Submitted:
27 August 2025
Posted:
28 August 2025
You are already at the latest version
Abstract
Intestinal microbiota dysbiosis represents a critical determinant of clinical outcomes in patients undergoing allogeneic hematopoietic stem cell transplantation (allo-HSCT), with distinct microbiota patterns serving as potential prognostic biomarkers and therapeutic targets. However, the exponential growth in microbiota research and analytical complexity have created significant interpretive challenges for clinicians. This review provides a synthesis of current literature examining microbiota fingerprints and their clinical implications. We analyzed key studies evaluating the clinical implications of intestinal microbiota fingerprints in allo-HSCT. Additionally, we examined current therapeutic strategies for microbiota modulation and approaches for translating research findings into clinical practice. We identified three major microbiota fingerprints: 1) decreased intestinal diversity, 2) reduced abundance of short-chain fatty acid-producing bacteria, and 3) Enterococcus domination. These fingerprints are associated with critical clinical outcomes including overall survival, graft-versus-host disease, transplant-related mortality, and infectious complications. While fecal microbiota transplantation and dietary interventions appear promising, current studies suffer from limited sample sizes and lack standardized protocols. Despite advances in microbiota research, biological, methodological, and logistical challenges continue to impede clinical translation. Understanding microbiota fingerprints represents a promising avenue for improving allo-HSCT outcomes. However, successful clinical implementation requires standardized methodologies, mechanistic studies, and multi-center collaborations to translate research into actionable clinical tools.
Keywords:
gastrointestinal microbiome
; microbiota
; stem cell transplantation
; mortality
; graft vs host disease
1. Introduction
Although allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a curative therapy for several malignant and non-malignant diseases, its effectiveness remains limited due to underlying disease or transplant related life-threatening complications [1,2,3,4,5,6]. These life-threatening complications include neutropenic fever, relapse and acute graft versus host disease (aGvHD) [1,2,3,4,5,6]. aGvHD is the leading cause of non-relapse mortality and can occur in up to 70% of patients [1,2,3,4]. Relapse remains the most significant cause of treatment failure, with studies reporting incidence rates of up to 40% [6,7]. Similarly, neutropenic fever is highly prevalent occurring in up to 80% of patients, especially prior to the engraftment period [5]. Thus, allo-HSCT still associated with considerable morbidity. During the allo-HSCT, the intestinal microbiota has emerged as a key player that can shape the development of these poor outcomes. Specific patterns of intestinal microbiota disruption – often referred to as “microbiota fingerprints” has been linked to these poor outcomes. Consequently, understanding these microbiota fingerprints is increasingly recognized as crucial for predicting outcomes and developing new therapeutic interventions in the transplantation context.
In recent years, there has been a significant increase in studies investigating the role of the intestinal microbiota in allo-HSCT. These studies consistently demonstrate the strong link between intestinal microbiota disruptions and poor clinical outcomes. Nevertheless, the growing volume of data and the complexity of microbiota analysis may pose significant barriers to a clear understanding of how these fingerprints may impact patients undergoing allo-HSCT. Furthermore, most microbiota studies are observational, mechanistically inconsistent and not easily translated into clinical practice. In this review, we aim to clarify this conundrum by summarizing key studies that have evaluated intestinal microbiota fingerprints and their clinical implications for patients undergoing allo-HSCT. After unrevealing this conundrum, we will also provide a critical overview of challenges and strategies to: 1) modulate the intestinal microbiota, and 2) facilitate the integration of intestinal microbiota research into clinical practice.
2. The Dynamics of Intestinal Microbiota Through the Patient Journey
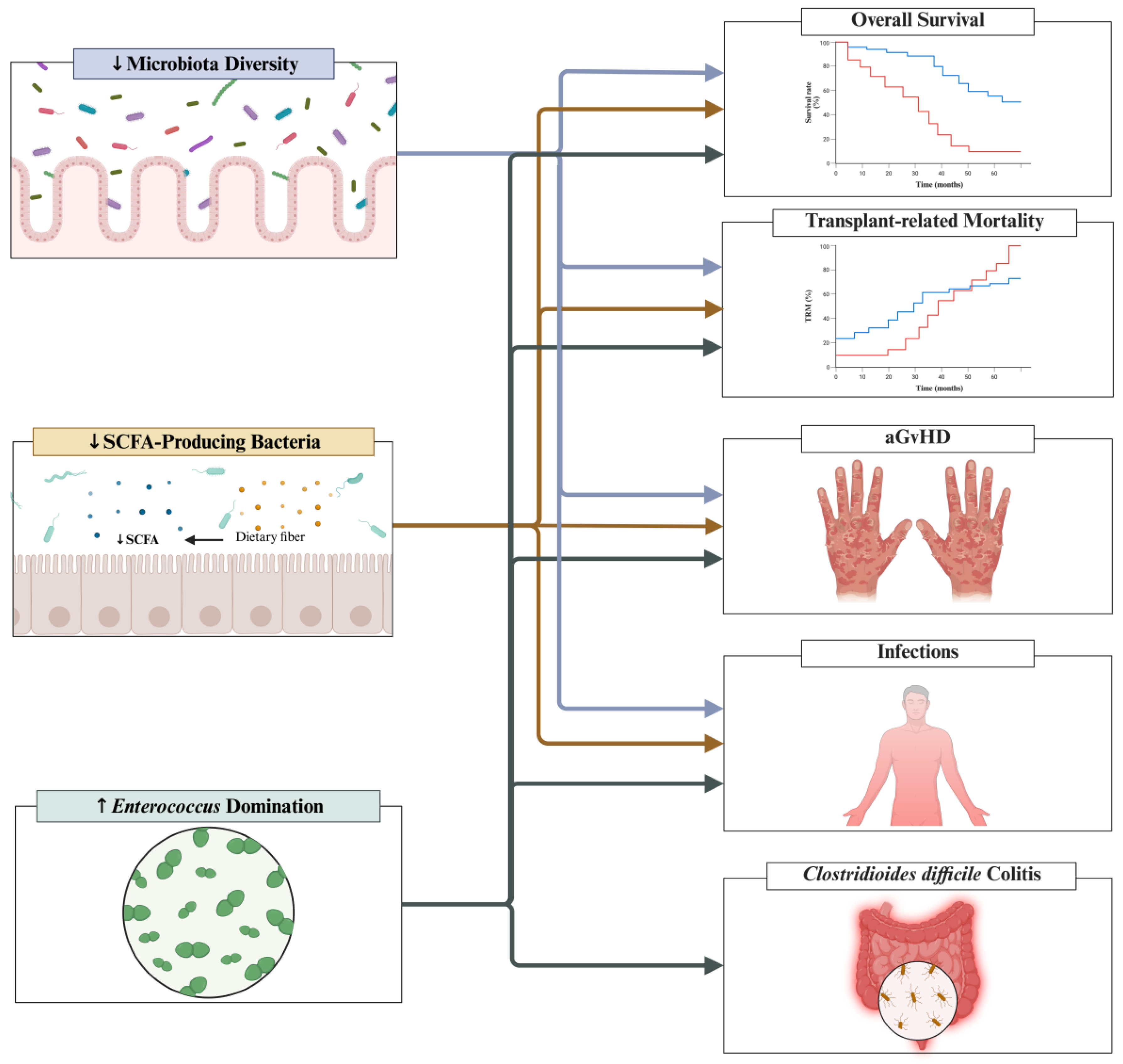
The patient journey until the allo-HSCT is marked by dynamic and progressive disruptions in the intestinal microbiota. The intestinal microbiota may starts to change to a disease-associated layout since the diagnosis of the underlying condition [8,9]. Several studies have demonstrated key features of intestinal dysbiosis even prior to the allo-HSCT [10,11,12,13,14,15]. As patients progress through the allo-HSCT, the intestinal microbiota undergoes further dysbiosis, which can be so severe that recovery may require a long time or may not be complete [11,13]. Overall, through the patient journey until completing the allo-HSCT procedure, key intestinal microbiota fingerprints may emerge. Most important intestinal microbiota fingerprints identified across studies are: 1) decreased intestinal diversity [12,13,16,17,18,19,20,21,22,23]; 2) decreased abundance of SCFA (short chain fatty acid)-producing bacteria [10,21,24,25,26]; and 3) Enterococcus domination (see Figure 1) [18,20,27,28,29,30]. These fingerprints may contribute to the development of several clinical outcomes, such as overall survival, transplantation-related mortality, aGvHD, infections and Clostridioides difficile colitis (see Figure 2). Given that these intestinal dysbiosis fingerprints have prognostic significance, understanding the factors driving it is critical to improve patients’ outcomes.
Key factors driving these intestinal dysbiosis fingerprints through the patient journey include chemotherapies, dietary changes and the use of broad-spectrum antibiotics [10,11,16,17,26,31,32,33,34,35]. The relationship between antibiotic exposure and intestinal dysbiosis was demonstrated in a study including 96 patients [16]. When compared to patients (n = 34) without antibiotics exposure, patients (n = 62) receiving any antibiotic in the 3 months prior to allo-HSCT had significantly lower alpha diversity (41.5 ± 26.54 vs. 61.26 ± 25.93; p = 0.001) [16]. Similar findings were also reported in a study including 57 patients undergoing allo-HSCT – prior antibiotic use was significantly associated with lower bacterial diversity (p = 0.003) [12]. In this study, other factors associated with intestinal dysbiosis were 1) severe underlying hematologic disease (p < 0.0001); 2) CMV (cytomegalovirus) seropositivity (p = 0.006), 3) gastrointestinal or hepatic comorbidities (p = 0.004), and 4) recent microbial infection (p = 0.006) [12]. The impact of different conditioning regimens on the intestinal microbiota has also been evaluated. For example, in a study involving 96 patients undergoing allo-HSCT, those who received myeloablative conditioning exhibited distinct shifts in microbiota composition compared to patients who received reduced-intensity regimens [16]. These findings suggest that several factors contribute to the development of intestinal dysbiosis during allo-HSCT. Nevertheless, whether these factors act individually or synergistically to drive these intestinal dysbiosis fingerprints desires future studies. With a better understanding of the potential drivers of these fingerprints, the following sections will explore the key moments at which these patterns emerge and their potential implications for clinical outcomes.
Figure 1.
The intestinal microbiota through the allo-HSCT journey. Allo-HSCT = allogeneic hematopoietic stem cell transplantation; SCFA = Short-chain fatty acid.
Figure 1.
The intestinal microbiota through the allo-HSCT journey. Allo-HSCT = allogeneic hematopoietic stem cell transplantation; SCFA = Short-chain fatty acid.
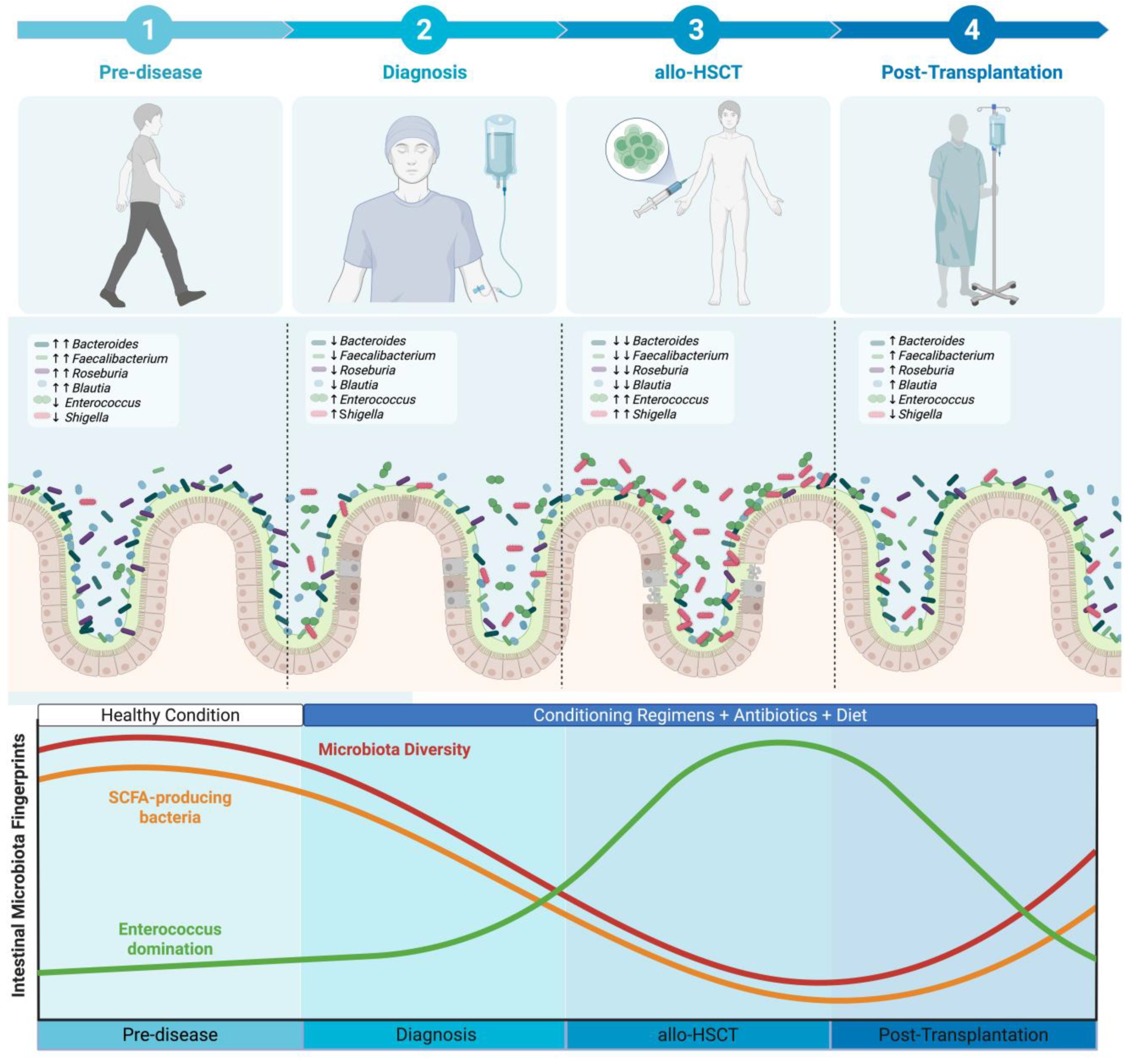
Figure 2.
Associations between intestinal microbiota fingerprints and clinical outcomes. aGvHD = acute graft versus host disease; SCFAs = Short-chain fatty acids.
Figure 2.
Associations between intestinal microbiota fingerprints and clinical outcomes. aGvHD = acute graft versus host disease; SCFAs = Short-chain fatty acids.
3. Intestinal Microbiota Fingerprints Prior to Allo-HSCT
In patients undergoing allo-HSCT, there is extensive evidence suggesting that the intestinal microbiota is disrupted even prior to the transplantation [10,11,12,13,14,15,36]. Prior to allo-HSCT, the most important intestinal dysbiosis fingerprint is decreased intestinal diversity [10,11,15,16,31,32,33,34,36]. Studies have also shown that patients already exhibit a distinct microbiota composition prior to undergoing allo-HSCT (see Supplementary Table 1) [10,11,15,16,31,32,33,34]. When compared to a control group (paired HLA-matched sibling donors), patients undergoing allo-HSCT (n = 57) had lower bacterial diversity (p = 0.0002) and different phylogenetic membership (p = 0.001) with increased relative abundances of facultative anaerobic bacteria (such as Enterococcaceae and Streptococcaceae) [12]. Furthermore, when compared to healthy volunteers, patients undergoing allo-HSCT had significantly lower abundance of butyrate-producing bacteria (a key microbiota metabolite that helps maintain a healthy gut), such as Anaerostipes (p = 0.036), Butyricimonas (p = 0.041), Coprococcus (p < 0.001), Faecalibacterium (p = 0.014), and Lachnospiraceae (p < 0.001) [10]. Similarly, in another study including fecal samples from 606 patients prior to allo-HSCT, the intestinal microbiota was significantly different than healthy adult volunteers and subjects from the Human Microbiome Project [13]. In this study, patients undergoing allo-HSCT had lower intestinal diversity (p < 0.001) and a distinct microbiota composition based on enterotype (p < 0.001) [13]. Taken together, these and other studies in the literature suggest that intestinal dysbiosis exist even prior to allo-HSCT [10,11,12,13,14,15]. Given that these intestinal dysbiosis fingerprints have prognostic significance, the next step is to clarify their implication for patient’s outcomes.
These early intestinal dysbiosis fingerprints are not only present but can significantly shape the course and prognosis of patients undergoing allo-HSCT. These early fingerprints can contribute to the following outcomes: 1) overall survival [12,13,16,17]; 2) transplantation-related mortality [13]; 3) aGvHD [16,17,35,37]; 4) and infections [16]. Among the aforementioned fingerprints, the most evaluated prior to allo-HSCT is the intestinal microbiota diversity – an index that measure the variety (richness) and balance (evenness) of bacteria living in the gastrointestinal tract (see Table 1). Across studies, a consistent finding is that decreased intestinal microbiota diversity prior to allo-HSCT is associated with poor outcomes, such as increased mortality and GvHD.[12,13,17,37] Among the available studies, the most robust in terms of statistical power and sample size was an international multi-center study involving 606 patients undergoing allo-HSCT. In this study, higher intestinal diversity prior to the transplant was associated with a 59% reduction in the risk of death (HR 0.41; 95% CI 0.24-0.71) and a 56% reduction in transplant-related mortality (HR 0.44; 95% CI 0.22=0.87) [13].

Table 1.
Implications of Intestinal Diversity Prior to allo-HSCT.
| Outcomes |
Author, year N |
Finding |
| Overall Survival[12,13,17] | Peled 2020[13] 606 |
↓Overall Mortality Higher alpha diversity prior to allo-HSCT was associated with a lower risk of mortality (HR 0.41; 95% CI 0.24-0.71) |
| Liu 2017[12] 57 |
↓Overall Mortality Patients with higher phylogenetic diversity had lower overall mortality rates (HR 0.37; 95% CI 0.18-0.77; p = 0.008) |
|
| Masetti 2023[17]β 90 |
↑Overall Survival Patients with higher intestinal diversity exhibited a higher probability of overall survival (88.9% ± 5.7% vs. 62.7% ± 8.2%; p = 0.011). |
|
| Transplantation-related mortality[13] | Peled 2020[13] 606 |
↓Transplant-related mortality Higher alpha diversity prior to allo-HSCT was associated with a lower risk of transplant-related mortality (HR 0.44; 95% CI 0.22-0.87). |
| aGvHD[17] | Masetti 2023[17]β 90 |
↓aGvHD The cumulative incidence of grade 2 to 4 aGvHD was significantly lower in the higher diversity group than in the lower diversity group (20.0% ± 6.0% [SE] vs 44.4% ± 7.4% [SE]; p = .017). The cumulative incidence of grade 3 to 4 aGvHD was significantly lower in the higher diversity group than in the lower diversity group (2.2% ± 2.2% [SE] vs 20.0% ± 6.0% [SE]; p = .007). |
| Biagi 2019[37] 36 |
The diversity between pre-HSCT samples were greater in individuals who developed intestinal GvHD (0.86 ± 0.15) than in individuals without GvHD (0.72 ± 0.15, p = 0.001) and individuals who developed less severe skin GvHD (0.77 ± 0.15, p = 0.02). |
Allo-HSCT = Allogeneic hematopoieitic stem cell transplantation; CI = Confidence interval; aGvHD = acute graft versus host disease; HR = Hazard ratio; N = number of patients included in this analysis; SE = Standard error; = decreased; = increased; = included only pediatric patients;.
The other fingerprint relates to specific bacterial compositions prior to allo-HSCT that are associated with either protection against or increased risk for poor outcomes (see Supplementary Table 2). For example, higher abundance of Blautia, which produce SCFA and promote gut homeostasis, was associated with lower risk of aGvHD development in two studies [17,37]. Given the prognostic significance of these intestinal dysbiosis fingerprints, future studies should evaluate strategies on how to incorporate them into risk stratification tools that can be used in clinical practice.
4. Intestinal Microbiota Fingerprints During Allo-HSCT
The available literature has demonstrated that during allo-HSCT, the already compromised intestinal microbiota undergoes further dysbiosis (see Figure 1) [16,17,18,19,20,21,22]. As the intestinal microbiota changes, all three key fingerprints emerge: 1) decreased intestinal diversity [16,17,18,19,20,21,22,23,38]; 2) decreased abundance of SCFA-producing bacteria [21,24]; and 3) intestinal domination by a single taxon [18,20,27,28,29,30]. In the following subsections, we will revise pivotal studies that have both described these fingerprints and examined their clinical implications.
4.1. Intestinal Diversity and Implications to Clinical Outcomes
During allo-HSCT, the intestinal diversity continues to decline and may not return to baseline levels [13,16,17,18,19,20,21,23,39]. In a previous allo-HSCT study including 96 patients, stools samples were collected at three timepoints: 1) baseline (prior to the conditioning regimen), 2) D+10, and 3) D+30 [16]. Compared to baseline, samples collected at both D+10 and D+30 showed a significant reduction in intestinal diversity (D+10: 4.65 ± 1.36 vs. 3.08 ± 1.77; p < 0.001; D+30: 4.65 ± 1.36 vs. 2.62 ± 1.62; p < 0.001) [16]. This study also identified a significant reduction in intestinal diversity in samples collected at D+30 when compared to D+10 samples (2.62 ± 1.62 vs. 3.08 ± 1.77; p = 0.020) [16]. Similar findings were also reported in a study involving 100 patients, which collected stool samples at four timepoints: 1) baseline (prior to the conditioning regimen), 2) around the day of stem cell infusion (D-4 to D0), 3) engraftment (D+4 to D+28), and 4) late post-HSCT (after D+28) [20]. This study showed a significant reduction in intestinal diversity when comparing baseline samples to those collected around the day of stem cell infusion (p < 0.05) and engraftment (p < 0.01) [20]. Although intestinal diversity significantly increased in late post-HSCT samples compared to those collected during engraftment (p < 0.05), it remained below baseline levels [20]. Taken together, these and other studies suggest that intestinal diversity reaches its lowest values within 30 days after the allo-HSCT and gradually increases thereafter; however, it often remains below baseline even in samples collected 100 days post-transplant (see Supplementary Table 3) [13,16,17,18,19,20,21,23,39]. Thus, future studies are needed to explore strategies to preserve and restore intestinal diversity over the allo-HSCT course.
Strategies to preserve and restore the intestinal diversity have become a priority as research has shown it to be a key prognostic factor in patients undergoing allo-HSCT [11,40,41]. In the literature, intestinal diversity during allo-HSCT has been linked to overall survival [13,19,20], aGvHD [16,22,24,36,42], and transplantation-related mortality (see Table 2) [19,20,36]. In most of the studies, lower intestinal diversity in samples collected at the engraftment period has been associated with these poor outcomes [13,16,19,20,24,36,42]. Furthermore, lower intestinal diversity at the time of aGvHD diagnosis has been linked with a severe disease phenotype (see Table 2 for details) [22].
Table 2.
Clinical Implications of Intestinal Diversity Over The allo-HSCT.
| Outcome |
Author, year N Sample Timing |
Finding |
| Overall Survival[13,19,20] | Peled 2020[13] 704 At engraftment |
↑Overall Survival Patients were categorized into low- vs. high- diversity groups based on the median value. High diversity at engraftment was associated with a significant improve in overall survival (HR 0.75; 95% CI 0.58-0.96). This association was also identified after multivariable adjustment for age, intensity of the conditioning regimen, graft source and HCT-CI (HR 0.71; 95% CI 0.55-0.92). When considered as a continuous variable, high intestinal diversity was also associated with improved overall survival in both univariate (HR 0.58; 95% CI 0.37-0.91) and multivariate (HR 0.50; 95% CI 0.31-0.80) analysis. |
| Taur 2014[19] 80 At engraftment |
↑Overall Survival Overall survival at 3 years was 36%, 60% and 67% for low, intermediate and high diversity groups (p = 0.19). Patients with low diversity (inverse Simpson <2) were 3 times more likely to die within the follow-up when compared to those with higher microbial diversity (HR 3.13, 95% CI 1.39-7.98; p=0.05; adjusted HR 2.56; 95% CI 1.03-7.23; p = 0.42). Low diversity showed a strong effect on mortality after multivariate adjustment for other clinical predictors (transplant related mortality: adjusted hazard ratio, 5.25; p = 0.014). |
|
| Gu 2022[20] 86 At engraftment |
↑Overall Survival Patients were categorized into low- vs. high- diversity groups based on the median Shannon Index value. When compared to patients with low diversity, patients with high diversity had significantly higher two-year overall survival (83.7% vs. 60.6%; p=0.026). After adjusting for disease risk, pretransplant comorbidity, and previous chemotherapy, low intestinal diversity was an independent predictor of all-cause death (HR 2.62; 95% CI 1.06-6.49; p = 0.038) in a multivariate analysis. |
|
| Transplantation-related mortality[19,20,36] | Taur 2014[19] 80 At engraftment |
↑Transplant-related mortality Transplant-related mortality was 9%, 23%, and 53% for high, intermediate and low diversity groups, respectively (p = 0.03). Patients with low diversity (inverse Simpson <2) were 7.5 times more likely to experience transplant-related mortality within the follow-up when compared to those with higher microbial diversity (HR 7.54; 95% CI 2.12-47.88; p=0.001; adjusted hazard ratio, 5.25; 95% CI 1.36-35.07; p = 0.014). |
| Gu 2022[20] 86 At engraftment |
↑Transplantation-related Mortality When compared to patients in the high diversity group, patients in the low-diversity group had higher estimated 2-year transplanted related mortality (20.0% vs. 4.7%; p = 0.04). After adjusting for pretransplant comorbidity, disease status at the time of allo-HSCT and previous chemotherapy, low intestinal diversity was an independent predictor of transplant-related mortality (HR 4.95; 95% CI 1.03-23.76; p = 0.046). |
|
| Galloway-Pena 2019[36] 44 At engraftment |
↓Transplantation-related Mortality The Shannon diversity index at the time of engraftment was significantly associated with TRM (coefficient = -1.44; p = 0.02) |
|
| aGvHD[16,19,22,24,36,42] | Jenq 2015[24] 64 D+12 |
↓GvHD-related mortality Increased intestinal diversity was associated with reduced GvHD-related mortality (p = 0.005). |
| Mancini 2017[16] 96 D+10 |
↑aGvHD Decreased intestinal diversity at D+10 was associated with increased risk of early onset aGvHD (OR 7.833; 95% CI 2.141-28.658; p = 0.038). |
|
| Taur 2014[19] 80 At engraftment |
↑GvHD-related mortality GvHD-related mortality was higher in patients with low diversity (p = 0.018). |
|
| Payen 2020[22] 70 At the onset of GvHD |
↑aGvHD severity Patients with severe aGvHD had significantly lower indexes of alpha diversity: Chao1 (p = 0.039) and Simpson (p = 0.013) |
|
| Golob 2017[42] 66 At engraftment Weekly samples from prior to allo-HSCT until D+100 |
↑aGvHD severity Patients with severe aGvHD had a significantly lower alpha diversity index compared to both the control group and patients without severe aGvHD (p < 0.05). This finding was statistically significant when analyzing all stool samples collected over the allo-HSCT and when analyzing only samples collected at the engraftment period. |
|
| Galloway-Pena 2019[36] 44 At engraftment |
The Shannon diversity index at the time of engraftment was significantly associated with the incidence of aGvHD (P = 0.02) | |
| Infections[19] | Taur 2014[19] 80 At engraftment |
↑Infection-related mortality Infection related mortality was higher in patients with low diversity (p = 0.018). |
Allo-HSCT = allogeneic hematopoietic stem cell transplantation; N = number of patients included in the analysis; aGvHD = acute graft versus host disease.
4.2. SCFA-Producting Bacteria and Implications to Clinical Outcomes
SCFAs are key microbiota metabolites involved in the mechanisms through which the intestinal microbiota may influence clinical outcomes following allo-HSCT [21,22,24,25,26,38,43,44,45,46]. SCFAs, which includes butyrate, propionate and acetate, play important roles in promoting gut homeostasis and regulating the immune system [38,43,44,45].
During allo-HSCT, there is extensive evidence demonstrating a decrease in SCFAs levels and SCFA-producing bacteria (see Figure 1) [21,24,25,38]. In a study with 42 patients undergoing allo-HSCT, fecal butyrate and propionate were measured at three timepoints: 1) Prior to allo-HSCT (baseline), 2) D+7, and 3) D+14 [21]. Compared to baseline, samples collected at D+7 and D+14 showed significantly decreased levels of both butyrate and propionate (p-values NR) [21]. In another study involving 201 patients, stool samples were collected longitudinally at seven timepoints: 1) Prior to allo-HSCT, 2) D0, 3) D+7, 4) D+14, 5) D+21, 6) D+30, and 7) D+90 [26]. This study demonstrated a strong and prolonged suppression of fecal butyrate levels, with significant reductions observed from prior to allo-HSCT to D0 (p = 0.01; r = 0.5) and between prior to allo-HSCT and D+7 (p = 0.003; r = 0.6) [26]. Similarly, in a study of 360 patients, SCFA-producing bacteria were assessed at the time of engraftment [25]. The majority of patients had either a low relative abundance (40.8%) or no detectable (40%) SCFA-producing bacteria, while only 19.2% had a high relative abundance [25]. These findings consistently outline a profound depletion of SCFA and their producers over the allo-HSCT journey, reinforcing their potential role in post-transplantation outcomes.
Indeed, previous studies have demonstrated that decreased levels of SCFAs and their producers contribute to poor allo-HSCT outcomes (see Table 3). Important clinical outcomes modulated by SCFA and their producers are: 1) Overall survival [24]; 2) GvHD [21,22,24,26,38]; 3) Transplantation-related mortality [26]; and 4) Viral lower respiratory tract infection [25]. For instance, in a study involving 360 patients, a high abundance of SCFA-producing bacteria at the engraftment period was independently associated with a fivefold decrease in the risk of viral lower respiratory tract infection (HR 0.22; 95% CI 0.04-0.69; p = 0.06) [25]. Furthermore, in a study of 64 allo-HSCT recipients, a higher abundance of Blautia (a key SCFA-producing genus), was independently associated with lower GvHD-related mortality (HR 0.18; 95% CI 0.05-0.63; p = 0.007) and reduced risk of refractory GvHD (HR 0.3; 95% CI 0.14-0.64; p = 0.002) [24]. These and other studies in the literature highlight the clinical relevance of preserving SCFA-producing bacteria over the allo-HSCT journey as a key strategy to improve patient outcomes.
Table 3.
Implications of SCFA-producing Bacteria and SCFA Levels Over allo-HSCT.
| Outcomes |
Author, year N Sample Timing |
Finding |
| Overall Survival[24] | Jenq 2015[24] 64 D+12 |
↑Overall Survival Increased Blautia abundance was strongly associated with improved overall survival (p < 0.001). |
|
Transplantation-related Mortality[26] |
Meedt, 2022[26] 201 aGvHD onset // D+30 |
↑Transplant-related Mortality Low BCoAT copy numbers at D+30/GvHD were significantly associated with increased risk of transplant related mortality (HR 4.459; 95% CI 1.1018-19.530; p = 0.047). |
| aGvHD[21,22,24,26,38] | Jenq 2015[24] 64 D+12 |
↓GvHD-related mortality By using a taxonomic discovery analysis, increase in the genus Blautia was significantly associated with reduced GvHD-related mortality (p = 0.01). By stratifying patients based on Blautia median abundance, patients with higher abundance had reduced GvHD-related mortality (p = 0.04). In a multivariable analysis, Blautia abundance remained associated with GvHD-related mortality (HR 0.18; 95% CI 0.05-0.63; p = 0.007). ↓Refractory GvHD Increased Blautia abundance was associated with reduced development of acute GvHD that required treatment with systemic corticosteroids or was steroid refractory (p = 0.01). In a multivariable analysis, Blautia abundance remained associated with refractory GvHD (HR 0.3; 95% CI 0.14-0.64; p = 0.002). ↓Liver GvHD Increased Blautia abundance was associated with reduced liver GvHD (p = 0.02). |
| Payen 2020[22] 70 aGvHD onset |
↓aGvHD severity When compared to controls (patients undergoing allo-HSCT without GvHD), patients with severe GvHD had a significant depletion of the Blautia coccoides group (p = 0.07). Similar findings were found when compared to patients with mild aGvHD (p = 0.036). ↓aGvHD severity When compared to controls (patients undergoing allo-HSCT without GvHD), patients with severe GvHD had a significant depletion of Anaerostipes (p = 0.015). ↓aGvHD severity When compared to controls (patients undergoing allo-HSCT without GvHD), patients with severe GvHD had a significant depletion of Faecalibacterium (p = 0.011). ↓aGvHD severity When compared to controls (patients undergoing allo-HSCT without GvHD), patients with severe GvHD had a significant depletion of Lachnoclostridium (p = 0.019). ↓GvHD severity When compared to controls (patients undergoing allo-HSCT without GvHD), patients with severe GvHD had significantly lower levels of total SCFAs (12.50 vs. 2.42; p = 0.0003), acetate (8.87 vs. 2.15; p = 0.002), butyrate (1.11 vs. 0.06; p = 0.001), and propionate (2.33 vs. 0.10; p = 0.0009). |
|
| Romick-Rosendale 2018[21] 42 D+14 |
↓GvHD When compared to patients that developed GvHD, patients without GvHD had significantly higher levels of butyrate (1.77 vs. 0.0550; p = 0.0142), propionate (6.63 vs. 0.208; p = 0.0108) and acetate (39.6 vs. 7.92; p = 0.047) at samples collected at D+14. |
|
| Meedt, 2022[26] 201 aGvHD onset // D+30 |
↑GI-GvHD severity Low BCoAT copy numbers at GvHD onset were correlated with GI-GvHD severity (p = 002; r = 0.3). ↑GI-GvHD Patients with GI-GvHD had lower BCoAT copy numbers than patients with other organs manifestations (0 copies vs. 3.16 x 106 copies; p = 0.006; r = 0.3). ↑GvHD-related Mortality Patients with low BCoAT copy numbers displayed significantly higher GvHD-associated mortality rate than those with high BCoAT concentrations (p = 0.04). |
|
| Artacho 2024[38] 70 Prior to allo-HSCT and Engraftment |
↑GvHD A significant decrease in acetate levels was detected in patients who developed GvHD (log2FC median = -2.36; p = 0.049). |
|
| Infections[25] | Haak 2018[25] 360 At engraftment |
↓LRTI The incidence of viral LRTI at 180 days was 17.3% and 16.1% for groups in which butyrate-producing bacteria were absent or low, respectively, and 3.2% for the high butyrate-producing group (p = 0.005). Patients with the highest abundance of butyrate-producing bacteria were independently associated with a fivefold decrease in risk of viral LRTI (HR 0.22; 95% CI 0.04-0.69; p = 0.06). |
Allo-HSCT = allogeneic hematopoietic stem cell transplantation; BCoAT = Butyryl-CoA:Acetate CoA-Transferase Gene Copy; CI = Confidence interval; D = day; LRTI = Lower respiratory tract infection; GvHD = graft versus host disease; SCFA = Short chain fatty acid; HR = Hazard ratio; N = number of patients included in the analysis.
4.3. Intestinal Domination and Implications to Clinical Outcomes
In patients undergoing allo-HSCT, another important microbiota fingerprint is the expansion of a single microbiota genus leading to intestinal domination. Intestinal domination is a frequent fingerprint that can occur in 28 to 65% of patients undergoing allo-HSCT [13,18,20,27,28,29,30,47]. Although intestinal domination is a prevalent fingerprint, the specific genus driving these events may vary across studies (see Supplementary Table 5). For example, in a multi-center study including 1,325 patients undergoing allo-HSCT, Enterococcus domination occurred in 65% of patients and was the most common genus to dominate the microbiota [28]. Similarly, Enteroccocus was also the most common genus to dominate the microbiota in an allo-HSCT study including 94 patients [30]. Nevertheless, in a study including 98 patients undergoing allo-HSCT, Streptococcus was identified as the most common genus associated with domination events, occurring in 42% of patients [18]. In this study, other genera responsible for intestinal domination during allo-HSCT in increasing order were: 1) Akkermansia (28%), 2) Blautia (28%), 3) Lactobacillus (28%), 4) Enterococcus (36%), and Bacteroides (38%) [18]. Overall, these findings suggest that while the dominant genus may vary across cohorts, Enterococcus consistently emerge as a key driver of intestinal domination events [13,18,20,27,28,29,30,47].
Enterococcus is not only a key driver of intestinal domination, but it is also the one most likely associated with poor outcomes. Indeed, while previous studies have linked Enterococcus domination with poor outcomes, domination by other genera does not appear to carry the same prognostic significance (see Table 4) [13,18,20,27,28,29,30,47]. For instance, in a study with 98 patients undergoing allo-HSCT, Enterococcus domination was associated with the following outcomes: bloodstream infection (63% vs. 35%; p = 0.01), Clostridioides difficile colitis (34% vs. 16%; p = 0.04), overall survival (p = 0.01), and treatment-related mortality (p = 0.02) [18]. In this same study, however, overall survival was not impacted by domination for the following genera: Bacteroides (p = 0.08), Akkermansia (p = 0.14), Blautia (p-value NR), 4) Lactobacillus (p = 0.52), and 5) Streptococcus (p = 0.70) [18]. Other studies have also highlighted the implications of Enterococcus domination. In an allo-HSCT study including 1,325 patients, Enterococcus domination was an independent risk factor for decreased overall survival (HR 2.06; 95% CI 1.50-2.82; p < 0.0001) [28]. Enterococcus domination was also associated with a nine-fold increase in the risk of bloodstream infections (HR 9.35; 95% CI 2.43-45.44; p = 0.001) in a study including 94 patients [30]. These studies suggest that Enterococcus domination is a key fingerprint with prognostic significance over the allo-HSCT. Therefore, future studies should explore strategies to modulate Enterococcus domination.
Table 4.
Implications of Intestinal Domination to Clinical Outcomes.
| Outcomes |
Autor, year N Sample Timing |
Implication |
| Overall Survival[18,28] | Messina 2024[18] 98 Stools were collected once prior to HSCT, weekly until D+30 and then at days D+45, D+90 and D+180 |
↓Overall survival Patients with Enterococcus domination had decreased overall survival (p = 0.01). Overall survival Bacteroides domination at any time point was not significantly associated with overall survival (p = 0.08). Akkermansia domination at any time point was not significantly associated with overall survival (p = 0.14). Blautia domination at any time point was not significantly associated with overall survival (p value NR). Lactobacillus domination was not significantly associated with overall survival (p = 0.52). Streptococcus domination was not significantly associated with overall survival (p = 0.70). |
| Stein-Thoeringer 2019[28] 1325 Samples were collected in the early post-transplant period (D0 to D+21) |
↓Overall survival Patients with Enterococcus domination in the early-post transplant period had significantly reduced overall survival in univariate analysis (HR 1.97; 95% CI 1.45 – 2.66; p < 0.001). This finding remained significant in a multivariate analysis adjusted for graft source, age, conditioning intensity, gender and underlying disease (HR 2.06; 95% CI 1.50-2.82; p < 0.0001). |
|
| Transplantation-related Mortality[18] | Messina 2024[18] 98 Stools were collected once prior to HSCT, weekly until D+30 and then at days D+45, D+90 and D+180 |
↑Treatment-related mortality Patients with Enterococcus domination had increased treatment-related mortality (p = 0.02). |
| aGvHD[28] | Stein-Thoeringer 2019[28] 1325 Samples were collected in the early post-transplant period (D0 to D+21) |
↑GvHD-related mortality Patients with Enterococcus domination in the early-post transplant period had significantly increased GvHD-related mortality in univariate analysis (HR 2.04; 95% CI 1.18-3.52; p = 0.05). This finding remaining significant in a multivariate analysis adjusted for graft source, age, conditioning intensity, gender and underlying disease (HR 2.60; 95% CI 1.46-4.62; p < 0.01). ↑GvHD severity (grade 2-4) Patients with Enterococcus domination in the early-post transplant period had significantly increased GvHD severity (grade 2-4) in univariate analysis (HR 1.44; 95% CI 1.10-1.88; p < 0.01). This finding remaining significant in a multivariate analysis adjusted for graft source, age, conditioning intensity, gender and underlying disease (HR 1.32; 95% CI 1.00-1.75; p < 0.05). |
| Infections[18,30] | Messina 2024[18] 98 Stools were collected once prior to HSCT, weekly until D+30 and then at days D+45, D+90 and D+180 |
↑BSI Patients with Enterococcus domination at any time point had increased risk for BSI (63% vs. 35%; p = 0.01). |
| Taur 2012[30] 94 Prior to allo-HSCT After allo-HSCT (until D+35) |
↑BSI Patients with Enterococcus domination had a 9-fold increased risk of VRE bacteremia (HR 9.35; 95% CI 2.43-45.44; p = 0.001). |
|
| Taur 2012[30] 94 Prior to allo-HSCT After allo-HSCT (until D+35) |
↑BSI Patients with Proteobacteria domination had a 5-fold increased risk of gram-negative bacteremia (HR 5.46; 95% CI 1.03-19.91; p = 0.047). |
|
| Clostridioides difficile colitis[18] | Messina 2024[18] 98 Stools were collected once prior to HSCT, weekly until D+30 and then at days D+45, D+90 and D+180 |
↑Clostridioides difficile colitis Patients with Enterococcus domination at any time point had increased risk for BSI (34% vs. 16%; p = 0.04). |
| Other[18] | Messina 2024[18] 98 Stools were collected once prior to HSCT, weekly until D+30 and then at days D+45, D+90 and D+180 |
↑Relapse-related mortality Patients with Enterococcus domination had increased relapse-related mortality (p = 0.08). |
Allo-HSCT = allogeneic hematopoietic stem cell transplantation; BSI = Bloodstream infection; CI = Confidence interval; D = day; GvHD = graft versus host disease; N = Number of patients included in this analysis; HR = Hazard ratio.
5. Strategies to Modulate the Intestinal Microbiota During Allo-HSCT
Given the prognostic significance of microbiota fingerprints, several studies have explored strategies to modulate the intestinal microbiota during allo-HSCT [28,48,49]. Overall, two major strategies have been investigated: 1) fecal microbiota transplantation (FMT), and 2) dietary interventions [28,48,49,50,51,52]. These are promising strategies because they can modulate the complex relationship between microbiota and immune system throughout mechanisms that control alloreactivity without further compromising the immune system [53]. These strategies have not only demonstrated the ability to restore microbiota diversity and key microbiota metrics, but have also been associated with better clinical outcomes during allo-HSCT [33,48].
FMT is a procedure in which stool from healthy donors (allogeneic FMT) or from the patient prior to dysbiosis (autologous FMT) is administered to restore intestinal microbiota balance [33,48]. In the allo-HSCT setting, FMT is an emerging therapy that has been shown to be feasible [48,53]. However, given the compromised immune system in patients undergoing allo-HSCT, safety concerns remain an important issue [54]. Despite these concerns, studies are showing that severe adverse events, especially infections, are rare in the allo-HSCT setting [54]. Therefore, FMT has been used both as a prophylactic and therapeutic intervention for patients undergoing allo-HSCT[11,48].
Clinical outcomes that have been improved by FMT include: 1) GvHD [53,55], 2) Drug-resistant bacteria colonization [55,56,57,58], 3) BSI [58], mortality [57], and 4) Clostridioides difficile collitis [59,60,61]. For instance, in a study involving 15 patients with steroid-refractory or steroid-dependent GvHD that received allogeneic FMT, 66.7% achieved a complete clinical response (resolution of GvHD symptoms) within one month after treatment [53]. Furthermore, patients who responded to the FMT exhibited a significant increase in both intestinal diversity and the abundance of SCFA-producing bacteria [53]. Another study examined 19 patients colonized with multidrug-resistant organisms, of whom 8 received FMT [62]. Compared to those who did not receive FMT, patients treated with FMT demonstrated significantly higher 12-month overall survival (70% vs. 36%; p = 0044) and required fewer intensive care admission (0% vs. 46%; p = 0.045) [62]. Although these studies show promising data, significant challenges remain before FMT can become a standardized treatment in the allo-HSCT setting [54,63]. The available literature demonstrate heterogeneity in FMT approaches, including differences in manufacturing process, route of administration, timing, dosing strategies and donor selection. Thus, while these preliminary data are encouraging, further large randomized clinical trials with standardized methodologies are warranted.
Dietary interventions represent another promising therapeutic strategy, encompassing 1) Prebiotics, 2) Probiotics, 3) Symbiotics, and 4) Route of nutritional support [28,51,52,64,65,66,67]. These dietary interventions have been mostly associated with improvement in the following allo-HSCT clinical outcomes: 1) GvHD [28,50,51,52], 2) Diarrhea [66], 3) Mortality [52,64,66], and 4) Mucositis [66]. In a pilot randomized clinical trial including 40 patients, 20 patients received daily symbiotics (seven bacterial strains + fructo-oligosaccharides) [51]. When compared to the control group, patients receiving symbiotics had lower rates of severe GvHD (0% vs. 25%; p = 0.047) [51]. Similarly, in another study including 44 patients, 22 patients received GFO (combination of glutamine, fiber and oligosaccharides) [66]. Patients receiving GFO had a statistically significant reduction in diarrhea duration (3.73 vs. 7.68 days; p < 0.0001) and mucositis duration (3.86 vs. 6.00 days; p < 0.0330). GFO administration was also associated with higher survival rate 100 days after allo-HSCT (100% vs. 77.3%; p = 0.0091). Nevertheless, it is important to note that most available studies are observational with small sample sizes. Furthermore, studies demonstrate significant heterogeneity across multiple parameters, including substance dosage, administration timing and routes, and strain selection. Therefore, future research employing larger sample sizes and standardized methodologies is warranted to strengthen the evidence base.
6. Challenges in Translating Intestinal Microbiota Research into Allo-HSCT Clinical Practice
Although significant advances have been made in elucidating the role of intestinal microbiota in the allo-HSCT context, microbiota research remains distant from clinical implementation [68,69]. This loss of translation between microbiota research and allo-HSCT clinical practice stems from several factors, including biological, methodological and logistical challenges [68,69].
The biological challenges are fundamentally rooted in the paucity of evidence supporting mechanistic hypotheses that causally link intestinal microbiota alterations to allo-HSCT outcomes [68,69]. Most available literature remains associative and, thus, it remains unclear whether intestinal microbiota changes represent a cause or consequence of clinical outcomes throughout the allo-HSCT process [68]. For instance, the presence of the aforementioned fingerprints could be the consequence of several allo-HSCT variables, such as severe underlying disease, multiple hospitalization, infectious complications and antibiotic use. Methodological challenges arise primarily from the substantial inter-study variability regarding protocols for intestinal microbiota analysis. Studies exhibit substantial variability across multiple parameters, including sample collection techniques, collection timing, DNA sequencing methodologies and bioinformatics pipelines [68]. Furthermore, the effects of confounding variables that may influence the intestinal microbiota are not consistently accounted for, such as dietary patterns, environmental factors and concurrent medications [68]. Additionally, while microbiota research endorses personalized therapeutic strategies, the logistical challenges associated with implementing microbiota profiling and patient-tailored treatment protocols present substantial barriers to clinical translation [68]. Finally, microbiota studies are often single-center studies that include small to modest cohorts, which hamper the generalizability of the findings [68]. These challenges, when coupled with the inherent complexity of microbiome analyses, prevents most clinicians from integrating microbiota research into allo-HSCT clinical practice [68].
To overcome the aforementioned challenges, a multifaceted strategy involving coordinated actions and stakeholders is required [68]. The most critical intervention may be the standardization of microbiota research, which is currently advancing through initiatives such as the STORMS checklist (“Strengthening The Organization and Reporting of Microbiome Studies”), FDA (Food and Drug Administration) oversight and consensus guidelines [63,69,70]. This standardization should ideally encompass all phases of microbiota research, spanning from initial test indication to the reporting and clinical interpretation of microbiota findings [69]. Additionally, interventional studies should comply with FDA regulations when assessing the efficacy and safety of fecal microbiota transplantation products [63]. Equally important is addressing logistical challenges and designing microbiota studies that answer relevant clinical questions and provide outputs applicable to clinical practice [68,69]. To this end, studies should conduct rigorous sample size estimation to enhance reliability and generalizability [68,69]. Additionally, researchers should prioritize clinical outcomes with direct relevance to clinical practice [68]. Furthermore, researchers should aim to translate complex microbiota findings into accessible clinical tools that assist physicians with patient stratification and prognosis. Finally, fostering communication between microbiota scientists and the medical community through targeted educational initiatives and translational grant opportunities will equip physicians with the requisite knowledge to integrate microbiota research into clinical practice [68].
7. Conclusions and Future Directions
This review identified three key intestinal microbiota fingerprints associated with allo-HSCT outcomes: decreased intestinal diversity, reduced abundance of SCFA-producing bacteria, and Enterococcus domination. Although intestinal microbiota represents a key prognostic factor and therapeutic target in patients undergoing allo-HSCT, further translation of this knowledge into clinical practice is needed. Future large-scale clinical studies with standardized microbiota methodologies and mechanistic evaluation should be designed in collaboration with key stakeholders, including physicians, microbiome scientists, and patients. Such collaborative approaches will enhance study reliability, generalizability, and assessment of outcomes directly relevant to clinical practice.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Table S1: Key Studies Evaluating the Intestinal Microbiota Prior to allo-HSCT; Table S2: Implications of Intestinal Microbiota Fingerprints Prior to Allo-HSCT; Table S3. Key Studies Evaluating the Dynamics of Intestinal Diversity Over the Allo-HSCT; Table S4. Key Studies Evaluating the Dynamics of SCFA-producing Bacteria and SCFA Levels Over the Allo-HSCT. Table S5. Dynamics of Intestinal Domination Over Allo-HSCT.
Author Contributions
All authors contributed significantly to the development of this study and manuscript. GLVO and ASFJ conceived the study. ASFJ developed the review protocol with input from other authors. GLVO and ASFJ gathered funding for this project. GLVO and ASFJ contributed to project administration. All authors contributed to data interpretation. ASFJ and BFRS wrote the first full manuscript draft. All authors contributed to the manuscript and critically reviewed it for important intellectual content. All authors approved the final version to be published.
Funding
This research was funded by the São Paulo Research Foundation (FAPESP), process numbers #2022/12989-6 (Research grant for GLVO); #2023/08142-0 (Fellowship for ASFJ), and by the Brazilian National Council for Scientific and Technological Development (CNPq), process number #313190/2021-6 (Fellowship for GLVO), and by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. The content in this manuscript is solely the responsibility of the authors and does not in any way represent the official views of the funders.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
Not Applicable.
Acknowledgments
During the preparation of this manuscript, the author(s) used ChatGPT solely for grammatical corrections. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Allo-HSCT | Allogeneic hematopoietic stem cell transplantation |
| BSI | Bloodstream infection |
| CI | Confidence interval |
| D | Day |
| FDA | Food and Drug Administration |
| FMT | Fecal microbiota transplantation |
| LRTI | Lower respiratory tract infection |
| SCFA | Short-chain fatty acid |
| SE | Standard error |
| STORMS | Strengthening The Organization and Reporting of Microbiome Studies |
| GvHD | Graft versus host disease |
| GFO | Glutamine, fiber and oligosaccharides |
| HR | Hazard Ratio |
| TRM | Transplantation-related mortality |
References
- Hill, G.R.; Betts, B.C.; Tkachev, V.; Kean, L.S.; Blazar, B.R. Current Concepts and Advances in Graft-Versus-Host Disease Immunology. Annu. Rev. Immunol. 2021, 39, 19–49. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, J.L.; Levine, J.E.; Reddy, P.; Holler, E. Graft-versus-Host Disease. The Lancet 2009, 373, 1550–1561. [Google Scholar] [CrossRef] [PubMed]
- Jagasia, M.; Arora, M.; Flowers, M.E.D.; Chao, N.J.; McCarthy, P.L.; Cutler, C.S.; Urbano-Ispizua, A.; Pavletic, S.Z.; Haagenson, M.D.; Zhang, M.-J.; et al. Risk Factors for Acute GVHD and Survival after Hematopoietic Cell Transplantation. Blood 2012, 119, 296–307. [Google Scholar] [CrossRef]
- Ilett, E.E.; Jørgensen, M.; Noguera-Julian, M.; Nørgaard, J.C.; Daugaard, G.; Helleberg, M.; Paredes, R.; Murray, D.D.; Lundgren, J.; MacPherson, C.; et al. Associations of the Gut Microbiome and Clinical Factors with Acute GVHD in Allogeneic HSCT Recipients. Blood Advances 2020, 4, 5797–5809. [Google Scholar] [CrossRef]
- Nesher, L.; Rolston, K.V.I. Febrile Neutropenia in Transplant Recipients. In Principles and Practice of Transplant Infectious Diseases; Safdar, A., Ed.; Springer New York: New York, NY, 2019; ISBN 978-1-4939-9032-0. [Google Scholar]
- Barrett, A.J.; Battiwalla, M. Relapse after Allogeneic Stem Cell Transplantation. Expert Review of Hematology 2010, 3, 429–441. [Google Scholar] [CrossRef]
- Horowitz, M.; Schreiber, H.; Elder, A.; Heidenreich, O.; Vormoor, J.; Toffalori, C.; Vago, L.; Kröger, N. Epidemiology and Biology of Relapse after Stem Cell Transplantation. Bone Marrow Transplant 2018, 53, 1379–1389. [Google Scholar] [CrossRef]
- Rashidi, A.; Kaiser, T.; Shields-Cutler, R.; Graiziger, C.; Holtan, S.G.; Rehman, T.U.; Wasko, J.; Weisdorf, D.J.; Dunny, G.; Khoruts, A.; et al. Dysbiosis Patterns during Re-Induction/Salvage versus Induction Chemotherapy for Acute Leukemia. Sci Rep 2019, 9, 6083. [Google Scholar] [CrossRef]
- Galloway-Peña, J.R.; Smith, D.P.; Sahasrabhojane, P.; Ajami, N.J.; Wadsworth, W.D.; Daver, N.G.; Chemaly, R.F.; Marsh, L.; Ghantoji, S.S.; Pemmaraju, N.; et al. The Role of the Gastrointestinal Microbiome in Infectious Complications during Induction Chemotherapy for Acute Myeloid Leukemia. Cancer 2016, 122, 2186–2196. [Google Scholar] [CrossRef]
- Kusakabe, S.; Fukushima, K.; Maeda, T.; Motooka, D.; Nakamura, S.; Fujita, J.; Yokota, T.; Shibayama, H.; Oritani, K.; Kanakura, Y. Pre- and Post-serial Metagenomic Analysis of Gut Microbiota as a Prognostic Factor in Patients Undergoing Haematopoietic Stem Cell Transplantation. Br J Haematol 2020, 188, 438–449. [Google Scholar] [CrossRef]
- Henig, I.; Yehudai-Ofir, D.; Zuckerman, T. The Clinical Role of the Gut Microbiome and Fecal Microbiota Transplantation in Allogeneic Stem Cell Transplantation. haematol 2020. [Google Scholar] [CrossRef]
- Liu, C.; Frank, D.N.; Horch, M.; Chau, S.; Ir, D.; Horch, E.A.; Tretina, K.; Van Besien, K.; Lozupone, C.A.; Nguyen, V.H. Associations between Acute Gastrointestinal GvHD and the Baseline Gut Microbiota of Allogeneic Hematopoietic Stem Cell Transplant Recipients and Donors. Bone Marrow Transplant 2017, 52, 1643–1650. [Google Scholar] [CrossRef]
- Peled, J.U.; Gomes, A.L.C.; Devlin, S.M.; Littmann, E.R.; Taur, Y.; Sung, A.D.; Weber, D.; Hashimoto, D.; Slingerland, A.E.; Slingerland, J.B.; et al. Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation. N Engl J Med 2020, 382, 822–834. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, C.; Zhang, A. Gut Microbiota in Acute Leukemia: Current Evidence and Future Directions. Front. Microbiol. 2022, 13, 1045497. [Google Scholar] [CrossRef] [PubMed]
- Holler, E.; Butzhammer, P.; Schmid, K.; Hundsrucker, C.; Koestler, J.; Peter, K.; Zhu, W.; Sporrer, D.; Hehlgans, T.; Kreutz, M.; et al. Metagenomic Analysis of the Stool Microbiome in Patients Receiving Allogeneic Stem Cell Transplantation: Loss of Diversity Is Associated with Use of Systemic Antibiotics and More Pronounced in Gastrointestinal Graft-versus-Host Disease. Biology of Blood and Marrow Transplantation 2014, 20, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Mancini, N.; Greco, R.; Pasciuta, R.; Barbanti, M.C.; Pini, G.; Morrow, O.B.; Morelli, M.; Vago, L.; Clementi, N.; Giglio, F.; et al. Enteric Microbiome Markers as Early Predictors of Clinical Outcome in Allogeneic Hematopoietic Stem Cell Transplant: Results of a Prospective Study in Adult Patients. Open Forum Infectious Diseases 2017, 4, ofx215. [Google Scholar] [CrossRef] [PubMed]
- Masetti, R.; Leardini, D.; Muratore, E.; Fabbrini, M.; D’Amico, F.; Zama, D.; Baccelli, F.; Gottardi, F.; Belotti, T.; Ussowicz, M.; et al. Gut Microbiota Diversity before Allogeneic Hematopoietic Stem Cell Transplantation as a Predictor of Mortality in Children. Blood 2023, 142, 1387–1398. [Google Scholar] [CrossRef]
- Messina, J.A.; Tan, C.Y.; Ren, Y.; Hill, L.; Bush, A.; Lew, M.; Andermann, T.; Peled, J.U.; Gomes, A.; Van Den Brink, M.R.M.; et al. Enterococcus Intestinal Domination Is Associated With Increased Mortality in the Acute Leukemia Chemotherapy Population. Clinical Infectious Diseases 2024, 78, 414–422. [Google Scholar] [CrossRef]
- Taur, Y.; Jenq, R.R.; Perales, M.-A.; Littmann, E.R.; Morjaria, S.; Ling, L.; No, D.; Gobourne, A.; Viale, A.; Dahi, P.B.; et al. The Effects of Intestinal Tract Bacterial Diversity on Mortality Following Allogeneic Hematopoietic Stem Cell Transplantation. Blood 2014, 124, 1174–1182. [Google Scholar] [CrossRef]
- Gu, Z.; Xiong, Q.; Wang, L.; Wang, L.; Li, F.; Hou, C.; Dou, L.; Zhu, B.; Liu, D. The Impact of Intestinal Microbiota in Antithymocyte Globulin–Based Myeloablative Allogeneic Hematopoietic Cell Transplantation. Cancer 2022, 128, 1402–1410. [Google Scholar] [CrossRef]
- Romick-Rosendale, L.E.; Haslam, D.B.; Lane, A.; Denson, L.; Lake, K.; Wilkey, A.; Watanabe, M.; Bauer, S.; Litts, B.; Luebbering, N.; et al. Antibiotic Exposure and Reduced Short Chain Fatty Acid Production after Hematopoietic Stem Cell Transplant. Biology of Blood and Marrow Transplantation 2018, 24, 2418–2424. [Google Scholar] [CrossRef]
- Payen, M.; Nicolis, I.; Robin, M.; Michonneau, D.; Delannoye, J.; Mayeur, C.; Kapel, N.; Berçot, B.; Butel, M.-J.; Le Goff, J.; et al. Functional and Phylogenetic Alterations in Gut Microbiome Are Linked to Graft-versus-Host Disease Severity. Blood Advances 2020, 4, 1824–1832. [Google Scholar] [CrossRef]
- Sardzikova, S.; Andrijkova, K.; Svec, P.; Beke, G.; Klucar, L.; Minarik, G.; Bielik, V.; Kolenova, A.; Soltys, K. Gut Diversity and the Resistome as Biomarkers of Febrile Neutropenia Outcome in Paediatric Oncology Patients Undergoing Hematopoietic Stem Cell Transplantation. Sci Rep 2024, 14, 5504. [Google Scholar] [CrossRef] [PubMed]
- Jenq, R.R.; Taur, Y.; Devlin, S.M.; Ponce, D.M.; Goldberg, J.D.; Ahr, K.F.; Littmann, E.R.; Ling, L.; Gobourne, A.C.; Miller, L.C.; et al. Intestinal Blautia Is Associated with Reduced Death from Graft-versus-Host Disease. Biology of Blood and Marrow Transplantation 2015, 21, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Haak, B.W.; Littmann, E.R.; Chaubard, J.-L.; Pickard, A.J.; Fontana, E.; Adhi, F.; Gyaltshen, Y.; Ling, L.; Morjaria, S.M.; Peled, J.U.; et al. Impact of Gut Colonization with Butyrate Producing Microbiota on Respiratory Viral Infection Following Allo-HCT. Blood 2018, blood-2018-01-828996. [CrossRef]
- Meedt, E.; Hiergeist, A.; Gessner, A.; Dettmer, K.; Liebisch, G.; Ghimire, S.; Poeck, H.; Edinger, M.; Wolff, D.; Herr, W.; et al. Prolonged Suppression of Butyrate-Producing Bacteria Is Associated With Acute Gastrointestinal Graft-vs-Host Disease and Transplantation-Related Mortality After Allogeneic Stem Cell Transplantation. Clinical Infectious Diseases 2022, 74, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, S.; Szabo, A.; Clurman, A.; McShane, K.; Waters, N.; Eastwood, D.; Samanas, L.; Fei, T.; Armijo, G.; Abedin, S.; et al. Mitigation of Gastrointestinal Graft-versus-Host Disease with Tocilizumab Prophylaxis Is Accompanied by Preservation of Microbial Diversity and Attenuation of Enterococcal Domination. haematol 2022, 108, 250–256. [Google Scholar] [CrossRef]
- Stein-Thoeringer, C.K.; Nichols, K.B.; Lazrak, A.; Docampo, M.D.; Slingerland, A.E.; Slingerland, J.B.; Clurman, A.G.; Armijo, G.; Gomes, A.L.C.; Shono, Y.; et al. Lactose Drives Enterococcus Expansion to Promote Graft-versus-Host Disease. Science 2019, 366, 1143–1149. [Google Scholar] [CrossRef]
- Fujimoto, K.; Hayashi, T.; Yamamoto, M.; Sato, N.; Shimohigoshi, M.; Miyaoka, D.; Yokota, C.; Watanabe, M.; Hisaki, Y.; Kamei, Y.; et al. An Enterococcal Phage-Derived Enzyme Suppresses Graft-versus-Host Disease. Nature 2024, 632, 174–181. [Google Scholar] [CrossRef]
- Taur, Y.; Xavier, J.B.; Lipuma, L.; Ubeda, C.; Goldberg, J.; Gobourne, A.; Lee, Y.J.; Dubin, K.A.; Socci, N.D.; Viale, A.; et al. Intestinal Domination and the Risk of Bacteremia in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Clinical Infectious Diseases 2012, 55, 905–914. [Google Scholar] [CrossRef]
- Luo, Y.; Sheikh, T.M.M.; Li, X.; Yuan, Y.; Yao, F.; Wang, M.; Guo, X.; Wu, J.; Shafiq, M.; Xie, Q.; et al. Exploring the Dynamics of Gut Microbiota, Antibiotic Resistance, and Chemotherapy Impact in Acute Leukemia Patients: A Comprehensive Metagenomic Analysis. Virulence 2024, 15, 2428843. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. The Effect of Antibiotics on the Composition of the Intestinal Microbiota - a Systematic Review. Journal of Infection 2019, 79, 471–489. [Google Scholar] [CrossRef]
- Taur, Y.; Coyte, K.; Schluter, J.; Robilotti, E.; Figueroa, C.; Gjonbalaj, M.; Littmann, E.R.; Ling, L.; Miller, L.; Gyaltshen, Y.; et al. Reconstitution of the Gut Microbiota of Antibiotic-Treated Patients by Autologous Fecal Microbiota Transplant. Sci Transl Med 2018, 10, eaap9489. [Google Scholar] [CrossRef]
- Masetti, R.; D’Amico, F.; Zama, D.; Leardini, D.; Muratore, E.; Ussowicz, M.; Fraczkiewicz, J.; Cesaro, S.; Caddeo, G.; Pezzella, V.; et al. Febrile Neutropenia Duration Is Associated with the Severity of Gut Microbiota Dysbiosis in Pediatric Allogeneic Hematopoietic Stem Cell Transplantation Recipients. Cancers 2022, 14, 1932. [Google Scholar] [CrossRef]
- Doki, N.; Suyama, M.; Sasajima, S.; Ota, J.; Igarashi, A.; Mimura, I.; Morita, H.; Fujioka, Y.; Sugiyama, D.; Nishikawa, H.; et al. Clinical Impact of Pre-Transplant Gut Microbial Diversity on Outcomes of Allogeneic Hematopoietic Stem Cell Transplantation. Ann Hematol 2017, 96, 1517–1523. [Google Scholar] [CrossRef] [PubMed]
- Galloway-Peña, J.R.; Peterson, C.B.; Malik, F.; Sahasrabhojane, P.V.; Shah, D.P.; Brumlow, C.E.; Carlin, L.G.; Chemaly, R.F.; Im, J.S.; Rondon, G.; et al. Fecal Microbiome, Metabolites, and Stem Cell Transplant Outcomes: A Single-Center Pilot Study. Open Forum Infectious Diseases 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Biagi, E.; Zama, D.; Rampelli, S.; Turroni, S.; Brigidi, P.; Consolandi, C.; Severgnini, M.; Picotti, E.; Gasperini, P.; Merli, P.; et al. Early Gut Microbiota Signature of aGvHD in Children given Allogeneic Hematopoietic Cell Transplantation for Hematological Disorders. BMC Med Genomics 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Artacho, A.; González-Torres, C.; Gómez-Cebrián, N.; Moles-Poveda, P.; Pons, J.; Jiménez, N.; Casanova, M.J.; Montoro, J.; Balaguer, A.; Villalba, M.; et al. Multimodal Analysis Identifies Microbiome Changes Linked to Stem Cell Transplantation-Associated Diseases. Microbiome 2024, 12. [Google Scholar] [CrossRef]
- Biagi, E.; Zama, D.; Nastasi, C.; Consolandi, C.; Fiori, J.; Rampelli, S.; Turroni, S.; Centanni, M.; Severgnini, M.; Peano, C.; et al. Gut Microbiota Trajectory in Pediatric Patients Undergoing Hematopoietic SCT. Bone Marrow Transplant 2015, 50, 992–998. [Google Scholar] [CrossRef]
- Azhar Ud Din, M.; Lin, Y.; Lyu, C.; Yi, C.; Fang, A.; Mao, F. Advancing Therapeutic Strategies for Graft-versus-Host Disease by Targeting Gut Microbiome Dynamics in Allogeneic Hematopoietic Stem Cell Transplantation: Current Evidence and Future Directions. Mol Med 2025, 31, 2. [Google Scholar] [CrossRef]
- Rashidi, A.; Ebadi, M.; Rehman, T.U.; Elhusseini, H.; Kazadi, D.; Halaweish, H.; Khan, M.H.; Hoeschen, A.; Cao, Q.; Luo, X.; et al. Randomized Double-Blind Phase II Trial of Fecal Microbiota Transplantation Versus Placebo in Allogeneic Hematopoietic Cell Transplantation and AML. JCO 2023, 41, 5306–5319. [Google Scholar] [CrossRef]
- Golob, J.L.; Pergam, S.A.; Srinivasan, S.; Fiedler, T.L.; Liu, C.; Garcia, K.; Mielcarek, M.; Ko, D.; Aker, S.; Marquis, S.; et al. Stool Microbiota at Neutrophil Recovery Is Predictive for Severe Acute Graft vs Host Disease After Hematopoietic Cell Transplantation. Clinical Infectious Diseases 2017, 65, 1984–1991. [Google Scholar] [CrossRef]
- Du, Y.; He, C.; An, Y.; Huang, Y.; Zhang, H.; Fu, W.; Wang, M.; Shan, Z.; Xie, J.; Yang, Y.; et al. The Role of Short Chain Fatty Acids in Inflammation and Body Health. IJMS 2024, 25, 7379. [Google Scholar] [CrossRef] [PubMed]
- Xiong, R.-G.; Zhou, D.-D.; Wu, S.-X.; Huang, S.-Y.; Saimaiti, A.; Yang, Z.-J.; Shang, A.; Zhao, C.-N.; Gan, R.-Y.; Li, H.-B. Health Benefits and Side Effects of Short-Chain Fatty Acids. Foods 2022, 11, 2863. [Google Scholar] [CrossRef] [PubMed]
- Mann, E.R.; Lam, Y.K.; Uhlig, H.H. Short-Chain Fatty Acids: Linking Diet, the Microbiome and Immunity. Nat Rev Immunol 2024, 24, 577–595. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Lao, J.; Wang, L.; Liu, S. Research Advances on Short-Chain Fatty Acids in Gastrointestinal Acute Graft- versus -Host Disease. Therapeutic Advances in Hematology 2024, 15, 20406207241237602. [Google Scholar] [CrossRef]
- Rolling, T.; Zhai, B.; Gjonbalaj, M.; Tosini, N.; Yasuma-Mitobe, K.; Fontana, E.; Amoretti, L.A.; Wright, R.J.; Ponce, D.M.; Perales, M.A.; et al. Haematopoietic Cell Transplantation Outcomes Are Linked to Intestinal Mycobiota Dynamics and an Expansion of Candida Parapsilosis Complex Species. Nat Microbiol 2021, 6, 1505–1515. [Google Scholar] [CrossRef]
- Yu, J.; Sun, H.; Cao, W.; Han, L.; Song, Y.; Wan, D.; Jiang, Z. Applications of Gut Microbiota in Patients with Hematopoietic Stem-Cell Transplantation. Exp Hematol Oncol 2020, 9, 35. [Google Scholar] [CrossRef]
- Metafuni, E.; Di Marino, L.; Giammarco, S.; Bellesi, S.; Limongiello, M.A.; Sorà, F.; Frioni, F.; Maggi, R.; Chiusolo, P.; Sica, S. The Role of Fecal Microbiota Transplantation in the Allogeneic Stem Cell Transplant Setting. Microorganisms 2023, 11, 2182. [Google Scholar] [CrossRef]
- Yoshifuji, K.; Inamoto, K.; Kiridoshi, Y.; Takeshita, K.; Sasajima, S.; Shiraishi, Y.; Yamashita, Y.; Nisaka, Y.; Ogura, Y.; Takeuchi, R.; et al. Prebiotics Protect against Acute Graft-versus-Host Disease and Preserve the Gut Microbiota in Stem Cell Transplantation. Blood Advances 2020, 4, 4607–4617. [Google Scholar] [CrossRef]
- Yazdandoust, E.; Hajifathali, A.; Roshandel, E.; Zarif, M.N.; Pourfathollah, A.A.; Parkhideh, S.; Mehdizadeh, M.; Amini-Kafiabad, S. Gut Microbiota Intervention by Pre and Probiotics Can Induce Regulatory T Cells and Reduce the Risk of Severe Acute GVHD Following Allogeneic Hematopoietic Stem Cell Transplantation. Transplant Immunology 2023, 78, 101836. [Google Scholar] [CrossRef]
- Beckerson, J.; Szydlo, R.M.; Hickson, M.; Mactier, C.E.; Innes, A.J.; Gabriel, I.H.; Palanicawandar, R.; Kanfer, E.J.; Macdonald, D.H.; Milojkovic, D.; et al. Impact of Route and Adequacy of Nutritional Intake on Outcomes of Allogeneic Haematopoietic Cell Transplantation for Haematologic Malignancies. Clinical Nutrition 2019, 38, 738–744. [Google Scholar] [CrossRef]
- Van Lier, Y.F.; Davids, M.; Haverkate, N.J.E.; De Groot, P.F.; Donker, M.L.; Meijer, E.; Heubel-Moenen, F.C.J.I.; Nur, E.; Zeerleder, S.S.; Nieuwdorp, M.; et al. Donor Fecal Microbiota Transplantation Ameliorates Intestinal Graft-versus-Host Disease in Allogeneic Hematopoietic Cell Transplant Recipients. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Shirsalimi, N.; Hashempour, Z.; Salehi Omran, H.; Sedighi, E.; Beigi, F.; Mortezazadeh, M. Safety and Efficacy of Fecal Microbiota Transplantation (FMT) as a Modern Adjuvant Therapy in Various Diseases and Disorders: A Comprehensive Literature Review. Front. Immunol. 2024, 15, 1439176. [Google Scholar] [CrossRef] [PubMed]
- Biernat, M.M.; Urbaniak-Kujda, D.; Dybko, J.; Kapelko-Słowik, K.; Prajs, I.; Wróbel, T. Fecal Microbiota Transplantation in the Treatment of Intestinal Steroid-Resistant Graft-versus-Host Disease: Two Case Reports and a Review of the Literature. J Int Med Res 2020, 48. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Malard, F.; Rubio, M.T.; Ruggeri, A.; Mamez, A.C.; Brissot, E.; Giannotti, F.; Dulery, R.; Joly, A.C.; Baylatry, M.T.; et al. Fecal Microbiota Transplantation before or after Allogeneic Hematopoietic Transplantation in Patients with Hematologic Malignancies Carrying Multidrug-Resistance Bacteria. Haematologica 2019, 104, 1682–1688. [Google Scholar] [CrossRef]
- Innes, A.J.; Mullish, B.H.; Fernando, F.; Adams, G.; Marchesi, J.R.; Apperley, J.F.; Brannigan, E.; Davies, F.; Pavlů, J. Faecal Microbiota Transplant: A Novel Biological Approach to Extensively Drug-Resistant Organism-Related Non-Relapse Mortality. Bone Marrow Transplant 2017, 52, 1452–1454. [Google Scholar] [CrossRef]
- Ghani, R.; Mullish, B.H.; McDonald, J.A.K.; Ghazy, A.; Williams, H.R.T.; Brannigan, E.T.; Mookerjee, S.; Satta, G.; Gilchrist, M.; Duncan, N.; et al. Disease Prevention Not Decolonization: A Model for Fecal Microbiota Transplantation in Patients Colonized With Multidrug-Resistant Organisms. Clinical Infectious Diseases 2021, 72, 1444–1447. [Google Scholar] [CrossRef]
- Neemann, K.; Eichele, D.D.; Smith, P.W.; Bociek, R.; Akhtari, M.; Freifeld, A. Fecal Microbiota Transplantation for Fulminant CLostridium Difficile Infection in an Allogeneic Stem Cell Transplant Patient. Transplant Infectious Dis 2012, 14. [Google Scholar] [CrossRef]
- De Castro, C.G.; Ganc, A.J.; Ganc, R.L.; Petrolli, M.S.; Hamerschlack, N. Fecal Microbiota Transplant after Hematopoietic SCT: Report of a Successful Case. Bone Marrow Transplant 2015, 50, 145–145. [Google Scholar] [CrossRef]
- Bluestone, H.; Kronman, M.P.; Suskind, D.L. Fecal Microbiota Transplantation for Recurrent Clostridium Difficile Infections in Pediatric Hematopoietic Stem Cell Transplant Recipients. Journal of the Pediatric Infectious Diseases Society 2018, 7, e6–e8. [Google Scholar] [CrossRef]
- Innes, A.J.; Mullish, B.H.; Ghani, R.; Szydlo, R.M.; Apperley, J.F.; Olavarria, E.; Palanicawandar, R.; Kanfer, E.J.; Milojkovic, D.; McDonald, J.A.K.; et al. Fecal Microbiota Transplant Mitigates Adverse Outcomes Seen in Patients Colonized With Multidrug-Resistant Organisms Undergoing Allogeneic Hematopoietic Cell Transplantation. Front. Cell. Infect. Microbiol. 2021, 11. [Google Scholar] [CrossRef]
- Carlson, P.E. Regulatory Considerations for Fecal Microbiota Transplantation Products. Cell Host & Microbe 2020, 27, 173–175. [Google Scholar] [CrossRef]
- Iyama, S.; Tatsumi, H.; Shiraishi, T.; Yoshida, M.; Tatekoshi, A.; Endo, A.; Ishige, T.; Shiwa, Y.; Ibata, S.; Goto, A.; et al. Possible Clinical Outcomes Using Early Enteral Nutrition in Individuals with Allogeneic Hematopoietic Stem Cell Transplantation: A Single-Center Retrospective Study. Nutrition 2021, 83, 111093. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, F.; Biagi, E.; Rampelli, S.; Fiori, J.; Zama, D.; Soverini, M.; Barone, M.; Leardini, D.; Muratore, E.; Prete, A.; et al. Enteral Nutrition in Pediatric Patients Undergoing Hematopoietic SCT Promotes the Recovery of Gut Microbiome Homeostasis. Nutrients 2019, 11, 2958. [Google Scholar] [CrossRef] [PubMed]
- Iyama, S.; Sato, T.; Tatsumi, H.; Hashimoto, A.; Tatekoshi, A.; Kamihara, Y.; Horiguchi, H.; Ibata, S.; Ono, K.; Murase, K.; et al. Efficacy of Enteral Supplementation Enriched with Glutamine, Fiber, and Oligosaccharide on Mucosal Injury Following Hematopoietic Stem Cell Transplantation. Case Rep Oncol 2014, 7, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Riwes, M.M.; Golob, J.L.; Magenau, J.; Shan, M.; Dick, G.; Braun, T.; Schmidt, T.M.; Pawarode, A.; Anand, S.; Ghosh, M.; et al. Feasibility of a Dietary Intervention to Modify Gut Microbial Metabolism in Patients with Hematopoietic Stem Cell Transplantation. Nat Med 2023, 29, 2805–2813. [Google Scholar] [CrossRef]
- Porcari, S.; Ng, S.C.; Zitvogel, L.; Sokol, H.; Weersma, R.K.; Elinav, E.; Gasbarrini, A.; Cammarota, G.; Tilg, H.; Ianiro, G. The Microbiome for Clinicians. Cell 2025, 188, 2836–2844. [Google Scholar] [CrossRef]
- Porcari, S.; Mullish, B.H.; Asnicar, F.; Ng, S.C.; Zhao, L.; Hansen, R.; O’Toole, P.W.; Raes, J.; Hold, G.; Putignani, L.; et al. International Consensus Statement on Microbiome Testing in Clinical Practice. The Lancet Gastroenterology & Hepatology 2025, 10, 154–167. [Google Scholar] [CrossRef]
- Mirzayi, C.; Renson, A.; Genomic Standards Consortium; Massive Analysis and Quality Control Society; Furlanello, C.; Sansone, S.-A.; Zohra, F.; Elsafoury, S.; Geistlinger, L.; Kasselman, L.J.; et al. Reporting Guidelines for Human Microbiome Research: The STORMS Checklist. Nat Med 2021, 27, 1885–1892. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



