studies will be systematically extracted using a standardised data extraction form developed a prior to ensure consistency and comprehensiveness (Peters et al., 2020). Extracted information will include:
- Author(s) and year of publication: To track publication trends and contextualise findings.
- Study design and methodology: To understand the research approaches and quality.
- Sample characteristics, including age, gender distribution, and geographical location, are used to describe the population.
- Setting: Details of where the intervention occurred, such as schools, community centres, or clinics.
- Type and description of physical activity intervention: Including intervention format, duration, frequency, and delivery method.
- Mental health outcomes assessed, such as depression, anxiety, stress, or other psychological well-being measures.
- Main findings and conclusions: To summarise intervention effectiveness and key insights.
Two reviewers will independently perform data extraction, discrepancies resolved through discussion or the participation of a third reviewer, as necessary, according to the best practices for reviewing the scope [20].
3. Results
3.1. Study Selection
The systematic search was conducted across Google Scholar, PubMed, and CINAHL. The search identified 42,384 records (Google Scholar: 21,700; PubMed: 8,658; CINAHL: 12,026). After removing 10,142 duplicates, 32,242 records remained for title and abstract screening. Following this stage, 160 articles were selected for full-text review based on relevance to the eligibility criteria. Of these, 12 studies met the inclusion criteria and were included in the final synthesis. A PRISMA-ScR flow diagram summarising the study selection process is presented in Figure 1.
3.2. Characteristics of Included Studies
The 12 studies varied in design, population, and outcomes (Table 2). They included six cross-sectional studies, two qualitative studies, one intervention development study, one systematic review, one scoping review, and one conceptual paper. Sample sizes ranged from fewer than 50 (qualitative interviews) to several hundred participants (cross-sectional surveys). Most studies were school- or community-based, with a few focusing on healthcare providers or national datasets.
Narrative Summary of Individual Studies
- Asare [16] conducted a cross-sectional study among adolescents in KwaZulu-Natal, finding that higher physical activity levels were significantly associated with fewer behavioural problems and enhanced prosocial behaviour, underscoring PA’s role in resilience-building.
- Kinsman [24] used qualitative interviews and focus groups with rural adolescent girls in Mpumalanga. They highlighted barriers such as body image concerns, identity issues, and safety concerns, and proposed a model for increasing participation among girls.
- Micklesfield [14] examined 381 adolescents in a rural surveillance site in Mpumalanga. The study showed low levels of moderate-to-vigorous physical activity (MVPA), particularly among girls, and identified socioeconomic factors shaping PA and sedentary behaviour.
- Vancampfort [25] reviewed studies from Sub-Saharan Africa. They found policy- and community-level interventions were limited but essential for addressing the mental health needs of people with psychiatric conditions, indirectly reinforcing the importance of context-driven PA programs.
- Marais [26] interviewed South African mental health professionals and found positive attitudes toward PA as an adjunctive therapy, though most reported insufficient training and institutional support to integrate exercise into care.
- Burger [27] presented a conceptual model advocating for the integration of sport and exercise psychiatry into South Africa’s mental health systems, highlighting feasibility but calling for professional capacity-building.
- Zimu [28] developed the Nyakaza–Move-for-Health program in KwaZulu-Natal, a culturally tailored school- and community-based PA intervention. The program successfully improved adolescent engagement and demonstrated the importance of cultural adaptation.
- Siduli [29] conducted a cross-sectional survey of adolescents in the Eastern Cape. They reported positive associations between PA participation, body composition, and mental well-being, further emphasising PA’s dual health benefits.
- Draper [30] studied young women in urban Soweto and found that high sedentary behaviour correlated with poorer mental health outcomes. Although urban, the findings offer insight into likely patterns in rural youth with even fewer opportunities for PA.
- Bermejo-Cantarero [31] carried out a systematic review and meta-analysis of global RCTs in adolescents, confirming that structured PA interventions significantly improved health-related quality of life and emotional well-being.
- Kunene & Taukobong [32] examined PA levels among healthcare professionals in rural KwaZulu-Natal and found very low engagement, raising concerns about their role as promoters of active lifestyles.
- Mumbauer [33] conducted a scoping review of youth-focused interventions in South Africa and recommended culturally relevant, school-based approaches to integrate PA into broader mental health promotion strategies.
3.3. Overall Synthesis
Taken together, these studies consistently affirm that physical activity has protective effects on youth mental health, but most available evidence is cross-sectional and urban-focused. Interventions specifically targeting rural youth were rare, with Nyakaza–Move-for-Health being the strongest example of a context-sensitive model. Methodological limitations, weak reporting, and under-representation of rural adolescents highlight significant gaps that require attention and improvement.
4. Discussion
This scoping review set out to examine existing evidence on physical activity (PA) interventions aimed at managing mental health disorders among rural youth in South Africa. The review responded to the increasing mental health burden among adolescents and young adults and the growing recognition of exercise as a non-pharmacological treatment for depression, anxiety, and behavioural challenges. Across the 12 included studies, evidence suggests that physical activity has positive implications for the mental health of youth. However, implementing these interventions remains limited, with context-specific challenges affecting uptake and sustainability, particularly in rural areas where infrastructure, resources, and cultural dynamics differ significantly from urban centres.
4.1. Summary of Key Findings
This review synthesised findings from 12 studies, demonstrating that physical activity (PA) is positively associated with youth mental health, yet participation levels remain low, especially in rural South Africa. Evidence from empirical studies shows that higher PA engagement is linked to fewer behavioural problems and stronger prosocial functioning among adolescents [16], while insufficient PA was reported in a large rural surveillance site, with gender gaps disadvantaging girls [14]. Similarly [29] found positive associations between PA, body composition, and mental well-being among Eastern Cape adolescents, reinforcing exercise’s dual psychological and physical benefits. Although conducted in an urban setting, research confirmed that sedentary behaviour is strongly linked to poor mental health, a trend likely magnified in rural youth where infrastructure is more limited [30].
Promising intervention models were identified. The Nyakaza–Move-for-Health programme in KwaZulu-Natal demonstrated how culturally adapted interventions can enhance adolescent PA engagement [28]. Similarly, a rural Mpumalanga model targeting adolescent girls addressed safety, body image, and identity as barriers to participation [24]. These findings highlight that contextualisation, cultural sensitivity, and school–community partnerships are critical to effective program delivery.
At the systems level, [26] reported that although mental health professionals value exercise as an adjunctive therapy, most lack the training and institutional support to integrate it into clinical practice. Low PA participation among healthcare providers themselves [33] further complicates their role as promoters of active lifestyles. To address these gaps, [27] proposed a South African sport-and-exercise psychiatry model for LMICs, advocating for specialist roles within mental health services.
Global and regional reviews strengthen the case for PA as a mental health strategy. A meta-analysis confirmed that structured PA improves health-related quality of life and emotional well-being in adolescents [31], while a Sub-Saharan Africa review highlighted the importance of community and policy interventions to scale PA for people with mental illness [25]. A recent South African scoping review highlighted the need for culturally grounded, school-based mental health promotion strategies for youth, aligning with local interventions such as Nyakaza–Move-for-Health [33].
In sum, these studies consistently affirm PA’s protective role for youth mental health while exposing persistent challenges: very low participation rates, gender disparities, limited rural-focused interventions, and inadequate professional capacity. They collectively argue for culturally relevant, community-driven, and school-integrated approaches to bridge the gap between evidence and practice in rural South Africa.
4.2. Interventions and Context-Specific Models
Among the reviewed studies, intervention-focused research provided particularly valuable insights into culturally grounded and contextually relevant strategies. Som researchers introduced Nyakaza-Move-for-Health, a school- and community-based intervention tailored to adolescents in KwaZulu-Natal [28]. By integrating local cultural practices, involving caregivers, and using participatory design, this program successfully enhanced both engagement and perceived benefits of physical activity. Likewise [24] developed a model targeting rural adolescent girls, highlighting the importance of identity, body image, and safety concerns in shaping participation. These interventions illustrate that programs designed in collaboration with communities and responsive to local socio-cultural dynamics are more likely to succeed.
In contrast, studies [30], which examined physical activity and mental health in Soweto (an urban setting), demonstrated the urban bias in much of the existing literature. Although relevant for understanding adolescent behaviour, such studies are less applicable to rural communities where access to infrastructure, cultural norms, and safety dynamics differ substantially. This indicates the need for more rural-specific interventions to avoid misalignment between research evidence and real-world applicability.
4.3. Health Systems and Professional Perspectives
The integration of physical activity into formal healthcare services remains limited. One study found that while South African mental health professionals recognise the therapeutic potential of exercise, few are adequately trained to implement physical activity interventions in practice [26]. Systemic barriers, such as a lack of guidelines, limited infrastructure, and insufficient funding, further hinder integration. Another study echoed these findings in their conceptual paper, calling for the establishment of sport and exercise psychiatry models in South Africa and other low- and middle-income countries [27]. Their framework emphasised the importance of creating specialised professional roles to champion exercise as medicine within mental health services.
4.4. Global Comparisons and Broader Insights
Findings from South Africa align with international evidence confirming that physical activity is an effective strategy for improving youth mental health. Global reviews, [6,9] report that structured exercise interventions, including aerobic and resistance training, reduce depression and anxiety in young populations. More recently conducted meta-analysis demonstrates that physical activity interventions improved health-related quality of life and emotional well-being among adolescents across diverse contexts [31].
However, the South African context differs significantly from those of high-income countries, where interventions often benefit from greater infrastructure, school-based delivery systems, and policy support. In rural South Africa, challenges such as limited recreational facilities, inadequate transportation, and socio-cultural perceptions around gender and physical activity remain barriers. Comparable studies from rural Australia and New Zealand also highlight these structural and cultural barriers, underscoring the global importance of tailoring interventions to the specific needs of rural populations [10].
4.5. Gaps in the Literature
This review highlights several critical gaps. First, most included studies were cross-sectional [14,16], limiting the ability to draw causal inferences. Few randomised controlled trials (RCTs) or quasi-experimental evaluations exist that test the efficacy of physical activity interventions for rural youth. Without stronger designs, it is difficult to establish long-term effectiveness or determine optimal intervention components.
Secondly, rural youth remain underrepresented. Even when rural populations were included, findings were often not disaggregated by geographic location, which reduced their applicability. Studies illustrate this urban focus, leaving rural youth, who are among the most vulnerable groups, overlooked [11].
Third, poor reporting remains a problem. Globally, many studies fail to provide adequate details on intervention frequency, duration, and adherence. This limitation reduces replicability and hinders scalability [9].
Finally, certain vulnerable groups, including out-of-school youth, adolescents with disabilities, and LGBTQ+ populations, are rarely represented. This omission perpetuates inequities and restricts understanding of how physical activity may benefit diverse youth subgroups in rural contexts.
4.6. Implications for Research, Policy, and Practice
The evidence generated by this review suggests that physical activity should be recognised as a critical tool for addressing youth mental health challenges in South Africa. To be effective, programs must be community-driven and culturally sensitive, engaging youth, families, and local leaders in design and implementation. Given their reach and potential for structured, sustainable programming, school settings should be leveraged as primary delivery platforms for these initiatives. Some research offers a successful example of how cultural tailoring and school-community partnerships can improve outcomes [34].
Policy alignment is also vital. Integrating physical activity into existing national strategies on mental health, education, and sport development can ensure institutional backing, resource mobilisation, and inter-sectoral coordination. Building capacity among mental health professionals, as recommended by some studies is essential for embedding physical activity into both clinical and community-based care [26,27].
Researchers urgently need to conduct longitudinal and experimental studies to establish causal pathways and evaluate the effectiveness of interventions in rural contexts. Mixed-methods approaches could further explore how cultural, gender, and infrastructural factors shape participation. Including marginalised youth subgroups is necessary to ensure interventions are equitable and inclusive. Scaling up physical activity as a mental health intervention in rural South Africa requires rigorous evidence and robust implementation systems. Community ownership, school integration, and policy support represent the pillars for sustainable change. If pursued, these approaches can help reduce the rural–urban mental health gap and provide young people with accessible, non-stigmatising pathways to well-being.
5. Conclusions
This scoping review found consistent evidence that physical activity improves mental health outcomes among youth in South Africa, reducing depression, anxiety, and behavioural challenges while enhancing resilience and prosocial behaviours. However, participation levels remain low, and rigorous intervention trials targeting rural youth are scarce. Policy and practice efforts should focus on integrating physical activity into youth mental health promotion through schools, community centres, and primary healthcare systems, particularly in rural areas. Cross-sector collaboration between health, education, and sport development is essential to ensure sustainability, scalability, and equity. Building the capacity of healthcare professionals to deliver and advocate for PA-based interventions will further strengthen implementation.
Looking forward, these findings underscore the need for integrated health and education interventions that embed culturally tailored physical activity programs within broader youth development agendas. In LMIC contexts such as South Africa, such strategies can reduce rural–urban disparities, provide non-stigmatising pathways to care, and promote long-term well-being for vulnerable youth populations. This review was conducted in accordance with a prospectively registered protocol on the Open Science Framework.
Author Contributions
M.O.L. Conceptualisation and drafted the literature review, literature search, M.O.L drafted the Plan for methodology of the literature and literature search, L.T. literature search, critically read and added academic value to the systematic review. L.T., M.O.L & V.R. final reviewed and edited the literature review.
Funding
The study was not funded.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
All authors have read and agreed to publish the version of the manuscript. Protocol Registration: This review protocol was prospectively registered on the Open Science Framework (OSF; DOI: https://doi.org/10.17605/OSF.IO/HKY6G).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PTSD | Post-Traumatic Stress Disorder |
| PA | Physical Activity |
| RISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| OSF | Open Science Framework |
References
- Burns, J.K. The mental health gap in South Africa, a human rights issue. Equal Rights Review 2011, 6, 99–113. [Google Scholar]
- World Health Organization. Mental health of adolescents. Fact sheet. Retrieved from https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health.
- Herman, A.A.; Stein, D.J.; Seedat, S.; Heeringa, S.G.; Moomal, H.; Williams, D.R. The South African Stress and Health (SASH) study: 12-month and lifetime prevalence of common mental disorders. South African Medical Journal 2009, 99, 339–344. [Google Scholar] [PubMed]
- Kilian, S.; Burns, J.K.; Seedat, S.; Ramlall, S. Factors associated with depression and anxiety symptoms in South African adolescents living in low-resource communities. South African Journal of Psychiatry 2019, 25, a1224. [Google Scholar] [CrossRef]
- Lund, C.; Breen, A.; Flisher, A.J.; Kakuma, R.; Corrigall, J.; Joska, J.A.; Patel, V. Poverty and common mental disorders in low- and middle-income countries: A systematic review. Social Science & Medicine 2010, 71, 517–528. [Google Scholar] [CrossRef]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating depression with physical activity in adolescents and young adults: A systematic review and meta-analysis of randomised controlled trials. Psychological Medicine 2018, 48, 1068–1083. [Google Scholar] [CrossRef] [PubMed]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; VanderLannotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychology Review 2015, 9, 366–378. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. British Journal of Sports Medicine 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Bailey, A.P.; Craike, M.; Carter, T.; Patten, R.; Stepto, N.K.; Parker, A.G. Poor reporting of physical activity and exercise interventions in youth mental health trials: A brief report. Early Intervention in Psychiatry 2021, 15, 1414–1422. [Google Scholar] [CrossRef]
- Dennehy, J.; Cameron, M.; Phillips, T.; Kolbe-Alexander, T. Physical activity interventions among youth living in rural and remote areas: A systematic review. Australian and New Zealand Journal of Public Health 2024, 48, 100137. [Google Scholar] [CrossRef]
- Draper, C.E.; Cook, C.J.; Redinger, S.; Rochat, T.; Prioreschi, A.; Rae, D.E.; Ware, L.J.; Lye, S.J.; Norris, S.A. Cross-sectional associations between mental health indicators and social vulnerability, with physical activity, sedentary behaviour and sleep in urban African young women. International Journal of Behavioural Nutrition and Physical Activity 2022, 19, 82. [Google Scholar] [CrossRef]
- Van Zyl, S.; Van der Merwe, M.; Smith, M. Youth mental health and access to services in rural areas of South Africa. South African Journal of Psychology 2021, 51, 519–530. [Google Scholar] [CrossRef]
- Mendenhall, E.; De Silva, M.J.; Hanlon, C.; Petersen, I.; Shidhaye, R.; Jordans, M.; Tomlinson, M. Acceptability and feasibility of using non-specialist health workers to deliver mental health care: Stakeholder perceptions from the PRIME district sites in Ethiopia, India, Nepal, South Africa, and Uganda. Social Science & Medicine 2014, 118, 33–42. [Google Scholar] [CrossRef]
- Micklesfield, L.K.; Pedro, T.M.; Kahn, K.; Kinsman, J.; Pettifor, J.M.; Tollman, S.; Norris, S.A. Physical Activity and Sedentary Behaviour Among Adolescents in Rural South Africa: Levels, Patterns, and Correlates. BMC Public Health 2014, 14, 40. [Google Scholar] [CrossRef]
- Sorsdhal, K.; Flisher, A.J.; Wilson, Z.; Stein, D.J. Explanatory models of mental disorders and treatment practices among traditional healers in Mpumalanga, South Africa. African Journal of Psychiatry 2010, 13, 284–290. [Google Scholar] [CrossRef]
- Asare, K.; Ntlantsana, V.; Ranjit, K.; Tomita, A. Relationship between physical activity and behaviour challenges of adolescents in South Africa. South African Journal of Psychiatry 2023, 29, 2124. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, M.; Swartz, L.; Kruger, L.M.; Gureje, O. Manifestations of mental disorders in sub-Saharan Africa: An overview. African Journal of Psychiatry 2009, 12, 104–108. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implementation Science 2010, 5, 69. [Google Scholar] [CrossRef]
- Munyangane, O.L.; Thaga, L.F.; Vele, R. Exercise as therapy: A scoping review of physical activity interventions for mental health among rural youth in South Africa [Protocol]. Open Science Framework, 2025. [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. Journal of the Medical Library Association 2017, 105, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A., Eds. Cochrane handbook for systematic reviews of interventions (Version 6.4); Cochrane, 2022.
- Kinsman, J.; Norris, S.A.; Kahn, K.; Twine, R.; Riggle, K.; Goudge, J. A model for promoting physical activity among rural South African youth: A qualitative case study of the Agincourt health and socio-demographic surveillance site. BMC Public Health 2015, 15, 318. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; De Hert, M.; Du Plessis, C.; Gbiri, C.A.O.; Kibet, J.; Mugisha, J. A systematic review of physical activity policy recommendations and interventions for people with mental health problems in Sub-Saharan African countries. Pan African Medical Journal 2017, 26, 104. [Google Scholar] [CrossRef]
- Marais, B.S. South African mental healthcare providers’ views about exercise for people with mental illness. South African Journal of Psychiatry 2024, 30, 2227. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.W.; Mafuze, B.; Brooker, J.; Patricios, J.S. Championing mental health: sport and exercise psychiatry for low- and middle-income countries using a model from South Africa. British Journal of Sports Medicine 2024, 58, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Zimu, P.M.; van Heerden, H.J.; Grace, J.M. Nyakaza-Move-for-Health: A culturally tailored physical activity intervention for adolescents in South Africa using the intervention mapping protocol. Journal of Primary Care & Community Health 2024, 15, Article–21501319241278849. [Google Scholar] [CrossRef]
- Siduli, Z.; van Gent, M.M.; Van Niekerk, R.L. Relationship between body composition, physical activity, and mental well-being in Eastern Cape adolescents, South Africa. African Journal for Physical Activity and Health Sciences 2025, 31, 177–190. [Google Scholar] [CrossRef]
- Draper, C.E.; Cook, C.J.; Redinger, S.; Rochat, T.; Prioreschi, A.; Rae, D.E.; Ware, L.J.; Lye, S.J.; Norris, S.A. Cross-sectional associations between mental health indicators and social vulnerability, with physical activity, sedentary behaviour and sleep in urban African young women. International Journal of Behavioral Nutrition and Physical Activity 2022, 19, 82. [Google Scholar] [CrossRef]
- Bermejo-Cantarero, A.; Sánchez-López, M.; García-González, J. Are physical activity interventions effective in improving health-related quality of life and emotional well-being in adolescents? Sports Health 2024, 16, 246–255. [Google Scholar] [CrossRef]
- Kunene, S.H.; Taukobong, N.P. Level of physical activity of health professionals in a district hospital in KwaZulu-Natal, South Africa. South African Journal of Physiotherapy 2015, 71, 234. [Google Scholar] [CrossRef]
- Mumbauer, A.E.; D’Sa, M.; Patel, V. Targeting youth mental health in a demographically young country: A scoping review focused on South Africa. Journal of Child and Adolescent Mental Health 2024, 36, 1–14. [Google Scholar] [CrossRef]
- Tweed, L.M.; Rogers, E.N.; Kinnafick, F.E. Literature on peer-based community physical activity programmes for mental health service users: A scoping review. Health Psychology Review 2021, 15, 287–313. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA-ScR diagram. Adapted from: Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness, L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230. https://doi.org/10.1002/cl2.1230
Figure 1.
PRISMA-ScR diagram. Adapted from: Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness, L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230. https://doi.org/10.1002/cl2.1230
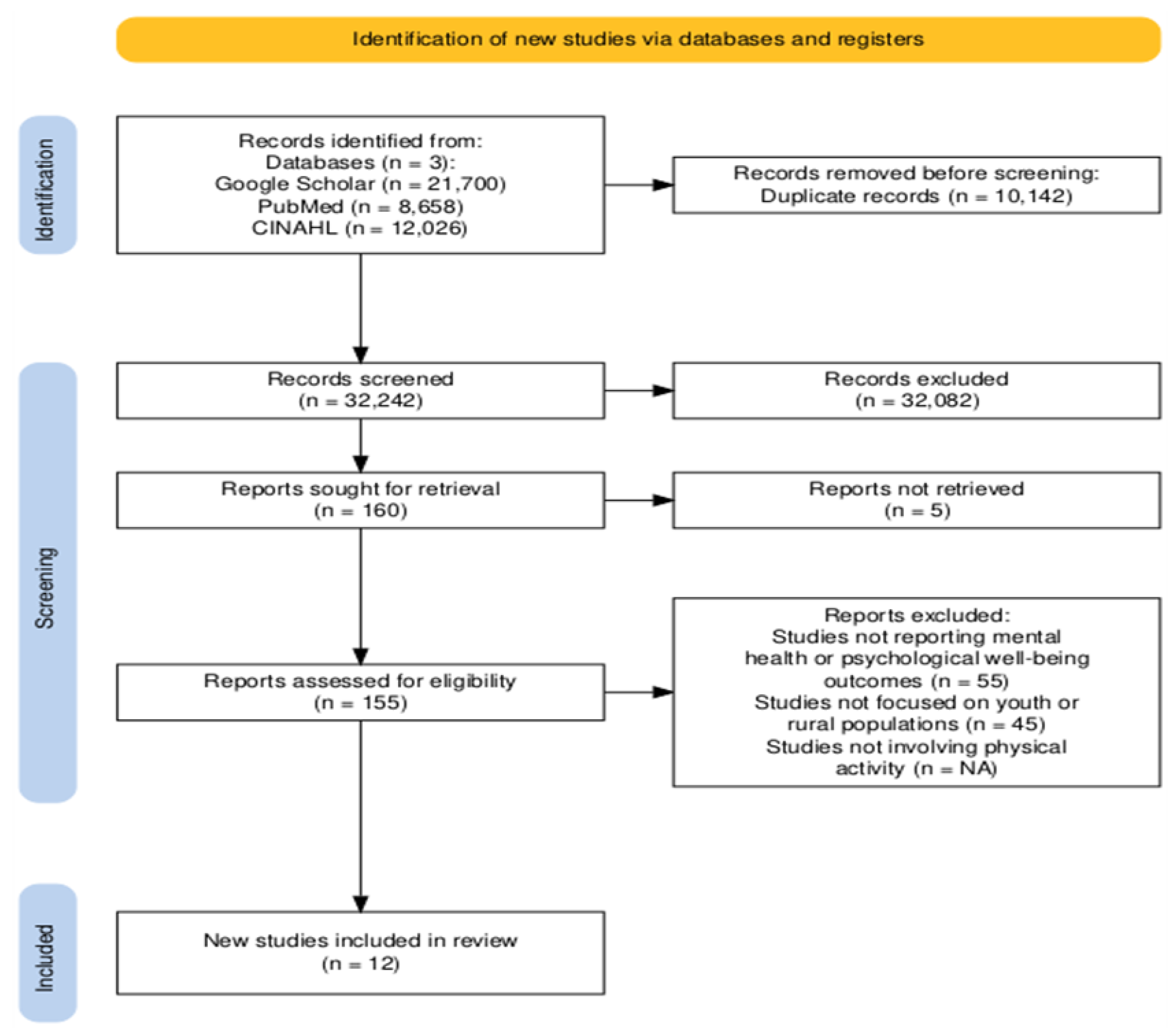
Table 2.
Summary of included Studies
| Author (Year) | Design | Location | Sample and Sampling Technique | Instrument | Outcomes | Intervention |
|---|---|---|---|---|---|---|
| Asare et al. (2023) | Cross-sectional | South Africa – KwaZulu-Natal | 187 adolescents; convenience sample | Strengths & Difficulties Questionnaire, PA recall | Behavioural challenges, prosocial behaviour | None (PA levels and mental health correlation) |
| Kinsman et al. (2015) | Qualitative (model development) | South Africa – rural Mpumalanga | Adolescent girls; purposive sampling | Interviews, FGDs | Barriers to activity, identity, and body image | Model for promoting PA among rural girls |
| Micklesfield et al. (2014) | Cross-sectional | South Africa – Agincourt HDSS, Mpumalanga | 381 adolescents; random cluster sampling | Self-reported PA, SES, and BMI | MVPA, sedentary behaviour | None (baseline behaviour analysis) |
| Vancampfort et al. (2017) | Systematic review | Sub-Saharan Africa | Studies across SSA countries | Not specified | Mental health outcomes in people with MH problems | Policy-level and community interventions |
| Marais (2024) | Qualitative (interviews) | South Africa – National | Mental healthcare providers: purposive sampling | Semi-structured interviews | Attitudes toward exercise for mental illness | Advocacy for integrating PA into mental healthcare |
| Burger et al. (2024) | Commentary/Model proposal | South Africa | N/A – conceptual paper | Not applicable | Advocacy and implementation feasibility | Proposes an SA-based sport and exercise psychiatry model for LMICs |
| Zimu et al. (2024) | Intervention development study | South Africa – KwaZulu-Natal | Adolescents, community and school sampling | Intervention Mapping Protocol | Physical activity engagement, cultural appropriateness | “Nyakaza-Move-for-Health” – culturally tailored adolescent PA programme |
| Siduli et al. (2025) | Cross-sectional | South Africa – Eastern Cape | Adolescents (n ≈ 300); stratified sampling | Body composition measures, PA recall, mental well-being questionnaire | Mental well-being, PA levels, and BMI | Observational – no direct intervention |
| Draper et al. (2022) | Cross-sectional | South Africa – Soweto (urban) | Young women (18–25 years); cohort-based sampling | GHQ-28, accelerometers, sleep logs | Mental health indicators, PA/sedentary behaviour | Observational: highlights associations |
| Bermejo-Cantarero et al. (2024) | Systematic review & meta-analysis | Global | RCTs in children and adolescents | HRQoL scales (PedsQL, SF-36, etc.) | Health-related quality of life (HRQoL) | Evaluated the impact of PA interventions on HRQoL |
| Kunene & Taukobong (2015) | Cross-sectional | South Africa – KwaZulu-Natal | Health professionals in rural district hospital (n=63); convenience sampling | IPAQ – short form | Physical activity levels among health workers | Observational – no intervention |
| Mumbauer et al. (2024) | Scoping review | South Africa | Youth-focused studies (15–24 years) | Review of national data & literature | Youth mental health trends, interventions | Recommends integrated, culturally relevant mental health/PA models |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



