
Submitted:
20 September 2025
Posted:
22 September 2025
You are already at the latest version
Abstract
Background/Objectives: Very early pediatric onset multiple sclerosis (POMS) is rare; clinical studies using disease modifying treatments (DMTs) have not been performed. Clinicians rely on studies performed at older age. This review resulted due to difficulties faced by clinicians and off label use of DMTs at this age. Methods: A literature review be-tween 1980 – 2025 of very early POMS with onset before age 5 has been performed searching for outcome without or with DMTs. The curated database of the selected patients was analyzed using computed descriptive and integrated cohort-level estimates. The clinical, paraclinical, treatment and outcome characteristics were analyzed. Statistical analysis used JASP, with GenAI-assisted verification. Treatment outcome of a 16 year old patient with very early POMS starting at 2 years 4 months that consecutively received interferon, immunoglobulins and natalizumab is presented. Results: 101 patients with very early POMS presented at onset ataxic syndrome (57.4%), pyramidal syndrome (41.4%), ophthalmoplegia (10.3%) and optic neuritis (6.9%). In evolution 22.7% had seizures. Half of the patients were not treated. Among those treated, acute steroid therapy was administered; 11 received DMTs: interferon, glatiramer acetate, dimethyl fumarate, azathioprine (three) and only two – high-efficacy therapies (natalizumab, rituximab). Our patient had partial remission under interferon, relapses when stopped and replaced by immunoglobulins and 9 years relapse-free interval when natalizumab was introduced. Conclusions: Early treatment with high efficiency DMTs should be considered in very early POMS; association with known increased neuroplasticity at this age may improve prognosis, allowing good recovery of acquired disability.
Keywords:
very early onset multiple sclerosis
; disease modifying treatment
; pediatric onset multiple sclerosis (POMS)
; natalizumab
; interferon
; immunoglobulins
; acute treatment
1. Introduction
Prior literature typically defines POMS as <18 years and considers early-onset cases those <10 years. In this work, we define very early POMS cases with onset before 5 years of age. POMS represents 3% to 5% of all multiple sclerosis cases, with less than 1% starting before age 10 years (early POMS) meaning 0,09/100 000 population [1]. Prevalence and incidence of very early POMS are unknown [2,3,4]. Due to the very low incidence of MS at this age, there are no powerful studies concerning DMT benefits or adverse effects. Due to its rarity, only isolated case reports or small case-series exist [5,6]. Therefore, clinicians treating these cases need information to manage diagnosis and treatment for very early POMS. DMTs are of off label and in many countries not covered by insurance system, the patients receiving only acute therapy and sometimes intravenous immunoglobulins, with uncertain efficacy and accumulation of disability [6].
Authors of this review faced difficult decisions for treating a patient with very early POMS in a female with onset at age 2 years 4 month. She initially had frequent episodes of neurological involvement treated with acute steroid therapy with complete remission. DMTs used in sequence (Interferon, intravenous immunoglobulins (IVIGs), and Natalizumab) has different effects. The case presentation is available in section 3.3. Clinical vignette.
This case is the reason for the extensive literature review presented in this publication, aiming to offer our pediatric colleagues a summary of the published cases of very early POMS including clinical aspects and treatment choices.
2. Materials and Methods
Literature Search
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
PubMED, Scopus, Cochraine, Elybrary.ru, Arab World Research Source, CINAHL, OpenGrey were searched using following search terms: (("Multiple Sclerosis"[Mesh] OR "multiple sclerosis"[tiab] OR "pediatric multiple sclerosis"[tiab]) AND ("Child, Preschool"[Mesh] OR "Infant"[Mesh] OR child[tiab] OR children[tiab] OR toddler[tiab] OR preschool[tiab] OR "younger than 5"[tiab] OR "under 5"[tiab] OR "before age 5"[tiab]) AND ("Therapeutics"[Mesh] OR "Drug Therapy"[Mesh] OR "Treatment Outcome"[Mesh] OR treatment[tiab] OR therapy[tiab] OR corticosteroids[tiab] OR interferon[tiab] OR "disease modifying therapy"[tiab] OR DMT[tiab] OR glatiramer[tiab] OR rituximab[tiab] OR cyclophosphamide[tiab] OR "dimethyl fumarate"[tiab])) OR ("natalizumab"[Mesh] OR natalizumab[tiab])
Articles found after manual search in the hospital literature database (selected articles on the topic) and in the references of the selected articles were added.
Articles selection was performed independently by two reviewers (P.G. and D.A.). Inclusion and exclusion criteria were applied consistently at the title, abstract, and full-text to ensure transparency and reproducibility.
The inclusion criteria were: 1. Age at onset below 5 years; 2. Publication date after 1982, in order to include the use of paraclinical investigations introduced by the Poser criteria (with subsequent selection of the cases using McDonald 2001 criteria); 3. Design of the study – case reports, series of cases, clinical trials, literature review articles; 4. Publication language: English, Spanish, Arabic, Russian, and Chinese. Google translate was used from any language to English.
Studies that did not fulfill the contemporary diagnostic requirements for multiple sclerosis at the time of publication, studies that failed to provide clinical and paraclinical details of individual patients or cohorts over 5 years of age were excluded.
Generative artificial intelligence (GenAI) has been used to generate the PRISMA flow diagram, Figure 1. (to illustrate the process of study identification, screening, eligibility assessment, and final inclusion).
A relevant case study of multiple sclerosis with very early onset was described as an example of different DMTs used off label for age; evolution is described and compared with literature findings.
Data Analysis
Authors analyzed following information: 1. Demographic and clinical data 2. Paraclinical data 3. Treatment at episode and DMTs and their effect – see Supplementary material S1: Collected data classification; patients and their characteristics are presented in supplementary material S2: Patients characteristics from selected articles (https://drive.google.com/drive/folders/1uB6k06BwdyNwYM78FjFu6Rh__KROJBtM?usp=sharing).
Statistical Analysis
The statistical analyses and figures were produced in JASP (version 095.1). Verification, cross-checks, and iterative re-analysis of the results were assisted by GenAI under author verification; GenAI was only used to support calculations, code expressions, and interpretation and not to generate or alter primary data.
Descriptive results (counts and percentages) were calculated for demographic, clinical, paraclinical and treatment data.
Authors hypothesized a strong association between younger onset age and a higher incidence of ataxia or seizures at onset. Therefore, Pearson and Spearman rank correlations with 95% CIs were run after excluding records with unknown evolution and cohorts without individual-level data. Ataxia – age association was adjusted for cerebellar lesions, and seizures – age association was adjusted for cortical/subcortical lesions using binomial logistic regression analysis. Models were restricted to cases with Magnetic Resonance Immaging (MRI) data.
The hypothesis whether incomplete remission differed by treatment exposure was examined with χ² test across three groups (no treatment, steroid therapy only, and steroid therapy + DMT) for complete or incomplete remission followed by binomial logistic regression with incomplete remission as outcome (odd ratio with 95% CIs; p value < 0.05).
3. Results
3.1. Literature Search
3.2. Data Analysis
3.2.1. Demographic and Clinical Data
A total of 101 patients were identified (Table 1). The female-to-male ratio was 1.4:1. The mean age at onset was 36 months (range: 10 months–5 years). The mean number of relapses was 4.1, with an average of 2.3 relapses within the first two years of life.
Onset signs. The most frequent presenting syndromes were ataxic syndrome (57.4%), pyramidal syndrome (41.4%), fever with or without altered consciousness (17.2%), ophthalmoplegia (10.3%) and optic neuritis (6.9%).
Signs in evolution. Ataxic gait was the most common symptom (42.9%), followed by hemiparesis (35%) and seizures (22.7%) (Table 2).
In the majority of cases, both the initial presentation and early relapses were monosymptomatic (74.3%).
An onset resembling ADEM, with fever, lethargy, impaired consciousness, and vomiting, was reported in 17.8% of cases, all of whom developed classical recurrent remitting multiple sclerosis (RRMS) later on.
3.2.2. Paraclinical Data
- Imaging. MRI was performed in 98 cases. Supratentorial lesions predominated (57.4%), most commonly periventricular (59.1%); infratentorial lesions were primarily located in the brainstem (32.7% of all cases) (Table 3). Cerebellar lesions were observed in 10 cases (10.2% of all cases) and spinal lesions in 12 cases (10.2% of all cases). Six patients underwent computer tomography (CT) examination (3 had only CT-scan), of which five revealed hypointense lesions. Two of the patients had a normal CT but abnormal IRM at the follow-up. The other one with normal CT had MS characteristic lesions were confirmed by necropsy.
- Cerebrospinal fluid (CSF) analysis performed in 99 cases showed pleocytosis (45 out of 999 cases/45.5%), hyper-proteinorrachia (27 out of 99 cases/27.3%), positive oligoclonal bands (32 out of 99 cases/ 32.3%), elevated IgG index (5 of 9 tested/ 55.5%) and anti-myelin basic protein antibodies (3 out of 3 cases /100%).
- Visual evoked potentials (VEP) were abnormal in 10 out of 30 patients (33,3%) of patients. Autopsy was performed in two deceased patients, revealing multiple small sclerotic lesions, some with cystic components, distributed within the white matter, predominantly supratentorial periventricular.
3.2.3. Treatment
- Regarding treatment, 43 of all treated patients (95.6%) received steroids for at least one relapse (Table 4). In most cases, high-dose intravenous methylprednisolone was used, with or without subsequent tapering with oral prednisone.
- Three additional patients received intravenous immunoglobulin (IVIGs) and steroids.
- Disease-modifying therapies were initiated in 11 cases (24.4% of all treated patients), of which 6 received low-efficacy agents (4 interferon, 1 dimethyl fumarate, 1 glatiramer acetate) and 2 received high-efficacy agents (1 natalizumab, 1 rituximab). Azathioprine was administered in 3 cases.
3.2.4. Outcomes
- Complete remission was documented in 88% of cases.
- Poor outcomes were observed in 12 cases, characterized by multiple relapses with incomplete recovery, progressive course, or lack of remission. Two deaths occurred, both in patients from the pre-2001 cohort who had not received treatment. Among patients with incomplete remission, 8 were treated with steroids, and 1 with steroids and dimethyl fumarate.
- Escalation to higher efficacy therapies (rituximab, natalizumab, azathioprine) occurred in 3 cases, with adequate disease control achieved in the first two cases.
3.2.5. Statistical Analysis of Treatment Outcomes
No significant associations were detected between age at onset and symptoms at onset: ataxia (Pearson r = 0.364, p = 0.088, 95% CI − 0.057 to 0.675) or seizures (Pearson r = − 0.261, p = 0.229, 95% CI − 0.608 to 0.169). MRI lesions may introduce a bias for epilepsy (the cortical lesions) and ataxia (the cerebellar and spinal lesions). In the adjusted logistic models with MRI lesions as confounder), the statistical associations did not change.
The contingency test assessing remission in treated patients was not statistically significant (χ² = 1.26, p = 0.53), although proportion for incomplete remission has a decreasing trend in relation to more complex treatments: 50% incomplete remission in untreated group, 31% for patients treated with steroids only, and 17% for steroids and DMTs. Consistently, logistic regression using steroids and DMTs group as the reference estimated higher odds (but non-significant) for incomplete remission for steroids only group (OR = 2.22, p > 0.05) and no treatment group (OR = 5.00, p > 0.05). Overall, results do not show statistically significant associations, but the statistical model estimates that adding a DMT on top of corticosteroids likely reduces the chance of incomplete remission, consistent with a clinically favorable effect (Figure 2).
3.3. Clinical Vignette
A 16-year-old female patient is presented. She was born by vaginal delivery after an uncomplicated pregnancy and had normal milestones achievement. Family history was unremarkable for the patients’ disease. She had 11 episodes of neurological involvement with stormy onset at 2 years 4 months. As a characteristic, her episodes were long at onset, with complete recovery of short duration (but more than 30 days). After the third episode residual neurological symptoms were noted. The clinical symptoms at onset and subsequent episodes are listed in Table 5. and Figure 3.
3.3.1. Workup
The initial symptoms were rapidly progressive gait and equilibrium disturbances and irritability without a prior history of infectious disease. In another hospital a suspicion of ADEM was raised, but clinical and paraclinical data, including imaging, and clinical evolution, with new relapses led to the diagnosis or RRMS after the 3rd episode. Table 6. shows the workup and differential diagnosis.
Infectious and Inflammatory-Immune Disorders Were Ruled Out
The diagnosis of RRMS was established at that time based on Mc Donalds criteria 2010 [29]: she had more than 2 attacks proving dissemination in time (DIT) and objective clinical and MRI evidence of dissemination in space (DIS). On MRI she had lesions in all 4 – periventricular, juxtacortical, infratentorial and spinal cord regions proving DIS; these lesions had different ages proving DIT (Figure 4).
3.3.2. Evolution Under Treatment
The patient received steroid therapy at every acute event.
Episode I and II: small doses of ACTH (0,33 mg/day for 14 days), followed by Prednisone (0,5 mg/kg), 7 days were administered in the county hospital. She had complete remission 5 weeks after onset.
The second episode started after 30 days (Table 5, Figure 3). No other investigations were carried out by the local physician. Treatment with Dexamethasone 8 mg/day – 3 days and Synachten 0.5 mg/day - 7 days was followed by complete remission within 5 weeks and another 35 days without neurological symptoms. MRI was performed at onset and after remission (Figure 4) of the third episode showing an increased number of MRI lesions.
For the third episode she was admitted in our clinic with cerebellar syndrome (severe ataxia and saccadic speech, pyramidal syndrome (left more than right), irritability. Treatment included acute pulse-therapy with Methylprednisolone 30 mg/kg/day for 6 days; patient was initiated on DMT (disease modifying treatment) off label – Interferone Beta-1a 22 µg/dose, 3 doses/week; premedication with paracetamol was initiated; no adverse reactions were recorded; periodical follow-up (clinical and biological) showed IFN was well tolerated. She had another two mild and short relapses (1 week each) with 4 weeks intervals between episodes, followed by another 2 relapses of 2 days each with 8 weeks intervals between them (Table A.I., Figure A.1.). With IFN treatment Expanded Disability Status Scale (EDSS) score decreased continuously from 4 to 2 and even 1.5. The sponsor could not support donation of IFN anymore due to legal constraints and it was discontinued. She relapsed dramatically after 10 weeks (episode VIII) and she was initiated on IVIGs (intravenous immunoglobulins) 2 g/kg/cure infused in 3 days, monthly. As a result, she had mild relapses at intervals of 11-13 weeks lasting no more than 1 week each, but EDSS remained 4 also during the “free” intervals between relapses.
Due to international collaboration with colleagues with experience in treating pediatric patients with Natalizumab, the patient was initiated at age 7 years on Natalizumab, 300 mg/dose, monthly administrations. Check-up for JCV (John Cunningham virus, Human polyomavirus 2) has been performed before and then monthly and MRI performed for PML (progressive multifocal leukoencephalopathy) at each relapse and yearly for follow-up; both JCV and MRI were done during IFN and Natalizumab therapies. No relapses were recorded after Natalizumab initiation during the next 9 years, until present; EDSS score decreased to 3.5 (persistent disability).
Cognitive involvement. Parents didn’t notice changes in patient’s cognitive performances. At age 3 years she was evaluated (Romanian validated tests). Denver II showed delayed development in personal-social and gross motor domains with normal functioning for language and fine motor and adaptative behavior domains. Nepsy test showed decreased scores in all domains: attention/executive functions 58, -3SD (standard deviation); language 74, -2SD; sensory-motor 66, -3SD; visuo-spatial 77, -2SD; memory 80, -2SD (Figure...). During testing she collaborated with psychologists, but showed severe inattention, and a mild lack of interest.
She was reevaluated at age 4years 1month by the same psychologists. Denver II showed delayed development in all four domains. Nepsy proved decreased scores for language, visuo-spatial and memory compared with previous examination: attention/executive functions 67, -3SD; language 67, -3SD; sensory-motor 66, -3SD; visuo-spatial 74, -2SD; memory 70, -3SD (Figure 3). The patient showed opposing and provoking behavior, inappropriate verbal and emotional reactions, difficulties in maintaining attention, resulting in lack of collaboration during testing.
She was re-evaluated age 15.5 years, and she has an average normal IQ – 91 with social and adaptative impairment, but she is attending normal high-school (admitted by contest). No complex evaluation was performed.
4. Discussion
Multiple sclerosis is extremely rare before the age of 5 years. Isolated case reports and small case series have been published, and some cases are documented in national registries [20,30].
The case reported in the vignette is an MS patient with an exceptionally early onset (age 2 years 4 month). It is to be speculated an even earlier subclinical onset or unnoticed clinical signs due to the small age of the patient. As described, even earlier onset (10 months old) were previously reported by other groups [20]. It is unknown whether very early onset multiple sclerosis shares the same pathophysiology as in adult patients, or whether distinct underlying biological mechanisms may trigger it. It was hypothesized, but not yet proven, that copy number variation (CNV) may influence genes in large genomic regions involved in disease mechanisms, and contribute to very early onset [31]. Genetic background may play a major role in early onset MS and further studies are expected.
Age-specific incidence: While pediatric-onset multiple sclerosis (POMS) accounts for 3%-5% of all MS cases, with fewer than 1% starting under the age of 10, there is substantial variability in incidence rates based on geographic location and environmental exposures. Regions with higher latitude, such as Scandinavia and Canada, demonstrate significantly higher pediatric MS prevalence due to possible correlations with lower vitamin D levels [2]. These data highlight the importance of understanding regional susceptibility alongside diagnostic patterns, which show that early-onset MS might still be underdiagnosed in populations from lower-income countries.
A marked discrepancy can be observed between the high number of pediatric MS cases with onset before 5 years of age reported during 1980–2000 compared with those, fewer, published between 2001–2025. This phenomenon can largely be attributed to the absence of modern diagnostic criteria before year 2000, limited availability of advanced neuroimaging, and, most importantly, the still undescribed related neuroinflammatory demyelinating disorders such as neuromyelitis optica spectrum disorder (NMOSD), MOG antibody–associated disease (MOGAD), or autoimmune encephalitis [32,33].
In the present review we identified 19 published patients who had been diagnosed with MS but who no longer meet contemporary diagnostic criteria [34,35,36,37,38,39,40,41,42,43]. All of these cases were reported between 1981 and 1994. Among them, three patients would now probably classify as MOGAD, two as ADEM, one as NMOSD, and one as autoimmune encephalitis, due to clinical and MRI aspects. For the majority, however, insufficient clinical and paraclinical data were available to fulfill current diagnostic requirements for MS, although the diagnosis cannot be definitively excluded. These articles were excluded from our review.
Symptoms and Early MRI Trends: Ataxia was observed as the most frequent presenting manifestation in our cohort, consistent with prior studies indicating that cerebellar and brainstem involvement is more pronounced in younger MS patients [20,44,45]. Additionally, patients with seizure onset, although infrequent, displayed a suggestive association with cortical lesions. This aligns with previous reports linking epilepsy to MS regardless of age [46].
Treatment remains a challenge under 5 years of age due to the absence of clinical studies with DMTs. In the analyzed group half of the patients were not treated. Among those treated, acute-phase steroid therapy was administered; DMTs were administered in 11 patients: most received low-efficacy agents such as interferon, glatiramer acetate, or dimethyl fumarate, three were treated with azathioprine [11,20,21] and only two patients received high-efficacy therapies (natalizumab or rituximab) [5,14,24,27]. A patient reported by Sotgiu et al. with disease onset at age 5 years and treated with natalizumab since age 5 years and 5 months had nearly complete remission with significant EDSS score improvement [27]. An Italian observational study using Natalizumab in MS pediatric patients showed good tolerability and good response when administered as early as 4 years of age. [47,48].
A groundbreaking advancement in treating POMS with high-efficacy therapies is highlighted by the study of Menascu et al [49]. The multicenter research focuses on outcomes in pediatric MS treated with natalizumab, revealing significant benefits in reducing relapse rates and stabilizing disease over long-term follow-up. The study demonstrated a significant decrease in EDSS scores and relapse rates in children as young as 5 years of age during natalizumab therapy. Reported adverse events were mild or moderate, and periodic John Cunningham virus (JCV) screening was implemented to mitigate the risk of progressive multifocal leukoencephalopathy (PML). These findings suggest that natalizumab, though off-label for children under 18 years [50], may be a critical tool in cases of highly active POMS, particularly under rigorous monitoring protocols.
After partial response when treated with interferon and no response with IVIGs, our vignette patient similarly benefited from natalizumab, initiated at 7 years of age, experiencing no relapses during a 9-year follow-up period. These results correlate strongly with Menascu et al.'s findings, supporting natalizumab's safety and efficacy for early-onset MS.
Early treatment with high efficiency DMTs may improve prognosis in very early onset pediatric multiple sclerosis cases, especially because association with known increased neuroplasticity at this age, allowing good recovery of acquired disability [51].
Statistical analysis. Overall, our statistical modeling demonstrated trends favoring early introduction of high-efficacy disease-modifying therapies like natalizumab in patients with very early onset multiple sclerosis. Moreover, interventions targeting children under 5 years may provide a critical neurological therapeutic window due to heightened neuroplasticity at these ages.
To deepen understanding, future studies should focus on global multicenter efforts to consolidate real-world pediatric data into standardized cohorts. This approach would better define the molecular mechanisms, genetic predispositions, and therapeutic responses specific to very early-onset multiple sclerosis. Integrating multicenter approaches, such as that described by Menascu et al., could further optimize strategies for long-term disability prevention and improved quality of life in these pediatric populations.
Supplementary Materials
The following supporting information can be downloaded at: https://drive.google.com/drive/folders/1uB6k06BwdyNwYM78FjFu6Rh__KROJBtM?usp=sharing: Table S1: Collected data classification; Table S2: Patients characteristics from selected articles.
Author Contributions
Conceptualization, D.C. and G.P.; methodology, D.C. and G.P.; formal analysis, G.P.; Investigation, D.C. and G.P.; resources, D.C., A.D., M.S., S.M., C.P., and G.P.; data curation, G.P., D.C.; writing—original draft preparation, G.P., D.C.; writing—review and editing, G.P., D.C., C.P., A.D., M.S., S.M., ; visualization, G.P., D.C.; supervision, D.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Analyzed data available online – Supplementary materials S1 and S2 (see above).
Acknowledgments
During the preparation of this manuscript, the authors used JASP (version 095.1) for statistical analyses and related figures generation [52]. Generative artificial intelligence (GenAI) has been used for the purposes of generating the PRISMA flow diagram, Figure 1., and verification, cross-checks, and iterative re-analysis of the statistical data results [53] under author verification; GenAI was only used to support calculations, code expressions, and interpretation and not to generate or alter primary data. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Abbreviations
| The following abbreviations are used in this manuscript | . |
| ADEM | Acute disseminated encephalomyelitis |
| ANA | Anti-nuclear antibodies |
| anti dsDNA | anti-double-stranded DNA antibody |
| anti-Sm | Anti-Smith Antibody |
| AQP4 | serum aquaporin-4 autoantibodies |
| CI | confidence interval |
| CSF | cerebrospinal fluid |
| CT | computer tomography |
| DIS | dissemination in time |
| DIT | dissemination in space |
| DMT | Disease Modifying Therapy |
| EBV | Epstein-Barr Virus |
| EDSS | Expanded Disability Status Scale |
| GenAI | Generative artificial intelligence |
| HBV | Hepatitis B virus |
| HIV | human immunodeficiency virus |
| IVIGs | intravenous immunoglobulins |
| JCV | John Cunningham virus |
| LP | lumbar puncture |
| MOG | Myelin Oligodendrocyte Glycoprotein |
| MOGAD | Myelin Oligodendrocyte Glycoprotein Associated Disease |
| MRI | Magnetic resonance imaging |
| MRI | Magnetic Resonance Imaging |
| MS | Mmultiple sclerosis |
| NMO | Neuromyelitis optica |
| NMOSD | Neuromyelitis Optic Spectrum Disorder |
| OCB | Oligoclonal Bands |
| POMS | Pediatric Onset Multiple Sclerosis |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RRMS | Relapsing remitting multiple sclerosis |
| S | Steroids |
| SD | standard deviation |
| VEP | Visual Evoked Potentials |
References
- Kauth, F.; et al. Characterization of children with early onset pediatric multiple sclerosis. Eur. J. Paediatr. Neurol. 2025, 54, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, T.; Glanz, B.; Jaffin, S.; Healy, B. Demographics of pediatric-onset multiple sclerosis in an MS center population from the Northeastern United States. Mult. Scler. 2009, 15, 627–631. [Google Scholar] [CrossRef]
- Ness, J.M.; Chabas, D.; Sadovnick, A.D.; Pohl, D.; Banwell, B.; Weinstock-Guttman, B.; International Pediatric MS Study Group. Clinical features of children and adolescents with multiple sclerosis. Clinical features of children and adolescents with multiple sclerosis. Neurology 2007, 68 (Suppl. 2), S37–S45. [Google Scholar] [CrossRef]
- Venkateswaran, S.; Banwell, B. Pediatric multiple sclerosis. Neurologist 2010, 16, 92–105. [Google Scholar] [CrossRef]
- Arkar, U.; Vipotnik Vesnaver, T.; Osredkar, D.; Perković Benedik, M.; Bizjak, N. Multiple sclerosis in a 4-year-old boy: a case report and literature review. Front. Neurol. 2024, 15, 1359938. [Google Scholar] [CrossRef]
- Mavridi, A.; Bompou, M.E.; Redmond, A.; Archontakis-Barakakis, P.; Vavougios, G.D.; Mitsikostas, D.D.; Mavridis, T. Current and emerging treatment options in pediatric onset multiple sclerosis. Sclerosis 2024, 2, 88–107. [Google Scholar] [CrossRef]
- Carvalho, I.V.; Dos Santos, C.S.; Amaral, J.; Ribeiro, J.A.; Pereira, C.; Pais, R.P.; Palavra, F. Multiple sclerosis under the age of ten: the challenge of a rare diagnosis in a special population— a case series. Front. Neurosci. 2023, 17, 1297171. [Google Scholar] [CrossRef]
- Cole, G.F.; Auchterlonie, L.A.; Best, P.V. Very early onset multiple sclerosis. Dev. Med. Child Neurol. 1995, 37, 667–672. [Google Scholar] [CrossRef]
- Calcii, C.; Aminov, D.; Sprincean, M.; Marga, S.; Anton-Paduraru, D.-T.; Revenco, N.; Groppa, S.; Palii, I.; Pirtu, L.; Hadjiu, S. Very rare incident of pediatric onset multiple sclerosis complicated with status epilepticus: a case report. Austin Neurol. Neurosci. 2023, 6, 1028. [Google Scholar]
- Gaccon, L. A case of childhood multiple sclerosis. Br. Ir. Orthopt. J. 2006, 3, 44–46. [Google Scholar] [CrossRef]
- Gargouri, L.; Safi, F.; Fourati, H.; Kmiha, S.; Turki, F.; Zidi, F.; Mnif, Z.; Mahfoudh, A. Early-onset of multiple sclerosis in a 5-year-old girl. Arch. Pediatr. 2014, 21, 291–295. [Google Scholar] [CrossRef]
- Guilhoto, L.M.F.F.; et al. Pediatric multiple sclerosis: report of 14 cases. Brain Dev. 1995, 17, 9–12. [Google Scholar] [CrossRef]
- Hauser, S.L.; et al. Immunoregulatory T-cells and lymphocytotoxic antibodies in active multiple sclerosis: weekly analysis over a six-month period. Ann. Neurol. 1983, 13, 418–425. [Google Scholar] [CrossRef]
- Hwang, J.S.; Kim, S.J.; Yu, Y.S.; Chung, H. Clinical characteristics of multiple sclerosis and associated optic neuritis in Korean children. J. AAPOS 2007, 11, 559–563. [Google Scholar] [CrossRef]
- Maeda, Y.; Kitamoto, I.; Kurokawa, T.; Ueda, K.; Hasuo, K.; Fujioka, K. Infantile multiple sclerosis with extensive white matter lesions. Pediatr. Neurol. 1989, 5, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Mikaeloff, Y.; et al. Prognostic factors for early severity in a childhood multiple sclerosis cohort. Pediatrics 2006, 118, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Fernández, V.; Martínez-Salcedo, E.; Climent-Oltra, V.; Domingo-Jiménez, R.; Casas-Fernández, C. Esclerosis múltiple: a propósito de un caso de inicio muy precoz. Rev. Neurol. 1999, 28, 488–491. [Google Scholar] [CrossRef]
- Rai, B.; Riazat, M.I.; Sharif, F. P652: An unusual case of recurring demyelinating neurological disorder in a 3-year-old. Arch. Dis. Child. 2019, 104, [Abstract P652]. [Google Scholar]
- Rodríguez Núñez, A.; et al. Esclerosis múltiple en la edad preescolar: aportación diagnóstica de la resonancia magnética. An. Esp. Pediatr. 1992, 37, 405–407. [Google Scholar]
- Ruggieri, M.; Polizzi, A.; Pavone, L.; et al. Multiple sclerosis in children under 6 years of age. Neurology 1999, 53, 478–484. [Google Scholar] [CrossRef]
- Rushdi, R.; Shalaby, N. Pediatric multiple sclerosis: unveiling the trajectory of a toddler-onset case. Neuroimmunol. Rep. 2024, 6, 100222. [Google Scholar] [CrossRef]
- Saijo, N.; Abe, Y.; Oikawa, Y.; Okubo, Y.; Endo, W.; Numata-Uematsu, Y.; Takahashi, T.; Uematsu, M. Successful treatment with dimethyl fumarate in a child with relapsing–remitting multiple sclerosis. Brain Dev. 2022, 44, 353–356. [Google Scholar] [CrossRef]
- Sánchez-Calderón, M.; et al. Esclerosis múltiple en la infancia: nuestra experiencia y revisión de la literatura. Rev. Neurol. 1998, 27, 237–241. [Google Scholar] [CrossRef]
- Sawant, T.A.; et al. A child with early onset multiple sclerosis. BMJ Paediatr. Open 2024, 8(Suppl. 1), A115 (Abstract EPAC.189).
- Shaw, C.-M.; Alvord, E.C. Multiple sclerosis beginning in infancy. J. Child Neurol. 1987, 2, 252–256. [Google Scholar] [CrossRef]
- Sivaraman, I.; Moodley, M. Multiple sclerosis in the very young: a case report and review of the literature. Neurodegener. Dis. Manag. 2016, 6, 31–36. [Google Scholar] [CrossRef]
- Sotgiu, S.; Nieddu, A.; Pruna, D.; et al. On a 5-year-old girl with multiple sclerosis treated with natalizumab. Neurol. Sci. 2023, 44, 2963–2965. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.H.; Weinshenker, B.G.; Filippi, M.; Banwell, B.L.; Cohen, J.A.; Freedman, M.S.; Galetta, S.L.; Hutchinson, M.; Johnson, R.T.; Kappos, L.; Kira, J.; Lublin, F.D.; McFarland, H.F.; Montalban, X.; Panitch, H.; Richert, J.R.; Reingold, S.C.; Polman, C.H. Differential diagnosis of suspected multiple sclerosis: a consensus approach. Mult. Scler. 2008, 14, 1157–1174. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; Lublin, F.D.; Montalban, X.; O'Connor, P.; Sandberg-Wollheim, M.; Thompson, A.J.; Waubant, E.; Weinshenker, B.; Wolinsky, J.S. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Huppke, P.; Huppke, B.; Ellenberger, D.; Rostasy, K.; Hummel, H.; Stark, W.; Brück, W.; Gärtner, J. Therapy of highly active pediatric multiple sclerosis. Mult. Scler. 2019, 25, 72–80. [Google Scholar] [CrossRef]
- McElroy, J.P.; Krupp, L.B.; Johnson, B.A.; McCauley, J.L.; Qi, Z.; Caillier, S.J.; Gourraud, P.A.; Yu, J.; Nathanson, L.; Belman, A.L.; Hauser, S.L.; Waubant, E.; Hedges, D.J.; Oksenberg, J.R. Copy number variation in pediatric multiple sclerosis. Mult. Scler. 2013, 19, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Chou, I.J.; Wang, H.S.; Whitehouse, W.P.; Constantinescu, C.S. Paediatric multiple sclerosis: update on diagnostic criteria, imaging, histopathology and treatment choices. Curr. Neurol. Neurosci. Rep. 2016, 16, 68. [Google Scholar] [CrossRef] [PubMed]
- Fadda, G.; Waters, P.; Woodhall, M.; Brown, R.A.; O’Mahony, J.; Castro, D.A.; Longoni, G.; Yeh, E.A.; Marrie, R.A.; Arnold, D.L.; Banwell, B.; Bar-Or, A. Serum MOG-IgG in children meeting multiple sclerosis diagnostic criteria. Mult. Scler. 2022, 28, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Vergani, M.I.; Reimão, R.; Silva, A.M.; Muskat, M.; Espósito, S.; Diament, A. Multiple sclerosis with early childhood onset. A case report. Arq. Neuropsiquiatr. 1988, 46, 195–197. [Google Scholar] [CrossRef]
- Asai, K.; Inagaki, M.; Maegaki, Y.; Yamamoto, T.; Suzaki, I.; Ohta, S. An early-onset case of multiple sclerosis with thalamic lesions on MRI. Acta Paediatr. Jpn. 1994, 36, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Matsuishi, T.; Shimizu, T.; Yamashita, Y.; Nagamitsu, S.; Kojima, K.; Kato, H.; Tabira, T. Baló’s concentric sclerosis in a 4-year-old Japanese infant. Brain Dev. 1998, 20, 250–252. [Google Scholar] [CrossRef]
- Bejar, J.M.; Ziegler, D.K. Onset of multiple sclerosis in a 24-month-old child. Arch. Neurol. 1984, 41, 881–882. [Google Scholar] [CrossRef]
- Brandt, S.; Gyldensted, C.; Offner, H.; Melchior, J.C. Multiple sclerosis with onset in a two-year old boy. Neuropediatrics 1981, 12, 75–82. [Google Scholar] [CrossRef]
- Hanefeld, F.; Bauer, H.J.; Christen, H.J.; Kruse, B.; Bruhn, H.; Frahm, J. Multiple sclerosis in childhood: report of 15 cases. Brain Dev. 1991, 13, 410–416. [Google Scholar] [CrossRef]
- Bauer, H.J.; Hanefeld, F.; Christen, H.J. Multiple sclerosis in early childhood. Lancet 1990, 336, 1190. [Google Scholar] [CrossRef]
- Boutin, B.; Esquivel, E.; Mayer, M.; Chaumet, S.; Ponsot, G.; Arthuis, M. Multiple sclerosis in children: report of clinical and paraclinical features of 19 cases. Neuropediatrics 1988, 19, 118–123. [Google Scholar] [CrossRef]
- Bye, A.M.E.; Kendall, B.; Wilson, J. Multiple sclerosis in childhood: a new look. Dev. Med. Child Neurol. 1985, 27, 215–222. [Google Scholar] [CrossRef]
- Haas, G.; Schroth, G.; Krägeloh-Mann, I.; Buchwald-Saal, M. Magnetic resonance imaging of the brain of children with multiple sclerosis. Dev. Med. Child Neurol. 1987, 29, 586–591. [Google Scholar] [CrossRef]
- Dică, A.D.; Craiu, D.; Linca, F.I.; Budișteanu, M.; Iliescu, C.; Sandu, C.; Pomeran, C.; Bârcă, D.; Butoianu, N.; Burloiu, C.; et al. Age-onset-related particularities of pediatric MS—understanding the spectrum: a tertiary center experience. Diseases 2025, 13, 193. [Google Scholar] [CrossRef]
- Renoux, C.; et al. Natural history of multiple sclerosis with childhood onset. N. Engl. J. Med. 2007, 356, 2603–2613. [Google Scholar] [CrossRef] [PubMed]
- Neuß, F.; et al. Epileptic seizures in multiple sclerosis: prevalence, competing causes and diagnostic accuracy. J. Neurol. 2021, 268, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Baroncini, D.; Simone, M.; Iaffaldano, P.; Brescia Morra, V.; Lanzillo, R.; Filippi, M.; Romeo, M.; Patti, F.; Chisari, C.G.; Cocco, E.; Fenu, G.; Salemi, G.; Ragonese, P.; Inglese, M.; Cellerino, M.; Margari, L.; Comi, G.; Zaffaroni, M.; Ghezzi, A.; Italian MS Registry. Risk of persistent disability in patients with pediatric-onset multiple sclerosis. JAMA Neurol. 2021, 78, 726–735.
- Baroncini, D.; Ghezzi, A.; Guaschino, C.; et al. Long-term follow-up (up to 11 years) of an Italian pediatric MS cohort treated with natalizumab: a multicenter, observational study. Neurol. Sci. 2022, 43, 6415–6423. [Google Scholar] [CrossRef]
- Menascu, S.; Fattal-Valevski, A.; Vaknin-Dembinsky, A.; Milo, R.; Geva, K.; Magalashvili, D.; Dolev, M.; Flecther, S.; Kalron, A.; Miron, S.; Hoffmann, C.; Aloni, R.; Gurevich, M.; Achiron, A. Effect of natalizumab treatment on the rate of No Evidence of Disease Activity in young adults with multiple sclerosis in relation to pubertal stage. J. Neurol. Sci. 2022, 432, 120074. [Google Scholar] [CrossRef] [PubMed]
- Tysabri, INN: natalizumab. ANNEX I, SUMMARY OF PRODUCT CHARACTERISTICS. Available online: https://ec.europa.eu/health/documents/community-register/2016/20160425134515/anx_134515_en.pdf (accessed on 16. September.2025).
- Simone IL, Carrara D, Tortorella C, Liguori M, Lepore V, Pellegrini F, Bellacosa A, Ceccarelli A, Pavone I, Livrea P. Course and prognosis in early-onset MS: comparison with adult-onset forms. Neurology. 2002 Dec 24;59(12):1922-8.
- JASP (version 095.1). Available online: https://jasp-stats.org/download (accessed on 4. September.2025).
- Generative artificial intelligence (GenAI). Available online: https://chat.chatbot.app/gpt5?utm_source=GoogleAds&utm_medium=cpc&utm_campaign={campaign}&utm_id=22665487438&utm_term=182338911722&utm_content=757447283652&gad_source=1&gad_campaignid=22665487438&gbraid=0AAAAA_a6ETsikdcm2etAVUS29TfmeuBPM&gclid=CjwKCAjw2brFBhBOEiwAVJX5GJ2EQ0nD506CWe1T2v9U%20R1wOyA211E_GT__p4-lcIctgJfiOpggp8xoCW9wQAvD_BwE (accessed on 4. September.2025).
Figure 1.
PRISMA flow.

Figure 2.
Predicted probability (95% CI) of incomplete remission by treatment group from binomial logistic regression. The plot illustrates a decreasing probability for incomplete remission with increasing treatment intensity. Big black dots represent model-based estimates; bars indicate 95% CIs; light dots show individual remission outcomes tendencies (jitter). S=steroids.
Figure 2.
Predicted probability (95% CI) of incomplete remission by treatment group from binomial logistic regression. The plot illustrates a decreasing probability for incomplete remission with increasing treatment intensity. Big black dots represent model-based estimates; bars indicate 95% CIs; light dots show individual remission outcomes tendencies (jitter). S=steroids.
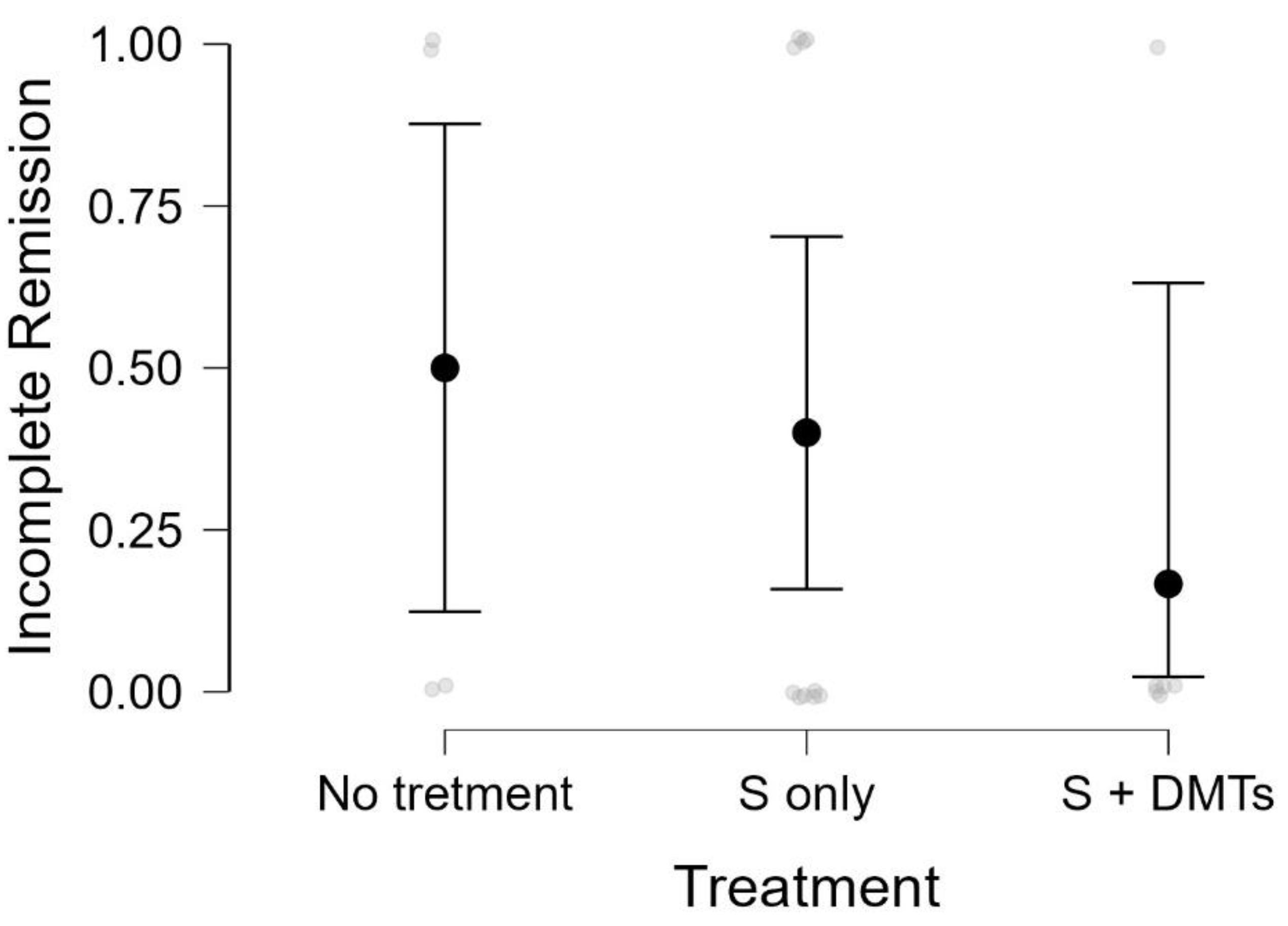
Figure 3.
Patient clinical and imaging evolution correlated to treatment.
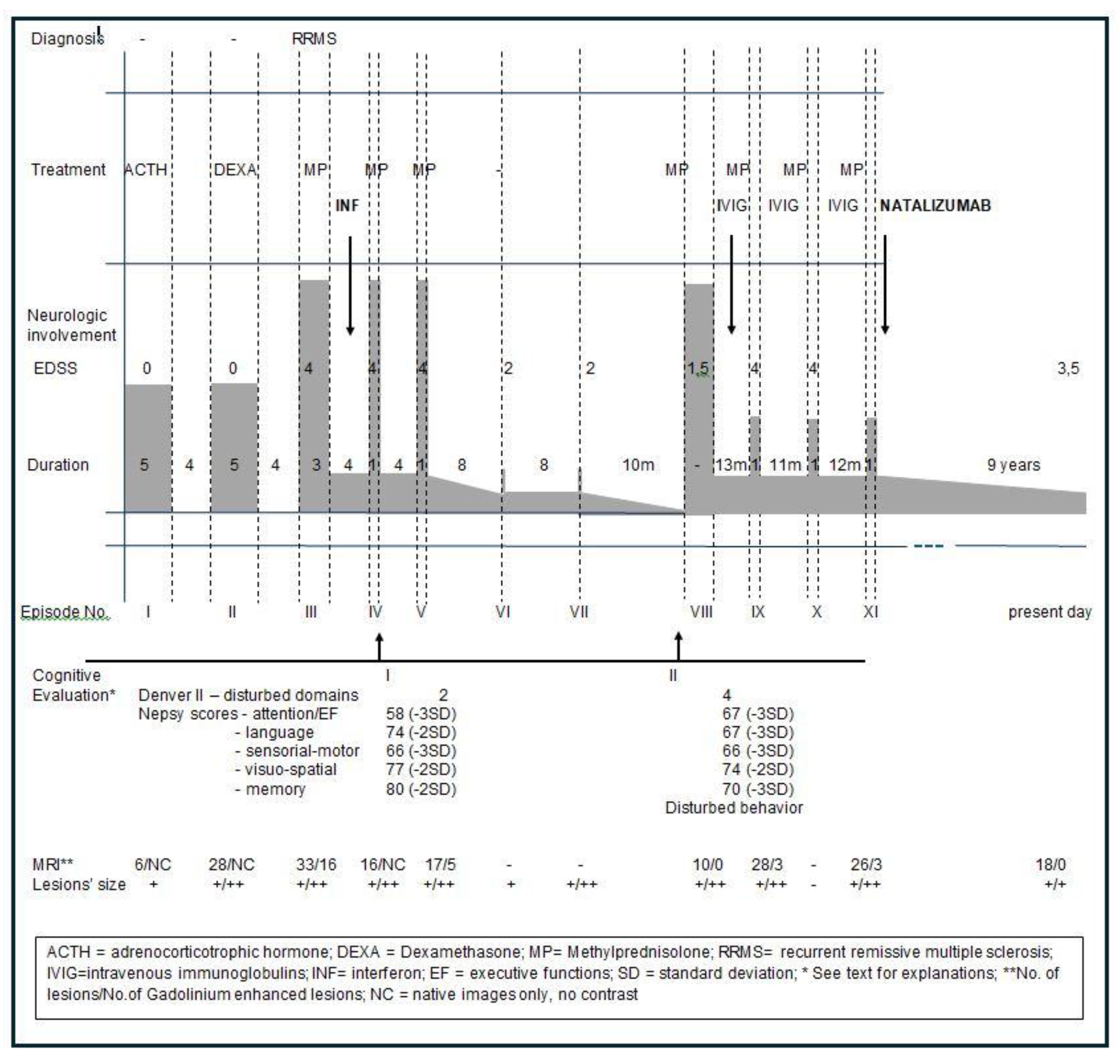
Figure 4.
MRI at onset and in evolution.
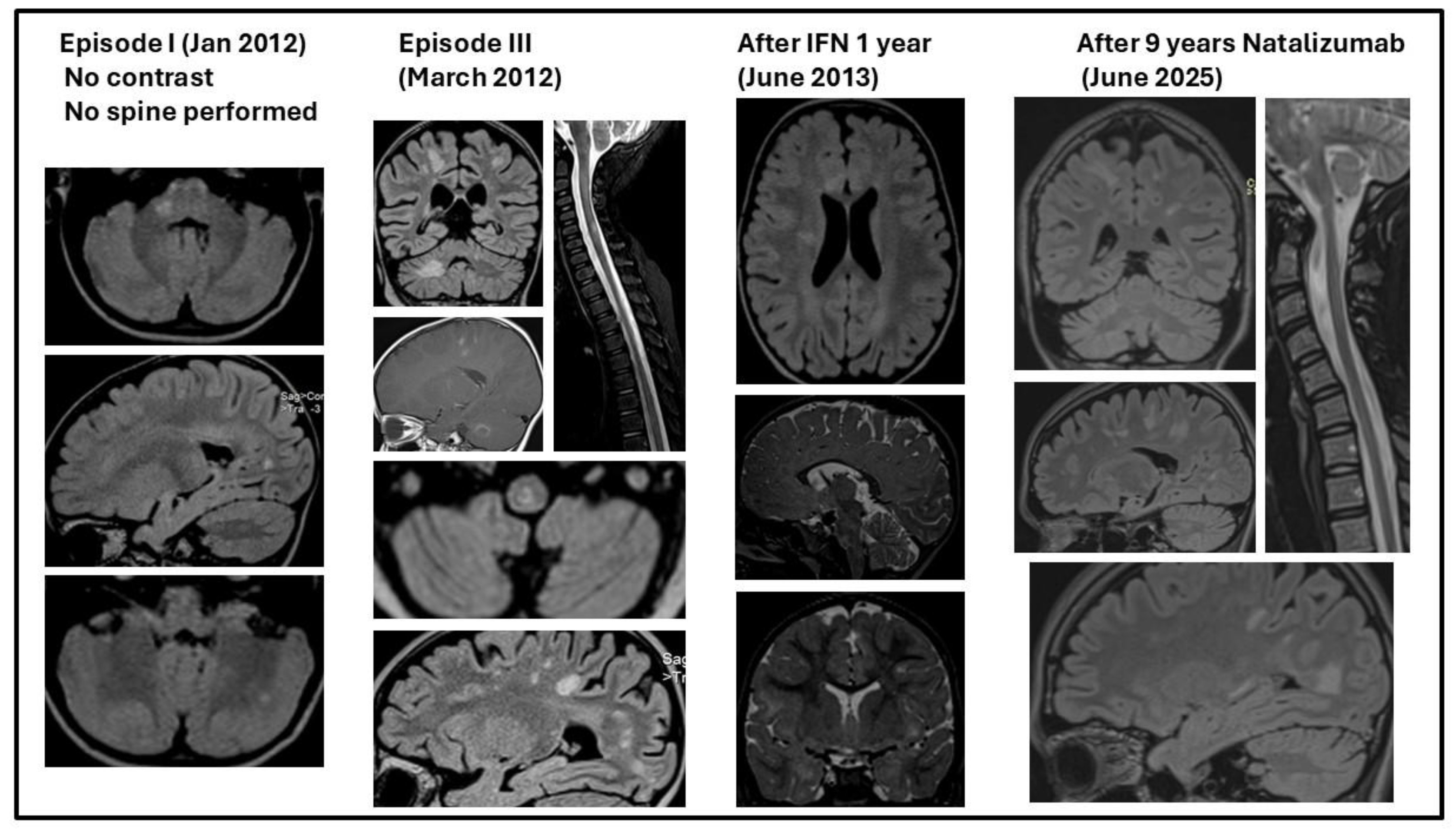

Table 1.
Demographic features and follow-up.
| Features | |
| Sex | |
| Male | 42 |
| Female | 59 |
| F:M ratio | 1.47:1 |
| Age at onset (mo.) mean ± SD (range) | 36 ± 13.29 (10-60) |
| Mean total number of attacks | 4.1 |
| Mean number of attacks in the first 2 years | 2.3 |
| Follow-up time (mo.) mean (range) | 26.4 (10-48) |
Abbreviations: mo.=months; SD = standard deviation.
Table 2.
Clinical Features and Presentation during course of disease.
| Features | Onset (%of cases) | Evolution (% of cases) |
| Symptoms | ||
| Ataxia | 57.4% | 42.9.% |
| Pyramidal | 41.4% | 47.5% |
| Fever +- Lethargy / Altered Consciousness | 17.2% | 4.9% |
| Ophthalmoplegia | 10.3% | 3.9% |
| Optic neuritis | 6.9% | 21.7% |
| Seizures | 4.3% | 22.7% |
| Neurogenic Bladder | 3.9% | 3.9% |
| Other Cranial Nerve palsy | 3.4% | 19.8% |
Table 3.
Diagnostic work-up summary.
| Features | % of all cases | % of tested cases |
| MRI | ||
| Supratentorial lesions | 57.4% | 59.1% |
| Periventricular | 57.4% | 59.1% |
| Cortical/Subcortical | 24.7% | 25.5% |
| Infratentorial lesions | 36.6% | 37.7% |
| Brainstem | 31.7% | 32.7% |
| Spinal cord | 11.9% | 12.2% |
| Cerebellum | 9.9% | 10.2% |
| CSF | ||
| Normal CSF | 11.9% | 12.1% |
| Oligoclonal bands (positive) | 31.7% | 32.3% |
| Pleocytosis | 44.5% | 45.5% |
| Elevated protein | 26.7% | 27.3% |
| VEP | ||
| Abnormal VEP | 9.9% | 33.3% |
| Normal VEP | 19.8% | 66.7% |
Abbreviations: CSF=cerebrospinal fluid; VEP = visual evoked potentials; MRI=magnetic resonance imaging.
Table 4.
Treatment overview.
| Features | Number | % of all cases | % of treated cases |
| Steroid therapy | 44 | 43.5% | 80% |
| Methylprednisolone | 26 | 25.7% | 47.3% |
| Prednisone/ Prednisolone | 17 | 16.8% | 30.9% |
| Other steroids | 3 | 2.9% | 3.7% |
| Intravenous immunoglobulin | 3 | 2.9% | 3.7% |
| Disease-modifying therapy | 11 | 10.9% | 20.0% |
| Interferons | 4 | 4.0% | 7.3% |
| Azathioprine | 3 | 2.9% | 3.7% |
| Dimethyl fumarate | 1 | 1.0% | 1.8% |
| Glatiramer acetate | 1 | 1.0% | 1.8% |
| Natalizumab | 1 | 1.0% | 1.8% |
| Rituximab | 1 | 1.0% | 1.8% |
Table 5.
Detailed description of the episodes and treatment.
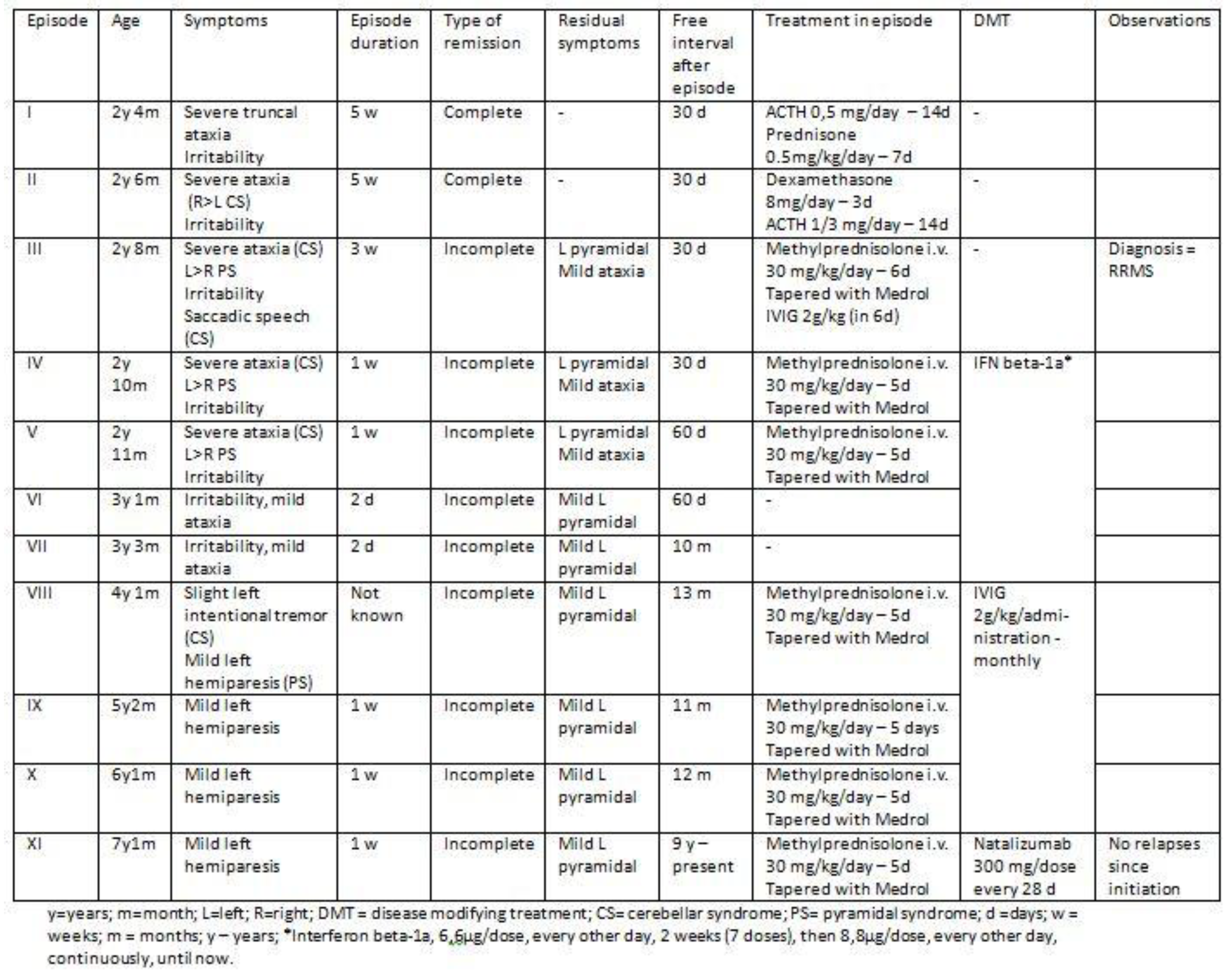 |
Table 6.
Workup and differential diagnosis [28].
Table 6.
Workup and differential diagnosis [28].
| Differential diagnosis | Observations | Investigation |
| NMO, recurrent | - No optic neuritis - Spinal cord involvement less than 3 spinal segments |
AQP4 negative Oligoclonal bands negative |
| ADEM, recurrent | - No encephalopathy (except behavioral symptoms at first episode) - Remission of the initial symptoms followed by new symptoms after an interval of 1 month (MS more probable) Miller et al. [28] |
MRI – DIT, DIS, lesions typical for MS |
| Infectious diseases including Borreliosis, HIV, HBV, EBV, cysticercosis | - no fever - no other organ involvement |
LP - CSF and blood serology negative |
| Autoimmune disorders | - no other organ involvement | Blood serology negative (ANA, anti-dsDNA antibodies, anti Sm antibodies, serum Complement) |
| Mitochondrial disorder | - no other organ involvement - clinical evolution typical for MS - treatment - efficacious |
Lactic acid negative – blood and CSF; MRI – lesions typical for MS |
NMO=neuromyelitis optica; AQP4=serum aquaporin-4 autoantibodies; ADEM=Acute disseminated encephalomyelitis; MS=multiple sclerosis; MRI=magnetic resonance imaging; DIT=dissemination in time; DIS=dissemination in space; HIV=human immunodeficiency virus; HBV=Hepatitis B virus; EBV=Epstein-Barr Virus; LP=lumbar puncture; CSF=cerebrospinal fluid; ANA=Anti-nuclear antibodies; anti dsDNA=anti-double-stranded DNA antibody; anti-Sm=Anti-Smith Antibody.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



