Submitted:
21 August 2025
Posted:
01 September 2025
You are already at the latest version
Abstract
Keratoacanthoma (KA) is a rapidly growing epithelial neoplasm characterized by clinical and histopathological features that often overlap with well-differentiated squamous cell carcinoma (SCC), posing diagnostic challenges. This review provides a comprehensive overview of KA, emphasizing advances in non-invasive diagnostic techniques such as dermoscopy, reflectance confocal microscopy (RCM), and line-field confocal optical coherence tomography (LC-OCT), which improve lesion characteriza-tion and differentiation from SCC. We discuss the histopathological phases of KA and highlight key features aiding in diagnosis. Furthermore, we explore the emerging role of human papillomavirus (HPV), particularly β-genus types, as a cofactor in KA car-cinogenesis through modulation of apoptosis and DNA damage response pathways, especially under ultraviolet (UV) radiation exposure. Therapeutic strategies remain centred on complete surgical excision; however, alternative treatments, including ra-diotherapy, cryotherapy, topical agents, and systemic retinoids, are discussed with their respective benefits and limitations. Finally, we review current HPV vaccines and novel vaccine candidates targeting a broad spectrum of mucosal and cutaneous HPV types, alongside promising off-label therapeutic applications. This review underscores the importance of integrated diagnostic and therapeutic approaches to optimize KA management and highlights future directions in understanding its pathogenesis and treatment.
Keywords:
keratoacanthoma
; human papillomavirus
; non-melanoma skin cancer
; dermoscopy
; reflectance confocal microscopy
; line-field confocal optical coherence tomography
; carcinogenesis
; therapies
; vaccines
1. Introduction
Keratoacanthoma (KA) is classified among the non-melanoma skin cancers (NMSC), typically arising on the head and neck areas. It is still controversial whether KA is a distinct neoplasm or a subtype of well-differentiated squamous cell carcinoma (SCC). Although the exact cause of KA remains uncertain, ultraviolet (UV) rays play a significant role in its development, rendering fair-skinned individuals particularly vulnerable. Other potential triggers include human papillomavirus (HPV), immunosuppression, immunodeficiency, trauma, radiation, chemicals, cell-cycle-modulating medications, and foreign bodies [1]. Additionally, KA is more commonly seen in older adults, particularly those with prolonged sun exposure or immunosuppression, and it occurs more frequently in men than in women. KA is thought to originate from the hair follicle and can appear in solitary, multiple, or eruptive forms, with the solitary type being the most prevalent [2]. Clinically, the most common presentation is a solitary lesion measuring 1 to 2 cm in diameter. Less common variants include giant KA—defined as a solitary tumor larger than 20 mm, typically found on the eyelid or nose—and KA centrifugum marginatum, characterized by peripheral expansion with central healing, which can also exceed 20 mm in diameter [3]. Typically, KA progresses through three clinical phases: a proliferative phase, a stabilization phase, and a regression phase [4]. Several signaling pathways have been implicated in KA pathogenesis, including the Wnt/retinoic acid pathway, B-Raf, H-Ras, p27, and the Hedgehog signaling pathway [5,6,7,8].
Some patients affected by specific genetic syndromes, such as Muir-Torre syndrome, xeroderma pigmentosum, Ferguson-Smith disease, Witten-Zac syndrome, and Grzybowski syndrome, may present multiple KAs [9,10]. The last syndrome is characterized by thousands of eruptive KAs that could resolve over several months, and tumors may also develop in the airway. The appearance of the tumors may resemble milia or eruptive xanthomas [9].
Regarding therapy, surgery with traditional excision or Mohs micrographic surgery is considered the gold standard treatment, mainly for single forms of KA. Other therapies that have been proposed include radiation, destructive therapies, topical therapies, and systemic therapies. However, to date, there is no consensus guideline on alternative therapies for KAs, except for surgery. Some case series report the use of methotrexate and interferon injected into the tumor, and tretinoin used for multiple-type KA [11,12,13].
This article aims to explore the key aspects of KA, including its clinical presentation, pathogenesis, histological aspects, and the available treatment options, providing an insight into the management of this tumor.
2. Epidemiology of Keratoacanthoma
Epidemiological data about KA are still inconsistent due to underestimation arising from shared morphological features with SCC, especially in the case of well-differentiated SCC. The reported incidence of KA ranges between 100 and 150 cases per 100,000 individuals [14,15]. Recently, the KA peak incidence has shifted toward the age group 65 to 71 years from 50 to 69 years observed in the 1990s [16]. Men are more often affected than women [16]. KA affects mostly fair-skinned people and has not yet been reported in native Australians [14]. Major risk factors include excessive UV exposure, radiation, immunosuppression, chronic non-healing wounds, and HPV infection, as also reported for well-differentiated SCC [17]. In addition, cutaneous trauma (e.g., laser therapy, resurfacing procedures, or surgery) has been reported as an additional risk factor in KA development, suggesting that dysregulated inflammatory responses may play a further role in its pathogenesis [18,19].
3. Etiology
The etiology of KA is still not completely understood. It is presumed to originate from the hair follicle, usually located on the hair-bearing, sun-exposed parts of elderly individuals, and it is characterized by a triphasic trend of rapid development, stabilization, and regression, which mimics the hair cycle [20,21]. Multiple factors have been suggested, including UV radiation exposure, chemical carcinogens, immunosuppression, medications, genetic predisposition such as mutations of p53 or H-Ras, viral infection by HPV, and cutaneous trauma or surgery to the location [22].
In the literature, cases of KA have been reported after COVID-19 vaccination, including both multiple and eruptive KA and solitary KA strictly located on the site of vaccination [23,24]. It has been hypothesized that the onset of KA after vaccination may have been initiated by an immune-mediated, pro-inflammatory mechanism.
KA is widely reported also after cutaneous trauma, including tattooing [25], site injection of cosmetic collagen filler [26], and at the recipient site of skin graft [27].
KA can also be triggered by medications, including BRAF inhibitors (such as pembrolizumab) [28], but also kinase inhibitor drugs (such as sorafenib), PD-1 inhibitors (such as sintilimab) [29], and immunosuppressive disease-modifying antirheumatic drugs - DMARDs- (such as leflunomide) [30].
KA may also be associated with various genetic syndromes: Muir-Torre syndrome (MTS), multiple self-healing squamous epithelioma (MSSE, Ferguson-Smith syndrome), multiple familial KA of Witten and Zak (MFKWZ), xeroderma pigmentosum (XP), multiple self-healing palmoplantar carcinoma (MSPC), incontinentia pigmenti (IP), and eruptive KA of Grzybowski [31].
Recently, the key role of HPV in cutaneous keratinocyte tumors development has been highlighted [32]. Beta-HPVs have been reported as the main etiologic agent of SCC in patients with epidermodysplasia verruciformis (EV) and organ transplant recipients [33]. Several studies have shown that samples from KA contain HPV DNA in more than 90% of cases, unlike well-differentiated SCC, suggesting a co-factor role for HPV [34].
Epidemiological studies have pointed out that SCCs are associated with beta-HPV infections more often than the general population [35]. However, their role in NMSC progression in the general population is still unclear [35].
In a recent systematic review, 321 KAs were analysed for the presence of different HPV genotypes, detecting a high presence of beta genus types (50.31%) and an equal proportion between alpha (24.84%) and gamma (24.84%) genera [32]. However, most of the HPV types found in NMSC were the consequence of multiple infections with different HPV types, which were detected at very low viral loads (<1 copy/1000 cells), depending on the polymerase chain reaction (PCR) primers, which raises the issue of bias in detecting only HPV types with high similarity to the primers employed, potentially overlooking others [36].
4. Clinical Manifestations
KA is usually a solitary and sporadic tumor [2]. It can vary from a few millimeters up to more than 20 mm in KA centrifugum marginatum [3]. KA usually starts as a small papule, while the mature KA is a dome-shaped, well-demarcated umbilicated nodule with a hyperkeratotic plug in the center [2]. KA usually arises on sun-exposed areas and evolves in three clinical stages, namely proliferative, mature, and resolving [2]. This process usually occurs within 4 to 6 months and can lead to atrophic hypopigmented scars [2]. Rarely, solitary KA can arise on mucous membranes, mostly in the oral cavity [37,38,39,40,41,42,43,44]. Several studies suggest that KA arises more frequently on non-chronically sun-damaged skin (i.e., chest or arms) while SCC always arises in the context of severely photodamaged skin, usually surrounded by actinic keratosis and/or associated with a field of cancerization. According to these proposed classifications, KA can be clinically recognized as a rapidly growing nodule with a central crateriform area not surrounded by signs of the field of cancerization, while well-differentiated SCC develops upon sun damage and actinic keratosis, proposing a possible different etiopathogenesis between the two tumors.
Multiple KAs are rare and can be sporadic or familial. Multiple KAs centrifugum marginatum belong to the first group and are characterized by a coral reef-like appearance [45]. Rarely multiple KAs can be associated with prurigo nodularis [46]. Multiple familial KAs can be described in multiple MSSE, an autosomal-dominant skin cancer condition characterized by multiple SCC-like locally invasive cutaneous tumors, also known as Ferguson-Smith disease [47]. Furthermore, patients affected by generalized eruptive KA (GEKA) of Grzybowski develop multiple eruptive KAs, especially on sun-exposed areas, such as the face and the upper trunk, and on intertriginous areas [48,49]. Finally, several KAs develop in patients with multiple familial KAs of Witten and Zak type, a disease that is still not well characterized and combines clinical features of MSSE and GEKA in the same patient [50,51].
4. Dermoscopy
Dermoscopic examination of KA may present several distinct features that help in differentiating it from other skin tumors [52]:
1. Central Keratin Plug: One of the hallmark features of KA is the presence of a central, well-defined, yellowish or whitish keratin plug. This central crater is visible in most cases and is a key diagnostic feature.
2. Rolled Border: The lesion typically displays a smooth, well-demarcated, and elevated border that is slightly rolled. This appearance is characteristic of KA and helps in differentiating it from other tumors that may have irregular borders.
3. Vascular Patterns: Dermoscopy often shows vessels that are linear, dotted, or hairpin-shaped in the peripheral areas of the lesion. These vessels may be more prominent around the edge of the keratin plug, contributing to the lesion’s raised appearance. Inflammatory and hyperplastic changes in the epidermis contribute to these vascular patterns.
4. Homogeneous Pink or White Background: The background of the lesion may show a homogeneous pink or white color due to the underlying inflammatory changes and epithelial proliferation. This feature, when seen with the characteristic keratin plug, helps in the diagnosis.
5. Yellowish Structures: Apart from the keratin plug, the lesion may exhibit yellowish areas or streaks within the lesion, which correspond to the presence of keratinized material beneath the surface.
6. Regular Pattern: In most cases, the dermoscopic pattern of KA is regular, with no irregular pigment network or atypical vessels, which further helps to differentiate it from malignancies such as melanoma.
Dermoscopically, it is not easy to differentiate KA from SCC because they share some common features [53]. Keratin has the highest sensitivity to differentiate KA and SCC from other amelanotic nodules, while white circles have the highest specificity, and they are typically detected in SCC tumors but not in KA. Another important clue for differentiating SCC from KA is the predominantly white color, more frequently detected in SCC, which histologically corresponds to fibrosis and hyperkeratosis. These dermoscopic findings, together with dot vessels, are helpful for the diagnosis of KA and SCC [52].
5. Reflectance Confocal Microscopy (RCM) and Line-Field Confocal Optical Coherence Tomography (LC-OCT)
As previously explained, KA is a rapidly growing epithelial neoplasm that often poses diagnostic challenges due to its clinical and histological similarities with well-differentiated SCC. Non-invasive imaging techniques such as reflectance confocal microscopy (RCM) and line-field confocal optical coherence tomography (LC-OCT) have emerged as valuable tools for the real-time, in vivo evaluation of skin tumors, offering near-histologic resolution without the need for tissue excision.
RCM allows a face imaging of the epidermis and superficial dermis, generally reaching a maximum depth of approximately 200–250 microns. This limitation in penetration depth may hinder complete visualization of thick lesions such as KA, which often exhibits marked central hyperkeratosis and deep epidermal proliferation. Nevertheless, RCM can provide useful information, particularly at the lateral and superficial portions of the tumor [54]. On RCM analysis, KA typically presents with epidermal hyperplasia and architectural disarray, often accompanied by a large, highly reflective central structure corresponding to the compact keratin plug. The surrounding keratinocytes may appear atypical, yet they tend to preserve an organized honeycomb pattern, distinguishing KA from more aggressive forms of SCC. Vascular features such as dilated and tortuous capillaries within the dermal papillae, as well as perivascular inflammatory infiltrates, are frequently observed and may support the diagnosis [55].
On the other hand, LC-OCT, with its capacity to acquire both vertical (B-scan) and horizontal (en face) images and a penetration depth of up to 500 microns, offers a more complete structural assessment of KA compared to RCM [56]. The hallmark feature of KA in LC-OCT analysis is the presence of a cup-shaped epidermal invagination filled with a hyperreflective material, corresponding to the crateriform morphology and central keratin seen histologically. The surrounding epidermis typically appears markedly thickened, with abrupt lateral transition zones separating the lesion from the adjacent normal skin. In the vertical plane, broad strands and islands of keratinocytes can often be seen extending downward into the dermis, mimicking the appearance of histologic sections. Although cytological details are not as clearly defined in LC-OCT as in RCM, the architectural pattern is usually well visualized and can aid in distinguishing KA from invasive SCC [57].
Despite their utility, both RCM and LC-OCT have inherent limitations that must be considered. The depth of penetration may be insufficient to evaluate the full extent of the lesion, particularly at the base, and the dense keratin content can attenuate signal penetration, reducing image quality. Furthermore, distinguishing KA from well-differentiated SCC remains challenging, especially in cases where the imaging captures only a portion of the lesion. The interpretation of images is also observer-dependent and may vary based on the examiner’s level of experience and training.
Nonetheless, these techniques can serve as helpful adjuncts in the clinical evaluation of KA, especially in cases where biopsy is contraindicated, where the lesion is in regression, or when monitoring over time is required. The correlation between imaging findings and histopathology, particularly regarding the overall architecture, further supports their integration into the diagnostic pathway for KA.
6. Histology of Keratoacanthoma
Differentiating KA from well-differentiated SCC on routine histology can be tricky due to shared features. Furthermore, inadequate biopsies fail to include the complete tumor architecture, leading to a diagnosis of SCC and potentially overtreatment [58]. KA histopathological features depend on the development phase, namely, proliferative, mature, and regressive phases [59]. The proliferative phase is characterized by marked hyperkeratosis and exophytic or endophytic proliferation of pale squamous cells in lobules that can resemble distorted infundibular structures, which become more cystic and hyperkeratotic in a later stage, coalescing into a central keratin plug [60]. In the mature stage, most peripheral tumor islands infiltrate the edges of the central mass [60]. Typically, the peripheral keratinocytes show enlarged, pink, glassy-appearing cytoplasm, a low nuclear-to-cytoplasmic ratio, and minimal nuclear atypia [60]. In addition, a mixed infiltrate of inflammatory cells can be commonly detected [60]. Regressing lesions show a well-formed crater of keratin with thinning of the surrounding squamous epithelium, reduced squamous lobules, and underlying dermal fibrosis [60]. The most significant histopathological features that help to confirm the diagnosis of KA are symmetry, the absence of extension beyond the sweat glands, lack of infiltration or desmoplasia, and the little-to-moderate nuclear atypia [61]. Some cases of metastatic KA have been reported in the literature [62]. However, it could be possible that in these cases either a SCC has arisen within a KA [63] or a SCC with a distinct follicular pattern of differentiation was misdiagnosed as KA [64]. In addition, it has been reported that immunocompromised patients with large KA have developed metastasis of unclear significance [65].
7. Human Papillomavirus and Carcinogenesis
HPV belongs to the Papillomaviridae family, which includes more than 440 genotypes of small DNA viruses, classified into five genera: α, β, γ, μ, and ν [66]. Only a few of them, mainly within α and β genera, can cause significant risks to human health and have received the most attention from researchers [67].
HPV particles are characterized by the presence of circular, 7.9-kb double-stranded DNA included in a nonenveloped icosahedral capsid constituted by 360 copies of the L1 protein [68] and a smaller amount of L2 gene product [69]. The HPV genome encodes eight main expressed proteins: the core proteins involved in genome replication (E1 and E2), the core proteins involved in virus assembly (L1 and L2), and the accessory proteins (E4, E5, E6, and E7). A fusion protein with regulatory functions, E8^E2C, was also described [70]. Whereas the core proteins are highly conserved among all HPV genotypes, the accessory proteins are highly variable [71]. E6 and E7 are considered the major HPV oncoproteins, required to establish persistent infection and propagation of both α and β HPVs and for malignant transformation of the host cell [72,73] and thus represent attractive antitumoral drug targets [74].
The types α and β of HPV show significant differences in tissue tropism: β types can infect only cutaneous anatomic sites, whereas α types predominantly infect mucosal tissues. Among α types, it is important to distinguish between high-risk (HR) αHPVs, such as 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59 genotypes, which show a tissue tropism limited to mucosal tissues, and low-risk (LR) αHPVs, which can infect both cutaneous and mucosal tissues. Generally, infections sustained by β types remain subclinical, but certain infections, mainly those caused by HPV5 and HPV8, can become clinically relevant, leading to the development of NMSC in high-risk patients (e.g., immunocompromised organ-transplant individuals or patients affected by the genetic disorder EV) [75,76,77].
HR-αHPVs are strongly carcinogenic, even though the infection seems to be a necessary but insufficient element for neoplastic transformation. Conversely, βHPVs are not intrinsically carcinogenic but behave as facilitators for cancer initiation, by interfering with apoptotic pathway activation upon UV damage [78,79]. As is well-known from the literature, UV-B rays (290-320 nm) are considered strong physical factors damaging macromolecules (i.e., DNA, proteins, lipids) and, in turn, cell integrity [80]. The result of UV-induced DNA damage is represented by specific photoproducts, such as the pyrimidine dimers, resulting from the covalent bond of two adjacent pyrimidine bases [80]. Normally, these photoproducts are efficiently removed by the Nucleotide Excision Repair (NER) pathway [81]. If not properly repaired, pyrimidine dimers can lead to mutations [82]. DNA damage response activates the oncosuppressor proteins p53 and p21waf1 that arrest the cell cycle. The p53 protein, which is considered the “guardian of the genome”, undergoes some post-translational modifications, mainly phosphorylation and acetylation, which regulate the assembly of p53 monomer into a tetramer, inhibit its degradation, and induce its transcriptional activity, allowing the expression of the cell-cycle inhibitor p21waf1 or the activation of apoptotic pathways [83,84]. P53 has been extensively reported as the best-characterized target of HPV E6 oncoprotein [85]. The HR-αHPV E6 oncoprotein promotes degradation of p53 via the interaction with the E6-associated protein (E6AP) ubiquitin ligase. This interaction allows the formation of an intermediate ternary complex E6-E6AP-p53, resulting in the ubiquitination and proteasome-mediated degradation of the cellular oncosuppressor [86,87,88]. In contrast, most of the βHPV E6 oncoproteins do not interact with E6AP and do not degrade p53, but interfere with both acetylation and phosphorylation of p53, finally inhibiting the assembly of the p53 monomer into a tetramer [89,90] (Figure 1). However, some important exceptions have been reported: E6 protein from HPV49, HPV75, and HPV 76 genotypes behave similarly to αHPV E6 protein [91]; E6 protein produced by HPV38 and HPV92 can interact with E6AP and stabilize p53 [92,93]. Moreover, the stabilization of wild-type p53 mediated by E6 from HPV38 results in the accumulation of ΔNp73 [94], which is the carcinogenic isoform of p73 and works as an antagonist of p53 itself [95]. In detail, HPV38 E6 and E7 stabilize ΔNp73 by inducing its IκB kinase beta (IKKβ)- mediated phosphorylation, finally increasing its half-life [96]. Other intracellular targets for βHPV E6 oncoprotein have been extensively investigated: BAX and BAK are two proapoptotic factors belonging to the BCL-2 family, transcriptionally regulated by p53 and involved in mitochondrial membrane permeabilization occurring during the apoptotic process, required for the release of cytochrome c and other proapoptotic proteins in the cytosolic space [97]. βHPV E6-induced, proteasome-mediated degradation of BAK is the result of its interaction with βHPV E6 in an E6AP-dependent manner [98,99,100]. Conversely, the exact mechanism of βHPV E6-induced degradation of BAX has not yet been elucidated.
The other major HPV oncoprotein is E7. For HR-αHPV types, the interactions of E7 with its targets, i.e., the retinoblastoma protein (pRb) [101], p107 [102], p130 [103,104], PTPN14 [105,106], PTPN21 [107], and Memo1 [108], have been extensively investigated and characterized. The sequence of E7 oncoproteins from both βHPV and HR-αHPV types contains the LXCXE motif, which is directly involved in the binding of E7 to pRb [109]. In the case of HR-αHPV types, this interaction triggers the proteasome-mediated pRb degradation and abrogates its negative regulation of cell cycle progression in infected cells. In particular, pRb binds to and inhibits transcription factors belonging to E2F family, controlling S-phase entry [110]. Nevertheless, the presence of the LXCXE in E7 sequence does not seem sufficient to allow this effect in βHPV host cells. Indeed, the ability to interact with pRb with an affinity quite similar to that shown by HR-αHPV E7, and to promote its destabilization has been reported only for HPV38 E7 [111]. For βHPV, the effects of E7 interactions are less well understood, but in general do not seem able to interfere with pRb activity in the infected cell.
Overall, βHPV represents a cofactor that can enhance the effects of UVB damage. Indeed, the presence of βHPV confers resistance to the cell towards apoptosis as well as increases the susceptibility to UVB-mediated DNA damage [112].
7. Therapy
The first-line therapy for KA remains the complete surgical removal. However, about 8% of KAs may exhibit a recurrence after complete surgical excision [113]. Radiotherapy (RT) and cryotherapy are physical therapies for treating KAs. Although the effectiveness of RT on KA has been demonstrated [114,115,116], RT is rarely used. Indeed, RT is generally unsuitable for younger patients, and the several doses required make it burdensome for older patients. Furthermore, RT may induce eruptive KAs [117]. However, RT could be an option for cosmetically sensitive, non-operable regions. Although cryotherapy has not been widely studied as a therapeutic option, its effectiveness has been reported in about 87% of KAs [118]. Photodynamic therapy (PDT) belongs to the group of physical therapies, too. However, only limited data are available on the use of PDT for KAs. On the one hand, PDT has been reported as effective in treating KAs, but on the other hand, the development of KAs after PDT use has been reported [119]. The argon lasers have also been used for KAs. Solitary KAs of the face and auricles were successfully treated in 65% of the patients, while 35% achieved healing with mild scarring [120]. Topical 5-fluorouracil (5-FU) and imiquimod represent two valuable alternatives for KAs. 5-FU is an inhibitor of thymidylate synthase, disrupts DNA synthesis, and leads to lethal DNA damage [121]. Topical 5-FU has a good safety profile and could be considered as a first-line treatment for KAs, particularly in cosmetically sensitive areas [122]. Indeed, the use of topical 5-FU led to a complete resolution of the lesion within six weeks in a retrospective analysis [122]. 5-FU can also be used for intralesional applications [123]. An average of three injections in three weeks has been reported as effective [123]. Furthermore, 5-FU has been effectively used in combination with systemic retinoids [124] and Er:YAG lasers [13]. Topical 5% imiquimod, a toll-like receptor 7 and 8 agonist able to stimulate immune response, also represents an effective alternative for treating KAs topically. However, imiquimod should be applied for 9 - 11 weeks, three to four times a week, to obtain a complete remission [125]. Systemic therapies for KAs include retinoids and erlotinib. Systemic retinoids act with several mechanisms, including inhibition of keratinization and Wnt-related KAs proliferation, modulation of terminal differentiation of epidermal cells, and an increase in both IL-2 production and mitogen-induced lymphocyte proliferation [5]. Oral retinoids represent a valuable option for generalized eruptive KAs of Grzybowski and Ferguson-Smith disease [126,127,128]. Erlotinib, an epidermal growth factor receptor (EGFR) inhibitor, has also been proposed for the treatment of resistant, multiple KAs [129]. However, experience with it is still limited. A summary of the above-described therapeutic options for the treatment of KAs is provided in Table 1.
8. Anti-HPV Vaccines
Three main vaccines are commercially available and approved to prevent cervical cancer caused by the most common HR-HPV genotypes: Gardasil®, Gardasil®9, and Cervarix®. They all are based on non-infectious virus-like particles (VLPs) containing the major capsid protein L1 from the specific HPV genotype they target and are approved for the prevention of premalignant ano-genital lesions (cervical, vulvar, vaginal and anal), cervical and anal cancers causally related to certain oncogenic HPV types. Gardasil® targets HPV6, 11, 16, and 18, while Cervarix® is specific for HPV16 and 18, and Gardasil®9 is a nonavalent vaccine targeting HPV6, 11, 16, 18, 31, 33, 45, 52, and 58 [130].
The employment of the three available vaccines, which are both safe and effective, had a great success for the prevention of HPV-related cancers. Nevertheless, they have several drawbacks: being based on L1, which is poorly conserved among different HPV types, they can target just the specific corresponding genotype, with incomplete cross-protection; having low thermostability, they need uninterrupted cold chains for transport and distribution, thus limiting the availability in developing countries; the manufacturing procedure is time-consuming and expensive [131]. Therefore, many efforts have been made by researchers to develop novel strategies with the aim of overcoming these drawbacks. In this regard, a research group developed PANHPVAX, which is based on the hyper-thermostable thioredoxin scaffold, wherein a sequence of epitopes of the minor capsid protein L2, derived from the 20–38 amino acid region of various HPV types, has been incorporated [132]. It is noteworthy that, in contrast to L1, L2 is highly conserved among both mucosal and cutaneous HPV genotypes and carries several epitopes of linear nature, which can be inserted into various scaffolds. The safety profile and the immunogenicity of PANHPVAX, which is assumed to target mucosal genotypes of HPV, are under investigation in a phase I clinical trial, which is still ongoing [133]. Following this research line, the same research group reported the development of other promising vaccine candidates, containing the L2 polytope, i.e., a synthetic antigen composed of concatenated conserved epitopes from the L2 protein of the cutaneous HPV types, fused to the thioredoxin scaffold (Figure 2). These candidates were tested in vivo in both mice and guinea pigs, resulting in a broad immunization against 19 cutaneous HPV genotypes. Interestingly, the investigated vaccine prototypes elicited cross-protective neutralizing antibodies against multiple mucosal HPV types, including the HR HPV16 and HPV18, as well as some LR genotypes [134].
Finally, the intralesional administration of the nonavalent vaccine Gardasil®9 was proposed for the treatment of HPV-related recalcitrant warts in a retrospective case series [135]. In detail, within a cohort of 20 individuals (13 adults and 7 children), 12 (60%) achieved a complete response, whereas 8 (40%) exhibited a partial response. This study suggested that Gardasil®9, whose safety profile has already been demonstrated and has already been approved as a prophylactic vaccine for HPV-related cervical cancer, could also be considered as an alternative strategy for the treatment of recalcitrant cutaneous warts.
8. Materials and Methods
Given the narrative nature of the present review, no predefined inclusion or exclusion criteria were established prior to the literature search.
A comprehensive search of the PubMed and Scopus databases was conducted to identify relevant publications. The key terms used for the search strategy included: “keratoacanthoma” OR “KA” AND “pathogenesis” OR “etiology” OR “human papillomavirus” OR “HPV” OR “management” OR “treatment” OR “therapy” OR “diagnosis” OR “dermoscopy” OR “reflectance confocal microscopy” OR “RCM” OR “line-field confocal optical coherence tomography” OR “LC-OCT” OR “Histopathology”. No language or publication date restrictions were applied. The database search was performed from inception to 7th August 2025. Additional relevant articles were identified by manual cross-referencing from the bibliographies of retrieved papers. Preference was given to peer-reviewed original articles, systematic reviews, meta-analyses, and significant case series that addressed the epidemiology, clinical presentation, diagnostic tools, histopathological features, molecular mechanisms, and therapeutic strategies for KA.
The following PICO (Population, Intervention or exposure, Comparison, Outcome) algorithm was applied to guide the literature selection: (i) Population: patients with KA (solitary, multiple, or eruptive forms); (ii) Intervention/exposure: diagnostic and therapeutic approaches, as well as studies on etiopathogenesis and HPV involvement; (iii) Comparator: other cutaneous epithelial tumors, particularly well-differentiated SCC; (iv) Outcome: advances in understanding pathogenesis, improvements in diagnostic accuracy, and evaluation of therapeutic efficacy.
9. Conclusions
KA is a rapidly growing epithelial neoplasm that often poses diagnostic challenges due to its clinical and histological resemblance to well-differentiated SCC. Accurate diagnosis benefits from various non-invasive imaging techniques, such as dermoscopy, RCM, and LC-OCT, which allow for near-histologic, real-time in vivo evaluation, although they are limited by penetration depth and keratin density. Histopathological examination remains essential, with key features including symmetry, absence of extension beyond sweat glands, lack of stromal infiltration, and minimal nuclear atypia helping to distinguish KA from SCC. However, inaccurate biopsies may lead to misdiagnosis and overtreatment. HPVs, particularly cutaneous β types, act as cofactors in skin carcinogenesis by interfering with cellular responses to UV-induced DNA damage and promoting lesion development. The complex interplay between viral factors, UV exposure, and host susceptibility continues to be an important area of research. Surgical excision remains the first-line treatment for KA, though non-surgical options—including radiotherapy, cryotherapy, photodynamic therapy, topical agents such as 5-fluorouracil and imiquimod, and systemic therapies like retinoids and erlotinib—offer valuable alternatives in select cases, especially for multiple or difficult-to-treat lesions. Available prophylactic HPV vaccines, targeting HR mucosal genotypes, have substantially advanced cancer prevention, while novel vaccine candidates based on the conserved L2 protein hold promise for broader protection against both cutaneous and mucosal HPV types. Intralesional administration of the nonavalent Gardasil®9 vaccine has also shown potential as a therapeutic approach for recalcitrant HPV-related warts.
Integrating advances in diagnostic approaches, understanding of pathogenetic mechanism, and therapeutic strategies is critical for optimizing the management of KA and HPV-associated lesions, to improve diagnostic accuracy, minimizing overtreatment, and developing more effective prevention measures.
Author Contributions
“Conceptualization, M.H., D.D, E.D. and L.F.; writing—original draft preparation, M.H., D.D, A.D.G., C.C (Conforti)., E.D. and L.F; writing—review and editing, M.H., D.D, D.A., F.M, F.R., C.B., A.L.,G.D.L., A.D.G., A.P., C.C. (Chello), C.C. (Conforti), E.D. and L.F.; funding acquisition, D.A., A.L.. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Associazione Italiana per la Ricerca sul Cancro, AIRC, Italy, grant number IG 2021 - ID. 25899 (to A.L.); by EU funding within the NextGenerationEU-MUR PNRR Extended Partnership initiative on Emerging Infectious Diseases (Project no. PE00000007, INF-ACT) (to A.L.); by Ministero dell'Università e della Ricerca, Italy, grants PRIN 2022-cod. 20223RYYFC and PRIN 2022 PNRR - cod. P20222YKP8 (to A.L.); and by “Progetto Ricerca Corrente 2024” from the Italian Ministry of Health (to D.A.).
Data Availability Statement
Data is available within the article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| KA | Keratoacanthoma |
| SCC | Squamous Cell Carcinoma |
| RCM | Reflectance Confocal Microscopy |
| LC-OCT | Line-Field Confocal Optical Coherence Tomography |
| HPV | Human Papillomavirus |
| UV | Ultraviolet |
| MTS | Muir-Torre Syndrome |
| MSSE | Multiple Self-healing Squamous Epithelioma |
| MFKWZ | Multiple Familial KA of Witten and Zak |
| XP | Xeroderma Pigmentosum |
| IP | Incontinentia Pigmenti |
| EV | Epidermodysplasia Verruciformis |
| GEKA | Generalized Eruptive Keratoacanthoma |
| HR | High-Risk |
| LR | Low-Risk |
| NER | Nucleotide Excision Repair |
| E6AP | E6-Associated Protein |
| pRb | Retinoblastoma protein |
| RT | Radiotherapy |
| PDT | Photodynamic therapy |
| 5-FU | 5-Fluorouracil |
| EGFR | Epidermal Growth Factor Receptor |
References
- Robertson, S.J.; Bashir, S.J.; Pichert, G.; Robson, A.; Whittaker, S. Severe exacerbation of multiple self-healing squamous epithelioma (Ferguson–Smith disease) with radiotherapy, which was successfully treated with acitretin. Clin Exp Dermatol 2010, 35(4), e100–2. [Google Scholar] [CrossRef]
- Kwiek, B.; Schwartz, R.A. Keratoacanthoma (KA): An update and review. J Am Acad Dermatol 2016, 74(6), 1220–33. [Google Scholar] [CrossRef]
- Miedzinski, F.; Kozakiewicz, J. Keratoacanthoma centrifugum--a special variety of keratoacanthoma. Hautarzt 1962, 13, 348–52. [Google Scholar] [PubMed]
- Ramselaar, C.G.; Ruitenberg, E.J.; Kruizinga, W. Regression of induced keratoacanthomas in anagen (hair growth phase) skin grafts in mice. Cancer Res 1980, 40(5), 1668–73. [Google Scholar] [PubMed]
- Zito, G.; Saotome, I.; Liu, Z.; Ferro, E.G.; Sun, T.Y.; Nguyen, D.X.; Bilguvar, K.; Ko, C.J.; Greco, V. Spontaneous tumour regression in keratoacanthomas is driven by Wnt/retinoic acid signalling cross-talk. Nat Commun 2014, 5, 3543. [Google Scholar] [CrossRef]
- Hu, W.; Cook, T.; Oh, C.W.; Penneys, N.S. Expression of the cyclin-dependent kinase inhibitor p27 in keratoacanthoma. J Am Acad Dermatol 2000, 42(3), 473–5. [Google Scholar] [CrossRef] [PubMed]
- Su, F.; Viros, A.; Milagre, C.; Trunzer, K.; Bollag, G.; Spleiss, O.; Reis-Filho, J.S.; Kong, X.; Koya, R.C.; Flaherty, K.T.; Chapman, P.B.; Kim, M.J.; Hayward, R.; Martin, M.; Yang, H.; Wang, Q.; Hilton, H.; Hang, J.S.; Noe, J.; Lambros, M.; Geyer, F.; Dhomen, N.; Niculescu-Duvaz, I.; Zambon, A.; Niculescu-Duvaz, D.; Preece, N.; Robert, L.; Otte, N.J.; Mok, S.; Kee, D.; Ma, Y.; Zhang, C.; Habets, G.; Burton, E.A.; Wong, B.; Nguyen, H.; Kockx, M.; Andries, L.; Lestini, B.; Nolop, K.B.; Lee, R.J.; Joe, A.K.; Troy, J.L.; Gonzalez, R.; Hutson, T.E.; Puzanov, I.; Chmielowski, B.; Springer, C.J.; McArthur, G.A.; Sosman, J.A.; Lo, R.S.; Ribas, A.; Marais, R. RAS mutations in cutaneous squamous-cell carcinomas in patients treated with BRAF inhibitors. N Engl J Med 2012, 366(3), 207–15. [Google Scholar] [CrossRef]
- Corominas, M.; Kamino, H.; Leon, J.; Pellicer, A. Oncogene activation in human benign tumors of the skin (keratoacanthomas): is HRAS involved in differentiation as well as proliferation? Proc Natl Acad Sci USA 1989, 86(16), 6372–6. [Google Scholar] [CrossRef]
- Karampinis, E.; Kostopoulou, C.; Toli, O.; Marinos, L.; Papadimitriou, G.; Roussaki Schulze, A.V.; Zafiriou, E. Multiple Keratoacanthoma-like Syndromes: Case Report and Literature Review. Medicina (Kaunas) 2024, 60(3), 371. [Google Scholar] [CrossRef]
- Dobre, A.; Nedelcu, R.I.; Turcu, G.; Brinzea, A.; Struna, I.; Tudorache, G.; Ali, A.; Hulea, I.; Balasescu, E.; Fertig, T.E.; Gherghiceanu, M.; Harwood, C.; Ion, D.A.; Forsea, A.M. Multiple Keratoacanthomas Associated with Genetic Syndromes: Narrative Review and Proposal of a Diagnostic Algorithm. Am J Clin Dermatol 2025, 26(1), 45–59. [Google Scholar] [CrossRef]
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; van Akkooi, A.; Bataille, V.; Bastholt, L.; Dreno, B.; Dummer, R.; Fargnoli, M.C.; Forsea, A.M.; Harwood, C.A.; Hauschild, A.; Hoeller, C.; Kandolf-Sekulovic, L.; Kaufmann, R.; Kelleners-Smeets, N.W.; Lallas, A.; Leiter, U.; Malvehy, J.; Del Marmol, V.; Moreno-Ramirez, D.; Pellacani, G.; Peris, K.; Saiag, P.; Tagliaferri, L.; Trakatelli, M.; Ioannides, D.; Vieira, R.; Zalaudek, I.; Arenberger, P.; Eggermont, A.M.M.; Röcken, M.; Grob, J.J.; Lorigan, P.; EADO; EDF; ESTRO; UEMS; EADV; and EORTC. European consensus-based interdisciplinary guideline for invasive cutaneous squamous cell carcinoma: Part 2. Treatment-Update 2023. Eur J Cancer; 2023; 193, p. 113252. [Google Scholar]
- Cohen, P.R.; Schulze, K.E.; Teller, C.F.; Nelson, B.R. Intralesional methotrexate for keratoacanthoma of the nose. Skinmed 2005, 4(6), 393–5. [Google Scholar]
- Kiss, N.; Avci, P.; Bánvölgyi, A.; Lőrincz, K.; Szakonyi, J.; Gyöngyösi, N.; Fésűs, L; Lee, G; Wikonkál, N. Intralesional therapy for the treatment of keratoacanthoma. Dermatol Ther. 2019, 32(3), e12872. [Google Scholar] [CrossRef]
- Sullivan, J.J. Keratoacanthoma: the Australian experience. Australas J Dermatol 1997, 38, S36–39. [Google Scholar]
- Reizner, G.T.; Chuang, T.Y.; Elpern, D.J.; Stone, J.L.; Farmer, E.R. Basal cell carcinoma and keratoacanthoma in Hawaiians: an incidence report. J Am Acad Dermatol 1993, 29 5 Pt 1, 780–2. [Google Scholar] [CrossRef]
- Vergilis-Kalner, I.J.; Kriseman, Y.; Goldberg, L.H. Keratoacanthomas: overview and comparison between Houston and minneapolis experiences. J Drugs Dermatol 2010, 9(2), 117–21. [Google Scholar]
- Fania, L.; Didona, D.; Di Pietro, F.R.; Verkhovskaia, S.; Morese, R.; Paolino, G.; Donati, M.; Ricci, F.; Coco, V.; Ricci, F.; Candi, E.; Abeni, D.; Dellambra, E. Cutaneous Squamous Cell Carcinoma: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2021, 9(2), 171. [Google Scholar] [CrossRef]
- Goldberg, L.H.; Silapunt, S.; Beyrau, K.K.; Peterson, S.R.; Friedman, P.M.; Alam, M. Keratoacanthoma as a postoperative complication of skin cancer excision. J Am Acad Dermatol 2004, 50(5), 753–8. [Google Scholar] [CrossRef]
- Gleich, T.; Chiticariu, E.; Huber, M.; Hohl, D. Keratoacanthoma: a distinct entity? Exp Dermatol 2016, 25(2), 85–91. [Google Scholar] [CrossRef]
- Ambur, A.; Clark, A.; Nathoo, R. An Updated Review of the Therapeutic Management of Keratoacanthomas. J Clin Aesthet Dermatol 2022, 15(11), 30–6. [Google Scholar]
- Joshi, S.; De Angelis, P.M.; Zucknick, M.; Schjølberg, A.R.; Andersen, S.N.; Clausen, O.P.F. Role of the Wnt signaling pathway in keratoacanthoma. Cancer Rep (Hoboken) 2020, 3(2), e1219. [Google Scholar] [CrossRef]
- Zito, P.M.; Scharf, R. Keratoacanthoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [accessed online 2025 Apr 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK499931/.
- Ilaria, P.; Nevena, S.; Ersilia, T.; Federica, T.; Felice, F.; Agnieszka Ewa, D.; Francesco, F.; Concetta, P. Generalized Eruptive Keratoacanthoma (GEKA) after Pfizer mRNABNT162b2 (Comirnaty®) COVID-19 Vaccination Successfully Treated with Cemiplimab. Viruses. 2024, 16(8), 1260. [Google Scholar] [CrossRef]
- Yumeen, S.; Robinson-Bostom, L.; Firoz, E.F. Solitary Eruptive Keratoacanthoma Developing at Site of COVID-19 Vaccine Injection. R I Med J 2023, 106(11), 49–51. [Google Scholar]
- Mitri, F.; Hartschuh, W.; Toberer, F. Multiple Keratoacanthomas after a Recent Tattoo: A Case Report. Case Rep Dermatol 2021, 13(1), 23–7. [Google Scholar] [CrossRef]
- Brongo, S.; Moccia, L.S.; Nunziata, V.; D’Andrea, F. Keratoacanthoma arising after site injection infection of cosmetic collagen filler. Int J Surg Case Rep 2013, 4(4), 429–31. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, S.H.; Hong, S.P.; Kim, J.; Kim, S.W. Solitary Keratoacanthoma at the Recipient Site of a Full-Thickness Skin Graft: A Case Report and Review of the Literature. Arch Plast Surg 2023, 50(1), 59–62. [Google Scholar] [CrossRef]
- Fradet, M.; Sibaud, V.; Tournier, E.; Lamant, L.; Boulinguez, S.; Brun, A.; Pages, C.; Meyer, N. Multiple Keratoacanthoma-like Lesions in a Patient Treated with Pembrolizumab. Acta Derm Venereol 2019, 99(13), 1301–2. [Google Scholar] [CrossRef]
- Li, S.; Ye, X.; Li, X.; Yang, Y. Case Report: Multiple cutaneous keratoacanthoma-like lesions in a colorectal cancer patient treated with sintilimab. Front Immunol 2025, 16, 1535220. [Google Scholar] [CrossRef]
- Frances, L.; Guijarro, J.; Marin, I.; Leiva-Salinas, M. del C, Bouret, A.M. Multiple eruptive keratoacanthomas associated with leflunomide. Dermatol Online J 2013, 19(7), 18968. [Google Scholar] [CrossRef]
- Dobre, A.; Nedelcu, R.I.; Turcu, G.; Brinzea, A.; Struna, I.; Tudorache, G.; Ali, A.; Hulea, I.; Balasescu, E.; Fertig, T.E.; Gherghiceanu, M.; Harwood, C.; Ion, D.A.; Forsea, A.M. Multiple Keratoacanthomas Associated with Genetic Syndromes: Narrative Review and Proposal of a Diagnostic Algorithm. Am J Clin Dermatol 2025, 26(1), 45–59. [Google Scholar] [CrossRef]
- Neagu, N.; Dianzani, C.; Venuti, A.; Bonin, S.; Voidăzan, S.; Zalaudek, I.; Conforti, C. The role of HPV in keratinocyte skin cancer development: A systematic review. J Eur Acad Dermatol Venereol 2023, 37(1), 40–6. [Google Scholar] [CrossRef]
- Ljubojevic, S.; Skerlev, M. HPV-associated diseases. Clin Dermatol 2014, 32(2), 227–34. [Google Scholar] [CrossRef]
- Conforti, C.; Paolini, F.; Venuti, A.; Dianzani, C.; Zalaudek, I. The detection rate of human papillomavirus in well-differentiated squamous cell carcinoma and keratoacanthoma: is there new evidence for a viral pathogenesis of keratoacanthoma? Br J Dermatol 2019, 181(6), 1309–11. [Google Scholar] [CrossRef]
- McLaughlin-Drubin, M.E. . Human papillomaviruses and non-melanoma skin cancer. Semin Oncol 2015, 42, 284–290. [Google Scholar] [CrossRef]
- Arroyo Mühr, L.S.; Hultin, E.; Bzhalava, D.; Eklund, C.; Lagheden, C.; Ekström, J.; Johansson, H.; Forslund, O.; Dillner, J. Human papillomavirus type 197 is commonly present in skin tumors. Int J Cancer 2015, 136(11), 2546–55. [Google Scholar]
- Eversole, L.R.; Leider, A.S.; Alexander, G. Intraoral and labial keratoacanthoma. Oral Surg Oral Med Oral Pathol 1982, 54(6), 663–7. [Google Scholar]
- Cristalli, M.P. ; Marini, R; La Monaca, G.; Vitolo, D.; Pompa, G.; Annibali, S. Double localization of keratoacantho-ma on the cutaneous and mucosal sides of the lower lip: report of a case. Oral Implantol (Rome) 2013, 6, 94–98. [Google Scholar]
- Janette, A.; Pecaro, B.; Lonergan, M.; Lingen, M.W. Solitary intraoral keratoacanthoma: report of a case. J Oral Maxillofac Surg 1996, 54(8), 1026–30. [Google Scholar]
- Habel, G; O’Regan, B. ; Eissing, A.; Khoury, F.; Donath, K. Intra-oral keratoacanthoma: an eruptive variant and review of the literature. Br Dent J 1991, 170(9), 336–9. [Google Scholar] [CrossRef]
- Whyte, A.M.; Hansen, L.S.; Lee, C. The intraoral keratoacanthoma: a diagnostic problem. Br J Oral Maxillofac Surg 1986, 24(6), 438–41. [Google Scholar] [CrossRef]
- Heidenreich, R.K.; Gongloff, R.K.; Wescott, W.B. A solitary, exophytic, crateriform lesion on the mandibular retromolar gingiva. J Am Dent Assoc 1986, 112(3), 377–9. [Google Scholar]
- Svirsky, J.A.; Freedman, P.D.; Lumerman, H. Solitary intraoral keratoacanthoma. Oral Surg Oral Med Oral Pathol 1977, 43(1), 116–22. [Google Scholar] [PubMed]
- Zegarelli, D.J. Solitary intraoral keratoacanthoma. Oral Surg Oral Med Oral Pathol 1975, 40(6), 785–8. [Google Scholar] [PubMed]
- Divers, A.K.; Correale, D.; Lee, J.B. Keratoacanthoma centrifugum marginatum: a diagnostic and therapeutic challenge. Cutis 2004, 73(4), 257–62. [Google Scholar]
- Wu, T.P.; Miller, K.; Cohen, D.E.; Stein, J.A. Keratoacanthomas arising in association with prurigo nodules in pruritic, actinically damaged skin. J Am Acad Dermatol 2013, 69(3), 426–30. [Google Scholar]
- Goudie, D.R.; D’Alessandro, M.; Merriman, B.; Lee, H.; Szeverényi, I.; Avery, S.; O'Connor, B.D.; Nelson, S.F.; Coats, S.E.; Stewart, A.; Christie, L.; Pichert, G.; Friedel, J.; Hayes, I.; Burrows, N.; Whittaker, S.; Gerdes, A.M.; Broesby-Olsen, S.; Ferguson-Smith, M.A.; Verma, C.; Lunny, D.P.; Reversade, B.; Lane, E.B. Multiple self-healing squamous epithelioma is caused by a disease-specific spectrum of mutations in TGFBR1. Nat Genet 2011, 43(4), 365–9. [Google Scholar]
- Grzybowski, M. A case of peculiar generalized epithelial tumours of the skin. Br J Dermatol Syph 1950, 62, 310–313. [Google Scholar]
- Anzalone, C.L.; Cohen, P.R. Generalized eruptive keratoacanthomas of Grzybowski. Int J Dermatol 2014, 53(2), 131–6. [Google Scholar]
- Agarwal, M.; Chander, R.; Karmakar, S.; Walia, R. Multiple familial keratoacanthoma of Witten and Zak - A report of three siblings. Dermatology 1999, 198(4), 396–9. [Google Scholar]
- Boateng, B.; Hornstein, O.P.; von den Driesch, P.; Kiesewetter, F. [Multiple keratoacanthomas (Witten-Zak type) in prurigo simplex subacuta]. Hautarzt 1995, 46(2), 114–7. [Google Scholar]
- Rosendahl, C.; Cameron, A.; Argenziano, G.; Zalaudek, I.; Tschandl, P.; Kittler, H. Dermoscopy of squamous cell carcinoma and keratoacanthoma. Arch Dermatol 2012, 148(12), 1386–92. [Google Scholar] [PubMed]
- Zalaudek, I.; Giacomel, J.; Schmid, K.; Bondino, S.; Rosendahl, C.; Cavicchini, S.; Tourlaki, A.; Gasparini, S.; Bourne, P.; Keir, J.; Kittler, H.; Eibenschutz, L.; Catricalà, C.; Argenziano, G. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: a progression model. J Am Acad Dermatol 2012, 66(4), 589–97. [Google Scholar] [CrossRef]
- Wang, X.; Wang, Y.; Wang, H.; Zheng, L.; Guo, Z.; Fan, X.; Gao, M. The first report of diagnosing of keratoacanthoma in Chinese Han patients using dermoscopy and reflectance confocal microscopy. Skin Res Technol 2021, 27(3), 422–7. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.P.; Peppelman, M.; Hoogedoorn, L.; Van Erp, P.E.J.; Gerritsen, M.J.P. The current role of in vivo reflectance confocal microscopy within the continuum of actinic keratosis and squamous cell carcinoma: a systematic review. Eur J Dermatol 2016, 26(6), 549–65. [Google Scholar] [PubMed]
- Latriglia, F.; Ogien, J.; Tavernier, C.; Fischman, S.; Suppa, M.; Perrot, J.L.; Dubois, A. Line-Field Confocal Optical Coherence Tomography (LC-OCT) for Skin Imaging in Dermatology. Life (Basel) 2023, 13(12), 2268. [Google Scholar]
- Cinotti, E.; Brunetti, T.; Cartocci, A.; Tognetti, L.; Suppa, M.; Malvehy, J.; Perez-Anker, J.; Puig, S.; Perrot, J.L.; Rubegni, P. Diagnostic Accuracy of Line-Field Confocal Optical Coherence Tomography for the Diagnosis of Skin Carcinomas. Diagnostics (Basel) 2023, 13(3), 361. [Google Scholar] [PubMed]
- Schwartz, R.A. Keratoacanthoma: a clinico-pathologic enigma. Dermatol Surg 2004, 30 2 Pt 2, 326–33. [Google Scholar]
- Ogita, A.; Ansai, S.I.; Misago, N.; Anan, T.; Fukumoto, T.; Saeki, H. Histopathological diagnosis of epithelial crateriform tumors: Keratoacanthoma and other epithelial crateriform tumors. J Dermatol 2016, 43(11), 1321–31. [Google Scholar]
- Takai, T. Advances in histopathological diagnosis of keratoacanthoma. J Dermatol 2017, 44(3), 304–14. [Google Scholar] [CrossRef]
- Cribier, B.; Asch, P.; Grosshans, E. Differentiating squamous cell carcinoma from keratoacanthoma using histopathological criteria. Is it possible? A study of 296 cases. Dermatology 1999, 199(3), 208–12. [Google Scholar]
- Savage, J.A.; Maize, J.C. Keratoacanthoma clinical behavior: a systematic review. Am J Dermatopathol 2014, 36(5), 422–9. [Google Scholar] [CrossRef]
- Kossard, S.; Tan, K.B.; Choy, C. Keratoacanthoma and infundibulocystic squamous cell carcinoma. Am J Dermatopathol 2008, 30(2), 127–34. [Google Scholar] [PubMed]
- Weedon, D.D.; Malo, J.; Brooks, D.; Williamson, R. Squamous cell carcinoma arising in keratoacanthoma: a neglected phenomenon in the elderly. Am J Dermatopathol 2010, 32(5), 423–6. [Google Scholar] [PubMed]
- Piscioli, F.; Boi, S.; Zumiani, G.; Cristofolini, M. A gigantic, metastasizing keratoacanthoma. Report of a case and discussion on classification. Am J Dermatopathol 1984, 6(2), 123–9. [Google Scholar] [CrossRef]
- Nelson, C.W.; Mirabello, L. Human papillomavirus genomics: Understanding carcinogenicity. Tumour Virus Research 2023, 15, 200258. [Google Scholar] [CrossRef] [PubMed]
- Skelin, J.; Tomaić, V. Comparative analysis of alpha and beta HPV E6 oncoproteins: Insights into functional distinctions and divergent mechanisms of pathogenesis. Viruses 2023, 15(11), 2253. [Google Scholar] [CrossRef]
- Doorbar, J.; Quint, W.; Banks, L.; Bravo, I.G.; Stoler, M.; Broker, T.R.; Stanley, M.A. The biology and life-cycle of human papillomaviruses. Vaccine 2012, 30 (Suppl 5), F55–70. [Google Scholar] [CrossRef]
- Buck, C.B.; Cheng, N.; Thompson, C.D.; Lowy, D.R.; Steven, A.C.; Schiller, J.T.; et al. Arrangement of L2 within the papillomavirus capsid. J. Virol 2008, 82(11), 5190–7. [Google Scholar]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front Oncol 2019, 9, 355. [Google Scholar] [CrossRef]
- Schiffman, M.; Doorbar, J.; Wentzensen, N.; De Sanjosé, S.; Fakhry, C.; Monk, B.J.; Stanley, M.A.; Franceschi, S. Carcinogenic human papillomavirus infection. Nat. Rev. Dis. Primers 2016, 2(1), 16086. [Google Scholar] [CrossRef]
- Müller, M.; Prescott, E.L.; Wasson, C.W.; Macdonald, A. Human papillomavirus E5 oncoprotein: Function and potential target for antiviral therapeutics. Future Virol 2015, 10(1), 27–39. [Google Scholar] [CrossRef]
- Pešut, E.; Đukić, A.; Lulić, L.; Skelin, J.; Šimić, I.; Milutin Gašperov, N.; Tomaić, V.; Sabol, I.; Grce, M. Human Papillomaviruses-Associated Cancers: An Update of Current Knowledge. Viruses. 2021, 13(11), 2234. [Google Scholar] [CrossRef] [PubMed]
- Messa, L.; Loregian, A. HPV-induced cancers: preclinical therapeutic advancements. Expert Opin Investig Drugs 2022, 31(1), 79–93. [Google Scholar] [CrossRef] [PubMed]
- Egawa, N.; Egawa, K.; Griffin, H.; Doorbar, J. Human Papillomaviruses; Epithelial Tropisms, and the Development of Neoplasia. Viruses. 2015, 7(7), 3863–90. [Google Scholar] [CrossRef]
- Tampa, M.; Mitran, C.I.; Mitran, M.I.; Nicolae, I.; Dumitru, A.; Matei, C.; Manolescu, L.; Popa, G.L.; Caruntu, C.; Georgescu, S.R. The Role of Beta HPV Types and HPV-Associated Inflammatory Processes in Cutaneous Squamous Cell Carcinoma. J Immunol Research 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Orth, G. Genetics of Epidermodysplasia Verruciformis: Insights into Host Defense against Papillomaviruses. Semin Immunol 2006, 18, 362–74. [Google Scholar] [CrossRef]
- Quint, K.D.; Genders, R.E.; de Koning, M.N.; Borgogna, C.; Gariglio, M.; Bouwes Bavinck, J.N.; Doorbar, J.; Feltkamp, M.C.W. Human Beta-Papillomavirus Infection and Keratinocyte Carcinomas. J Pathol 2015, 235, 342–54. [Google Scholar] [CrossRef]
- Hufbauer, M.; Akgül, B. Molecular Mechanisms of Human Papillomavirus Induced Skin Carcinogenesis. Viruses 2017, 9, 187. [Google Scholar] [CrossRef]
- Schuch, A.P.; Moreno, N.C.; Schuch, N.J.; Menck, C.F.M.; Garcia, C.C.M. Sunlight Damage to Cellular DNA: Focus on Oxidatively Generated Lesions. Free Radic Biol Med 2017, 107, 110–24. [Google Scholar] [CrossRef]
- Douki, T.; von Koschembahr, A.; Cadet, J. Insight in DNA Repair of UV-Induced Pyrimidine Dimers by Chromatographic Methods. Photochem Photobiol 2017, 93, 207–15. [Google Scholar] [CrossRef]
- Brash, D.E.; Ziegler, A.; Jonason, A.S.; Simon, J.A.; Kunala, S.; Leffell, D.J. Sunlight and Sunburn in Human Skin Cancer: p53, Apoptosis, and Tumor Promotion. J Investig Dermatol Symp Proc 1996, 1, 136–42. [Google Scholar] [PubMed]
- Wahl, G.M.; Carr, A.M. The Evolution of Diverse Biological Responses to DNA Damage: Insights from Yeast and p53. Nat Cell Biol 2001, 3, E277–86. [Google Scholar] [CrossRef]
- el-Deiry, W.S.; Harper, J.W.; O’Connor, P.M.; Velculescu, V.E.; Canman, C.E.; Jackman, J.; Pietenpol, J.A.; Burrell, M.; Hill, D.E.; Wang, Y.; Wiman, K.G.; Mercer, W.E.; Kastan, M.B.; Kohn, K.W.; Elledge, S.J.; Kinzler, K.W.; Vogelstein, B. WAF1/CIP1 Is Induced in p53-Mediated G1 Arrest and Apoptosis. Cancer Res 1994, 54, 1169–74. [Google Scholar] [PubMed]
- Scheffner, M.; Werness, B.A.; Huibregtse, J.M.; Levine, A.J.; Howley, P.M. The E6 Oncoprotein Encoded by Human Papillomavirus Types 16 and 18 Promotes the Degradation of p53. Cell 1990, 63, 1129–36. [Google Scholar] [CrossRef] [PubMed]
- Hengstermann, A.; Linares, L.K.; Ciechanover, A.; Whitaker, N.J.; Scheffner, M. Complete Switch from Mdm2 to Human Papillomavirus E6-Mediated Degradation of p53 in Cervical Cancer Cells. Proc Natl Acad Sci USA 2001, 98, 1218–23. [Google Scholar] [CrossRef]
- Li, S.; Hong, X.; Wei, Z.; Xie, M.; Li, W.; Liu, G.; Guo, H.; Yang, J.; Wei, W.; Zhang, S. Ubiquitination of the HPV Oncoprotein E6 Is Critical for E6/E6AP-Mediated p53 Degradation. Front Microbiol 2019, 10, 2483. [Google Scholar] [CrossRef]
- Martinez-Zapien, D.; Ruiz, F.X.; Poirson, J.; Mitschler, A.; Ramirez, J.; Forster, A.; Cousido-Siah, A.; Masson, M.; Vande Pol, S.; Podjarny, A.; Travé, G.; Zanier, K. Structure of the E6/E6AP/p53 Complex Required for HPV-Mediated Degradation of p53. Nature 2016, 529, 541–5. [Google Scholar] [CrossRef]
- Muench, P.; Probst, S.; Schuetz, J.; Leiprecht, N.; Busch, M.; Wesselborg, S.; Stubenrauch, F.; Iftner, T. Cutaneous Papillomavirus E6 Proteins Must Interact with p300 and Block p53-Mediated Apoptosis for Cellular Immortalization and Tumorigenesis. Cancer Res 2010, 70, 6913–24. [Google Scholar] [CrossRef]
- Muschik, D.; Braspenning-Wesch, I.; Stockfleth, E.; Rösl, F.; Hofmann, T.G.; Nindl, I. Cutaneous HPV23 E6 Prevents p53 Phosphorylation through Interaction with HIPK2. PLoS ONE 2011, 6, e27655. [Google Scholar] [CrossRef]
- Minoni, L.; Romero-Medina, M.C.; Venuti, A.; Sirand, C.; Robitaille, A.; Altamura, G.; Tommasino, M.; Accardi, R. Transforming Properties of Beta-3 Human Papillomavirus E6 and E7 Proteins. mSphere 2020, 5, e00398. [Google Scholar] [CrossRef] [PubMed]
- Cornet, I.; Bouvard, V.; Campo, M.S.; Thomas, M.; Banks, L.; Gissmann, L.; Tommasino, M. Comparative Analysis of Transforming Properties of E6 and E7 from Different Beta Human Papillomavirus Types. J Virol 2012, 86, 2366–70. [Google Scholar] [CrossRef]
- White, E.A.; Kramer, R.E.; Tan, M.J.A.; Hayes, S.D.; Harper, J.W.; Howley, P.M. Comprehensive Analysis of Host Cellular Interactions with Human Papillomavirus E6 Proteins Identifies New E6 Binding Partners and Reflects Viral Diversity. J Virol 2012, 86, 13174–86. [Google Scholar] [PubMed]
- Accardi, R.; Dong, W.; Smet, A.; Cui, R.; Hautefeuille, A.; Gabet, A.; Tommasino, M. Skin Human Papillomavirus Type 38 Alters p53 Functions by Accumulation of ΔNp73. EMBO Rep 2006, 7, 334–40. [Google Scholar] [CrossRef] [PubMed]
- Di, C.; Yang, L.; Zhang, H.; Ma, X.; Zhang, X.; Sun, C.; Zhu, H. Mechanisms, Function and Clinical Applications of ΔNp73. Cell Cycle 2013, 12, 1861–7. [Google Scholar] [CrossRef]
- Accardi, R.; Scalise, M.; Gheit, T.; Hussain, I.; Yue, J.; Carreira, C.; Tommasino, M. IκB Kinase β Promotes Cell Survival by Antagonizing p53 Functions through ΔNp73α Phosphorylation and Stabilization. Mol Cell Biol 2011, 31, 2210–26. [Google Scholar] [CrossRef] [PubMed]
- Peña-Blanco, A.; García-Sáez, A.J. Bax, Bak and Beyond — Mitochondrial Performance in Apoptosis. FEBS J 2018, 285, 416–31. [Google Scholar] [CrossRef]
- Jackson, S.; Harwood, C.; Thomas, M.; Banks, L.; Storey, A. Role of Bak in UV-Induced Apoptosis in Skin Cancer and Abrogation by HPV E6 Proteins. Genes Dev 2000, 14, 3065–73. [Google Scholar] [CrossRef]
- Thomas, M.; Banks, L. Inhibition of Bak-Induced Apoptosis by HPV-18 E6. Oncogene 1998, 17, 2943–54. [Google Scholar] [CrossRef]
- Magal, S.S.; Jackman, A.; Ish-Shalom, S.; Botzer, L.E.; Gonen, P.; Schlegel, R.; Shai, A. Downregulation of Bax mRNA Expression and Protein Stability by the E6 Protein of Human Papillomavirus 16. J. Gen. Virol. 2005, 86, 611–21. [Google Scholar] [CrossRef]
- Lee, J.O.; Russo, A.A.; Pavletich, N.P. Structure of the Retinoblastoma Tumour-Suppressor Pocket Domain Bound to a Peptide from HPV E7. Nature 1998, 391, 859–65. [Google Scholar] [CrossRef]
- Davies, R.; Hicks, R.; Crook, T.; Morris, J.; Vousden, K. Human Papillomavirus Type 16 E7 Associates with a Histone H1 Kinase and with p107 through Sequences Necessary for Transformation. J Virol 1993, 67, 2521–28. [Google Scholar]
- Zhang, B.; Chen, W.; Roman, A. The E7 Proteins of Low- and High-Risk Human Papillomaviruses Share the Ability to Target the pRB Family Member p130 for Degradation. Proc Natl Acad Sci USA 2006, 103, 437–42. [Google Scholar] [CrossRef]
- Münger, K.; Werness, B.A.; Dyson, N.; Phelps, W.C.; Harlow, E.; Howley, P.M. Complex Formation of Human Papillomavirus E7 Proteins with the Retinoblastoma Tumor Suppressor Gene Product. EMBO J 1989, 8, 4099–105. [Google Scholar] [CrossRef] [PubMed]
- Szalmás, A.; Tomaić, V.; Basukala, O.; Massimi, P.; Mittal, S.; Kónya, J.; Banks, L. The PTPN14 Tumor Suppressor Is a Degradation Target of Human Papillomavirus E7. J Virol 2017, 91, e00057–17. [Google Scholar] [CrossRef]
- Hatterschide, J.; Bohidar, A.E.; Grace, M.; Nulton, T.J.; Kim, H.W.; Windle, B.; Morgan, I.M. PTPN14 Degradation by High-Risk Human Papillomavirus E7 Limits Keratinocyte Differentiation and Contributes to HPV-Mediated Oncogenesis. Proc Natl Acad Sci USA 2019, 116, 7033–42. [Google Scholar] [CrossRef]
- Lee, H.S.; Kim, M.W.; Jin, K.S.; Shin, H.C.; Kim, W.K.; Lee, S.C.; Park, J.H. Molecular Analysis of the Interaction between Human PTPN21 and the Oncoprotein E7 from Human Papillomavirus Genotype 18. Mol Cells 2021, 44, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Trejo-Cerro, O.; Massimi, P.; Broniarczyk, J.; Myers, M.; Banks, L. Repression of Memo1, a Novel Target of Human Papillomavirus Type 16 E7, Increases Cell Proliferation in Cervical Cancer Cells. J Virol 2022, 96. [Google Scholar] [CrossRef] [PubMed]
- Romero-Masters, J.C.; Lambert, P.F.; Munger, K. Molecular Mechanisms of MmuPV1 E6 and E7 and Implications for Human Disease. Viruses 2022, 14. [Google Scholar] [CrossRef]
- Giarrè, M.; Caldeira, S.; Malanchi, I.; Ciccolini, F.; Leão, M.J.; Tommasino, M. Induction of pRb Degradation by the Human Papillomavirus Type 16 E7 Protein Is Essential To Efficiently Overcome p16^INK4a^-Imposed G1 Cell Cycle Arrest. J Virol 2001, 75(10), 4705–12. [Google Scholar] [CrossRef]
- Caldeira, S.; Zehbe, I.; Accardi, R.; Malanchi, I.; Dong, W.; Giarrè, M.; Tommasino, M. The E6 and E7 Proteins of the Cutaneous Human Papillomavirus Type 38 Display Transforming Properties. J Virol 2003, 77(3), 2195–206. [Google Scholar] [CrossRef]
- Wallace, N.A.; Robinson, K.; Howie, H.L.; Galloway, D.A. HPV 5 and 8 E6 Abrogate ATR Activity Resulting in Increased Persistence of UVB Induced DNA Damage. PLoS Pathog 2012, 8(7), e1002807. [Google Scholar] [CrossRef]
- Tran, D.C.; Li, S.; Henry, S.; Wood, D.J.; Chang, A.L.S. An 18-year retrospective study on the outcomes of keratoacanthomas with different treatment modalities at a single academic centre. Br J Dermatol 2017, 177(6), 1749–51. [Google Scholar] [CrossRef]
- Caccialanza, M.; Sopelana, N. Radiation therapy of keratoacanthomas: results in 55 patients. Int J Radiat Oncol Biol Phys 1989, 16(2), 475–7. [Google Scholar] [CrossRef] [PubMed]
- Donahue, B.; Cooper, J.S.; Rush, S. Treatment of aggressive keratoacanthomas by radiotherapy. J Am Acad Dermatol 1990, 23 3 Pt 1, 489–93. [Google Scholar] [CrossRef]
- Shimm, D.S.; Duttenhaver, J.R.; Doucette, J.; Wang, C.C. Radiation therapy of keratoacanthoma. Int J Radiat Oncol Biol Phys 1983, 9(5), 759–61. [Google Scholar] [CrossRef]
- Shaw, J.C.; Storrs, F.J.; Everts, E. Multiple keratoacanthomas after megavoltage radiation therapy. J Am Acad Dermatol 1990, 23 5 Pt 2, 1009–11. [Google Scholar] [CrossRef]
- Kuflik, E.G. Cryosurgery for cutaneous malignancy: An update. Dermatol Surg 1997, 23(11), 1081–87. [Google Scholar] [CrossRef]
- Gogia, R.; Grekin, R.C.; Shinkai, K. Eruptive self-resolving keratoacanthomas developing after treatment with photodynamic therapy and microdermabrasion. Dermatol Surg 2013, 39, 1717–20. [Google Scholar] [CrossRef]
- Neumann, R.A.; Knobler, R.M. Argon laser treatment of small keratoacanthomas in difficult locations. Int J Dermatol 1990, 29(10), 733–6. [Google Scholar] [CrossRef]
- Yoshioka, A.; Tanaka, S.; Hiraoka, O.; Koyama, Y.; Hirota, Y.; Ayusawa, D.; Nishimoto, I. Deoxyribonucleoside triphosphate imbalance. 5-Fluorodeoxyuridine-induced DNA double strand breaks in mouse FM3A cells and the mechanism of cell death. J Biol Chem 1987, 262, 8235–41. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.J.; Ravits, M.; Silvers, D.N. Clinical efficacy of short contact topical 5-Fluorouracil in the treatment of keratoacanthomas: a retrospective analysis. J Clin Aesthet Dermatol 2014, 7(11), 35–7. [Google Scholar]
- Goette, D.K.; Odom, R.B. Successful treatment of keratoacanthoma with intralesional fluorouracil. J Am Acad Dermatol 1980, 2(3), 212–6. [Google Scholar] [CrossRef] [PubMed]
- Thiele, J.J.; Ziemer, M.; Fuchs, S.; Elsner, P. Combined 5-fluorouracil and Er:YAG laser treatment in a case of recurrent giant keratoacanthoma of the lower leg. Dermatol Surg 2004, 30 12 Pt 2, 1556–60. [Google Scholar]
- Jeon, H.C.; Choi, M.; Paik, S.H.; Ahn, C.H.; Park, H.S.; Cho, K.H. Treatment of keratoacanthoma with 5% imiquimod cream and review of the previous report. Ann Dermatol 2011, 23(3), 357–61. [Google Scholar] [CrossRef]
- Gavric, G.; Lekic, B.; Milinkovic Sreckovic, M.; Bosic, M.; Zivanovic, D. Keratoacanthoma centrifugum marginatum associated with mechanical trauma: Response to acitretin—A case report and review of the literature. Dermatol Ther 2020, 33(3), e13397. [Google Scholar] [CrossRef]
- Mizuta, H.; Takahashi, A.; Mori, T.; Namikawa, K.; Nakano, E.; Muto, Y.; et al. Efficacy of oral retinoids for keratoacanthoma centrifugum marginatum. Dermatol Ther 2020, 33(3), e13291. [Google Scholar] [CrossRef]
- Zhang, S.; Han, D.; Wang, T.; Liu, Y. Multiple keratoacanthoma and oral lichen planus successfully treated with systemic retinoids and review of multiple keratoacanthoma associated with lichen planus. Int J Dermatol 2018, 57, 1125–7. [Google Scholar] [CrossRef]
- Reid, D.C.; Guitart, J.; Agulnik, M.; Lacouture, M.E. Treatment of multiple keratoacanthomas with erlotinib. Int. J. Clin. Oncol. 2010, 15, 413–5. [Google Scholar] [CrossRef] [PubMed]
- Pogoda, C.S.; Roden, R.B.S.; Garcea, R.L. Immunizing against Anogenital Cancer: HPV Vaccines. PLoS Pathog 2016, 12, e1005587. [Google Scholar] [CrossRef]
- Pouyanfard, S.; Spagnoli, G.; Bulli, L.; Balz, K.; Yang, F.; Odenwald, C.; et al. Minor Capsid Protein L2 Polytope Induces Broad Protection against Oncogenic and Mucosal Human Papillomaviruses. J Virol 2018, 92, e01930–17. [Google Scholar] [CrossRef]
- Seitz, H.; Ribeiro-Müller, L.; Canali, E.; Bolchi, A.; Tommasino, M.; Ottonello, S.; et al. Robust In Vitro and In Vivo Neutralization against Multiple High-Risk HPV Types Induced by a Thermostable Thioredoxin-L2 Vaccine. Cancer Prev Res 2015, 8, 932–41. [Google Scholar] [CrossRef] [PubMed]
- German Cancer Research Center. PANHPVAX, Study of a New HPV Vaccine in Healthy Volunteers (PANHPVAX). 2023 [cited 2025 Aug 8]. Available from: https://clinicaltrials.gov/study/NCT05208710?intr=Cyclic.
- Mariz, F.C.; Balz, K.; Dittrich, M.; Zhang, Y.; Yang, F.; Zhao, X.; et al. A broadly protective vaccine against cutaneous human papillomaviruses. NPJ Vaccines 2022, 7, 116. [Google Scholar] [CrossRef] [PubMed]
- Bar-Ilan, E.; Bar, J.; Baniel, A.; Slodownik, D.; Artzi, O.; Samuelov, L.; et al. Intralesional human papillomavirus vaccine for the treatment of recalcitrant cutaneous warts. J Dermatol 2023, 50, 1373–80. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Best-characterized molecular mechanism involved in carcinogenesis occurring in HPV-infected skin cell. UV radiation induces damage on DNA, which is normally repaired by the Nucleotide Excision Repair (NER) pathway. If NER fails and the DNA damaged is maintained, in the healthy skin cells (a) p53 tetramer is activated, leading to apoptosis and p21-mediated cell cycle block in G1 phase. When NER pathway fails in the skin cell infected by β-HPV (b), the presence of E6 interferes with the assembly of p53 monomer into tetramer, finally resulting in loss of apoptotic pathway activation and cell cycle progression.
Figure 1.
Best-characterized molecular mechanism involved in carcinogenesis occurring in HPV-infected skin cell. UV radiation induces damage on DNA, which is normally repaired by the Nucleotide Excision Repair (NER) pathway. If NER fails and the DNA damaged is maintained, in the healthy skin cells (a) p53 tetramer is activated, leading to apoptosis and p21-mediated cell cycle block in G1 phase. When NER pathway fails in the skin cell infected by β-HPV (b), the presence of E6 interferes with the assembly of p53 monomer into tetramer, finally resulting in loss of apoptotic pathway activation and cell cycle progression.
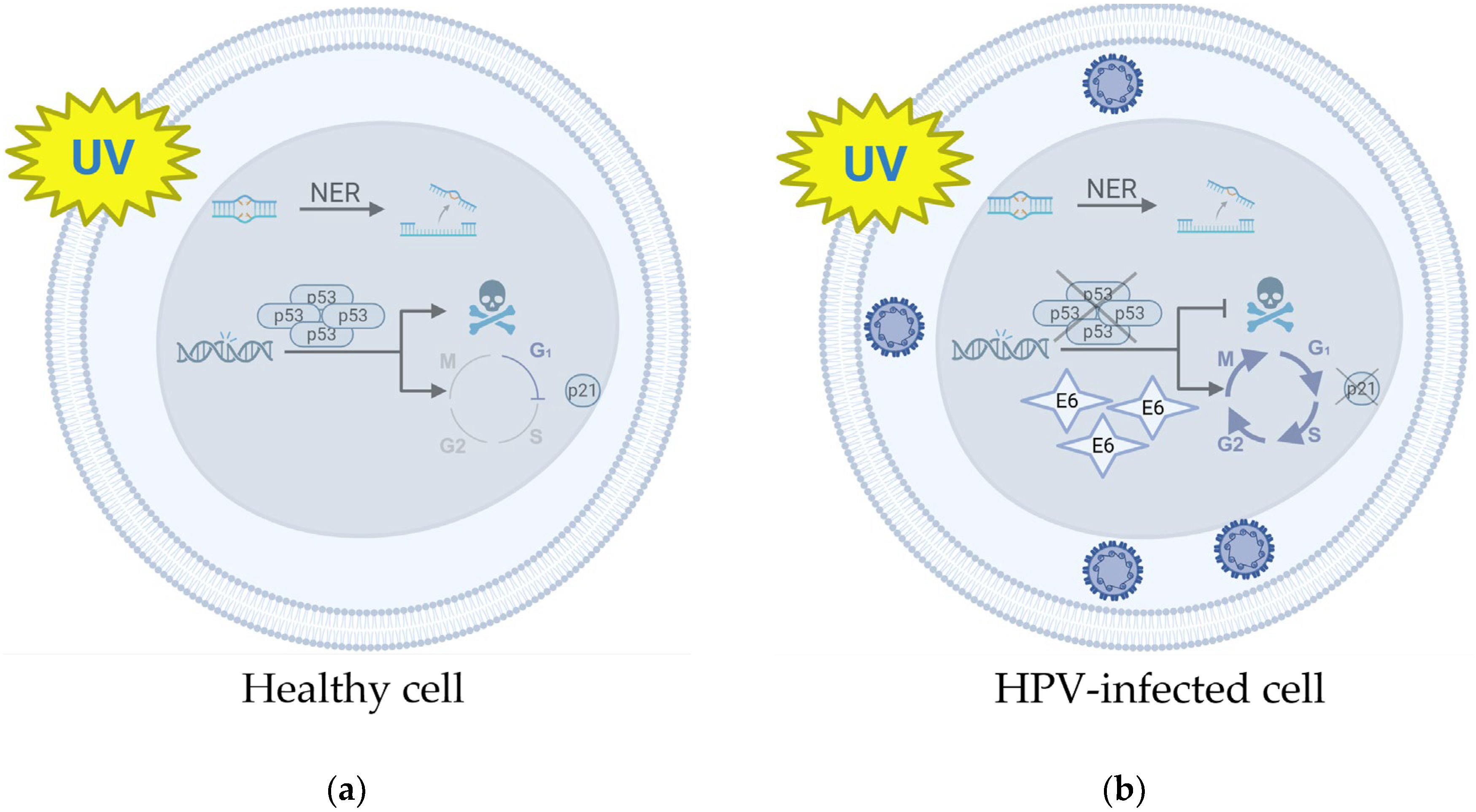
Figure 2.
Schematic representation of new promising vaccine candidates, containing the L2 polytope of the cutaneous HPV types, fused to the thioredoxin scaffold.
Figure 2.
Schematic representation of new promising vaccine candidates, containing the L2 polytope of the cutaneous HPV types, fused to the thioredoxin scaffold.
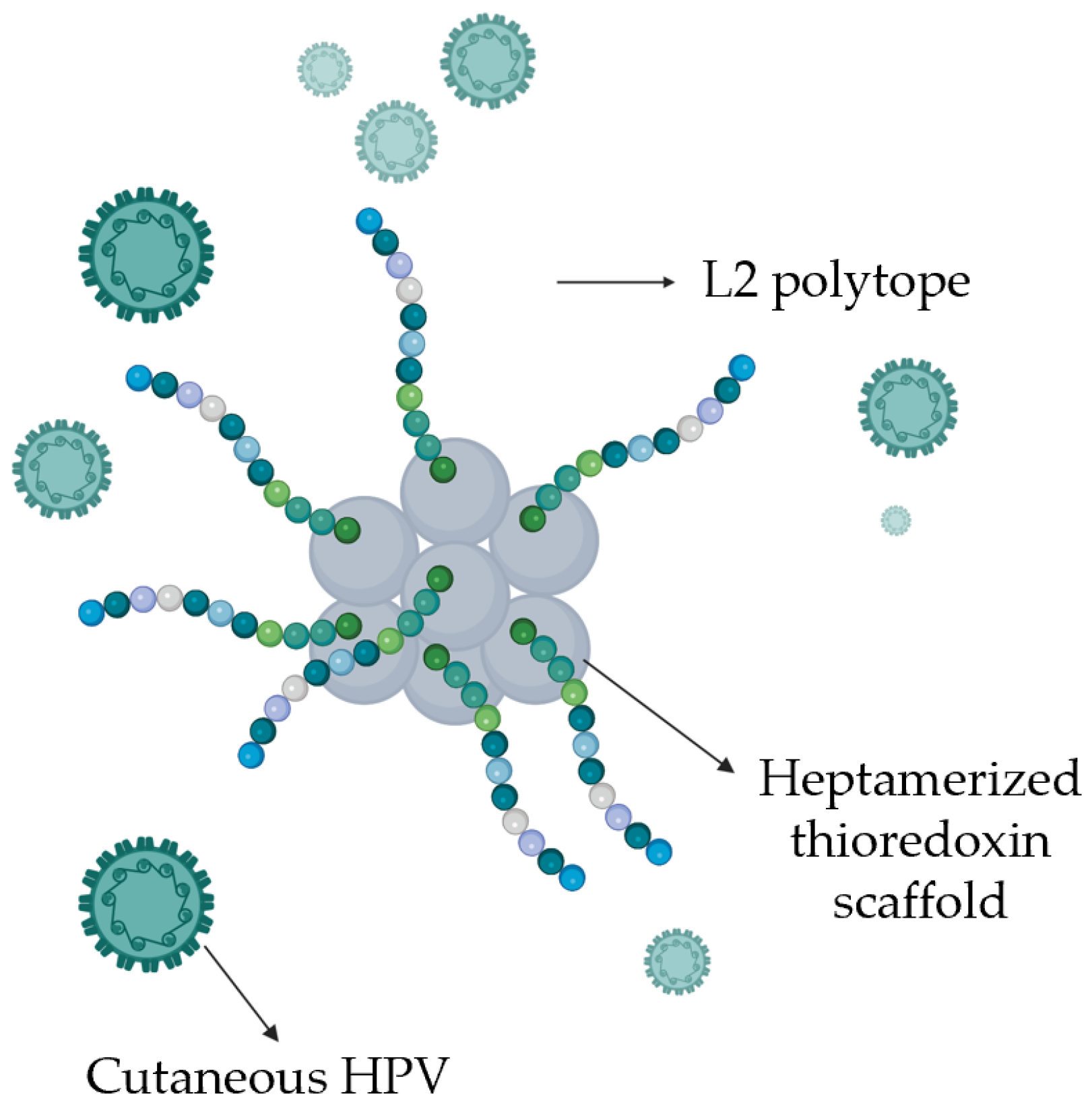

Table 1.
Summary of currently available therapeutic options for the treatment of KA.
| Therapy type | Description | Mechanism | Effectiveness | ||
|---|---|---|---|---|---|
 surgical |
Complete surgical removal | Surgical removal with histopathological control | Gold-standard, but 8% recurrence | ||
 physical |
Radiotherapy | Targeted destruction of lesions via | Energy | Effective, but rarely used | |
| Cryotherapy | Cold | Effective (~87%), but not widely studied | |||
| PDT1 | Locally activated drug | Limited available data | |||
| Argon laser | Laser | Effective for solitary KA2 | |||
 topical |
Local application of | 5-FU3 | Inhibition of DNA synthesis | Very effective, first-line treatment | |
| Imiquimod | Local immune response activation | Effective | |||
 systemic |
Retinoids | Control of proliferation, differentiation, and immune response | Valuable option for generalized eruptive KA2 | ||
| Erlotinib | EGFR4 inhibition | Still limited experience | |||
1 PDT: Photodynamic therapy. 2 KA: Keratoacanthoma. 3 5-FU: 5-fluorouracil. 4 EGFR:.Epidermal Growth Factor Receptor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



