Submitted:
22 September 2025
Posted:
24 September 2025
You are already at the latest version
Abstract
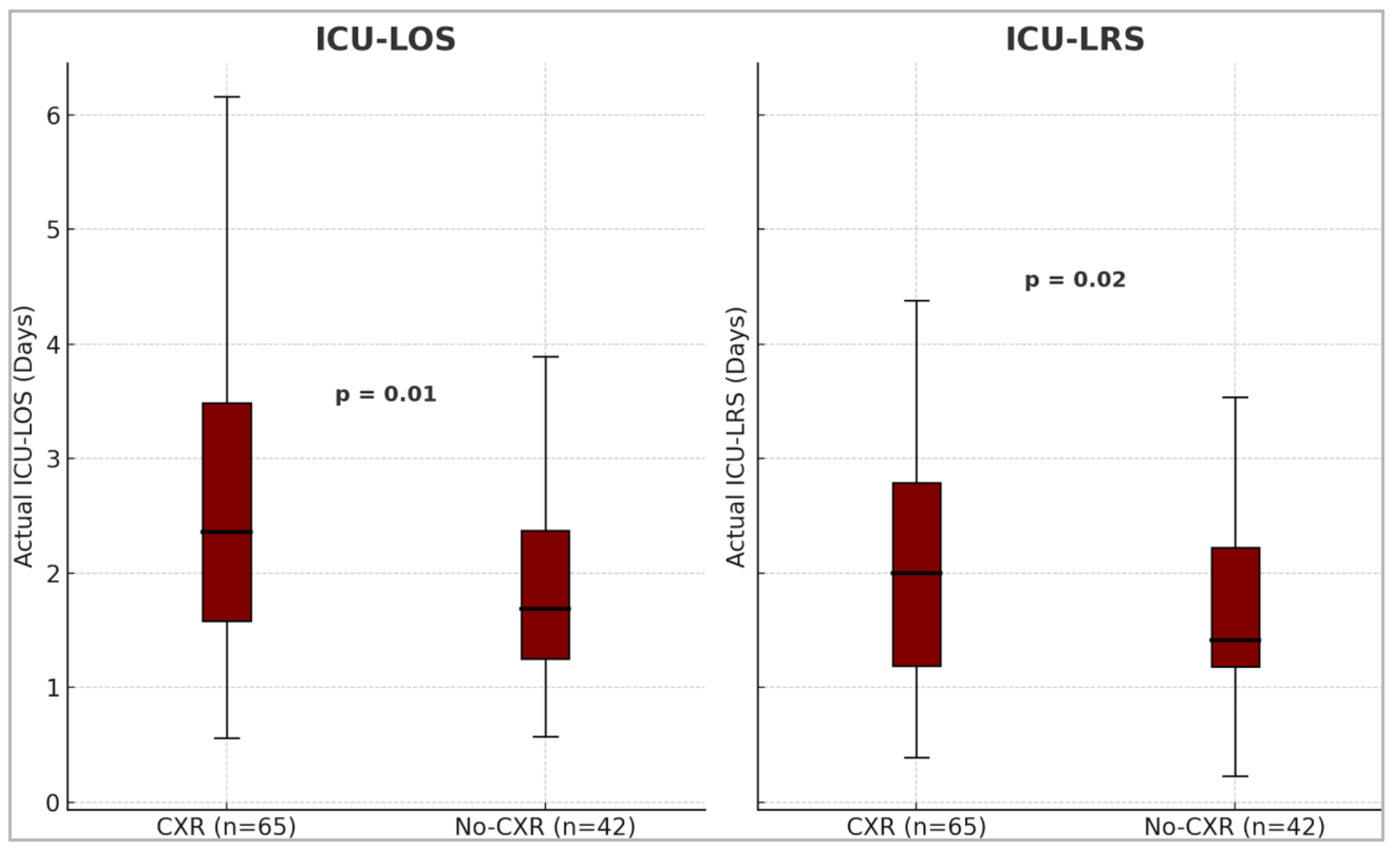
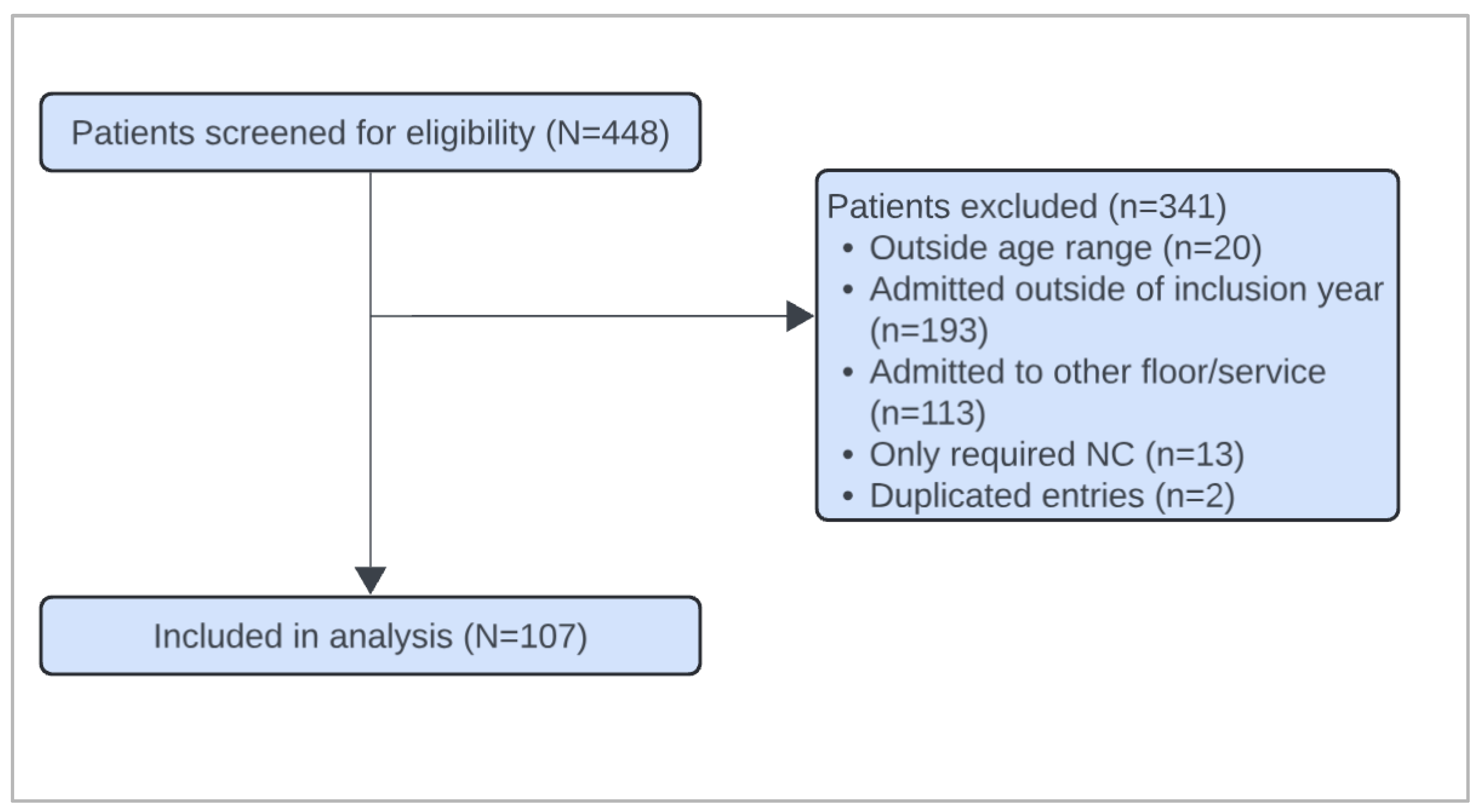
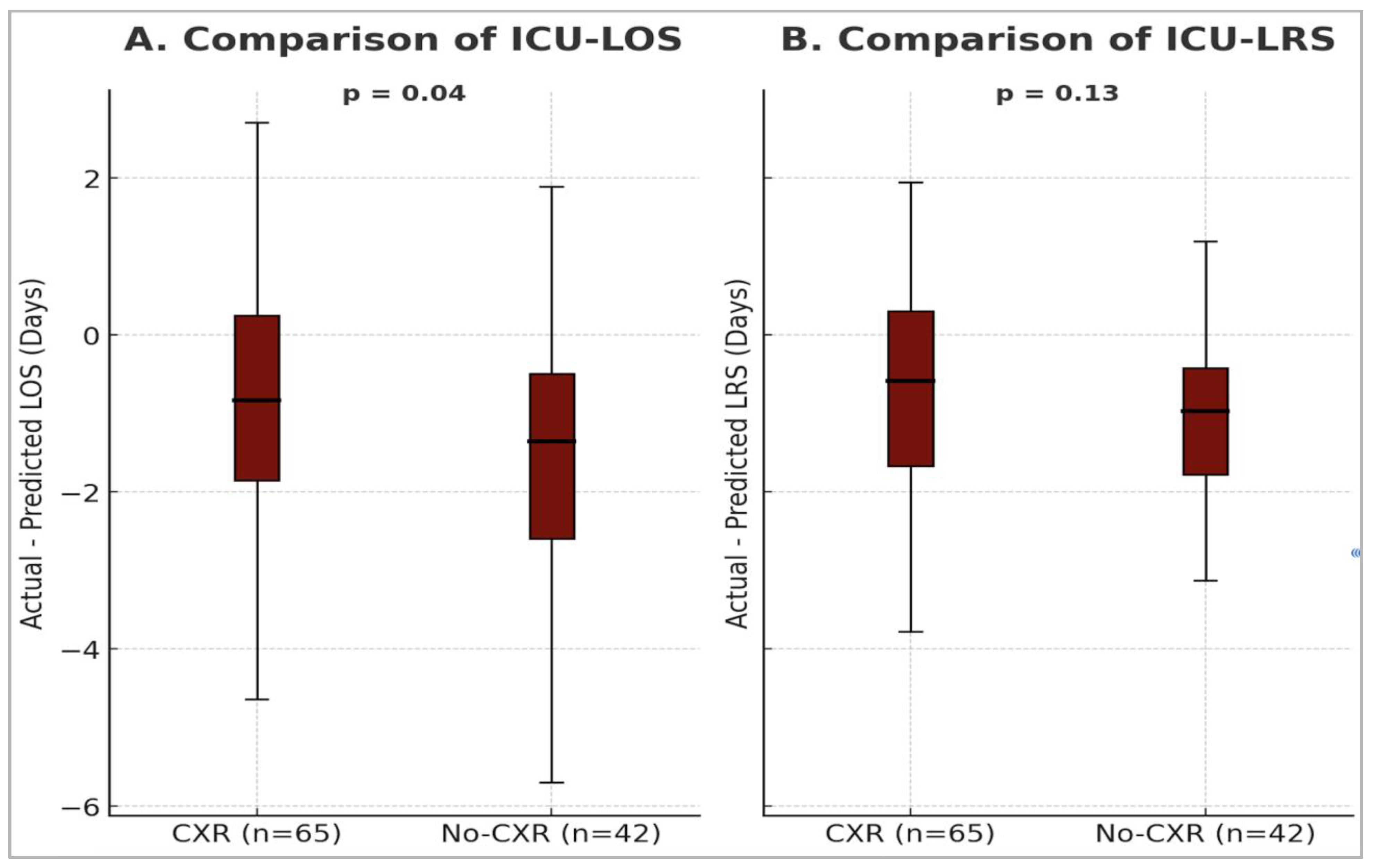
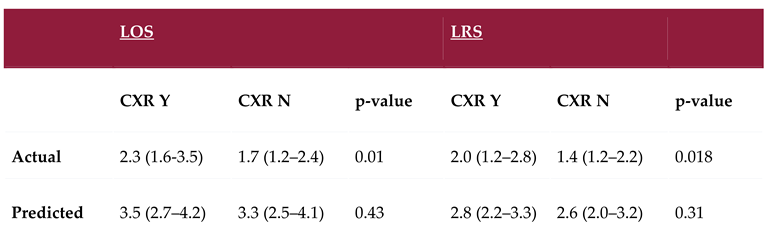
Background: Routine chest X-rays (CXR) are not recommended by the American Academy of Pediatrics in bronchiolitis, yet remain a mainstay in diagnostics. We aimed to understand the impact of obtaining CXRs in patients with critical bronchiolitis, assessing intensive care unit length of stay (ICU-LOS) and intensive care unit level of respiratory support (ICU-LRS). Methods/Design: This single-center retrospective cohort study assessed children less than three years of age admitted to the PICU, pediatric step-down ICU, and pediatric cardiac ICU. Two groups were used for analysis: patients with CXR and no-CXR. The primary outcome was the difference in ICU-LOS and ICU-LRS between the groups. The critical bronchiolitis score (CBS) was used to calculate a predicted ICU-LOS and ICU-LRS. The secondary outcome was the difference between actual and predicted ICU-LOS and ICU-LRS, comparing the groups. Results: Of the 107 patients included, 65 patients (61%) received a CXR. Patients who received a CXR had significantly longer ICU-LOS (p = 0.01) and ICU-LRS (p = 0.02), despite no difference in predicted illness severity (ICU-LOS, p = 0.4; ICU-LRS, p = 0.3). The difference between actual and predicted ICU-LOS was greater in the no-CXR group (–1.4 days) compared to the CXR group (–0.8 days; p = 0.04). A similar trend was observed in ICU-LRS (–0.1 vs. –0.6 days; p = 0.1), though not statistically significant. Conclusion: Routine CXRs are common in critically ill bronchiolitis patients and may be associated with longer ICU-LOS and ICU-LRS, despite similar illness severity.
Keywords:
Introduction
Materials and Methods
Study Overview
Outcome Measure
Data Collection
Statistical Analysis
Results
Discussion
Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent
Data Availability
Acknowledgments
Conflicts of Interest
Abbreviations
| PICU | Pediatric intensive care unit |
| SDICU | Step-down intensive care unit |
| PCTICU | Pediatric cardiac intensive care unit |
| ICU | Intensive care unit |
| LOS | Length of stay |
| CBS | Critical Bronchiolitis Score |
| LRS | Level of respiratory support |
| HR | Heart rate |
| RR | Respiratory rate |
| GCS | Glasgow Coma Scale |
| pCO₂ | Partial pressure of carbon dioxide |
| SBP | Systolic blood pressure |
| BUN | Blood urea nitrogen |
| HFNC | High-flow nasal cannula |
| NIMV | Non-invasive mechanical ventilation |
| IMV | Invasive mechanical ventilation |
| CXR | Chest X-ray |
| IQR | Interquartile range |
| AAP | American Academy of Pediatrics |
Appendix A

| Variable | Units | Concept |
|---|---|---|
| Demographic data | - | Patient characteristics |
| Past medical history | - | Medical conditions prior to admission |
| Past surgical history | - | Surgical procedures prior to admission |
| Past family history of atopy in a first-degree relative | - | Family predisposition to atopic conditions |
| Home-oxygen use | Yes/No | Pre-admission oxygen therapy at home |
| Day-of-illness on presentation | Days | Duration of illness before presentation |
| Month and year of presentation | Month/ Year | Temporal factors of admission |
| Presence of viral infection | Names of virus identified | Confirmed viral etiology |
| ICU-LOS | Days | Length of ICU stay |
| Hospital LOS | Days | Length of hospital stay |
| HFNC use | Yes/No, L/Kg, Days | Duration of respiratory support |
| NIMV use (including nCPAP) | Yes/No, Highest PIP/PEEP/RR/ FiO2, Days | Duration of respiratory support |
| IMV use (including HFOV) | Yes/No, Highest PIP/PEEP/MAP/RR/ FiO2, Days | Duration of respiratory support |
| CXR use | Yes/No | Diagnostic modality |
| Other imaging- US, Echocardiography, CT | Yes/No | Diagnostics |
| Antibiotic use | Yes/No | Clinical management |
| Nebulizations- Albuterol, 3%, racemic epinephrine | Yes/No | Adjunctive therapies |
| Highest RR | Breaths per minute | Vital signs |
| Highest HR | Beats per minute | Vital signs |
| Highest temperature | °C or °F | Vital signs |
| Worst GCS | GCS score | Clinical decision tool |
| Lowest serum bicarbonate | mmol/L | Measure of dehydration |
| Lowest pH/highest pCO2 ratio | pH, mmHg | Measure of respiratory acidosis |
| Highest BUN | mg/dL | Measure of dehydration |
| Lowest SBP | mmHg | Vital signs |
References
- Nicolai, A.; Ferrara, M.; Schiavariello, C.; Gentile, F.; Grande, M. E.; Alessandroni, C.; Midulla, F. Viral bronchiolitis in children: a common condition with few therapeutic options. Early Hum. Dev. 2013, 89, S7–S11. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S. L.; Lieberthal, A. S.; Meissner, H. C.; Alverson, B. K.; Baley, J. E.; Gadomski, A. M.; Johnson, D. W.; Light, M. J.; Maraqa, N. F.; Mendonca, E. A.; Phelan, K. J.; Zorc, J. J.; Stanko-Lopp, D.; Brown, M. A.; Nathanson, I.; Rosenblum, E.; Sayles, S., 3rd; Hernandez-Cancio, S.; American Academy of Pediatrics. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014, 134, e1474–e1502.
- Zurca, A. D.; González-Dambrauskas, S.; Colleti, J.; Vasquez-Hoyos, P.; Prata-Barbosa, A.; Boothe, D.; Combs, B. E.; Lee, J. H.; Franklin, D.; Pon, S.; Karsies, T.; Shein, S. L. Intensivists' reported management of critical bronchiolitis: more data and new guidelines needed. Hosp. Pediatr. 2023, 13, 660–670. [Google Scholar] [CrossRef] [PubMed]
- Almadani, A.; Noël, K. C.; Aljassim, N.; Maratta, C.; Tam, I.; Papenburg, J.; Quach, C.; Thampi, N.; McNally, J. D.; Lefebvre, M. A.; Zavalkoff, S.; O'Donnell, S.; Jouvet, P.; Fontela, P. S. Bronchiolitis management and unnecessary antibiotic use across 3 Canadian PICUs. Hosp. Pediatr. 2022, 12, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Tsugawa, Y.; Brown, D. F.; Mansbach, J. M.; Camargo, C. A., Jr. Trends in bronchiolitis hospitalizations in the United States, 2000–2009. Pediatrics 2013, 132, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Yong, J. H.; Schuh, S.; Rashidi, R.; Vanderby, S.; Lau, R.; Laporte, A.; Nauenberg, E.; Ungar, W. J. A cost effectiveness analysis of omitting radiography in diagnosis of acute bronchiolitis. Pediatr. Pulmonol. 2009, 44, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Mount, M. C.; Ji, X.; Kattan, M. W.; Slain, K. N.; Clayton, J. A.; Rotta, A. T.; Shein, S. L. Derivation and validation of the Critical Bronchiolitis Score for the PICU. Pediatr. Crit. Care Med. 2022, 23, e45–e54. [Google Scholar] [CrossRef] [PubMed]
- Christakis, D. A.; Cowan, C. A.; Garrison, M. M.; Molteni, R.; Marcuse, E.; Zerr, D. M. Variation in inpatient diagnostic testing and management of bronchiolitis. Pediatrics 2005, 115, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Purcell, K.; Fergie, J. Concurrent serious bacterial infections in 2396 infants and children hospitalized with respiratory syncytial virus lower respiratory tract infections. Arch. Pediatr. Adolesc. Med. 2002, 156, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Chao, J. H.; Lin, R. C.; Marneni, S.; Pandya, S.; Alhajri, S.; Sinert, R. Predictors of airspace disease on chest X-ray in emergency department patients with clinical bronchiolitis: a systematic review and meta-analysis. Acad. Emerg. Med. 2016, 23, 1107–1118. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J. N.; Rieder, M. J.; Walton, J. M.; Canadian Paediatric Society, Acute Care Committee, Drug Therapy and Hazardous Substances Committee. Bronchiolitis: recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatr. Child Health 2014, 19, 485–498. [CrossRef] [PubMed]
- Chao, J. H.; Lin, R. C.; Marneni, S.; Pandya, S.; Alhajri, S.; Sinert, R. Predictors of airspace disease on chest X-ray in emergency department patients with clinical bronchiolitis: a systematic review and meta-analysis. Acad. Emerg. Med. 2016, 23, 1107–1118. [Google Scholar] [CrossRef] [PubMed]
- Schuh, S.; Lalani, A.; Allen, U.; Manson, D.; Babyn, P.; Stephens, D.; MacPhee, S.; Mokanski, M.; Khaikin, S.; Dick, P. Evaluation of the utility of radiography in acute bronchiolitis. J. Pediatr. 2007, 150, 429–433. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Bronchiolitis in children: diagnosis and management. NICE Guideline NG9, 2nd edition. 2015, updated 2021.
- Friedman, J. N.; Rieder, M. J.; Walton, J. M.; Canadian Paediatric Society, Acute Care Committee; Drug Therapy and Hazardous Substances Committee. Bronchiolitis: recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatr. Child Health 2014, 19, 485–498. [CrossRef] [PubMed]
- Reiter, J.; Breuer, A.; Breuer, O.; Hashavya, S.; Rekhtman, D.; Kerem, E.; Cohen-Cymberknoh, M. A quality improvement intervention to reduce emergency department radiography for bronchiolitis. Respir. Med. 2018, 137, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Frazier, S. B.; Walls, C.; Jain, S.; Plemmons, G.; Johnson, D. P. Reducing chest radiographs in bronchiolitis through high-reliability interventions. Pediatrics 2021, 148, e2020014597. [Google Scholar] [CrossRef] [PubMed]
 |
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



