Submitted:
12 October 2025
Posted:
13 October 2025
You are already at the latest version
Abstract
Diabetes mellitus is a rapidly growing global health challenge, with over 589 million affected individuals and a projected prevalence exceeding 853 million by 2050. The complexity of its management, involving continuous monitoring, multifactorial interventions, and long-term complication prevention, has highlighted the need for innovative approaches. Artificial intelligence (AI), encompassing machine learning (ML), deep learning (DL), and natural language processing (NLP), is increasingly applied in diverse domains of diabetes care. AI supports early diagnosis, individualized treatment, prediction of complications, and patient engagement through digital health platforms. Moreover, AI-driven closed-loop insulin delivery systems represent a paradigm shift toward personalized, automated glucose regulation. This narrative review synthesizes the current evidence regarding the applications, benefits, and limitations of AI in diabetes management. Emphasis is given to diagnostic prediction models, glycemic control, complication surveillance, digital coaching, and integration into healthcare systems. Challenges such as data heterogeneity, algorithmic bias, and regulatory frameworks are critically analyzed. Future perspectives include federated learning, multimodal precision diabetology, and ethical frameworks for equitable implementation. The integration of AI into clinical practice offers transformative potential, but requires rigorous validation, patient-centered design, and interdisciplinary collaboration.
Keywords:
artificial intelligence
; diabetes
; monitoring
; diabetes care
Introduction
Diabetes mellitus (DM) is among the foremost causes of global morbidity, mortality, and disability-adjusted life years (DALYs) [1]. The International Diabetes Federation (IDF) reported that in 2024 approximately 589 million adults aged 20–79 years are living with diabetes globally, with projections estimating that number will rise to 853 million by 2050 [2]. This escalating burden reflects both demographic shifts and rising exposure to metabolic risk factors. The pathophysiology of diabetes is inherently complex, involving genetic predisposition, insulin resistance, pancreatic β-cell dysfunction, inflammation, and environmental influences; accordingly, the disease demands not just precise diagnosis but sustained, multifaceted management to forestall acute events (e.g. hyperglycemia, ketoacidosis) and long-term complications (e.g. microvascular and macrovascular) [3].
Despite decades of therapeutic advances, including new insulin analogues, incretin therapies, and glucose sensor technologies, achieving glycemic targets remains a difficult challenge. In many settings, fewer than 50 % of individuals with diabetes consistently attain guideline-recommended HbA₁c thresholds, exposing them to elevated risk of complications [4]. This gap underscores the need for adjunctive strategies to enhance personalization and responsiveness in care.
Concurrently, modern healthcare systems are generating ever-larger volumes of data. Electronic health records (EHRs), continuous glucose monitoring (CGM) streams, wearable sensors, imaging data, and multi-omic platforms are producing dense, high-dimensional datasets that exceed traditional analytic capacity. In this milieu, artificial intelligence (AI), defined as computational systems that mimic human intelligence in problem-solving and decision-making [5], and encompassing machine learning (ML), deep learning (DL), and related methods, offers a compelling paradigm. AI can discern subtle, non-linear patterns across heterogeneous data modalities, enabling earlier detection of risk, more individualized therapeutic recommendations, and prediction of complications before clinical manifestation [6].
This review undertakes a comprehensive, narrative synthesis of AI applications in diabetes care. We critically appraise evidence across domains including early detection, glycemic management, complication forecasting, patient engagement, and health system integration, while highlighting current limitations and proposing future directions. Our goal is to map both the promise and the challenges of AI in diabetology, guiding researchers and clinicians toward responsible, effective translation.
Methods
This study was designed as a narrative review and conducted in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA), which provides a structured framework to enhance methodological rigor and transparency [7]. The SANRA criteria emphasize justification of the review’s importance, comprehensive literature search, critical appraisal of sources, scientific reasoning, appropriate presentation, and balanced referencing. Adhering to these principles, we aimed to provide a coherent and scientifically grounded synthesis of the current state of knowledge regarding the application of AI in diabetes management.
To ensure a broad and representative coverage of the field, a comprehensive search strategy was developed. The primary databases selected were PubMed, Scopus, and Web of Science, as they collectively encompass biomedical, clinical, and interdisciplinary scientific literature. The time frame was restricted to January 2018 through September 2025, thereby capturing the most recent and clinically relevant developments in the rapidly evolving field of AI-driven healthcare.
A combination of controlled vocabulary terms and free-text keywords was employed. The search strategy incorporated terms such as “artificial intelligence,” “machine learning,” “deep learning,” “natural language processing,” “diabetes mellitus,” “prediction,” “diagnosis,” “management,” and “complications.” Boolean operators and database-specific filters were used to maximize sensitivity while maintaining focus on relevant domains.
The inclusion criteria comprised: (1) peer-reviewed original research articles, (2) systematic or scoping reviews, and (3) translational or clinical studies that reported real-world applications of AI in diabetes care. We intentionally prioritized studies that demonstrated clinical or healthcare-related outcomes, as opposed to purely computational or algorithmic advances. The exclusion criteria were defined as (1) theoretical AI frameworks without clinical validation or applicability, and (2) articles published in languages other than English, to ensure interpretability and accuracy of analysis.
Following retrieval, the identified literature was screened by relevance, with emphasis on methodological soundness, novelty, and translational significance. A qualitative synthesis was then performed, whereby findings were organized into thematic domains reflecting the main application areas of AI in diabetes: early diagnosis and risk prediction, glycemic control and insulin delivery, patient engagement and treatment adherence, prediction and prevention of complications, health system integration and limitations, challenges, and future perspectives.
This thematic grouping allowed for a coherent discussion of how AI technologies are shaping different facets of diabetes care, while also highlighting common opportunities and challenges across domains.
Results
A comprehensive search retrieved 1180 records (Figure 1). After removing 220 duplicates, 960 records remained for title and abstract screening. Of these, 790 were excluded as they did not meet the eligibility criteria. The full text of 170 articles was assessed, and 103 were excluded due to reasons such as theoretical without clinical validation, insufficient methodological rigor, or irrelevance to the study aim, non-English upon inspection, retracted at full-text. Ultimately, 67 studies were included in the review.
Early Diagnosis and Risk Prediction
Timely identification of individuals at high risk for type 2 diabetes (T2D) is the cornerstone of preventive diabetology, enabling targeted lifestyle and pharmacological interventions before glycaemia crosses diagnostic thresholds [8]. Traditional scores such as FINDRISC, typically built on logistic regression with a limited set of clinical and anthropometric variables, remain useful for low-cost screening; yet their discriminative performance is modest and varies across populations [9]. Contemporary evaluations confirm that while FINDRISC is practical, its accuracy is outperformed by newer models that learn from richer data modalities [10,11].
AI expands both the breadth and the granularity of risk information by integrating high-dimensional features, ranging from longitudinal electronic health records (EHRs) to lifestyle traces and multi-omics, thereby capturing non-linear interactions that elude conventional approaches [12]. In longitudinal cohorts, machine-learning classifiers such as random forests and gradient-boosting machines consistently equal or surpass regression baselines for incident T2D prediction, often with area under the receiver operating characteristic curve (AUC) values around 0.80–0.90 when trained on routinely collected EHR variables [13,14]. These gains have been replicated across settings and summarized in recent systematic reviews, underscoring the translational maturity of ML for prediabetes and T2D risk prediction [15].
A parallel success story comes from ophthalmic imaging. Deep convolutional neural networks (CNNs) trained on retinal fundus photographs detect diabetic retinopathy (DR) with sensitivities and specificities that match or exceed expert graders, and the first prospective, pivotal trial of an autonomous DR-diagnosis system in primary care demonstrated high diagnostic accuracy without clinician over-read, an important precedent for point-of-care risk stratification workflows [16]. These results have since been validated across multiethnic datasets and, more recently, in real-world evaluations showing productivity gains when autonomous AI is embedded in care pathways [17].
Risk stratification is also moving “beyond the clinic” through passive, continuous phenotyping [18]. Wearables provide dense streams of activity, sleep, and heart-rate variability data that reflect insulin sensitivity and autonomic tone. Emerging studies demonstrate that ML models trained on such digital biomarkers can estimate interstitial glucose dynamics non-invasively and predict insulin resistance or dysglycemia when combined with basic demographics and routine laboratory values, opening the door to scalable, low-burden screening in the general population and to digitally delivered prevention programs [19]. Although several reports are early-phase and some remain preprints, peer-reviewed work now supports the feasibility of deriving glucose-related signals from wrist-worn sensors [20].
All together, these advances suggest a shift from static, questionnaire-based scoring toward dynamic, multimodal risk modeling. In practice, the near-term pathway is hybrid: established scores (e.g., FINDRISC) for broad triage, followed by AI-enhanced models that fuse EHR, imaging, and wearable data to refine individual risk and trigger tailored interventions. As these systems are externally validated across ancestries and care settings, and as deployment studies continue to report operational and equity outcomes, the promise of earlier, more precise prevention appears increasingly attainable.

Table 1.
Selected studies applying AI to diabetes prediction and diagnosis.
| AI Approach | Application | Data Source | Performance Metrics | Key Findings | Reference |
|---|---|---|---|---|---|
| Random Forest | T2DM risk prediction | Electronic health records (EHR) | AUC 0.85–0.90 | Outperformed traditional logistic regression; captured non-linear interactions in longitudinal data | Duan et al. 2025 [21] |
| Gradient Boosting Machine | T2DM incident prediction | EHR with routine clinical variables | AUC 0.80–0.90 | Consistently equaled or surpassed regression baselines across diverse populations | Lv et al. 2023 [13] |
| Deep CNN (fundus images) | DR screening | Retinal fundus photographs | Sensitivity 91%, Specificity comparable to expert graders | Autonomous diagnosis without clinician over-read; validated in primary care settings | Abràmoff et al. 2018 [17] |
| Machine Learning (wearable data) | Prediabetes/insulin resistance screening | Wrist-worn sensors + demographics + labs | AUC not specified; feasibility demonstrated | Non-invasive glucose dynamics estimation; enables scalable population screening | Huang et al. 2025 [19] |
| Gradient Boosting | Gestational diabetes risk | Clinical and anthropometric variables | AUC 0.87 | Early identification enables targeted prenatal interventions | Liu et al. 2022 [22] |
| Random Forest + ML | T2DM diagnosis and prognosis | Tailored heterogeneous feature subsets | High accuracy (specific values vary by subset) | Personalized feature selection improved model performance across populations | Navarro-Cerdán et al. 2025 [14] |
Glycemic Control and Insulin Delivery
AI has become a cornerstone in the evolution of insulin delivery systems, underpinning the development of closed-loop “artificial pancreas” technologies [23]. These systems integrate continuous glucose monitoring (CGM) with algorithm-driven insulin pumps to achieve real-time glucose regulation. Unlike traditional hybrid closed-loop approaches that rely on pre-set parameters, reinforcement learning models continuously update insulin dosing strategies by adapting to glycemic variability induced by meals, exercise, stress, and circadian rhythms [24]. Recent trials demonstrate that such adaptive algorithms improve glycemic control without increasing hypoglycemia risk, marking an important step toward autonomous glucose regulation [25].
Beyond hardware integration, AI also informs decision support tools embedded in smartphone applications. These platforms employ machine-learning algorithms to deliver individualized insulin titration advice and bolus recommendations, outperforming conventional rule-based calculators. Clinical studies indicate that AI-guided bolus support not only improves adherence but also reduces glycemic excursions in both type 1 and insulin-treated type 2 diabetes [26].
A critical metric in modern diabetology, time in range (TIR), has been optimized through AI-based CGM analytics. Machine learning models that detect and predict glucose trends can proactively recommend micro-adjustments, extending TIR and lowering glycemic variability beyond what is achievable through clinician-only interventions [27]. The overall functioning of this AI-driven closed-loop “artificial pancreas” system is illustrated in Figure 2.
Patient Engagement and Treatment Adherence
Self-management lies at the heart of effective diabetes care: patients must constantly balance diet, medication, physical activity, glucose monitoring, and psychosocial stress [28]. In this complex daily endeavor, AI offers promising tools to augment engagement, sustain adherence, and detect early signs of burnout.
One major avenue is mHealth chatbots powered by NLP. These virtual assistants operate 24/7, offering tailored reminders (e.g. “take your insulin,” “check glucose”), motivational messages, and lifestyle suggestions in conversational formats. A recent randomized trial of an AI chatbot in type 2 diabetes showed improved health literacy and engagement compared to control arms [29]. Moreover, systematic reviews of chatbots in chronic disease management report modest but consistent improvements in physical activity, diet, and sleep, interventions that are tangential but relevant to glycemic control [30].
Complementing chatbots, AI-driven digital coaching platforms dynamically personalize behavioral advice by continuously analyzing user data streams (e.g. activity, glucose trends, sleep). In a recent clinical trial combining AI coaching and sensor data, over 70 % of participants with type 2 diabetes achieved HbA1c < 6.5 % within 12 months while reducing pharmacotherapy burden [31]. A meta-analysis of conversational agent interventions in diabetes care also documented mean HbA1c reductions of roughly –0.49 % [32]. These results suggest that AI coaching goes beyond passive support, actively tailoring interventions to individual responses in real time.
Finally, AI can help psychological monitoring and support. Using sentiment analysis and natural language processing of patient-reported text (e.g. journal entries, chatbot conversations), algorithms can flag users at risk of diabetes distress, burnout, or disengagement. In one feasibility study, an automated conversational agent delivered psychoeducational support over three weeks and achieved a statistically greater reduction in diabetes distress compared to self-help book controls (mean DDS reduction ~0.305) in a 156-participant sample [33]. Another study implementing a self-compassion chatbot in diabetes care showed promising reductions in distress and boosts in resilience and self-efficacy [34].
Together, these AI modalities (mHealth chatbots, adaptive coaching, and sentiment-based psychological support) form a synergistic framework for enhancing self-management, sustaining motivation, and supporting emotional well-being in people with diabetes (Figure 3). Continuous evaluation in controlled trials, attention to usability, and safeguarding privacy will be essential as these tools mature.
Prediction and Prevention of Complications
Diabetic patients suffer of different complications, because of the disease [1,35]. The vascular complications are the most dangerous [36]. AI offers powerful new pathways to detect micro- and macrovascular complications of diabetes earlier and more sensitively than traditional clinical markers. In renal disease, for example, machine learning models applied to urinary proteomic data, which quantify peptide patterns excreted in the urine, have been shown to predict progressive loss of kidney function more accurately than conventional markers like albuminuria or estimated glomerular filtration rate (eGFR) [37,38]. A recent large-scale proteomic study in diabetic patients established a protein risk score that significantly enhances prediction of chronic kidney disease progression over baseline clinical variables [39]. Likewise, explainable ML approaches combining serum metabolite features have achieved AUCs up to 0.966 in screening for diabetic nephropathy, demonstrating the potential to flag high-risk individuals well before overt clinical decline [40].
In the domain of neuropathy, AI applications remain emergent but promising [41,42]. For instance, an optimized AI algorithm applied in diabetic populations has shown capability to screen for diabetic peripheral neuropathy (DPN) risk, potentially enabling more targeted evaluation and early intervention [43]. Although robust, controlled, large-scale trials are still limited, the potential to detect subclinical nerve dysfunction prior to symptom onset is compelling when combined with nerve conduction studies or other electrophysiological testing [44].
Cardiovascular comorbidities might be detected using AI-enhanced electrocardiogram (ECG) analysis [45]. Deep learning models trained on standard 12-lead ECGs have been validated to distinguish patients with angiographically confirmed coronary artery disease with high accuracy, suggesting that noninvasive ECGs might flag silent ischemia or elevated cardiovascular risk in diabetic populations [46]. In this retrospective study, an AI-ECG model outperformed traditional risk factors and allowed localization of obstructed vessels from ECG patterns alone.
The application of AI in diabetes foot ulcers (DFUs) management is another important aspect of its potential usefulness in medicine. The pathophysiology of DFUs is complex, mostly originating from a combination of peripheral neuropathy, which diminishes protective sensation, and peripheral arterial disease, which impairs perfusion [47]. This dual pathology renders the foot highly susceptible to injury from repetitive mechanical stress or unnoticed trauma [48]. Two of the most prominent applications of AI in this field are the analysis of thermal imaging and data from smart insoles.
Thermal imaging analysis: Before an ulcer manifests on the skin's surface, underlying inflammatory processes in the subcutaneous tissue cause a localized increase in temperature. Using thermal cameras to capture temperature distribution maps of the plantar surface, AI algorithms can analyze these images to identify "hotspots", areas with statistically significant temperature elevations. This process enables the early detection of pre-ulcerative inflammation, facilitating timely medical intervention before irreversible tissue damage occurs [49,50].
Smart insole data analysis: Abnormal and sustained mechanical pressure is a primary risk factor for DFU development. Smart insoles, embedded with pressure sensors, continuously collect real-time data on plantar pressure distribution as the patient ambulates. This complex data stream is then processed by AI models to identify abnormal peak pressure points or excessively prolonged loading times. The system can provide immediate alerts to the patient via a connected device, prompting them to offload the high-risk area. Furthermore, this longitudinal data provides clinicians with objective insights into a patient's gait and lifestyle, enabling personalized interventions such as custom footwear design and tailored offloading strategies [51].
Together, these AI-driven methods advance the paradigm from reactive diagnosis toward proactive surveillance offer complementary windows into early microvascular and macrovascular damage in diabetes, as summarized in Table 2. Ongoing validation, rigorous prospective trials, and integration with multimodal clinical data will be vital to translate these tools into routine clinical practice.
Health System Integration
AI is progressively being woven into the healthcare systems to support and enhance diabetes care at multiple levels. One of the most mature applications lies in clinical decision support systems (CDSS). In the context of diabetes, AI-based CDSS modules analyze patient-specific data, such as demographics, comorbidities, glucose trends, and medication history, to generate therapeutic recommendations aligned with ADA/EASD guidelines. For example, a recent study described an AI-based CDSS aimed at optimizing basal insulin titration in type 2 diabetes; it demonstrated improved glycemic outcomes and better adherence to evidence-based therapy protocols compared to conventional approaches [53]. A separate usability evaluation documented how clinicians and staff adapted an AI CDSS for diabetes management in real settings, offering insights into challenges and facilitators for adoption [54].
At the population health level, predictive analytics powered by AI help stratify large patient cohorts to flag those at high risk of hospitalization, emergency visits, or deterioration. By anticipating adverse events, health systems can allocate resources more efficiently and apply preventive interventions before crises occur. A commentary on AI and population health underlines how such systems can shift the focus from reactive to proactive care delivery [55]. In diabetes care specifically, this approach allows more effective scheduling of outreach, intensified monitoring, or case management for patients with unstable control or progressive complication risk.
In parallel, telemedicine platforms are being synergized with AI tools to enhance virtual diabetes clinics. AI algorithms can triage incoming messages and alerts (e.g. severe glucose excursions, alarming symptoms) by urgency and relevance, reducing clinician burden and improving response efficiency (Figure 4). Moreover, remote monitoring systems that integrate AI-driven trend detection can flag deviations needing intervention, enabling more timely teleconsultations. Analyses of AI outside hospital settings highlight this potential to extend continuous care beyond traditional clinical boundaries [56].
These system-level AI integrations (clinical decision support, predictive population stratification, and telemedicine augmentation) hold promises to make diabetes care more efficient, proactive, and scalable. Their real-world impact will depend on rigorous validation, integration with workflows, and user acceptance.
Limitations, Challenges, and Future Perspectives
While AI promises to transform diabetes care, its real-world deployment is hindered by significant limitations and ethical challenges that must be carefully investigated. One major obstacle is data heterogeneity and still limited generalizability. Many AI algorithms are developed on single-population cohorts or single-site datasets, which restricts their external applicability. For example, in a recent scoping review of AI models for type 2 diabetes risk prediction, only a minority of studies (5 out of 40) conducted external validation beyond their training population, raising concerns about reproducibility across diverse settings [57]. Without such validation, models may perform poorly when applied to new populations with different demographics, comorbidity profiles, or practice patterns.
Algorithmic bias is closely related. When minority groups or underrepresented subpopulations are not adequately represented in training data, AI systems may perpetuate or even amplify existing health disparities. Recent surveys on fairness in AI healthcare emphasize the risk that biased algorithms could systematically under-predict risk in marginalized groups, leading to missed interventions [58].
Integration barriers remain daunting. Embedding AI into clinical workflows requires interoperability with electronic health record (EHR) systems, standard data formats, and seamless clinician interfaces, challenges often underestimated in pilot studies. Additionally, clinicians face “alert fatigue” and usability hurdles when AI tools force new workflows or generate excessive false alerts. A review of AI adoption barriers in healthcare highlights that usability, training, and institutional readiness are major inhibitors to successful integration [59].
The fields of regulation and ethics are still evolving [60]. The lack of clear frameworks for accountability, liability, auditability, and certification of AI medical tools slows adoption. Some proposals suggest embedding “AI passports,” audit trails, and continuous performance monitoring to mitigate risks. Explainability constraints exacerbate this: many high-performance AI models are “black boxes,” limiting clinician trust. Critics argue that explainable AI is no panacea; transparent explanations can mislead, oversimplify, or instill false confidence if poorly designed [61].
Finally, patient trust and privacy concerns pose critical barriers. People may hesitate to enroll in AI-driven interventions if they perceive data misuse, algorithmic opacity, or lack of human oversight. Without clear explanations and strong data protections, acceptance will lag [62]. The challenges are summarized in Table 3.
Looking forward, several strategies may help overcome these hurdles. Federated learning allows decentralized model training across institutions without centralizing patient-level data, preserving privacy while enhancing generalizability [63]. Multimodal AI, which fuses genomic, metabolomic, microbiome, imaging, and clinical data, may push the frontier of precision diabetology by modeling interactions across biological scales [64,65]. To build confidence, explainable AI (XAI) methodologies must be embedded throughout development to elucidate reasoning in clinician-usable forms [66,67]. Ethical frameworks that emphasize equity, accountability, and patient empowerment should guide deployment. Importantly, the field must move toward prospective, large-scale randomized clinical trials that test not only accuracy, but clinical effectiveness, safety, and system-level impact. Only through rigorous validation and transparent, patient-centric design AI can fulfill its promise in diabetes care.
Limitations of the study: The principal limitations of this narrative review are several. First, its non-systematic methodology inherently allows for selection bias and may lead to incomplete or uneven coverage of relevant literature, as narrative reviews lack fixed protocols and transparency in study selection. Second, the narrative synthesis approach limits reproducibility and prevents formal evidence grading or risk-of-bias assessment common in systematic reviews. Third, many of the concepts and models discussed lack robust external validation across diverse populations, constraining generalizability. Fourth, the exclusion of non-English publications may have led to omission of important findings published in other languages. Finally, by not conducting a quantitative meta-analysis, the review cannot produce pooled effect sizes or formally assess heterogeneity among studies.
Conclusion
Artificial intelligence offers unprecedented opportunities to transform diabetes care. By enabling earlier diagnosis, personalized therapy, optimized glycemic control, and proactive complication prevention, AI has the potential to reduce the burden of disease and improve quality and quantity of life. Nonetheless, challenges related to validation, fairness, and regulation must be addressed to ensure safe and equitable implementation. Interdisciplinary collaboration among clinicians, data scientists, policymakers, and patients will determine whether AI fulfills its promise as a cornerstone of future diabetology.
Acknowledgments
We extend our sincere gratitude to the Fondazione Paolo Procacci for their invaluable support and assistance throughout the publication process and valuable discussions. We are also grateful to John Shaw for his assistance with the final English revision.
Author Contributions
Conceptualization, G.V.; methodology, G.V., M.L.G.L.; data curation, G.V., M.L.G.L., A.A.A.A., T.V.Y., P.V.P., and D.C.; writing—original draft preparation, G.V., M.L.G.L., and G.F.; writing—review and editing, M.L.G.L., G.F., T.V.Y, P.V.P, and A.C.; supervision, G.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available upon reasonable request to the corresponding author.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process
During the preparation of this manuscript the authors used ChatGPT in order to improve the language. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the contents of the published article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADA | American Diabetes Association |
| AI | Artificial Intelligence |
| AUC | Area Under the ROC Curve |
| CAD | Coronary Artery Disease |
| CDSS | Clinical Decision Support System |
| CGM | Continuous Glucose Monitoring |
| CNN | Convolutional Neural Network |
| CVD | Cardiovascular Disease |
| DALY(s) | Disability-Adjusted Life Year(s) |
| DFU | Diabetic Foot Ulcer |
| DL | Deep Learning |
| DM | Diabetes Mellitus |
| DPN | Diabetic Peripheral Neuropathy |
| DR | Diabetic Retinopathy |
| EASD | European Association for the Study of Diabetes |
| ECG | Electrocardiogram |
| eGFR | Estimated Glomerular Filtration Rate |
| EHR(s) | Electronic Health Record(s) |
| FINDRISC | Finnish Diabetes Risk Score |
| FL | Federated Learning |
| GBDT / GBM | Gradient Boosted Decision Trees / Gradient Boosting Machine |
| GDM | Gestational Diabetes Mellitus |
| HbA1c | Hemoglobin A1c |
| HL7 FHIR | (Health Level Seven) Fast Healthcare Interoperability Resources |
| IDF | International Diabetes Federation |
| mHealth | Mobile Health |
| ML | Machine Learning |
| NLP | Natural Language Processing |
| PCA | Principal Component Analysis |
| RF | Random Forest |
| RL | Reinforcement Learning |
| ROC | Receiver Operating Characteristic |
| SANRA | Scale for the Assessment of Narrative Review Articles |
| T2D / T2DM | Type 2 Diabetes (Mellitus) |
| TIR | Time In Range |
| XAI | Explainable Artificial Intelligence |
References
- Olanrewaju, O.A.; Sheeba, F.; Kumar, A.; Ahmad, S.; Blank, N.; Kumari, R.; Kumari, K.; Salame, T.; Khalid, A.; Yousef, N.; Varrassi, G.; Khatri, M.; Kumar, S.; Mohamad, T. Novel Therapies in Diabetes: A Comprehensive Narrative Review of GLP-1 Receptor Agonists, SGLT2 Inhibitors, and Beyond. Cureus. 2023, 15, e51151. [Google Scholar] [CrossRef]
- International Diabetes Federation (IDF). Diabetes around the world in 2024. Available at: https://idf.org/about-diabetes/diabetes-facts-figures/.
- Banday, M.Z.; Sameer, A.S.; Nissar, S. Pathophysiology of diabetes: An overview. Avicenna J Med. 2020, 10, 174–188. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Cho, Y.; Seo, D.H.; Ahn, S.H.; Hong, S.; Suh, Y.J.; Chon, S.; Woo, J.T.; Baik, S.H.; Lee, K.W.; Kim, S.H. Impact of diabetes distress on glycemic control and diabetic complications in type 2 diabetes mellitus. Sci Rep. 2024, 14, 5568. [Google Scholar] [CrossRef] [PubMed]
- Bini, S.A. Artificial Intelligence, Machine Learning, Deep Learning, and Cognitive Computing: What Do These Terms Mean and How Will They Impact Health Care? J Arthroplasty. 2018, 33, 2358–2361. [Google Scholar] [CrossRef] [PubMed]
- Dankwa-Mullan, I.; Rivo, M.; Sepulveda, M.; Park, Y.; Snowdon, J.; Rhee, K. Transforming Diabetes Care Through Artificial Intelligence: The Future Is Here. Popul Health Manag. 2019, 22, 229–242. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef]
- Narayan, K.M.; Chan, J.; Mohan, V. Early identification of type 2 diabetes: policy should be aligned with health systems strengthening. Diabetes Care. 2011, 34, 244–6. [Google Scholar] [CrossRef]
- Pesaro, A.E.; Bittencourt, M.S.; Franken, M.; Carvalho, J.A.M.; Bernardes, D.; Tuomilehto, J.; Santos, R.D. The Finnish Diabetes Risk Score (FINDRISC), incident diabetes and low-grade inflammation. Diabetes Res Clin Pract. 2021, 171, 108558. [Google Scholar] [CrossRef]
- Acosta-Reyes, J.; Rodríguez Garrido, D.P.; Vergara, T.A.; Aschner, P.; Fraga, C.A.; Vazquez-Fernandez, A.; Tuomilehto, J.; Gabriel, R. Finnish diabetes risk score (findrisc) for type 2 diabetes screening compared with the oral glucose tolerance test: A systematic review and meta-analysis of diagnostic test accuracy. Diabetes Res Clin Pract. 2025, 112480. [Google Scholar] [CrossRef]
- Jude, E.B.; Saluja, S.; Heald, A.; Widiatmoko, D.; Schaper, N.; Anderson, S.G. Improving Diabetes and Pre-Diabetes Detection in the UK: Insights From HbA1c Screening in an Acute Hospital's Emergency Department. Diabetes Ther. 2025, 16, 1917–1932. [Google Scholar] [CrossRef]
- Song, C.M.; Lin, T.H.; Huang, H.T.; Yao, J.Y. Illuminating diabetes via multi-omics: Unraveling disease mechanisms and advancing personalized therapy. World J Diabetes. 2025, 16, 106218. [Google Scholar] [CrossRef]
- Lv, K.; Cui, C.; Fan, R.; Zha, X.; Wang, P.; Zhang, J.; Zhang, L.; Ke, J.; Zhao, D.; Cui, Q.; Yang, L. Detection of diabetic patients in people with normal fasting glucose using machine learning. BMC Med. 2023, 21, 342. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Cerdán, J.R.; Pons-Suñer, P.; Arnal, L.; Arlandis, J.; Llobet, R.; Perez-Cortes, J.C.; Lara-Hernández, F.; Moya-Valera, C.; Quiroz-Rodriguez, M.E.; Rojo-Martinez, G.; Valdés, S.; Montanya, E.; Calle-Pascual, A.L.; Franch-Nadal, J.; Delgado, E.; Castaño, L.; García-García, A.B.; Chaves, F.J. A machine learning approach for type 2 diabetes diagnosis and prognosis using tailored heterogeneous feature subsets. Med Biol Eng Comput. 2025, 63, 2733–2752. [Google Scholar] [CrossRef] [PubMed]
- Deberneh, H.M.; Kim, I. Prediction of Type 2 Diabetes Based on Machine Learning Algorithm. Int J Environ Res Public Health. 2021, 18, 3317. [Google Scholar] [CrossRef]
- Abbasi, R.; Amin, F.; Alabrah, A.; Choi, G.S.; Khan, S.; Bin Heyat, M.B.; Iqbal, M.S.; Chen, H. Diabetic retinopathy detection using adaptive deep convolutional neural networks on fundus images. Sci Rep. 2025, 15, 24647. [Google Scholar] [CrossRef]
- Abràmoff, M.D.; Lavin, P.T.; Birch, M.; Shah, N.; Folk, J.C. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digit Med. 2018, 1, 39. [Google Scholar] [CrossRef]
- Wagner, R.; Heni, M.; Tabák, A.G.; Machann, J.; Schick, F.; Randrianarisoa, E.; Hrabě de Angelis, M.; Birkenfeld, A.L.; Stefan, N.; Peter, A.; Häring, H.U.; Fritsche, A. Pathophysiology-based subphenotyping of individuals at elevated risk for type 2 diabetes. Nat Med. 2021, 27, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Schmelter, F.; Seitzer, C.; Martensen, L.; Otzen, H.; Piet, A.; Witt, O.; Schröder, T.; Günther, U.L.; Marshall, L.; Grzegorzek, M.; Sina, C. Digital biomarkers for interstitial glucose prediction in healthy individuals using wearables and machine learning. Sci Rep. 2025, 15, 30164. [Google Scholar] [CrossRef]
- Li, T.; Wang, Q.; Lei, L.; An, Y.; Guo, L.; Ren, L.; Chen, X. Improvement of Non-Invasive Glucose Estimation Accuracy Through Multi-Wavelength PPG. IEEE J Biomed Health Inform. 2025, 29, 5465–5478. [Google Scholar] [CrossRef]
- Duan, J.; Nayan, N.M. Type 2 Diabetes Prediction Model in China: A Five-Year Systematic Review. Healthcare (Basel). 2025, 13, 2007. [Google Scholar] [CrossRef]
- Liu, Q.; Zhou, Q.; He, Y.; Zou, J.; Guo, Y.; Yan, Y. Predicting the 2-Year Risk of Progression from Prediabetes to Diabetes Using Machine Learning among Chinese Elderly Adults. J Pers Med. 2022, 12, 1055. [Google Scholar] [CrossRef]
- Trevitt, S.; Simpson, S.; Wood, A. Artificial Pancreas Device Systems for the Closed-Loop Control of Type 1 Diabetes: What Systems Are in Development? J Diabetes Sci Technol. 2016, 10, 714–23. [Google Scholar] [CrossRef]
- Bergenstal, R.M.; Nimri, R.; Beck, R.W.; Criego, A.; Laffel, L.; Schatz, D.; Battelino, T.; Danne, T.; Weinzimer, S.A.; Sibayan, J.; Johnson, M.L.; Bailey, R.J.; Calhoun, P.; Carlson, A.; Isganaitis, E.; Bello, R.; Albanese-O'Neill, A.; Dovc, K.; Biester, T.; Weyman, K.; Hood, K.; Phillip, M.; FLAIR Study Group. A comparison of two hybrid closed-loop systems in adolescents and young adults with type 1 diabetes (FLAIR): a multicentre, randomised, crossover trial. Lancet. 2021, 397, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Rosales, N.; De Battista, H.; Garelli, F. Hypoglycemia prevention: PID-type controller adaptation for glucose rate limiting in Artificial Pancreas System. Biomedical Signal Processing and Control. 2022, 71, 103106. [Google Scholar] [CrossRef]
- Vettoretti, M.; Cappon, G.; Facchinetti, A.; Sparacino, G. Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring Sensors. Sensors (Basel). 2020, 20, 3870. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; Cobelli, C.; Dassau, E.; DeVries, J.H.; Donaghue, K.C.; Dovc, K.; Doyle FJ3rd Garg, S.; Grunberger, G.; Heller, S.; Heinemann, L.; Hirsch, I.B.; Hovorka, R.; Jia, W.; Kordonouri, O.; Kovatchev, B.; Kowalski, A.; Laffel, L.; Levine, B.; Mayorov, A.; Mathieu, C.; Murphy, H.R.; Nimri, R.; Nørgaard, K.; Parkin, C.G.; Renard, E.; Rodbard, D.; Saboo, B.; Schatz, D.; Stoner, K.; Urakami, T.; Weinzimer, S.A.; Phillip, M. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Balakrishnanpillai, J.; Kesavadev, J.; Saboo, B. Harmony in Health: A Narrative Review Exploring the Interplay of Mind, Body, and Diabetes with a Special Emphasis on Emotional Stress. Journal of Diabetology. 2024, 15, 123–30. [Google Scholar] [CrossRef]
- Kelly, A.; Noctor, E.; Ryan, L.; van de Ven, P. The Effectiveness of a Custom AI Chatbot for Type 2 Diabetes Mellitus Health Literacy: Development and Evaluation Study. J Med Internet Res. 2025, 27, e70131. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Olds, T.; Brinsley, J.; Dumuid, D.; Virgara, R.; Matricciani, L.; Watson, A.; Szeto, K.; Eglitis, E.; Miatke, A.; Simpson, C.E.M.; Vandelanotte, C.; Maher, C. Systematic review and meta-analysis of the effectiveness of chatbots on lifestyle behaviours. NPJ Digit Med. 2023, 6, 118. [Google Scholar] [CrossRef]
- Pantalone, K.M.; Xiao, H.; Bena, J.; Morrison, S.; Downie, S.; Boyd, A.M.; Shah, L.; Willis, B.; Beharry-Diaz, J.; Milinovich, A.; Joshi, S. Type 2 Diabetes Pharmacotherapy De-Escalation Through AI-Enabled Lifestyle Modifications: A Randomized Clinical Trial. NEJM Catalyst Innovations in Care Delivery. 2025, 6, CAT–25. [Google Scholar] [CrossRef]
- Shegal, M.; Hu, L.T.; Friesen, E.; Minian, N.; Maslej, M.; Rodak, T.; Whitmore, C.; Sherifali, D.; Selby, P.; Melamed, O.C. Conversational agent interventions in diabetes care: a systematic review. Diabetes Res Clin Pract. 2025, 228, 112429. [Google Scholar] [CrossRef]
- Bruijnes, M.; Kesteloo, M.; Brinkman, W.P. Reducing social diabetes distress with a conversational agent support system: a three-week technology feasibility evaluation. Front Digit Health. 2023, 5, 1149374. [Google Scholar] [CrossRef]
- Boggiss, A.L.; Babbott, K.; Milford, Ā.; Ellett, S.; Consedine, N.; Reid, S.; Cao, N.; Cavadino, A.; Hopkins, S.; Jefferies, C.; de Bock, M.; Serlachius, A. The usability and feasibility of a self-compassion chatbot (COMPASS) for youth living with type 1 diabetes. Diabet Med. 2025, e70115. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Irfan, M.; Khan, M.; Khan, M.K.; Awan, S.K.; Raza, S.S.; Adil, A.N.K.; Varrassi, G. From Glycemia to Grip: A Comprehensive Review of Musculoskeletal Complications in Diabetic Patients. Cureus. 2025, 17, e90838. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, W.; Liu, J.; Xie, M.; Liu, Q.; Li, S. Vascular complications of diabetes: A narrative review. Medicine (Baltimore). 2023, 102, e35285. [Google Scholar] [CrossRef] [PubMed]
- Massy, Z.A.; Lambert, O.; Metzger, M.; Sedki, M.; Chaubet, A.; Breuil, B.; Jaafar, A.; Tack, I.; Nguyen-Khoa, T.; Alves, M.; Siwy, J.; Mischak, H.; Verbeke, F.; Glorieux, G.; Herpe, Y.E.; Schanstra, J.P.; Stengel, B.; Klein, J.; CKD-REIN study group. Machine Learning-Based Urine Peptidome Analysis to Predict and Understand Mechanisms of Progression to Kidney Failure. Kidney Int Rep. 2022, 8, 544–555. [Google Scholar] [CrossRef]
- Zheng, Y.; Liao, S.; Yang, X.; Zhao, N.; Xiang, J.; Zhou, S.; Wu, S.; Yuan, X.; Luo, Y.; Zeng, L. Identification of Potential Urine Biomarkers of Hypertensive Nephropathy for Predicting Disease Progression Based on Metabolomics and Peptidomics. J Proteome Res. 2025, 24, 4478–4490. [Google Scholar] [CrossRef]
- Ye, Z.; Zhang, Y.; Zhang, Y.; Yang, S.; He, P.; Liu, M.; Zhou, C.; Gan, X.; Huang, Y.; Xiang, H.; Hou, F.F.; Qin, X. Large-Scale Proteomics Improve Prediction of Chronic Kidney Disease in People With Diabetes. Diabetes Care. 2024, 47, 1757–1763. [Google Scholar] [CrossRef]
- Yin, J.M.; Li, Y.; Xue, J.T.; Zong, G.W.; Fang, Z.Z.; Zou, L. Explainable Machine Learning-Based Prediction Model for Diabetic Nephropathy. J Diabetes Res. 2024, 2024, 8857453. [Google Scholar] [CrossRef]
- El-Tallawy, S.N.; Pergolizzi, J.V.; Vasiliu-Feltes, I.; Ahmed, R.S.; LeQuang, J.K.; El-Tallawy, H.N.; Varrassi, G.; Nagiub, M.S. Incorporation of "Artificial Intelligence" for Objective Pain Assessment: A Comprehensive Review. Pain Ther. 2024, 13, 293–317. [Google Scholar] [CrossRef]
- Corriero, A.; Giglio, M.; Soloperto, R.; Preziosa, A.; Stefanelli, C.; Castaldo, M.; Gloria, F.; Paladini, A.; Guardamagna, V.A.; Puntillo, F. The Missing Link: Integrating Interventional Pain Management in the Era of Multimodal Oncology. Pain Ther. 2025, 14, 1223–1246. [Google Scholar] [CrossRef]
- Sartore, G.; Ragazzi, E.; Pegoraro, F.; Pagno, M.G.; Lapolla, A.; Piarulli, F. Artificial Intelligence Algorithm to Screen for Diabetic Neuropathy: A Pilot Study. Biomedicines. 2025, 13, 1075. [Google Scholar] [CrossRef]
- van Doorn, I.N.; Eftimov, F.; Wieske, L.; van Schaik, I.N.; Verhamme, C. Challenges in the Early Diagnosis and Treatment of Chronic Inflammatory Demyelinating Polyradiculoneuropathy in Adults: Current Perspectives. Ther Clin Risk Manag. 2024, 20, 111–126. [Google Scholar] [CrossRef]
- Muzammil, M.A.; Javid, S.; Afridi, A.K.; Siddineni, R.; Shahabi, M.; Haseeb, M.; Fariha, F.N.U.; Kumar, S.; Zaveri, S.; Nashwan, A.J. Artificial intelligence-enhanced electrocardiography for accurate diagnosis and management of cardiovascular diseases. J Electrocardiol. 2024, 83, 30–40. [Google Scholar] [CrossRef]
- Huang, P.S.; Tseng, Y.H.; Tsai, C.F.; Chen, J.J.; Yang, S.C.; Chiu, F.C.; Chen, Z.W.; Hwang, J.J.; Chuang, E.Y.; Wang, Y.C.; Tsai, C.T. An Artificial Intelligence-Enabled ECG Algorithm for the Prediction and Localization of Angiography-Proven Coronary Artery Disease. Biomedicines. 2022, 10, 394. [Google Scholar] [CrossRef]
- Ramachandran, V.; Mohanasundaram, T.; Karunakaran, D.; Gunasekaran, M.; Tiwari, R. Physiological and Pathophysiological Aspects of Diabetic Foot Ulcer and its Treatment Strategies. Current Diabetes Reviews 19, 127–139. [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. New England Journal of Medicine. 2017, 376, 2367–75. [Google Scholar] [CrossRef]
- Ghosh, A.; Ray, S.; Garg, M.K.; Chowdhury, S.; Mukhopadhyay, S. The role of infrared dermal thermometry in the management of neuropathic diabetic foot ulcers. Diabetic Medicine. 2021, 38, e14368. [Google Scholar] [CrossRef]
- Najafi, B.; Reeves, N.D.; Armstrong, D.G. Leveraging smart technologies to improve the management of diabetic foot ulcers and extend ulcer-free days in remission. Diabetes/Metabolism Research and Reviews. 2020, 36, e3239. [Google Scholar] [CrossRef]
- Agrawal, D.K.; Jongpinit, W.; Pojprapai, S.; Usaha, W.; Wattanapan, P.; Tangkanjanavelukul, P.; et al. Smart Insole-Based Plantar Pressure Analysis for Healthy and Diabetic Feet Classification: Statistical vs. Machine Learning Approaches. Technologies. 2024, 12, 231. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Pasquale, L.R.; Peng, L.; Campbell, J.P.; Lee, A.Y.; Raman, R.; Tan, G.S.W.; Schmetterer, L.; Keane, P.A.; Wong, T.Y. Artificial intelligence and deep learning in ophthalmology. Br J Ophthalmol. 2019, 103, 167–175. [Google Scholar] [CrossRef]
- Thomsen, C.H.N.; Kronborg, T.; Hangaard, S.; Vestergaard, P.; Jensen, M.H. Developing an AI-Based clinical decision support system for basal insulin titration in type 2 diabetes in primary Care: A Mixed-Methods evaluation using heuristic Analysis, user Feedback, and eye tracking. Int J Med Inform. 2025, 195, 105783. [Google Scholar] [CrossRef]
- Liaw, W.R.; Ramos Silva, Y.; Soltero, E.G.; Krist, A.; Stotts, A.L. An Assessment of How Clinicians and Staff Members Use a Diabetes Artificial Intelligence Prediction Tool: Mixed Methods Study. JMIR AI. 2023, 2, e45032. [Google Scholar] [CrossRef]
- Mutharasan, R.K.; Walradt, J. Population Health and Artificial Intelligence. JACC: Advances. 2024, 3, 101092. [Google Scholar] [CrossRef]
- Aggarwal, N.; Ahmed, M.; Basu, S.; Curtin, J.J.; Evans, B.J.; Matheny, M.E.; Nundy, S.; Sendak, M.P.; Shachar, C.; Shah, R.U.; Thadaney-Israni, S. Advancing Artificial Intelligence in Health Settings Outside the Hospital and Clinic. NAM Perspect. 2020, 2020, 10.31478/202011f. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, F.; Al-Absi, H.R.H.; Yousri, N.A.; El Hajj, N.; Shah, Z. A scoping review of artificial intelligence-based methods for diabetes risk prediction. NPJ Digit Med. 2023, 6, 197. [Google Scholar] [CrossRef]
- Chinta, S.V.; Wang, Z.; Palikhe, A.; Zhang, X.; Kashif, A.; Smith, M.A.; Liu, J.; Zhang, W. AI-driven healthcare: Fairness in AI healthcare: A survey. PLOS Digit Health. 2025, 4, e0000864, Erratum in: PLOS Digit Health. 2025 Aug 21;4(8):e0000994. [Google Scholar] [CrossRef]
- Hassan, M.; Kushniruk, A.; Borycki, E. Barriers to and Facilitators of Artificial Intelligence Adoption in Health Care: Scoping Review. JMIR Hum Factors. 2024, 11, e48633. [Google Scholar] [CrossRef]
- Cascella, M.; Shariff, M.N.; Viswanath, O.; Leoni, M.L.G.; Varrassi, G. Ethical Considerations in the Use of Artificial Intelligence in Pain Medicine. Curr Pain Headache Rep. 2025, 29, 10. [Google Scholar] [CrossRef]
- Ghassemi, M.; Oakden-Rayner, L.; Beam, A.L. The false hope of current approaches to explainable artificial intelligence in health care. Lancet Digit Health. 2021, 3, e745–e750. [Google Scholar] [CrossRef]
- Pergolizzi JVJr LeQuang, J.A.K.; El-Tallawy, S.N.; Varrassi, G. What Clinicians Should Tell Patients About Wearable Devices and Data Privacy: A Narrative Review. Cureus. 2025, 17, e81167. [Google Scholar] [CrossRef]
- Lu, Y.; Zhang, B.; Tong, J.; Chen, Y. Meta-Analysis and Federated Learning over Decentralized Distributed Research Networks. Annu Rev Biomed Data Sci. 2025, 8, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Simon, B.D.; Ozyoruk, K.B.; Gelikman, D.G.; Harmon, S.A.; Türkbey, B. The future of multimodal artificial intelligence models for integrating imaging and clinical metadata: a narrative review. Diagn Interv Radiol. 2025, 31, 303–312. [Google Scholar] [CrossRef]
- Buess, L.; Keicher, M.; Navab, N.; Maier, A.; Tayebi Arasteh, S. From large language models to multimodal AI: a scoping review on the potential of generative AI in medicine. Biomed Eng Lett. 2025, 15, 845–863. [Google Scholar] [CrossRef]
- Jung, J.; Lee, H.; Jung, H.; Kim, H. Essential properties and explanation effectiveness of explainable artificial intelligence in healthcare: A systematic review. Heliyon. 2023, 9, e16110. [Google Scholar] [CrossRef]
- van Leersum, C.M.; Maathuis, C. Human centred explainable AI decision-making in healthcare. J Respons Technol. 2025, 21, 100108. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram illustrating the study selection process.
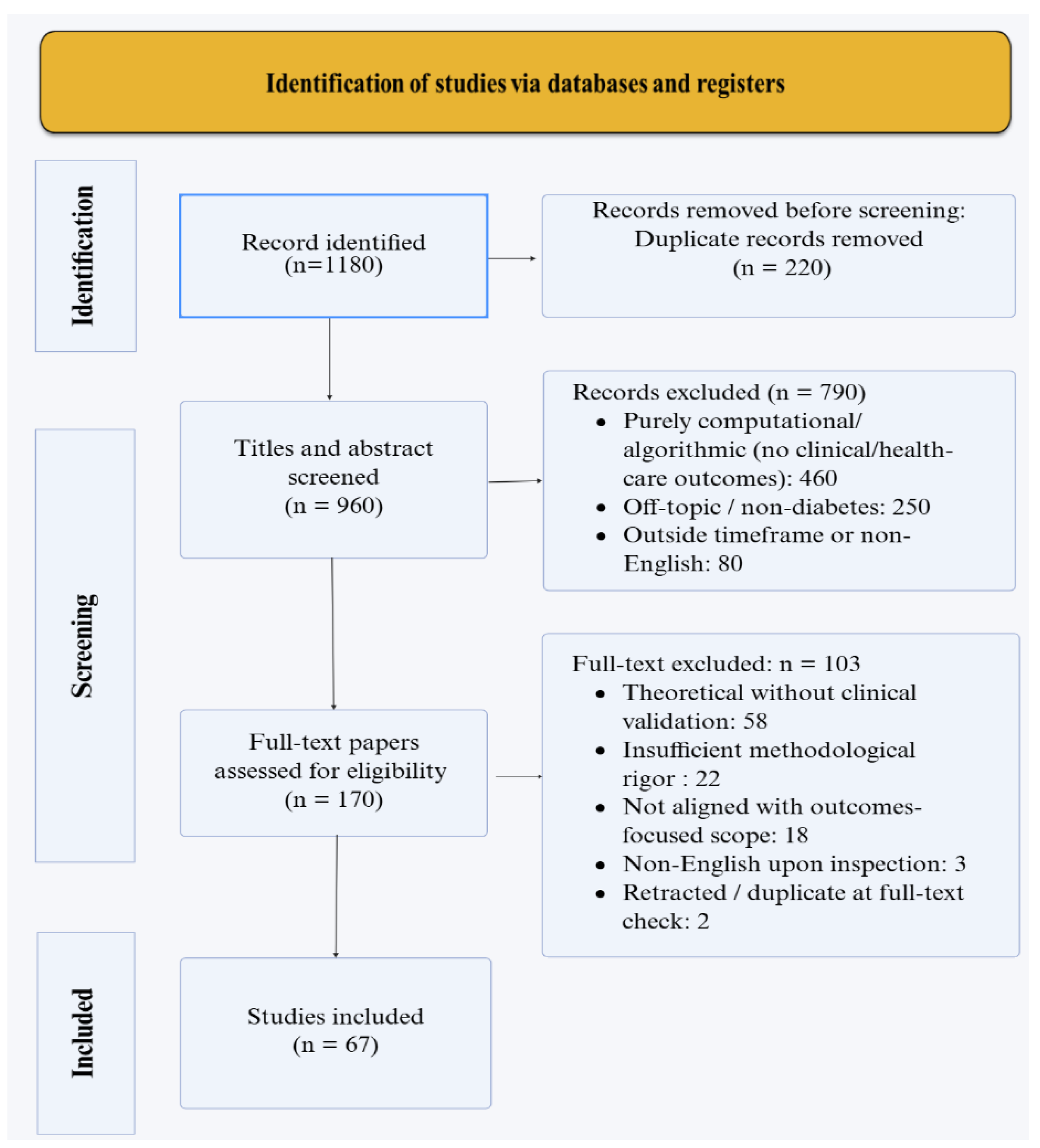
Figure 2.
Schematic representation of AI-driven closed-loop “artificial pancreas” system. CGM devices collect real-time glycemic variability inputs, reflecting fluctuations due to diet, activity, and physiological factors, which are processed by AI algorithms to predict glucose trends and optimize insulin dosing.
Figure 2.
Schematic representation of AI-driven closed-loop “artificial pancreas” system. CGM devices collect real-time glycemic variability inputs, reflecting fluctuations due to diet, activity, and physiological factors, which are processed by AI algorithms to predict glucose trends and optimize insulin dosing.
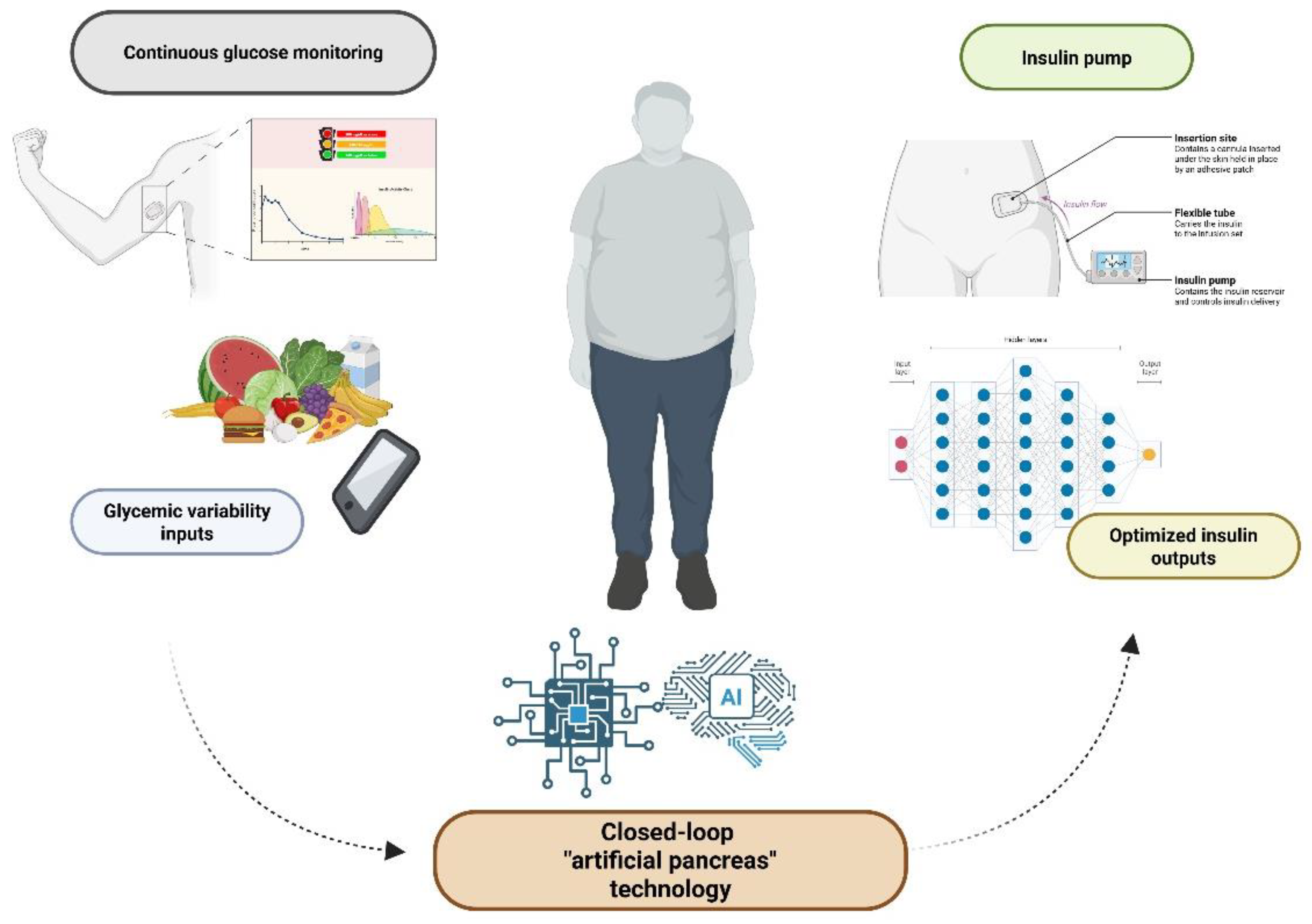
Figure 3.
- AI-powered self-management in diabetes. The figure depicts how mobile health (mHealth) chatbots, wearable sensors, and AI-driven coaching systems integrate continuous behavioral and physiological data to support personalized feedback, motivation, and emotional well-being. These interconnected components form an adaptive digital ecosystem that empowers patients in daily diabetes self-care.
Figure 3.
- AI-powered self-management in diabetes. The figure depicts how mobile health (mHealth) chatbots, wearable sensors, and AI-driven coaching systems integrate continuous behavioral and physiological data to support personalized feedback, motivation, and emotional well-being. These interconnected components form an adaptive digital ecosystem that empowers patients in daily diabetes self-care.
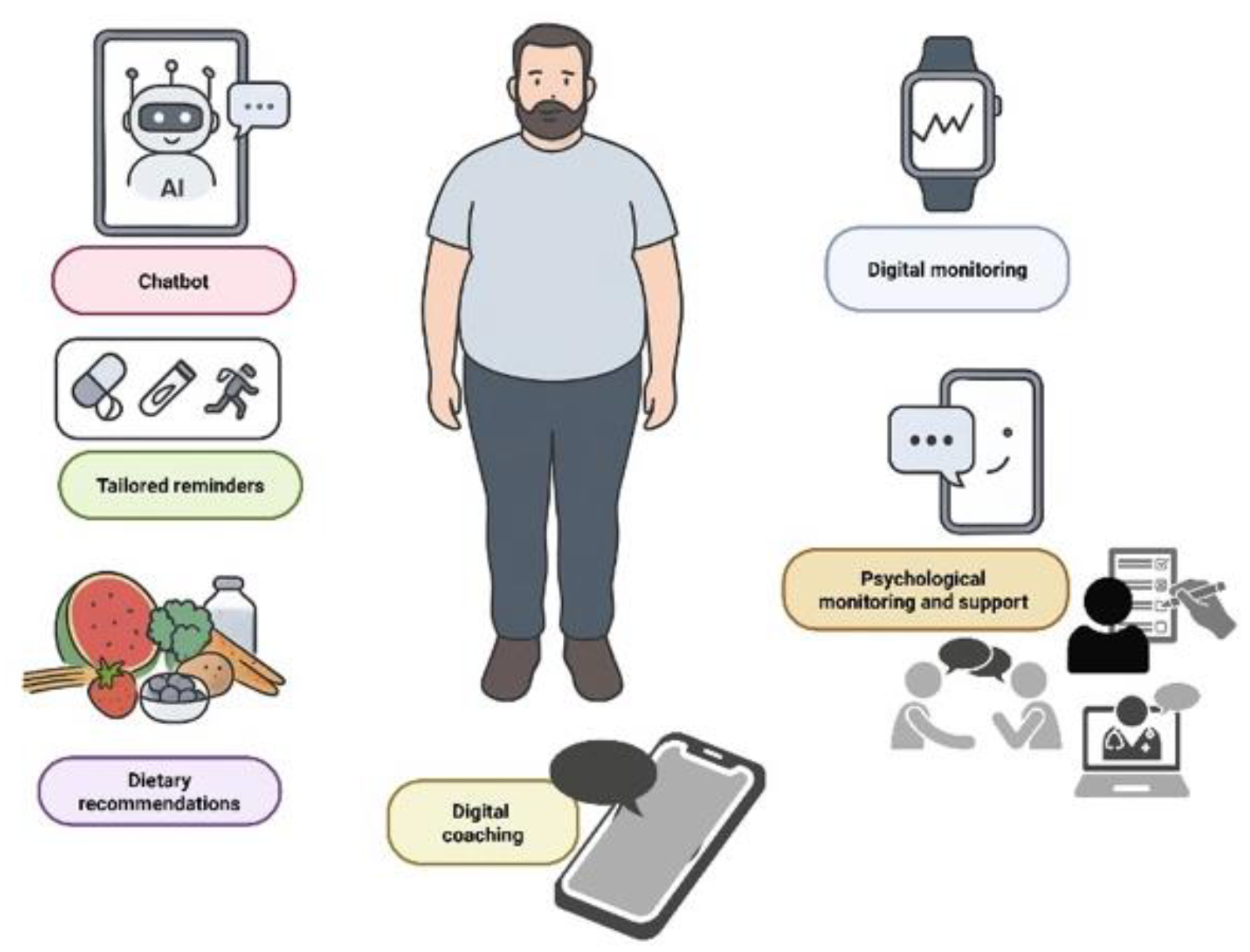
Figure 4.
AI-enabled virtual diabetes clinic.
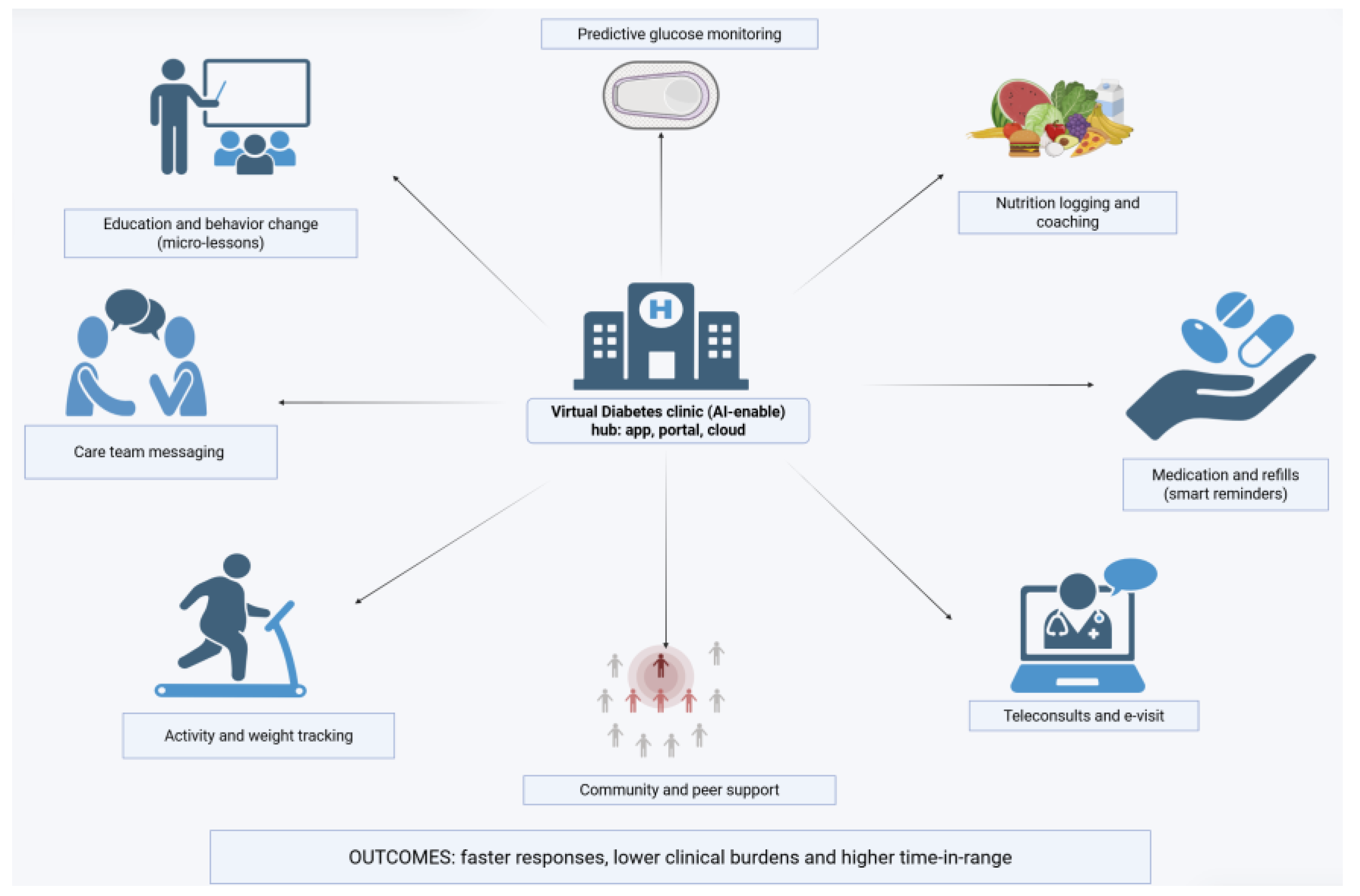
Table 2.
AI Applications in Diabetes Complication Prediction and Detection.
| Complication | AI Technique | Data Modality | Performance | Clinical Utility | Validation Status | Reference |
|---|---|---|---|---|---|---|
| Diabetic Nephropathy | Gradient Boosting on proteomic data | Urinary peptide patterns | AUC 0.88 | Predicts progressive kidney function loss more accurately than albuminuria or eGFR alone | Large-scale proteomic validation | Massy et al. 2022 [38] |
| Diabetic Nephropathy | Explainable ML (metabolomics) | Serum metabolite profiles | AUC 0.966 | Flags high-risk individuals before overt clinical decline; interpretable predictions | Peer-reviewed screening study | Yin et al. 2024 [41] |
| Chronic Kidney Disease | Proteomic risk scoring | Large-scale plasma proteomics | Significantly enhanced prediction over clinical variables | Protein biomarkers improve risk stratification in diabetic populations | Large cohort validation | Ye et al. 2024 [40] |
| Diabetic Peripheral Neuropathy (DPN) | Optimized AI algorithm | Clinical + electrophysiological data | Screening capability demonstrated | Enables targeted early intervention before symptom onset | Pilot study phase | Sartore et al. 2025 [44] |
| Cardiovascular Disease | Deep Learning on ECG | 12-lead electrocardiogram + labs | AUC 0.85 | Detects silent ischemia and localizes obstructed vessels non-invasively | Retrospective validation with angiography correlation | Muzammil et al. 2024 [46]; Huang et al. 2022 [47] |
| Diabetic Retinopathy | Deep CNN | Fundus photography | Accuracy >90%, Sensitivity/Specificity match expert graders | Point-of-care autonomous screening; reduces n |
Table 3.
Challenges in AI for Diabetes and Mitigation Strategies.
| Challenge/Barrier | Description/Risks | Proposed Mitigation Strategies |
|---|---|---|
| Data heterogeneity and limited generalizability | Many AI models are developed on homogeneous, single-center or demographically narrow datasets. Without external validation, their performance may degrade in new populations. | Use multicenter datasets and external validation cohorts. Adopt domain adaptation/transfer learning techniques to adjust models to new populations. Promote federated learning across institutions to preserve data privacy while diversifying training data |
| Algorithmic bias and equity | Underrepresentation of minority, socioeconomically disadvantaged, or rare subpopulations can lead to biased predictions and unequal outcomes. | Proactively oversample or include diverse populations in training. Use fairness-aware learning or debiasing techniques. Rigorous subgroup performance reporting and audits |
| Integration and interoperability barriers | AI tools often fail to harmonize with electronic health record (EHR) systems or existing clinical workflows; clinician adoption may be hindered by usability and alert fatigue. | Develop standards-based APIs and data models (e.g. HL7 FHIR). Co-design AI interfaces with clinicians to fit workflow. Implement human-centered design and usability testing |
| Regulation, accountability and ethics | Regulatory frameworks for AI medical tools are nascent. Questions of liability, auditability, and post-market monitoring remain unresolved. | Establish audit trails and transparent performance logging. Use explainability tools and model provenance records. Engage regulators, ethicists, and stakeholders early in development |
| Patient trust, explainability and privacy | Black-box AI and concerns over data misuse reduce patient and clinician acceptance. | Integrate explainable AI (XAI) approaches to provide interpretable insights. Use privacy-enhancing technologies (e.g. differential privacy, secure aggregation). Provide clear informed consent, transparent communication |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



