Submitted:
08 October 2025
Posted:
10 October 2025
You are already at the latest version
Abstract
Syphilis is a chronic infectious disease caused by Treponema pallidum which stands as one of the most significant imitators in clinical medicine. Its wide variety of manifestations can mimic autoimmune, inflammatory, and neoplastic disorders. Hereby we present a case of a 27-year-old male initially suspected of cutaneous T-cell lymphoma (CTCL) based on lymphadenopathy, systemic weight loss, ulcerative cutaneous lesions, and fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET-CT) findings of hypermetabolic nodes above and below the diaphragm. Histopathological analysis suggested pleomorphic lymphoid proliferation, while imaging supported the suspicion of malignancy. However, subsequent biopsies revealed plasmacytic and lymphocytic infiltration without clonality, and treponemal serologies confirmed secondary syphilis. The patient was referred for anti-treponemal therapy resulting in the resolution of the initial symptoms. This case highlights how syphilis can closely imitate hematologic malignancy, particularly CTCL, at both clinical and histopathological levels. We also review published reports of syphilis masquerading as malignancies and propose a structured diagnostic algorithm. We believe that the early inclusion of syphilis in differential diagnosis is critical to avoid misdiagnosis and appropriate treatment delays.
Keywords:
syphilis
; differential diagnosis
; malignancy
; hematologic malignancy
; lymphoma
1. Introduction
Syphilis, caused by Treponema pallidum, has long been known as “the great imitator,” owing to its complex presentations across dermatologic, neurologic, cardiovascular, and hematologic systems [1]. In its secondary stage, syphilis frequently manifests with mucocutaneous lesions and generalized lymphadenopathy, but in atypical cases, its features overlap with malignant or autoimmune diseases [2,3]. This diagnostic challenge is compounded by the nonspecificity of modern imaging, such as FDG-PET-CT, which may show hypermetabolic lymph nodes in both malignant lymphoma and reactive infections [4,5].
Unusual presentations of syphilis have been reported, including pulmonary nodules, gastric masses, cervical ulcerations, skin rash, and widespread lymphadenopathy, often leading to an initial misdiagnosis of lymphoma or carcinoma [5,6,7,8,9,10,11], as presented in Table 1. Malignant syphilis, particularly in immunocompromised individuals such as those with HIV, may histologically and clinically resemble cutaneous T-cell lymphomas (CTCL) [7].
Given its rising incidence globally, especially among at-risk populations, syphilis should remain an essential part of differential diagnoses when assessing patients with systemic symptoms, lymphadenopathy, and cutaneous lesions suspicious for malignancy [2,12]. Herein, we present a patient initially suspected of CTCL, ultimately diagnosed with secondary syphilis, provide a review of similar cases from the literature, and propose a diagnostic algorithm.
2. Case Report
A 27-year-old male suffering from ankylosing spondylitis (HLA-B27 positive) was suspected of being affected by CTCL. The initial manifestation in June 2022 included progressive right cervical lymphadenopathy with a non-healing ulceration of the overlying skin. Also, the patient experienced an unintentional weight loss of 8 kg within 1.5 months (from 80 kg to 72 kg) without night sweats or fever. Laboratory tests revealed a mild, new-onset anemia (drop of hemoglobin concentration from 16 g/dL to 12.8 g/dL (N: 14-18 g/dL) in the observation period). In September 2022, an excisional biopsy of head and neck lesions and involved skin revealed an infiltration of pleomorphic CTCL (CD3 +++,CD20 +, Ki67 + in 10% of cells, Melan A -, HMB-45 +/-, MITF -, SOX10 -). At that time, a FDG-PET-CT scan showed active proliferative disease involving lymph nodes above and below the diaphragm with cutaneous involvement. Additional tests were carried out in October 2022, including:
Biopsy of the ulcerated skin - abundant infiltration of plasmocytes and lymphocytes in the dermis proper without neoplastic lesions (Fig. 1A-D);
Bone marrow biopsy - medium-density marrow, without the presence of abnormal cells, with changes in granulocytes and platelets consistent with vitamin B12 deficiency;
Bone marrow cells flow cytometry - no evidence of abnormal clonal T-lymphocytes;
Cytogenetics - no detectable TCRβ or TCRαδ gene rearrangements;
Trephine biopsy - no presence of lymphoproliferative disease, consistent with reactive or inflammatory changes;
Testing for infectious or autoimmune diseases (negative for HBV, HCV, HIV, HSV 1/2, VZV, HTLV I/II, EBV, CMV, antinuclear, intrinsic factor and gastric parietal cell antibodies).
With these results, in March 2023, the patient was admitted to our ward in order to continue the diagnostic workup. He was in good general condition, with persistent left cervical and bilateral inguinal lymphadenopathy (lymph nodes up to 1.5 cm and 1 cm, respectively). Cutaneous involvement was present as infiltrative skin lesions including the scar after lymph node biopsy on the neck, chest, trunk, back, and scrotum, without pruritus or scaling (Figure 1E, 1F). Further testing revealed an IgG4 level within normal ranges with, however, a positive result of the Waaler-Rose, fluorescent treponemal antibody absorption (antibody titre 1/4000), treponema pallidum hemagglutination assay (antibody titre 1/10240), and venereal disease research laboratory (antibody titre 1/128) tests. Considering the positive treponema pallidum tests, and results of trephine and ulcerated skin biopsy (Figure 1A-D) suggesting the occurrence of an inflammatory process, a suspected syphilis diagnosis with skin involvement was made. The higher lymph node metabolic activity both above and below the diaphragm in the PET-CT scan from October 2022 was deemed secondary to the ongoing inflammatory process. As a consequence, in April 2023, the patient was referred to the Infectious Disease Department for treatment continuation.
4. Case Report
Syphilis continues to present significant diagnostic challenges due to its ability to mimic both hematologic and solid malignancies. In our case, the initial constellation of cervical lymphadenopathy, systemic weight loss, ulcerative cutaneous lesions, and FDG-PET-CT findings raised a strong suspicion of CTCL. Histopathology revealed pleomorphic lymphoid infiltration, while FDG-PET-CT demonstrated widespread hypermetabolic lymph nodes, further supporting this suspicion. However, repeated biopsies showed reactive plasmacytic infiltration without clonality, and subsequent treponemal serologies confirmed secondary syphilis. This illustrates the remarkable ability of syphilis to imitate lymphoma at multiple diagnostic levels [6,13].
The histopathological features of syphilitic lymphadenitis - including follicular hyperplasia, non-necrotizing granulomas, and polytypic plasma-cell infiltrates - may closely resemble those seen in lymphoma or IgG4-related disease [5,12,14]. Immunophenotyping often reveals a mixture of T- and B-lymphocytes without clear clonality, which can be interpreted as an early lymphoproliferative disorder unless molecular studies exclude it [6]. Similarly, FDG-PET-CT imaging, while highly sensitive for malignant lymphoma, lacks specificity; syphilitic lymphadenitis can demonstrate marked FDG uptake indistinguishable from aggressive lymphoma [4,5,8]. Thus, reliance solely on histology or imaging may perpetuate misdiagnosis.
Several case reports highlight this dilemma, as demonstrated in Table 1. Ohta et al. described generalized lymphadenopathy with pulmonary lesions mimicking lymphoma, ultimately diagnosed as syphilis after treponemal serology [4]. Cerchione et al. reported a patient with FDG-PET-CT hypermetabolic nodes initially misdiagnosed as lymphoma until a late syphilis diagnosis was established [6]. Yamashita et al. presented malignant syphilis in an HIV-positive patient, clinically and histologically resembling CTCL but lacking T-cell receptor clonality [7]. Other reports document gastric syphilis mimicking adenocarcinoma or lymphoma [5], skin manifestations initially diagnosed as drug eruption after antifungal therapy and primary cutaneous marginal zone lymphoma [9]. Cervical lymph node involvement with pulmonary nodules has also been misinterpreted as lymphoma [8,10].
Common diagnostic pitfalls across these cases include reliance on imaging suggestive of malignancy, nonspecific histology, and failure to consider syphilis serology early in the workup. Ultimately, serological testing, confirmatory immunohistochemistry or PCR for T. pallidum, and clinical resolution following penicillin therapy provide the final diagnostic confirmation. Our case adds to the already present scientific reports that polytypic plasma-cell infiltration without clonality and FDG-PET-CT findings of widespread hypermetabolism should always prompt consideration of syphilis, particularly in young patients or those with risk factors. Based on our expertise and on previous scientific reports, we propose a diagnostic algorithm that may be of use to clinicians in their daily clinical practice (Figure 2).
5. Conclusions
This case and reviewed literature emphasize that syphilis remains an important imitator of hematologic and non-hematologic malignancies. When patients present with lymphadenopathy, systemic symptoms, and cutaneous lesions suspicious for lymphoma, syphilis should be included early in the differential diagnosis, especially in patients at risk. Serologic testing is widely available, hence its implementation may prevent invasive diagnostics and inadequate therapies. Histopathology showing reactive plasmacytic infiltration without clonality, or a positive FDG-PET-CT with tracer uptake not proportionate to clinical presentation, should especially incline towards considering syphilis. A multidisciplinary approach is essential to avoid delays in diagnosis and, eventually, reduce patient morbidity. Ultimately, systematic inclusion of syphilis in diagnostic workups can avert misdiagnosis and unnecessary treatment, underscoring its relevance as “the great imitator” in modern hematology and internal medicine [1,2,12].
Author Contributions
Conceptualization, U.G., J.D., J.K.; methodology, U.G., J.D., J.K.; investigation, U.G.; software, K.Z., Z.D.; data curation, U.G., Z.D.; writing— U.G; original draft preparation, U.G.; writing—review and editing, U.G., J.D.; supervision, J.D., M.M-D., J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This manuscript received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to local regulations: case reports are not required to be approved by local ethical committee if they describe standard diagnostic and therapeutical procedures. Our cases were diagnosed and treated according to internationally and locally approved standards.
Informed Consent Statement
Informed consent was obtained from the patient involved in the study. Written informed consent has also been obtained from the subject to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FDG-PET-CT | Fluorodeoxyglucose positron emission tomography–computed tomography |
| CTCL | Cutaneous T-cell lymphoma |
| HIV | Human immunodeficiency virus |
| FNAC | Fine needle aspiration cytology |
| CE-CT | Contrast-enhanced computed tomography |
| RPR | Rapid plasma reagin test |
| TPHA | Treponema pallidum hemagglutination assay |
| STD | Sexually transmitted diseases |
| CBC | Complete blood count |
| ESR | Erythrocyte sedimentation rate |
| CRP | C-reactive protein |
| HBV | Hepatitis B virus |
| HCV | Hepatitis C virus |
| VDRL | Venereal Disease Research Laboratory test |
| FTA-Abs | Fluorescent treponemal antibody absorption test |
| CT | Computed tomography |
| PCR | Polymerase chain reaction |
References
- Hook, E.W., 3rd; Marra, C.M. Acquired Syphilis in Adults. N. Engl. J. Med. 1992, 326, 1060–1069. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, K.G.; Ram, S.; Rice, P.A. The Modern Epidemic of Syphilis. N. Engl. J. Med. 2020, 382, 845–854. [Google Scholar] [CrossRef] [PubMed]
- French, P. Syphilis. BMJ 2007, 334, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Ohta, A.; Furusyo, N.; Kishihara, Y.; Eiraku, K.; Murata, M.; Kainuma, M.; Toyoda, K.; Ogawa, E.; Hayashi, T.; Koga, T. Secondary Syphilis with Pulmonary Involvement. Intern. Med. 2018, 57, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.-M.; Yang, S.-W.; Dai, M.-G.; Ye, B.; He, F.-Y. Gastric Syphilis Mimicking Gastric Cancer: A Case Report. World J. Clin. Cases 2021, 9, 7798–7804. [Google Scholar] [CrossRef] [PubMed]
- Cerchione, C.; Maraolo, A.E.; Marano, L.; Pugliese, N.; Nappi, D.; Tosone, G.; Cimmino, I.; Cozzolino, I.; Martinelli, V.; Pane, F.; et al. Secondary Syphilis Mimicking Malignancy: A Case Report and Review of Literature. J. Infect. Chemother. 2017, 23, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Fujii, Y.; Ozaki, K.; Urano, Y.; Iwasa, M.; Nakamura, S.; Fujii, S.; Abe, M.; Sato, Y.; Yoshino, T. Human Immunodeficiency Virus-Positive Secondary Syphilis Mimicking Cutaneous T-Cell Lymphoma. Diagn. Pathol. 2015, 10, 185. [Google Scholar] [CrossRef] [PubMed]
- Maci, C.; Canetti, D.; Tassan Din, C.; Bruzzesi, E.; Lucente, M.F.; Badalucco Ciotta, F.; Candela, C.; Ponzoni, M.; Castagna, A.; Nozza, S. Malignant Syphilis Mimicking Lymphoma in HIV: A Challenging Case and a Review of Literature Focusing on the Role of HIV and Syphilis Coinfection. Microorganisms 2025, 13, 968. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.; Prieto, V.; Cho, W.C.; Torres-Cabala, C.; Lenskaya, V. (virtual) the Misleading Syphilis: Two Cases Masquerading as Lymphomas. In Proceedings of the ASDP 61st Annual Meeting; ASDP Proceedings, November 4 2024.
- Komeno, Y.; Ota, Y.; Koibuchi, T.; Imai, Y.; Iihara, K.; Ryu, T. Secondary Syphilis with Tonsillar and Cervical Lymphadenopathy and a Pulmonary Lesion Mimicking Malignant Lymphoma. Am. J. Case Rep. 2018, 19, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Hodak, E.; David, M.; Rothem, A.; Bialowance, M.; Sandbank, M. Nodular Secondary Syphilis Mimicking Cutaneous Lymphoreticular Process. J. Am. Acad. Dermatol. 1987, 17, 914–917. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.E.; Romanowski, B. Syphilis: Review with Emphasis on Clinical, Epidemiologic, and Some Biologic Features. Clin. Microbiol. Rev. 1999, 12, 187–209. [Google Scholar] [CrossRef] [PubMed]
- Ohta, M. Secondary Syphilis with Generalized Lymphadenopathy and Pulmonary Involvement Mimicking Lymphoma. Intern Med 2019, 58, 1813–1816. [Google Scholar]
- Bledsoe, J.R.; Della-Torre, E.; Rovati, L.; Deshpande, V. IgG4-Related Disease: Review of the Histopathologic Features, Differential Diagnosis, and Therapeutic Approach. APMIS 2018, 126, 459–476. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Histopathological examination of the ulcerated skin from October 2022 (A-D; HE x20, x40, x200, x400, respectively). Histologically skin lesions presented as ulcerated tumors, composed mostly of ill-defined non-necrotizing granulomas and numerous mature plasma cells, which were polytypic on kappa/lambda immunohistochemistry. Mature lymphocytes, predominantly T-cells, were relatively sparse. There were some dispersed immunoblasts. Diagnosis of reactive, inflammatory lesions was rendered with suggestion of infectious disease. Ulceration in the right submandibular space in the scar after biopsy (E). Disseminated lesions on the skin of the chest and abdomen (F).
Figure 1.
Histopathological examination of the ulcerated skin from October 2022 (A-D; HE x20, x40, x200, x400, respectively). Histologically skin lesions presented as ulcerated tumors, composed mostly of ill-defined non-necrotizing granulomas and numerous mature plasma cells, which were polytypic on kappa/lambda immunohistochemistry. Mature lymphocytes, predominantly T-cells, were relatively sparse. There were some dispersed immunoblasts. Diagnosis of reactive, inflammatory lesions was rendered with suggestion of infectious disease. Ulceration in the right submandibular space in the scar after biopsy (E). Disseminated lesions on the skin of the chest and abdomen (F).
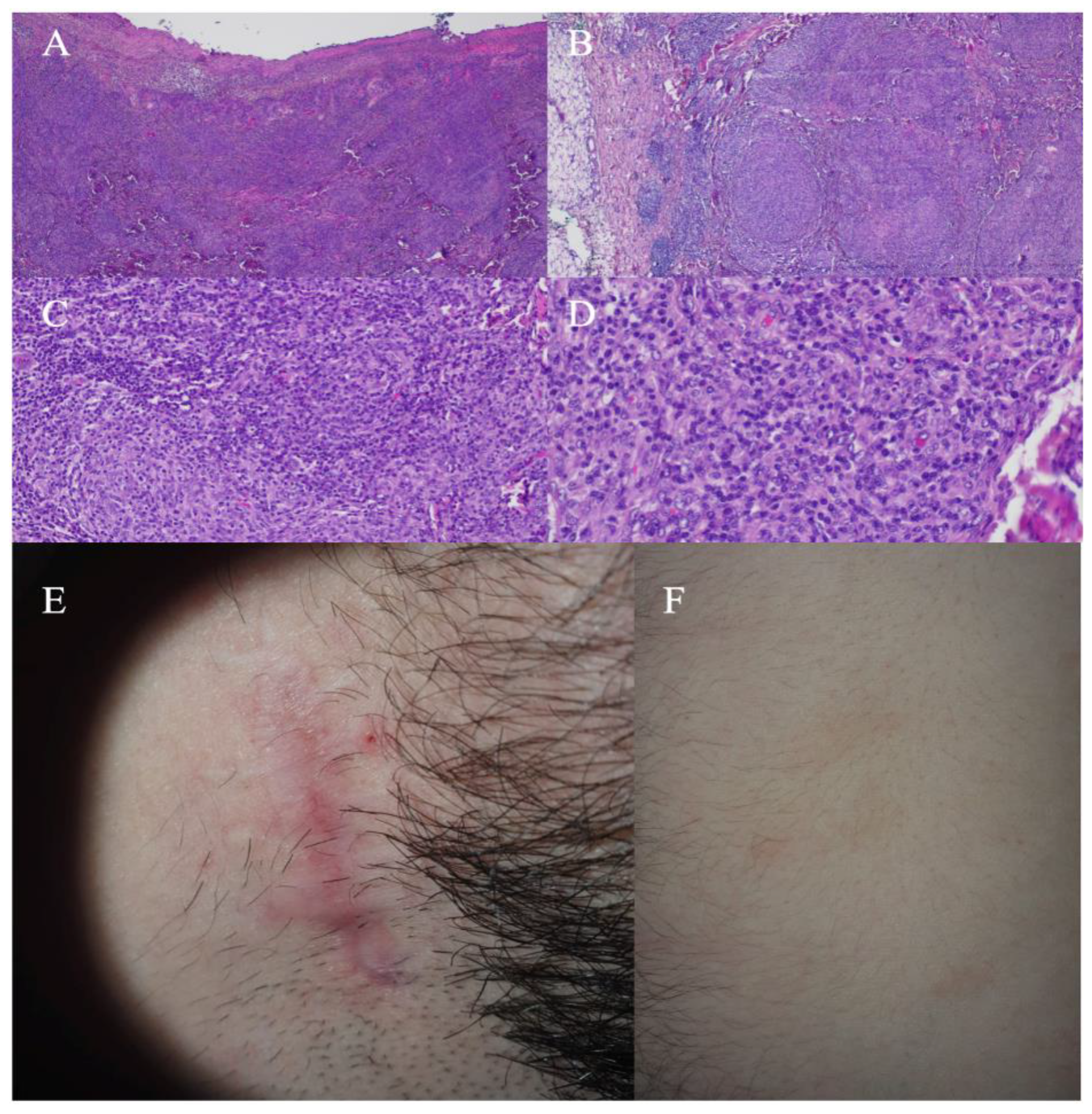
Figure 2.
Proposed diagnostic workup of syphilis. Abbreviations: STD - sexually transmitted diseases; CBC complete blood count; ESR - erythrocyte sedimentation rate; CRP - C-reactive protein; HIV - human immunodeficiency virus; HBV - hepatitis B virus; HCV - hepatitis C virus; RPR - rapid plasma reagin test; VDRL - Venereal Disease Research Laboratory test; FTA-Abs - fluorescent treponemal antibody absorption; TPHA - Treponema pallidum hemagglutination assay; CT - computed tomography, FDG-PET-CT fluorodeoxyglucose positron emission tomography combined with computed tomography; PCR - polymerase chain reaction.
Figure 2.
Proposed diagnostic workup of syphilis. Abbreviations: STD - sexually transmitted diseases; CBC complete blood count; ESR - erythrocyte sedimentation rate; CRP - C-reactive protein; HIV - human immunodeficiency virus; HBV - hepatitis B virus; HCV - hepatitis C virus; RPR - rapid plasma reagin test; VDRL - Venereal Disease Research Laboratory test; FTA-Abs - fluorescent treponemal antibody absorption; TPHA - Treponema pallidum hemagglutination assay; CT - computed tomography, FDG-PET-CT fluorodeoxyglucose positron emission tomography combined with computed tomography; PCR - polymerase chain reaction.
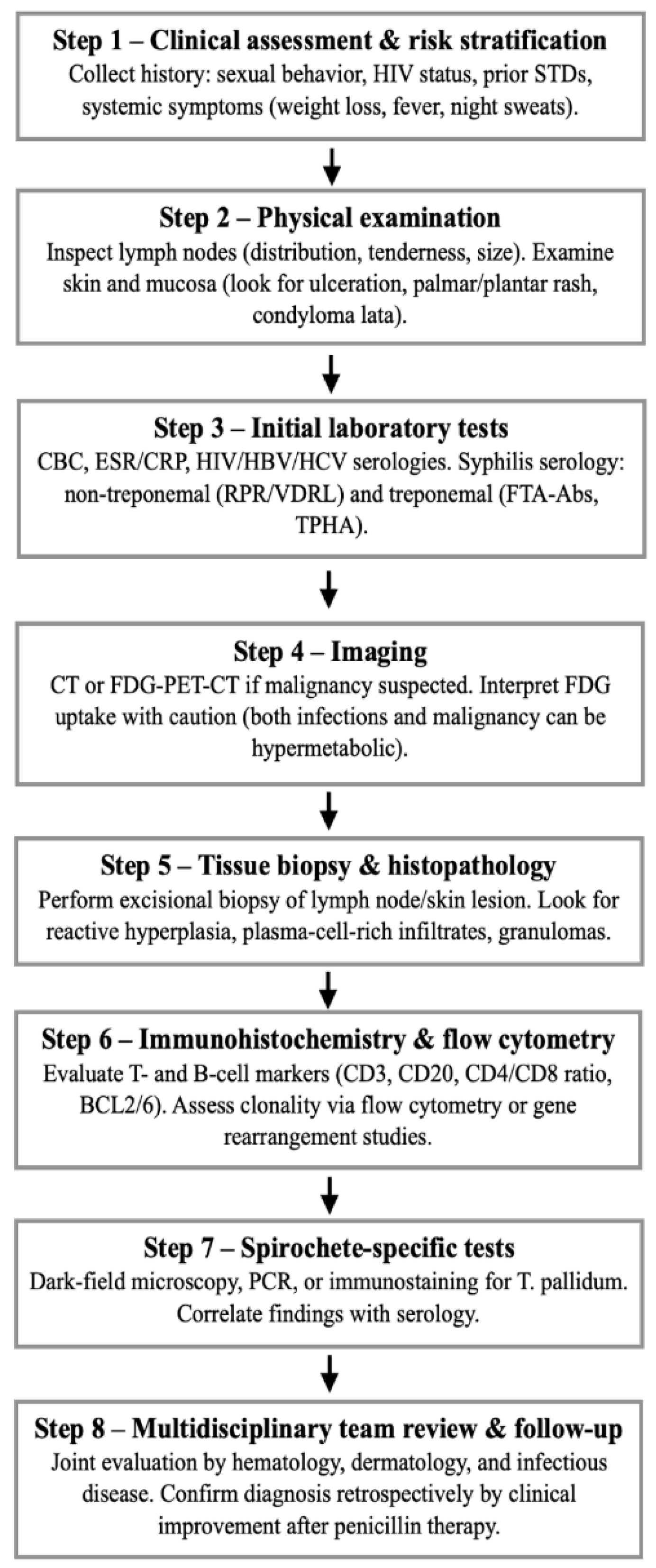

Table 1.
Reported cases of syphilis misdiagnosed as hematologic or non-hematologic malignancies. Abbreviations: FDG-PET-CT - fluorodeoxyglucose positron emission tomography-computed tomography; CTCL - cutaneous T-cell lymphoma; HIV - human immunodeficiency virus; FNAC - fine needle aspiration cytology; CE-CT - contrast-enhanced computed tomography; RPR - rapid plasma reagin test; TPHA - treponema pallidum hemagglutination assay.
Table 1.
Reported cases of syphilis misdiagnosed as hematologic or non-hematologic malignancies. Abbreviations: FDG-PET-CT - fluorodeoxyglucose positron emission tomography-computed tomography; CTCL - cutaneous T-cell lymphoma; HIV - human immunodeficiency virus; FNAC - fine needle aspiration cytology; CE-CT - contrast-enhanced computed tomography; RPR - rapid plasma reagin test; TPHA - treponema pallidum hemagglutination assay.
| First author (Year) | Clinical presentation | Initial suspected diagnosis | Diagnostic pitfall | Final clue leading to syphilis diagnosis |
|---|---|---|---|---|
| Ohta et al. (2018) [4] | Chest pain, rash, stomatitis, generalized lymphadenopathy, pulmonary nodules | Metastatic lung cancer / lymphoma | FDG-PET-CT uptake in mediastinal/axillary nodes and lung nodules, nonspecific lymph node biopsy | Positive RPR/TPHA serology, resolution with antibiotics, contracted lung nodular shadows following treatment |
| Cerchione et al. (2017) [6] | Generalized lymphadenopathy, fever, weight loss, rash, hepatomegaly, splenomegaly, nocturnal sweating | Non-Hodgkin lymphoma | FDG-PET-CT hypermetabolic nodes, FNAC showing reactive hyperplasia, delayed rash misinterpreted as viral exanthema, negative flow cytometry assay for B/T cell clonality | Treponemal serology positive after repeated testing, regression with penicillin, high-risk sexual intercourse |
| Yamashita et al. (2015) [7] | HIV positivity, ulcerated skin lesions, fever, headache, and myalgia without lymphadenopathy |
CTCL | Histology resembling CTCL with only CD8+ T-cell infiltrates | Negative TCR rearrangement, positive treponemal tests, detection of spirochetes |
| Lan et al. (2021) [5] | Epigastric pain, weight loss, endoscopic gastric mass | Gastric adenocarcinoma or lymphoma | Endoscopy and biopsy showing antral gastric ulcer with gastric retention, CE-CT and FDG-PET-CT suggesting gastric cancer |
Immunohistochemistry for Treponema pallidum, positive serology, promiscuous partner, histopathology negative for cancer cells |
| Salah et al. (2024) – Case 1 [9] | Generalized erythematous plaques | Primary cutaneous marginal zone lymphoma | Skin biopsy - lymphocytic infiltrate with CD3+T-cells and CD20+ B-cells, B-cells positive for BCL2 and BCL6. Predominance of kappapositive plasma cells |
Positive syphilis serology, immunohistochemical study showing spirochetes, negative flow cytometry |
| Salah et al. (2024) – Case 2 [9] | Severe gastritis and esophageal candidiasis followed by disseminated eruption | Drug eruption after antifungal therapy |
Biopsy -lymphocytic infiltrate with atypical CD3+, CD8+, TCRbetaF1+ CD7 + T-cells, immunoreactivity for TIA-1 and granzyme B |
Unremarkable bone marrow biopsy and flow cytometry, immunohistochemical study showing spirochetes, positive syphilis serology |
| Hodak et al. (1987) [11] | Cutaneous eruption with plasma cell infiltrate | Cutaneous lymphoma | Histology suggested lymphoma; histological reactive pattern | Serologic tests positive for syphilis, dark-field microscopy demonstrating spirochetes in a nodular lesion, clinical resolution after penicillin |
| Komeno et al. (2018) [10] | Bilateral cervical lymphadenopathy, pulmonary nodule, periportal lymph node |
Malignant lymphoma | Histology of lymph nodes with adipose tissue with fibrosis, infiltration by lymphocytes with mildly expanded nuclei | Treponemal serology positive, clinical resolution after penicillin, history of oral sex with partners |
| Maci et al. (2025) [8] | HIV positivity under antiretroviral therapy, five-day history of fever and multiple lymphadenopathies, lung consolidation |
Hematologic malignancy | Lymph node biopsy revealing disrupted architecture with multiple granulomas multinucleated giant cells, negative anti-treponema immunoreaction |
Serological tests, clinical resolution after penicillin, regression of the lung consolidation by FDG-PET-CT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



