Submitted:
24 September 2025
Posted:
25 September 2025
Read the latest preprint version here
Abstract
Background/Objectives: Multiple myeloma (MM) remains incurable despite decades of pharmacological advances. Triplet and quadruplet regimens improve survival, yet their cumulative toxicity and escalating costs limit long-term value. Cellular immunotherapies such as BCMA-directed CAR-T cells have demonstrated unprecedented efficacy, but they are often reserved for late relapse, when benefit is reduced. This study aimed to evaluate the cost-effectiveness of CAR-T compared with historical and contemporary regimens. Methods: We developed a cost-effectiveness framework using ECOG performance-based utility scores to calculate quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs). Historical treatments were anchored to Dr. Solly’s 1844 case as baseline, while modern regimens and CAR-T trials were analyzed using stand-ardized survival and drug cost data. A See-Saw model was applied to visualize cumula-tive QALY and ICER values across treatment sequences. Results: Conventional regimens frequently exceeded USD 3–4 million per patient with limited QALY gains. In contrast, BCMA-directed CAR-T therapies (ide-cel, cilta-cel), despite 2025 upfront costs of USD 700,000–1,000,000, produced superior ICER values and higher cumulative QALYs, par-ticularly in high-risk and refractory cohorts. Earlier integration of CAR-T projected both economic and clinical superiority, while delayed use reduced its effectiveness. Conclu-sions: Our analysis reframes CAR-T as not a financial burden but a cost-effective, ethically imperative therapy. Earlier adoption could reduce cumulative expenditure, enhance qual-ity-adjusted survival, and mitigate inequities in MM care. Aligning innovation with access is essential to ensure that the right to live longer and better does not depend on wealth.
Keywords:
multiple myeloma
; CAR-T Cell Therapy
; QALY
; Patient-centered outcomes
1. Introduction
Dedication This work is dedicated to all patients and families living with multiple myeloma, whose resilience continues to inspire. Our goal is not only to advance science, but to restore dignity, equity, and hope in treatment. May these findings serve as a reminder that true progress is measured not solely in survival curves, but in the quality of lives preserved.
Multiple myeloma is a clonal plasma cell malignancy marked by progressive marrow infiltration, end-organ damage, and inevitable relapse. Over the past two decades, therapeutic advances including immunomodulatory drugs (IMiDs), proteasome inhibitors (PIs), monoclonal antibodies, and multidrug combinations have improved survival, yet the disease remains incurable [1].
Despite these innovations, current practice still relies heavily on mid-20th century strategies such as alkylating agents and high-dose melphalan with autologous stem cell transplantation. These regimens, though foundational, dominate frontline algorithms and accumulate toxicity over time. Successive therapies often drive marrow exhaustion, T-cell dysfunction, and reduced eligibility for advanced immunotherapies [2,3,4].
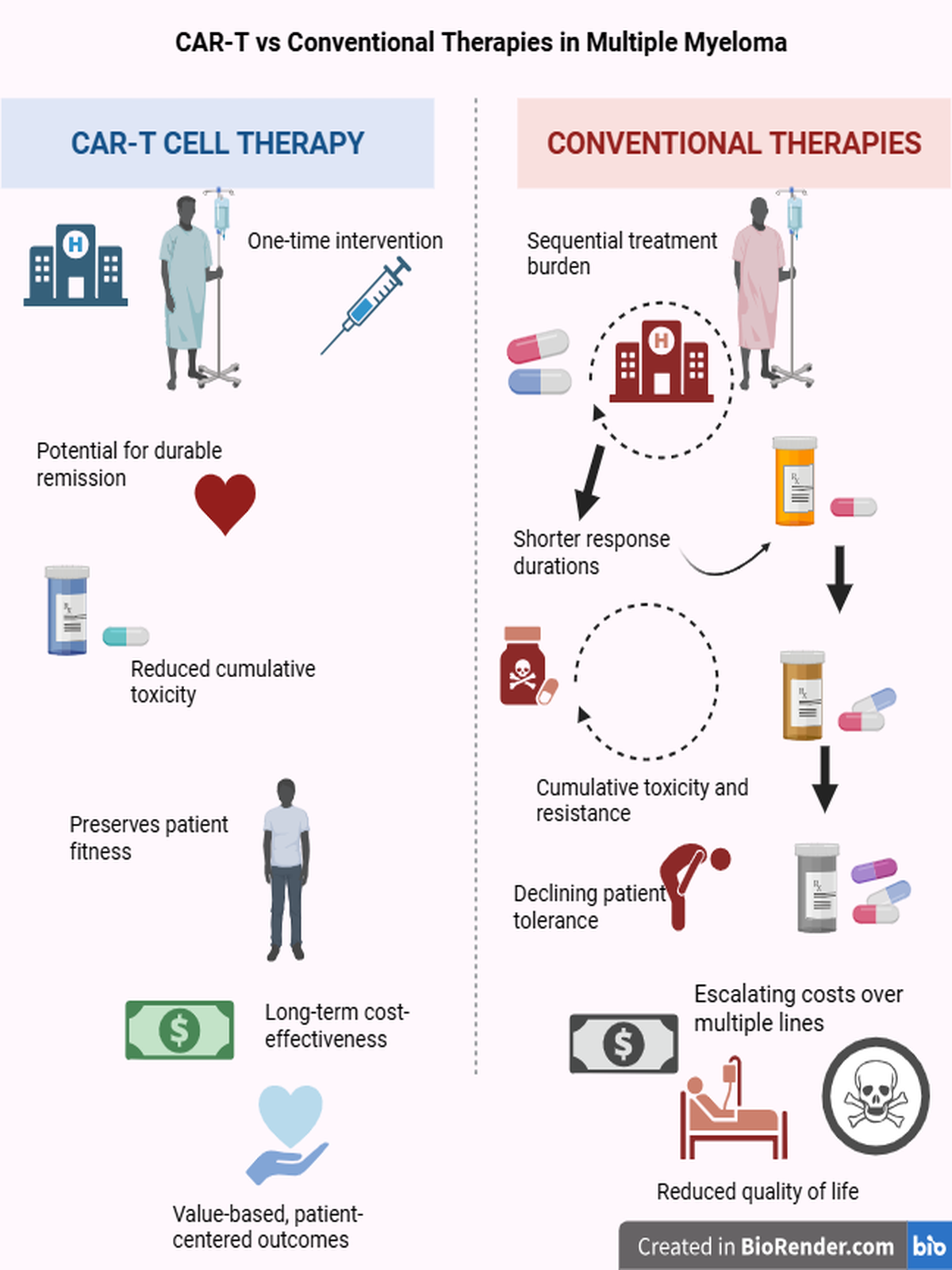
Consequently, patients encounter novel options like chimeric antigen receptor (CAR) T-cell therapy only after years of exposure to less effective and toxic regimens precisely when risk is highest and benefit attenuated. This entrenched sequencing reflects not only clinical inertia but also economic prejudice, with CAR-T frequently dismissed as prohibitively expensive.
Here, we reframe the role of CAR-T in multiple myeloma. Integrating survival outcomes with quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs), we demonstrate that the value of CAR-T surpasses conventional approaches when analyzed in terms of both efficacy and cost-utility. By emphasizing timing and measurable benefit, we argue that CAR-T should be reconsidered not as a last-resort experiment, but as a rational and pragmatic therapeutic option.
2. Myeloma Therapies
Cancer has been recognized since antiquity, with treatments ranging from heavy metals and herbal remedies to surgical resection and dietary interventions. Multiple myeloma, however, was first described in the 1840s, and early therapies included rhubarb, opium, corsets, and leeches rudimentary measures that reflect both the limits and persistence of early medical practice [5]. Multiple myeloma (MM) is a plasma-cell malignancy and the second most common haematological cancer, predominantly affecting older adults. It is characterised by clonal plasma-cell expansion, monoclonal protein secretion, and organ damage defined by the CRAB criteria (hypercalcaemia, renal impairment, anaemia, bone disease) [1].
Over the past two decades, treatment has evolved from conventional alkylators and autologous stem cell transplantation to immunomodulatory drugs (IMiDs), proteasome inhibitors (PIs), and monoclonal antibodies, increasingly delivered in triplet or quadruplet regimens. Despite these advances, MM remains incurable: drug-resistant subclones persist, survival plateaus at ~50% at 5 years, and outcomes vary widely across countries depending on healthcare access. The need for transformative therapies is therefore pressing [6].
The 20th century reshaped oncology through global upheavals. Both World Wars accelerated scientific discovery, and in the post-war era, multiple myeloma reached its first true therapeutic milestone with the advent of bone marrow transplantation [7,8,9]. Until the early 2000s, myeloma management reflected a broader pharmacological paradigm drug development was largely driven by geopolitical competition and the pharmaceutical race that followed. As a result, treatment remained anchored in successive pharmacologic regimens, mirroring the trajectory of many solid and hematologic malignancies. Only in recent years has the field shifted toward cellular and immune-based therapies, reopening a vision reminiscent of ancient holistic medicine one that emphasizes individualized, patient-centered, and precision-guided approaches.
The Cold War transformed oncology into a pharmacological race. In the context of geopolitical rivalry, successive drugs were rapidly synthesized and introduced, often without long-term evaluation [10]. Even tragedies such as the thalidomide [11] disaster did not halt this momentum; instead, compounds were reformulated and reintroduced, spawning analogs such as lenalidomide and pomalidomide alongside dexamethasone-based regimens. Melphalan, itself derived from nitrogen mustard used as chemical warfare in the First World War [12], remains embedded in frontline myeloma protocols to this day. Our purpose is not to discard therapies that still provide benefit, but to critically reassess toxic, decades-old regimens and create space for more effective, safer, and innovative approaches. In this context, the entrenched skepticism toward cellular therapies such as CAR-T reflects inertia rather than evidence (Table 1).
Today the therapeutic landscape of multiple myeloma shifted toward more targeted drug classes. Proteasome inhibitors, HDAC6 inhibitors, and XPO1 inhibitors represented a new generation of pharmacology still drug-based, but increasingly mechanism-specific. In parallel, monoclonal antibody development brought therapies such as daratumumab into clinical practice, marking a departure from purely cytotoxic regimens toward immune-based approaches [1,6]. This period bridged the traditional chemotherapeutic era and today’s paradigm of cellular and precision-guided therapies (summarized in Table A1 (Appendix A).)
Importantly, in this modern era, treatment success is no longer defined solely by survival gains; quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs) have emerged as essential metrics, reflecting that efficacy must be weighed against toxicity, cost, and patient quality of life.
Although multiple myeloma originates from clonal plasma cells, it is no longer regarded as a purely cell-autonomous disease. The bone marrow microenvironment (BMME) provides the niche that sustains hematopoiesis and immune surveillance, but in MM this architecture is hijacked tumor cells evade immune detection, suppress hematopoiesis, and promote osteolysis and infection risk. Resistance often stems not only from the tumor cell itself but also from stromal, immune, and endothelial interactions [24,25,26]. This paradigm has redirected therapeutic strategies toward targeting both the tumor and its niche. Approaches include adhesion inhibitors (e.g., VLA-4 antagonists), cytokine/chemokine blockade (IL-6, CXCR4), anti-angiogenic and osteoclast-inhibiting therapies, and immunotherapies such as CAR-T cells, bispecific antibodies, and checkpoint blockade. Exosome-disrupting agents are also under investigation for interrupting intercellular communication [27,28,29].
Among immune-based strategies, antibody-drug conjugates (ADCs) provide proof of principle. Belantamab mafodotin, an anti-BCMA ADC, showed activity in triple-class refractory disease in the DREAMM-2 [30] trial but was limited by ocular toxicity, leading to its withdrawal from the US market. Nevertheless, it remains under study in combination regimens and in settings where CAR-T or bispecifics are not available, illustrating the expanding but heterogeneous nature of the BCMA-targeting arsenal [31].
3. From Immunotherapy Origins to Car-T
Immunotherapy has long been intertwined with oncology, tracing back to William Coley’s late 19th-century bacterial vaccines, which for the first time suggested that immune activation could drive tumor regression. Though primitive, Coley’s toxins reframed cancer as more than a cell-autonomous disease [32]. This idea re-emerged in the cytokine era of the 1970s and 1980s, when interferon-α and interleukin-2 were introduced into clinical oncology. These agents revealed the capacity of exogenous immune stimulation to induce tumor responses, yet their efficacy was modest and toxicity profound, underscoring the need for more precise immune manipulation.
The 1990s marked the true molecular revolution. Advances in genetic engineering enabled the creation of T-cell receptors with redirected specificity, and in 1993 the first chimeric antigen receptor (CAR) was described. By fusing an antibody-derived binding domain with intracellular signaling motifs, CARs could bypass MHC restriction and target tumor antigens directly. The incorporation of co-stimulatory domains such as CD28 and 4-1BB further enhanced T-cell persistence, expansion, and metabolic fitness, transforming early prototypes into clinically viable platforms [33,34].
Proof of principle came with CD19-directed CAR-T cells. Preclinical experiments demonstrated regression of aggressive B-cell lymphomas in murine models, followed by remarkable clinical responses in patients with relapsed or refractory acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), and non-Hodgkin lymphoma. Deep and durable remissions, accompanied by the persistence of functional memory T cells, established CAR-T therapy as one of the most disruptive innovations in hematology [35,36,37,38] (see Figure 1).
For multiple myeloma, these breakthroughs were especially consequential. Myeloma had long been treated with successive pharmacological regimens that yielded incremental benefits but failed to overcome relapse biology. The ability to engineer autologous T cells against plasma cell antigens most notably B-cell maturation antigen (BCMA) opened a new therapeutic horizon. CAR-T was no longer an experimental curiosity confined to lymphoid malignancies, but a rational extension into plasma cell disorders, with the promise of converting transient responses into durable remissions [35,38].
4. First in Class Approvals: Ide-Cel and Cilta-Cel
The therapeutic milestone for multiple myeloma arrived with B-cell maturation antigen (BCMA) as a target. Two autologous CAR-T products are now approved. Idecabtagene vicleucel (ide-cel, Abecma) received FDA approval in April 2021 (KarMMa trials) and, in heavily pretreated patients (≥3 prior lines including PI, IMiD, and anti-CD38), achieved an overall response rate (ORR) of 76% versus 32% with standard care, ≥VGPR of 58% versus 14%, one-year progression-free survival (PFS) of 55% versus 30%, and minimal residual disease (MRD) negativity of ~20%. Common toxicities include neutropenia, leukopenia, and cytokine release syndrome (CRS), with grade ≥3 CRS in ~14% [39,40].
Ciltacabtagene autoleucel (cilta-cel, Carvykti) received FDA approval in February 2022 as a second-generation BCMA CAR-T with dual epitope binding, demonstrating median overall survival (OS) of ~56 months, median PFS of ~18 months, and MRD negativity of ~68% by 2025 analyses. Toxicities include CRS (mostly low-grade), ICANS, cytopenias, and infections [39,41]. Despite transformative efficacy, accessibility remains limited: ide-cel is available in only a handful of countries (United States, France, Switzerland, Japan, Germany), while cilta-cel is approved only in the United States and Germany, with manufacturing delays and patient selection criteria further restricting broader use [42].
Beyond BCMA, relapse after CAR-T underscores the need for alternative strategies, including novel targets such as CS1/SLAMF7, CD138, GPRC5D, and FcRH5 to circumvent BCMA-negative relapse; enhanced designs such as dual-target CARs (e.g., BCMA + CS1), armored CAR-Ts secreting cytokines (IL-15), and allogeneic “off-the-shelf” constructs to reduce antigen escape and overcome manufacturing bottlenecks; and combination approaches integrating CAR-T with IMiDs, checkpoint inhibitors, or γ-secretase inhibitors to deepen and prolong responses [39].
5. Why Bcma Is an Ideal Target in Multiple Myeloma
B-cell maturation antigen (BCMA, also known as TNFRSF17) has emerged as the leading target for cellular and antibody-based immunotherapies in multiple myeloma. Several biological features make BCMA uniquely suitable: it is highly and consistently expressed on malignant plasma cells with limited distribution in normal tissues, thereby reducing off-tumor toxicity; it plays a central role in plasma cell survival through interactions with ligands such as BAFF and APRIL, meaning that its blockade not only identifies but also biologically disrupts myeloma cell fitness; its high antigen density enhances CAR-T recognition and killing efficiency; and, unlike CD19 or CD20 in other B-cell malignancies, its expression persists even in late-stage and refractory disease, allowing targeting across multiple treatment lines. These properties explain why BCMA-directed CAR-T therapies (ide-cel, cilta-cel) have achieved deep and durable responses and why BCMA has become the benchmark target for bispecific antibodies and antibody–drug conjugates. At the same time, however, antigen escape and downregulation underscore the need for next-generation approaches such as dual-target CARs, armored constructs, and alternative antigens (CS1, GPRC5D, FcRH5) to sustain efficacy [43].
6. Challenges and Future Directions
CAR-T cell therapy introduces unique risks-CRS, ICANS, prolonged cytopenias that demand specialized management. Furthermore, relapse mechanisms include antigen loss, T-cell exhaustion, and microenvironmental resistance. Integration with biomarker-guided monitoring, earlier-line application, and rational combinations will be crucial to sustain durable benefit [44]. Most importantly, success is not defined by survival curves alone. In an era of rising healthcare costs, QALY and ICER analyses contextualize CAR-T within a framework of value, not just efficacy. These metrics suggest that CAR-T, though logistically demanding, offers pragmatic and measurable benefit compared with entrenched, toxic regimens.
CAR-T therapies such as ide-cel and cilta-cel have shown remarkable efficacy, yet access remains limited. Ide-cel is available only in a handful of countries including the United States, France, Switzerland, Japan, and Germany while cilta-cel is currently approved in just the United States and Germany. Even where approvals exist, practical barriers slow down implementation: manufacturing slots are scarce, certified centers are few, and referral often comes very late in the disease course. By the time patients reach CAR-T, they have already received multiple lines of toxic therapy, their T cells are exhausted, and the window for maximum benefit has narrowed [42]. (see Figure 2 for therapy path).
This delay feeds into the common prejudice that CAR-T is “too expensive for too little gain.” In reality, cost should be seen in context. Traditional myeloma care relies on years of continuous drug combinations, hospital visits, toxicity management, and supportive treatments each with its own burden and expense. A one-time CAR-T infusion is often labeled as “too expensive,” largely because the entire cost is charged upfront. Yet when placed in context, the picture changes. Patients with multiple myeloma routinely cycle through years of triplet or quadruplet drug regimens, autologous stem cell transplantation (ASCT), and supportive care. The cumulative cost of these conventional strategies many of which extend life by only a few years can approach or even exceed 3 million USD per patient [45,46,47,48]. By contrast, CAR-T consolidates this expense into a single treatment, with the potential for deeper and longer-lasting remissions. In countries where CAR-T is approved, much of the cost is already covered by national health systems; the “sticker shock” comes not from actual excess, but from the visibility of a lump-sum charge. In reality, it is the so-called “cheaper” therapies that often prove more expensive in the long run, while CAR-T offers a concentrated investment with measurable value. Indeed, when the cost of ASCT is combined with years of ongoing pharmacological regimens, the total expense often surpasses that of CAR-T, underscoring the need to reassess what we call “expensive” or “affordable [42].
More importantly, treatment success today is not measured only in how long patients live, but also in how well they live. Analyses of quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs) suggest that CAR-T can deliver measurable value, especially if used earlier in the treatment course.
Instead of asking whether CAR-T is “too expensive,” the more relevant question is whether we are using it at the right time and in the right patients. Earlier referral, streamlined manufacturing, and safer outpatient management of toxicities could improve both patient outcomes and cost-effectiveness. Seen through this lens, CAR-T is not a last-resort luxury, but a rational, pragmatic therapy that deserves a central place in modern myeloma care.
7. Materials and Methods
This study analyzed historical and current treatment strategies for multiple myeloma (MM) in terms of cost, treatment duration, and mean overall survival (OS). When available, Kaplan-Meier survival curves were digitized using WebPlotDigitizer. The area under the curve (AUC) was estimated via the trapezoidal rule to calculate mean OS. Accuracy was cross-validated through geometric approximation and visual estimation. The graphs of the obtained data were analyzed using Graphpad Prism 8 (see method abstract below Figure 3).
In cases where Kaplan-Meier plots were unavailable and mean OS was not explicitly reported, median OS values were extracted and multiplied by a correction factor of 1.3, as recommended by prior modeling studies [49,50] , to approximate mean OS. All OS values were converted into total days using the standard monthly average (30.44 days).
We developed a novel ECOG-based QALY framework tailored for multiple myeloma. Each therapy was assigned quality-of-life weights according to ECOG performance status, and QALYs were derived by combining these coefficients with survival data from phase II/III trials. Drug costs were retrieved from publicly available pricing sources (e.g., Drugs.com), and incremental cost-effectiveness ratios (ICERs) were calculated by comparing total cost per QALY gained across regimens.
To anchor the analysis historically, we used Samuel Solly’s first reported myeloma case in 1844 as a baseline comparator: one year of survival, assumed at ECOG 3, treated with rhubarb and opium at negligible cost. This provided a reference point against which modern therapies could be contextualized. All therapies from early alkylating agents to contemporary CAR-T products were evaluated using the same assumptions and optimization model, enabling direct comparison across eras.
Treatment duration was modeled in cycles by dividing survival time by average cycle length, with drug dosages calculated assuming full administration across standardized body parameters (BSA 1.73 m², weight 70 kg). Costs were derived from dosing requirements and public pricing data.
Health-related quality of life (HRQoL) was estimated using a novel ECOG-based utility model, developed to compensate for the lack of validated mappings between ECOG status and utility values in multiple myeloma. While frameworks such as EQ-5D and EORTC exist in other malignancies, no standard approach was available for MM; thus, we constructed a consensus utility scale that reflects the disease’s chronic yet progressive course.
- ECOG 0 → 0.9
- ECOG 1 → 0.7
- ECOG 2 → 0.5
- ECOG 3 → 0.3
- ECOG 4 → 0.1
- ECOG 5 → 0
Research manuscripts reporting large datasets that are deposited in a publicly available database should specify where the data have been deposited and provide the relevant accession numbers. If the accession numbers have not yet been obtained at the time of submission, please state that they will be provided during review. They must be provided prior to publication.
These estimates are not empirically derived but provide a transparent and reproducible framework for scenario-based cost-utility modeling. The scale balances optimistic full-health assumptions against conservative underestimation and enables comparative evaluation across treatment strategies within a consistent methodological structure. Quality-adjusted life years (QALYs) were calculated as the product of estimated mean overall survival and the corresponding utility score derived from ECOG performance status:
QALY= Life years x Utility
Cost-effectiveness was evaluated using the standard incremental cost-effectiveness ratio (ICER) formula:

Historical anchor: The earliest reported myeloma case, described by Dr. Samuel Solly in 1844, survived approximately 12 months after diagnosis and was treated with rhubarb, opium, and orange peel supportive rather than disease-modifying therapy. Based on functional decline, we estimated a Karnofsky score <50 (ECOG 3), corresponding to a utility value of 0.3. This case was used as a baseline reference (ΔQALY = 0.3) against which subsequent therapeutic developments were contextualized (see details Supplementary Tables S2–S5, Appendix A).
Introducing the See-Saw Framework to illustrate the cumulative therapeutic burden: Across stratified patient populations in multiple myeloma (MM), we introduce the See-Saw Model) a conceptual and visual framework designed to complement traditional cost-effectiveness approaches. Unlike conventional models that evaluate isolated treatment regimens, the model integrates:
- Total ICER values
- QALY outputs
- Across transplant-eligible, ineligible, and frail patient groups
This framework visually demonstrates the disproportionate economic and clinical load borne by different subgroups, highlighting how high-cost, low-benefit regimens can destabilize overall health system equity especially in vulnerable populations. Designed for accessibility and adaptability, the model serves as a practical decision-support tool for:
- Policymakers
- Clinicians
- Health economists
It can be applied to both disease-specific evaluations and broader healthcare resource allocation analyses.
8. Results
8.1. Therapy Costs
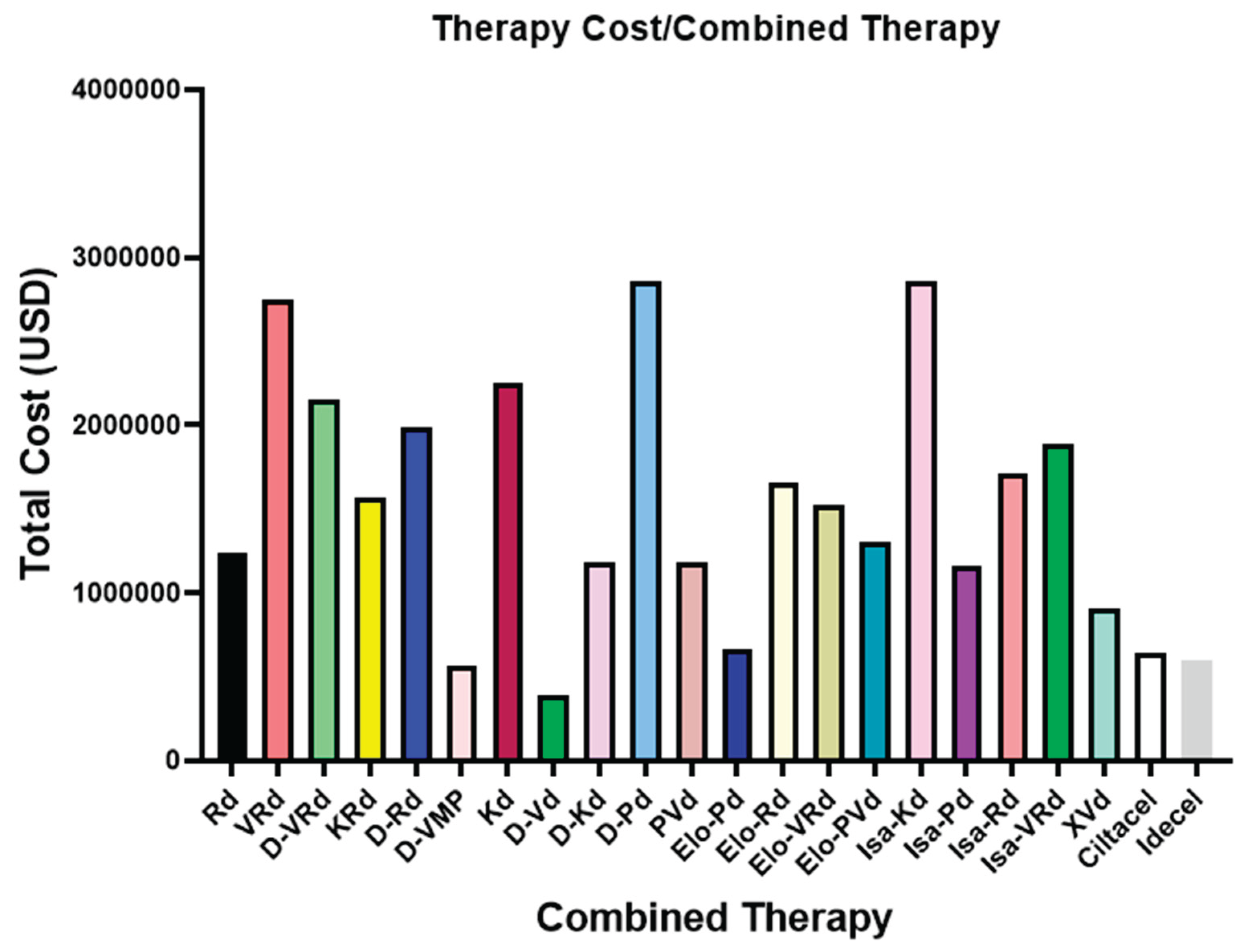
The cumulative costs of myeloma therapies varied widely across both monotherapy and combination regimens. As shown in Appendix B; Figure B1 [51,52,53,54,55,56,57,58,59,60,61] and Figure B2 [61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91] (Supplementary Figure S1,S2) traditional agents such as melphalan remain relatively inexpensive, while prolonged regimens based on immunomodulatory drugs, proteasome inhibitors, or monoclonal antibodies accumulate costs exceeding one million USD. Combination therapies such as VRd, D-VRd, and Isa-VRd often surpass 2-3 million USD per patient, reflecting not only drug prices but also prolonged treatment duration. By contrast, the upfront costs of CAR-T therapies (ide-cel, cilta-cel) appear high but remain comparable or in some cases lower than the cumulative expense of multi-year pharmacological strategies (Supplementary Material Table S1,S2).
8.2. QALY Outcomes
While conventional and combination regimens often achieve measurable improvements in survival, their QALY profiles reveal important nuances. Low-intensity regimens such as elotuzumab-based combinations (Elo-Pd, Elo-Rd, Elo-VRd) provide only modest gains (2–3 QALYs) despite prolonged administration. Patients remain under continuous drug exposure, with accumulating toxicity and diminished quality of life. In contrast, cilta-cel consistently outperforms expectations, delivering more than 3.5 QALYs as a one-time therapy exceeding the cumulative benefit of multi-drug regimens such as Elo-based protocols. This paradox highlights a key message: treatments that appear “lighter” or less toxic can, over time, yield less value than an intensive but finite cellular intervention. Similarly, isatuximab and daratumumab improve QALY relative to historical standards but still require ongoing cycles. CAR-T, by eliminating the need for continuous therapy, reframes cost-effectiveness in terms of both financial and human burden. QALY gains with cilta-cel are not only higher, but cleaner: patients spend more time off treatment and in better health (see Figure 4) [51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91]. Importantly, elotuzumab-based regimens are typically administered before referral to CAR-T therapy. Despite being delivered later in the disease course, when patients are more fragile and their T-cell fitness diminished, cilta-cel still surpasses Elo-based combinations in QALY gain. This finding strongly argues against the perception of CAR-T as a “last-resort” option and supports its evaluation in earlier treatment lines, where preserved immune function could further enhance its cost-effectiveness (Supplementary Table S3,S4).
8.3. ICER Comparisions.
Incremental cost-effectiveness ratios (ICERs) revealed striking discrepancies between perceived and actual therapeutic value (see Appendix B, Figure 3 and Figure 4) [51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91]. Traditional agents such as melphalan appeared inexpensive with low ICERs, but their clinical benefit was minimal, rarely exceeding 1 QALY. By contrast, widely used immunomodulators and proteasome inhibitors (e.g., lenalidomide, pomalidomide, bortezomib) displayed elevated ICERs due to high cumulative drug costs and only modest quality-adjusted survival gains. Monoclonal antibodies (daratumumab, isatuximab) improved QALY relative to older regimens but incurred ICER values in the mid-to-high range, reflecting ongoing costs of continuous therapy. Elotuzumab-based combinations were particularly notable: despite being perceived as relatively “light” and tolerable, they generated some of the highest ICERs across combination regimens, underscoring poor value when cost is normalized to QALY gain. In contrast, BCMA-directed CAR-T therapies demonstrated a paradoxical profile. While upfront costs were high, their ICER values were lower than many multi-drug regimens. For example, cilta-cel exhibited one of the most favorable ICERs among modern therapies, outperforming continuous regimens that accumulate costs over years. Even when administered late in the disease course, CAR-T provided superior cost-effectiveness relative to several pharmacological strategies, challenging the notion that it is prohibitively expensive. Taken together, these ICER comparisons highlight the importance of evaluating therapies not by sticker price alone, but by their cost per quality-adjusted year of life. By this standard, CAR-T stands not as an outlier of excess, but as a rational and value-driven therapy in multiple myeloma (Supplementary Figure S5,S6).
8.4. Aggregated Cost–Effectiveness Outcomes and the See-Saw Model
To capture the cumulative burden of sequential therapies, we introduced the concept of cumulative QALY and cumulative ICER. These measures were derived by summing quality-adjusted survival and incremental cost-effectiveness across all therapeutic lines, thereby reflecting the true longitudinal impact of treatment sequencing.
As shown in Table 2, transplant-eligible low/intermediate-risk patients achieved the most favorable balance, with cumulative ICER values around 3.4 million USD/QALY and cumulative QALY gains approaching 18.5. In contrast, high-risk transplant-ineligible patients fared poorly, with cumulative ICERs exceeding 5 million USD/QALY despite achieving only 13.5 QALYs.
This indicates that repeated pharmacological layering in high-risk patients leads to diminishing value returns [61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91]. To visualize this dynamic, we applied the See-Saw Model (Figure 5).
The ICER panel demonstrates that the cumulative economic burden tilts toward high-risk, transplant-ineligible patients, reflecting greater cost-effectiveness challenges in this group. By contrast, the QALY panel shows the balance favoring transplant-eligible patients (both low- and high-risk), who accumulate the largest quality-adjusted survival gains. This divergence highlights the complexity of modern myeloma care: the populations deriving the greatest clinical benefit are not necessarily those for whom therapies are most cost-effective. This model should be interpreted as a pilot conceptual framework, based on the most recent phase II/III clinical trial data rather than a meta-analysis, acknowledging the limited availability of long-term outcomes for novel therapies.
In this framework, transplant eligibility and risk status act as opposing forces:
This see-saw representation underscores the inequity embedded within current sequencing paradigms: the patients most in need of innovation (high-risk, ineligible populations) derive the least value from conventional pharmacological escalation.
9. Discussion
Multiple myeloma has transitioned from a disease once managed with purely palliative strategies to one treated with targeted, immunologic, and gene-modified approaches. Our analysis demonstrates that evaluating therapies only by survival endpoints or upfront cost is incomplete; instead, quality-adjusted survival and long-term value must guide decision-making.
Historically, therapies perceived as “cheap” such as melphalan or corticosteroid-based regimens achieved minimal QALY gains (≤1.0). In contrast, modern triplet and quadruplet regimens frequently exceed USD 3-4 million per patient over the course of treatment, while delivering only moderate improvements in QALY and survival. This creates a paradox: what appears affordable is often the most expensive when cumulative costs are considered, and what appears prohibitively expensive CAR-T therapy may in fact deliver the best value. Our ICER results confirm that cilta-cel, despite upfront pricing of USD 700,000–1,000,000 in 2025, outperforms many continuous regimens in terms of cost per QALY gained.
CAR-T is currently approved as a late-line therapy, typically offered after years of treatment, immune exhaustion, and marrow toxicity. Even under these compromised conditions, CAR-T outperforms several regimens, including elotuzumab-based combinations. This strongly suggests that earlier deployment, in fitter patients, would amplify both QALY gains and cost-effectiveness. Delaying access does not merely reduce efficacy; it represents an ethical failure, withholding the most effective therapy until its benefit is blunted.
The restricted availability of CAR-T (ide-cel and cilta-cel approved in only a few countries) creates profound inequities. Patients in high-income settings may receive one-time cellular therapy with durable remission, while patients in lower-resource regions remain trapped in cycles of outdated or toxic pharmacological regimens. From a health policy perspective, reimbursement structures must recognize that upfront CAR-T costs replace years of cumulative drug expenditure, hospitalizations, and toxicity management. Governments already absorb the majority of these expenses; redirecting investment toward CAR-T would reduce long-term costs and improve outcomes.
Value in oncology cannot be reduced to survival curves alone. Reports of depression and even suicide among trial participants remind us that biological success without dignity is human failure. Quality of life must be central to therapeutic evaluation. Our QALY framework provides one such tool, quantifying not only time lived but how that time is experienced.
The current sequencing paradigm compounds inequity: those at highest risk and least transplant-eligible derive the least cumulative value, as illustrated by our See-Saw model. Meanwhile, access to CAR-T is dictated by geography and wealth rather than biology or need. The right to live longer and better should not depend on financial privilege. True progress in multiple myeloma requires aligning science with justice, compassion, and reform ensuring that the benefits of innovation are shared equitably across populations.
10. Conclusions
Multiple myeloma has evolved from a fatal, palliatively managed disease into one where cellular immunotherapies redefine the horizon of survival. Yet cost and access remain at the center of debate. Our QALY and ICER based framework demonstrates that long-term pharmacological sequencing is not only toxic but cumulatively more expensive than CAR-T therapy, despite the latter’s high upfront price. Importantly, delaying CAR-T until late relapse diminishes its value; earlier integration could maximize both clinical benefit and cost-effectiveness. Beyond numbers, this is an ethical imperative: patients deserve not only longer lives, but better ones. Ensuring equitable access to CAR-T and other advanced therapies requires policy reform that aligns innovation with justice, sustainability, and human dignity.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Guluzar Gulnur Itez and Asuman Sunguroglu; methodology, Guluzar Gulnur Itez; validation, Guluzar Gulnur Itez and Asuman Sunguroglu; formal analysis, Guluzar Gulnur Itez; investigation, Guluzar Gulnur Itez; resources, Asuman Sunguroglu; data curation, Guluzar Gulnur Itez; writing original draft preparation, Guluzar Gulnur Itez; writing review and editing, Guluzar Gulnur Itez and Asuman Sunguroglu; visualization, Guluzar Gulnur Itez; supervision, Asuman Sunguroglu; project administration, Asuman Sunguroglu; funding acquisition, Asuman Sunguroglu. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by Ankara University, Institute of Health Sciences.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created in this study. Data supporting the findings of this study are available within the cited clinical trial publications.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (GPT-5, OpenAI, 2025) for assistance with text refinement and figure caption editing. The authors reviewed and edited all outputs and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ADC | Antibody-Drug Conjugates |
| ALL | Acute Lymphoblastic Leukemia |
| APRIL | A Proliferation-Inducing Ligand |
| ASCT | Autologous Stem Cell Transplantation |
| BAFF | B cell-activating factor belonging to the TNF family |
| BCMA | B-Cell Maturation Antigen |
| BMME | Bone Marrow Microenvironment |
| CAR-T | Chimeric Antigen Receptor T |
| CD | Cluster of Differentiation |
| CLL | Chronic Lymphocytic Leukemia |
| CRAB | (hypercalcaemia, renal impairment, anaemia, bone disease) |
| CRS | Cytokine Release Syndrome |
| CXCR4 | Chemokine Receptor Type 4 |
| ECOG | The Eastern Cooperative Oncology Group |
| FDA | Food and Drug Administration |
| HD | High-Dose |
| HDAC6 | Histone Deacetylase 6 |
| ICAN | Immune Effector Cell-Associated Neurotoxicity |
| ICER | Incremental Cost-Effectiveness Ratios |
| ImiDs: | Immunomodulatory Drugs |
| IL | Interleukin |
| MHC | Major Histocompatibility Complex |
| MM | Multiple Myeloma |
| MRD | Minimal Residual Disease |
| NDMM | Newly Diagnosed Multiple Myeloma |
| ORR | Overall Response Rate |
| PFS | Progression-Free Survival |
| PIs | Proteasome Inhibitors |
| QALYs | Quality-Adjusted Life Years |
| XPO1 | Exportin 1 |
| USD | United States Dollar |
| VGPR | Very Good Partial Response |
| VLA-4 | Integrin α4β1 (very late antigen-4) |
Appendix A
Appendix A.1

Table A1.
Modern Therapies in Multiple Myeloma: Clinical Role
| Therapy / Class | Year (Approval / Milestone) | Mechanism / Target | Current Use in MM | Key Toxicities |
|---|---|---|---|---|
| Autologous Stem Cell Transplant (ASCT) [19] | 1983 (MM application) | Hematopoietic rescue | Standard in eligible patients | Myelosuppression, infection risk |
| Bortezomib (first PI) [20,21] | 2003 | Reversible 20S proteasome inhibitor | Backbone of induction (VRd etc.) | Peripheral neuropathy |
| Carfilzomib (2nd-gen PI) [21] | 2012 | Irreversible PI | Relapsed/refractory, combo regimens | Cardiac toxicity |
| Ixazomib (oral PI) [21] | 2015 | Oral PI | Maintenance, frail patients | GI, mild cytopenias |
| Thalidomide (IMiD) reintroduced [11] | 1997 (MM) | Immunomodulation, anti-angiogenesis | Limited due to toxicity | Neuropathy, sedation |
| Lenalidomide (IMiD) [22] | 2005 | IMiD, cytokine modulation, T-cell activation | Frontline & maintenance backbone | Cytopenias, thrombosis |
| Pomalidomide (IMiD) [23] | 2013 | Next-gen IMiD | Relapsed/refractory settings | Cytopenias, infections |
| Daratumumab (anti-CD38 mAb) [1,6] | 2015 | ADCC, CDC, ADCP, direct apoptosis | Widely used frontline & RRMM | Neutropenia, infusion reactions |
| Isatuximab (anti-CD38 mAb) [1,6] | 2020 | Distinct CD38 epitope, direct apoptosis | Combo with Pd in RRMM | Neutropenia, infections |
| Selinexor (XPO1 inhibitor) [1,6] | 2019 | Nuclear export inhibition, p53 reactivation | Triple-class refractory | GI toxicity, cytopenias |
| Venetoclax (BCL-2 inhibitor) [1,6] | Investigation | BCL-2 inhibition | Targeted subgroup (t(11;14)) | Tumor lysis, cytopenias |
| Melflufen (peptide-drug conjugate) [1,6] | 2021 (revoked FDA approval) | Alkylating payload via peptide conjugate | EMA-approved, not FDA | Cytopenias, survival concern |
| HDAC inhibitors (e.g. panobinostat) [1,6] | 2015 (panobinostat FDA) | Histone deacetylase inhibition | Adjunct in refractory disease | GI, fatigue, cytopenias |
| Checkpoint inhibitors (PD-1/PD-L1) [1,6] | Trials (halted in MM) | Immune checkpoint blockade | Investigational only | Immune toxicities |
| Bispecific Abs / CAR-T / NK [1,6] | 2020s | Redirected T/NK cytotoxicity | Rapidly emerging | CRS, neurotoxicity, cytopenias |
Appendix B
Figure A1.
Total cost of monotherapies used in the treatment of multiple myeloma. Therapies are ranked from lowest to highest cumulative cost. Data are presented in USD based on 2025 estimated prices. Lenalidomide represents the highest cost burden among all options.
Figure A1.
Total cost of monotherapies used in the treatment of multiple myeloma. Therapies are ranked from lowest to highest cumulative cost. Data are presented in USD based on 2025 estimated prices. Lenalidomide represents the highest cost burden among all options.
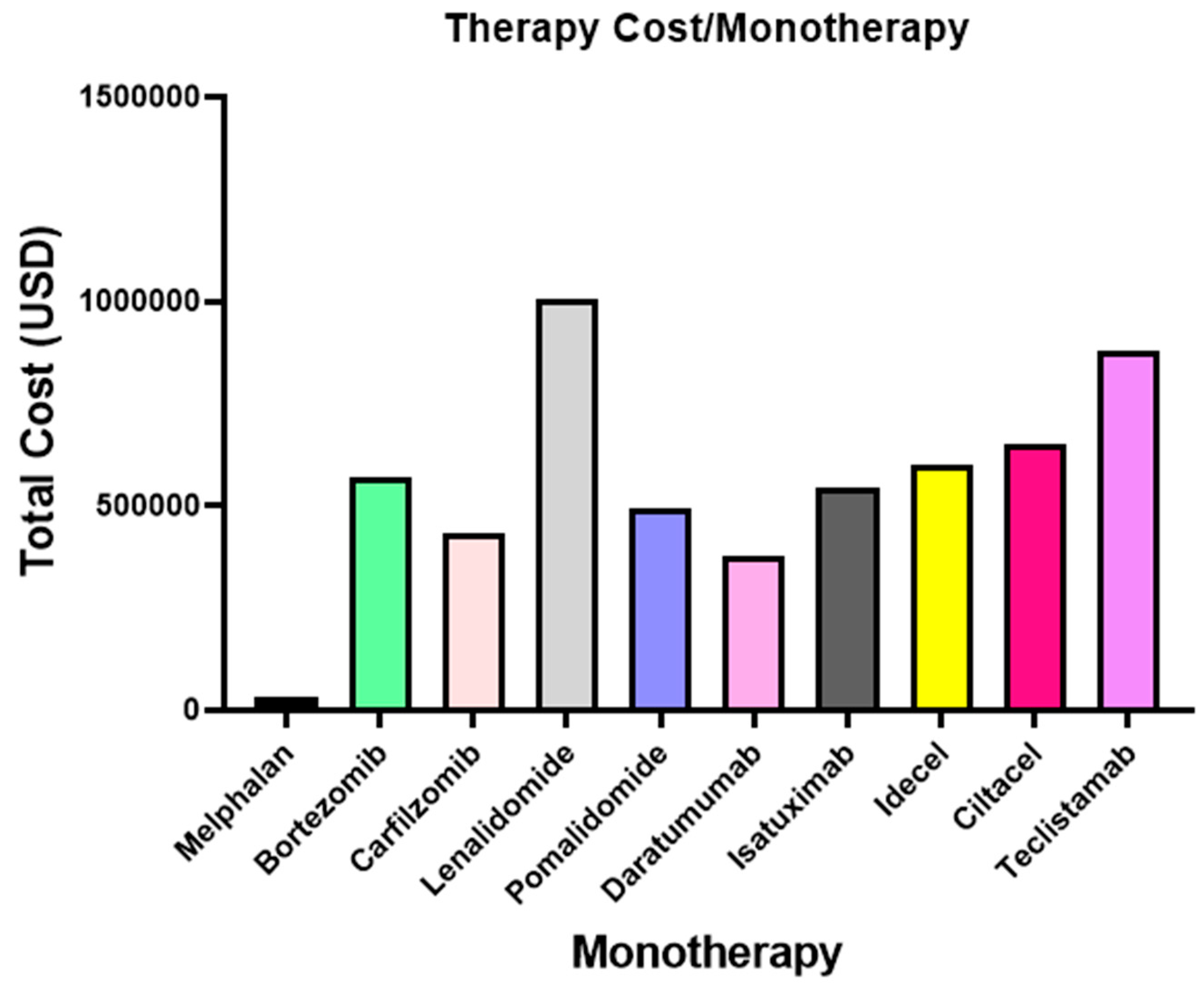
Figure A2.
Total cost of combined therapies used in the treatment of multiple myeloma. Data are presented in USD based on 2025 estimated prices. D-Pd and Isa-Kd represent the highest cost burden among all options.
Figure A2.
Total cost of combined therapies used in the treatment of multiple myeloma. Data are presented in USD based on 2025 estimated prices. D-Pd and Isa-Kd represent the highest cost burden among all options.
References
- Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024 Sep;99(9):1802-1824. doi: 10.1002/ajh.27422. Epub 2024 Jun 28. PMID: 38943315; PMCID: PMC11404783. [CrossRef]
- Binder AF, Walker CJ, Mark TM, Baljevic M. Impacting T-cell fitness in multiple myeloma: potential roles for selinexor and XPO1 inhibitors. Front Immunol. 2023 Oct 26;14:1275329. doi: 10.3389/fimmu.2023.1275329. PMID: 37954586; PMCID: PMC10637355. [CrossRef]
- Kim HY, Moon JY, Ryu H, Choi YS, Song IC, Lee HJ, Yun HJ, Kim S, Jo DY. Bortezomib inhibits the survival and proliferation of bone marrow stromal cells. Blood Res. 2015 Jun;50(2):87-96. doi: 10.5045/br.2015.50.2.87. Epub 2015 Jun 25. PMID: 26157778; PMCID: PMC4486164.
- Krejcik J, Casneuf T, Nijhof IS, Verbist B, Bald J, Plesner T, Syed K, Liu K, van de Donk NW, Weiss BM, Ahmadi T, Lokhorst HM, Mutis T, Sasser AK. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood. 2016 Jul 21;128(3):384-94. doi: 10.1182/blood-2015-12-687749. Epub 2016 May 24. PMID: 27222480; PMCID: PMC4957162.
- Solly S. Remarks on the pathology of mollities ossium; with cases. Med Chir Trans. 1844;27:435-498.8. doi: 10.1177/095952874402700129. PMID: 20895811; PMCID: PMC2116942.
- El Khatib HH, Abdulla K, Nassar LK, Ellabban MG, Kakarougkas A. Advancements in multiple myeloma therapies: a comprehensive review by disease stage. Lymphatics. 2025;3(1):2. [CrossRef]
- Van Way C 3rd. War and Trauma: A History of Military Medicine - Part II. Mo Med. 2016 Sep-Oct;113(5):336-340. PMID: 30228491; PMCID: PMC6139825.
- Smith SL. War! What is it good for? Mustard gas medicine. CMAJ. 2017 Feb 27;189(8):E321-E322. doi: 10.1503/cmaj.161032. PMID: 28246228; PMCID: PMC5325736.
- Gahrton G, Tura S, Ljungman P, Belanger C, Brandt L, Cavo M, et al. Allogeneic bone marrow transplantation in multiple myeloma. European Group for Bone Marrow Transplantation. N Engl J Med. 1991 Oct 31;325(18):1267-73. doi: 10.1056/NEJM199110313251802. PMID: 1922221.
- ALWALL N. Urethane and stilbamidine in multiple myeloma report on two cases. Lancet. 1947 Sep 13;2(6472):388. doi: 10.1016/s0140-6736(47)90375-9. PMID: 20263550.
- Beninger P. Thalidomide: Following tragedy, a repurposed molecule with continuing opportunities for clinical benefit. Clin Ther. 2025;47(4):249–51. [CrossRef]
- Goodman LS, Wintrobe MM, Dameshek W, Goodman MJ, Gilman A, McLennan MT. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl) amine hydrochloride and tris(beta-chloroethyl) amine hydrochloride for Hodgkin's disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. By Louis S. Goodman, Maxwell M. Wintrobe, William Dameshek, Morton J. Goodman, Alfred Gilman and Margaret T. McLennan. JAMA. 1984 May 4;251(17):2255-61. doi: 10.1001/jama.251.17.2255. PMID: 6368885.
- Fu W, Bang SM, Huang H, Kim K, Li W, An G, et.al. Bortezomib, Melphalan, and Prednisone With or Without Daratumumab in Transplant-ineligible Asian Patients With Newly Diagnosed Multiple Myeloma: The Phase 3 OCTANS Study. Clin Lymphoma Myeloma Leuk. 2023 Jun;23(6):446-455.e4. doi: 10.1016/j.clml.2023.02.009. Epub 2023 Mar 4. PMID: 37024420.
- Herzog H, Oliveto EP. A history of significant steroid discoveries and developments originating at the Schering Corporation (USA) since 1948. Steroids. 1992;57(12):617–23. [CrossRef]
- Case DC Jr, Lee DJ 3rd, Clarkson BD. Improved survival times in multiple myeloma treated with melphalan, prednisone, cyclophosphamide, vincristine and BCNU: M-2 protocol. Am J Med. 1977 Dec;63(6):897-903. doi: 10.1016/0002-9343(77)90543-5. PMID: 605911.
- Vazquez S, Gold J, Spirollari E, Akmal S, Hanft SJ. The story of dexamethasone and how it became one of the most widely used drugs in neurosurgery. J Neurosurg. 2023 Nov 24;140(4):1191-1197. doi: 10.3171/2023.9.JNS231099. PMID: 38000066.
- Usmani SZ, Hoering A, Ailawadhi S, Sexton R, Lipe B, Hita SF, et.al; SWOG1211 Trial Investigators. Bortezomib, lenalidomide, and dexamethasone with or without elotuzumab in patients with untreated, high-risk multiple myeloma (SWOG-1211): primary analysis of a randomised, phase 2 trial. Lancet Haematol. 2021 Jan;8(1):e45-e54. doi: 10.1016/S2352-3026(20)30354-9. Epub 2020 Dec 22. PMID: 33357482; PMCID: PMC8601389.
- Thorn CF, Oshiro C, Marsh S, Hernandez-Boussard T, McLeod H, Klein TE, Altman RB. Doxorubicin pathways: pharmacodynamics and adverse effects. Pharmacogenet Genomics. 2011 Jul;21(7):440-6. doi: 10.1097/FPC.0b013e32833ffb56. PMID: 21048526; PMCID: PMC3116111.
- Morè S, Corvatta L, Manieri VM, Saraceni F, Scortechini I, Mancini G, Fiorentini A, Olivieri A, Offidani M. Autologous Stem Cell Transplantation in Multiple Myeloma: Where Are We and Where Do We Want to Go? Cells. 2022 Feb 10;11(4):606. doi: 10.3390/cells11040606. PMID: 35203257; PMCID: PMC8870632.
- Sogbein O, Paul P, Umar M, Chaari A, Batuman V, Upadhyay R. Bortezomib in cancer therapy: Mechanisms, side effects, and future proteasome inhibitors. Life Sci. 2024 Dec 1;358:123125. doi: 10.1016/j.lfs.2024.123125. Epub 2024 Oct 15. PMID: 39413903.
- Fricker LD. Proteasome Inhibitor Drugs. Annu Rev Pharmacol Toxicol. 2020 Jan 6;60:457-476. doi: 10.1146/annurev-pharmtox-010919-023603. Epub 2019 Sep 3. PMID: 31479618.
- Zhang CW, Wang YN, Ge XL. Lenalidomide use in multiple myeloma (Review). Mol Clin Oncol. 2023 Nov 28;20(1):7. doi: 10.3892/mco.2023.2705. PMID: 38125742; PMCID: PMC10729307.
- Hoy SM. Pomalidomide: A Review in Relapsed and Refractory Multiple Myeloma. Drugs. 2017 Nov;77(17):1897-1908. doi: 10.1007/s40265-017-0833-y. PMID: 29110190.
- Kamrani S, Naseramini R, Khani P, Razavi ZS, Afkhami H, Atashzar MR, Nasri F, Alavimanesh S, Saeidi F, Ronaghi H. Mesenchymal stromal cells in bone marrow niche of patients with multiple myeloma: a double-edged sword. Cancer Cell Int. 2025 Mar 26;25(1):117. doi: 10.1186/s12935-025-03741-x. PMID: 40140850; PMCID: PMC11948648.
- Lopes R, Caetano J, Ferreira B, Barahona F, Carneiro EA, João C. The Immune Microenvironment in Multiple Myeloma: Friend or Foe? Cancers (Basel). 2021 Feb 5;13(4):625. doi: 10.3390/cancers13040625. PMID: 33562441; PMCID: PMC7914424.
- Ghoshal D, Petersen I, Ringquist R, Kramer L, Bhatia E, Hu T, Richard A, Park R, Corbin J, Agarwal S, Thomas A, Ramirez S, Tharayil J, Downey E, Ketchum F, Ochal A, Sonthi N, Lonial S, Kochenderfer JN, Tran R, Zhu M, Lam WA, Coskun AF, Roy K. Multi-Niche Human Bone Marrow On-A-Chip for Studying the Interactions of Adoptive CAR-T Cell Therapies with Multiple Myeloma. bioRxiv [Preprint]. 2024 Apr 12:2024.04.08.588601. doi: 10.1101/2024.04.08.588601. Update in: Biomaterials. 2025 May;316:123016. doi: 10.1016/j.biomaterials.2024.123016. PMID: 38644993; PMCID: PMC11030357.
- Hathi D, Chanswangphuwana C, Cho N, Fontana F, Maji D, Ritchey J, O'Neal J, Ghai A, Duncan K, Akers WJ, Fiala M, Vij R, DiPersio JF, Rettig M, Shokeen M. Ablation of VLA4 in multiple myeloma cells redirects tumor spread and prolongs survival. Sci Rep. 2022 Jan 7;12(1):30. doi: 10.1038/s41598-021-03748-0. PMID: 34996933; PMCID: PMC8741970.
- Fröbel J, Landspersky T, Percin G, Schreck C, Rahmig S, Ori A, et.al. The Hematopoietic Bone Marrow Niche Ecosystem. Front Cell Dev Biol. 2021 Jul 22;9:705410. doi: 10.3389/fcell.2021.705410. PMID: 34368155; PMCID: PMC8339972.
- Menu E, Vanderkerken K. Exosomes in multiple myeloma: from bench to bedside. Blood. 2022 Dec 8;140(23):2429-2442. doi: 10.1182/blood.2021014749. PMID: 35271699; PMCID: PMC10653045.
- Nooka AK, Cohen AD, Lee HC, Badros A, Suvannasankha A, Callander N, Abdallah AO, Trudel S, Chari A, Libby EN, Chaudhry M, Hultcrantz M, Kortüm KM, Popat R, Sborov D, Hakim S, Lewis E, Gorsh B, Bhushan B, McKeown A, Gupta I, Opalinska J, Richardson PG, Lonial S. Single-agent belantamab mafodotin in patients with relapsed/refractory multiple myeloma: Final analysis of the DREAMM-2 trial. Cancer. 2023 Dec 1;129(23):3746-3760. doi: 10.1002/cncr.34987. Epub 2023 Aug 25. PMID: 37622738; PMCID: PMC11055177.
- Beksaç M, Sahli E, Rabea A, Saydam G, Tombak A, Alhuraiji A, Mutahar EY, Hosny M, Alhejazi A, Mattar M, Dal MS, Marashi M, Palamar M. Practical Guidance on the Clinical Management of Belantamab Mafodotin for Patients With Relapsed/Refractory Multiple Myeloma: Recommendations From the Middle East and North Africa Expert Panel. Clin Lymphoma Myeloma Leuk. 2025 May 20:S2152-2650(25)00184-3. doi: 10.1016/j.clml.2025.05.019. Epub ahead of print. PMID: 40579284.
- McCarthy EF. The toxins of William B. Coley and the treatment of bone and soft-tissue sarcomas. Iowa Orthop J. 2006;26:154-8. PMID: 16789469; PMCID: PMC1888599.
- Eshhar Z, Waks T, Gross G, Schindler DG. Specific activation and targeting of cytotoxic lymphocytes through chimeric single chains consisting of antibody-binding domains and the gamma or zeta subunits of the immunoglobulin and T-cell receptors. Proc Natl Acad Sci U S A. 1993 Jan 15;90(2):720-4. doi: 10.1073/pnas.90.2.720. PMID: 8421711; PMCID: PMC45737.
- Maher J, Brentjens RJ, Gunset G, Rivière I, Sadelain M. Human T-lymphocyte cytotoxicity and proliferation directed by a single chimeric TCRzeta /CD28 receptor. Nat Biotechnol. 2002 Jan;20(1):70-5. doi: 10.1038/nbt0102-70. PMID: 11753365.
- Brentjens RJ, Latouche JB, Santos E, Marti F, Gong MC, Lyddane C, et.al. Eradication of systemic B-cell tumors by genetically targeted human T lymphocytes co-stimulated by CD80 and interleukin-15. Nat Med. 2003 Mar;9(3):279-86. doi: 10.1038/nm827. Epub 2003 Feb 10. PMID: 12579196.
- Kalos M, Levine BL, Porter DL, Katz S, Grupp SA, Bagg A, June CH. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci Transl Med. 2011 Aug 10;3(95):95ra73. doi: 10.1126/scitranslmed.3002842. PMID: 21832238; PMCID: PMC3393096.
- Kochenderfer JN, Wilson WH, Janik JE, Dudley ME, Stetler-Stevenson M, Feldman SA., et.al. Eradication of B-lineage cells and regression of lymphoma in a patient treated with autologous T cells genetically engineered to recognize CD19. Blood. 2010 Nov 18;116(20):4099-102. doi: 10.1182/blood-2010-04-281931. Epub 2010 Jul 28. PMID: 20668228; PMCID: PMC2993617.
- Ruella M, Maus MV. Catch me if you can: Leukemia Escape after CD19-Directed T Cell Immunotherapies. Comput Struct Biotechnol J. 2016 Sep 28;14:357-362. doi: 10.1016/j.csbj.2016.09.003. PMID: 27761200; PMCID: PMC5061074.
- Sheykhhasan M, Ahmadieh-Yazdi A, Vicidomini R, Poondla N, Tanzadehpanah H, Dirbaziyan A, et.al. CAR T therapies in multiple myeloma: unleashing the future. Cancer Gene Ther. 2024 May;31(5):667-686. doi: 10.1038/s41417-024-00750-2. Epub 2024 Mar 4. PMID: 38438559; PMCID: PMC11101341.
- Rodriguez-Otero P, Ailawadhi S, Arnulf B, Patel K, Cavo M, Nooka AK, et.al. Ide-cel or Standard Regimens in Relapsed and Refractory Multiple Myeloma. N Engl J Med. 2023 Mar 16;388(11):1002-1014. doi: 10.1056/NEJMoa2213614. Epub 2023 Feb 10. PMID: 36762851.
- Goel U, Zanwar S, Cowan AJ, Banerjee R, Khouri J, Dima D. Ciltacabtagene Autoleucel for the Treatment of Relapsed/Refractory Multiple Myeloma: Efficacy, Safety, and Place in Therapy. Cancer Manag Res. 2025 Feb 19;17:357-372. doi: 10.2147/CMAR.S510408. PMID: 39990276; PMCID: PMC11847446.
- Rasche L, Hudecek M, Einsele H. CAR T-cell therapy in multiple myeloma: mission accomplished? Blood. 2024 Jan 25;143(4):305-310. doi: 10.1182/blood.2023021221. PMID: 38033289.
- Zheng H, Xian H, Zhang W, Lu C, Pan R, Liu H, Xu Z. BCMA-targeted therapies for multiple myeloma: latest updates from 2024 ASH annual meeting. J Hematol Oncol. 2025 Mar 1;18(1):23. doi: 10.1186/s13045-025-01675-5. PMID: 40025529; PMCID: PMC11872297.
- Zugasti I, Espinosa-Aroca L, Fidyt K, Mulens-Arias V, Diaz-Beya M, Juan M, Urbano-Ispizua Á, Esteve J, Velasco-Hernandez T, Menéndez P. CAR-T cell therapy for cancer: current challenges and future directions. Signal Transduct Target Ther. 2025 Jul 4;10(1):210. doi: 10.1038/s41392-025-02269-w. PMID: 40610404; PMCID: PMC12229403.
- Martin T, Dimopoulos MA, Mikhael J, Yong K, Capra M, Facon T, et.al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized Phase 3 study. Blood Cancer J. 2023 May 9;13(1):72. doi: 10.1038/s41408-023-00797-8. Erratum in: Blood Cancer J. 2023 Sep 27;13(1):152. doi: 10.1038/s41408-023-00923-6. PMID: 37156782; PMCID: PMC10166682.
- Bahlis NJ, Samaras C, Reece D, Sebag M, Matous J, Berdeja JG., et al. Pomalidomide/Daratumumab/Dexamethasone in Relapsed or Refractory Multiple Myeloma: Final Overall Survival From MM-014. Clin Lymphoma Myeloma Leuk. 2024 Dec;24(12):852-862. doi: 10.1016/j.clml.2024.07.014. Epub 2024 Aug 8. PMID: 39237427.
- Ocio EM, Perrot A, Bories P, San-Miguel JF, Blau IW, Karlin L, et.al. Efficacy and safety of isatuximab plus bortezomib, lenalidomide, and dexamethasone in patients with newly diagnosed multiple myeloma ineligible/with no immediate intent for autologous stem cell transplantation. Leukemia. 2023 Jul;37(7):1521-1529. doi: 10.1038/s41375-023-01936-7. Epub 2023 Jun 14. PMID: 37316728; PMCID: PMC10264885.
- Usmani SZ, Quach H, Mateos MV, Landgren O, Leleu X, Siegel D, et.al. Final analysis of carfilzomib, dexamethasone, and daratumumab vs carfilzomib and dexamethasone in the CANDOR study. Blood Adv. 2023 Jul 25;7(14):3739-3748. doi: 10.1182/bloodadvances.2023010026. PMID: 37163358; PMCID: PMC10368773.
- Briggs AH, Sculpher MJ, Claxton K. Decision modelling for health economic evaluation. Oxford: Oxford University Press; 2006.
- Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making. 2013 Aug;33(6):743-54. doi: 10.1177/0272989X12472398. Epub 2013 Jan 22. PMID: 23341049.
- Alexanian R, Bergsagel DE, Migliore PJ, Vaughn WK, Howe CD. Melphalan therapy for plasma cell myeloma. Blood. 1968 Jan;31(1):1-10. PMID: 5638562.
- Kyle RA, Rajkumar SV. Multiple myeloma. Blood. 2008;111(6):2962–72. [CrossRef]
- Orlowski RZ, Nagler A, Sonneveld P, Bladé J, Hajek R, Spencer A, et.al. Final overall survival results of a randomized trial comparing bortezomib plus pegylated liposomal doxorubicin with bortezomib alone in patients with relapsed or refractory multiple myeloma. Cancer. 2016 Jul 1;122(13):2050-6. doi: 10.1002/cncr.30026. Epub 2016 May 18. PMID: 27191689; PMCID: PMC5701574.
- Iida S, Watanabe T, Matsumoto M, Suzuki K, Sunami K, Ishida T., et.al. Carfilzomib monotherapy in Japanese patients with relapsed or refractory multiple myeloma: A phase 1/2 study. Cancer Sci. 2019 Sep;110(9):2924-2932. doi: 10.1111/cas.14139. Epub 2019 Aug 10. PMID: 31336012; PMCID: PMC6726678.
- Moreau P, Mateos MV, Berenson JR, Weisel K, Lazzaro A, Song K., et.al. Once weekly versus twice weekly carfilzomib dosing in patients with relapsed and refractory multiple myeloma (A.R.R.O.W.): interim analysis results of a randomised, phase 3 study. Lancet Oncol. 2018 Jul;19(7):953-964. doi: 10.1016/S1470-2045(18)30354-1. Epub 2018 Jun 1. Erratum in: Lancet Oncol. 2018 Aug;19(8):e382. doi: 10.1016/S1470-2045(18)30492-3. PMID: 29866475.
- Matsela LM, Cleary S, Wilkinson T. Cost utility and budget impact analysis of dexamethasone compared with bortezomib and lenalidomide for the treatment of second line multiple myeloma from a South African public health perspective. Cost Eff Resour Alloc. 2022 Dec 12;20(1):69. doi: 10.1186/s12962-022-00399-4. PMID: 36510230; PMCID: PMC9746097.
- Kropff M, Baylon HG, Hillengass J, Robak T, Hajek R, Liebisch P., et.al. Thalidomide versus dexamethasone for the treatment of relapsed and/or refractory multiple myeloma: results from OPTIMUM, a randomized trial. Haematologica. 2012 May;97(5):784-91. doi: 10.3324/haematol.2011.044271. Epub 2011 Dec 1. PMID: 22133776; PMCID: PMC3342984.
- Olry de Labry Lima A, Gimeno-Ballester V, Ríos Tamayo R, Epstein D, Matas Hoces A, Ríos Sánchez E, García Mochón L, Alegre-Del Rey EJ. Cost-effectiveness of lenalidomide maintenance in patients with multiple myeloma who have undergone autologous transplant of hematopoietic progenitor cells. Bone Marrow Transplant. 2019 Nov;54(11):1908-1919. doi: 10.1038/s41409-019-0574-5. Epub 2019 May 31. PMID: 31150015.
- Richardson PG, Siegel DS, Vij R, Hofmeister CC, Baz R, Jagannath S., et.al. Pomalidomide alone or in combination with low-dose dexamethasone in relapsed and refractory multiple myeloma: a randomized phase 2 study. Blood. 2014 Mar 20;123(12):1826-32. doi: 10.1182/blood-2013-11-538835. Epub 2014 Jan 13. Erratum in: Blood. 2014 May 15;123(20):3208-9. PMID: 24421329; PMCID: PMC3962162.
- Usmani SZ, Weiss BM, Plesner T, Bahlis NJ, Belch A, Lonial S., et.al. Clinical efficacy of daratumumab monotherapy in patients with heavily pretreated relapsed or refractory multiple myeloma. Blood. 2016 Jul 7;128(1):37-44. doi: 10.1182/blood-2016-03-705210. Epub 2016 May 23. PMID: 27216216; PMCID: PMC4937359.
- Dimopoulos M, Bringhen S, Anttila P, Capra M, Cavo M, Cole C., et.al. Isatuximab as monotherapy and combined with dexamethasone in patients with relapsed/refractory multiple myeloma. Blood. 2021 Mar 4;137(9):1154-1165. doi: 10.1182/blood.2020008209. PMID: 33080623; PMCID: PMC7933767.
- Dimopoulos MA, Oriol A, Nahi H, San-Miguel J, Bahlis NJ, Usmani SZ.,et.al. Overall Survival With Daratumumab, Lenalidomide, and Dexamethasone in Previously Treated Multiple Myeloma (POLLUX): A Randomized, Open-Label, Phase III Trial. J Clin Oncol. 2023 Mar 10;41(8):1590-1599. doi: 10.1200/JCO.22.00940. Epub 2023 Jan 4. PMID: 36599114; PMCID: PMC10022849.
- Durie BGM, Hoering A, Sexton R, Abidi MH, Epstein J, Rajkumar SV., et.al. Longer term follow-up of the randomized phase III trial SWOG S0777: bortezomib, lenalidomide and dexamethasone vs. lenalidomide and dexamethasone in patients (Pts) with previously untreated multiple myeloma without an intent for immediate autologous stem cell transplant (ASCT). Blood Cancer J. 2020 May 11;10(5):53. doi: 10.1038/s41408-020-0311-8. PMID: 32393732; PMCID: PMC7214419.
- Yamamoto C, Minakata D, Koyama S, Sekiguchi K, Fukui Y, Murahashi R., et.al. Daratumumab in first-line therapy is cost-effective in transplant-eligible patients with newly diagnosed myeloma. Blood. 2022 Aug 11;140(6):594-607. doi: 10.1182/blood.2021015220. PMID: 35580269; PMCID: PMC9373013.
- Usmani SZ, Facon T, Hungria V, Bahlis NJ, Venner CP, Braunstein M., et al. Daratumumab plus bortezomib, lenalidomide and dexamethasone for transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma: the randomized phase 3 CEPHEUS trial. Nat Med. 2025 Apr;31(4):1195-1202. doi: 10.1038/s41591-024-03485-7. Epub 2025 Feb 5. Erratum in: Nat Med. 2025 Apr;31(4):1366. doi: 10.1038/s41591-025-03581-2. PMID: 39910273; PMCID: PMC12003169.
- Maziarz RT, Devine S, Garrison LP, Agodoa I, Badaracco J, Gitlin M, Perales MA. Estimating the Lifetime Medical Cost Burden of an Allogeneic Hematopoietic Cell Transplantation Patient. Transplant Cell Ther. 2023 Oct;29(10):637.e1-637.e9. doi: 10.1016/j.jtct.2023.06.013. Epub 2023 Jun 24. PMID: 37364775; PMCID: PMC11035010.
- Lee JH, Choi J, Min CK, Park SS, Jo JC, Lee YJ., et.al. Superior outcomes and high-risk features with carfilzomib, lenalidomide, and dexamethasone combination therapy for patients with relapsed and refractory multiple myeloma: results of the multicenter KMMWP2201 study. Haematologica. 2024 Nov 1;109(11):3681-3692. doi: 10.3324/haematol.2024.285534. PMID: 38841794; PMCID: PMC11532698.
- Stewart AK, Rajkumar SV, Dimopoulos MA, Masszi T, Špička I, Oriol A, et.al.; ASPIRE Investigators. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N Engl J Med. 2015 Jan 8;372(2):142-52. doi: 10.1056/NEJMoa1411321. Epub 2014 Dec 6. PMID: 25482145.
- Benboubker L, Dimopoulos MA, Dispenzieri A, Catalano J, Belch AR, Cavo M., et.al.; FIRST Trial Team. Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med. 2014 Sep 4;371(10):906-17. doi: 10.1056/NEJMoa1402551. PMID: 25184863.
- Fu W, Bang SM, Huang H, Kim K, Li W, An G, et.al. Bortezomib, Melphalan, and Prednisone With or Without Daratumumab in Transplant-ineligible Asian Patients With Newly Diagnosed Multiple Myeloma: The Phase 3 OCTANS Study. Clin Lymphoma Myeloma Leuk. 2023 Jun;23(6):446-455.e4. doi: 10.1016/j.clml.2023.02.009. Epub 2023 Mar 4. PMID: 37024420.
- Mateos MV, Dimopoulos MA, Cavo M, Suzuki K, Jakubowiak A, Knop S, et.al.; ALCYONE Trial Investigators. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N Engl J Med. 2018 Feb 8;378(6):518-528. doi: 10.1056/NEJMoa1714678. Epub 2017 Dec 12. PMID: 29231133.
- Mateos MV, Cavo M, Blade J, Dimopoulos MA, Suzuki K, Jakubowiak A., et.al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet. 2020 Jan 11;395(10218):132-141. doi: 10.1016/S0140-6736(19)32956-3. Epub 2019 Dec 10. PMID: 31836199.
- Mateos MV, Dimopoulos MA, Gay F, San-Miguel J, Dytfeld D, Spencer A, et al. Iberdomide plus dexamethasone in relapsed or refractory multiple myeloma (CC-220-MM-001): a multicentre, multicohort, open-label, phase 1/2 trial. Lancet Oncol. 2025;26(5):423–35. [CrossRef]
- Usmani SZ, Quach H, Mateos MV, Landgren O, Leleu X, Siegel D, et.al. Final analysis of carfilzomib, dexamethasone, and daratumumab vs carfilzomib and dexamethasone in the CANDOR study. Blood Adv. 2023 Jul 25;7(14):3739-3748. doi: 10.1182/bloodadvances.2023010026. PMID: 37163358; PMCID: PMC10368773.
- Martin T, Dimopoulos MA, Mikhael J, Yong K, Capra M, Facon T, et.al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized Phase 3 study. Blood Cancer J. 2023 May 9;13(1):72. doi: 10.1038/s41408-023-00797-8. Erratum in: Blood Cancer J. 2023 Sep 27;13(1):152. doi: 10.1038/s41408-023-00923-6. PMID: 37156782; PMCID: PMC10166682.
- Richardson PG, Perrot A, Miguel JS, Beksac M, Spicka I, Leleu X et.al. Isatuximab-pomalidomide-dexamethasone versus pomalidomide-dexamethasone in patients with relapsed and refractory multiple myeloma: final overall survival analysis. Haematologica. 2024 Jul 1;109(7):2239-2249. doi: 10.3324/haematol.2023.284325. PMID: 38299578; PMCID: PMC11215383.
- Leleu X, Hulin C, Lambert J, Bobin A, Perrot A, Karlin L et.al. Isatuximab, lenalidomide, dexamethasone and bortezomib in transplant-ineligible multiple myeloma: the randomized phase 3 BENEFIT trial. Nat Med. 2024 Aug;30(8):2235-2241. doi: 10.1038/s41591-024-03050-2. Epub 2024 Jun 3. PMID: 38830994; PMCID: PMC11333283.
- Mateos MV, Engelhardt M, Leleu X, Mesa MG, Cavo M, Dimopoulos M, et.al. Impact of prior treatment on selinexor, bortezomib, dexamethasone outcomes in patients with relapsed/refractory multiple myeloma: Extended follow-up subgroup analysis of the BOSTON trial. Eur J Haematol. 2024 Aug;113(2):242-252. doi: 10.1111/ejh.14223. Epub 2024 May 1. PMID: 38693052.
- Moreau P, Garfall AL, van de Donk NWCJ, Nahi H, San-Miguel JF, Oriol A, et.al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med. 2022 Aug 11;387(6):495-505. doi: 10.1056/NEJMoa2203478. Epub 2022 Jun 5. PMID: 35661166; PMCID: PMC10587778.
- Mateos MV, Leleu X, Yimer HA, Song KW, Nooka AK, Goldschmidt H, et al. Talquetamab versus belantamab mafodotin in patients with relapsed/refractory multiple myeloma: an interim analysis of the phase 3 MonumenTAL-3 trial. Lancet Haematol. 2024;11(6):e230–44. [CrossRef]
- Bahlis NJ, Samaras C, Reece D, Sebag M, Matous J, Berdeja JG., et al. Pomalidomide/Daratumumab/Dexamethasone in Relapsed or Refractory Multiple Myeloma: Final Overall Survival From MM-014. Clin Lymphoma Myeloma Leuk. 2024 Dec;24(12):852-862. doi: 10.1016/j.clml.2024.07.014. Epub 2024 Aug 8. PMID: 39237427.
- Dimopoulos M, Weisel K, Moreau P, Anderson LD Jr, White D, San-Miguel J., et.al. Pomalidomide, bortezomib, and dexamethasone for multiple myeloma previously treated with lenalidomide (OPTIMISMM): outcomes by prior treatment at first relapse. Leukemia. 2021 Jun;35(6):1722-1731. doi: 10.1038/s41375-020-01021-3. Epub 2020 Sep 7. PMID: 32895455; PMCID: PMC8179841.
- Richardson PG, Oriol A, Beksac M, Liberati AM, Galli M, Schjesvold F, et.al; OPTIMISMM trial investigators. Pomalidomide, bortezomib, and dexamethasone for patients with relapsed or refractory multiple myeloma previously treated with lenalidomide (OPTIMISMM): a randomised, open-label, phase 3 trial. Lancet Oncol. 2019 Jun;20(6):781-794. doi: 10.1016/S1470-2045(19)30152-4. Epub 2019 May 13. PMID: 31097405.
- Paludo J, Mikhael JR, LaPlant BR, Halvorson AE, Kumar S, Gertz MA, et.al. Pomalidomide, bortezomib, and dexamethasone for patients with relapsed lenalidomide-refractory multiple myeloma. Blood. 2017 Sep 7;130(10):1198-1204. doi: 10.1182/blood-2017-05-782961. Epub 2017 Jul 6. PMID: 28684537; PMCID: PMC5606008.
- Dimopoulos MA, Dytfeld D, Grosicki S, Moreau P, Takezako N, Hori M, et.al. Elotuzumab Plus Pomalidomide and Dexamethasone for Relapsed/Refractory Multiple Myeloma: Final Overall Survival Analysis From the Randomized Phase II ELOQUENT-3 Trial. J Clin Oncol. 2023 Jan 20;41(3):568-578. doi: 10.1200/JCO.21.02815. Epub 2022 Aug 12. PMID: 35960908; PMCID: PMC9870233.
- Gentile M, Specchia G, Derudas D, Galli M, Botta C, Rocco S, et.al. Elotuzumab, lenalidomide, and dexamethasone as salvage therapy for patients with multiple myeloma: Italian, multicenter, retrospective clinical experience with 300 cases outside of controlled clinical trials. Haematologica. 2021 Jan 1;106(1):291-294. doi: 10.3324/haematol.2019.241513. PMID: 32107338; PMCID: PMC7776255.
- Bruzzese A, Derudas D, Galli M, Martino EA, Rocco S, Conticello C, et.al. Elotuzumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: Extended 3-year follow-up of a multicenter, retrospective clinical experience with 319 cases outside of controlled clinical trials. Hematol Oncol. 2022 Oct;40(4):704-715. doi: 10.1002/hon.3031. Epub 2022 Jun 1. PMID: 35608183.
- Usmani SZ, Hoering A, Ailawadhi S, Sexton R, Lipe B, Hita SF, et.al; SWOG1211 Trial Investigators. Bortezomib, lenalidomide, and dexamethasone with or without elotuzumab in patients with untreated, high-risk multiple myeloma (SWOG-1211): primary analysis of a randomised, phase 2 trial. Lancet Haematol. 2021 Jan;8(1):e45-e54. doi: 10.1016/S2352-3026(20)30354-9. Epub 2020 Dec 22. PMID: 33357482; PMCID: PMC8601389.
- Yee AJ, Laubach JP, Campagnaro EL, Lipe BC, Nadeem O, Friedman RS, et.al. Elotuzumab in combination with pomalidomide, bortezomib, and dexamethasone in relapsed and refractory multiple myeloma. Blood Adv. 2025 Mar 11;9(5):1163-1170. doi: 10.1182/bloodadvances.2024014717. PMID: 39626297; PMCID: PMC11925518.
- Lawton S, Bishton MJ, Clark P, Thackray K, Smith D. Daratumumab, bortezomib and dexamethasone for previously treated myeloma – comparing real-world outcomes in England to the CASTOR phase III clinical trial. Blood. 2024;144(Suppl 1):3778. [CrossRef]
- Sonneveld P, Chanan-Khan A, Weisel K, Nooka AK, Masszi T, Beksac M, et.al. Overall Survival With Daratumumab, Bortezomib, and Dexamethasone in Previously Treated Multiple Myeloma (CASTOR): A Randomized, Open-Label, Phase III Trial. J Clin Oncol. 2023 Mar 10;41(8):1600-1609. doi: 10.1200/JCO.21.02734. Epub 2022 Nov 22. PMID: 36413710; PMCID: PMC10022857.
Figure 1.
Mechanism of CAR-T Cell Therapy Patient T cells are collected from the bloodstream and genetically modified ex vivo using a viral vector to express a chimeric antigen receptor (CAR). These engineered CAR-T cells are expanded and reinfused into the patient, where they recognize and kill myeloma cells expressing the target antigen.
Figure 1.
Mechanism of CAR-T Cell Therapy Patient T cells are collected from the bloodstream and genetically modified ex vivo using a viral vector to express a chimeric antigen receptor (CAR). These engineered CAR-T cells are expanded and reinfused into the patient, where they recognize and kill myeloma cells expressing the target antigen.
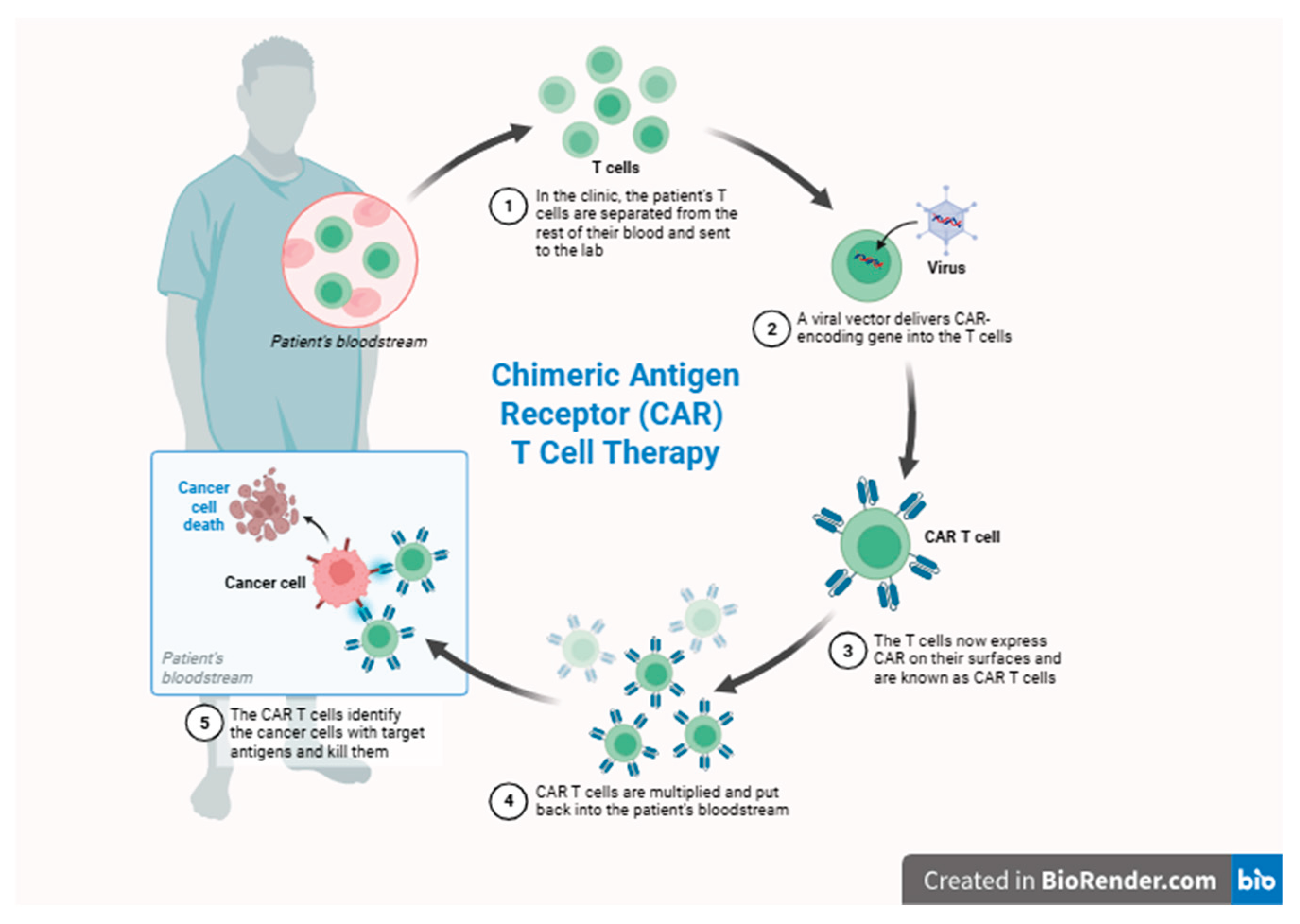
Figure 2.
Treatment Pathways by Transplant Eligibility, Risk Stratification, and Treatment Failure in Multiple Myeloma. A stepwise therapeutic algorithm for patients with multiple myeloma based on transplant eligibility, cytogenetic risk profile, frailty status (ECOG ≥2), and treatment refractoriness (e.g., PI, IMiD, anti-CD38). CAR-T eligibility is indicated for biologically appropriate and clinically fit patients. Frail patients with limited performance status are categorized as ineligible for high-toxicity regimens. Treatment options beyond double or triple failure include novel agents such as Teclistamab, Talquetamab, Selinexor-based regimens, and bispecific antibodies. (d:Dexamethasone, P: Pomalidomide, V: Bortezomib, R: Lenalidomide, D: Daratumumab, Elo: Elotuzumab, Isa: Isatuximab, X: Selinexor, K: Carfilzomib, M: Melphalan).
Figure 2.
Treatment Pathways by Transplant Eligibility, Risk Stratification, and Treatment Failure in Multiple Myeloma. A stepwise therapeutic algorithm for patients with multiple myeloma based on transplant eligibility, cytogenetic risk profile, frailty status (ECOG ≥2), and treatment refractoriness (e.g., PI, IMiD, anti-CD38). CAR-T eligibility is indicated for biologically appropriate and clinically fit patients. Frail patients with limited performance status are categorized as ineligible for high-toxicity regimens. Treatment options beyond double or triple failure include novel agents such as Teclistamab, Talquetamab, Selinexor-based regimens, and bispecific antibodies. (d:Dexamethasone, P: Pomalidomide, V: Bortezomib, R: Lenalidomide, D: Daratumumab, Elo: Elotuzumab, Isa: Isatuximab, X: Selinexor, K: Carfilzomib, M: Melphalan).
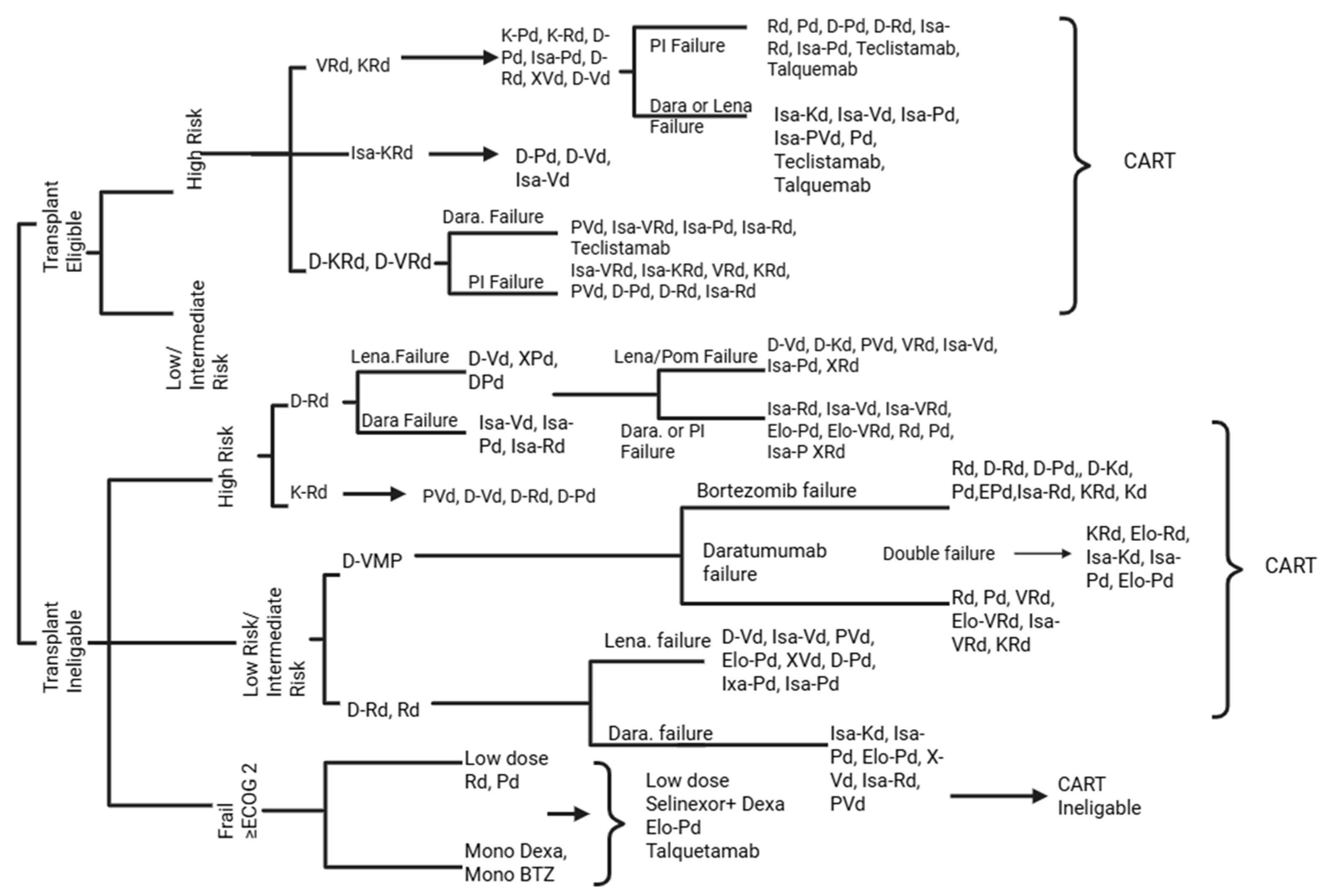
Figure 3.
Methodological framework for QALY and ICER calculation in multiple myeloma. The analysis follows six steps: (1) successive stages of the disease are identified, (2) overall survival (OS) values are derived from large-scale studies for each therapy class, (3) cumulative medication exposure is calculated for the OS period, (4) treatment costs are determined based on current drug prices, (5) QALYs are calculated from survival gains and associated costs, and (6) cumulative values are obtained by summing QALYs, costs, and ICER across all treatment steps.
Figure 3.
Methodological framework for QALY and ICER calculation in multiple myeloma. The analysis follows six steps: (1) successive stages of the disease are identified, (2) overall survival (OS) values are derived from large-scale studies for each therapy class, (3) cumulative medication exposure is calculated for the OS period, (4) treatment costs are determined based on current drug prices, (5) QALYs are calculated from survival gains and associated costs, and (6) cumulative values are obtained by summing QALYs, costs, and ICER across all treatment steps.
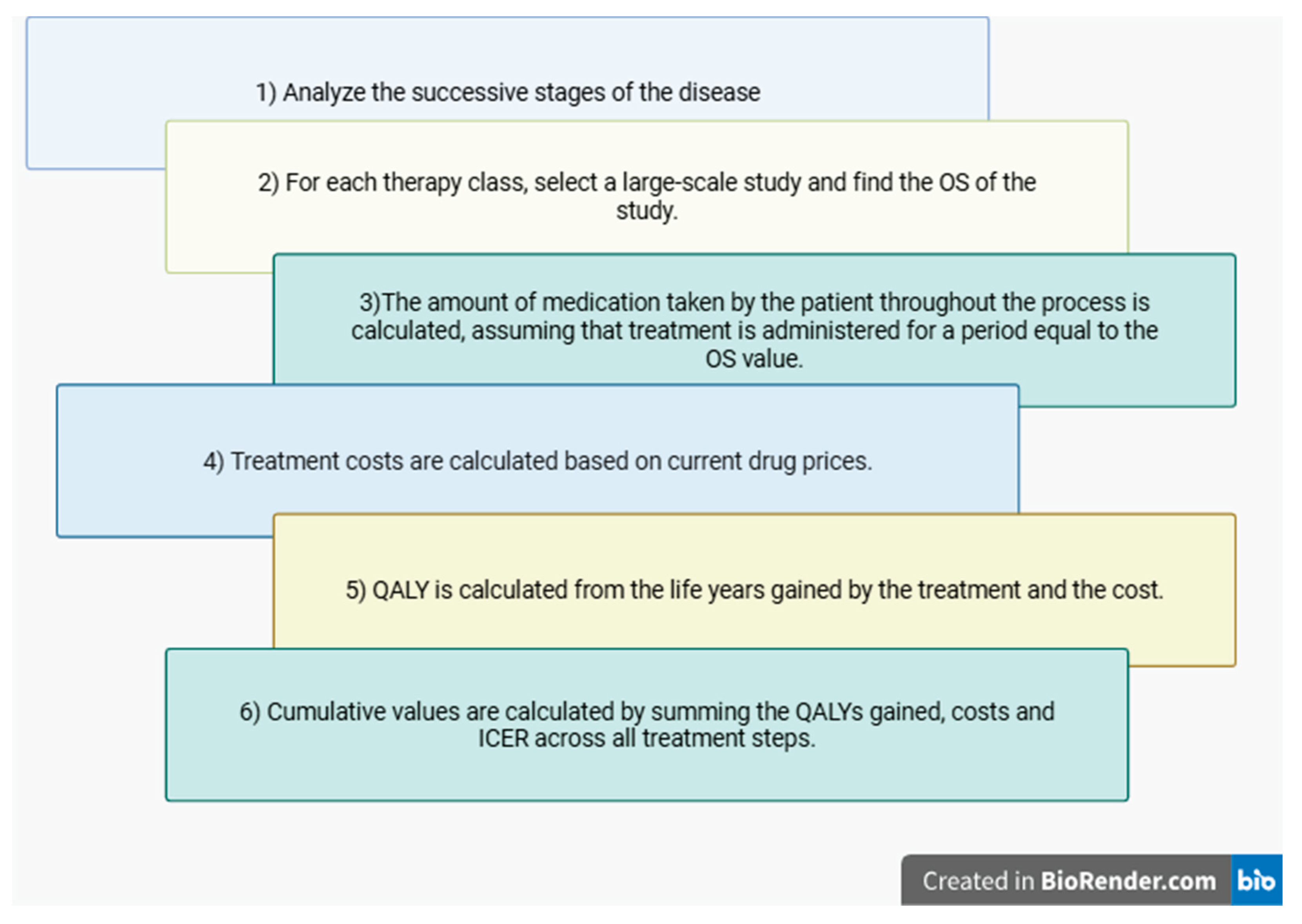
Figure 4.
QALY Outcomes of Monotherapies (left) and Combined Therapies (right) in Multiple Myeloma. Our analysis shows Melphalan and Teclistamab provide the lowest QALY gain among monotherapies. In contrast, cilta-cel, offered the highest QALY benefit, supporting its potential as a cost-effective option when normalized to utility-adjusted survival. Among combination regimens, D-VMP demonstrated the highest QALY, suggesting robust efficacy over prolonged periods. Conversely, certain combinations such as Isa-Kd or Elo-Pd yielded lower QALY despite their intensive nature, highlighting the need to balance treatment complexity with measurable benefit. Notably, Cilta-cel, although monotherapies, provided higher QALY than several combination regimens. It should be acknowledged that the high QALY outcomes observed in regimens such as D-VMP, VRd, and D-VRd may partially reflect the favorable baseline characteristics of transplant-eligible patients with newly diagnosed multiple myeloma (NDMM). These regimens are often used in conjunction with autologous stem cell transplantation (ASCT), contributing significantly to the observed long-term survival and quality-of-life benefits.
Figure 4.
QALY Outcomes of Monotherapies (left) and Combined Therapies (right) in Multiple Myeloma. Our analysis shows Melphalan and Teclistamab provide the lowest QALY gain among monotherapies. In contrast, cilta-cel, offered the highest QALY benefit, supporting its potential as a cost-effective option when normalized to utility-adjusted survival. Among combination regimens, D-VMP demonstrated the highest QALY, suggesting robust efficacy over prolonged periods. Conversely, certain combinations such as Isa-Kd or Elo-Pd yielded lower QALY despite their intensive nature, highlighting the need to balance treatment complexity with measurable benefit. Notably, Cilta-cel, although monotherapies, provided higher QALY than several combination regimens. It should be acknowledged that the high QALY outcomes observed in regimens such as D-VMP, VRd, and D-VRd may partially reflect the favorable baseline characteristics of transplant-eligible patients with newly diagnosed multiple myeloma (NDMM). These regimens are often used in conjunction with autologous stem cell transplantation (ASCT), contributing significantly to the observed long-term survival and quality-of-life benefits.
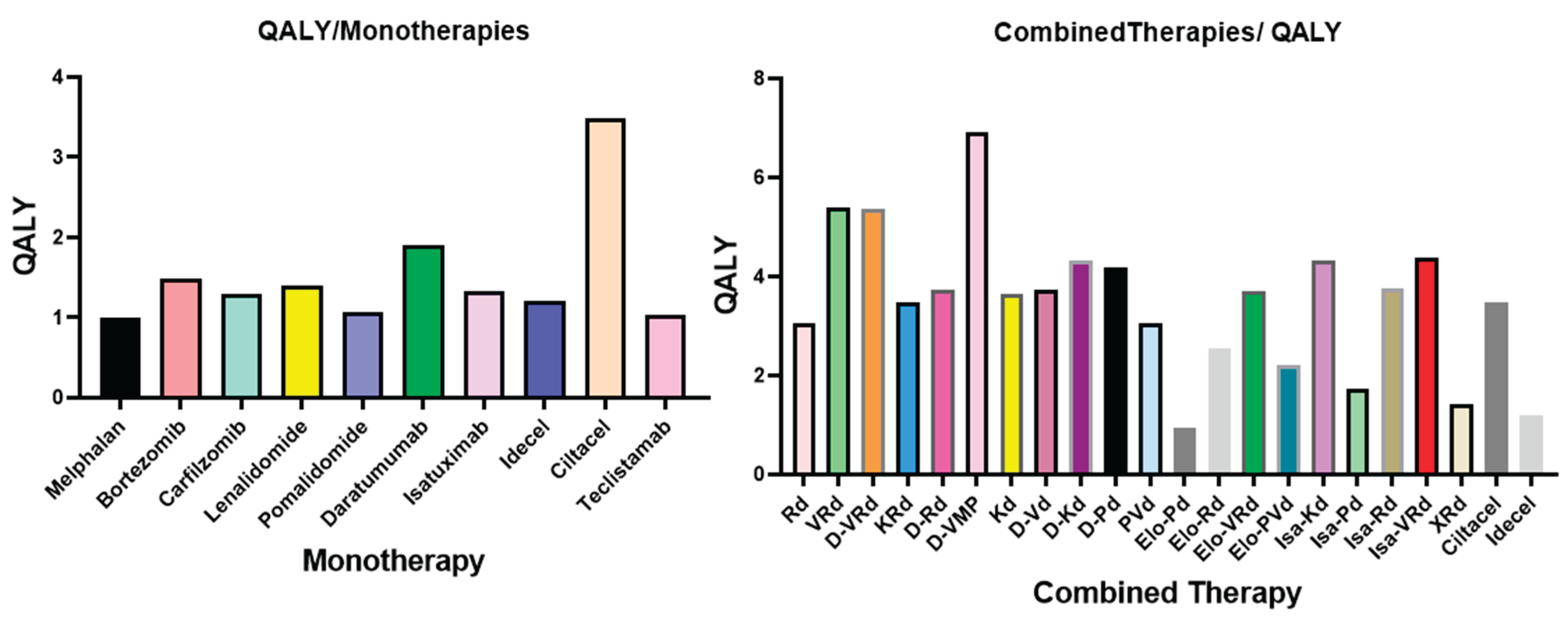
Figure 5.
See-saw model illustrating cumulative ICER (top) and QALY (bottom) outcomes in multiple myeloma therapies.
Figure 5.
See-saw model illustrating cumulative ICER (top) and QALY (bottom) outcomes in multiple myeloma therapies.
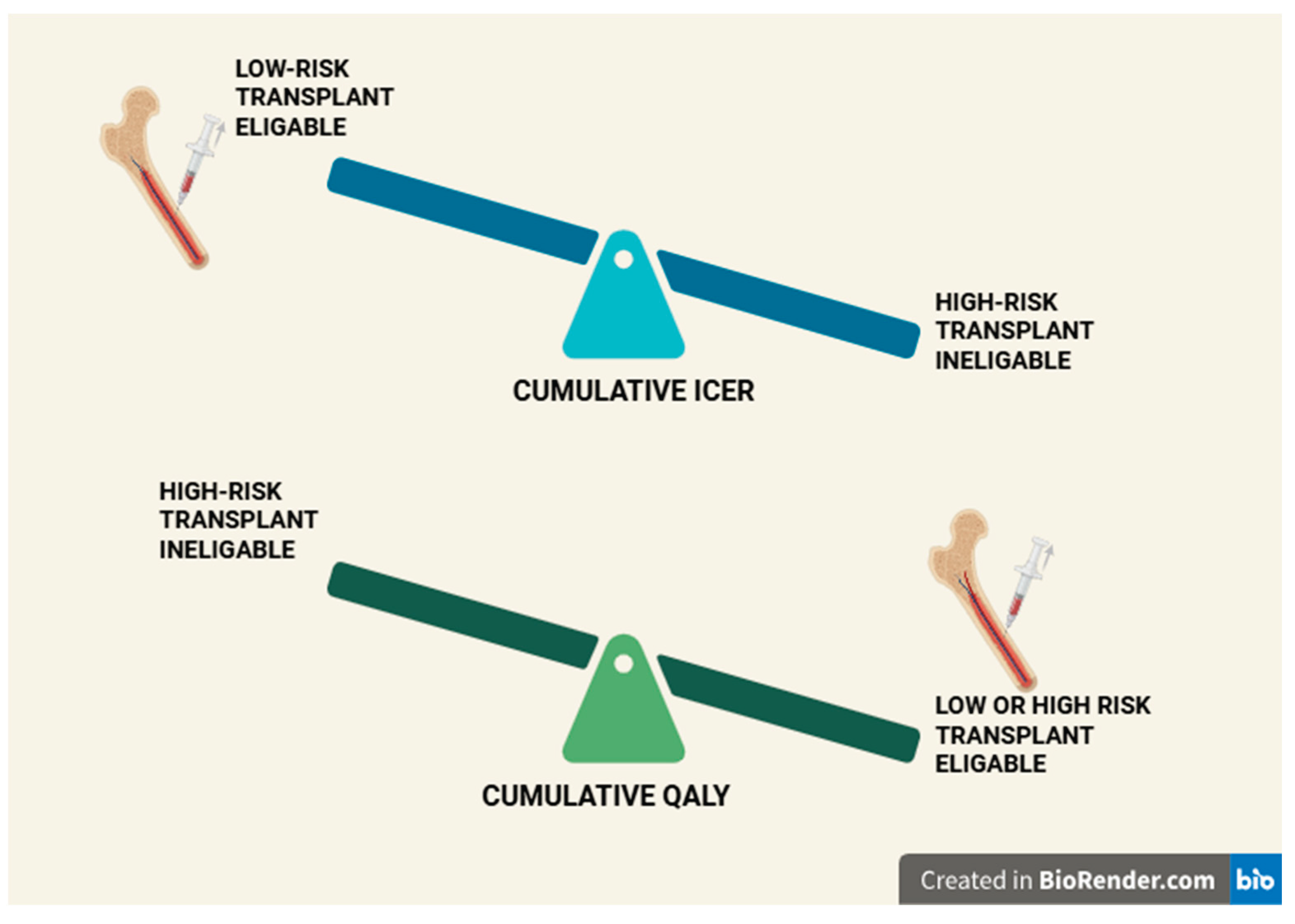
Table 1.
Evolution of Pharmacologic Therapies in Multiple Myeloma.
| Agent/Regimen | Year Introduced | Origin/Context | Current Status in MM Therapy |
|---|---|---|---|
| Melphalan | 1953 | Derived from nitrogen mustard (Great War I) | Still used in transplant conditioning (HD Melphalan) [12,13]. |
| Prednisone | 1950’s | US Army synthesis; corticosteroid | Still used, often in combination regimens [13,14]. |
| M2 Protocol | 1977 | Multi-agent alkylator+ steroid regimen | Historical relevance, rarely used today [15]. |
| Thalidomide | 1953 1997 |
Sedative, Anti-myeloma | Limited due to toxicity; replaced by analogs [11] |
| Dexamethasone | 1960’s | Synthetic glucocorticoid | Still used in most frontline and salvage regimens [16,17]. |
| Doxorubicin | 1969 | Anthracycline (from Streptomyces peucetius) | Still used selectively, limited by cardiotoxicity [18]. |
Table 2.
Aggregated Cost-Effectiveness Outcomes by Treatment Group and Risk Stratification.
| Treatment Group | Risk | Path | Total Cost (USD) | Total QALYs | Total ICER (Cost/ QALY) |
Cumulative ICER (USD/QALY) |
|---|---|---|---|---|---|---|
| TE | High | D-VRd→(ASCT)→D-Kd→PVd→CART→ Teclistamab→ | 6,163,033.28 USD | 18.1 | 340,499 | 3,240,643.15 |
| TE | Low / Intermediate |
D-VRd→KRd→ Isa-Kd→CART→Teclistamab | 8,426,332 USD | 18.576 | 453,613.9 | 3,419,842.55 |
| TI | High | D-Rd→Isa-Kd→Elo-Pd→CART→ Teclistamab | 7,043,070 USD | 13.528 | 520,629 | 5,093,778.66 |
| TI | Low/ Intermediate | D-VMP→ Isa-Kd→Elo-Pd→CART→Teclistamab | 5,625,073.5 USD | 16.693 | 336,972 | 3,594,452.68 |
TE: Transplant Eligible; TI: Transplant Ineligible.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



