Submitted:
25 August 2025
Posted:
25 August 2025
You are already at the latest version
Abstract
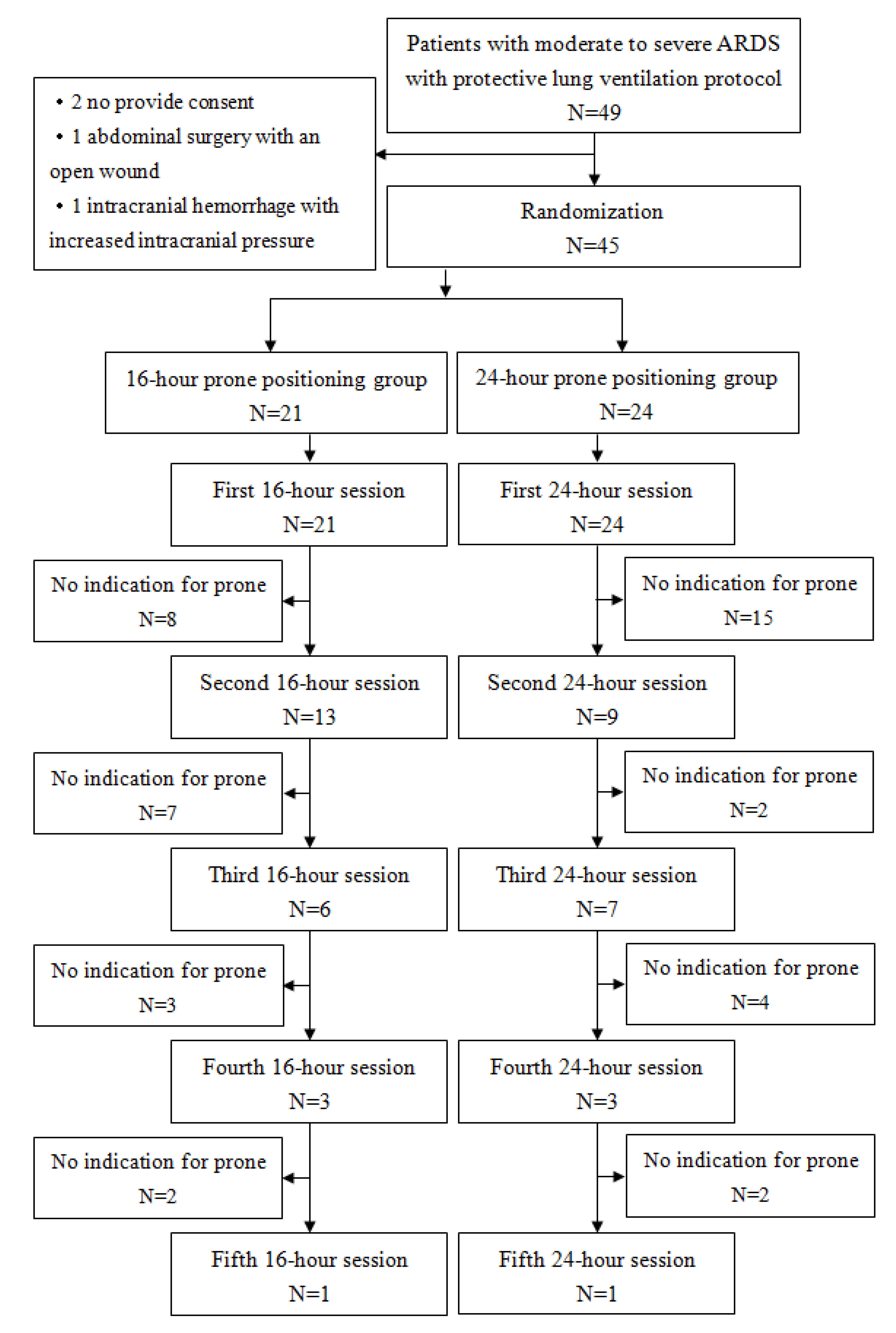
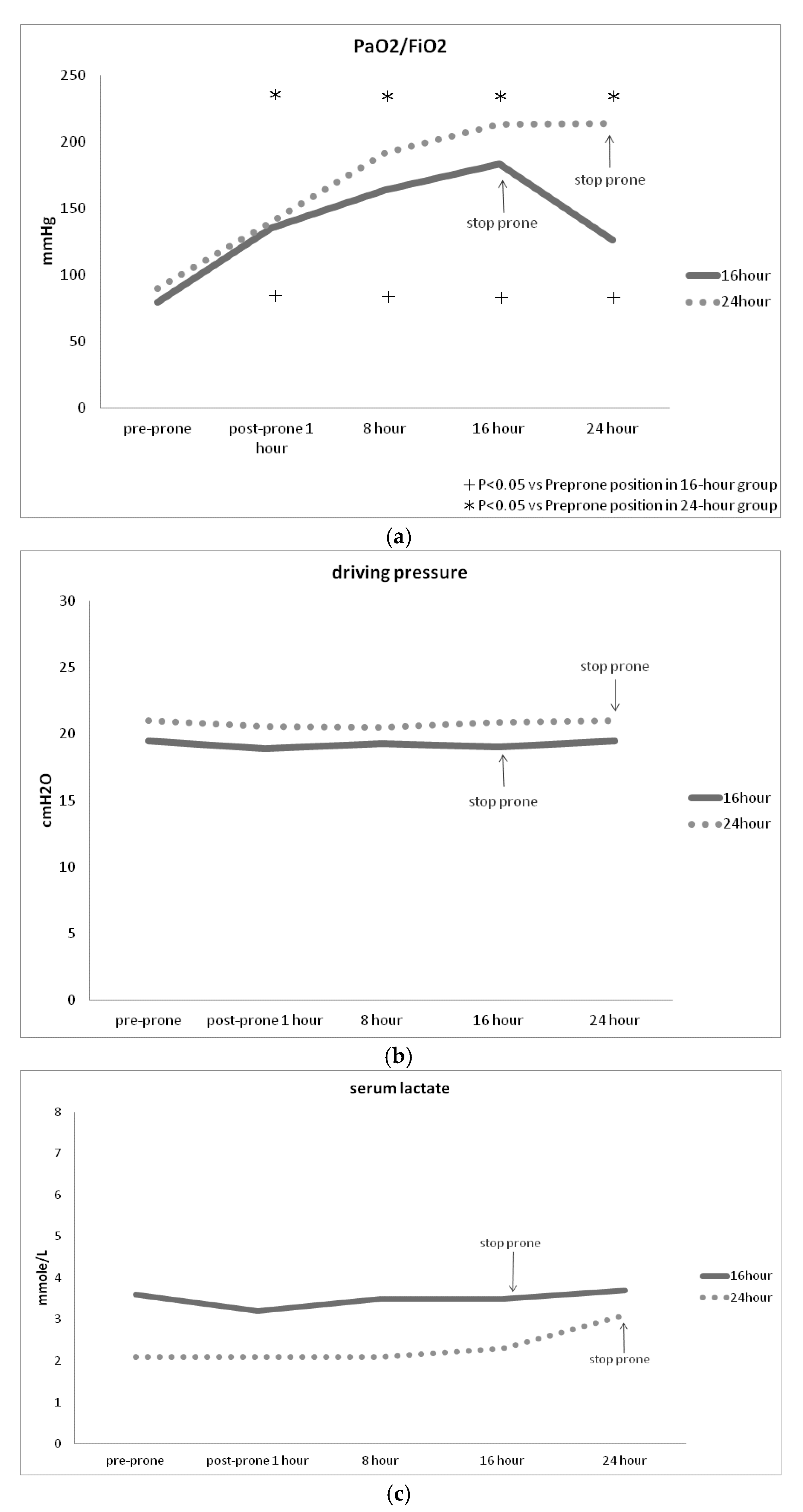
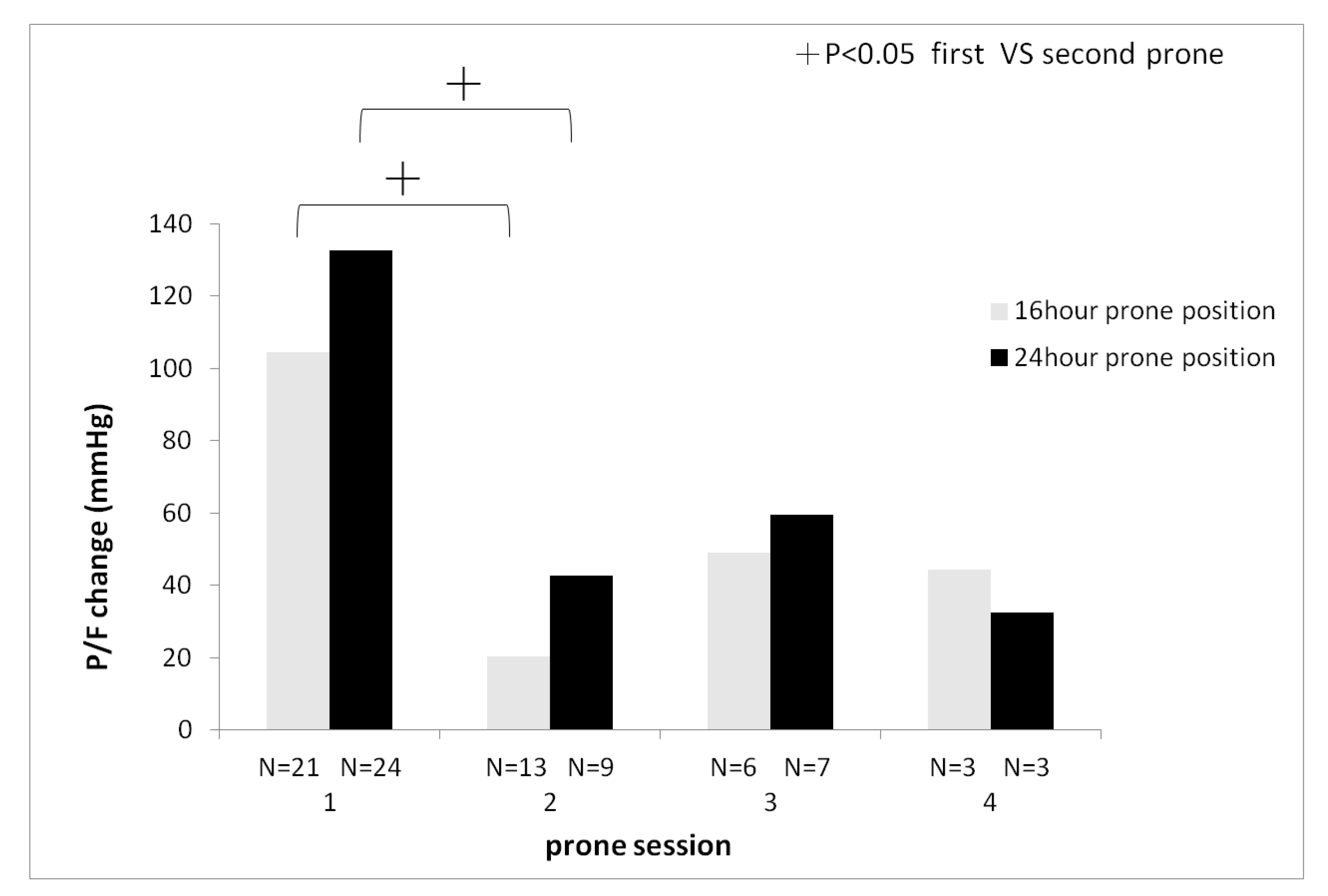
Introduction: Prolonged prone positioning, exceeding 16 hours, has been associated with decreased mortality rates among patients diagnosed with moderate to severe acute respiratory distress syndrome (ARDS). Extending the duration of prone positioning may confer greater therapeutic benefits. This study aims to assess the clinical disparities between 16-hour and 24-hour prone positioning therapy in patients with moderate to severe ARDS. Methods: This prospective randomized clinical trial was conducted in the intensive care unit of a university-affiliated tertiary medical center. Patients were randomly assigned to receive either 16-hour or 24-hour prone positioning therapy. All participants followed a protocol incorporating low tidal volume and protective lung strategies. Results: Forty-five patients diagnosed with moderate to severe ARDS requiring mechanical ventilation, 21 were allocated to the 16-hour prone positioning group, while 24 were assigned to the 24-hour group. Findings revealed no significant differences in PaO2 / FiO2 ratios, driving pressure, or serum lactate levels between the two groups. The first session of prone positioning has significantly higher PaO2 / FiO2 improvement than the second session of prone positioning (). The 24-hour group displayed a tendency toward requiring fewer prone positioning sessions compared to the 16-hour group. Secondary endpoint did not significantly differ between the two groups. Conclusions: There is a trend suggesting that the 24-hour prone positioning group necessitates fewer sessions than the 16-hour group, potentially reducing clinical workload. The first session of prone position has better improvement of oxygenation than the second session of prone position.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Enrollment
2.2. Randomization
2.3. Observations
2.4. Definitions
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Demographics
3.2. Primary Endpoints
3.3. Secondary Clinical Outcomes
4. Discussion
5. Conclusions
Institutional Review Board Statements
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, E.; Del Sorbo, L.; Goligher, EC.; Hodgson, CL.; Munshi, L.; Walkey, AJ.; Adhikari, NJK.; Amato, MBP.;, Branson, R.; Brower, RG. ; et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care. Med. 2017,195:1253-1263. [CrossRef]
- Meduri, GU.; Bridges, L.; Shih, MC.; Marik, PE.; Siemieniuk, RAC.; Kocak, M. Prolonged glucocorticoid treatment is associated with improved ARDS outcomes: analysis of individual patients' data from four randomized trials and trial-level meta-analysis of the updated literature. Intensive. Care. Med. 2016,42:829-840. [CrossRef]
- Bryan, AC. Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil's advocate. Am. Rev. Respir. Dis. 1974,110:143-144. [CrossRef]
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, JD.; Combes, A.; Dreyfuss, D.; Guérin, C.; Jaber, S.; Mekontso-Dessap, A.; Mercat, A.; et al. Formal guideline: management of acute respiratory distress syndrome. Ann. Intensive. Care. 2019,9:69. [CrossRef]
- Abroug, F.; Ouanes-Besbes, L.;Dachraoui, F.; Ouanes, I.;Brochard, L. An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury. Crit. Care. 2011,15:R6. [CrossRef]
- McAuley, DF.; Giles, S.; Fichter, H.; Perkins, GD.; Gao, F. What is the optimal duration of ventilation in the prone position in acute lung injury and acute respiratory distress syndrome?. Intensive. Care. Med. 2002,28:414-418. [CrossRef]
- Guerin, C.; Reignier, J.; Richard, JC.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013,368:2159-2168. [CrossRef]
- Amato, MB.; Barbas, CS.; Medeiros, DM.; Magaldi, RB.; Schettino, GP.; Lorenzi-Filho, G.; Kairalla, RA.;, Deheinzelin, D.; Munoz, C.; Oliveira, R.; Takagaki, TY.; et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N. Engl. J. Med. 1998,338:347-354. [CrossRef]
- Ferguson, ND.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: an expanded rational, justification, and supplementary material. Intensive. Care. Med. 2012,38:1573-1582. [CrossRef]
- Miller, PR.; Johnson, JC 3rd.; Karchmer, T.; Hoth, JJ.; Meredith, JW.; Chang, MC. National Nosocomial Infection Surveillance System: From benchmark to bedside in trauma patients. J. Trauma. 2006,60:98-103. [CrossRef]
- Kallet, RH. A Comprehensive Review of Prone Position in ARDS. Respir. Care. 2015,60:1660-1687. [CrossRef]
- Lamm, WJ.; Graham, MM.; Albert, RK. Mechanism by which the prone position improves oxygenation in acute lung injury. Am. J. Respir. Crit. Care. Med. 1994,150:184-193. [CrossRef]
- Albert, RK.; Leasa, D.; Sanderson, M.; Robertson, HT.; Hlastala, MP. The prone position improves arterial oxygenation and reduces shunt in oleic-acid-induced acute lung injury. Am. Rev. Respir. Dis. 1987,135:628-633. [CrossRef]
- Albert, RK.; Hubmayr, RD. The prone position eliminates compression of the lungs by the heart. Am. J. Respir. Crit. Care. Med. 2000,161:1660-1665. [CrossRef]
- Malbouisson, LM.; Busch, CJ.; Puybasset, L.; Lu, Q.; Cluzel, P.; Rouby, JJ. Role of the heart in the loss of aeration characterizing lower lobes in acute respiratory distress syndrome. CT Scan ARDS Study Group. Am. J. Respir. Crit. Care. Med. 2000,161:2005-2012. [CrossRef]
- Amato, MB.; Meade, MO.; Slutsky, AS.; Brochard, L.; Costa, EL.; Schoenfeld, DA.; Stewart, TE.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015,372:747-755. [CrossRef]
- Ladha, K.; Vidal Melo, MF.; McLean, DJ.; Wanderer, JP.; Grabitz, SD.; Kurth, T.; Eikermann, M. Intraoperative protective mechanical ventilation and risk of postoperative respiratory complications: hospital based registry study. BMJ. 2015,351:h3646. [CrossRef]
- Roca, O.; Peñuelas, O.; Muriel, A.; García-de-Acilu, M.; Laborda, C.; Sacanell, J.; Riera, J.; Raymondos, K.; Du, B.; Thille, AW.; et al. Driving pressure is a risk factor for ARDS in mechanically ventilated subjects without ARDS. Respir. Care. 2021,66:1505-1513. [CrossRef]
- Riad, Z.; Mezidi, M.; Subtil, F.; Louis, B.; Guérin, C. Short-term effects of the prone positioning manoeuver on lung and chest wall mechanics in ARDS Patients. Am. J. Respir. Crit. Care. Med. 2018,197:1355-1358. [CrossRef]
- Munshi, L.; Del Sorbo, L.; Adhikari, NKJ.; Hodgson, CL.; Wunsch, H.; Meade, MO.; Uleryk, E.; Mancebo, J.; Pesenti, A.; Ranier, VM.; et al. Prone Position for Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis. Ann. Am. Thorac. Soc. 2017,14:S280-S288. [CrossRef]
- Kraut ,JA.; Madias, NE. Lactic acidosis. N. Engl. J. Med. 2014,371:2309-2319. [CrossRef]
- Yoshida, T.; Tanaka, A.; Roldan, R.; Quispe, R.; Taenaka, H.; Uchiyama, A.; Fujino, Y. Prone position reduces spontaneous inspiratory effort in patients with acute respiratory distress syndrome: A bicenter study. Am. J. Respir. Crit. Care. Med. 2021,203:1437-1440. [CrossRef]
- Johannigman, JA.; Davis, K Jr.; Miller, SL.; Campbell, RS.; Luchette, FA.; Frame, SB.; Branson, RD. Prone positioning for acute respiratory distress syndrome in the surgical intensive care unit: Who when and how long? Surgery. 2000,128:708-716. [CrossRef]
- Blanch, L.; Mancebo, J.; Perez, M.; Martinez, M.; Mas, A.; Betbese, AJ.; Joseph, D.; BalluÂs, J.; Lucangelo, U. Short-term effects of prone position in critically ill patients with acute respiratory distress syndrome. Intensive. Care. Med. 1997,23:1033-1039. [CrossRef]
- Gattinoni, L.; Vagginelli, F.; Carlesso, E.; Taccone, P.; Conte, V.; Chiumello, D.; Valenza, F.; Caironi, P.; Pesenti, A. Decrease in PaCO2 with prone position is predictive of improved outcome in acute respiratory distress syndrome. Crit. Care. Med. 2003,31:2727-2733. [CrossRef]
- Lee, DL.; Chiang, HT.; Lin, SL.; Ger, LP.; Kun, MH.; Huang, YC. Prone position ventilation induces sustained improvement in oxygenation in patients with acute respiratory distress syndrome who have a large shunt. Crit. Care. Med. 2002,30:1446-1452. [CrossRef]
- L’Her, E.; Renault, A.; Oger, E.; Robaux, MA.; Boles, JM. A prospective survey of early 12-h prone positioning effects in patients with acute respiratory distress syndrome. Intensive. Care. Med. 2002,28:570-575. [CrossRef]
- Girard, R.; Baboi, L.; Ayzac, L.; Richard, J-C.; Guérin, C.; Group, PT. The impact of patient positioning on pressure ulcers in patients with severe ARDS: results from a multicentre randomised controlled trial on prone positioning. Intensive. Care. Med. 2014,40:397-403. [CrossRef]
- Lee, JM.; Bae, W.; Lee, YJ.; Cho, Y-J. The efficacy and safety of prone positional ventilation in acute respiratory distress syndrome: updated study-level meta-analysis of 11 randomized controlled trials. Crit. Care. Med. 2014,42:1252-1262. [CrossRef]
- Page, DB.; Russell, DW.; Gandotra, S.; Dransfield, MT. Prolonged prone position for COVID-19-induced acute respiratory distress syndrome: a randomized pilot clinical trial. Ann. Am. Thoracic. Soc. 2022,19:685-687. [CrossRef]

| Characteristic | 16-hour (N=21) |
24-hour (N=24) |
P value |
|---|---|---|---|
| Gender (M/F) | 11/10 | 10/14 | 0.47 |
| Age, year | 71.1± 13.6 | 69.0 ± 11.2 | 0.59 |
| BMI (kg/m2) | 23.2 ± 3.3 | 24.9 ± 6.3 | 0.27 |
| Organ failure number | 2.3 ± 1.2 | 2.3 ± 1.1 | 1.00 |
| APACHE II score | 26.6 ± 7.3 | 27.4 ± 7.7 | 0.72 |
| Sedation (%) | 21 (100) | 24 (100) | 0.99 |
| Muscle relaxant (%) | 18 (85.7) | 24 (100) | 0.06 |
| Vasopressor (%) | 18 (85.7) | 17 (70.8) | 0.22 |
| Steroid (%) | 17 (81.0) | 20 (83.3) | 0.81 |
| ARDS to prone day | 1.1 ± 1.9 | 1.0 ± 1.3 | 0.91 |
| Pulmonary ARDS (%) | 16 (76.2) | 20 (83.3) | 0.55 |
| Extrapulmonary ARDS (%) | 5 (23.8) | 4 (16.7) | 0.55 |
| Serum lactate (mmole/L) | 3.6 ± 3.5 | 2.1 ± 1.1 | 0.08 |
| Characteristic | 16-hour (N=21) |
24-hour (N=24) |
P value |
|---|---|---|---|
| PaO2/ FiO2 (mmHg) | 79.3 ± 31.9 | 89.7 ± 30.5 | 0.27 |
| PaO2 (mmHg) | 75.4 ± 28.9 | 78.9 ± 23.4 | 0.67 |
| PaCO2 (mmHg) | 46.3 ± 28.9 | 53.3 ± 18.5 | 0.12 |
| pH | 7.4 ± 0.1 | 7.3 ± 0.1 | 0.13 |
| Respiratory rate (breath/minute) | 23.1 ± 4.9 | 22.1 ± 5.8 | 0.55 |
| Tidal Volume (mL) | 456.4 ± 120.4 | 462.8 ± 117.2 | 0.86 |
| PEEP (cmH2O) | 12.0 ± 3.1 | 11.5 ± 2.6 | 0.53 |
| Compliance (mL/cmH2O) | 23.8 ± 8.9 | 23.2 ± 8.8 | 0.82 |
| Driving pressure (cmH2O) | 19.5 ± 4.5 | 21.0 ± 4.2 | 0.25 |
| Mean airway pressure (mmHg) | 19.2 ± 3.1 | 19.3 ± 3.6 | 0.92 |
| Characteristic | 16-hour (N=21) |
24-hour (N=24) |
P value |
|---|---|---|---|
| Session >1 of prone position (%) | 13 (61.9) | 9 (37.5) | 0.06 |
| Change of P/F after stopping prone position (mmHg) | 111.4 ± 134.7 | 74.8 ± 71.9 | 0.28 |
| Tube dislodgement (%) | 1 (4.8) | 0 (0) | 0.28 |
| Endotracheal tube obstruction (%) | 1 (4.8) | 2 (8.3) | 0.63 |
| Pressure sore (%) | 1 (4.8) | 4 (16.7) | 0.13 |
| Ventilator-associated pneumonia (%) | 1 (4.8) | 3 (12.5) | 0.35 |
| Weaning ventilator (%) | 9 (42.9) | 9 (37.5) | 0.71 |
| Mortality (%) | 12 (57.1) | 13 (54.2) | 0.86 |
| Change of PaCO2 (mmHg) | 3.2 ± 10.9 | 9.6 ± 15.3 | 0.12 |
| Change of P/F after prone position (mmHg) | 104.4 ± 84.9 | 123.1 ± 105.2 | 0.52 |
| PaO2/ FiO2 responder (%) | 20 (95.2) | 23 (95.8) | 0.88 |
| Rescue ECMO (%) | 0 (0) | 0 (0) | 0.99 |
| 30-day outcomes | |||
| ICU-free days | 18.2 ± 7.7 | 14.4 ± 7.2 | 0.28 |
| Ventilator-free days | 16.1 ± 9.1 | 9.7 ± 7.3 | 0.16 |
| Alive and liberated from ventilator (%) | 8 (38.1) | 7 (29.2) | 0.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



