
Submitted:
25 August 2025
Posted:
26 August 2025
You are already at the latest version
Abstract
The brainstem represents a structure of prominent importance for the genera-tion and control of eye movements (saccades, smooth pursuit, the vestibulo-ocular re-flex, VOR, vergence and gaze holding). Besides its several physiological functions of vi-tal importance, the brainstem plays a role in the coordination of balance and move-ments. Therefore, eye movement disorders of brainstem origin are frequently associat-ed with vertigo, imbalance, unsteady gait and walk and diplopia upon changing head and body posture. Nonetheless, an adequate knowledge of the neural structures in-volved in oculomotor and vestibular control allows for the identification and accurate localization of a wide variety of brainstem syndrome. However, oculomotor abnormali-ties arising from brainstem disease constitute an extremely complex challenge for the otoneurologist by virtue of the remarkable diversity of causes (vascular, traumatic, de-generative, neoplastic) of their variable severity, of their clinical course (acute, fluctu-ating or progressive) and finally by virtue of concomitant involvement of other central structures (mainly cerebellum). F Nonetheless, an adequate knowledge of the neural structures involved in oculomotor and vestibular control allows for the identification and accurate localization of a wide variety of brainstem syndrome. or these reasons, eye movement disorders and nystagmus of brainstem origin are frequently associated not only with vertigo and imbalance but with a wide range of other neurological signs. This short review describes the pathophysiology and the clinical characteristics of oculomo-tor disorders and nystagmus in brainstem disorders.
Keywords:
brainstem
; vertigo
; nystagmus
; ocular motor
; vestibular central disorders
; eye movements
1. Introduction
The term "central vestibular dysfunction" covers a wide range of pathologies, ranging from a single acute event such as a cerebellar stroke to chronic and fluctuating conditions such as vestibular migraine. A central vestibular disorder can be defined as a condition originating from lesions in the brain, cerebellar and brainstem. Evaluating and treating all these pathological conditions originating from different brain sectors represents an extremely complex challenge for the otoneurologist by virtue of the remarkable diversity of causes (vascular, traumatic, degenerative, neoplastic) of their variable severity and based on the progressive nature of some diagnoses of central vestibular pathology. Going into specifics, the brainstem represents a structure of prominent importance for the generation and control of eye movements (saccades, smooth pursuit, the vestibulo-ocular reflex, VOR, vergence and gaze holding [1]. Besides its several physiological functions of vital importance, the brainstem plays a role in the coordination of balance and movements. This process is based upon the activity of the oculo-vestibular pathway system. This system consists of a vestibular part which controls the body position, and its activity is coordinated with that of the regulatory neurons, which regulate the postural skeletal muscles and the eye movements. Therefore, eye movement disorders of brainstem origin are frequently associated with vertigo, imbalance, unsteady gait and walk and diplopia upon changing head and body posture. For these reasons, an accurate characterization of the eye movement anomalies represents a fundamental moment in the diagnosis of central vestibular syndromes, being also able to identify and localize, at least in a high number of cases, the role of each unit and/or neural circuit in the genesis of the oculomotor lesion (Table 1)2.
2. Symptoms and Signs in Brainstem Lesions
The disorders of the central vestibular manifest with non-specific symptoms (dizziness and vertigo): whether we are faced with a central or peripheral problem, the symptoms are few and not localized to a particular area:
- -
- rotatory vertigo
- -
- postural instability or unsteadiness
- -
- postural crises
- -
- unclear or blurred vision.
However, none of these symptoms are indicative of the site of the lesion: rotatory vertigo is typical of an acute disorder of the peripheral vestibular receptor but is also present in Wallemberg syndrome or in other vascular disorders related to brainstem or cerebellum. At the same time, chronic instability or dizziness with no rotatory vertigo can be due to a neoplastic or degenerative disease of the central nervous system but also to a bilateral peripheral vestibular dysfunction. A latero-pulsion and subsequent risk of fall characterized by a sudden onset and rapid resolution can be present in the neurovascular conflict of the eighth cranial nerve or in patients with vertebro-basilar insufficiency, as well as in Tumarkin’s otolithic crises in late Menière’s Disease [3]. For this reason, it is not possible to attempt a diagnosis based only on the type of vertigo ("objective" or "subjective", or as proposed more recently, without substantial changes in meaning, "external" or "internal"). Unlike subjective, objective symptoms can be highly specific for location and the oto-neurological examination can provide the additional sign that, demonstrating a spatial-temporal dissemination, allows the Neurologist to make a diagnosis in case of Vertebro-Basilar Insufficiency or Multiple Sclerosis. Many brainstem centers are involved in controlling eye movements, but a simple clinical rule can be used in clinical practice: horizontal eye movements are generated and controlled in the pontine region, whereas vertical (and torsional) eye movements originate in the midbrain (Figure 1); consequently, the recognition of the various pattern of oculomotor disturbances could allow a topographic diagnosis of the lesions occurring at diverse levels in the brainstem. Classically, symptoms and signs of brainstem involvement are classified as medullary, pontine and mesencephalic syndromes [4,5]. in the next paragraphs, the oculomotor abnormalities of greatest otoneurological interest to otoneurology will be reported.
2.1. Abnormal Eye Movements in Medullary Lesions.
A lot of medullary structures are involved in the control of eye movements (vestibular nuclei, nucleus propositus hypoglossi, NPH, nucleus intercalatus, nucleus of Roller, inferior olivary nucleus, inferior cerebellar peduncle and cell groups of the paramedian tract. A lesion of one or more of this area could produce various pattern of nystagmus and vertigo. Acute rotatory vertigo with spontaneous torsional or horizontal-rotary unidirectional nystagmus could be the initial symptomatology of Wallenberg’s syndrome (lateral medullary infarction), often mimicking a vestibular neuritis [6]. The presence of some additional signs (alterations in facial sensation, dysarthria and dysphagia, ipsilateral Horner’s syndrome) could help to a correct diagnosis. However, the combination of ocular lateropulsione and saccadic dysmetria with a partial or complete ipsilesional Ocular Tilt Reaction (OTR) is indicative of a lateral medullary lesion [7,8]. On the contrary a medial medullary infarction, beside a contralateral hemiparesis and ipsilesional tongue paralysis, produce a ipsilateral horizontal (sometimes upbeating for involvement of perihypoglossal nuclei) nystagmus and a horizontal gaze evoked nystagmus (GEN) more intense looking to the affected side (caused by a damage of NPH) [9]. Unilateral lesions of NPH induce intense vertigo and unsteadiness associated with ipsilesional-beating spontaneous nystagmus or horizontal GEN more intense on looking toward the ipsilesional side, central patterns of head shaking nystagmus (HSN), impaired smooth pursuit (SP), and static contralateral ocular deviation [10]. Furthermore, patients with NPH lesions showed decreased head impulse VOR gains for the contralesional horizontal semicircular canal and increased gains for both anterior semicircular canals [11]. The inferior cerebellar peduncle, via the juxtarestiform body, allows a direct connection between the vestibular nuclei and the cerebellum and a lesion involving this structure create acute vertigo associated with ipsilesional spontaneous nystagmus (horizontal and/or torsional) and contralateral ocular Tilt Reaction (OTR), caused by a loss of cerebellar inhibition the vestibular nuclei [12,13] (Figure 2). A lesion of the nucleus of Roller could generate an upbeat nystagmus just as a lesion of the cell groups of the paramedian tracts can produce a downbeat or upbeat nystagmus, this structure being involved in the processing of the vertical position of the eyes [14,15,16].
2.2. Abnormal Eye Movements in Pontine Lesions
At pontine level is located the center for horizontal saccades, the paramedian pontine reticular formation (PPRF); this structure, together NPH, the vestibular nuclei and the vestibulo-cerebellum represent the center for the conjugate horizontal gaze-holding function, the so-called “neuronal integrator.” Clinically this means that isolated horizontal saccadic palsy indicates a pontine lesion, and a unilateral PPRF (or sixth nerve nucleus) lesion will result in saccadic disturbances on the side of the lesion. Isolated palsy of horizontal saccades on both sides was found in spinocerebellar ataxia type 2 or brainstem tumor [17,18]. A purely horizontal GEN originates from a pontine lesion [1]. On the other hand, a vertical GEN and impaired vertical smooth pursuit and saccades may appear because of an involvement of the pontine areas connected by the medial longitudinal fascicule (MLF) to the midbrain area involved with vertical gaze [19]. Another key structure at pontine level is the medial longitudinal fascicle (MLF) whose damage causes the onset of the so called internuclear ophthalmoplegia (INO), caused by an interruption of the MLF between the nuclei of the third cranial nerve on one side and the contralateral sixth. The INO can be unilateral or bilateral and may present with or without (neurologically isolated) other brainstem findings. Unilateral INO (caused mainly by ischemia) is characterized by impaired adduction of the ipsilateral eye and abducting nystagmus of the contralateral eye sometimes associated with skew deviation (SD) characterized by hypertropia of ipsilesional eye and contraversive head tilt [1,20,21] (Figure 3). Bilateral INO is characterized by bilateral adduction lag and bilateral abduction nystagmus, associated with spontaneous (upbeating) and gaze evoked vertical nystagmus [1,16,22] and the most common etiology is infarction of the midbrain in older patients and demyelinating disease in young patients [20,23,24]. However, an MLF lesion could cause vertical (upbeating, more in the contralesional eye and downbeating, more in the ipsilesional eye) or torsional nystagmus each of which may cause oscillopsia [1,7]. A lesion involving the PPRF and the MLF produces “one and a half syndrome.” This syndrome is characterized by the loss of all horizontal movements except abduction in the contralateral eye, so the only preserved horizontal eye movement is abduction of the contralateral eye [25,26]. This condition is frequently associate with an involvement of one or more cranial nerve [27].
2.3. Abnormal Eye Movements in Midbrain Lesions
The midbrain contains the third and fourth nerve nuclei, the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) and the interstitial nucleus of Cajal (INC). These structures represent the center involved in vertical saccades and in vertical gaze-holding function [28]. Clinically a midbrain lesion induces an isolated vertical saccadic paresis and/or isolated vertical GEN [29,31]. However, it must be emphasized that a lot of the lesions affecting the brainstem, in different pathologies (degenerative, neoplastic, vascular), lead not only to the onset of oculomotor abnormalities and/or nystagmus. The midbrain, pons, and medulla are components of the brainstem which control basic body functions such as consciousness, breathing, proprioception, heart rate, and blood pressure: for the reason a lesion of these structures also lead to other neurological symptoms such as headache, sensory disturbances, and altered function of some cranial nerves (Table 2), often making the above described oculomotor anomalies a part (albeit a significant one) of a more complex neurological clinical picture. Nonetheless, [29,31] an adequate knowledge of the neural structures involved in oculomotor and vestibular control allows for the identification and accurate localization of a wide variety of brainstem syndrome.
Table 2 summarizes the main symptoms and signs of brainstem disorders and the relative involved structures.
3. Vascular Disorders of the Brainstem
Posterior circulation strokes involving the brainstem can result in subsequent oculomotor and vestibular disorders. Approximately 20-25% of ischemic stroke involve the posterior circulation [33]. The brainstem is supplied by the vertebro-basilar system, which includes the following arteries: vertebral arteries, basilar arteries, posterior inferior cerebellar artery (PICA), anterior inferior cerebellar artery (AICA), superior cerebellar artery, and labyrinthine artery. Strokes involving the arteries supplying the brainstem can result in a variety of different neurologic manifestations—such as ocular motor palsies, lid retraction, ptosis, diplopia, gaze palsies, nystagmus, SD, issues with accommodation, and abnormal pupillary function. Among the possible causes of acute vertigo, disorders of the posterior circulation constitute one of the most common central forms. Approximately 10% to 20% of patients with acute vertigo presenting to the Emergency Department have stroke [34,35], particularly involving the brainstem or, more frequently, cerebellum, 95% ischemic [35] as a cause. For these reasons, in the most recent studies, the Authors have concentrated a lot and with some success, on the differential diagnosis between a peripheral and central cause of acute vertigo: in the last years methods and tests have been proposed to allow the differential diagnosis [36,37,38,39], even if with a sensitivity that does not reach one hundred percent [40]. On the other hand, the coexistence of other neurological signs and symptoms is crucial for the diagnosis of acute vertigo of central origin. Nevertheless, differential diagnosis between an acute vertigo of peripheral origin and brainstem or cerebellar infarction may be challenging as focal strokes affecting the root entry zone of the eighth nerve, the vestibular nuclei, or the pathways (in the cerebellar peduncle) from the vestibular nucleus to the cerebellar flocculus and vermis could mimic a peripheral acute vertigo due to a vestibular neuritis. In these cases, in the absence of sign or symptoms clearly attributable to the central nervous system involvement, an accurate bedside vestibular examination could be more sensitive in the diagnosis of an ischemic event than MRI in the first 24–48 hours [39]. Some diagnostic algorithms based on easy bedside tests have been proposed to avoid misdiagnosis in an emergency setting, such as HINTS (assessing HIT, direction of spontaneous nystagmus and SD), HINTS plus (HINTS + evaluation of hearing loss) and STANDING (assessing direction of spontaneous and positional nystagmus, HIT and gait) [37,39,41,42]. In fact, multidirectional (gaze-evoked) or mainly vertical/torsional spontaneous nystagmus, a negative HIT, a significant SD and severe unsteadiness should address towards a central origin and should prompt further investigations. However, unlike cerebellar infarction, which can manifest itself in a significant percentage of cases with a clinical picture very similar to acute peripheral vertigo [43], brainstem infarction is much more frequently associated with neurological signs. As already mentioned above, a lateral medullary stroke from an involvement of PICA (Wallenberg syndrome) can result in acute vertigo and imbalance with horizontal-torsional spontaneous nystagmus (with fixation the fast phase is directed toward the intact side, while with loss of fixation, the patients’ eyes deviated tonically toward the affected side), ipsilesional OTR, hypermetric saccades to the side of the lesion, hypometric to the other side accompanied by classic neurological signs including ipsilateral loss of pain and temperature sensation of the face (involvement of the descending nucleus and tract of the trigeminal nerve), contralateral loss of pain and temperature sensation in the trunk and limbs (spinothalamic tract), dysphagia (nucleus ambiguous), ipsilateral Horner syndrome (descending oculo-sympathetic tract), ipsilateral limb ataxia, gait ataxia, and lateropulsion (inferior cerebellar peduncle, ICP) [4,7,44]. A pontine ischemia of the pons induce a disruption of the horizontal gaze pathway resulting in sixth nerve palsy, INO, horizontal gaze palsies or a combinations of these pathologies as in one and a half syndrome. The oculomotor abnormalities and nystagmus can be associated to hemiparesis, facial nerve palsy, hemisensory loss, dysarthria, dysphagia, ataxia and pseudobulbar affect [45]. Finally, an infarction restricted to the l vestibular nuclear may present with acute isolated vertigo with features of both peripheral and central vestibulopathies: spontaneous torsional-horizontal nystagmus that beat away from the lesion side, direction-changing gaze-evoked nystagmus and positive HIT [46]. Accordingly, central signs including the HINTS and Standing should be carefully sought even in patients with features of peripheral vestibulopathy and negative MRI.
4. Oto-Neurological Signs Associated with Brainstem Involvement
Until a few years ago, it was believed that the pathology of the brainstem could not be monosymptomatic: the brainstem is so rich in structures involved not only in postural and oculomotor control, but also in maintaining consciousness, in controlling the sleep-wake cycle, the respiratory and cardiovascular activity and in the control of sensory inputs. By virtue of this extreme functional complexity, it seems logical to hypothesize that a lesion (vascular, neoplastic, degenerative, etc.), can generate numerous symptoms and signs of central origin. However, there are many cases in which the lesions of the brainstem can determine exclusively otoneurological signs.
4.1. Central Positional Nystagmus
Central positional nystagmus (CPN) can be caused by cerebellar and/or brainstem disorders involving the central vestibulo-cerebellar pathways. These include, among other, structural lesions (tumors, stroke, multiple sclerosis), auto-immune (paraneoplastic and non-paraneoplastic) degenerative disorders and genetic ataxias [47]. CPN could mimic a benign paroxysmal positional vertigo (BPVV), especially certain atypical and rarer forms of BPPV presenting with positional downbeat nystagmus, with upbeat nystagmus when the patient return to the sitting position or nystagmus that does not fatigue both in BPPV of posterior semicircular canal or in apogeotropic type of BPPV of horizontal semicircular canal [48]. CPN can appear as persistent (nystagmus present in one or more positions of the head which, in the single position, does not present any changes for as long as it lasts, whether it is short or long-lasting) or transitory or sometimes paroxysmal, even if the two forms can coexist or follow one another as in the case of a paroxysmal CPN which, maintaining the lying position, becomes persistent [49,50]. CPN can be associated with intense vertigo, oscillopsia, and neurovegetative symptoms, particularly the paroxysmal form.
CPN is probably caused by an abnormal integration of signals coming from semicircular canals and involving the cerebellar nodulus and uvula, inducing a disinhibition of irregular afferent signals converging on the vestibular nucleus [49]. The same cerebellar structures play a key role in the mathematical integration of signals from otolithic and semicircular canal input so that a graviceptive variation induced by the change of position could be the trigger for CPN in case of nodulus/uvula dysfunction nodulus/uvula [51]. For these reasons, CPN is more common in cerebellar disease and brainstem lesions were the cause of CPN only in 8.5% of all the cases [52]. In identifying the site of the lesion, it must be kept in mind that the inferior cerebellar peduncle originates anatomically from the brainstem but is functionally part of the cerebellum [53]. Features of central positional nystagmus include [47,49,52]:
- The CPN may have any trajectory, but pure downbeat and apogeotropic bidirectional horizontal forms are far more common than upbeat, torsional, or mixed forms.
- Nystagmus which occurs during or shortly after a change of position, with little or no latency, suggests a central cause.
- Failure to fatigue/persistence of nystagmus especially after repeated supine roll test suggests a central cause.
- Intense positional nystagmus with little to no vertiginous sensation may also suggest a central cause.
- Poor or no response to repeated repositioning maneuvers.
Obviously, in contrast to BPPV of peripheral otolithic origin, in the large majority of patients with CPN additional neurological or ocular motor symptoms or signs are typically present (GEN, saccadic smooth pursuit, central patterns of head shaking nystagmus, abnormalities of saccades, ataxia and other signs of brainstem dysfunction) [49,52,53]. The most common patterns of CPN are:
- Apogeotropic bidirectional horizontal nystagmus. More commonly associated with cerebellar disease [54], this type of CPN shows no latency and no associated vertigo, lasts as long as the position is maintained and is reproduced by returning the patient to the same position. A brainstem lesion could induce an apogeotropic CPN because of a damage of the connection from nodulus, uvula (and sometimes tonsil) to the vestibular nuclei [12,53,55] (Figure 4).
- Positional downbeating nystagmus (PDN). While in the past the presence of PDN during the head- hanging position and/or in Dix-Hallpike was considered a sign of central vestibular involvement, at the present time PDN is more frequently associated to an apogeotropic variant of posterior canal BPPV [56] or anterior canal BPPV [57]. Two patterns of PDN can be recognized: paroxysmal, with poor or no latency, duration less than 1 minute, and occasionally with a upbeating nystagmus when the patient return to the sitting position reversal; persistent, sometimes preceded by a paroxysmal component [58]. The pathophysiology of PDN during a brainstem lesion is similar to that described for the apogeotropic horizontal positional nystagmus. Recently a case of paroxysmal CPN mimicking posterior canal BPPV was described due to a pontine infarction [59]. Finally, upbeating nystagmus and central bidirectional geotropic nystagmus of central origine are much rarer.
4.2.1. Head Shaking Nystagmus (HSN)
HSN usually suggests a peripheral vestibular lesion. When after a head shaking performed on the horizontal plane a downbeat (more frequently), upbeat or torsional nystagmus appears or clearly superimpose over a concomitant horizontal spontaneous nystagmus, we are facing to a central pattern of HSN, the so-called perverted HSN [60]. Another central pattern of HSN is represented by the appearance of HSN after very few (2-3) cycles of passive oscillation of the head performed at a very low speed, a stimulus not capable of generating a “quantity” of energy sufficient to load the velocity storage mechanism [60,61]. The presence of HSN in central vestibular disorders has been revisited in patients with Wallenberg syndrome where HSN was observed in 14 of 16 patients and, in all cases, the horizontal component was ipsilesional. Even in the eight patients with contralesional spontaneous horizontal nystagmus, the HSNy was opposite to the spontaneous nystagmus. Three patients showed unusually strong HSN with a maximum slow-phase velocity greater than 60 degrees/second. MRI demonstrated in all the cases a lateral medullary infarction involving the caudal and middle part of vestibular nuclei with sparing of the rostral part [62]. A perverted HSN was described in caudal medullary lesion [62,63] and in pontine lesion [64,65]. In 23 cases of vertebrobasilar stroke, 17% of atypical HSNy were detected; only in 1 case MRI showed a medullary infarction with a direction of HSN opposite to spontaneous nystagmus associate with evident ataxia [66].
4.2.2. Smooth Pursuit and Saccades Abnormalities in Brainstem Lesions
Smooth Pursuit (SP) are induced by retinal slip on the retina with the purpose to keep the image of a slowly moving object stable within the fovea along with a role in suppressing or reinforcing the VOR during visual stimulation. Therefore, in case of cerebellar or brainstem lesions, smooth pursuit, optokinetic reflex, and visual control of the VOR usually show the same degree of impairment. In lateral medullary syndrome, impaired smooth pursuit toward the opposite side of the lesion is observed [7,8]. A brainstem lesion at the caudal level can cause a reduction in the gain of the contralateral direct smooth pursuit, while the ipsilateral slow movements are preserved [67]. In 12 patients with ventromedial pontine infarction, 7 had pursuit with saccadic substitutions but only two of them had vertigo [68]. An asymmetric alteration of pursuit, which is normal in one direction and low gain in the other, may be suggestive of cerebellar or brainstem lesion, while the bilateral and symmetric alteration is nonspecific for location [67,68]. Other regions in the brainstem may cause abnormalities in smooth pursuit if infarcted, but smooth pursuit deficits are commonly overshadowed by other more significant neurologic deficits.
Saccades are responsible for rapidly moving the gaze from one fixation point to another; abnormalities of accuracy, latency and velocity of saccades such as intrusion and saccadic oscillation can occur involuntarily in pathological conditions [1]. The riMLF and PPRF burst neurons affect the velocity and initiation of saccades in vertical and horizontal directions, respectively. This phenomenon can be caused by lesions in various structures such as the cerebellum, brainstem, basal ganglia, and cerebral hemispheres, and it prevents the gaze from staying in one place. A decrease in the speed or absence of saccadic movements in horizontal plane is instead typical of the brainstem, due to lesions affecting the MLF or the PPRF [7,8,17,18,19]. Hypermetric saccades to the side of the lesion, hypometric to the other side are typically encountered in Wallemberg syndrome and this pattern of saccadic abnormalities associate with ocular ipsipulsion is highly localizing for this syndrome [2,29,44]. The far less common medial medullary lesion could produce an opposite pattern: ipsilesional saccadic hypometria and contralesional hypermetric saccades, sometimes associated with ocular lateropulsion [9]. In milder cases of INO, patients may only demonstrate slowed adducting saccades, so-called adduction lag [69]. As already described a midbrain lesion produces an isolated vertical saccadic paresis sometimes associated with isolated vertical GEN [29,30,31]. A combination of ipsilesional hypometric saccades, contralesional saccadic smooth pursuit, and unilateral gaze-evoked nystagmus has been considered as typical of a focal brainstem (pontine) lesion [70].
4.4. Ocular Tilt Reaction (OTR)
The otolithic pathways that mediate modulate the VOR originate from the utricular and saccular maculae and project to the ipsilateral vestibular nuclei at the pontine-medullary junction. This pathway then decussates to the contralateral side at pontine level to reach the pons and midbrain in the MLF until to the supranuclear centers for vertical-torsional eye movements in the rostral midbrain (riMLF and INC which activity not only generate vertical and torsional saccades but also acts as the neural integrator for vertical and torsional gaze holding) [71,72]. A lesion along this pathway (from the peripheral organ to the supratentorial structures) determinates the so-called Ocular Tilt Reaction (OTR) consisting of SD, ocular torsion, head tilt, and deviation of the subjective visual vertical, all tilted toward the lower (hypotropic) eye [71]:
- Skew deviation is a vertical misalignment of the eyes due to unilateral impairment of the otolith-ocular reflex. Hypotropia of the eye (on the side of the lesion if the damage affects the peripheral receptor and/or the pathways before their crossing, contralaterally in case of deficit after the commissure) (Figure 5)
- Ocular torsion (in the case of the right labyrinth, counterclockwise torsion from the viewer point of view in case of pre-decussation lesion, clockwise in case of post-decussation lesion)
- Head tilt (to the side of the lesion if the damage affects the peripheral receptor and/or the pathways before their crossing, contralaterally in case of deficit after the commissure).
The pathway for the otolithic ocular responses decussates in the pons: hence static ocular tilt reactions from hypofunction are ipsiversive (lower eye on the side of the lesion) with peripheral vestibular and pontomedullary lesions and contraversive with ponto-mesencephalic lesions [71,72,73] (Figure 6). Whereas most cases of OTR are tonic and due to a decrease in tonic neural activity, paroxysmal OTR is due to intermittent unilateral hyperfunction, with tilt in the direction opposite to that of tonic ocular tilt reactions. A paroxysmal OTR was described in case of upper brainstem lesions [74,75]. In presence of an acute spontaneous vertigo, evaluating SD in bedside examination as part of HINTS paradigm is a crucial sign for differential diagnosis between a peripheral or central vestibular disease: usually large amplitude SD points to a central lesion [76,77]. For this latter purpose, when spontaneous horizontal nystagmus is associated OTR, a correlation between nystagmus direction and SD could provide additional useful information. If the nystagmus has the fast phase away from the hypertropic eye (called UPHILL nystagmus) this could be considered a peripheral marker; on the contrary if the nystagmus is towards the hypotropic eye (called DOWNHILL) this could be considered as a central marker [78].
4.2.2.1. Spontaneous Acquired Nystagmus in Brainstem Lesion
Downbeat Nystagmus (DBN) is the most common form of acquired central nystagmus. Usually, the fast phase beat in a downward direction and it increase when looking down and in lateral gaze with associated static and dynamic postural instability and, sometimes, oscillopsia [79,80]. Although DBN is mostly due to a cerebellar disease (especially flocculus lesion [1,79]), some individual cases of DBN were described in case of paramedian lesions of the medulla oblongata [14,15,79,80] or from vascular pathologies such as dolichoectasia of the vertebro-basilar circulation and compression of the vertebral artery [81,82]. Upbeat Nystagmus (UBN) is a type of central vestibular nystagmus that is less common than DBN. UBN usually increases with upward gaze, and it is associated with impaired upward pursuit; usually, it does not increase on lateral gaze and may evolve into downbeat nystagmus with convergence [1,16]. UBN can be observed only during the acute stage of illness and resolved earlier than other ocular motor abnormalities [83]. Another very peculiar feature of UBN is its possible spontaneous transformation, in the course of the disease, into a hemi-seesaw, horizontal, and above all DBN [84]. Although the exact mechanisms remain to be elucidated, it is believed that critical structures for UBN is located at the midline in the lower medulla (ventral tegmental tract, the superior vestibular nucleus, the nucleus of Roller and the solitary nucleus) [14,80]. UBN occurs as a result of lesions in various locations and is often seen associated with pontomedullary and pontomesencehalic lesions [7,80,83] and in contrast to downbeat nystagmus, lesions of the paramedian brainstem are frequent in upbeat nystagmus [9,84,85,86]; usually UBN is associated with other brainstem signs, such as ataxia or dysarthria [85]. Torsional nystagmus (TN) often occurs as a consequence of pontomedullary junction lesions [87]. Primarily TN arises from lesions in neural pathways involved in controlling torsional movements: the medulla (vestibular nuclei) and midbrain (INC and riMLF) [87]. Disruption of the otolithic–ocular pathways cause unbalanced torsional inputs to the ocular motor nuclei, leading to rotation of the eyes around the visual axis. TN especially if isolated, suggests brainstem or vestibular nucleus lesions (e.g. Wallenberg syndrome [6,88], lesion of MLF and/or ICP [12,13]) and often coexists with vertical or gaze-evoked components [87]. Gaze Evoked Nystagmus (GEN) arise from an impairment of the cerebellar-brainstem mediated horizontal or vertical gaze-holding mechanism [29] inducing an inability to hold the eyes in a position of eccentric fixation. Horizontal GEN is a central sign with an excellent specificity [26] and, when combined with testing for other oculomotor signs (SD, HIT), is very useful in order to diagnose a central vestibular lesion in patients with acute vertigo [35,36,37,38,39,40]. Unlike end-point nystagmus (a benign finding, conjugate, in both right and left directions of gaze, transient, more prominent with age), GEN is sustained, larger in amplitude, possibly asymmetric, and is often associated with DBN. GEN is frequently correlated to cerebellar diseases, but it is a common finding in case of medial medullary infarction [9] and in unilateral lesions of NPH [10] and it was also described in pontine lesions [1]. On the other hand, a vertical GEN because of an involvement of the pontine areas connected by the medial longitudinal fascicule (MLF) to the midbrain area involved with vertical gaze [19]. Other rare types of nystagmus encountered in brainstem lesions are Seesaw nystagmus: seesaw nystagmus refer to mixed torsional–vertical nystagmus with one eye moving upward and incyclorotates, and the other eye moves downward and excyclorotates. During the next half cycle, the vertical and torsional movements reverse. Hemi seesaw nystagmus is a jerky nystagmus in which the slow phase corresponds to one-half cycle and the quick phase to the other [1,89] and it can be a finding of a medial [84] or lateral [89] medullary syndrome and midbrain lesion [90]. Periodic Alternating nystagmus is a horizontal, conjugate, jerk nystagmus that periodically alternates its direction of fast phase. It is a very rare finding in brainstem lesion, and it was described occasionally in lesion involving area of the central-dorsal medulla, including the bilateral NPH [91]. Acquired Pendular Nystagmus is characterized by slow-phase eye movements in the horizontal, vertical, and torsional planes, resulting in nearly sinusoidal movement. This nystagmus, commonly associated with oculo-palatal tremor, is related to an abnormal activity in central gaze-holding structures (NPI, medial vestibular nuclei, and INC92), especially induced by multiple sclerosis [20,93] and, less frequently by other diseases affecting the brainstem [94]. Convergence-retraction nystagmus is the most characteristic clinical sign of dorsal lesions of the rostral midbrain: this nystagmus consists in rapid inward-outward movement of the eye, followed by a slow return movement of protrusion and divergence when the patient is asked to look upward. It may be associated with upward gaze palsy in Parinaud syndrome [1,95]. In the context of the so called “nystagmoid movements” we must remember the ocular flutter, characterized by are rapid, short-duration ocular oscillations on the horizontal plane that appear spontaneously during fixation and end abruptly. Ocular flutter is often triggered by blinking or voluntary eye movements. This condition reflects dysfunction in saccade-generating brainstem circuits, especially the PPRF and cerebellar fastigial nucleus [96]. Ocular bobbing is a vertical nystagmoid movement characterized by rapid downward eye jerks followed by slow upward drifts and is typically associated with lesions in the PPRF in ventral pons where omnipause neurons disrupts saccadic inhibition, allowing uncontrolled vertical saccades [97].
5. Conclusions
Besides its several physiological functions of vital importance, the brainstem represents a structure of prominent importance for the generation and control of eye movements (saccades, smooth pursuit, the vestibulo-ocular reflex, VOR, vergence and gaze holding). The clinical examination of the different eye movements and nystagmus allows in most cases topographic-anatomic diagnosis of central vestibular lesions due to brainstem abnormalities both in degenerative and progressive diseases and in acute (vascular) disorders [98]. As a general rule, isolated impairments of vertical eye movements (in addition to pupillary and eyelid abnormalities) are indicative of a midbrain damage, while isolated impairments of horizontal eye movements are more typical of a lesion in the pons [2,4,98]. However, oculomotor abnormalities arising from brainstem disease constitute an extremely complex challenge for the otoneurologist by virtue of the remarkable diversity of causes (vascular, traumatic, degenerative, neoplastic) of their variable severity, of their clinical course (acute, fluctuating or progressive) and finally by virtue of concomitant involvement of other central structures (mainly cerebellum). For these reasons, eye movement disorders and nystagmus of brainstem origin are frequently associated not only with vertigo and imbalance but with a wide range of other neurological signs. Consequently, an accurate characterization of the eye movement anomalies represents a fundamental moment in the diagnosis of central vestibular syndromes, being also able to identify and localize, at least in a good number of cases, the role of each unit and/or neural circuit in the genesis of the oculomotor lesion.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Video S1: torsional spontaneous nystagmus in patient with multiple sclerosis involving the interior cerebellar peduncle. Video S2: patient suffering from positional vertigo. Bedside examination: apogeotropic bidirectional persistent positional nystagmus refractory to repeated repositioning maneuver.
Author Contributions
Conceptualization, methodology, resources, writing—original draft preparation, writing—review and editing A.P.C.; methodology, resources, writing—original draft preparation M.G.; writing—original draft preparation, N.D.; and conceptualization, validation, writing—review and editing G.A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
this a review involving previous published study so Ethical review and approval were waived for this study.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VOR | Vestibulo-Ocular Reflex |
| NPH | Nucleus propositus Hypoglossi |
| NR | Nucleus of Roller |
| OTR | Ocular Tilt Reaction |
| PPRF | Paramedian Pontine Reticular Formation |
| GEN | Gaze Evoked Nystagmus |
| HSN | Head Shaking Nystagmus |
| SP | Smooth Pursuit |
| MLF | Medial Longitudinal Fascicle |
| INO | Internuclear Ophthalmoplegia |
| SD | Skew Deviation |
| riMLF | rostral interstitial Nucleus of the Medial Longitudinal Fasciculus |
| PICA | Posterior-Inferior Cerebellar Artery |
| AICA | Anterior-Inferior Cerebellar Artery |
| ICP | Inferior Cerebellar peduncle |
| MRI | Magnetic Resonance Imaging |
| HIT | Head Impulse Test |
| CNP | Central Positional Nystagmus |
| PDN | Positional Downbeating Nystagmus |
| BPPV | Benign Paroxysmal Positional Vertigo |
| DBN | Downbeat Nystagmus |
| UBN | Upbeat Nystagmus |
| TN | Torsional Nystagmus |
References
- Leigh, R.J.; Zee, D.S. The Neurology of Eye Movements, 5th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Strupp, M.; Hüfner, K.; Sandmann, R.; Zwergal, A.; Dieterich, M.; Jahn, K.; Brandt, T. Central oculomotor disturbances and nystagmus: A window into the brainstem and cerebellum. Dtsch Arztebl Int 2011, 108, 197–204. [Google Scholar]
- Dieterich, M. Central vestibular disorders. J Neurol 2007, 254, 559–568. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, H.J.; Kim, J.S. Ocular motor dysfunction due to brainstem disorders. J Neuroophthalmol 2018, 13, 393–412. [Google Scholar] [CrossRef]
- Brandt, T.; Dieterich, M. The dizzy patient: Don’t forget disorders of the central vestibular system. Nat Rev Neurol 2017, 13, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Kattah, J.C.; Saber Tehrani, A.S.; Roeber, S.; Gujrati, M.; Bach, S.E.; Newman Toker, D.E.; Blitz, A.M.; Horn, A.K.E. Transient Vestibulopathy in Wallenberg’s Syndrome: Pathologic Analysis. Front. Neurol. 2017, 8, 191. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.Y.; Gold, D.R. Ocular Motor and Vestibular Disorders in Brainstem Disease. J Clin Neurophysiol 2019, 36, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, M.; Brandt, T. Wallenberg’s syndrome: Lateropulsion, cyclorotation, and subjective visual vertical in thirty-six patients. Ann Neurol 1992, 31, 399–408. [Google Scholar] [CrossRef]
- Kim, J.S.; Moon, S.Y.; Kim, K.Y.; Kim, H.C.; Park, S.H.; Yoon, B.W.; Roh, J.K. Ocular contrapulsion in rostral medial medullary infarction. Neurology 2004, 63, 1325–1327. [Google Scholar] [CrossRef]
- Kim, S.H.; Zee, D.S.; Du Lac, S.; Kim, H.J.; Kim, J.S. Nucleus prepositus hypoglossi lesions produce a unique ocular motor syndrome. Neurology 2016, 87, 2026–2033. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kim, H.J.; Kim, J.S. Recent advances in head impulse test findings in central vestibular disorders. Neurology 2018, 90, 602–612. [Google Scholar] [CrossRef]
- Choi, J.H.; Seo, J.D.; Choi, Y.R.; Kim, M.J.; Kim, H.J.; Kim, J.S.; Choi, K.D. Inferior cerebellar peduncular lesion causes a distinct vestibular syndrome. Eur J Neurol 2015, 22, 1062–1067. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, S.H.; Kim, H.J.; Kim, J.S. Isolated central vestibular syndrome. Ann New York Acad Sci 2015, 1343, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Pierrot Deseilligny, C.; Milea, D. Vertical nystagmus: Clinical facts and hypotheses. Brain 2005, 128, 1237–1246. [Google Scholar] [CrossRef]
- Nakamagoe, K.; Shimizu, K.; Koganezawa, T.; Tamaoka, A. Downbeat nystagmus due to a paramedian medullary lesion. J Clin Neurosci 2012, 19, 1597–1599. [Google Scholar] [CrossRef]
- Marcelli, V.; Giannoni, B.; Volpe, G.; Faralli, M.; Marcelli, E.; Cavaliere, M.; Fetoni, A.R.; Pettorossi, V.E. Upbeat nystagmus: A clinical and pathophysiological review. Front Neurol 2025, 16, 1601434. [Google Scholar] [CrossRef]
- Geiner, S.; Horn, A.K.; Wadia, N.H.; Sakai, H.; Buttner-Ennever, J.A. The neuroanatomical basis of slow saccades in spinocerebellar ataxia type 2 (Wadia-subtype). Prog Brain Res 2008, 171, 575–581. [Google Scholar]
- Nishida, T.; Tychsen, L.; Corbett, J.J. Resolution of saccadic palsy after treatment of brain-stem metastasis. Arch Neurol 1986, 43, 1196–1197. [Google Scholar] [CrossRef] [PubMed]
- Bhidayasiri, R.; Plant, G.T.; Leigh, R.J. A hypothetical scheme for the brainstem control of vertical gaze. Neurology 2000, 54, 1985–1993. [Google Scholar] [CrossRef] [PubMed]
- Frohman, E.M.; Frohman, T.C.; Zee, D.S.; McColl, R.; Galetta, S. The neuro-ophthalmology of multiple sclerosis. Lancet Neurol 2005, 4, 111–121. [Google Scholar] [CrossRef]
- Zwergal, A.; Cnyrim, C.; Arbusow, V.; Glaser, M.; Fesl, G.; Brandt, T.; Strupp, M. Unilateral INO is associated with ocular tilt reaction in pontomesencephalic lesions: INO plus. Neurology 2008, 71, 590–593. [Google Scholar] [CrossRef]
- Lee, S.U.; Kim, H.J.; Kim, J.S. Evolution of symmetric upbeat into dissociated torsional-upbeat nystagmus in internuclear ophthalmoplegia. Clin Neurol Neurosurg 2013, 115, 1882–1884. [Google Scholar]
- Prasad, S.; Galetta, S.L. Eye movement abnormalities in multiple sclerosis. Neurol Clin 2010, 28, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S. Internuclear ophthalmoplegia as an isolated or predominant symptom of brainstem infarction. Neurology 2004, 62.9, 1491–1496. [Google Scholar] [CrossRef]
- de Seze, J.; Lucas, C.; Leclerc, X.; Sahli, A.; Vermersch, P.; Leys, D. One-and-a-half syndrome in pontine infarcts: MRI correlates. Neuroradiology 1999, 41, 666–669. [Google Scholar] [CrossRef]
- Bronstein, A.M.; Rudge, P.; Gresty, M.A.; Du Boulay, G.; Morris, J. Abnormalities of horizontal gaze. Clinical, oculographic and magnetic resonance imaging findings. II. Gaze palsy and internuclear ophthalmoplegia. J Neurol Neurosurg Psych 1990, 53, 200–207. [Google Scholar] [CrossRef]
- Xue, F.; Zhang, L.; Zhang, L.; Ying, Z.; Sha, O.; Ding, Y. One-and-a-half syndrome with its spectrum disorders. Quantitative imaging in medicine and surgery 2017, 7, 691. [Google Scholar] [CrossRef]
- Takahashi, M.; Sugiuchi, Y.; Shinoda, Y. Brainstem neural circuits triggering vertical saccades and fixation. Journal of Neuroscience 2024, 44, 1. [Google Scholar]
- Strupp, M.; Kremmyda, O.; Adamczyk, C.; Böttcher, N.; Muth, C.; Yip, C.W.; Bremova, T. Central ocular motor disorders, including gaze palsy and nystagmus. J. Neurol 2014, 261, 542–558. [Google Scholar] [CrossRef]
- Suzuki, Y.; Buttner-Ennever, J.A.; Straumann, D.; Hepp, K.; Hess, B.J.; Henn, V. Deficits in torsional and vertical rapid eye movements and shift of listing’s plane after uni- and bilateral lesions of the rostral interstitial nucleus of the medial longitudinal fasciculus. Exp Brain Res 1995, 106, 215–232. [Google Scholar]
- Helmchen, C.; Rambold, H.; Fuhry, L.; Büttner, U. Deficits in vertical and torsional eye movements after uni- and bilateral muscimol inactivation of the interstitial nucleus of Cajal of the alert monkey. Exp. Brain Res 1998, 119, 436–452. [Google Scholar]
- Helmchen, C.; Rambold, H.; Kempermann, U.; Buttner-Ennever, J.A.; Buttner, U. Localizing value of torsional nystagmus in small midbrain lesions. Neurolog. 2002, 59, 1956–1964. [Google Scholar] [CrossRef]
- Merwick, A.; Werring, D. Posterior circulation ischaemic stroke. Bmj 2014, 348, g3175. [Google Scholar] [CrossRef]
- Kerber, K.A.; Meurer, W.J.; Brown, D.L.; Burke, J.F.; Hofer, T.P.; Tsodikov, A.; Hoeffner, E.G.; Fendrick, A.M.; Adelman, E.E.; Morgenstern, L.B. Stroke risk stratification in acute dizziness presentations: A prospective imaging-based study. Neurology 2015, 85, 1869–1878. [Google Scholar] [CrossRef] [PubMed]
- Tarnutzer, A.A.; Berkowitz, A.L.; Robinson, K.A.; Hsieh, Y.H.; Newman-Toker, D.E. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ 2011, 183, E571–E592. [Google Scholar] [CrossRef] [PubMed]
- Saber Tehrani, A.S.; Kattah, J.C.; Kerber, K.A.; Gold, D.R.; Zee, D.S.; Urrutia, V.C.; Newman-Toker, D.E. Diagnosing Stroke in Acute Dizziness and Vertigo: Pitfalls and Pearls. Stroke 2018, 49, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Vanni, S.; Vannucchi, P.; Pecci, R.; Pepe, G.; Paciaroni, M.; Pavellini, A.; Ronchetti, M.; Pelagatti, L.; Bartolucci, M.; Konze, A.; Castellucci, A.; Manfrin, M.; Fabbri, A.; de Iaco, F.; Casani, A.P. Consensus paper on the management of acute isolated vertigo in the emergency department. Intern. Emerg. Med 2024, 19, 1181–1202. [Google Scholar] [CrossRef]
- Cnyrim, C.D.; Newman-Toker, D.; Karch, C.; Brandt, T.; Strupp, M. Bedside differentiation of vestibular neuritis from central “vestibular pseudoneuritis”. J Neurol Neurosurg Psych 2008, 79, 458–460. [Google Scholar] [CrossRef]
- Kattah, J.C.; Talkad, A.V.; Wang, D.Z.; Hsieh, Y.H.; Newman-Toker, D.E. HINTS to diagnose stroke in the acute vestibular syndrome: Three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke 2009, 2009 40, 3504–3510. [Google Scholar] [CrossRef]
- Edlow, J.A. Distinguishing Peripheral from Central Causes of Dizziness and Vertigo without using HINTS or STANDING J Emerg Med 2024, 67, e622–e633. 67 2024, 67, e622–e633. [Google Scholar]
- Carmona, S.; Martinez, C.; Zalazar, G.; Moro, M.; Batuecas-Caletrio, A.; Luis, L.; Gordon, C. The Diagnostic Accuracy of Truncal Ataxia and HINTS as Cardinal Signs for Acute Vestibular Syndrome. Front. Neurol 2016, 7, 125. [Google Scholar] [CrossRef]
- Tarnutzer, A.A.; Edlow, J.A. Bedside Testing in Acute Vestibular Syndrome—Evaluating HINTS Plus and Beyond—A Critical Review. Audiol. Res 2023, 13, 670–685. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sohn, S.I.; Cho, Y.W.; Lee, S.R.; Ahn, B.H.; Park, B.R.; Baloh, R.W. Cerebellar infarction presenting isolated vertigo: Frequency and vascular topographical patterns. Neurology 2006, 67, 1178–1183. [Google Scholar] [CrossRef]
- Baloh, R.W.; Yee, R.D.; Honrubia, V. Eye movements in patients with Wallenberg’s syndrome. Ann NY Acad.Sci 1981, 374, 600–613. [Google Scholar] [CrossRef]
- Kumral, E.; Bayulkem, G.; Evyapan, D. Clinical spectrum of pontine infarction: Clinical—MRI correlations. J. Neurol 2002, 249, 1659–1670. [Google Scholar] [CrossRef]
- Frohman, E.M.; Frohman, T.C.; Fleckenstein, J.; Racke, M.K.; Hawker, K.; Kramer, P.D. Ocular contrapulsion in multiple sclerosis: Clinical features and pathophysiological mechanisms. J Neurol Neurosurg Psych 2001, 70, 688–692. [Google Scholar] [CrossRef]
- Lemos, J.; Strupp, M. Central positional nystagmus: An update. J Neurol 2021, 269.4, 1851–1860. [Google Scholar] [CrossRef]
- Kim, J.M.; Lee, S.H.; Kim, H.J.; Kim, J.S. Less talked variants of benign paroxysmal positional vertigo. J Neurol Sci 2022, 442, 120440. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Kim, J.H.; Kim, H.J.; Glasauer, S.; Kim, J.S. Central paroxysmal positional nystagmus: Characteristics and possible mechanisms. Neurology 2015, 84, 2238–2246. [Google Scholar] [CrossRef]
- De Schutter, E.; Adham, Z.O.; Kattah, J.C. Central positional vertigo: A clinical-imaging study. Prog Brain Res 2019, 249, 345–360. [Google Scholar] [PubMed]
- Walker, M.F.; Tian, J.; Shan, X.; Tamargo, R.J.; Ying, H.; Zee, D.S. The cerebellar nodulus/uvula integrates otolith signals for the translational vestibulo-ocular reflex. PLoS ONE 2010, 5, e13981. [Google Scholar] [CrossRef]
- Macdonald, N.K.; Kaski, D.; Saman, Y.; Sulaiman, A.A.-S.; Anwer, A.; Bamiou, D.E. Central Positional Nystagmus: A Systematic Literature Review. Front Neurol 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.U.; Kim, H.J.; Lee, E.S.; Choi, J.H.; Choi, J.Y.; Kim, J.S. Central positional nystagmus in inferior cerebellar peduncle lesions: A case series. J Neurol 2021, 268, 2851–2857. [Google Scholar] [CrossRef]
- Buttner, U.; Helmchen, C.; Brandt, T. Diagnostic Criteria for Central Versus Peripheral Positioning Nystagmus and Vertigo: A Review. Acta Otolaryngol. 1999, 119, 1–5. [Google Scholar]
- Imai, T.; Horii, A.; Takeda, N.; Higashi-Shingai, K.; Inohara, H. A case of apogeotropic nystagmus with brainstem lesion: An implication for mechanism of central apogeotropic nystagmus. Auris Nasus Larynx 2010, 37, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Califano, L.; Mazzone, S.; Salafia, F.; Melillo, M.G.; Manna, G. Less common forms of posterior canal benign paroxysmal positional vertigo. Acta Otorhinolaryngol Ital 2021, 41, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Casani, A.P.; Cerchiai, N.; Dallan, I.; Sellari-Franceschini, S. Anterior canal lithiasis: Diagnosis and treatment. Otolaryngol Head Neck Surg 2011, 144, 412–418. [Google Scholar] [CrossRef]
- Yacovino, D.A.; Cherchi, M. Clinical spectrum of positional downbeat nystagmus: A diagnostic approach. J Neurol 2025, 272, 163. [Google Scholar] [CrossRef]
- Kwon, E.; Jeong, H.S.; Jeong, S.H.; Kim, H.J.; Kim, J.S. Central paroxysmal positional nystagmus mimicking posterior canal benign paroxysmal positional vertigo in pontine infarction: A case report and literature review. J Neurol 2024, 271, 3672–3677. [Google Scholar] [CrossRef]
- Kim, H.A.; Lee, H.; Sohn, S.I.; Kim, J.S.; Baloh, R.W. Perverted head shaking nystagmus in focal pontine infarction. J Neurol Sci 2011, 301, 93–95. [Google Scholar] [CrossRef]
- Hain, T.C.; Spindler, J. Head-shaking nystagmus. In The Vestibulo-Ocular Reflex and Vertigo; Sharpe, J.A., Barber, H.O., Eds.; Raven Press: New York, NY, USA, 1993; pp. 217–228. [Google Scholar]
- Choi, K.D.; Oh, S.Y.; Park, S.H.; Kim, J.H.; Koo, J.W.; Kim, J.S. Head-shaking nystagmus in lateral medullary infarction: Patterns and possible mechanisms. Neurology 2007, 68, 1337–1344. [Google Scholar] [CrossRef]
- Minagar, A.; Sheremata, W.A.; Tusa, R.J. Perverted head-shaking nystagmus: A possible mechanism. Neurology 2001, 57, 887–889. [Google Scholar] [CrossRef]
- Kim, H.A.; Lee, H.; Sohn, S.I.; Kim, J.S.; Baloh, R.W. Perverted head shaking nystagmus in focal pontine infarction. J Neurol Sci 2011, 301, 93–95. [Google Scholar] [CrossRef]
- Choi, J.Y.; Jung, I.; Jung, J.M.; Kwon, D.Y.; Park, M.H.; Kim, H.J.; Kim, J.S. Characteristics and mechanism of perverted head-shaking nystagmus in central lesions: Video-oculography analysis. Clin Neurophysiol 2016, 127, 2973–2978. [Google Scholar] [CrossRef]
- Kim, M.B.; Boo, S.H.; Ban, J.H. Nystagmus-based approach to vertebrobasilar stroke presenting as vertigo without initial neurologic signs. Eur Neurol 2013, 70, 322–328. [Google Scholar] [CrossRef]
- Johnston, J.L.; Sharpe, J.A.; Morrow, M.J. Paresis of contralateral smooth pursuit and normal vestibular smooth eye movements after unilateral brainstem lesions. Ann Neurol 1992, 31, 495–502. [Google Scholar] [CrossRef]
- Fracica, E.; Hale, D.; Gold, D.R. Diagnosing and localizing the acute vestibular syndrome–beyond the HINTS exam. J NeurolSci 2022, 442, 120451. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, J.M.; Kim, J.S. Update on the medial longitudinal fasciculus syndrome. Neurol Sci 2022, 43, 3533–3540. [Google Scholar] [CrossRef]
- Bianchi, F.; Vidailhet, M.; Gaymard, B. Ipsilateral Saccade Hypometria and Contralateral Saccadic Pursuit in a Focal Brainstem Lesion: A Rare Oculomotor Pattern. Cerebellum 2018, 17, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Brandt, T.; Dieterich, M. Vestibular syndromes in the roll plane: Topographic diagnosis from brainstem to cortex. Ann Neurol 1994, 36, 337–347. [Google Scholar] [CrossRef]
- Brodsky, M.C.; Donahue, S.P.; Vaphiades, M.; Brandt, T. Skew deviation revisited. Surv Ophthalmol 2006, 51, 105–128. [Google Scholar] [CrossRef] [PubMed]
- Halmagyi, G.; Brandt, T.; Dieterich, M.; Curthoys, I.; Stark, R.; Hoyt, W. Tonic contraversive ocular tilt reaction due to unilateral meso-diencephalic lesion. Neurology 1990, 40, 1503–1509. [Google Scholar] [CrossRef]
- Hedges, T.R.D.; Hoyt, W.F. Ocular tilt reaction due to an upper brainstem lesion: Paroxysmal skew deviation, torsion, and oscillation of the eyes with head tilt. Ann Neurol 1982, 11, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.R.; Egan, R.A.; Barton, J.J. Pearls & Oy-sters: Paroxysmal ocular tilt reaction. Neurology 2009, 72, e67–e68. [Google Scholar] [CrossRef]
- Kattah, J.C. Update on HINTS Plus, With Discussion of Pitfalls and Pearls. J Neurol Phys Ther 2019, 43, S42–S45. [Google Scholar] [CrossRef]
- Korda, A.; Zamaro, E.; Wagner, F.; Morrison, M.; Caversaccio, M.D.; Sauter, T.C.; Schneider, E.; Mantokoudis, G. Acute vestibular syndrome: Is skew deviation a central sign? J Neurol 2022, 269, 1396–1403. [Google Scholar] [CrossRef]
- Gufoni, M. Uphill/downhill nystagmus. Acta Otorhinolaryngol Ital 2017, 37, 513–518. [Google Scholar] [CrossRef]
- Wagner, J.N.; Glaser, M.; Brandt, T.; Strupp, M. Downbeat nystagmus: Aetiology and comorbidity in 117 patients. J Neurol Neurosurg Psych 2008, 79, 672–677. [Google Scholar] [CrossRef]
- Marcelli, V.; Giannoni, B.; Volpe, G.; Faralli, M.; Fetoni, A.R.; Pettorossi, V.E. Downbeat nystagmus: A clinical and pathophysiological review. Front Neurol 2024, 15, 1394859. [Google Scholar] [CrossRef] [PubMed]
- Himi, T.; Kataura, A.; Tokuda, S.; Sumi, Y.; Kamiyama, K.; Shitamichi, M. Downbeat nystagmus with compression of the medulla oblongata by the dolichoectatic vertebral arteries. Am J Otol 1995, 16, 377–81. [Google Scholar]
- Rosengart, A.; Hedges, T.R., 3rd; Teal, P.A.; DeWitt, L.D.; Wu, J.K.; Wolpert, S.; Caplan, L.R. Intermittent downbeat nystagmus due to vertebral artery compression. Neurology 1993, 43, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Yoon, B.; Choi, K.D.; Oh, S.Y.; Park, S.H.; Kim, B.K. Upbeat nystagmus: Clinicoanatomical correlations in 15 patients. J Clin Neurol 2006, 2, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.D.; Jung, D.S.; Park, K.P.; Jo, J.W.; Kim, J.S. Bowtie and upbeat nystagmus evolving into hemi-seesaw nystagmus in medial medullary infarction: Possible anatomic mechanisms. Neurology 2004, 62, 663–665. [Google Scholar] [CrossRef]
- Hirose, G.; Ogasawara, T.; Shirakawa, T.; Kawada, J.; Kataoka, S.; Yoshioka, A.; Halmagyi, G.M. Primary position upbeat nystagmus due to unilateral medial medullary infarction. Ann Neurol 1998, 43, 403–406. [Google Scholar] [CrossRef]
- Gilman, N.; Baloh, R.W.; Tomiyasu, U. Primary position upbeat nystagmus. Clinicopathol Study Neurol 1977, 27, 294–298. [Google Scholar] [CrossRef]
- Lopez, L.; Bronstein, A.M.; Gresty, M.A.; Rudge, P.; du Boulay, E.P. Torsional nystagmus. A neuro-otological and MRI study of thirty-five cases. Brain 1992, 115, 1107–1124. [Google Scholar] [CrossRef] [PubMed]
- Morrow, M.J.; Sharpe, J.A. Torsional nystagmus in the lateral medullary syndrome. Ann Neurol 1988, 1988 24, 390–398. [Google Scholar] [CrossRef]
- Khan, S.R.; Lueck, C.J. Hemi-seesaw nystagmus in lateral medullary syndrome. Neurology 2013, 80, 1261–1262. [Google Scholar] [CrossRef] [PubMed]
- Halmagy, G.; Aw, S.; Dehaene, I.; Curthoys, I.; Todd, M. Jerk-waveform see-saw nystagmus due to unilateral meso-diencephalic lesion. Brain 1994, 117, 789–803. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, T.; Ikeda, T.; Kikuchi, S. Periodic alternating nystagmus caused by a medullary lesion in acute disseminated encephalomyelitis. Otol Neurotol 2014, 35, 861–865. [Google Scholar] [CrossRef]
- Averbuch-Heller, L.; Zivotofsky, A.Z.; Das, V.E.; DiScenna, A.O.; Leigh, R.J. Investigations of the pathogenesis of acquired pendular nystagmus. Brain 1995, 118, 369–378. [Google Scholar] [CrossRef]
- Gresty, M.A.; Ell, J.J.; Findley, L.J. Acquired pendular nystagmus: Its characteristics, localising value and pathophysiology. J Neurol Neurosurg Psych 1982, 45, 431–439. [Google Scholar] [CrossRef]
- Kang, S.; Shaikh, A.G. Acquired pendular nystagmus. J Neurol Sci 2017, 375, 8–17. [Google Scholar] [CrossRef]
- Rambold, H.; Kömpf, D.; Helmchen, C. Convergence retraction nystagmus: A disorder of vergence? Ann Neurol 2001, 50, 677–681. [Google Scholar] [CrossRef]
- Schon, F.; Hodgson, T.L.; Mort, D.; Kennard, C. Ocular flutter associated with a localized lesion in the paramedian pontine reticular formation. Ann Neurol 2001, 50, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.P.; Gold, D.R.; Otero-Millan, J.; Huang, B.R.; Zee, D.S. Pendular oscillation and ocular bobbing after pontine hemorrhage. Cerebellum 2021, 20, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Gurnani, B.; Kaur, K.; Chaudhary, S.; Gandhi, A.S.; Balakrishnan, H.; Mishra, C.; Gosalia, H.; Dhiman, S.; Joshi, S.; Nagtode, A.H.; Jain, S.; Aguiar, M.; Rustagi, I.M. Nystagmus in Clinical Practice: From Diagnosis to Treatment—A Comprehensive Review. Clinical Ophthalmol 2025, 1617–1657. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
schematic illustration of brainstem structures involved in ocular motor control and relative consequence in case of lesion. INC: Interstitial nucleus of Cajal; MLF: medial longitudinal fascicle; NPH: nucleus propositus hypoglossi; riMLF: Rostral interstitial nucleus of the medial longitudinal fasciculus; RN: nucleus of Roller; III: oculomotor nerve; IV: trochlear nerve; VI: abducens nerve.
Figure 1.
schematic illustration of brainstem structures involved in ocular motor control and relative consequence in case of lesion. INC: Interstitial nucleus of Cajal; MLF: medial longitudinal fascicle; NPH: nucleus propositus hypoglossi; riMLF: Rostral interstitial nucleus of the medial longitudinal fasciculus; RN: nucleus of Roller; III: oculomotor nerve; IV: trochlear nerve; VI: abducens nerve.
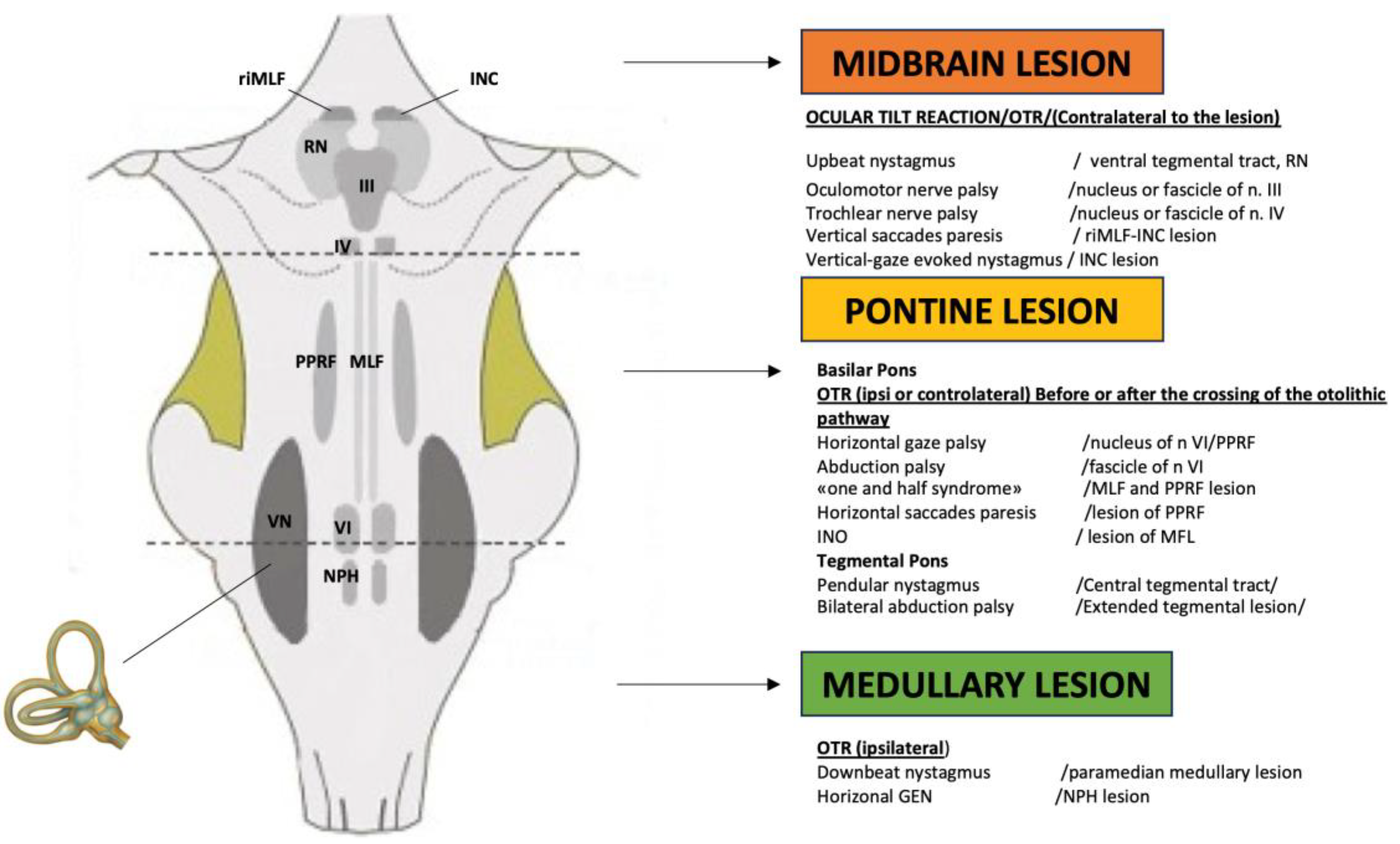
Figure 2.
Female, 46 years, complaining of acute spinning vertigo presented to the emergency room: the bedside examination reveals pure torsional nystagmus (see supplementary material); MRI reveals a demyelinating focal disorder localized in the right posterior medulla at the level of the inferior cerebellar peduncle (red circle).
Figure 2.
Female, 46 years, complaining of acute spinning vertigo presented to the emergency room: the bedside examination reveals pure torsional nystagmus (see supplementary material); MRI reveals a demyelinating focal disorder localized in the right posterior medulla at the level of the inferior cerebellar peduncle (red circle).
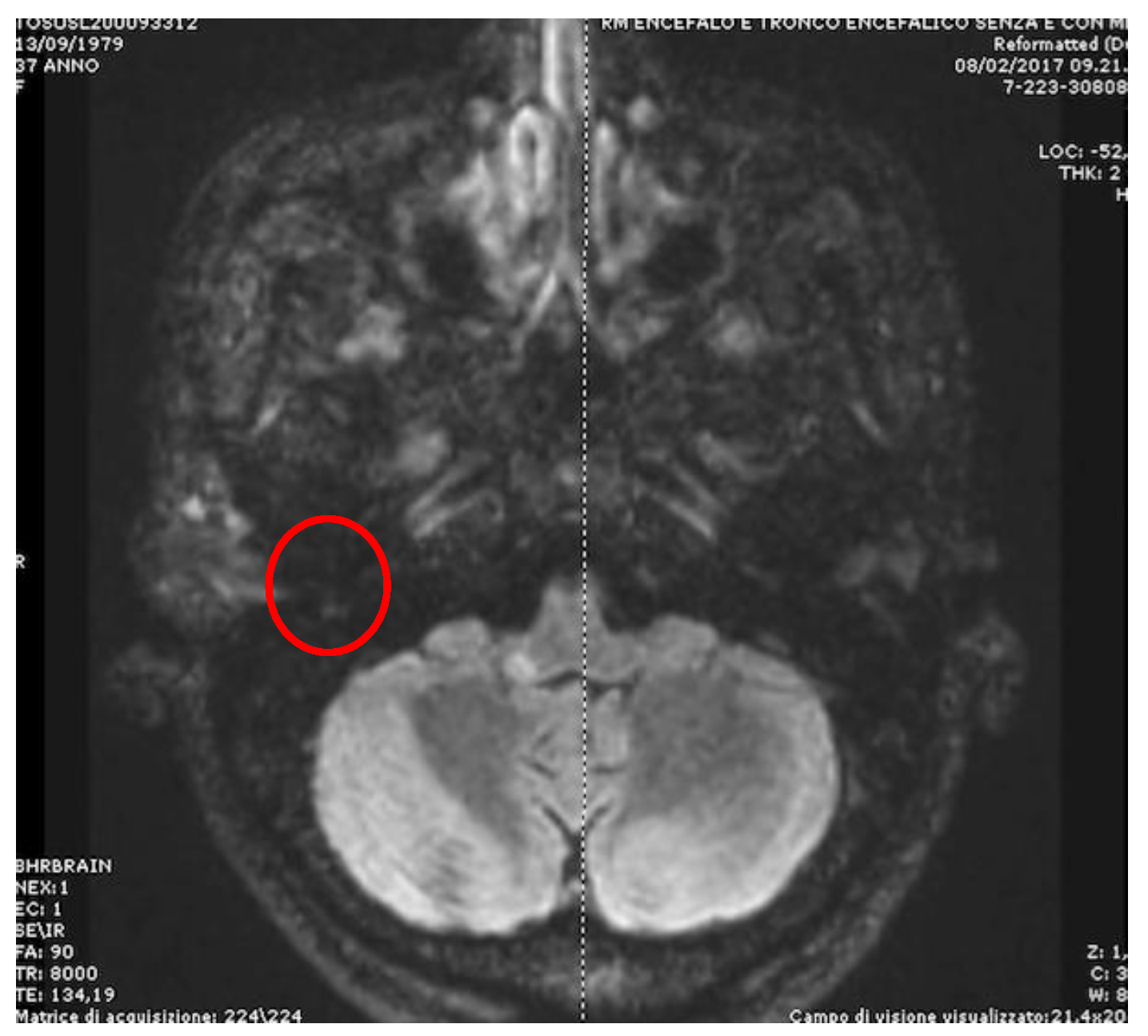
Figure 3.
right internuclear ophthalmoplegia. Primary Gaze: no ocular abnormalities. Ipsilateral gaze: normal. Contralateral gaze: no adduction in right eye and abducing nystagmus in left eye. The convergence is bilaterally preserved.
Figure 3.
right internuclear ophthalmoplegia. Primary Gaze: no ocular abnormalities. Ipsilateral gaze: normal. Contralateral gaze: no adduction in right eye and abducing nystagmus in left eye. The convergence is bilaterally preserved.
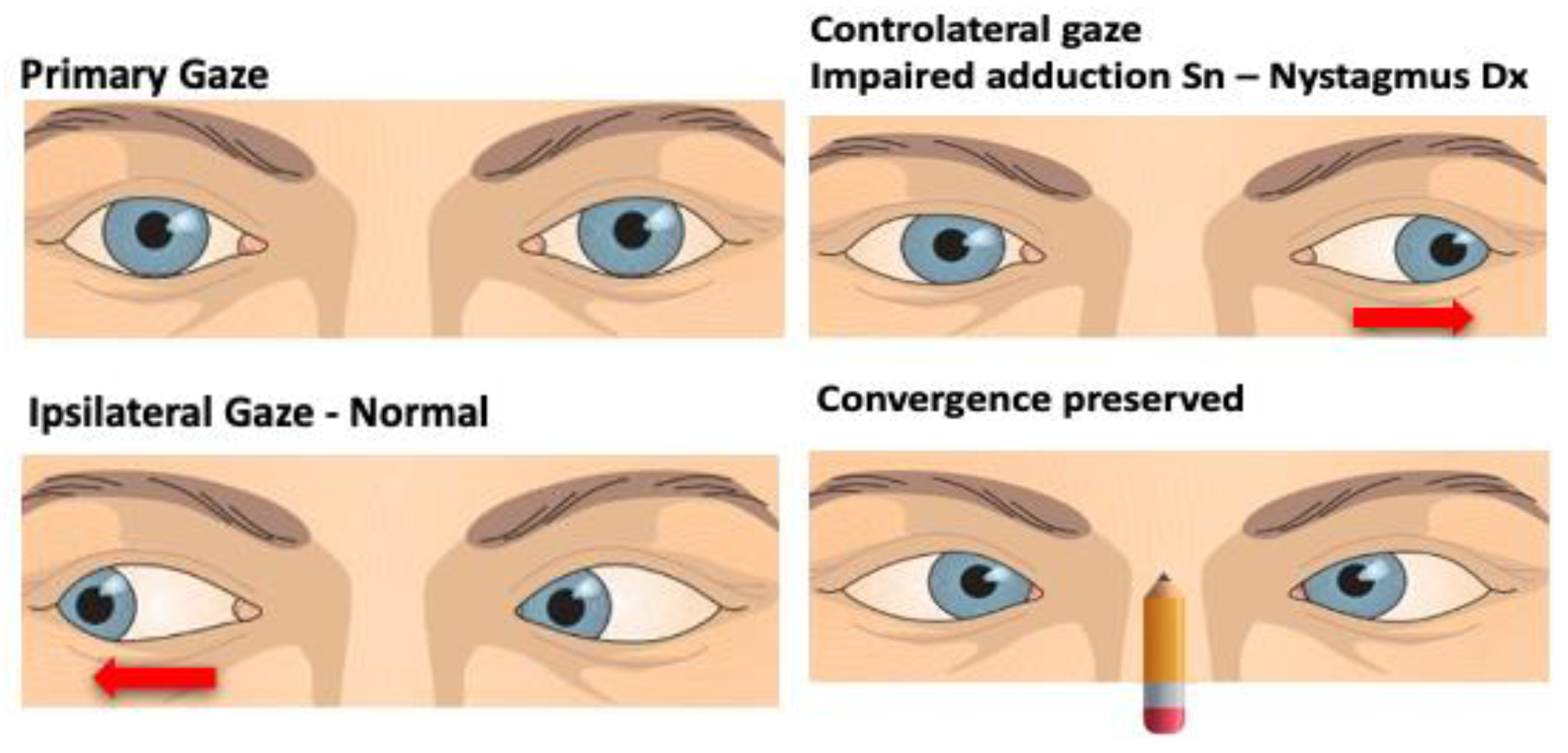
Figure 4.
male, 72 showing at bedside examination a positional bidirectional apogeotropic nystagmus (see supplementary material) not responding to repeated repositioning maneuvers. Axial MRI image shows a small vascular lesion located at medial/paramedial right center-pontine level (red circle).
Figure 4.
male, 72 showing at bedside examination a positional bidirectional apogeotropic nystagmus (see supplementary material) not responding to repeated repositioning maneuvers. Axial MRI image shows a small vascular lesion located at medial/paramedial right center-pontine level (red circle).
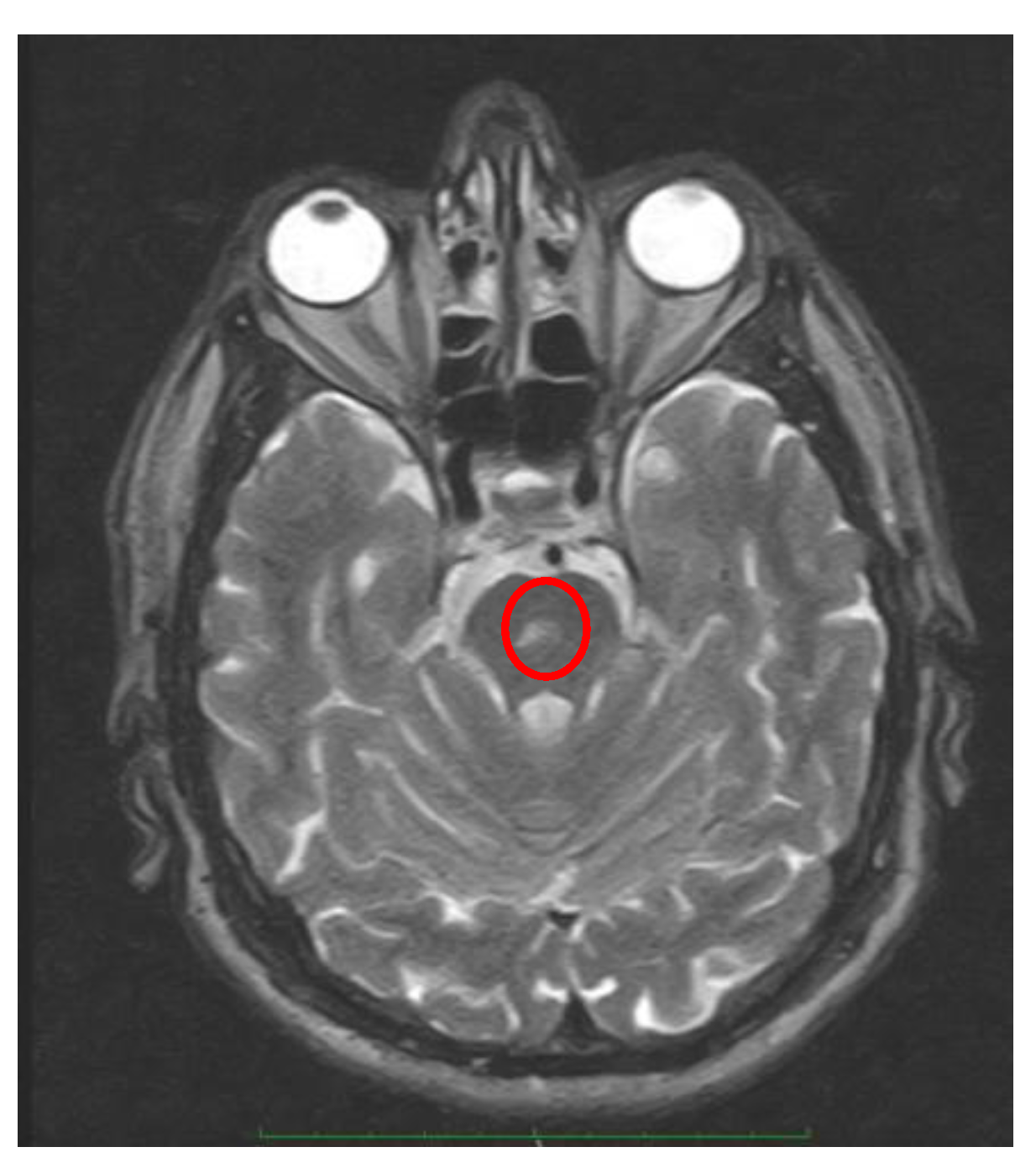
Figure 5.
Skew Deviation. The right eye is clearly higher than the left eye. The picture was taken with a tripod-mounted device with a horizontal-plane arrangement. The patient wears Frenzel glasses only to make the position of the eyes more evident, but the misalignment is clearly visible even to the naked eye.
Figure 5.
Skew Deviation. The right eye is clearly higher than the left eye. The picture was taken with a tripod-mounted device with a horizontal-plane arrangement. The patient wears Frenzel glasses only to make the position of the eyes more evident, but the misalignment is clearly visible even to the naked eye.

Figure 6.
Depending on the location of the lesion (before or after decussation), the side of the hypotropic eye may or may not coincide with the side of the lesion.
Figure 6.
Depending on the location of the lesion (before or after decussation), the side of the hypotropic eye may or may not coincide with the side of the lesion.
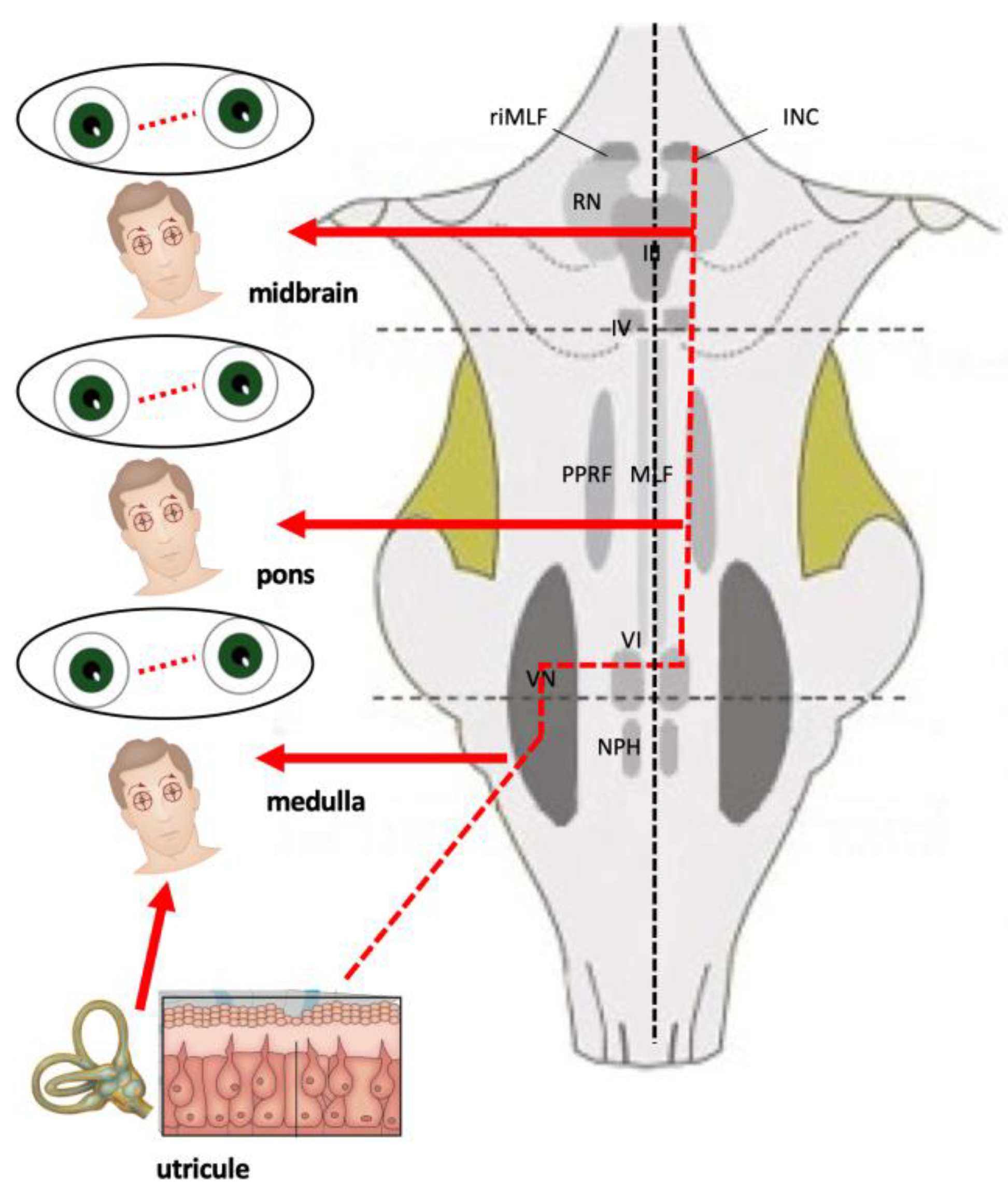

Table 1.
the examination of the ocular motor and the vestibular systems. VOR: Vestibulo-Ocular Reflex.
Table 1.
the examination of the ocular motor and the vestibular systems. VOR: Vestibulo-Ocular Reflex.
| Type of Examination | Search for |
|---|---|
| Head Posture | Head Tilt |
| Eye Movements Position of the eyes Straight ahead, look to the right, left, upward and downward, Cover test |
Primary misalignment, Spontaneous nystagmus Gaze function End point nystagmus |
| Smooth Pursuit | Saccadic, |
| Reduction of gain | |
| Saccades | Latency, velocity, accuracy |
| VOR functionality Clinical Head Impulse Test |
Presence of corrective saccades |
| Visual fixation suppression of the VOR | No suppression of VOR (mainly occur in cerebellar diseases) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



