Submitted:
23 August 2025
Posted:
26 August 2025
Read the latest preprint version here
Abstract
Background and objectives: Gold-based therapies are increasingly being studied for their potential to alleviate symptoms of osteoarthritis (OA), although their overall ev-idence remains inconclusive.
Methods: We conducted a systematic review and meta-analysis (search date: April 7, 2025) across five databases. We included both human and animal cohort studies, as well as randomized controlled trials, that reported on the effects of bead implants (GBI), nanoparticles (AuNP), and gold microparticles (µGold) on osteoarthritic symptoms. The risk of bias was assessed using the Cochrane, CAMARADES, and ROBINS-I tools. When appropriate, log odds ratio, Cohen’s d and Freeman-Tukey proportions were used to estimate effect size under a random-effects model.
Results: A total of 22 studies met the inclusion criteria. We analyzed ten studies on GBI, nine on AuNP, and three on µGold, grouping them based on study type. For the 14 randomized controlled studies, the log odds ratio for the number of patients improved with GBI for human knee and cervical OA (two studies) was 1.61 (-1.04, 4.27), p = 0.23. For the number of patients improved with GBI for dog hip OA (three studies), the log odds ratio was 0.86 (-0.06, 1.79), p = 0.07. The effect size for the osteoarthritic score for AuNP in small animal OA (four studies) was -2.48 (-3.80, -1.15), p < 0.001, and for TNF-alpha in AuNP for small animal OA (five studies), it was -2.70 (-4.24, -1.15), p < 0.001. In the eight cohort studies, the success proportion of GBI for dog OA (five studies) was 0.88 (0.77, 0.96), p < 0.001, while for µGold in human OA (three studies), it was 0.75 (0.68, 0.82), p < 0.001.
Conclusions: Notably, µGold offers an advantage in localized delivery through single intra-articular administration and greater potential for the release of gold ions compared to both GBI and AuNP. Although the evidence is classified as low to moder-ate and shows a moderate degree of heterogeneity, the results favor the use of GBI, AuNP, and µGold for OA treatment.
Keywords:
osteoarthritis
; gold microparticles
; gold nanoparticles
; gold bead implants
; human studies
; animal model
; systematic review
; meta‐analysis
1. Introduction
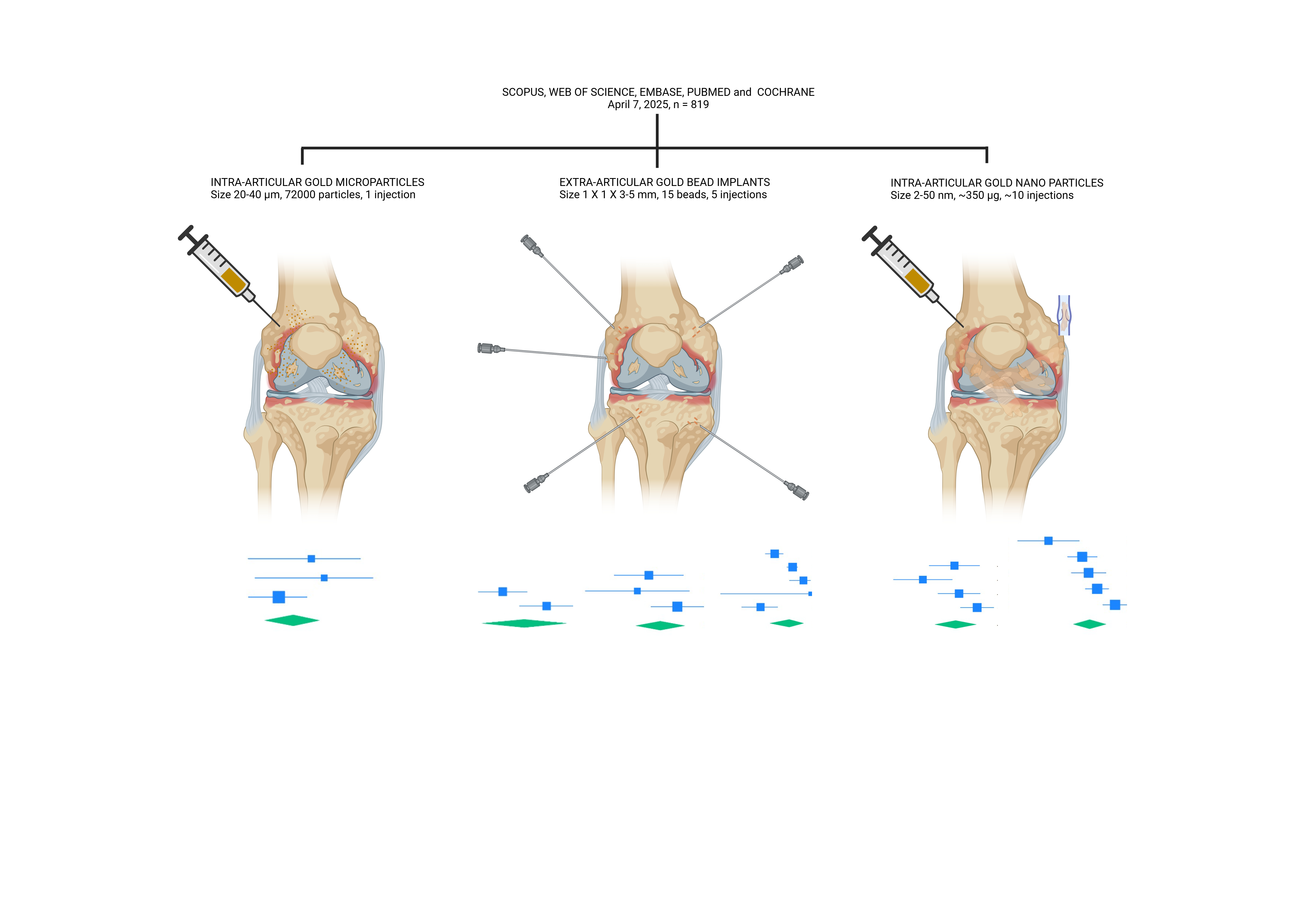
Gold-based therapies have been extensively studied for their potential to treat inflammatory and degenerative diseases, especially joint disorders like osteoarthritis and rheumatoid arthritis [1]. Among these approaches, gold bead implantation (GBI) [2,3], gold microparticles (µGold) [4,5], and gold nanoparticles (AuNP) [6] have emerged as prominent modalities, each with distinct properties influencing their clinical use. Both µGold and GBI interventions seek to harness gold’s anti-inflammatory properties and biocompatibility; however, their differences in size, delivery method, and therapeutic efficacy define their clinical applications [2,3,4,5]. Although AuNP is utilized in diagnostics, imaging, photothermal therapy, radiotherapy, and drug delivery [6], it has not been reported for use in clinical treatment on its own.
GBI, traditionally used in permanent implantation procedures, has been employed in veterinary and human medicine, particularly in chronic pain management and degenerative joint conditions [2,3,7,8,9]. Their localized presence provides long-term therapeutic pain relief and anti-inflammatory effects, but potential concerns remain regarding implant migration, localized fibrosis, and surgical risks associated with implantation [10,11]. Traditionally, GBI involves the surgical placement of small gold beads into specific anatomical locations, such as around artificial joints or acupuncture points to provide long-term pain relief and anti-inflammatory effects [7,8,9].
In contrast, µGold offer a minimally invasive alternative, administered via intra-articular injection or targeted delivery systems, potentially reducing procedural risks while maintaining effective immune modulation and anti-inflammatory effects [1,4,5]. µGold therapy involves the intra-articular injection of gold microparticles directly into the affected joint [4,5,12,13]. This minimally invasive technique aims to reduce inflammation and alleviate pain without the need for surgical implantation. Recent exploratory human studies have shown promising results using intra-articular injections of gold microparticles in patients with knee and hip osteoarthritis that led to significant pain reduction and improved joint function, with no reported adverse effects [4,12,13]. These outcomes suggest that µGold may offer a safer and more effective alternative to traditional GBI.
The effectiveness of gold-based local anti-inflammatory treatments is closely linked to the distribution of gold ions within the inflamed tissue [14,15]. The finding of a few mm spread of gold ions into the interstitial cellular fluid and cells from the gold surfaces [14,15] make it obvious why a multitude of gold particles, 72000 BMI gold particles in 2 ml suspension medium of synovial fluid or hyaluronic acid [4,12,13] offers superior therapeutic outcomes compared to larger implants [2,3] or repeated injection of AuNP’s [6,16,17]. The micron-sized particles compose of 99.99% pure gold further expand the available gold surface drastically compared to gold beads and substantially increase the amount of released gold ions. The tiny particles can be injected directly into joints without any side effects [4,12,13]. Another advantage is that a thin 21G needle can be used to apply gold microparticles, making the treatment easier and almost painless compared to using a 14G needle and stylet to inject millimeter-sized gold beads [2,3,7].
This study aims to investigate the research question of whether there is a spatial advantage among µGold, BMI, and AuNP. It is hypothesized that µGold therapy, which involves a minimally invasive single injection, is more effective than GBI and repeated injections of AuNP in treating joint diseases. The rationale behind this hypothesis is that having more gold implant particles present and stable in proximity to the inflamed tissue is expected to enhance the dissolucytotic and immunosuppressive effects, ultimately improving outcomes and reducing side effects.
2. Materials and Methods
2.1. Reporting and Registration
This report follows the PRISMA guidelines [18]. The completed PRISMA checklist is provided in the Supplementary Materials (S1). The protocol is registered in PROSPERO.
2.2. Information Sources and Search Strategy
This study identified human and animal studies of local injection of gold microparticles (µGold), gold bead implantation (GBI) and gold nanoparticles (AuNP) for osteoarthritis and other inflammatory joint disorders. Five databases were searched: Medline (PubMed), Embase, Cochrane, Scopus and Web of Science, without restriction on language or date of publication. The categories used were: (“gold microparticles” OR “gold implantation” OR “gold bead implantation” OR “gold nanoparticles”) AND ("osteoarthritis" OR "joint disease" OR "rheumatoid arthritis" OR "joint inflammation" OR "cartilage repair" OR "synovial inflammation" OR "degenerative joint disease") AND ("clinical trial" OR "human study" OR "animal study" OR "preclinical study" OR "in vivo" OR "in vitro") NOT ("gold dental implant" OR "gold stent" OR "gold alloy"). The search was conducted by SR and SK, Aalborg University, Denmark, on April 7, 2025, to investigate the effect of µGold, GBI and AuNP on osteoarthritis and other inflammatory joint disorders. Complete details of the electronic search strategies are provided in Appendix A.
2.3. Study Selection
Duplicate entries were manually identified and removed by the authors, and the authors independently performed the screening of eligible studies in two steps based on the PRISMA Guidelines [18]. In the first step, we screened all titles and abstracts according to the predefined inclusion and exclusion criteria. The inclusion criteria consisted of human and animal studies that investigate the effects of µGold, GBI, and AuNP on osteoarthritis and other inflammatory joint diseases, with quantifiable data (N, n1, n2, number improved, ratio, mean, SD, or SEM) required for each group. In cases of conflicts, the authors re-evaluated the title and abstract and reached a mutual consensus after discussion.
In the second step, the two reviewers individually read all full-text articles included in the previous step. In addition to the previously mentioned inclusion criteria, the final inclusion criteria were human and animal studies investigating the effects of µGold, GBI, and AuNP locally injected periarticular or intraarticular, specifically for measuring the number of subjects improved in randomized and cohort studies or the mean and SD of inflammatory markers in randomized studies. Additionally, for each study, the number of injections used is specified. Only studies reporting outcomes after a minimum of 8 weeks were included to ensure that the initial intention to treat, local and general anaesthesia had subsided, allowing for a clearer evaluation of early mid-stage to late-stage treatment outcomes. Reasons for exclusion were pre-specified as follows: 1) no in-vivo experiment, 2) no extractable or available data, 3) wrong route of administration, and 4) not µGold, GBI, or AuNP.
2.4. Quality Assessment
The quality of the included randomised human studies was assessed for bias by the Cochrane Collaboration’s tool for assessing risk of bias [19], which includes an assessment of bias in: Random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. The authors conducted the quality assessment, and any disagreements that arose were resolved through discussion.
The quality of the included randomized animal studies was assessed by the Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES) checklist [20,21]. The tool includes 14 questions designed to identify potential biases in the study design. Scores range from 0 to 14, with a higher score reflecting a greater methodological quality of the study [20,22].
The quality of the included non-randomized studies was assessed for bias by the Cochrane Collaboration’s tool for assessing risk of bias [23] version 2 of the ROBINS-I tool, launched on 22 November 2024 [24], which includes an assessment of bias in seven domains: (1) bias due to confounding (control for confounders (different size of animals included, different joints treated, different causes of osteoarthritis) and control for postintervention variables (time varying, other treatment); (2) bias in classification of interventions (clearly defined intervention groups); (3) bias in selection of participants into the study (or into the analysis) (selection of participants into the study (or into the analysis) based on participant characteristics observed after the start of intervention); (4) bias due to deviations from intended interventions (deviations from the intended intervention beyond what would be expected in usual practice, and adheres to the assigned intervention regimen); (5) bias due to missing data (outcome data available for all, or nearly all, participants, and participants excluded due to missing data on other variables needed for the analysis); (6) bias arising from measurement of the outcome (outcome measure influenced by knowledge of the intervention received, outcome assessors aware of the intervention received by study participants, and systematic errors in measurement of the outcome related to the intervention received); (7) and bias in selection of the reported results (multiple outcome measurements, multiple analyses of the intervention-outcome relationship, and different subgroups). Each bias domain is evaluated as low, moderate, serious, or critical according to the ROBINS-I framework. The quality assessment was conducted by the authors, and any disagreements were resolved by discussion.
2.5. Data Extraction
For each eligible study, the following characteristics were extracted: year of publication, number of participants, type and formulation of gold used (e.g. µGold, GBI, AuNP), target condition (e.g., osteoarthritis or other inflammatory joint diseases), and route of administration (i.e., extra-articular or intra-articular injection). For randomized and cohort studies, we extracted data on the number of subjects who improved. For randomized studies with quantifiable outcomes, we extracted group-level data (N, n1, n2, number improved, proportion, mean, SD or SEM) on inflammatory markers.
2.6. Statistical Analysis
To conduct the analyses, the statistical software Stata MP 18.0 was utilized. We tested for statistical heterogeneity by including Tau-squared (τ²), H-squared (H²), and I-squared (I²). This approach provides a more comprehensive understanding of the variability among the results, allowing us to determine whether differences in study outcomes are likely due to actual differences in study variables rather than random variability. For randomized studies, we calculated the pooled standardized mean odds ratio (OR) with a 95% confidence interval (CI). The effect size measure for continuous data was determined using the inverse-variance method, considering both within-study and between-study variance. For incidence data, the log odds ratio was calculated using the same inverse-variance method, accounting for both types of variances. In the case of cohort studies, we used a new option in Stata MP 18.0 to calculate the Freeman-Tukey transformed proportions, also employing the inverse-variance method [25,26]. The results are presented in forest and tunnel plots.
Generative artificial intelligence (GenAI) has not been used in this paper (e.g., to generate text, data, or graphics, or to assist in study design, data collection, analysis, or interpretation).
3. Results
3.1. Study Selection
The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
On April 7, 2025, the search yielded a total of 829 studies after removing duplicates. Of these, 784 were excluded based on irrelevance from title and abstract. After the assessment of 45 full-text articles 22 studies were included in the final meta-analysis[2,3,4,7,8,9,12,13,17,27,28,29,30,31,32,33,34,35,36,37,38].
3.2. Study Characteristics
The studies were published between 1992 and 2024. Table 1, Table 2 and Table 3 presents the characteristics of the included studies.
The study characteristics display a heterogeneous group of studies that can be divided into 14 randomized trials [2,3,7,8,9,17,27,28,29,30,31,32,33,34] and eight cohorts [4,12,13,35,36,37,38,39], in 17 animal [7,8,9,17,27,28,29,30,31,32,33,34,35,36,37,38,39] and five human studies [2,3,4,12,13], in ten studies using GBI [2,3,7,8,9,35,36,37,38,39], nine studies using AuNP [17,27,28,29,30,31,32,33,34], and three studies using µGold [4,12,13].
The GBI studies [2,3,7,8,9,35,36,37,38,39] (Table 1, Table 2 and Table 3) were dog and human trials using 3 mm-sized GBI (diameter 1 mm, length 2-4 mm) in three or more points around the osteoarthritic joint. The follow-up period is between one month and one year. No adverse events are reported in three studies [2,3,37], and four studies do not report events [7,8,36,38]. Bleeding is reported in one study [39], and one case of infection in another study [9]. Durkes [35], who reported the first study on BMI and included the largest number of individuals, observed several possible adverse events. Intra-articular placed BMI may cause pain and must be removed. The most common problem is superficial infection due to improper sterile technique, and another remark is the possibility of injuring the sciatic nerve. The number of injections of three beads ranged between 3 and 16. The dosage of gold ranged between 91 and 728 mg, and the total surface between 0.71 and 1.78 cm2.
The AuNP studies [17,27,28,29,30,31,32,33,34] were all performed in small animal trials and employed a wide range of formulations, delivery strategies, and follow-up (Table 3). The studies were performed on rat ankle and knee OA, but one on mouse knee OA [29]. In four of the studies, the AuNPs were conjugated to different proteins [17,29,31,32]. The number of injections ranged between 1 and 15, and follow-up ranged between 9 and 60 days. The AuNP size ranged between 2.2 and 50 nm. The total dosage is between 27 and 687.5 µg, and the total surface is between 0.81 and 135.9 cm2.
The µGold studies [4,12,13] were performed on human knee [4,12] and hip [13] OA using a single injection. The patient’s synovial fluid [4] and hyaluronic acid [12,13] were used as carriers of the µGold. The dosage of µGold was 20 mg gold microparticles (72,000 50particles, 20–40 μm in diameter) with a total surface of 2.05 cm2. No adverse effects were observed during the two years following the treatment.
3.3. Study Quality and Publication Bias
The Cochrane Collaboration's tool for assessing risk of bias [19,40] was applied to two studies [2,3], resulting in a low risk of bias (Table 4).
The CAMARADES checklist for assessing risk of bias [20,21] was used for the randomized animal trials [7,8,9,17,27,28,29,30,31,32,33,34] (Table 5). All studies (n = 12) were published in peer-reviewed journals using mice, rats, or dogs as animal models. The risk of bias scores ranged from 2 to 13, with a median score of 7.
The Cochrane Collaboration’s tool for assessing risk of bias [23] version 2 of the ROBINS-I tool, launched on 22 November 2024 [24], was used for the human [4,12,13] and animal cohort studies[35,36,37,38,39] (Table 6). Table 6 tabulates five serious and 20 critical risks of bias out of 35 assessments of the animal studies.
3.4. Statistical Analysis Results
The 22 randomized and cohort studies examining the effects of BMI, AuNP, and µGold were organized into six meta-analyses, employing a random effects model for pooled effects and the inverse-variance method to analyze publication bias (Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7). In the analysis of randomized studies on BMI for human and animal osteoarthritis (OA), no significant difference was found between the intervention and control groups (Figure 2 and Figure 3). The randomized studies examining AuNP for animal OA revealed a significant difference between the intervention and control groups (Figure 4 and Figure 5). The cohort studies assessing the success of BMI in animals and µGold in humans both demonstrated a significant difference between the intervention and control groups (Figure 6 and Figure 7). Overall, the forest plots indicated a high degree of heterogeneity, with four analyses exhibiting a I² value exceeding 50% (Figure 2, Figure 4, Figure 5 and Figure 6). Furthermore, the funnel plots reflected low study precision, with seven studies outside the 95% confidence interval lines, suggesting a moderate degree of bias.
4. Discussion
The analysis of the study characteristics revealed that the µGold trials utilized a single injection, whereas the GBI and AuNP trials involved multiple injections. When calculating the total gold surface area that facilitates the diffusion of gold ions into the interstitial cellular fluid and cells from the gold surfaces [14,15], the area for this process, known as dissolucytosis [4,15,41], was greater in the µGold studies compared to the BMI studies and the majority of AuNP studies.
This systematic review is the first to evaluate the effects of extra-articular and intra-articular gold treatments for osteoarthritis (OA) in both human and animal trials. The meta-analyses revealed a significant effect of extra-articular GBI interventions in five animal cohort studies [35,36,37,38,39] (Figure 6). However, no significant effects were found in two human randomized trials and three animal randomized trials when comparing GBI to placebo [2,3,7,8,9] (Figure 2 and Figure 3). Additionally, the meta-analysis indicated a significant effect of intra-articular gold nanoparticles (AuNP) on OA in nine animal randomized trials compared to placebo [17,27,28,29,30,31,32,33,34] (Figure 4 and Figure 5). There was also a significant effect of intra-articular microgold (µGold) on OA in three human cohort studies [4,12,13] (Figure 7). The forest plots demonstrated a high degree of heterogeneity in four of the analyses (Figure 2, Figure 4, Figure 5 and Figure 6), while the funnel plots indicated some bias and low study precision. The meta-analysis and the examination of study characteristics support the hypothesis that µGold offers a spatial advantage compared to GBI and AuNP. The findings indicate that a single injection of µGold, its large surface area conducive to dissolucytosis, and the low heterogeneity observed across the µGold studies all bolster this hypothesis. However, some weaknesses include the limited number of studies in each category and the fact that the µGold studies are uncontrolled cohorts.
The use of gold to treat inflammatory diseases like rheumatoid arthritis became significant in the early 20th century and is well documented [4,42]. However, the used gold thiocompounds (i.e., sulfur-containing gold-based drugs such as auranofin) must be administered with care as they are toxic to the liver, kidney, and skin, and are replaced by more modern disease-modifying antirheumatic drugs [43]. Later, it became evident that gold ions alter antigen-processing and reduce the cytokine expression of macrophages [44]. With the introduction of GBI for treatment of animal OA using acupuncture points for the insertion in the 70-ties [35,45] it became interesting to investigate the effect of different gold therapies for OA [4,6,16,17,27], based on the limited benefit of the intra-articular injections that is a major part of the treatment program for osteoarthritis, that include exercise, analgesics and dietary weight management [46,47]. The intra-articular treatment with corticosteroid and hyaluronic acid has limited benefits for 3-4 weeks [46,47], systematic reviews do not support viscosupplementation [48], and there is no evidence for platelet-rich plasma [49], stem cells [50] or micro-fragmented adipose tissue [51].
The effectiveness of intra-articular AuNP may be reduced by macrophages' ability to remove and scavenge nanoparticles [28,41,52], which can explain the need for multiple injections. Intravenous [53] and intraperitoneal [54] injections and oral administration [55] of AuNP can relieve OA symptoms in animal studies and demonstrate the macrophages’ ability to remove and transport the AuNP to all other tissues [56], and indicate there is a systemic effect of AuNP. There is an accumulation of injected AuNP in the liver, spleen, and lungs [56,57] and granular degeneration is observed in these tissues [56], which may be a risk. There is an intracellular release of gold ions from the AuNP that initiates the anti-inflammatory and other response [14,58]. Even if AuNPs are considered as highly compatible nano constructs, a potential toxicity mainly related to internalization modality has been demonstrated from the release of free gold ions in different cells and tissues [59].
The macrophages are not able to remove or transport µGold and GBI and the gold microparticles and beads stay in place. Only cells close to the µGold and GBI become loaded with gold ions and imply that no gold is spread to other organs and may exclude any toxic effect [14,15,41].
In the forest plots, we used the odds ratio for binomial outcomes and mean difference for continuous outcomes of controlled studies and Freeman-Tukey’s proportion for binomial outcomes of uncontrolled cohort studies. There is a risk of overemphasis of statistical significance when the confidence interval crosses the null line [60]. It is crucial to examine individual studies when the pooled estimate indicates no overall effect, as shown in Figure 2 and Figure 3. This lack of effect may be due to study limitations, such as small sample sizes or insufficient duration, rather than a genuine absence of effect. Additionally, it is important to consider heterogeneity greater than 50%, as seen in Figure 2, Figure 4, Figure 5 and Figure 6; in these cases, the overall effect must be interpreted with caution [61]. If negative or neutral studies are underrepresented, the forest plot may overestimate the treatment effect. In our analysis, four studies found no effect [2,7,9,34]. We employed a random effects model that assumes the study outcomes may vary.
The funnel plots indicated some bias in the studies and a lack of precision. The studies are to some degree asymmetrically distributed around the overall effect. Additionally, the small number of studies for each analysis may limit our ability to draw firm conclusions.
5. Conclusions
µGold has a spatial advantage in using a single intra-articular administration and a higher possibility of release of gold ions compared to GBI and AuNP. GBI, AuNP, and µGold can relieve OA symptoms in animal and human studies, supporting their potential as therapeutic agents. The evidence is low to moderate with a moderate degree of heterogeneity. Large randomized, double-blind human studies comparing intra-articular µGold and AuNP to a placebo are necessary for proper conclusions.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization: Sten Rasmussen, Stephen Gunaratnam Klavsen; Methodology: Sten Rasmussen, Stephen Gunaratnam Klavsen; Formal analysis: Sten Rasmussen, Stephen Gunaratnam Klavsen; Investigation: Sten Rasmussen, Stephen Gunaratnam Klavsen; Writing – original draft: Sten Rasmussen, Stephen Gunaratnam Klavsen; Writing – review & editing: Sten Rasmussen.
Funding
This study received no external funding.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OA | Osteoarthritis |
| µGold | Gold microparticles |
| GBI | Gold bead implants |
| AuNP | Gold nano particles |
| e.a. | Extra articular |
| i.a. | Intra articular |
Appendix A
Search strategy, April 7, 2025:
Scopus
(“gold microparticles” OR “gold implantation” OR “gold bead implantation” OR “gold nanoparticles”) AND ("osteoarthritis" OR "joint disease" OR "rheumatoid arthritis" OR "joint inflammation" OR "cartilage repair" OR "synovial inflammation" OR "degenerative joint disease") AND ("clinical trial" OR "human study" OR "animal study" OR "preclinical study" OR "in vivo" OR "in vitro") NOT ("gold dental implant" OR "gold stent" OR "gold alloy").
N = 305
Web op Science
TS=("gold microparticles" OR "gold implantation" OR "gold bead implantation" OR “gold nanoparticles”) AND TS=("osteoarthritis" OR "joint disease" OR "rheumatoid arthritis" OR "joint inflammation" OR "cartilage repair" OR "synovial inflammation" OR "degenerative joint disease")
225
Embase
('gold microparticles'/exp OR 'gold implantation'/exp OR 'gold bead implantation'/exp OR 'gold nanoparticles'/exp) AND ('osteoarthritis'/exp OR 'joint disease'/exp OR 'rheumatoid arthritis'/exp OR 'joint inflammation'/exp OR 'cartilage repair'/exp OR 'synovial inflammation'/exp OR 'degenerative joint disease'/exp) AND ('clinical trial'/exp OR 'human study'/exp OR 'animal study'/exp OR 'preclinical study'/exp OR 'in vivo study'/exp)
N=206
Pubmed:
(“gold microparticles” OR “gold implantation” OR “gold bead implantation” OR “gold nanoparticles”) AND ("osteoarthritis" OR "joint disease" OR "rheumatoid arthritis" OR "joint inflammation" OR "cartilage repair" OR "synovial inflammation" OR "degenerative joint disease")
N = 79
Cochrane
("gold microparticles" OR "gold nanoparticles" OR "gold implantation" OR "gold bead implantation") AND ("osteoarthritis" OR "joint disease" OR "rheumatoid arthritis" OR "joint inflammation" OR "cartilage repair" OR "synovial inflammation" OR "degenerative joint disease")
N = 4
References
- Rasmussen, S.; Frederickson, C.; Danscher, G. Inhibition of Local Inflammation by Implanted Gold: A Narrative Review of the History and Use of Gold. J. Rheumatol. 2023, 50. [Google Scholar] [CrossRef]
- Nejrup, K.; de Fine Olivarius, N.; Jacobsen, J.L.; Siersma, V. Randomised Controlled Trial of Extraarticular Gold Bead Implantation for Treatment of Knee Osteoarthritis: A Pilot Study. Clin Rheumatol 2008, 27, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Kjerkegaard, H.K.; Kirkeby, R.; Christensen, T.B.; Schlünzen, L. Double-Blinded, Placebo-Controlled Trial of the Pain-Relieving Effect of Gold Bead Implantation on Cervical Osteoarthritis. Med Acupunct 2011, 23, 87–91. [Google Scholar] [CrossRef]
- Rasmussen, S.; Kjær Petersen, K.; Kristiansen, M.K.; Skallerup, J.; Aboo, C.; Thomsen, M.E.; Skjoldemose, E.; Jørgensen, N.K.; Stensballe, A.; Arendt-Nielsen, L. Gold Micro-Particles for Knee Osteoarthritis. European Journal of Pain (United Kingdom) 2022, 26. [Google Scholar] [CrossRef] [PubMed]
- Märki, N.; Witte, S.; Kuchen, S.; Reichenbach, S.; Ramseyer, A.; Gerber, V.; Spadavecchia, C. Safety of Intra-Articular Gold Microimplants in Horses–A Randomized, Blinded, Controlled Experimental Study. J Equine Vet Sci 2018, 60, 59–66.e2. [Google Scholar] [CrossRef]
- Huang, H.; Liu, R.; Yang, J.; Dai, J.; Fan, S.; Pi, J.; Wei, Y.; Guo, X. Gold Nanoparticles: Construction for Drug Delivery and Application in Cancer Immunotherapy. Pharmaceutics 2023, 15, 1868. [Google Scholar] [CrossRef]
- Hielm-Bjorkman, A.; Raekallio, M.; Kuusela, E.; Saarto, E.; Markkola, A.; Tulamo, R. Double-blind Evaluation of Implants of Gold Wire at Acupuncture Points in the Dog as a Treatment for Osteoarthritis Induced by Hip Dysplasia. Veterinary Record 2001, 149, 452–456. [Google Scholar] [CrossRef]
- Jaeger, G.T.; Larsen, S.; Søli, N.; Moe, L. Double-blind, Placebo-controlled Trial of the Pain-relieving Effects of the Implantation of Gold Beads into Dogs with Hip Dysplasia. Veterinary Record 2006, 158, 722–726. [Google Scholar] [CrossRef]
- Bolliger, C.; DeCamp CE; Stajich, M. ; Flo, G.; Martinez, S.; Bennett, R.; Bebchuk, T. Gait Analysis of Dogs with Hip Dysplasia Treated with Gold Bead Implantation Acupuncture. Journal of The European Society for Veterinary Orthopaedics and Traumatology 2002, 15, 116–122. [Google Scholar]
- Lie, K.-I.; Jæger, G.; Nordstoga, K.; Moe, L. Inflammatory Response to Therapeutic Gold Bead Implantation in Canine Hip Joint Osteoarthritis. Vet Pathol 2011, 48, 1118–1124. [Google Scholar] [CrossRef]
- Jæger, G.T.; Stigen, Ø.; Devor, M.; Moe, L. Gold Bead Implantation in Acupoints for Coxofemoral Arthrosis in Dogs: Method Description and Adverse Effects. Animals 2012, 2, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.; Petersen, K.K.; Aboo, C.; Andersen, J.S.; Skjoldemose, E.; Jørgensen, N.K.; Stensballe, A.; Arendt-Nielsen, L. Intra-Articular Injection of Gold Micro-Particles with Hyaluronic Acid for Painful Knee Osteoarthritis. BMC Musculoskelet Disord 2024, 25, 211. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.; Skjoldemose, E.; Jørgensen, N.K. Intraarticular Gold Microparticles Using Hyaluronic Acid as the Carrier for Hip Osteoarthritis. A 2-Year Follow-up Pilot Study. Sci Rep 2024, 14, 26249. [Google Scholar] [CrossRef] [PubMed]
- Danscher, G. In Vivo Liberation of Gold Ions from Gold Implants. Autometallographic Tracing of Gold in Cells Adjacent to Metallic Gold. Histochem Cell Biol 2002, 117, 447–452. [Google Scholar] [CrossRef]
- Larsen, A.; Stoltenberg, M.; Danscher, G. In Vitro Liberation of Charged Gold Atoms: Autometallographic Tracing of Gold Ions Released by Macrophages Grown on Metallic Gold Surfaces. Histochem Cell Biol 2007, 128, 1–6. [Google Scholar] [CrossRef]
- Filho, M.C.B.; dos Santos Haupenthal, D.P.; Zaccaron, R.P.; de Bem Silveira, G.; de Roch Casagrande, L.; Lupselo, F.S.; Alves, N.; de Sousa Mariano, S.; do Bomfim, F.R.C.; de Andrade, T.A.M.; et al. Intra-articular Treatment with Hyaluronic Acid Associated with Gold Nanoparticles in a Mechanical Osteoarthritis Model in Wistar Rats. Journal of Orthopaedic Research 2021, 39, 2546–2555. [Google Scholar] [CrossRef]
- Sarkar, A.; Carvalho, E.; D’souza, A.A.; Banerjee, R. Liposome-Encapsulated Fish Oil Protein-Tagged Gold Nanoparticles for Intra-Articular Therapy in Osteoarthritis. Nanomedicine 2019, 14, 871–887. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. J Clin Epidemiol 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928–d5928. [Google Scholar] [CrossRef]
- Macleod, M.R.; O’Collins, T.; Howells, D.W.; Donnan, G.A. Pooling of Animal Experimental Data Reveals Influence of Study Design and Publication Bias. Stroke 2004, 35, 1203–1208. [Google Scholar] [CrossRef]
- Ritskes-Hoitinga, M.; Leenaars, M.; Avey, M.; Rovers, M.; Scholten, R. Systematic Reviews of Preclinical Animal Studies Can Make Significant Contributions to Health Care and More Transparent Translational Medicine. In Cochrane Database of Systematic Reviews; Tovey, D., Ed.; John Wiley & Sons, Ltd: Chichester, UK, 2014. [Google Scholar]
- Wilson, E.; Ramage, F.J.; Wever, K.E.; Sena, E.S.; Macleod, M.R.; Currie, G.L. Designing, Conducting, and Reporting Reproducible Animal Experiments. Journal of Endocrinology 2023, 258. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, i4919. [Google Scholar] [CrossRef]
- Sterne, J.; Higgins, J. ROBINS-1 V2 Tool.
- Clopper, C. ; Pearson ES The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Lin, L.; Xu, C. Arcsine-Based Transformations for Meta-Analysis of Proportions: Pros, Cons, and Alternatives. Health Sci Rep 2020, 3, e178. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.; Shiau, A.; Chen, S.; Chen, Y.; Cheng, P.; Chang, M.; Chen, D.; Chou, C.; Wang, C.; Wu, C. Amelioration of Collagen-induced Arthritis in Rats by Nanogold. Arthritis Rheum 2007, 56, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Leonavičienė, L.; Kirdaitė, G.; Bradūnaitė, R.; Vaitkienė, D.; Vasiliauskas, A.; Zabulytė, D.; Ramanavičienė, A.; Ramanavičius, A.; Ašmenavičius, T.; Mackiewicz, Z. Effect of Gold Nanoparticles in the Treatment of Established Collagen Arthritis in Rats. Medicina (Kaunas) 2012, 48, 91–101. [Google Scholar] [CrossRef]
- Campos, W.N. da S.; Leite, A.E.T.; Sonego, D.A.; Andrade, M.A. de; Pizzinatto, F.D.; Marangoni, V.S.; Zucolotto, V.; Nakazato, L.; Colodel, E.M.; Souza, R.L. de Síntese e Caracterização de Nanopartículas de Ouro Conjugadas Com Curcumina e Seus Efeitos Na Osteoartrite Experimental Induzida. Ciência Rural 2017, 47. [Google Scholar] [CrossRef]
- Kirdaite, G.; Leonaviciene, L.; Bradunaite, R.; Vasiliauskas, A.; Rudys, R.; Ramanaviciene, A.; Mackiewicz, Z. Antioxidant Effects of Gold Nanoparticles on Early Stage of Collagen-Induced Arthritis in Rats. Res Vet Sci 2019, 124, 32–37. [Google Scholar] [CrossRef]
- Shahen, S.M.; Mohamed, M.R.; Ali, M.R.K.; Samaka, R.M.; Hamdy, G.M.; Talaat, R.M. Therapeutic Potential of Targeted-gold Nanospheres on Collagen-induced Arthritis in Rats. Clin Exp Pharmacol Physiol 2021, 48, 1346–1357. [Google Scholar] [CrossRef]
- Wei, Y.; Nie, Y.; Han, Z.; Huang, H.; Liao, X.; Wang, X.; Fan, Z.; Zheng, Y. Au@polydopamine Nanoparticles/Tocilizumab Composite as Efficient Scavengers of Oxygen Free Radicals for Improving the Treatment of Rheumatoid Arthritis. Materials Science and Engineering: C 2021, 118, 111434. [Google Scholar] [CrossRef]
- Abdel-Hakem, N.; Abo-El-Atta, A.; Samaka, R.; El-Shahat, M.; Bassyouni, I.; Talaat, R. Improving the Anti-Inflammatory/Anti-Angiogenic Properties of Gold Nanoparticles in the Treatment of Experimental Rheumatoid Arthritis. Curr Trends Immunol 2022, 23, 33–42. [Google Scholar]
- dos Santos Haupenthal, D.P.; Resmini, M.B.; Da Silva, L.A.; Colares, M.C.; de Roch Casagrande, L.; Milanez Venturini, L.; de Andrade, T.A.M.; do Bomfim, F.R.C.; Thirupathi, A.; Emilio Feuser, P.; et al. Intra-Articular Treatment with Triamcinolone Hexacetonide Associated with Gold Nanoparticles Reduces Cartilage Degeneration in an Animal Model of Osteoarthritis. Curr Drug Targets 2023, 24, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Durkes, T. Gold Bead Implants. Probl Vet Med 1992, 4, 207–211. [Google Scholar] [PubMed]
- Klitsgaard, J. Gold Implants - Practical Experiences with 400 Hip Dysplasia Cases in the Dog. In Proceedings of the International Veterinary Acupuncture Society Proceedings 22nd International Congress; Spiez, Schweiz, September 5 1996; pp. 1–5. [Google Scholar]
- Thoresen, S. A “New” Method of Placing Gold Implants to Treat Hip Dysplasia in the Dog. In Description and Evaluation of 50 Cases 1990-1996. In Proceedings of the International Veterinary Acupuncture Society Proceedings 22nd Annual International Congress ; Spiez, Schweiz, September 5 1996; pp. 1–7. [Google Scholar]
- Kothbauer, O. Über Die Implantation von Goldpartikeln Zur Therapeutischen Beeinflussung von Schmerzhaften Prozessen Im Hüftgelenksbereich von Hunden – Dargestellt an Drei Fallbeispielen. Wien Tierarztl Monatsschr 1997, 84, 47–52. [Google Scholar]
- Bartholomé, M.; Schulze, E. Efficacy of Gold Bead Acupuncture Treatment of Chronic Hip, Elbow and Spine Pain in 79 Dogs Following Unsuccessful Conventional Treatments. American Journal of Traditional Chinese Veterinary Medicine 2020, 15, 17–30. [Google Scholar]
- Ryan, R.; Hill, S.; Prictor, M.; McKenzie, J. Study Quality Guide; Cochrane Consumers and Communication Review Group: Melbourne, Australia, May 2013. [Google Scholar]
- Danscher, G.; Rasmussen, S. NanoGold and ΜGold Inhibit Autoimmune Inflammation: A Review. Histochem Cell Biol 2023, 159. [Google Scholar] [CrossRef]
- Berners-Price, S.J.; Filipovska, A. Gold Compounds as Therapeutic Agents for Human Diseases. Metallomics 2011, 3, 863. [Google Scholar] [CrossRef]
- Clark, P.; Tugwell, P.; Bennett, K.J.; Bombardier, C.; Shea, B.; Wells, G.A.; Suarez-Almazor, M.E. Injectable Gold for Rheumatoid Arthritis. Cochrane Database of Systematic Reviews 1997. [Google Scholar] [CrossRef]
- Burmester, G.R.; Barthel, H.R. [Mechanism of Action of Gold in Treatment of Rheumatoid Arthritis]. Z Rheumatol 1996, 55, 299–306. [Google Scholar]
- Yoo, H.-G.; Yoo, W.-H. Acupuncture with Gold Thread for Osteoarthritis of the Knee. New England Journal of Medicine 2013, 369, e37. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Osteoarthritis Cartilage 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.J.; Driban, J.B.; McAlindon, T.E. Pharmaceutical Treatment of Osteoarthritis. Osteoarthritis Cartilage 2023, 31, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Pereira, T. V; Jüni, P.; Saadat, P.; Xing, D.; Yao, L.; Bobos, P.; Agarwal, A.; Hincapié, C.A.; da Costa, B.R. Viscosupplementation for Knee Osteoarthritis: Systematic Review and Meta-Analysis. BMJ 2022, e069722. [Google Scholar] [CrossRef] [PubMed]
- Peck, J.; Slovek, A.; Miro, P.; Vij, N.; Traube, B.; Lee, C.; Berger, A.A.; Kassem, H.; Kaye, A.D.; Sherman, W.F.; et al. A Comprehensive Review of Viscosupplementation in Osteoarthritis of the Knee. Orthop Rev (Pavia) 2021, 13. [Google Scholar] [CrossRef]
- Kim, K.-I.; Kim, M.-S.; Kim, J.-H. Intra-Articular Injection of Autologous Adipose-Derived Stem Cells or Stromal Vascular Fractions: Are They Effective for Patients With Knee Osteoarthritis? A Systematic Review With Meta-Analysis of Randomized Controlled Trials. Am J Sports Med 2023, 51, 837–848. [Google Scholar] [CrossRef]
- Barfod, K.W.; Blønd, L.; Mikkelsen, R.K.; Bagge, J.; Hölmich, L.R.; Kallemose, T.; Troelsen, A.; Hölmich, P. Treatment of Knee Osteoarthritis with a Single Injection of Autologous Micro-Fragmented Adipose Tissue Is Not Superior to a Placebo Saline Injection: A Blinded Randomised Controlled Trial with 2-Year Follow-Up. Br J Sports Med 2025, bjsports-2024-108732. [CrossRef]
- Logozzi, M.; Mizzoni, D.; Bocca, B.; Di Raimo, R.; Petrucci, F.; Caimi, S.; Alimonti, A.; Falchi, M.; Cappello, F.; Campanella, C.; et al. Human Primary Macrophages Scavenge AuNPs and Eliminate It through Exosomes. A Natural Shuttling for Nanomaterials. European Journal of Pharmaceutics and Biopharmaceutics 2019, 137, 23–36. [Google Scholar] [CrossRef]
- Li, X.; Wang, H.; Zou, X.; Su, H.; Li, C. Methotrexate-Loaded Folic Acid of Solid-Phase Synthesis Conjugated Gold Nanoparticles Targeted Treatment for Rheumatoid Arthritis. European Journal of Pharmaceutical Sciences 2022, 170, 106101. [Google Scholar] [CrossRef]
- Ruvalcaba-Ontiveros, R.I.; González-Chávez, S.A.; Carrasco-Hernández, A.R.; López-Loeza, S.M.; Castellanos-Ponce, I.; Vázquez-Olvera, G.; Neri-Flores, M.Á.; Espino-Solís, G.P.; Duarte-Moller, J.A.; Pacheco-Tena, C.; et al. Treatment with Silica–Gold Nanostructures Decreases Inflammation-Related Gene Expression in Collagen-Induced Arthritis. Biomater Sci 2022, 10, 5216–5229. [Google Scholar] [CrossRef]
- Koliyote, S.; Shaji, J. The in Vivo Antiarthritic Activity of Guggulosomes Prepared Using Gold Nanoparticles Generated from Stem Extract of Tinospora Cardifolia (Thunb.) Miers. Annals of Phytomedicine: An International Journal 2022, 11. [Google Scholar] [CrossRef]
- Terentyuk, G.S.; Maslyakova, G.N.; Suleymanova, L. V.; Khlebtsov, B.N.; Kogan, B.Ya.; Akchurin, G.G.; Shantrocha, A. V.; Maksimova, I.L.; Khlebtsov, N.G.; Tuchin, V. V. Circulation and Distribution of Gold Nanoparticles and Induced Alterations of Tissue Morphology at Intravenous Particle Delivery. J Biophotonics 2009, 2, 292–302. [Google Scholar] [CrossRef]
- Sadauskas, E.; Jacobsen, N.R.; Danscher, G.; Stoltenberg, M.; Vogel, U.; Larsen, A.; Kreyling, W.; Wallin, H. Biodistribution of Gold Nanoparticles in Mouse Lung Following Intratracheal Instillation. Chem Cent J 2009, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Pinho, R.A.; Haupenthal, D.P.S.; Fauser, P.E.; Thirupathi, A.; Silveira, P.C.L. Gold Nanoparticle-Based Therapy for Muscle Inflammation and Oxidative Stress. J Inflamm Res 2022, 15, 3219–3234. [Google Scholar] [CrossRef] [PubMed]
- Sabella, S.; Carney, R.P.; Brunetti, V.; Malvindi, M.A.; Al-Juffali, N.; Vecchio, G.; Janes, S.M.; Bakr, O.M.; Cingolani, R.; Stellacci, F.; et al. A General Mechanism for Intracellular Toxicity of Metal-Containing Nanoparticles. Nanoscale 2014, 6, 7052. [Google Scholar] [CrossRef] [PubMed]
- Bown, M.J.; Sutton, A.J. Quality Control in Systematic Reviews and Meta-Analyses. European Journal of Vascular and Endovascular Surgery 2010, 40, 669–677. [Google Scholar] [CrossRef]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Statistical Heterogeneity in Systematic Reviews of Clinical Trials: A Critical Appraisal of Guidelines and Practice. J Health Serv Res Policy 2002, 7, 51–61. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram.
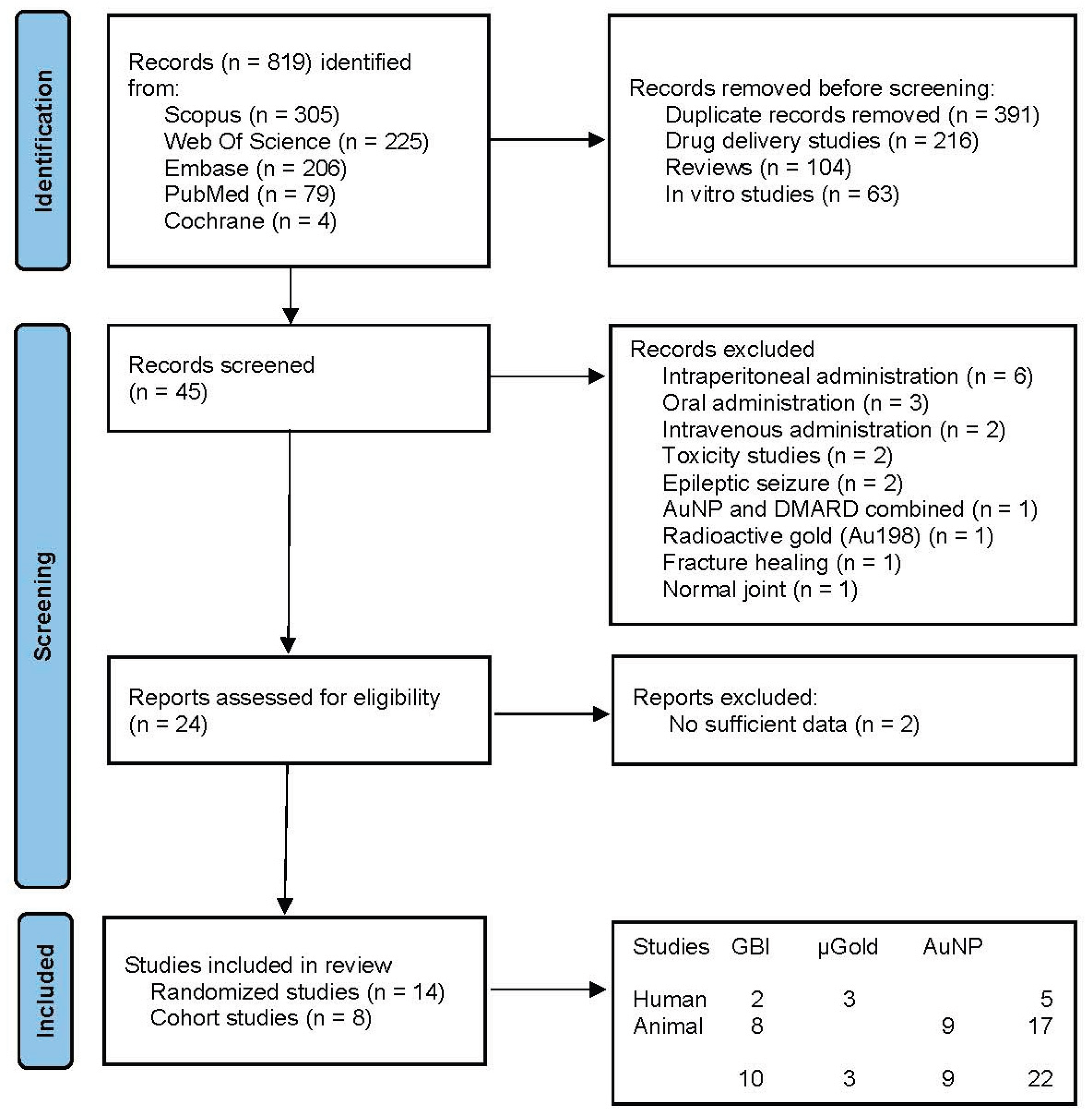
Figure 2.
Forest plot (A) and funnel plot (B) of pooled effect for number improved of GBI for human knee and cervical OA.
Figure 2.
Forest plot (A) and funnel plot (B) of pooled effect for number improved of GBI for human knee and cervical OA.
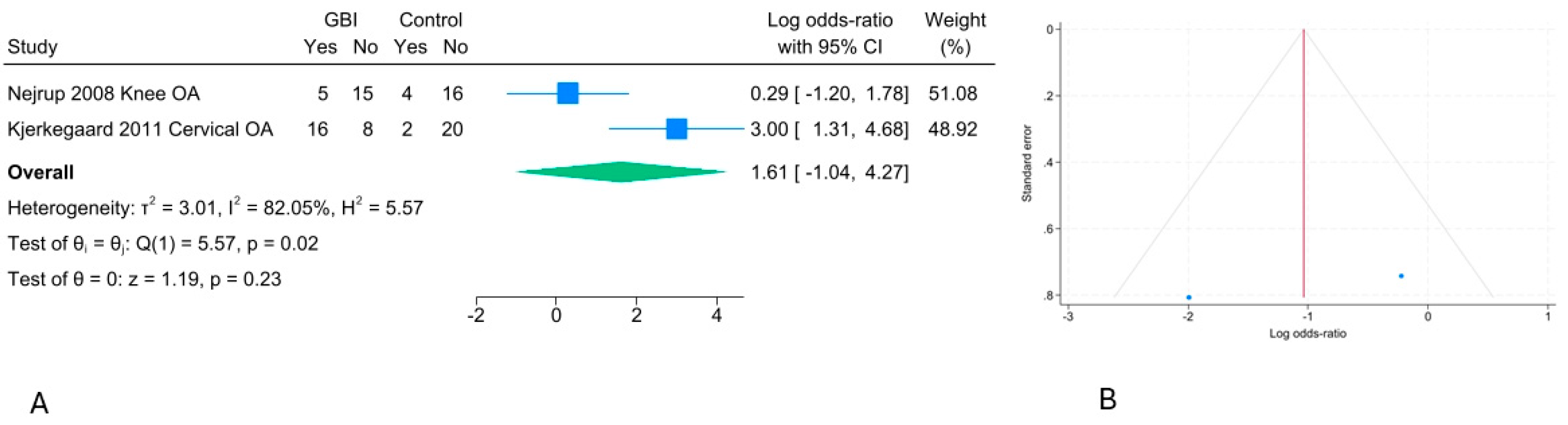
Figure 3.
Forest plot (A) and funnel plot (B) of pooled effect for number improved of GBI for dog hip OA.
Figure 3.
Forest plot (A) and funnel plot (B) of pooled effect for number improved of GBI for dog hip OA.
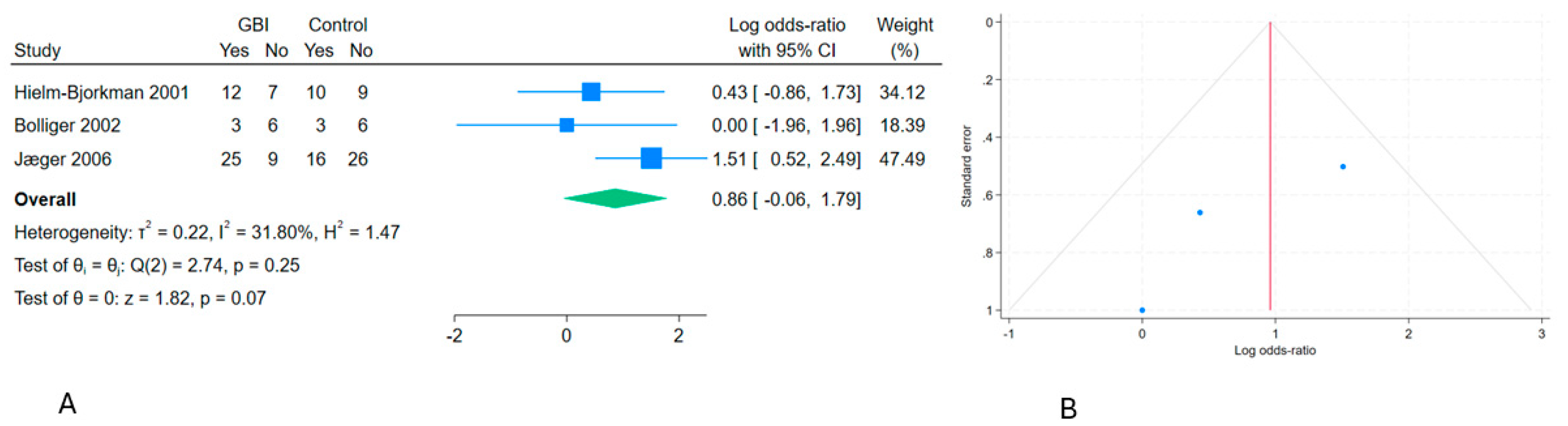
Figure 4.
Forest plot (A) and funnel plot (B) of pooled effect for osteoarthritic score of AuNP for small animal OA.
Figure 4.
Forest plot (A) and funnel plot (B) of pooled effect for osteoarthritic score of AuNP for small animal OA.
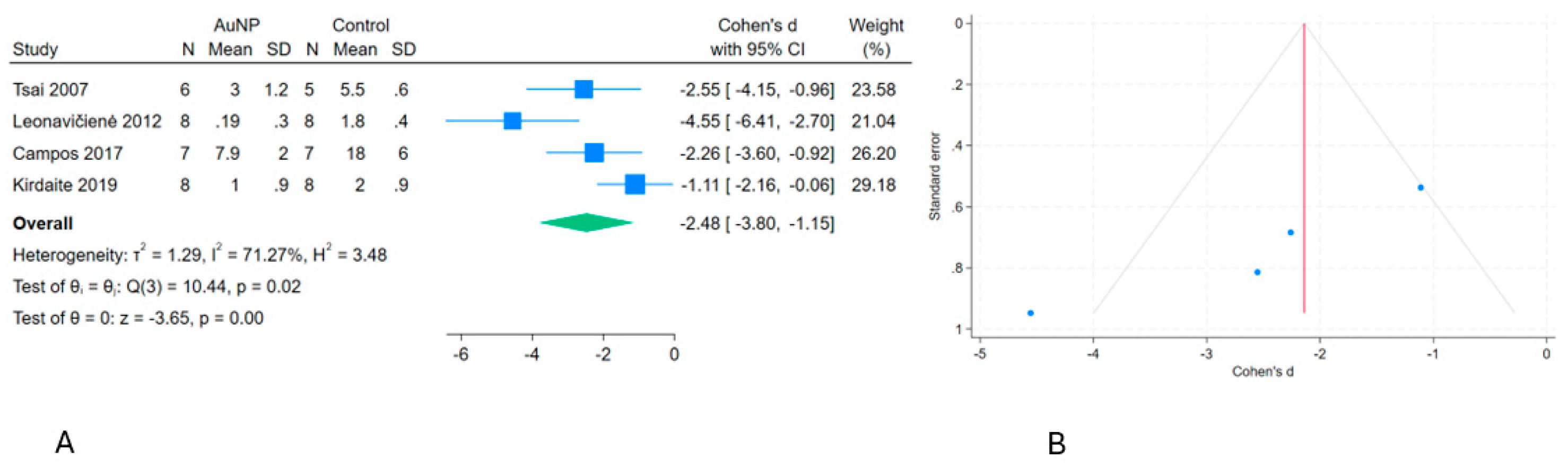
Figure 5.
Forest plot (A) and funnel plot (B) of pooled effect for TNF-Alfa of AuNP for small animal OA.
Figure 5.
Forest plot (A) and funnel plot (B) of pooled effect for TNF-Alfa of AuNP for small animal OA.
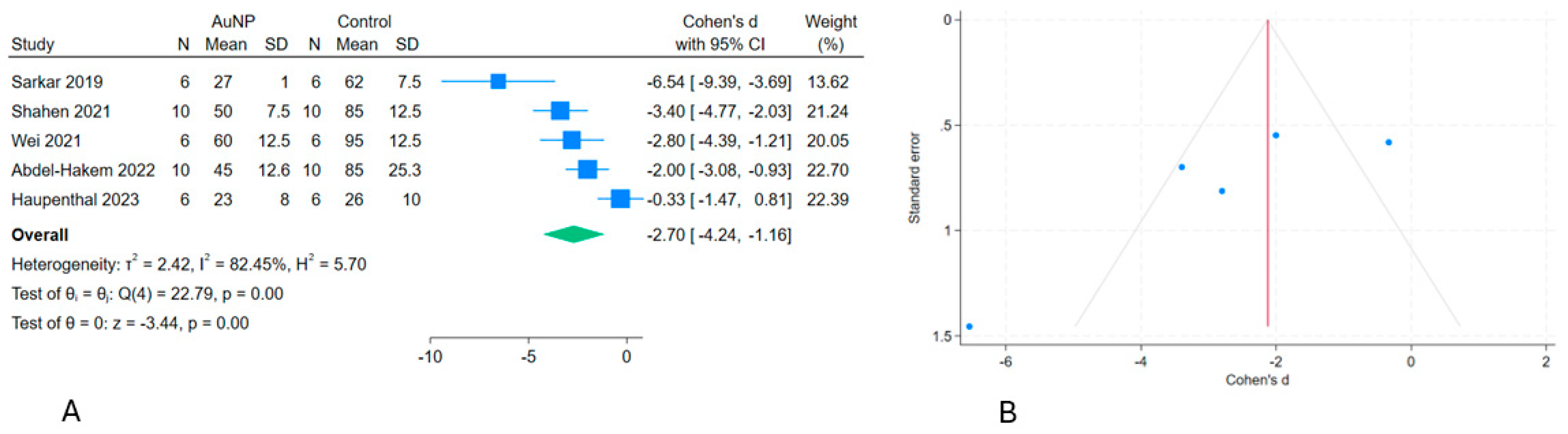
Figure 6.
Forest plot (A) and funnel plot (B) of pooled effect for number of successes of GBI for dog OA.
Figure 6.
Forest plot (A) and funnel plot (B) of pooled effect for number of successes of GBI for dog OA.
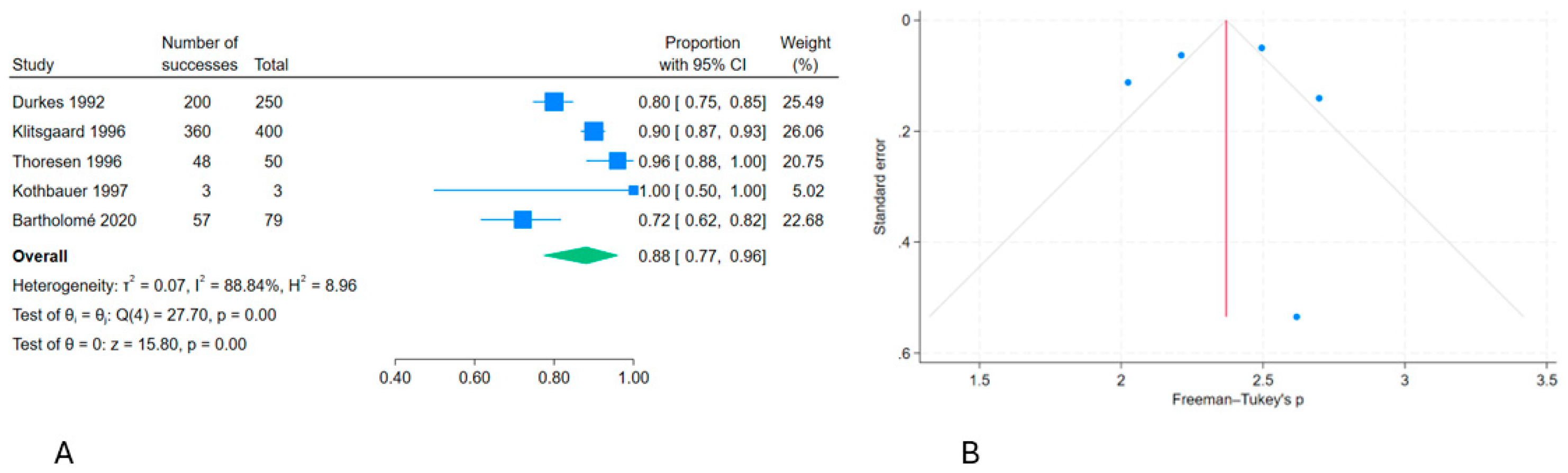
Figure 7.
Forest plot (A) and funnel plot (B) of pooled effect for number of successes of BMI for human OA.
Figure 7.
Forest plot (A) and funnel plot (B) of pooled effect for number of successes of BMI for human OA.
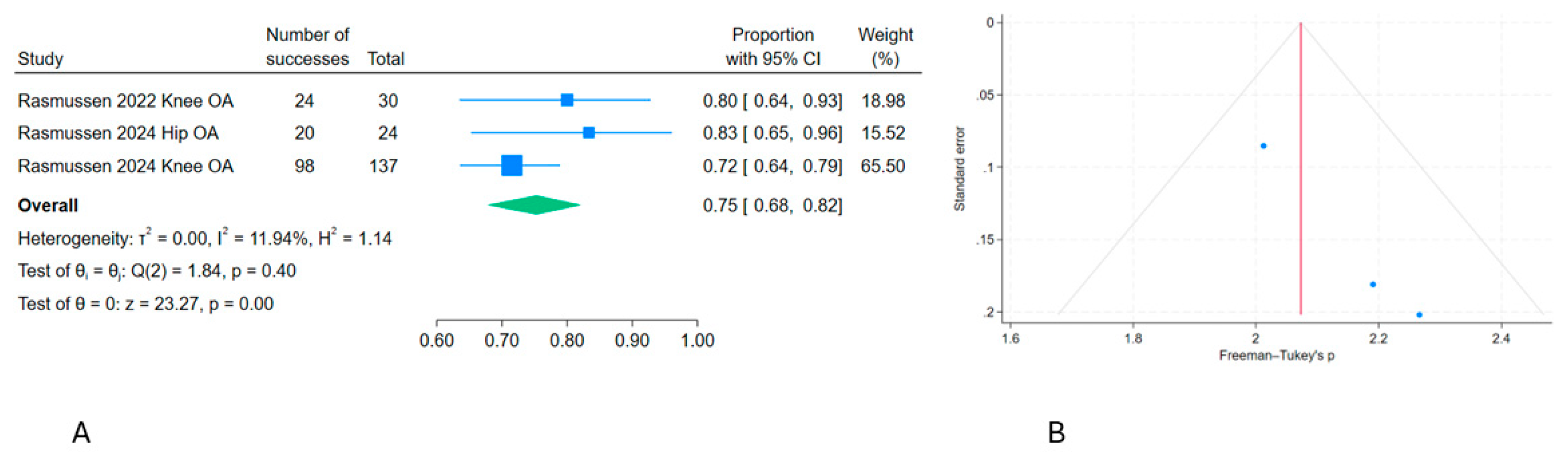

Table 1.
Study characteristics of two human randomized controlled trials of GBI for knee and cervical osteoarthritis. N = number of individuals; I = intervention group; C = control group; F-u = follow-up. Results in number improved.
Table 1.
Study characteristics of two human randomized controlled trials of GBI for knee and cervical osteoarthritis. N = number of individuals; I = intervention group; C = control group; F-u = follow-up. Results in number improved.
| Study | N-I | N-C | Intervention | Size/Weight/Area | Control | F-u | Measure | I | C |
|---|---|---|---|---|---|---|---|---|---|
| Nejrup 2008 [2] | 20 | 20 | Knee OA; 3 GBI at 5 points | 1x2.5mm/454mg/1.18cm2 | Needle | 1 y | Improved | 5 | 4 |
| Kjerkegaard 2011 [3] | 24 | 22 | Cervical OA; 3 GBI at 2-3 lamina | 1x2.5mm/>364mg/>0.942cm2 | Needle | 1 y | Improved | 16 | 2 |
Table 2.
Study characteristics of 12 animal randomized controlled studies evaluating gold bead particles (GBI) and gold nanoparticles (AuNP) for osteoarthritis. N = number of individuals; I = intervention group; C = control group; F-u = follow-up; e.a. = extra articular; i.a. = intra articular; AuNP-P = AuNP conjugated with a protein; n.a. = not available. Results in number improved or in mean and SD.
Table 2.
Study characteristics of 12 animal randomized controlled studies evaluating gold bead particles (GBI) and gold nanoparticles (AuNP) for osteoarthritis. N = number of individuals; I = intervention group; C = control group; F-u = follow-up; e.a. = extra articular; i.a. = intra articular; AuNP-P = AuNP conjugated with a protein; n.a. = not available. Results in number improved or in mean and SD.
| Study | Diagnosis | N-I | N-C | Intervention | Size/Weight/Area | Control | F-u | Measure | I | C |
|---|---|---|---|---|---|---|---|---|---|---|
| Hielm-Bjorkman 2001 [7] | Dog hip OA | 19 | 19 | 3 GBI x 3 e.a. | 1x2mm/273mg/0.71cm2 | Needle | 24w | Improved | 12 | 10 |
| Bolliger 2002 [9] | Dog hip OA | 9 | 9 | 3 GBI x ≥ 3 e.a. | 1mm/>91mg/>0.282 cm2 | Needle | 3 m | Improved | 3 | 3 |
| Jæger 2006 [8] | Dog hip OA | 36 | 42 | 3 GBI x 5 e.a. | 1x2mm/455mg/1.78cm2 | Needle | 6 m | Improved | 25 | 16 |
| Tsai 2007 [27] | Rat ankle OA | 6 | 5 | AuNP x 1, i.a. | 20nm/27µg/6.45cm2 | Buffer | 9 d | OA score 0-5 | 3(1.2) | 5.5(.6) |
| Leonavičienė 2012 [28] | Rat ankle OA | 8 | 8 | AuNP x 12 i.a. | 50nm/225.6µg/14.01cm2 | Saline | 28 d | OA score 0-3 | .19(.3) | 1.8(.4) |
| Campos 2017 [29] | Mice knee OA | 7 | 7 | AuNP-P x 15 i.a. | n.a. | Saline | 7 w | OA score 24 | 7.9(2) | 18.(6) |
| Kirdaite 2019 [30] | Rat ankle OA | 8 | 8 | AuNP x 7 i.a. | 50nm/131.6µg/8.18cm2 | Saline | 10 d | OA score 0-3 | 1 (.9) | 2 (.9) |
| Sarkar 2019 [17] | Rat knee OA | 6 | 6 | AuNP-P x 3 i.a. | 2.2nm/240µg/338.2cm2 | Saline | 15 d | TNF alfa | 27 (1) | 62(7.5) |
| Shahen 2021 [31] | Rat ankle OA | 10 | 10 | AuNP-P x 1 i.a. | n.a. | None | 42 d | TNF alfa | 50(7.5) | 85(12.5) |
| Wei 2021 [32] | Rat ankle OA | 6 | 6 | AuNP-P x 1 i.a. | 11.4nm/500µg/135.9cm2 | Saline | n.a. | TNF alfa | 60(12.5) | 95(12.5) |
| Abdel-Hakem 2022 [33] | Rat ankle OA | 10 | 10 | AuNP x1 i.a. | 25nm/6.5µg/0.81cm2 | None | 35 d | TNF alfa | 45(12.6) | 85(25.3) |
| Haupenthal 2023 [34] | Rat knee OA | 6 | 6 | AuNP x 2 i.a. | 20nm/687.5µg/106.8cm2 | None | 60 d | TNF alfa | 23(8) | 26(10) |
Table 3.
Study characteristics of 8 animal and human non-controlled studies of GBI and µGold for osteoarthritis. F-u. = follow-up; e.a. = extra articular; i.a. = intra articular; n.a. = not available.
Table 3.
Study characteristics of 8 animal and human non-controlled studies of GBI and µGold for osteoarthritis. F-u. = follow-up; e.a. = extra articular; i.a. = intra articular; n.a. = not available.
| Study | Individuals and diagnosis | Intervention | Size/Weight/Area | F-u | Measure | Results |
|---|---|---|---|---|---|---|
| Durkes 1992 [35] | 250 dogs, hip OA, dysplasia | 3 GBI at 3-16 point e.a. | 1x3mm/364mg/0.879cm2 | >3 m | Improved | 200 |
| Klitsgaard 1996 [36] | 400 dogs, hip OA or dysplasia | 3 GBI at 3 points e.a. | 1x2.5mm/341mg/0.848cm2 | 2 m | Improved | 360 |
| Thoresen 1996 [37] | 50 dogs, hip OA and dysplasia | 1 GBI at 1 point e.a. | n.a. | 1 m | Improved | 48 |
| Kothbauer 1997 [38] | 3 dogs, hip OA and dysplasia | 3 GBI at 3 points e.a. | 1x2mm/272mg0.707cm2 | >1 y | Improved | 3 |
| Bartholomé 2020 [39] | 79 dogs, hip, elbow, spine OA | 3 GBI at 3-5 points e.a. | 1x3-5mm/728mg/1.70cm2 | 2 m | Improved | 57 |
| Rasmussen 2022 [4] | 30 patients with knee OA | µGold 20 mg i.a. | 20-40nm/20mg/2.05cm2 | 2 y | Improved | 24 |
| Rasmussen 2024 [13] | 24 patients with hip OA | µGold 20 mg + HA i.a. | 20-40nm/20mg/2.05cm2 | 2 y | Improved | 20 |
| Rasmussen 2024 [12] | 137 patients with knee OA | µGold 20 mg + HA i.a. | 20-40nm/20mg/2.05cm2 | 2 y | Improved | 98 |
Table 4.
Risk of bias in 2 human randomized controlled studies investigating extraarticular gold bead implant (GBI) for osteoarthritis using the Cochrane Collaboration’s tool for assessing risk of bias. Random sequence generation (randomization), allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias.
Table 4.
Risk of bias in 2 human randomized controlled studies investigating extraarticular gold bead implant (GBI) for osteoarthritis using the Cochrane Collaboration’s tool for assessing risk of bias. Random sequence generation (randomization), allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias.
| Id | Randomization | Allocation | Blinding | Assessment | Data | Reporting | Other |
|---|---|---|---|---|---|---|---|
| Nejrup 2008 [2] | Low | Low | Low | Low | Low | Low | Low |
| Kjerkegaard 2011 [3] | Low | Low | Low | Low | Low | Low | Unclear |
Table 5.
Risk of bias in 12 animal RCT’s investigating gold for osteoarthritis, arthritic joint disease or hip dysplasia using the CAMARADES checklist. Studies fulfilling the criteria of: (1) peer reviewed publication; (2) control of temperature; (3) random allocation to treatment or control; (4) allocation concealment; (5) blinded assessment of outcome; (6) use of anesthetic without significant intrinsic neuroprotective activity; (7) animal model (osteoarthritis, arthritis and/or hip dysplasia); (8) sample size calculation; (9) compliance with animal welfare regulations; (10) statement of potential conflict of interests; (11) physiological monitoring; (12) prespecified in- and exclusion criteria; (13) reporting animals excluded from analysis; (14) and reporting of study funding.
Table 5.
Risk of bias in 12 animal RCT’s investigating gold for osteoarthritis, arthritic joint disease or hip dysplasia using the CAMARADES checklist. Studies fulfilling the criteria of: (1) peer reviewed publication; (2) control of temperature; (3) random allocation to treatment or control; (4) allocation concealment; (5) blinded assessment of outcome; (6) use of anesthetic without significant intrinsic neuroprotective activity; (7) animal model (osteoarthritis, arthritis and/or hip dysplasia); (8) sample size calculation; (9) compliance with animal welfare regulations; (10) statement of potential conflict of interests; (11) physiological monitoring; (12) prespecified in- and exclusion criteria; (13) reporting animals excluded from analysis; (14) and reporting of study funding.
| Id | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hielm-Bjorkman 2001 [7] | Dog, GBI | x | x | x | x | x | x | x | x | x | x | x | x | 12 | ||
| Bolliger 2002 [9] | Dog, GBI | x | x | x | x | x | x | x | 7 | |||||||
| Jæger 2006 [8] | Dog, GBI | x | x | x | x | x | x | x | x | x | x | x | x | 12 | ||
| Tsai 2007 [27] | Rat, AuNP | x | x | 2 | ||||||||||||
| Leonavičienė 2012 [28] | Rat, AuNP | x | x | x | x | x | x | x | x | 8 | ||||||
| Campos 2017 [29] | Mice, AuNP | x | x | x | x | x | x | x | 7 | |||||||
| Kirdaite 2019 [30] | Rat, AuNP | x | x | x | x | x | x | 6 | ||||||||
| Sarkar 2019 [17] | Rat, AuNP | x | x | x | x | x | x | x | 7 | |||||||
| Shahen 2021 [31] | Rat, AuNP | x | x | x | x | x | x | 6 | ||||||||
| Wei 2021 [32] | Rat, AuNP | x | x | x | x | 4 | ||||||||||
| Abdel-Hakem 2022 [33] | Rat, AuNP | x | x | x | x | x | x | 6 | ||||||||
| Haupenthal 2023 [34] | Rat, AuNP | x | x | x | x | x | x | x | x | x | x | 10 |
Table 6.
Risk of bias in 8 non-randomized cohort studies investigating gold for osteoarthritis, arthritic joint disease or hip dysplasia using the ROBINS-I V2 tool. Studies fulfilling the criteria of: (1) bias due to confounding; (2) bias in classification of interventions; (3) bias in selection of participants into the study (or into the analysis); (4) bias due to deviations from intended interventions; (5) bias due to missing data; (6) bias arising from measurement of the outcome; (7) and bias in selection of the reported results. Each bias domain is evaluated as low (L), moderate (M), serious (S) or critical (C).
Table 6.
Risk of bias in 8 non-randomized cohort studies investigating gold for osteoarthritis, arthritic joint disease or hip dysplasia using the ROBINS-I V2 tool. Studies fulfilling the criteria of: (1) bias due to confounding; (2) bias in classification of interventions; (3) bias in selection of participants into the study (or into the analysis); (4) bias due to deviations from intended interventions; (5) bias due to missing data; (6) bias arising from measurement of the outcome; (7) and bias in selection of the reported results. Each bias domain is evaluated as low (L), moderate (M), serious (S) or critical (C).
| Id | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|
| Durkes 1992 [35] | Dog, GBI | S | L | C | L | C | C | C |
| Klitsgaard 1996 [36] | Dog, GBI | S | L | C | L | C | C | C |
| Thoresen 1996 [37] | Dog, GBI | C | L | C | C | C | C | C |
| Kothbauer 1997 [38] | Dog, GBI | C | L | C | C | C | C | C |
| Bartholomé 2020 [39] | Dog, GBI | S | L | M | L | L | S | S |
| Rasmussen 2022 [4] | Human, µGold | L | L | L | L | L | M | M |
| Rasmussen 2024 [13] | Human, µGold | M | L | L | L | L | M | M |
| Rasmussen 2024 [12] | Human, µGold | M | L | L | L | L | M | M |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



