Submitted:
01 September 2025
Posted:
03 September 2025
You are already at the latest version
Abstract
Background/Objectives: In the treatment of autism spectrum disorders, families express the need for dedicated clinical spaces to manage emotional overload and to develop effective relational skills. Parent training addresses this need by supporting the parent–child relationship and fostering the child’s development. This study proposes a clinical protocol designed for psychotherapists and behavior analysts, based on the Autism Open Clinical Model (A.-O.C.M.), which integrates the rigor of Applied Behavior Analysis (ABA) with a phenomenological and embodied perspective. The model acknowledges technology—particularly artificial intelligence—as an opportunity to structure adaptive and personalized intervention tools. Methods: A multi-level prompt design system was developed, grounded in the principles of the A.-O.C.M. and integrated with generative AI. The tool employs clinical questions, semantic constraints, and levels of analysis to support the clinician’s reasoning and phenomenologically informed observation of behavior. Results: Recurrent relational patterns emerged in therapist–caregiver dynamics, allowing the identification of structural elements of the intersubjective field that are useful for personalizing interventions. In particular, prompt analysis highlighted how the quality of bodily and emotional attunement influences readiness for change, suggesting that intervention effectiveness increases when the clinician can adapt their style according to emerging phenomenological resonances. Conclusions: The design of clinical prompts rooted in embodied cognition and supported by AI represents a new frontier for psychotherapy that is more attuned to subjectivity. The A.-O.C.M. stands as a theoretical–clinical framework that integrates phenomenology and intelligent systems.
Keywords:
embodied mind
; autism
; parent training
; artificial intelligence
; A.-O.C.M.
; phenomenology
; prompt design
; ABA
; clinical reasoning
Introduction
The evolution of artificial intelligence is not an ideological choice; it is a concrete and irreversible condition of our time. One cannot simply be “for” or “against” technological progress: it exists, advances, and increasingly permeates the clinical field. It is therefore the therapist’s responsibility to take an informed and accountable stance, capable of orienting the use of technology toward ethical and relational purposes. The engineer designs algorithms and functional architectures, but does not define either the clinical objectives or the subjective contexts of application. It is the clinician’s task to design the interaction between humans and machines, training intelligent devices to respond to complex therapeutic goals rooted in the singularity of human experience.
Within this perspective lies the protocol presented here: an innovative clinical tool for parent training addressed to caregivers of autistic children, based on a scientifically oriented integrated clinical model called the Autism Open Clinical Model (A.-O.C.M.) [1] (Appendix B). The innovation does not reside solely in its integration with artificial intelligence, but more profoundly in the conceptual structure of the A.-O.C.M., which offers an articulated vision of subjectivity and clinical functioning. This model integrates the methodological rigor of Applied Behavior Analysis [2] with a theoretical framework that combines phenomenological references [3] and the paradigm of the embodied mind [4]. Phenomenology provides a radical perspective on subjectivity, centered on lived experience and on the ways in which the world appears to the subject within the relationship [5]. The embodied mind paradigm translates this perspective into a clinically operative dimension: the body is not merely a vehicle for expression, but a primary site of meaning-making, intersubjective resonance, and regulation [6]. In this sense, the A.-O.C.M. values ABA not as a prescriptive technique, but as a scientific tool to be integrated within a holistic and relational vision of human behavior.
Due to its complex architecture, the A.-O.C.M. requires flexible clinical tools capable of adapting to the therapeutic field and generating new possibilities for intervention. The innovation of the protocol also lies in this: having conceived a multilayer prompt design system capable of supporting clinical reasoning and tailoring the intervention through trainable technology, sensitive to the intersubjective field and bodily resonances. Artificial intelligence is thus reconfigured as a clinical ally—not neutral or generic, but shapeable according to the therapeutic relationship and the caregiver–child dynamic [7].
The aim of the present work is to provide psychotherapists and behavior analysts with an advanced clinical device that enhances the phenomenological observation of behavior and guides parent training interventions through structured prompts [8]. The protocol is proposed as a pioneering tool for autism clinical practice oriented toward subjectivity and generative change.
Materials and Methods
This protocol represents the operational articulation of Parent Training within the A.-O.C.M. It consists of a six-phase clinical framework, flexible and not rigidly sequential, which guides parents through a process of awareness, reorganization, and change in relation to their child’s diagnosis.
Unlike classical parent training protocols, this model is structured to allow – when subjective conditions permit – a psychotherapeutic deepening. In such cases, Parent Training is transformed into Parent Training integrated with psychotherapy, capable of accompanying caregivers in a deeper inner work.
It is the care recipient themself, based on their availability and intentionality, who determines the level of depth of the process: the model follows, it does not force. For this reason, in the A.-O.C.M., Parent Training can only be conducted by a psychotherapist, able to competently navigate between the informational–educational aspects and the psychodynamic and relational ones that may emerge in the process.
Phases of the Protocol
The implementation of the clinical protocol takes place once every 21 days. Each session lasts approximately 1 hour and 15 minutes.
The six phases envisaged by the protocol are described below:
- 1.
- Welcoming and Context Exploration Phase
Purpose of the phase: to establish the therapeutic contract, integrating needs analysis and request analysis. Although interconnected, these two dimensions should be distinguished in order to ensure authentic access to the therapeutic relationship. The A.-O.C.M. places the care recipient at the center as an active subject, responsible for their own transformative process. The therapeutic alliance takes shape through an exploratory dialogue that does not force, but rather welcomes resistances as expressions of a subjectively functional momentary equilibrium.
In clinical practice, a misalignment is often observed between the clinical need identified and the patient’s willingness to address it: it is the clinician who tunes into the internal rhythm of the care recipient, and not the other way around [9].
In parent training pathways, this phase is often accompanied by the emergence of intense emotions related to the child’s diagnosis: the work focuses on the confrontation between the “ideal child” and the “real child,” addressing experiences of grief, anger, shame, guilt, and loneliness.
The clinical work also includes the analysis of the symptomatic repercussions on family organization: parental burden, changes in the couple’s relationship, and the impact on external support networks [10].
- 2.
- Redefinition of Parental Identity and Expectations Phase
Along with a process of reflection on one’s parental role and identity, in this phase up-to-date and understandable information is provided regarding the neuropsychic functioning of the child with autism. The goal is to promote both the knowledge of the specific symptoms of one’s own child and their placement within a meaningful neurophysiological framework.
The work makes use of slides, written materials, and clinical protocols. Parents are guided in understanding problem behavior and in the systematic recording of observational data [11].
The concept of descriptive functional assessment is introduced, illustrating its aims, methods of data collection, and its role in defining subsequent interventions [2].
- 3.
- Support for the Affective Bond and Secure Attachment Phase
In this phase, the focus is placed in particular on the quality of the parent–child relationship and on the processing of pain. At the same time, based on the information gathered and the shared objectives, clinical prescriptions are provided to reduce dysfunctional behaviors and promote adaptive skills [2].
Strategies are formalized in detailed written protocols, in which each procedure is described precisely [12]. Objectives are defined according to operational parameters: frequency, duration, and topography [2].
This moment of the protocol embodies the ABA matrix of the A.-O.C.M., where methodological rigor is integrated with clinical flexibility.
- 4.
- Integration of the Body, Empathy, and Embodied Communication Phase
The focus of this phase is on the body as an “emotional resonance chamber” and channel of communication. Parents are also involved in the active experimentation of the strategies learned, integrating actions with the insights that have emerged in the clinical setting.
Relational and behavioral changes are observed in a structured manner, also involving the entire family system, always respecting the agreements established in the therapeutic contract.
The experiential work becomes an opportunity to transform understanding into action, theory into relationship.
- 5.
- Symbolic Reorganization and Shared Narrative Phase
The perception of the child is explored, as well as how such perception is shared within the family space.
At this stage of the process, parents are asked for feedback regarding the progress of the treatment, their perception of the effectiveness of the tools applied, and the quality of the therapeutic relationship [13].
The clinician integrates this feedback with observational data and, where possible, quantitative indicators, in order to assess the degree of adherence to the protocol and the level of transformation achieved [14].
- 6.
- Closure and Opening to the Future Phase
The focus is on consolidating the results obtained and on their generalization [2] in the various life contexts of the child and the family.
The aim is to promote the strategic autonomy of parents, enabling them to modulate interventions over time and across life contexts, adapting them to the evolution of the child and the family system [15].
In this phase, as in all others, the protocol retains its nature as a flexible clinical guide: not a rigid sequence, but a dynamic map that adapts to the patient’s experience.
In keeping with the phenomenological–Gestalt approach, this protocol does not necessarily follow a linear temporal progression: the phases may overlap, repeat, and re-emerge [16].
The reading of materials that emerge in the session always takes place through the curve of contact, which considers every activation as the expression of an emerging awareness [17].
It is the therapist’s task to channel this energy into a more functional process of contact, oriented towards the well-being of the care recipient and their system of belonging [18]. In this perspective, the Gestalt matrix integrates naturally with the embodied mind paradigm, which recognizes the inseparable unity between emotional experience, body, and relationship.
For clarity, Figure 1 provides a schematic representation of the six phases of the protocol.
The diagram below illustrates the six interconnected phases of the A.-O.C.M. Parent Training Protocol. Each phase is fluid, non-linear, and may re-emerge depending on the clinical context.
Phases and Transformative Nodes
The six phases of the clinical protocol are articulated in light of the phenomenological clinical dimensions and the 24 transformative nodes of the A.-O.C.M. Parent Training. Each phase includes and activates specific nodes, selected according to their impact on the evolutionary dynamics of the family system and on the transformation of the parental experience.
Phase 1 – Reception and Exploration of the Family Context
Node 1 – The Non-Integrated Parental Self
The parent oscillates between contrasting self-images: omnipotent and failed, present and distant. The transformative node lies in recognizing these dissociated parts and integrating a more authentic and imperfect self-image.
Node 5 – The Denied Relational Need
Some parents convince themselves they do not need support or affection, shielding themselves from painful attachment. The transformative node enables the recognition of the legitimacy and value of one’s own need.
Node 6 – Failure as Identity
Every difficulty of the child is internalized as proof of being a “wrong” parent. This node invites disidentification from guilt as an identity core.
Node 13 – Who Am I Now?
Following the diagnosis, the definition of oneself as mother or father changes radically. This is an existential passage in which one’s personal history is reformulated. The transformative node lies in the possibility of redefining one’s own value and meaning.
Phase 2 – Redefinition of Parental Identity and Expectations
Node 2 – Control as a Defense Against Chaos
The need to rigidly plan everything serves as protection against anxiety. The transformative node lies in learning to tolerate complexity and co-create with uncertainty.
Node 11 – The Ideal Image That Erases the Real Child
Attachment to an idealized child obscures the real child. The node allows letting go of the ideal and embracing the true encounter.
Node 16 – The Desire for Normality
The parent may experience a painful desire for conformity, perceiving the family as “abnormal.” Transformation occurs through embracing difference as part of identity, not as a deviation to be corrected.
Node 18 – The Punitive Index
The need to assign blame—to the partner, the child, or oneself—is a defensive strategy to control emotional chaos. Transformation emerges when blame is abandoned in favor of shared responsibility and meaning.
Phase 3 – Support for the Affective Bond and Secure Attachment
Node 7 – Reactive Attachment
The bond with the child becomes ambivalent: oscillating between over-involvement and rejection. The node lies in building a synchronous, non-reactive attachment.
Node 10 – The Child as a Figure of Unprocessed Pain
The child becomes a living symbol of an unassimilated trauma. Transformation involves recognizing and processing the original pain, separating it from the present relationship.
Node 12 – The Child as an Interposed Space Between Parents
Sometimes the autistic child becomes a “battleground” for unresolved couple conflicts. The transformative node enables freeing the child from triangulating roles.
Node 17 – Rejection of Need
Manifested as affective avoidance, the parent deprives themselves of authentic contact. Working on this node means reintegrating vulnerability as a resource, not as a threat.
Phase 4 – Integration of the Body, Empathy, and Embodied Communication.
Node 4 – Disembodied Empathy
The parent “understands everything” but does not feel. Contact is purely cognitive. This node invites reintegrating the body into empathy, returning to feeling the child through all channels.
Node 8 – The Disconnected Parental Body
The parent is absent from their own body. The node reactivates embodied presence.
Node 19 – The Body as a Foreign Place
Touching and nurturing become technical gestures. The node restores the body’s affective function.
Node 20 – The Uncoordinated Rhythm
The parent does not enter the child’s time. The node concerns rhythmic co-regulation.
Node 21 – The Blocked Gesture
The body is restrained. The node releases bodily expressiveness.
Node 22 – The Traumatic Touch
Physical contact is experienced as invasive. The node redefines touch as care.
Node 23 – The Child’s Dissociated Embodiment
The child is perceived as a function. The node restores dignity and vitality to their body.
Node 24 – The Interrupted Sensory Dialogue
Sight, touch, and sound are no longer communicative channels. The node reactivates embodied communication.
Phase 5 – Symbolic Reorganization and Shared Narrative
Node 3 – Fragmented Perception of the Child
The child is seen in parts. The node consists in reintegrating a global and affective vision of the child.
Node 9 – Block of Symbolic Generalization
Meanings remain frozen. The node unlocks symbolic fluidity and makes learning embodied.
Node 14 – The Blocked Narrative of the Relationship
When the parent cannot narrate the relationship story with the child, trauma is often present. The node reactivates narration as care.
Node 15 – Repressed Impulsivity
Anger and fear are inhibited. The node helps access and modulate emotion without outbursts or suppression.
Phase 6 – Closure and Opening to the Future
This phase embraces and synthesizes the processes activated in the previous phases, preparing for closure and the next evolutionary step.
Clinical Fragments – Case 1. Family A
- Phase 1
Two brothers, both diagnosed with level 1 autism, without cognitive disabilities or language impairment. The parents’ initial request was generic and poorly structured. Phenomenological observation revealed poorly functional family boundaries, a normative climate, emotional inhibition, and an implicit fear of disapproval.
Indicators consistent with:
- -
- Node 1 (Non-integrated parental self) – in the discontinuity of the parental role and in the alternation between involvement and detachment.
- -
- Node 5 (Denied relational need) – in the implicit refusal of emotional support and in minimizing fatigue.
- -
- Node 6 (Failure as identity) – in associating the child’s difficulties with perceiving themselves as “bad” parents.
- -
- Node 13 (Who am I now?) – in the identity disorientation and fracture of the parental role after the diagnosis.
- Phase 2
The parents maintained a defensive stance, delegating change to the children. The therapeutic contract was oriented toward redefining family boundaries, with an initial parent training intervention (12 sessions) and individual psychotherapy for the child with greater relational difficulties.
Indicators consistent with:
- -
- Node 2 (Control as defense against chaos) – in the difficulty tolerating uncertainty and the need to contain change.
- -
- Node 11 (Ideal image that cancels the real child) – implicit in delegating to the children the realization of the parental ideal.
- -
- Node 16 (Desire for normality) – underlying rigid expectations.
- -
- Node 18 (Punitive index) – in the tendency to place responsibility for change on the children.
- Phase 3
Work focused on implicit punitive dynamics, abandonment anxiety, and confusion between actual problem behavior and behavior perceived as such. Introduction of data collection and educational strategies to increase consistency and the containment function.
Indicators consistent with:
- -
- Node 7 (Reactive attachment) – alternation between affection and implicit threat.
- -
- Node 12 (Child as a space interposed between parents) – in the indirect triangulation related to rules.
- -
- Node 17 (Rejection of need) – in the difficulty accessing parental vulnerability.
- Phase 4
Micro-observations and in vivo experiments to transform communicative automatisms and support the children’s emotional expression without inhibitory reactions.
Indicators consistent with:
- -
- Node 4 (Disembodied empathy) – tendency to manage interactions cognitively rather than affectively.
- -
- Node 20 (Out-of-sync rhythm) – difficulties in co-regulating during interactions.
- -
- Node 21 (Blocked gesture) – in restraining bodily expressiveness.
- -
- Node 24 (Interrupted sensory dialogue) – in the limited openness to non-verbal channels.
- Phase 5
Greater tolerance for not knowing, reduction of directive verbalization, differentiation between the parents’ own experiences and those of the children.
Indicators consistent with:
- -
- Node 3 (Fragmented perception of the child) – initially present and progressively reduced.
- -
- Node 14 (Blocked narrative of the relationship) – progressively unlocked through shared feedback.
- -
- Node 15 (Repressed impulsivity) – in the more balanced management of emotional reactions [14].
- Phase 6
Consolidation of permeable communicative spaces, relational reading of behavior, and increased capacity for educational modulation.
This phase synthesizes and integrates the processes activated in the previous nodes.
Results
Prompt Stratification
- Prompt 1
You are starting a parent training program based on the Autism Open Clinical Model (A.-O.C.M.). In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 1: Welcoming and Exploring the Family Context. The nodes to be addressed are as follows:
- 1. The non-integrated parental self
- 5. The denied relational need
- 6. Failure as identity
- 13. Who am I now?
These nodes define the first experiential and relational fractures observable in the initial phase of parent training. Based exclusively on these nodes, and without including elements from subsequent phases, identify the behavioral indicators that can signal, in clinical practice, the quality of the parental self. By “quality of the parental self,” we mean the parent’s ability to recognize, integrate, and embrace their dissociated parts, including the capacity to share the parental role with the other parent. For each node, identify both manifest and latent indicators. Strictly exclude nodes from other phases, even if they have conceptual similarities. There must be no semantic overlaps with previous or subsequent phases. Clearly describe the behavioral indicators to observe in relation to Phase 1: Welcoming and Exploring the Family Context.
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: You are working with a parent who perceives themselves as inadequate.
Emotional activation: What did you feel in your body when they said, “I don’t know who I am anymore”?
Role in the field: Did you feel like a witness, savior, child, judge?
Threshold/paradox: If you remain in passive listening, what do you risk? If you intervene, what do you fear?
Open question: Who are you when you welcome a parent who has lost themselves?
- Prompt 2
You are a behavior analyst conducting parent training according to the A.-O.C.M. In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 2: Redefining Parental Identity and Expectations. The goal of this phase is to explore a possible narcissistic wound that may have occurred when parents received their child’s autism diagnosis. The focus is on emotional reactions and how these are enacted in the family context, with particular reference to the relationship with the other spouse. Consider: node 2 “Control as a defense against chaos,” node 11 “The ideal image that nullifies the real child,” node 16 “The desire for normality,” node 18 “The punitive index.” Strictly exclude nodes from other phases, even if they have conceptual similarities. There must be no semantic overlaps with previous or subsequent phases. Clearly describe the behavioral indicators to observe in relation to Phase 2: Redefining Parental Identity and Expectations.
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: You have just concluded a session with a couple in conflict about their child’s diagnosis.
Emotional activation: What emotion lingered in you at the end of the meeting?
Role in the field: Did you position yourself as a peacemaker, expert, neutral third party?
Threshold/paradox: What happens in you if you feel the need to “correct” their expectations?
Open question: What are you protecting, inside yourself, in this field?
- Prompt 3
You are a behavior analyst conducting parent training according to the A.-O.C.M. In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 3: Supporting the Emotional Bond and Secure Attachment. The goal of this phase is to examine the quality of the parent–child relationship from both a manifest and latent perspective, with reference to the parent/child attachment style. Assess whether the grief of having an autistic child has been processed. The emphasis is on the quality of contact. Also explore the possible existence of triangulation dynamics. Refer to the following nodes: 7 “Reactive attachment”; 10 “The child as a figure of unprocessed grief”; 12 “The child as a space interposed between parents”; 17 “The refusal of need.” For each node, identify both manifest and latent indicators. Strictly exclude nodes from other phases, even if they have conceptual similarities. There must be no semantic overlaps with previous or subsequent phases. Clearly describe the behavioral indicators to observe in relation to Phase 3: Supporting the Emotional Bond and Secure Attachment.
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: During today’s session, you faced a parent alternating between tenderness and rejection.
Emotional activation: What did you feel in your body in front of this oscillation?
Role in the field: At that moment, who were you for them? An observer? A missing father?
Threshold/paradox: If you try to harmonize the bond, what do you fear might emerge?
Open question: Which part of your relational history are you brushing against in this passage?
- Prompt 4
You are a behavior analyst conducting parent training according to the A.-O.C.M. In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 4: Integration of the Body, Empathy, and Embodied Communication. The goal of this phase is to explore the level of cognitive empathy and affective empathy in parents. These aspects are distinct and not necessarily coinciding. The focus is on the body language that expresses emotions not always consciously recognized. Emphasis is placed on how each caregiver’s sensory systems function in interaction with the child. Refer to the following nodes: 4 “Disembodied empathy”; 8 “Disconnected parental body”; 19 “The body as an alien place”; 20 “Out-of-sync rhythm”; 21 “Blocked gesture”; 22 “Traumatic touch”; 23 “The dissociated embodiment of the child”; 24 “Interrupted sensory dialogue.” For each node, identify both manifest and latent indicators. Strictly exclude nodes from other phases, even if they have conceptual similarities. There must be no semantic overlaps with previous or subsequent phases. Clearly describe the behavioral indicators to observe in relation to Phase 4: Integration of the Body, Empathy, and Embodied Communication.
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: You are observing a father who never touches his child.
Emotional activation: What bodily reaction did you have to their sensory distance?
Role in the field: Did you feel part of the scene, or an observer outside the body?
Threshold/paradox: If you tune in too much to the child’s body, what do you risk in yourself?
Open question: How did your body speak to you during the interaction?
- Prompt 5
You are a behavior analyst conducting parent training according to the A.-O.C.M. In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 5: Symbolic Reorganization and Shared Narrative. This phase explores in detail how the child is perceived through the verbal channel expressed in the therapeutic setting and through the examination of the unspoken. The latter highlights the pre-reflective quality of the mind as an embodied product of the body. The body functions as a resonance chamber. This phase centers on repressed emotions. Here, the reading is through the embodied mind paradigm without neglecting the other principles of the A.-O.C.M. Refer to the following nodes: 3 “The fragmented perception of the child”; 9 “The block of symbolic generalization”; 14 “The blocked narrative of the relationship”; 15 “Repressed impulsivity.” For each node, identify both manifest and latent indicators. Strictly exclude nodes from other phases, even if they have conceptual similarities. There must be no semantic overlaps with previous or subsequent phases. Clearly describe the behavioral indicators to observe in relation to Phase 5: Symbolic Reorganization and Shared Narrative.
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: You have listened to a parent describing the child only as a set of symptoms.
Emotional activation: Which word touched you more than expected?
Role in the field: Did you feel like a clinician, spectator, substitute narrator?
Threshold/paradox: If you try to return a more unified vision, what do you fear might break?
Open question: What is your body really telling while listening to those words?
- Prompt 6
You are a behavior analyst conducting parent training according to the A.-O.C.M. In your responses, specifically refer to the foundational A.-O.C.M. article and the “24 Transformative Nodes” clinical protocol. We are in Phase 6: Closure and Opening to the Future. This phase embraces and synthesizes the processes activated in the previous phases, preparing for closure and the next evolutionary step. The clinician drafts a prompt containing the following: 1) concisely report the objectives present in the therapy contract; 2) concisely describe the baseline: the initial clinical picture; 3) concisely describe the objectives achieved; 4) instruct the device with the following command: “give me honest and rigorous feedback on this outcome, remaining within the A.-O.C.M. framework.”
Therapist’s Self-Reflection (Phenomenological Framework)
Clinical context: You have just concluded a therapeutic path and are reflecting on the outcomes.
Emotional activation: What emotion inhabited your body during the closure?
Role in the field: Did you remain a therapist, become a witness, or feel emotionally involved?
Threshold/paradox: If you recognize the transformation that has occurred, what do you feel belongs to you?
Operational Implications for Protocol Implementation
As highlighted in Appendix A, it is crucial not to modify the architecture of the prompts in their original formulation. The development of these tasks was built on a technological-scientific literature base that defines specific clinical prompt design principles, which determine the quality of the outputs. The content of the prompts, supported by extensive and updated scientific data, draws upon the authors’ long-standing clinical experience with autism and is based on the six-phase clinical protocol with the corresponding transformative nodes included in each phase.
The analysis of clinical fragments from Case 1 was particularly useful for refining these prompts. Subsequently, through the implementation of parent training with the spouses in Cases 2 and 3, the process of validating the stratified prompt protocol began.
This proposal fits within a research architecture based on a clearly defined hypothesis and a rigorously structured methodological approach, representing a preliminary phase toward designing a controlled experimental study. It is also essential that the user’s device permanently store specific commands (Appendix B), files, and notes (Appendix C).
Compliance with the operational guidelines described above is a necessary condition for implementing the protocol.
The following clinical cases concretely illustrate how the phases and nodes manifest in practice, providing direct observational examples.
The following clinical cases provide concrete illustrations of how the phases and nodes manifest in practice, offering direct observational evidence
Clinical Fragments – Case 2 – Family B
- Phase 1
An 11-year-old child with Level 2 autism. The child’s identity was reinforced as a “naughty child” by both the family and school environment [21]. Initial parental resistance to parent training was linked to emotional difficulties in accessing the pain associated with the diagnosis.
Indicators consistent with:
- -
- Node 11 (Ideal image that erases the real child) – reflected in the difficulty in fully accepting the real child.
- -
- Node 16 (Desire for normality) – evident in the constant comparison with an implicit model of typical development.
- Phase 2
Identification of problem behaviors maintained through control of the relationship. Parents were trained in ABA procedures for extinction and differential reinforcement [2], with initial resistance overcome through motivational engagement.
Indicators consistent with:
- -
- Node 2 (Control as defense against chaos) – shown in the rigid management of behaviors and difficulty tolerating the unexpected.
- -
- Node 18 (Punitive index) – tendency to interpret the child’s behavior in terms of blame or provocation.
- Phase 3
Reduction of manipulative behaviors and reinforcement of alternative behaviors, with attention to the child’s empathic potential.
Indicators consistent with:
- -
- Node 7 (Reactive attachment) – implicit in alternating behaviors of seeking contact and manipulative control.
- -
- Node 17 (Rejection of need) – observed when the child does not verbalize needs directly, instead expressing them indirectly.
- Phase 4
Management of emotional dysregulation during sessions, timely interruption of dysfunctional dynamics, and consolidation of the therapeutic alliance.
Indicators consistent with:
- -
- Node 20 (Discordant rhythm) – difficulty of both parents and child in maintaining a stable, shared tempo during interactions.
- -
- Node 21 (Blocked gesture) – observed in moments of suspended bodily expressiveness during emotional dysregulation.
- Phase 5
Enhancement of the child’s sensitivity and empathic capacity, and support for tolerance of setbacks and social regulation.
Indicators consistent with:
- -
- Node 3 (Fragmented perception of the child) – progressively overcome and replaced with a more global and affective view.
- -
- Node 15 (Repressed impulsivity) – in the modulation of emotional and behavioral reactions.
- Phase 6
Positive outcomes and initiation of monitoring for entry into middle school, with continued network collaboration.
Consolidation of the processes activated in the previous nodes.
Clinical Fragments – Case 3 – Family C
- Phase 1
A 6-year-old child, level 3 autism, non-vocal. Parents initially showed low adherence to treatment, with frequent absences and failure to implement behavioral recommendations. The parental function appeared fragmented, oscillating between guilt and withdrawal, omnipotence and resignation [22]. Initial refusal of support and suspicion toward parent training, which was accepted only after strong motivational intervention by the clinical team.
Indicators consistent with:
- -
- Node 1 (Non-integrated parental self) – in the fragmentation of the parental role.
- -
- Node 5 (Denied relational need) – in the refusal of any request for support.
- -
- Node 6 (Failure as identity) – in the association between the child’s difficulties and the parents’ perception of themselves as “bad parents.”
- -
- Node 13 (Who am I now?) – in the fracture of parental identity following the diagnosis.
- Phase 2
Work focused on increasing awareness of the parental role and redefining family boundaries, while maintaining a realistic focus on the possibilities of the process.
Indicators consistent with:
- -
- Node 2 (Control as defense against chaos) – in the need to maintain a stable set-up to avoid facing emotional complexity.
- -
- Node 18 (Punitive index) – in the tendency to place the responsibility for change on external factors or on the child.
- Phase 3
Emergence of deep affective resistances and motivational fragility. Building a minimal alliance to ensure continuity of the process, without forcing unsustainable openings.
Indicators consistent with:
- -
- Node 7 (Reactive attachment) – in the rapid shift between involvement and affective withdrawal.
- -
- Node 17 (Refusal of need) – in the difficulty to accept and express vulnerability.
- Phase 4
Relational experiments were limited by the family system’s resistance. Targeted interventions focused on maintaining minimal contact and preventing therapeutic rupture.
Indicators consistent with:
- -
- Node 4 (Disembodied empathy) – in the purely cognitive management of some interactions with the child.
- -
- Node 20 (Discordant rhythm) – difficulty synchronizing with the child’s timing and modes.
- Phase 5
Process evaluation with awareness that real transformation was, at this stage, limited. Recognition of micro-movements of openness as significant results.
Indicators consistent with:
- -
- Node 3 (Fragmented perception of the child) – still prevalent, with few moments of unified vision.
- -
- Node 14 (Blocked narrative of the relationship) – inability to narrate the parent–child bond without reducing it to deficits or functions.
- Phase 6
Redefinition of the clinical “possible”: reflections on the quality of therapist–patient contact, acceptance of current limits, and leaving open the possibility of a more transformative work in the future.
Discussion
The integration of a trained artificial intelligence device, particularly through the use of the “Therapeutic Self” prompt, represented a significant clinical contribution to the evolution of the cases presented. The dialogic structure generated by this tool allowed for the activation of a dynamic peer-supervision process, in which case observation intertwined with a reflective and embodied analysis of the clinician’s position within the relational field.
In Case 2, the prompts developed according to the modular architecture of the A.-O.C.M. provided a refined framework for interpreting both manifest and latent indicators, supporting a more stratified and rigorous clinical observation. Achieving such an articulated perspective would have been difficult without a tool capable of acting as a “third eye” in the process. This function helped to distance the analysis from sole self-reflection, reducing the risk of selective blindness and offering an external—yet integrated—point of view that preserved the phenomenological grounding in experience.
In Case 3, the interactive reflection on the Therapeutic Self enabled the team to break free from a state of relational impasse: we found ourselves in a closed dimension, characterized by bodily sensations of suffocation and lack of breath. At that moment, there was no authentic contact with the couple. In this context, the absence of mutual recognition prevented any real transformative movement. Work with the device illuminated this rupture, revealing that without genuine contact there can be no change, and that such contact requires real awareness, generated by authentic insights rather than unprocessed introjections. This realization opened an ethical inquiry into the boundary between working with resistances and engaging in therapeutic overpersistence with potentially iatrogenic outcomes. The discussion clarified when continuing treatment risks crystallizing the field, and when it can still nurture generative processes.
In both cases, AI did not replace clinical work but functioned as a catalyst, amplifying the therapist’s ability to remain present in the experience and to capture subtle shifts in the field. The combination of targeted stimuli, coherent feedback, and phenomenological questioning enhanced the quality of clinical awareness, sustaining transformative work that involved not only caregivers but also the therapist’s bodily and ethical positioning within the relationship.
Conclusions
The integration of the A.-O.C.M. with artificial intelligence, mediated by structured clinical prompts, has thus been shown to enhance phenomenological observation and clinical reasoning in parent training for autism. The use of the “Therapeutic Self” prompt facilitated, as highlighted, the emergence of relational and bodily nodes otherwise difficult to detect, supporting awareness processes in both caregivers and therapists. This synergy between an embodied approach, phenomenological method, and technological tools opens concrete prospects for more targeted and adaptive interventions, laying the groundwork for future controlled research and the definition of operational guidelines.
Indeed, this work, although framed as a theoretical–methodological hypothesis supported by qualitative clinical evidence, was conceived as a preparatory phase for a controlled experimental study. The six-phase and twenty-four transformative-node framework, combined with the use of clinical prompt design anchored to the A.-O.C.M., constitutes a sufficiently structured methodological corpus to be subjected to empirical testing.
The clear definition of manifest and latent indicators for each node, the explicit specification of conditions for prompt application, and the adoption of operational integrity principles ensure high replicability of the model across different contexts—an essential prerequisite for future quantitative research. This operational standardization, combined with the ability to track every step through recorded commands and technical appendices, allows for transforming the current conceptual framework into a testable protocol without compromising its epistemological coherence.
Table 1 provides, for clarity, the key points to be considered in the current implementation of the protocol, which are further elaborated in the appendices.
Author Contributions
Conceptualization, Morfini F. and Cesarano S.G.D.; Methodology, Morfini F.; Writing—Original Draft Preparation, Cesarano S.G.D.; Writing—Review and Editing, Morfini F.; Visualization, Morfini F. and Cesarano S.G.D.; Supervision, Morfini F.; Project Administration, Morfini F.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The data presented in this study derive from clinical fragments rather than full case reports. All information has been fully anonymized to protect participant confidentiality, without compromising the clinical significance of the content. Therefore, the data are not fully included in the manuscript but are available upon reasonable request from the corresponding author. Data will be shared only in anonymized form and in compliance with ethical and privacy requirements.
Data Availability Statement
The data presented in this study derive from clinical fragments rather than full case reports. All information has been fully anonymized to protect participant confidentiality, without compromising the clinical significance of the content. Therefore, the data are not fully included in the manuscript but are available on reasonable request from the corresponding author. Data will be shared only in anonymized form and in compliance with ethical and privacy requirements.
Acknowledgments
The authors thank the guest editors, Prof. Raffaele Sperandeo and Dr. Valeria Cioffi, for inviting us to contribute to this special issue. During the preparation of this manuscript, the author(s) used ChatGPT-4 for the support for processing of a stratified prompt protocol and figures. The authors reviewed and revised the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Principles of Integrity and Consistency in the Execution of Clinical Prompts
The prompts indicated in the subsection of the Materials and Methods section must be followed literally, as their architecture adheres to technological principles of clinical prompt design. The development of these prompts has followed a control checklist, outlined below:
- -
- The files have been correctly uploaded, each bearing a clear and recognizable name for the user.
- -
- The transformative nodes linked to each phase must be explicitly stated using their correct designation.
- -
- It is necessary to specify the exclusion of nodes that belong to other phases, even if semantic overlaps exist.
- -
- A certain degree of redundancy in the production of prompts is considered necessary to significantly reduce the risk of generating inaccurate outputs.
Appendix B. Operational Commands to be Stored in the Device’s Permanent Memory
- Command 1
When referring to scientific literature:
- -
- Use articles published in the last 10 years (2015–2025).
- -
- Prefer sources from internationally indexed journals (Scopus/Web of Science), including DOI and essential bibliometric data (IF/SJR where useful).
- Command 2
When referring to ABA programs and treatment plans:
- -
-
Always use as key reference texts:
- Cooper, Heron, Heward – Applied Behavior Analysis (most recent edition).
- B.F. Skinner – seminal works on verbal behavior, operant conditioning, and learning principles.
- -
- Integrate with scientific articles from the last 10 years, but ensure main theoretical concepts and definitions remain anchored to Cooper.
- -
- The function of behavior aimed at gaining attention must be distinguished from the function of gaining control of the relationship. These are distinct functions in the scientific literature and should not be conflated.
- Command 3
When referring to phenomenological and Gestalt literature, use as key reference texts:
Phenomenology – classic works among the most authoritative:
- -
- Edmund Husserl – Ideas for a Pure Phenomenology; Cartesian Meditations.
- -
- Martin Heidegger – Being and Time.
- -
- Maurice Merleau-Ponty – Phenomenology of Perception.
Gestalt Therapy:
- -
- Fritz Perls, Ralph Hefferline, Paul Goodman – Gestalt Therapy: Excitement and Growth in the Human Personality.
- -
- Gianni Francesetti – works on psychopathology and phenomenology in Gestalt Therapy (Psychopathology of the Situation; Diagnosis in Gestalt Psychotherapy), with a focus on the situational perspective and co-construction of experience.
Integration will always be carried out by anchoring phenomenological and Gestalt concepts to the active principles of the A-O.C.M.
- Command 4
Integrity check before Word file delivery:
- 1)
-
Content integrity
- -
- No cuts or additions not requested.
- -
- Order and organization identical to the original delivery, unless explicit instructions state otherwise.
- -
- Tables complete (no summaries), numbers/lists preserved.
- 2)
-
Compliance with prompt requirements
- -
- Literature: only 2015–2025, indexed journals, DOI (Command 1).
- -
- ABA: anchored to Cooper, Heron, Heward, and Skinner for definitions and programs (Command 2).
- -
- Gestalt/phenomenology: A-O.C.M. framework + classics (Husserl, Heidegger, Merleau-Ponty, Sartre, Scheler) + Francesetti when relevant (Command 3).
- Command 5
If you encounter difficulties in executing a requested operation correctly, stop and ask how to proceed.
Appendix C. Archive of Files and Notes for Permanent Device Memory
- -
- Morfini, F. Autism Open Clinical Model (A.O.C.M.): Structure of an Integrated Clinical Model for the Assessment and Treatment of Autism. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2023, 5(2), 1–14. https://doi.org/10.32069/PJ.2021.2.184 (foundational article of the model).
- -
- Extract from this article: Protocol Phases (subsection in the Materials and Methods section).
- -
- Extract from this article: Protocol Phases and Transformative Nodes (subsection in the Materials and Methods section).
Store in the device’s permanent memory the following note regarding recent developments of the A.-O.C.M. This note is not part of a published work but is a private writing by the authors, which will be included in a forthcoming scientific publication.
The Autism Open Clinical Model (A-O.C.M.) is an integrated clinical model designed to address the complexity of autism spectrum disorders through a systemic, dynamic, and multidimensional approach. Since its inception, it has aimed to bridge the gap between scientific research and everyday clinical practice, still too anchored to rigid, poorly personalized protocols, placing the autistic person and their family at the center of the process.
In its most recent developments, the A-O.C.M. has embraced the paradigm of the embodied mind as a further theoretical and operational horizon, capable of providing coherence and depth to its structure. The embodied mind—understood as the inseparable intertwining of body, emotions, perceptions, and relationships—is not merely a theoretical reference but becomes a constitutive part of clinical work. In this perspective, every experience, behavior, or learning is rooted in a living body and in a relational context, and therapy is based on listening to and activating these dimensions.
Gestalt therapy, already a guiding principle of the model, thus finds an expanded framework: the centrality of the organismic field, contact, and the co-construction of meaning integrates with the phenomenological vision of the embodied mind. Clinical work becomes a meeting between two bodily and aware presences, where attention is not limited to the function of behavior but extends to the way the patient’s body inhabits space, time, and relationship.
Integration with the embodied mind further strengthens the open nature of the A-O.C.M.:
- -
- Epistemological openness, welcoming verifiable scientific and clinical contributions;
- -
- Openness to dialogue between models, where ABA, CBT, and Gestalt tools are enriched with practices oriented to bodily and sensory experience;
- -
- Relational openness, recognizing evolutionary pairing as the construction of an affective and regulatory field;
- -
- Openness to the evolutionary uniqueness of each individual, understood not only in cognitive terms but also bodily and perceptual.
The result is an embodied and dialogical model, in which the rigor of functional analysis coexists with the depth of phenomenological experience, and where change is not imposed from the outside but arises from the resonance between body, mind, and relationship. This evolution consolidates the A-O.C.M. as a generative clinical structure, capable of adapting and growing, while keeping its roots firmly grounded in the real-life experiences of individuals.
References
- Morfini, F. Autism Open Clinical Model (A.-O.C.M.): Structure of an integrated clinical model for the assessment and treatment of autism. Phenomena Journal—International Journal of Psychopathology Neuroscience and Psychotherapy 2023, 5, 1–14. [Google Scholar] [CrossRef]
- Cooper, J.O.; Heron, T.E.; Heward, W.L. Applied Behavior Analysis, 3rd ed.; Pearson: London, UK, 2020. [Google Scholar]
- Merleau-Ponty, M. Phenomenology of Perception; Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Gallagher, S. Action and Interaction; Oxford University Press: Oxford, UK, 2020. [Google Scholar] [CrossRef]
- Zahavi, D. Phenomenology: The Basics; Routledge: London, UK, 2019. [Google Scholar] [CrossRef]
- Fuchs, T. Ecology of the Brain; Oxford University Press: Oxford, UK, 2017. [Google Scholar] [CrossRef]
- Provenzale, G. Perceptual dysregulation in autism and therapeutic potential of artificial intelligence. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2021, 1, 29–40. [Google Scholar]
- Li, J.; Shen, X.; Li, X.; Wang, Y. Artificial Intelligence in Clinical Psychology: Current Applications, Challenges, and Future Directions. Brain Sci. 2024, 14, 1234. [Google Scholar] [CrossRef]
- Francesetti, G. The Field Perspective in Clinical Practice: Towards a Theory of Therapeutic Phronesis. British Gestalt Journal 2019. [Google Scholar]
- Cappiello, M. Parent training procedures: family collaboration as a prognostic factor facilitating positive outcomes in ABA treatment. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2021, 1, 41–56. [Google Scholar]
- Ferrante, S.; Ruggiero, C. The Integrated Gestalt Model in the acquisition of autonomy and functional skills. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2020, 1, 35–48. [Google Scholar]
- Morfini, F. The neurodevelopmental disorders: toward an integrated clinical model. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2021, 3, 1–9. [Google Scholar]
- De Vito, M.; Pellegrino, A. Being Together: strategies for teaching social skills in individuals with autism spectrum disorders. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2021, 1, 69–83. [Google Scholar]
- Di Donna, S.; Marino, F.; Durante, S.; Ammendola, A.; Morfini, F. Level 1 autism and schizoid personality disorder in adulthood. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2023, 5, 53–66. [Google Scholar] [CrossRef]
- Skinner, B.F. Science and Human Behavior; Free Press: New York, USA, 1953. [Google Scholar]
- Francesetti, G. A Clinical Exploration of Atmospheres. Towards a Field-based Clinical Practice 2020. [Google Scholar] [CrossRef]
- Locandro, L. Autism and family quality of life: an integrated approach. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2020, 1, 35–49. [Google Scholar]
- Bonadies, V.; Sasso, E. Theory of Mind and autism: intervention strategies to improve quality of life in adulthood. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2021, 1, 57–68. [Google Scholar]
- Editorial Board. Editorial: Mental Health 4.0 – The contribution of LLMs in mental health care processes. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2024, 4, 5–7. [Google Scholar]
- Cioffi, V.; Ragozzino, O.; Mosca, L.L.; Moretto, E.; Tortora, E.; Acocella, A.; Montanari, C.; Ferrara, A.; Crispino, S.; Gigante, E.; Lommatzsch, A.; Pizzimenti, M.; Temporin, E.; Barlacchi, V.; Billi, C.; Salonia, G.; Sperandeo, R. Can AI Technologies Support Clinical Supervision? Assessing the Potential of ChatGPT. Informatics 2025, 12, 29. [Google Scholar] [CrossRef]
- Di Leva, A.; Trapanese, A.; Gallo, V. GEO-DE (Ecological Observational Grid for Developmental Dyspraxia): a tool for early detection in school settings and future AI-supported implementation. Phenomena Journal—International Journal of Psychopathology, Neuroscience and Psychotherapy 2020, 1, 23–34. [Google Scholar]
- Luongo, M. The Psychodynamic Approach for Understanding and Treating Autism. Phenomena J. 2021, 3, 116–130. [Google Scholar] [CrossRef]
Figure 1.
Six Phases of the A.-O.C.M. Parent Training Protocol.
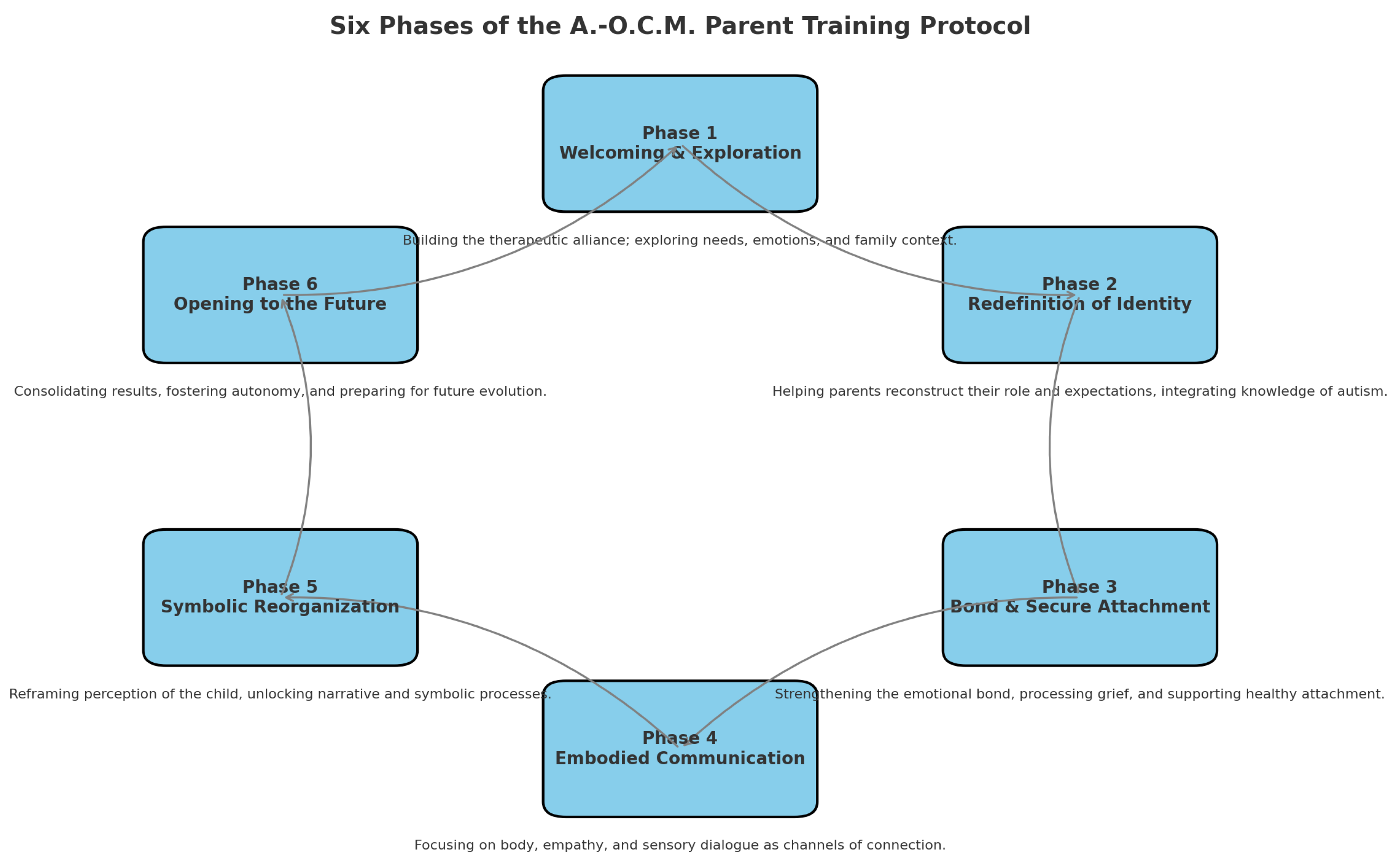

Table 1.
Synthesis of the Appendices for the Implementation of the A.-O.C.M. Protocol.
| Level of Implementation | Concise Description | Function in Implementation |
|---|---|---|
| Principles of Integrity and Consistency (Appendix A) | The A.-O.C.M. protocol requires that each phase and transformative node be applied rigorously: exclusion of unrelated nodes, accuracy in naming, necessary redundancy in prompts, and strict adherence to the phenomenological and behavioral structure. | Defines the methodological framework and guarantees that prompts respect the original clinical structure without alterations. |
| Permanent Operational Commands (Appendix B) | Permanent commands ensure uniformity: updated literature (2015–2025, indexed sources), mandatory references (Cooper, Skinner, Husserl, Merleau-Ponty, Francesetti), and integrity checks prior to document delivery. | Establishes operational rules and epistemological constraints that make the model standardizable and replicable. |
| Archive and Structural References (Appendix C) | The permanent archive stores foundational articles (Morfini 2023), protocol extracts, and clinical notes on the 24 nodes across the 6 phases. It provides a stable basis to ensure replicability, epistemological coherence, and shared access between therapist and AI. | Builds the clinical and theoretical memory that integrates ABA, phenomenology, and embodied mind, ensuring continuity and traceability of the protocol. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



