
Submitted:
18 September 2025
Posted:
22 September 2025
You are already at the latest version
Abstract
Informal caregivers play a vital role in cancer care, frequently managing complex emo-tional, physical, and logistical responsibilities. While caregiving can be rewarding, it is often associated with psychological distress and diminished wellbeing. Emerging evi-dence suggests that sociodemographic characteristics may significantly influence how caregivers experience this burden. This scoping review aimed to synthesize recent lit-erature on the associations between caregiver sociodemographic factors and wellbeing outcomes in the context of cancer care. A systematic search of the PubMed database was conducted in accordance with the PRISMA-ScR guidelines, targeting studies pub-lished between 2020 and 2025. The final search strategy included terms related to fami-ly caregiving, cancer, sociodemographics, and wellbeing. After screening for eligibility and applying inclusion criteria, 12 peer-reviewed studies were selected. Data were ex-tracted on cancer type, caregiver characteristics, sociodemographic variables, wellbeing outcomes, and significant findings. The included studies examined caregivers of pa-tients with breast, pediatric, and oral cancers. Primary wellbeing outcomes included stress, depression, anxiety, resilience, quality of life, and preparedness for caregiving or end-of-life support. Low income, limited formal education, female gender, and un-employment consistently emerged as predictors of poorer psychological outcomes. Eleven of the twelve studies reported statistically significant associations between so-ciodemographic disadvantage and increased distress. In contrast, marital status, reli-gious affiliation, and prior caregiving experience were occasionally associated with greater resilience or reduced burden. This review underscores that caregiver wellbeing in cancer contexts is shaped not only by clinical demands but also by structural and so-cial inequalities. Sociodemographic disadvantage is a consistent predictor of mental health vulnerability. Equity-focused, culturally sensitive, and targeted support strate-gies are needed to mitigate the psychosocial toll of caregiving, particularly among high-risk and underserved populations.
Keywords:
cancer caregiving
; sociodemographic factors
; caregiver wellbeing
1. Introduction
Cancer is a complex disease that profoundly affects not only patients but also the informal caregivers—often family members—who support them through diagnosis, treatment and survivorship or end-of-life care. These caregivers perform a range of demanding tasks, including emotional support, medical coordination and daily physical assistance. Gender norms often position women as default caregivers, exposing them to cumulative stress and role conflict While caregiving can bring personal meaning, it frequently results in emotional exhaustion, depression, anxiety and reduced quality of life [1,2].
Importantly, caregiving outcomes are shaped by sociodemographic conditions. Numerous studies show that women, individuals with lower education and economically disadvantaged caregivers report significantly worse mental health and wellbeing [3,4,5]. These disparities reflect not only individual stress but also structural inequalities that affect access to health resources, social support and coping capacity.
Theoretical frameworks such as the Stress Process Model [6] and Social Determinants of Health [7] explain how external social conditions shape internal psychological responses. These models help explain why caregiving stress may be compounded by unemployment, poor housing, or limited health literacy, especially in contexts of advanced cancer care. Moreover, Resilience Theory suggests that positive psychological traits and strong social ties can buffer caregivers against stress—but these are also unevenly distributed along socioeconomic lines [8].
Despite rising recognition of these disparities, no recent synthesis has mapped how sociodemographic variables influence caregiver wellbeing specifically within cancer contexts. Understanding these associations is essential to informing equitable caregiving support programs and designing interventions that address both emotional and structural vulnerabilities.
This scoping review aims to identify and synthesize empirical studies published in the last five years that examine the relationship between sociodemographic characteristics and wellbeing outcomes among caregivers of cancer patients. This review aims to synthesise current evidence and identify key trends in order to guide future research and inform best practices in psycho-oncology and caregiver support.
2. Materials and Methods
This review follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [9], a tool specifically designed to guide the development and transparent reporting of scoping reviews. Unlike systematic reviews, which aim to answer narrowly defined questions often focused on intervention effectiveness, scoping reviews are used to map the breadth and depth of research activity in a given field, identify knowledge gaps, clarify concepts and explore how research is conducted on a particular topic.
Given the exploratory nature of our review objectives (mapping the existing literature on sociodemographic factors influencing the wellbeing of caregivers of cancer patients), a scoping review approach was considered most appropriate. PRISMA-ScR was developed by an expert panel to improve the rigor and transparency of such reviews and its use in this study ensures alignment with methodological standards.
Information Sources and Search Strategy
The literature search was conducted using the PubMed database. The search strategy was iterative, beginning broadly and then refined using filters and Boolean operators to focus on relevant studies.
Searches used to refine and validate this final result included:
- family caregivers - 113,761 articles,
- (family caregivers) AND (cancer) - 5,754 articles (last 5 years),
- (family caregivers) AND (cancer) AND (sociodemographic) - 144 articles (free/full text).
The final search string used was: (family caregivers) AND (cancer) AND (sociodemographic) AND (wellbeing). Filters applied referred to the publication date (last 5 years, 2020–2025) and text availability (free full text and full text only).
This search yielded 23 articles [1,2,3,4,5,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. The final dataset was reviewed to confirm relevance to the research question. Titles and abstracts of retrieved articles were screened for relevance to the inclusion criteria. Full-text reviews were conducted by the authors to confirm eligibility.
Studies were included if they: focused on family or informal caregivers of individuals diagnosed with cancer, examined sociodemographic factors (e.g., age, gender, education, income, ethnicity, marital status) in relation to caregiver wellbeing (e.g., psychological, emotional, or general quality of life), were original research articles, published in English in the last five years, were accessible as full-text articles via PubMed (free full text or full text).
Articles were excluded if they did not directly investigate sociodemographic influences on wellbeing or focused on patient wellbeing instead of caregivers'.
Exclusion criteria:
3. Results
Data found in the 12 studies included in this review is synthesized in Table 1.
The majority of included studies focused on caregivers of patients with breast, pediatric or oral cancers. Most were cross-sectional and used validated tools such as DASS-21, SF-12 and PMHS. Commonly measured outcomes included stress, depression, anxiety, resilience, quality of life and preparedness for caregiving or death. Low income, lower education levels, female gender and unemployment were the most frequently reported predictors of poor mental health outcomes. Some studies also highlighted the protective influence of marital status, religious affiliation and prior caregiving experience on caregiver wellbeing. at least one statistically significant association between sociodemographic factors and caregiver wellbeing were reported in 11 of the 12 studies. Only one study examined an intervention, providing qualitative or descriptive support for benefit but lacked formal statistical testing [15]
The keyword co-occurrence network visualization generated with Voviewer illustrates the relationships between the most frequently used terms in the papers included in the final analysys (Figure 2).
The network shows that caregiver wellbeing in cancer care research is strongly associated with psychosocial outcomes (like stress and resilience), demographic variables (such as age, gender and relationship to the patient) and disease context (e.g., cancer type, treatment stage). “Age” appears central, suggesting that many studies focused on this variable.
A synthesized overview of the 12 included studies, highlighting the sociodemographic variables investigated, the specific wellbeing outcomes assessed and the statistically significant associations identified is provided Table 2.
4. Discussion
In the analyzed studies, sociodemographic factors significantly influenced various aspects of cancer caregivers' well-being and quality of life, including stress levels, mental health (depression, anxiety, distress), quality of life (physical and mental) and resilience.
4.1. Age, Gender, and Marital Status
Older age (≥ 36-40 years) was associated with higher levels of stress [16] and predisposition to experience anxiety and depression [2] ], whereas younger caregivers (18–39 years) reported higher physical and mental QoL [3].Age influenced the "sense of coherence" (SOC) profile, with caregivers under the age of 44 being more likely to fit into the "low sense of coherence-meaning group" profile [5]. Low associations have been found between the age of the caregiver and the importance given to the patient's quality of life, the patient's physical and emotional well-being, as well as the opinions of the oncology team in making treatment decisions [1].
Female gender was a factor that negatively influenced both the physical and mental quality of caregivers in most studies, , consistent with global literature [12,28]. Significant associations of small magnitude were found between the gender of the caregiver and the opinions/feelings of the oncology team in making treatment decisions [1,3]. In one study, no differences in the level of resilience were detected when assessing the overall scores of male and female carers [3], and in another, gender was not a significant predictor of depression, anxiety, or distress [4].
Marital status has been a determining factor in the well-being of caregivers [9]. Divorced or widowed caregivers reported higher stress levels than married caregivers , results similar to those obtained in other studies in the general population [29]. Only one study found that married caregivers were twice as likely to have depression compared to single caregivers [2]. Yet another determined that married caregivers showed higher scores on resilience, especially in the social competence factor, compared to those in domestic partnerships [21].
4.2. Socioeconomic Determinants and Employment
This scoping review highlights that socioeconomic disadvantage—particularly low income, limited formal education and unemployment—was a persistent determinant of poorer caregiver outcomes across diverse cancer care settings. Caregivers from lower socioeconomic backgrounds consistently reported higher levels of psychological distress, including depression, anxiety and caregiver burden [2,4]. Financial strain was also associated with increased perceived stress and reduced coping capacity, emphasizing the need to address material hardships as part of psychosocial oncology care [16,17]. Unemployment or lack of work has been associated with a lower quality of physical and mental life [9,13]. In the study conducted by Branley et al, the share of employed parents decreased significantly with the increase in the number of chronic conditions of the care recipients [14]. Occupation was not a significant predictor of depression or anxiety in caregivers in some studies [2] and in another, half of caregivers (49%) were employed, of whom 63% took time off to care [27].
Lower levels of education were associated with increased distress [4], moderate levels of resilience [3,13. and a lower likelihood of anxiety and depression compared to those with higher education [2]. Caregivers with undergraduate or postgraduate education reported lower stress levels [16] and better resilience [11].
Low economic status was a significant predictor of stress and moderate levels of resilience [3,13]. Food insecurity, which increases with the number of chronic patient conditions, is associated with negative impacts on caregiver health [14]. Financial difficulties influenced the SOC profile of caregivers, with those with a "heavy" financial burden being more likely to fall into the profile with a "low sense of coherence" [8].
4.3. Rurality, Caregiver Role, and Family Composition
Caregivers in rural areas reported more stress than those in urban areas [13]. Residency influenced the SOC profile, with caregivers in rural areas more likely to fall into the "low sense of coherence" profile [5] while caregivers from other regions (outside a specific region) reported better mental health [9].
Being a close family member (parent, spouse, brother/sister) was associated with a significant negative effect on caregivers' mental health [3,11,16] in most studies, with caregivers being the patient's mothers. The caregiver-patient relationship (spouse/partner, family, friend) was not significantly associated with the importance given to most factors in treatment decision-making [1] and no significant predictor of depression or anxiety in caregivers [7].
4.4. Cultural and Religious Influences
Catholic caregivers showed greater resilience, specifically in the structural factor (the ability to organize, plan and have rules and activities even in situations of adversity) compared to other religions [3].
In the Egyptian context, spirituality often serves as a source of strength and resilience. Self-efficacy and a healthy lifestyle have also been negatively correlated with stress. Engaging in self-care activities (exercise, proper nutrition, stress management techniques) can significantly reduce caregiver stress [13]. Generally, studies that have examined this topic have found that religion was associated with protective effects. The buffering effects of social support and religiosity align with Windle’s Resilience Theory [8].
Significant associations of small magnitude were found between the race/ethnicity of the caregiver and factors considered important in making treatment decisions (patient quality of life, physical well-being, lifespan and opinions of the oncology team). Non-Hispanic white caregivers more often considered physical well-being, lifespan and the opinions of the oncology team to be more important [10].
4.5. Patient Characteristics and Contextual Factors
During the analysis we also discovered patient-related factors that impact the caregiver's well-being. The advanced stage of the patient's cancer was a significant predictor of caregiver depression [4], being associated with caregivers' importance of certain factors in making treatment decisions, such as the patient's physical well-being, lifespan and the opinions of the oncology team [1]. Caregivers of stage I-IV patients were about 2.5 times more likely to have anxiety and 3 times more likely to have depression, compared to those who were not aware about the stage of the cancer [7], and in the study made by Wang et al., the stage of the cancer influenced the SOC profile, with caregivers of stage II cancer patients being more likely to fall into the "low sense of coherence" profile [8].
In the study by Amin et al., caregiver stress was significantly affected by the age of the child (caregivers of children over 10 years of age reported greater stress) and the order of birth of the child with cancer [13]. Length of diagnosis/duration of care was a factor that significantly affected caregiver stress, with caregivers of patients diagnosed for a longer period (≥ 4 years) reporting higher stress [13]. A shorter duration of care (<3 months) was associated with a high SOC profile [8]. Time since diagnosis or length of hospital stay were not significant predictors of resilience in a single study [3]. Patient's type of cancer had a significant impact on caregivers' mental health, with caregivers of patients with genitourinary cancers reporting a better quality of mental life [3].
Carers report moderate to high levels of care, family and financial stress [13]. A substantial prevalence of depressive symptoms (65.1%), anxiety (69.5%) and perceived distress (74.7%) was found among caregivers [4]. Another study reported that 45% of caregivers had depression and 52% anxiety [7]. Only one study reported that anxiety and depression in caregivers remained, in most cases, at minimal to moderate levels [3].
The physical and mental QoL of caregivers is affected [16], being influenced by gender, age, marital status and professional status [3]. The patient's QoL, the patient's physical well-being and lifespan, as well as the patient's emotional well-being, are among the most important factors for caregivers in making treatment decisions [1]. Quality of life was a positive predictor of resilience in caregivers [3], but the same leading author found two years later in another study that Positive Mental Health Scale (PMHS) scores were independent of quality of life and other psychological builders [21].
Carers of children with cancer have reported high levels of resilience [3], positively associated with quality of life ,psychological well-being and religious beliefs (Catholicism) and negatively associated with depression, anxiety and caregiver burden. Communication and support from health professionals was determined to improve caregiver readiness and resilience [27]. SOC is closely related to the psychological well-being and subjective well-being (SWB) of caregivers. Caregivers with a high and moderate sense of coherence showed relatively high levels of subjective well-being [8].
4.6. Psychosocial and Health System Support
Support from healthcare professionals has been significantly associated with care preparation and death preparedness [24]. Caregivers' physiological and psychological needs, as well as role conflict, are positive predictors of stress alongside community sources [13]. The opinions and feelings of the oncology team were among the most important factors for caregivers when helping patients make treatment decisions [10].
It is important to note that some studies have revealed contradictory results for certain factors (e.g., marital status, financial status, occupation, gender), which can be attributed to differences in the populations studied, the methodologies used, or the specificity of the measured outcomes (stress, anxiety, QoL, etc.).
4.7. Contradictions and Methodological Diversity
Despite general trends, contradictory findings emerged, particularly concerning gender, marital status and employment. These inconsistencies may reflect heterogeneity in caregiver populations, cultural contexts, outcome measures, and methodological designs. The absence of standard psychometric instruments and variability in theoretical frameworks (e.g., stress-coping theory, SOC) further complicates cross-study comparisons.
5. Conclusions
This scoping review demonstrates that informal caregiving in cancer settings is deeply shaped by sociodemographic context [6,7]. Caregivers facing socioeconomic disadvantage—particularly those with low income, limited education, and unemployment—consistently reported higher levels of psychological distress, including depression, anxiety, and caregiver burden. Gender also influenced caregiver outcomes, with female caregivers often experiencing greater stress yet engaging more actively in supportive interventions. Religion and spirituality, particularly in Catholic contexts, were associated with enhanced resilience and structured coping strategies. Marital status emerged as both a protective and risk factor, depending on the context, suggesting the need for nuanced approaches to social support.
Overall, these findings underscore the need for caregiver support programs to be equity-focused, culturally sensitive, and attuned to the lived realities of structurally disadvantaged populations. Cancer caregiving is not only a medical or emotional labor but a socially stratified experience. To improve caregiver well-being, oncology services and policymakers must incorporate socio-contextual dimensions into psychosocial support models. Tailored interventions addressing financial strain, health literacy, and spiritual needs can contribute to improved resilience and quality of life among caregivers.
Research Gaps and Future Directions
Although this scoping review provided a comprehensive overview of sociodemographic factors influencing the wellbeing of cancer caregivers, several important research gaps remain that limit the depth and applicability of current evidence.
Despite robust patterns, the literature remains methodologically limited. Most of the included studies employed cross-sectional designs, capturing a snapshot of caregiver experiences at a single point in time. While useful for identifying associations, such designs cannot establish causality or account for changes in wellbeing over the caregiving trajectory. Moreover, only a minority employed theory-driven approaches or tested moderating/mediating pathways, leaving much of the explanatory work at a descriptive level. Longitudinal studies are urgently needed to assess how sociodemographic factors interact with disease progression, treatment phases and bereavement.
Few studies anchored their analyses in theoretical frameworks such as the Stress Process Model, Resilience Theory or Social Determinants of Health. As a result, many findings remain descriptive or isolated, rather than contributing to a cumulative understanding of caregiver vulnerability and adaptation. Future research should explicitly integrate theory to guide hypothesis formulation, variable selection and interpretation.
The sparse application of theoretical models like the Social Determinants of Health Framework [7], limits our understanding of the mechanisms by which sociodemographic variables exert influence.
These gaps highlight the need for longitudinal, theory-guided research using standardized wellbeing measures. In addition, interventions addressing caregiver support must not be one-size-fits-all but should be tailored to the structural vulnerabilities caregivers face—particularly women and low-income populations—who consistently emerge as at-risk groups.
There is a notable underrepresentation of male caregivers, non-heteronormative family structures and minority ethnic groups. Although several studies included diverse samples, few performed subgroup analyses or culturally tailored assessments. Moreover, caregivers of patients with other cancer types were infrequently represented, limiting generalizability across the cancer care spectrum.
Although many studies measured wellbeing (e.g., stress, QoL, resilience), the tools used varied widely. Instruments such as the DASS-21, SF-12 and PMHS were used inconsistently, making comparisons across studies difficult. The field would benefit from adopting core outcome sets for caregiver mental health and burden to enable meta-analyses and benchmarking.
Although the importance of spirituality appeared across several studies, this domain remains under-theorized. Future studies should explore how spiritual beliefs, practices, and affiliations buffer against distress or promote resilience in cancer caregiving. While many studies reported bivariate associations between sociodemographic factors and wellbeing outcomes, multivariate models were often lacking or poorly reported. This limits the ability to control confounding variables and identify independent predictors. More robust statistical modeling, including mediation/moderation analysis, could uncover pathways by which structural inequality affects wellbeing.
None of the reviewed studies explicitly described the medical rehabilitation interventions employed by recipients for pain management, which limits the ability to examine potential associations between these interventions, the patients’ well-being and that of their caregivers [30]. The integration of rehabilitation into primary healthcare, as highlighted by Iancu et al., underscores the role of multidisciplinary interventions in preserving functionality and quality of life in elderly patients, an approach that can be extrapolated to cancer care, where enhancing patients’ independence may indirectly support the well-being of caregivers by reducing the burden of dependency and disability [31].
Finally, only one study explored a psychosocial intervention (dance/movement therapy) and even that lacked inferential analysis. The field remains heavily focused on burden documentation rather than solution testing. There is an urgent need for intervention studies that address sociodemographic disparities in caregiver stress, with attention to feasibility, cultural adaptation and cost-effectiveness.
6. Study Limitations
This review was limited to free full-text articles published in English and indexed in PubMed. Thus, it may exclude relevant studies in other databases or languages. The review also did not assess the risk of bias.
The heterogeneity of included studies—with respect to cancer types, caregiving roles and measurement tools—made synthesis challenging. Although some studies were not cancer-specific they were included based on their focus on sociodemographic influences on caregiver wellbeing.
Finally, most studies employed cross-sectional and descriptive designs, limiting causal inference and the ability to assess the longitudinal impacts of caregiving. The scarcity of intervention trials further restricts actionable insights into improving caregiver wellbeing.
Several limitations should be considered when interpreting the findings of this review. First, the scope of the search was limited to PubMed and restricted to free full-text English-language articles published in the last five years, which may have excluded relevant studies indexed elsewhere or written in other languages. Second, data heterogeneity across the included studies—such as variation in cancer types, caregiver roles and wellbeing measures—limited the ability to synthesize findings quantitatively.
Although most studies reported statistically significant associations, many did not present complete statistical metrics (e.g., effect sizes, confidence intervals), reducing comparability. Additionally, some included studies relied on cross-sectional designs, which preclude conclusions about causality. Finally, one study, [15] lacked inferential analysis, providing only descriptive data.
Despite these limitations, this review provides a comprehensive overview of the current landscape and identifies key gaps in the literature, especially regarding underrepresented populations and intervention-based research.
Author Contributions
Conceptualization, S.T., A.K., C.G.; methodology, S.T., A.K., C.G..; software, S.T., A.K., C.G..; validation, S.T., A.K., C.G.; formal analysis, S.T., A.K., C.G..; investigation, S.T., A.K., C.G..; data curation, S.T., A.K., C.G.; writing—original draft preparation, S.T., A.K., C.G.; writing—review and editing, S.T., A.K., C.G.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is available upon reasonable request..
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bechthold, A.C.; Azuero, A.; Puga, F.; Ejem, D.B.; Kent, E.E.; Ornstein, K.A.; Ladores, S.L.; Wilson, C.M.; Knoepke, C.E.; Miller-Sonet, E.; et al. What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey. Cancers 2023, 15, 4792. [Google Scholar] [CrossRef]
- Sharma, B.P.; Haque, Md.I.; Hossain, Md.B.; Sarker, R.J.; Abedin, E.S.; Shahinuzzaman, Md.; Saifuddin, K.; Kabir, R.; Alauddin Chowdhury, A. Depression and Anxiety Status among Informal Caregivers of Patients with Cancer Treated at Selected Tertiary Hospitals in Nepal. Journal of Taibah University Medical Sciences 2024, 19, 482–491. [Google Scholar] [CrossRef]
- Bourissi, H.; Bourkhime, H.; El Rhazi, K.; Mellas, S. Exploring Factors Influencing the Physical and Mental Quality of Life of Caregivers of Cancer Patients: A Cross-Sectional Study at Hassan II University Hospital Center. Cureus 2024. [Google Scholar] [CrossRef]
- Belapurkar, P.; Acharya, S.; Shukla, S.; Kumar, S.; Khurana, K.; Acharya, N. Prevalence of Anxiety, Depression, and Perceived Stress Among Family Caregivers of Patients Diagnosed With Oral Cancer in a Tertiary Care Hospital in Central India: A Cross-Sectional Study. Cureus 2023. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wu, Y.; Huang, X.; Yan, H. Relationship between Sense of Coherence and Subjective Well-Being among Family Caregivers of Breast Cancer Patients: A Latent Profile Analysis. Front. Psychiatry 2025, 15, 1515570. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the Stress Process: An Overview of Concepts and Their Measures. The Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.; Taylor, S. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. The Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Windle, G. What Is Resilience? A Review and Concept Analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Dionne-Odom, J.N.; Azuero, A.; Taylor, R.A.; Wells, R.D.; Hendricks, B.A.; Bechthold, A.C.; Reed, R.D.; Harrell, E.R.; Dosse, C.K.; Engler, S.; et al. Resilience, Preparedness, and Distress among Family Caregivers of Patients with Advanced Cancer. Support Care Cancer 2021, 29, 6913–6920. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Luna, D.; Moral De La Rubia, J.; Martínez Valverde, S.; Bermúdez Morón, C.A.; Salazar García, M.; Vasquez Pauca, M.J. Psychosocial Factors Predicting Resilience in Family Caregivers of Children with Cancer: A Cross-Sectional Study. IJERPH 2021, 18, 748. [Google Scholar] [CrossRef] [PubMed]
- Doege, D.; Frick, J.; Eckford, R.D.; Koch-Gallenkamp, L.; Schlander, M.; Baden-Württemberg Cancer Registry; Arndt, V. Anxiety and Depression in Cancer Patients and Survivors in the Context of Restrictions in Contact and Oncological Care during the COVID -19 Pandemic. Intl Journal of Cancer 2025, 156, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Johnston, E.A.; Goodwin, B.C.; Myers, L.; March, S.; Aitken, J.F.; Chambers, S.K.; Dunn, J. Support-seeking by Cancer Caregivers Living in Rural Australia. Australian and New Zealand Journal of Public Health 2022, 46, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Pasek, M.; Suchocka, L. A Model of Social Support for a Patient–Informal Caregiver Dyad. BioMed Research International 2022, 2022, 4470366. [Google Scholar] [CrossRef]
- Bryl, K.; Tortora, S.; Whitley, J.; Kim, S.-D.; Raghunathan, N.J.; Mao, J.J.; Chimonas, S. Utilization, Delivery, and Outcomes of Dance/Movement Therapy for Pediatric Oncology Patients and Their Caregivers: A Retrospective Chart Review. Current Oncology 2023, 30, 6497–6507. [Google Scholar] [CrossRef]
- Amin, S.M.; Khedr, M.A.; Mansy, A.M.A.; El-Monshed, A.H.; Malek, M.G.N.; El-Ashry, A.M. Assessing Caregiver Stress and Resource Needs in Pediatric Cancer Care. BMC Nurs 2024, 23, 911. [Google Scholar] [CrossRef]
- Branley, C.E.; Goulding, M.; Tisminetzky, M.; Lemon, S.C. The Association between Multimorbidity and Food Insecurity among US Parents, Guardians, and Caregivers. BMC Public Health 2025, 25, 1487. [Google Scholar] [CrossRef]
- Hurtado-de-Mendoza, A.; Gonzales, F.; Song, M.; Holmes, E.J.; Graves, K.D.; Retnam, R.; Gómez-Trillos, S.; Lopez, K.; Edmonds, M.C.; Sheppard, V.B. Association between Aspects of Social Support and Health-Related Quality of Life Domains among African American and White Breast Cancer Survivors. J Cancer Surviv 2022, 16, 1379–1389. [Google Scholar] [CrossRef]
- Monteiro, A.L.; Kuharic, M.; Pickard, A.S. A Comparison of a Preliminary Version of the EQ-HWB Short and the 5-Level Version EQ-5D. Value in Health 2022, 25, 534–543. [Google Scholar] [CrossRef]
- Patel, S.I.; Ghebre, R.; Dwivedi, R.; Macheledt, K.; Watson, S.; Duffy, B.L.; Rogers, E.A.; Pusalavidyasagar, S.; Guo, C.; Misono, S.; et al. Academic Clinician Frontline-Worker Wellbeing and Resilience during the COVID-19 Pandemic Experience: Were There Gender Differences? Preventive Medicine Reports 2023, 36, 102517. [Google Scholar] [CrossRef]
- Chavan, P.P.; Weitlauf, J.C.; LaMonte, M.J.; Sisto, S.A.; Tomita, M.; Gallagher-Thompson, D.; Shadyab, A.H.; Bidwell, J.T.; Manson, J.E.; Kroenke, C.H.; et al. Caregiving and All-cause Mortality in Postmenopausal Women: Findings from the Women’s Health Initiative. J American Geriatrics Society 2024, 72, 24–36. [Google Scholar] [CrossRef]
- Park, Y.; Kim, S.; Kim, N.; Park, J.H.; Bang, G.; Kang, D.; Yoon, S.E.; Kim, K.; Cho, J.; Kim, S.J. Different Level and Difficulties with Financial Burden in Multiple Myeloma Patients and Caregivers: A Dyadic Qualitative Study. Seminars in Oncology Nursing 2025, 151848. [Google Scholar] [CrossRef]
- Amonoo, H.L.; Guo, M.; Boardman, A.C.; Acharya, N.; Daskalakis, E.; Deary, E.C.; Waldman, L.P.; Gudenkauf, L.; Lee, S.J.; Joffe, H.; et al. A Positive Psychology Intervention for Caregivers of Hematopoietic Stem Cell Transplantation Survivors (PATH-C): Initial Testing and Single-Arm Pilot Trial. Transplantation and Cellular Therapy 2024, 30, 448.e1–448.e14. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Jiménez, S.; Moral De La Rubia, J.; Merino-Soto, C.; Rivera-Rivera, L. Positive Mental Health Scale (PMHS) in Parents of Children with Cancer: A Psychometric Evaluation Using Item Response Theory. Cancers 2023, 15, 2744. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, K.L.; Anunwah, E.; Gilmore, S.; Griffiths-Randolph, U.; Karvonen, K.A.; Moore, D.; Miller, K.; Overall, J.; Wooten, L.; Afulani, P.A. Gaps, Successes, and Opportunities Related to Social Drivers of Health from the Perspectives of Black Preterm Infant Caregivers: A Qualitative Study. The Journal of Pediatrics 2025, 282, 114598. [Google Scholar] [CrossRef] [PubMed]
- Aguirre Vergara, F.; Pinker, I.; Fischer, A.; Seuring, T.; Tichomirowa, M.A.; De Beaufort, C.; Kamp, S.-M.; Fagherazzi, G.; Aguayo, G.A. Readiness of Adults with Type 1 Diabetes and Diabetes Caregivers for Diabetes Distress Monitoring Using a Voice-Based Digital Health Solution: Insights from the PsyVoice Mixed Methods Study. BMJ Open 2025, 15, e088424. [Google Scholar] [CrossRef] [PubMed]
- Häger Tibell, L.; Årestedt, K.; Holm, M.; Wallin, V.; Steineck, G.; Hudson, P.; Kreicbergs, U.; Alvariza, A. Preparedness for Caregiving and Preparedness for Death: Associations and Modifiable Thereafter Factors among Family Caregivers of Patients with Advanced Cancer in Specialized Home Care. Death Studies 2024, 48, 407–416. [Google Scholar] [CrossRef]
- Pinquart, M.; Sorensen, S. Gender Differences in Caregiver Stressors, Social Resources, and Health: An Updated Meta-Analysis. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 2006, 61, P33–P45. [Google Scholar] [CrossRef]
- Rada, C. Intergenerational Family Support in Romania. Rev. Psih. 2014, 60(4), 293–303. [Google Scholar]
- Bordinc, E.; Irsay, L. Indications and Contraindications of Physiotherapy in Breast Cancer Patients. BALNEO 2014, 5, 99–107. [Google Scholar] [CrossRef]
- Iancu, M.A.; Dumitra, G.G.; Ivanov, S.M.; Ivanov, A.M.; Sandu, M.N.; Ticarau, A.; Calin, R.D.; Popescu, D.; Condur, L.M.; Popovici, C.; et al. Rehabilitation of the Elderly in Primary Healthcare. Balneo and PRM Research Journal 2025, 16, 791–791. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram.
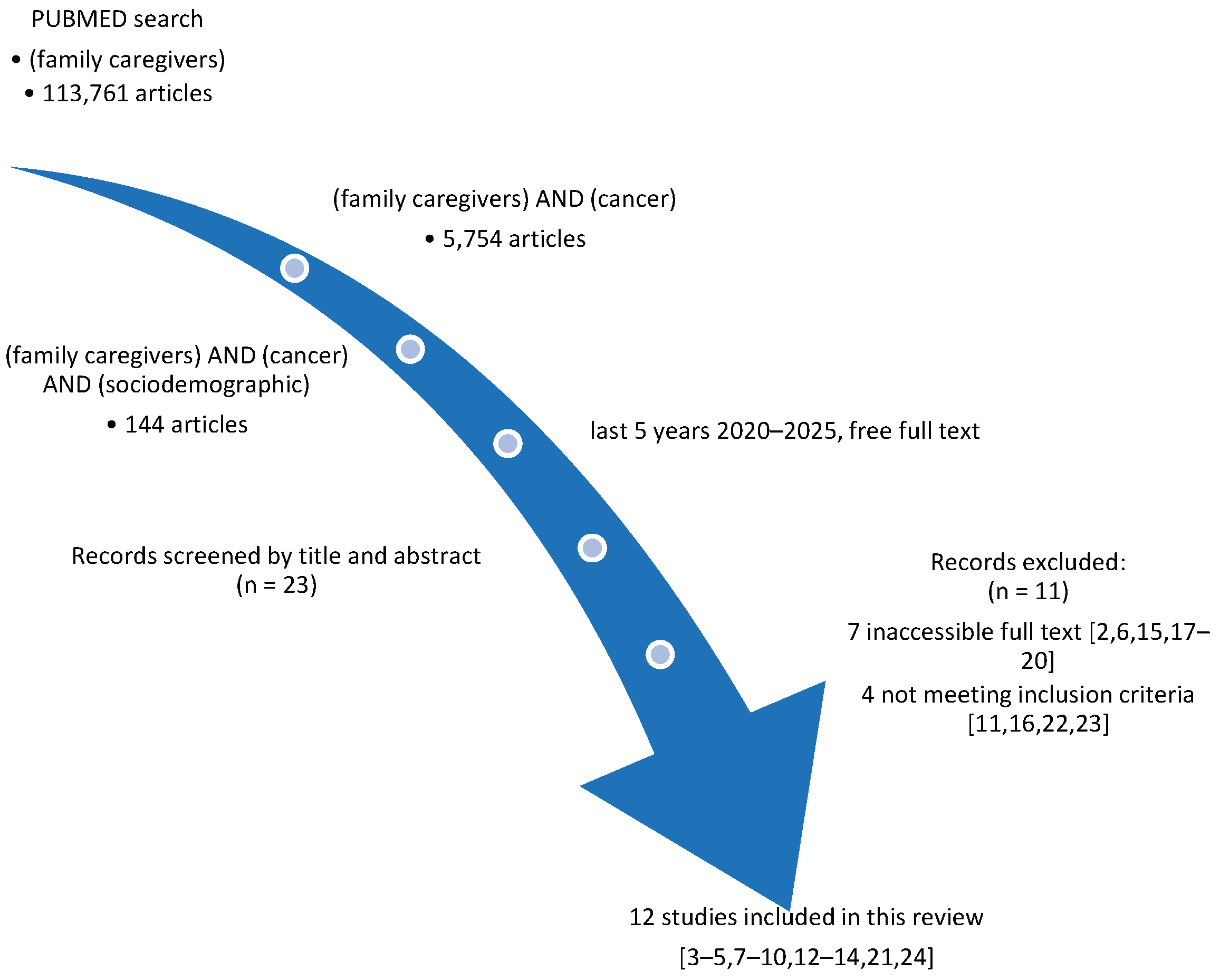
Figure 2.
Keyword co-occurrence network in the selected studies.
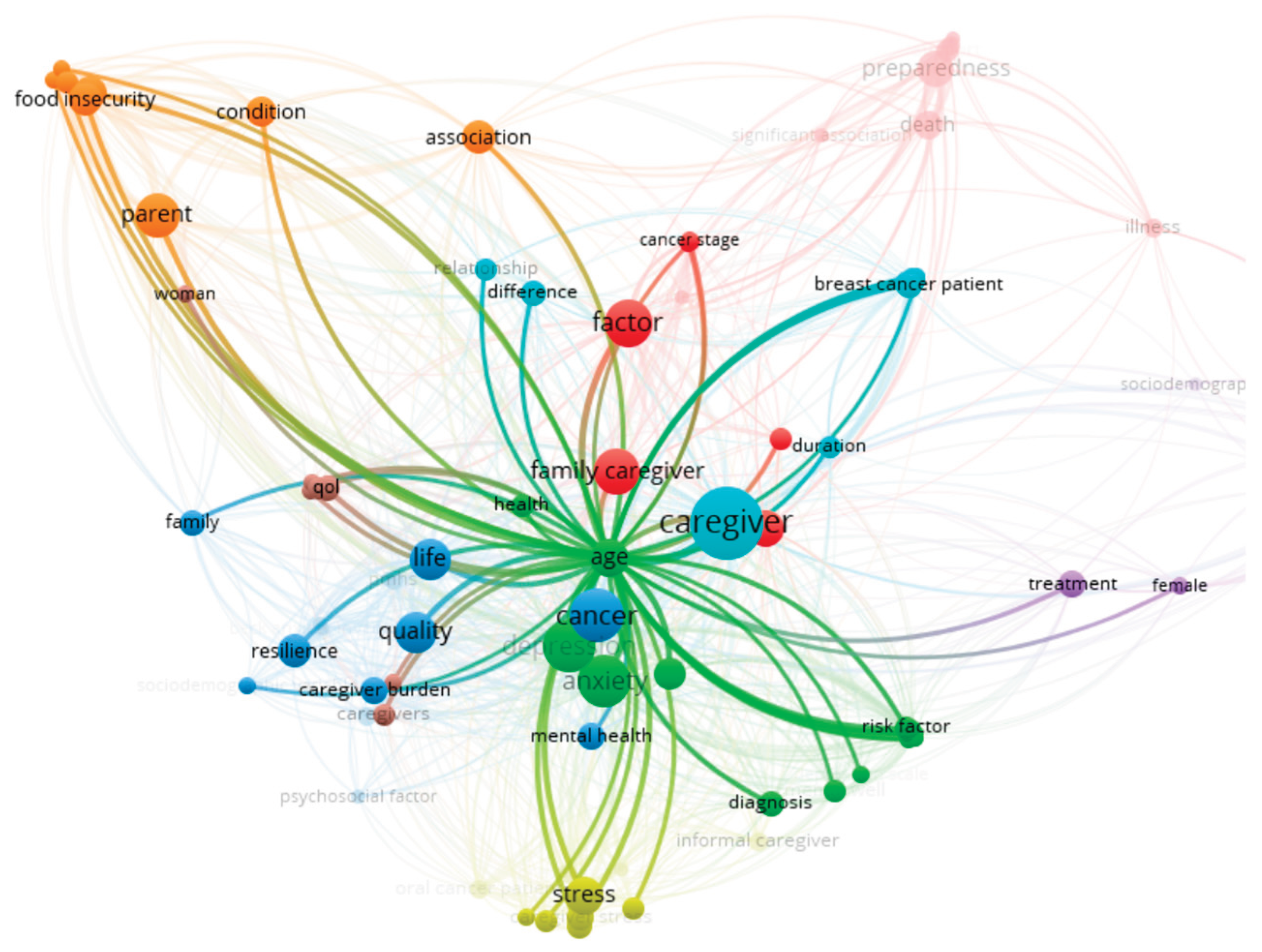

Table 1.
General data from the 12 studies.
| Study | Year | Study Type/Design | Population & Setting | Cancer Type | Factors Examined | Wellbeing Outcomes | Key Findings | Implications |
|---|---|---|---|---|---|---|---|---|
| Amin et al. | 2024 | Cross-sectional descriptive study | 258 caregivers of pediatric cancer patients, Egypt | Pediatric cancer | Age, education, marital status, income, number of children, child’s age, diagnosis duration | Caregiver stress (KCSS), resource needs (CNRA) | Higher stress linked to lower income, higher education; number of children, age, diagnosis duration significant; psychological needs increased stress | Support programs should consider income and educational background; psychological/spiritual support is crucial |
| Bechthold et al. | 2023 | National survey; quantitative analysis with mixed models | 1,661 US caregivers, various cancer types | Various cancer types | Age, race, gender, ethnicity | Values in decision-making (QoL, emotional wellbeing, etc.) | Top factors: QoL, physical/emotional wellbeing; importance of oncology team opinions varied by age, race, gender | Care planning should incorporate diverse caregiver values; culturally sensitive decision-making needed |
| Belapurkar et al. | 2023 | Cross-sectional survey | 82 caregivers of oral cancer patients, India | Oral cancer | Education, employment, income, cancer stage | Depression (BDI-II), Anxiety (MAS), Stress (PSS-10) | High rates of depression (65.1%), anxiety (69.5%), stress (74.7%); lower education and income correlated with worse outcomes | Highlights urgent need for mental health and financial support for low-SES caregivers |
| Bourissi et al. | 2024 | Cross-sectional study | 247 caregivers at Moroccan university hospital | Various (Moroccan setting) | Age, gender, employment, marital status, relationship to patient, cancer type | Physical and mental QoL (SF-12) | Older age, female gender, unemployment and close relation to patient worsened mental and physical QoL | Need for targeted social and economic support interventions for vulnerable subgroups |
| Branley et al. | 2025 | Cross-sectional survey using national data | 26,579 US caregivers (NHIS data) | Various (NHIS caregivers) | Chronic disease count, income, race, gender | Food insecurity | Multimorbidity (esp. with mental conditions) strongly associated with higher food insecurity; disparities across racial/ethnic groups | Public health policies should address chronic health and food security among caregivers, especially in disadvantaged communities |
| Bryl et al. | 2023 | Retrospective chart review | Pediatric oncology patients and their caregivers, US hospital | Pediatric cancer | Not detailed | Intervention participation, psychosocial outcomes | Dance/movement therapy sessions well-received; suggested positive impact on caregiver-child interaction and stress relief | Integrative therapies may benefit both patients and caregivers in pediatric oncology |
| Doege et al. | 2025 | Observational study during COVID-19 | 2439 cancer patients and survivors (including caregivers), Germany | Various cancers | Not caregiver-specific;age, gender, education, marital status, income, living situation | Anxiety, depression during pandemic restrictions | Significant mental health burden noted; caregiver roles contributed to increased anxiety/depression levels | Pandemic preparedness in oncology care should include mental health support for caregivers |
| Häger Tibell et al. | 2024 | Cross-sectional study | 39 Family caregivers in specialized home care, Sweden | Advanced cancer | Gender, relationship to patient, time spent caregiving, age, education, enployment | Preparedness for caregiving and death | Higher preparedness linked with prior training and experience; emotional readiness predicted post-death adaptation | Training programs for end-of-life care could enhance caregiver wellbeing and resilience |
| Sharma et al. | 2024 | Cross-sectional study | 383 Caregivers of cancer patients, Nepal | Various | Age, gender, education, employment, income, marital status | Depression and anxiety (DASS-21) | High prevalence of moderate to severe anxiety and depression; females and unemployed most affected | Mental health screening and support crucial, especially for vulnerable caregivers |
| Toledano-Toledano et al. | 2021 | Cross-sectional study | 330 caregivers of children with cancer, Mexico | Pediatric cancer | Age, gender, education, marital status, religion, income, number of children, caregiver relationship | Resilience (RESI-M), depression, anxiety, QoL, caregiver burden, psychological wellbeing | Resilience positively associated with education, psychological wellbeing and QoL; negatively with depression, anxiety, burden; married and Catholic caregivers showed higher resilience | Tailored psychosocial interventions should consider educational level, marital status and religious support to enhance resilience |
| Toledano-Toledano et al. | 2023 | Cross-sectional psychometric evaluation using IRT | 623 caregivers of children with cancer, Mexico | Pediatric cancer | Age, gender, education, income, family status, religion | Positive mental health (PMHS), depression, anxiety, QoL, caregiver burden, resilience | PMHS is a valid and reliable tool for assessing caregiver mental health; positive mental health moderately independent of depression/anxiety | PMHS can be used in caregiver interventions to monitor mental wellbeing; policies should focus on holistic health support for caregiving parents |
| Wang et al. | 2025 | Latent profile analysis | 360 caregivers of breast cancer patients, China | Breast cancer | Age, gender, income, education, caregiving time, residence, income | Sense of coherence, subjective wellbeing | Three caregiver profiles identified; high coherence linked to better wellbeing; income and education major predictors | Interventions should tailor support based on caregiver profiles and SES |
Table 2.
Significant statistics found in the studies.
| Study | Year | Factors Examined | Wellbeing Outcomes | Key Findings |
| Amin et al. | 2024 | Age, education, marital status, income, number of children, children’s age, diagnosis duration, spirituality | Caregiver stress (KCSS), resource needs (CNRA) | Higher stress linked to lower income, rural residence, marital status and higher age (p < 0.01), higher education was a protective factor (p < 0.05); number of children, diagnosis duration (p < 0.05) influenced stress; higher psychological needs increased stress (p < 0.01), spirituality negatively corellated with stress (p < 0.05). |
| Bechthold et al. | 2023 | Age, race, gender, ethnicity | Decision-making preferences, support needs | Caregivers with lower education/income more likely to need treatment information (OR 2.1, p = 0.032); female and non-White caregivers had distinct support preferences (p < 0.05). significant associations between caregiver age and patient quality of life, physical and emotional well-being and the opinions/feelings of the oncology team (p < 0.001); caregiver gender (p = 0.006) and race (p = 0.009) and the opinions/feelings of the oncology team Cramer’s V = 0.079) and caregiver ethnicity and patient physical well-being (p = 0.004) |
| Belapurkar et al. | 2023 | Education, employment, income, cancer stage | Depression (BDI-II), Anxiety (MAS), Stress (PSS-10) | High rates of depression (65.1%), anxiety (69.5%), stress (74.7%); lower education and income significantly associated with worse caregiver outcomes (p < 0.001). Depresion was linked to cancer stage, employment status and lower income to anxiety and educational attainment to distress and anxiety. |
| Bourissi et al. | 2024 | Income, education, employment, marital status | Physical and mental quality of life | Lower education and lower income predicted worse physical and mental QoL (p < 0.05); married caregivers showed better scores (p = 0.041). higher age (over 40), gender (female), close family ties to the pacient and unemployment vere predictors of lower QoL. Regional differences were also found. |
| Branley et al. | 2025 | Chronic disease count, income, race, gender | Food insecurity | Caregivers with 3+ chronic conditions had 2.7× higher odds of food insecurity (95% CI: 1.9–3.6, p < 0.001) and reported more frequently depression and anxiety; race and income disparities were statistically significant. |
| Bryl et al. | 2023 | Caregiver participation, therapy exposure | Engagement, perceived benefit | Therapy decreased caregiver’s burden and improved relationship with the care beneficiar was reported. |
| Doege et al. | 2025 | General caregiver roles (within patient sample) | Anxiety, depression | Significantly increased anxiety (GAD-7, mean = 10.3) and depression (PHQ-9, mean = 11.8) during COVID-19 care restrictions (p < 0.001). |
| Häger Tibell et al. | 2024 | Gender, relationship to patient, time spent caregiving, age, education, enployment | Preparedness for caregiving and death | Higher preparedness correlated with prior caregiving experience (p = 0.008) and emotional readiness (p < 0.01); predictive of better coping after patient death. No result on sociodemographic factors found during review. |
| Sharma et al. | 2024 | Income, rural residence, education, age, gender, employment, income, marital status | Depression, anxiety | Depression and anxiety were significantly higher in rural, low-income caregivers, over 36 years old (p < 0.001); education level also predictive (p = 0.013). married caregivers were more depressed. Hospital type (gouvernamental or not) and pacient cancer stage were also predictors for depression and anxiety. |
| Toledano-Toledano et al. | 2021 | Age, gender, education, marital status, religion, income, number of children, caregiver relationship | Resilience (RESI-M), depression, anxiety, QoL, caregiver burden, psychological wellbeing | Higher resilience linked to education (p = 0.002), psychological wellbeing (p < 0.01); negatively correlated with depression, anxiety, caregiver burden (all p < 0.001). Being married and Catholic predicted higher resilience. Education, income and support networs buffer the effects of care. |
| Toledano-Toledano et al. | 2023 | Income, marital status, age, gender, education, family status, religion | Positive mental health (PMHS) | PMHS scores were independent of resilience, depression, anxiety, caregiver burden and quality of life, |
| Wang et al. | 2025 | Age, gender, income, education, caregiving time, type of residence, cancer stage | Sense of coherence, subjective wellbeing | Profile analysis highlighted that high sense of coherence group had best wellbeing (p < 0.001). Age, residence, income and education, caregiving duration are significant predictors(p < 0.01) of positive mental health and subjective wellbeing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



