Submitted:
10 October 2025
Posted:
14 October 2025
Read the latest preprint version here
Abstract
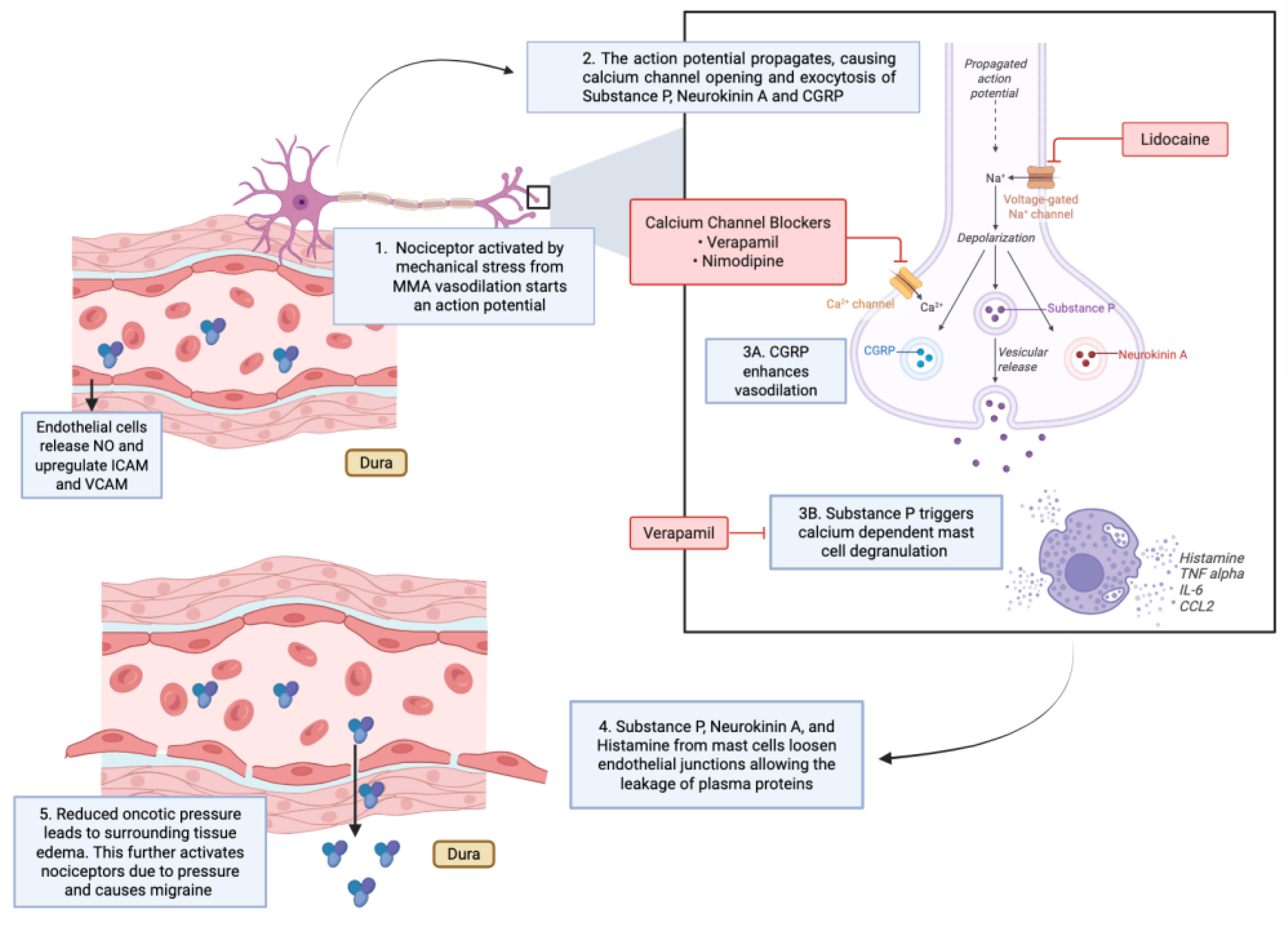
Background: The middle meningeal artery (MMA) plays a central role in migraine pathophysiology as a vascular and neuroimmune interface driving the throbbing pain. Inhibition of this cascade has been explored as a therapeutic approach, yet fewer than a dozen centers worldwide have published procedural or mechanistic data. Given the nascency of this field and the need for standardization, this review synthesizes the mechanistic and clinical evidence supporting intra-arterial pharmacologic modulation of the MMA for migraine treatment. Methods: A focused narrative review was conducted using limited but high-impact studies from pioneering groups exploring intra-arterial approaches to the MMA. Literature was arranged thematically and organized by the sites of cascade interruption and associated outcomes. Results: Since 2009, the use of intra-arterial therapies for severe headache syndromes has evolved from nimodipine for vasospasm-related headaches to verapamil for reversible cerebral vasoconstriction and, more recently, lidocaine for refractory or status migrainosus cases, sometimes with MMA embolization. Current research reframes migraines as an immunologically mediated neurovascular process, rather than purely a vascular or neuronal phenomenon. Recent studies have identified interleukins such as IL-1β, TNF-α, and IL-6 as key amplifiers of trigeminovascular activation, while emerging evidence implicates purinergic (P2X3, P2Y13) and PACAP/VIP pathways in modulating MMA excitability and neuropeptide release. Novel CGRP receptor antagonists, including zavegepant further reinforce the artery’s role as a therapeutic target. Conclusion: Our findings highlight a transition toward immune-modulating intra-arterial strategies, suggesting that future migraine therapies may increasingly focus on cytokine and neuroimmune signaling within the MMA rather than traditional vasodilatory control.
Keywords:
1. Introduction
2. Materials and Methods
3. Operative technique
4. Pharmacologic Interruption of the Cascade
6. Other Pharmacological Targets

| Vasoactive Substance | Use | Mechanism of Action (MOA) | Citations |
|---|---|---|---|
| Nimodipine (CCB) | Case use in RCVS-related vasospasm and migraine relief | Inhibits L-type calcium channels in MMA smooth muscle → reduces vasomotion and pulsatile stress; stabilizes vascular tone | Elstner et al., 2009 |
| Verapamil (non-DHP CCB) | RCVS treatment; diagnostic and therapeutic intra-arterial use for vasoconstriction-driven headaches | Smooth muscle relaxation via calcium channel blockade; modest immunomodulatory effects (↓ inflammatory signaling) | Farid et al., 2011 Ospel et al., 2020 Sequeiros et al., 2020 |
| Lidocaine | Refractory headaches, status migrainosus, SAH-related headache | Blocks voltage-gated sodium channels on trigeminal afferents → silences action potentials; prevents CGRP/substance P release; stabilizes mast cells; ↓ NF-κB signaling & cytokines; preserves endothelial junctions. | Qureshi et al., 2014; Khattar et al., 2025; Mancuso-Marcello et al., 2023; Sirakov et al., 2025; Jaikumar et al., 2025 |
| Lidocaine + MMA Embolization (Onyx, PVA, etc.) | Refractory migraine and chronic headache (combined strategy) | Combines sodium channel blockade with embolization-induced reduction of dural vascular contribution to pain | Catapano et al., 2022; Vanzin & Manzato, 2025 |
| Purinergic Receptor Modulators (P2Y13 agonists, P2 × 3 antagonists) | Experimental/preclinical migraine targets | Modulate MMA vasoreactivity and trigeminal neuropeptide release | Haanes et al., 2019 |
| VPAC1 Receptor Modulation (PACAP/VIP pathways) | Experimental/preclinical | PACAP and VIP cause vasodilation of MMA; receptor modulation may attenuate vasodilatory/mast cell-mediated pathways | Boni et al., 2009; Bhatt et al., 2013 |
| CGRP Receptor Antagonists (e.g., zavegepant) | Translational/clinical migraine therapy | Block CGRP-induced MMA dilation. | De Vries et al., 2023 |
5. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Christensen, C.E.; Younis, S.; Lindberg, U.; et al. Intradural artery dilation during experimentally induced migraine attacks. Pain 2021, 162, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Fiorella, D.; Monteith, S.J.; Hanel, R.; et al. Embolization of the middle meningeal artery for chronic subdural hematoma. N Engl J Med 2025, 392, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.M.; Knopman, J.; Mokin, M.; et al. Adjunctive middle meningeal artery embolization for subdural hematoma. N Engl J Med 2024, 391, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Elstner, M.; Linn, J.; Müller-Schunk, S.; Straube, A. Reversible cerebral vasoconstriction syndrome: a complicated clinical course treated with intra-arterial application of nimodipine. Cephalalgia 2009, 29, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Farid, H.; Tatum, J.K.; Wong, C.; et al. Reversible cerebral vasoconstriction syndrome: treatment with combined intra-arterial verapamil infusion and intracranial angioplasty. AJNR Am J Neuroradiol 2011, 32, E184–7. [Google Scholar] [CrossRef] [PubMed]
- Ospel, J.M.; Wright, C.H.; Jung, R.; et al. Intra-Arterial Verapamil Treatment in Oral Therapy-Refractory Reversible Cerebral Vasoconstriction Syndrome. AJNR Am J Neuroradiol 2020, 41, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Sequeiros, J.M.; Roa, J.A.; Sabotin, R.P.; et al. Quantifying Intra-Arterial Verapamil Response as a Diagnostic Tool for Reversible Cerebral Vasoconstriction Syndrome. AJNR Am J Neuroradiol 2020, 41, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Khattar, N.K.; Arthur, A.S.; Santori, D.; et al. Middle meningeal artery lidocaine infusion for refractory headache. J Neurointerv Surg 2025. [CrossRef] [PubMed]
- Qureshi, A.; Bains, N.; Bhatti, I.; et al. Abstract TMP6: Intra-arterial Lidocaine Administration of Lidocaine in Middle Meningeal Artery for Treatment of Subarachnoid Hemorrhage-Related Headaches. Stroke 2025;56.
- Sirakov, A.; Ninov, K.; Sirakova, K.; Sirakov, S.S. Blazing the trail! Interv Neuroradiol 2025.
- Qureshi, A.I.; Pfeiffer, K.; Babar, S.; et al. Intra-arterial injection of lidocaine into middle meningeal artery to treat intractable headaches and severe migraine. J Neuroimaging 2021, 31, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Catapano, J.S.; Karahalios, K.; Srinivasan, V.M.; et al. Chronic headaches and middle meningeal artery embolization. J Neurointerv Surg 2022, 14, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Vanzin, J.R.; Manzato, L.B. Chronic migraine and bilateral occlusion of the middle meningeal artery. Interv Neuroradiol 2025:15910199251337520.
- Jaikumar, V.; Moser, M.; Lim, J.; et al. Advanced Treatment Approach: Intra-arterial Lidocaine Injection and Middle Meningeal Artery Embolization With Onyx for Relief of Refractory Migraine: 2-Dimensional Operative Video. Oper Neurosurg (Hagerstown) 2025. [CrossRef] [PubMed]
- Mancuso-Marcello, M.; Qureshi, A.I.; Nikola, C.; et al. Intra-arterial lidocaine therapy via the middle meningeal artery for migraine headache: Theory, current practice and future directions. Interv Neuroradiol 2023:15910199231195470.
- Haanes, K.A.; Labastida-Ramírez, A.; Blixt, F.W.; et al. Exploration of purinergic receptors as potential anti-migraine targets using established pre-clinical migraine models. Cephalalgia 2019, 39, 1421–1434. [Google Scholar] [CrossRef] [PubMed]
- Boni, L.J.; Ploug, K.B.; Olesen, J.; et al. The in vivo effect of VIP, PACAP-38 and PACAP-27 and mRNA expression of their receptors in rat middle meningeal artery. Cephalalgia 2009, 29, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.K.; Gupta, S.; Olesen, J.; Jansen-Olesen, I. PACAP-38 infusion causes sustained vasodilation of the middle meningeal artery in the rat: possible involvement of mast cells. Cephalalgia 2014, 34, 877–886. [Google Scholar] [CrossRef] [PubMed]
- De Vries, T.; Boucherie, D.M.; van den Bogaerdt, A.; et al. Blocking the CGRP Receptor: Differences across Human Vascular Beds. Pharmaceuticals (Basel) 2023;16.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



