
Submitted:
25 September 2025
Posted:
26 September 2025
You are already at the latest version
Abstract
Diabetic retinopathy (DR) is a major microvascular complication of diabetes and a leading cause of vision loss in working-age adults worldwide. The pathophysiology of DR is complex and involves oxidative stress, inflammation, retinal pigment epithelium (RPE) dysfunction, and abnormal angiogenesis. Recent insights into the molecular mechanisms underlying DR have opened new avenues for targeted and personalized therapeutic strategies. In this review, we examine the advances in the understanding of oxidative damage, RPE impairment, and proangiogenic signaling in DR progression. We also highlight emerging treatment modalities, including anti-VEGF agents, gene therapy, and nutraceutical interventions. Future directions emphasize the integration of omics technologies and precision medicine approaches for individualized management. This work provides a critical synthesis of recent findings and identifies promising avenues for research and clinical intervention in DR.
Keywords:
diabetic retinopathy
; oxidative stress
; angiogenesis
; retinal pigment epithelium
; precision medicine
; targeted therapy
1. Diabetic Retinopathy (DR)
Current worldwide estimations show that near to 463 million of adults suffer from diabetes, with a projected increased prevalence of 693 million by 2045, making it a condition of serious public health concern [1,2]. Prevalences of children and adolescents with diabetes have been increasing, with estimations of more than one million children and adolescents below 20 years diagnosed with type 1 diabetes [2].
Diabetes is one of the top 10 leading causes of global death, that negatively affects improvements in life expectancy [3]. There is evidence that shows that diabetes is associated with an increased mortality from infections, cardiovascular disease, stroke, chronic kidney disease, chronic liver disease, and cancer [3,4,5,6].
Diabetes is a chronic condition characterized by high levels of glucose in blood, due to insulin production that could be non-existent, insufficient or wrongly utilized [7]. In addition to hyperglycemia, diabetes may be accompanied by dyslipidemia and neurovascular damage [7,8].
Hyperglycemia effects may develop microvascular (that includes retinopathy, nephropathy, and neuropathy) and macrovascular complications (that involves ischemic heart disease, peripheral vascular disease, and cerebrovascular disease) [9]. Increases in protein glycation can affect tissues, in diabetic retinopathy, this process generates apoptosis of retinal pericytes, overproduction of endothelial growth factors, increased neovascularization, and vascular inflammation, contributing to an elevated risk of microthrombosis formation, capillary blockage, and retinal ischemia [10].
One of the most common microvascular complications is diabetic retinopathy, which affects nearly 103 million of adult population with diabetes, and has a predicted increased prevalence of 160 million by 2045 [1].
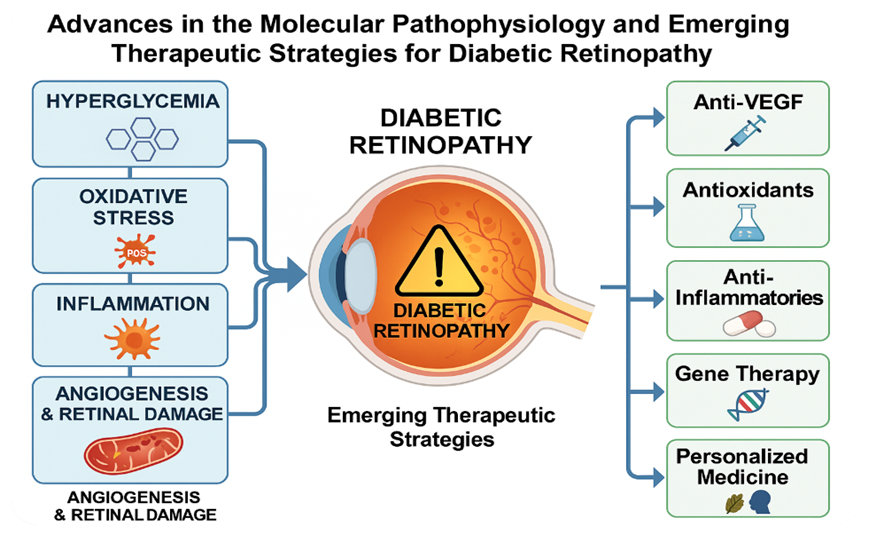
Diabetic retinopathy is a chronic, progressive, and multifactorial disease affecting the retinal microvasculature. Figure 1 shows the molecular pathways in DR.
Hyperglycemia-induced metabolic disturbances lead to pericyte loss, endothelial dysfunction, and blood-retinal barrier (BRB) breakdown, ultimately resulting in retinal ischemia and neovascularization [11]. Retinal lesions, that are used to classify eyes as having one of the conditions in the categories of DR, are microaneurysms (small balloon-like bulges or tiny dots in the blood vessels in the retina), hemorrhages, venous beading (dilation and constriction of venular walls, resulting in changes of venous caliber), intraretinal microvascular abnormalities, hard exudates (yellow-white deposits, composed by leaked lipids and lipoproteins from the blood vessels), and retinal neovascularization (abnormal growing of new, often fragile, blood vessels that may be prone to bleeding) [12,13,14,15]. Diabetic retinopathy can be broadly categorized into non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR) stages, with diabetic macular edema (DME) being a significant cause of visual impairment in both [13].
Non-proliferative diabetic retinopathy consists in the presence of many usual DR lesions, with the absence of neovascularization. This condition includes different stages, where the eyes can progress from no DR through mild, moderate and severe NPDR. Proliferative Diabetic Retinopathy is the most advanced stage of DR, characterized by the presence of neovascularization, and considered an angiogenic response to the reduction or interruption of blood flow of retina blood vessels [13]. The most common classification system for DR is the International Classification of DR scale [16], that locates the different stages of NPDR and PDR (Table 1).
An optimal identification of DR severity stages is crucial to predict the risk of worsening DR and visual loss risk, and thus helps by giving directions to determine an appropriate referral, follow-up and treatment recommendations [13,17,18]. Usual recommendations on eye examinations for people diagnosed with type 2 diabetes without DR consist of an initial examination at the time of type 2 diabetes diagnosis, followed by an annual dilated eye examination. For people with type 1 diabetes diagnosis without DR, eyes should be initially examined five years after type 1 diabetes diagnosis and must have yearly ophthalmic examination [17].
2. Diabetic Retinopathy in the Context of Other Eye Diseases
The growing global burden of diabetes mellitus (DM) as the population ages is accompanied by a high prevalence of not only diabetic retinopathy (DR), but also other eye diseases associated with pathology of internal organs [19,20]. At the same time, although DR is the most specific complication of chronic hyperglycemia, people with DM may experience other eye diseases associated with this pathology such as cataracts, glaucoma, age-related macular degeneration (AMD), retinal vascular occlusion, and acute ischemic optic neuropathy, which collectively impairs vision in people with DM. especially in old age [21].
Based on the literature data, cataracts, glaucoma, age-related macular degeneration (AMD), etc. are among the main causes of visual impairment worldwide [20]. The question of whether there is a link between diabetes and most eye diseases has been the subject of controversy in the past, when little attention was paid to the general aging of mankind [22]. In the current situation, due to the aging of the population, diabetic patients began to develop age-related eye diseases more often, leading to visual impairment, while previously they died prematurely from cardiovascular complications [23]. In addition, the latest technological and therapeutic innovations both in the field of diabetes treatment and in ophthalmology require updating existing knowledge about the eye condition in patients with diabetes. Currently, there is no doubt that diabetes itself and long-term chronic hyperglycemia, against the background of sharp fluctuations in glucose levels, initiates the manifestation of numerous eye diseases (Table 2).
Thus, prolonged hyperglycemia promotes the accumulation of reactive oxygen species and reduces the antioxidant function of the aging retina, thereby accelerating the development of other diseases. Aging also causes mitochondrial dysfunction, which in turn contributes to the accumulation of reactive oxygen species, followed by apoptosis of trabecular meshwork cells. These processes increase the resistance to the outflow of intraocular fluid, which leads to a pathological increase in intraocular pressure and the development of glaucoma.
At the same time, the combination of aging and inflammation factors is accompanied by destabilization of the tear film, making it hyperosmotic and triggering a vicious cycle of inflammation in dry eye syndrome, which exacerbates the course of the disease [19]. Inhibitors or drugs that affect these processes, such as aldose reductase inhibitors, antioxidants, natural flavonoid compounds, and nanotechnology-based drugs, show promising prospects in the prevention and treatment of diabetic cataracts [24].
Early detection and correction of metabolic and inflammatory factors can also contribute to the development of effective strategies for the prevention of cataract development in the elderly. A Wisconsin epidemiological study by Dr. showed that the 10-year risk of developing cataracts ranges from 8.3% to 24.8% in type 1 and type 2 diabetics, respectively [23].
Aging causes mitochondrial dysfunction, which in turn contributes to the accumulation of reactive oxygen species, causing apoptosis of trabecular meshwork cells. These processes increase the resistance to the outflow of intraocular fluid, which leads to a pathological increase in intraocular pressure and the development of glaucoma. Thus, elderly people who control diabetes are significantly less likely to develop glaucoma, DR, or AMD than those who have not been diagnosed or controlled with diabetes [25]. In the English study, patients with controlled diabetes had a 1.29-fold higher adjusted chance of developing glaucoma (95% CI 1.01-1.65) than those without diabetes. The adjusted odds of developing diabetic eye disease were 1.20 times higher (95% CI 1.00-1.45) in individuals with uncontrolled DM; and the adjusted odds of developing AMD were 1.38 times higher (95% CI 1.04 -1.82) among individuals with undiagnosed DM [19].
Noteworthy are works demonstrating a common genetic correlation between DR, AMD, glaucoma, retinal detachment, and myopia. The revealed genetic correlation of common single nucleotide polymorphisms characterizes the significant commonality of the genetic structure of these diseases and their genetic relationship between AMD, DR, and glaucoma [26].
Studies conducted in recent years confirm the existence of a correlation between the gut, microbiota, and eyes, suggesting the concept of the "gut-eye" axis, which is involved in the pathogenesis of major eye diseases, including AMD, uveitis, etc., dry eye syndrome, and glaucoma [27].
Thus, eye diseases can have common clinical symptoms and epidemiological comorbidity and simultaneously cause age-related macular degeneration (AMD), glaucoma, and diabetic retinopathy (DR) [28].
Based on the conducted studies, it can be assumed that the presence of common pathogenetic mechanisms in the most common eye diseases, such as inflammation, genetic correlations, dysbiosis, abnormal angiogenesis, gives grounds to express an opinion on the possibility of general preventive and therapeutic measures that can prevent or slow down the occurrence and progression of a common pathology. In this regard, there is an assumption about the possibility of introducing the term "chronic eye disease" if the patient has a combined pathology in the elderly and senile, especially since there is already a similar precedent in clinical medicine as "chronic kidney disease". This will make it possible to quickly and fully utilize all the advantages of comprehensive prevention and treatment of combined eye pathology, especially in the elderly with a wide range of somatic pathologies, including diseases of the cardiovascular system, digestive organs, and systemic pathology, including diseases directly or indirectly related to metabolic syndrome.
3. Oxidative Stress
Oxidative stress is a central contributor to DR pathogenesis (Figure 2). Oxidative stress is the reduced capacity of human body to neutralize the imbalanced production of reactive oxygen species (ROS), which are damaging molecules. ROS can harm the tissues in and around the retinal blood vessels, promoting the development of DR. It has been stablished that four key metabolic disturbances are linked to oxidative stress caused by hyperglycemia in the retina: the activation of the protein kinase C (PKC) signaling pathway, increased activity in the polyol pathway, stimulation of the hexosamine pathway, and formation of advanced glycation end products (AGEs) inside cells [29].
Chronic hyperglycemia enhances mitochondrial superoxide production, triggering downstream pro-inflammatory and pro-apoptotic pathways [30]. Reactive oxygen species (ROS) activate the NF-κB pathway, increase cytokine release (e.g., IL-1β, TNF-α), and disrupt tight junctions in retinal endothelial cells [31]. NADPH oxidase (NOX) enzymes and advanced glycation end-products (AGEs) also amplify oxidative damage, creating a vicious cycle of cellular injury [32].
4. Retinal Pigment Epithelium (RPE)
Although traditionally associated with outer retina function, RPE cells are increasingly recognized as active participants in DR. Hyperglycemia induces oxidative damage and mitochondrial dysfunction in RPE cells, leading to impaired phagocytosis of photoreceptor outer segments and increased secretion of angiogenic factors such as VEGF [33]. RPE dysfunction disrupts the outer BRB and facilitates photoreceptor degeneration.
5. Angiogenesis
Angiogenesis in DR is predominantly driven by hypoxia-induced overexpression of vascular endothelial growth factor (VEGF). This growth factor increases vascular permeability and promotes neovascularization [34], which characterizes PDR. The HIF-1α/VEGF axis is a major therapeutic target. Anti-VEGF agents (e.g., ranibizumab, aflibercept, bevacizumab) are now first-line treatments for DME and PDR [35,36]. However, incomplete responses and resistance highlight the need for alternative angiogenic modulators like angiopoietin-2 inhibitors and integrin antagonists [37]. In addition to VEGF, there are other angiogenic factors such as platelet-derived growth factor (PDGF) and fibroblast growth factor (FGF). Platelet-derived growth factors comprise a group of signaling proteins that regulate cell proliferation and tissue growth. Upon activation, platelets, smooth muscle cells, endothelial cells, and activated macrophages release PDGFs, which play essential roles in embryonic vasculogenesis and in directing mesenchymal cell migration, proliferation, and chemotaxis [38]. There is evidence in animal models that shows increased retinal angiogenesis due to augmented levels of PDGF-BB in diabetic retinal cells [39]. Fibroblast growth factors involves 23 members of a family (FGF 1-23) that have a crucial role on the regulation of metabolic balance and cell biological processes related to some chronic diseases, such as diabetes, obesity, chronic kidney disease, cancer, among others [40]. In DR, FGF-16 is involved in the regulation of high glucose-induced glomerular endothelial cell dysfunction and cell proliferation [41,42].
6. Current Treatment of DR
Laser Treatment: Panretinal photocoagulation (PRP) is the most widely employed conventional laser therapy for diabetic retinopathy, with well-established long-term efficacy in preserving retinal and choroidal neurovascular integrity [43].The therapeutic effect of retinal laser treatment is based on the induction of thermal damage and protein denaturation in pigment-containing target tissues via light absorption, leading to permanent chorioretinal scarring whose extent and healing dynamics are determined by the intensity of the applied laser energy.
Retinal laser photocoagulation primarily exerts its therapeutic effect by reducing photoreceptor-mediated oxygen consumption, thereby increasing oxygen diffusion from the choriocapillaris through glial scarring to the inner retina, which alleviates hypoxia, downregulates vasoactive mediators such as VEGF and PKC, inhibits neovascularization, reduces capillary hydrostatic pressure and retinal edema, and facilitates direct choroidal oxygen delivery [44,45].
A secondary proposed mechanism of retinal laser photocoagulation suggests that the therapy reduces levels of pro-angiogenic stimuli by selectively ablating cells involved in neovascular signaling, while concurrently promoting the release of anti-angiogenic factors (like TGF-β, EPO, and PEDF) from the scar tissue formed during retinal repair [46,47,48]. Additionally, conventional focal laser treatment for retinal edema is thought to seal leaking microaneurysms, thereby limiting cytokine-mediated inflammation and facilitating macular edema reabsorption, whereas grid laser photocoagulation may alleviate macular edema by enhancing retinal oxygenation, relieving hypoxia, and inducing retinal artery dilation through decreased autoregulatory tone [48].
Long-term use of conventional laser photocoagulation has been associated with significant adverse effects, including permanent retinal scarring, iatrogenic macular edema from excessive thermal injury, choroidal detachment, peripheral visual field loss, delayed dark adaptation, and atrophic creep [49]; to address these limitations, modern laser systems have introduced refinements in pulse duration, wavelength, and spot size to improve precision and safety [50,51,52].
Technological advancements have led to the development of various clinical laser and delivery platforms aimed at enhancing the precision and safety of retinal therapies. Endpoint management algorithms now allow for fine-tuned control of laser energy relative to titration thresholds, enabling delivery of subvisible retinal burns with high accuracy [53]. Additionally, image-guided systems, such as navigational lasers, integrate fundus imaging with laser delivery devices to facilitate highly targeted and predetermined photocoagulation, particularly in the treatment of diabetic macular edema [54].
Despite the widespread use of anti-VEGF and corticosteroid agents for DR and DME, laser photocoagulation remains a valuable therapeutic option due to its cost-effectiveness, durability, and reduced dependency on frequent follow-up in real-world clinical settings. Conventional approaches such as PRP provide long-term efficacy and help prevent progression to vision-threatening complications like vitreous hemorrhage and neovascular glaucoma, while also decreasing the frequency of anti-VEGF injections in combined therapies [48]. However, conventional laser treatment (characterized by long pulse durations) can induce adverse effects including retinal scarring, subretinal fibrosis, inflammation, visual field loss, and transient VEGF upregulation, potentially exacerbating DME; these limitations highlight the need for combination regimens and further development of advanced laser platforms that minimize collateral damage and optimize visual outcomes [55].
Surgical Treatment: Vitrectomy is a key surgical intervention for managing advanced stages of DR, particularly in cases involving intravitreal hemorrhage or tractional and rhegmatogenous retinal detachment. The procedure involves removal of the vitreous gel, along with blood and fibrovascular membranes, to relieve retinal traction and inhibit vitreoretinal proliferation, ultimately aiming to preserve or stabilize visual function. In less complex cases, such as non-clearing vitreous hemorrhage with minimal fibrovascular proliferation and posterior vitreous detachment, a straightforward vitrectomy may suffice; however, more extensive pathology affecting the macula requires complex surgical planning and technique [56].
Over recent decades, vitrectomy techniques have evolved significantly, shifting from traditional 20G systems to minimally invasive 23/25/27G platforms equipped with 3D visualization and wide-angle viewing systems like Resight® [57,58,59]. These advances have allowed for smaller incisions, reduced surgical trauma, greater cutting efficiency, and improved intraoperative visualization, thereby enhancing safety and outcomes. Additionally, preoperative intravitreal administration of anti-VEGF agents in complex PDR cases has been shown to reduce intra and postoperative bleeding, decrease the need for intraoperative electrocoagulation, shorten operative time, and lower complication rates [60,61].
Despite these technological improvements, some patients still experience suboptimal visual recovery following vitrectomy. Membrane peeling can lead to intraoperative bleeding or iatrogenic retinal injury, and postoperative complications such as paracentral acute middle maculopathy, intraocular inflammation, neovascular glaucoma, and vitreous rebleeding may occur. Combining vitrectomy with intravitreal injections of anti-VEGF agents or corticosteroids has demonstrated potential in optimizing perioperative conditions, reducing retinal fibrosis, and minimizing postoperative complications, representing a promising strategy for improving overall surgical outcomes in DR patients [56,61,62,63].
In proliferative diabetic retinopathy, the posterior hyaloid membrane has a key role in the formation of fibrovascular membranes and the development of retinal traction and further - retinal detachment. Observational studies have shown that the cases with complete posterior vitreous detachment patients have a lower risk of neovascularization progression, while the preserved posterior hyaloid membrane contributes to traction and the growth of new vessels [64].
That suggests that vitrectomy in cases with early signs of proliferative activity may provide better functional results and reduce the incidence of severe complications compared to delayed surgical treatment. Induction and removal of the posterior hyaloid membrane in the early stages is considered a preventive measure that can reduce the risk of tractional detachment and the progression of PDR to advanced stages [65].
Intravitreal Corticosteroids: Corticoids exert broad anti-inflammatory effects by reducing vascular permeability, suppressing the transcription of pro-inflammatory cytokines, and modulating the activity of fibroblasts and endothelial cells, thereby limiting tissue edema and neovascular processes in inflammatory and ischemic retinal conditions [66]. Corticosteroids, particularly Intravitreal triamcinolone acetonide, has been utilized in the treatment of DME due to its strong anti-inflammatory and anti-angiogenic properties, with multiple randomized controlled trials reporting significant improvements in retinal thickness and visual acuity [67,68,69]. However, many of these studies were limited by small sample sizes and short follow-up durations, and the treatment has been associated with notable adverse effects, including increased intraocular pressure, cataract progression, and risk of intraocular infection [70].
Recent advances in sustained intraocular drug delivery have led to the development of intravitreal and retinal implants for DME, offering prolonged therapeutic effects [70]. In a randomized controlled trial, the surgically implanted fluocinolone acetonide device (Retisert) demonstrated significantly greater DME resolution and visual acuity improvement at 3 years compared to standard care; however, it was associated with high rates of cataract formation and glaucoma, with 5% of patients requiring implant removal [71].
Intravitreal Antiangiogenesis Agents: Vascular endothelial growth factor (VEGF), particularly the VEGF-A isoform, plays a central role in the pathophysiology of DR and DME by promoting endothelial cell proliferation, migration, vascular leakage, and pathological angiogenesis in hypoxic retinal tissues. VEGF-A is considered the most potent angiogenic factor among the VEGF family and is critically upregulated in response to retinal ischemia and hyperpermeability, making it a key therapeutic target in DR management [72,73,74,75].
Intravitreal anti-VEGF agents (including ranibizumab, aflibercept, and bevacizumab) have become first-line treatments for DME and proliferative DR due to their ability to inhibit abnormal neovascularization and reduce vascular leakage . Clinical trials have demonstrated their efficacy in improving visual acuity and reducing macular thickness. Pegaptanib, an agent targeting the VEGF165 isoform, showed significant visual and anatomical benefits in DME patients, with a low incidence of serious adverse events [76,77,78]. Similarly, ranibizumab and bevacizumab, originally developed for neovascular age-related macular degeneration (AMD), have shown promising results in DME and DR, with ongoing trials evaluating their comparative effectiveness and safety profiles [75].
Despite their clinical efficacy, concerns remain regarding systemic safety (particularly for off-label agents like bevacizumab) and the need for repeated intravitreal injections poses challenges in long-term disease management [79]. Combination therapies with laser photocoagulation are being explored to reduce injection frequency and improve outcomes. Overall, anti-VEGF therapy represents a cornerstone in the current treatment paradigm for DR and DME [70,75].
7. What Is Next for DR? Future Directions: Personalized Medicine and Targeted Therapies
With advancements in genomics, transcriptomics, and metabolomics, personalized medicine is emerging as a promising paradigm. Individual genetic variations (e.g., SNPs in VEGF, RAGE, and HIF1A genes) influence DR susceptibility and treatment response [38]. Precision diagnostics and molecular profiling may soon allow clinicians to stratify patients and tailor interventions based on individual risk signatures. Epigenetic regulators (miRNAs, lncRNAs) are also being explored as biomarkers and therapeutic targets.
The future of diabetic retinopathy (DR) management is moving rapidly toward personalized medicine, driven by advances in genomics, transcriptomics, proteomics, and metabolomics. Increasing evidence demonstrates that individual genetic and epigenetic variations significantly modulate susceptibility to DR and response to therapies (Table 3).
For example, single nucleotide polymorphisms (SNPs) in angiogenic and inflammatory genes such as VEGF-A, RAGE, and HIF1A influence both disease progression and therapeutic efficacy, while circulating epigenetic regulators—including microRNAs (miR-21, miR-126, miR-200b) and long non-coding RNAs (MALAT1, MIAT)—emerge as promising biomarkers and therapeutic targets [38,72,73]. Integrating these molecular signatures into precision diagnostics may allow clinicians to stratify patients into subgroups characterized by angiogenic, inflammatory, or oxidative stress profiles, enabling risk prediction and individualized therapy selection. Moreover, epigenetic modifications underpin the phenomenon of 'metabolic memory,' whereby prior poor glycemic control leaves long-lasting damage despite subsequent normalization, suggesting that early intervention guided by molecular profiling is essential for altering disease trajectories [29,30,38].
Parallel to these discoveries, the integration of multi-omics with artificial intelligence (AI) and machine learning is transforming predictive modeling in DR. AI-driven algorithms trained on retinal imaging, systemic metabolic data, and genetic profiles can detect subclinical disease, forecast progression, and identify likely responders to anti-VEGF or corticosteroid therapies with increasing precision [61,72,74]. Emerging 'digital twin' models simulate patient-specific disease trajectories, offering clinicians a powerful tool to design adaptive and personalized treatment plans [75]. At the therapeutic level, pharmacogenomics is clarifying interindividual variability in drug response, paving the way for genotype-guided dosing of anti-VEGF agents or corticosteroids [38,73]. Furthermore, innovations in drug delivery systems, such as nanotechnology-based carriers (liposomes, dendrimers, micelles) and long-acting gene therapies (AAV2-sFLT01 vectors), promise to enhance intraocular bioavailability, prolong therapeutic effect, and reduce injection burden [61,70]. Stem cell therapies, particularly induced pluripotent stem cell (iPSC)-derived retinal cells, also represent a regenerative frontier, offering potential for tissue replacement and restoration of neurovascular integrity in advanced disease [70,75].
Looking ahead, personalized nutraceutical and lifestyle-based strategies are expected to complement high-technology therapeutics. Nutrients such as lutein, zeaxanthin, resveratrol, curcumin, and omega-3 fatty acids have shown differential benefits depending on patient-specific oxidative stress and lipidomic profiles, suggesting that dietary and nutraceutical interventions could be tailored to molecular phenotypes [11,40,70]. Integration of wearable glucose sensors, continuous retinal imaging, and telemedicine platforms will further support individualized disease monitoring and real-time adaptation of therapy [8,19,75]. Nonetheless, significant challenges remain, including high costs, limited access to omics technologies in low-resource settings, and ethical concerns regarding data privacy and equitable distribution of precision treatments [72,74]. Ultimately, the convergence of multi-omics, AI, regenerative medicine, and advanced drug delivery platforms has the potential to transform DR care into a truly personalized paradigm, reducing the global burden of blindness by delivering the right intervention to the right patient at the right time [38,70,75].
8. Targeted Therapies
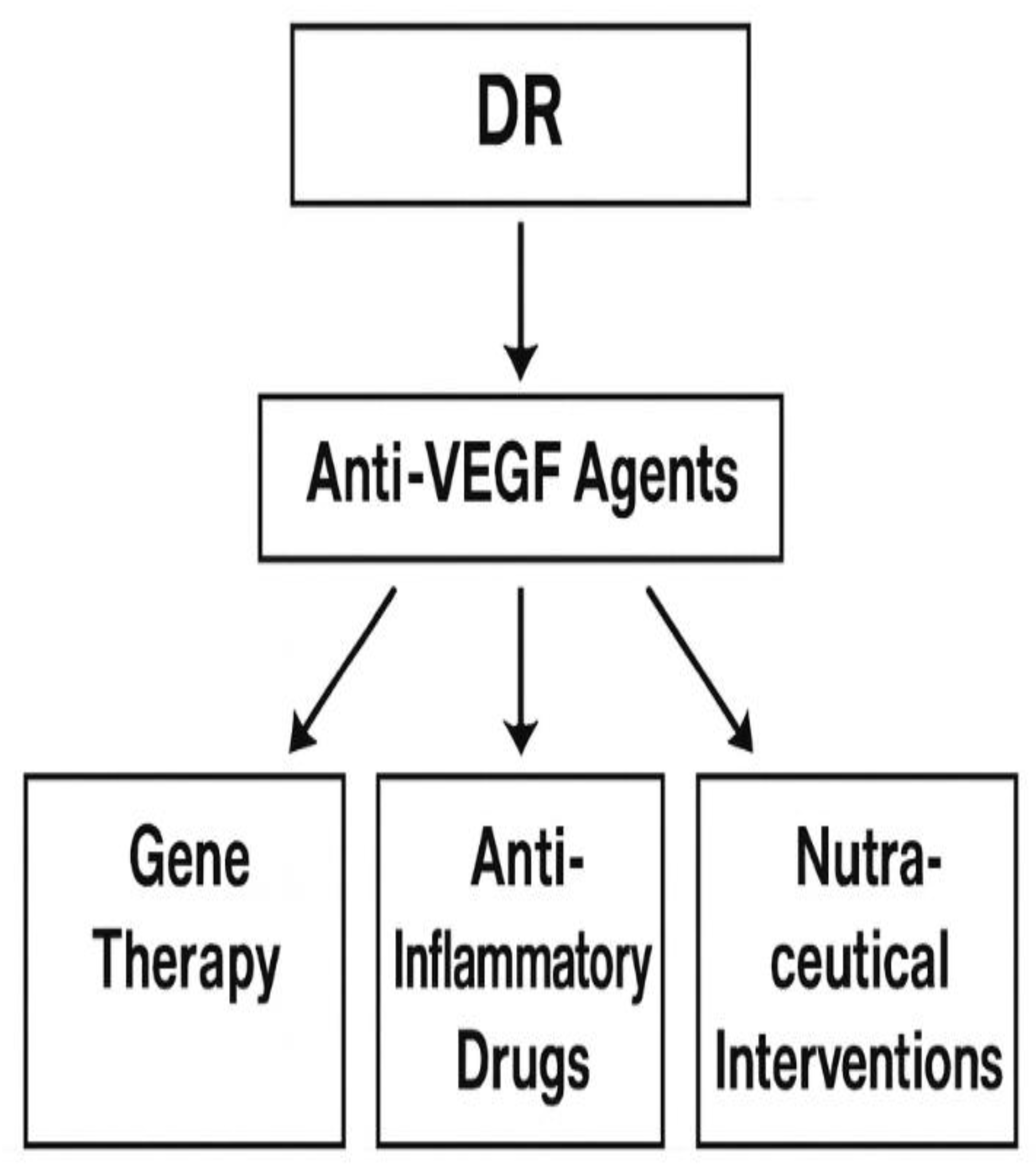
The development of targeted therapies for diabetic retinopathy (DR) (Figure 3) represents a crucial step in overcom[72,74ing the limitations of conventional anti-VEGF treatments. Gene therapy has emerged as a particularly promising avenue, aiming to provide long-term suppression of pathogenic pathways through single or infrequent interventions. Adeno-associated viral (AAV) vectors, such as AAV2-sFLT01, deliver soluble VEGF receptors to neutralize VEGF activity and reduce neovascularization [38,70]. Early-phase clinical trials suggest that gene-based approaches can achieve sustained intraocular expression of therapeutic proteins, reducing the frequency of injections compared to conventional biologics [61]. Beyond VEGF blockade, ongoing research explores the delivery of genes that encode anti-inflammatory mediators, neuroprotective factors, or antioxidative enzymes, expanding the therapeutic landscape toward multi-targeted interventions [75].
Figure 3.
Therapeutic Targets in Diabetic Retinopathy. Overview of current and emerging therapeutic strategies, including anti-VEGF agents, antioxidants, anti-inflammatory drugs, gene therapy, and nutraceutical interventions. These targets aim to mitigate molecular alterations associated with DR. (Adapted from Sheikpranbabu et al., 2009; Ma et al., 2017).
Figure 3.
Therapeutic Targets in Diabetic Retinopathy. Overview of current and emerging therapeutic strategies, including anti-VEGF agents, antioxidants, anti-inflammatory drugs, gene therapy, and nutraceutical interventions. These targets aim to mitigate molecular alterations associated with DR. (Adapted from Sheikpranbabu et al., 2009; Ma et al., 2017).
In parallel, antioxidant therapies have garnered considerable interest, given the central role of oxidative stress in DR pathogenesis. Compounds such as resveratrol, curcumin, quercetin, and N-acetylcysteine (NAC) have demonstrated the ability to modulate redox homeostasis, inhibit mitochondrial dysfunction, and attenuate ROS-mediated inflammatory signaling [29,40]. Preclinical studies confirm that these molecules can prevent retinal endothelial apoptosis and pericyte loss, while clinical studies are beginning to validate their adjunctive use in DR patients with poor glycemic control [72]. The challenge remains in achieving sufficient intraocular bioavailability; thus, nano formulations of polyphenols and synthetic antioxidant mimetics are actively being investigated to enhance stability, penetration, and sustained release [61].
Anti-inflammatory strategies are equally important, as inflammation is a key driver of microvascular injury and neovascularization in DR. Therapeutics targeting cytokines such as IL-6, IL-1β, MCP-1, or signaling cascades like JAK/STAT and NF-κB have shown efficacy in reducing leukostasis, vascular leakage, and blood–retinal barrier breakdown [31,73]. Agents such as tocilizumab (IL-6R inhibitor) and novel small molecules targeting microglial activation are under clinical evaluation, offering potential alternatives or adjuncts to anti-VEGF monotherapy [74]. Importantly, combined inhibition of angiogenic and inflammatory pathways appears to yield superior outcomes, underscoring the need for multi-modal targeted therapy approaches.
Finally, nutraceutical and nanotechnology-based delivery systems are being increasingly recognized as promising complementary strategies. Nutrients such as lutein, zeaxanthin, omega-3 fatty acids, and vitamin D exhibit neuroprotective and anti-inflammatory effects, with evidence suggesting they can reduce oxidative damage in the retinal pigment epithelium and photoreceptors [11,70]. The challenge of ocular drug delivery, however, is compounded by the anatomical and physiological barriers of the eye, including the cornea, conjunctiva, sclera, blood–aqueous barrier (BAB), and blood–retinal barrier (BRB). Advances in nanotechnology—including liposomes, dendrimers, polymeric nanoparticles, and hydrogels—offer solutions to overcome these barriers, enabling controlled, targeted, and prolonged release of both small molecules and biologics [61,75]. Such innovations are expected to revolutionize the therapeutic management of DR, providing safer and more efficient alternatives to current intravitreal injection regimens.
9. Analysis of Key Findings in DR Research
Diabetic retinopathy (DR) is driven by a tightly interconnected triad of oxidative stress, inflammation, and aberrant angiogenesis. A robust body of evidence links systemic and intraocular oxidative stress markers with DR incidence, severity, and progression, including activation of mitochondrial ROS, hexosamine and polyol pathway flux, and AGE formation that perpetuate vascular injury [29,30,31,32]. These mechanisms promote pericyte apoptosis, endothelial dysfunction, and blood–retinal barrier (BRB) breakdown, providing a biologic rationale for antioxidant and redox-restoring strategies as adjuncts to standard care [29,30]. Concurrently, inflammatory signaling (e.g., NF-κB activation, leukostasis mediated by IL-1β, TNF-α) further amplifies microvascular damage and crosstalks with hypoxia-inducible pathways to upregulate VEGF, thereby closing the loop between oxidative injury and pathological angiogenesis [31,32,34].
Across randomized trials and real-world cohorts, intravitreal anti-VEGF agents (ranibizumab, aflibercept, and bevacizumab) consistently reduce macular edema, improve or stabilize vision, and suppress neovascularization in DME and proliferative DR [72,73,74,75,76,77,78]. Head-to-head and network syntheses generally show superior or at least non-inferior anatomic and functional outcomes with anti-VEGF compared with intravitreal corticosteroids, while avoiding steroid-related adverse events such as intraocular pressure rise and cataract progression [66,67,68,69,70,75]. Beyond anti-VEGF, biologics that target inflammatory mediators (e.g., anti-TNF agents such as infliximab) have been investigated off-label or in early studies, reflecting the recognized role of inflammation in DR and the potential to complement angiogenesis inhibition [73,74,75]. Importantly, perioperative use of intravitreal agents can improve surgical fields and outcomes in complex PDR—reducing intraoperative bleeding, operative time, and postoperative complications when used adjunctively with vitrectomy [60,61,75].
A rapidly advancing frontier involves molecular and extracellular vesicle biomarkers that enable minimally invasive disease monitoring and treatment stratification. Circulating and aqueous humor microRNAs (including those packaged within exosomes) mirror retinal pathophysiology and correlate with DR stages, offering promise as non-invasive indicators of activity and response to therapy [7,38]. In parallel, multi-omics signatures (genomic variants in VEGF pathways, inflammatory gene expression modules, metabolomic fingerprints) are being integrated with imaging biomarkers (OCT, ultra-widefield angiography) and artificial intelligence models to predict progression and forecast individual treatment response, ultimately informing precision-guided regimens [8,18,38,61,72].
Therapeutically, combination and sequencing strategies, like anti-VEGF with navigated or subthreshold laser, or anti-VEGF followed by corticosteroid rescue in partial responders, can reduce injection burden and improve anatomical durability in selected patients [48,70,75]. Emerging modalities, including sustained-delivery implants and gene-based anti-VEGF expression (e.g., AAV2-sFLT01), aim to deliver longer-lasting disease control, whereas nanotechnology platforms are being optimized to traverse ocular barriers and achieve targeted posterior-segment delivery with fewer administrations [61,70,75]. Collectively, these advances underscore a shift from a one-size-fits-all approach toward pathway-directed and patient-tailored therapy that addresses the heterogeneity of DR biology and clinical expression [38,70,75].
10. Conclusions
Diabetic retinopathy (DR) remains a major cause of preventable blindness worldwide, with pathogenesis driven by oxidative stress, retinal pigment epithelium (RPE) dysfunction, chronic inflammation, and pathological angiogenesis [29,30,31,32,33,34]. Current anti-VEGF therapies have revolutionized management of diabetic macular edema (DME) and proliferative DR, yet incomplete responses, injection burden, and variability among patients emphasize the need for multi-targeted approaches [72,73,74,75]. Evidence indicates that persistent mitochondrial ROS, advanced glycation end-products (AGEs), and NF-κB–mediated cytokine activation amplify vascular damage, highlighting the importance of complementary antioxidant and anti-inflammatory interventions [29,30,31,32].
Emerging innovations include gene therapy (e.g., AAV2-sFLT01) and sustained-delivery implants, which aim to reduce treatment frequency while maintaining efficacy [61,70,75]. Nanotechnology-based carriers further promise to overcome ocular barriers, achieving targeted posterior-segment drug release. In parallel, advances in multi-omics and artificial intelligence (AI) are reshaping risk prediction, integrating genomic variants, transcriptomic modules, and metabolomic profiles with imaging biomarkers to identify patients at highest risk and tailor treatment intensity [8,18,61,72]. Circulating exosomal microRNAs also offer minimally invasive biomarkers for real-time monitoring of disease activity and treatment response [7,38].
Future research must prioritize randomized trials and mechanistic studies that validate biomarker-guided therapy, evaluate combined antioxidant, anti-inflammatory, and anti-angiogenic regimens, and assess the durability of next-generation delivery systems. Importantly, strategies must address challenges of cost, accessibility, and equitable distribution to ensure broad clinical adoption [70,72,73,74,75]. By integrating targeted therapies with precision diagnostics, the field is advancing toward personalized, durable interventions capable of preserving vision and reducing the global burden of DR.
References
- Teo, Z. L.; Tham, Y.-C.; Yu, M.; Chee, M. L.; Rim, T. H.; Cheung, N.; Bikbov, M. M.; Wang, Y. X.; Tang, Y.; Lu, Y.; Wong, I. Y.; Ting, D. S. W.; Tan, G. S. W.; Jonas, J. B.; Sabanayagam, C.; Wong, T. Y.; Cheng, C.-Y. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, (11), 1580-1591. [CrossRef]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P. F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci. Rep. 2020, 10, (1), 14790.
- GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, (10440), 2100-2132.
- Alegre-Díaz, J.; Herrington, W.; López-Cervantes, M.; Gnatiuc, L.; Ramirez, R.; Hill, M.; Baigent, C.; McCarthy, M. I.; Lewington, S.; Collins, R.; Whitlock, G.; Tapia-Conyer, R.; Peto, R.; Kuri-Morales, P.; Emberson, J. R. Diabetes and Cause-Specific Mortality in Mexico City. N. Engl. J. Med. 2016, 375, (20), 1961-1971. [CrossRef]
- Bragg, F.; Holmes, M. V.; Iona, A.; Guo, Y.; Du, H.; Chen, Y.; Bian, Z.; Yang, L.; Herrington, W.; Bennett, D.; Turnbull, I.; Liu, Y.; Feng, S.; Chen, J.; Clarke, R.; Collins, R.; Peto, R.; Li, L.; Chen, Z. Association Between Diabetes and Cause-Specific Mortality in Rural and Urban Areas of China. JAMA 2017, 317, (3), 280-289. [CrossRef]
- Yang, J. J.; Yu, D.; Wen, W.; Saito, E.; Rahman, S.; Shu, X.-O.; Chen, Y.; Gupta, P. C.; Gu, D.; Tsugane, S.; Xiang, Y.-B.; Gao, Y.-T.; Yuan, J.-M.; Tamakoshi, A.; Irie, F.; Sadakane, A.; Tomata, Y.; Kanemura, S.; Tsuji, I.; Matsuo, K.; Nagata, C.; Chen, C.-J.; Koh, W.-P.; Shin, M.-H.; Park, S. K.; Wu, P.-E.; Qiao, Y.-L.; Pednekar, M. S.; He, J.; Sawada, N.; Li, H.-L.; Gao, J.; Cai, H.; Wang, R.; Sairenchi, T.; Grant, E.; Sugawara, Y.; Zhang, S.; Ito, H.; Wada, K.; Shen, C.-Y.; Pan, W.-H.; Ahn, Y.-O.; You, S.-L.; Fan, J.-H.; Yoo, K.-Y.; Ashan, H.; Chia, K. S.; Boffetta, P.; Inoue, M.; Kang, D.; Potter, J. D.; Zheng, W. Association of Diabetes With All-Cause and Cause-Specific Mortality in Asia: A Pooled Analysis of More Than 1 Million Participants. JAMA Network Open 2019, 2, (4), e192696-e192696.
- Jenkins, A. J.; Joglekar, M. V.; Hardikar, A. A.; Keech, A. C.; O'Neal, D. N.; Januszewski, A. S. Biomarkers in Diabetic Retinopathy. Rev. Diabet. Stud. 2015, 12, (1-2), 159-95.
- Wong, T. Y.; Tan, T. E. The Diabetic Retinopathy "Pandemic" and Evolving Global Strategies: The 2023 Friedenwald Lecture. Invest. Ophthalmol. Vis. Sci. 2023, 64, (15), 47. [CrossRef]
- Khalid, M.; Petroianu, G.; Adem, A. Advanced Glycation End Products and Diabetes Mellitus: Mechanisms and Perspectives. Biomolecules 2022, 12, (4). [CrossRef]
- Stitt, A. W. The role of advanced glycation in the pathogenesis of diabetic retinopathy. Exp. Mol. Pathol. 2003, 75, (1), 95-108. [CrossRef]
- Antonetti, D. A.; Barber, A. J.; Bronson, S. K.; Freeman, W. M.; Gardner, T. W.; Jefferson, L. S.; Kester, M.; Kimball, S. R.; Krady, J. K.; LaNoue, K. F.; Norbury, C. C.; Quinn, P. G.; Sandirasegarane, L.; Simpson, I. A. Diabetic retinopathy: seeing beyond glucose-induced microvascular disease. Diabetes 2006, 55, (9), 2401-11.
- Wiley, H. E.; Ferris, F. L., Chapter 47 - Nonproliferative Diabetic Retinopathy and Diabetic Macular Edema. In Retina (Fifth Edition), Ryan, S. J.; Sadda, S. R.; Hinton, D. R.; Schachat, A. P.; Sadda, S. R.; Wilkinson, C. P.; Wiedemann, P.; Schachat, A. P., Eds. W.B. Saunders: London, 2013; pp 940-968.
- Wong, T. Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V. C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M. M. K.; Resnikoff, S.; Verdaguer, J.; Zhao, P.; Ferris, F.; Aiello, L. P.; Taylor, H. R. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for Screening, Follow-up, Referral, and Treatment Based on Resource Settings. Ophthalmology 2018, 125, (10), 1608-1622.
- Gupta, A.; Bansal, R.; Sharma, A.; Kapil, A., Retinal Hard Exudates. In Ophthalmic Signs in Practice of Medicine, Springer Nature Singapore: Singapore, 2023; pp 59-79.
- Campochiaro, P. A. Ocular neovascularization. J. Mol. Med. (Berl.) 2013, 91, (3), 311-21.
- Wilkinson, C. P.; Ferris, F. L.; Klein, R. E.; Lee, P. P.; Agardh, C. D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J. T. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003, 110, (9), 1677-1682. [CrossRef]
- Flaxel, C. J.; Adelman, R. A.; Bailey, S. T.; Fawzi, A.; Lim, J. I.; Vemulakonda, G. A.; Ying, G. S. Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology 2020, 127, (1), P66-p145.
- Yang, Z.; Tan, T. E.; Shao, Y.; Wong, T. Y.; Li, X. Classification of diabetic retinopathy: Past, present and future. Front. Endocrinol. (Lausanne) 2022, 13, 1079217. [CrossRef]
- Lin, C.; Jivraj, S. Are diabetes and blood sugar control associated with the diagnosis of eye diseases? An English prospective observational study of glaucoma, diabetic eye disease, macular degeneration and cataract diagnosis trajectories in older age. BMJ Open 2025, 15, (6), e091816. [CrossRef]
- Feldman-Billard, S.; Dupas, B. Eye disorders other than diabetic retinopathy in patients with diabetes. Diabetes Metab. 2021, 47, (6), 101279. [CrossRef]
- Terheyden, J. H.; Fink, D. J.; Mercieca, K.; Wintergerst, M. W. M.; Holz, F. G.; Finger, R. P. Knowledge about age-related eye diseases in the general population in Germany. BMC Public Health 2024, 24, (1), 409. [CrossRef]
- Jeganathan, V. S.; Wang, J. J.; Wong, T. Y. Ocular associations of diabetes other than diabetic retinopathy. Diabetes Care 2008, 31, (9), 1905-12.
- Chen, L.; Islam, R. M.; Wang, J.; Hird, T. R.; Pavkov, M. E.; Gregg, E. W.; Salim, A.; Tabesh, M.; Koye, D. N.; Harding, J. L.; Sacre, J. W.; Barr, E. L. M.; Magliano, D. J.; Shaw, J. E. A systematic review of trends in all-cause mortality among people with diabetes. Diabetologia 2020, 63, (9), 1718-1735.
- Li, Y.; Pan, A. P.; Yu, A. Y. Recent Progression of Pathogenesis and Treatment for Diabetic Cataracts. Semin. Ophthalmol. 2025, 40, (4), 275-282. [CrossRef]
- Fang, C.; He, D.; Shen, M.; Chen, R.; Shen, X. Association between stress hyperglycemia ratio and neovascular glaucoma in patients with proliferative diabetic retinopathy. BMC Ophthalmol. 2025, 25, (1), 163. [CrossRef]
- Xue, Z.; Yuan, J.; Chen, F.; Yao, Y.; Xing, S.; Yu, X.; Li, K.; Wang, C.; Bao, J.; Qu, J.; Su, J.; Chen, H. Genome-wide association meta-analysis of 88,250 individuals highlights pleiotropic mechanisms of five ocular diseases in UK Biobank. EBioMedicine 2022, 82, 104161. [CrossRef]
- Campagnoli, L. I. M.; Varesi, A.; Barbieri, A.; Marchesi, N.; Pascale, A. Targeting the Gut-Eye Axis: An Emerging Strategy to Face Ocular Diseases. Int. J. Mol. Sci. 2023, 24, (17). [CrossRef]
- Chen, S.; Lin, M.; Hong, Y. The causal effect of glaucoma and diabetic retinopathy: a Mendelian randomization study. Diabetol. Metab. Syndr. 2025, 17, (1), 80. [CrossRef]
- Kang, Q.; Yang, C. Oxidative stress and diabetic retinopathy: Molecular mechanisms, pathogenetic role and therapeutic implications. Redox Biol. 2020, 37, 101799. [CrossRef]
- Kowluru, R. A.; Chan, P. S. Oxidative stress and diabetic retinopathy. Exp. Diabetes Res. 2007, 2007, 43603.
- Tang, J.; Kern, T. S. Inflammation in diabetic retinopathy. Prog. Retin. Eye Res. 2011, 30, (5), 343-58.
- Forbes, J. M.; Cooper, M. E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, (1), 137-88.
- Madsen-Bouterse, S. A.; Kowluru, R. A. Oxidative stress and diabetic retinopathy: pathophysiological mechanisms and treatment perspectives. Rev. Endocr. Metab. Disord. 2008, 9, (4), 315-27. [CrossRef]
- Behl, T.; Kotwani, A. Exploring the various aspects of the pathological role of vascular endothelial growth factor (VEGF) in diabetic retinopathy. Pharmacol. Res. 2015, 99, 137-48. [CrossRef]
- Schmidt-Erfurth, U.; Garcia-Arumi, J.; Bandello, F.; Berg, K.; Chakravarthy, U.; Gerendas, B. S.; Jonas, J.; Larsen, M.; Tadayoni, R.; Loewenstein, A. Guidelines for the Management of Diabetic Macular Edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica 2017, 237, (4), 185-222.
- Simó, R.; Sundstrom, J. M.; Antonetti, D. A. Ocular Anti-VEGF therapy for diabetic retinopathy: the role of VEGF in the pathogenesis of diabetic retinopathy. Diabetes Care 2014, 37, (4), 893-9. [CrossRef]
- Sajovic, J.; Cilenšek, I.; Mankoč, S.; Tajnšek, Š.; Kunej, T.; Petrovič, D.; Globočnik Petrovič, M. Vascular endothelial growth factor (VEGF)-related polymorphisms rs10738760 and rs6921438 are not risk factors for proliferative diabetic retinopathy (PDR) in patients with type 2 diabetes mellitus (T2DM). Bosn. J. Basic Med. Sci. 2019, 19, (1), 94-100. [CrossRef]
- Pei, X.; Huang, D.; Li, Z. Genetic insights and emerging therapeutics in diabetic retinopathy: from molecular pathways to personalized medicine. Frontiers in Genetics 2024, Volume 15 - 2024. [CrossRef]
- Gong, C. Y.; Lu, B.; Sheng, Y. C.; Yu, Z. Y.; Zhou, J. Y.; Ji, L. L. The Development of Diabetic Retinopathy in Goto-Kakizaki Rat and the Expression of Angiogenesis-Related Signals. Chin. J. Physiol. 2016, 59, (2), 100-8. [CrossRef]
- Zhang, C. Y.; Yang, M. Roles of fibroblast growth factors in the treatment of diabetes. World J. Diabetes 2024, 15, (3), 392-402. [CrossRef]
- Meng, Z.; Li, F.; Wang, B. miR-372-3p is a potential diagnostic factor for diabetic nephropathy and modulates high glucose-induced glomerular endothelial cell dysfunction via targeting fibroblast growth factor-16. Arch. Med. Sci. 2023, 19, (3), 703-716. [CrossRef]
- Chen, C.; Zhao, C.; Gu, C.; Cui, X.; Wu, J. MiRNA-144-3p inhibits high glucose induced cell proliferation through suppressing FGF16. Biosci. Rep. 2019, 39, (7). [CrossRef]
- Huang, T.; Li, X.; Xie, J.; Zhang, L.; Zhang, G.; Zhang, A.; Chen, X.; Cui, Y.; Meng, Q. Long-Term Retinal Neurovascular and Choroidal Changes After Panretinal Photocoagulation in Diabetic Retinopathy. Front. Med. 2021, Volume 8 - 2021. [CrossRef]
- Stefánsson, E. The therapeutic effects of retinal laser treatment and vitrectomy. A theory based on oxygen and vascular physiology. Acta Ophthalmol. Scand. 2001, 79, (5), 435-440. [CrossRef]
- Lu, L.; Jiang, Y.; Jaganathan, R.; Hao, Y. Current Advances in Pharmacotherapy and Technology for Diabetic Retinopathy: A Systematic Review. J. Ophthalmol. 2018, 2018, (1), 1694187.
- Ogata, N.; Tombran-Tink, J.; Jo, N.; Mrazek, D.; Matsumura, M. Upregulation of pigment epithelium-derived factor after laser photocoagulation. Am. J. Ophthalmol. 2001, 132, (3), 427-429. [CrossRef]
- Wang, W.; Lo, A. C. Y. Diabetic Retinopathy: Pathophysiology and Treatments. Int. J. Mol. Sci. 2018, 19, (6), 1816. [CrossRef]
- Wang, S.; Hua, R.; Zhao, Y.; Liu, L. Laser Treatment for Diabetic Retinopathy: History, Mechanism, and Novel Technologies. J. Clin. Med. 2024, 13, (18), 5439. [CrossRef]
- Tsilimbaris, M. K.; Kontadakis, G. A.; Tsika, C.; Papageorgiou, D.; Charoniti, M. Effect of panretinal photocoagulation treatment on vision-related quality of life of patients with proliferative diabetic retinopathy. Retina 2013, 33, (4), 756-61. [CrossRef]
- Blumenkranz, M. S.; Yellachich, D.; Andersen, D. E.; Wiltberger, M. W.; Mordaunt, D.; Marcellino, G. R.; Palanker, D. Semiautomated patterned scanning laser for retinal photocoagulation. Retina 2006, 26, (3), 370-6. [CrossRef]
- Paulus, Y. M.; Kaur, K.; Egbert, P. R.; Blumenkranz, M. S.; Moshfeghi, D. M. Human histopathology of PASCAL laser burns. Eye (Lond.) 2013, 27, (8), 995-6. [CrossRef]
- Inan, S.; Polat, O.; Yıgıt, S.; Inan, U. U. PASCAL laser platform produces less pain responses compared to conventional laser system during the panretinal photocoagulation: a randomized clinical trial. Afr. Health Sci. 2018, 18, (4), 1010-1017. [CrossRef]
- Lai, K.; Zhao, H.; Zhou, L.; Huang, C.; Zhong, X.; Gong, Y.; Li, L.; Xu, F.; Li, C.; Lu, L.; Jin, C. Subthreshold Pan-Retinal Photocoagulation Using Endpoint Management Algorithm for Severe Nonproliferative Diabetic Retinopathy: A Paired Controlled Pilot Prospective Study. Ophthalmic Res. 2020, 64, (4), 648-655. [CrossRef]
- Kozak, I.; Oster, S. F.; Cortes, M. A.; Dowell, D.; Hartmann, K.; Kim, J. S.; Freeman, W. R. Clinical evaluation and treatment accuracy in diabetic macular edema using navigated laser photocoagulator NAVILAS. Ophthalmology 2011, 118, (6), 1119-24. [CrossRef]
- Deschler, E. K.; Sun, J. K.; Silva, P. S. Side-Effects and Complications of Laser Treatment in Diabetic Retinal Disease. Semin. Ophthalmol. 2014, 29, (5-6), 290-300. [CrossRef]
- Patel, N. C.; Hsieh, Y. T.; Yang, C. M.; Berrocal, M. H.; Dhawahir-Scala, F.; Ruamviboonsuk, P.; Pappuru, R. R.; Dave, V. P. Vitrectomy for diabetic retinopathy: A review of indications, techniques, outcomes, and complications. Taiwan J. Ophthalmol. 2024, 14, (4), 519-530. [CrossRef]
- Fujii, G. Y.; De Juan, E., Jr.; Humayun, M. S.; Pieramici, D. J.; Chang, T. S.; Awh, C.; Ng, E.; Barnes, A.; Wu, S. L.; Sommerville, D. N. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology 2002, 109, (10), 1807-12; discussion 1813. [CrossRef]
- Eckardt, C. Transconjunctival sutureless 23-gauge vitrectomy. Retina 2005, 25, (2), 208-11. [CrossRef]
- Oshima, Y.; Wakabayashi, T.; Sato, T.; Ohji, M.; Tano, Y. A 27-gauge instrument system for transconjunctival sutureless microincision vitrectomy surgery. Ophthalmology 2010, 117, (1), 93-102.e2. [CrossRef]
- Tomita, Y.; Kurihara, T.; Uchida, A.; Nagai, N.; Shinoda, H.; Tsubota, K.; Ozawa, Y. Wide-Angle Viewing System versus Conventional Indirect Ophthalmoscopy for Scleral Buckling. Sci. Rep. 2015, 5, 13256. [CrossRef]
- Wang, Z.; Zhang, N.; Lin, P.; Xing, Y.; Yang, N. Recent advances in the treatment and delivery system of diabetic retinopathy. Front. Endocrinol. (Lausanne) 2024, Volume 15 - 2024. [CrossRef]
- Nakashima, H.; Iwama, Y.; Tanioka, K.; Emi, K. Paracentral Acute Middle Maculopathy following Vitrectomy for Proliferative Diabetic Retinopathy: Incidence, Risk Factors, and Clinical Characteristics. Ophthalmology 2018, 125, (12), 1929-1936. [CrossRef]
- Sun, D.; Lin, Y.; Zeng, R.; Yang, Z.; Deng, X.; Lan, Y. The incidence and risk factors of neovascular glaucoma secondary to proliferative diabetic retinopathy after vitrectomy. Eur. J. Ophthalmol. 2021, 31, (6), 3057-3067. [CrossRef]
- Anderson, W.; Piggott, K.; Bao, Y. K.; Pham, H.; Kavali, S.; Rajagopal, R. Complete Posterior Vitreous Detachment Reduces the Need for Treatment of Diabetic Macular Edema. Ophthalmic Surg. Lasers Imaging Retina 2019, 50, (11), e266-e273. [CrossRef]
- Shaikh, N.; Kumar, V.; Ramachandran, A.; Venkatesh, R.; Tekchandani, U.; Tyagi, M.; Jayadev, C.; Dogra, M.; Chawla, R. Vitrectomy for cases of diabetic retinopathy. Indian J. Ophthalmol. 2024, 72, (12). [CrossRef]
- Sobrin, L.; D'Amico, D. J. Controversies in Intravitreal Triamcinolone Acetonide Use. Int. Ophthalmol. Clin. 2005, 45, (4), 133-141. [CrossRef]
- Jonas, J. B.; Kreissig, I.; Söfker, A.; Degenring, R. F. Intravitreal Injection of Triamcinolone for Diffuse Diabetic Macular Edema. Arch. Ophthalmol. 2003, 121, (1), 57-61. [CrossRef]
- Martidis, A.; Duker, J. S.; Greenberg, P. B.; Rogers, A. H.; Puliafito, C. A.; Reichel, E.; Baumal, C. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology 2002, 109, (5), 920-927. [CrossRef]
- Avitabile, T.; Longo, A.; Reibaldi, A. Intravitreal Triamcinolone Compared With Macular Laser Grid Photocoagulation for the Treatment of Cystoid Macular Edema. Am. J. Ophthalmol. 2005, 140, (4), 695.e1-695.e10. [CrossRef]
- Mohamed, Q.; Gillies, M. C.; Wong, T. Y. Management of diabetic retinopathy: a systematic review. JAMA 2007, 298, (8), 902-16.
- Pearson, P.; Levy, B.; Comstock, T.; Group, F. A. I. S. Fluocinolone Acetonide Intravitreal Implant to Treat Diabetic Macular Edema: 3–Year Results of a Multi–Center Clinical Trial. Invest. Ophthalmol. Vis. Sci. 2006, 47, (13), 5442-5442.
- Gupta, N.; Mansoor, S.; Sharma, A.; Sapkal, A.; Sheth, J.; Falatoonzadeh, P.; Kuppermann, B.; Kenney, M. Diabetic retinopathy and VEGF. Open Ophthalmol. J. 2013, 7, 4-10. [CrossRef]
- Rodrigues, E. B.; Farah, M. E.; Maia, M.; Penha, F. M.; Regatieri, C.; Melo, G. B.; Pinheiro, M. M.; Zanetti, C. R. Therapeutic monoclonal antibodies in ophthalmology. Prog. Retin. Eye Res. 2009, 28, (2), 117-44. [CrossRef]
- Bahrami, B.; Hong, T.; Gilles, M. C.; Chang, A. Anti-VEGF Therapy for Diabetic Eye Diseases. Asia. Pac. J. Ophthalmol. (Phila). 2017, 6, (6), 535-545. [CrossRef]
- Chen, Y.-T.; Radke, N. V.; Amarasekera, S.; Park, D. H.; Chen, N.; Chhablani, J.; Wang, N.-K.; Wu, W.-C.; Ng, D. S. C.; Bhende, P.; Varma, S.; Leung, E.; Zhang, X.; Li, F.; Zhang, S.; Fang, D.; Liang, J.; Zhang, Z.; Liu, H.; Zhao, P.; Sharma, T.; Ruamviboonsuk, P.; Lai, C.-C.; Lam, D. S. C. Updates on medical and surgical managements of diabetic retinopathy and maculopathy. Asia. Pac. J. Ophthalmol. (Phila). 2025, 14, (2), 100180. [CrossRef]
- Macugen Diabetic Retinopathy Study Group. Changes in Retinal Neovascularization after Pegaptanib (Macugen) Therapy in Diabetic Individuals. Ophthalmology 2006, 113, (1), 23-28. [CrossRef]
- Macugen Diabetic Retinopathy Study Group. A Phase II Randomized Double-Masked Trial of Pegaptanib, an Anti–Vascular Endothelial Growth Factor Aptamer, for Diabetic Macular Edema. Ophthalmology 2005, 112, (10), 1747-1757. [CrossRef]
- Sultan, M. B.; Zhou, D.; Loftus, J.; Dombi, T.; Ice, K. S. A Phase 2/3, Multicenter, Randomized, Double-Masked, 2-Year Trial of Pegaptanib Sodium for the Treatment of Diabetic Macular Edema. Ophthalmology 2011, 118, (6), 1107-1118. [CrossRef]
- Fortin, P.; Mintzes, B.; Innes, M. A Systematic Review of Intravitreal Bevacizumab for the Treatment of Diabetic Macular Edema. CADTH Technol. Overv. 2013, 3, (1).
- Li, J. Q.; Welchowski, T.; Schmid, M.; Letow, J.; Wolpers, C.; Pascual-Camps, I.; Holz, F. G.; Finger, R. P. Prevalence, incidence and future projection of diabetic eye disease in Europe: a systematic review and meta-analysis. Eur. J. Epidemiol. 2020, 35, (1), 11-23. [CrossRef]
- Chen, X.; Shi, C.; He, M.; Xiong, S.; Xia, X. Endoplasmic reticulum stress: molecular mechanism and therapeutic targets. Signal Transduct. Target Ther. 2023, 8, (1), 352. [CrossRef]
- Haghshenas, L.; Banihashemi, S.; Malekzadegan, Y.; Catanzaro, R.; Moghadam Ahmadi, A.; Marotta, F. Microbiome as an endocrine organ and its relationship with eye diseases: Effective factors and new targeted approaches. World J. Gastrointest. Pathophysiol. 2024, 15, (5), 96446. [CrossRef]
- Gwon, H.-N.; Son, H.-J.; Shin, Y.-J. Association of Body Metrics and Ocular Diseases. J. Clin. Med. 2025, 14, (16). [CrossRef]
- Datta, S.; Koka, S.; Boini, K. M. Understanding the Role of Adipokines in Cardiometabolic Dysfunction: A Review of Current Knowledge. Biomolecules 2025, 15, (5). [CrossRef]
- Greenberg, M. J.; Bamba, S. Diabetic cataracts. Dis. Mon. 2021, 67, (5), 101134.
- Tian, C.; Chen, Y.; Xu, B.; Tan, X.; Zhu, Z. Association of triglyceride-glucose index with the risk of incident aortic dissection and aneurysm: a large-scale prospective cohort study in UK Biobank. Cardiovasc. Diabetol. 2024, 23, (1), 282. [CrossRef]
- Tang, Y.; Shi, Y.; Fan, Z. The mechanism and therapeutic strategies for neovascular glaucoma secondary to diabetic retinopathy. Front. Endocrinol. (Lausanne) 2023, 14, 1102361. [CrossRef]
- Liu, Y. C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J. S. Cataracts. Lancet 2017, 390, (10094), 600-612.
- Wei, B.; Hu, X.; Shu, B. L.; Huang, Q. Y.; Chai, H.; Yuan, H. Y.; Zhou, L.; Duan, Y. C.; Yao, L. L.; Dong, Z. E.; Wu, X. R. Association of triglyceride-glucose index and derived indices with cataract in middle-aged and elderly Americans: NHANES 2005-2008. Lipids Health Dis. 2025, 24, (1), 48. [CrossRef]
- Mishra, D.; Kashyap, A.; Srivastav, T.; Yadav, A.; Pandey, S.; Majhi, M. M.; Verma, K.; Prabu, A.; Singh, V. Enzymatic and biochemical properties of lens in age-related cataract versus diabetic cataract: A narrative review. Indian J. Ophthalmol. 2023, 71, (6), 2379-2384. [CrossRef]
- Hom, M.; De Land, P. Self-reported dry eyes and diabetic history. Optometry (St. Louis, Mo.) 2006, 77, (11), 554-8.
- Brar, G. K.; Bawa, M.; Chadha, C.; Gupta, T.; Kaur, H. Proportion of dry eye in type II diabetics. J. Family Med. Prim. Care 2024, 13, (4), 1311-1315. [CrossRef]
- Manchikanti, V.; Kasturi, N.; Rajappa, M.; Gochhait, D. Ocular surface disorder among adult patients with type II diabetes mellitus and its correlation with tear film markers: A pilot study. Taiwan J. Ophthalmol. 2021, 11, (2), 156-160. [CrossRef]
- Mangoli, M. V.; Bubanale, S. C.; Bhagyajyothi, B. K.; Goyal, D. Dry eye disease in diabetics versus non-diabetics: Associating dry eye severity with diabetic retinopathy and corneal nerve sensitivity. Indian J. Ophthalmol. 2023, 71, (4), 1533-1537. [CrossRef]
- Lima-Fontes, M.; Barata, P.; Falcão, M.; Carneiro, Â. Ocular findings in metabolic syndrome: a review. Porto Biomed. J. 2020, 5, (6), e104. [CrossRef]
Figure 1.
Molecular Pathways in Diabetic Retinopathy. Schematic representation of interconnected molecular mechanisms involved in DR pathogenesis: hyperglycemia induces oxidative stress, which contributes to retinal pigment epithelium (RPE) dysfunction, inflammation, and angiogenesis, ultimately leading to retinal damage and vision loss. (Adapted from Kowluru et al., 2007; Tang & Kern, 2011).
Figure 1.
Molecular Pathways in Diabetic Retinopathy. Schematic representation of interconnected molecular mechanisms involved in DR pathogenesis: hyperglycemia induces oxidative stress, which contributes to retinal pigment epithelium (RPE) dysfunction, inflammation, and angiogenesis, ultimately leading to retinal damage and vision loss. (Adapted from Kowluru et al., 2007; Tang & Kern, 2011).
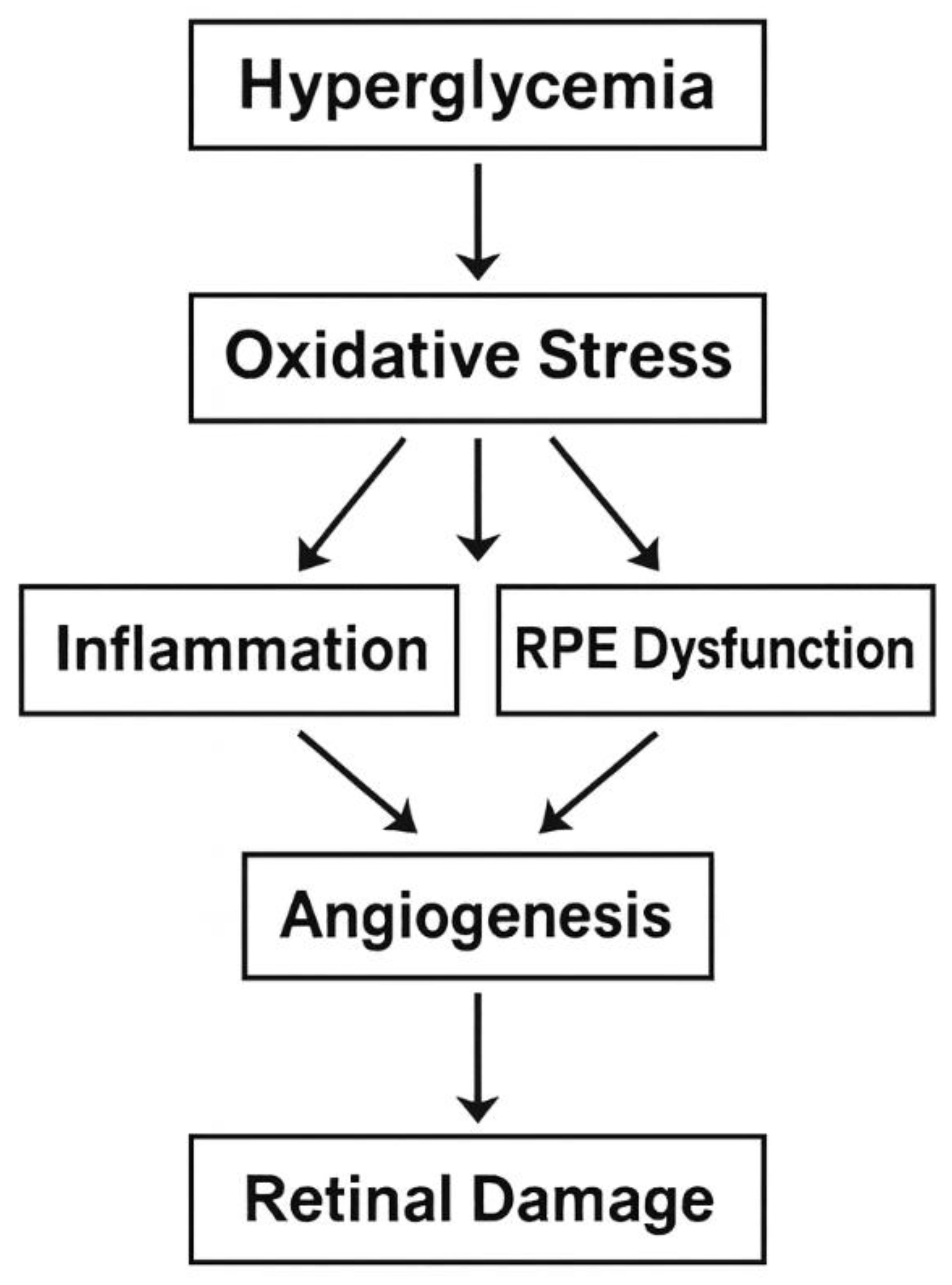
Figure 2.
Oxidative Damage in Retinal Cells. Illustration of oxidative stress-induced damage in retinal pigment epithelium and neuronal cells, including mitochondrial dysfunction, ROS accumulation, and inflammatory signaling. (Adapted from Madsen-Bouterse & Kowluru, 2008).
Figure 2.
Oxidative Damage in Retinal Cells. Illustration of oxidative stress-induced damage in retinal pigment epithelium and neuronal cells, including mitochondrial dysfunction, ROS accumulation, and inflammatory signaling. (Adapted from Madsen-Bouterse & Kowluru, 2008).
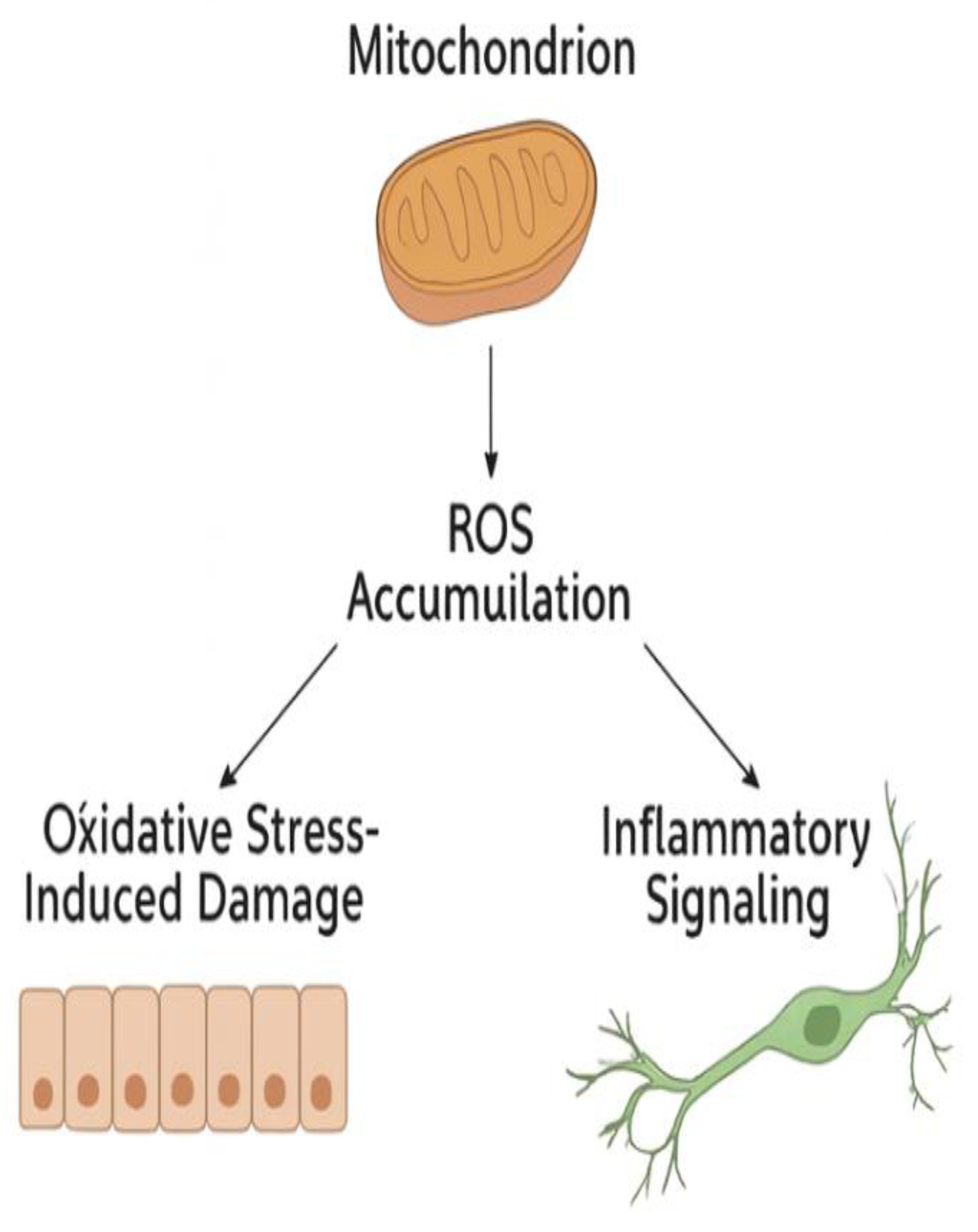

Table 1.
Stages and Clinical Features of Diabetic Retinopathy. Summary of progression stages, characteristic features, typical fundus findings, and associated visual impairments. (Adapted from Schmidt-Erfurth et al., 2017.).
Table 1.
Stages and Clinical Features of Diabetic Retinopathy. Summary of progression stages, characteristic features, typical fundus findings, and associated visual impairments. (Adapted from Schmidt-Erfurth et al., 2017.).
| Stage | Key Features | Fundus Findings | Visual Impact |
|---|---|---|---|
| Non-Proliferative (NPDR) | Microaneurysms, dot hemorrhages | Cotton wool spots, hard exudates | Mild to moderate |
| Proliferative (PDR) | Neovascularization | Vitreous hemorrhage, retinal detachment | Severe vision loss |
| Diabetic Macular Edema (DME) | Retinal thickening in macula | Cystoid spaces in OCT | Blurred central vision |
Table 2.
Diabetic retinopathy in the context of other eye diseases.
| Diagnosis | Frequency of occurrence in patients with diabetes | Association with chronic hyperglycemia | The main pathogenetic mechanisms Associated diseases and conditions | Associated diseases and conditions |
|---|---|---|---|---|
| Diabetic retinopathy (DR) | The total frequency of occurrence is 20-25.7%. In patients with type 1 diabetes, 54.4%, in patients with type 2 diabetes [1,80]. | A decrease in blood glucose by 10 mg/dl is directly related to a decrease in intraocular pressure by 0.09 mmHg [20]. |
Oxidative stress. Dysfunction of the retinal pigment epithelium. Abnormal angiogenesis. Inflammation of the retina. Disruption of neurotransmitter production. Violation of the production of trophic factors in the retina. Similar genetic correlations with OTHER dysbiosis of the ocular and intestinal microbiota [26,80,81,82]. | Fatness. Cardiovascular diseases. Dyslipidemia. Atherosclerosis. Non-alcoholic fatty liver disease. Chronic kidney disease. Old age Intestinal diseases [27,83,84]. |
| Cataract | Prevalence: 3.3% vs. 1.9% in patients with diabetes compared to the control group. The incidence of cataracts in people with diabetes is 3-5 times higher than in healthy people. Up to 20% of all cataract surgeries are performed in patients with diabetes mellitus [85]. |
The risk of developing cataracts depends on the duration of diabetes and the severity of hyperglycemia [85]. | Metabolic disorders Oxidative stress Old age Denaturation of lens proteins Dyslipidemia Smoking Similar genetic correlations with others) [26,81,86,87]. |
Obesity and metabolic syndrome. Old age. Cardiovascular diseases. High degree of myopia. Smoking. Exposure to sunlight. Therapy with steroids. Local injuries) Intestinal diseases [26,86,88,89,90] |
| Glaucoma | DR is the main cause of glaucoma, accounting for 30% to 52.38% of cases. glaucoma [22,87]. |
The probable risk of glaucoma in patients with chronic hyperglycemia is high [22,87]. |
Similar genetic correlations with others. Degeneration of axons. Neuroinflammation. Transynaptic degeneration of retinal ganglion cells. Dysbiosis of ocular and intestinal microbiota [22,82]. |
Old age. Systemic diseases Cardiovascular diseases [87]. |
| Age-related macular degeneration (AMD) | Ambiguous results: The same prevalence or risk of developing DR or its progression. The number of people living with diabetes and AMD, DR is expected to grow rapidly due to the aging population and the additional risk of visual impairment outside of DR [20,26]. |
High risk of developing DR with chronic hyperglycemia for more than 5 years [26]. | Abnormal angiogenesis Inflammation Dyslipidemia Similar genetic correlations with others. Dysbiosis of the ocular and intestinal microbiota. [26,81,82]. |
Old age Cardiovascular diseases Fatness Intestinal diseases [26,82]. |
| Dry eye syndrome |
Higher prevalence from 20% to 53% in patients with diabetes and others compared to the general population [91,92]. |
High risk in uncontrolled diabetes [92]. | Similar genetic correlations with others. Instability of the tear film. Hyperosmolarity. Chronic inflammation. Violation of the production of tear proteins. Structural abnormality in the corneal nerve fibers. Autonomic neuropathy [93,94]. |
Old age Fatness Encephalopathy Cardiovascular diseases [92,95]. |
Table 3.
Current and Emerging Therapies for Diabetic Retinopathy. Comparison of therapies based on targets, mechanisms of action, and clinical development stage. (Adapted from Boye et al., 2014; Dugel et al., 2020.).
Table 3.
Current and Emerging Therapies for Diabetic Retinopathy. Comparison of therapies based on targets, mechanisms of action, and clinical development stage. (Adapted from Boye et al., 2014; Dugel et al., 2020.).
| Therapy | Target | Mechanism | Clinical Stage |
| Anti-VEGF (e.g., ranibizumab) | VEGF-A | Inhibits angiogenesis | Approved |
| Corticosteroids | Inflammation | Suppress cytokine release | Approved |
| Antioxidants (e.g., lutein) | ROS | Reduces oxidative stress | Preclinical/Clinical |
| Gene therapy | VEGF, PEDF | Long-term suppression or overexpression | Experimental |
| Stem cell therapy | Retinal regeneration | Replaces damaged cells | Experimental |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



