
Submitted:
01 October 2025
Posted:
02 October 2025
You are already at the latest version
Abstract
Background/Objectives: Environmental contamination of dental surfaces is a signifi-cant source of cross-infection. Ultraviolet-C (UVC) irradiation offers rapid, resi-due-free decontamination, but quantitative data for dental surfaces are limited. We aimed to evaluate the germicidal efficacy of UVC on three high-touch surfaces: a wooden work table, a stainless-steel consumables table, and a dental unit table. Meth-ods: Surfaces were sampled at baseline, after 5 min (27 mJ/cm²), and after 10 min (54 mJ/cm²) of UVC exposure at 90 µW/cm². Colony-forming units (CFU/cm²) were enu-merated using Mueller–Hinton agar. Results: Baseline contamination exceeded 200 CFU/cm², predominantly Staphylococcus spp. A 5-minute exposure reduced counts by >99%, and a 10-minute exposure eradicated vegetative bacteria, with a single Ba-cillus colony detected. Material properties (porosity, reflectivity, and grooves), along with quantified parameters like surface roughness (Ra) and contact angle, influenced minor differences in decontamination. Conclusions: Used with appropriate safety protocols, short-duration UVC irradiation effectively decontaminates dental surfaces and can complement chemical disinfection. To accurately assess UVC efficacy under realistic clinical conditions, future studies must incorporate artificially soiled surfaces, biofilms, and emerging far-UVC/UV-LED technologies.
Keywords:
UVC disinfection
; dental surfaces
; material porosity
; infection control
; Bacillus spores
; far-UVC
; UV-LED
1. Introduction
Dental practices generate aerosols and splatter that readily deposit on surfaces, creating reservoirs for microorganisms, including Staphylococcus aureus, Streptococcus mutans, Enterococcus faecalis, Pseudomonas aeruginosa, and methicillin-resistant S. aureus (MRSA) [1,2,3,4]. Effective surface decontamination is essential to reduce cross-infection risk.
Chemical disinfectants (alcohols, quaternary ammonium compounds, sodium hypochlorite) remain routine but have drawbacks (surface compatibility, operator dependence, residues) [5]. Ultraviolet (UV) light—particularly UVC (100–280 nm; germicidal peak near 254 nm)—inactivates microbes by inducing pyrimidine dimers and other photoproducts in nucleic acids, preventing replication [6]. Modern approaches include low-pressure mercury lamps (254 nm), far-UVC (200–230 nm) sources that may be safer for occupied spaces [7], UV-LEDs for compact systems [8], and pulsed xenon devices for short high doses [9].
Although UVC has been validated in hospital settings for surface and air disinfection [6,7,8,9,10], comparative data on dental cabinet materials (wood, stainless steel, and plastic/composite surfaces of dental units) are limited. Material characteristics such as porosity, surface roughness, UV reflectivity/absorbance, and grooves or seams influence dose delivery, shadowing, and microbial sheltering; therefore, material-specific data are needed to produce practical protocols for dentistry.
While qualitative surface descriptions provide useful context, quantitative assessment of surface roughness, wettability, and reflectivity is essential to understand how material properties influence UVC dose delivery. These parameters directly affect microbial shielding, contaminant adhesion, and secondary scattering of UVC photons [10,11]. Therefore, in addition to microbial reduction outcomes, this study incorporated quantitative measurements of Ra, contact angle, and spectral reflectance to explore material-dependent variability in UVC efficacy.
This study quantifies UVC efficacy on three representative dental cabinet surfaces, reports results as a dose–response (mJ/cm²), and evaluates how material properties may affect observed outcomes. We also situate findings among current technologies (far-UVC, UV-LED) and discuss safety and implementation for dental practice.
2. Materials and Methods
2.1. Study Design and Setting
An experimental study was conducted in a dental clinic treatment room. Three high-touch surfaces were selected: a varnished oak work table, a polished stainless-steel consumables table (AISI 304), and a dental unit table (medical-grade polymer composite with grooves).
2.2. Surface Characterization (Materials)
Because surface properties influence UVC effectiveness, each surface was documented:
- -
- -
- Stainless-steel consumables table (AISI 304, mirror/matte finish) — Reflectivity: polished stainless steel reflects a portion of incident UVC, increasing irradiance in some directions but also producing specular reflections and potential shadow cancellation; smooth surfaces minimize micro-sheltering [14,15,16].
- -
2.2.1. Quantitative Surface Property Assessment
To establish a direct correlation between material properties and UVC susceptibility, the following parameters were quantitatively measured on test squares adjacent to the microbial sampling areas before the UVC exposure trials:
- -
- Surface Roughness (Ra): The arithmetic average of the absolute values of the profile height deviations from the mean line (Ra) was measured in triplicate on each material using a calibrated profilometer (Mitutoyo Surftest SJ-210). Measurements were taken across the grain on the wood, along the lay on the metal, and across a flat area on the dental unit polymer to quantify the micro-topography that can create “micro-shadowing” effects.
- -
- Contact Angle: The static contact angle was measured in triplicate for each surface using the sessile drop method with a goniometer (KRÜSS DSA100) and 5 μL of deionized water. This measurement indicates the surface’s hydrophobicity, which influences how contaminants and water-based aerosols adhere, potentially affecting the UVC dose received by microorganisms.
- -
- Spectral Reflectance (254 nm): The percentage of 254 nm UVC light reflected by each surface was measured using a calibrated spectroradiometer with an integrating sphere accessory. This helps determine how material reflectivity (e.g., for the stainless steel) might enhance the germicidal dose via scattered radiation.
2.3. UVC Device and Dosimetry
UVC irradiation was delivered by a dual-lamp low-pressure mercury device (2 × 40 W, nominal emission 253.7 nm) mounted 50 cm above surfaces. Irradiance was measured with a calibrated UVC radiometer. Measured irradiance at 50 cm: 90 µW/cm². Dose calculation:
Dose (mJ/cm2) = Irradiance (µW/cm2)×time (s)/1000
- -
- 5 min (300 s): 90 × 300 / 1000 = 27 mJ/cm²
- -
- 10 min (600 s): 90 × 600 / 1000 = 54 mJ/cm²
Radiometer specifications and calibration – details of the instrument used to verify UVC lamp output are:
- -
- Instrument: Solar Light PMA2100 Radiometer (Serial Number: 2024-A-7215)
- -
- Spectral range: 200–280 nm
- -
- Measurement resolution: ±1 µW/cm²
- -
- Calibration: Traceable to the National Institute of Standards and Technology (NIST); most recent calibration performed on 25 March 2025.
UVC Lamp Specifications are:
- -
- Lamp type: Dual low-pressure mercury lamps (2 × 40 W)
- -
- Emission peak: 253.7 nm
- -
- Lamp height above samples: 50 cm
- -
- Irradiance at 50 cm: 90 µW/cm² (mean of three measurements)
- -
- Operating hours at time of test: ~250 hours
- -
- All experiments were performed under controlled ambient conditions(22.5 ∘°C, 55% RH).
Figure 1 is a schematic photo of the experimental setup showing the lamp height (50 cm) used for bacterial reduction.
2.4. Sampling Protocol
Each surface was divided into nine 5 × 5 cm squares. Sampling was performed in triplicate from three adjacent squares for each condition and time point (baseline; after 5 min UVC; after 10 min cumulative UVC). Swabbing followed a standard approach aligned with ISO 18593 environmental surface sampling recommendations: sterile synthetic swabs, pre-moistened with sterile saline, stroked with firm rotational motion over the entire square area [20]. Swabs were placed into 1 mL sterile saline and vortexed for 10 seconds.
2.5. Culture and Identification
Aliquots (100 µL) were plated on Mueller-Hinton agar using a 10 µL loop, streaked in three directions, air-dried for 10 minutes, then incubated at 35 °C for 18 hours. Colony-forming units (CFUs) were counted and converted to CFU/cm² according to:
CFU/cm2=Colonies×10/25
Selected colonies were Gram-stained to determine basic morphology (Gram-positive cocci consistent with Staphylococcus spp.; one Gram-positive rod, presumptively Bacillus). Full species identification (e.g., MALDI-TOF or 16S sequencing) was not performed in this pilot and is recommended for follow-up work.
2.6. Data Handling and Statistics
Counts >200 CFU/cm² (too numerous to count) were conservatively set to 220 CFU/cm² for descriptive statistics. Mean ± SD and percentage reduction from baseline were calculated for each surface and condition. Differences across time points and statistical comparisons to detect differences among materials were assessed using one-way ANOVA or, when normality assumptions were not met, the Kruskal–Wallis test, followed by Tukey’s post hoc comparisons. A significance level of α = 0.05 was applied.
2.7. Limitations (Stated Within Methods)
We proactively acknowledge methodological limits: only culturable organisms were measured (no molecular detection); sample size was small (triplicates), limiting statistical power; no deliberate organic soiling or biofilm models were used; species-level identification was not performed.
3. Results
3.1. Baseline Contamination
To better contextualize the slight differences observed among wooden, metal, and composite dental-unit tables, we compiled literature values describing how surface microstructure and optical properties can affect UVC delivery to microorganisms (Table 1). These data help explain the modest residual contamination occasionally detected on polymer or grooved substrates.
All three surfaces exhibited high baseline contamination (>200 CFU/cm²), predominantly Gram-positive cocci consistent with Staphylococcus spp. No Gram-negative bacteria were cultured under these sampling conditions.
Quantitative measurements revealed significant material-dependent differences (Table 2).
3.2. Reduction After UVC Exposure
After 5 min (27 mJ/cm²), counts dropped markedly (>99%) on all surfaces; after 10 min (54 mJ/cm²), no colonies were observed except a single colony of a Gram-positive rod (presumptively Bacillus) on one dental unit sample (Figure 2).
Table 3 provides a powerful visual summary of the study’s primary finding: the rapid and near-complete elimination of bacterial load by UVC irradiation across different dental surface materials; it emphasizes the high-impact results and statistical significance.
Figure 3 represents dose–response bar panels (three panels) showing mean CFU/cm² (log scale) ± SD for each surface at Baseline, 5 min (27 mJ/cm²), 10 min (54 mJ/cm²).
Comparison across time points indicated a statistically significant reduction from baseline to 5 minutes and 10 minutes (p < 0.001). Differences between 5 and 10 minutes were small and not statistically significant for most surfaces due to near-zero counts (floor effect).
The data in Table 4 demonstrate the high germicidal efficacy of UVC light, achieving significant log reductions across all tested dental materials. A Log10 reduction of 2.0 means 99% of the bacteria were eliminated, while 3.0 means 99.9%. All materials achieved a Log10 reduction greater than 2.3 after just 5 minutes (27 mJ/cm2); this means the bacterial load was reduced by over 99.5%. The Wood and Metal surfaces showed Log10 reductions of ≥2.73, indicating the elimination of nearly all vegetative bacteria down to the study’s limit of detection (LOD). The Dental Unit Polymer surface achieved the highest measured reduction at 2.85 Log10, effectively reducing the initial microbial population from over 213 CFU/cm2 to an average of just 0.3 CFU/cm2.
How these numbers were obtained:
- -
- Limit of detection (LOD) = 0.4 CFU/cm² (one colony on a plate → CFU/cm² = 10/25 = 0.4).
- -
- Example calculation (Wood, 10 min with no colonies): log₁₀(220.0 / 0.4) = 2.74 → reported as ≥2.74.
4. Discussion
This study shows that UVC irradiation at 253.7 nm rapidly and substantially reduces culturable bacterial loads on three common dental cabinet surfaces. A dose of 27 mJ/cm² (5 min at 90 µW/cm²) produced >99% reduction; 54 mJ/cm² (10 min) eradicated vegetative bacteria in these experimental conditions, with the lone exception of a Bacillus colony attributed to spore resistance.
UVC kills microorganisms primarily by causing DNA/RNA photoproducts (pyrimidine dimers) that prevent replication and transcription [6]. The material properties of surfaces can modulate UVC efficacy. Even varnished wood presents unique challenges for UVC disinfection due to its intrinsic microstructure. Microscopic grain and fissures can provide protective niches where microorganisms are shielded from direct irradiation, a phenomenon often called micro-shadowing. The organic wood constituents can absorb UVC energy, reducing the effective surface dose [11,12,13]. Complete microbial elimination on wood was observed after 10 minutes of exposure. Nevertheless, subtle sheltering effects cannot be excluded, and these would likely become more pronounced under conditions involving biofilm formation or heavy soiling.
Stainless steel exhibits almost the opposite behavior, owing to its smooth, reflective properties. UVC light can undergo specular reflection, which enhances irradiance in angled or partially obstructed areas. However, this effect produces complex angular light distribution and can create secondary shadowing behind adjacent objects or at surface seams [14,15,16]. Thus, while reflectivity may support overall decontamination when lamp positioning is optimal, stainless steel remains susceptible to microbial persistence in shadowed microsites.
Plastics, such as those used in dental units, add further complexity. Surface grooves, seams, and non-uniform finishes form sheltered recesses where microorganisms persist despite UVC exposure. Moreover, plastics typically absorb a portion of UVC radiation, and the presence of organic plasticizers can alter light–surface interactions [17,18,19]. These combined factors suggest that effective decontamination of plastic components requires careful consideration of lamp angulation and, in many cases, the use of multiple lamp positions to minimize protected areas.
These considerations explain why proper lamp placement, avoidance of occluding objects, and possible multiple irradiance positions or longer exposure times are crucial for real-world effectiveness.
The measured values support and clarify the microbial reduction results. The higher roughness of wood and polymer surfaces (Ra > 0.9 µm) is consistent with micro-shadowing that may shelter bacteria. Stainless steel, with minimal roughness (Ra ≈ 0.08 µm), provides fewer shelters, explaining its rapid decontamination. Contact angle differences indicate varying hydrophobicity, influencing microbial adhesion: stainless steel exhibited the highest hydrophobicity (83.6°), which may reduce microbial retention but could also alter droplet behavior in clinical settings. Reflectance at 254 nm was highest for stainless steel (28.5%), suggesting secondary scattering could enhance fluence, while wood and polymer surfaces absorbed most incident UVC (<8%). Collectively, these findings show that quantitative surface parameters directly correlate with UVC susceptibility and should be integrated into decontamination protocol design.
A Bacillus colony’s survival after 54 mJ/cm² aligns with well-documented spore resistance: spores possess multiple protective layers, small acid-soluble spore proteins, and dipicolinic acid that stabilizes DNA and reduces photochemical damage. Sporicidal action generally requires higher UVC doses (often >100 mJ/cm²), combined modalities (e.g., heat + UVC), or chemical sporicides [11,21].
UVC offers quick, residue-free surface decontamination. Chemical agents (e.g., sodium hypochlorite, hydrogen peroxide, quats) are effective but require contact times, thorough coverage, drying time, and can corrode or discolor materials; staff adherence varies [5,10]. Costs and environmental disposal of chemical wipes also matter. UVC, when correctly applied, reduces reliance on consumable chemicals but must be used with safe protocols.
The study’s observation of a single Bacillus colony after a 10-minute UVC exposure highlights a crucial aspect of microbial resistance: spore biology. While UVC light is highly effective against vegetative bacteria, bacterial spores are considerably more resistant, often requiring 10 to 50 times the radiation dose to achieve inactivation [23,24]. This resilience is attributed to their distinct structural and biochemical characteristics, including a protective dipicolinic acid (DPA) chelate surrounding the DNA and an altered DNA configuration [24].
The primary mechanism of UVC inactivation is the absorption of photons by DNA, leading to the formation of pyrimidine dimers that inhibit transcription and replication, ultimately leading to cell death [23]. However, some microorganisms can repair this damage through photoreactivation and dark repair, which can weaken the disinfection’s effectiveness [23,25]. Therefore, for an optimal germicidal action, the UVC dose must be sufficient to damage the DNA and overwhelm the organism’s repair mechanisms [23].
UVC disinfection presents a sustainable alternative or supplement to traditional chemical disinfectants. Unlike chemical agents, UVC leaves no residue and is chemical-free [25,26]. This reduces the environmental burden of chemical agents’ production, use, and disposal. The sustainability of UVC technology is further enhanced by the development of UV-LEDs, which offer a safer and more efficient alternative to conventional mercury vapor lamps, eliminating the hazardous materials found in the latter [26]. This innovation also allows for operation at multiple wavelengths, providing greater versatility in disinfection [24,25].
The widespread adoption of UVC technology in healthcare necessitates strict adherence to safety standards. Direct exposure to UVC light harms human skin and eyes, potentially causing “sunburn” and photokeratitis [25,26]. Consequently, safety regulations mandate fail-safe systems to prevent lamps from operating when the device’s cover is removed or when personnel are present [8,25]. Recent innovations, however, include Far-UVC technology (around 222 nm), which is considered safe for use in occupied spaces as its short wavelength does not penetrate the skin’s outer dead cell layer or the tear layer of the eyes [24]. This allows for continuous decontamination without interrupting daily operations [24].
A comprehensive cost-benefit analysis is crucial for evaluating the adoption of UVC systems. While the initial investment in UVC devices can be significant, the technology offers a substantial return on investment by improving patient outcomes and operational efficiency [25,26,27]. UVC technology can reduce infection rates, shorten patient stays, and decrease readmission rates [26,27]. Moreover, it streamlines the disinfection process, reducing the time required for cleaning between procedures and minimizing human error [27]. One study found that UVC sanitizing devices were more cost-effective than relying solely on hand hygiene protocols, with a potential for significant long-term savings [28].
The findings of this study reinforce the value of a bundled approach to infection control, where UVC irradiation is used in conjunction with other methods. While UVC is highly effective on surfaces it can reach, its germicidal efficacy is limited by the “shadowing effect,” where areas not directly exposed to the light remain contaminated [26,29]. This makes it an ideal supplement to manual cleaning and chemical disinfection. Studies have shown that combining UVC light with antibacterial tablets can result in statistically superior disinfection outcomes [29]. This integrated strategy leverages the strengths of both methods, ensuring a more comprehensive and robust approach to infection prevention in dental practices.
Conventional 254 nm UVC can damage skin and eyes upon direct exposure (erythema, photokeratitis) [12,30]. Mitigation strategies include operation only in unoccupied rooms, safety interlocks, motion sensors, and shielded enclosures. Far-UVC (200–230 nm) has emerged as a promising alternative: studies show effective microbial inactivation with reduced penetration into the living human epidermis and cornea, suggesting lower risk for occupied spaces [7,22]. UV-LED modules (varied wavelengths) offer compact form factors, longer life, instant on/off control, and no mercury content [8].
The present study and evidence from the broader literature support the integration of UVC irradiation as an adjunct to conventional infection-control measures in dental environments. Our findings indicate that a short exposure to germicidal UVC can reduce surface contamination, provided dosing and operational factors are carefully controlled.
For routine, between-patient decontamination of flat work surfaces, an exposure of approximately 5 minutes at 50 cm (≥27 mJ/cm²) is sufficient to diminish the vegetative bacterial load. This duration aligns with reports demonstrating rapid inactivation of common clinical isolates at comparable fluence rates. When surfaces are likely to carry higher microbial burdens—such as after aerosol-generating procedures or in the presence of visible contamination—10 minutes (≥50 mJ/cm²) or the combined use of chemical disinfectants and UVC is recommended to ensure deeper log-reductions.
Operational considerations strongly influence efficacy. Surfaces should remain unobstructed during irradiation to avoid shadowing effects; where complex geometries are unavoidable, repositioning lamps or employing multiple lamp angles can help achieve uniform coverage. In rooms that remain occupied during decontamination, the use of far-UVC (207–222 nm) sources or shielded UV-LED enclosures may provide an additional safety margin, and conventional 254 nm devices should be equipped with interlocks or motion sensors to prevent accidental exposure.
Finally, sustainable implementation requires appropriate organizational measures. Staff should receive lamp positioning training, safety precautions, and fluence monitoring. Written protocols and checklists can support consistent practice, and maintenance records—particularly lamp operating hours and periodic radiometer checks—are essential to verify that devices continue to deliver the intended dose.
By incorporating these practical steps, dental teams can enhance environmental hygiene and reduce the risk of cross-contamination, while ensuring safe and efficient use of UVC technology.
The current study has several limitations, necessitating the implementation of findings into real-world clinical practice through clinical research. The study’s design, including a small sample size (triplicate), the absence of biofilm or heavy-soil models, and a lack of detailed microbial identification and surface characterization, provides a valuable foundation but does not fully reflect the complexities of a dental environment.
A primary limitation is the study’s use of clean surfaces, which does not account for biofilms and heavy organic soiling—common in dental operatories [31,32]. Biofilms are complex microbial communities encased in a protective matrix, offering significant resistance to disinfection [31]. To accurately assess UVC efficacy under realistic clinical conditions, future studies must incorporate artificially soiled surfaces and established biofilm models. Furthermore, the microbial identification in this study was limited to Gram staining, which provides a general classification but lacks species-level detail [33]. Advanced techniques like Matrix-Assisted Laser Desorption/Ionization-Time of Flight (MALDI-TOF) mass spectrometry or 16S ribosomal RNA (rRNA) gene sequencing should be used to enhance the scientific value of future work. These methods provide precise species identification and can profile the presence of highly resistant pathogens, such as Methicillin-resistant Staphylococcus aureus (MRSA) and Enterococcus faecalis, which pose a significant risk of healthcare-associated infections [33,34].
A limitation of this pilot study is that surface roughness (Ra) and contact angle were not quantitatively assessed; instead, qualitative observations noted that the wooden surface appeared matte and textured, the metal was smooth and reflective, and the dental unit showed grooves and a non-uniform texture. Since the effectiveness of UVC is strongly influenced by surface properties, future studies should include quantitative spectral measurements of Ra, contact angle, and UV reflectance. Contact angle reflects surface hydrophobicity, which can influence contaminant adhesion and the UVC dose received, while spectral reflectance indicates how much UVC light is reflected; higher reflectivity can increase germicidal efficacy by scattering radiation into occluded areas [35,36].
The study focused on conventional UVC systems. Future research should explore emerging technologies, particularly far-UVC and UV-LED systems [7,8,29,37]. Far-UVC, with a shorter wavelength (e.g., 222 nm), is considered safe. Important parameters to assess include Surface Roughness (Ra), which can generate micro-shadows that protect microorganisms from UVC light in occupied spaces, presenting a potential strategy for continuous disinfection [35]. UV-LEDs are a more sustainable alternative to mercury lamps containing hazardous materials [34].
Finally, a comprehensive cost-benefit analysis is crucial for justifying the widespread implementation of UVC technology in clinical settings. This analysis should compare the initial capital investment and energy costs of UVC deployment against the ongoing consumable costs of chemical disinfectants, factoring in labor, storage, and waste disposal [36]. Such data will provide a robust economic argument for a shift toward more efficient and environmentally friendly disinfection strategies.
5. Conclusions
UVC irradiation is highly effective for rapid surface disinfection and can complement chemical cleaning protocols in dental clinics. Short exposure times are sufficient to inactivate vegetative bacteria on common dental materials (wood, stainless steel, and polymer). However, bacterial spores remain resistant at tested doses, and disinfection efficacy is strongly influenced by material properties such as porosity, roughness, and reflectivity. These factors should guide lamp placement and exposure time to ensure reliable outcomes. Future studies should evaluate UVC performance involving biofilms and organic debris. Emerging technologies such as Far-UVC and UV-LED systems warrant investigation to develop safer, continuous, and more sustainable disinfection protocols.
Author Contributions
Conceptualization, S.T. and D.M.; methodology, S.T. and M.P.; software, E.B.; validation, S.T., S.M.B., and D.M.; formal analysis, D.M.; investigation, S.T. and E.B.; resources, M.P. and A.M.; data curation, S.M.B.; writing—original draft preparation, S.T.; writing—review and editing, M.P. and D.M.; visualization, E.B. and S.M.B.; supervision, D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We thank the dental clinic staff for facility access and assistance during sampling.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Szymańska, J.; Sitkowska, J.; Dutkiewicz, J. Microbial Contamination of Dental Unit Waterlines. Ann. Agric. Environ. Med. 2008, 15, 173–179. [Google Scholar]
- Pardo, A.; Fiorini, V.; Zangani, A.; Faccioni, P.; Signoriello, A.; Albanese, M.; Lombardo, G. Topical Agents in Biofilm Disaggregation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 2179. [Google Scholar] [CrossRef]
- Marsh, P.D.; Moter, A.; Devine, D.A. Dental Plaque Biofilms: Communities, Conflict and Control. Periodontol. 2000 2011, 55, 16–35. [Google Scholar] [CrossRef]
- Al-Hammadi, S.; Al-Shehari, W.A.; Edrees, W.H.; et al. Prevalence of Methicillin-Resistant Staphylococcus aureus (MRSA) among Patients with Oral Infections in Sana’a City, Yemen. BMC Oral Health 2025, 25, 1047. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W.A.; Weber, D.J. Disinfection, Sterilization, and Antisepsis: Principles, Practices, Current Issues, New Research, and New Technologies. Am. J. Infect. Control 2019, 47S, A1–A2. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, W. Ultraviolet Germicidal Irradiation Handbook; Springer, 2009. [Google Scholar]
- Buonanno, M.; Welch, D.; Shuryak, I.; Brenner, D.J. Far-UVC Light (222 nm) Efficiently and Safely Inactivates Airborne Human Coronaviruses. Sci. Rep. 2020, 10, 10285. [Google Scholar] [CrossRef]
- Kebbi, Y.; Muhammad, A.I.; Sant’Ana, A.S.; do Prado-Silva, L.; Liu, D.; Ding, T. Recent Advances on the Application of UV-LED Technology for Microbial Inactivation: Progress and Mechanism. Compr. Rev. Food Sci. Food Saf. 2020, 19, 3501–3527. [Google Scholar] [CrossRef]
- Nerandzic, M.M.; Thota, P.; Sankar, C.T.; et al. Evaluation of a Pulsed Xenon Ultraviolet Disinfection System for Reduction of Healthcare-Associated Pathogens in Hospital Rooms. Infect. Control Hosp. Epidemiol. 2015, 36, 192–197. [Google Scholar] [CrossRef]
- Di Martino, G.; Pasqua, S.; Douradinha, B.; Monaco, F.; Di Bartolo, C.; Conaldi, P.G.; D’Apolito, D. Efficacy of Three Commercial Disinfectants in Reducing Microbial Surfaces’ Contaminations of Pharmaceuticals Hospital Facilities. Int. J. Environ. Res. Public Health 2021, 18, 779. [Google Scholar] [CrossRef]
- Duanis-Assaf, D.; Kenan, E.; Sionov, R.; Steinberg, D.; Shemesh, M. Proteolytic Activity of Bacillus subtilis upon κ-Casein Undermines Its “Caries-Safe” Effect. Microorganisms 2020, 8, 221. [Google Scholar] [CrossRef] [PubMed]
- Sliney, D.H.; Stuck, B.E. A Need to Revise Human Exposure Limits for Ultraviolet UV-C Radiation. Photochem. Photobiol. 2021, 97, 485–492. [Google Scholar] [CrossRef]
- Reed, N.G. The History of Ultraviolet Germicidal Irradiation for Air Disinfection. Public Health Rep. 2010, 125, 15–27. [Google Scholar] [CrossRef]
- Kujundzic, E.; Matalkah, F.; Howard, C.J.; Hernandez, M.; Miller, S.L. UV Air Cleaners and Upper-Room Air Ultraviolet Germicidal Irradiation for Controlling Airborne Bacteria and Fungal Spores. J. Occup. Environ. Hyg. 2006, 3, 536–546. [Google Scholar] [CrossRef]
- Kowalski, W.; Bahnfleth, W.; Hernandez, M. A Genomic Model for Predicting the Ultraviolet Susceptibility of Viruses and Bacteria. IUVA News 2006, 8, 33–38. [Google Scholar]
- Albertini, R.; Colucci, M.E.; Coluccia, A.; et al. An Overview on the Use of Ultraviolet Radiation to Disinfect Air and Surfaces. Acta Biomed. 2023, 94, e2023165. [Google Scholar] [CrossRef]
- Jeon, M.-J.; Choi, Y.-S.; Seo, D.-G. Bactericidal Effects of Ultraviolet-C Light-Emitting Diode Prototype Device Through Thin Optical Fiber. Appl. Sci. 2025, 15, 4504. [Google Scholar] [CrossRef]
- Kvam, E.; Benner, K. Mechanistic Insights into UV-A Mediated Bacterial Disinfection via Endogenous Photosensitizers. J. Photochem. Photobiol. B 2020, 209, 111899. [Google Scholar] [CrossRef] [PubMed]
- Imada, K.; Tanaka, S.; Ibaraki, Y.; Yoshimura, K.; Ito, S. Antifungal Effect of 405-nm Light on Botrytis cinerea. Lett. Appl. Microbiol. 2014, 59, 670–676. [Google Scholar] [CrossRef]
- Mikelonis, A.M.; Abdel-Hady, A.; Aslett, D.; Ratliff, K.; Touati, A.; Archer, J.; Serre, S.; Mickelsen, L.; Taft, S.; Calfee, M.W. Comparison of Surface Sampling Methods for an Extended Duration Outdoor Biological Contamination Study. Environ. Monit. Assess. 2020, 192, 455. [Google Scholar] [CrossRef]
- Setlow, B.; Korza, G.; Blatt, K.M.; Fey, J.P.; Setlow, P. Mechanism of Bacillus subtilis Spore Inactivation by and Resistance to Supercritical CO₂ plus Peracetic Acid. J. Appl. Microbiol. 2016, 120, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Hessling, M.; Haag, R.; Sieber, N.; Vatter, P. The Impact of Far-UVC Radiation (200–230 nm) on Pathogens, Cells, Skin, and Eyes—A Collection and Analysis of a Hundred Years of Data. GMS Hyg. Infect. Control 2021, 16, Doc07. [Google Scholar] [CrossRef]
- Blau, K.; Gallert, C. Efficacy of UV-C 254 nm Light and a Sporicidal Surface Disinfectant in Inactivating Spores from Clostridioides difficile Ribotypes In Vitro. Pathogens 2024, 13, 965, Öberg, R.; Sil, T.B.; Johansson, A.C.; Malyshev, D.; Landström, L.; Johansson, S.; Andersson, M.; Andersson, P.O. UV-Induced Spectral and Morphological Changes in Bacterial Spores for Inactivation Assessment. J. Phys. Chem. B 2024, 128, 1638–1646. https://doi.org/10.1021/acs.jpcb.3c07062. [Google Scholar] [CrossRef] [PubMed]
- Hashemzadeh, F.; Geppert, A.; Jackson, L.J.; Harrison, J.J.; Achari, G. Hydrogen Peroxide Augments the Disinfection Efficacy of 280 nm Ultraviolet LEDs against Antibiotic-Resistant Uropathogenic Otherwise Tolerant to Germicidal Irradiation. ACS Omega 2025, 10, 29558–29568. [Google Scholar] [CrossRef]
- Duque-Sarango, P.; Delgado-Armijos, N.; Romero-Martínez, L.; Cruz, D.; Pinos-Vélez, V. Advancing Waterborne Fungal Spore Control: UV-LED Disinfection Efficiency and Post-Treatment Reactivation Analysis. Water 2025, 17, 922. [Google Scholar] [CrossRef]
- Sun, Y.; Wu, Q.; Liu, J.; Wang, Q. Effectiveness of ultraviolet-C disinfection systems for reduction of multi-drug resistant organism infections in healthcare settings: A systematic review and meta-analysis. Epidemiol Infect. 2023, 151, e149. [Google Scholar] [CrossRef]
- Cook, D.C.; Olsen, M.; Tronstad, O.; et al. Ultraviolet-C-based sanitization is a cost-effective option for hospitals to manage health care-associated infection risks from high touch mobile phones. Front Health Serv. 2025, 4, 1448913. [Google Scholar] [CrossRef] [PubMed]
- Nicolau, T.; Gomes Filho, N.; Padrão, J.; Zille, A. A Comprehensive Analysis of the UVC LEDs’ Applications and Decontamination Capability. Materials 2022, 15, 2854. [Google Scholar] [CrossRef]
- Welch, D.; Aquino de Muro, M.; Buonanno, M.; Brenner, D.J. Wavelength-Dependent DNA Photodamage in a 3-D Human Skin Model over the Far-UVC and Germicidal UVC Wavelength Ranges from 215 to 255 nm. Photochem. Photobiol. 2022, 98, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Abushahba, F.; Algahawi, A.; Areid, N.; Vallittu, P.K.; Närhi, T. Efficacy of biofilm decontamination methods of dental implant surfaces: A systematic review of in vitro studies. Eur J Oral Sci. 2025, 133, e70005. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Khan, S.A.; Zachar, J.; Yang, Z.; Kiran, R.; Walsh, L.J. Efficacy of Ultrasonic Cleaning Products with Various Disinfection Chemistries on Dental Instruments Contaminated with Bioburden. Int. Dent. J. 2025, 75, 1632–1639. [Google Scholar] [CrossRef]
- Szabó, S.; Feier, B.; Capatina, D.; Tertis, M.; Cristea, C.; Popa, A. An Overview of Healthcare Associated Infections and Their Detection Methods Caused by Pathogen Bacteria in Romania and Europe. J. Clin. Med. 2022, 11, 3204. [Google Scholar] [CrossRef]
- Velazquez-Meza, M.E.; Galarde-López, M.; Cornejo-Juárez, P.; Carrillo-Quiroz, B.A.; Velázquez-Acosta, C.; Bobadilla-del-Valle, M.; Ponce-de-León, A.; Alpuche-Aranda, C.M. Multidrug-Resistant Staphylococcus sp. and Enterococcus sp. in Municipal and Hospital Wastewater: A Longitudinal Study. Microorganisms 2024, 12, 645. [Google Scholar] [CrossRef]
- Razavifar, M.; Abdi, A.; Nikooee, E.; et al. Quantifying the Impact of Surface Roughness on Contact Angle Dynamics under Varying Conditions. Sci. Rep. 2025, 15, 16611. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, R.A.; Navne, J.; Adelmark, M.V.; Shkondin, E.; Crovetto, A.; Hansen, O.; Bachmann, J.; Taboryski, R. Understanding the Light Induced Hydrophilicity of Metal-Oxide Thin Films. Nat. Commun. 2024, 15, 124. [Google Scholar] [CrossRef] [PubMed]
- Griffin, D.T.; Gourlay, T.; Maclean, M. The Antibacterial Efficacy of Far-UVC Light: A Combined-Method Study Exploring the Effects of Experimental and Bacterial Variables on Dose–Response. Pathogens 2024, 13, 698. [Google Scholar] [CrossRef] [PubMed]
- Duering, H.; Westerhoff, T.; Kipp, F.; Stein, C. Short-Wave Ultraviolet-Light-Based Disinfection of Surface Environment Using Light-Emitting Diodes: A New Approach to Prevent Health-Care-Associated Infections. Microorganisms 2023, 11, 386. [Google Scholar] [CrossRef]
Figure 1.
UVC Bacterial Reduction.
Figure 2.
Bacterial growth on culture media at different stages of UVC exposure: (A) initial growth (baseline), (B) after 5 minutes of UVC exposure, and (C) after 10 minutes of UVC exposure. Each row represents triplicate assessments performed under identical conditions.
Figure 2.
Bacterial growth on culture media at different stages of UVC exposure: (A) initial growth (baseline), (B) after 5 minutes of UVC exposure, and (C) after 10 minutes of UVC exposure. Each row represents triplicate assessments performed under identical conditions.
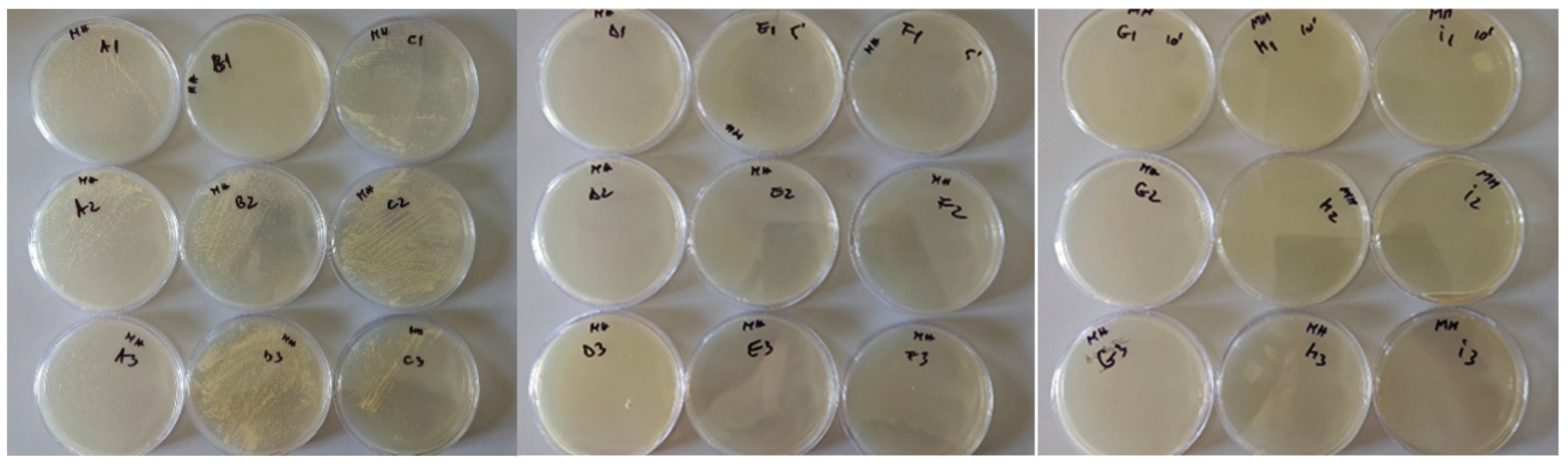
Figure 3.
Bacterial load (CFU/cm²) on wooden, stainless-steel, and dental unit surfaces before and after UVC exposure (mean ± SD, n = 3). The y-axis log scale helps visualize baseline vs post-treatment counts. The logarithmic y-axis emphasizes the drastic reduction from baseline (>200 CFU/cm²) to <2 CFU/cm² after UVC exposure.
Figure 3.
Bacterial load (CFU/cm²) on wooden, stainless-steel, and dental unit surfaces before and after UVC exposure (mean ± SD, n = 3). The y-axis log scale helps visualize baseline vs post-treatment counts. The logarithmic y-axis emphasizes the drastic reduction from baseline (>200 CFU/cm²) to <2 CFU/cm² after UVC exposure.
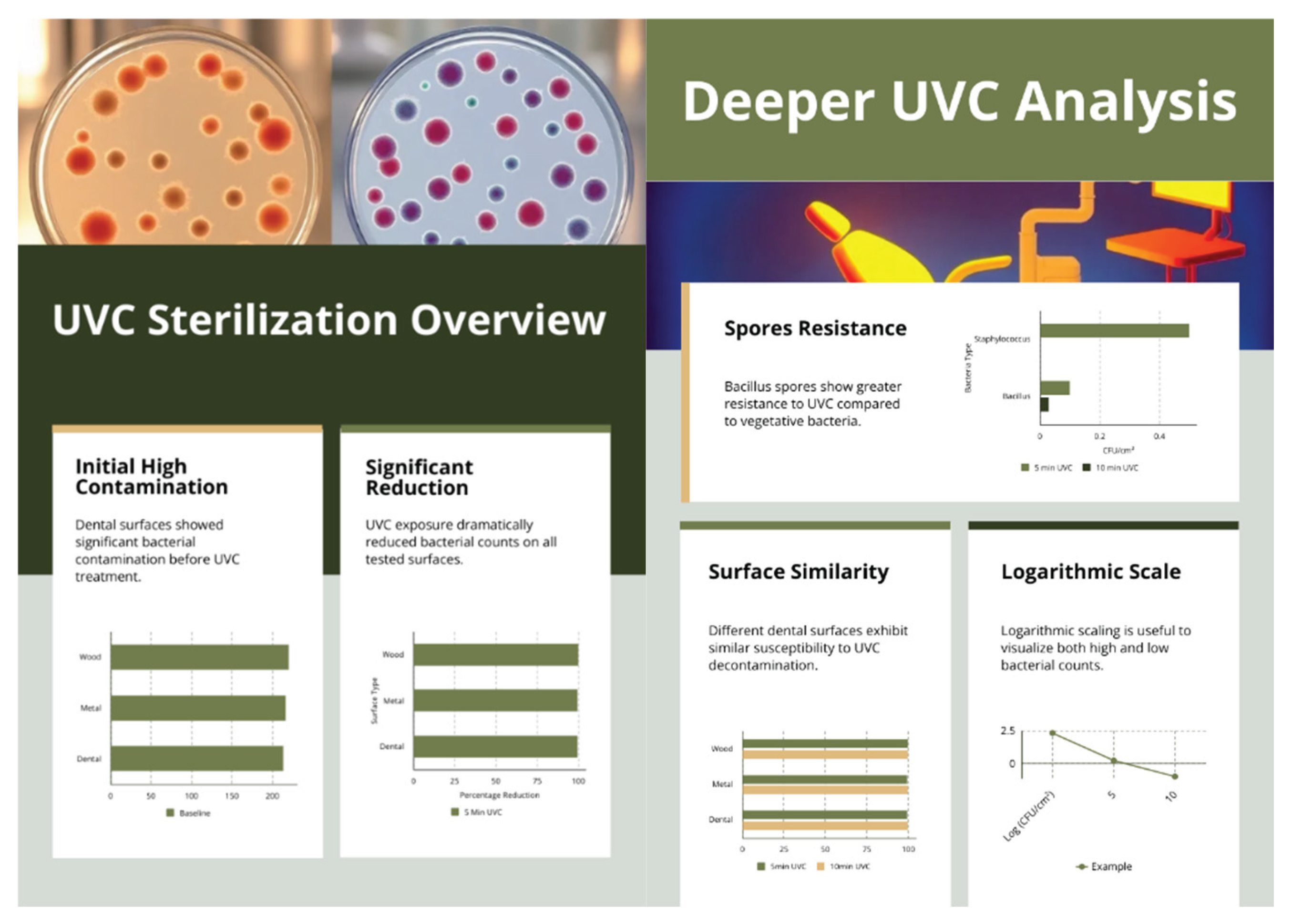

Table 1.
Estimated material characteristics influencing UVC efficacy (values from representative studies).
Table 1.
Estimated material characteristics influencing UVC efficacy (values from representative studies).
| Surface | Porosity /Roughness | Typical UVC Reflectance (254 nm) | Likely effect on decontamination | References |
| Varnished oak (wood) | Moderate porosity; grain-aligned micro-crevices even after varnish | 5–12% (varies with coating thickness and pigment) | Absorption and “micro-shadowing” may protect cells lodged in pores or along fibres | [11,12,13] |
| Stainless steel (AISI 304) | Ra ≈ 0.05–0.2 µm (polished) | 25–30% | High reflectivity can enhance fluence on adjacent points; minimal micro-sheltering if free of debris | [14,15,16] |
| Dental-unit polymer/composite | Grooves and seams; matte areas | < 8% (most plastics); varies by pigment | Absorption and irregular topology reduce direct fluence; seams may shield bacteria | [17,18,19] |
Note: Values are indicative averages from optical/engineering literature; they were not measured on the tested items.
Table 2.
Quantitative Surface Properties of Tested Materials.
| Surface Material | Surface Roughness (Ra) | Static Contact Angle | Spectral Reflectance (254 nm) |
| Wood (Varnished Oak) | 1.5±0.2 μm | 68.4∘±2.5∘ | 7.2%±0.4% |
| Stainless Steel (AISI 304) | 0.08±0.01 μm | 83.6∘±1.8∘ | 28.5%±1.2% |
| Dental Unit Polymer | 0.9±0.1 μm | 76.2∘±3.1∘ | 5.1%±0.3% |
Table 3.
Mean bacterial load (CFU/cm²) ± SD with 95% confidence intervals and significance versus baseline. (n = 3 per condition, one-way ANOVA with Tukey’s post hoc test, α = 0.05).
Table 3.
Mean bacterial load (CFU/cm²) ± SD with 95% confidence intervals and significance versus baseline. (n = 3 per condition, one-way ANOVA with Tukey’s post hoc test, α = 0.05).
| Surface | Condition | Mean CFU/cm² ± SD | 95% CI | p vs baseline |
| Wood | Baseline | 220.0 ± 10.0 | 209.6–230.4 | — |
| 5 min UVC | 0.7 ± 0.6 | 0.1–1.3 | < 0.001 | |
| 10 min UVC | 0.0 ± 0.0 | 0.0–0.0 | < 0.001 | |
| Metal | Baseline | 216.7 ± 7.6 | 208.8–224.5 | — |
| 5 min UVC | 1.0 ± 1.0 | 0.0–2.1 | < 0.001 | |
| 10 min UVC | 0.0 ± 0.0 | 0.0–0.0 | < 0.001 | |
| Dental | Baseline | 213.3 ± 7.6 | 205.5–221.2 | — |
| 5 min UVC | 1.0 ± 1.0 | 0.0–2.1 | < 0.001 | |
| 10 min UVC | 0.3 ± 0.6 | 0.0–0.9 | < 0.001 |
Note: CI = Confidence Interval; values truncated at 0 when lower bound <0. Baseline not tested against itself.
Table 4.
Log₁₀ reductions of bacterial load after UVC exposure (n = 3).
| Baseline mean (CFU/cm²) | 5 min mean (CFU/cm²) | 5 min log₁₀ reduction | 10 min mean (CFU/cm²) | 10 min log₁₀ reduction | |
| Wood | 220.0 | 0.7 | 2.50 | 0.0 (<LOD) | ≥2.74 |
| Metal | 216.7 | 1.0 | 2.34 | 0.0 (<LOD) | ≥2.73 |
| Dental | 213.3 | 1.0 | 2.33 | 0.3 | 2.85 |
Note: CFU conversion: CFU/cm² = (colonies × 10) / 25 → one colony ≈ 0.4 CFU/cm², so the experimental limit of detection (LOD) is 0.4 CFU/cm². For mean counts below the LOD (reported as 0.0 in the dataset), log reductions are reported as “≥” the value calculated using the LOD (conservative lower bound). Log₁₀ reduction = log₁₀ (Baseline mean / post-treatment mean).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



