Submitted:
06 September 2025
Posted:
09 September 2025
You are already at the latest version
Abstract
ST-segment elevation myocardial infarction (STEMI) represents a time-critical medical emergency where complete coronary artery occlusion initiates progressive myocardial necrosis. The fundamental principle of modern STEMI care - "Time is Muscle" - establishes that ischemic duration directly determines infarct size and clinical outcomes. Each minute of delay correlates with increased mortality, larger infarcts, and a higher risk of heart failure development. Total ischemic time encompasses both patient-mediated delays (often the largest component) and system-related delays, each influenced by distinct factors requiring targeted interventions. This comprehensive review analyzes the components of total ischemic time, quantifies the clinical consequences of delay, and evaluates evidence-based mitigation strategies. We examine the evolution from fibri-nolysis to primary percutaneous coronary intervention and the resulting logistical challenges. System-level interventions - including public awareness campaigns, re-gionalized STEMI networks, pre-hospital ECG acquisition, and standardized hospital protocols - have dramatically reduced treatment times. However, persistent disparities based on geography, presentation timing, sex, race, and age remain problematic. Emerging technologies, particularly artificial intelligence for ECG interpretation, offer promise for further time reduction.
Keywords:
ST-segment elevation myocardial infarction
; ischemic time
; door-to-balloon time
; reperfusion delay
; occlusion myocardial infarction
; STEMI networks
1. Introduction
1.1. The Emerging Paradigm: From STEMI to Occlusion Myocardial Infarction
ST-segment elevation myocardial infarction (STEMI) has traditionally been defined by complete, persistent occlusion of one or more coronary arteries, typically following atherosclerotic plaque rupture or erosion that triggers acute thrombosis [1,2,3]. This abrupt
cessation of myocardial perfusion initiates ischemic injury progressing in a “wave-front” pattern from the vulnerable subendocardial layer outward toward the epicardium (Figure 1) [4,5]. While ST-segment elevation in two or more contiguous leads has been the hallmark diagnostic finding [1,2,3], emerging evidence reveals significant limitations of this paradigm.
For decades, the STEMI/non-ST-segment elevation MI (NSTEMI) dichotomy has guided acute MI management, relying on ST-segment elevation as the primary indicator for acute coronary occlusion requiring emergent reperfusion [1,2]. However, mounting evidence reveals critical limitations in this approach. Multiple large-scale meta-analyses involving tens of thousands of patients consistently demonstrate that approximately 25-33% of patients diagnosed with NSTEMI have a totally occluded culprit artery on subsequent angiography [6,7,8,9]. This misclassification has serious clinical implications. These patients face significantly higher risks of adverse outcomes, with a pooled short-term relative risk of all-cause mortality of 1.67 compared to NSTEMI patients without occlusion [10]. The excess mortality stems from systematic delays in reperfusion therapy: despite sharing the same underlying pathophysiology as STEMI patients, those with NSTEMI related to totally occluded culprit artery are denied emergent intervention due to the absence of classic ECG findings [7]. This recognition has prompted a paradigm shift toward the occlusion MI (OMI)/non-occlusion MI (NOMI) classification system [7,8,9]. The absence of classic ST-elevation in patients with a totally occluded culprit artery often results from well-developed collateral circulation. These collateral vessels can maintain sufficient myocardial viability to prevent the full-thickness transmural ischemia necessary to generate ST-segment elevation. The diagnosis incorporates multiple elements: classic ST-elevation, “STEMI-equivalent” patterns (De Winter T-waves, posterior MI patterns, hyperacute T-waves), refractory ischemic symptoms, and adjunctive tools like bedside echocardiography [8,9,11]. Also, when discussing inferior/posterior wall infarctions, it’s crucial to emphasize that ST depressions often represent reciprocal changes mirroring ST elevations that would be visible with additional leads - particularly V7-V9 for posterior wall assessment. This highlights a critical limitation: while 12-lead ECG remains the standard, circumflex or marginal artery occlusions may manifest only as subtle depressions or remain entirely invisible without extended lead placement. This creates a dangerous paradox: while collateral circulation initially protects the myocardium, it masks the ECG signal that would trigger emergent reperfusion, leading directly to treatment delays associated with higher rates of cardiogenic shock and increased mortality in the NSTEMI with a totally occluded culprit artery population [7,12]. Additionally, the STEMI paradigm is compromised by a substantial false-positive rate, with 15-35% of emergency catheterization laboratory activations triggered by patients presenting with “STEMI mimics”. Conditions including pericarditis, benign early repolarization, and Takotsubo cardiomyopathy can produce ST-segment elevation that leads to unnecessary invasive procedures - interventions that are costly and potentially harmful to patients [7,13,14,15]. Despite compelling and growing evidence supporting the OMI paradigm, the newly released 2025 AHA/ACC Guideline for the Management of Patients With Acute Coronary Syndromes explicitly states that it did not incorporate the OMI vs. NOMI classification into its recommendations [1]. The writing committee’s rationale, as articulated in a related JACC editorial, is that the foundational randomized clinical trials upon which the guidelines are based were designed and executed using the traditional STEMI/NSTEMI framework [16]. On the other hand, while this review uses “STEMI” terminology reflecting existing literature, the principles of timely reperfusion in our opinion apply equally to all OMI patients - many currently missed by conventional STEMI-centric approaches [7,8,9,17,18].
1.2. The “Time Is Muscle” Doctrine
Eugene Braunwald’s foundational concept that “Time is Muscle” underpins modern management of all acute coronary occlusions [19]. Final infarct size, directly proportional to ischemic duration, represents the primary predictor of long-term outcomes including heart failure development and mortality [19,20]. This relationship holds true whether patients present with classic STEMI or other OMI patterns [7]. The non-linear relationship between time and salvageable myocardium - with greatest benefit within the first hours - applies universally across the OMI spectrum (Figure 1). Importantly, infarct size is also shaped by the location of the occlusion (with anterior infarctions typically causing larger damage), extent of collateral circulation (better collaterals markedly reduce infarct size), and ischemic preconditioning (brief, controlled ischemia episodes locally or remotely can halve or significantly lessen myocardial necrosis) [19,20].
1.3. Evolution of Reperfusion Strategies
Despite therapeutic advances, in-hospital mortality in STEMI remains substantial at 4-12% in European registries [2,21,22,23]. Reperfusion therapy has evolved from pharmacological to mechanical approaches [1,2,24] (Table 1). Fibrinolysis involves intravenous administration of thrombolytic agents, achieving successful reperfusion [Trombolysis in Myocardial Infarction (TIMI) grade 2-3 flow] in approximately 65% of patients [2,25]. While rapidly deployable in any emergency setting, its efficacy is highest within two hours of symptom onset. Primary percutaneous coronary intervention (PCI) mechanically opens the occluded vessel via balloon angioplasty/thrombectomy and stenting, achieving normal (TIMI grade 3) flow restoration in >95% of patients [2]. This superior efficacy translates to lower mortality, reinfarction, and stroke rates compared to fibrinolysis [26]. However, PCI’s effectiveness depends entirely on rapid access to specialized facilities and experienced teams [1,2,27]. Additionally, invasive strategies not only restore vessel patency but also visualize and stabilize the culprit lesion with stenting, making fibrinolysis - which cannot address the underlying plaque - no longer considered definitive treatment for myocardial infarction.
The paradigm shift to primary PCI transformed acute coronary occlusion management from a pharmacological to a logistical challenge [27,28,29,30]. Additionally, reperfusion paradoxically induces further injury through oxidative stress and calcium overload, potentially accounting for up to 50% of final infarct size [31,32]. This underscores the absolute urgency of minimizing initial ischemic time before irreversible injury occurs - a principle that applies equally to all patients with acute coronary occlusion, whether meeting traditional STEMI criteria or presenting with other OMI patterns [1,2,20].
2. Components and Determinants of Total Ischemic Time
2.1. Patient-Mediated Delays
The interval from symptom onset to first medical contact (FMC) consistently represents the longest and most variable component of total ischemic time. Median patient decision delay approximates 100 minutes, constituting nearly 60% of pre-hospital delay [18,33,34,35].
- Sociodemographic factors: advanced age, female sex, rural residence, low education, social isolation, diabetes mellitus
- Cognitive factors: symptom misinterpretation, particularly with atypical presentations (dyspnea, sweating, non-chest pain) common in women, elderly, and diabetics
- Behavioral factors: initial contact with general practitioners instead of emergency medical services (EMS) activation; self-transport versus ambulance utilization
Framing this as “patient delay” misleadingly assigns individual responsibility for what often reflects systemic public health failures. The American Heart Association recognizes patient delay as one of the “greatest obstacles” to successful STEMI care, calling for comprehensive public awareness campaigns [41].
2.2. Pre-Hospital System Delays
The pre-hospital phase from FMC / STEMI diagnosis to hospital arrival accounts for over 83% of symptom-to-treatment time [18,33,34,35,37,38,39,40]. Key components include:
DIDO time emerges as a crucial determinant of overall treatment effectiveness. De Luca et al. provided evidence demonstrating that prolonged inter-hospital transfer delays were independently associated with impaired myocardial perfusion, increased infarct size, and significantly higher 1-year mortality rates in patients undergoing primary PCI [44].
2.3. In-Hospital System Delays
The in-hospital phase encompasses door-to-needle time for fibrinolysis and door-to-balloon time for primary PCI. Guidelines establish quality targets of door-to-needle ≤30 minutes and door-to-balloon ≤90 minutes [1,2]. The door-to-activation interval critically determines overall door-to-balloon time - achieving activation within 20 minutes yields 89% probability of meeting the 90-minute goal versus 28% when exceeding 20 minutes [45]. Off-hours presentation, diagnostic uncertainty, and patient instability contribute to delays [46,47]. Table 2 summarizes the components and benchmarks of total ischemic time.
3. Clinical Consequences of Delayed Reperfusion
3.1. Mortality Impact
The relationship between reperfusion timing and mortality is both direct and continuous, yet its interpretation requires nuance. While shorter door-to-balloon times clearly benefit individual patients, population-level impacts have proven complex. Major registry data from the NCDR CathPCI Registry reveal a striking “door-to-balloon paradox”: despite significant improvements in national median door-to-balloon times (from 83 to 67 minutes), adjusted in-hospital mortality remained essentially unchanged at 4.7-5.0% [48]. This paradox does not diminish the importance of door-to-balloon time. Rather, it underscores that door-to-balloon represents only one component of total ischemic time, and that impressive in-hospital gains may be negated by stagnant progress in the larger, more variable pre-hospital phase [1,2]. The focus must therefore shift to the entire chain of survival, from symptom onset to reperfusion. For individual patients, the risk associated with door-to-balloon time follows a continuous, non-linear trajectory. Landmark analyses demonstrate that adjusted in-hospital mortality rises progressively: from 3.0% at 30 minutes to 3.5% at 60 minutes, 4.3% at 90 minutes, and 7.0% at 150 minutes [49]. These data support an “as short as possible” reperfusion philosophy rather than a “meet the benchmark” approach, as every minute of delay increases risk [27,41,50,51].
However, excessive focus on the 90-minute metric can produce unintended consequences. It may incentivize operators to choose faster femoral access over safer radial access or encourage selective exclusion of complex cases from quality reporting [1,2]. Furthermore, the mortality advantage of PCI over fibrinolysis diminishes with increasing PCI-related delay, reaching equipoise at 110-120 minutes [52,53,54]. For high-risk patients with large anterior infarctions presenting early, this threshold may be as short as 40-60 minutes [54,55].
3.2. Myocardial Salvage and Infarct Size
Delayed reperfusion directly increases final infarct size [5,19,56]. The myocardial salvage index - the proportion of area at risk preserved from necrosis - shows strong inverse correlation with ischemic time [57,58]. Reperfusion within two hours yields the greatest salvage and the highest myocardial salvage index [59]. Longer symptom-to-balloon times independently predict larger infarcts, increased microvascular obstruction, and reduced ejection fraction [57,58,60]. Higher myocardial salvage index powerfully predicts long-term event-free survival [59].
3.3. Long-Term Morbidity
Quantitatively, each 30-minute reperfusion delay increases one-year mortality risk by 7.5% [61]. Larger infarcts from delayed reperfusion create substrate for adverse ventricular remodeling - progressive dilatation and dysfunction culminating in heart failure [62,63,64]. Patients presenting ≥12 hours after symptom onset show significantly higher heart failure hospitalization rates: one-year death or heart failure hospitalization reaches 29% versus 17% for those treated within 12 hours [65,66]. This reframes the speed imperative beyond preventing acute death to preventing chronic disease.
3.4. Magnified Impact in High-Risk Populations
Delay’s impact is catastrophically amplified in cardiogenic shock patients, where mortality approaches 33-61% [67,68]. For every 10-minute FMC-to-device delay between 60-90 minutes, absolute mortality increases 4-7% in shock patients versus <0.5% without shock [68]. This exponential relationship mandates risk-stratified triage protocols prioritizing the most unstable patients.
4. Evidence-Based Strategies to Mitigate Delay
4.1. Public Health Initiatives
Given patient delay’s dominance, public awareness campaigns represent critical interventions [27,69]. One national campaign evaluation found 64% patient awareness, significantly associated with shorter patient delay (≤1 hour) and pre-hospital delay (≤2 hours) [70]. Effective campaigns address symptom misinterpretation, denial, and emphasize EMS activation over self-transport [1,2,70].
4.2. Optimizing Pre-Hospital Care
Pre-hospital strategies transform sequential care into parallel processing:
- Pre-hospital ECG: As a Class I recommendation, pre-hospital ECG serves as a cornerstone intervention in acute MI management [1,2]. A systematic review and meta-analysis demonstrated its association with substantial reductions in door-to-balloon time (mean difference >26 minutes) and significantly lower short-term mortality (odds ratio 0.72) [71]. The survival benefit is most pronounced in high-risk subgroups, including patients with cardiogenic shock or diabetes [72]. This finding reframes pre-hospital ECG beyond its role as a time-saving tool - it becomes a critical instrument for early risk stratification, enabling healthcare systems to preferentially accelerate care for the most vulnerable patients [1,2]. The “Stent - Save a Life!” initiative recognizes pre-hospital ECG as fundamental to effective STEMI networks [27].
- Regionalized networks: The “Stent - Save a Life!” initiative provides a structured methodology for establishing STEMI networks categorized by available resources: primary PCI networks (optimal), hub-and-spoke networks (acceptable long-term), pharmaco-invasive networks (transitional), and fibrinolysis networks (basic care requiring urgent upgrade) [1,2,27,73]. Direct transport protocols to PCI-capable centers significantly reduce mortality [75].
4.3. Streamlining In-Hospital Processes
Standardized “Code STEMI” protocols dramatically reduce door-to-balloon times [76,77,78]. Key components include:
- Emergency physician activation authority without cardiology consultation
- Single-call team notification systems
- 24/7 team availability within 20-30 minutes
- Regular performance feedback
National quality initiatives reduced median US door-to-balloon times from 94 minutes (2005) to <60 minutes currently [79]. The success of primary PCI extends beyond individual procedural excellence to require comprehensive system-wide organization with standardized operating procedures and rigorous time monitoring. Every component - from EMS activation and pre-hospital ECG transmission to catheterization lab mobilization and door-to-balloon times - must function as a coordinated chain with continuous quality metrics tracking. This systematic approach, with regular audits of time intervals and protocol adherence, transforms primary PCI from an isolated intervention into a high-reliability healthcare delivery system.
4.4. Fibrinolysis and Pharmaco-Invasive Strategy
When anticipated FMC-to-device time exceeds 120 minutes per ESC guidelines, the pharmaco-invasive strategy - early fibrinolysis followed by routine angiography within 2-24 hours - provides a crucial alternative [1,2]. These recommendations are supported by results from a large network meta-analysis demonstrating that the pharmaco-invasive approach ranked second after primary PCI, with a mortality odds ratio of 0.79 (95% CI, 0.59–1.08) compared with conventional fibrinolytic therapy alone [80]. The “Stent - Save a Life!” initiative recognizes pharmaco-invasive networks as transitional solutions that should be upgraded to full PCI capability but acknowledges their critical role in providing timely reperfusion when geography or resources preclude immediate PCI access [27]. For patients facing unavoidable long delays, pharmaco-invasive strategy yields superior long-term survival compared to delayed primary PCI [30,81]. Healthcare systems must maintain flexible, hybrid approaches deploying appropriate reperfusion modality based on real-time assessment of geography and anticipated delay. However, implementing this flexibility requires maintaining pre-hospital fibrinolysis capability in ambulances, which poses significant practical challenges - drugs must be readily available, staff trained, and systems must achieve door-to-needle times within 10 minutes of STEMI recognition [1,2]. Given the sporadic indications for this strategy in most regions, healthcare systems face a fundamental choice between investing in rarely-used fibrinolysis infrastructure versus optimizing transfer networks to minimize delays to primary PCI [27].
4.5. Upstream Glycoprotein IIb-IIIa Inhibitors
Initial enthusiasm for this appealing strategy was supported by results from an individual patient data meta-analysis (EGYPT) [82,83], the On-TIME II trial pooled analysis [84,85], and several prospective registries [72,86,87]. These studies demonstrated benefits in pre- and post-procedural TIMI flow, reduced distal embolization, and improved survival with early versus late administration of glycoprotein (GP) IIb-IIIa inhibitors. However, the negative results of the FINESSE trial [88] substantially diminished interest in upstream GP IIb-IIIa inhibitor use, leading to its near abandonment and a Class III recommendation in clinical guidelines.
The FINESSE trial results [88] should be interpreted considering several limitations: relatively long ischemic times, potentially insufficient pretreatment duration (randomization was permitted at hub centers, thus including patients not requiring transfer), and a lower-risk patient profile compared to studies showing positive results. Indeed, subsequent subanalyses demonstrated clear benefits in high-risk patients who underwent transfer and had ischemic times <4 hours [89,90]. This observation aligns with the established relationship between thrombus composition and ischemic time, whereby platelets comprise a larger proportion of thrombi within the first three hours after symptom onset. The clinical relevance of time-dependent thrombus composition has been confirmed in subanalyses of both the large HORIZONS trial [91] and the On-TIME II study [92].
Zalunfiban, a novel subcutaneous GP IIb-IIIa inhibitor currently in development, may substantially improve STEMI treatment. This agent achieves rapid onset of action (≤15 minutes) following subcutaneous administration, with high-grade inhibition of platelet function in response to ADP and thrombin receptor agonists [93,94]. Several innovative features make zalunfiban an ideal candidate for upstream strategy in patients with acute coronary occlusion: user-friendly administration, short duration of action (~2 hours) that may minimize bleeding risk, and reduced thrombocytopenia risk compared to current GP IIb-IIIa inhibitors due to its distinct mechanism of action [95].
The proportion of STEMI patients presenting within the first hours of symptom onset - and therefore suitable for this strategy - is expected to increase in coming years through public awareness campaigns, technological improvements, and refinement of STEMI networks enabling faster diagnosis and treatment. The recently completed CELEBRATE trial [96] enrolled 2,499 STEMI patients within 4 hours of symptom onset, randomizing them to receive a single subcutaneous injection of zalunfiban at 0.110 mg/kg, zalunfiban at 0.130 mg/kg, or placebo. With enrollment now complete, results are anticipated shortly. This trial may potentially revitalize this abandoned yet still promising therapeutic strategy.
5. Persistent Challenges and Disparities
5.1. Geographic Disparities
Rural patients experience longer delays at every stage, receive less primary PCI, and more fibrinolysis [97]. Paradoxically, adjusted mortality shows no urban-rural difference [97], possibly reflecting higher baseline risk in urban populations receiving superior care that equalizes outcomes with lower-risk rural patients receiving inferior care. However, this pattern of rural disadvantage may not be universal. In contrast to these US findings, a recent French study found no difference in five-year outcomes in rural and urban groups [98]. This geographic variation suggests that rural-urban disparities in cardiac care may be significantly mitigated by local healthcare infrastructure and policies [99].
5.2. Temporal Disparities
The “weekend effect” persists in STEMI care, with off-hours presentation associated with longer door-to-balloon times and small but significant mortality increases [47,100,101]. Despite 24/7 protocols, equitable care regardless of arrival time remains unrealized [100]. These disparities may be further exacerbated during large-scale system stressors such as the COVID-19 pandemic [51,102,103,104] or regional armed conflicts [105,106] - which disrupt emergency networks, reallocate critical resources, and disproportionately amplify delays in already vulnerable off-hours or resource-limited settings.
5.3. Demographic Disparities
- Women: Women with STEMI consistently present at older ages with greater comorbidity burdens, including diabetes and hypertension, which complicate their clinical presentation [36,107,108,109,110,111,112]. They more frequently experience atypical symptoms - shortness of breath, nausea, fatigue, and interscapular pain - leading to diagnostic and care-seeking delays [36,109]. These factors result in less timely reperfusion therapy and higher rates of in-hospital complications, including stroke and major bleeding, ultimately contributing to increased mortality compared with men [1,2,113].
- Racial/ethnic minorities: Black and Hispanic patients with STEMI face substantial disparities, experiencing lower odds of receiving timely, guideline-directed care such as prehospital ECGs and achieving door-to-balloon targets [114,115,116]. These populations consistently undergo invasive therapies like coronary angiography and PCI less frequently - a disparity that persists after adjusting for clinical and socioeconomic factors.
- Elderly: Older adults with STEMI experience particular vulnerability to systematic treatment delays, with the pre-hospital phase representing the most significant contributor [1,2,22,36,114,115,117]. These delays often stem from atypical presentations - confusion or weakness rather than chest pain - which patients and caregivers may attribute to other age-related conditions [118]. Even within established regionalized systems, elderly patients receive delayed reperfusion, partially explaining their elevated in-hospital mortality rates [1,2,118,119,120,121].
Notably, standardized protocols effectively eliminate these disparities [108,110]. Systems-based care approaches have demonstrated remarkable success in reducing inequities. One study showed that a comprehensive four-step protocol - incorporating ED catheterization laboratory activation, safe handoff checklists, immediate patient transfer, and radial-first PCI - successfully eliminated sex-based differences in door-to-balloon times and guideline-directed medical therapy administration [108]. This care standardization not only improved outcomes across all patient groups but also significantly narrowed the 30-day mortality gap between men and women, demonstrating that protocol-driven approaches represent powerful tools for achieving healthcare equity [108,110].
5.4. Challenges in Low- and Middle-Income Countries
The challenges discussed thus far primarily reflect high-resource settings (Table 3). For the majority of the world’s population living in low- and middle-income countries, barriers to timely reperfusion are fundamentally different and more profound [53,122,123]. These healthcare systems face multiple interconnected challenges: inadequate or absent EMS, resulting in few ambulance arrivals; prolonged transit times (median 300 minutes to hospital presentation in India); severe shortages of PCI-capable facilities concentrated in urban centers; and critical deficits in trained specialists [123]. The most significant barrier, however, is the prohibitive out-of-pocket cost of primary PCI. This financial burden creates a “fear of finance” that both deters patients from seeking care and dictates treatment decisions [27,122,123]. Consequently, the pharmaco-invasive strategy - early fibrinolysis followed by planned PCI - represents not merely an alternative for managing long delays but often the only feasible reperfusion strategy for most of the population [2,27,123,124]. Recognizing these distinct realities is essential for developing globally relevant STEMI care strategies (Table 4).
6. Future Directions
6.1. Technological Innovation
- Artificial Intelligence: AI-ECG systems show promise for detecting not only classic STEMI but also subtle OMI patterns that traditional criteria often miss [8,9,125,126,127]. However, AI remains a promising yet unproven intervention facing substantial implementation hurdles. While many applications demonstrate strong performance in retrospective studies, prospective randomized controlled trials validating their safety and real-world impact on patient outcomes remain critically absent [128]. Implementation faces significant practical and ethical barriers. Practical challenges include high development costs, requirements for vast quantities of high-quality, unbiased training data, and the technical complexity of integrating AI tools with fragmented hospital IT systems [129]. Ethical and social challenges prove equally profound. Algorithmic bias may cause models to underperform in populations underrepresented in training data. Automation complacency risks clinicians over-relying on AI suggestions, while selective adherence may lead them to follow only recommendations that confirm pre-existing beliefs [129]. The “black box” problem of AI transparency and the need for clear accountability frameworks for AI-driven decisions must be addressed before widespread adoption [130]. Progress requires rigorous evaluation and cautious, ethically-grounded implementation - not merely technological advancement.
- Telemedicine: Real-time communication platforms between field crews and PCI centers reduce diagnostic uncertainty and optimize preparation [2,16,27]. Fifth-generation cellular technology provides the critical infrastructure for advanced mobile healthcare, offering robust communication pipeline which transforms ambulances into mobile diagnostic hubs, enabling high-definition video consultations and seamless transmission of large data files from paramedic-performed ultrasounds [131]. The technology allows expert-level clinical decision-making to begin at the patient’s bedside [132].
Wearable-based MI prediction: While consumer smartwatches and other wearables demonstrate efficacy in detecting arrhythmias such as atrial fibrillation, their application for acute MI diagnosis remains unvalidated and confronts substantial technical limitations, including inadequate signal quality and the absence of 12-lead ECG equivalency [133]. In the immediate future, these devices will likely serve primarily in long-term cardiovascular risk stratification and preliminary abnormality detection for subsequent clinical evaluation, rather than functioning as primary diagnostic instruments for acute STEMI [130,133].
Re-evaluating prehospital pharmacotherapy: Routine prehospital administration of P2Y12 inhibitors (“pretreatment”) has been largely discontinued following disappointing trial results [1,2]. Current 2024 ESC and 2025 AHA/ACC guidelines reflect this clinical shift by recommending dual antiplatelet therapy without mandating prehospital initiation [1,2]. However, a new subcutaneous GP IIb-IIIa inhibitor (zalunfiban) has shown promising initial results and is currently being tested as a facilitation strategy in a large randomized trial [134]. This development may prove valuable in accelerating treatment for STEMI patients and reducing reperfusion delays in the coming years. Another, possibility might be administration of agents mitigating ischemia/reperfusion injury [135]. Future research will likely emphasize selective, individualized approaches rather than universal pretreatment protocols.
6.2. System Evolution
Future STEMI care requires fully integrated regional “chains of survival” functioning as coordinated units from 1-1-2 / 9-1-1 call to reperfusion [1,2,136]. The “Stent - Save a Life!” initiative outlines a systematic approach for network development, defining implementation phases [27]:
- Preparation: Establish task force and action plan with regional stakeholders
- Mapping: Identify PCI/non-PCI centers, assess transport times, confirm EMS availability
- Building: Assign roles based on available resources and network type
- Quality Assessment: Monitor key performance indicators continuously
Essential network characteristics include 24/7 service availability, structured cooperation following standardized protocols, regular stakeholder meetings, and continuous self-assessment [2,16,27]. Sustaining performance demands transparent auditing and feedback on metrics including presentation timing, treatment rates, procedural success, and mortality.
6.3. Research Priorities
- Optimal timing for pharmaco-invasive PCI (2-24 hour window) and new subcutaneaous upstream antithrombotic therapies
- Effective public awareness campaign design
- Targeted interventions for persistent disparities
- Prospective validation of AI technologies
7. Conclusions
The evidence unequivocally demonstrates that in acute coronary occlusion, time equals myocardium. Every minute from symptom onset to reperfusion increases mortality, infarct size, and heart failure risk - whether patients present with classic STEMI or other OMI patterns. The emerging OMI paradigm reveals that 25-34% of patients with acute coronary occlusion are missed by traditional STEMI criteria, experiencing systematic treatment delays despite similar pathophysiology and outcomes. While system-based approaches have achieved remarkable improvements through regional networks, pre-hospital protocols, and standardized hospital processes, significant challenges persist. These challenges encompass variable patient delays, failure to recognize the full spectrum of acute coronary occlusion, and profound care disparities driven by geography, demographics, and socioeconomic factors - particularly in low- and middle-income countries. AI-based ECG interpretation capable of detecting the complete range of OMI patterns offers a promising pathway to ensure timely reperfusion for all patients with acute coronary occlusion. The battle against time in STEMI requires coordinated, evidence-based, equitable care extending from patient’s home to catheterization laboratory. By targeting each delay source with proven interventions (Table 4), the medical community can continue improving survival and preserving quality of life for patients experiencing this devastating emergency.
Author Contributions
Conceptualization, A.D. and T.R.; writing—original draft preparation, A.D. and T.R.; writing—review and editing, A.D., B.Z., W.W. and D.L.G.; visualization, A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Acknowledgments
None
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACC | American College of Cardiology |
| AHA | American Heart Association |
| AI | Artificial intelligence |
| ED | Emergency department |
| ECG | Electrocardiogram |
| EMS | Emergency medical services |
| ESC | European Society of Cardiology |
| FMC | First medical contact |
| GP | Glycoprotein |
| MI | Myocardial infarction |
| NOMI | Non-occlusion myocardial infarction |
| NSTEMI | Non-ST-segment elevation myocardial infarction |
| OMI | Occlusion myocardial infarction |
| PCI | Percutaneous coronary intervention |
| PPCI | Primary percutaneous coronary intervention |
| SCAI | Society for Cardiovascular Angiography and Interventions |
| STEMI | ST-segment elevation myocardial infarction |
| TIMI | Thrombolysis In Myocardial Infarction (flow grade) |
References
- Rao, S.V.; O’Donoghue, M.L.; Ruel, M.; Rab, T.; Tamis-Holland, J.E.; Alexander, J.H.; Baber, U.; Baker, H.; Cohen, M.G.; Cruz-Ruiz, M.; et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2025, 151, e771–e862. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, T.; West, N.E.; El-Omar, M. ST Elevation Myocardial Infarction. Clin. Med. Lond. Engl. 2016, 16, 277–282. [Google Scholar] [CrossRef]
- Reimer, K.A.; Lowe, J.E.; Rasmussen, M.M.; Jennings, R.B. The Wavefront Phenomenon of Ischemic Cell Death. 1. Myocardial Infarct Size vs Duration of Coronary Occlusion in Dogs. Circulation 1977, 56, 786–794. [Google Scholar] [CrossRef]
- Maroko, P.R. Editorial: Assessing Myocardial Damage in Acute Infarcts. N. Engl. J. Med. 1974, 290, 158–159. [Google Scholar] [CrossRef]
- De Luca, G.; Brener, S.J.; Mehran, R.; Lansky, A.J.; McLaurin, B.T.; Cox, D.A.; Cristea, E.; Fahy, M.; Stone, G.W. Implications of Pre-Procedural TIMI Flow in Patients with Non ST-Segment Elevation Acute Coronary Syndromes Undergoing Percutaneous Coronary Revascularization: Insights from the ACUITY Trial. Int. J. Cardiol. 2013, 167, 727–732. [Google Scholar] [CrossRef]
- Ayyad, M.; Albandak, M.; Gala, D.; Alqeeq, B.; Baniowda, M.; Pally, J.; Allencherril, J. Reevaluating STEMI: The Utility of the Occlusive Myocardial Infarction Classification to Enhance Management of Acute Coronary Syndromes. Curr. Cardiol. Rep. 2025, 27, 75. [Google Scholar] [CrossRef]
- Frick, W.H.; McLaren, J.T.T.; Meyers, H.P.; Smith, S.W. Occlusion Myocardial Infarction: A Revolution in Acute Coronary Syndrome. Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2025, 21, 139–143. [Google Scholar] [CrossRef]
- McLaren, J.; de Alencar, J.N.; Aslanger, E.K.; Meyers, H.P.; Smith, S.W. From ST-Segment Elevation MI to Occlusion MI: The New Paradigm Shift in Acute Myocardial Infarction. JACC Adv. 2024, 3, 101314. [Google Scholar] [CrossRef]
- Khan, A.R.; Golwala, H.; Tripathi, A.; Bin Abdulhak, A.A.; Bavishi, C.; Riaz, H.; Mallipedi, V.; Pandey, A.; Bhatt, D.L. Impact of Total Occlusion of Culprit Artery in Acute Non-ST Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis. Eur. Heart J. 2017, 38, 3082–3089. [Google Scholar] [CrossRef] [PubMed]
- Gołąbek, N.; Jakubowski, W.; Król, S.; Kozioł, M.; Niewiara, Ł.; Kleczyński, P.; Legutko, J.; Dziewierz, A.; Surdacki, A.; Chyrchel, M. ECG Patterns Suggestive of High-Risk Coronary Anatomy in Non-ST-Segment Elevation Acute Coronary Syndrome – an Analysis of Real-World Patients. Adv. Interv. Cardiol. 2023, 19, 326–332. [Google Scholar] [CrossRef]
- Trzeciak, P.; Tajstra, M.; Wojakowski, W.; Cieśla, D.; Kalarus, Z.; Milewski, K.; Hrapkowicz, T.; Mizia-Stec, K.; Smolka, G.; Nadolny, K.; et al. Temporal Trends in In-Hospital Mortality of 7 628 Patients with Myocardial Infarction Complicated by Cardiogenic Shock Treated in the Years 2006–2021. An Analysis from the SILCARD Database. Pol. Heart J. 2024. [Google Scholar] [CrossRef]
- Leader, J.H.; Kanji, R.; Gorog, D.A. Spontaneous Reperfusion in STEMI: Its Mechanisms and Possible Modulation. Pol. Heart J. 2024, 82, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.C.; Ahn, Y. False Positive ST-Segment Elevation Myocardial Infarction. Korean Circ. J. 2013, 43, 368–369. [Google Scholar] [CrossRef] [PubMed]
- Zalas, K.; Kuliczkowski, W.; Pachana, J.; Mycka, R.; Rakoczy, B. Is ST-Segment Elevation Myocardial Infarction Always a Simple Diagnosis? Adv. Interv. Cardiol. 2023, 19, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.V. The 2025 American College of Cardiology/American Heart Association Acute Coronary Syndrome Guideline: A Personal Perspective. J. Am. Coll. Cardiol. 2025, 85, 2068–2070. [Google Scholar] [CrossRef]
- Silvain, J.; Rakowski, T.; Lattuca, B.; Liu, Z.; Bolognese, L.; Goldstein, P.; Hamm, C.; Tanguay, J.-F.; Ten Berg, J.; Widimsky, P.; et al. Interval From Initiation of Prasugrel to Coronary Angiography in Patients With Non–ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 906–914. [Google Scholar] [CrossRef]
- Dziewierz, A.; De Luca, G.; Rakowski, T. Every Minute of Delay (Still) Counts! Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2025, 21, 1–3. [Google Scholar] [CrossRef]
- Maroko, P.R.; Kjekshus, J.K.; Sobel, B.E.; Watanabe, T.; Covell, J.W.; Ross, J.; Braunwald, E. Factors Influencing Infarct Size Following Experimental Coronary Artery Occlusions. Circulation 1971, 43, 67–82. [Google Scholar] [CrossRef]
- Windecker, S.; Bax, J.J.; Myat, A.; Stone, G.W.; Marber, M.S. Future Treatment Strategies in ST-Segment Elevation Myocardial Infarction. The Lancet 2013, 382, 644–657. [Google Scholar] [CrossRef]
- Siudak, Z.; Hawranek, M.; Kleczyński, P.; Bartuś, S.; Kusa, J.; Milewski, K.; Opolski, M.P.; Pawłowski, T.; Protasiewicz, M.; Smolka, G.; et al. Interventional Cardiology in Poland in 2022. Annual Summary Report of the Association of Cardiovascular Interventions of the Polish Cardiac Society (AISN PTK) and Jagiellonian University Medical College. Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2023, 19, 82–85. [Google Scholar] [CrossRef]
- Riehle, L.; Gothe, R.M.; Ebbinghaus, J.; Maier, B.; Bruch, L.; Röhnisch, J.-U.; Schühlen, H.; Fried, A.; Stockburger, M.; Theres, H.; et al. Implementation of the ESC STEMI Guidelines in Female and Elderly Patients over a 20-Year Period in a Large German Registry. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2023, 112, 1240–1251. [Google Scholar] [CrossRef]
- Siudak, Z.; Grygier, M.; Tomaniak, M.; Kałużna-Oleksy, M.; Kleczyński, P.; Milewski, K.; Opolski, M.P.; Smolka, G.; Sabiniewicz, R.; Malinowski, K.P.; et al. Interventional Cardiology in Poland in 2023. Annual Summary Report of the Association of Cardiovascular Interventions of the Polish Cardiac Society (AISN PTK) and Jagiellonian University Medical College. Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2024, 20, 379–381. [Google Scholar] [CrossRef]
- Lee, S.H.; Hong, Y.J.; Ahn, Y.; Jeong, M.H. Past, Present, and Future of Management of Acute Myocardial Infarction. J. Cardiovasc. Interv. 2023, 2, 51. [Google Scholar] [CrossRef]
- White, H.D.; Van De Werf, F.J.J. Thrombolysis for Acute Myocardial Infarction. Circulation 1998, 97, 1632–1646. [Google Scholar] [CrossRef] [PubMed]
- Keeley, E.C.; Boura, J.A.; Grines, C.L. Primary Angioplasty versus Intravenous Thrombolytic Therapy for Acute Myocardial Infarction: A Quantitative Review of 23 Randomised Trials. Lancet Lond. Engl. 2003, 361, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Candiello, A.; Alexander, T.; Delport, R.; Toth, G.G.; Ong, P.; Snyders, A.; Belardi, J.A.; Lee, M.K.Y.; Pereira, H.; Mohamed, A.; et al. How to Set up Regional STEMI Networks: A “Stent - Save a Life!” Initiative. EuroIntervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2022, 17, 1313–1317. [Google Scholar] [CrossRef]
- Kleczyński, P.; Siudak, Z.; Dziewierz, A.; Tokarek, T.; Rakowski, T.; Legutko, J.; Bartuś, S.; Dudek, D. The Network of Invasive Cardiology Facilities in Poland in 2016 (Data from the ORPKI Polish National Registry). Kardiol. Pol. 2018, 76, 805–807. [Google Scholar] [CrossRef]
- Januś, B.; Rakowski, T.; Dziewierz, A.; Fijorek, K.; Sokołowski, A.; Dudek, D. Effect of Introducing a Regional 24/7 Primary Percutaneous Coronary Intervention Service Network on Treatment Outcomes in Patients with ST Segment Elevation Myocardial Infarction. Kardiol. Pol. 2015, 73, 323–330. [Google Scholar] [CrossRef]
- Dudek, D.; Dziewierz, A.; Siudak, Z.; Rakowski, T.; Zalewski, J.; Legutko, J.; Mielecki, W.; Janion, M.; Bartus, S.; Kuta, M.; et al. Transportation with Very Long Transfer Delays (>90 Min) for Facilitated PCI with Reduced-Dose Fibrinolysis in Patients with ST-Segment Elevation Myocardial Infarction. Int. J. Cardiol. 2010, 139, 218–227. [Google Scholar] [CrossRef]
- Bertero, E.; Popoiu, T.-A.; Maack, C. Mitochondrial Calcium in Cardiac Ischemia/Reperfusion Injury and Cardioprotection. Basic Res. Cardiol. 2024, 119, 569–585. [Google Scholar] [CrossRef]
- Fröhlich, G.M.; Meier, P.; White, S.K.; Yellon, D.M.; Hausenloy, D.J. Myocardial Reperfusion Injury: Looking beyond Primary PCI. Eur. Heart J. 2013, 34, 1714–1722. [Google Scholar] [CrossRef]
- Mackay, M.H.; Chruscicki, A.; Christenson, J.; Cairns, J.A.; Lee, T.; Turgeon, R.; Tallon, J.M.; Helmer, J.; Singer, J.; Wong, G.C.; et al. Association of Pre-Hospital Time Intervals and Clinical Outcomes in ST-Elevation Myocardial Infarction Patients. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12764. [Google Scholar] [CrossRef]
- O’Connor, C.T.; Ibrahim, A.; Buckley, A.; Maguire, C.; Kumar, R.; Kumar, J.; Arnous, S.; Kiernan, T.J. Total Ischaemic Time in STEMI: Factors Influencing Systemic Delay. Br. J. Cardiol. 2022, 29, 17. [Google Scholar] [CrossRef]
- Rawles, J.M.; Metcalfe, M.J.; Shirreffs, C.; Jennings, K.; Kenmure, A.C. Association of Patient Delay with Symptoms, Cardiac Enzymes, and Outcome in Acute Myocardial Infarction. Eur. Heart J. 1990, 11, 643–648. [Google Scholar] [CrossRef]
- Dziewierz, A.; Rakowski, T.; Mamas, M.A.; Tkaczyk, F.; Sowa, Ł.; Malinowski, K.P.; Olszanecka, A.; Siudak, Z. Impact of Historical Partitions of Poland on Reperfusion Delay in Patients with ST-Segment Elevation Myocardial Infarction Referred for Primary Percutaneous Coronary Intervention (from the ORPKI Registry). Pol. Arch. Intern. Med. 2024, 134, 16793. [Google Scholar] [CrossRef] [PubMed]
- Rivero, F.; Bastante, T.; Cuesta, J.; Benedicto, A.; Salamanca, J.; Restrepo, J.-A.; Aguilar, R.; Gordo, F.; Batlle, M.; Alfonso, F. Factors Associated With Delays in Seeking Medical Attention in Patients With ST-Segment Elevation Acute Coronary Syndrome. Rev. Espanola Cardiol. Engl. Ed 2016, 69, 279–285. [Google Scholar] [CrossRef]
- Qian, L.; Ji, K.; Nan, J.; Lu, Q.; Zhu, Y.; Wang, L.; Liao, L.; Tang, J. Factors Associated with Decision Time for Patients with ST-Segment Elevation Acute Myocardial Infarction. J. Zhejiang Univ. Sci. B 2013, 14, 754–758. [Google Scholar] [CrossRef]
- Khraim, F.M.; Carey, M.G. Predictors of Pre-Hospital Delay among Patients with Acute Myocardial Infarction. Patient Educ. Couns. 2009, 75, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Beig, J.R.; Tramboo, N.A.; Kumar, K.; Yaqoob, I.; Hafeez, I.; Rather, F.A.; Shah, T.R.; Rather, H.A. Components and Determinants of Therapeutic Delay in Patients with Acute ST-Elevation Myocardial Infarction: A Tertiary Care Hospital-Based Study. J. Saudi Heart Assoc. 2017, 29, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, A.K.; Ali, M.J.; Best, P.J.; Bieniarz, M.C.; Bufalino, V.J.; French, W.J.; Henry, T.D.; Hollowell, L.; Jauch, E.C.; Kurz, M.C.; et al. Systems of Care for ST-Segment–Elevation Myocardial Infarction: A Policy Statement From the American Heart Association. Circulation 2021, 144. [Google Scholar] [CrossRef]
- Studnek, J.R.; Garvey, L.; Blackwell, T.; Vandeventer, S.; Ward, S.R. Association Between Prehospital Time Intervals and ST-Elevation Myocardial Infarction System Performance. Circulation 2010, 122, 1464–1469. [Google Scholar] [CrossRef]
- Miedema, M.D.; Newell, M.C.; Duval, S.; Garberich, R.F.; Handran, C.B.; Larson, D.M.; Mulder, S.; Wang, Y.L.; Lips, D.L.; Henry, T.D. Causes of Delay and Associated Mortality in Patients Transferred With ST-Segment–Elevation Myocardial Infarction. Circulation 2011, 124, 1636–1644. [Google Scholar] [CrossRef]
- De Luca, G.; Ernst, N.; Suryapranata, H.; Ottervanger, J.P.; Hoorntje, J.C.A.; Gosselink, A.T.M.; Dambrink, J.-H.; de Boer, M.-J.; van ’t Hof, A.W.J. Relation of Interhospital Delay and Mortality in Patients with ST-Segment Elevation Myocardial Infarction Transferred for Primary Coronary Angioplasty. Am. J. Cardiol. 2005, 95, 1361–1363. [Google Scholar] [CrossRef] [PubMed]
- McCabe, J.M.; Armstrong, E.J.; Hoffmayer, K.S.; Bhave, P.D.; MacGregor, J.S.; Hsue, P.; Stein, J.C.; Kinlay, S.; Ganz, P. Impact of Door-to-Activation Time on Door-to-Balloon Time in Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarctions: A Report from the Activate-SF Registry. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.-T.; Hung, J.-F.; Zhang, S.-Q.; Yeh, Y.-N.; Tsai, M.-J. The Impact of Emergency Department Arrival Time on Door-to-Balloon Time in Patients with ST-Segment Elevation Myocardial Infarction Receiving Primary Percutaneous Coronary Intervention. J. Clin. Med. 2023, 12, 2392. [Google Scholar] [CrossRef] [PubMed]
- Tokarek, T.; Dziewierz, A.; Plens, K.; Rakowski, T.; Jaroszyńska, A.; Bartuś, S.; Siudak, Z. Percutaneous Coronary Intervention during On- and off-Hours in Patients with ST-Segment Elevation Myocardial Infarction. Hell. J. Cardiol. HJC Hell. Kardiologike Epitheorese 2021, 62, 212–218. [Google Scholar] [CrossRef]
- Menees, D.S.; Peterson, E.D.; Wang, Y.; Curtis, J.P.; Messenger, J.C.; Rumsfeld, J.S.; Gurm, H.S. Door-to-Balloon Time and Mortality among Patients Undergoing Primary PCI. N. Engl. J. Med. 2013, 369, 901–909. [Google Scholar] [CrossRef]
- Rathore, S.S.; Curtis, J.P.; Chen, J.; Wang, Y.; Nallamothu, B.K.; Epstein, A.J.; Krumholz, H.M. ; National Cardiovascular Data Registry Association of Door-to-Balloon Time and Mortality in Patients Admitted to Hospital with ST Elevation Myocardial Infarction: National Cohort Study. BMJ 2009, 338, b1807. [Google Scholar] [CrossRef]
- Bychowski, J.; Michalski, T.; Bachorski, W.; Jaguszewski, M.; Gruchała, M. Treatment Delays and In-Hospital Outcomes in Patients with ST-Segment Elevation Myocardial Infarction from the Tertiary Center in Poland. Pol. Arch. Intern. Med. 2024. [Google Scholar] [CrossRef]
- Tokarek, T.; Dziewierz, A.; Malinowski, K.P.; Rakowski, T.; Bartuś, S.; Dudek, D.; Siudak, Z. Treatment Delay and Clinical Outcomes in Patients with ST-Segment Elevation Myocardial Infarction during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 3920. [Google Scholar] [CrossRef]
- Armstrong, P.W.; Gershlick, A.H.; Goldstein, P.; Wilcox, R.; Danays, T.; Lambert, Y.; Sulimov, V.; Rosell Ortiz, F.; Ostojic, M.; Welsh, R.C.; et al. Fibrinolysis or Primary PCI in ST-Segment Elevation Myocardial Infarction. N. Engl. J. Med. 2013, 368, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Lassen, J.F.; Bøtker, H.E.; Terkelsen, C.J. Timely and Optimal Treatment of Patients with STEMI. Nat. Rev. Cardiol. 2013, 10, 41–48. [Google Scholar] [CrossRef]
- Boersma, E.; Primary Coronary Angioplasty, vs. Thrombolysis Group Does Time Matter? A Pooled Analysis of Randomized Clinical Trials Comparing Primary Percutaneous Coronary Intervention and in-Hospital Fibrinolysis in Acute Myocardial Infarction Patients. Eur. Heart J. 2006, 27, 779–788. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Cassetti, E.; Marino, P. Percutaneous Coronary Intervention-Related Time Delay, Patient’s Risk Profile, and Survival Benefits of Primary Angioplasty vs Lytic Therapy in ST-Segment Elevation Myocardial Infarction. Am. J. Emerg. Med. 2009, 27, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.J.; Swinford, R.D.; Gadde, P.; Lillis, O. Acute Effects of Delayed Reperfusion on Myocardial Infarct Shape and Left Ventricular Volume: A Potential Mechanism of Additional Benefits from Thrombolytic Therapy. J. Am. Coll. Cardiol. 1991, 17, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Bucciarelli-Ducci, C.; Carbone, I.; Canali, E.; Scardala, R.; Calabrese, F.A.; Sardella, G.; Mancone, M.; Catalano, C.; Fedele, F.; et al. Impact of Primary Coronary Angioplasty Delay on Myocardial Salvage, Infarct Size, and Microvascular Damage in Patients with ST-Segment Elevation Myocardial Infarction: Insight from Cardiovascular Magnetic Resonance. J. Am. Coll. Cardiol. 2009, 54, 2145–2153. [Google Scholar] [CrossRef]
- Smalling, R.W. Ischemic Time: The New Gold Standard for ST-Segment Elevation Myocardial Infarction Care. J. Am. Coll. Cardiol. 2009, 54, 2154–2156. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Ma, Q.; Jiao, Y.; Wu, J.; Yu, T.; Hou, Y.; Sun, Z.; Zheng, L.; Sun, Z. Prognostic Value of Myocardial Salvage Index Assessed by Cardiovascular Magnetic Resonance in Reperfused ST-Segment Elevation Myocardial Infarction. Front. Cardiovasc. Med. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Redfors, B.; Mohebi, R.; Giustino, G.; Chen, S.; Selker, H.P.; Thiele, H.; Patel, M.R.; Udelson, J.E.; Ohman, E.M.; Eitel, I.; et al. Time Delay, Infarct Size, and Microvascular Obstruction After Primary Percutaneous Coronary Intervention for ST-Segment–Elevation Myocardial Infarction. Circ. Cardiovasc. Interv. 2021, 14. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Ottervanger, J.P.; Antman, E.M. Time Delay to Treatment and Mortality in Primary Angioplasty for Acute Myocardial Infarction: Every Minute of Delay Counts. Circulation 2004, 109, 1223–1225. [Google Scholar] [CrossRef]
- Lazar, M.; Francuz, P.; Podolecki, T.; Kowalczyk, J.; Mitręga, K.; Olma, A.; Kalarus, Z.; Streb, W. Predictive Factors of Left Ventricular Ejection Fraction Improvement after Myocardial Infarction Treated Invasively. Adv. Interv. Cardiol. 2023, 19, 225–232. [Google Scholar] [CrossRef]
- Węgiel, M.; Surmiak, M.; Malinowski, K.P.; Dziewierz, A.; Surdacki, A.; Bartuś, S.; Rakowski, T. In-Hospital Levels of Circulating MicroRNAs as Potential Predictors of Left Ventricular Remodeling Post-Myocardial Infarction. Med. Kaunas Lith. 2024, 60, 149. [Google Scholar] [CrossRef]
- Galli, A.; Lombardi, F. Postinfarct Left Ventricular Remodelling: A Prevailing Cause of Heart Failure. Cardiol. Res. Pract. 2016, 2016, 2579832. [Google Scholar] [CrossRef] [PubMed]
- Nepper-Christensen, L.; Lønborg, J.; Høfsten, D.E.; Sadjadieh, G.; Schoos, M.M.; Pedersen, F.; Jørgensen, E.; Kelbæk, H.; Haahr-Pedersen, S.; Flensted Lassen, J.; et al. Clinical Outcome Following Late Reperfusion with Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Uleberg, B.; Bønaa, K.H.; Halle, K.K.; Jacobsen, B.K.; Hauglann, B.; Stensland, E.; Førde, O.H. The Relation between Delayed Reperfusion Treatment and Reduced Left Ventricular Ejection Fraction in Patients with ST-Segment Elevation Myocardial Infarction: A National Prospective Cohort Study. Eur. Heart J. Open 2025, 5. [Google Scholar] [CrossRef]
- Van Diepen, S.; Zheng, Y.; Senaratne, J.M.; Tyrrell, B.D.; Das, D.; Thiele, H.; Henry, T.D.; Bainey, K.R.; Welsh, R.C. Reperfusion in Patients With ST-Segment–Elevation Myocardial Infarction With Cardiogenic Shock and Prolonged Interhospital Transport Times. Circ. Cardiovasc. Interv. 2024, 17. [Google Scholar] [CrossRef]
- Kochan, A.; Lee, T.; Moghaddam, N.; Milley, G.; Singer, J.; Cairns, J.A.; Wong, G.C.; Jentzer, J.C.; Van Diepen, S.; Alviar, C.; et al. Reperfusion Delays and Outcomes Among Patients With ST-Segment–Elevation Myocardial Infarction With and Without Cardiogenic Shock. Circ. Cardiovasc. Interv. 2023, 16. [Google Scholar] [CrossRef]
- Odongo, M. Health Communication Campaigns and Their Impact on Public Health Behaviors. J. Commun. 2024, 5, 55–69. [Google Scholar] [CrossRef]
- Bray, J.E.; Stub, D.; Ngu, P.; Cartledge, S.; Straney, L.; Stewart, M.; Keech, W.; Patsamanis, H.; Shaw, J.; Finn, J. Mass Media Campaigns’ Influence on Prehospital Behavior for Acute Coronary Syndromes: An Evaluation of the Australian Heart Foundation’s Warning Signs Campaign. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Moxham, R.N.; d’Entremont, M.-A.; Mir, H.; Schwalm, J.; Natarajan, M.K.; Jolly, S.S. Effect of Prehospital Digital Electrocardiogram Transmission on Revascularization Delays and Mortality in ST-Elevation Myocardial Infarction Patients: Systematic Review and Meta-Analysis. CJC Open 2024, 6, 1199–1206. [Google Scholar] [CrossRef]
- Ortolani, P.; Marzocchi, A.; Marrozzini, C.; Palmerini, T.; Saia, F.; Taglieri, N.; Alessi, L.; Nardini, P.; Bacchi Reggiani, M.-L.; Guastaroba, P.; et al. Pre-Hospital ECG in Patients Undergoing Primary Percutaneous Interventions within an Integrated System of Care: Reperfusion Times and Long-Term Survival Benefits. EuroIntervention 2011, 7, 449–457. [Google Scholar] [CrossRef]
- Guagliumi, G. Emerging Data and Decision for Optimizing STEMI Management: The European Perspective. Eur. Heart J. Suppl. 2009, 11, C19–C24. [Google Scholar] [CrossRef]
- Bagai, A.; Al-Khalidi, H.R.; Muñoz, D.; Monk, L.; Roettig, M.L.; Corbett, C.C.; Garvey, J.L.; Wilson, B.H.; Granger, C.B.; Jollis, J.G. Bypassing the Emergency Department and Time to Reperfusion in Patients With Prehospital ST-Segment–Elevation: Findings From the Reperfusion in Acute Myocardial Infarction in Carolina Emergency Departments Project. Circ. Cardiovasc. Interv. 2013, 6, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Le May, M.R.; Wells, G.A.; So, D.Y.; Glover, C.A.; Froeschl, M.; Maloney, J.; Dionne, R.; Marquis, J.-F.; O’Brien, E.R.; Dick, A.; et al. Reduction in Mortality as a Result of Direct Transport From the Field to a Receiving Center for Primary Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2012, 60, 1223–1230. [Google Scholar] [CrossRef]
- Alyahya, A.A.; Alghammass, M.A.; Aldhahri, F.S.; Alsebti, A.A.; Alfulaij, A.Y.; Alrashed, S.H.; Faleh, H.A.; Alshameri, M.; Alhabib, K.; Arafah, M.; et al. The Impact of Introduction of Code-STEMI Program on the Reduction of Door-to-Balloon Time in Acute ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention: A Single-Center Study in Saudi Arabia. J. Saudi Heart Assoc. 2018, 30, 172–179. [Google Scholar] [CrossRef]
- Ginanjar, E.; Sjaaf, A.C.; Alwi, I.; Sulistiadi, W.; Suryadarmawan, E.; Wibowo, A.; Liastuti, L.D. CODE STEMI Program Improves Clinical Outcome in ST Elevation Myocardial Infarction Patients: A Retrospective Cohort Study. Open Access Emerg. Med. 2020, Volume 12, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.Q.; Tong, D.C.; Sriamareswaran, R.; Yeap, A.; Yip, B.; Wu, S.; Perera, P.; Menon, S.; Noaman, S.A.; Layland, J. In-hospital ‘CODE STEMI’ Improves Door-to-balloon Time in Patients Undergoing Primary Percutaneous Coronary Intervention. Emerg. Med. Australas. 2018, 30, 222–227. [Google Scholar] [CrossRef]
- Di Pasquale, G. The Avoidable Delay in the Care of STEMI Patients Is Still a Priority Issue. IJC Heart Vasc. 2022, 39, 101011. [Google Scholar] [CrossRef] [PubMed]
- Fazel, R.; Joseph, T.I.; Sankardas, M.A.; Pinto, D.S.; Yeh, R.W.; Kumbhani, D.J.; Nallamothu, B.K. Comparison of Reperfusion Strategies for ST-Segment–Elevation Myocardial Infarction: A Multivariate Network Meta-analysis. J. Am. Heart Assoc. 2020, 9. [Google Scholar] [CrossRef]
- Jortveit, J.; Pripp, A.H.; Halvorsen, S. Outcomes after Delayed Primary Percutaneous Coronary Intervention vs. Pharmaco-Invasive Strategy in ST-Segment Elevation Myocardial Infarction in Norway. Eur. Heart J. - Cardiovasc. Pharmacother. 2022, 8, 442–451. [Google Scholar] [CrossRef]
- De Luca, G.; Gibson, C.M.; Bellandi, F.; Murphy, S.; Maioli, M.; Noc, M.; Zeymer, U.; Dudek, D.; Arntz, H.-R.; Zorman, S.; et al. Early Glycoprotein IIb-IIIa Inhibitors in Primary Angioplasty (EGYPT) Cooperation: An Individual Patient Data Meta-Analysis. Heart Br. Card. Soc. 2008, 94, 1548–1558. [Google Scholar] [CrossRef] [PubMed]
- DE Luca, G.; Bellandi, F.; Huber, K.; Noc, M.; Petronio, A.S.; Arntz, H.-R.; Maioli, M.; Gabriel, H.M.; Zorman, S.; DE Carlo, M.; et al. Early Glycoprotein IIb-IIIa Inhibitors in Primary Angioplasty-Abciximab Long-Term Results (EGYPT-ALT) Cooperation: Individual Patient’s Data Meta-Analysis. J. Thromb. Haemost. JTH 2011, 9, 2361–2370. [Google Scholar] [CrossRef]
- Van’t Hof, A.W.J.; Ten Berg, J.; Heestermans, T.; Dill, T.; Funck, R.C.; van Werkum, W.; Dambrink, J.-H.E.; Suryapranata, H.; van Houwelingen, G.; Ottervanger, J.P.; et al. Prehospital Initiation of Tirofiban in Patients with ST-Elevation Myocardial Infarction Undergoing Primary Angioplasty (On-TIME 2): A Multicentre, Double-Blind, Randomised Controlled Trial. Lancet Lond. Engl. 2008, 372, 537–546. [Google Scholar] [CrossRef] [PubMed]
- ten Berg, J.M.; van ’t Hof, A.W.J.; Dill, T.; Heestermans, T.; van Werkum, J.W.; Mosterd, A.; van Houwelingen, G.; Koopmans, P.C.; Stella, P.R.; Boersma, E.; et al. Effect of Early, Pre-Hospital Initiation of High Bolus Dose Tirofiban in Patients with ST-Segment Elevation Myocardial Infarction on Short- and Long-Term Clinical Outcome. J. Am. Coll. Cardiol. 2010, 55, 2446–2455. [Google Scholar] [CrossRef] [PubMed]
- Huber, K.; Holmes, D.R.; van ’t Hof, A.W.; Montalescot, G.; Aylward, P.E.; Betriu, G.A.; Widimsky, P.; Westerhout, C.M.; Granger, C.B.; Armstrong, P.W. Use of Glycoprotein IIb/IIIa Inhibitors in Primary Percutaneous Coronary Intervention: Insights from the APEX-AMI Trial. Eur. Heart J. 2010, 31, 1708–1716. [Google Scholar] [CrossRef]
- Dudek, D.; Siudak, Z.; Janzon, M.; Birkemeyer, R.; Aldama-Lopez, G.; Lettieri, C.; Janus, B.; Wisniewski, A.; Berti, S.; Olivari, Z.; et al. European Registry on Patients with ST-Elevation Myocardial Infarction Transferred for Mechanical Reperfusion with a Special Focus on Early Administration of Abciximab -- EUROTRANSFER Registry. Am. Heart J. 2008, 156, 1147–1154. [Google Scholar] [CrossRef]
- Ellis, S.G.; Tendera, M.; de Belder, M.A.; van Boven, A.J.; Widimsky, P.; Janssens, L.; Andersen, H.R.; Betriu, A.; Savonitto, S.; Adamus, J.; et al. Facilitated PCI in Patients with ST-Elevation Myocardial Infarction. N. Engl. J. Med. 2008, 358, 2205–2217. [Google Scholar] [CrossRef]
- Ellis, S.G.; Tendera, M.; de Belder, M.A.; van Boven, A.J.; Widimsky, P.; Andersen, H.R.; Betriu, A.; Savonitto, S.; Adamus, J.; Peruga, J.Z.; et al. 1-Year Survival in a Randomized Trial of Facilitated Reperfusion: Results from the FINESSE (Facilitated Intervention with Enhanced Reperfusion Speed to Stop Events) Trial. JACC Cardiovasc. Interv. 2009, 2, 909–916. [Google Scholar] [CrossRef]
- Herrmann, H.C.; Lu, J.; Brodie, B.R.; Armstrong, P.W.; Montalescot, G.; Betriu, A.; Neuman, F.-J.; Effron, M.B.; Barnathan, E.S.; Topol, E.J.; et al. Benefit of Facilitated Percutaneous Coronary Intervention in High-Risk ST-Segment Elevation Myocardial Infarction Patients Presenting to Nonpercutaneous Coronary Intervention Hospitals. JACC Cardiovasc. Interv. 2009, 2, 917–924. [Google Scholar] [CrossRef]
- Schoos, M.M.; De Luca, G.; Dangas, G.D.; Clemmensen, P.; Ayele, G.M.; Mehran, R.; Stone, G.W. Impact of Time to Treatment on the Effects of Bivalirudin vs. Glycoprotein IIb/IIIa Inhibitors and Heparin in Patients Undergoing Primary Percutaneous Coronary Intervention: Insights from the HORIZONS-AMI Trial. EuroIntervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2016, 12, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Heestermans, T.; de Boer, M.-J.; van Werkum, J.W.; Mosterd, A.; Gosselink, A.T.M.; Dambrink, J.-H.E.; van Houwelingen, G.; Koopmans, P.; Hamm, C.; Zijlstra, F.; et al. Higher Efficacy of Pre-Hospital Tirofiban with Longer Pre-Treatment Time to Primary PCI: Protection for the Negative Impact of Time Delay. EuroIntervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2011, 7, 442–448. [Google Scholar] [CrossRef]
- Bor, W.L.; Zheng, K.L.; Tavenier, A.H.; Gibson, C.M.; Granger, C.B.; Bentur, O.; Lobatto, R.; Postma, S.; Coller, B.S.; van ’t Hof, A.W.J.; et al. Pharmacokinetics, Pharmacodynamics, and Tolerability of Subcutaneous Administration of a Novel Glycoprotein IIb/IIIa Inhibitor, RUC-4, in Patients with ST-Segment Elevation Myocardial Infarction. EuroIntervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2021, 17, e401–e410. [Google Scholar] [CrossRef]
- Bentur, O.S.; Li, J.; Jiang, C.S.; Martin, L.H.; Kereiakes, D.J.; Coller, B.S. Application of Auxiliary VerifyNow Point-of-Care Assays to Assess the Pharmacodynamics of RUC-4, a Novel αIIbβ3 Receptor Antagonist. TH Open Companion J. Thromb. Haemost. 2021, 5, e449–e460. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Henry, T.D.; DeMaria, A.N.; Bentur, O.; Carlson, M.; Seng Yue, C.; Martin, L.H.; Midkiff, J.; Mueller, M.; Meek, T.; et al. First Human Use of RUC-4: A Nonactivating Second-Generation Small-Molecule Platelet Glycoprotein IIb/IIIa (Integrin αIIbβ3) Inhibitor Designed for Subcutaneous Point-of-Care Treatment of ST-Segment-Elevation Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e016552. [Google Scholar] [CrossRef]
- Rikken, S.A.O.F.; Selvarajah, A.; Hermanides, R.S.; Coller, B.S.; Gibson, C.M.; Granger, C.B.; Lapostolle, F.; Postma, S.; van de Wetering, H.; van Vliet, R.C.W.; et al. Prehospital Treatment with Zalunfiban (RUC-4) in Patients with ST- Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention: Rationale and Design of the CELEBRATE Trial. Am. Heart J. 2023, 258, 119–128. [Google Scholar] [CrossRef]
- Hillerson, D.; Li, S.; Misumida, N.; Wegermann, Z.K.; Abdel-Latif, A.; Ogunbayo, G.O.; Wang, T.Y.; Ziada, K.M. Characteristics, Process Metrics, and Outcomes Among Patients With ST-Elevation Myocardial Infarction in Rural vs Urban Areas in the US: A Report From the US National Cardiovascular Data Registry. JAMA Cardiol. 2022, 7, 1016. [Google Scholar] [CrossRef]
- Boukhris, M.; Buache, J.; Chenard, P.; Pradel, V.; Virot, P.; Aboyans, V. Rural Urban Differences in Management and Outcomes of Patients with ST-Segment Elevation Myocardial Infarction; Insights from SCALIM a French Regional Registry. Eur. J. Prev. Cardiol. 2025, 32. [Google Scholar] [CrossRef]
- Kardas, P.; Kwiatek, A.; Włodarczyk, P.; Urbański, F.; Ciabiada-Bryła, B. Is the KOS-Zawał Coordinated Care Program Effective in Reducing Long-Term Cardiovascular Risk in Coronary Artery Disease Patients in Poland? Insights from Analysis of Statin Persistence in a Nationwide Cohort. Pol. Heart J. 2024, 82, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Khoshchehreh, M.; Groves, E.M.; Tehrani, D.; Amin, A.; Patel, P.M.; Malik, S. Changes in Mortality on Weekend versus Weekday Admissions for Acute Coronary Syndrome in the United States over the Past Decade. Int. J. Cardiol. 2016, 210, 164–172. [Google Scholar] [CrossRef]
- Kumar, G.; Deshmukh, A.; Sakhuja, A.; Taneja, A.; Kumar, N.; Jacobs, E.; Nanchal, R. Acute Myocardial Infarction: A National Analysis of the Weekend Effect over Time. J. Am. Coll. Cardiol. 2015, 65, 217–218. [Google Scholar] [CrossRef] [PubMed]
- Jankowska-Sanetra, J.; Sanetra, K.; Synak, M.; Milewski, K.; Gerber, W.; Buszman, P.P. The Impact of the Coronavirus Pandemic on Patients Hospitalized Due to Acute Coronary Syndrome. Adv. Interv. Cardiol. 2023, 19, 86–98. [Google Scholar] [CrossRef]
- De Luca, G.; Verdoia, M.; Cercek, M.; Jensen, L.O.; Vavlukis, M.; Calmac, L.; Johnson, T.; Ferrer, G.R.; Ganyukov, V.; Wojakowski, W.; et al. Impact of COVID-19 Pandemic on Mechanical Reperfusion for Patients With STEMI. J. Am. Coll. Cardiol. 2020, 76, 2321–2330. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, M.; Karpiak, J.; Zaręba, L.; Przybylski, A. High In-Hospital Mortality and Prevalence of Cardiogenic Shock in Patients with ST-Segment Elevation Myocardial Infarction and Concomitant COVID-19. Adv. Interv. Cardiol. 2023, 19, 22–30. [Google Scholar] [CrossRef]
- Zeymer, U. Maintaining Optimal Care for Acute Myocardial Infarction Patients during War Times. Pol. Arch. Intern. Med. 2024, 134. [Google Scholar] [CrossRef]
- Mamas, M.A.; Martin, G.P.; Grygier, M.; Wadhera, R.K.; Mallen, C.; Curzen, N.; Wijeysundera, H.C.; Banerjee, A.; Kontopantelis, E.; Rashid, M.; et al. Indirect Impact of the War in Ukraine on Primary Percutaneous Coronary Interventions for ST-Elevation Myocardial Infarction in Poland. Pol. Arch. Intern. Med. 2024. [Google Scholar] [CrossRef]
- Dziewierz, A.; Siudak, Z.; Rakowski, T.; Kleczyński, P.; Dubiel, J.S.; Dudek, D. Early Administration of Abciximab Reduces Mortality in Female Patients with ST-Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention (from the EUROTRANSFER Registry). J. Thromb. Thrombolysis 2013, 36, 240–246. [Google Scholar] [CrossRef]
- Huded, C.P.; Johnson, M.; Kravitz, K.; Menon, V.; Abdallah, M.; Gullett, T.C.; Hantz, S.; Ellis, S.G.; Podolsky, S.R.; Meldon, S.W.; et al. 4-Step Protocol for Disparities in STEMI Care and Outcomes in Women. J. Am. Coll. Cardiol. 2018, 71, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M.; et al. The Lancet Women and Cardiovascular Disease Commission: Reducing the Global Burden by 2030. The Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Doolub, G.; Mamas, M.A.; Malinowski, K.P.; Zabojszcz, M.; Dardzińska, N.; Jaskulska, P.; Hawranek, M.; Siudak, Z. Closing Gender Gap in Time Delays and Mortality in STEMI: Insights from the ORPKI Registry. Pol. Arch. Intern. Med. 2025. [Google Scholar] [CrossRef]
- Dziewierz, A.; Vogel, B.; Zdzierak, B.; Kuleta, M.; Malinowski, K.P.; Rakowski, T.; Piotrowska, A.; Mehran, R.; Siudak, Z. Operator-Patient Sex Discordance and Periprocedural Outcomes of Percutaneous Coronary Intervention (from the ORPKI Polish National Registry). Adv. Interv. Cardiol. 2023, 19, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Dziewierz, A.; Zdzierak, B.; Malinowski, K.P.; Siudak, Z.; Zasada, W.; Tokarek, T.; Zabojszcz, M.; Dolecka-Ślusarczyk, M.; Dudek, D.; Bartuś, S.; et al. Diabetes Mellitus Is Still a Strong Predictor of Periprocedural Outcomes of Primary Percutaneous Coronary Interventions in Patients Presenting with ST-Segment Elevation Myocardial Infarction (from the ORPKI Polish National Registry). J. Clin. Med. 2022, 11, 6284. [Google Scholar] [CrossRef]
- Kałużna-Oleksy, M.; Paradies, V. Women in Interventional Cardiology – Patients’ and Operators’ Perspectives. Adv. Interv. Cardiol. 2023, 19, 79–81. [Google Scholar] [CrossRef]
- Bansal, M.; Mehta, A.; Balakrishna, A.M.; Saad, M.; Ventetuolo, C.E.; Roswell, R.O.; Poppas, A.; Abbott, J.D.; Vallabhajosyula, S. Race, Ethnicity, and Gender Disparities in Acute Myocardial Infarction. Crit. Care Clin. 2024, 40, 685–707. [Google Scholar] [CrossRef]
- Glickman, S.W.; Granger, C.B.; Ou, F.-S.; O’Brien, S.; Lytle, B.L.; Cairns, C.B.; Mears, G.; Hoekstra, J.W.; Garvey, J.L.; Peterson, E.D.; et al. Impact of a Statewide ST-Segment–Elevation Myocardial Infarction Regionalization Program on Treatment Times for Women, Minorities, and the Elderly. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 514–521. [Google Scholar] [CrossRef]
- Ya’qoub, L.; Lemor, A.; Dabbagh, M.; O’Neill, W.; Khandelwal, A.; Martinez, S.C.; Ibrahim, N.E.; Grines, C.; Voeltz, M.; Basir, M.B. Racial, Ethnic, and Sex Disparities in Patients With STEMI and Cardiogenic Shock. JACC Cardiovasc. Interv. 2021, 14, 653–660. [Google Scholar] [CrossRef]
- Dziewierz, A.; Siudak, Z.; Rakowski, T.; Dubiel, J.S.; Dudek, D. Age-Related Differences in Treatment Strategies and Clinical Outcomes in Unselected Cohort of Patients with ST-Segment Elevation Myocardial Infarction Transferred for Primary Angioplasty. J. Thromb. Thrombolysis 2012, 34, 214–221. [Google Scholar] [CrossRef]
- Jervis Somo, L.; Okobi, O.E.; Asomugha-Okwara, A.; Osias, K.; Mordi, P.O.; Enyeneokpon, E.; Etakewen, P.O.; Okoro, C. Retrospective Analysis of Atypical Chest Pain Presentations in Older Adults and Their Association With Missed Acute Coronary Syndrome Diagnosis in the Emergency Department: National Hospital Ambulatory Medical Care Survey (NHAMCS)-Based Study. Cureus 2025. [Google Scholar] [CrossRef] [PubMed]
- Konuş, A.H.; Özderya, A.; Çırakoğlu, Ö.F.; Sayın, M.R.; Yerlikaya, M.G. The Relationship between Advanced Lung Cancer Inflammation Index and High SYNTAX Score in Patients with Non-ST-Elevation Myocardial Infarction. Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2024, 20, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Lu, C.; Mo, J.; Wang, T.; Li, X.; Yang, Y. Efficacy and Safety of Different Revascularization Strategies in Patients with Non-ST-Segment Elevation Myocardial Infarction with Multivessel Disease: A Systematic Review and Network Meta-Analysis. Postepy W Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2024, 20, 382–392. [Google Scholar] [CrossRef]
- Blumer, V.; Kanwar, M.K.; Barnett, C.F.; Cowger, J.A.; Damluji, A.A.; Farr, M.; Goodlin, S.J.; Katz, J.N.; McIlvennan, C.K.; Sinha, S.S.; et al. Cardiogenic Shock in Older Adults: A Focus on Age-Associated Risks and Approach to Management: A Scientific Statement From the American Heart Association. Circulation 2024, 149. [Google Scholar] [CrossRef] [PubMed]
- Gopar-Nieto, R.; González-Pacheco, H.; Arias-Mendoza, A.; Briseño-De-la Cruz, J.L.; Araiza-Garaygordobil, D.; Sierra-Lara Martínez, D.; Mendoza-García, S.; Altamirano-Castillo, A.; Dattoli-García, C.A.; Manzur-Sandoval, D.; et al. Infarto de miocardio con elevación del ST no reperfundido: nociones de un país de ingresos bajos a medios. Arch. Cardiol. México 2023, 93. [Google Scholar] [CrossRef]
- Mathew, A.; Moolla, M.; Jeemon, P.; Punnoose, E.; Ashraf, S.M.; Pisharody, S.; Viswanathan, S.; Jayakumar, T.G.; Jabir, A.; Mathew, J.P.; et al. Timeliness of Reperfusion in ST-Segment Elevation Myocardial Infarction and Outcomes in Kerala, India: Results of the TRUST Outcomes Registry. Postgrad. Med. J. 2025, 101, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.; Doğan, Z. ST-Segment Elevation Myocardial Infarction for Pharmacoinvasive Strategy or Primary Percutaneous Coronary Intervention in Gaza (STEPP 2- PCI) Trial. Arch. Med. Sci. – Atheroscler. Dis. 2024, 9, 202–206. [Google Scholar] [CrossRef]
- Karim, S.R.; Helseth, H.C.; Baker, P.O.; Keller, G.A.; Meyers, H.P.; Herman, R.; Smith, S.W. Artificial Intelligence Detection of Occlusive Myocardial Infarction from Electrocardiograms Interpreted as “Normal” by Conventional Algorithms. J. Pers. Med. 2025, 15, 130. [Google Scholar] [CrossRef]
- Johnson, L.S.; Zadrozniak, P.; Jasina, G.; Grotek-Cuprjak, A.; Andrade, J.G.; Svennberg, E.; Diederichsen, S.Z.; McIntyre, W.F.; Stavrakis, S.; Benezet-Mazuecos, J.; et al. Artificial Intelligence for Direct-to-Physician Reporting of Ambulatory Electrocardiography. Nat. Med. 2025, 31, 925–931. [Google Scholar] [CrossRef]
- Lee, S.-H.; Jeon, K.L.; Lee, Y.-J.; You, S.C.; Lee, S.-J.; Hong, S.-J.; Ahn, C.-M.; Kim, J.-S.; Kim, B.-K.; Ko, Y.-G.; et al. Development of Clinically Validated Artificial Intelligence Model for Detecting ST-Segment Elevation Myocardial Infarction. Ann. Emerg. Med. 2024, 84, 540–548. [Google Scholar] [CrossRef]
- Hsieh, P.-H.; Lin, C.; Lin, C.-S.; Liu, W.-T.; Lin, T.-K.; Tsai, D.-J.; Hung, Y.-J.; Chen, Y.-H.; Lin, C.-Y.; Lin, S.-H.; et al. Economic Analysis of an AI-Enabled ECG Alert System: Impact on Mortality Outcomes from a Pragmatic Randomized Trial. Npj Digit. Med. 2025, 8. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Nichol, A.A.; Martinez-Martin, N.; Larson, D.B.; Abramoff, M.; Wolf, R.M.; Char, D. Ethical Considerations in the Design and Conduct of Clinical Trials of Artificial Intelligence. JAMA Netw. Open 2024, 7, e2432482. [Google Scholar] [CrossRef]
- Sonicki, Z. Large Multi-Modal Models – the Present or Future of Artificial Intelligence in Medicine? Croat. Med. J. 2024, 65, 1–2. [Google Scholar] [CrossRef]
- Aldajani, A.; Chaabo, O.; Brouillette, F.; Anchouche, K.; Lachance, Y.; Akl, E.; Dandona, S.; Martucci, G.; Pelletier, J.-P.; Piazza, N.; et al. Impact of a Mobile, Cloud-Based Care-Coordination Platform on Door-to-Balloon Time in Patients With STEMI: Initial Results. CJC Open 2024, 6, 1094–1098. [Google Scholar] [CrossRef] [PubMed]
- Damaševičius, R.; Bacanin, N.; Misra, S. From Sensors to Safety: Internet of Emergency Services (IoES) for Emergency Response and Disaster Management. J. Sens. Actuator Netw. 2023, 12, 41. [Google Scholar] [CrossRef]
- Chen, X.; Manshaii, F.; Tioran, K.; Wang, S.; Zhou, Y.; Zhao, J.; Yang, M.; Yin, X.; Liu, S.; Wang, K. Wearable Biosensors for Cardiovascular Monitoring Leveraging Nanomaterials. Adv. Compos. Hybrid Mater. 2024, 7. [Google Scholar] [CrossRef]
- De Luca, G.; Verburg, A.; Hof, A.V.; Ten Berg, J.; Kereiakes, D.J.; Coller, B.S.; Gibson, C.M. Current and Future Roles of Glycoprotein IIb–IIIa Inhibitors in Primary Angioplasty for ST-Segment Elevation Myocardial Infarction. Biomedicines 2024, 12, 2023. [Google Scholar] [CrossRef]
- Naito, H.; Nojima, T.; Fujisaki, N.; Tsukahara, K.; Yamamoto, H.; Yamada, T.; Aokage, T.; Yumoto, T.; Osako, T.; Nakao, A. Therapeutic Strategies for Ischemia Reperfusion Injury in Emergency Medicine. Acute Med. Surg. 2020, 7. [Google Scholar] [CrossRef]
- Kronick, S.L.; Kurz, M.C.; Lin, S.; Edelson, D.P.; Berg, R.A.; Billi, J.E.; Cabanas, J.G.; Cone, D.C.; Diercks, D.B.; Foster, J. (Jim); et al. Part 4: Systems of Care and Continuous Quality Improvement: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132. [Google Scholar] [CrossRef]
Figure 1.
Time-dependent evolution of myocardial injury following coronary occlusion. Schematic representation of myocardial tissue viability over time following acute coronary occlusion in ST-segment elevation myocardial infarction. The diagram illustrates the progressive transition from normally perfused myocardium (red) through reversibly injured but salvageable tissue (pink, ischemic zone) to irreversibly damaged myocardium (yellow, infarcted zone). The area of salvageable tissue diminishes rapidly with increasing ischemic time, with the most dramatic losses occurring after 2-3 hours. Early reperfusion therapy maximizes the myocardial salvage index by preserving the ischemic zone before irreversible injury occurs. The non-linear relationship between time and tissue loss underscores why the greatest clinical benefit occurs with reperfusion within the first 1-2 hours after symptom onset.
Figure 1.
Time-dependent evolution of myocardial injury following coronary occlusion. Schematic representation of myocardial tissue viability over time following acute coronary occlusion in ST-segment elevation myocardial infarction. The diagram illustrates the progressive transition from normally perfused myocardium (red) through reversibly injured but salvageable tissue (pink, ischemic zone) to irreversibly damaged myocardium (yellow, infarcted zone). The area of salvageable tissue diminishes rapidly with increasing ischemic time, with the most dramatic losses occurring after 2-3 hours. Early reperfusion therapy maximizes the myocardial salvage index by preserving the ischemic zone before irreversible injury occurs. The non-linear relationship between time and tissue loss underscores why the greatest clinical benefit occurs with reperfusion within the first 1-2 hours after symptom onset.
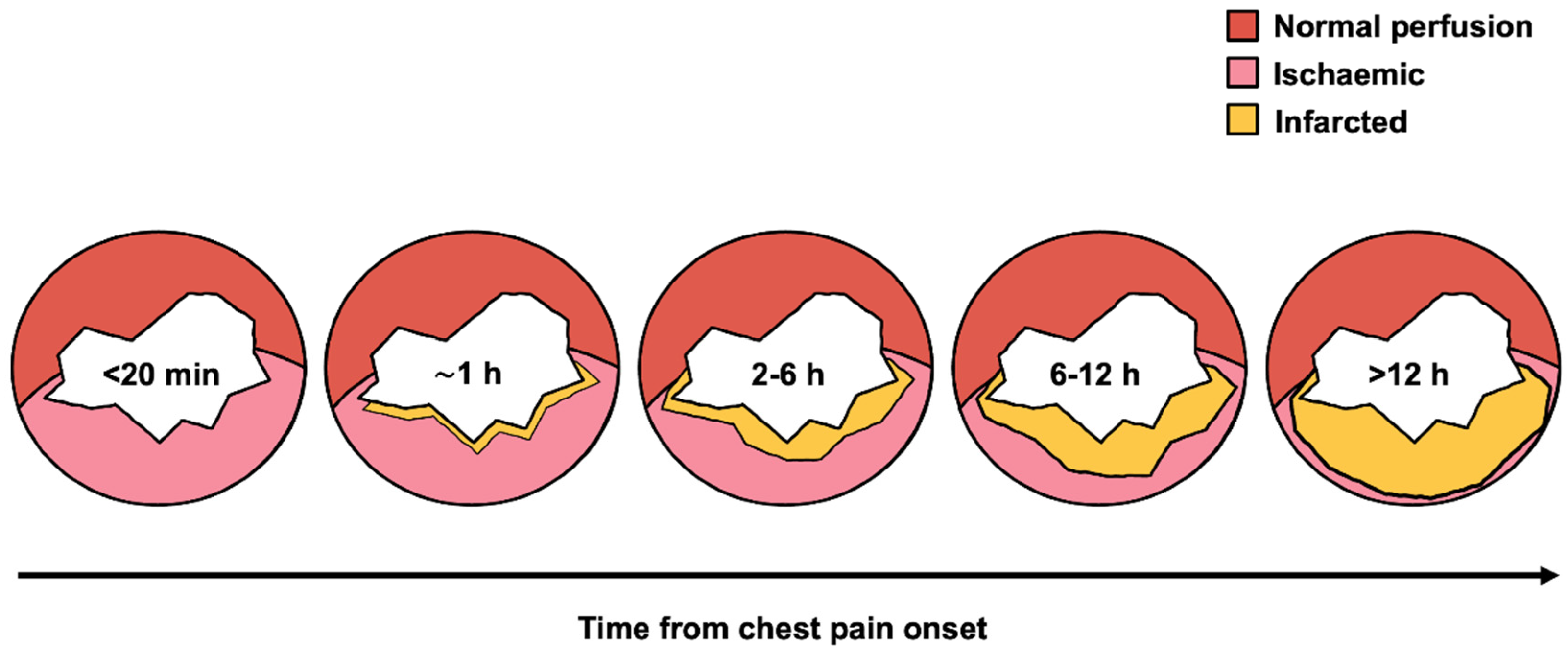
Figure 2.
Factors affecting STEMI reperfusion timelines. This diagram shows the four key domains that influence time to reperfusion in STEMI patients: patient/community factors (symptom recognition, health-seeking behavior), geographical factors (transport times, distance to centers), pre-hospital system factors (EMS protocols, field diagnosis), and in-hospital factors (cathlab activation, transfer protocols). Targeted interventions within each domain may help reduce total ischemic time and improve clinical outcomes. Abbreviations: EMS = emergency medical services; FMC = first medical contact; PPCI = primary percutaneous coronary intervention; STEMI = ST-elevation myocardial infarction.
Figure 2.
Factors affecting STEMI reperfusion timelines. This diagram shows the four key domains that influence time to reperfusion in STEMI patients: patient/community factors (symptom recognition, health-seeking behavior), geographical factors (transport times, distance to centers), pre-hospital system factors (EMS protocols, field diagnosis), and in-hospital factors (cathlab activation, transfer protocols). Targeted interventions within each domain may help reduce total ischemic time and improve clinical outcomes. Abbreviations: EMS = emergency medical services; FMC = first medical contact; PPCI = primary percutaneous coronary intervention; STEMI = ST-elevation myocardial infarction.


Table 1.
Comparison of reperfusion strategies.
| Feature | Primary PCI | Fibrinolysis | Pharmaco-invasive |
|---|---|---|---|
| Mechanism | Mechanical opening | Thrombus dissolution |
Initial lysis followed by coronary angiogram / PCI |
| Time indication | FMC-to-device ≤120 min | PCI unavailable or >120 min | FMC-to-device >120 min |
| Advantages | >95% success definitive treatment |
Rapid deployment anywhere | Combines speed with definitive therapy |
| Disadvantages | Time-dependent; infrastructure needs |
~65% success bleeding risk |
Intracranial hemorrhage risk requires coordination |
| Delayed presentation efficacy | Benefit diminishes significantly |
Efficacy declines after hours | Superior to delayed primary PCI |
Abbreviations: FMC = first medical contact; PCI = percutaneous coronary intervention.
Table 2.
Components and benchmarks of total ischemic time in STEMI.
| Time interval | Definition | Guideline target | Common delay sources |
|---|---|---|---|
| Patient delay | Symptom onset to FMC | Minimize | Symptom misinterpretation, denial, general practitioner contact, self-transport |
| Pre-hospital system | FMC to hospital arrival | Minimize | EMS dispatch, scene time, transport distance |
| Door-in-door-out | Non-PCI hospital arrival to departure | ≤30 min | Transport availability, ED processes, diagnostics |
| FMC / Door-to-ECG | FMC / Hospital arrival to ECG | ≤10 min | Triage delays, symptom recognition failure |
| Door-to-activation | Hospital arrival to cath lab activation | ≤20 min | ECG interpretation, decision-making |
| FMC / Door-to-balloon | FMC / Hospital arrival to device inflation | ≤90 min | Team assembly, complex procedures, instability |
| Total ischemic time | Symptom onset to reperfusion | ≤120 min (optimal | All combined delays |
Abbreviations: FMC = first medical contact; EMS = emergency medical services; ED = emergency department; ECG = electrocardiogram; PCI = percutaneous coronary intervention.
Table 3.
Comparative barriers to timely reperfusion in high- and low-resource settings.
| Barrier domain | High-resource setting | Low/middle-income setting |
|---|---|---|
| Patient/community | Symptom misinterpretation; denial; failure to use EMS | Lack of basic awareness; fear of catastrophic cost; reliance on traditional medicine |
| Pre-hospital system | EMS on-scene time; inter-hospital transfer delays; “weekend effect” | Lack of organized EMS; no pre-hospital ECG/triage; long transport over poor infrastructure |
| In-hospital system | Cath lab activation delays; ED dwell time; simultaneous presentations | Paucity of PCI-capable centers; lack of trained specialists; inability to provide 24/7 service |
| Financial | Insurance co-pays/deductibles; market share competition between hospitals | Prohibitive out-of-pocket cost of PCI; lack of universal health coverage |
| Primary reperfusion strategy | Primary PCI (default) | Pharmaco-invasive (often the only feasible option) |
Abbreviations: FMC = first medical contact; EMS = emergency medical services; ED = emergency department; ECG = electrocardiogram; PCI = percutaneous coronary intervention.
Table 4.
Targeted interventions to minimize STEMI treatment delays.
| Stakeholder | Key recommendations | Specific actions |
|---|---|---|
|
Policymakers & public health officials |
Fund sustained public awareness campaigns |
• Focus on typical and atypical symptoms • Emphasize immediate activation of emergency medical services (e.g., 1-1-2 / 9-1-1) • Ensure cultural competency |
| Support regional STEMI networks |
• Define protocols for rural/remote areas • Ensure pharmaco-invasive strategy availability • Mandate performance reporting |
|
|
Healthcare system leaders |
Implement standardized protocols |
• Establish emergency physician activation authority • Deploy single-call notification systems • Monitor performance continuously |
| Address temporal disparities | • Ensure 24/7 equivalent care quality • Optimize off-hours staffing models |
|
| Use standardization to promote equity |
• Reduce care variability • Target vulnerable populations |
|
| Clinicians | Maintain guideline adherence | • Minimize all controllable delays • Focus on door-to-ECG and door-to-balloon metrics |
| Embrace flexible strategies | • Utilize pharmaco-invasive approach when appropriate • Implement risk-stratified triage protocols |
|
| Recognize bias potential | • Maintain heightened awareness for atypical presentations • Address disparities proactively |
|
| Researchers | Identify priority research areas | • Develop patient delay reduction strategies • Create disparity elimination interventions • Optimize pharmaco-invasive approaches • Validate AI-based risk stratification and triage tools in diverse populations |
Abbreviations: AI = artificial intelligence; ECG = electrocardiogram; STEMI = ST-elevation myocardial infarction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



