
Submitted:
09 September 2025
Posted:
10 September 2025
You are already at the latest version
Abstract
Background: Women in perimenopause, menopause, and post-menopause experience significant biological, psychological, and social changes, including vasomotor symptoms, urogenital atrophy, sleep disturbances, and cognitive shifts. Despite the impact on quality of life, productivity, and social participation, these life stages are underrepresented in national and international health policies compared to reproductive years.Methods: A systematic review following PRISMA guidelines was conducted. English-language national and international policy documents published up to March 2025 were retrieved from PubMed, Science Direct, Google Scholar, WHO, UNFPA, and national health ministry websites. Policies were included if they addressed women’s health during perimenopause, menopause, or post-menopause. Data extraction captured policy focus, target populations, chronic disease management, cancer screening, menopause care, equity considerations, and alignment with global standards. Thematic and conceptual analyses synthesized findings into key domains and gaps.Results: Thirty policies from 13 jurisdictions were reviewed, addressing women’s health across the reproductive life course, including peri-menopause, menopause, and post-menopause. Common priorities included chronic disease management, menopause symptom management, cancer prevention and screening, mental health support, and management of reproductive disorders such as PCOS, endometriosis, and infertility. Equity considerations focused on underserved populations, including rural women, socioeconomically disadvantaged groups, Indigenous and ethnic minorities, and other high-risk populations such as sex workers and adolescents. Conclusion: Policies addressing later reproductive years remain heterogeneous, with inconsistent integration of chronic disease management, cancer screening, and reproductive health care. Strengthening equitable, evidence-based policy frameworks is crucial to support women’s health, reduce disparities, and improve quality of life during perimenopause, menopause, and post-menopause.
Keywords:
perimenopause
; menopause
; post-menopause
; women’s health
; policy
; chronic disease
; PCOS
; endometriosis
; cancer screening
; health equity
Introduction
Through women’s life course, perimenopause, menopause, and the post-menopausal periods are critical transitions for women because most women spend approximately more than 30% of their lives in this stage, especially in elderly ages [1]. Through these years, there are significant biological, psychological, and social changes, including vasomotor symptoms, sleep disturbances, cognitive shifts, and urogenital atrophy [2]. In addition to physical changes for women through these years, there are significant changes in the women’s quality of life, productivity, social participation, and health equity [3]. Regardless of mentioned challenges and issues, international and national health agendas mostly neglect appropriate actions and policies for perimenopause, menopause, and the post-menopausal periods compared to reproductive years such as maternity health [4].
Women’s health can be considered as a foundation of public health, with important implications for population health, economic growth, and social developments [5]. Policies for women’s health are important to addressing and shaping the inequities that challenges affect women throughout their lives [6]. However, appropriate policies for women in their perimenopause, menopause, and the post-menopausal years are poorly integrated into health systems, or inadequately implemented [4]. For example, hormone replacement therapy (HRT) is an appropriate treatment for menopausal women to alleviate many related symptoms such as hot flushes, sleep problems, mood swings, and vaginal dryness, which affecting significantly the women’s quality of life and their social participation [7]. However, in low- and lower-middle-income countries (LMICs), multiple factors such as high costs, absence of supportive policies, and inadequate regulation significantly limit access to this medication for many women who need it [8,9]. Furthermore, although some policies and actions address the medical challenges of these years, psychosocial needs, workplace equity, and cultural contexts are often neglected, limiting access to essential services and exacerbating disparities in health outcomes [10,11].
Rationale
The KATHERINE Project addresses a critical policy blind spot: the needs of young-to-middle-aged women navigating the menopausal transition including premature, early, surgical and medically induced menopause who are often overlooked in frameworks geared to older populations. A systematic evaluation of perimenopause, menopause and post-menopause policies is required to map strengths, expose gaps in prevention, diagnosis, treatment access, workplace protections and social protection, and to identify inequities experienced by women at the intersection of gender, age, race/ethnicity, disability, migration status and socioeconomic position. By interrogating policy content, implementation fidelity and real-world impact against global equity-focused standards, KATHERINE will generate a rigorous, comparative assessment that surfaces where policies fail younger cohorts such as fragmented care pathways, fertility and contraception considerations, mental health, violence and safeguarding, and return-to-work supports. Focusing this paper on young-to-middle-aged groups is therefore strategic: it captures the period of highest role intensity such as employment, caregiving, parenting, when poorly designed policies magnify health and economic harms and widen lifetime inequalities. The project’s ultimate aim is to deliver evidence-based, actionable recommendations that strengthen policy design and implementation so that women experiencing perimenopause through post-menopause particularly in younger and midlife stages can realise their health, rights and participation in society.
Methods and Materials
Study Design
This review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Figure 1). The methodological approach was established in advance to ensure transparency and reproducibility. Although the review was not formally registered, the structure adhered closely to PRISMA requirements, and each stage of the process was prospectively defined.
Search Strategy
A comprehensive search was conducted on MEDLINE/PubMed, Science Direct, and Google scholar until March 30, 2025. The search utilized keywords such as “women’s Health”, “maternal health”, “reproductive health”, and “policy”. Additional studies were identified by national and International Websites such as WHO (World Health Organization), UNFDP (United Nations Financial Disclosure Programme), and the ministry of health of countries.
Study Selection and Data Extraction
Three reviewers screened the collected articles to identify studies that met the following inclusion criteria: (1) Population: women; (2) Intervention: health policy interventions; (3) Comparison: absence of such interventions; (4) Outcome: health policy related outcomes; (5) Setting/Time: all settings and time periods; and (6) Study design: observational, interventional, or qualitative studies. Discrepancies among reviewers were resolved through discussion and consensus. The selection process was documented in detail and summarized in a PRISMA flow diagram (Figure 1) [12]. Studies or policies without an available English version were excluded.
Quality Assessment
Two reviewers independently assessed the quality of the included studies using the AACODS (Authority, Accuracy, Coverage, Objectivity, Date, Significance) checklist, a critical appraisal tool designed specifically for grey literature sources. The overall quality ranged from low to high. Studies scoring ≥25 were considered high quality, those scoring ≥19 but <25 were classified as moderate quality, and those scoring <19 were rated as low quality. Full details of the quality assessment are provided in the Supplementary Data.
Data Analysis
The synthesis followed a dual approach. Thematic and contextual analysis was used to identify recurring patterns in governance, eligibility, inclusivity, financing, and ethical framing. Descriptive statistics were generated to summarise numerical variables such as age limits, Body Mass Index (BMI) thresholds, inclusivity provisions, and financing arrangements across jurisdictions. Comparative matrices were constructed to contrast commonalities and differences between national and subnational contexts, and findings were mapped against underpinning legal instruments. The results were consolidated into a master thematic table that captured themes, sub-themes, indicators, exposures, determinants, intersections, and policy strengths and weaknesses
Results
Overview of Included Policies
A total of thirty national and international policies, strategies, and guidelines published between 1980 and 2025 were reviewed [13,14,15,16,17,18,19,20,21,22]. These policies spanned diverse geographic and socio-economic contexts, including high income countries (HIC) such as Australia, Sweden, the United Kingdom, and Israel, as well as low - middle income countries (LMIC) countries including Ghana, Tanzania, South Africa, Rwanda, India, Nepal, Bhutan, Sudan, Botswana, Mauritius, and Mongolia [15,16,18,19,20,22,23,24]. The policy types encompassed national women’s health strategies, reproductive health policies, cervical cancer and human papilloma virus (HPV) screening guidelines, maternal health frameworks, sexual and reproductive health rights initiatives, and action plans targeting chronic conditions and menopause management. Collectively, these documents reflected a broad spectrum of health priorities, ranging from clinical and preventive care to rights-based and equity-oriented approaches, demonstrating both the influence of international frameworks such as CEDAW, ICPD, and SDGs, and national socio-cultural and political contexts [25,26].
Among these policies, HICs consistently embedded equity, intersectionality, and life-course approaches into health planning. For example, Australia’s National Women’s Health Strategy 2020–2030, the chronic conditions policy brief (2017), and Scotland’s Women’s Health Plan (2021–2024) integrated menopause care, reproductive health, and mental health considerations with attention to marginalized groups, including Indigenous women, rural populations, and migrants. In contrast, low- and middle-income countries often prioritized maternal survival, family planning, and reproductive service accessibility, frequently shaped by donor-supported initiatives, as evident in Ghana’s Free Delivery Care Policy (2007), Tanzania’s Population Policy (2006), and Rwanda’s RMNCAH policy [15]. Across all settings, adolescents and younger women remained inconsistently addressed, with policies tending to focus on reproductive prevention rather than the broader spectrum of sexual, mental, and chronic health needs.
Study Characteristics
The 30 policies represented a wide geographical distribution, including sub-Saharan Africa (Ghana, Tanzania, Rwanda, Botswana, South Africa, Swaziland), South Asia (India, Nepal, Bhutan), Southeast Asia (Myanmar), East Asia (Mongolia), the Middle East (Israel), and high-income settings such as Australia, New Zealand, Sweden, Scotland, Wales, and England [16,17,20,21,22,23,27,28]. The policies varied in scope, with some focused narrowly on reproductive health, family planning, or cancer screening (e.g., Ghana’s National Reproductive Health Service Policy, South Africa’s Cervical Cancer Guidelines), while others adopted a more comprehensive life-course approach integrating chronic disease, menopause, and equity dimensions (e.g., Australia’s National Women’s Health Strategy 2020–2030, NHS Wales Women’s Health Plan 2024 [29]. Policy formats ranged from national strategies and legislative acts to technical guidelines and policy briefs, reflecting diverse approaches to addressing women’s health needs across reproductive, perimenopausal, and postmenopausal stages.

Table 1.
Characteristics of the studies included in the systematic review.
| Study ID | Policy/ articles name | Year | Policy Level | Country/Region | Policy Focused Area | Targeted Population | Policy Status | Objective | Outcomes | Equity Consideration | Global Alignment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ghana's Free Delivery Care Policy [29] | 2003 | National | Ghana | Maternal Health Policy | Women of reproductive age who had recent live births | Implemented | Evaluate the impact of the free delivery policy on utilization and quality of delivery services, delivery outcomes, and the economic consequences for households. | The policy covered the following maternal health services: 1. Normal deliveries Assisted deliveries, including Caesarean sections Management of medical and surgical complications from deliveries, including: Repair of vesico-vaginal fistulae Repair of recto-vaginal fistulae 2. Services were provided across: Public health facilities Private health facilities Faith-based health facilities |
Universal Health Coverage | -Millennium Development Goals |
| 2 | National Women’s Health Strategy 2020–2030 | 2020 | National | Australia | Women’s health across the life course: reproductive, sexual, maternal, mental health, chronic illness, ageing, violence | All Australian women, with emphasis on those most at risk (e.g., rural, socially disadvantaged, Aboriginal and Torres Strait Islander women) | Implemented, Active | To improve women’s health across Australia and reduce inequities | 1. Reproductive health and sexuality 2. Health of ageing women 3. Emotional and mental health 4. Violence against women 5. Occupational health and safety 6. Health needs of carers 7. Health effects of sex role stereotyping |
All women and girls in Australia, with additional focus on priority populations (e.g. Aboriginal and Torres Strait Islander women, rural/remote, low socioeconomic status, those with disability, LBTI communities, women affected by violence or justice system, veterans) | SDG3; SDG5; SDG10 |
| 3 | Israel: Reproduction and Abortion: Law and Policy [27] | 2012 | National | Israel | Funding of Reproductive care; Universal health coverage; equitable access to healthcare services | All Israeli residents | Implemented, Active | To analyse Israel’s specific policies and law on reproductive technologies and abortions and discusses their social, religious, and political context. |
1. Access to essential medical services 2. Prevention and treatment of diseases 3. Maternal and child health (Access to prenatal care, Safe delivery services) 4. Mental health 5. Chronic disease management 6. Prevention of genetic disorders 7. Reproductive autonomy and family planning |
Vulnerable Populations (such as low-income individuals, elderly, those with chronic conditions) | Not mentioned ( Indirectly associated with Universal Health access) |
| 4 | National Population Policy | 2006 | National | Tanzania | "Population and development integration Reproductive health Gender equality Nutrition Environmental conservation Education Research Advocacy and communication (IEC)" |
Entire Tanzanian population, with special focus on women, youth, and vulnerable groups | Revised and Active | To evaluate progress in implementing reproductive health policies and programs after the 1994 ICPD (International Conference on Population and Development). | "Reproductive Health Services Addressed Antenatal Care (ANC) Childbirth care Obstetric emergency care Newborn care Postpartum care Post-abortion care Family planning Prevention and management of STIs and HIV/AIDS Cancer care Childhood illnesses and immunisable diseases Nutrition Prevention and management of fistulae and pregnancy-related morbidities" |
Yes, Adherence to gender equality and equity, children’s rights and rights for other vulnerable groups | National Development Vision 2025 Millennium Development Goals |
| 5 | Reproductive Health Policy Brief | 2019 | National | Australia | Reproductive Health | Australian women | Advisory/Research-informed (not direct implementation, supports National Women’s Health Policy 2010) | Highlight findings from ALSWH (2010–2018) to inform policy on reproductive health | Identified prevalence of PCOS (10%), endometriosis (10%), infertility (18.6%); menopause age data; hysterectomy impact; links to chronic diseases | Recognizes disparities in reproductive health outcomes (e.g., obesity, mental health, fertility problems) | Linked to National Women’s Health Policy 2010; indirectly aligned with global reproductive health frameworks (ICPD, WHO women’s health agenda |
| 6 | National Reproductive Health Service Policy and Standards (3rd Edition) | 2014 | National | Ghana | Reproductive health, maternal and child health, family planning, safe motherhood | Women, children, adolescents, couples, general population | Implemented | aimed at making explicit the direction of reproductive health in the context of universal access to care | Cancer screening Family planing Infertility care unsafe abortion and post-abortion care menopause Gender based violence |
Yes – includes vulnerable groups and promotes access for all | ICPD 1994 and WHO standards on reproductive and maternal health |
| 7 | HPV Screening, Invasive Cervical Cancer and Screening Policy in Australia | 2017 | National | Australia | Cervical cancer screening | Women aged 25–69 eligible for cervical screening | Implemented | To estimate the likely impact of Australia’s new 5-yearly primary HPV screening policy (Renewal Policy) on the incidence of cervical cancer compared with the previous 2-yearly cytology screening policy. | Reduce incidence of oncogenic HPV infections (by 20% by 2030) in women and adolescent girls; decrease age-standardised mortality rate from cervical cancer (to 20% by 2030). Improve quality of life of women with terminal cancer. Reduce incidence of invasive cancer (to 20% by 2030) | Focused on age group 30–69; didn't assess stratified outcomes for First Nations or migrant women | WHO/IARC-aligned in purpose; raises concern re: SDG 3.4 (premature mortality reduction); aligns with UN’s caution on overdiagnosis |
| 8 | National Guidelines for Cervical Cancer Screening Programme | 2012 | National (with separate expectations between Community, PHC, District, Regional, and Tertiary) | South Africa | Cervical Cancer Screening | Women 30 years and older | Implemented | To achieve a screening coverage of 70% among women aged 30 to 50 years by 2010. To offer at least three free Pap smears per woman over her lifetime, |
Reduction of incidence and mortality of cervical cancer (by >60%); Screening at least 70% of target population within 10 years of programme initiation | The programme was meant to be delivered through the primary health care system, making screening available at local clinics rather than centralised urban hospitals. | Millennium Development Goals (MDGs) |
| 9 | Cervical Cancer Prevention and Control Policy(30) | 2017 | National | South Africa | Cervical Cancer Screening; Cervical Cancer Prevention | Low risk asymptomatic women (30-50 years old); Women living with HIV and women with other immunosuppressive conditions; sex workers; adolescents; migrants | Implemented | – Implement a comprehensive prevention and control programme comprising three interlinked strategies: (1) reducing oncogenic HPV infections; (2) detecting and treating cervical precancer; and (3) ensuring timely treatment and palliative care for invasive cancer. | Reduce incidence of oncogenic HPV infections (by 20% by 2030) in women and adolescent girls; decrease age-standardised mortality rate from cervical cancer (to 20% by 2030). Improve quality of life of women with terminal cancer. Reduce incidence of invasive cancer (to 20% by 2030) | Adds HPV vaccination for girls aged 9–12 via strengthened school health services, expanding access to primary prevention. | Explicitly aligns with global frameworks, notably Sustainable Development Goal 3 (universal access to sexual and reproductive health, by 2030), Global Strategy for Women’s, Children’s and Adolescents’ Health, and targets such as universal health coverage and NCD mortality reduction |
| 10 | Sweden’s international policy on Sexual and Reproductive Health and Rights [22] | 2021 | International | Sweden | Safe abortions; maternity care; neonatal care; access to contraceptives; promotion of gender equality; HIV/AIDS and sexually transmitted infections | Women; new-born babies; infants; men | Implemented | o increase access to SRHR interventions, enhance knowledge, shift social norms, and strengthen accountability, with special focus on deprived areas and vulnerable groups, including LGBTQI populations | Reduce maternal mortality rates; reduce infant mortality; prevention of transmission of HIV to new-born babies and infants; reducing spread of HIV and AIDS | Focus on inclusion of women and minorities as subjects in clinical research. Planning, conducting, reporting of analyses for sex/gender and race/ethnicity differences. | - |
| 11 | Women's Health Plan: A plan for 2021-2024 | 2024 | National | Scotland | Women's Health and Gender Equality | Women (see equity considerations) | Implemented | o reduce avoidable health inequalities experienced by women and girls across their lifespans—from puberty through later years—by focusing on areas commonly stigmatized, overlooked, or dismissed as “women’s issues,” including heart health, menopause, menstrual health, endometriosis, contraception, abortion services, and access to information | "• ensure women who need it have access to specialist menopause services for advice and support on the diagnosis and management of menopause; • improve access for women to appropriate support, speedy diagnosis and best treatment for endometriosis; • improve access to information for girls and women on menstrual health and management options; • improve access to abortion and contraception services; • ensure rapid and easily accessible postnatal contraception; • reduce inequalities in health outcomes for women’s general health, including work on cardiac disease." |
Considers gender inequities as a factor influencing SRHRs. Defines sexual rights as meaning all people irrespective of sex, age, ethnicity, disability, gender identity, or sexual orientation have a right to their own body and sexuality. | Yes. bilateral, multilateral, operational, and nomative work that Sweden in different ways carries out in international contexts. |
| 12 | The NHS Wales Women's Health Plan | 2024 | National | Wales | Women's Health and Gender Equality | Women (see equity considerations) | Implemented | To close the gender health gap in Wales by transforming the way healthcare services are designed and delivered for women and those assigned female at birth—ensuring they are listened to, their health needs are understood, and care is equitable across the lifespan | "Menstrual Health (Including: Heavy Menstrual Bleeding (HMB), Endometriosis, Fibroids, Adenomyosis, Polycystic Overy Syndrome (PCOS), Pre-menstual Syndromes (PMS), Pre-menstrual Dysphoric Disorder (PMDD)); Endometriosis and Adenomyosis; Contraception, Post-Natal Contraception and Abortion Care; Preconception Health; Pelvic Health and Incontinence; Menopause; Violence Against Women, Domestic Abuse and Sexual Violence; Aging Well and Long-term Conditions Across the Life Course (Including: Adolescent Health and Wellbeing; Sexual Health, HIV and Blood Borne Viruses; Mental Health and Wellbeing; Alzheimer's and Dementia; Diabetes; Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Cardiovascular Disease; Cancer Recovery; Musculoskeletal Conditions; Palliative and End of Life Care)" |
"Includes transgender men, non-binary people, and intersex people or people with variations in sex characteristics." |
e NHS Wales Women’s Health Plan is globally aligned through its commitment to the SDGs, WHO’s life-course approach, and international frameworks on gender equality and health equity |
| 13 | Women's Health Strategy for England | 2022 | National | England | Improvement of women's health | Women | Implementation | - | "Tackling disparities in access to services and experiences of services and outcomes. Women with additional risk factors or barriars to have equitable access. Menstrual health and gynaecological conditions (heavy menstrual bleeding, premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD), endometriosis, adenomyosis, fibrosis, polycystic ovary syndrome (PCOS) (and also urogynaecological conditions including urinary incontinence, vaginal prolapse, recurrent urinary tract infections), and gynaecological cancers. Fertility, pregnancy, pregnancy loss, and postnatal support (contraception, preconception health, fertility and infertility, pregnancy loss and stillbirth, birth trauma, support for expectant and new mothers and their partners. Personalised care. Menopause. Mental Health and Wellbeing. Cancers (uterus, ovarian, cervical, vulval, vaginal)." |
Includes trans men and non-binary people recorded female at birth. Addresses wider determinants of health (ranging across social, economic, and environmental factors). Notes that black and minority ethnic groups and disabled and lone parent women face especially worse health disparities. Intersectionality and vulnerability is addressed. | Though not explicitly named in the strategy, its focus on equitable access, improved health systems, and rights-based care supports SDG 3 (Good Health & Well-Being) and SDG 5 (Gender Equality). The fiscal framing also resonates with global economic rationale for investing in women’s health |
| 14 | Chronic conditions policy brief | 2019 | National | Australia | Chronic disease conditions of women | Women (ages ranging from 30s to 90s), specifically from Australian Longitudinal Study on Women’s Health (ALSWH) | Implemented | The brief synthesizes key findings from ALSWH data (since around 2010) on chronic conditions among Australian women, aiming to inform and guide the development of national health policies— | Multimorbidity, frailty, mental health, urinary incontinence, injury from falls, obesity, diabetes, stroke, arthritis, cancer, cardiovascular disease | Addressed transgender men and non-binary people with female reproductive organs wrt cancer screening. Addresses disparities experienced by "women from under-served and seldom-heard groups". Considers groups with barriers to health, such as women experiencing: homelessness, refugees, asylum seekers, women in prisons; also: disabled women, lesbian and bisexual women, and black and Asian women. | While primarily national in scope, the brief aligns with international frameworks by recognizing chronic conditions as life-course, non-communicable diseases, advocating evidence-based, equity-focused strategies—paralleling WHO priorities and Sustainable Development Goal 3 on universal health and NCD reduction. |
| 15 | Pregnancy and maternal health policy brief | 2019 | National | Australia | Pregnancy and maternal health | Women in reproductive age | Ongoing | highlight maternal mortality and morbidity trends, underscore gaps in prenatal/postnatal care, and recommend strategic interventions—like improved access to quality services, care continuum strengthening, and workforce capacity building | Gestational diabetes, hypertension, low birth weight, maternal depression and anxiety, childhood obesity, antenatal health behavior | Emphasis typically on reducing disparities—addressing racial/ethnic, socioeconomic, and geographic inequities in maternal outcomes; promoting culturally responsive care, inclusive data collection, and community-based support. | Alignment with SDG 3, especially Target 3.1 (maternal mortality reduction) and 3.8 (universal health coverage); adherence to WHO’s human-rights based, life-course maternal health frameworks; often reflects the reproductive justice approach, which centers intersectional, rights-based access to care |
| 16 | Sexual and health policy brief [28] | 2019 | National | 2017 | Sexual health policy brief | Australian women | Ongoing | To present key research findings on sexually transmitted infections (STIs) and contraceptive use among Australian women, with the goal of informing national health policy and improving sexual health outcomes | STIs (e.g., chlamydia), thrush, contraceptive behavior, reproductive heal | highlights disparities in sexual health outcomes across ages, regions (urban vs rural), socio-economic status, and cultural or identity groups | Aligns implicitly with global health efforts such as the Sustainable Development Goals (SDG 3) related to sexual and reproductive health and the WHO’s STI prevention frameworks |
| 17 | Women’s Health: Best Practices in Sex Education Implemented by Local Governments [20] | 2017 | National | Japan | Sexual and reproductive health education; HIV/AIDS and STD prevention; youth sex education | Students (elementary to high school), school teachers, and education stakeholders | Ongoing | to contribute to the promotion of sex education within educational institutions throughout Japan through the wide sharing of these practices |
Knowledge of STDs, contraception, reproductive health, sexual behaviors, HIV/AIDS prevention | Emphasizes clear policy, long-term implementation, evaluation, and multi-stakeholder collaboration—ensuring culturally and regionally responsive inclusion | WHO health priorities on reproductive health access, STI s |
| 18 | National action plan for endometriosis [31] | 2017 | National | Australia | Endometriosis awareness, early diagnosis, treatment, and support | Public population | Active and Ongoing | improved quality of life for women living with endometriosis and reduced burden of disease for individuals and for the nation | Chronic pelvic pain, infertility, fatigue, mental health impacts, delayed diagnosis | Not mentioned | Aligned with WHO/UNESCO recommendations on Comprehensive Sexuality Education (CSE) |
| 19 | RANZCOG Submission to the National Women’s Health Strategy [21] | 2023 | National | Australia and New Zealand | Women’s health equity, reproductive health, maternal health, gynaecological care | Women and girls | Implemented | aims to evaluate strategies for advancing women’s health by (1) placing wāhine/women+ at the centre of care through addressing knowledge gaps, inequities, and social determinants of health; (2) ensuring integrated, accessible, and fully funded multidisciplinary services spanning community, hospital, and maternity care; (3) strengthening leadership, governance, and data systems to enhance accountability and quality; and (4) developing sustainable workforce planning and support mechanisms | Improved maternal care, abortion access, reproductive choice, chronic disease management, menopause support, culturally safe care | Not mentioned | Australian Health Ministers’ Advisory Council (AHMAC) |
| 20 | Sexual and Reproductive Health Rights under the Reproductive and Child Health Policy – Compromising Women's Dignity [17] |
2010 | National | India | maternal health, child mortality, gender equality and HIV/AIDS | women's and children's | Implemented | To bring women's and children's health to the attention of Parliamentarians, with detailed policy recommendations and actions for MPs. | women in the intervention districts reported an increase in their discussions about family planning with spouses, from 42.3% to 90%; an increase in the use of family planning methods, from 7% to 35%; more women reported being involved in decision-making at home, up from 49% to 71%; more women reported that they felt they had a right to refuse sex if they wished, from 37% to 95%; and more women reported expressing sexual needs to her spouse, from 25.4% to 67.5% | Yes, Inner Spaces Outer Faces Initiative (ISOFI): A Gender and Sexuality Project in Uttar Pradesh |
Yes, achieving the Millennium Development Goals |
| 21 | National Sexual and Reproductive Health and Rights Policy [17] | 2022 | National | Myanmar | Sexual and Reproductive Health |
General population | Implemented | 1. To inform decision makers, development/implementing partners, health providers, and beneficiaries about the policy and ensure that they are supported by the policy in their work and/or lives. 2. To aid in the reform of existing laws, regulations, and definitions that restrict access to essential SRHR information and services, especially among adolescents, youth, and marginalized and vulnerable groups. |
Comprehensive, high-quality health information and services will be provided to all women throughout pregnancy, childbirth, and the postpartum period. All individuals of reproductive age will have equitable access to quality and inclusive FP information, commodities, and services and will have the freedom to decide on the desired number of children and determine the healthy timing and spacing of pregnancies. The highest achievable standard of sexual and reproductive health for all adolescents will be pursued by protecting and fulfilling adolescents’ right to information, quality and inclusive services, in addition to promoting enabling environments and opportunities to develop life skills. All individuals will have their dignity and rights upheld, including their right to health. Gender-sensitive approaches will be mainstreamed throughout all levels of the health system, and individuals affected by GBV will have timely access to quality, comprehensive sexual and reproductive health services. All women, men, and young people will have access to information, prevention, early diagnosis, and care for reproductivze health morbidities. |
Assuring gender equality in health through gender-sensitive approaches to be mainstreamed throughout all levels of the health system, and individuals affected by gender-based violence will have ready access to quality, comprehensive sexual and reproductive health services | 1. Beijing Platform for Action 2. Every Woman, Every Child 3. Family Planning 2020 & 2030 4. Millennium Development Goals 5. Sustainable Development Goals (SDGs) 6. International Conference on Population and Development (ICPD) Programme of Action 7. Convention on the Elimination of All Forms of Discrimination against Women 8. Convention on the Rights of the Child |
| 22 | National Reproductive Health Policy [18] | 2010 | National | Sudan | reproductive health | General population | Implemented | To assure quality reproductive and sexual health care that women survive pregnancy and childbirth and enjoy a good family life; adolescent and young children have optimal physical and sexual development; the sexually transmitted infections/HIV, reproductive tract infections, cervical cancer and other RH morbidities, including fistula, are combated; traditional practices harmful for reproductive and sexual health are prevented; and family planning services are made available | Provision of post-abortion care, antenatal care including PMTCT, skilled assistance during childbirth, essential obstetric care, postnatal care, and appropriate management of fistula cases. Provision of “continuum of care” model by addressing the three delays: delay in decision-making to seek medical care during obstetric emergencies; delay in transporting woman to an appropriate referral hospital; and delay in receiving adequate care at the hospital. Provision of neonatal care with special emphasis on improving the antitetanus coverage to both mothers and the neonates. Services regarding reproductive choices and birth spacing methods provided free of charge. General practitioners and specialist physicians shall provide the whole range of family planning services. At primary health care level, health visitors and medical assistants shall provide family planning information and services for child spacing and welfare of women. In remote villages and nomadic settings, village midwives and community health workers shall act as change agent and in addition to providing hormonal contraceptives and condoms, refer clients to health facilities. The induction of abortion, except under medical advice, is pronounced illegal by this policy. Emphasizes promoting adolescent reproductive and sexual health, including combating sexually transmitted infections, and reproductive tract infections. Measures shall be taken for ensuring early diagnosis of cervical cancer and that other RH morbidities including complications of unsafe abortion and vesico-vaginal fistula are combated. Pre-marital care for the health and life of the family and future generations; this shall be incorporated within the provided services. Premarital counseling, to include counseling on nutrition, HIV testing, genetically transmitted diseases, harmful behaviors and misconceptions regarding sexual and reproductive health/ Traditional practices that are harmful for reproductive and sexual health particularly female genital mutilation, early marriage, and GBVs are prevented. Procedures like cloning and semen donation are prohibited and not allowed under law; therefore are not supported by this policy. |
Yes, unity and empowerment in accessing and availing reproductive health care is seen in the policy in the context of social determinants of health. |
Yes , o achieving MDG 5, thus contributing to the Millennium Declaration for Achieving MDGs, particularly 3, 4, 5 and 6 |
| 23 | NatioNal Medical StaNdard For reproductive HealtH [20] | 2020 | National | Nepal | reproductive HealtH | General population | Implemented | to provide policymakers, health officers, hospital directors or health facility in-charges, clinical supervisors and service providers of all level of governments in federal context with accessible, clinically-oriented information to guide the provision of reproductive health services in Nepal |
Information: right to accurate, appropriate, understandable, and unambiguous information related to reproductive health and sexuality, and to overall health. Information and materials for clients need to be available in all parts of the healthcare facility. Access to services: right to services that are affordable, are available at convenient times and places, are fully accessible with no physical barriers, and have no inappropriate eligibility requirements or social barriers, including discrimination based on sex, gender, age, marital status, fertility, nationality or ethnicity, social class, religion, or sexual orientation. Informed choice: right to make a voluntary, well-considered decision that is based on options, comprehensible information, and understanding. The informed choice process is a continuum that begins in the community, where people get information even before they come to a facility for services. It is the service provider’s responsibility either to confirm that a client has made an informed choice or to help the client reach an informed choice. Safe services: Clients have a right to safe services, which require skilled providers, attention to infection prevention, and appropriate and effective medical practices. Safe services also mean proper use of service-delivery guidelines, quality assurance mechanisms within the facility, counselling and instructions for clients, and recognition and management of complications related to medical and surgical procedures. Privacy and confidentiality: Clients have a right to privacy and confidentiality during the delivery of services. This includes privacy and confidentiality during counselling, physical examinations, and clinical procedures, as well as in the staff’s handling of clients’ medical records and other personal information. Dignity, comfort, and expression of opinion: right to be treated with respect and consideration. Service providers need to ensure that clients are as comfortable as possible during the procedures. Clients should be encouraged to express their views freely, even when their views differ from those of service providers. Continuity of care: right to continuity of services, supplies, referrals, and follow-up necessary to maintaining their health. |
Yes, attention to equity for ELEMENTS Of Care | International Reference Texts/Materials e.g. FP Global Handbook 2018, Medical Eligibility Criteria, 2015 (WHO) Scientific Research/Evidence |
| 24 | Reproductive, Maternal, Newborn Child and Adolescent + Health of Ageing(RMNCAH+A) Strategy | 2025 | National | Bhutan | RMNCAH+ Healthy ageing strategy | women, children, and adolescents | implemented | provide strategic guidance to the national and district level managers to implement the life course approach and continuum of evidence-based interventions along the life course in achieving the human capital to its fullest potential | There are four strategic outcomes that are inter-related and mutually reinforcing and contribute to 13th FYP health outcome of “improved health and wellbeing for all Bhutanese”. The strategic outcomes are linked to several outputs identified by the MOH in the health sector section of the 13th FYP | Yes, Enhance the capability of at national and subnational levels to carry out stewardship functions with special focus on PHC. PHC oriented health systems are critical for better health outcomes, equity and efficiency | Yes. Aligned with SGD and WHO and UNFDP indicators |
| 25 | National Health Policy [19] | 2011 | National | Botswana | Comprehensive national health system policy | All people living in Botswana | Implemented | Strengthen health system to ensure universal access, address disease burden | Expanded facilities; improved ART access; progress on malaria reduction; persistent inequities in maternal/child mortality & HRH shortages | Explicit focus on reducing inequities across social groups, regions, gender, disadvantaged; incorporates social determinants of health | Anchored in WHO health system “six building blocks,” MDGs, Ouagadougou Declaration, Paris Declaration on Aid Effectiveness |
| 26 | National Sexual and Reproductive Health Policy | 2022 | National | Mauritius | Sexual and Reproductive Health | General population | Implemented | to provide guidance to the Ministry of Health and Wellness and all stakeholders on the coordination and implementation of relevant programmes in response to the country’s Sexual and Reproductive Health and Rights and needs. | have their bodily integrity, privacy, and personal autonomy respected; • freely define their own sexuality, including sexual orientation and gender identity and expression; • decide whether and when to be sexually active; • choose their sexual partners; • have safe and pleasurable sexual experiences; • decide whether, when, and whom to marry; • decide whether, when, and by what means to have a child or children, and how many children to have; and • have access over their lifetimes to the information, resources, services, and support necessary to achieve all the above, free from discrimination, coercion, exploitation, and violence. |
Mainstream SRHR issues of equity and empowerment | UNDP’s Sustainable Developments Goals WHO’s Reproductive Health strategy 2004 International Conference on Population and Development (ICPD) 1994 4th World Conference on Women (Beijing) 1995 |
| 27 | National Policy on Sexual and Reproductive Health [14] | 2013 | National | The kingdom of Swaziland | Sexual and Reproductive Health | Women, men, adolescents, youth, ageing population | Implemented | Provide coordinated, integrated SRH services; improve maternal and child health; reduce HIV/STI burden; promote gender equity and rights | Increased ANC coverage (94%); facility deliveries (74%); integration of HIV/SRH; policy guidelines for FP, PMTCT, cervical cancer | Emphasis on gender equality, community participation, rights-based approach | Explicitly aligned with ICPD PoA, FWCW, MDGs, AU SRHR framework, Maputo Plan of Action, SADC protocols |
| 28 | National Reproductive Maternal,, Newborn, Child And Adolescent Health (RMNCAH) Policy [15] | 2018 | National | Rwanda | Reproductive maternal, newborn, child and adolescent health | women, new born, children and adolescents | Implemented | The continuum of care throughout the life cycle and health system which has been proved to have a high impact on reducing maternal, neonatal and child mortality and morbidity. | Strengthen inter-sectoral collaboration and coordination and harmonize existing policies to address the social determinants of poor RMNCAH outcomes, and conduct research to identify major obstacles and the most effective coordination mechanisms. Implement and monitor a harmonized, integrated and sustainable package of quality client and youth-friendly essential RMNCAH promotion, prevention and treatment interventions, commodities and innovative technologies at hospital, health centre and community levels and conduct research on the cost-effectiveness of interventions. Build capacity of training institutions, managers and health care providers in integrated RMNCAH care so that health staff at all levels from community upwards are able to deliver quality, integrated, client and youth-friendly RMNCAH services. Strengthen health systems and research towards universal coverage of RMNCAH services paying attention to the deployment and retention of health staff, financial and geographical access to services by under-served and vulnerable groups/ beneficiaries and use the HMIS to monitor equity. Intensify health promotion efforts to increase community knowledge and skills on RMNCAH interventions and promote health seeking behaviour. Strengthen governance systems and accountability (joint planning, budget allocation, implementation, monitoring and evaluation) of integrated RMNCAH interventions at central, decentralised and community levels, including with public-private partnerships and through Imihigo and performance- based contracts. |
Yes, All women, new born babies, children and adores- cents - without distinction of age, gender, marital status, ability (mental or physical), race, religion, sexuality, political beliefs, geographical situation, or socio-economic status - have a right to equal and universal access to RMNCAH interventions | Millennium Develop- mint Goals |
| 29 | Population and Reproductive Health Policy | 1998 | National | Sri Lanka | "Population stabilization Reproductive health Family planning Gender equality Youth/adolescent health Elderly care Migration and urbanization Public awareness Data systems" |
Women of reproductive age, the elderly, urban migrants, general population, national policymakers and institutions. | Implemented | to review existing data and discover emerging issues of population in Sri Lanka in order to propose appropriate policy interventions which will facilitate the promotion of overall development in the country |
Safe motherhood Maternal morbidity and mortality Subfertility and infertility Anemia in reproductive-aged women and pregnant mothers Unwanted pregnancies Reproductive tract infections (RTIs) Sexually transmitted infections (STIs) and HIV/AIDS Reproductive cancers (e.g., cervical, ovarian, breast, prostate) |
Yes,Emphasis on gender equity, underserved areas, rural/urban balance | Not mentioned, Aligns with ICPD 1994, MDG 5, SDGs (esp. SDG 3, 5) |
| 30 | Reproductive Health, Gender & Rights in Mongolia [16] | 2000 | National | Mangilao | Reproductive Health, Gender & Rights | General population | Implemented | Aims at creating a favorable environment for positive support and actions in the field of reproductive health, through advocacy with law and policy-makers and programme managers at all levels | This report provides a critical analysis of the legal environment related to reproductive health and gender, and as such provides the necessary background to identify gaps which need to be addressed in the current laws. The workshop mentioned above provides us with a series of recommendations for such changes to be advocated for and these are presented in Appendix 1. It is hoped that this report will be a useful reference tool for Members of Parliament, for policy-makers, decision-makers and programme-managers, for NGOs, for international donors for a better understanding of the legal environment in Mongolia for reproductive health and for gender. | It was relatively straightforward for government to implement strong legal guarantees for equality in employment under a centrally planned system. | Yes |
Table 2.
AACODS Scoring Table of Included studies.
| Study ID | Policy/ article name | Year | Country | Authority (5) | Accuracy (5) | Coverage (5) | Objectivity (5) | Date (5) | Significance (5) | Total score (30) | Total Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ghana's Free Delivery Care Policy [29] | 2003 | Ghana | 5 | 3 | 3 | 3 | 3 | 5 | 22 | Medium |
| 2 | National Women’s Health Strategy 2020–2030 | 2020 | Australia | 5 | 4 | 4 | 3 | 5 | 5 | 26 | High |
| 3 | Israel: Reproduction and Abortion: Law and Policy [27] | 2012 | Israel | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 4 | National Population Policy | 2006 | Tanzania | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 5 | Reproductive Health Policy Brief | 2019 | Australia | 4 | 3 | 3 | 3 | 5 | 4 | 22 | Medium |
| 6 | National Reproductive Health Service Policy and Standards (3rd Edition) | 2014 | Ghana | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 7 | HPV Screening, Invasive Cervical Cancer and Screening Policy in Australia | 2017 | Australia | 5 | 4 | 3 | 3 | 4 | 5 | 24 | Medium |
| 8 | National Guidelines for Cervical Cancer Screening Programme | 2012 | South Africa | 5 | 4 | 3 | 3 | 4 | 5 | 24 | Medium |
| 9 | Cervical Cancer Prevention and Control Policy [30] | 2017 | South Africa | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 10 | Sweden’s international policy on Sexual and Reproductive Health and Rights [22] | 2021 | Sweden | 5 | 4 | 4 | 4 | 5 | 5 | 27 | High |
| 11 | Women's Health Plan: A plan for 2021-2024 | 2024 | Scotland | 5 | 4 | 4 | 4 | 5 | 5 | 27 | High |
| 12 | The NHS Wales Women's Health Plan | 2024 | Wales | 5 | 4 | 4 | 4 | 5 | 5 | 27 | High |
| 13 | Women's Health Strategy for England | 2022 | England | 5 | 4 | 4 | 4 | 5 | 5 | 27 | High |
| 14 | Chronic conditions policy brief | 2019 | Australia | 4 | 4 | 4 | 3 | 5 | 4 | 24 | Medium |
| 15 | Pregnancy and maternal health policy brief | 2019 | Australia | 4 | 4 | 4 | 3 | 5 | 4 | 24 | Medium |
| 16 | Sexual and health policy brief [28] | 2019 | Australia | 4 | 3 | 3 | 3 | 5 | 4 | 22 | Medium |
| 17 | Women’s Health: Best Practices in Sex Education Implemented by Local Governments [20] | 2017 | Japan | 4 | 3 | 3 | 3 | 4 | 4 | 21 | Medium |
| 18 | National action plan for endometriosis [13] | 2017 | Australia | 5 | 4 | 3 | 3 | 4 | 4 | 23 | Medium |
| 19 | RANZCOG Submission to the National Women’s Health Strategy [21] | 2023 | Australia & New Zeland | 5 | 4 | 4 | 4 | 5 | 4 | 26 | High |
| 20 | Sexual and Reproductive Health Rights under the Reproductive and Child Health Policy – Compromising Women's Dignity [17] |
2010 | India | 5 | 4 | 4 | 3 | 3 | 4 | 23 | Medium |
| 21 | National Sexual and Reproductive Health and Rights Policy [17] | 2022 | Myanmar | 5 | 4 | 4 | 3 | 5 | 5 | 26 | High |
| 22 | National Reproductive Health Policy [18] | 2010 | Sudan | 5 | 4 | 4 | 3 | 3 | 4 | 23 | Medium |
| 23 | NatioNal Medical StaNdard For reproductive HealtH [20] | 2020 | Nepal | 5 | 4 | 4 | 3 | 5 | 4 | 25 | High |
| 24 | Reproductive, Maternal, Newborn, Child and Adolescent + Health of Ageing (RMNCAH+A) Strategy [23] | 2025 | Bhutan | 5 | 4 | 4 | 3 | 5 | 5 | 26 | High |
| 25 | National Health Policy [19] | 2011 | Botswana | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 26 | National Sexual and Reproductive Health Policy | 2022 | Mauritius | 5 | 4 | 4 | 3 | 5 | 5 | 26 | High |
| 27 | National Policy on Sexual and Reproductive Health [14] | 2013 | The kingdom of Swaziland | 5 | 4 | 4 | 3 | 4 | 5 | 25 | High |
| 28 | National Reproductive Maternal, Newborn, Child and Adolescent Health (RMNCAH) Policy [15] | 2018 | Rwanda | 5 | 3 | 3 | 3 | 4 | 4 | 22 | Medium |
| 29 | Population and Reproductive Health Policy | 1998 | Sri Lanka | 5 | 4 | 4 | 3 | 2 | 4 | 22 | Medium |
| 30 | Reproductive Health, Gender & Rights in Mongolia [16] | 2000 | Mongolia | 4 | 3 | 3 | 3 | 2 | 4 | 19 | Medium–Low |
Table 3.
Combined Thematic and Contextual Analysis.
| Theme | Contextual Evidence | Findings/ Patterns | Implications for IVF & Geriatric Mothers |
|---|---|---|---|
| Legal & Policy Frameworks | Policies such as Israel’s Reproduction and Abortion Law (2012), Sweden’s Sexual and Reproductive Health and Rights policy (2006), and Australia’s National Women’s Health Strategy (2020–2030) provide frameworks for reproductive rights, access to assisted reproductive technologies, and menopause care(22). | Rights-based approaches have increasingly replaced purely maternal/child-focused policies, yet implementation is inconsistent. Many LMIC policies reference reproductive health broadly but lack explicit provisions for IVF or age-related fertility interventions. | IVF access for older women is often constrained by age limits, religious or cultural norms, and coverage gaps. Legal clarity and supportive regulation are needed to ensure older women have equitable access to reproductive technologies and fertility counseling. |
| Financing & Coverage | Ghana’s Free Delivery Care Policy (2007) and Nigeria’s Saving One Million Lives illustrate targeted financing models; Australia’s strategy includes dedicated funding for chronic conditions and reproductive health [29]. | Fee removal, insurance coverage, and government subsidies can improve service uptake, but LMICs face sustainability challenges and hidden costs that reduce access for older or IVF-seeking women. | Older women seeking IVF or geriatric maternal care may face high out-of-pocket costs in LMICs, while HICs provide better coverage through insurance and public health financing. Dedicated funding streams for assisted reproductive technologies are essential. |
| Service Delivery & Workforce | Decentralization in Argentina (abortion care), Scotland and Wales (menopause services), and Sri Lanka’s integrated MCH services demonstrate workforce adaptation to population needs. | Nurse- and midwife-led services expand access; integration of reproductive, chronic, and menopause care improves continuity. Gaps persist in provider training, age-specific care, and adolescent-sensitive approaches. | Geriatric mothers and older IVF patients require specialized clinical expertise, including high-risk pregnancy management and menopausal support. Workforce training in these areas ensures safer outcomes and patient-centered care. |
| Equity & Structural Determinants | Australia’s equity focus on Indigenous, rural, and LBTI women; South Africa’s cervical cancer screening policy for high-risk groups; Ghana’s reproductive health policies highlighting rural and poor populations. | Policies increasingly recognize social, economic, and cultural barriers, but targeted interventions for marginalized older women or IVF patients are limited. | Older women and IVF patients often face compounded inequities, including rural residence, low income, and cultural barriers. Equity-oriented policies should prioritize access, counseling, and support services for these groups. |
| Perimenopause, Menopause, Post-Menopause | Australian Reproductive Health Policy, NHS Wales Women’s Health Plan, Scotland’s Women’s Health Plan, and Ghana’s reproductive health policies address menopause care, HRT, and chronic condition management. | Recognition of menopausal symptoms and chronic disease management is increasing. Integration into primary care remains limited in many LMICs; guidance is inconsistent regarding fertility, late pregnancies, and hormonal support. | Older women pursuing IVF or experiencing late pregnancies need tailored menopause management, HRT counseling, and screening for chronic conditions. Policies must integrate reproductive planning and geriatric maternal care for optimal health outcomes. |
Combined Thematic and Contextual Analysis
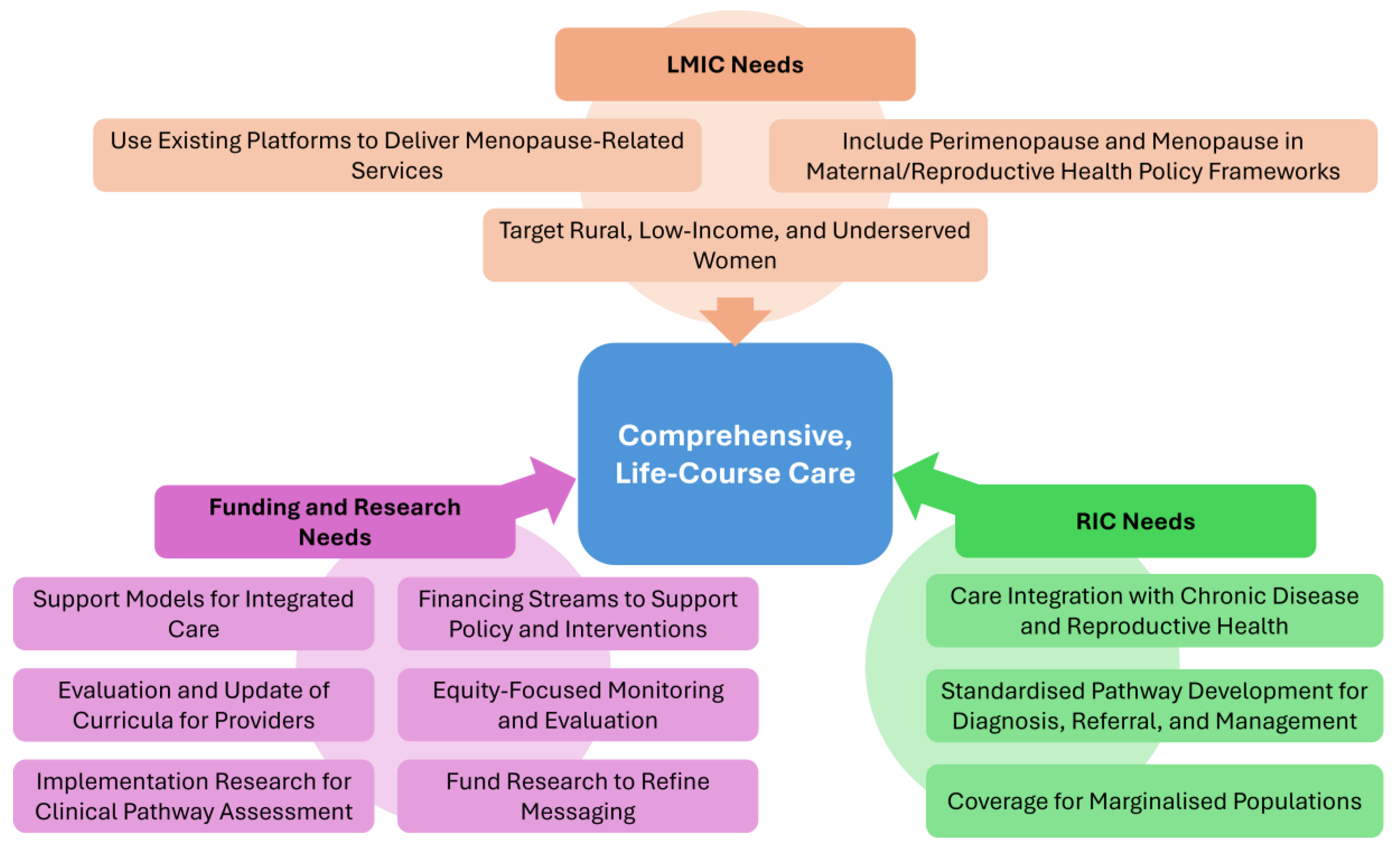
Figure 2.
Key international actions required to ensure comprehensive, life-course care for menopause.
Figure 2.
Key international actions required to ensure comprehensive, life-course care for menopause.
Peri-Menopause, Menopause, and Post-Menopause Health
Menopause-specific considerations were addressed in only a subset of policies, primarily in HICs. Australia, Scotland, England, and the NHS Wales strategies explicitly incorporated menopause and peri-menopause care, including vasomotor symptom management, chronic disease prevention, mental health support, and hormone therapy. Data from these policies highlighted that the average age of natural menopause ranged from 51 to 52 years, with 2–8% of women experiencing early or late menopause, and vasomotor, genitourinary, and psychosocial symptoms were common. Awareness, diagnostic services, and culturally appropriate education were identified as critical gaps, as noted in Australia’s national action plan for endometriosis and chronic conditions briefs [13]. The FDA’s recent approval of Veozah (fezolinetant) underscores the potential for novel non-hormonal therapies to broaden treatment choices and help destigmatize menopause care. However, whether HIC governments will integrate fezolinetant into national strategies and public funding mechanisms remains uncertain, highlighting a policy gap between therapeutic innovation and equitable access [32].
LMIC policies appeared to generally marginalize menopause care, focusing instead on maternal health and reproductive capacity. Ghana’s National Reproductive Health Policy (2014) and Tanzania’s Population Policy (2006) acknowledged midlife women indirectly through chronic disease or family planning initiatives but lacked actionable guidelines for menopause management [24,29]. This gap illustrates the broader trend in global health policy where midlife women are under-prioritised, despite evidence of significant morbidity associated with menopause transition and postmenopausal conditions.
Financing and Health System Capacity
Financial accessibility and health system capacity emerged as critical determinants of policy effectiveness. In Ghana, the removal of delivery fees increased service utilization but disproportionately benefited wealthier populations due to indirect costs and variable facility-level implementation. Similarly, Australia and the UK invested in comprehensive health service coverage, including cervical cancer screening, chronic disease prevention, and menopause care. South Africa’s cervical cancer screening programs demonstrated partial financial accessibility through free lifetime smears, though high-risk populations such as women living with HIV and adolescents remained vulnerable due to structural inequities [30].
Across these contexts, financial reforms improved theoretical access but did not fully eliminate structural barriers. Adolescents and women in midlife were particularly sensitive to hidden costs, transport barriers, and service gaps, which could delay preventive care, including HPV vaccination, cancer screening, and menopause management [30].
Service Delivery Models and Health Workforce
Service delivery models evolved from a narrow focus on maternal–child health to integrated reproductive and midlife health approaches. In Australia, clinical guidelines addressed peri-menopause and chronic conditions through preventive and individualized care, while Scotland and England emphasised menopause awareness, workplace health, and mental well-being. Nurses and midwives remained central to delivering reproductive health and screening services in both high- and low-income countries, but limited training on age- and context-specific needs hindered effective service provision. Confidentiality, provider bias, and insufficient youth-friendly or midlife-focused care were consistent barriers across several policies, including Ghana, South Africa, and Rwanda [15,29,30].
Policy Drivers and Global Influences
The review revealed a strong influence of global frameworks in shaping national agendas. High-income countries were able to align policy goals with the Sustainable Development Goals, WHO recommendations, and international rights conventions, translating these into integrated strategies that addressed both reproductive and chronic health, including menopause. For instance, Sweden’s international policy on Sexual and Reproductive Health and Rights (2006) and Australia’s multiple health briefs emphasized equitable access to care, preventive health, and chronic disease management, while also recognizing the social determinants of health and age-specific needs of women in midlife [22].
Low- and middle-income countries demonstrated more selective adoption of global frameworks, often focusing on immediate maternal health needs and fertility regulation. Ghana’s Free Delivery Care Policy, Tanzania’s reproductive health initiatives, and Rwanda’s RMNCAH policy illustrate donor-driven priorities, where adolescents and women’s midlife health were frequently integrated into broader maternal health strategies but rarely operationalized as targeted interventions [15,29]. This reflects a tension between aspirational commitments to equity and reproductive rights, and the practical limitations imposed by resource constraints, institutional capacity, and competing priorities [15,29].
Equity and Structural Determinants
Equity was a prominent theme in high-income countries, which explicitly addressed intersectional vulnerabilities in their national strategies. For example, Australia’s Women’s Health Strategy, Scotland’s Women’s Health Plan, and the NHS Wales plan highlighted disparities affecting rural women, Indigenous populations, migrants, and those with disabilities. In contrast, low- and middle-income countries often focused equity discussions on poverty reduction and geographic access, with limited attention to age, chronic disease, or social determinants such as education and employment.
Legal and rights-based policies further underscored the importance of structural determinants. Sweden’s SRHR policy, South Africa’s cervical cancer prevention policy, and Australia’s reproductive health strategy demonstrated how recognition of rights could enhance women’s agency in health decision-making, yet operationalization remained uneven, particularly for marginalized or younger populations [22,30].
Narrative Synthesis
Overall, the 30 policies demonstrate that while women’s health policies have progressively incorporated life-course, rights-based, and equity-oriented approaches, peri-menopause and post-menopause care remain inconsistently addressed. High-income countries provide models of integrated care that combine preventive, chronic, and menopause-focused services, often with attention to marginalized populations. Low- and middle-income countries, constrained by financial and systemic limitations, continue to prioritize maternal survival and fertility management, leaving older women underserved. Adolescents and young women remain inconsistently addressed across both contexts, highlighting the need for age-specific, life-course-responsive, and equity-driven health policy frameworks.
Discussion
This systematic evaluation show most policies focusing on later reproductive years are scarce, particularly in the LMIC settings. Although there are policies aligned to chronic disease management, menopause symptom management, reproductive disorders including PCOS, endometriosis, and adenomyosis, and cancer prevention, their implementation and comprehensiveness vary considerably. HICs such as Australia have integrated structured approaches with dedicated services and inclusive equity considerations, while LMICs like Sri Lanka, Ghana, and South Africa often demonstrate fragmented policy frameworks, limited access to menopause management, and underdeveloped psychosocial support [28,29]. The UK demonstrates policy variability across England, Wales and Scotland, which could attribute to health inequalities and limitations to health service infrastructure development. Cancer screening programs are generally more established in high-income settings, with LMICs showing considerable gaps in accessibility and coverage. Across all settings, policies frequently recognize equity as a principle but often fail to operationalise it fully, particularly for marginalized populations including rural, low-SES, ethnic minority, and transgender or non-binary individuals.
Over the past two decades, there has been a shift from narrowly framed maternal and reproductive health priorities toward a broader, life-course, and rights-based perspective. Equity considerations are often limited, leaving rural, socioeconomically disadvantaged, and marginalized populations at a disadvantage. These gaps underscore the continued need for comprehensive, age- and stage-specific health strategies that bridge policy rhetoric with clinical practice.
The findings highlight a global disparity in the prioritization and operationalization of women’s health policies beyond reproductive years. Despite the growing life expectancy and the significant portion of women’s lives spent in perimenopause, menopause, and post-menopause, policies continue to emphasize maternity and reproductive-age health. Chronic diseases, which disproportionately affect women during these later life stages, are variably addressed, and targeted management strategies for conditions such as cardiovascular disease, diabetes, and osteoporosis remain inconsistent. Reproductive disorders such as PCOS and endometriosis conditions with substantial impacts on quality of life and productivity receive limited attention outside high-income settings [13]. Psychosocial needs, workplace equity, and cultural considerations are particularly underrepresented, reflecting broader systemic gaps in addressing social determinants of health.
Comparison with Prior Policy Trajectories
The trajectory of women’s health policy, as reflected in these 30 policies, aligns with three broad phases: the maternal survival era, the reproductive health and rights era, and the life-course and equity-based era. In the maternal survival era, early policies emphasized safe childbirth, skilled attendance, and fertility control. For example, Ghana’s Free Delivery Care Policy (2007) focused on access to facility-based deliveries, benefiting maternal mortality outcomes but failing to address later life stages, including menopause [29]. During the reproductive health and rights era, policies incorporated family planning, fertility management, and safe abortion, as seen in Tanzania’s Population and Reproductive Health Policy (2006) and Israel’s reproductive care legislation (2012) [27]. Although these policies recognized women’s reproductive agency, the focus remained primarily on fertility and early maternal outcomes, leaving midlife health largely unaddressed. The life-course and equity-based phase is exemplified by policies from Australia, Scotland, and England, which included chronic disease management, menopause care, sexual health, and palliative care. These policies reflect a broader recognition of the diversity of women’s needs throughout life. Yet, despite these advances, age- and stage-specific interventions remain insufficient, particularly for women experiencing perimenopause or early menopause, highlighting persistent gaps between policy rhetoric and clinical reality.
Implications for Perimenopause, Menopause, and Post-Menopause
Among these policies, only a subset explicitly addressed menopause. Key gaps include insufficient guidance on symptom management (e.g., vasomotor symptoms, sleep disturbances, mood changes), limited access to hormonal and non-hormonal therapies, and a lack of structured screening or preventive programs targeting midlife women.
Policies that successfully integrated menopause into broader women’s health strategies, such as Australia’s Reproductive Health Policy and Scotland’s Women’s Health Plan, demonstrate the importance of combining preventive care, chronic disease management, and mental health support. Conversely, policies from LMICs like Ghana and Tanzania acknowledged menopause largely in descriptive terms, without operational guidance, resulting in inconsistent service provision [24,28,29].
The absence of early-perimenopause-specific interventions also suggests that women entering the menopausal transition are underrepresented in policy frameworks. This omission risks delayed identification of symptoms, reduced access to hormonal therapies, and underdiagnosis of associated chronic conditions, such as osteoporosis or cardiovascular disease.
Clinical Implications
The findings highlight the need for healthcare systems to integrate menopause and perimenopause care into routine primary and reproductive health services. Clinicians should adopt a life-course perspective, screening for common menopausal symptoms, providing guidance on hormone replacement therapy where appropriate, and addressing comorbid chronic conditions.
Training for healthcare providers should include menopause-specific care, mental health support, and patient-centered communication to reduce stigma and improve adherence. Policies should also promote preventive interventions such as cervical cancer screening, HPV vaccination, and management of endometriosis and PCOS, which have implications for midlife health [31].
Additionally, equity-focused implementation is essential. Rural, socioeconomically disadvantaged, and minority women often face barriers to accessing menopause care, and clinical services must be adapted to reach these groups. Integrating adolescent, perimenopausal, and post-menopausal care under the same life-course framework can enhance continuity and improve long-term health outcomes.
Strengths and Limitations
This is the first systematic evaluation of global women’s healthcare policies focusing on the later reproductive years. The lack of access to hard-copy policies and those in languages other than English is a limitation. Furthermore, heterogeneity in policy scope and format limited the ability to perform quantitative comparisons.
Policy Recommendations
The review of 30 policies reveals a gradual but uneven global transition towards a life-course approach in women’s health, with significant disparities between HICs and low- and LMICs. While some HICs have begun to integrate perimenopause and menopause into national health strategies through clear clinical pathways, provider training, and service standards, LMICs remain primarily focused on maternal and reproductive health, with limited attention to midlife health. Across all settings, adolescents and midlife women are underrepresented, resulting in fragmented care and restricted access to targeted interventions. To close these gaps, policies must explicitly address perimenopause and menopause, backed by dedicated financing and robust monitoring systems with age- and menopause-stage disaggregated data. Public education campaigns are essential to reduce stigma and promote uptake of services, while integration with chronic disease and reproductive health care will enable holistic, continuous support. Real-time research and evaluation particularly in LMICs are critical to generate evidence on prevalence, symptom burden, and intervention effectiveness. Without enforceable policy entitlements, secure funding, and integrated service delivery, efforts will remain aspirational and fail to produce meaningful improvements in the health and rights of women throughout the life course.
Table 4.
Evidence-Based Policy Considerations for Perimenopause and Menopause.
| Domain | High-Income Countries (HICs) | Low- and Middle-Income Countries (LMICs) | Funding & Research Needs |
|---|---|---|---|
| Policy Integration | Embed menopause in national women’s health strategies with enforceable entitlements and service standards. | Expand beyond maternal/reproductive health to explicitly include perimenopause and menopause in policy frameworks. | Multi-donor and domestic financing streams to support real-time policy development and pilot interventions. |
| Clinical Pathways | Develop clear, standardized pathways for diagnosis, referral, and management, linked to workforce training. | Create simplified, scalable clinical guidelines adaptable for rural and resource-limited settings. | Fund implementation research to assess clinical pathway effectiveness. |
| Provider Training | Incorporate menopause-specific education into medical, nursing, and allied health curricula. | Strengthen training for primary care and community health workers to identify and manage midlife health needs. | Continuous evaluation and updating of curricula based on emerging evidence. |
| Service Delivery | Integrate menopause care with chronic disease and reproductive health services for seamless care. | Use existing maternal and reproductive health platforms to deliver menopause-related services where new services are not yet feasible. | Support pilot models for integrated care, with funding for scale-up. |
| Equity and Access | Ensure coverage for marginalized populations, including migrants, LGBTQ+ individuals, and low-income groups. | Target rural, low-income, and underserved women, reducing financial and geographic barriers to care. | Establish equity-focused monitoring and evaluation frameworks with disaggregated data. |
| Public Awareness | Implement campaigns to normalize menopause and reduce stigma, engaging workplaces and communities. | Address cultural barriers and misinformation through locally adapted education and outreach. | Fund qualitative and participatory research to refine messaging. |
| Monitoring & Evaluation | Establish robust systems with age- and menopause-stage disaggregated data for quality and outcome tracking. | Build basic data collection capacity within health information systems to track service uptake and outcomes. | Support real-time digital tools for data collection and policy feedback loops. |
| Research & Evidence Base | Support longitudinal studies on menopause trends, interventions, and workforce impacts [28]. | Prioritize baseline epidemiological studies to map prevalence, symptom burden, and access gaps. | Allocate funding for cross-country comparative studies and policy evaluations. |
Conclusions
Effective policy for perimenopause and menopause requires enforceable entitlements, secure financing, and integrated service delivery that address women’s diverse and evolving needs. Without dedicated investment in data, research, and monitoring, policies risk remaining aspirational rather than achieving tangible improvements in women’s health and rights. Bridging the gap between HICs and LMICs through equitable, evidence-based strategies is essential to ensure all women can access comprehensive, life-course care.
Author Contributions
GD developed the ELEMI program and conceptualised this paper as part of the KATHERINE project. GD conducted the analysis. NW wrote the first draft and furthered by GD,MH,EL and NR. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
Not funded.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
No participants were involved within this paper.
Data Availability Statement
The data shared within this manuscript is publicly available.
Conflicts of interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- Minkin MJ. Menopause: Hormones, Lifestyle, and Optimizing Aging. Obstetrics and Gynecology Clinics of North America. 2019. [CrossRef]
- Kimberly Peacock; Karen Carlson; Kari M. Ketvertis; Chaddie Doerr. Menopause (Nursing): StatPearls [Internet]. 2023.
- Mohammad Haddadi F-sT, Isa Akbarzadeh, Tahereh Eftekhar, Sedigheh Hantoushzadeh, Fatemeh Hedayati, Sepideh Ahmadi & Ahmad Delbari The sleep quality in women with surgical menopause compared to natural menopause based on Ardakan Cohort Study on Aging (ACSA). 2025. [CrossRef]
- World Health Organization. Menopause 2024 [Available from: Menopause [Internet]. [cited 2025 Aug 27]. Available from: https://www.who.int/news-room/fact-sheets/detail/menopause.
- Remme M VA, Fernando G, Bloom DE. Investing in the health of girls and women: a best buy for sustainable development. BMJ 2020. [CrossRef]
- Kathryn Godburn Schubert CEB, Katy Kozhimmanil, Susan F Wood,. To Address Women's Health Inequity, It Must First Be Measured. 2022. [CrossRef]
- NHS. Hormone Replacement Thaerapy 2023 [Available from: [cited 2025 Aug 27]. Hormone replacement therapy (HRT). Available from: https://www.nhs.uk/medicines/hormone-replacement-therapy-hrt/.
- YelaGabriela Pravatta RezendeRenan Massao NakamuraCristina Laguna Benetti-PintoIrfan MuhammadRabia KareemJeremy van VlymenAshish ShettyGanesh DangalSuman PantNirmala RathnayakeLanka DassanayakeJian Qing ShiOm KurmiSaval KhanalSohier ElneilMARIE Consortium GDGBPTPMBCHAPST-KM-AFKUEEMM-HTY-KSA. A Perspective on Economic Barriers and Disparities to Access Hormone Replacement Therapy in Low and Middle-Income Countries (MARIE-WP2d) 2025 [.
- Rakibul M Islam JR, Sadia Katha, Md Anwer Hossain, Siraj Us Salekin, Anika Tasneem Chowdhury, Ashraful Kabir, Lorena Romero, Susan R Davis,. Menopause in low and middle-income countries: a scoping review of knowledge, symptoms and management. Climacteric. 2025. [CrossRef]
- Manisha Gore & Julia Morgan. Indigenous women’s experiences, symptomology and understandings of menopause: a scoping review. BMC Women's Health. 2025. [CrossRef]
- Walker-Bone K DS. Menopause, women and the workplace. Climacteric. 2025. [CrossRef]
- David Moher AL, Jennifer Tetzlaff, Douglas G Altman; PRISMA Group,. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 2009. [CrossRef]
- Australian goverment-department of health. National action plan for endometriosis. 2018.
- Health TKOS-Mo. National policy on reproductive and sexual health. 2013.
- Republic of Rwanda-Ministry of Health. National reproductive maternal, newborn, child and adolescent (RMNCAH) health policy. 2018.
- Arthi Patel L, Australian Volunteers International, D. Amarsanaa, Centre for Human Rights and Development,. Reproductive Health, Gender & Rights in Mongolia. 2000.
- Ministry of health-Myanmar. National Sexual and Reproductive Health and Rights Policy. 2022.
- Sudan Government of National Unity - Federal Ministry of Health. National Reproductive Health Policy. 2010.
- Ministry of Health G-B. National Health Policy-“Towards a Healthier Botswana”. 2011.
- Government of Nepal- Ministry of Health and Population. National Medical Standard For Reproductive Health. 2020.
- Submission of the Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Aotearoa New Zealand- Women’s Health Strategy. 2023.
- Public health agency of Sweden. National Strategy for Sexual and Reproductive Health and Rights (SRHR). 2022.
- Ministry of Health - Royal Government of Bhutan. REPRODUCTIVE, MATERNAL, NEWBORN, CHILD AND ADOLESCENT + HEALTH OF AGEING (RMNCAH+A) STRATEGY. 2025-2029.
- Lisa Ann Richey. Women's Reproductive Health & Population Policy: Tanzania. Review of African Political Econom. 2003. [CrossRef]
- Government of New Zealand. Women in New Zealand - United Nations Convention on the Elimination of All Forms of Discrimination against Women. 2016.
- UNFPA. ANNUAL REPORT 2017. 2017.
- The Law Library of Congress. Israel: Reproduction and Abortion: Law and Policy. 2012.
- Hsiu-Wen Chan and Gita Mishra. Sexual Health Policy Brief -Australian Longitudenal study on Women health. Women’s health. 2019.
- Ofori-Adjei D. Ghana’s Free Delivery Care Policy. GHANA MEDICAL JOURNAL. 2007.
- Department of health- South Africa. National guideline for cervical cancer screening programme. 2000.
- Gayathri Delanerolle PP, Sohier Elneil,Vikram Talaulikar, George U Eleje, Rabia Kareem, Ashish Shetty, Lucky Saraswath, *Om Kurmi,Cristina Laguna Benetti-Pinto, Ifran Muhammad, Nirmala Rathnayake, Teck-Hock Toh, Ieera Madan Aggarwal, Jian Qing Shi, Julie Taylor,, Kathleen Riach KP, Ian Litchfield, Helen Felicity Kemp, Paula Briggs, and the MARIE collaborative. Menopause: a global health and wellbeing issue that needs urgent attention. The Lancet Global helath. 2025. [CrossRef]
- Chukwuka Elendu TWO, George S. Blewusi, Oluwatobi O.M., Meduoye, Emmanuel C. Ogelle, Arube R. Egbo, Vivian C. Nwankwo,Kingsley C. Amaefule,, SLE, Abdirahman A. Mohamed, Oyinkansola S. Ogedengbe, Ovonomor P. Aggreh, Dorin I. Obi, Victor I. Orji, Sikiru O. Bakare, Fahidah D. Adediran, Fiyinfoluwa Adetoye, Babatunde A. Akande, Omolara C. Ogunsola, Aishat M. Olanlege,. FDAapprovesVeozah(Fezolinetant)for menopausalsymptoms:anewnonhormonaloption. Annals of medicine and surgery. 2025.
Figure 1.
The study selection process is detailed in the PRISMA flow diagram.
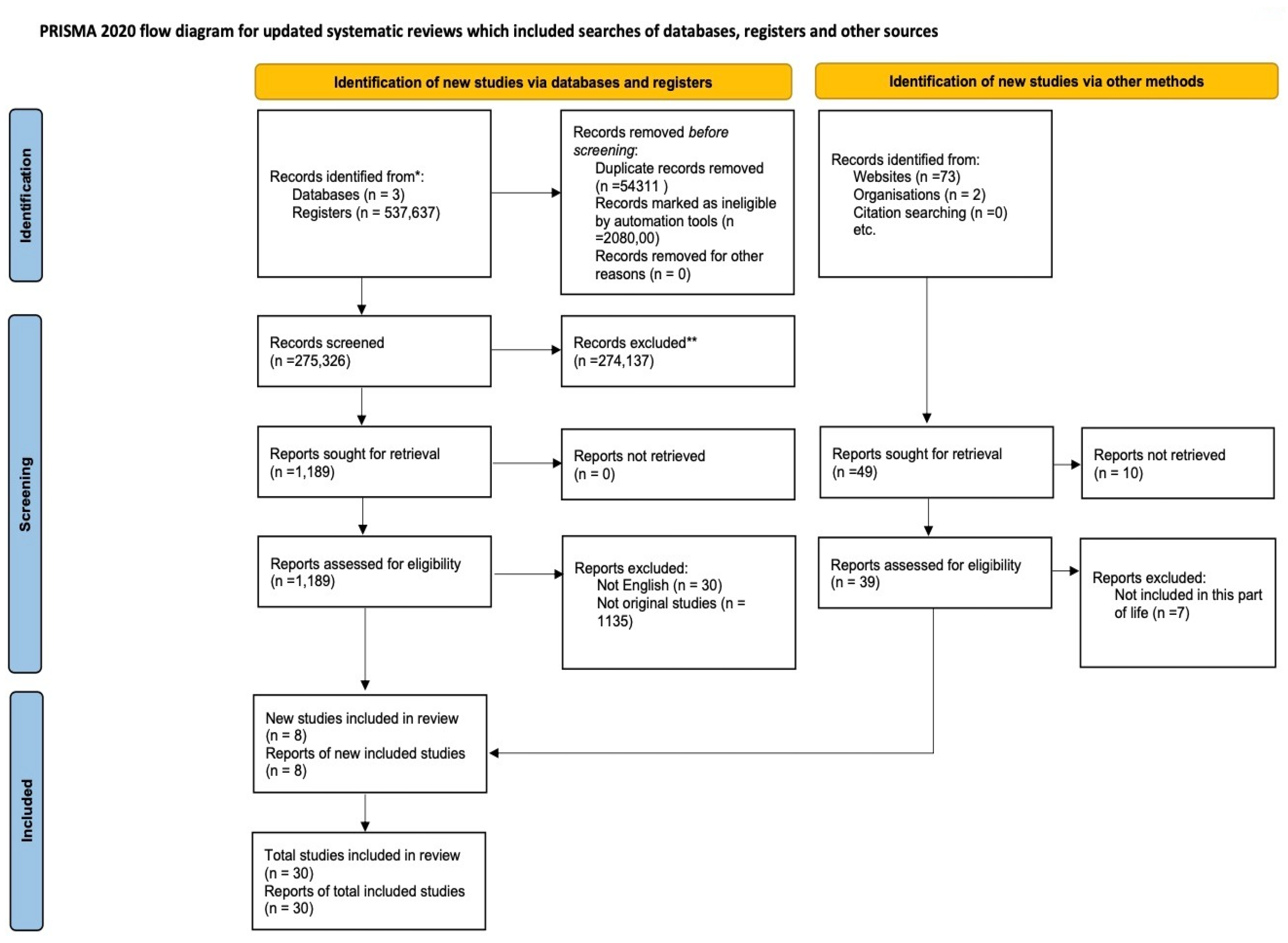
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



