Submitted:
05 October 2025
Posted:
06 October 2025
You are already at the latest version
Abstract
Background/objectives: High-quality pediatric critical care includes supporting children nearing the end-of-life (EOL) and their families. Cataloging existing interventions for children dying in the pediatric intensive care unit (PICU) establishes critical areas for future research. In this scoping review, we evaluated characteristics of PICU EOL in-terventions. Methods: A librarian guided a search of OVID Medline, CINAHL, OVID PsycINFO, OVID Embase, Cochrane Central, and Web of Science, plus backwards and forwards reference searching. We included interprofessional interventions, defined as any sys-tematic change (e.g., educational programs, symptom management, electronic medical record, etc.), for children dying from any cause. Studies were independently screened by two reviewers. Data were extracted by one team member and reviewed by a second. We extracted intervention elements, contextual factors, and implementation barri-ers/facilitators and generated frequencies from qualitative coding. Results: Of 11,643 screened articles; 44 met inclusion criteria. Most were in neonatal ICUs (28/44, 64%) and general PICUs (10/44, 23%). Most interventions aimed to improve cli-nician knowledge (25/44; 57%), augment clinical structures and processes (11/44; 25%), or enhance communication (N=8/44; 18%). Common delivery methods included clinical practice changes (N=25/44; 57%; e.g. protocols, order sets [N=12]) and educational sessions (N=20/44; 45%). Outcomes included clinician knowledge (N=17/44; 39%), qualitative feedback (N=18/44; 41%), feasibility/acceptability (N=12/44; 27%), or treatment utilization (N=11/44; 25%). Few examined families’ mental health (N=3; 7%) or bereavement (N=2; 5%). Few reported implementation facilitators or barriers. Conclusions: Most included studies targeted clinician outcomes through education. De-signing, testing, and implementing interventions focused on family outcomes is a critical next step.
Keywords:
pediatric critical care
; interdisciplinary
; end-of-life care
; palliative care
1. Introduction
A child’s death is life-altering, leading to life-long grief for their families [1,2,3,4,5,6,7]. Many children and families navigate the terminal phases of an illness or injury in the pediatric intensive care unit (PICU) [8,9,10]. A multidisciplinary, team-based approach is crucial to addressing end-of-life needs in the PICU, including tending to a child’s symptoms, family spiritual and emotional needs, and meaning-making opportunities [7,11,12]. Parents who self-report feeling unprepared for end-of-life (EOL) more frequently perceive EOL suffering, or experience decisional regret and decreased social functioning [13,14,15]. As the clinicians most frequently at the bedside, nurses are well-positioned to support and prepare families for EOL. Interprofessional EOL care that fully leverages nurses’ roles is therefore critical to supporting patients and families.
To date, studies of family and clinician experiences illuminate several gaps in PICU EOL care that exacerbate parental distress [16,17,18,19]. These include fragmented communication, strained relationships within and between clinical teams and families, and limited structural support for families and clinicians, among others [16,17,18,19]. Generally low pediatric mortality rates mean that clinicians may rarely apply palliative and EOL skills learned during pre-licensure training, instead learning on the job. Thus, there is a pressing need for supportive EOL interventions that can be readily integrated into routine PICU care to address these known barriers to high-quality EOL care.
Although EOL care interventions are increasingly common, systematic evaluations of their components — including who, how, and when interventions are delivered and implemented — remain lacking. Systematically cataloging existing interventions is necessary to ensure all dying children in the PICU receive compassionate, evidence-based care from well-trained clinicians. We therefore conducted a scoping review to evaluate interventions for children nearing EOL in the PICU.
2. Materials and Methods
2.1. Design
This scoping review [20] followed Arksey and O’Malley’s method [21] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22]. The review protocol was registered on Open Science Foundation (https://doi.org/10.17605/OSF.IO/7ST2E). The following research question guided the review: How are pediatric EOL interventions designed and delivered, who delivers and receives them, what outcomes do they aim to effect, and what factors facilitate or inhibit their implementation?
2.2. Search Strategy
A medical librarian (JB) and the first author (EGBA) developed a search strategy that was peer-reviewed by another medical librarian (Supplement 1). Electronic databases included Ovid MEDLINE(R) ALL, OVID APA PsycINFO, OVID Embase, CINAHL, Cochrane Central, and Web of Science. Search terms included both controlled vocabulary and synonymous free text to capture these concepts: population (children with life-threatening conditions), care settings (intensive care units) and interventions (intervention, education, training, etc.). We used citationchaser [23] to identify additional articles using backward and forward reference searching.
2.3. Selection Criteria
To capture interprofessional interventions, articles with the search terms in the title, abstract, or subheadings and the word “nurse” within the full text were included. We included reports of empirically evaluated interventions designed to support EOL care for children (i.e., last days of life) dying from any cause in any intensive care setting (e.g., neonatal, pediatric, and cardiac). We sought to include interventions that meaningfully involved nurses in their implementation and impact. We defined intervention broadly as any practice change focused on bedside EOL care (e.g., educational programs, symptom management, communication training, order sets, electronic medical record modifications, etc.). Eligible articles formally evaluated the interventions using quantitative, qualitative, or mixed methods, with outcomes reported by patients, families, or clinicians. We included all research designs and quality improvement efforts.
To capture as many interventions as possible, we made no exclusions based on publication year, location, or language. We translated articles published in languages other than English using Google translate [24] or ChatGPT (OpenAI) if needed. Studies were included if they reported results specific to ICU populations or if > 50% of patients died in the ICU. Studies not explicitly focused on the EOL period were included only if >50% of patients died during the study period. We excluded reviews, opinion articles, dissertations, and editorials. Articles describing practice changes without formal evaluation were excluded.
2.4. Screening and Data Management
Search results were uploaded and deduplicated in EndNote (version 20 – Thompson Reutres) then uploaded into COVIDENCE systematic review software (Veritas Health Information) [25]. Two reviewers from a team of four authors (EGBA, NO, SEW, IJEU) independently screened study titles and abstracts. Discrepancies were resolved by a third reviewer from the team of four. Full texts studies that met criteria were reviewed using the same process and team.
2.5. Data Extraction and Quality Appraisal
We developed and pilot tested a standardized data extraction form in REDCap [26,27]. Three authors (EGBA, NO, or SEW) independently extracted article information and reviewed extracted data, with discrepancies resolved through discussion. We extracted intervention elements, contextual factors, and implementation barriers and facilitators (Supplement 2). Intervention elements (Figure 1: Box 1) included development processes, goal or intended impact, delivery methods, interventionists and recipients of the intervention, and outcome measures (quantitative metrics and qualitative questions). Contextual factors included sample characteristics, ICU type (neonatal, general PICU, cardiac PICU), and hospital characteristics. Unit- and hospital-level intervention implementation facilitators and barriers were based on the Consolidated Framework for Implementation Research [28]. We extracted palliative care focus — physical, psychological, spiritual/existential, and/or social [29]. We evaluated methodological rigor using the Mixed Methods Appraisal Tool (MMAT; Supplement 3) [30]; we did not evaluate quality improvement, program evaluation, or implementation project rigor given their small number and heterogeneous designs.
2.6. Analysis:
Quantitative data were summarized in STATA [31] using frequencies for categorical and means/medians for continuous variables. For qualitative data, the coding team (EGBA, NO, SW, IJEU) generated descriptive categories from extracted free text about intervention elements and implementation barriers and facilitators,[28,32] then collaboratively coded 10% of articles in Dedoose [33] before proceeding independently with all coding verified by the first author (EGB). Code frequencies describing intervention elements and implementation barriers and facilitators were generated. Categories were not mutually exclusive and thus do not sum to 100% in reporting.
To assess if interventions targeted parent priorities, we mapped intervention goals and outcomes to parent-identified gaps in EOL care. Based on two systematic reviews of parent PICU EOL experiences and one qualitative study of bereaved parents recommendations for PICU EOL care [16,19,34], we identified seven parent-identified gaps from these three articles: communication and information sharing, comfort and symptom management, family psychosocial and spiritual care, structural support (e.g., visitation policies), meaning making (e.g., memento-making), grief and bereavement care, and parental role acknowledgement and empowerment. Among the total sample of articles in our review, we tabulated the number addressing each of these gaps and intervention goals/outcomes.
3. Results
We screened 11,643 articles, assessed 286 full texts for eligibility; and 44 met inclusion criteria (Figure 2). Most research teams used non-randomized quantitative (17/44, 39%) or quantitative descriptive designs (12/44, 27%); see Table 1. The neonatal ICU was the most common site (28/44, 64%) followed by general PICU (10/44, 23%). Four (9%) studies were conducted in pediatric cardiac ICUs. Most interventions focused on multiple palliative care domains (38/44, 86%).
3.1. Intervention Elements
Here we summarize intervention elements, contextual factors, implementation facilitators and barriers, and study rigor. Appendix 3: Table of Evidence contains study details and all citations.
Development: Eleven of 44 (25%) interventions were developed from prior evidence (e.g., based on prior research, adapted existing interventions) and 5 (11%) were informed by clinical experience. Eighteen interventions (41%) engaged key partners (e.g., clinicians) in study development; three (7%) involved family members. For example, Zhang et al. engaged bereaved parents to develop a protocol for transferring infants to a specified NICU room with parent sleeping space [35]. Development processes were not explicitly reported in 21/44 (48%) articles.
Goals: Most (25/44; 57%) interventions focused on improving clinician knowledge or comfort with EOL care. Eleven (25%) interventions focused on improving clinical structures and processes. For example, Younge et al. integrated a palliative care protocol, order set, nursing care plan, and comfort medication guidelines into NICU EOL care [36]. Eight (18%) interventions aimed to enhance communication within clinical teams and with families, by increasing regular case discussions [37] or bereavement debriefings for families [38]. Six interventions (14%) integrated palliative care into the PICU; two (5%) supported decision-making, [39,40] such as through meetings about discontinuation of life-sustaining treatments [40]. Nine (20%) interventions focused on staff debriefing. Interventions addressing patient and family experiences (12/44; 27%) included symptom management (N=5; 11%), [36,41,42,43,44] memento-making activities (N=4; 9%), [35,45,46,47] and support for parents (N=3; 7%) [35,48,49].
Delivery: Most interventions were delivered through clinical practice changes (25/44; 57%). These included protocols/pathways (N=12; 27%), team/family meeting processes/structures (N=9; 20%), order set or medication administration instructions (N=4; 9%),[36,41,42] electronic health records (N=2; 5%),[50,51] or environmental modifications (N=4; 9%) [35,48,49,52]. For example, Carter et al. incorporated EOL content into NICU morbidity and mortality conferences [53]. Other delivery methods included educational sessions (20/44; 45%) and simulations (N=6; 14%). Ten of 44 (23%) interventions used reflective debriefings, such as peer support [54], emotional debriefing sessions for staff [52,55,56,57,58,59] or follow-up meetings with families [38,60]. Some interventions (7/44; 16%) were delivered by preparing specific personnel (e.g., champions, palliative care teams).
Timing and frequency of interventions: Some interventions were integrated (N=20/44; 45%) or separate (N=24/44; 54%) from clinical processes. Four of 44 (9%) interventions occurred once (e.g., singular memory-making experience) [35,45,46,47], and 16 (36%) repeated changes within the practice setting, (e.g., medication administration over the last days of a child’s life) [41]. Eleven (25%) interventions occurred once outside clinical practice (e.g., a one-time simulation) [61] and thirteen (30%) included multiple events outside clinical practice (e.g., simulations throughout PICU fellowship) [62]. Four interventions (9%) included post-mortem processes (e.g., a reflective debriefing, family bereavement meeting) [38,58,59,60].
Interventionists: About a quarter (24%) of interventionists included multiple disciplines (e.g., medicine, nursing, social work), and 5 (12%) used ICU-based teams. Three (7%) had nurse interventionists [41,48,63] and 2 (5%) interventionist teams included parents (Table 1) who completed intervention procedures such as photography [47] and educational content [64].
Subspecialty palliative care: Thirteen (39%) studies explicitly involved subspecialty palliative care in intervention development or delivery. In two (5%), no palliative care team was available [65,66], while three (7%) mentioned palliative care teams that were not part of the study [44,49,57]. Nineteen (43%) did not reference palliative care team involvement.
Summary of outcomes: Clinician knowledge, attitudes, or beliefs about palliative and EOL care practices were evaluated in 17/44 (39%) studies. Eighteen (41%) studies examined qualitative feedback. Twelve (27%) studies evaluated treatment utilization metrics (e.g., mechanical ventilation at time of death) [39]; twelve evaluated feasibility/acceptability (27%). Four (9%) evaluated medication use [36,42,43,65]. Five (11%) projects evaluated goals of care documentation or meetings [36,40,51,65,67], and/or patient symptoms/experience [41,42,43,44,67]. Three (7%) studies evaluated clinician mental health (e.g., burnout), [54,56,59] and three (7%) evaluated family mental health [35,39,44]. Two (5%) studies examined parent bereavement (e.g., meaning making [38], grief experience [52]).
Mapping to parent-identified gaps: Parent-identified gaps with the most corresponding interventions (Figure 3) were communication and information sharing (14 interventions) and comfort/symptom management (11 interventions). Six interventions addressed family psychosocial and spiritual support, through integrating palliative care or improving clinical processes like psychosocial consultations. These were evaluated using treatment utilization metrics (N=3) [35,51,68], or patient/family experience, (e.g., parent depression/anxiety (N=2)) [35,44]. Five interventions addressed structural support for parents through clinical structures/processes, addressing family experience (e.g., specific spaces for EOL) [35,49,52], or enhancing communication (e.g., increasing family conferences) [52]. Structural interventions evaluated family outcomes, treatment utilization metrics, and/or qualitative data.
Four interventions supported meaning making through memento-making activities which were evaluated qualitatively [45,46,47,48]. Four interventions included grief and bereavement care, through integrating palliative care (N=2) [39,69], supporting decision making (N=1) [39], improving clinical structures (N=1) [67], and/or enhancing communication. [52] For example, Morillo Palma et al.’s palliative care protocol included systematic bereavement follow-up for families. [67] Two interventions [35,48] helped support parental role empowerment by improving clinical structures and processes and addressing patient and family clinical experience, evaluated through family mental health outcomes and qualitative feedback. Specifically, Kymre et al. evaluated nurse-facilitated parent skin-to-skin opportunities for dying neonates. [48]
3.2. Contextual Factors
Most studies (25/44; 57%) were conducted in academic institutions. Thirteen (30%) were in freestanding children’s hospitals and 6/44 (14%) in community or government hospitals. Six of 44 studies (14%) described multisite approaches.
3.3. Implementation Barriers and Facilitators
Unit-level implementation facilitators included high volume (12/44; 27%); existing family-centered, palliative, or EOL care infrastructure (8/44; 18%); invested individuals (8/44; 18%); and staff enthusiasm (2/44; 5%) [44,57]. Unit-level implementation barriers included technology or procedural issues (10/44; 23%); scheduling (10/44; 23%); lack of palliative or EOL care infrastructure (3/44; 7%); [61,70,71] and individual hesitations (2/44; 5%) [41,60]. For example, nurses who used an oral or transmucosal comfort medication protocol in Drolet et al.’s study reported discomfort interrupting families’ privacy [41].
Hospital-level implementation facilitators included committed intervention champions (7/44; 16%), support for required time/resources (4/44; 9%) [59,68,70,72], established hospital EOL, palliative, or bereavement programming (7/44; 16%). Barriers included lack of programming (4/44; 9%) [50,65,69,70]. Many studies (26/44; 59%) did not report about hospital-level implementation factors.
3.4. Study Rigor
Common threats to rigor included potential selection or sampling bias (Appendix 3: MMAT Results). Many studies (15/44; 34%) did not report sample demographic data. Most studies utilized a quasi-experimental design, often without a control group, introducing the potential for confounding.
4. Discussion
This scoping review cataloged EOL care intervention elements and implementation considerations in neonatal and pediatric ICUs. Most interventions aimed to improve clinician knowledge about palliative and EOL care through educational programming or improved clinical processes (e.g., team meeting procedures or assessment protocols). Few studies examined family outcomes. Parent-identified gaps of communication and comfort/symptom management were addressed by >10 interventions, whereas just two interventions addressed parental role empowerment. Implementation facilitators included structural factors like established palliative or bereavement programs. Barriers often included scheduling or operational challenges. These findings highlight common strategies used to enhance EOL care in the PICU and illuminate critical areas for future research and family engagement.
Most interventions relied on educational sessions, simulations, or protocols to improve clinicians’ knowledge about palliative and EOL care. Educational interventions tailored to the PICU are critical to upholding quality EOL care since most pre-licensure EOL care education focuses on non-pediatric populations, and pediatric ICU mortality is low, meaning clinicians may not receive much on-the-job PICU EOL training [73,74,75,76]. The impact of educational interventions depends on successful integration into complex clinical workflows [77,78,79]. Yet, many studies did not routinely consider implementation facilitators or barriers, which may limit interventions scalability or integration into clinical care [77,78].
Mapping intervention goals and outcomes to EOL care gaps reported by parents [16,19,34] revealed important future priorities. Many parents recount issues with how information was shared during their child’s terminal hospitalization [16,19,34]. We identified fourteen studies focused on improving information sharing during clinical care, through integrating palliative care, supporting decision making, improving clinical structures, and enhancing communication. However, outcomes were mostly clinician perspectives or medical record data, rather than family reports. Few interventions focused on enhancing parental role empowerment, [35,48] despite perceived importance by bereaved parents [34,80]. Prior qualitative findings retrospectively articulate how clinicians can effectively partner with parents during serious illness [81] and EOL care [4,12,80]. However, prospectively operationalizing and implementing family role empowerment during the uncertainty of PICU EOL care is complex and warrants careful design and evaluation of family-driven interventions.
Many studies support early palliative care during a child’s serious illness [82,83]. However, few studies in our sample included subspecialty pediatric palliative care in the development, design, or implementation of intervention studies. Fostering research collaborations between PICU and palliative care teams to develop and test family-centered interventions may be a critical step to strengthen the evidence base for PICU EOL care. While 41% of intervention teams included nurses, only 3 (%) studies evaluated nurse-led interventions, and most interventions did not impact routine nursing practice. Given nurses’ uniquely close involvement with children and families during EOL, future interventions should consider leveraging nursing workflows to enhance EOL care.
Limitations of Included Studies
Most screened articles were excluded for describing EOL care without implementing an intervention. No randomized trials met our inclusion criteria; most studies used quantitative non-randomized or descriptive designs, often without control groups or detailed demographic data. These study features limit generalizability or transferability to other populations outside the study context. While randomized controlled trials may be challenging to conduct during intensive EOL care, alternative designs, such as pragmatic trials, cluster and hybrid effectiveness trials, or causal approaches such as interrupted time series analysis may be feasible [78,84]. Additionally, few studies engaged families in intervention design or study procedures.
Strengths and Limitations of Review
This scoping review followed a comprehensive, peer-reviewed search strategy and rigorous methodological standards. However, our findings should be interpreted considering several limitations. Publication bias limits our analysis to interventions that have been evaluated and reported in published literature. The search terms we used were comprehensive and corresponded with leading causes of mortality but may not have captured all causes of death. We limited our sample to interventions conducted in PICUs and NICUs using interprofessional interventions and contained the word nurse in the report. Intervention studies conducted in other settings, such as pediatric oncology, or that did not use an interprofessional approach, could have applicable elements. We limited our focus to last days of life; studies focused on earlier serious illness communication, advanced care planning, or shared decision making could be informative to designing EOL interventions. Although assessing intervention effects was outside of the scope of this review, future studies should aim to analyze outcomes to inform evidence-based EOL practice.
5. Conclusions
Empirically evaluated EOL interventions in pediatric and neonatal intensive care units are scarce. Most published EOL care intervention studies focus on improving clinician knowledge of palliative and EOL care using educational approaches or clinical practice changes evaluated with pre-post designs. Few interventions target parent-reported gaps in EOL care, especially parental role empowerment, include families in intervention development, use designs that account for selection bias or confounding factors, or consider implementation barriers/facilitators. These are important areas of future research to strengthen EOL care.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplement: Search strategy, Extraction form, Table of Evidence, Mixed Methods Appraisal Tool Results.
Author Contributions
EGBA: 1) study conceptualization, 2) data acquisition, analysis, interpretation, 3) manuscript original draft and edits, 4) accountable for manuscript. NO: 1) study conceptualization, 2) data acquisition, analysis, interpretation, 3) manuscript original draft and edits, 4) accountable for manuscript. SW: 1) study conceptualization, 2) data acquisition, analysis, interpretation, 3) manuscript original draft and edits, 4) accountable for manuscript. IJEU: 1) study conceptualization, 2) data acquisition, analysis, interpretation, 3) manuscript original draft and edits, 4) accountable for manuscript. JB: 1) study conceptualization, 2) data acquisition, 3) manuscript edits, 4) accountable for manuscript. DKC: 1) study conceptualization, 2) manuscript edits, 3) accountable for manuscript. SF: 1) study conceptualization, 2) data interpretation, 3) manuscript edits, 4) accountable for manuscript. JS: 1) study conceptualization, 2) data interpretation, 3) manuscript edits, 4) accountable for manuscript
Funding
Dr. Broden Arciprete was supported by NIH 5T32HS017589 and by CTSA Grant Number TL1 TR001864.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
Authors would like to thank Tom Mead and Vermetha Polite from the Cushing/Whitney Medical Library at Yale University School of Medicine for peer reviewing the search strategy and providing technical support, respectively.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PICU | Pediatric Intensive Care Unit |
| EOL | End-of-life |
| ICU | Intensive care unit |
| NICU | Neonatal intensive care unit |
References
- Wheeler, I. Parental Bereavement: The Crisis of Meaning. Death Studies 2001, 25, 51–66. [CrossRef]
- Klass, D. Parental Grief: Solace and Resolution; Springer Publishing Company, 1988; ISBN 978-0-8261-5930-4.
- Snaman, J.M.; Morris, S.E.; Rosenberg, A.R.; Holder, R.; Baker, J.; Wolfe, J. Reconsidering Early Parental Grief Following the Death of a Child from Cancer: A New Framework for Future Research and Bereavement Support. Support Care Cancer 2020, 28, 4131–4139. [CrossRef]
- Broden, E.G.; Werner-Lin, A.; Curley, M.A.Q.; Hinds, P.S. Shifting and Intersecting Needs: Parents’ Experiences During and Following the Withdrawal of Life Sustaining Treatments in the PICU. Intensive & Critical Care Nursing 2021, (in review. [CrossRef]
- Davies, R. New Understandings of Parental Grief: Literature Review. Journal of Advanced Nursing 2004, 46, 506–513. [CrossRef]
- Lannen, P.K.; Wolfe, J.; Prigerson, H.G.; Onelov, E.; Kreicbergs, U.C. Unresolved Grief in a National Sample of Bereaved Parents: Impaired Mental and Physical Health 4 to 9 Years Later. Journal of Clinical Oncology 2008, 26, 5870. [CrossRef]
- Meert, K.L.; Briller, S.; Schim, S.M.; Thurston, C.; Kabel, A. Examining the Needs of Bereaved Parents in the Pediatric Intensive Care Unit: A Qualitative Study. Death Studies 2009, 33, 712–740. [CrossRef]
- Moynihan, K.M.; Alexander, P.M.A.; Schlapbach, L.J.; Millar, J.; Jacobe, S.; Ravindranathan, H.; Croston, E.J.; Staffa, S.J.; Burns, J.P.; Gelbart, B.; et al. Epidemiology of Childhood Death in Australian and New Zealand Intensive Care Units. Intensive Care Med 2019, 45, 1262–1271. [CrossRef]
- Burns JP; Sellers DE; Meyer EC; Lewis-Newby M; Truog RD Epidemiology of Death in the PICU at Five U.S. Teaching Hospitals*. Crit Care Med 2014, 42, 2101–2108. [CrossRef]
- Moynihan, K.M.; Lelkes, E.; Kumar, R.K.; DeCourcey, D.D. Is This as Good as It Gets? Implications of an Asymptotic Mortality Decline and Approaching the Nadir in Pediatric Intensive Care. European Journal of Pediatrics 2021. [CrossRef]
- Butler, A.E.; Hall, H.; Copnell, B. The Changing Nature of Relationships between Parents and Healthcare Providers When a Child Dies in the Paediatric Intensive Care Unit. J Adv Nurs 2018, 74, 89–99. [CrossRef]
- Brooten, D.; Youngblut, J.M.; Seagrave, L.; Caicedo, C.; Hawthorne, D.; Hidalgo, I.; Roche, R. Parent’s Perceptions of Health Care Providers Actions around Child ICU Death: What Helped, What Did Not. The American Journal of Hospice & Palliative Care 2013, 30, 40–49. [CrossRef]
- Broden, E.G.; Mazzola, E.; DeCourcey, D.D.; Blume, E.D.; Wolfe, J.; Snaman, J.M. The Roles of Preparation, Location, and Palliative Care Involvement in Parent-Perceived Child Suffering at the End of Life. Journal of Pediatric Nursing 2023. [CrossRef]
- Wiener, L.; Tager, J.; Mack, J.; Battles, H.; Bedoya, S.Z.; Gerhardt, C.A. Helping Parents Prepare for Their Child’s End of Life: A Retrospective Survey of Cancer-Bereaved Parents. Pediatric Blood and Cancer 2020, 67. [CrossRef]
- Feifer, D.; Broden, E.G.; Xiong, N.; Mazzola, E.; Baker, J.N.; Wolfe, J.; Snaman, J.M. Mixed-Methods Analysis of Decisional Regret in Parents Following a Child’s Death from Cancer. Pediatric Blood & Cancer 2023, n/a, e30541. [CrossRef]
- Adistie, F.; Neilson, S.; Shaw, K.L.; Bay, B.; Efstathiou, N. The Elements of End-of-Life Care Provision in Paediatric Intensive Care Units: A Systematic Integrative Review. BMC Palliative Care 2024, 23, 184. [CrossRef]
- Mu, P.-F.; Tseng, Y.-M.; Wang, C.-C.; Chen, Y.-J.; Huang, S.-H.; Hsu, T.-F.; Florczak, K.L. Nurses’ Experiences in End-of-Life Care in the PICU: A Qualitative Systematic Review. Nurs Sci Q 2019, 32, 12–22. [CrossRef]
- Barrett, L.; Fraser, L.; Noyes, J.; Taylor, J.; Hackett, J. Understanding Parent Experiences of End-of-Life Care for Children: A Systematic Review and Qualitative Evidence Synthesis. Palliat Med 2023, 37, 178–202. [CrossRef]
- Tezuka, S.; Kobayashi, K. Parental Experience of Child Death in the Paediatric Intensive Care Unit: A Scoping Review. BMJ Open 2021, 11, e057489. [CrossRef]
- Toh, T.S.W.; Lee, J.H. Statistical Note: Using Scoping and Systematic Reviews. Pediatric Critical Care Medicine 2021, 22, 572. [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. International Journal of Social Research Methodology 2005, 8, 19–32. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [CrossRef]
- Haddaway, N.R.; Grainger, M.J.; Gray, C.T. Citationchaser: An R Package and Shiny App for Forward and Backward Citations Chasing in Academic Searching 2021.
- Jackson, J.L.; Kuriyama, A.; Anton, A.; Choi, A.; Fournier, J.-P.; Geier, A.-K.; Jacquerioz, F.; Kogan, D.; Scholcoff, C.; Sun, R. The Accuracy of Google Translate for Abstracting Data From Non–English-Language Trials for Systematic Reviews. Ann Intern Med 2019, 171, 677–679. [CrossRef]
- Covidence - Better Systematic Review Management Available online: https://www.covidence.org/ (accessed on 5 March 2025).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. Journal of Biomedical Informatics 2019, 95, 103208. [CrossRef]
- Harris, P.; Taylor, R.; R, T.; Payne, J.; Gonzalez, N.; Conde, J. Research Electronic Data Capture (REDCap) – A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. Journal of Biomedical Informatics 2009, 42, 377–381. [CrossRef]
- Damschroder, L.J.; Reardon, C.M.; Opra Widerquist, M.A.; Lowery, J. Conceptualizing Outcomes for Use with the Consolidated Framework for Implementation Research (CFIR): The CFIR Outcomes Addendum. Implementation Science 2022, 17, 7. [CrossRef]
- Saunders, C. Care of Patients Suffering from Terminal Illness. Nursing Mirror 1964.
- Hong, Q.; Pluye, P.; Fabregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool; McGill, 2018;
- Stata Statistical Software: Release 17 2021.
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering Implementation of Health Services Research Findings into Practice: A Consolidated Framework for Advancing Implementation Science. Implementation Sci 2009, 4, 50. [CrossRef]
- Dedoose Available online: https://www.dedoose.com/?gad_source=1&gclid=CjwKCAiAm-67BhBlEiwAEVftNqFH47mAqW8sT8QxIw-3DjbgoymUQpW2tedyXZuy09LVGGjecoyTVxoCyEgQAvD_BwE (accessed on 6 January 2025).
- Butler, A.E.; Copnell, B.; Hall, H. When a Child Dies in the PICU: Practice Recommendations From a Qualitative Study of Bereaved Parents. Pediatr Crit Care Med 2019, 20, e447–e451. [CrossRef]
- Zhang, R.; Tang, Q.; Zhu, L.H.; Peng, X.M.; Zhang, N.; Xiong, Y.E.; Chen, M.H.; Chen, K.L.; Luo, D.; Li, X.; et al. Testing a Family Supportive End of Life Care Intervention in a Chinese Neonatal Intensive Care Unit: A Quasi-Experimental Study With a Non-Randomized Controlled Trial Design. Frontiers in Pediatrics 2022, 10, 870382. [CrossRef]
- Younge, N.; Smith, P.B.; Goldberg, R.N.; Brandon, D.H.; Simmons, C.; Cotten, C.M.; Bidegain, M. Impact of a Palliative Care Program on End-of-Life Care in a Neonatal Intensive Care Unit. Journal of Perinatology 2015, 35, 218–222. [CrossRef]
- Allen, J.D.; Shukla, R.; Baker, R.; Slaven, J.E.; Moody, K. Improving Neonatal Intensive Care Unit Providers’ Perceptions of Palliative Care through a Weekly Case-Based Discussion. Palliative Medicine Reports 2021, 2, 93–100. [CrossRef]
- Meert, K.L.; Eggly, S.; Kavanaugh, K.; Berg, R.A.; Wessel, D.L.; Newth, C.J.L.; Shanley, T.P.; Harrison, R.; Dalton, H.; Michael Dean, J.; et al. Meaning Making during Parent-Physician Bereavement Meetings after a Child’s Death. Health psychology 2015, 34, 453–461. [CrossRef]
- Kwon, J.E.; Kim, Y.H. Changes in the End-of-Life Process in Patients with Life-Limiting Diseases through the Intervention of the Pediatric Palliative Care Team. Journal of Clinical Medicine 2023, 12, 6588. [CrossRef]
- Cremer, R.; Binoche, A.; Noizet, O.; Fourier, C.; Leteurtre, S.; Moutel, G.; Leclerc, F. Are the GFRUP’s Recommendations for Withholding or Withdrawing Treatments in Critically Ill Children Applicable? Results of a Two-Year Survey. Journal of Medical Ethics 2007, 33, 128–133. [CrossRef]
- Drolet, C.; Roy, H.; Laflamme, J.; Marcotte, M.-E. Feasibility of a Comfort Care Protocol Using Oral Transmucosal Medication Delivery in a Palliative Neonatal Population. Journal of Palliative Medicine 2016, 19, 442–450. [CrossRef]
- Burns, J.; Jackson, K.; Sheehy, K.A.; Finkel, J.C.; Quezado, Z.M. The Use of Dexmedetomidine in Pediatric Palliative Care: A Preliminary Study. Journal of Palliative Medicine 2017, 20, 779–783. [CrossRef]
- Tripathi, S.; Laksana, E.; McCrory, M.C.; Hsu, S.; Zhou, A.X.; Burkiewicz, K.; Ledbetter, D.R.; Aczon, M.D.; Shah, S.; Siegel, L.; et al. Analgesia and Sedation at Terminal Extubation: A Secondary Analysis from Death One Hour after Terminal Extubation Study Data*. Pediatric Critical Care Medicine 2023, 24, 463–472. [CrossRef]
- Parry, S.M.; Staenberg, B.; Weaver, M.S. Mindful Movement: Tai Chi, Gentle Yoga, and Qi Gong for Hospitalized Pediatric Palliative Care Patients and Family Members. Journal of Palliative Medicine 2018, 21, 1212–1213. [CrossRef]
- Andrews, E.; Hayes, A.; Cerulli, L.; Miller, E.G.; Slamon, N. Legacy Building in Pediatric End-of-Life Care through Innovative Use of a Digital Stethoscope. Palliative Medicine Reports 2020, 1, 149–155. [CrossRef]
- Akard, T.F.; Duffy, M.; Hord, A.; Randall, A.; Sanders, A.; Adelstein, K.; Anani, U.E.; Gilmer, M.J. Bereaved Mothers’ and Fathers’ Perceptions of a Legacy Intervention for Parents of Infants in the NICU. J Neonatal Perinatal Med 2018, 11, 21–28. [CrossRef]
- Martel, S.L.; Ives-Baine, L. “Most Prized Possessions”: Photography as Living Relationships Within the End-of-Life Care of Newborns. Illness, Crisis & Loss 2014, 22, 311–332. [CrossRef]
- Kymre, I.G.; Bondas, T. Skin-to-Skin Care for Dying Preterm Newborns and Their Parents - A Phenomenological Study from the Perspective of NICU Nurses. Scandinavian Journal of Caring Sciences 2013, 27, 669–676. [CrossRef]
- Vesely, C.; Newman, V.; Winters, Y.; Flori, H. Bringing Home to the Hospital: Development of the Reflection Room and Provider Perspectives. Journal of Palliative Medicine 2017, 20, 120–126. [CrossRef]
- Czynski, A.J.; Souza, M.; Lechner, B.E. The Mother Baby Comfort Care Pathway: The Development of a Rooming-In-Based Perinatal Palliative Care Program. Advances in neonatal care : official journal of the National Association of Neonatal Nurses 2022, 22, 119–124. [CrossRef]
- Casas, J.; Jeppesen, A.; Peters, L.; Schuelke, T.; Magdoza, N.R.K.; Hesselgrave, J.; Loftis, L. Using Quality Improvement Science to Create a Navigator in the Electronic Health Record for the Consolidation of Patient Information Surrounding Pediatric End-of-Life Care. Journal of Pain and Symptom Management 2021, 62, E218–E224. [CrossRef]
- Harmon, R.J.; Glicken, A.D.; Siegel, R.R. Neonatal Loss in the Intensive Care Nursery. Effects of Maternal Grieving and a Program for Intervention. Journal of the American Academy of Child Psychiatry 1984, 23, 68–71. [CrossRef]
- Carter, B.S.; Guthrie, S.O. Utility of Morbidity and Mortality Conference in End-of-Life Education in the Neonatal Intensive Care Unit. Journal of Palliative Medicine 2007, 10, 375–380. [CrossRef]
- Kang, H.J.; Bang, K.S. Development and Evaluation of a Self-Reflection Program for Intensive Care Unit Nurses Who Have Experienced the Death of Pediatric Patients. Journal of Korean Academy of Nursing 2017, 47, 392–405. [CrossRef]
- Rushton, C.H.; Reder, E.; Hall, B.; Comello, K.; Sellers, D.E.; Hutton, N. Interdisciplinary Interventions to Improve Pediatric Palliative Care and Reduce Health Care Professional Suffering. Journal of Palliative Medicine 2006, 9, 922–933. [CrossRef]
- Delgado-Corcoran, C.; Wawrzynski, S.E.; Mansfield, K.; Fuchs, E.; Yeates, C.; Flaherty, B.F.; Harousseau, M.; Cook, L.; Epps, J.V. Grieving Children’ Death in an Intensive Care Unit: Implementation of a Standardized Process. Journal of palliative medicine 2023, 27, 236-NA. [CrossRef]
- Woolgar, F.; Archibald, S.-J. An Exploration of Neonatal Intensive Care Unit (NICU) Staff Experiences of Attending Pre-Brief and Debrief Groups Surrounding a Patient’s Death or Redirection of Care. Journal of Neonatal Nursing 2021, 27, 352–357. [CrossRef]
- Bateman, S.T.; Dixon, R.; Trozzi, M. The Wrap-up: A Unique Forum to Support Pediatric Residents When Faced with the Death of a Child. Journal of Palliative Medicine 2012, 15, 1329–1334. [CrossRef]
- Hawes, K.; Goldstein, J.; Vessella, S.; Tucker, R.; Lechner, B.E. Providing Support for Neonatal Intensive Care Unit Health Care Professionals: A Bereavement Debriefing Program. American Journal of Perinatology 2022, 39, 401–408. [CrossRef]
- Clarke, P.; Booth, D. Copying Medical Summaries on Deceased Infants to Bereaved Parents. Acta Paediatrica, International Journal of Paediatrics 2011, 100, 1262–1266. [CrossRef]
- Williams, B.K.; Pendergrass, T.L.; Grooms, T.R.; Florez, A.R. End of Life Simulation in a Pediatric Cardiac Intensive Care Unit. Clinical Simulation in Nursing 2021, 60, 3–10. [CrossRef]
- Brock, K.E.; Tracewski, M.; Allen, K.E.; Klick, J.; Petrillo, T.; Hebbar, K.B. Simulation-Based Palliative Care Communication for Pediatric Critical Care Fellows. Am J Hosp Palliat Care 2019, 36, 820–830. [CrossRef]
- Nesbit, M.J.; Hill, M.; Peterson, N. A Comprehensive Pediatric Bereavement Program: The Patterns of Your Life. Critical Care Nursing Quarterly 1997, 20, 48–62. [CrossRef]
- Scheurer, J.M.; Norbie, E.; Bye, J.K.; Villacis-Calderon, D.; Heith, C.; Woll, A.; Shu, D.; McManimon, K.; Kamrath, H.; Goloff, N. Pediatric End-of-Life Care Skills Workshop: A Novel, Deliberate Practice Approach. Academic Pediatrics 2023, 23, 860–865. [CrossRef]
- Samsel, C.; Lechner, B.E. End-of-Life Care in a Regional Level IV Neonatal Intensive Care Unit after Implementation of a Palliative Care Initiative. Journal of Perinatology 2015, 35, 223–228. [CrossRef]
- Haut, C.M.; Michael, M.; Moloney-Harmon, P. Implementing a Program to Improve Pediatric and Pediatric ICU Nurses’ Knowledge of and Attitudes Toward Palliative Care. Journal of Hospice & Palliative Nursing 2012, 14, 71–79. [CrossRef]
- Morillo Palomo, A.; Clotet Caba, J.; Camprubi Camprubi, M.; Blanco Diez, E.; Silla Gil, J.; Riverola de Veciana, A. Implementing Palliative Care, Based on Family-Centered Care, in a Highly Complex Neonatal Unit. Jornal de Pediatria 2023. [CrossRef]
- Wolff, T.; Dorsett, C.; Connolly, A.; Kelly, N.; Turnbull, J.; Deorukhkar, A.; Clements, H.; Griffin, H.; Chhaochharia, A.; Haynes, S.; et al. Chameleon Project: A Children’s End-of-Life Care Quality Improvement Project. Bmj Open Quality 2021, 10, 9. [CrossRef]
- Ishak Tayoob, M.; Rayala, S.; Doherty, M.; Singh, H.B.; Alimelu, M.; Lingaldinna, S.; Palat, G. Palliative Care for Newborns in India: Patterns of Care in a Neonatal Palliative Care Program at a Tertiary Government Children’s Hospital. Health services insights 2024, 17, 11786329231222858-NA. [CrossRef]
- Abuhammad, S.; Almasri, R. Impact of Educational Programs on Nurses’ Knowledge and Attitude toward Pediatric Palliative Care. Palliative & Supportive Care 2022, 20, 397–406. [CrossRef]
- Harris, L.L.; Placencia, F.X.; Arnold, J.L.; Minard, C.G.; Harris, T.B.; Haidet, P.M. A Structured End-of-Life Curriculum for Neonatal-Perinatal Postdoctoral Fellows. The American journal of hospice & palliative care 2015, 32, 253–261. [CrossRef]
- Asuncion, A.M.; Cagande, C.; Schlagle, S.; McCarty, B.; Hunter, K.; Milcarek, B.; Staman, G.; Da Silva, S.; Fisher, D.; Graessle, W. A Curriculum to Improve Residents’ End-of-Life Communication and Pain Management Skills During Pediatrics Intensive Care Rotation: Pilot Study. Journal of graduate medical education 2013, 5, 510–513. [CrossRef]
- Shorey, S.; Chua, C. Nurses and Nursing Students’ Experiences on Pediatric End-of-Life Care and Death: A Qualitative Systematic Review. Nurse Education Today 2022, 112, 105332. [CrossRef]
- Lyons, K.A.; Middleton, A.A.; Farley, A.A.; Henderson, N.E.; Peterson, E.B. End-of-Life Care Education in Pediatric Critical Care Medicine Fellowship Programs: Exploring Fellow and Program Director Perspectives. J Palliat Med 2023, 26, 1217–1224. [CrossRef]
- Hirani, R.; Khuram, H.; Elahi, A.; Maddox, P.A.; Pandit, M.; Issani, A.; Etienne, M. The Need for Improved End-of-Life Care Medical Education: Causes, Consequences, and Strategies for Enhancement and Integration. Am J Hosp Palliat Care 2024, 41, 5–7. [CrossRef]
- Li, J.; Smothers, A.; Fang, W.; Borland, M. Undergraduate Nursing Students’ Perception of End-of-Life Care Education Placement in the Nursing Curriculum. J Hosp Palliat Nurs 2019, 21, E12–E18. [CrossRef]
- Woods-Hill, C.Z.; Wolfe, H.; Malone, S.; Steffen, K.M.; Agulnik, A.; Flaherty, B.F.; Barbaro, R.P.; Dewan, M.; Kudchadkar, S. Implementation Science Research in Pediatric Critical Care Medicine. Pediatr Crit Care Med 2023, 24, 943–951. [CrossRef]
- Ista, E.; van Dijk, M. Moving Away From Randomized Controlled Trials to Hybrid... : Pediatric Critical Care Medicine.
- Steffen, K.M.; Holdsworth, L.M.; Ford, M.A.; Lee, G.M.; Asch, S.M.; Proctor, E.K. Implementation of Clinical Practice Changes in the PICU: A Qualitative Study Using and Refining the iPARIHS Framework. Implementation Science 2021, 16, 15. [CrossRef]
- Butler, A.E.; Hall, H.; Copnell, B. Becoming a Team: The Nature of the Parent-Healthcare Provider Relationship When a Child Is Dying in the Pediatric Intensive Care Unit. Journal of Pediatric Nursing: Nursing Care of Children and Families 2018, 40, e26–e32. [CrossRef]
- Barratt, M.; Bail, K.; Lewis, P.; Paterson, C. Nurse Experiences of Partnership Nursing When Caring for Children with Long-Term Conditions and Their Families: A Qualitative Systematic Review. Journal of Clinical Nursing 2024, 33, 932–950. [CrossRef]
- Short, S.R.; Thienprayoon, R. Pediatric Palliative Care in the Intensive Care Unit and Questions of Quality: A Review of the Determinants and Mechanisms of High-Quality Palliative Care in the Pediatric Intensive Care Unit (PICU). Transl Pediatr 2018, 7, 326–343. [CrossRef]
- Boss, R.; Nelson, J.; Weissman, D.; Campbell, M.; Curtis, R.; Frontera, J.; Gabriel, M.; Lustbader, D.; Mosenthal, A.; Mulkerin, C.; et al. Integrating Palliative Care into the PICU: A Report from the Improving Palliative Care in the ICU Advisory Board. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies 2014, 15, 762–767. [CrossRef]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The Stepped Wedge Cluster Randomised Trial: Rationale, Design, Analysis, and Reporting. BMJ 2015, 350, h391. [CrossRef]
Figure 1.
Extracted intervention elements. Alt text: A text box containing definitions of intervention elements.
Figure 1.
Extracted intervention elements. Alt text: A text box containing definitions of intervention elements.
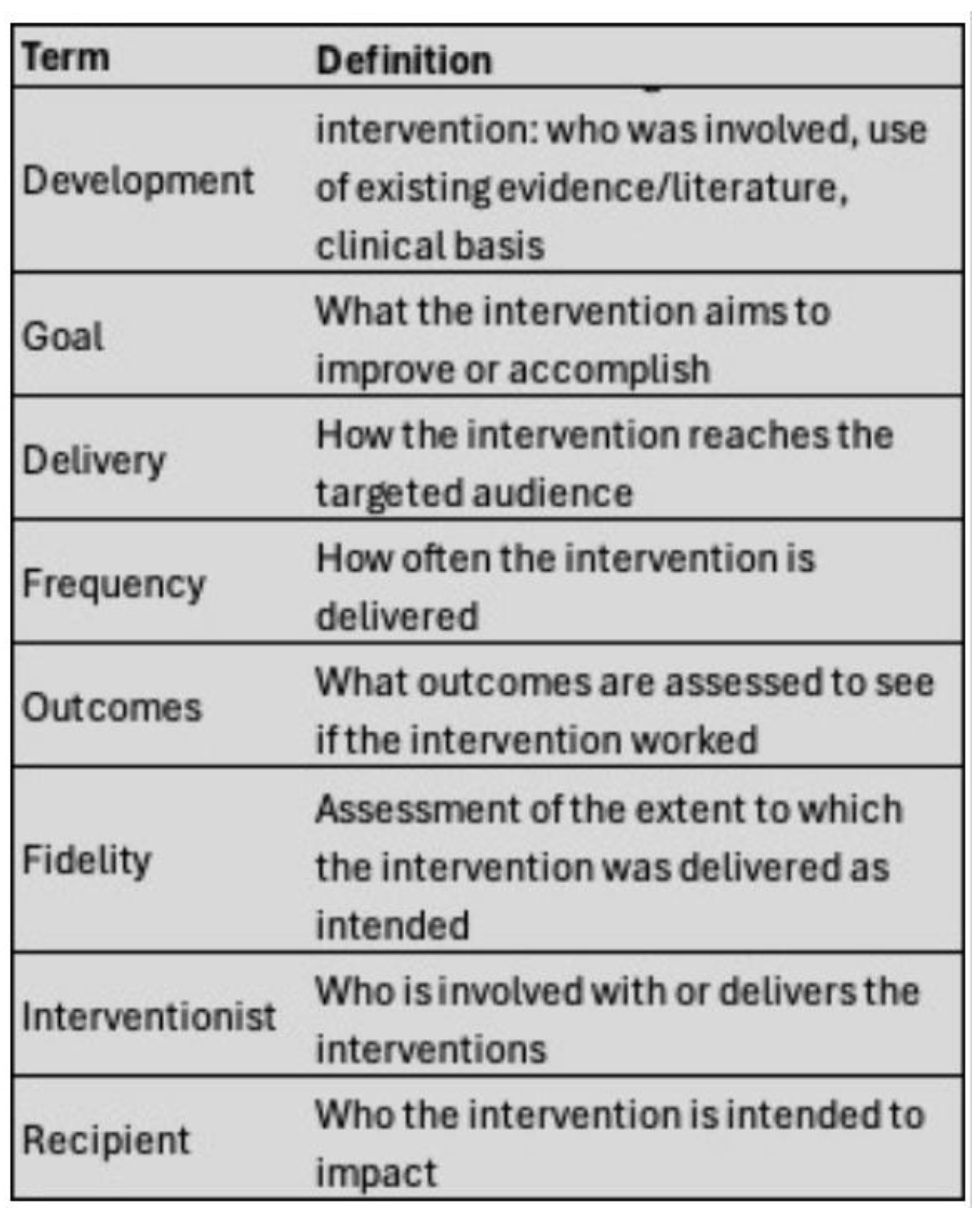
Figure 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flowchart. Alt text: A flowchart of review screening and study selection procedures.
Figure 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flowchart. Alt text: A flowchart of review screening and study selection procedures.
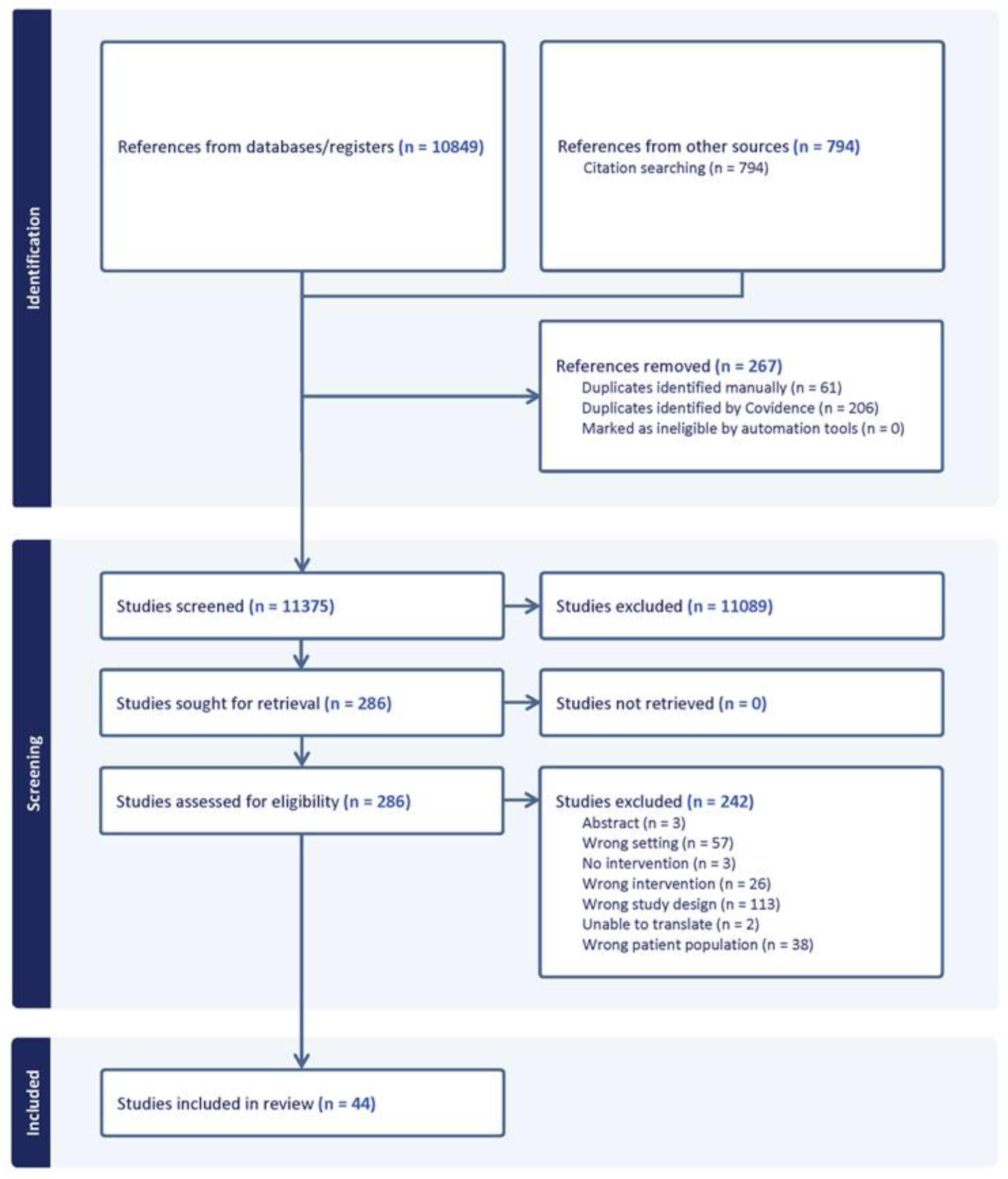
Figure 3.
Heat Map of Intervention Goals and Outcomes vs. Parent Identified Gaps in End-of-Life Care. Alt text: Heat map showing how often different intervention types addressed parent-identified gaps in pediatric end-of-life care. Green indicates more studies addressing a gap with a modality; red indicates fewer.
Figure 3.
Heat Map of Intervention Goals and Outcomes vs. Parent Identified Gaps in End-of-Life Care. Alt text: Heat map showing how often different intervention types addressed parent-identified gaps in pediatric end-of-life care. Green indicates more studies addressing a gap with a modality; red indicates fewer.
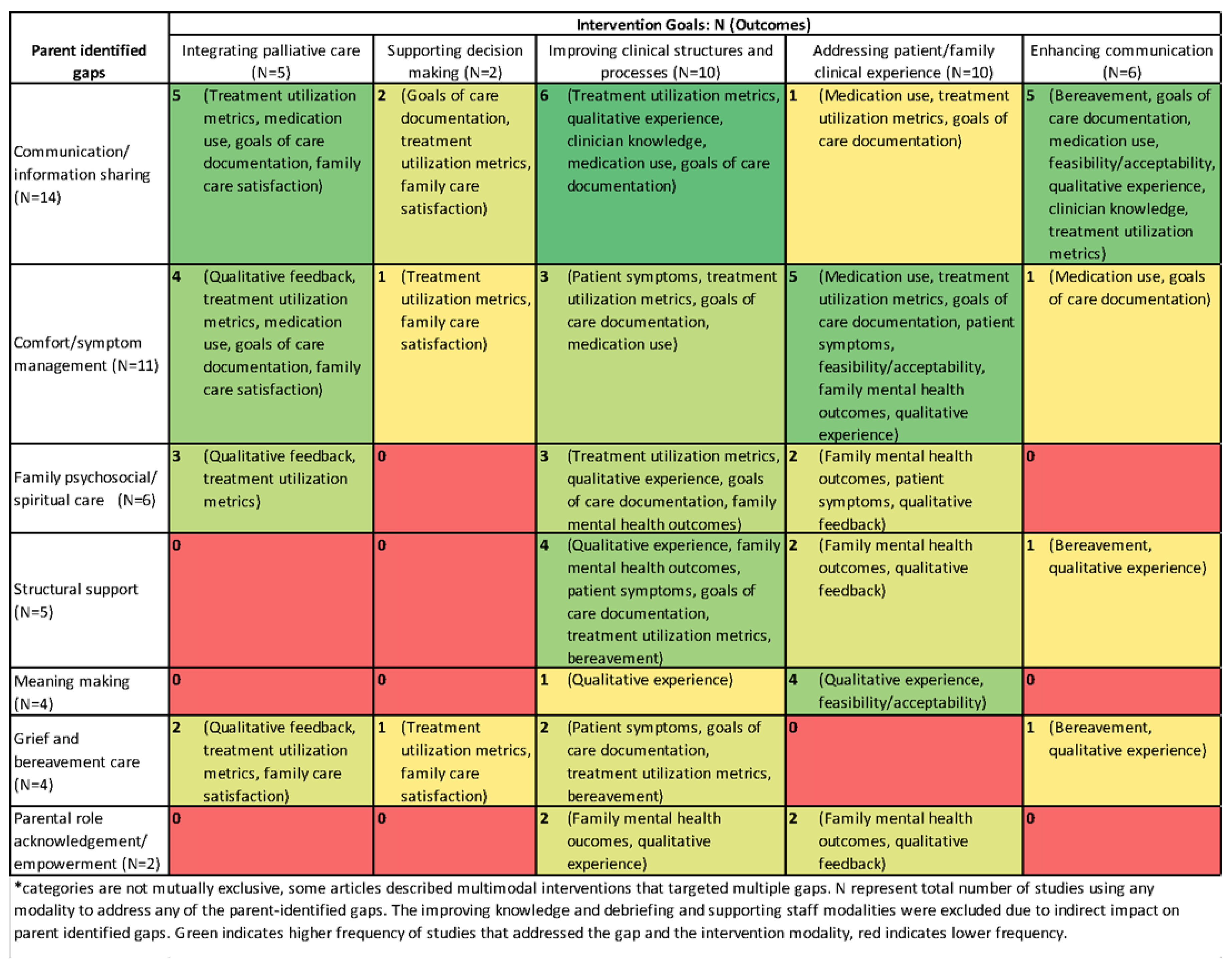

Table 1.
Aggregate Study Characteristics.
| Category | Variable | N (%) |
|---|---|---|
| Total | 44 | |
| Study design | Mixed Methods | 3 (7%) |
| Other1 | 8 (18%) | |
| Qualitative | 4 (9%) | |
| Quantitative descriptive | 12 (27%) | |
| Quantitative non-randomized | 17 (39%) | |
| Unit type2 | General PICU | 10 (23%) |
| PCICU | 4 (9%) | |
| NICU | 28 (64%) | |
| Other unit type | 2 (5%) | |
| Palliative care domains* | Physical | 34 (77%) |
| Physical alone | 5 (11%) | |
| Emotional/psychological | 38 (86%) | |
| Emotional alone | 1 (2%) | |
| Spiritual Domain | 25 (57%) | |
| Spiritual alone | 0 | |
| Social Domain | 30 (68%) | |
| Social Alone | 0 | |
| Multiple | 38 (86%) | |
| Interventionist Role3 | Interprofessional team + family | 2 (5%) |
| Research team | 4 (10%) | |
| Supportive care consultants | 7 (17%) | |
| Physician | 6 (14%) | |
| Nurse | 3 (7%) | |
| Interprofessional team | 10 (24%) | |
| ICU clinical team | 5 (12%) | |
| Palliative care team | 2 (5%) | |
| External education team | 3 (7%) | |
| Nurse(s) involved | 18 (41%) | |
| Sample* | Patients | 14 (32%) |
| Parent/family | 10 (23%) | |
| Clinicians | 28 (64%) |
1 Other designs included implementation, quality improvement, informal evaluation, multimethod. 2 Other unit types include interventions where all pediatric units were eligible and over half of intervention participants were in intensive care setting. 3 2 interventionist roles were unreported or unclear. *indicates categories that are not mutually exclusive.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



