Submitted:
28 August 2025
Posted:
04 September 2025
You are already at the latest version
Abstract
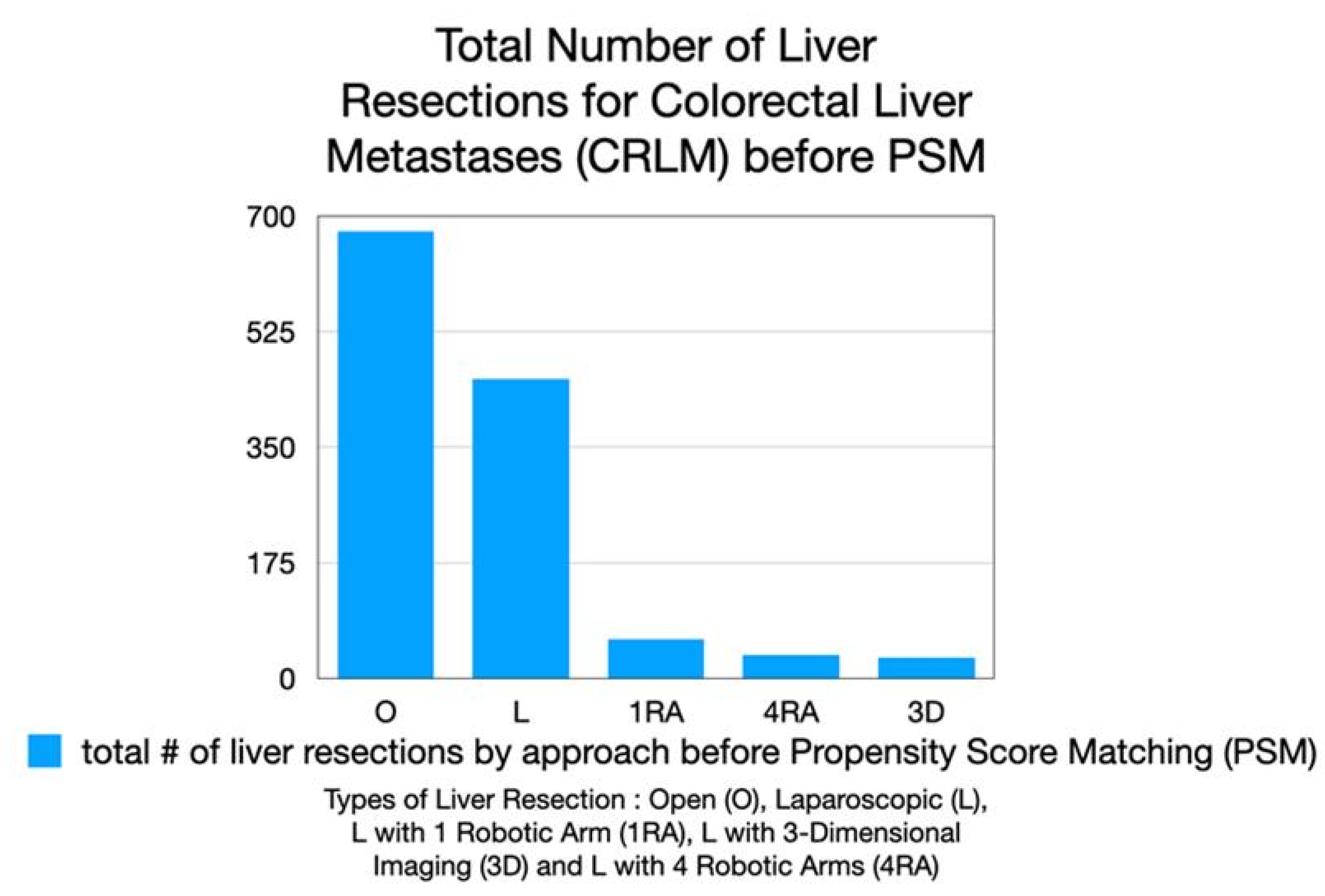
Introduction: This international multicenter study compared five surgical approaches for liver resection in colorectal metastases: open (O), standard laparoscopy (L), laparoscopy with 3D imaging (3D), laparoscopy with single robotic-arm assistance (1RA), and with complete robotic systems utilizing 4 robotic arms(4RA). A subcohort analysis was done for enhanced L, this cohort was termed collaborative assisted robotics (cobotic surgery) and consisted of L with the addition of 3D imaging or a single robotic arm to hold the laparoscope. This study aimed to evaluate whether 4RA offers any significant advantages over laparoscopy with and without cobotic enhancements. Methods: We analyzed 1,257 patients across five centers using propensity score matching. Surgical approaches were compared for blood loss, operative time, hospital stay, resection margins (R0 status), and major complications (Clavien-Dindo grade ≥3). Statistical analysis used Student's t-test and Mann-Whitney U-test for continuous variables, with p<0.05 considered significant. Results: Minimally invasive techniques without 3-D imaging, a solitary robotic arm to hold the laparoscope or utilization of handheld robotic GIA staplers showed superior outcomes to open surgery. Laparoscopic approaches demonstrated significantly reduced blood loss (L: 553 mL vs O: 695 mL, p<0.001) and shorter hospital stays when compared to open surgery (L: 8 days vs O: 14 days, p<0.001). The 4RA cohort had similar benefits when compared to O resection (blood loss: 382 mL vs 542 mL, p<0.001; LOS: 8 vs 24 days, p<0.001), but longer operative times (280 vs 305 minutes (min), p<0.001). The 1RA and 3D approaches showed comparable outcomes to 4RA in most measures. Conclusions: While robotic assistance offers technical advantages, complete robotic systems (4RA) did not demonstrate clear superiority over laparoscopy with or without cobotics. Cost-effective modular enhancements to standard laparoscopy may provide future benefits while allowing resource allocation toward AI-driven surgical innovations. Future studies should employ prospective designs with standardized protocols to validate these findings and assess long-term oncologic outcomes.
Keywords:
1. Introduction
2. Methods
2.1. Patient Selection & Indication for Surgery
2.2. Study Endpoints
2.3. Data Analysis
2.4. Propensity Score Matching (PSM)
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gumbs, A.A.; et al. Study: International Multicentric Minimally Invasive Liver Resection for Colorectal Liver Metastases (SIMMILR-CRLM). Cancers (Basel) 2022, 14, 6. [Google Scholar] [CrossRef]
- Gumbs, A.A.; TJ Tsai, and J.Hoffman. Initial experience with laparoscopic hepatic resection at a comprehensive cancer center. Surg Endosc 2012, 26, 480–487. [Google Scholar] [CrossRef]
- Andrew, A.G.; et al. What is Artificial Intelligence Surgery? Artificial Intelligence Surgery 2021, 1, 1–10. [Google Scholar] [CrossRef]
- Andrew, A.G. and G. Brice, Why Artificial Intelligence Surgery (AIS) is better than current Robotic-Assisted Surgery (RAS). Artificial Intelligence Surgery 2022, 2, 207–212. [CrossRef]
- Gumbs, A.A.; et al. Artificial Intelligence Surgery: How Do We Get to Autonomous Actions in Surgery? Sensors (Basel) 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Gumbs, A.A.; et al. The Advances in Computer Vision That Are Enabling More Autonomous Actions in Surgery: A Systematic Review of the Literature. Sensors (Basel) 2022, 22, 13. [Google Scholar] [CrossRef]
- Gumbs, A.A.; et al. Modified robotic lightweight endoscope (ViKY) validation in vivo in a porcine model. Surg Innov 2007, 14, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Andrew, A.G.; et al. Keeping surgeons in the loop: are handheld robotics the best path towards more autonomous actions? (A comparison of complete vs. handheld robotic hepatectomy for colorectal liver metastases). Artificial Intelligence Surgery 2021, 1, 38–51. [Google Scholar] [CrossRef]
- Gumbs, A.A.; et al. Survival Study: International Multicentric Minimally Invasive Liver Resection for Colorectal Liver Metastases (SIMMILR-2). Cancers (Basel) 2022, 14, 17. [Google Scholar] [CrossRef]
- Fretland, A.A.; et al. Laparoscopic Versus Open Resection for Colorectal Liver Metastases: The OSLO-COMET Randomized Controlled Trial. Ann Surg 2018, 267, 199–207. [Google Scholar] [CrossRef]
- Kuemmerli, C.; et al. Is prolonged operative time associated with postoperative complications in liver surgery? An international multicentre cohort study of 5424 patients. Surg Endosc 2024, 38, 7118–7130. [Google Scholar] [CrossRef]
- Guerra, F.; et al. Outcomes of robotic liver resections for colorectal liver metastases. A multi-institutional analysis of minimally invasive ultrasound-guided robotic surgery. Surg Oncol 2019, 28, 14–18. [Google Scholar] [CrossRef]
- Lorenz, E.; et al. Robotic and laparoscopic liver resection-comparative experiences at a high-volume German academic center. Langenbecks Arch Surg 2021, 406, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Perrakis, A.; et al. Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery. J Clin Med 2021, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; et al. International experts consensus guidelines on robotic liver resection in 2023. World J Gastroenterol 2023, 29, 4815–4830. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; et al. Propensity Score-matched Analysis Comparing Robotic Versus Laparoscopic Minor Liver Resections of the Anterolateral Segments: an International Multi-center Study of 10,517 Cases. Ann Surg 2024. [CrossRef]
- Rahimli, M.; et al. Learning curve analysis of 100 consecutive robotic liver resections. Surg Endosc 2025, 39, 2512–2522. [Google Scholar] [CrossRef]
- Rahimli, M.; et al. Robotic and laparoscopic liver surgery for colorectal liver metastases: an experience from a German Academic Center. World J Surg Oncol 2020, 18, 333. [Google Scholar] [CrossRef]
- Rahimli, M.; et al. Does Robotic Liver Surgery Enhance R0 Results in Liver Malignancies during Minimally Invasive Liver Surgery? Cancers (Basel) 2022, 14, 14. [Google Scholar] [CrossRef]
- Wang, Y.; et al. Current trends in three-dimensional visualization and real-time navigation as well as robot-assisted technologies in hepatobiliary surgery. World J Gastrointest Surg 2021, 13, 904–922. [Google Scholar] [CrossRef]
- Chan, K.S. and V. J Laparoendosc Adv Surg Tech A 2023, 33, 678–690. [Google Scholar] [CrossRef]
- Velayutham, V.; et al. 3D visualization reduces operating time when compared to high-definition 2D in laparoscopic liver resection: a case-matched study. Surg Endosc 2016, 30, 147–153. [Google Scholar] [CrossRef]
- Yang, Z.; et al. Application of three-dimensional visualization technology in early surgical repair of bile duct injury during laparoscopic cholecystectomy. BMC Surgery 2024, 24, 271. [Google Scholar] [CrossRef] [PubMed]
- Qiu, D.; H Zhuang, and F. Han, Effect and influence factor analysis of intrahepatic Glisson's sheath vascular disconnection approach for anatomical hepatectomy by three-dimensional laparoscope. J BUON 2017, 22, 157–161.
- Kawai, T.; et al. 3D vision and maintenance of stable pneumoperitoneum: a new step in the development of laparoscopic right hepatectomy. Surg Endosc 2018, 32, 3706–3712. [Google Scholar] [CrossRef] [PubMed]
- Witowski, J.S.; et al. 3D Printing in Liver Surgery: A Systematic Review. Telemed J E Health 2017, 23, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Giehl-Brown, E.; et al. 3D liver model-based surgical education improves preoperative decision-making and patient satisfaction-a randomized pilot trial. Surg Endosc 2023, 37, 4545–4554. [Google Scholar] [CrossRef]
- Huber, T.; et al. Computer-assisted intraoperative 3D-navigation for liver surgery: a prospective randomized-controlled pilot study. Ann Transl Med 2023, 11, 346. [Google Scholar] [CrossRef]
- Ruzzenente, A.; et al. Hyper accuracy three-dimensional (HA3D) technology for planning complex liver resections: a preliminary single center experience. Updates Surg 2023, 75, 105–114. [Google Scholar] [CrossRef]
- Banchini, F.; et al. 3-D reconstruction in liver surgery: a systematic review. HPB (Oxford) 2024, 26, 1205–1215. [Google Scholar] [CrossRef]
- Mike, S.; et al. Contribution of 3D virtual modeling in locating hepatic metastases, particularly "vanishing tumors": a pilot study. Artificial Intelligence Surgery 2024, 4, 331–347. [Google Scholar] [CrossRef]
- Zeng, X.; et al. Impact of three-dimensional reconstruction visualization technology on short-term and long-term outcomes after hepatectomy in patients with hepatocellular carcinoma: a propensity-score-matched and inverse probability of treatment-weighted multicenter study. Int J Surg 2024, 110, 1663–1676. [Google Scholar] [CrossRef]
- Takeaki, I. , "Bon mariage" of artificial intelligence and intraoperative fluorescence imaging for safer surgery. Artificial Intelligence Surgery 2023, 3, 163–165. [Google Scholar]
- Achterberg, F.B.; et al. ICG-Fluorescence Imaging for Margin Assessment During Minimally Invasive Colorectal Liver Metastasis Resection. JAMA Netw Open 2024, 7, e246548. [Google Scholar] [CrossRef]
- Abu Hilal, M.; et al. The Brescia internationally validated European guidelines on minimally invasive liver surgery. Br J Surg 2025, 112, 6. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, D.A.; et al. Artificial Intelligence in Surgery: Promises and Perils. Ann Surg 2018, 268, 70–76. [Google Scholar] [CrossRef]
- Christina, B.; et al. Artificial intelligence in hepatopancreaticobiliary surgery - promises and perils. Artificial Intelligence Surgery 2022, 2, 213–223. [Google Scholar] [CrossRef]
- Ward, T.M.; et al. Artificial intelligence prediction of cholecystectomy operative course from automated identification of gallbladder inflammation. Surg Endosc 2022, 36, 6832–6840. [Google Scholar] [CrossRef] [PubMed]
- Andrew, A.G.; et al. Surgomics and the Artificial intelligence, Radiomics, Genomics, Oncopathomics and Surgomics (AiRGOS) Project. Artificial Intelligence Surgery 2023, 3, 180–185. [Google Scholar] [CrossRef]
- Loftus, T.J.; et al. Artificial Intelligence-enabled Decision Support in Surgery: State-of-the-art and Future Directions. Ann Surg 2023, 278, 51–58. [Google Scholar] [CrossRef]
- Giulia, C.; et al. White paper: ethics and trustworthiness of artificial intelligence in clinical surgery. Artificial Intelligence Surgery 2023, 3, 111–122. [Google Scholar] [CrossRef]
- Rashidian, N.; et al. Ethics and trustworthiness of artificial intelligence in Hepato-Pancreato-Biliary surgery: a snapshot of insights from the European-African Hepato-Pancreato-Biliary Association (E-AHPBA) survey. HPB (Oxford) 2025, 27, 502–510. [Google Scholar] [CrossRef] [PubMed]

| Demographics, Confounding Variables | Open (O)(n=257) | Laparoscopy (L) (n=257) | p-value | Open (O) (n=36) | 4 Arm Robotic (4RA) (n=36) | p-value | Laparoscopy (L) (n=35) | 4 Arm Robotic (4RA)(n=35) | p-value |
|---|---|---|---|---|---|---|---|---|---|
| Age, mean (range) | 62 (19-86) | 63.5 (23-90) | 0.2 | 58.7 (25-81) | 60.5 (35-83) | 0.6 | 60.8 (34-79) | 61 (34-81) | 0.9 |
| M : F | 159M : 98F | 154M : 103F | 0.2 | 24 M : 12 F | 22 M 14 F | 0.6 | 18:16 | 20:14 | 0.6 |
| ASA | 0.8 | 0.9 | 0.7 | ||||||
| 1 | 30 | 28 | 2 | 1 | 3 | 2 | |||
| 2 | 164 | 158 | 21 | 19 | 19 | 17 | |||
| 3 | 61 | 70 | 12 | 15 | 12 | 15 | |||
| 4 | 2 | 1 | 1 | 1 | 0 | 0 | |||
| BMI kg/m2 (range) | 26.6 | 26 | 25.6 (19.1-40.5) | 25.9 (16.2-37.2) | 0.6 | 24.3 (17.0-34.4) | 25.8 (16.2-30.8) | 0.6 | |
| Previous Surgery (%) | 213 (83.0) | 206 (80.0) | 0.4 | 30 (83.3) | 24 (63.9) | 0.6 | 21 (78.8) | 16(52.9) | 0.2 |
| Neoadjuvant Therapy, n (%) | 185 (72.0) | 180 (70.0) | 0.6 | 16 (44.4) | 16 (44.4) | 0.9 | 26 (76.5) | 23(67.6) | 0.8 |
| Chemotherapy | 157 | 153 | 0.4 | 13 | 12 | 23 | 20 | ||
| Chemoradiotherapy | 14 | 16 | 1 | 1 | 2 | 2 | |||
| Immunotherapy | 14 | 8 | 2 | 3 | 1 | 3 | |||
| Metastasis Size mm (range) | 34.7 (2.5-170) | 34 (6-170) | 0.1 | 39.3 (18-57) | 38.6 (11-85) | 0.3 | 40.5 (7-170) | 38.8 (11-60) | 0.3 |
| Number of Resected Tumors (range) | 1.87 (1-8) | 1.85 (1-6) | 0.5 | 2.1 (1-3) | 1.8 (1-3) | 0.06 | 1.6 (1-3) | 1.7 (1-3) | 0.2 |
| Location in Deep Segments (%) | 183 (71.2) | 164 (63.8) | 0.07 | 23 (63.9) | 18 (55.6) | 0.2 | 16(47.1) | 19 (55.9) | 0.5 |
| Major Resection % | 42 | 48 | 0.06 | 11 (30.1) | 12 (33.3) | 0.5 | 10 (29.4) | 11 (32.4) | 0.8 |
| Demographics, Confounding Variables | Laparoscopy (L) (n=21) | 3-D Laparoscopy (3D) n=21) | p-value | Laparoscopy (L) (n=41) | 1 Arm Robotic-Assisted (1RA) (n=41) | p-value | 3-D Laparoscopy (3D) (n=11) | 1 Arm Robotic-Assisted (1RA) (n=11) | p-value |
|---|---|---|---|---|---|---|---|---|---|
| Age, mean (range) | 70.6 (44-86) | 69.2 (50-83) | 0.4 | 55.0 (23-70) | 58.3 (30-87) | 0.3 | 64.5 (50-71) | 66.5 (38-84) | 0.4 |
| M : F | 10 M : 11 F | 10 M : 11 F | 1 | 22 M : 19 F | 23 M 18 F | 0.8 | 6 M : 5 F | 5 M : 6 F | 0.7 |
| ASA | 1 | 0.7 | 0.6 | ||||||
| 1 | 1 | 1 | 1 | 2 | 0 | 0 | |||
| 2 | 14 | 14 | 24 | 20 | 9 | 8 | |||
| 3 | 6 | 6 | 26 | 19 | 2 | 3 | |||
| 4 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| BMI kg/m2 (range) | 27.1 (24.7-34.4) |
26.1 (19.3-39.2) | 0.3 | 30.4 (25-37) | 30.6 (27-40) | 0.6 | 30.3 (22-39) | 29.8 (23-39) | 0.9 |
| Previous Surgery (%) | 16 (76.2) | 20 (95.2) | 0.08 | 27 (65.8) | 28 (68.3) | 0.8 | 8 (72.7) | 11 (100) | 0.2 |
| Neoadjuvant Therapy | 17 (81.0) | 13 (61.9) | 0.2 | 31 (75.6) | 32 (78.0) | 1 | 8 (72.7) | 9 (81.8) | 1 |
| Chemotherapy | 17 | 13 | 29 | 30 | 8 | 9 | |||
| Chemoradiotherapy | 0 | 0 | 1 | 1 | 0 | 0 | |||
| Immunotherapy | 0 | 0 | 1 | 1 | 0 | 0 | |||
| Metastasis Size mm (range) | 30.4 (5-50) | 31.5 (8-100) | 0.6 | 26.6 (5-85) | 31.5 (10-115) | 0.5 | 36.4 (8-100) | 37.6 (10-115) | 0.8 |
| Number of Tumors (range) | 1.34 (1-3) | 1.67 (1.2) | 0.08 | 1.7 (1-5) | 1.5 (1-8) | 0.2 | 1.8 (1-2)) | 1.4 (1-3) | 0.07 |
| Location in Deep Segments (%) | 11 (52.4) | 14 (66.7) | 0.3 | 26 (63.4) | 27 (65.8) | 0.8 | 7 (63.6) | 8 (81.8) | 0.6 |
| Major Resection % | 4(19.0) | 6(28.6) | 0.5 | 20 (48.8) | 21 (51.2) | 0.8 | 4 (36.4) | 2 (18.2) | 0.3 |
| Demographics, Confounding Variables | 3D (n=13) | 4 RA (n=13) | p-value | 1 RA (n=9) | 4 RA (n=9) | p-value |
|---|---|---|---|---|---|---|
| Age, mean (range) | 68.8 (50-78) | 66.2 (34-83) | 1 | 60.2 (32-75) | 60.1 (34-83) | 0.9 |
| M : F | 7 M : 6 F | 10 M : 3 F | 0.2 | 3 M : 6 F | 5 M : 4 F | 0.3 |
| ASA | 0.8 | 0.06 | ||||
| 1 | 0 | 1 | 0 | 1 | ||
| 2 | 7 | 6 | 7 | 2 | ||
| 3 | 6 | 6 | 2 | 6 | ||
| 4 | 0 | 0 | 0 | 0 | ||
| BMI kg/m2 (range) | 26.6 (16.2-39.2) | 21.6 (16.2-37.2) | 0.7 | 31.9 (30.6-40) | 31.1 (26.9-37.2) | 0.7 |
| Previous Surgery (%) | 12 (92.3) | 10 (77.0) | 0.3 | 6 (66.7) | 6 (66.7) | 1 |
| Neoadjuvant Therapy, n (%) | 8 (61.5) | 5 (38.5) | 0.2 | 4 (44.4) | 3 (33.3) | 0.6 |
| Chemotherapy | 8 | 5 | 4 | 3 | ||
| Chemoradiotherapy | 0 | 0 | 0 | 0 | ||
| Immunotherapy | 0 | 0 | 0 | 0 | ||
| Metastasis Size mm (range) | 38.2 (11-100) | 34.7 (11-45) | 0.7 | 45.0 (20-115) | 30.8 (11-39) | 0.67 |
| Number of Tumors (range) | 2 (1-3) | 11.8 (1-3) | 0.2 | 1.2 (1-3) | 1.8 (1-2) | 0.09 |
| Location in Deep Segments (%) | 9 (69.2) | 7 (53.8) | 0.4 | 6 (66.7) | 5 (55.6) | 0.6 |
| Major Resection % | 3 (23.1) | 2 (15.4) | 0.6 | 3 (33.3) | 2 (22.2) | 0.6 |
| Outcome Variables | Open (O) (n=257) | Laparoscopy (L) (n=257) | p-value | Open (O) (n=36) | 4 Arm Robotic (4RA) (n=36) | p-value | Laparoscopy (L) (n=35) | 4 Arm Robotic (4RA) (n=35) | p-value |
|---|---|---|---|---|---|---|---|---|---|
| EBL, mL (range) | 695 (50-3500) | 553 (0-2500) | <0.0001 | 541.6 (300-600) | 382.2 (100-900) | 0.0006 | 504.5 (40-2500) | 375.0 (50-900) | 0.3 |
| OR Time, min (range) | 245.7 (90-900) | 259.9 (60-540) | <0.0001 | 280.1 (81-290) | 305.4 (107-522) | 0.342 | 233.7(60-489) | 300.5 (107-537) | <0.001 |
| LOS, days (range) | 13.6 (2-108) | 8.3 (1-168) | <0.0001 | 23.6 (4-108) | 7.8 (1-39) | < 0.00001 | 6.2 (1-57) | 6.8(1-39) | 0.3 |
| Conversion Rate, n (%) | NA | 21 (8.4) | NA | NA | 0 | NA | 5 (14.7) | 1 (2.9) | 0.09 |
| Postoperative Clavien-Dindo morbidity ≥ grade 3, n (%) | 34 (26.3) | 20 (16.5) | 0.04 | 7 (19.4) | 2 (17.1) | 0.07 | 2(5.9) | 2(5.9) | 1 |
| 30-day mortality, n (%) | 23(10.5) | 2 (0.8) | 0.00002 | 0 | 0 | 1 | 0 | 0 | 1 |
| 90-day mortality, n (%) | 24(17.7) | 2 (1.0) | <0.00001 | 0 | 0 | 1 | 0 | 0 | 1 |
| R1 resection, n (%) | 24 (25.1) | 23 (9.7) | 0.0001 | 8 (22.2) | 10 (33.3) | 0.586 | 4 (11.8) | 12 (36.4) | 0.022 |
| Outcome Variables | Laparoscopy (L) (n=21) | 3-D Laproscopy (3D) (n=21) | p-value | Laparoscopy (L) (n=41) | 1 Arm Robotic-Assisted (1RA) (n=41) | p-value | 3-D Laproscopy (3D) (n=11) | 1 Arm Robotic-Assisted (1RA) (n=11) | p-value |
|---|---|---|---|---|---|---|---|---|---|
| EBL, mL (range) | 424.4 (0-1500) | 218.8 (0-1800) | 0.02 | 434.5 (0-2300) | 414.4 (0-3000) | 0.1 | 636.4 (0-3000) | 300 (0-1800) | 1 |
| OR Time, min (range) | 198.3 (50-370) | 206.2 (87-290) | 0.7 | 235.2 (80-540) | 234.7 (36-620) | 0.7 | 211.8 (87-290) | 356.6 (187-620) | 0.002 |
| LOS, days (range) | 5.1 (1-10) | 6.55 (1-11) | 0.09 | 9 (1-168) | 4 (1-13) | 0.07 | 10.8 (5-24) | 5.7 (1-13) | 0.008 |
| Conversion Rate, n (%) | 3 (14.3) | 2 (9.5) | 0.6 | 5 (12.2) | 1 (2.4) | 0.09 | 1 (9.1) | 1 (9.1) | 1 |
| Postoperative Clavien-Dindo morbidity ≥ grade 3, n (%) | 2 (9.5) | 6 (28.6) | 0.1 | 2 (4.9) | 2 (4.9) | 1 | 3 (27.3) | 1 (9.1) | 0.3 |
| 30-day mortality, n (%) | 0 (0) | 3 (23.8) | 0.2 | 0 | 1 (2.4) | 1 | 2 (18.2) | 0 (0) | 0.5 |
| 90-day mortality, n (%) | 0 (0) | 3 (23.8) | 0.2 | 0 | 1 (2.4) | 1 | 2 (18.2) | 0 (0) | 0.5 |
| R1 resection, n (%) | 2 (10) | 0 (0) | 0.5 | 3 (7.3) | 2 (4.9) | 0.6 | 0 (0) | 0 (0) | 1 |
| Outcome Variables | 3D (n=13) | 4 RA (n=13) | p-value | 1 RA (n=9) | 4 RA (n=9) | p-value |
|---|---|---|---|---|---|---|
| EBL, mL (range) | 325 (0-1800) | 283.7 (50-800) | 0.5 | 371.1 (0-1200) | 211.1 (50-900) | 1 |
| OR Time, min (range) | 209 (98-279) | 277.8 (107-314) | 0.01 | 217.9 (60-480) | 235.7 (107-290) | 0.3 |
| LOS, days (range) | 9.4 (5-24) | 5.4 (1-11) | 0.03 | 3.9 (1-8) | 4.2 (1-8) | 0.8 |
| Conversion Rate, n (%) | 0 | 0 | 1 | 0 | 0 | 1 |
|
Postoperative Clavien-Dindo morbidity≥ grade 3, n (%) |
0 | 1 (7.7) | 1 | 0 | 1 (11.1) | 1 |
| 30-day mortality, n (%) | 2 (23.1) | 0 | 0.5 | 0 | 0 | 1 |
| 90-day mortality, n (%) | 2 (23.1) | 0 | 0.5 | 0 | 0 | 1 |
| R1 resection, n (%) | 0 | 3 (23.1) | 0.2 | 0 | 2 (22.2) | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



