Submitted:
01 September 2025
Posted:
03 September 2025
You are already at the latest version
Abstract
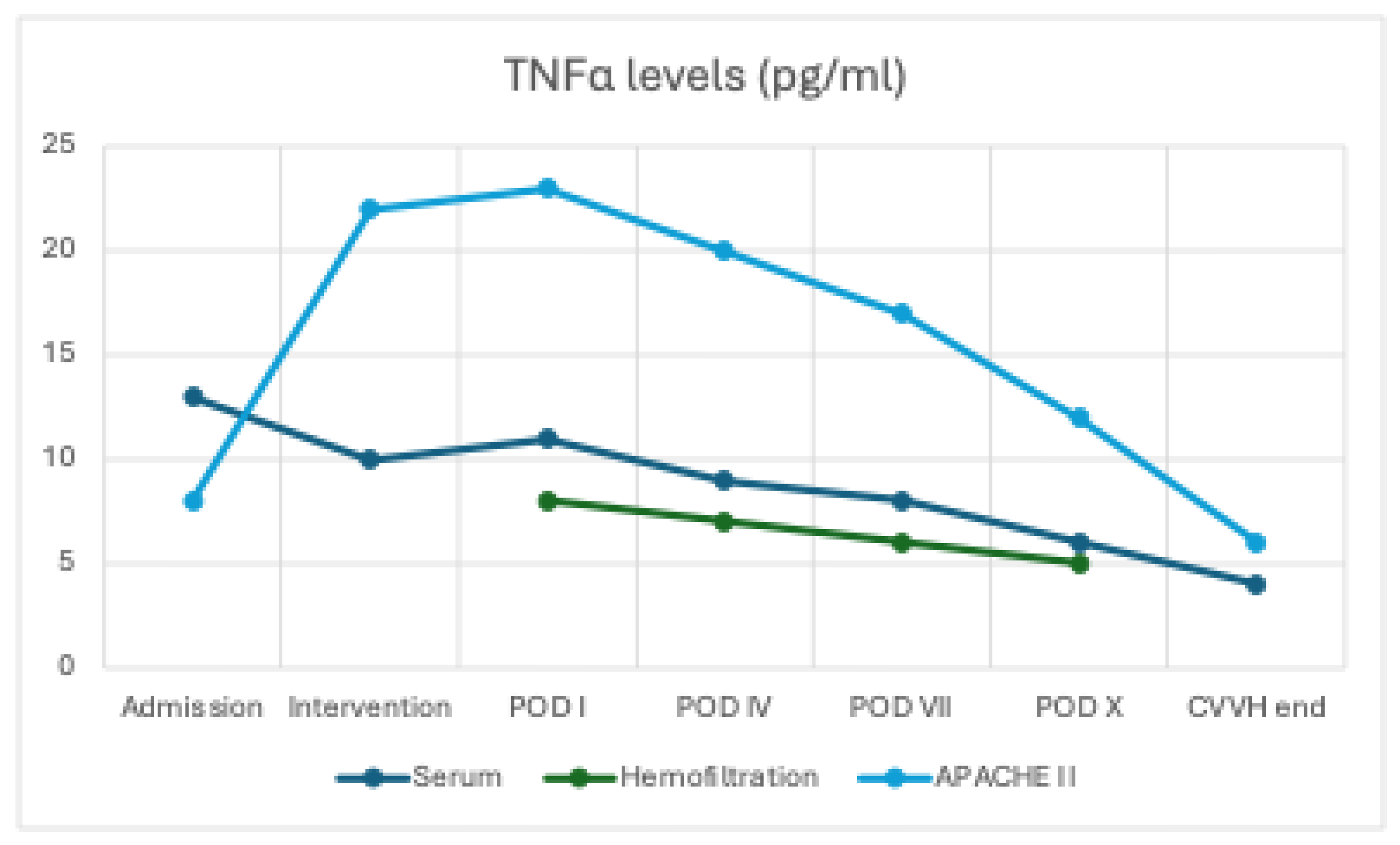
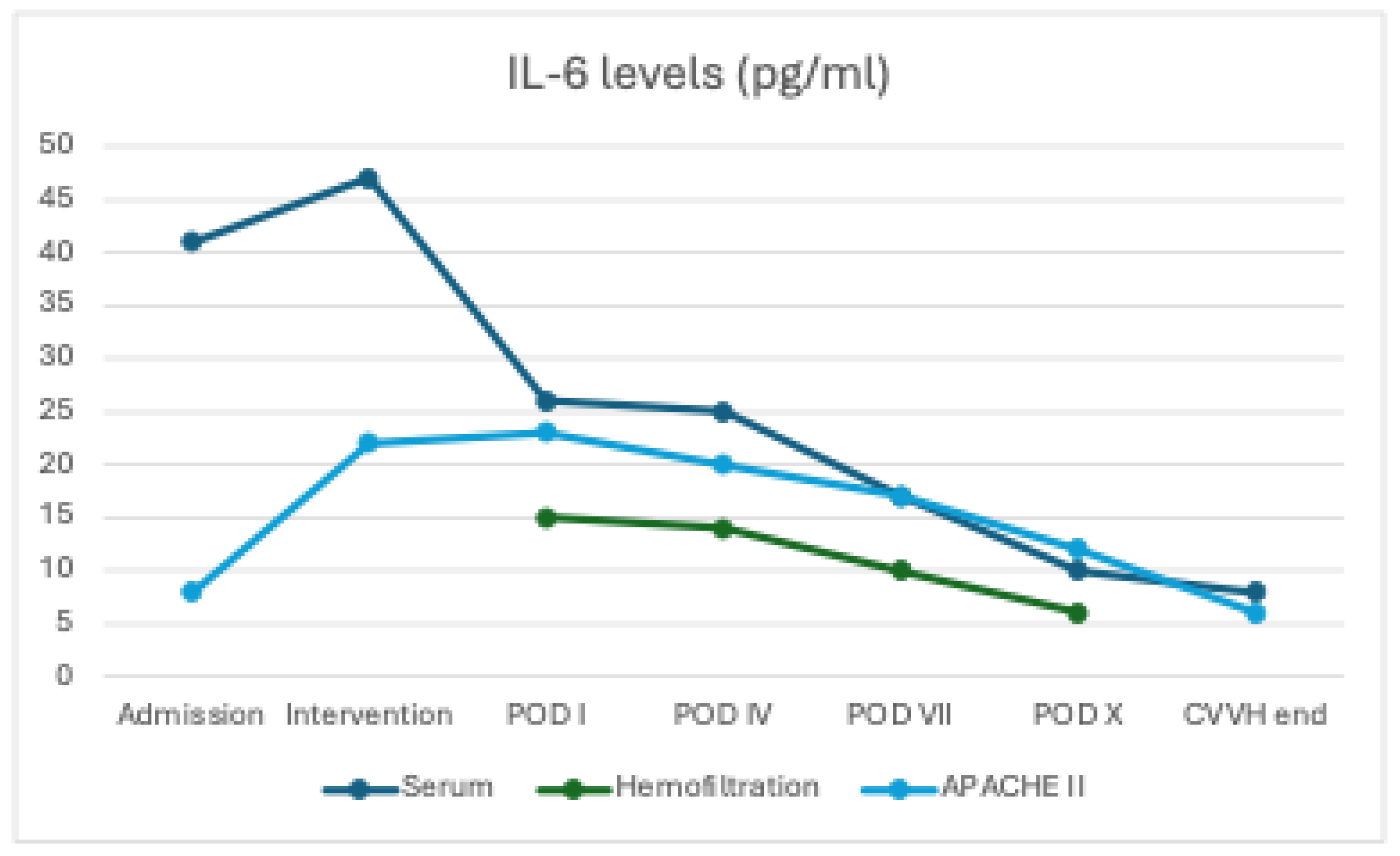
Background Severe acute pancreatitis (SAP) presents with Multiple Organ Dysfunction Syndrome (MODS) in ~15% of cases, accounting for ~35% of early deaths within 48h. Major complications—shock, renal failure, and respiratory insufficiency—arise from an overwhelming systemic inflammatory response driven by markedly elevated pro-inflammatory cytokines. Massive release of IL-2, IL-6, and TNF-α underlies the systemic inflammatory response syndrome (SIRS). Continuous veno-venous hemofiltration (CVVH) with the oXiris filter, adsorbing endotoxins and cytokines, has been used in sepsis and applied early in SAP to reduce cytokine load and organ injury. Aims To evaluate the efficacy and safety of early CVVH with the oXiris filter in modulating the systemic inflammatory response by removing toxic cytokines from the bloodstream in patients with SAP complicated by organ dysfunction and refractory sepsis. Methods This single-centre, retrospective, observational study was conducted at a tertiary university hospital between 2000 and 2022. Forty-eight consecutive patients with SAP at onset, defined according to the 2012 Atlanta Classification, with APACHE II score ≥ 19 and persistent organ dysfunction, were included. All patients were unresponsive to initial intensive care within the first 24 hours and underwent urgent laparotomy with extensive peritoneal lavage, pancreatic necrosectomy, and placement of multiple abdominal drains, followed by transfer to the intensive care unit. CVVH (Prismax system) with the oXiris filter was initiated within 12 hours post-surgery. IL-6 and TNF-α were selected as inflammatory markers and measured in both serum and ultrafiltrate at baseline (0 h) and at 24, 48, 72, and 96 hours, and correlated with clinical parameters and prognostic scores (APACHE II, SOFA). Results Treatment was well tolerated in all patients. The 28-day survival rate was 97.9%. There was a significant time-dependent decrease in IL-6 (p = 0.019) and TNF-α (p = 0.008) concentrations in the ultrafiltrate, consistent with high early adsorption followed by a reduced cytokine burden, whereas serum levels showed a non-significant downward trend (IL-6 p=0.08; TNF-α p=0.310). The APACHE II score decreased from 23 postoperatively to 8 by the second week (−65.2%; p = 0.013), with a statistically significant correlation between cytokine reduction and clinical improvement. Adverse events were rare and manageable. Conclusions Early CVVH with the oXiris filter in SAP complicated by MODS and refractory sepsis proved safe, well tolerated, and potentially effective in reducing cytokine burden and improving prognostic indices. These findings support the hypothesis of a relevant immunomodulatory effect, warranting prospective controlled trials to confirm its true impact on survival and organ recovery.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design and Clinical Setting
2.2. Patient Selection Criteria
2.3. Preoperative Assessment and Surgical Procedure
2.4. Hemofiltration with oXiris Filter
- Filter: oXiris (AN69 membrane modified with polyethyleneimine coating and heparinised), with adsorption capacity for endotoxins and cytokines.
- Mode: continuous convective hemofiltration (pre-dilution).
- Blood flow rate: ≥ 75 mL/min (standard 180 mL/min).
- Ultrafiltration dose: 35 mL/kg/h, delivered with balanced replacement solution (PrismaSol) in pre-dilution.
- Anticoagulation: low-molecular-weight heparin continuous infusion (5–10 U/kg/h) or citrate.
- Filter replacement: every 24 hours or earlier in the event of circuit clotting.
- Treatment duration: minimum 72 hours, extended until haemodynamic stabilisation and reduction of inflammatory markers (mean 5 days, range 3–7 days).
- Cytokines adsorbed (TNF-α, IL-6) were measured in serum and ultrafiltrate at baseline and every 24 hours thereafter.
2.5. Outcome Measures and Data Collection
- Demographic and clinical data: age, sex, aetiology of pancreatitis, comorbidities.
- Inflammatory markers: leukocyte count, serum C-reactive protein (CRP), procalcitonin (PCT), TNF-α and IL-6 measured in serum, peritoneal lavage fluid, and CVVH ultrafiltrate.
- Haemodynamic parameters: heart rate, mean arterial pressure (MAP), lactate levels, pH, and base excess.
- Organ function indices: serum creatinine, PaO₂/FiO₂ ratio, intra-abdominal pressure.
- Intraoperative microbiological cultures from intra-abdominal collections.
- Prognostic scores: APACHE II and SOFA, calculated daily.
- Adverse events: hypotension, filter clotting, electrolyte disturbances.
- The primary outcome was the change in TNF-α and IL-6 levels between T0 and T96 hours. Secondary outcomes included changes in APACHE II and SOFA scores, haemodynamic parameters, and incidence of adverse events. Twenty-eight-day survival was recorded as a descriptive endpoint.
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Population and Clinical Characteristics
3.2. Primary and Secondary Outcomes
4. Discussion
4.1. Pathophysiological Mechanisms Involved
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| SAP | Severe acute pancreatitis |
| MODS | Multiple Organ Dysfunction Syndrome |
| SIRS | Systemic Inflammatory Response Syndrome |
| CVVH | Continuous Veno-Venous Hemofiltration |
| HVHF | High-Volume Hemofiltration |
| CRRT | Continuous Renal Replacement Therapy |
| AN69 | Acrylonitrile–metallyl sulfonate sodium copolymer 69 |
| PEI | Polyethyleneimine |
| TMP | TransMembrane Pressure |
| APACHE II | Acute Physiology And Chronic Health Evaluation II |
| SOFA | Sequential Organ Failure Assessment |
| ICU | Intensive Care Unit |
| POD | Post-Operative Day |
| CVC | Central Venous Catheter |
| COPD | Chronic Obstructive Pulmonary Disease |
| CKD | Chronic Kidney Disease |
| DM | Diabetes Mellitus |
| ALL | Acute Lymphoblastic Leukemia |
| CRP | C-Reactive Protein |
| PCT | Procalcitonin |
| MAP | Mean Arterial Pressure |
| ARDS | Acute Respiratory Distress Syndrome |
References
- Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14:27. doi:10.1186/s13017-019-0247-0.
- Pupelis G, Plaudis H, Grigane A, Zeiza K, Purmalis G. Continuous veno-venous haemofiltration in the treatment of severe acute pancreatitis: 6-year experience. HPB (Oxford). 2007;9(4):295-301. doi:10.1080/13651820701329225.
- Hu Y, Xiong W, Li C, Cui Y. Continuous blood purification for severe acute pancreatitis: A systematic review and meta-analysis. Medicine (Baltimore). 2019;98(12):e14873. doi:10.1097/MD.0000000000014873.
- Zerem E. Treatment of severe acute pancreatitis and its complications. World J Gastroenterol. 2014;20(38):13879-13892. doi:10.3748/wjg.v20.i38.13879.
- Xu J, Yang H, Tian X. Effects of early hemofiltration on organ function and intra-abdominal pressure in severe acute pancreatitis patients with abdominal compartment syndrome. Clin Nephrol. 2019;91(4):237-243. doi:10.5414/CN109435.
- Petrov MS, Shanbhag S, Chakraborty M, Phillips AR, Windsor JA. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology. 2010;139(3):813-820. doi:10.1053/j.gastro.2010.06.010.
- Li Y, Sun P, Chang K, et al. Effect of continuous renal replacement therapy with the oXiris hemofilter on critically ill patients: A narrative review. J Clin Med. 2022;11(22):6719. doi:10.3390/jcm11226719.
- Wang G, He Y, Guo Q, Zhao Y, He J, Chen Y, et al. Continuous renal replacement therapy with the adsorptive oXiris filter may be associated with the lower 28-day mortality in sepsis: A systematic review and meta-analysis. Crit Care. 2023;27:54. doi:10.1186/s13054-023-04555-x.
- Zhou Y, Wu C, Ouyang L, Peng Y, Zhong D, Xiang X, Li J. Application of oXiris-continuous hemofiltration adsorption in patients with sepsis and septic shock: A single-centre experience in China. Front Public Health. 2022;10:1012998. doi:10.3389/fpubh.2022.1012998.
- Tang J, Cao T. CRRT with the oXiris filter attenuates IL-6 in a patient with severe COVID-19. J Am Soc Nephrol. 2021;32:10S1103C. doi:10.1681/ASN.20213210S1103C.
- Wong E, Ong V, Remani D, Wong W, Haroon S, Lau T, et al. Filter life and safety of heparin-grafted membrane for continuous renal replacement therapy: A randomized controlled trial. Semin Dial. 2021;34(4):300-308. doi:10.1111/sdi.12951.
- Broman ME, Hansson F, Vincent JL, Bodelsson M. Endotoxin and cytokine reducing properties of the oXiris membrane in patients with septic shock: A randomized crossover double-blind study. PLoS One. 2019;14(8):e0220444. doi:10.1371/journal.pone.0220444.
- Zhou Y, Liu MJ, Lin X, Jiang JH, Zhuo HC. Comparative efficacy of two hemopurification filters for treating intra-abdominal sepsis: A retrospective study. Chin J Traumatol. 2025;28(2):82-88. doi:10.1016/j.cjtee.2024.12.003.
- Wei T, Chen Z, Li P, et al. Early use of endotoxin absorption by oXiris in abdominal septic shock: A case report. Medicine (Baltimore). 2020;99(28):e19632. doi:10.1097/MD.0000000000019632.
- Wang J, Wei SR, Ding T, et al. Continuous renal replacement therapy with oXiris® in patients with hematologically malignant septic shock: A retrospective study. World J Clin Cases. 2023;11(26):6073-6082. doi:10.12998/wjcc.v11.i26.6073.
- Chen X, Sun M, Mao X, Liu X, Sun W. Effectiveness of continuous veno-venous hemofiltration in the treatment of severe acute pancreatitis. Exp Ther Med. 2019;17(4):2720-2724. doi:10.3892/etm.2019.7192.
- Guo Y, Cao F, Li C, et al. Continuous hemofiltration reduces mortality in severe acute pancreatitis: A meta-analysis. Emerg Med Int. 2020;2020:6474308. doi:10.1155/2020/6474308.
- Huang H, Zhou Q, Chen M. High-volume hemofiltration reduces short-term mortality with no influence on the incidence of MODS, hospital stay, and hospitalization cost in patients with severe acute pancreatitis: A meta-analysis. Artif Organs. 2021;45(12):1411-1424. doi:10.1111/aor.14016.
- Wang Y, Dai GF, Xiao WB, et al. Effects of continuous venous-venous hemofiltration with or without hemoperfusion on patients with hypertriglyceride acute pancreatitis. Clin Res Hepatol Gastroenterol. 2025;49(5):102572. doi:10.1016/j.clinre.2025.102572.
- Sun S, He L, Bai M, et al. High-volume hemofiltration plus hemoperfusion for hyperlipidemic severe acute pancreatitis: A controlled pilot study. Ann Saudi Med. 2015;35(5):352-358. doi:10.5144/0256-4947.2015.352.
- Cui HX, Xu JY, Li MQ. Efficacy of continuous renal replacement therapy in the treatment of severe acute pancreatitis associated acute respiratory distress syndrome. Eur Rev Med Pharmacol Sci. 2014;18(17):2523-2526.
- Yadav SC, Zhang B. Effect of early continuous veno-venous haemofiltration in severe acute pancreatitis for the prevention of local pancreatic complications. Gastroenterol Res Pract. 2022;2022:7575231. doi:10.1155/2022/7575231.
- Jiang HL, Xue WJ, Li DQ, et al. Influence of continuous veno-venous hemofiltration on the course of acute pancreatitis. World J Gastroenterol. 2005;11(31):4815-4821. doi:10.3748/wjg.v11.i31.4815.
- Mielnicki W, Dyla A, Zając M, et al. Does continuous renal replacement therapy with oXiris in septic shock have any positive impact? Single-centre experience with oXiris therapy in septic shock patients. J Clin Med. 2024;13(24):7527. doi:10.3390/jcm13247527.
- Lin Y, He S, Gong J, et al. Continuous veno-venous hemofiltration for severe acute pancreatitis. Cochrane Database Syst Rev. 2019;10(10):CD012959. doi:10.1002/14651858.CD012959.pub2.
- Xie Y, Yuan Y, Su W, et al. Effect of continuous hemofiltration on severe acute pancreatitis with different intra-abdominal pressure: A cohort study. Medicine (Baltimore). 2021;100(44):e27641. doi:10.1097/MD.0000000000027641.
- Wang Y, Gao Y, Zhao L, Kang K. Continuous renal replacement therapy in combination with oXiris haemofilter in a paediatric patient with sodium valproate-induced acute pancreatitis. BMJ Case Rep. 2025;18:e258126. doi:10.1136/bcr-2023-258126.
- Caronna R, Benedetti M, Morelli A, et al. Clinical effects of laparotomy with perioperative continuous peritoneal lavage and postoperative hemofiltration in patients with severe acute pancreatitis. World J Emerg Surg. 2009;4:45. Published 2009 Dec 16. doi:10.1186/1749-7922-4-45.
- Guo J, Huang W, Yang XN, et al. Short-term continuous high-volume hemofiltration on clinical outcomes of severe acute pancreatitis. Pancreas. 2014;43(2):250-254. doi:10.1097/01.mpa.0000437321.06857.fc.

| Sex, n (%) |
F: 30 (62.5) M: 18 (37.5) |
| Age, years, mean ± SD | 60.4 ± 18 |
| Etiology, n (%) | Biliary lithiasis, 34 (70.8) Alcoholic pancreatitis, 8 (16.7) Hypertriglyceridemia, 3 (6.3) Asparaginase-induced pancreatitis (ALL), 3 (6.3) |
| Comorbidities, n (%) | Arterial hypertension, 21 (43.8) COPD, 4 (8.3) CKD, 6 (12.5) DM, 9 (18.8) Obesity (BMI > 30),17 (35.4) |
| Primary Outcomes | |
| Tolerability, n (%) | 48 (100) |
| Survival, n (%) | 47 (97.9) |
| Secondary Outcomes | |
| Surgical Complications, n (%) | Enteric fistula, 1 (2.1) Major bleeding – ischemic complications – |
| Hospital Stay, days, mean ± SD | 28.5 ± 19 |
| Microorganisms isolated from intraoperative cultures, n (%) | Enterococcus spp, 30 (62.5) Escherichia Coli, 10 (20.8) Pseudomonas Aeruginosa, 5 (10.4) Acinetobacter baumannii, 1 (2.1) Sterile cultures, 2 (4.2) |
| ICU stay, days, mean ± SD | 13.3 ± 11 |
| CVVH adverse events, n (%) | Fever from CVC, 1 (2.1) Hypophosphatemia, 2 (4.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



