Submitted:
27 August 2025
Posted:
28 August 2025
You are already at the latest version
Abstract
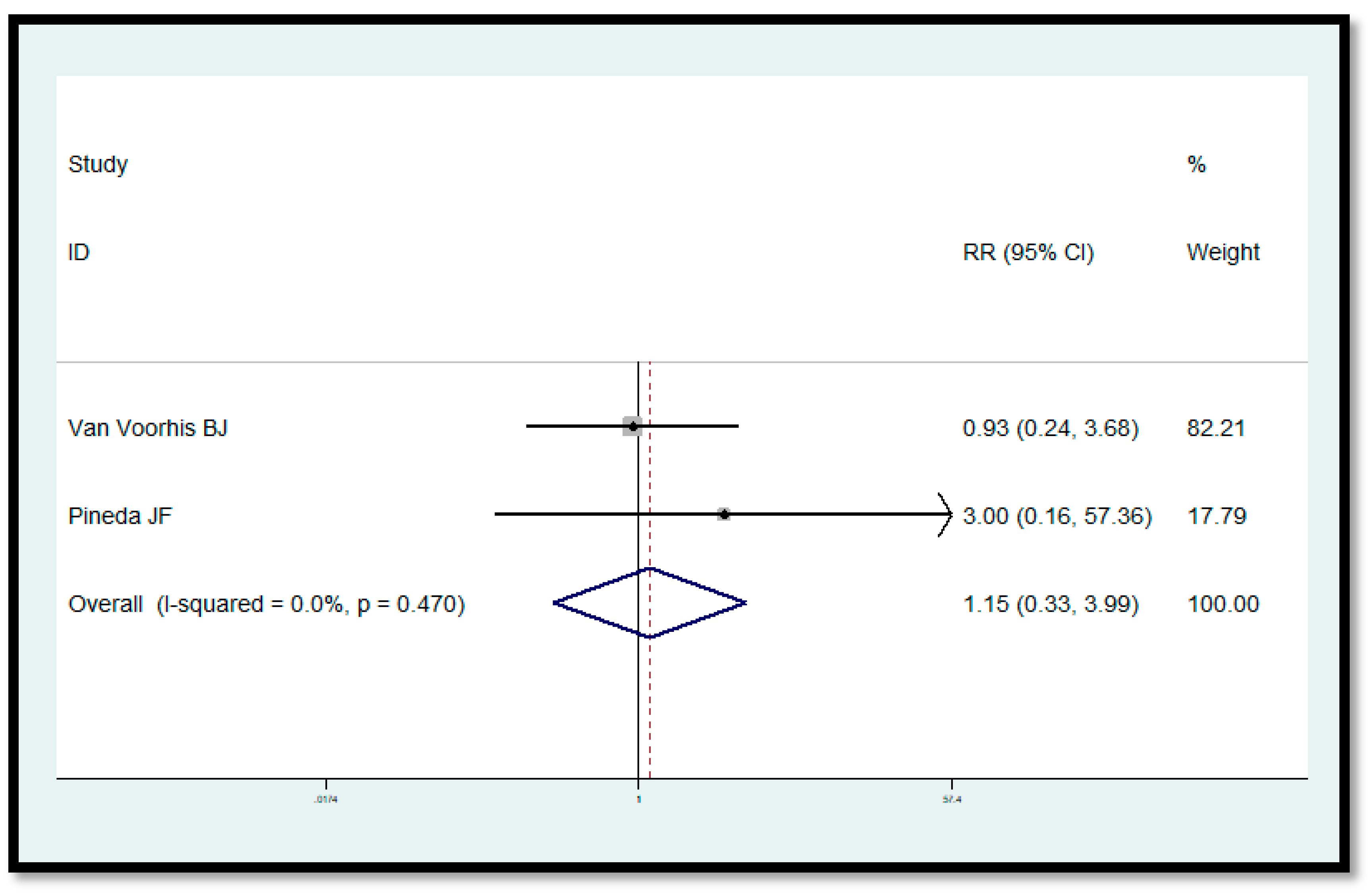
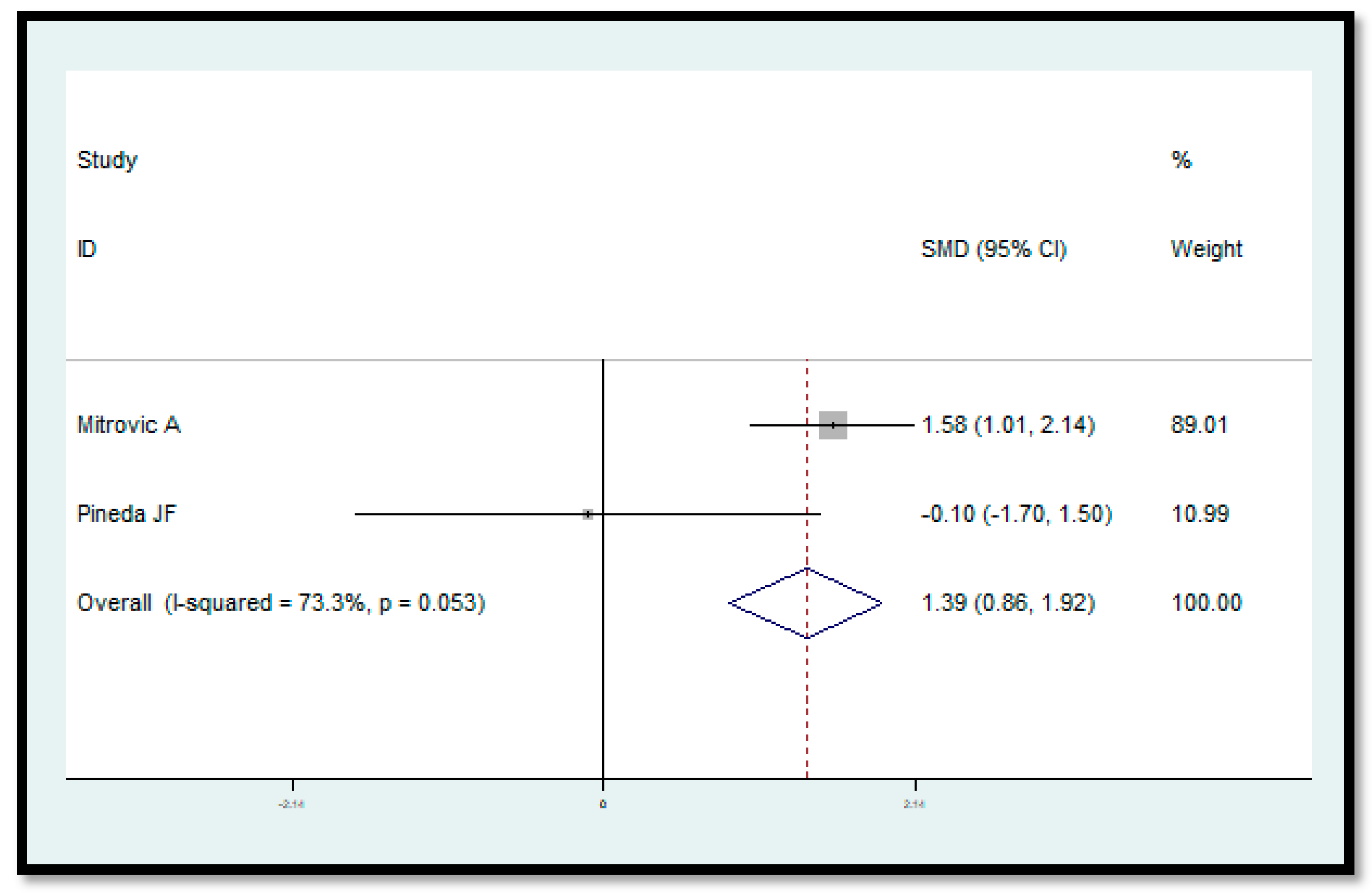
Importance: Infertility is a widespread problem and the scientific world is constantly looking for possible solutions that can increase the chances of a pregnancy. Objective: We perform a systematic review with meta-analysis to compare the different current intervention methodologies to treat female infertility with hyperbaric oxygen therapy (HBOT). This review also introduces the molecular theoretical hypothesis of how the use of HBOT could regulate the expression of sirtuins, in particular, SIRT1 through the well-known hyperoxia-hypoxia paradox. Data sources: We performed research among the results of the major electronic databases (Cochrane, Lilacs, Scopus, Pubmed) and internet search engines (Google, Google Scholar) for studies that evaluated the correlation between female infertility and HBOT. Study selection and synthesis: Studies that match the following criteria were included: (1) every type of published or ongoing study on specified databases dealing with (a) female infertility of every cause and (b) hyperbaric oxygen therapy or (c) oxygen therapy linked. Thanks to the analysis of the various observational and non-observational studies, we try to answer some questions considered relevant to the topic based on Evidence-Based Medicine (EBM). The program used here to produce the following methodological review is Cochrane Review Manager 5.4. Then, the review was checked and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (www.prisma-statement.org). Meta-analysis was performed using the ‘metan’ routine by the Stata statistics software (version 13 for Windows Stata Corporation, 2016). The evaluation of evidence and risk of bias assessment was done with the GRADEpro tool, available at https://gdt.gradepro.org/. Main outcome(s): Association between HBOT and female infertility. Results: Included articles and methodology are specified in the article. A significant change in endometrial thickness was observed in the meta-analysis, the SMD was 1.388, p<0.001. No difference in conceived with HBO therapy (versus no HBO therapy) was observed in the meta-analysis, RR=1.149, p=0.827. Conclusion and relevance: The studies present in the literature, despite the vast heterogeneity, suggest that there is a possible link between HBOT and female infertility. However, more studies are needed to evaluate this new link in the management and possible treatment of women with infertility.
Keywords:
Capsule
1. Introduction
1.1. Rationale
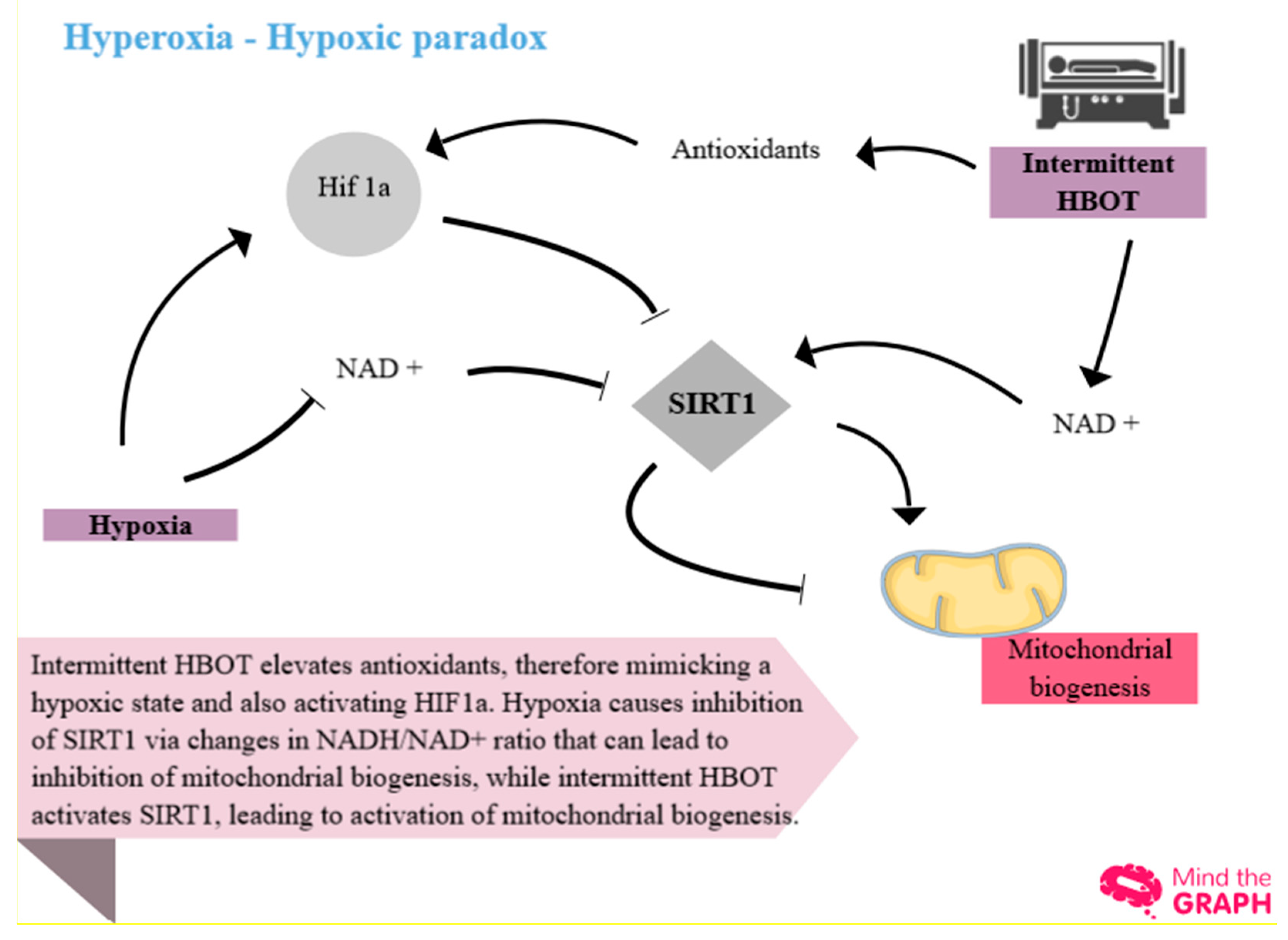
1.1.1. Focus on SIRT 1
1.1.2. Relationship Between Sirtuins and HBOT
1.1.3. Description of the Methods Being Investigated
1.1.4. How These Methods Might Work
1.1.5. Why It Is Important to Do This Review
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Selection Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.4.1. Selection of Studies
2.4.2. Data Extraction and Management
2.4.3. Types of Studies
2.4.4. Types of Data
2.4.5. Types of Methods
2.4.6. Electronic Searches
2.4.7. Searching Other Resources
2.5. Data Collection Process
2.5.1. Data Collection and Analysis
2.6. Study Risk of Bias Assessment
2.6.1. Assessment of Reporting Biases
2.7. Effect Measures
2.7.1. Types of Outcome Measures
2.7.2. Primary Outcomes
2.7.3. Secondary Outcomes
2.8. Synthesis Methods
2.8.1. Measures of the Effect of the Methods
2.8.2. Dealing with Missing Data
2.8.3. Assessment of Heterogeneity
2.8.4. Data Synthesis
2.8.5. Sensitivity Analysis
2.9. Reporting Bias Assessment
2.9.1. Assessment of Risk of Bias in Included Studies
2.10. Certainty Assessment
2.10.1. Main Results
3. Results
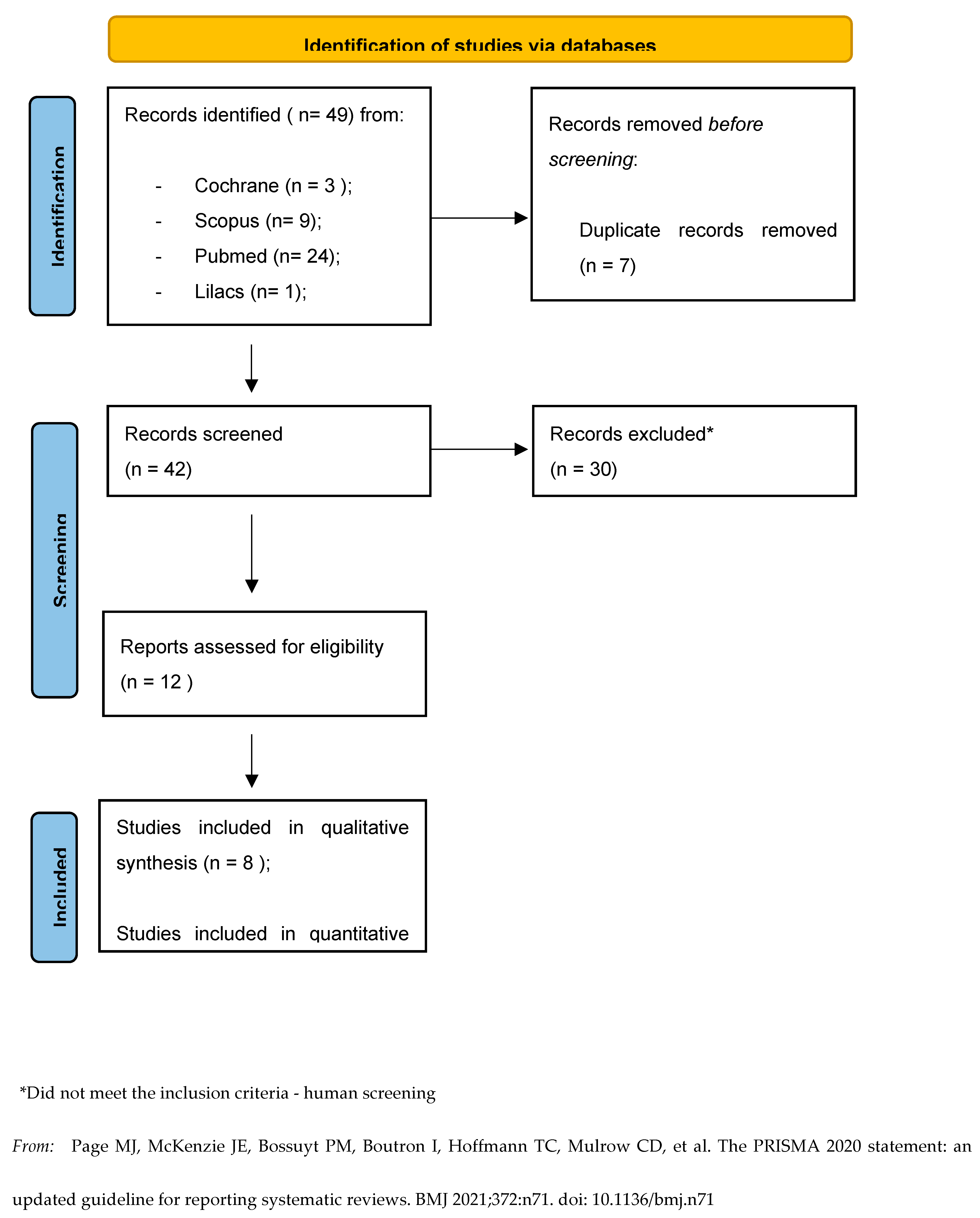
3.1. Study Selection
3.1.1. Description of Studies
3.1.2. Results of the Search
3.1.3. Included Studies
3.1.4. Excluded Studies
3.2. Study Characteristics
3.2.1. Characteristics of Included Studies
3.2.2. Summary of Findings Tables
3.3. Risk of Bias in Studies
3.4. Results Of Individual Studies
3.4.1. Does HBOT Increase Pregnancy Probability? (Analysis 1.1) 3.4.2. Does HBOT Increase Endometrial Thickness? (Analysis 1.2) 3.4.3. Does HBOT Increase AMH Levels? (Analysis 1.3)
3.5. Results of Syntheses
3.5.1. Data and Analyses
3.6. Reporting Biases
3.7. Certainty of Evidence
3.7.1. Summary of Main Results
3.7.2. Overall Completeness and Applicability of Evidence
3.7.3. Quality of the Evidence
4. Discussion
5. Conclusions
- 5.1.1. Authors' Conclusions
- 5.1.2. Implications of the Results for Practice and Future Research
Supplementary Materials
Funding
Acknowledgements
Data Availability Statement
Attestation Statement
References
- Carafa V, Rotili D, Forgione M, Cuomo F, Serretiello E, Hailu GS; et al. Sirtuin functions and modulation: From chemistry to the clinic. Clin Epigenetics [Internet]. [CrossRef]
- Yamamoto H, Schoonjans K, Auwerx J. Sirtuin functions in health and disease. Mol Endocrinol. 2007, 21, 1745–1755. [Google Scholar] [CrossRef] [PubMed]
- Di Emidio G, Falone S, Artini PG, Amicarelli F, D’alessandro AM, Tatone C. Mitochondrial sirtuins in reproduction. Antioxidants. 2021, 10, 1–26. [Google Scholar]
- Tatone C, di Emidio G, Barbonetti A, Carta G, Luciano AM, Falone S; et al. Sirtuins in gamete biology and reproductive physiology: Emerging roles and therapeutic potential in female and male infertility. Hum Reprod Update. 2018, 24, 267–289. [Google Scholar] [CrossRef] [PubMed]
- Alam F, Syed H, Amjad S, Baig M, Khan TA, Rehman R. Interplay between oxidative stress, SIRT1, reproductive and metabolic functions. Curr Res Physiol. 2021, 4, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Schottlender N, Gottfried I, Ashery U. Hyperbaric oxygen treatment: Effects on mitochondrial function and oxidative stress. Biomolecules. 2021, 11, 1–17. [Google Scholar]
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Gallardo Pineda JF, López Ortiz CGS, De Siu Moguel GJ, Castro Lopez CRE, Alcocer HM, Velasco ST. Improvement in serum anti-Müllerian hormone levels in infertile patients after hyperbaric oxygen (Preliminary results). J Bras Reprod Assist. 2015, 19, 87–90. [Google Scholar]
- Mitrović A, Nikolić B, Dragojević S, Brkić P, Ljubić A, Jovanović T. Hyperbaric oxygenation as a possible therapy of choice for infertility treatment. Bosn J Basic Med Sci. 2006, 6, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Verdini F, Cannellotto M, Romero-feris D. Oxigenación hiperbárica en el tratamiento de la infertilidad Hyperbaric oxygenation for infertility treatment. 39, 3–8.
- Feng J, Wang J, Zhang Y, Zhang Y, Jia L, Zhang D; et al. The Efficacy of Complementary and Alternative Medicine in the Treatment of Female Infertility. Evidence-based Complement Altern Med. 2021, 2021.
- Leverment J, Turner R, Bowman M, Cooke CJ. Report of the use of hyperbaric oxygen therapy (HBO2) in an unusual case of secondary infertility. Undersea Hyperb Med J Undersea Hyperb Med Soc Inc. 2004, 31, 245–250. [Google Scholar]
- Van Voorhis BJ, Greensmith JE, Dokras A, Sparks AET, Simmons ST, Syrop CH. Hyperbaric oxygen and ovarian follicular stimulation for in vitro fertilization: A pilot study. Fertil Steril. 2005, 83, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Wang D, Jiang Y, Feng J, Gao J, Yu J, Zhao J; et al. Evidence for the Use of Complementary and Alternative Medicine for Pelvic Inflammatory Disease: A Literature Review. Evidence-based Complement Altern Med. 2022, 2022.
- Yu J, Qi YL, Lu DW, Fang QJ, Li L, Sang L. Multiple Protocols Combined with Hyperbaric Oxygen Therapy on the Maintenance of Ovarian Function in Patients After Ovarian Cystectomy. Front Surg. 2022, 9.
- Available online: https://www.who.int/news-room/fact-sheets/detail/infertility.
- Available online: https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12621001671853.
- Available online: https://www.reproductivemedicine.com/toc/auto_abstract.php?id=24805.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



