
Submitted:
10 September 2025
Posted:
11 September 2025
You are already at the latest version
Abstract
Therapist responsiveness is a crucial factor in the effectiveness of psychotherapy, yet its role in group settings remains underexplored. This scoping review examines therapist responsiveness within group psychotherapy, highlighting its theoretical underpinnings, empirical findings, and implications for practice. A scoping review was conducted in major academic databases (PubMed, ProQuest, APA PsycArticles, ScienceDirect, and PMC). A total of 11 articles were identified, and relevant experimental studies were reviewed. Findings indicate that therapist responsiveness plays a central role in fostering group climate, personalizing treatment and promoting reflexivity and mentalization within the group. However, challenges exist in defining and measuring the construct, particularly across different therapeutic models and cultural contexts. While current research suggests a strong link between therapist responsiveness and treatment efficacy, methodological limitations such as small sample sizes and a lack of standardized assessment tools remain barriers to generalizability. Future research should focus on developing validated measures, exploring cultural variations, and assessing therapist responsiveness in online group therapy settings. This study underscores the importance of a responsive therapeutic stance in group psychotherapy and calls for further empirical investigation to refine theoretical models and enhance clinical applications.
Keywords:
responsiveness
; group therapy
; psychotherapist
; group dynamics
; scoping review
1. Introduction
Responsiveness in psychotherapy refers to the therapist's ability to attend to and respond promptly to the specific needs of the patient. Bacal (2025) [1] introduced the term 'optimal responsiveness', meaning the ability of therapists to adapt all their behaviors to the uniqueness of the therapeutic relationship, transcending the theoretical reference model. Stiles et al. (1998) [2] added that the response must be 'appropriate' in the sense that it must support the patient's needs in the context of their life. This implies a commitment to always doing the 'right thing' at the 'right time', pursuing therapeutic goals and taking into account the specific history of the relationship, including the resources and limitations of the context (Hayes et al., 1998) [3]. Responsiveness can thus be seen as a pervasive feature of the therapeutic relationship (Kramer and Stiles, 2015) [4] and an important contributor to treatment effectiveness (Zuroff et al. 2010; Baldwin et al., 2007) [5,6]. Recent literature has further explored the multifaceted nature of therapist responsiveness, emphasizing its overlap with constructs such as attunement, flexibility, and empathy. Although responsiveness may be similar to other therapist characteristics, such as active listening and emotional closeness, as highlighted by Rogers (1993) [7], it can be defined as an umbrella term encompassing several dimensions activated simultaneously. These include the ability to understand the patient's needs arising in the present moment of the therapy and respond promptly. This overlap presents challenges in the clear operationalization and assessment of responsiveness, yet it underscores its critical role in effective therapeutic outcomes (Esposito et al. 2024) [8]. Recently, scientific debate has expanded the construct of responsiveness beyond individual therapy, examining its role in group psychotherapy (Kramer et al., 2025) [9], both in relation to the treatment of specific patients (Culina, 2025; Pellens et al., 2025) [10,11] and in relation to assessment tools (Esposito et al., 2024; Spagnuolo Lobb et al., 2024; Cozzolino et al, (2024); Snyder and Silberschatz, 2017) [8,12,13,14]. According to Watson and Wiseman (2021) [15], research should explore therapist responsiveness in training and supervision, organisational/institutional and cross-cultural settings (Hahn et al., 2022; Moertl, et al., 2017; Friedlander, 2012; Mihai and Butiu, 2012) [16,17,18,19]. The development of therapist responsiveness has been linked to training processes that enhance technical skills, supervision, and coursework. Studies suggest that these educational components are instrumental in fostering a therapist's ability to adapt interventions to the unique needs of clients, thereby improving therapeutic outcomes (Friedlander, 2012 [18]; Orlinsky and Rønnestad, 2005) [20]. Research in group psychotherapy has grown significantly in recent years. Today, group psychotherapy is a widely used and effective tool for adults and adolescents with different specific psychopathologies (Craig et al., 2021; Sharma et al., 2017; Lo Coco et al., 2015) [21,22,23]. In group settings, where interpersonal interactions and shared experiences drive the therapeutic process, therapist responsiveness plays a fundamental role in managing group dynamics, mitigating conflict, and ensuring that all members feel heard, validated, and engaged. However, empirical research on therapist responsiveness within group psychotherapy remains limited. Groups are conducted with different theoretical models, such as group-analytic (Vlastelica, (2011) [24], cognitive-behavioural (Cuijpers et al., 2008 [25] and systemic (Blow et al., 2017 [26]. In general, responsiveness within groups may be similar to other constructs such as therapeutic alliance (Lo Coco, et al., 2012), cohesion and climate (Rosendahl et al., 2021; Shechtman & Kiezel, 2016; van Andel at al., 2003) [27,28,29,30] and dynamics between group members (Rosenthal, 1992) [31]. Research has also highlighted the importance of therapist responsiveness in group settings, noting that adaptive interventions by the therapist can facilitate client reflexivity and the assimilation of problematic experiences. This process is crucial for clients dealing with issues such as social phobia, as it promotes deeper self-understanding and therapeutic progress (Leiman and Stiles, 2001) [32]. Furthermore, research has extensively examined various therapist characteristics that contribute to effective responsiveness (Davì et al., 2024) [33]. The ethics of the therapist are closely linked to their responsiveness, as they relate to their internal personal dimension expressed within a relational context. Ethical conduct establishes trust and safety within the therapeutic environment. Therapists' self-awareness and cultural competence are also vital, especially in transcultural contexts, where understanding diverse cultural backgrounds ensures respectful and effective interventions. The transcultural group provides a particular opportunity to encounter and understand otherness. The need to consider cultural diversity arises when new meanings are co-constructed with patients. Finally, although therapists may feel less comfortable and satisfied with online work than with in-person groups, and may experience difficulties managing avoidance and conflict in online group therapy settings (Gullo et al., 2022) [34], they must adapt to technological mediums while maintaining empathy and engagement. In summary, therapist responsiveness, characterized by ethical behavior, cultural competence, adaptability to various contexts, and the ability to create collaborative environments, is essential for the success of group therapy.
2. The Group Therapist
The role of a group therapist is multifaceted, requiring the integration of various interpersonal, cognitive, and emotional skills to facilitate therapeutic processes within a group setting. Unlike individual therapy, which is characterized by a dyadic relationship, group therapy involves navigating complex interpersonal interactions, fostering group cohesion, and managing diverse emotional responses among members. The primary responsibilities of the group therapist include establishing a safe and supportive environment, guiding discussions, addressing conflicts, and ensuring that all participants feel acknowledged and valued. Drawing upon the foundational work of Foulkes (2018) [35] in group analysis, the group therapist functions not merely as a directive authority but as a conductor, orchestrating communication and interaction rather than dominating discourse. Foulkes emphasized the relational network within the group, in which the therapist acts as a catalyst for shared insights and mutual influence among members. His concept of the group matrix, a shared psychological space that binds members together, highlights the necessity for therapists to remain attuned to both individual and collective processes. This perspective aligns with contemporary research emphasizing the importance of group dynamics, transference, and mirroring processes in therapeutic change (Yalom and Leszcz, 2008) [36]. Ultimately, a skilled group therapist integrates responsiveness, emotional attunement, and an understanding of group dynamics to facilitate both individual transformation and collective healing. According to Yalom and Leszcz, the group setting itself provides unique opportunities for members to receive feedback, observe others, and engage in corrective emotional experiences that promote psychological growth. By facilitating open communication, conflict resolution, and emotional expression within the group, the therapist helps create a supportive community that nurtures both individual and collective change. These therapeutic mechanisms, alongside the therapist’s ability to navigate group dynamics and validate each participant, contribute to group therapy's efficacy in promoting change (Burlingame et al., 2011; Burlingame et al. 2003) [37,38].
A group therapist embodies a set of key characteristics that are crucial for creating a safe, effective, and supportive therapeutic environment. These characteristics allow the therapist to navigate the complexities of group dynamics, manage diverse personalities, and guide individuals toward personal growth within a specific setting.
The most studied characteristics of the group therapist include:
- Empathy: a fundamental trait for any therapist, empathy enables the group therapist to deeply understand and resonate with the emotional experiences of group members. This emotional attunement fosters trust and openness, enhancing the therapeutic alliance within the group (Bohart and Tallman, 2010) [39].
- Active Listening: a skilled therapist engages in active listening, attending to both verbal and non-verbal cues. This skill is essential for ensuring that each member feels understood and for recognizing underlying emotions and unspoken needs, which are crucial for effective interventions (Burlingame et al., 2003) [38].
- Emotional Regulation and Attunement: emotional attunement refers to the therapist’s ability to recognize and appropriately respond to the emotional states of clients. This includes managing one’s own emotions and being sensitive to the emotional atmosphere of the group. Effective emotional regulation allows the therapist to maintain balance and guide the group through challenging moments, helping prevent emotional overwhelm or regression (Yalom and Leszcz, 2008) [36].
- Cultural Sensitivity: in increasingly diverse therapeutic settings, cultural competence is essential. A group therapist must be aware of cultural differences in emotional expression, communication styles, and group dynamics. This sensitivity ensures that all members feel respected and understood, and it helps prevent misinterpretations or conflicts arising from cultural misunderstandings (Sue et al., 2009) [40].
- Flexibility and Adaptability: group therapy involves ever-evolving dynamics, and the therapist must be able to adjust their approach to suit the needs of the group. This adaptability is key in managing shifting group energies, addressing conflict, and responding to different levels of engagement from participants (Yalom and Leszcz, 2008) [36].
- Strong Therapeutic Alliance Skills: the therapist must build and maintain a strong therapeutic alliance with each group member, creating trust, respect, and mutual collaboration. Research has shown that a solid alliance is linked to positive therapy outcomes, as it creates a foundation for vulnerability, feedback, and personal growth (Burlingame et al., 2018, Bohart and Tallman, 2010) [38,39].
- Group Process Knowledge: a profound understanding of group dynamics is critical for effective facilitation. This knowledge allows for the successful resolution of conflicts, the promotion of healthy interactions, and the cultivation of a shared therapeutic purpose (Foulkes, 1948; Holmes and Kivlighan, 2000) [35,41].
- Ethical and Professional Integrity: ethical conduct is essential in maintaining the safety and well-being of group members. A group therapist must be transparent, set clear boundaries, and maintain confidentiality. They also need to possess a strong sense of ethical responsibility, guiding the group with professionalism and accountability (Bacal, 2025) [1].
- Leadership and Facilitation Skills: while the group therapist is not meant to dominate the group, they must take on a leadership role in guiding the group process. This involves structuring sessions, encouraging participation, managing conflicts, and ensuring that the group remains focused on its therapeutic objectives (Yalom and Leszcz, 2008; Tschuschke and Dies, 1994 [36,42].
- Self-Reflection and Ongoing Growth: an effective group therapist is committed to continuous self-reflection and professional development. Examining personal biases, emotional reactions, and their influence on the group process is essential for maintaining a high standard of practice. This commitment to self-awareness and growth allows the therapist to remain open to feedback and refine their therapeutic approach (Christensen et al., 2021) [43].
In summary, the role of a group therapist extends beyond traditional clinical expertise, requiring a combination of interpersonal sensitivity, emotional intelligence, and an in-depth understanding of group dynamics. Integrating foundational theories from Foulkes (2018) [35] and Yalom and Leszcz, (2008) [36] with contemporary research, an effective therapist fosters a therapeutic space that supports both individual and collective growth.
A crucial aspect of this role is therapist responsiveness, which involves adapting interventions based on the group's evolving needs, emotions, and interactions. Responsive therapists are attuned to shifts in group dynamics, modifying their approach to address conflicts, and facilitate meaningful exchanges. This adaptability has been shown to be a key predictor of therapeutic success, as it allows therapists to optimize interventions in real time and ensure that each participant feels seen and supported (Burlingame et al., 2011) [37]. By embodying key characteristics such as cultural sensitivity, emotional attunement, and ethical integrity, the therapist ensures the efficacy of group therapy in promoting psychological resilience and healing. Ultimately, the therapist's ability to facilitate open communication and support emotional expression plays a vital role in the transformative potential of group therapy.
3. Rationale and Aim
The experiences of psychotherapists have always been of interest in psychotherapy research, particularly in recent years. However, there are still no studies in the literature that examine the therapist's responsiveness within psychotherapy groups. This could be crucial, given the effectiveness of group treatment, particularly with certain patients. The present research has focused on the figure of the therapist, exploring its different characteristics (Alby et al., 2022, Sánchez-Bahíllo et al., 2014) [44,45], such as its ethics (Brabender, 2006; Bacal, 2025) [1,46], its perception (Bryde et al., 2020), [47] its role (Cella et al., 2016) [48] in different contexts, such as online (Brusadelli et al., 2021) [49] and transcultural (Carballeira Carrera et al., 2022; Grau et al., 2020; Sue et al., 2009) [40,50,51]. The present scoping review aims to explore the responsiveness of the group psychotherapist, excluding other characteristics that are similar to the construct, but not fully assimilated. To this end, a scoping review was conducted to describe the responsive attitude of therapists. This will help us better understand the specific characteristics of responsiveness, how to operationalize and evaluate them, and how to develop them through training and supervision.
4. Methods
4.1. Eligibility Criteria
Inclusion and exclusion criteria are listed below:
Included:
- Experimental research
- Full text scientific articles
- Studies on the relationship between therapist responsiveness and group psychotherapy since 2005 (The previous two decades)
Excluded:
- Reviews, systematic reviews and meta-analyses
- Abstracts
- Book chapters
4.2. Search
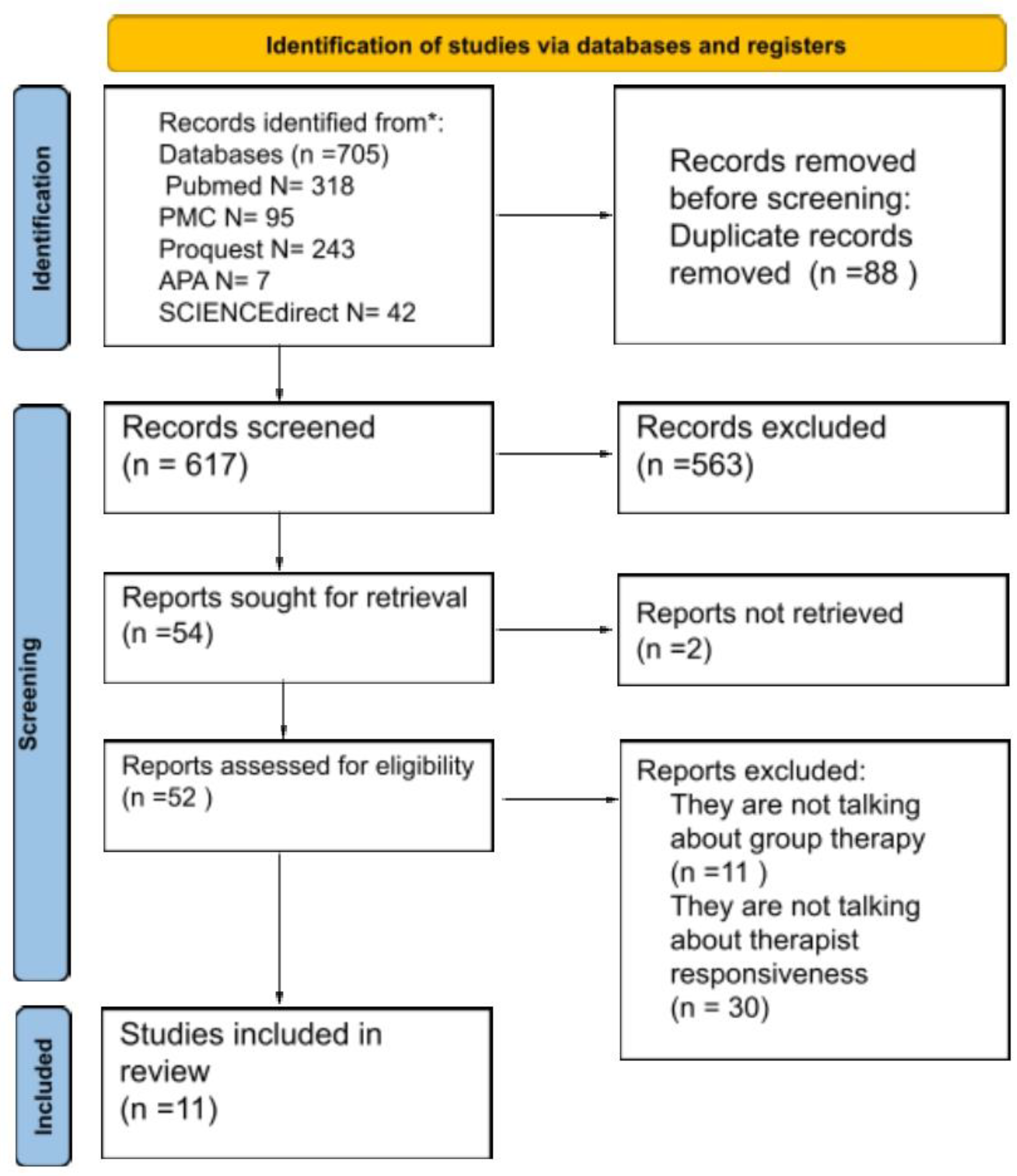
A preliminary search was conducted in Google Scholar to review the existing literature on the topic. A systematic search was then carried out between September and December 2024 using several academic databases, including PubMed, ProQuest, APA Psycarticles, ScienceDirect and PMC.These databases were chosen based on their comprehensive indexing of psychological and psychiatric literature, ensuring broad coverage of empirical studies on therapist responsiveness in psychotherapy. PubMed and PMC provide access to peer-reviewed medical and psychological studies, ProQuest includes dissertations and multidisciplinary research, APA PsycArticles focuses on psychology-specific articles, and ScienceDirect offers access to behavioral science research. The following keywords were used: “therapist responsiveness” AND “group psychotherapy”. These terms were selected to capture studies specifically examining therapist adaptability and its impact on group dynamics. Synonyms and related terms were considered but excluded to maintain specificity. Finally, PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were consulted, though not strictly followed.
4.3. Selection of Sources of Evidence
The study selection process involved title and abstract screening, followed by full-text evaluation, ensuring that included studies met the predefined criteria. This search yielded a total of N = 705 articles, categorised as follows: PubMed N=318, ProQuest N= 243, APA Psycarticles N= 7, Sciencedirect N= 42, PMC N= 95. The period examined begins in 1985, the year in which Bacal developed the construct of therapist responsiveness. Due to the limited number of included studies (n = 11), which were primarily qualitative, and the small sample size (n = 77), it was not possible to rigorously follow up on the synthesis and description of the results with regard to their heterogeneity and statistical characteristics. The scoping review adhered to the PRISMA checklist (available at https://prisma.shinyapps.io/checklist/) for all other items.
Figure 1.
.
5. Results
The reviewed studies describe psychotherapy groups conducted using different approaches: cognitive behavioural (n = 7), psychodynamic (n = 3) and art therapeutic (n = 1). Regarding cognitive behavioural groups, the first study examined is that of Beck and Coffey (2005) [52]. This is a case study of a small group of five women, aged between 33 and 56, who were treated for PTSD caused by a car accident. The group was led by two therapists. The case description portrays the therapists as alert, calm, and honest with patients. Another study, by Chen et al. (2008) [53], reports on two case studies: one involving a group of N=7 men and women (three white, one black, two Asian American and one Latina), aged between 60 and 75, with depression. This group was led by a 30-year-old white female therapist. The second study involved a support group for servicemen diagnosed with PTSD. This group was led by a 40-year-old Latino gay male therapist. Reports indicate that therapists' recognition of their own cultural affiliations facilitates understanding of others' experiences and improves the therapeutic climate. Penttinen et al. (2017) [54] present a case study involving two groups undergoing treatment for social phobia (total number of participants: N = 17). One group was led by a 50-year-old therapist with a PhD, who was also a licensed and experienced psychotherapist. A qualitative analysis of three conversational episodes shows how the therapist's responsiveness facilitated, or did not facilitate, the clients' assimilation process and increasing reflexivity. In Wendt et al.'s (2021) [55] study, female psychotherapists experienced in working with children and adolescents conducted a group with adolescents with Internet Gaming Disorder. The patients' ages at the time of treatment ranged from 12 to 18 years old. The most common comorbid conditions are ADHD and affective disorders. The interviews with therapists demonstrate that awareness of the specific issue (Internet Addiction) is favourable for understanding and treatment. In van Tilburg et al.'s (2022) [56] study, N=18 therapists participated in group psychotherapy sessions for intimate partner violence perpetrators. These sessions were recorded, with the therapists' responsive interventions highlighted. The case study by Grunberg et al. (2022) [57] involved a therapist leading a group of women with postpartum depression and anxiety symptoms in weekly 50-minute sessions. The therapist was particularly 'flexible' (p. 5) and attentive to the participants' experiences. The case study by Grysten et al. (2024) [58] involved five therapists and employed qualitative thematic analysis. The patients' primary psychopathology was depression, and some presented with comorbid diagnoses. Thematic analysis of the interviews revealed several themes related to therapeutic responsiveness, such as focusing on specific problems and developing an in-depth understanding of individual experiences. Regarding the studies describing psychodynamically led groups, the therapists in the article by Joyce et al. (2010) [59] were a 45-year-old psychologist, a 50-year-old psychologist, a 46-year-old sociologist, and a 62-year-old nurse. All of them had considerable experience in group therapy (13, 18, 19 and 25 years, respectively). In their accounts, the therapists came across as people who listened to and supported patients, using their interpretations to foster a more welcoming group climate. Furthermore, the study by Euler et al. (2018) [60] examined three psychodynamically led groups and found that N=23 patients with borderline personality disorder completed the Group Questionnaire (GQ). The mentalization-focused group (Mentalization-Based Group Therapy) was found to foster a strong therapeutic alliance, with leadership that encourages mentalization and a sense of belonging. In a recent study by Arias-Pujol and Anguera (2020) [61], N=6 adolescents aged 13–15 years were observed in relation to their learning and interpersonal skills. The authors used a mixed-methods design based on systematic direct observation, supplemented by indirect observation. The results showed changes in the techniques used from the beginning to the end of therapy, with mentalization interventions being more indicative of therapist effectiveness. Finally, Jaber and Slobodin (2024) [62] most recent research involved N=38 Arab-Israeli drama therapists (36 of whom were women) working in Arab-Israeli schools. Data were collected through semi-structured interviews with N=27 participants and playback theatre groups with N=12 participants. Thematic analysis revealed distinct approaches to attending to the cultural specificity of patients.
The results of all the studies are summarised in Table 1
6. Discussion
6.1. The Here and Now of the Group: An Empathetic Therapist Creates a Welcoming Atmosphere
Responsiveness is an "emergent" characteristic of the therapeutic setting (Davì et al., 2024 [33]; Spagnuolo Lobb et al., 2022; Kramer and Stiles, 2015) [4,33,63] that develops phenomenologically in the here and now. It has a positive and facilitative connotation (Sarnat, 2010; Jenkins and Asen, 65) [64,65]. Within the group, this emergent emotionality is referred to as the group climate. Psychotherapists enhance the group climate by demonstrating empathy and cooperation with other group members (Marshall and Burton, 2010) [66] and by providing positive feedback (Lawson and Brossart, 2009) [67]. The therapists in the reviewed studies generally express responsiveness by maintaining a supportive and accepting climate. For instance, in Joyce et al.'s (2010) [59] study, the therapist fosters an environment where group members can explore conflicts in the present moment. This approach encourages patients to express their feelings while avoiding immediate gratification. This ensures that patients have sufficient time to develop trust in other group members, opening them to dialogue and encouraging problem solving. Additionally, the therapist's empathic attitude encourages patients to get to know other group members, fostering an atmosphere of curiosity and openness. In Beck and Coffey's (2005) [52] study, the therapist is viewed as a coach who acknowledges group members' challenges and encourages them to push themselves further, fostering an environment of trust and optimism. In Grunberg et al.'s (2022) [57] study, mothers are understood in their need for time with their children. The therapist's approach in this study practice is to provide emotional, informational and social support for the complex and personal experiences of new mothers, who often feel isolated. Similarly, in Euler et al.'s (2018) [60] study, the therapist makes the setting an "inclusive place" to strengthen relationships between patients. The therapist interventions described in the studies by Gryesten et al. (2024) [58] and van Tilburg et al. (2022) [56] are characterized by empathy and understanding. These interventions create a relaxed atmosphere in which understanding flourishes. Research interest in therapist empathy in the online setting has recently increased (Sperandeo et al., 2021; Weinberg, 2020) [68,69]. According to Weinberg (2021) [70], responsiveness and the use of self-disclosure could strengthen the therapist's presence in the virtual group and increase their empathic attitude.
6.2. Recognizing the Group Member's Specific Experience: Personalization
The therapist's responsiveness promotes what can be called "personalization" (Davì et al., 2024) [33]. It is the ability to reserve the treatment for the patient with a specific problem under certain circumstances (Paul, 1967) [71]. In a group context, personalizing the intervention means understanding what is useful for the individual group member and implementing specific and different treatment pathways from the other patients in the same group. The group is not a collection of equal individuals, but a meeting of people, each with their own personal history and way of experiencing psychopathology. Paying attention to the needs of the individual member of the group, however, does not mean doing individual psychotherapy in the group (Karterud, 2015) [72]: but adopting an approach that could be definitively "intrasubjective," that is, taking for granted the constitutive intersubjective nature of the person and thus supporting the phenomenology of individual growth through exchange with others. The responsive group therapist provides ongoing feedback on the group member's personal experience in relation to the relationship with the therapist and other group members at a particular time in the group's history and in a particular climate. In this sense, the responsive group leader is attentive, understanding and respectful, and provides a safe foundation for group members (Wang et al., 2022) [73]. In the psychotherapy groups described in the studies reported in this review, the therapist is particularly attentive to the specific needs of the patient. Beck and Coffey (2005) [52] report the case of a psychotherapy group in which the therapist does not simply treat traumatic stress disorder in a generic way, but explores the subjective experience of the individual within the group, paying attention to all those aspects related to the individual's history. In this respect, this study describes a therapist who is careful to capture the subjective nuances of the patient's experience of suffering by providing written feedback on the patient's description of the traumatic experience to ensure that he or she has understood it correctly. In addition, the therapist recognizes the specific moment the patient is experiencing and assesses whether they are ready to take further steps. To explore the experiential dimension in Pettintten et al.'s (2017) [54] study, the Assimilation of Problematic Experiences Scale APES, (Stiles et al., 1991; Stiles, 2001, [74,75] specifically the assimilation of problematic experiences for assessing therapeutic change. A significant finding in the study by Gryesten et al. (2024) [58] related to patients' perceptions of therapists' recognition and individual attention. Patients reported that they appreciated moments when therapists talked to them outside the therapeutic group context. In addition, therapists reflected on the potential therapeutic benefits of additional individual sessions when needed, while acknowledging the therapeutic context of the group; finally, therapists in the study observed in retrospect that such individual attention would be useful for some patients who needed specific treatment for their disorders. The responsive therapist thus explores the nuances of experience and attempts to personalize a standardized intervention such as Cognitive Behavioral Therapy. Finally, in Wendt et al.'s (2021) [55] study, also conducted with a qualitative interview-based methodology, the therapist's experience with the specific disorder being treated (Internet Gaming Disorder) is required for personalized treatment and responsive care. Specific expertise in a type of psychopathology is also an indicator of a therapist's responsiveness. In this study, therapists are required to specialize not only in group psychotherapy, but also in a specific psychopathology (Internet gaming addiction). In order to respond, therapists need to be aware of the characteristics of addiction and online gaming (e.g. what nicknames are used). Recognizing patients' cultural specificities is another dimension of the relationship related to responsiveness (Grau et al., 2020; Sue et al., 2009) [40,51] According to Chen et al. (2008) [53], precisely because cultural minorities have been excluded from much of the group therapy research, it is essential that group therapists today are prepared to adapt treatment to their specific group. The need for multicultural competence is not static, but depends on the specific composition and characteristics of the group. This study defines the group therapist as a 'local clinical scientist' who provides interventions tailored to the cultural affiliation of patients. In this study, although there are differences in patients' individual experiences of suffering, the struggle against racial discrimination is a common experience among patients, and this contributes to the development of therapeutic factors such as universality and cohesion.The group psychotherapist then needs to know, investigate and explore, through ethnographic observation, the cultural affiliation of the patients and the context in which the intervention takes place. For example, in the study by Jaber and Slobodin's (2024) [62], 38 Arab-Israeli drama teachers (36 women) working in Arab-Israeli schools were interviewed. The thematic analysis of the interviews highlighted the importance of negotiating ethnic boundaries in the context of dramatherapy: therapists were challenged to use Western therapeutic approaches based on self-realization, autonomy, freedom and authenticity, in contrast to the values of the more collectivist and hierarchical Arab society (Haj Yahia, 2019) [76]. In this sense, the qualitative interview was also used in this study to learn about the subjective experience of the Arab-Israeli therapist and his vulnerabilities in the context of transcultural work. In online psychotherapy today, recognising the specific cultural dimension is essential. When therapists virtually enter their patients’ home who are often geographically distant, it implies a curiosity to explore the patients' context and inhabit the new virtual setting together.
6.3. Promoting Reflexivity and Mentalization Within the Group
Being a responsive therapist in a group means paying attention to the personalized needs of each group member. This involves developing the ability to reflect on and understand one's own and others' experiences in the group context. The therapist fosters this skill by taking advantage of the relational exchanges that occur within the group. The ability to adopt a self-reflexive stance is considered central to progress in psychotherapy (Rennie, 2010; Levitt et al, 2006) [77,78]. The concept of reflexivity has been used in psychotherapy research as a synonym for concepts such as metacognition, agency, reflexivity, self-monitoring, recursivity and self-awareness (Dimaggio and Lysaker, 2010) [79]. In Rennie's (2004) [80] definition, reflexivity is understood as the formation of intentions within self-awareness as a result of turning one's attention to oneself. It is about paying attention to one's own experiences and interpretations. Several studies have highlighted the potential benefits of promoting reflexivity in organisational (Farnese and Fida, 2014) [81] and educational (Parrello et al., 2021) [82] contexts. In Parrello et al.'s study, the online reflective methodology enhanced the participants' resilience. It encouraged group members to prioritise self-care, positively impacting their performance and ability to innovate. In the case study by Penttinen et al. (2017) [54], therapist responsiveness in a short-term group for social phobic patients is shown to increase patients' reflexivity, which correlates with progress in assimilating their problematic experiences (Stiles, 2001) [75]. Reflexivity, understood as the degree to which members of a group reflect on and communicate the group's goals, strategies, decision-making and communication processes, and adapt them to current or anticipated circumstances, is supported by the leader's responsiveness. What the patient really needs in groups, therefore, is an empathic attitude on the part of the therapist. Within this scenario, the ability to facilitate the mentalization of group members is another characteristic of the responsive therapist. Therapist interventions that promote mentalisation focus on encouraging reflection and understanding of oneself and one's relationships with others. Several studies have demonstrated the usefulness of these processes in the treatment of psychopathology in adults (Fonagy et al., 2019) [83] and adolescents (Griffiths et al., 2019; Brüne et al., 2013. [84,85] Arias-Pujol and Anguera's (2020) [61] study focuses on the role of the therapist as a facilitator of dialogue in an adolescent psychotherapy group. One way of facilitating dialogue is through mentalizing interventions. Mentalization is also a theoretical and operational assumption of psychotherapy groups for borderline patients in Euler et al’s, (2018) [60] study. Findings suggest that therapists' normalization and validation of clients' experiences during the first session are critical in establishing the therapeutic alliance with clients with borderline personality disorder (Culina et al., 2025) [10]. The therapist promotes self-reflection by encouraging patients to think about the questions asked by the group with the goal of increasing self-awareness in the study by van Tilburg et al., (2022) [56].
7. Responsiveness in Group Therapists: Common Dynamics Across Different Models
In the light of the studies reviewed, it is now possible to define more clearly the construct of responsiveness that characterizes the group psychotherapist. First, it seems to share similarities with responsiveness in dyadic settings, such as empathy and presence in the therapeutic here-and-now (Davì et al., 2024) [33]. The personalization offered by a responsive stance in a group context is much more evident and meaningful, as it transforms the intervention into a therapy that attends to subjective experience in plural contexts, which can then be extended conceptually to social and community contexts. The way in which the therapist empowers individuals within group settings, as highlighted in the literature, is by promoting mentalization and reflexivity. In contexts of collective anxiety, such as pandemics, climate crises and international wars, developing awareness of oneself and others can be a crucial resilience factor. Another crucial group dynamic that the therapist responsively addresses is attending to the circulation of patient affect within the therapeutic here-and-now. An empathic, supportive and accepting group climate promotes the development of a group culture focused on solidarity and conflict resolution. The responsive group therapist fosters listening among participants, enabling them to share their personal narratives beyond diagnostic labels, psychopathological diagnosis and treatment paradigms. The theoretical models reviewed - cognitive-behavioural and psychodynamic - despite their clear differences in approach and management of psychopathology, share a common thread: a focus on and curiosity about the experiences of the patients, the therapist and the group as a whole. Experience, understood as an attentive presence in the therapeutic relationship, can be considered a characteristic of a responsive way of doing therapy, regardless of the specific reference model (Davì et al., 2024) [33]. The analysis of the selected studies showed that experience is a characteristic not only of the bipersonal setting but also of group psychotherapy. A responsive attitude on the part of the group therapist is characterized by attentiveness to the subjective and specific experiences of each group member, rather than a one-size-fits-all approach based solely on a given psychopathological framework. This adaptability enables therapists to transcend rigid theoretical models and tailor interventions to the evolving needs of the group. One of the key insights from the reviewed studies is that different therapeutic approaches incorporate responsiveness in distinct ways. Cognitive-behavioral group therapy, for example, has been critiqued for its structured nature, which may limit flexibility in addressing individual needs (Bryde Christensen et al., 2020) [47]. However, emerging evidence suggests that therapists within these models are increasingly personalizing interventions to enhance engagement and therapeutic outcomes. Similarly, psychodynamic and art-based group therapies emphasize the recognition of personal narratives, cultural factors, and identity-related challenges, further reinforcing the therapist’s role in fostering a climate of trust, reflection, and emotional exploration. Specifically, the psychodynamic approach maintains a mainly relational and intersubjective working framework today. Through the study of therapeutic responsiveness, it can explore the emotional dimensions attuned to the patient and use them for the benefit of the group and itself. It takes care of its own experiences through training and supervision. Even more importantly, the study of the therapist's responsiveness in art and expressive therapy groups is valuable because they can identify and develop the creative potential of the group members, creating a new culture based on their shared experiences.
8. Limitations
This conceptual analysis provides valuable insights, but several limitations must be acknowledged. The small sample sizes and the predominance of qualitative studies restrict the generalizability of the findings. To address this issue, future research should employ larger and more diverse samples, as well as adopt quantitative methodologies. Additionally, the lack of standardized assessment tools poses a challenge in comparing results across different studies. Therefore, it is essential for future studies to develop validated instruments tailored specifically to group therapy settings. Another significant limitation is the under exploration of cultural factors, as only a few studies investigate how responsiveness varies among different cultural and linguistic groups. Moreover, the effectiveness of online group therapy settings requires further investigation. The use of virtual platforms may influence therapist responsiveness due to the reduction of non-verbal cues and altered group dynamics. Addressing these limitations in future research will enhance the understanding and applicability of the findings in diverse therapeutic contexts.
9. Conclusions and Future Directions
The findings of this conceptual analysis suggest that therapist responsiveness in group psychotherapy is a dynamic and multidimensional construct that plays a crucial role in facilitating therapeutic change. Furthermore, responsiveness has been shown to promote reflexivity and mentalization, essential components of psychological growth and self-awareness in group settings (Penttinen et al., 2017; Stiles, 2001) [54,75]. By encouraging self-reflection and open dialogue, responsive therapists facilitate deeper interpersonal connections within the group, creating an environment in which participants feel validated and supported. The group climate also plays a fundamental role in responsiveness. Therapists who cultivate a safe, accepting, and attuned atmosphere enable members to engage meaningfully with one another, process difficult emotions, and work through interpersonal conflicts (Grunberg et al., 2022 Joyce et al., 2010 [57,59]. In this sense, responsiveness is not merely a therapist characteristic but an emergent phenomenon shaped by the dynamic interactions within the group. Despite these insights, the limited sample size and predominantly qualitative nature of the studies reviewed represent methodological constraints. Although instruments exist to assess responsiveness at the individual level (Esposito et al., 2024; Spagnuolo Lobb et al., 2024; Cozzolino et al., 2024; Snyder and Silberschatz, 2017) [8,12,13,14] methods and tools to explore the construct in the group setting have not yet been developed. From what has emerged from this study, the dimensions that can be explored are: as far as the therapist is concerned (his or her level of empathy and capacity for mentalization), as far as the group is concerned, it is good to explore its affective climate and how, within the group, a sense of recognition of one's own specific experience and also a sense of acceptance develops. This can be achieved by developing and validating observational or self-report measures of therapist responsiveness within the group, and by proposing specific methodological designs (e.g. micro-process analysis and coding of therapist behavior in video recordings). Exploring cultural background is another important dimension to investigate using interviews, focus groups and other qualitative tools. Further research, particularly large-scale and longitudinal studies, is necessary to refine the construct of responsiveness in group psychotherapy and develop standardized assessment tools for its measurement. In addition, to develop psychotherapists' capacity for mentalization, given its connection to responsiveness, they should participate in Balint groups (Farkas et al. 2024) [86] and training groups for the development of deliberate practice (Diamond et al., 2025) [87]. Participating in supervision groups can help therapists to become more responsive and culturally sensitive (Chong et al., 2025; Ogren et al., 2005). [88,89] These groups can be held online (Weinberg, 2023) [69]. If the groups consist of colleagues from different countries, awareness of different cultures can be promoted. However, it would be beneficial for trainees to include modules on developing personal competencies and responsiveness towards patients. In conclusion, responsiveness in group psychotherapy appears to be a core element of therapeutic efficacy, reflecting the therapist’s ability to navigate the complexities of group dynamics while remaining attuned to the evolving needs of each individual. Compared to other characteristics of the group psychotherapist, responsiveness is a detailed focus on the person within plurality. This seems to be consistent with the need in this cultural context to be recognized as individuals with their own histories and characteristics within a borderless community such as the virtual. Future research should continue exploring how responsiveness interacts with different therapeutic modalities, cultural factors, and technological innovations to enhance treatment effectiveness across diverse populations.
Author Contributions
DD: Conceptualization, Writing—original draft. CP: Conceptualization, Writing—review & editing. NV: Writing—review & editing.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bacal, H. Optimal Responsiveness and the Therapeutic Process. In Discovering Therapeutic Efficacy; Routledge: London, 2025. [Google Scholar] [CrossRef]
- Stiles, W. B.; Honos-Webb, L.; Surko, M. Responsiveness in Psychotherapy. Clinical Psychology: Science and Practice 1998, 5, 439–458. [Google Scholar] [CrossRef]
- Hayes, J. A.; McCracken, J. E.; McClanahan, M. K.; Hill, C. E.; Harp, J. S.; Carozzoni, P. Therapist Perspectives on Countertransference: Qualitative Data in Search of a Theory. Journal of Counseling Psychology 1998, 45, 468–482. [Google Scholar] [CrossRef]
- Kramer, U.; Stiles, W. B. The Responsiveness Problem in Psychotherapy: A Review of Proposed Solutions. Clinical Psychology: Science and Practice 2015, 22, 277–295. [CrossRef]
- Zuroff, D. C.; Kelly, A. C.; Leybman, M. J.; Blatt, S. J.; Wampold, B. E. Between-therapist and Within-therapist Differences in the Quality of the Therapeutic Relationship: Effects on Maladjustment and Self-critical Perfectionism. J Clin Psychol 2010, 66, 681–697. [Google Scholar] [CrossRef]
- Baldwin, S. A.; Wampold, B. E.; Imel, Z. E. Untangling the Alliance-Outcome Correlation: Exploring the Relative Importance of Therapist and Patient Variability in the Alliance. Journal of Consulting and Clinical Psychology 2007, 75, 842–852. [Google Scholar] [CrossRef]
- Rogers, C. R. Un modo di essere: i più recenti pensieri dell’autore su una concezione di vita centrata-sulla-persona, Rist.; Psycho: Firenze, 1993. [Google Scholar]
- Esposito, G.; Cuomo, F.; Di Maro, A.; Passeggia, R. The Assessment of Therapist Responsiveness in Psychotherapy Research: A Systematic Review. RES PSYCHOTHER-PSYCH 2024. [CrossRef]
- Kramer, U.; Boehnke, J. R.; Esposito, G. Therapist Responsiveness in Psychotherapy: Introduction to the Special Section. Psychotherapy Research 2025, 35, 1–3. [Google Scholar] [CrossRef]
- Culina, I.; Ranjbar, S.; Nadel, I.; Kramer, U. Fluctuations in Therapist Responsiveness Facing Clients with Borderline Personality Disorder: Starting Therapy on the Right Foot. Psychotherapy Research 2025, 35, 32–41. [Google Scholar] [CrossRef]
- Pellens, H.; Vanhees, V.; Dezutter, J.; Luyten, P.; Vanhooren, S. Therapist Responsiveness in the Blank Landscape of Depression: A Qualitative Study among Psychotherapists. Psychotherapy Research 2025, 35, 67–83. [Google Scholar] [CrossRef]
- Spagnuolo Lobb, M.; Riggio, F.; Guerrera, C. S.; Sciacca, F.; Di Nuovo, S. The Aesthetic Relational Knowing of the Therapist: Factorial Validation of the ARK-T Scale Adapted for the Therapeutic Situation. Mediterranean Journal of Clinical Psychology 2024, Vol 12, No 2 (2024). [CrossRef]
- Cozzolino, M.; Ruggieri, R. A.; Fioretti, C.; Tessitore, F.; Girelli, L.; Tinella, L.; Borgese, M. N.; Arcangeli, I. C.; Faggi, D. XXIV National Congress Italian Psychological Association Clinical and Dynamic Section, Salerno, 12nd – 15th September 2024. Mediterranean Journal of Clinical Psychology 2024, Vol 12, No 2 Suppl. (2024). [CrossRef]
- Snyder, J.; Silberschatz, G. The Patient’s Experience of Attunement and Responsiveness Scale. Psychotherapy Research 2017, 27, 608–619. [Google Scholar] [CrossRef] [PubMed]
- The Responsive Psychotherapist: Attuning to Clients in the Moment.; Watson, J. C., Wiseman, H., Eds.; American Psychological Association: Washington, 2021. [CrossRef]
- Hahn, A.; Paquin, J. D.; Glean, E.; McQuillan, K.; Hamilton, D. Developing into a Group Therapist: An Empirical Investigation of Expert Group Therapists’ Training Experiences. American Psychologist 2022, 77, 691–709. [Google Scholar] [CrossRef] [PubMed]
- Moertl, K.; Giri, H.; Angus, L.; Constantino, M. J. Corrective Experiences of Psychotherapists in Training. J Clin Psychol 2017, 73, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, M. L. Therapist Responsiveness: Mirrored in Supervisor Responsiveness. The Clinical Supervisor 2012, 31, 103–119. [Google Scholar] [CrossRef]
- Mihai, A.; Butiu, O. The Family in Romania: Cultural and Economic Context and Implications for Treatment. International Review of Psychiatry 2012, 24, 139–143. [Google Scholar] [CrossRef]
- Orlinsky, D. E.; Rønnestad, M. H. ; Collaborative Research Network of the Society for Psychotherapy Research. How Psychotherapists Develop: A Study of Therapeutic Work and Professional Growth.; American Psychological Association: Washington, 2005. [Google Scholar] [CrossRef]
- Craig, S. L.; Eaton, A. D.; Leung, V. W. Y.; Iacono, G.; Pang, N.; Dillon, F.; Austin, A.; Pascoe, R.; Dobinson, C. Efficacy of Affirmative Cognitive Behavioural Group Therapy for Sexual and Gender Minority Adolescents and Young Adults in Community Settings in Ontario, Canada. BMC Psychol 2021, 9, 94. [Google Scholar] [CrossRef]
- Sharma, P.; Mehta, M.; Sagar, R. Efficacy of Transdiagnostic Cognitive-Behavioral Group Therapy for Anxiety Disorders and Headache in Adolescents. Journal of Anxiety Disorders 2017, 46, 78–84. [Google Scholar] [CrossRef]
- Coco, G. L.; Gullo, S.; Prestano, C.; Burlingame, G. M. Current Issues on Group Psychotherapy Research: An Overview. In Psychotherapy Research; Gelo, O. C. G., Pritz, A., Rieken, B., Eds.; Springer Vienna: Vienna, 2015. [Google Scholar] [CrossRef]
- Vlastelica, M. Group Analytic Psychotherapy (Im)Possibilities to Research. Mental Illness 2011, 3, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Van Straten, A.; Warmerdam, L. Are Individual and Group Treatments Equally Effective in the Treatment of Depression in Adults?: A Meta-Analysis. Eur. J. Psychiat. 2008, 22 (1). [CrossRef]
- Blow, A. J.; Karam, E. A. The Therapist’s Role in Effective Marriage and Family Therapy Practice: The Case for Evidence Based Therapists. Adm Policy Ment Health 2017, 44, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Lo Coco, G.; Gullo, S.; Kivlighan, D. M. Examining Patients’ and Other Group Members’ Agreement about Their Alliance to the Group as a Whole and Changes in Patient Symptoms Using Response Surface Analysis. Journal of Counseling Psychology 2012, 59, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, J.; Alldredge, C. T.; Burlingame, G. M.; Strauss, B. Recent Developments in Group Psychotherapy Research. APT 2021, 74, 52–59. [Google Scholar] [CrossRef]
- Shechtman, Z.; Kiezel, A. Why Do People Prefer Individual Therapy Over Group Therapy? International Journal of Group Psychotherapy 2016, 66, 571–591. [Google Scholar] [CrossRef]
- Van Andel, P.; Erdman, R. A. M.; Karsdorp, P. A.; Appels, A.; Trijsburg, R. W. Group Cohesion and Working Alliance: Prediction of Treatment Outcome in Cardiac Patients Receiving Cognitive Behavioral Group Psychotherapy. Psychother Psychosom 2003, 72, 141–149. [Google Scholar] [CrossRef]
- Rosenthal, L. The New Member: “Infanticide” in Group Psychotherapy. International Journal of Group Psychotherapy 1992, 42, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Leiman, M.; Stiles, W. B. Dialogical Sequence Analysis and the Zone of Proximal Development as Conceptual Enhancements to the Assimilation Model: The Case of Jan Revisited. Psychotherapy Research 2001, 11, 311–330. [Google Scholar] [CrossRef]
- Davì, D.; Prestano, C.; Vegni, N. Exploring Therapeutic Responsiveness: A Comparative Textual Analysis across Different Models. Front. Psychol. 2024, 15, 1412220. [Google Scholar] [CrossRef]
- Gullo, S.; Lo Coco, G.; Leszcz, M.; Marmarosh, C. L.; Miles, J. R.; Shechtman, Z.; Weber, R.; Tasca, G. A. Therapists’ Perceptions of Online Group Therapeutic Relationships during the COVID-19 Pandemic: A Survey-Based Study. Group Dynamics: Theory, Research, and Practice 2022, 26, 103–118. [CrossRef]
- Foulkes, S. H. Introduction to Group-Analytic Psychotherapy: Studies in the Social Integration of Individuals and Groups, 1st ed.; Routledge, 2018. [CrossRef]
- Yalom, I. D.; Leszcz, M. The Theory and Practice of Group Psychotherapy; Basic Books: New York, 2008. [Google Scholar]
- Burlingame, G. M.; McClendon, D. T.; Alonso, J. Cohesion in Group Therapy. Psychotherapy 2011, 48, 34–42. [Google Scholar] [CrossRef]
- Burlingame, G. M.; Fuhriman, A.; Mosier, J. The Differential Effectiveness of Group Psychotherapy: A Meta-Analytic Perspective. Group Dynamics: Theory, Research, and Practice 2003, 7, 3–12. [CrossRef]
- Bohart, A. C.; Tallman, K. Psychotherapy. In The heart and soul of change: Delivering what works in therapy, 2nd ed.; Duncan, B. L., Miller, S. D., Wampold, B. E., Hubble, M. A., Eds.; American Psychological Association: Washington, 2010. [Google Scholar] [CrossRef]
- Sue, S.; Zane, N.; Nagayama Hall, G. C.; Berger, L. K. The Case for Cultural Competency in Psychotherapeutic Interventions. Annu. Rev. Psychol. 2009, 60, 525–548. [Google Scholar] [CrossRef]
- Holmes, S. E.; Kivlighan, D. M. Comparison of Therapeutic Factors in Group and Individual Treatment Processes. Journal of Counseling Psychology 2000, 47, 478–484. [Google Scholar] [CrossRef]
- Tschuschke, V.; Dies, R. R. Intensive Analysis of Therapeutic Factors and Outcome in Long-Term Inpatient Groups. International Journal of Group Psychotherapy 1994, 44, 185–208. [Google Scholar] [CrossRef]
- Bryde Christensen, A.; Wahrén, S.; Reinholt, N.; Poulsen, S.; Hvenegaard, M.; Simonsen, E.; Arnfred, S. “Despite the Differences, We Were All the Same”. Group Cohesion in Diagnosis-Specific and Transdiagnostic CBT Groups for Anxiety and Depression: A Qualitative Study. IJERPH 2021, 18, 5324. [CrossRef]
- Alby, F.; Zucchermaglio, C.; Fatigante, M. Becoming a Psychotherapist: Learning Practices and Identity Construction Across Communities of Practice. Front. Psychol. 2022, 12, 770749. [Google Scholar] [CrossRef]
- (Sánchez-Bahíllo, Á.; Aragón-Alonso, A.; Sánchez-Bahíllo, M.; Birtle, J. Therapist Characteristics That Predict the Outcome of Multipatient Psychotherapy: Systematic Review of Empirical Studies. Journal of Psychiatric Research 2014, 53, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Brabender, V. The Ethical Group Psychotherapist. International Journal of Group Psychotherapy 2006, 56, 395–414. [Google Scholar] [CrossRef]
- Bryde Christensen, A.; Svart, N.; Bokelund, H.; Reinholt, N.; Eskildsen, A.; Poulsen, S.; Hvenegaard, M.; Simonsen, E.; Arnfred, S. Therapists’ Perceptions of Individual Patient Characteristics That May Be Hindering to Group CBT for Anxiety and Depression. Psychiatry 2020, 83, 344–357. [Google Scholar] [CrossRef] [PubMed]
- Cella, M.; Reeder, C.; Wykes, T. Group Cognitive Remediation for Schizophrenia: Exploring the Role of Therapist Support and Metacognition. Psychol Psychother 2016, 89, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Brusadelli, E.; Ferrari, L.; Benetti, M.; Bruzzese, S.; Tonelli, G. M.; Gullo, S. Online Supportive Group as Social Intervention to Face COVID Lockdown. A Qualitative Study on Psychotherapists, Psychology Trainees and Students, and Community People. ResPsy 2021, 23 (3). [CrossRef]
- Carballeira Carrera, L.; Lévesque-Daniel, S.; Moro, M. R.; Mansouri, M.; Lachal, J. Becoming a Transcultural Psychotherapist: Qualitative Study of the Experience of Professionals in Training in a Transcultural Psychotherapy Group. Transcult Psychiatry 2022, 59, 143–153. [Google Scholar] [CrossRef]
- Grau, L.; Carretier, E.; Moro, M.-R.; Revah-Levy, A.; Sibeoni, J.; Lachal, J. A Qualitative Exploration of What Works for Migrant Adolescents in Transcultural Psychotherapy: Perceptions of Adolescents, Their Parents, and Their Therapists. BMC Psychiatry 2020, 20, 564. [Google Scholar] [CrossRef]
- Beck, J. G.; Coffey, S. F. Group Cognitive Behavioral Treatment for PTSD: Treatment of Motor Vehicle Accident Survivors. Cognitive and Behavioral Practice 2005, 12, 267–277. [Google Scholar] [CrossRef]
- Chen, E. C.; Kakkad, D.; Balzano, J. Multicultural Competence and Evidence-based Practice in Group Therapy. J Clin Psychol 2008, 64, 1261–1278. [Google Scholar] [CrossRef]
- Penttinen, H.; Wahlström, J.; Hartikainen, K. Assimilation, Reflexivity, and Therapist Responsiveness in Group Psychotherapy for Social Phobia: A Case Study. Psychotherapy Research 2017, 27, 710–723. [Google Scholar] [CrossRef]
- Wendt, L. M.; Austermann, M. I.; Rumpf, H.-J.; Thomasius, R.; Paschke, K. Requirements of a Group Intervention for Adolescents with Internet Gaming Disorder in a Clinical Setting: A Qualitative Interview Study. IJERPH 2021, 18, 7813. [Google Scholar] [CrossRef]
- Van Tilburg, C. A.; Van Dam, A.; De Wolf-Jacobs, E.; De Ruiter, C.; Smeets, T. Group Cognitive–Behavioral Therapy in a Sample of Dutch Intimate Partner Violence Perpetrators: Development of a Coding Manual for Therapist Interventions. International Journal of Group Psychotherapy 2022, 72, 305–330. [Google Scholar] [CrossRef] [PubMed]
- Grunberg, V. A.; Geller, P. A.; Durham, K.; Bonacquisti, A.; Barkin, J. L. Motherhood and Me (Mom-Me): The Development of an Acceptance-Based Group for Women with Postpartum Mood and Anxiety Symptoms. JCM 2022, 11, 2345. [Google Scholar] [CrossRef]
- Gryesten, J. R.; Poulsen, S.; Moltu, C.; Biering, E. B.; Møller, K.; Arnfred, S. M. Patients’ and Therapists’ Experiences of Standardized Group Cognitive Behavioral Therapy: Needs for a Personalized Approach. Adm Policy Ment Health 2024, 51, 617–633. [Google Scholar] [CrossRef] [PubMed]
- Joyce, A. S.; Ogrodniczuk, J. S.; Piper, W. E.; Sheptycki, A. R. Interpersonal Predictors of Outcome Following Short-term Group Therapy for Complicated Grief: A Replication. Clin Psychology and Psychoth 2010, 17, 122–135. [Google Scholar] [CrossRef]
- Euler, S.; Wrege, J.; Busmann, M.; Lindenmeyer, H. J.; Sollberger, D.; Lang, U. E.; Gaab, J.; Walter, M. Exclusion-Proneness in Borderline Personality Disorder Inpatients Impairs Alliance in Mentalization-Based Group Therapy. Front. Psychol. 2018, 9, 824. [Google Scholar] [CrossRef]
- Arias-Pujol, E.; Anguera, M. T. A Mixed Methods Framework for Psychoanalytic Group Therapy: From Qualitative Records to a Quantitative Approach Using T-Pattern, Lag Sequential, and Polar Coordinate Analyses. Front. Psychol. 2020, 11, 1922. [Google Scholar] [CrossRef]
- Jaber, M.; Slobodin, O. Identity Development of Arab Drama Therapists: The Role of Ethnic Boundary Work. The Arts in Psychotherapy 2024, 91, 102225. [Google Scholar] [CrossRef]
- Spagnuolo Lobb, M.; Sciacca, F.; Iacono Isidoro, S.; Di Nuovo, S. The Therapist’s Intuition and Responsiveness: What Makes the Difference between Expert and in Training Gestalt Psychotherapists. EJIHPE 2022, 12, 1842–1851. [Google Scholar] [CrossRef] [PubMed]
- Sarnat, J. Key Competencies of the Psychodynamic Psychotherapist and How to Teach Them in Supervision. Psychotherapy: Theory, Research, Practice, Training 2010, 47, 20–27. [CrossRef]
- Jenkins, H.; Asen, K. Family Therapy without the Family: A Framework for Systemic Practice. Journal of Family Therapy 1992, 14, 1–14. [Google Scholar] [CrossRef]
- Marshall, W. L.; Burton, D. L. The Importance of Group Processes in Offender Treatment. Aggression and Violent Behavior 2010, 15, 141–149. [Google Scholar] [CrossRef]
- Lawson, D. M.; Brossart, D. F. Attachment, Interpersonal Problems, and Treatment Outcome in Group Therapy for Intimate Partner Violence. Psychology of Men & Masculinity 2009, 10, 288–301. [CrossRef]
- Sperandeo, R.; Cioffi, V.; Mosca, L. L.; Longobardi, T.; Moretto, E.; Alfano, Y. M.; Scandurra, C.; Muzii, B.; Cantone, D.; Guerriera, C.; Architravo, M.; Maldonato, N. M. Exploring the Question: “Does Empathy Work in the Same Way in Online and In-Person Therapeutic Settings? Front. Psychol. 2021, 12, 671790. [Google Scholar] [CrossRef]
- Weinberg, H. Online Training Process Groups for Therapists: A Proposed Model. International Journal of Group Psychotherapy 2023, 73, 141–165. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, H. Obstacles, Challenges, and Benefits of Online Group Psychotherapy. APT 2021, 74, 83–88. [Google Scholar] [CrossRef]
- Paul, G. L. Strategy of Outcome Research in Psychotherapy. Journal of Consulting Psychology 1967, 31, 109–118. [Google Scholar] [CrossRef]
- Karterud, S. Mentalization-Based Group Therapy (MBT-G): A Theoretical, Clinical, and Research Manual; Oxford University Press, 2015. [CrossRef]
- Wang, L.; Wei, M.; Kivlighan, D. M.; Koay, E. Y. Y. Unpacking Leader Responsiveness Effects of Emotional Cultivation Groups: Using the Variance Partitioning Method. Journal of Counseling Psychology 2022, 69, 711–721. [Google Scholar] [CrossRef]
- Stiles, W. B.; Morrison, L. A.; Haw, S. K.; Harper, H.; Shapiro, D. A.; Firth-Cozens, J. Longitudinal Study of Assimilation in Exploratory Psychotherapy. Psychotherapy: Theory, Research, Practice, Training 1991, 28, 195–206. [CrossRef]
- Stiles, W. B. Assimilation of Problematic Experiences. Psychotherapy: Theory, Research, Practice, Training 2001, 38, 462–465. [CrossRef]
- Mental Health and Palestinian Citizens in, Israel; Haj-Yahia, M. M. Mental Health and Palestinian Citizens in Israel; Haj-Yahia, M. M., Nakash, O., Levav, I., Eds.; Indiana University Press, 2019. [CrossRef]
- Rennie, D. L. Humanistic Psychology at York University: Retrospective: Focus on Clients’ Experiencing in Psychotherapy: Emphasis of Radical Reflexivity. The Humanistic Psychologist 2010, 38, 40–56. [Google Scholar] [CrossRef]
- Levitt, H.; Butler, M.; Hill, T. What Clients Find Helpful in Psychotherapy: Developing Principles for Facilitating Moment-to-Moment Change. Journal of Counseling Psychology 2006, 53, 314–324. [Google Scholar] [CrossRef]
- Metacognition and Severe Adult Mental Disorders: From Research to Treatment; Dimaggio, G., Lysaker, P. H., Eds.; Routledge: London New York, 2010. [CrossRef]
- Rennie, D. L. Reflexivity and Personcentered Counseling. Journal of Humanistic Psychology 2004, 44, 182–203. [Google Scholar] [CrossRef]
- Farnese, M. L.; Fida, R. Come La Riflessività Promuove l’apertura Delle Organizzazioni Verso l’innovazione: Il Ruolo Delle Pratiche Di Riflessività e Del Clima Di Gruppo per l’innovazione. RISORSA UOMO 2014, No. 1, 87–102. [Google Scholar] [CrossRef]
- Parrello, S.; Fenizia, E.; Gentile, R.; Iorio, I.; Sartini, C.; Sommantico, M. Supporting Team Reflexivity During the COVID-19 Lockdown: A Qualitative Study of Multi-Vision Groups In-Person and Online. Front. Psychol. 2021, 12, 719403. [Google Scholar] [CrossRef]
- Fonagy, P.; Luyten, P.; Allison, E.; Campbell, C. Mentalizing, Epistemic Trust and the Phenomenology of Psychotherapy. Psychopathology 2019, 52, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, H.; Duffy, F.; Duffy, L.; Brown, S.; Hockaday, H.; Eliasson, E.; Graham, J.; Smith, J.; Thomson, A.; Schwannauer, M. Efficacy of Mentalization-Based Group Therapy for Adolescents: The Results of a Pilot Randomised Controlled Trial. BMC Psychiatry 2019, 19, 167. [Google Scholar] [CrossRef]
- Brüne, M.; Dimaggio, G.; Edel, M.-A. MENTALIZATION-BASED GROUP THERAPY FOR INPATIENTS WITH BORDERLINE PERSONALITY DISORDER: PRELIMINARY FINDINGS.
- Farkas, K.; Csukly, G.; Fonagy, P. Is the Balint Group an Opportunity to Mentalize? Brit J Psychotherapy 2024, 40, 55–75. [Google Scholar] [CrossRef]
- Diamond, G.; Wlodek, B.; Arthey, S.; Parker, S. A Systematic Review of Deliberate Practice in Psychotherapy: Definitions, Operationalization, and Preliminary Outcomes. Psychotherapy 2025, 62, 113–131. [Google Scholar] [CrossRef]
- Chong, E. S. K.; Chen, H.; Chui, H.; Luk, S. Perceived Cultural Humility in Supervision Group and Trainees’ Cultural Responsiveness Self-Efficacy. Psychotherapy 2025, 62, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Ögren, M.-L.; Jonsson, C.-O.; Sundin, E. C. Group Supervision in Psychotherapy: The Relationship between Focus, Group Climate, and Perceived Attained Skill. J. Clin. Psychol. 2005, 61, 373–388. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Group Therapy Responsiveness.
| Study ID | Country | Sample Characteristic | Design | Theoretical Model | Group Characteristic | Identified Elements of Therapist’s Responsiveness | Main Finding |
| Beck and Coffey (2005) | USA | N=2 Therapists N=1 Therapist N= 1 Co-Therapist |
Case Study | Cognitive Behavioural | N=1 Group Participants: N=5 women,(ages 33 to 56) with PTSD caused by a Serious motor vehicle accident (12 sessions) |
Case example: “It is critical that the therapists be alert to an individual feeling”(p.10) “Therapists' role in this treatment is conceptualized as that of a coach—someone who has awareness and appreciation for the individual's current struggles yet encourages them to push the boundary slightly”(p.10) |
Therapists take a personalised approach with each patient in the group, creating a welcoming atmosphere |
| Chen et al. (2008) | USA | N= 2 Therapists N=1 30-year-old white woman N=1 40-year-old, Latino, gay male |
Case Illustrations | Cognitive Behavioural | N=2 Groups Participants: Case 1: N=7 three white, one black, two Asian Americans, and one Latina (ages 60 to 75) with Depression Case 2: N=9 servicemen PTSD (ages 21 to 39) (Among the racial minority members in the group are two blacks and one Arab American |
Cases illustrations: Case 1: “Therapist adopts an active style with the group and introduces cognitive restructuring as a way to explore each member s experience with depression” (p.1262) Case 2: “The group therapist as a local clinical scientist deliberately considers, identifies, and implements culturally appropriate interventions, although they may be at variance from RSTs and practice guidelines” (p.1267) |
Therapist pay attention to the specific culture of the patients and their experiences |
| Joyce et al. (2010) | Canada | N= 4 Therapists N=2 women N= 2 men (ages 45 to 62). |
Comparative trial | Psychodynamic | N=18 Groups Participants: N=135 (ages 22 to 74) short-term groups (STG) for Complicated Grief (weekly 90-minutesessions for 12 weeks) |
Case descriptions: “During the sessions, the therapist attempts to create a climate of tolerable tension and deprivation wherein conflicts can be examined using here and-now experience” (p.125) “Therapist’s interpretations might be delivered with more tentativeness and openness to correction by the patient.” (p.133) |
Therapist creating a welcoming atmosphere |
| Penttinen et al. (2017) | Finland | =1 Therapist 50-year-old, male Ph.D, a licensed and experienced psychotherapist |
Case Study | Cognitive Behavioural | N= 2 Groups for Social Phobia Participants: N=17 Case 1: N=10 Case 2: N= 7 (12 weekly two-hour sessions) |
Qualitative analysis of three conversational episodes with one female patient: 1.”Therapist offered a formulation of her problematic experience which was relevant to the intention of her dominant voice, but did not in any way address the feelings” (p.11) 2. “Responded by listening empathically” (ibidem) 3: “Pointed to the significance of the client’s own construction of her problematic experience” (ibidem) |
Therapist's responsive attitude facilitates the patients' assimilation of their experience |
| Euler, et al. (2018) | Switzerland | N=2 Therapists N=1 senior psychiatrist N=1 advanced clinical psychologist (co-therapist) |
Cyberball Task | Psychodynamic | Mentalization-based groups psychotherapy Participants: N=23 patients with Borderline Personality Disorder N= 28 healthy participants three sessions of 75 min per week in their 2nd week after admission to the unit. |
Case Discussion “Even the exclusion-prone patients appeared to be capable of seeing the therapists not as malevolent” (p.7) “Anactive, responsive and reliable therapeutic stance has been described as a hallmark of all empirically supported therapies for BPD” (ibidem) “This fairly “inclusive”– to some extent perhaps even “over-inclusive”– attitude may partially explain why patients did not feel uncomfortable toward the therapists in our study” (p. 8) |
Patients feel welcome within the group that develops mentalization |
| Arias-Pujol and Anguera,(2020) |
Spain | N=2 Therapists N=1 expert lead therapist N=1 co-therapist |
Mixed methods | Psychodynamic | N=1 Group Participants: N= 6 Adolescents (Ages 13 to 15) with learning and interpersonal relationships (30 sessions) |
Clinical vignette: “The lead therapist (T) plays a very active role, encouraging participation so that the adolescents can get to know each other” (p.5) “The lead therapist (T) wants to know their opinions about the experience” (ibidem) |
Therapists facilitate communication and develop mentalization |
| Wendt, et al. (2021) | Germany | N= 2 Therapists,experts women psychological (child and adolescent) |
Qualitative interview | Cognitive Behavioural | N=1 Group Participants: N=7 Adolescents (ages 12-18) with Internet Gaming Disorder (8 modules of 90 min) |
Interviews with therapist: “In addition to knowledge about gaming addiction, being a group therapist also requires you to keep up to date with computer games. (p.14) “To stick strictly to the module is not possible with this topic anyway. [...] It requires a therapist who is also experienced enough to respond flexibly to the needs [of the patients] at that moment.” (p.16) |
Therapists customise the intervention based on their specialist knowledge of psychopathology |
| Van Tilburg et al (2022) | Netherland | N= 18 Therapists N= 10 women N=8 men with 5-10 years of experience |
Qualitative | Cognitive Behavioural | N= 25 Groups Participants: N=133 Men Intimate Partner Violence Perpetrators (60 sessions) |
Audio recording (therapist’s interventions “ Showing interest, enthusiasm and empathy when participants report positive behavior in the context of the treatment objectives, giving recognition, giving compliments, thanking someone for his input, wishing someone positive things, talking about the group atmosphere, putting someone at ease, social small talk.” (p.317) “Encouraging the participants” (p.314) “Using humor, self-deprecation or laughing about a joke the patient has made.” (p.317) |
Therapists show empathy, understanding and exploration of the specific experience and creates a welcoming atmosphere |
| Grunberget al. 2022) | USA | N= 1 Therapist | Case Illustration | Cognitive Behavioural |
N= 1 Group Participants: N= 3-6 women with Postpartum Mood and Anxiety Symptoms ( weekly 50 min group, 7 sessions) |
Case illustration “Therapists are flexible if women need to step out briefly to manage employment or child-related issues”(p.5) “The facilitator encourages” (p.9) |
Therapist creates a welcoming atmosphere and is flexible with patients |
| Gryesten, et al (2024) | Denmark | N = 5 Therapist Women (ages 33 to 54) with 4-10 years of experience | Hermeneutic-phenomenological thematic analysis | Cognitive Behavioural | N= 3 Group Participants: N=15 N=11 Women N= 4 Men with depression and comorbid diagnoses Routine Outcome Monitoring (ROM) (14 two-hour weekly sessions) |
Interviews with patients: “Five themes were identified: (1) Individual attention (2) Psychological exploration (3) A focus on the patient’s life outside of therapy (4) Extended assessment (5) Agreement on therapeutic task” (p.617) |
Therapists respond to the specific needs of their patients, exploring their unique experiences |
| Jaber and Slobodin, (2024) | Israel | N=38 Psychotherapists N= 36 women N= 2 Men (ages 30-58 years), with 7.42 average years of professional experience N=28 Muslim-Arab N= 6 Druze N= Christian-Arab |
Qualitative | Art therapy | Groups of Art-therapy in schools in the Northern District of Israel for Children and Adolescents | Semi-structured Interviews : “Three themes were identified: (1) Distinguishing Arab identity from drama therapy (2) Drama therapy is perceived as an act of challenging ethnic and gender boundaries (3) Negotiating ethnic boundaries within the context of drama therapy” (p.3) |
Therapists pay specific attention to their own culture, recognising its influence on their practice |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



