Submitted:
28 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Background and Aim: Standardisation is crucial for outcomes in minimally invasive colorectal surgery. Debate continues regarding the comparative efficacy of robotic versus laparoscopic platforms. This study evaluates perioperative outcomes for both approaches, performed by a single surgeon using an identical standardised technique to isolate the platform's effect. Methods: A retrospective cohort study of 250 patients undergoing colorectal resection (2019-2023) was conducted. Patients were divided into laparoscopic (n=121) and robotic (n=129) groups. Data included demographics, ASA grade, conversion rates, operative times, Clavien-Dindo complications, resection margin status (R0/R1), mortality, and length of stay. R software was used for analysis. Results: Demographics were matched, but fewer high-risk (ASA III) patients were in the robotic cohort (38.7% vs. 51.3%; p<0.05). The robotic approach showed a significantly lower conversion rate (0% vs. 6.6%). A non-significant trend toward higher-grade complications existed in the laparoscopic group (median grade II vs. I; p=0.12), with a significantly higher R1 resection rate (n=8 vs. n=2). Laparoscopic 30-day (2 vs. 0) and 90-day (4 vs. 0) mortality was higher. Anastomotic leak rates (1.6% each) and median hospital stay (5 days; p=0.71) were similar in both groups. Conclusion: Using a standardised technique, outcomes are comparable except for a significantly reduced conversion rate with robotics. The observed difference in R1 resection rates may be influenced by baseline differences in patient populations. For skilled surgeons, the choice of platform may be influenced more by economic factors and preference than by major differences in clinical efficacy. What does this paper add to the literature? Debate continues regarding the comparative efficacy of robotic versus laparoscopic platforms. This single-surgeon study compares outcomes in colorectal cancer using minimally invasive procedures and a standardised technique. The result of similar clinical efficacy suggests that standardisation reduces outcome variability and demonstrates that cost and preference may influence platform choices more.
Keywords:
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient demographics were comparable between groups
3.2. Analysis of intraoperative outcomes shows that conversion to open surgery was less likely with robotic surgery
3.3. Generic postoperative outcomes were not different between modalities
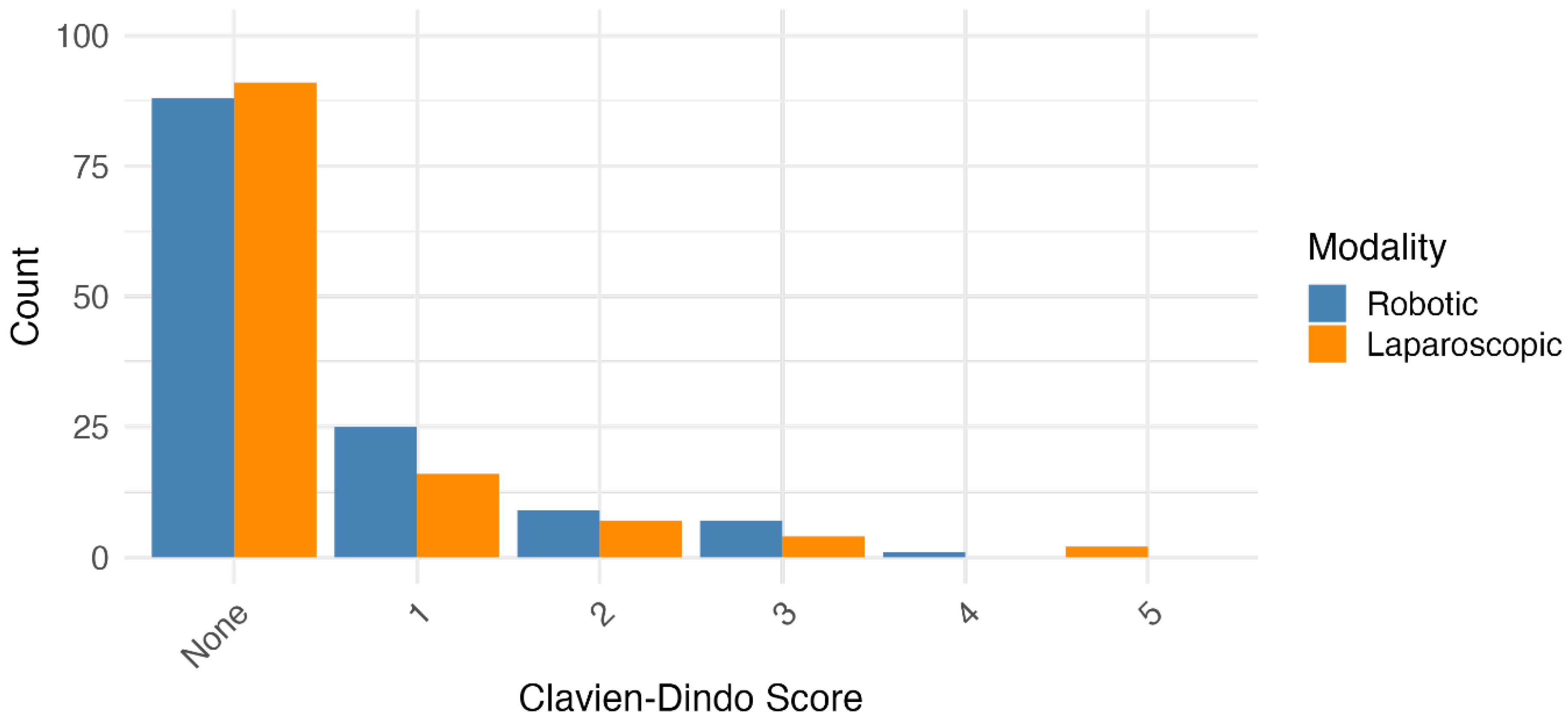
3.4. Severity and nature of postoperative complications were similar between surgical modalities
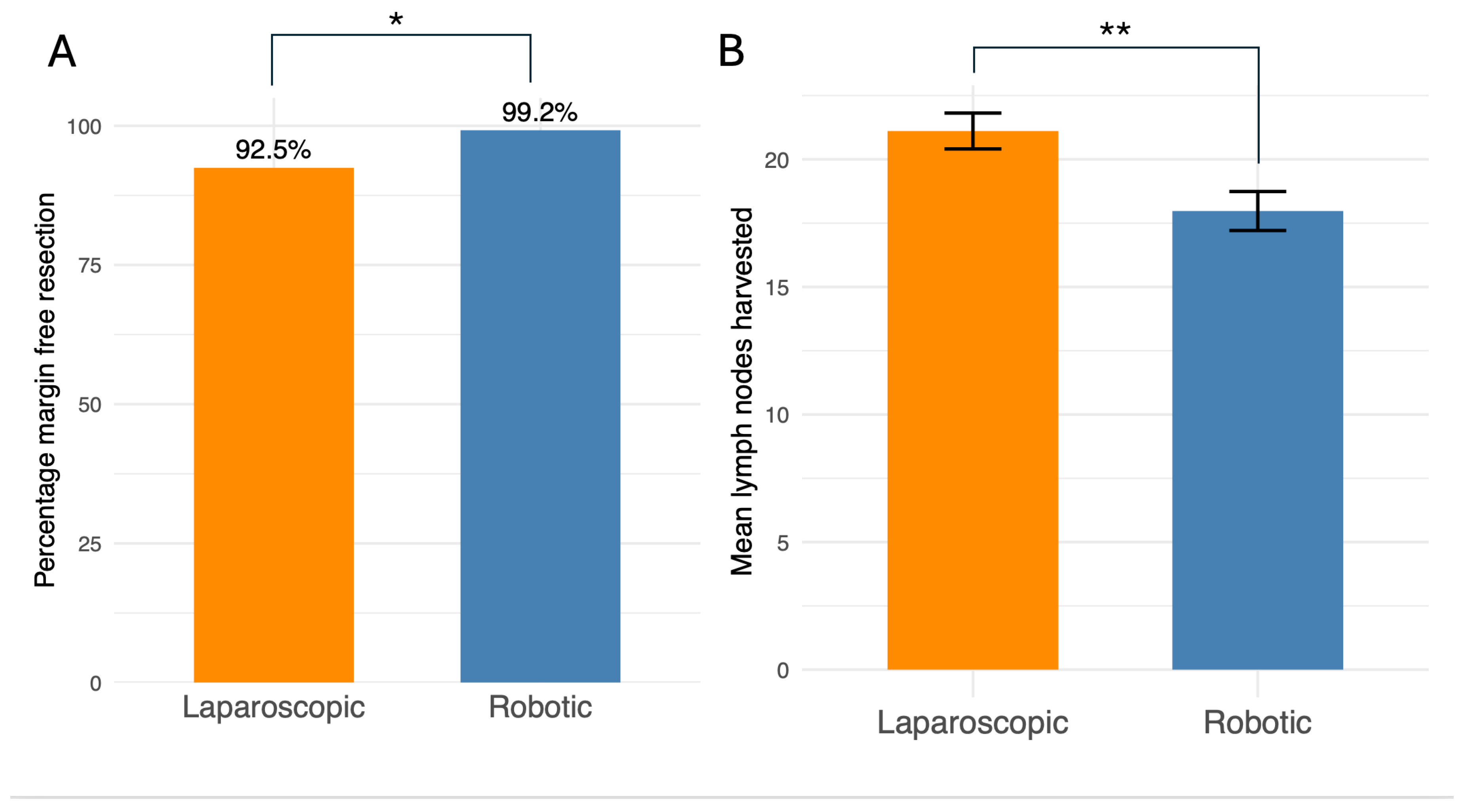
4. Robotic surgery was more likely to achieve complete resection of tumours
5. Discussion
6. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
Ethics
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209–49. [CrossRef]
- Wang W, Liu J, Wang J, Li L, Kong D, Wang J. Comparative study of robotic-assisted vs. laparoscopic surgery for colorectal cancer: a single-center experience. Front Oncol. 2025 Jan 7;14. [CrossRef]
- Butnari V, Sultana M, Mansuri A, Rao C, Kaul S, Boulton R, et al. Comparison of early surgical outcomes of robotic and laparoscopic colorectal cancer resection reported by a busy district general hospital in England. Sci Rep. 2024 Apr 22;14(1):9227. [CrossRef]
- Koc MA, Thomas MS, Mavrantonis S, Panteleimonitis S, Harper M, Sanjay C, et al. Structured training pathway for robotic colorectal surgery: Short-term outcomes from five UK centres. Colorectal Dis. 2024 Nov;26(11):1965–70. [CrossRef]
- Eto K, Urashima M, Kosuge M, Ohkuma M, Noaki R, Neki K, et al. Standardization of surgical procedures to reduce risk of anastomotic leakage, reoperation, and surgical site infection in colorectal cancer surgery: a retrospective cohort study of 1189 patients. Int J Colorectal Dis. 2018 Jun;33(6):755–62. [CrossRef]
- Walmsley J, Max S, Hughes G, Ahmed J. https://youtu.be/06q5JPCOjYo?feature=shared. 2021 [cited 2025 Sep 23]. A Stepwise Approach to Laparoscopic Right Hemi-Colectomy with D2 Excision. Available online: https://youtu.be/06q5JPCOjYo?feature=shared.
- Walmsley J, Marcu V, Riaz S, Ahmed J. https://youtu.be/spJKtqKjYb0?feature=shared. 2020 [cited 2025 Sep 23]. A Stepwise Approach to LAR. An Illustrated Video for Training Colorectal Surgeons. Available online: https://youtu.be/spJKtqKjYb0?feature=shared.
- Rehman A, Rehman M, Malik K, Ahmed J. https://youtu.be/1n3hJ5XPJv8?feature=shared. 2024 [cited 2025 Sep 23]. Robotic Right Hemicolectomy: CME Approach and D3 Lymphadenectomy. Available online: https://youtu.be/1n3hJ5XPJv8?feature=shared.
- Khan F, Rehman A, Ur-Rehman M, Ahmed J. https://youtu.be/uFL4aIKy_yE?feature=shared. 2025 [cited 2025 Sep 23]. Robotic Low Anterior Resection. Available online: https://youtu.be/uFL4aIKy_yE?feature=shared.
- Dindo D, Demartines N, Clavien PA. Classification of Surgical Complications. Ann Surg. 2004 Aug;240(2):205–13. [CrossRef]
- Liu Q, Huang M, Yang J, Jiang M, Zhao Z, Zhao H, et al. Association between the number of retrieved lymph nodes and demographic/tumour-related characteristics in colorectal cancer: a systematic review and meta-analysis. BMJ Open. 2023 Dec 22;13(12):e072244. [CrossRef]
- Allaix ME, Furnée EJB, Mistrangelo M, Arezzo A, Morino M. Conversion of laparoscopic colorectal resection for cancer: What is the impact on short-term outcomes and survival? World J Gastroenterol. 2016 Oct 7;22(37):8304–13. [CrossRef]
- Cleary RK, Mullard AJ, Ferraro J, Regenbogen SE. The cost of conversion in robotic and laparoscopic colorectal surgery. Surg Endosc. 2018 Mar;32(3):1515–24. [CrossRef]
- Giglio MC, Celentano V, Tarquini R, Luglio G, De Palma GD, Bucci L. Conversion during laparoscopic colorectal resections: a complication or a drawback? A systematic review and meta-analysis of short-term outcomes. Int J Colorectal Dis. 2015 Nov;30(11):1445–55. [CrossRef]
- Clancy C, O’Leary DP, Burke JP, Redmond HP, Coffey JC, Kerin MJ, et al. A meta-analysis to determine the oncological implications of conversion in laparoscopic colorectal cancer surgery. Colorectal Dis. 2015 Jun;17(6):482–90. [CrossRef]
- Wang X, Cao G, Mao W, Lao W, He C. Robot-assisted versus laparoscopic surgery for rectal cancer: A systematic review and meta-analysis. J Cancer Res Ther. 2020;16(5):979. [CrossRef]
- Flynn J, Larach JT, Kong JCH, Rahme J, Waters PS, Warrier SK, et al. Operative and oncological outcomes after robotic rectal resection compared with laparoscopy: a systematic review and meta-analysis. ANZ J Surg. 2023 Mar 10;93(3):510–21. [CrossRef]
- Cuk P, Kjær MD, Mogensen CB, Nielsen MF, Pedersen AK, Ellebæk MB. Short-term outcomes in robot-assisted compared to laparoscopic colon cancer resections: a systematic review and meta-analysis. Surg Endosc. 2022 Jan 1;36(1):32–46. [CrossRef]
- Waters PS, Cheung FP, Peacock O, Heriot AG, Warrier SK, O’Riordain DS, et al. Successful patient-oriented surgical outcomes in robotic vs. laparoscopic right hemicolectomy for cancer – a systematic review. Colorectal Disease. 2020 May 4;22(5):488–99. [CrossRef]
- Gahunia S, Wyatt J, Powell SG, Mahdi S, Ahmed S, Altaf K. Robotic-assisted versus laparoscopic surgery for colorectal cancer in high-risk patients: a systematic review and meta-analysis. Tech Coloproctol. 2025 Apr 8;29(1):98. [CrossRef]
- Asklid D, Ljungqvist O, Xu Y, Gustafsson UO. Short-term outcome in robotic vs. laparoscopic and open rectal tumor surgery within an ERAS protocol: a retrospective cohort study from the Swedish ERAS database. Surg Endosc. 2022 Mar;36(3):2006–17. [CrossRef]
- Hu DP, Zhu XL, Wang H, Liu WH, Lv YC, Shi XL, et al. Robotic-assisted versus conventional laparoscopic surgery for colorectal cancer: Short-term outcomes at a single center. Indian J Cancer. 2021;58(2):225–31. [CrossRef]
- Coleman MG, Hanna GB, Kennedy R, National Training Programme Lapco. The National Training Programme for Laparoscopic Colorectal Surgery in England: a new training paradigm. Colorectal Dis. 2011 Jun;13(6):614–6. [CrossRef]
- Panteleimonitis S, Miskovic D, Bissett-Amess R, Figueiredo N, Turina M, Spinoglio G, et al. Short-term clinical outcomes of a European training programme for robotic colorectal surgery. Surg Endosc. 2021 Dec;35(12):6796–806. [CrossRef]
- Panteleimonitis S, Popeskou S, Aradaib M, Harper M, Ahmed J, Ahmad M, et al. Implementation of robotic rectal surgery training programme: importance of standardisation and structured training. Langenbecks Arch Surg. 2018 Sep 20;403(6):749–60. [CrossRef]
- Negrut RL, Cote A, Caus VA, Maghiar AM. Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes-A Focus on Studies from 2020-2024. Cancers (Basel). 2024 Apr 18;16(8). [CrossRef]
- Park JS, Lee SM, Choi GS, Park SY, Kim HJ, Song SH, et al. Comparison of Laparoscopic Versus Robot-Assisted Surgery for Rectal Cancers. Ann Surg. 2023 Jul;278(1):31–8. [CrossRef]
- Dindo D, Demartines N, Clavien PA. Classification of Surgical Complications. Ann Surg. 2004 Aug;240(2):205–13. [CrossRef]

| Variable | Laparoscopic | Robotic | p-Value |
|---|---|---|---|
| Number of cases | 120 | 130 | |
| Mean age (SD) - years | 68 (12.8) | 66.8 (14.3) | 0.57 |
| Female gender - N (%) | 54 (45) | 59 (45.4) | 0.94 |
| Mean BMI (SD) | 27.1 (5.4) | 28.1 (5.1) | 0.13 |
| ASA Grade 1 | 2 (0.02) | 16 (0.12) | 0.05 |
| Number having neoadjuvant chemotherapy – N (%) | 51 (49) | 37 (30.3) | 0.006 |
| Variable | Laparoscopic | Robotic | |
|---|---|---|---|
| Number converted to open surgery (%) | 7 (5.8) | 0 (0) | 0.005 |
| Mean operative time in minutes (SD) | 223 (71) | 200 (74) | 0.07 |
| Variable | Laparoscopic | Robotic | p-Value |
|---|---|---|---|
| Median length of stay (IQR) - days | 5 (4) | 5 (4) | 0.51 |
| Number reoperated in 30 days (%) | 4 (3.3) | 10 (7.7) | 0.17 |
| Number died in 30 days (%) | 2 (1.7) | 0 (0) | 0.23 |
| Number with any postoperative complication (%) | 29 (24) | 42 (32) | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



