
Submitted:
17 September 2025
Posted:
21 September 2025
You are already at the latest version
Abstract
Background Human intervention to terminate a pregnancy, while medically effected through a range of pharmaceutical, surgical, and other approaches, is generally referred to in English as “abortion.” It is a fundamental aspect of reproductive healthcare and its availability, regulation, and limits (cultural, familial, legal) are well-documented determinants of women’s and girls’ health worldwide. Despite its routine nature in many health systems, it remains a deeply sensitive issue shaped by cultural, legal, religious, and political factors. Globally, an estimated 73 million abortions occur annually, yet access to safe and timely care is highly variable. In settings where abortion is legal and integrated into healthcare services, it is one of the safest medical procedures. Conversely, restrictive policies force individuals to seek unsafe alternatives, contributing to preventable maternal deaths and long-term health complications. Laws and regulations play a pivotal role in shaping access, but these are influenced by societal norms and often create inequities within and between countries. Methods A systematic review was conducted to identify, collate, and analyse publicly available abortion policies and legislation in English from 1980 to 2025. Data sources included peer-reviewed literature, legal databases, national government portals, and grey literature from global health organisations. Policies were screened, extracted, and appraised using a structured framework. A thematic and contextual analysis was undertaken to explore the legal, operational, and governance components of abortion policies and their implications for access and equity. ResultsPolicies from over 100 countries were included, demonstrating significant global variation. Liberal frameworks, such as those in Iceland, Sweden, England, and New Zealand, were associated with early, safe access through broad on-demand gestational limits and integrated care. Restrictive or grounds-based models, common in parts of Eastern Europe, the Middle East, and Latin America, relied on multi-clinician approvals, waiting periods, and documentation, creating delays and inequities. Federated systems, including the United States and Australia, showed marked regional disparities. Criminal penalties in several countries had a chilling effect, driving cross-border travel and unsafe abortion. Conclusion Global abortion policies vary widely, with many failing to translate legal rights into equitable, practical access. Evidence-informed reforms that integrate health systems research and cultural context are urgently needed to reduce preventable harm and promote reproductive justice.
Keywords:
abortion
; policy
; reproductive health
; thematic analysis
; contextual analysis
Background
Abortion is a critical component of reproductive healthcare and a central issue in the health and well-being of women and girls worldwide [1]. It generally refers to a set of intentional human interventions undertaken to terminate a pregnancy and can be performed safely using medical or surgical techniques when provided within appropriate clinical settings [2]. Despite its routine nature in healthcare systems, abortion remains one of the most sensitive and contested aspects of reproductive health. In the United States, for example, abortion is among the most commonly performed medical procedures, yet it continues to face intense political debate and restrictive regulation [1,3,4,5]. This sensitivity arises from the intersection of personal autonomy, social values, cultural expectations, and religious beliefs. Globally, it is estimated that over 73 million abortions occur annually, reflecting the substantial demand for pregnancy termination services across diverse settings [6]. However, access to safe and timely abortion care varies dramatically between and within countries. In settings where abortion is legal, accessible, and integrated into health systems, the procedure is one of the safest medical interventions, with minimal complication rates [2]. In contrast, restrictive laws or barriers to access lead many individuals to seek unsafe abortions, which contribute to approximately 39,000 maternal deaths each year [2,7], as well as severe long-term health consequences such as chronic pelvic pain, infertility, and psychological distress [8].
Beyond its clinical implications, abortion is deeply embedded in cultural, ethical, and religious contexts. In some societies, abortion is framed through an individual health lens and recognised as essential to gender equality and reproductive rights [9,10]. In others, it is viewed as morally or religiously unacceptable, with doctrines shaping societal attitudes and influencing both individual decision-making and collective policy responses [11,12]. These cultural and religious beliefs often underpin stigma and discrimination, discouraging women and girls from seeking care or disclosing their experiences. The result is a complex global landscape where the same health need may be supported, contested, or criminalised depending on geographic location, political climate, and prevailing social norms. This diversity highlights the urgent need to understand abortion not only as a healthcare service but also as a social phenomenon deeply shaped by context and power structures. Supplementary File 1 presents a narrative case study (‘A Call He Wasn’t Ready For’), which contextualises the clinical, ethical, and social dilemmas faced by physicians and patients under restrictive abortion laws.
Legislation and regulation play a pivotal role in determining whether abortion is accessible, safe, and equitable. Laws establish the parameters for who can provide abortion services, under what conditions, and at which gestational stages. They also set requirements for facility standards, reporting, consent, and financing, making policy frameworks central to the practical delivery of care. However, abortion legislation rarely exists in isolation from the broader socio-political environment. Cultural norms, religious doctrines, economic conditions, and political ideologies profoundly shape how laws are written and interpreted. For example, some countries adopt rights-based frameworks that prioritise autonomy and evidence-based practice, while others impose restrictions reflecting moral or religious beliefs, such as mandatory waiting periods [13,14], parental involvement for minors [15], or outright prohibitions [16]. These policies can either facilitate early, safe access or create barriers that force women and girls into unsafe alternatives. In federal or devolved systems, regional variation can lead to stark geographic inequities, with access determined by postcode rather than need. Understanding these dynamics is essential for identifying how legal frameworks influence health outcomes and perpetuate disparities.
Rationale
Despite the critical role of abortion policy, there has been no comprehensive, systematic analysis of global legislation and regulation spanning diverse regions and contexts. Previous studies have often been limited to single countries or specific regions, failing to capture the full spectrum of legal, operational, and cultural factors that influence access to safe abortion care. A global, systematic approach allows for the identification of patterns, gaps, and innovations across jurisdictions, offering insights into how different policy levers impact population health. This work aims to collate, appraise, and synthesise all available abortion policies in English over the past four decades, providing a unique resource for policymakers, clinicians, researchers, and advocates to highlight knowledge and practice, and identify areas for reform. Importantly, the analysis goes beyond legal texts to consider operational realities, such as provider roles, facility designations, and data systems, offering a holistic view of abortion care governance. In doing so, it contributes to the broader goal of reducing preventable maternal morbidity and mortality while promoting reproductive justice and gender equity.
Methods
This study employed a systematic review methodology to synthesise global evidence on abortion policies published over the past four decades. The review followed PRISMA 2020 guidelines to ensure methodological rigour, transparency, and reproducibility [17]. We aimed to identify, appraise, and synthesise all publicly available English-language abortion policy documents, peer-reviewed articles, reports, and grey literature describing the legal, ethical, structural, and implementation aspects of abortion care. This approach was selected to address the complexity and heterogeneity of abortion policies globally, capturing both legislative frameworks and contextual factors influencing access and practice.
Search Strategy
A comprehensive search strategy was developed in consultation with information specialists and subject matter experts. Databases searched included Google and PubMed supplemented by regional databases such as African Index Medicus (AIM), Latin American and Caribbean Health Sciences Literature (LILACS), and Indian Medlars Centre (IndMed) to capture literature from low- and middle-income countries (LMICs). Searches were conducted for documents published between 1 January 1980 and 31 August 2025, using controlled vocabulary and free-text terms for “abortion,” “termination of pregnancy,” “policy,” “legislation,” “law,” “governance,” and “regulation.” Boolean operators and truncation were applied to maximise sensitivity. To capture grey literature, we searched the World Health Organization (WHO), the United Nations Population Fund (UNFPA), Guttmacher Institute, and national government repositories, and targeted searches of non-governmental organisation (NGO) websites [18]. Reference lists of included studies were hand-searched, and experts were contacted to identify additional relevant sources.
Inclusion and Exclusion Criteria
Eligible documents included any publicly available abortion-related policies, laws, regulations, or national guidelines published in English. Policies were included if they provided detail on legal status, clinical guidance, service delivery models, or financing mechanisms. Studies analysing the implementation or outcomes of abortion policies were also included to capture real-world contextualisation.
Exclusion criteria were non-English publications, duplicate records, documents without explicit policy relevance, and publications limited solely to clinical outcomes without a policy focus. Abstracts, conference proceedings, and opinion pieces without empirical or policy evidence were also excluded.
Screening and Selection
All search results were imported into Covidence for systematic screening. Two reviewers independently screened titles and abstracts against the eligibility criteria, with conflicts resolved by a third reviewer. Full-text screening was then conducted to ensure that included studies met the scope and focus of the review. Inter-rater reliability was calculated using Cohen’s kappa, with a threshold of ≥0.80 considered acceptable for inclusion decisions.
Data Extraction and Quality Assessment
A standardised extraction template was developed and piloted to ensure consistency. Extracted data included: country or region, publication year, type of policy document, legal framework, gestational limits, provider roles, service delivery models, cost or financing arrangements, and evidence of implementation or enforcement. Quality appraisal was conducted using a modified version of the WHO Handbook for Guideline Development, assessing clarity, transparency, applicability, and equity considerations[19]. Studies were rated as high, moderate, or low quality, with sensitivity analyses performed to explore the influence of lower-quality evidence on overall findings.
Thematic and Contextual Analysis
Thematic and contextual analysis was used to synthesise and interpret the extracted data. The analysis was conducted in three interconnected stages. First, a descriptive synthesis summarised the key characteristics of abortion policies across countries and regions. Second, thematic coding identified recurring patterns and concepts, both inductively and deductively. This stage focused on emergent themes such as access restrictions, gestational limits, funding structures, provider roles, and regulatory oversight. Third, contextual mapping integrated the thematic findings with broader political, socio-economic, and health system factors to explore how abortion policies operate within and respond to structural determinants. This approach enabled a deeper understanding of the interplay between laws, health systems, and societal dynamics.
Figure 1 presents the analytical framework applied in this review. Global abortion policies were first collated and summarised through thematic analysis, which identified key categories such as access restrictions, gestational limits, and funding structures. These categories were then integrated into a broader contextual analysis to explore how policies interact with health systems, governance arrangements, and societal determinants. This staged approach enabled the synthesis of complex legal and regulatory data into a structured understanding of how abortion policies influence access, safety, and equity.
The synthesis of findings was presented narratively and through comparative tables and figures, illustrating trends over time and differences across regions. Attention was paid to intersectional dimensions, including how income level, geographic location, and migration pathways shape the real-world accessibility and impact of abortion policies. This systematic and iterative process ensured that the review provided both a comprehensive mapping of global policies and a nuanced interpretation of their implications for reproductive health and equity.
To ensure the reliability and validity of the thematic and contextual analysis, rigorous coding procedures were established. The codebook was piloted by a reviewer using a stratified sample of policy documents representing a range of contexts, including liberal, hybrid, and restrictive settings. During this pilot phase, the reviewer worked collaboratively with the study team to refine definitions and ensure that codes were both comprehensive and precise. Discrepancies were discussed and resolved through consensus, with iterative adjustments made to improve clarity and usability of the codebook. This process allowed the team to align on a shared understanding of each code’s operational definition, scope, and application.
At the document level, metadata were systematically captured to provide contextual information for each policy analysed. This included details such as the country or region, year of publication, type of instrument (e.g., act, regulation, policy), relevant legal citations, the broader health system context, and the funding model underpinning service delivery. Each coded excerpt was linked to a specific legal article, section, or clause to maintain traceability and to allow for direct verification during analysis and peer review. This level of granularity enabled a nuanced comparison of policies across diverse jurisdictions.
A crosswalk was created to map the codes to the five overarching synthesis headings that framed the analysis. Policies related to abortion at a woman’s request were coded using LA1 (Legal Access – abortion on request), PM1 (Policy Measure – general provision of services), PM3 (Policy Measure – eligibility criteria), PM4 (Policy Measure – service availability), and IMP1–IMP3 (Impact Tags – accessibility, quality, and equity implications). Legal grounds for gestational limits were captured using LA2 (Legal Access – risk to life), LA3 (Legal Access – health risk), LA4 (Legal Access – rape or incest), and LA5 (Legal Access – foetal impairment), often in conjunction with OG3 (Operational Guidance – gestational age clarification) and IMP1 (Impact Tag – accessibility implications). Additional requirements for accessing safe abortion care were identified through OG1–OG6 (Operational Guidance – including waiting periods, third-party authorisation, counselling mandates, and procedural steps) together with IMP1–IMP2 (Impact Tags – accessibility and quality implications). Conscientious objection provisions were coded using GOV1 (Governance – provider refusal policies) and GOV2 (Governance – institutional refusal policies), alongside IMP2–IMP3 (Impact Tags – quality and equity implications). Finally, penalties and enforcement mechanisms were captured through GOV4 (Governance – provider penalties) and GOV5 (Governance – patient penalties), combined with IMP1–IMP4 (Impact Tags – accessibility, quality, equity, and system-level implications). This crosswalk ensured alignment between the thematic framework and the final synthesis outputs.
The coding process followed a structured, stepwise approach to maximise consistency and completeness. The full set of codes, their operational definitions, and examples are presented in supplementary Tables 1–5. Each document was first scanned to identify the access window and legal grounds for abortion, with LA1 applied to capture on-request provisions and any of LA2 to LA6 applied to identify specific grounds-based access rules (supplementary Table 1). Next, pathway controls were identified, and OG1 to OG6 were used to capture requirements such as waiting periods, mandatory counselling, or facility designation rules (supplementary Table 2). Provider scope and service delivery arrangements were then coded using PM1 to PM4 (supplementary Table 3), followed by governance, conscientious objection, data reporting, and penalty structures, which were coded with GOV1 to GOV5 (supplementary Table 4). Finally, impact tags (IMP1 to IMP5) were applied to any provisions likely to affect timeliness, equity, stigma, cost, or data visibility (supplementary Table 5). Throughout the process, coders recorded the relevant legal panel for each coded passage to maintain audit integrity and facilitate cross-referencing.
The rationale for this coding illustrates the comprehensive nature of the approach. It allows for each component of the policy to be systematically identified and categorised, providing a robust basis for both thematic and contextual analysis. By linking codes to specific policy levers, determinants, and outcomes, the framework enables a nuanced understanding of how laws and regulations translate into lived experiences of access, safety, and equity. This stepwise, traceable methodology supports the synthesis of findings across diverse jurisdictions and underpins the integrity of the overall review.
Synthesis and Interpretation
Findings were synthesised narratively and through comparative matrices, highlighting regional trends and temporal changes in abortion policy. Intersectional analysis considered income level, region, and migration pathways to explore how structural inequities influence abortion access and care. The final synthesis was reviewed by an international panel of experts for contextual accuracy and relevance.
Results
Following a comprehensive database screening (Supplementary Figure 1), abortion-related policies worldwide were systematically identified, collated, and presented in Table 1 for subsequent analysis. In addition, Supplementary Table 6 presents the abortion policies separately by country.
Thematic Synthesis
Across jurisdictions, abortion policy clusters around a recurrent architecture: on-request access up to a defined gestation; specified legal grounds thereafter; operational gatekeeping approvals, waiting periods, referral rules; provider scope and place-of-care rules; and accountability mechanisms that range from safe-access protections to criminal penalties. Practical access is shaped as much by these operational levers as by the headline legality. Countries with on-request access typically set limits between 10 and 24 weeks, most often 10–14 in continental Europe, 18 in Sweden, 20 in New Zealand, and a clinical standard rather than statute in Canada (Table 1 and Supplementary Table 6 ). Beyond those limits, access is channelled through grounds such as risk to life or health and severe foetal anomaly, sometimes via committees [18].
Gatekeeping features, multi-clinician certification, mandatory counselling certificates, judicial orders for minors, or facility tiering slow care disproportionately affect those with the least resources. Where abortion remains criminalised or near-prohibited (for example, the Holy See, Malta pre-2023, parts of the Gulf, and Poland’s post-2020 narrowing), need is displaced into clandestine routes or across borders, with predictable safety and equity harms [18].
Provider models and financing matter: In South Africa, for example, trained midwives are legally permitted to provide early abortion care under the Choice on Termination of Pregnancy Act [20]. Because these services are also included in the publicly funded health system, women can access care earlier, which reduces complications and minimises financial burden. Where funding is partial or provision is concentrated in a few urban hospitals, nominal legality does not convert into equitable access. Telemedicine for early medical abortion (EMA) has widened reach in several jurisdictions such as Canada, the United Kingdom (UK), Argentina, the Netherlands, Australia, and New Zealand [21,22,23,24,25].
Conscientious objection is widespread. In some countries, such as Argentina and parts of Canada, laws require objecting providers to inform patients and make a timely referral [21,23]. These referral duties help prevent service deserts. By contrast, in places like Italy and several Balkan states, weak enforcement of referral obligations sustains regional inequities, even where abortion laws are generally permissive. In humanitarian settings, failure to operationalise lawful care for sexual assault survivors leaves profound gaps even where international standards apply. These gaps, alongside broader patterns observed across jurisdictions, are captured in Table 2, which summarises the identified themes, sub-themes, determinants, exposures, and aligned regulations.
The same small set of levers determines lived access everywhere: how far on-request extends; how later-term grounds are operationalised; whether approvals and waiting periods are required; who may provide care and where; and whether the state protects or criminalises users and clinicians. Systems that minimise non-evidence-based hurdles, clarify referral duties, fund services, and enable task-sharing and tele-EMA reach more people earlier and more safely; systems that layer authorisations, waiting periods, or criminal penalties systematically delay or deter care.
Contextual Analysis
Policy texts sit within political economies and social contracts. Rights-based welfare states, for example, Sweden, Iceland, and New Zealand, treat abortion as standard healthcare : broad on-request windows, streamlined later-term pathways, funded access, and protection from harassment. The result is predictable services and lower stigma. In hybrid models, for example, Norway, Portugal, ethical concerns around viability prompt structured review later in gestation; these safeguards are compatible with equity if approvals are fast and non-punitive, but they can introduce friction at the margins [18]. Federal or devolved systems, for example, Australia, UK, expose people to postcode lotteries when statutory frameworks and commissioning diverge; safe-access zones, tele-EMA, and nurse-led models reduce harm but cannot fully compensate for uneven supply and data gaps. In parts of Eastern and Central Europe, the law nominally permits early abortion on request yet layers counselling, waiting periods, and committee approvals; this state-controlled style delays care, especially in rural areas, and sustains stigma in clinical practice [18,21,22,23,24,25].
In prohibitionist or near-prohibitionist settings, for example, Poland after 2020, Malta until 2023, the Holy See, criminal law substitutes for regulated care, driving cross-border travel and unsafe practices; human-rights jurisprudence has begun to expose the resulting harms but has not yet normalised access [26,27,28]. Outside routine health systems, humanitarian contexts show the sharpest implementation failures: even where international law or national rules allow care for rape survivors, agencies often do not provide it, leaving survivors without timely options.
Comparative analysis by region
Northern and Western Europe
Iceland operates one of the most liberal regimes globally: abortion on request to 22 weeks, with provision beyond this point for non-viable pregnancies under a rights-based statute that recognises physical, mental, and social health. This breadth, coupled with universal coverage, minimises bureaucratic friction and supports early, safe access [29]. Sweden allows abortion on request to 18 weeks, with later-term access on defined health, foetal anomaly, or severe social grounds; protections reinforced by European human rights jurisprudence ensure that conscientious objection cannot impede care. Integration into universal healthcare sustains high safety and equity [30,31]. Norway offers a hybrid autonomy-oversight model: on request to 12 weeks; a medical committee assesses 12–18 weeks; beyond 18 weeks only under exceptional grounds, with a de facto viability ceiling at 22 weeks. While ethically coherent, committee stages can introduce delay risks at gestational margins [32]. Ireland’s post-2018 settlement remains tightly structured: on request to 12 weeks alongside mandatory counselling and a three-day wait; later-term care is restricted to narrow grounds. This two-tier design preserves lawful access but generates practical barriers and cross-border displacement. Latvia and Lithuania allow on-request abortion to 12 weeks and grounds-based access thereafter (commonly to ~22 weeks), but medicalised oversight, sanctions, and regional bureaucracy slow pathways, particularly for rural users [18].
Southern Europe
Portugal’s model permits on-request abortion to 10 weeks with broader grounds thereafter; in practice, mandatory waits and approvals can compress time for later-term indications [33]. Greece and Montenegro exemplify tiered systems where later-term access is lawful, but committee or multi-clinician processes add operational friction [18]. Malta remains an extreme outlier, historically near-prohibitionist with only a narrow life-risk exception entering statute; criminal law continues to exert a chilling effect despite limited reform [18] . Albania’s law is broader on paper, on a request to 12 weeks and grounds of 22 weeks, but criminal sanctions outside statutory pathways and uneven rural provision dampen realised access. Andorra’s total prohibition forces reliance on cross-border care or unsafe routes, sharply diverging from WHO guidance [18].
Eastern and Central Europe
The Czech Republic combines early on-request access (≤12 weeks) with extended grounds to 24 weeks for anomaly, rape, or maternal health, delivering a relatively broad legal scope within an integrated system [18]. Bulgaria and Belarus allow on-request to 12 weeks and grounds-based to ~20–22 weeks, but late-term committee approvals and designated facility rules create delay points and centre complexity in urban hospitals[18]. Hungary and Slovakia fit the regional pattern of early on-request access coupled with waiting periods and counselling certificates that defer care without clinical gain[18]. Poland’s 2020 removal of foetal anomaly as a ground illustrates legal retrenchment translating into cross-border travel, under-reporting, and heightened inequity, despite residual life and rape exceptions [27].
Nordic–Baltic Contrasts
Denmark integrates abortion into public health with clear, compassionate guidance; inclusion of social circumstances as valid grounds exemplifies a rights-based orientation[18]. Finland similarly embeds socio-economic considerations and extends limits for foetal anomalies, aligning with WHO’s broad health framing, while Estonia evidences greater regional disparity and administrative hurdles[18].
Americas
Canada regulates abortion within the health system rather than criminal law, with no federal gestational limit; real-world access is shaped by provincial capacity, with persistent rural gaps despite public funding. Expansion of nurse- and midwife-led medical abortion mitigates some inequities, but service geography and referral networks still determine timeliness beyond ~23–24 weeks [21]. The United States has fragmented sharply post-Dobbs, producing interstate inequities where legal status, funding rules, and clinic density interact to constrain access for low-income and rural populations [1]. Uruguay and Argentina demonstrate how harm-reduction logics, explicit referral duties, and universal coverage can normalise early medical abortion and reduce complications [18,23].
Oceania
New Zealand’s 2020 reform establishes a coherent national model: on request to 20 weeks; clinician-led later-term decisions; self-referral; mandated data; and ministerial accountability for service availability [34]. The design standardises care, supports equity monitoring, and curbs non-evidence-based hurdles. Australia remains federated and uneven: all states decriminalised, but gestational thresholds, multi-clinician approvals, conscientious objection rules, provider scopes, and safe-access zones vary materially. South Australia permits on request to 22+6 weeks with two-doctor oversight thereafter [35]; Queensland mirrors broad on-request access with strengthened safe-access environments [36]; the ACT and NSW foreground clinic protections but differ on late-term governance. Persistent rural maldistribution and out-of-pocket costs sustain postcode inequities despite tele-EMA expansion [24].
Africa and Humanitarian Settings
South Africa’s statute is unusually equity-attentive among LMICs: on request to 12 weeks; up to 20 weeks on health, anomaly, rape/incest, or socio-economic grounds; and thereafter for serious indications. Provision by trained midwives at ≤12 weeks and designated surgical facilities links lawful scope to deliverable capacity. Implementation challenges relate to facility readiness, stigma, and supply reliability, but the legal architecture remains a regional benchmark [20]. Elsewhere, contradictory or restrictive regimes (for example, in parts of East and Central Africa) impede lawful pathways and sustain unsafe abortion; humanitarian responses frequently fail to operationalise lawful care for rape survivors, leaving rights unrealised in practice [18].
Asia–Pacific and Gulf
In Indonesia and selected Gulf states, legal access hinges on layered approvals, documentation, and residency rules that compress clinical timelines against statutory gestational ceilings; these provisions disproportionately exclude migrants and survivors of sexual violence [18]. The United Arab Emirates’ framework typifies committee-centred eligibility with residency and police documentation requirements, embedding public-order and liability concerns into clinical pathways and shaping patient flows in a migration-dense system [18].
Abortion at a Woman’s Request
Where on-request windows are broader and unencumbered by non-clinical hurdles, presentation shifts earlier, and equity improves. Iceland (≤22 weeks) and Sweden (≤18 weeks exemplify this relationship within universal systems, while Ireland’s ≤12-week cap plus mandated wait demonstrates how short windows and process mandates create attrition and cross-border displacement [18]. Australia’s state variation shows how identical legality decriminalisation can yield divergent lived access without harmonised thresholds and referral rules [37].
Legal Grounds for Gestational Limit
Beyond on-request windows, most countries rely on health, including mental health, foetal anomaly, rape/incest, or socio-economic grounds. Norway’s committee stage (12–18 weeks) makes viability and proportionality explicit [18]; South Africa’s inclusion of socio-economic grounds directly targets structural inequality [20]; Czech and Portuguese frameworks add anomaly-based extensions with formal review. The practical determinant is not only the list of grounds, but the speed and clarity of approvals [18,33].
Additional Requirements for Accessing Safe Abortion Care
Waiting periods, counselling certificates, multi-clinician signatures, judicial bypass for minors, and designated-facility rules commonly delay care without clinical benefit. Ireland’s three-day wait and Eastern/Central European counselling-plus-approval combinations illustrate how cumulative frictions push people against legal limits [18] ; Australia’s inter-state variation and rural facility tiering replicate delay mechanisms through geography [36,37,38].
Conscientious Objection
Conscientious objection is common. In countries where the law requires providers who object to abortion to disclose their objection and make a timely referral, such as in parts of Canada and Argentina, service gaps are reduced. By contrast, in countries where referral duties are weak and objection rates are high, such as Italy and some Balkan states, access becomes uneven and geographically patchy, even though abortion laws are otherwise permissive [18].
Penalties
Criminal penalties for providers and, in some places, for those seeking care exert a chilling effect even when limited legal grounds exist. This drives over-compliance by clinicians, delays by patients, and increased unsafe abortion and cross-border travel, as seen in Poland and historically in Malta [27,28]. In humanitarian settings, failure to implementing lawful care effectively functions as structural violence.
Regional Patterns with Operational Consequences
Rights-based Nordic and New Zealand models show that broad on-request access, minimal non-clinical hurdles, standardised national data, and explicit protection of care environments translate into predictable, timely pathways [18,39]. Hybrid European systems balance autonomy with later-term oversight but must streamline approvals to avoid deadline-driven harms. Post-Soviet and parts of Southern/Eastern Europe illustrate how medicalised bureaucracy and waiting periods undermine statutory access and perpetuate stigma [18]. In federated systems such as Australia and the United States, geography and devolved regulation drive variability; tele-EMA, task-sharing, and safe-access zones partially offset maldistribution but do not substitute for harmonised standards and funding [1,24]. In LMIC and humanitarian contexts, statutory grounds without service readiness yield thin pathways; implementation workforce, supply chains, referral networks, and protection from harassment determine whether legal rights are realised [18].
Discussion
This global synthesis of abortion policies across more than one hundred countries reveals a complex landscape in which legality does not automatically translate into accessibility or equity. While a significant number of countries permit abortion on request during the first trimester, the operational realities of accessing safe care are shaped by additional requirements, geographic maldistribution of services, and cultural or political barriers[18]. Countries such as Iceland, Sweden, and New Zealand demonstrate that broad on-request windows, minimal non-clinical hurdles, and integration into publicly funded health systems support timely and safe care. In contrast, restrictive or grounds-only models—common in parts of Eastern Europe, the Middle East, and Latin America—rely on layers of authorisation, judicial involvement, or documentation that create structural delays and exclude marginalised populations [18,29,30,39]. Federated systems, including the United States and Australia, highlight the risk of geographic inequity, where identical national legality is fragmented by state or provincial interpretation [1,37]. Notably, criminal penalties for providers and, in some cases, for those seeking abortion continue to exert a chilling effect, pushing demand into clandestine channels and across borders. This variation underscores a fundamental gap between the legal presence of abortion services and the practical ability of individuals to obtain them safely, equitably, and without stigma.
Population Science: Implications for Global Health
From a population science perspective, the findings reveal how abortion policies act as determinants of maternal morbidity and mortality. Liberal frameworks with early on-demand access and decentralised provision, such as those in Sweden, Iceland, Uruguay, and parts of Canada, are associated with lower rates of unsafe abortion, earlier gestational presentation, and reduced clinical complications [40]. These models also support continuity of care through telemedicine and task-sharing with midwives or nurse practitioners, enabling equitable service delivery across urban and rural populations. Conversely, restrictive regimes where abortion is limited to life-saving circumstances or narrow legal grounds create predictable patterns of harm. Data from regions with near-total prohibitions, such as parts of Sub-Saharan Africa and the Middle East, show higher prevalence of unsafe abortion and delayed clinical presentation, contributing to preventable maternal deaths and long-term sequelae, including infertility and chronic pelvic pain [18]. These inequities are further compounded by social determinants of health such as poverty, migration status, and gender-based violence. For example, migrants in the Gulf states face exclusion due to residency or documentation requirements, while adolescents in Eastern Europe and Latin America experience delayed access due to parental consent or judicial bypass rules[18]. Thus, abortion policy functions as a measurable structural determinant of reproductive health outcomes and, when implemented effectively, can reduce disparities across and within populations.
Clinical Implications
The operationalisation of abortion policy has direct implications for clinical care pathways. Policies that facilitate early access to medical abortion through telemedicine, pharmacy provision, and primary care integration not only improve patient experience but also reduce health system costs and complications. Countries that authorise task-sharing, such as South Africa and parts of Australia, expand the provider base and mitigate the workforce bottlenecks that commonly delay care in rural or under-resourced settings. In contrast, models requiring multiple clinician signatures or committee approvals concentrate services in tertiary centres and drive inequitable access. Waiting periods, mandatory counselling certificates, and facility tiering requirements are not evidence-based and introduce unnecessary barriers that push individuals towards later gestational care, where clinical risks are higher. Moreover, the failure to enforce referral duties in contexts of conscientious objection—legally permitted in most countries—creates localised service deserts in several Southern and Eastern European states, undermining statutory legality. This reinforces the need for policies that are clinically informed, flexible, and supportive of provider capacity. Data integration across health systems is equally important: countries like New Zealand that mandate service reporting and monitoring can identify gaps and tailor resources, while settings without reliable data remain unable to plan effectively or respond to inequities.
Ethical and Cultural Implications
Abortion policy is deeply embedded in ethical, cultural, and religious contexts, influencing both the framing of law and its practical implementation [3,4,5]. In some jurisdictions, such as Iceland and New Zealand, policies reflect a rights-based framework that emphasises bodily autonomy and gender equality, aligning with international human rights standards [29,39]. These systems also include explicit measures to protect patients and providers from harassment, such as safe-access zones around clinics. Conversely, in countries where religious doctrine shapes policy, such as Malta, Poland, and the Holy See, abortion is restricted to the narrowest of circumstances or prohibited entirely [26–28). Such restrictions elevate moral considerations above clinical and public health evidence, resulting in systemic inequities and preventable harm. Even within liberal frameworks, conscientious objection remains a contested ethical issue. When managed with enforceable referral duties, objections can balance provider beliefs with patient rights [41,42]. However, when unmanaged or widespread, it creates substantial barriers to care and reinforces stigma. Culturally, abortion policies intersect with gender norms, migration dynamics, and socioeconomic status [3,4,5]. For instance, migrant women in the Gulf face layered exclusions through residency rules and documentation requirements, while adolescents are frequently subjected to paternalistic controls through mandatory parental or judicial involvement [18]. Recognising these cultural dynamics is essential for designing interventions that are respectful yet effective.
Towards Better Policy: Evidence-Informed Reform
Improving abortion policies globally requires a shift from purely legalistic frameworks towards evidence-informed models that integrate both quantitative and qualitative insights. Current policies often emerge from political negotiation rather than clinical need, resulting in fragmented and inconsistent care. A more effective approach would include five key strategies, which are summarised in Table 3.
Conclusions
This analysis highlights the urgent need for abortion policy reform that is grounded in empirical evidence and responsive to real-world contexts. Liberal laws without implementation mechanisms remain theoretical, while restrictive laws perpetuate cycles of harm. By combining quantitative population data with qualitative insights from communities, clinicians, and policymakers, countries can design policies that are equitable, operationally viable, and ethically sound. The global disparities observed here underscore that abortion is not merely a clinical service but a societal indicator of gender equality, human rights, and health system integrity. Optimising policy frameworks through evidence and inclusivity offers the clearest path to reducing maternal mortality, improving reproductive health outcomes, and ensuring that legal rights translate into lived realities.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
Not funded
Conflicts of interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care, or the Academic institutions.
Availability of data and material
The data shared within this manuscript is publicly available.
Code availability
Not applicable.
Author contributions
GD developed the ELEMI program and conceptualised this paper as part of the KATHERINE project. GD conducted the analysis. GD, MH and NW wrote the first draft. All authors critically appraised, reviewed, and commented on all manuscript versions. All authors read and approved the final manuscript.
Ethics approval
Not applicable.
Consent to participate
No participants were involved in this paper.
Consent for publication
All authors consented to publish this manuscript.
Acknowledgements
Not applicable.
References
- Haddadi M, Hedayati F, Hantoushzadeh S. Parallel paths: abortion access restrictions in the USA and Iran. Contracept Reprod Med [Internet]. 2025 July 25 [cited 2025 Sept 4];10(1):44. Available from: https://doi.org/10.1186/s40834-025-00382-3. [CrossRef]
- World Health Organization. www.who.int. 2022. Abortion care guideline. Available from: https://www.who.int/publications/i/item/9789240039483.
- Jerman J, Frohwirth L, Kavanaugh ML, Blades N. Barriers to Abortion Care and Their Consequences For Patients Traveling for Services: Qualitative Findings from Two States. Perspect Sex Reprod Health [Internet]. 2017 [cited 2025 Apr 30];49(2):95–102. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1363/psrh.12024. [CrossRef]
- Haddadi M, Sahebi L, Hedayati F, Shah IH, Parsaei M, Shariat M, et al. Induced abortion in Iran, Tehran University of Medical Sciences, the law and the diverging attitude of medical and health science students. PLOS ONE [Internet]. 2025 Mar 25 [cited 2025 Apr 22];20(3):e0320302. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0320302. [CrossRef]
- Aramesh K. Population, abortion, contraception, and the relation between biopolitics, bioethics, and biolaw in Iran. Dev World Bioeth. 2024 June;24(2):129–34. [CrossRef]
- Bearak J, Popinchalk A, Ganatra B, Moller AB, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: Estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020;8(9):e1152–61. [CrossRef]
- Figo [Internet]. 2022. New WHO guidelines on abortion – a landmark tool to prevent unsafe abortion | Figo. Available from: https://www.figo.org/news/new-who-guidelines-abortion-landmark-tool-prevent-unsafe-abortion.
- Major B, Beckman L, Dutton M, Russo N, West C. Mental Health and Abortion APA Task Force on Mental Health and Abortion Mark Appelbaum, PhD [Internet]. 2008. Available from: https://www.apa.org/pi/women/programs/abortion/mental-health.pdf.
- Termination Of Pregnancy Act, No. 43 [Internet]. Ministry of Health; 2019. Available from: https://www.government.is/library/04-Legislation/Termination%20of%20Pregnancy%20Act%20No%2043%202019.pdf.
- Abortion Services Aotearoa New Zealand: Annual Report 2022 [Internet]. Ministry of Health; 2022. Available from: https://www.health.govt.nz/system/files/2022-10/abortion-services-aotearoa-new-zealand-annual-report-2022-oct22.pdf.
- Pasieka A. The Politics of Morality. The Church, the State, and Reproductive Rights in Postsocialist Poland. By Joanna Mishtal. J Church State. 2018;60(1):139–41. [CrossRef]
- Ruibal A. Movement and counter-movement: a history of abortion law reform and the backlash in Colombia 2006–2014. Reprod Health Matters. 2014;22(44):42–51. [CrossRef]
- Joyce T, Henshaw S, Dennis A, Finer L, Blanchard K. The Impact of State Mandatory Counseling and Waiting Period Laws on Abortion: A Literature Review The Impact of State Mandatory Counseling And Waiting Period Laws on Abortion: A Literature Review [Internet]. 2009. Available from: https://www.guttmacher.org/sites/default/files/pdfs/pubs/MandatoryCounseling.pdf.
- The Legalization of Abortion: Law 194 of the Italian Republic, 1978 [Internet]. 1978. Available from: https://www.columbia.edu/itc/history/degrazia/courseworks/legge_194.pdf.
- White K, Narasimhan S, A. Hartwig S, Carroll E, McBrayer A, Hubbard S, et al. Parental Involvement Policies for Minors Seeking Abortion in the Southeast and Quality of Care. Sex Res Soc Policy. 2021;19. [CrossRef]
- Amnesty International [Internet]. 2015 [cited 2025 Jan 1]. El Salvador’s total abortion ban sentences children and families to trauma and poverty. Available from: https://www.amnesty.org/en/latest/press-release/2015/11/el-salvador-s-total-abortion-ban-sentences-children-and-families-to-trauma-and-poverty.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. 2021 Mar 29 [cited 2025 Apr 16];372:n71. Available from: https://www.bmj.com/content/372/bmj.n71. [CrossRef]
- GAPD - The Global Abortion Policies Database - The Global Abortion Policies Database is designed to strengthen global efforts to eliminate unsafe abortion [Internet]. [cited 2025 Sept 16]. Available from: https://abortion-policies.srhr.org/.
- WHO handbook for guideline development, 2nd Edition [Internet]. [cited 2025 Sept 12]. Available from: https://www.who.int/publications/i/item/9789241548960.
- Choice on Termination of Pregnancy Act 1996 [Internet]. [cited 2025 Sept 16]. Available from: https://www.saflii.org/za/legis/consol_act/cotopa1996325/.
- Renner RM, Ennis M, Kyeremeh A, Norman WV, Dunn S, Pymar H, et al. Telemedicine for First-Trimester Medical Abortion in Canada: Results of a 2019 Survey. Telemed J E-Health Off J Am Telemed Assoc. 2023 May;29(5):686–95. [CrossRef]
- Parsons JA, Romanis EC. 2020 developments in the provision of early medical abortion by telemedicine in the UK. Health Policy Amst Neth [Internet]. 2021 Jan [cited 2025 Sept 16];125(1):17–21. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8847102/. [CrossRef]
- Keefe-Oates B, Tejada CG, Zurbriggen R, Grosso B, Gerdts C. Abortion beyond 13 weeks in Argentina: healthcare seeking experiences during self-managed abortion accompanied by the Socorristas en Red. Reprod Health [Internet]. 2022 Aug 26 [cited 2025 Sept 16];19:185. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9419329/. [CrossRef]
- Australian Journal of General Practice [Internet]. [cited 2025 Sept 16]. Early medical abortion provision via telehealth in Victoria. Available from: https://www1.racgp.org.au/ajgp/2024/november/early-medical-abortion-provision-via-telehealth-in.
- Telemedicine for medical abortion: a systematic review - Endler - 2019 - BJOG: An International Journal of Obstetrics & Gynaecology - Wiley Online Library [Internet]. [cited 2025 Sept 16]. Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.15684. [CrossRef]
- Clarification on procured abortion [Internet]. [cited 2025 Sept 16]. Available from: https://www.vatican.va/roman_curia/congregations/cfaith/documents/rc_con_cfaith_doc_20090711_aborto-procurato_en.html.
- Impact of restrictive abortion law in Poland | 21-10-2024 | News | European Parliament [Internet]. 2024 [cited 2025 Sept 16]. Available from: https://www.europarl.europa.eu/news/en/agenda/briefing/2024-10-21/10/impact-of-restrictive-abortion-law-in-poland.
- Commissioner for Human Rights [Internet]. [cited 2025 Sept 16]. Need to reform abortion law in Malta - Commissioner for Human Rights - www.coe.int. Available from: https://www.coe.int/pl/web/commissioner/country-work/malta/-/asset_publisher/TZP8peUL0wDD/content/need-to-reform-abortion-law.
- Iceland’s parliament passes landmark abortion law | EPF [Internet]. [cited 2025 Sept 16]. Available from: https://www.epfweb.org/node/425.
- Sweden - Shhh [Internet]. [cited 2025 Sept 16]. Available from: https://shhh-stories.com/sweden.
- Kapelańska-Pręgowska J. The Scales of the European Court of Human Rights: Abortion Restriction in Poland, the European Consensus, and the State’s Margin of Appreciation. Health Hum Rights [Internet]. 2021 Dec [cited 2025 Sept 16];23(2):213. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8694290/.
- Lov om abort (abortloven) - Lovdata [Internet]. [cited 2025 Sept 16]. Available from: https://lovdata.no/dokument/NL/lov/2024-12-20-96?q=abortloven.
- Stifani BM, Vilar D, Vicente L. “Referendum on Sunday, working group on Monday”: A success story of implementing abortion services after legalization in Portugal. Int J Gynecol Obstet [Internet]. 2018 [cited 2025 Sept 16];143(S4):31–7. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/ijgo.12675. [CrossRef]
- T B, H P. Reconsidering post 20-week abortion in Aotearoa New Zealand. Aust N Z J Obstet Gynaecol [Internet]. 2023 Oct [cited 2025 Sept 16];63(5). Available from: https://pubmed.ncbi.nlm.nih.gov/37872722/.
- Information on Abortion in South Australia - SHINE SA [Internet]. [cited 2025 Sept 16]. Available from: https://shinesa.org.au/health-information/pregnancy/information-on-abortion-in-south-australia/.
- Queensland; c=AU; o=The S of. Termination of pregnancy | Pregnancy and family planning [Internet]. corporateName=The State of Queensland; jurisdiction=Queensland; [cited 2025 Sept 16]. Available from: https://www.qld.gov.au/health/children/pregnancy/termination-of-pregnancy.
- Abortion Law in Australia [Internet]. MSI Australia. [cited 2025 Sept 16]. Available from: https://www.msiaustralia.org.au/abortion-law-in-australia/.
- Information on Abortion in South Australia - SHINE SA [Internet]. [cited 2025 Sept 16]. Available from: https://shinesa.org.au/health-information/pregnancy/information-on-abortion-in-south-australia/.
- Abortion legislation | Ministry of Health NZ [Internet]. 2025 [cited 2025 Sept 16]. Available from: https://www.health.govt.nz/regulation-legislation/abortion/abortion-legislation.
- Recker F, Kagan KO, Maul H. Advancing knowledge and public health: a scientific exploration of abortion safety. Arch Gynecol Obstet [Internet]. 2025 [cited 2025 Sept 12];312(3):643–51. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374908/. [CrossRef]
- Giubilini A, Schuklenk U, Minerva F, Savulescu J. Defusing Arguments in Favour of Conscientious Objection. In: Rethinking Conscientious Objection in Health Care [Internet] [Internet]. Oxford University Press; 2025 [cited 2025 Sept 16]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK612562/.
- On conscientious objection to abortion: Questioning mandatory referral as compromise in the international human rights framework - Zoe L Tongue, 2022 [Internet]. [cited 2025 Sept 16]. Available from: https://journals.sagepub.com/doi/10.1177/09685332221119503. [CrossRef]
Figure 1.
Analytical Framework of Global Abortion Policies.
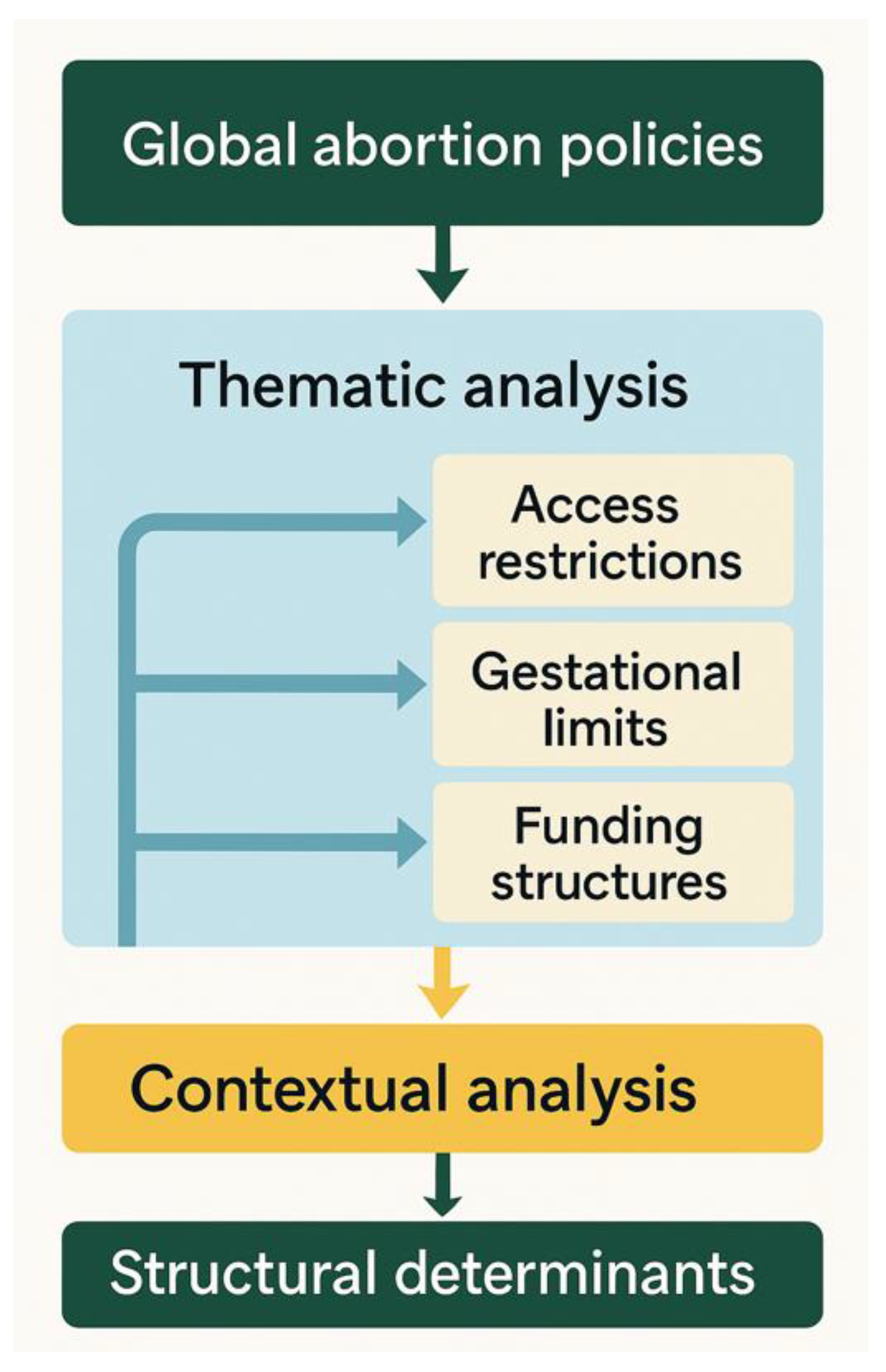

Table 2.
shows the identified themes, sub-themes, determinants, exposures, and aligned regulations/legislations.
Table 2.
shows the identified themes, sub-themes, determinants, exposures, and aligned regulations/legislations.
| Theme | Sub-themes | Exposures (policy levers) | Determinants | Aligned regulations/legislation | Impact |
| Legal architecture | On-request access | Typical limits 10–24 weeks (10–14 EU; 18 Sweden; 20 New Zealand; clinical standard in Canada) | Rights framing; welfare state capacity | Sweden Abortion Law 1975/2009; New Zealand Abortion Legislation Act 2020; Canada Health Act/jurisprudence | Timely early access; lower unsafe abortion; residual inequities where rural supply is thin Results Results |
| Legal architecture | Grounds-based later access | Grounds include risk to life/health, severe foetal anomaly, rape/incest; often committee-reviewed | Ethical/viability considerations; political compromise | Norway Abortion Act/Regs (amended 2021–22); Portugal Termination of Pregnancy Act 2007 | Safer later-term pathways but delays near limits from approvals Results Results |
| Gatekeeping | Third-party authorisation | Two-doctor signatures; counselling certificates; judicial orders; board approvals | Administrative culture; medico-legal risk | Germany, Slovakia, and Bulgaria commission models | Time costs, missed windows, disproportionate burden on low-income and rural users Results Results |
| Provider model | Task-sharing and scope | Midwife/nurse provision for early care; designated facilities for later procedures | Workforce distribution; rural access | South Africa Choice on TOP Act (midwife provision); Queensland/NSW reforms | Expanded throughput and reach; maintained surgical governance for complexity Results Results |
| Safe environments | Safe-access/safe-areas | 150 m protected zones; restrictions on harassment, filming | Stigma; clinic protests | New Zealand Safe Areas; NSW Public Health Amendment (Safe Access) 2018 | Reduced intimidation; improved dignity and service uptake Results Results |
| Access friction | Waiting periods | 2–7-day mandatory delays | Moralised policy tools; political bargaining | Portugal, Germany, Slovakia, Uruguay | No clinical benefit; higher logistical and financial burden Results |
| Adolescents | Parental/judicial involvement | Parental consent/notification; judicial bypass | Child protection norms; confidentiality risks | Multiple European and Latin American statutes | Delayed care; privacy risks; later-term presentations Results |
| Financing & delivery | Public funding, integration, tele-EMA | Universal coverage; mainstream hospital/primary care provision; telemedicine | Health system strength; digital readiness | Western/Northern Europe, Canada, Uruguay, UK/Argentina/Australia/NZ tele-EMA | Earlier access, fewer complications; digital access in remote areas Results |
| Criminal law | Criminalisation and penalties | Sanctions on women, providers, and assistants | Religious/political dominance; colonial legacies | Poland Constitutional Tribunal 2020; Malta Criminal Code 2023; Holy See Canon Law | Chilling effect; cross-border travel; unsafe abortion Results Results |
| Migration & status | Residency/ID controls | Residency duration; committee approvals; documentation (e.g., police reports) | Migration governance; public-order framing | UAE Cabinet Resolution 44/2024; Indonesia PP No. 28/2024 | Exclusion/delay for migrants and survivors; compressed timelines against gestational caps Results |
Table 3.
Framework for Improving Abortion Policy Quality and Evidence Integration.
| Domain | Current Challenge | Proposed Improvement | Evidence Source |
| Legal structure | Inconsistent gestational limits and grounds | Standardise to WHO-aligned thresholds and explicit definitions of grounds | Quantitative cross-country data |
| Access pathways | Waiting periods, committee approvals, geographic bottlenecks | Streamline processes, decentralise care via telemedicine, and task-sharing | Mixed-methods implementation studies |
| Data and accountability | Lack of reliable reporting and outcome tracking | Mandate national-level data collection and integrate it into health system planning. | Health systems research and audits |
| Ethics and rights | Unmanaged conscientious objection, patient harassment | Enforce referral duties and establish safe-access zones | Qualitative stakeholder interviews, legal reviews |
| Cultural adaptation | Policies are misaligned with the local context. | Co-produce policies with communities to ensure acceptability and feasibility | Participatory research and community engagement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



