
Submitted:
25 September 2025
Posted:
26 September 2025
You are already at the latest version
Abstract
Objective: to assess the combined effects of aVNS, TENS, and transmeatal photobiomodulation on tinnitus perception and discomfort. Methods: This was a retrospective quasi-experimental study using medical records of 120 patients with chronic somatosensory tinnitus treated at a specialized health center. Interventions included auricular vagus nerve stimulation (aVNS), cervical transcutaneous electrical nerve stimulation (TENS), and transmeatal photobiomodulation with laser. The Visual Analogue Scale (VAS) scores for tinnitus loudness and discomfort and Tinnitus Handicap Inventory (THI) scores were assessed pre- and post-intervention. Results: Non-parametric and frequency tests were used to compare outcomes, and effect sizes (ES) were calculated. Significant reductions were observed in VAS loudness (p = 0.001; ES = 2.01) and discomfort (p = 0.001; ES = 2.23), as well as THI scores (p = 0.001; ES = 2.28). The severity classifications of tinnitus, based on VAS and THI scores, also improved significantly. The effect sizes were very large for all variables, suggesting a synergistic beneficial effect from combined interventions. Conclusions: The combination of aVNS, TENS, and transmeatal photobiomodulation seems to be an effective therapeutic strategy for reducing tinnitus perception, discomfort, and self-perceived handicap. While these findings highlight the potential of this multimodal approach, further randomized controlled trials are necessary to confirm its efficacy and elucidate the underlying mechanisms.
Keywords:
electric stimulation
; low level laser
; autonomic nervous system
; therapy
1. Introduction
Tinnitus is characterized as the perception of sound or noise without any external source [1,2]. A comprehensive systematic review on the prevalence and incidence of tinnitus suggested that more than 740 million adults are currently globally affected [2]. Other 120 million people perceived tinnitus as a major issue in their daily life [2]. Approximately 20 to 25% of patients cannot cope with tinnitus [3]. Moreover, tinnitus generates substantial economic impact due to decreased productivity, absenteeism and increased health care costs [4]. Tinnitus is often associated with anxiety, depression, cognitive impairment and sleep disorders, becoming part of a mental disorder [2,5].
Somatosensory tinnitus is a subtype of tinnitus where the perception of sound is influenced or modulated by somatosensory inputs from the head, neck, or jaw regions [6,7]. It can be caused by cervical spine disorders, temporomandibular joint disorder, head and neck injuries, chronic muscle tension, stress, or poor posture [8]. Those factors disrupt the normal somatosensory input, interacting with auditory pathways, and potentially altering the auditory processing [7,9]. The dorsal cochlear nucleus in the brainstem plays a key role in integrating auditory and somatosensory information, and changes in somatosensory input from the cervical spine or temporomandibular joint can modify its neural activity, ultimately influencing tinnitus perception [10].
There is no consensus about the most effective therapeutic management for somatosensory tinnitus, but neuromodulatory techniques have shown positive results [5,11,12,13,14]. The electrical stimulation of the auricular vagus nerve branches (aVNS) is a promising technique that raised attention to treat tinnitus [15]. The auricular branch of the vagus nerve runs superficially in auricular regions, making it a favorable target for non-invasive stimulation techniques aimed at modulating vagal activity [16,17]. For this reason, some early-phase clinical trials have been conducted on a wide range of conditions and parameters [18,19]. The action of aVNS primarily affects the autonomic nervous system, particularly in cases of sympathetic arousal, where sustained sympathetic tone excitation disrupts homeostasis and leads to symptoms associated with anxiety, depression, deficits in executive functions (e.g., attention, memory, decision-making), as well as lack of emotional control in response to stressors [20,21]. As previously mentioned, in recent years an increasing number of clinical trials have explored the effect of aVNS (either alone or as an adjunct) on tinnitus, yielding promising results in reducing both perception and discomfort [15,22,23,24]. However, a recent meta-analysis showed that distinct parameters’ combinations were used to set the electrical current delivery, which allowed high heterogeneity on methods and results, impairing any definitive conclusion on the aVNS efficacy [25].
Another neuromodulatory technique with promising results in tinnitus treatment is transcutaneous electrical nerve stimulation (TENS), particularly in the cervical region (applied to the upper cervical region near the second cervical vertebra – C2) [6,13]. TENS applied to the skin near the ear area enhances the activation of the dorsal cochlear nucleus along the somatosensory pathway, potentially increasing the inhibitory role of the nucleus in the central nervous system and, consequently, alleviating tinnitus [26]. Electrical stimulation of the C2 dermatome is known to regulate the excitation and inhibition of the dorsal cochlear nucleus by targeting cells in the dorsal column nucleus [26].
Finally, infrared laser photobiomodulation has proven to be particularly useful in treating tinnitus, specifically in the transmeatal region [27,28]. Low-intensity laser therapy was proposed as a therapeutic procedure for tinnitus over a decade ago. It has been hypothesized that low-intensity laser irradiation enhances cell proliferation, ATP and collagen synthesis, and the release of neurotrophic factors [28,29]. This technique also promotes local blood flow in the inner ear and activates repair mechanisms through photochemical and photophysical stimulation of mitochondria in hair cells [27].
Although studies have evaluated the isolated efficacy of each of the above-mentioned techniques, there are gaps in the literature regarding how a complex intervention combining those techniques could benefit patients with tinnitus. Nonetheless, empirical and clinical observations suggest that such combinations might produce faster and more intense effects, enhancing the clinical outcomes. Therefore, the present study aimed to analyze the effects of the combined intervention (taVNS, TENS and transmeatal photobiomodulation) on the perception and discomfort generated by tinnitus through the analysis of patients’ medical records.
2. Materials and Methods
2.1. Participants
This quasi-experimental retrospective study was conducted using the medical records from 120 patients with tinnitus (Table 1). All patients were treated at the Cabugueira’s Health Center, RJ, Brazil. A post hoc two-tailed power analysis returned an actual power higher than 0.99, considering the sample of 120 participants, an alpha of 5%, and a calculated effect size of 2.01. Patients with various other associated ear diseases such as otosclerosis and otitis media were excluded. Patients with serious mental illness or systemic diseases such as cardiovascular and cerebrovascular diseases, those who were unable to complete the survey, and those with incomplete medical records were also excluded. A detailed explanation of our study was given to all patients. All subjects gave their informed consent by signing the consent form. All procedures were previously approved by the Federal University of Juiz de Fora Ethics Committee (identification number: CAAE 85801925.2.0000.5147).
2.2. Outcome Assessment
The records contained the audiometry results for hearing loss, the time length of tinnitus, the tinnitus’ location (left, right, or both sides), the assessment of tinnitus loudness (‘How loud is your tinnitus?’: 0 = ‘no tinnitus’ and 10 = ‘as loud as imaginable’), analyzed using the Visual Analogue Scale (VAS). The VAS includes a 10 cm straight line, indicating the absence of symptoms at one end and the most serious tinnitus condition at the other end. The VAS was also used to assess the tinnitus’ discomfort following the same previously mentioned description. The VAS results were qualitatively classified as follows: mild (0–3), moderate (4–7) and severe (8–10) [30].
The Tinnitus Handicap Inventory (THI) was developed by Newman and Jacobson, [31] consisting of a 25-item self-administered questionnaire. For this study, the validated Portuguese version of THI was used to assess the functional, emotional, and catastrophic dimensions of tinnitus disturbance [32]. The THI total score was subdivided into 5 grades according to the severity of self-perceived annoyance, as follows: Grade 1 (0–16): Slight (only heard in quiet environments); Grade 2 (18–36): Mild (easily masked by environmental sounds and easily forgotten with activities); Grade 3 (38– 56): Moderate (noticed in the presence of background noise, although daily activities can still be performed); Grade 4 (58– 76): Severe (almost always heard, leads to disturbed sleep patterns and can interfere with daily activities); Grade 5 (78– 100): Catastrophic (Always heard, disturbed sleep patterns, difficulty with any activities) [31,32]. All assessments were performed before and after the intervention protocols.
2.3. aVNS and TENS Protocols
A point finder device (EL 11, NKL, Brusque/SC, Brazil) was used with a reference electrode to detect the low-level impedance auricular points (Figure 1a), one at the left cymba conchae, and another at the internal side of the tragus. Both sites are mainly innervated by the auricular branch of the vagus nerve [16]. With the patient side lying, the ear was cleaned using 70% alcohol solution, and disposable acupuncture needles (Dux, 0.25x15 mm, Porto Alegre/RS, Brazil) was 2-mm inserted over the detected auricular points. Two alligator electrodes’ ends were then connected to the needles to apply the electrical current. The electrical stimulation was generated with a biphasic square wave (pulse width: 250 µs, pulse frequency: 20 Hz) using a 2-channel TENS device (Neurodyn Portable, Ibramed, Amparo/SP, Brazil) for 15 min, with the needle and needle to tissue interface resistance ~4–7 kΩ (Figure 1b). Depending on the patient’s discomfort, both the frequency and the time were reduced to 15 Hz and 12 min. The subjective tolerance threshold was set as the desired level for current’s intensity.
The C2 vertebrae was located by palpation, and two 3-cm diameter reusable circular electrodes (Valutrode, Arktus, Santa Teresa do Oeste, Paraná, Brazil) were positioned on the right and left sides of C2 nerves dermatomes (Figure 2). TENS (Neurodyn Portable, Ibramed, Amparo/SP, Brazil) consisted out of 30 min of biphasic rectangular electrical current with a pulse width at 150 µs. Over the first 10 minutes, the frequency was set at 40 Hz, followed by 10 min with a frequency set at 6 Hz, and the final 10 minutes in a burst mode (burst rate of 2 Hz, and within pulse frequency of 250 Hz). The subjective tolerance threshold was set as the desired level for current’s intensity. The aVNS and the TENS protocols were simultaneously delivered to the patient.
2.4. Photobiomodulation Protocol
After the simultaneous aVNS and TENS protocols, a diode semiconductor AlGaAs 808 nm wavelength class II laser (Therapy EC, DMC, São Carlos/SP, Brazil) with a power of 100 mW was used to irradiate the ear canal (in the second curve of the canal). The duration of irradiation was 180 s resulting in an energy density of about 18 J (Figure 3a). A second irradiation on the mastoid bone for 90 s delivered 9 J at the same wavelength (Figure 3b).
2.5. Statistical Analysis
Normality and homogeneity were tested using the Shapiro-Wilk and the Levene’s tests, respectively. As the normality was not accepted, the non-parametric Wilcoxon test was used to compare the within-group differences (pre vs. post). Central tendency was reported using the median, along with minimum and maximum as dispersion measures. The frequencies of the pre vs. post ordinal classification for THI severity levels and VAS were compared using the McNemar’s test. The effect sizes (ES) were calculated using the Cohen d coefficient, qualitatively interpreted using the following thresholds: <0.2, trivial; 0.2–0.6, small; 0.6–1.2, moderate; 1.2–2.0, large; 2.0–4.0, very large; and >4.0, nearly perfect. All statistics were performed using the Jamovi software. (The Jamovi project [2021]. Version 1.6. Retrieved from https://www.jamovi.org (accessed on 11 March 2021)).
3. Results
The VAS and THI continuous and ordinal data are summarized in Table 2. The pre-VAS was significantly higher than post-VAS for both loudness and discomfort (p = 0.001; ES = 2.01 [very large] and 2.23 [very large], respectively). Also, the pre-THI score was also higher compared to post-THI score (p = 0.001; ES = 2.28 [very large]). The tinnitus severity, classified by the THI (χ² = 71.9; p = 0.001), VAS loudness (χ² = 102; p = 0.001), and VAS discomfort (χ² = 107; p = 0.001) frequencies, decreased significantly after the intervention (Figure 4 and Figure 5).
4. Discussion
The current findings suggest within-group effectiveness of combining techniques to treat tinnitus. THI and both VAS (loudness and discomfort) scores were lower after the intervention compared to their baseline values. Also, the severity frequencies were also mitigated after the treatment. Marked differences were noted for almost all patients, with very large ES for all variables.
Analyzing the average ES for each technique, other studies observed mild to moderate sizes [11,27,33]. For aVNS, a meta-analysis showed a significant moderate effect on THI (ES = 0.69; p = 0.04), but not significant on VAS loudness (ES = −0.01; p = 0.97), nor for on tinnitus discomfort (ES = 0.31; p = 0.34) [25]. A meta-analysis demonstrated improvement in THI with TENS treatment with an ES of 0.62, with a reported mean difference of −7.5 (95% confidence interval, −10.93 to −4.18; p < 0.001), and the severity of tinnitus on VAS with an ES of 0.31, with a mean difference of −0.65 (95% CI, −0.99 to −0.30; p < 0.001) [14]. For photobiomodulation, a meta-analysis returned an even smaller non-significant ES of 0.12 for THI, with a mean difference of −2.85 (95% confidence interval, −8.99 to 3.28; p = 0.362) [34]. Another recent meta-analysis analyzed the placebo effect on THI in tinnitus patients [35]. Mean difference between pre vs. posttreatment THI scores of all placebo arms was 5.6 (95% confidence interval, 3.3 to 8.0; p < 0.001). For VAS loudness, the mean difference was 0.8 (95% confidence interval, 0.0 to 1.6; p = 0.05). As noticed, the interventions’ THI and VAS mean differences are close to placebo values, suggesting an even smaller effect using the isolated techniques. In the other hand, the present study showed very large ES considering the THI scores, and the VAS loudness and discomfort, with larger mean differences for all clinical variables, suggesting a possible techniques’ synergy.
The synergistic effect might be explained by the techniques’ neurophysiological mechanism of action. The auricular branch of the vagus nerve provides afferent signals to the nucleus of the solitary tract, which communicates with the locus coeruleus and the dorsal motor nucleus of the vagus nerve [25,36]. This network modulates the autonomic nervous system, balancing parasympathetic and sympathetic activity [16,37,38]. In tinnitus, a sustained sympathetic tone can exacerbate the symptoms by increasing arousal and stress [13,19,20,38]. As the aVNS decreases this tone, while relaxation and reduced auditory hyperexcitability is provided. Later fMRI studies have demonstrated that active aVNS significantly increases neural activity in regions such as the right caudate, bilateral anterior, left prefrontal cortex, cerebellum, and mid-cingulate compared to sham stimulation, also reducing functional connectivity between the posterior cingulate cortex and the lingual gyrus; and suppressing the activity in auditory, limbic, and other brain regions associated with tinnitus generation mechanisms [22]. Additionally, vagus nerve stimulation enhances plasticity by promoting long-term potentiation or long-term depression of neural circuits, potentially normalizing abnormal auditory signals [23,39,40]. By modulating the autonomic nervous system and promoting neural plasticity, aVNS likely reduces the perception and emotional distress of tinnitus. This aligns with studies showing improvements in anxiety and emotional regulation through vagus nerve modulation [41,42].
Similarly, TENS applied to the C2 dermatome stimulates afferent somatosensory fibers, which project to the dorsal column nucleus and dorsal cochlear nucleus (DCN) [6,13]. The DCN plays a pivotal role in integrating auditory and somatosensory signals. Tinnitus enhance hyperactivity in the DCN, particularly in somatosensory tinnitus, where altered somatosensory input amplifies auditory signaling [6]. TENS enhances the inhibition, normalizing the excitation-inhibition balance and reducing tinnitus perception [42,43]. Modulation of the DCN through somatosensory pathways alleviates aberrant auditory signals. Previous studies have shown that cervical TENS improves tinnitus symptoms in cases modulated by somatosensory input [6,13,14].
Photobiomodulation uses low-level laser light to stimulate cellular activity in the cochlea and auditory nerve [28,44]. The infrared laser light (808 nm wavelength) penetrates tissues, promoting mitochondrial activity and ATP production, which enhances cellular repair and neuroprotection [27,45]. Photobiomodulation increases blood flow in the cochlear region, supporting the recovery, reducing oxidative stress, both implicated in tinnitus pathology [45,46]. By reducing oxidative stress and promoting tissue repairing, the photobiomodulation can mitigate damage associated with tinnitus [47,48]. This aligns with findings that PBM improves hearing thresholds and reduces tinnitus severity in some patients.
Other studies combined distinct types of stimulation to treat tinnitus. A recent study compared auditory stimuli (music and white noise) with and without aVNS [49]. The group with aVNS showed significantly lower THI and mismatch negativity scores compared to the group without aVNS. To treat tinnitus, a recent study combined a bimodal therapy consisted by tongue electrical stimulation with sound therapy (pure tone bursts presented binaurally), and compared to sound therapy alone [50]. The bimodal therapy showed significant better results in THI scores than sound therapy alone. Despite those promising results, a study showed no between-group significant differences for THI, VAS and quality of life scores in tinnitus patients comparing a combination of transcranial random noise stimulation (tRNS) and acoustic stimulation with wideband noise [51]. However, the within-group ES was higher for the group receiving the combination compared to the tRNS alone group. Another study also failed to demonstrate the superiority of a bimodal intervention over a single technique [52]. In this study, the first group received only music therapy, while the second group listened to binaural alpha beats merged with the music therapy. Both groups showed improvements in tinnitus, but no between-group differences were observed. The current study showed not only within-group significant differences for THI, VAS loudness and discomfort, but also a very large ES using the combined intervention, suggesting that such synergy would greatly benefit the tinnitus’ patient.
Limitations must be addressed to the present study. Due to the retrospective design, no control group was added to the present analysis. As a retrospective quasi-experimental study, the lack of randomization and blinding introduces potential biases. For example, selection bias or observer bias could influence the results. Further studies must consider the inclusion of a sham group for between-group comparison. Also due to the clinical design, the study relies heavily on self-reported measures like VAS and THI, which are subjective and prone to bias. Objective measures, such as electrophysiological data or imaging, would strengthen the findings. The study does not assess the sustainability of the observed effects. Long-term follow-up is necessary to evaluate whether the benefits persist after treatment ends. The study examines the combined effect of aVNS, TENS, and photobiomodulation but does not isolate the contribution of each technique, limiting the understanding of which component(s) drive the observed benefits.
5. Conclusions
The findings of this retrospective study suggest that a combined intervention using auricular vagus nerve stimulation, cervical transcutaneous electrical nerve stimulation (TENS), and transmeatal photobiomodulation may significantly reduce tinnitus loudness and discomfort, as well as improve the overall perceived handicap caused by tinnitus. The very large effect sizes observed in this study indicate a potential synergistic effect of the neuromodulatory techniques, surpassing the results typically achieved with isolated interventions. The combined approach could represent an important step toward improving the quality of life for patients suffering from this challenging condition.
Author Contributions
Conceptualization, B.C.B. and A.C.B.; methodology, B.R.B., A.C.B., and B.C.B.; software, K.R.F.; validation, K.R.F., L.I., and M.A.B.; formal analysis, A.C.B., K.R.F., and G.L.G.; investigation, B.C.B., and B.R.B.; resources, G.L.G., A.C.B., and B.C.B.; data curation, L.I., K.R.F., and B.C.B.; writing—original draft preparation, K.R.F., A.C.B., and B.R.B.; writing—review and editing, M.A.B., and G.L.G.; visualization, A.C.B., L.I., and B.C.B.; supervision, G.L.G., M.A.B., and A.C.B.; project administration, A.C.B.; funding acquisition, A.C.B., and G.L.G. All authors have read and agreed to the published version of the manuscript.
Funding
Throughout the duration of this study, the researchers received financial support from the Coordination for the Improvement of Higher Education Personnel (CAPES) Code 001 and from the Research Support Foundation of the State of Minas Gerais (FAPEMIG) Code APQ 02040-18.
Institutional Review Board Statement
Ethics Committee of the Federal College of Juiz de Fora (number 85801925.2.0000.5147).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data from this study will be made available upon request.
Acknowledgments
The authors thank the Department of Physical Therapy of the Federal University of Juiz de Fora for providing all resources to the Non-Invasive Laboratory.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Li, L.; Shi, H.; Wang, M. A Pilot Randomized Controlled Trial of Transcutaneous Electrical Nerve Stimulation for Patients With Acute Tinnitus. Medicine (Baltimore). 2019, 98, e13793. [Google Scholar] [CrossRef]
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus. JAMA Neurol. 2022, 79, 888. [Google Scholar] [CrossRef]
- Hesser, H.; Weise, C.; Westin, V.Z.; Andersson, G. A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Cognitive–Behavioral Therapy for Tinnitus Distress. Clin. Psychol. Rev. 2011, 31, 545–553. [Google Scholar] [CrossRef]
- Verbist, B.; Connor, S.; Farina, D. ESR Essentials: Diagnostic Strategies in Tinnitus—Practice Recommendations by the European Society of Head and Neck Radiology. Eur. Radiol. 2025. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Adhia, D.; Langguth, B. Tinnitus and Brain Stimulation. In Current Topics in Behavioral Neurosciences; 2021; Vol. 51, pp. 249–293.
- Wadhwa, S.; Jain, S.; Patil, N.; Jungade, S. Cervicogenic Somatic Tinnitus: A Narrative Review Exploring Non-Otologic Causes. Cureus 2024, 16. [Google Scholar] [CrossRef]
- Costa, W.S.M. da; Araújo, L.B. de; Bedaque, H. de P.; Ferreira, L.M. de B.M.; Ribeiro, K.M.O.B. de F. Impact of the Somatosensory Influence on Annoyance and Quality of Life of Individuals with Tinnitus: A Cross-Sectional Study. Braz. J. Otorhinolaryngol. 2025, 91, 101542. [Google Scholar] [CrossRef] [PubMed]
- Didier, H.A.; Cappellari, A.M.; Sessa, F.; Giannì, A.B.; Didier, A.H.; Pavesi, M.M.; Caria, M.P.; Curone, M.; Tullo, V.; Di Berardino, F.; et al. Somatosensory Tinnitus and Temporomandibular Disorders: A Common Association. J. Oral Rehabil. 2023, 50, 1181–1184. [Google Scholar] [CrossRef]
- Spisila, T.; Fontana, L.C.; Hamerschmidt, R.; de Cássia Cassou Guimarães, R.; Hilgenberg-Sydney, P.B. Phenotyping of Somatosensory Tinnitus and Its Associations: An Observational Cross-sectional Study. J. Oral Rehabil. 2024, 51, 2008–2018. [Google Scholar] [CrossRef]
- Malfatti, T.; Ciralli, B.; Hilscher, M.M.; Leao, R.N.; Leao, K.E. Decreasing Dorsal Cochlear Nucleus Activity Ameliorates Noise-Induced Tinnitus Perception in Mice. BMC Biol. 2022, 20, 102. [Google Scholar] [CrossRef]
- Lefebvre-Demers, M.; Doyon, N.; Fecteau, S. Non-Invasive Neuromodulation for Tinnitus: A Meta-Analysis and Modeling Studies. Brain Stimul. 2021, 14, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Rabau, S.; Shekhawat, G.S.; Aboseria, M.; Griepp, D.; Van Rompaey, V.; Bikson, M.; Van de Heyning, P. Comparison of the Long-Term Effect of Positioning the Cathode in TDCS in Tinnitus Patients. Front. Aging Neurosci. 2017, 9, 1–8. [Google Scholar] [CrossRef]
- Tutar, B.; Atar, S.; Berkiten, G.; Üstün, O.; Kumral, T.L.; Uyar, Y. The Effect of Transcutaneous Electrical Nerve Stimulation (TENS) on Chronic Subjective Tinnitus. Am. J. Otolaryngol. 2020, 41, 102326. [Google Scholar] [CrossRef] [PubMed]
- Byun, Y.J.; Lee, J.A.; Nguyen, S.A.; Rizk, H.G.; Meyer, T.A.; Lambert, P.R. Transcutaneous Electrical Nerve Stimulation for Treatment of Tinnitus: A Systematic Review and Meta-Analysis. Otol. Neurotol. 2020, 41, e767–e775. [Google Scholar] [CrossRef] [PubMed]
- Stegeman, I.; Velde, H.M.; Robe, P.A.J.T.; Stokroos, R.J.; Smit, A.L. Tinnitus Treatment by Vagus Nerve Stimulation: A Systematic Review. PLoS One 2021, 16, e0247221. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The Anatomical Basis for Transcutaneous Auricular Vagus Nerve Stimulation. J. Anat. 2020, 236, 588–611. [Google Scholar] [CrossRef]
- Ahmed, U.; Chang, Y.-C.; Zafeiropoulos, S.; Nassrallah, Z.; Miller, L.; Zanos, S. Strategies for Precision Vagus Neuromodulation. Bioelectron. Med. 2022, 8, 9. [Google Scholar] [CrossRef]
- Sun, J.; Guo, C.; Ma, Y.; Gao, S.; Luo, Y.; Chen, Q.; Hong, Y.; Hou, X.; Xiao, X.; Yu, X.; et al. Immediate Modulatory Effects of Transcutaneous Auricular Vagus Nerve Stimulation on the Resting State of Major Depressive Disorder. J. Affect. Disord. 2023, 325, 513–521. [Google Scholar] [CrossRef]
- Raj-Koziak, D.; Gos, E.; Kutyba, J.; Ganc, M.; Jedrzejczak, W.W.; Skarzynski, P.H.; Skarzynski, H. Effectiveness of Transcutaneous Vagus Nerve Stimulation for the Treatment of Tinnitus: An Interventional Prospective Controlled Study. Int. J. Audiol. 2024, 63, 250–259. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, X.; Hu, L. Transcutaneous Auricular Vagus Nerve Stimulation Facilitates Cortical Arousal and Alertness. Int. J. Environ. Res. Public Health 2023, 20, 1402. [Google Scholar] [CrossRef]
- Gianlorenco, A.C.L.; de Melo, P.S.; Marduy, A.; Kim, A.Y.; Kim, C.K.; Choi, H.; Song, J.-J.; Fregni, F. Electroencephalographic Patterns in TaVNS: A Systematic Review. Biomedicines 2022, 10, 2208. [Google Scholar] [CrossRef]
- Yap, J.Y.Y.; Keatch, C.; Lambert, E.; Woods, W.; Stoddart, P.R.; Kameneva, T. Critical Review of Transcutaneous Vagus Nerve Stimulation: Challenges for Translation to Clinical Practice. Front. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Yakunina, N.; Nam, E.-C. Direct and Transcutaneous Vagus Nerve Stimulation for Treatment of Tinnitus: A Scoping Review. Front. Neurosci. 2021, 15. [Google Scholar] [CrossRef]
- Langguth, B. Non-Invasive Neuromodulation for Tinnitus. J. Audiol. Otol. 2020, 24, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Hernando, D.; Fernández-de-las-Peñas, C.; Machado-Martín, A.; Angulo-Díaz-Parreño, S.; García-Esteo, F.J.; Mesa-Jiménez, J.A. Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis. J. Clin. Med. 2023, 12, 3673. [Google Scholar] [CrossRef]
- Vanneste, S.; Plazier, M.; Van de Heyning, P.; De Ridder, D. Transcutaneous Electrical Nerve Stimulation (TENS) of Upper Cervical Nerve (C2) for the Treatment of Somatic Tinnitus. Exp. Brain Res. 2010, 204, 283–287. [Google Scholar] [CrossRef]
- Nikookam, Y.; Zia, N.; Lotfallah, A.; Muzaffar, J.; Davis-Manders, J.; Kullar, P.; Smith, M.E.; Bale, G.; Boyle, P.; Irving, R.; et al. The Effect of Photobiomodulation on Tinnitus: A Systematic Review. J. Laryngol. Otol. 2024, 138, 710–731. [Google Scholar] [CrossRef]
- Demirkol, N.; Usumez, A.; Demirkol, M.; Sari, F.; Akcaboy, C. Efficacy of Low-Level Laser Therapy in Subjective Tinnitus Patients with Temporomandibular Disorders. Photomed. Laser Surg. 2017, 35, 427–431. [Google Scholar] [CrossRef]
- Choi, J.E.; Lee, M.Y.; Chung, P.-S.; Jung, J.Y. A Preliminary Study on the Efficacy and Safety of Low Level Light Therapy in the Management of Cochlear Tinnitus: A Single Blind Randomized Clinical Trial. Int. Tinnitus J. 2019, 23, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, L.S.; Lozza, L.; Marchiori, D.M.; Almeida, D. De; Ciquinato, S.; Teixeira, D.D.C. Inflammatory Biomarkers and Tinnitus in Older Adults. 2024, 535–542. [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. - Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Paula Erika Alves, F.; Cunha, F.; Onishi, E.T.; Branco-Barreiro, F.C.A.; Ganança, F.F. Tinnitus Handicap Inventory: Cross-Cultural Adaptation to Brazilian Portuguese. Pro. Fono. 2005, 17, 303–310. [Google Scholar] [CrossRef]
- Lee, H.J.; Park, J.S.; Yang, H.W.; Shin, J.W.; Han, J.W.; Kim, K.W. A Normative Study of the Gait Features Measured by a Wearable Inertia Sensor in a Healthy Old Population. Gait Posture 2023, 103, 32–36. [Google Scholar] [CrossRef]
- Chen, C.-H.; Huang, C.-Y.; Chang, C.-Y.; Cheng, Y.-F. Efficacy of Low-Level Laser Therapy for Tinnitus: A Systematic Review with Meta-Analysis and Trial Sequential Analysis. Brain Sci. 2020, 10, 931. [Google Scholar] [CrossRef]
- Walters, R.K.; Durrant, F.G.; Nguyen, S.A.; Meyer, T.A.; Lambert, P.R. The Placebo Effect on Tinnitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Otol. Neurotol. 2024, 45, e263–e270. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.Y.; Marduy, A.; de Melo, P.S.; Gianlorenco, A.C.; Kim, C.K.; Choi, H.; Song, J.-J.J.; Fregni, F. Safety of Transcutaneous Auricular Vagus Nerve Stimulation (TaVNS): A Systematic Review and Meta-Analysis. Sci. Rep. 2022, 12, 22055. [Google Scholar] [CrossRef] [PubMed]
- Clancy, J.A.; Mary, D.A.; Witte, K.K.; Greenwood, J.P.; Deuchars, S.A.; Deuchars, J. Non-Invasive Vagus Nerve Stimulation in Healthy Humans Reduces Sympathetic Nerve Activity. Brain Stimul. 2014, 7, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, M.; Wienke, C.; Betts, M.J.; Zaehle, T.; Hämmerer, D. Current Challenges in Reliably Targeting the Noradrenergic Locus Coeruleus Using Transcutaneous Auricular Vagus Nerve Stimulation (TaVNS). Auton. Neurosci. 2021, 236, 102900. [Google Scholar] [CrossRef]
- Keute, M.; Gharabaghi, A. Brain Plasticity and Vagus Nerve Stimulation. Auton. Neurosci. Basic Clin. 2021, 236, 102876. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Mrudula, K.; Sreepada, S.S.; Sathyaprabha, T.N.; Pal, P.K.; Chen, R.; Udupa, K. An Overview of Noninvasive Brain Stimulation: Basic Principles and Clinical Applications. Can. J. Neurol. Sci. / J. Can. des Sci. Neurol. 2022, 49, 479–492. [Google Scholar] [CrossRef]
- Ferreira, L.M.A.; Brites, R.; Fraião, G.; Pereira, G.; Fernandes, H.; de Brito, J.A.A.; Pereira Generoso, L.; Maziero Capello, M.G.; Pereira, G.S.; Scoz, R.D.; et al. Transcutaneous Auricular Vagus Nerve Stimulation Modulates Masseter Muscle Activity, Pain Perception, and Anxiety Levels in University Students: A Double-Blind, Randomized, Controlled Clinical Trial. Front. Integr. Neurosci. 2024, 18. [Google Scholar] [CrossRef]
- Zhang, H.; Shan, A.; Wan, C.; Cao, X.; Yuan, Y.; Ye, S.; Gao, M.; Gao, L.; Tong, Q.; Gan, C.; et al. Transcutaneous Auricular Vagus Nerve Stimulation Improves Anxiety Symptoms and Cortical Activity during Verbal Fluency Task in Parkinson’s Disease with Anxiety. J. Affect. Disord. 2024, 361, 556–563. [Google Scholar] [CrossRef]
- Gerges, A.N.H.; Graetz, L.; Hillier, S.; Uy, J.; Hamilton, T.; Opie, G.; Vallence, A.; Braithwaite, F.A.; Chamberlain, S.; Hordacre, B. Transcutaneous Auricular Vagus Nerve Stimulation Modifies Cortical Excitability in Middle-aged and Older Adults. Psychophysiology 2024, 1–14. [Google Scholar] [CrossRef]
- Silva, M.R.; Scheffer, A.R.; de Assunção Bastos, R.S.; Chavantes, M.C.; Mondelli, M.F.C.G. The Effects of Photobiomodulation Therapy in Individuals with Tinnitus and without Hearing Loss. Lasers Med. Sci. 2022, 37, 3485–3494. [Google Scholar] [CrossRef]
- Dole, M.; Auboiroux, V.; Langar, L.; Mitrofanis, J. A Systematic Review of the Effects of Transcranial Photobiomodulation on Brain Activity in Humans. Rev. Neurosci. 2023, 34, 671–693. [Google Scholar] [CrossRef]
- Pruitt, T.; Wang, X.; Wu, A.; Kallioniemi, E.; Husain, M.M.; Liu, H. Transcranial Photobiomodulation (TPBM) With 1,064-Nm Laser to Improve Cerebral Metabolism of the Human Brain In Vivo. Lasers Surg. Med. 2020, 52, 807–813. [Google Scholar] [CrossRef]
- Vargas, E.; Barrett, D.W.; Saucedo, C.L.; Huang, L. Da; Abraham, J.A.; Tanaka, H.; Haley, A.P.; Gonzalez-Lima, F. Beneficial Neurocognitive Effects of Transcranial Laser in Older Adults. Lasers Med. Sci. 2017, 32, 1153–1162. [Google Scholar] [CrossRef]
- Ferraresi, C.; Huang, Y.Y.; Hamblin, M.R. Photobiomodulation in Human Muscle Tissue: An Advantage in Sports Performance? J. Biophotonics 2016, 9, 1273–1299. [Google Scholar] [CrossRef] [PubMed]
- Bolandi, M.; Javanbakht, M.; Shaabani, M.; Bakhshi, E. Effectiveness of Bimodal Stimulation of the Auditory-Somatosensory System in the Treatment of Tonal Tinnitus. Am. J. Otolaryngol. 2024, 45, 104449. [Google Scholar] [CrossRef] [PubMed]
- Boedts, M.; Buechner, A.; Khoo, S.G.; Gjaltema, W.; Moreels, F.; Lesinski-Schiedat, A.; Becker, P.; MacMahon, H.; Vixseboxse, L.; Taghavi, R.; et al. Combining Sound with Tongue Stimulation for the Treatment of Tinnitus: A Multi-Site Single-Arm Controlled Pivotal Trial. Nat. Commun. 2024, 15, 6806. [Google Scholar] [CrossRef]
- Emadi, M.; Faraji, R.; Hamidi Nahrani, M.; Heidari, A. Effect of Simultaneous Use of Neuromodulation and Acoustic Stimulation in the Management of Tinnitus. Indian J. Otolaryngol. Head Neck Surg. 2024, 76, 5495–5499. [Google Scholar] [CrossRef]
- Bakhtarikia, S.; Tavanai, E.; Rouhbakhsh, N.; Sayadi, A.J.; Sabet, V.K. Investigating the Effectiveness of Music Therapy Combined with Binaural Beats on Chronic Tinnitus: A Randomized Controlled Trial. Am. J. Otolaryngol. 2024, 45, 104308. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The aVNS protocol: a. point finder device locating the low-level impedance points; b. electrical stimulation using the percutaneous vagus nerve stimulation.
Figure 1.
The aVNS protocol: a. point finder device locating the low-level impedance points; b. electrical stimulation using the percutaneous vagus nerve stimulation.
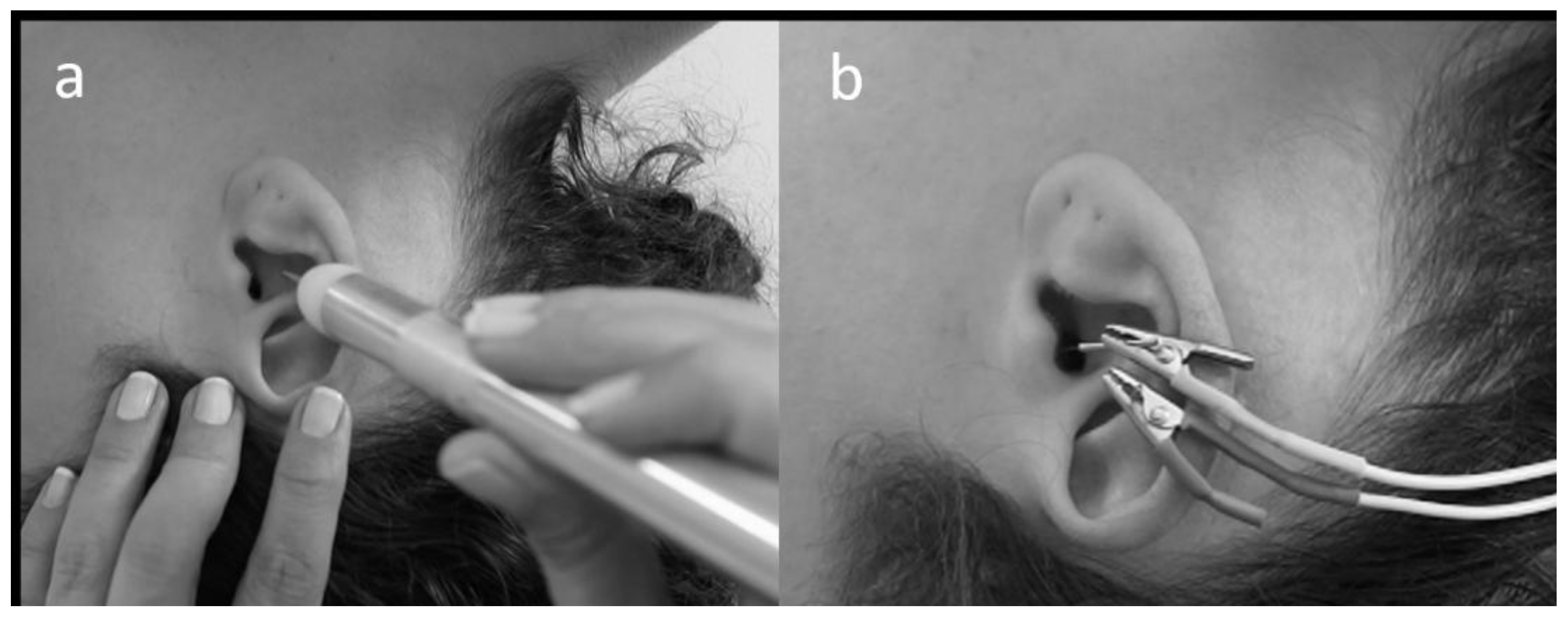
Figure 2.
TENS protocol: C2 electrodes positioning.
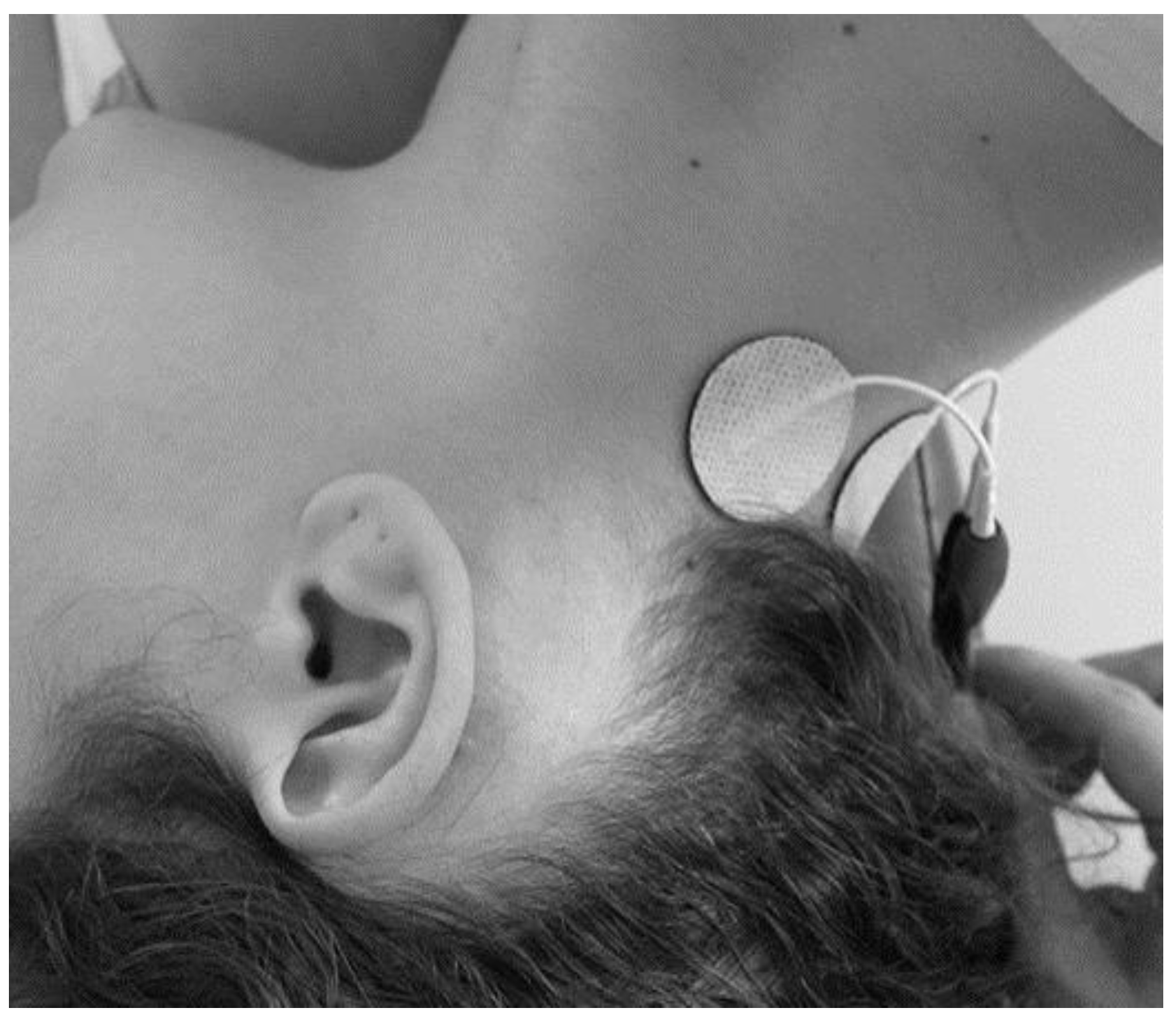
Figure 3.
Photobiomodulation protocol: a. transmeatal laser irradiation; b. mastoid irradiation.
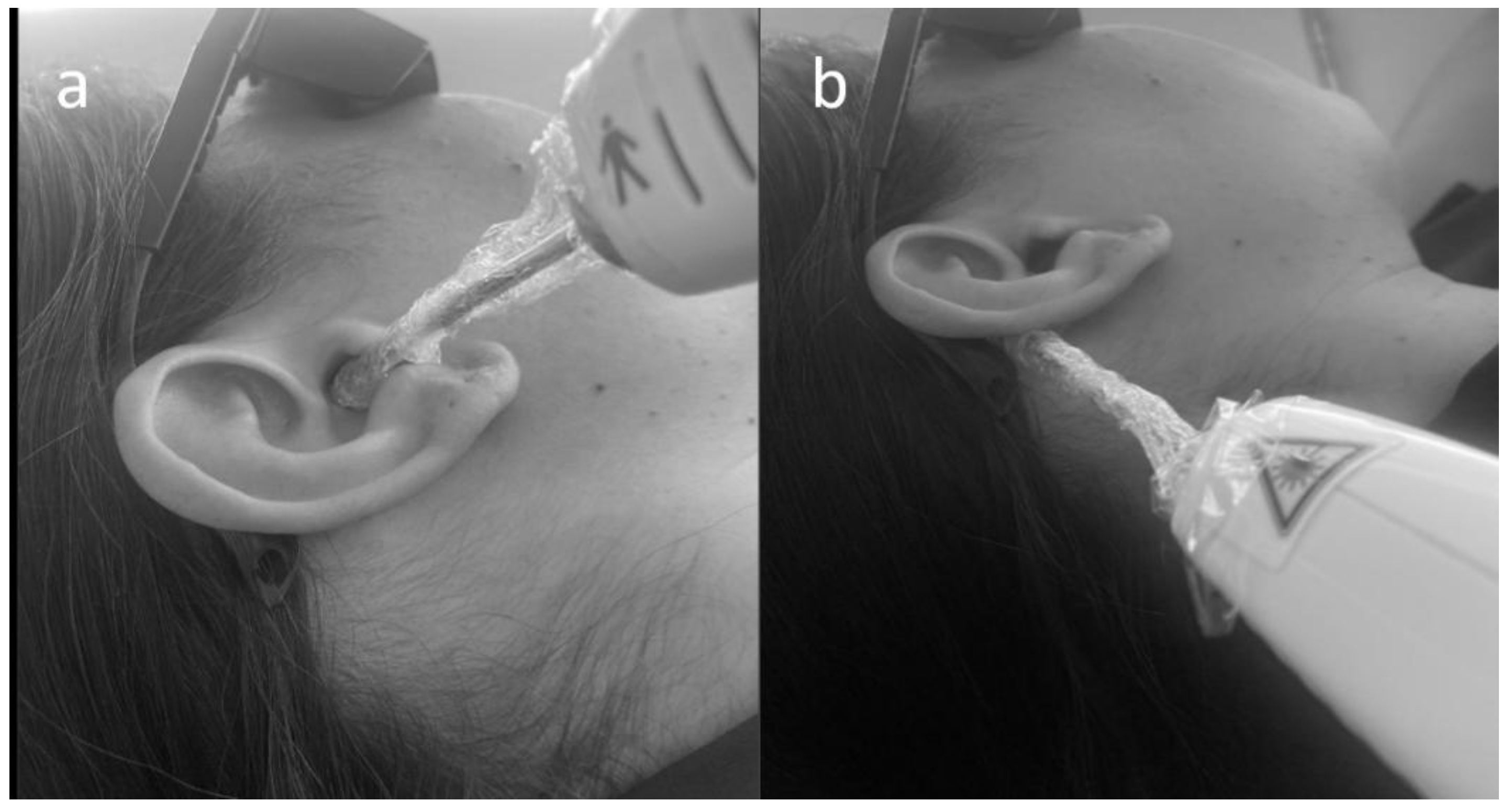
Figure 4.
THI frequencies at baseline and post-intervention.
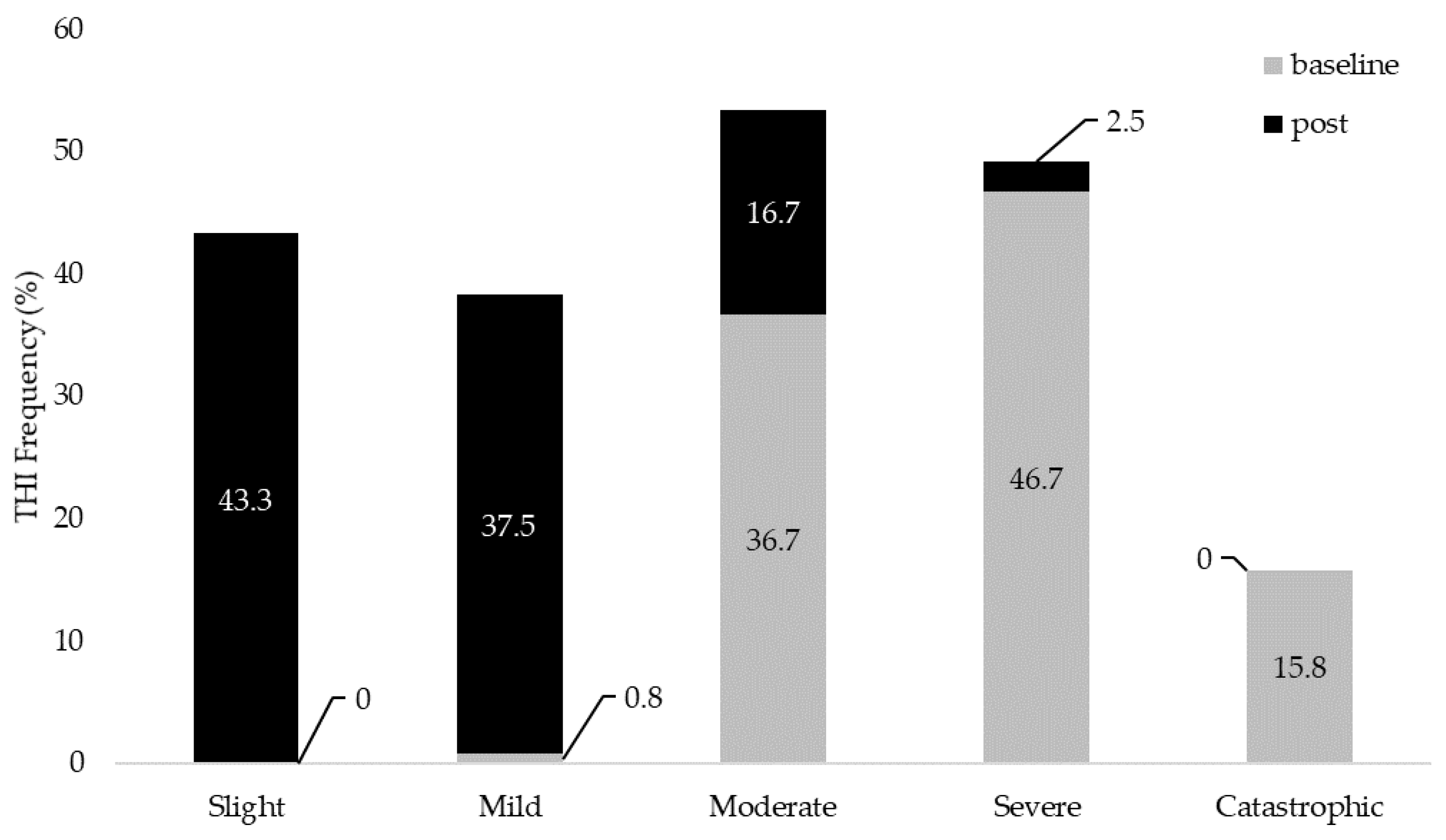
Figure 5.
VAS frequencies (Discomfort and Loudness) at baseline and post-intervention.
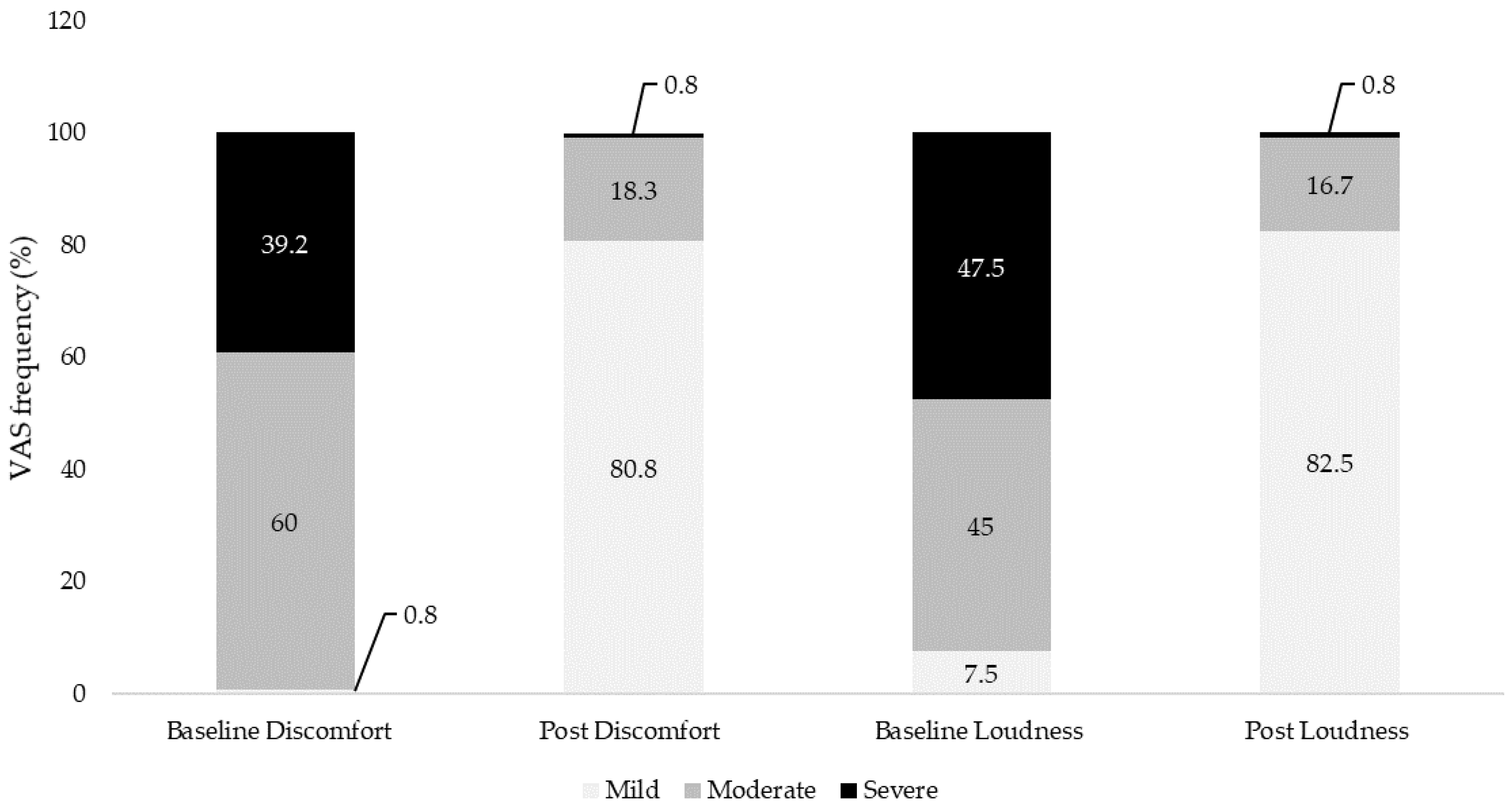

Table 1.
Participants’ characteristics.
| Characteristic | Value |
| Age | |
| Mean (SD) | 50.51 (12.88) |
| Med (Min; Max) | 49 (26;78) |
| Gender (n) | |
| Male (%) | 66 (55%) |
| Female (%) | 54 (45%) |
| Hearing loss | |
| No loss | 58 (48.3%) |
| Mild | 42 (35%) |
| Moderate | 20 (16.7%) |
| Laterality | |
| Right | 17 (18.9%) |
| Left | 18 (20%) |
| Bilateral | 55 (61%) |
| Duration of Tinnitus (months) | |
| < 6 | 4 (3.3%) |
| 6 | 14 (11.7%) |
| 7-12 | 43 (35.8%) |
| 13-24 | 20 (16.7%) |
| > 24 | 39 (32.5%) |
Table 2.
Tinnitus Handicap Inventory (THI) and Visual Analogue Scale (VAS) discomfort and loudness continuous and ordinal data.
Table 2.
Tinnitus Handicap Inventory (THI) and Visual Analogue Scale (VAS) discomfort and loudness continuous and ordinal data.
| Outcome |
THI baseline |
THI post |
VASdiscomfort baseline |
VASdiscomfort post |
VASloudness baseline |
VASloudness post |
|
| Median (min;max) | 62 (36;90) | 18 (0;68) | 7 (2;10) | 1 (0;7) | 7 (3;10) | 2 (0;7) | |
| Frequency n (%) |
Slight | 0 | 52 (43.3%) | N/A | N/A | N/A | N/A |
| Mild | 1 (0.8%) | 45 (37.5%) | 1 (0.8%) | 97 (80.8%) | 9 (7.5%) | 99 (82.5%) | |
| Moderate | 44 (36.7%) | 20 (16.7%) | 72 (60%) | 22 (18.3%) | 54 (45%) | 20 (16.7%) | |
| Severe | 56 (46.7%) | 3 (2.5%) | 47 (39.2%) | 1 (0.8%) | 57 (47.5%) | 1 (0.8%) | |
| Catastrophic | 19 (15.8%) | 0 | N/A | N/A | N/A | N/A | |
Legend: N/A = not applicable.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



