Submitted:
21 August 2025
Posted:
26 August 2025
You are already at the latest version
Abstract
Background: Muscle health is an emerging concept, increasingly cited in studies associated with physical performance and functional independence. However, the term lacks a clear operational or conceptual definition and often serves as a general descriptor of any muscle-related outcome. Clinical communication and research designs would benefit from a sound conceptual model of muscle health grounded in an established framework concerning physical health and muscle function. Methods: Thus, our proposed model is informed by a systematic literature review and synthesis regarding the multi-factorial measurement approaches used to characterize skeletal muscle. Three investigators screened 333 papers with search criteria for clinical and randomized controlled trials and "muscle health". Results: Of the 68 papers that met inclusion criteria, 31 studies provided an operational definition of "muscle health", while 37 inferred measurements without a clear definition. The identified measurements spanned four primary categories, with body composition/muscle mass being the most common (92.7%), followed by muscle performance (76.5%), physical function (61.8%), and tissue composition (30.9%). Most studies included more than one muscle health metric (94.1%). Common assessment methods included DXA (41.2%), grip strength (63.2%), and gait speed (26.5%). Conclusions: Using the framework of the International Classification of Functioning, Disability and Health, measurement categories identified aligned with muscle health components of muscle morphology/morphometry (e.g., muscle mass and composition), functional status (performance-based tasks), and physical capacity (objective maximal or submaximal measures of muscle performance). Consistently applying these measurement domains could aid the assessment of muscle health and facilitate further work to standardize specific approaches to testing and data interpretation across settings.
Keywords:
functional capacity
; morphology
; muscle performance
; physiology
; strength
; tissue composition
; muscle health
1. Introduction
Skeletal muscle tissue plays a critical role in maintaining overall health. Normal muscle function influences health in various ways, from regulating glucose and insulin homeostasis and storing amino acids to facilitating recovery from hospitalization and sustaining functional independence [1,2]. While the term ‘muscle health’ is widely used in research, it may denote various elements associated with muscle function that differ among researchers and practitioners [3,4]. Although components of muscle health are typically listed when the term is used in a study, standardized or operational definitions are rarely provided, or the term is used inconsistently [5]. Moreover, the frameworks used to provide theoretical constructs of muscle health are seldom provided in clinical studies [2,5]. Frameworks typically outline key constructs and their interrelationships, often drawing on existing literature, models, or theories. However, there is no consistent approach to the framework and components of muscle health when applied to clinical evaluations or outcome measurements in research settings. Without clear models or frameworks for muscle health, we will continue to observe a lack of proactive approaches to detect and manage common forms of muscle dysfunction associated with chronic disease and geriatric syndromes [5,6].
The traditional geriatric vital signs obtained during a physical examination include blood pressure, pulse, respiratory rate, and temperature [7]. Nevertheless, others have proposed expanding the geriatric physical examination by including additional tests and screening measures related to cognition, walking speed, and muscle performance [6,8,9]. The proposed expansion of the geriatric examination to include measures of muscle performance reflects the need to progress towards a standardized definition of muscle health. Ideally, establishing a standardized definition of muscle health precedes the attainment of consensus on key tests and measures as well as approaches to specific test protocols and data interpretation. Selected tests and measures must be aligned with components (e.g., categorical assessments of muscle tissue, muscle performance, and functional performance) that characterize accepted domains of muscle health. In turn, the domains associated with muscle health should be aligned with established conceptual frameworks regarding physical health and general principles that guide the physical examination process. The relationship among frameworks, domains, components, and assessment is depicted in Figure 1. Clarity regarding the framework for muscle health and approaches to objective measures that provide utility in both clinical and research settings would aid the clinical management of muscle in a variety of patient populations. A viable framework requires an understanding of how skeletal muscle tissue impacts physical health and determining selected tests and measures that appropriately characterize muscle tissue and physical performance.
1.1. What is health?
The concept of ‘health’ now encompasses physical, mental, and social well-being, rather than solely the absence of disease, illness, and disability [10]. John Ware and colleagues [11] further expand upon this view by describing multiple health dimensions comprising two global health measures: mental and physical health. Physical health encompasses being free from diseases or ailments that result in physical impairments, performing daily activities and functional tasks without restriction, and having the capacity for physical activity through adequate strength, flexibility, and endurance [12]. Ware et al., [11] have further indicated that the dimensions of overall physical health include physical functioning and limitations due to physical challenges. Multiple investigators have observed that declines in muscle strength are frequently associated with diminished performance in activities of daily living (ADL) and instrumental activities of daily living (IADL) [13,14].
This review broadly focuses on physical health, emphasizing how skeletal muscle tissue impacts physical functioning. Physical function (i.e., purposeful movement encompassing both basic and more complex tasks), requires complex interactions involving the musculoskeletal and nervous systems with support from the respiratory, cardiovascular, endocrine, skeletal, and integumentary systems [15]. Engaging in functional tasks and other forms of physical activity may demand the requisite muscle strength and endurance, but also dexterity, coordination, visual acuity, and balance. While functional assessments alone cannot confirm muscle impairments, functional assessments used in conjunction with other physiological measures can aid in the identification of various forms of muscle dysfunction.
Older adults tend to be most impacted by muscle dysfunction, with 35% percent of adults aged 65 years or above not being able to complete at least one ADL, and 53% not being able to complete at least one IADL [16]. In addition, estimates of low muscle mass and poor muscle composition have significant positive associations with poorer ADLs and IADL performance in older adults [17,18,19,20,21,22]. The emerging efforts to describe and assess muscle health specifically examine the role of skeletal muscle as a facilitator or inhibitor of physical health and the performance of functional tasks. Therefore, the assessment of muscle health should include direct or surrogate measures of skeletal muscle tissue that may range from morphology and morphometry to estimates of muscle mass. Identifying muscle pathology, poor muscle composition, or low muscle mass may aid the differential diagnosis process in clinical settings and identify when skeletal muscle significantly contributes to diminished physical health [2,6,20].
1.2. In Search of a Muscle Health Assessment Framework
Muscle health may be viewed as a subset of physical health. Given the interrelationship of these health concepts, the framework suggested by Koipysheva et al. [23] for assessing physical health pertains to muscle health. This assessment approach includes: 1) a physical examination, which may comprise anthropometric and/or physiologic measures (e.g., body composition estimates and/or muscle tissue morphological assessments), and 2) tests of “motor qualities” that are associated with functional tasks and physical capacity (e.g., functional tests and muscle performance measures). The application of this framework to assess muscle health is consistent with established typologies classifying health and related domains, such as the International Classification of Functioning, Disability and Health (ICF) [15,24], which delineates components of health and selected health-related aspects of well-being (Figure 1). Domains of ICF include 1) ‘Body Functions and Structures’, and 2) ‘Activities and Participation’ [15]. Considering muscle health within the context of the ICF, using the assessment approach suggested by Koipysheva and colleagues [23], ‘Body Functions’ may be represented by measures of muscle performance; ‘Body Structures’ include estimates of muscle mass and/or muscle composition; and ’Activities’ can be assessed through observed tests of physical performance using functional tasks. Incorporating this approach to assessing muscle health facilitates further integration with the ICF, as one considers how pathology may impair muscle performance and how muscle impairments may affect physical functioning and participation in various environmental settings.
Establishing a common understanding and lexicon for muscle health includes identifying clear measurement domains while also distinguishing this approach from other established frameworks [2,25]. The larger constructs inform muscle health, physical health, and physical capacity, with measurement domains for 1) body/muscle tissue composition, 2) muscle performance, and 3) functional status (Figure 1). However, another emerging construct related to the assessment of skeletal muscle is muscle quality [26]. The central physiological functions of muscle tissue have been previously categorized into the following domains: force production, metabolism, thermoregulation, and signaling/myokine production [2]. Assessments of muscle quality ultimately reflect the degree to which muscle tissue fulfills these physiologic roles while at rest and in response to increased physical demands [20,25,26]. Surrogate measures of muscle quality, such as muscle density assessed using computed tomography (CT) scans and estimates of muscle mass, have been increasingly linked to hospitalization risk and mobility loss in older adults [20,22,27]. Although muscle quality may be reflected in the proposed muscle health measurement domains of body/muscle tissue composition and muscle performance, it does not require an assessment of functional status. Therefore, the construct of muscle quality may be integrated into the framework for muscle health.
Within gerontology, factors related to hospitalization and recovery from illness are often expressed using the terms intrinsic capacity and physical resilience. Intrinsic capacity reflects one’s ability to maintain autonomy and independence in the face of physical stressors (such as illness, which may lead to hospitalization) [28]. The assessment of intrinsic capacity using World Health Organization guidelines allows for measures of muscle strength and mobility status, but not the evaluation of muscle mass or composition [29]. In contrast, resilience often refers to one’s ability to regain physical, mental, and social well-being after encountering stressors such as health challenges, functional declines, or significant life transitions [30,31]. The three main domains of resilience are cognitive, physical, and psychosocial, with physical resilience being defined as one’s ability to recover from health stressors or physically traumatic events [30,31,32]. Clinical assessments of physical resilience include subjective measures of functional status [32], but lack objective measures of body/tissue composition or muscle performance. The proposed framework for muscle health (Figure 1) identifies elements of the skeletal muscle system that impact patient outcomes and features measurement domains that are not fully represented in other health constructs, such as muscle quality, intrinsic capacity, and physical resilience.
Consequently, the objectives of this study are to determine how researchers define and evaluate muscle health in the current literature and to determine if the outcome measures in the cited works in this review align with the proposed muscle health framework. Our goal is to gather data to support consensus efforts regarding a common framework and standardized approach to defining muscle health. Establishing a standardized approach to assessing muscle health could enhance the identification of muscle dysfunction, support proactive strategies to address the consequences of muscle aging, and facilitate the use of common methodologies within this area of study.
2. Materials and Methods
A systematic review was conducted to identify papers using the term ‘muscle health’ to better understand the conceptual and operational definition of muscle health used by other investigators and document the assessment tools used to characterize muscle health. These study data and definitional terms were then extracted and combined where appropriate to synthesize the current use of the term ‘muscle health’. This information was then interpreted using the ICF framework to develop a proposed conceptual model for ‘muscle health’.
2.1. Eligibility
Research studies must have included muscle health assessment as an element of clinical investigation. Articles that were excluded are non-human studies, case studies, review articles, or studies lacking outcomes that characterize muscle tissue and/or muscle performance.
2.2. Information Sources and Search Strategy
Research articles were searched on the CINAHL and PubMed databases. The keyword ‘muscle health’ was searched. From those results, the articles were filtered only to include clinical or randomized controlled trials completed in the last five years from March 2025, with the full text available in English. Database results were downloaded and transferred to the Zotero reference manager (v6.0; Corporation for Digital Scholarship, Virginia, USA). Covidence (v2627; Melbourne, AUS; https://www.covidence.org/) was used to import all selected articles from the initial search. Duplicate articles were removed for appraisal. A total of three reviewers participated. Reviewers determined if the outcomes measured muscle health and how it was defined and measured in that study. Covidence was used to import and divide the literature among the reviewers. Every article imported was first screened independently based on the title and abstract by two reviewers. The criteria for the title/abstract screen were that 1) the article mentions ‘muscle health’ in the title/abstract, and 2) it is evident that the study featured outcome measures associated with muscle tissue and/or muscle function. A third reviewer was utilized if disagreements arose based on the eligibility criteria. Three independent reviewers then reviewed the full texts of the articles. The article must have provided an operational or conceptual definition of ‘muscle health’ as a criterion for full-text review. An additional reviewer was utilized if disagreements arose based on the eligibility criteria.
2.3. Data Extraction
The review of selected publications included the study premise, the population being studied, whether an operational or conceptual definition of ‘muscle health’ was provided, and how muscle health was being measured. The study's outcome was also included in the summary table (Table 1) if an operational definition was provided. Study characteristics were entered and analyzed in an Excel spreadsheet (Microsoft Corporation, Redmond, WA). Muscle health definitions were stripped of non-essential words (e.g., ‘and’, ‘the’, ‘along with’, ‘characterized by’), with continuous terms connected with dashes (e.g., ‘muscle mass’ vs. ‘muscle-mass’). Key terms from each operational definition were categorized into five general ‘muscle health’ components: ‘body composition’, ‘physical function’, ‘muscle performance’, ‘tissue composition’, and ‘other’. A word cloud visualization with component-based color coding was generated using OpenAI’s ChatGPT (GPT-4o, April 2025) to script and render the figure in Python, utilizing the WordCloud and Matplotlib libraries.
2.4. Data analysis and Interpretation
We employed a mixed synthesis approach combining quantitative tallying of measurement domains with qualitative thematic analysis to develop a proposed model of muscle health using the ICF framework. Each identified study was reviewed for the inclusion of assessments of body composition, tissue composition, muscle performance, and functional performance. Common language from operational definitions was extracted and analyzed (see Figure 3). Frequencies of inclusion across these domains were calculated (see Figure 4, Figure 5, Figure 6, Figure 7 and Figure 8). These data were interpreted in conjunction with the ICF framework and prior theoretical models [23], enabling us to identify recurring elements and their contextual applications. While we did not apply formal weighting algorithms, the frequency, co-occurrence, and contextual integration of each domain across studies informed the proposed components (body/muscle tissue composition, muscle performance, functional performance) for the model. The development of the conceptual muscle health model utilized a flexible approach that provides proposed domains and component categories suitable for clinical or research applications. Nevertheless, the final selection of tests and measures used to assess muscle health components and the recommended data interpretation standards are beyond the scope of this work. The identification of assessment standards consistent with a conceptual muscle health model is subject to further research and future consensus efforts.
3. Results
3.1. Data Extraction
The search strategy and results are summarized in Figure 2. The original search (up to May 2023) resulted in 261 studies gathered between databases CINAHL (n=198) and PubMed (n=63). Thirteen studies were removed due to duplicate studies between databases. After the initial title and abstract screen, 158 studies were excluded. A full-text review was performed of the remaining 88 studies, with 44 studies included in the review [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76]. Thirty-nine were excluded because the studies failed to meet the criteria for measuring or defining muscle health. Three studies were excluded due to insufficient study design: one due to an unfinished study and two due to access issues. The final search (May 2023 to March 2025) resulted in 90 hits (CINAHL=73; PubMed=17), with 10 duplicate pairs. Following title and abstract screening, 24 studies were accepted and added to the original batch of included studies [77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101]. In total, 68 studies were included in this review [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101].
3.2. Identified Study Characteristics
Of the 68 included studies [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101], all measured one or more components of muscle health, which included the categories: body composition, muscle tissue composition, muscle performance and functional tasks. Thirty-one studies provided an operational definition of ‘muscle health’ [33,37,38,41,43,45,47,51,52,55,57,58,61,64,65,66,68,72,73,74,76,77,79,80,82,87,88,91,92,93,94], while the other 37 assessed ‘muscle health’, but did not state an operational definition [34,35,36,39,40,42,44,46,48,49,50,53,54,56,59,60,62,63,67,69,70,71,75,78,81,83,84,85,86,89,90,95,96,97,98,99,100]. Studies with an operational definition are summarized in Table 1, while those lacking an operational definition are summarized in Table 2.
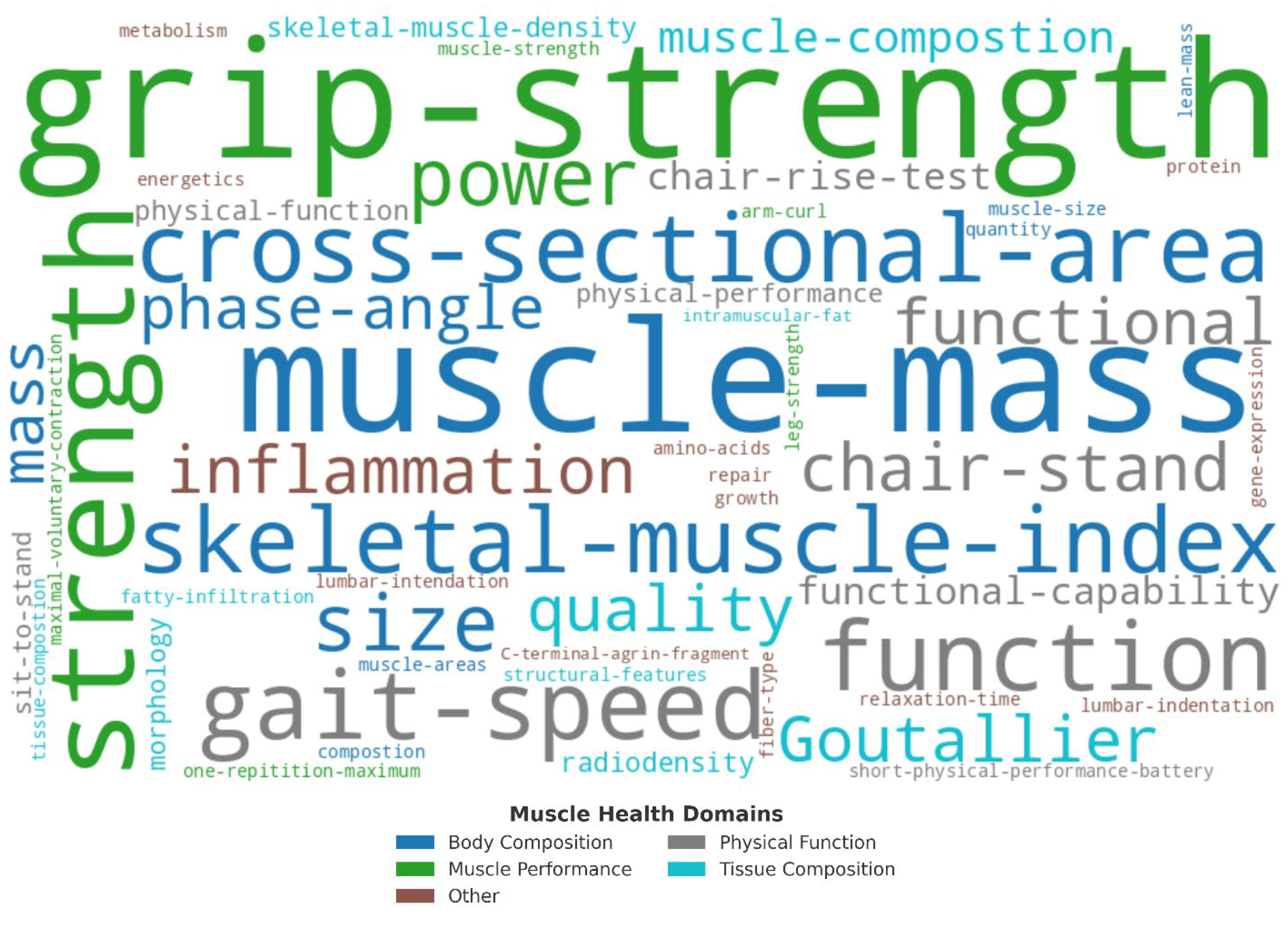
A word cloud of the 31 operational definitions [33,37,38,41,43,45,47,51,52,55,57,58,61,64,65,66,68,72,73,74,76,77,79,80,82,87,88,91,92,93,94], is provided in Figure 3. Operational definitions most commonly included ‘muscle mass’ (11), ‘grip-strength’ (9), ‘cross-sectional area’ (7), ‘function’ (6), ‘strength’ (6), ‘power’ (4), ‘gait speed’ (4), ‘skeletal muscle index’ (4), ‘Goutallier’ classification (4), ‘size’ (3), ‘quality’ (2), ‘physical performance’ (2), ‘mass’ (2), ‘phase angle’ (2), ‘lumbar indentation’ (2), and ‘chair stand’ (2).
Figure 3.
Word cloud visualization of key words extracted from 31 operational definitions of muscle health. Words were categorized into five components: body composition (blue), physical function (grey), muscle performance (green), tissue composition (teal), and other (rust). Word size reflects term frequency across definitions.
Figure 3.
Word cloud visualization of key words extracted from 31 operational definitions of muscle health. Words were categorized into five components: body composition (blue), physical function (grey), muscle performance (green), tissue composition (teal), and other (rust). Word size reflects term frequency across definitions.
Of the 31 studies providing an operational definition [33,37,38,41,43,45,47,51,52,55,57,58,61,64,65,66,68,72,73,74,76,77,79,80,82,87,88,91,92,93,94], all but one [47] (N=30, 96.8%) assessed body composition or muscle size, 20 (64.5%) measured muscle performance (e.g., grip strength, isometric or isokinetic strength) [37,41,45,51,52,55,57,61,64,66,68,72,76,79,80,82,91,92,93,94], 19 (61.3%) measured functional performance (e.g., short physical performance battery [SPPB], gait speed) [37,43,47,51,52,55,57,64,66,68,72,76,77,79,80,91,92,93,94], while 14 (45.2%) included tissue composition (e.g., echogenicity, intramuscular adipose tissue) assessments [33,37,38,41,52,58,65,73,74,82,87,88,93,94].
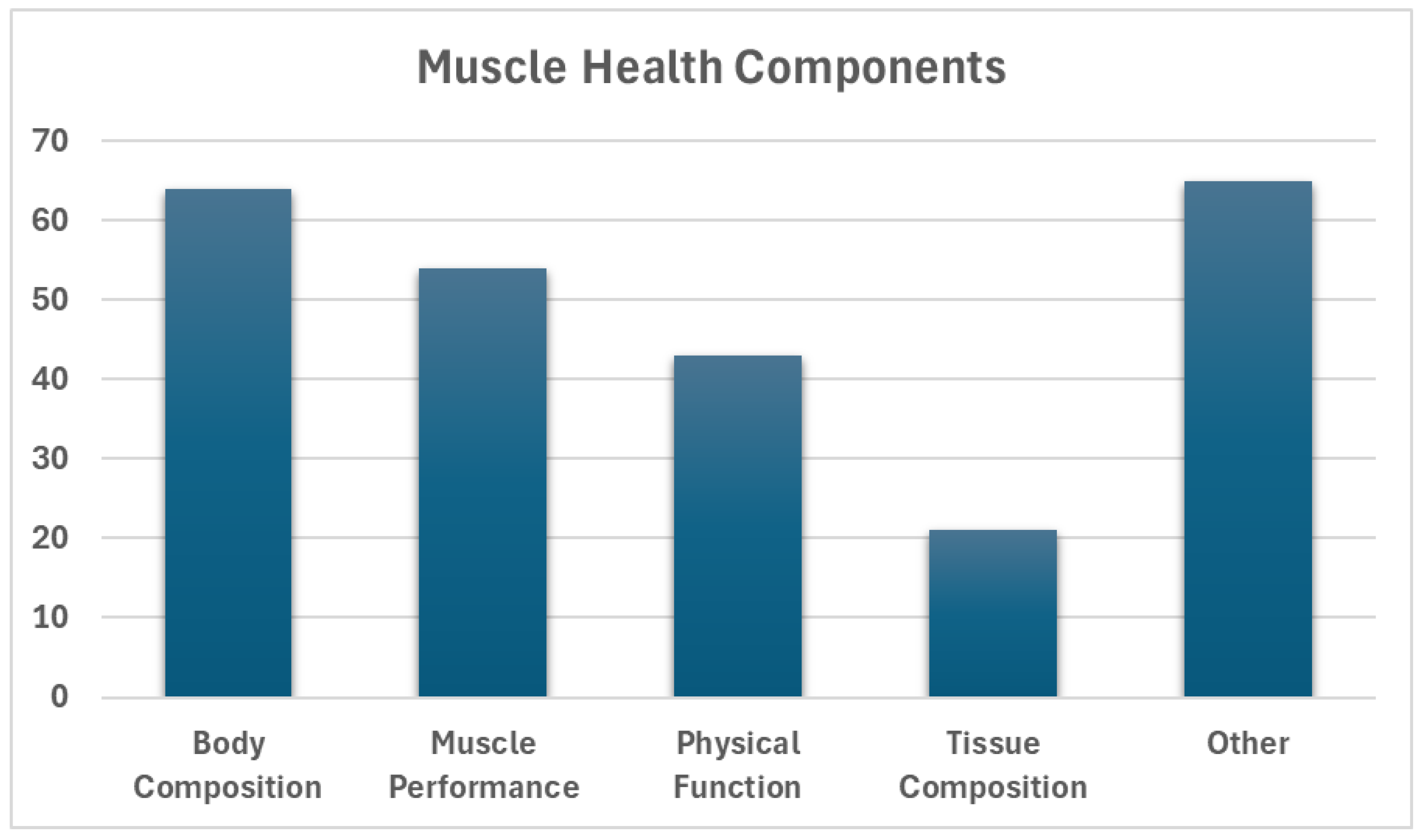
The frequency of defined and inferred ‘muscle health’ measures across all 68 identified studies is summarized in Figure 4. Sixty-three studies (92.7%) measured body composition in some way (e.g., total body fat percentage, appendicular lean mass) [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,49,50,51,52,53,54,55,56,57,58,59,60,61,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,97,98,99,100,101], 52 (76.5%) assessed muscle performance (e.g., grip strength, isometric force) [34,35,36,37,39,40,41,42,44,45,46,48,49,50,51,52,53,54,55,56,57,59,60,61,64,66,67,68,69,70,72,75,76,78,79,80,81,82,83,84,85,86,90,91,92,93,94,95,96,97,98,100], and 42 (61.8%) examined physical function (e.g., timed up-and-go [TUG], balance) [35,36,37,39,40,42,43,44,46,47,49,51,52,53,54,55,57,59,62,64,66,68,69,70,71,72,75,76,77,79,80,83,86,89,90,91,92,93,94,96,98,100], while 21 (30.9%) included at least one measure of tissue composition (e.g., echogenicity, intramuscular adipose tissue) [33,34,36,37,38,41,46,48,52,58,59,60,65,73,74,82,87,88,93,94,95]. Other common assessments included BMI (50, 73.5%) [33,34,35,36,39,40,43,44,45,46,47,48,49,51,53,54,55,56,58,59,60,63,64,66,67,68,69,70,71,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,92,93,94,98,99], metabolic biomarkers (32, 47.1%) [34,35,39,40,41,42,44,45,47,56,57,59,60,61,62,64,66,67,68,72,78,81,82,83,84,86,93,95,96,98,99,100], dietary/nutritional tracking (23, 33.8%) [34,35,36,37,40,46,49,50,51,53,55,56,57,66,70,76,80,81,82,85,86,90,91], activity, quality of life, and pain questionnaires (29, 42.7%) [38,39,42,43,44,45,48,49,52,53,55,59,60,64,67,68,69,70,73,74,78,79,83,84,85,86,88,89,94].
Figure 4.
Outline of identified ‘muscle health’ definitions included in articles obtained via search and screenings.
Figure 4.
Outline of identified ‘muscle health’ definitions included in articles obtained via search and screenings.
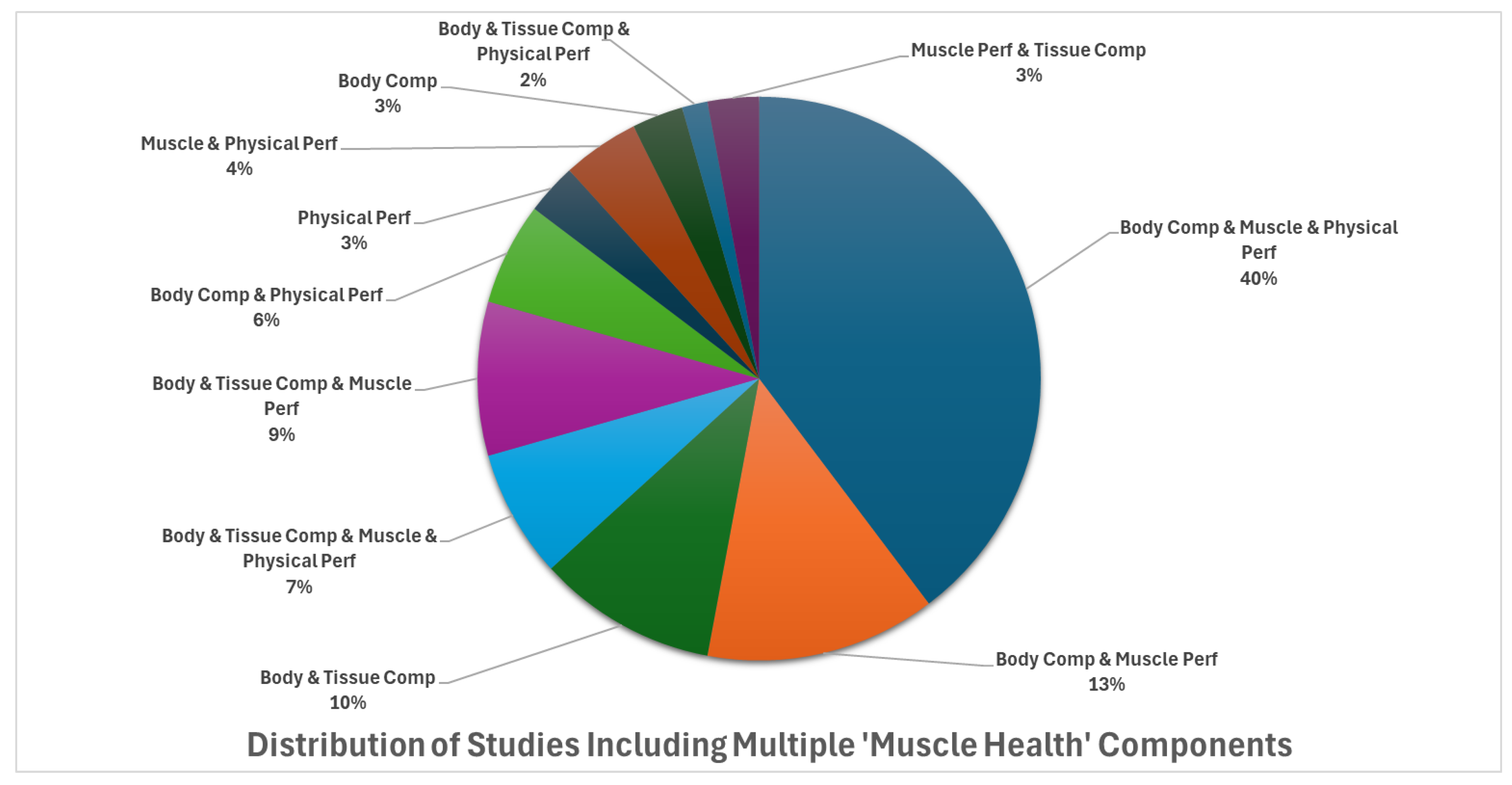
Nearly all studies (N=64, 94.1%) included more than one ‘muscle health’ component [33,34,35,36,37,38,39,40,41,42,43,44,45,46,48,49,50,51,52,53,54,55,56,57,58,59,60,61,63,64,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,100]. The distribution of this is illustrated in Figure 5. Only five studies (6.7%) included all four primary ‘muscle health’ components [36,37,52,59,93]. The most common combination (N=27, 39.7%) included body composition (e.g., muscle mass, body fat %), muscle performance (e.g., grip strength, knee extension torque), and physical function (e.g., TUG, sit-to-stand) [35,40,42,44,45,51,53,54,55,57,64,66,68,69,70,72,75,76,79,80,83,86,90,91,92,98,100]; followed by body composition and muscle performance (N=9, 13.2%) [50,56,61,67,78,81,84,85,97], and body and tissue composition (N=7, 10.3%) [33,38,58,65,87,88,94].
Figure 5.
Frequency of combined ‘muscle health’ components featured as outcome measures across all studies included in the review. Comp: composition; Perf: performance.
Figure 5.
Frequency of combined ‘muscle health’ components featured as outcome measures across all studies included in the review. Comp: composition; Perf: performance.
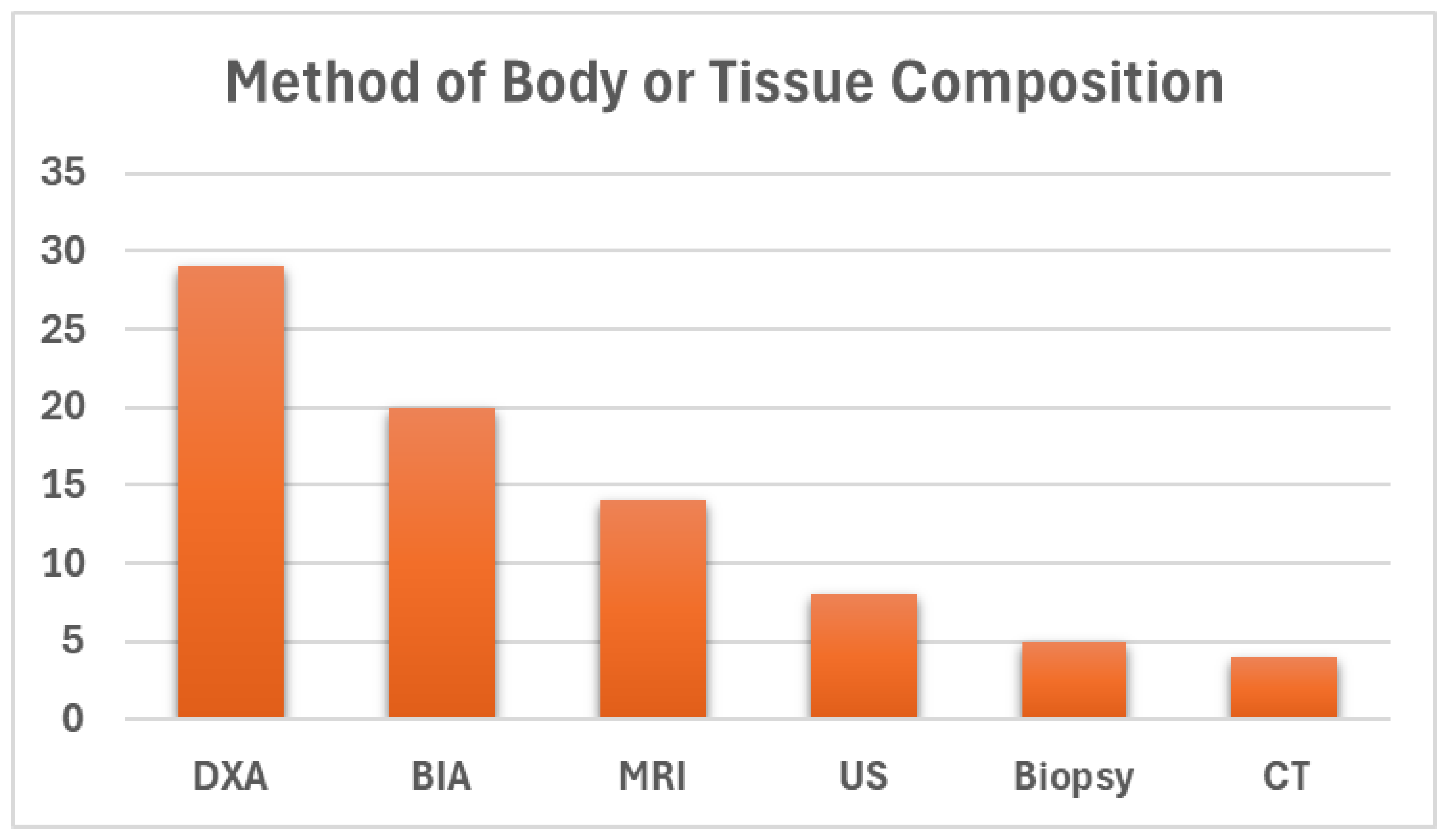
The methods of assessing body and tissue composition varied (Figure 6), with dual-energy X-ray absorptiometry (DXA) being the most used tool (N=29, 42.6%) [34,35,36,37,39,40,41,43,44,45,46,53,54,55,60,61,62,66,70,71,75,76,81,84,89,92,96,97,99], followed by bio-electrical impedance (BIA) (N=20, 29.4%) [42,49,50,51,56,57,59,64,67,68,69,78,83,85,86,90,91,93,98,100], magnetic resonance imaging (MRI) (N=14, 20.6%) [33,38,47,59,65,73,74,75,77,79,80,87,88,94], ultrasound (US) (N=8, 11.8%) [37,41,48,50,52,80,93,95], tissue biopsy (N=5, 7.4%) [33,34,36,37,41], and CT (N=4, 5.9%) [58,76,82,84].
Figure 6.
Identified methods of body and tissue composition assessment. DXA: dual-energy X-ray absorptiometry; BIA: bio-electrical impedance; MRI: magnetic resonance imaging; US: ultrasound; CT: computed tomography.
Figure 6.
Identified methods of body and tissue composition assessment. DXA: dual-energy X-ray absorptiometry; BIA: bio-electrical impedance; MRI: magnetic resonance imaging; US: ultrasound; CT: computed tomography.
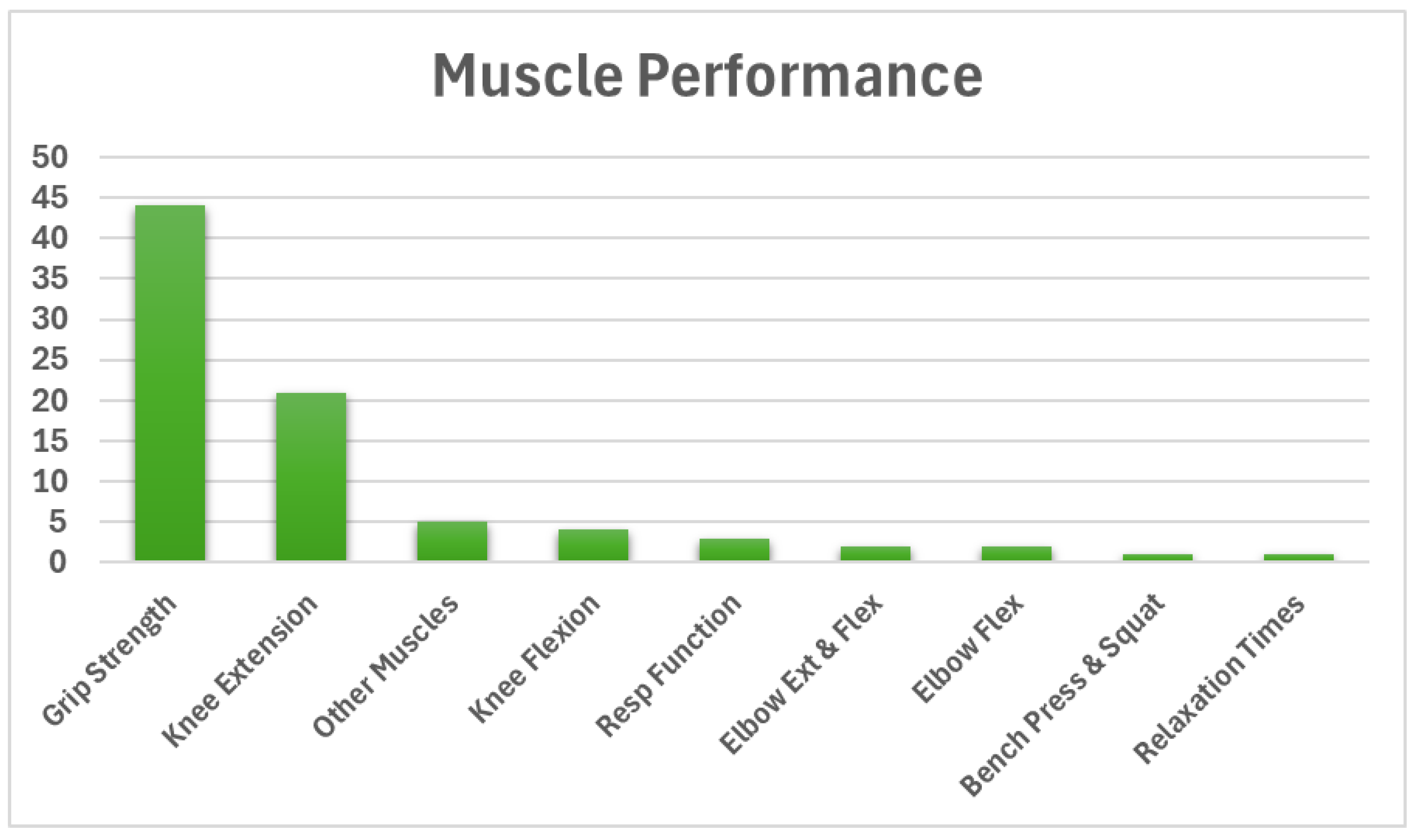
Muscle performance was measured using various methods (Figure 7). The most frequently used test was grip strength (N=43, 63.2%) [37,39,40,41,42,44,45,48,49,50,51,52,53,54,55,56,57,59,60,61,64,66,67,68,69,75,76,78,79,81,82,83,84,85,86,90,91,92,93,96,97,98,100], followed by knee extension (N=21, 30.1%) [34,35,36,37,41,44,45,46,60,62,70,75,76,79,80,84,86,94,95,96,97], and flexion (N=4, 5.9%) [39,40,75,76] force, torque, or power. A few studies utilized elbow and flexion strength (N=2, 2.9%) [39,40], bench press and squat strength (N=1, 1.5%) [72], or the strength of other single muscle groups (N=5, 7.4%), including ankle dorsiflexion, hip abductor, hip flexor, hip extensor, and hip adductor strength [38,46,70,76,80]. Other studies assessed respiratory muscle functions (e.g., inflationary pressure; N=3, 4.4%) [44,45,97], and electrical stimulation relaxation times (N=1, 1.5%) [47].
Figure 7.
Identified methods of muscle performance assessment. Resp: respiratory; Flex: flexion.
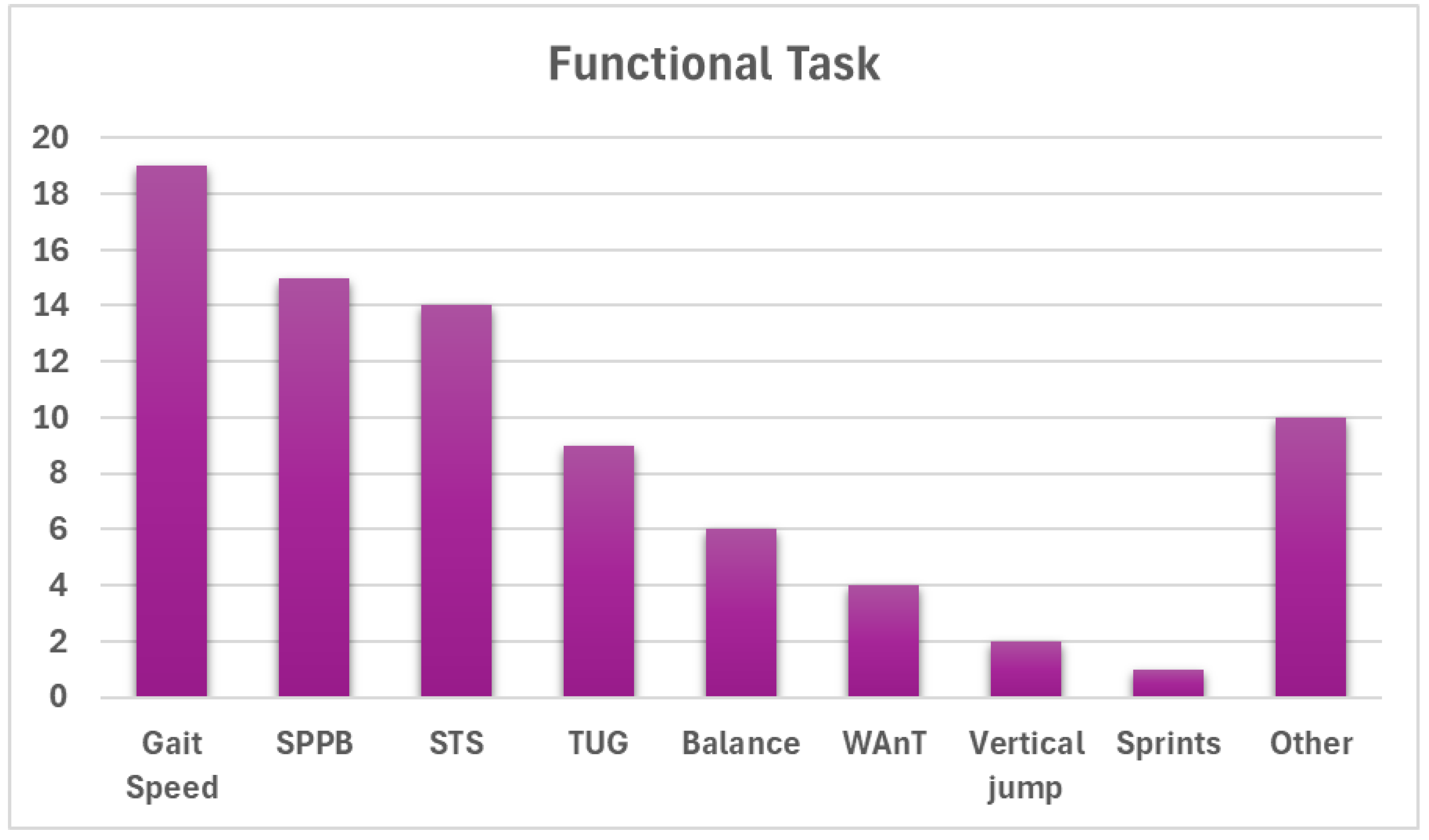
Methods used to assess physical function also varied widely (Figure 8), with gait speed (e.g., typical pace, maximal speed, time to a set distance) being the most common (N=18, 26.5%) [42,47,51,59,64,66,68,69,70,71,79,83,91,92,94,96,98,100]. Other common tests included the SPPB (N=14, 20.6%) [35,36,41,53,54,55,70,79,89,91,93,94,96,98], sit-to-stand/chair rise variations (N=13, 19.1%) [39,51,52,57,66,71,75,83,89,91,92,98,100], and TUG variations (N=9, 13.2%) [39,40,43,49,70,76,89,96,100]. A few studies also employed balance tests (N=6, 8.8%) [39,71,75,79,86,89], while power was assessed via Wingate (N=4, 5.9%) [35,36,37,46], vertical jump (N=2, 2.9%) [71,72], and sprint (N=1, 1.5%) tests [37]. Ten (14.7%) studies employed other single measures of physical function, such as self-reported physical activity levels or fatigue [44,47,79,80,86,89,90,92,94,100].
Figure 8.
Identified methods of assessing ‘functional’ performance. SPPB: short physical performance battery; STS: sit-to-stand; TUG: timed up-and-go; WAnT: Wingate anaerobic test. See table 1 for detailed ‘Other’ tests.
Figure 8.
Identified methods of assessing ‘functional’ performance. SPPB: short physical performance battery; STS: sit-to-stand; TUG: timed up-and-go; WAnT: Wingate anaerobic test. See table 1 for detailed ‘Other’ tests.
4. Discussion
While the term ‘muscle health’ is widely used, definitions, applications, and measurement methods vary greatly across the literature. Using a proposed framework for muscle health informed by the ICF, we conducted a systematic review to better understand the operational definitions of the term in the literature and synthesize these usage patterns where possible and appropriate. Overall, 68 studies were identified, with 31 providing an operational definition of ‘muscle health’. An additional 37 studies used the term ‘muscle health’ but did not provide an operational or conceptual definition. From the 68 studies, we characterized the study sample and outcome measures associated with muscle health categorized by their measurement domains: body/muscle tissue composition, muscle performance, and functional status.
4.1. Common Elements of Muscle Health
Body composition (e.g., muscle mass, fat percentage, appendicular lean mass) was measured in 92.7% of the studies. Nevertheless, the definitions of muscle health were variable across the selected studies. Thirty-one of the 68 studies defined muscle health by listing associated outcome measures such as muscle mass, grip strength, and physical function (e.g., gait speed, chair stand test, TUG). The lack of consensus was reflected in many studies that featured indirect outcome measures, such as BMI (73.5%) and metabolic biomarkers (47.1%), as components of muscle health. Notably, 94.1% of the reviewed studies integrated multiple outcomes, with 58.0% of the publications including at least three components of muscle health. The measurement domains in our proposed muscle health framework (i.e., body/muscle tissue composition, muscle performance, and functional status) were present in 47.0% of the reviewed studies.
Body composition, particularly muscle mass, has long been considered a cornerstone of muscle health. Our findings showed that the methods used to assess body and tissue composition varied throughout literature. Ultrasound is emerging as a method for estimating body/muscle tissue composition, which is used more frequently than tissue biopsy and CT imaging. Nonetheless, DXA, BIA, or MRI were used in over 92.2% of the studies. The variability in these measurement methods reflects the competing needs of accommodating available clinical and research resources with the effort to establish standardized approaches across studies. Given the importance of assessing muscle in patient settings that may range from community-based clinics to large medical centers, a stratified approach to evaluate muscle health must be considered. An analogous approach to musculoskeletal disorders has been adopted by organizations such as the American College of Rheumatology and the European Alliance of Associations for Rheumatology, which provide guidelines for diagnosing rheumatic conditions, both with and without laboratory values [102]. In a similar vein, characterizing the body/muscle tissue composition domain of muscle health may incorporate bioimaging devices ranging from ultrasound to MRI, depending on equipment access, cost limitations, and the complexity of the clinical environment.
The primary use of methods designed to estimate lean body mass (DXA: 41.2% and BIA: 29.4%), rather than specifically muscle mass, poses challenges to assessing muscle health. Bioimaging methods such as DXA, that estimate lean body mass as a surrogate measure of muscle mass, include a significant proportion of non-contractile tissue (i.e., approximately 25% of skin and connective tissue) [103]. In addition, DXA estimates of lean body mass often have low associations with frailty outcomes [104,105,106] and are less responsive to post-exercise regimen changes compared to local measures of muscle size, as measured via CT or MRI [107,108,109]. The extensive use of DXA in previous studies and its availability in hospital settings have been cited as reasons to maintain this bioimaging modality as a “reference” standard device and to continue using lean body mass as a component of muscle health [110]. However, contemporary reappraisals of this approach have noted that techniques such as D3-creatine may provide a more accurate estimate of whole-body muscle mass, and that bioimaging methods using MRI, CT, and ultrasound offer estimates of both muscle mass and tissue composition [111,112,113,114,115]. Consequently, the high frequency of DXA and other methods of lean body mass assessment cited in the reviewed studies may be an insufficient rationale to continue this methodological approach in future studies of muscle health. Additionally, the role of tissue composition (such as the extent of fatty infiltration in muscle) emerged as a significant factor influencing muscle health, suggesting that future definitions and assessments should integrate both mass and tissue quality [2].
Muscle performance is an essential domain of muscle health, as evident from the various strength assessment methods employed in these studies. Grip strength was the most frequently used technique (63.2%) to assess muscle performance, demonstrating its ease of use, portability, and presumed utility as a surrogate measure of whole-body strength. While the use of grip strength is limited by its low-to-moderate association with lower extremity strength [116,117], it remains an important outcome measure in field studies involving older adults due to its low testing burden and well-known psychometric properties [118,119]. Knee extension strength was the second most measured aspect of muscle performance (30.1%). Lower extremity muscle performance has a stronger relationship with physical functioning, such as gait speed, in comparison to upper extremity strength [116]. Overall, the strong association between muscle performance and mobility, as well as hospitalization risk, emphasizes its relevance as a predictor of health [120]. The findings of the current study support the inclusion of muscle performance as a standard part of muscle health assessments. Specific testing methods and muscle groups used to characterize muscle performance may vary depending on the availability of equipment, the population of interest, and the rationale for assessment (e.g., general screening versus an assessment of specific muscle groups).
Functional status is a crucial aspect of health-related quality of life, with gait speed being the most used method (26.5%) to characterize this domain of muscle health in the reviewed studies. Gait speed is a strong predictor of health outcomes such as mortality and hospitalization, and is a low-burden assessment, making it ideal for both research and clinical settings [121]. However, there are many variations in the methods used for testing gait speed (e.g., speed, distance, customary or fastest gait speed). A previous study involving older adults with muscle dysfunction revealed that individuals with significant lower extremity strength deficits may still maintain walking speeds that exceed 1.0 m/s [116]. More demanding functional tasks, such as one’s fastest walking speed [121], may show a stronger association with muscle strength in comparison to customary walking speed [116]. While variation in the testing method for gait speed allows assessment flexibility, this approach can also lead to methodological inconsistencies across studies. Following gait speed, the SPPB (20.6%), chair rise tests (19.1%), and TUG (13.2%) were the widely used functional assessments in the reviewed studies. These methods provide meaningful information on lower limb strength, balance, and overall mobility, which can directly impact activities of daily living. By combining selected functional tasks through assessment batteries, such as the SPPB, one can obtain a comprehensive assessment of functional status. Nevertheless, the multi-system contributions to functional status require an appropriate patient history and physical exam to determine if muscle dysfunction is a key contributor to observed functional limitations and diminished mobility. In addition, functional tests vary in their relative difficulty and bias towards muscle strength or power. Functional tasks with a focus on muscle power, such as the 30 second chair rise test, may reveal performance deficits earlier than other less demanding physical performance tasks [122]. An additional point of consideration is that diminished muscle health is often found in people with chronic conditions who are non-ambulatory or have other functional limitations [6]. Consequently, alternative methods to assess the functional domain of muscle health in adults with disabilities merit additional study.
4.2. Implications for Muscle Health Assessment
The assessment of muscle health has important implications for various patient populations, including older adults with sarcopenia and those with chronic health conditions [123,124,125]. Determining a viable model for muscle health and consistent measurement domains can ensure a more comprehensive evaluation of muscle health, aiding in the detection of early muscle loss or diminished quality in those at risk for muscle dysfunction. A proactive approach to screening or evaluating muscle-related impairments can help mitigate adverse outcomes, such as decreased independent mobility and compromised health-related quality of life. However, the findings from the current work revealed variability in the definitions and measurements of muscle health across studies, highlighting the need for consensus development and standardized assessment guidance. While 31 of the reviewed studies provided operational definitions of muscle health, it is essential to note that these definitions primarily served as documentation of muscle-related outcome measures. Rarely are frameworks or conceptual definitions provided or cited to provide a rationale for the collection of muscle-related outcomes featured in the reviewed study methods.
There have been notable recent efforts to standardize approaches to muscle-related outcome measures and provide a rationale for identifying components that characterize muscle health [5,126,127]. The Global Leadership Initiative in Sarcopenia (GLIS) has addressed competing definitions of sarcopenia and conducted an international Delphi Study to move toward a common classification approach [127,128]. The findings from the Delphi process indicated that three components of sarcopenia should comprise the conceptual definition of the condition: muscle mass (89.4%), muscle strength (93.1%), and muscle-specific strength (80.8%) [127]. While it could be argued that the efforts of the GLIS investigators are limited explicitly to sarcopenia, their recommendation to include measures of both muscle mass and strength is consistent with the proposed muscle health measurement domains for body/muscle tissue composition (muscle mass) and muscle performance (muscle strength and muscle-specific strength). Moreover, their identification of muscle-specific strength (e.g., strength standardized to muscle size or other scaling factors) raises an important point about strength assessment methodology. The studies featured in the review included standardized measures of strength assessment. Nonetheless, additional empirical findings and consensus efforts may inform the relative value of expressing muscle performance in terms of peak torque, work, power, and relative peak torque scaled to body stature or muscle size.
Heymsfield and colleagues [5] have also addressed the challenge of characterizing muscle health. The investigators note that form (e.g., body/muscle tissue composition) and functional measures are often framed as equivalent criteria in clinical decision-making algorithms. Instead, the classic biological concept of “function follows form” provides a hierarchy informed by the pathophysiological links between muscle characteristics and clinical outcomes [5]. A classification system informing the proposed muscle health framework in the current study is the ICF, which encompasses domains of ‘Body Functions’, ‘Structures’, ‘Activities’, and ‘Participation’ [15]. While the ICF is not based on a hierarchical model as proposed by Heymsfield and associates [5], there is consistency between the proposed domains of muscle health identified in this study (body/muscle tissue composition, muscle performance, and functional status) and elements of Heymsfield et al.’s “Outcomes Follow Function Rule” (form, function, and outcomes) [5,15]. The key difference between these conceptual approaches is that the recommendation in the current work categorizes direct measures of muscle performance separately from functional performance tasks such as gait speed or chair stands, given that body systems beyond the musculoskeletal system impact functional status. In contrast, Heymsfield et al. [5] categorize both muscle performance and functional status within the domain of “function” and distinguish between “outcomes” as global assessments of morbidity and mortality. Overall, the domains of muscle health proposed in this work are well-supported by existing frameworks for assessing physical health [23], consensus-based component measures [5,126,127], and the most frequently cited measures in the reviewed studies (Figure 9).
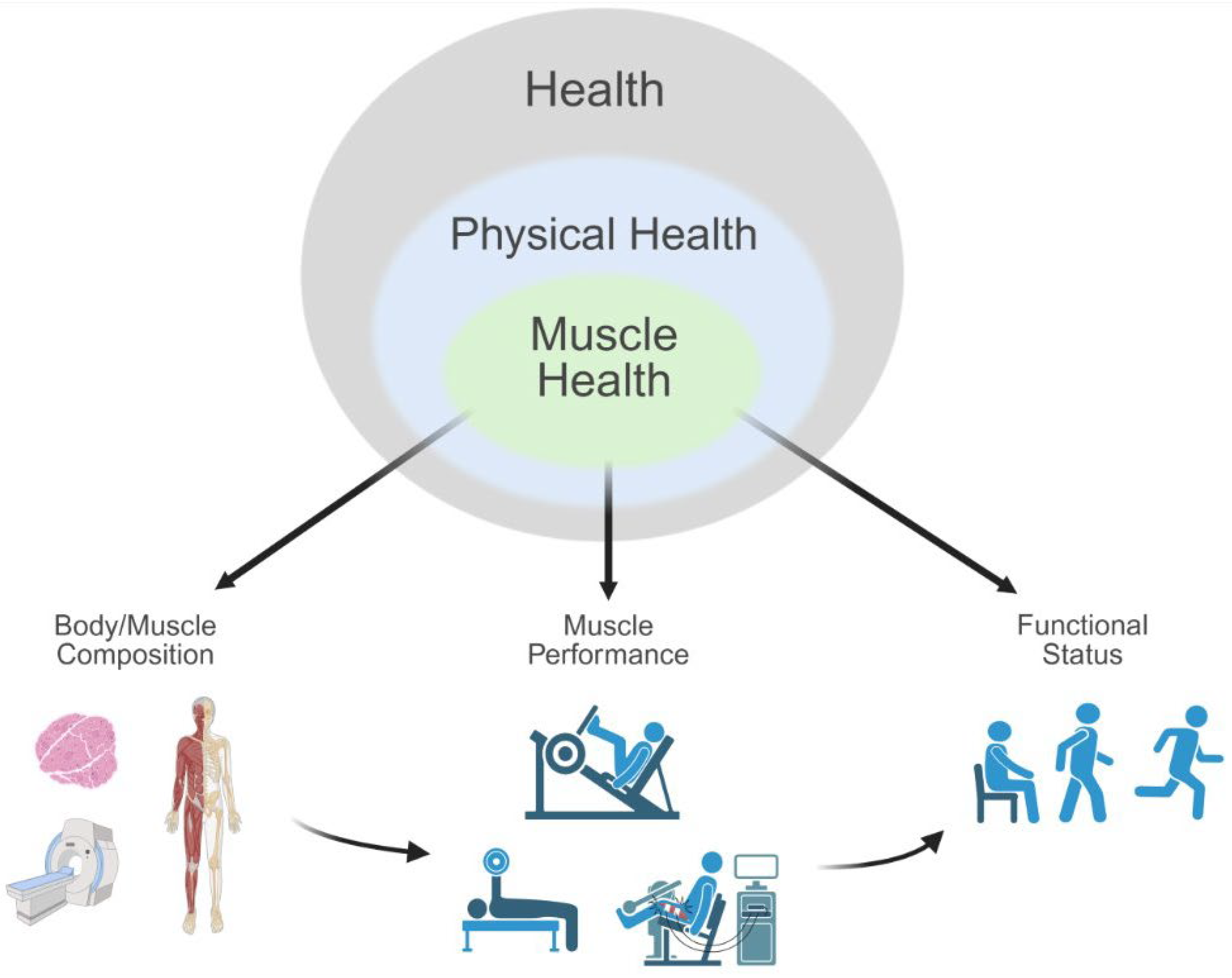
Figure 9.
The proposed conceptual model of ‘muscle health’ as informed by the framework of the International Classification of Functioning, Disability and Health (ICF). Muscle health encompasses three primary domains: body/muscle tissue composition, muscular performance, and functional status. Domains can be evaluated using dichotomous (e.g., impaired vs. unimpaired; cut-off scores for functional assessments) or continuous metrics (e.g., maximal peak torque or force) depending on context and modality. This conceptual model emphasizes the integration of structural, physiological, and functional components relevant to muscle-related outcomes.
Figure 9.
The proposed conceptual model of ‘muscle health’ as informed by the framework of the International Classification of Functioning, Disability and Health (ICF). Muscle health encompasses three primary domains: body/muscle tissue composition, muscular performance, and functional status. Domains can be evaluated using dichotomous (e.g., impaired vs. unimpaired; cut-off scores for functional assessments) or continuous metrics (e.g., maximal peak torque or force) depending on context and modality. This conceptual model emphasizes the integration of structural, physiological, and functional components relevant to muscle-related outcomes.
4.3. Limitations
Despite the comprehensive nature of this review, several limitations must be acknowledged. First, many studies inferred definitions of muscle health through outcomes without explicitly defining the term. Additionally, the inclusion criteria may have excluded relevant studies that did not expressly define or measure muscle health according to the stated review criteria. Furthermore, reliance on specific databases may have introduced a bias in the selection of studies, potentially overlooking pertinent research published elsewhere. In addition, heterogeneity in study design and participant samples makes generalizing the findings across all demographic groups challenging. Most importantly, although we conducted a systematic search to assess the current literature, the overarching narrative format of this review is susceptible to bias due to the perspective of the manuscript authors. Thus, our viewpoints are not infallible, and this paper is open to further and differing interpretations. Lastly, our review focused primarily on skeletal muscle health. This has the potential to limit the generalizability of our findings to other muscle types, such as cardiac or smooth muscle.
5. Conclusions
This review underscores the complexity of defining and assessing muscle health. While muscle mass remains a crucial outcome measure, muscle health is a multifaceted concept that encompasses not only muscle mass but also muscle performance, tissue composition, and physical function. As such, readers can, and likely should, interpret ‘muscle health’ as a term that is informed by general and physical health. Furthermore, these concepts can include muscle morphology and morphometry, muscle performance, and functional impairments and limitations, as observed in 47.1% of the selected studies for review. The muscle health domains recommended in this work are consistent with established frameworks for assessing physical health [23] and the ICF model to classify components of health and well-being [15]. The need for standardized definitions and consensus-based guidelines is evident, as is the importance of considering these elements in varied clinical and research settings. Healthcare providers can better manage the risks associated with muscle dysfunction and improve patient outcomes by adopting a holistic and proactive approach to assessing muscle health.
Author Contributions
Conceptualization, MHL; methodology, KLB, DJO, DGR, MHL; software, DJO, DGR; formal analysis, DJO; investigation, KLB, DJO, DGR; resources, MHL; data curation, DGR, KLB, DJO; writing—original draft preparation, KLB, DJO, DGR, MHL; writing—review and editing, EES, DMM; visualization, DJO, DGR, MHL; supervision, EES, DMM, MHL; project administration, DJO, MHL; funding acquisition, MHL. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Underlying data used to create figures are available upon request to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADL | Activities of daily living |
| IADL | Instrumental activities of daily living |
| ICF | International Classification of Functioning, Disability and Health |
| CT | Computed tomography |
| SPPB | Short physical performance battery |
| TUG | Timed up-and-go |
| BMI | Body-mass index |
| DXA | Dual-energy X-ray absorptiometry |
| BIA | Bio-electrical impedance |
| MRI | Magnetic resonance imaging |
| GLIS | Global Leadership Initiative in Sarcopenia |
References
- Miljkovic, I.; Zmuda, J.M. Epidemiology of myosteatosis. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 260–264. [Google Scholar] [CrossRef]
- Correa-De-Araujo, R.; Harris-Love, M.O.; Miljkovic, I.; Fragala, M.S.; Anthony, B.W.; Manini, T.M. The Need for Standardized Assessment of Muscle Quality in Skeletal Muscle Function Deficit and Other Aging-Related Muscle Dysfunctions: A Symposium Report. Front. Physiol. 2017, 8, 87. [Google Scholar] [CrossRef]
- Chao, Y.-P.; Fang, W.-H.; Chen, W.-L.; Peng, T.-C.; Yang, W.-S.; Kao, T.-W. Exploring Muscle Health Deterioration and Its Determinants Among Community-Dwelling Older Adults. Front. Nutr. 2022, 9, 817044. [Google Scholar] [CrossRef]
- Prado, C.M.; Landi, F.; Chew, S.T.; Atherton, P.J.; Molinger, J.; Ruck, T.; Gonzalez, M.C. Advances in muscle health and nutrition: A toolkit for healthcare professionals. Clin. Nutr. 2022, 41, 2244–2263. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Prado, C.M.; Gonzalez, M.C. Skeletal muscle-focused guideline development: hierarchical model incorporating muscle form, function, and clinical outcomes. Appl. Physiol. Nutr. Metab. 2023, 48, 751–756. [Google Scholar] [CrossRef]
- Falcon, L.J.; Harris-Love, M.O. Sarcopenia and the New ICD-10-CM Code: Screening, Staging, and Diagnosis Considerations. Fed. Pract. 2017, 34, 24–32. [Google Scholar]
- Chester, J.G.; Rudolph, J.L. Vital Signs in Older Patients: Age-Related Changes. J. Am. Med Dir. Assoc. 2011, 12, 337–343. [Google Scholar] [CrossRef]
- Schlicht, J.A.; Wingood, M.; Heled, Y.; Weitzel, K.; Rogers, M.E.; Seffens, P.R. The Physical Activity Vital Sign for Older Adults: Time for an Update. J. Am. Med Dir. Assoc. 2024, 25, 105020. [Google Scholar] [CrossRef]
- Carlson, C.; Merel, S.E.; Yukawa, M. Geriatric Syndromes and Geriatric Assessment for the Generalist. Med Clin. North Am. 2015, 99, 263–279. [Google Scholar] [CrossRef]
- World Health Organization Basic Documents: (Including Amendments Adopted up to ); 49th ed.; Geneva, 2020; ISBN 978-92-4-000051-3. 31 May.
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife Hand Grip Strength as a Predictor of Old Age Disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.; Grimby, G.; Karlsson, J. Muscle strength and speed of movement in relation to age and muscle morphology. J. Appl. Physiol. 1979, 46, 451–456. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization International Classification of Functioning, Disability and Health (ICF); Geneva, Switzerland, 2001;
- Millán-Calenti, J.C.; Tubío, J.; Pita-Fernández, S.; González-Abraldes, I.; Lorenzo, T.; Fernández-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: a meta-analysis. J. Cachex- Sarcopenia Muscle 2019, 11, 3–25. [Google Scholar] [CrossRef]
- Hirani, V.; Naganathan, V.; Blyth, F.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Longitudinal associations between body composition, sarcopenic obesity and outcomes of frailty, disability, institutionalisation and mortality in community-dwelling older men: The Concord Health and Ageing in Men Project. Age and Ageing 2016, 46, 413–420. [Google Scholar] [CrossRef]
- Broadwin, J.; Goodman-Gruen, D.; Slymen, D. Ability of Fat and Fat-Free Mass Percentages to Predict Functional Disability in Older Men and Women. J. Am. Geriatr. Soc. 2001, 49, 1641–1645. [Google Scholar] [CrossRef]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. ; for the Health ABC study Muscle Mass, Muscle Strength, and Muscle Fat Infiltration as Predictors of Incident Mobility Limitations in Well-Functioning Older Persons. J. Gerontol. Ser. A 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Meskers, C.G.M.; Reijnierse, E.M.; Numans, S.T.; Kruizinga, R.C.; Pierik, V.D.; van Ancum, J.M.; Slee-Valentijn, M.; Scheerman, K.; Verlaan, S.; Maier, A.B. Association of Handgrip Strength and Muscle Mass with Dependency in (Instrumental) Activities of Daily Living in Hospitalized Older Adults -The EMPOWER Study. J. Nutr. Heal. Aging 2019, 23, 232–238. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Mhs, K.M.F.; PhD, M.S.R.G.; Delmonico, M.J.; Chiou, C.-F.; Anthony, M.S.; Bs, A.S.; Goodpaster, B.; MD, D.S.S.; Cummings, S.R.; et al. Do Muscle Mass, Muscle Density, Strength, and Physical Function Similarly Influence Risk of Hospitalization in Older Adults? J. Am. Geriatr. Soc. 2009, 57, 1411–1419. [Google Scholar] [CrossRef]
- Koipysheva, E.A.; Lebedinsky, V.Yu.; Koipysheva, M.A. Physical Health (Definition, Semantic Content, Study Prospects). In The European Proceedings of Social & Behavioural Sciences; Nicosia: Irkutsk, Russia, 2018; ISBN 2357-1330. [Google Scholar]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.-H.; Fresk, M.; Besstrashnova, Y.; et al. 20 Years of ICF—International Classification of Functioning, Disability and Health: Uses and Applications around the World. Int. J. Environ. Res. Public Heal. 2022, 19, 11321. [Google Scholar] [CrossRef]
- Correa-De-Araujo, R.; Hadley, E. Skeletal Muscle Function Deficit: A New Terminology to Embrace the Evolving Concepts of Sarcopenia and Age-Related Muscle Dysfunction. Journals Gerontol. Ser. A 2014, 69, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Gonzalez, M.C.; Lu, J.; Jia, G.; Zheng, J. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc. Nutr. Soc. 2015, 74, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Senior, H.E.; Henwood, T.R.; Beller, E.M.; Mitchell, G.K.; Keogh, J.W. Prevalence and risk factors of sarcopenia among adults living in nursing homes. Maturitas 2015, 82, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ma, L. Intrinsic Capacity in Older Adults: Recent Advances. Aging Dis. 2022, 13, 353–359. [Google Scholar] [CrossRef]
- World Health Organization Integrated Care for Older People (ICOPE) Implementation Framework: Guidance for Systems and Services; World Health Organization: Geneva, 2019; ISBN 978-92-4-151599-3.
- Abadir, P.M.; Bandeen-Roche, K.; Bergeman, C.; Bennett, D.; Davis, D.; Kind, A.; LeBrasseur, N.; Stern, Y.; Varadhan, R.; Whitson, H.E. An overview of the resilience world: Proceedings of the American Geriatrics Society and National Institute on Aging State of Resilience Science Conference. J. Am. Geriatr. Soc. 2023, 71, 2381–2392. [Google Scholar] [CrossRef]
- Resnick, B.; Galik, E.; Dorsey, S.; Scheve, A.; Gutkin, S. Reliability and Validity Testing of the Physical Resilience Measure. Gerontol. 2011, 51, 643–652. [Google Scholar] [CrossRef]
- Hu, F.-W.; Lin, C.-H.; Yueh, F.-R.; Lo, Y.-T.; Lin, C.-Y. Development and psychometric evaluation of the Physical Resilience Instrument for Older Adults (PRIFOR). BMC Geriatr. 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Anderson, B.; Ordaz, A.; Zlomislic, V.; Allen, R.T.; Garfin, S.R.; Schuepbach, R.; Farshad, M.; Schenk, S.; Ward, S.R.; Shahidi, B. Paraspinal Muscle Health is Related to Fibrogenic, Adipogenic, and Myogenic Gene Expression in Patients with Lumbar Spine Pathology. BMC Musculoskelet. Disord. 2022, 23, 1–11. [Google Scholar] [CrossRef]
- Arentson-Lantz, E.; Galvan, E.; Wacher, A.; Fry, C.S.; Paddon-Jones, D. 2,000 Steps/Day Does Not Fully Protect Skeletal Muscle Health in Older Adults During Bed Rest. J. Aging Phys. Act. 2019, 27, 191–197. [Google Scholar] [CrossRef]
- Arentson-Lantz, E.J.; Galvan, E.; Ellison, J.; Wacher, A.; Paddon-Jones, D.; Newman, A. Improving Dietary Protein Quality Reduces the Negative Effects of Physical Inactivity on Body Composition and Muscle Function. Journals Gerontol. Ser. A 2019, 74, 1605–1611. [Google Scholar] [CrossRef]
- Arentson-Lantz, E.J.; Fiebig, K.N.; Anderson-Catania, K.J.; Deer, R.R.; Wacher, A.; Fry, C.S.; Lamon, S.; Paddon-Jones, D. Countering disuse atrophy in older adults with low-volume leucine supplementation. J. Appl. Physiol. 2020, 128, 967–977. [Google Scholar] [CrossRef]
- Bathgate, K.E.; Bagley, J.R.; Jo, E.; Talmadge, R.J.; Tobias, I.S.; Brown, L.E.; Coburn, J.W.; Arevalo, J.A.; Segal, N.L.; Galpin, A.J. Muscle health and performance in monozygotic twins with 30 years of discordant exercise habits. Eur. J. Appl. Physiol. 2018, 118, 2097–2110. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.B.; Padwal, J.; Johnson, S.; Englund, E.K.; Ward, S.R.; Shahidi, B. The effect of high-intensity resistance exercise on lumbar musculature in patients with low back pain: a preliminary study. BMC Musculoskelet. Disord. 2019, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bislev, L.S.; Rødbro, L.L.; Sikjær, T.; Rejnmark, L. Effects of Elevated Parathyroid Hormone Levels on Muscle Health, Postural Stability and Quality of Life in Vitamin D-Insufficient Healthy Women: A Cross-Sectional Study. Calcif. Tissue Int. 2019, 105, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Bislev, L.S.; Sundekilde, U.K.; Kilic, E.; Dalsgaard, T.K.; Rejnmark, L.; Bertram, H.C. Circulating Levels of Muscle-Related Metabolites Increase in Response to a Daily Moderately High Dose of a Vitamin D3 Supplement in Women with Vitamin D Insufficiency—Secondary Analysis of a Randomized Placebo-Controlled Trial. Nutrients 2020, 12, 1310. [Google Scholar] [CrossRef]
- Cegielski, J.; Brook, M.S.; Phillips, B.E.; Boereboom, C.; Gates, A.; Gladman, J.F.R.; Smith, K.; Wilkinson, D.J.; Atherton, P.J. The Combined Oral Stable Isotope Assessment of Muscle (COSIAM) reveals D-3 creatine derived muscle mass as a standout cross-sectional biomarker of muscle physiology vitality in older age. GeroScience 2022, 44, 2129–2138. [Google Scholar] [CrossRef]
- Cha, R.; Kang, S.H.; Han, M.Y.; An, W.S.; Kim, S.; Kim, J.C. Effects of AST-120 on muscle health and quality of life in chronic kidney disease patients: results of RECOVERY study. J. Cachex- Sarcopenia Muscle 2021, 13, 397–408. [Google Scholar] [CrossRef]
- Davis, J.A.; Mohebbi, M.; Collier, F.; Loughman, A.; Staudacher, H.; Shivappa, N.; Hébert, J.R.; Pasco, J.A.; Jacka, F.N. The role of diet quality and dietary patterns in predicting muscle mass and function in men over a 15-year period. Osteoporos. Int. 2021, 32, 2193–2203. [Google Scholar] [CrossRef]
- Engelen, M.P.; Kirschner, S.K.; Coyle, K.S.; Argyelan, D.; Neal, G.; Dasarathy, S.; Deutz, N.E. Sex related differences in muscle health and metabolism in chronic obstructive pulmonary disease. Clin. Nutr. 2023, 42, 1737–1746. [Google Scholar] [CrossRef]
- Engelen, M.P.K.J.; Jonker, R.; Sulaiman, H.; Fisk, H.L.; Calder, P.C.; Deutz, N.E.P. ω-3 polyunsaturated fatty acid supplementation improves postabsorptive and prandial protein metabolism in patients with chronic obstructive pulmonary disease: a randomized clinical trial. Am. J. Clin. Nutr. 2022, 116, 686–698. [Google Scholar] [CrossRef] [PubMed]
- English, K.L.; Mettler, J.A.; Ellison, J.B.; Mamerow, M.M.; Arentson-Lantz, E.; Pattarini, J.M.; Ploutz-Snyder, R.; Sheffield-Moore, M.; Paddon-Jones, D. Leucine partially protects muscle mass and function during bed rest in middle-aged adults. Am. J. Clin. Nutr. 2016, 103, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Finkel, R.S.; Finanger, E.; Vandenborne, K.; Sweeney, H.L.; Tennekoon, G.; Shieh, P.B.; Willcocks, R.; Walter, G.; Rooney, W.D.; Forbes, S.C.; et al. Disease-modifying effects of edasalonexent, an NF-κB inhibitor, in young boys with Duchenne muscular dystrophy: Results of the MoveDMD phase 2 and open label extension trial. Neuromuscul. Disord. 2021, 31, 385–396. [Google Scholar] [CrossRef]
- Gil, S.; Júnior, G.N.d.O.; Sarti, F.M.; Filho, W.J.; Longobardi, I.; Turri, J.A.O.; Shinjo, S.K.; Ferriolli, E.; Avelino-Silva, T.J.; Busse, A.L.; et al. Acute Muscle Mass Loss Predicts Long-Term Fatigue, Myalgia, and Health Care Costs in COVID-19 Survivors. J. Am. Med Dir. Assoc. 2022, 24, 10–16. [Google Scholar] [CrossRef]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2018, 37, 2260–2270. [Google Scholar] [CrossRef]
- Groenendijk, I.; Kramer, C.S.; Boeft, L.M.D.; Hobbelen, H.S.M.; van der Putten, G.-J.; de Groot, L.C.P.G.M. Hip Fracture Patients in Geriatric Rehabilitation Show Poor Nutritional Status, Dietary Intake and Muscle Health. Nutrients 2020, 12, 2528. [Google Scholar] [CrossRef]
- Jackson, K.L.; Gropper, S.S.; Hunt, D.; D’avolio, D.; Newman, D. Effectiveness of a Per-Meal Protein Prescription and Nutrition Education with versus without Diet Coaching on Dietary Protein Intake and Muscle Health in Middle-Aged Women. Nutrients 2022, 14, 375. [Google Scholar] [CrossRef]
- Jacob, I.; Johnson, M.I.; Jones, G.; Jones, A.; Francis, P. Age-related differences of vastus lateralis muscle morphology, contractile properties, upper body grip strength and lower extremity functional capability in healthy adults aged 18 to 70 years. BMC Geriatr. 2022, 22, 1–15. [Google Scholar] [CrossRef]
- Li, C.; Meng, H.; Wu, S.; Fang, A.; Liao, G.; Tan, X.; Chen, P.; Wang, X.; Chen, S.; Zhu, H. Daily Supplementation With Whey, Soy, or Whey-Soy Blended Protein for 6 Months Maintained Lean Muscle Mass and Physical Performance in Older Adults With Low Lean Mass. J. Acad. Nutr. Diet. 2021, 121, 1035–1048.e6. [Google Scholar] [CrossRef]
- Locquet, M.; Beaudart, C.; Bruyère, O.; Kanis, J.A.; Delandsheere, L.; Reginster, J.-Y. Bone health assessment in older people with or without muscle health impairment. Osteoporos. Int. 2018, 29, 1057–1067. [Google Scholar] [CrossRef]
- Locquet, M.; Beaudart, C.; Reginster, J.-Y.; Bruyère, O. Association Between the Decline in Muscle Health and the Decline in Bone Health in Older Individuals from the SarcoPhAge Cohort. Calcif. Tissue Int. 2018, 104, 273–284. [Google Scholar] [CrossRef]
- Matsumoto, A.; Yoshimura, Y.; Nagano, F.; Bise, T.; Kido, Y.; Shimazu, S.; Shiraishi, A. Statin use impairs muscle strength recovery in post-stroke patients with sarcopenia. Geriatr. Gerontol. Int. 2023, 23, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, K.-G.; Nilsson, A.; Nilsson, L.M.; Kadi, F. Healthy Eating Is Associated with Sarcopenia Risk in Physically Active Older Adults. Nutrients 2021, 13, 2813. [Google Scholar] [CrossRef] [PubMed]
- Parker, N.H.; Gorzelitz, J.; Ngo-Huang, A.; Caan, B.J.; Prakash, L.; Garg, N.; Petzel, M.Q.B.; Schadler, K.; Basen-Engquist, K.; Katz, M.H.G. The Role of Home-Based Exercise in Maintaining Skeletal Muscle During Preoperative Pancreatic Cancer Treatment. Integr. Cancer Ther. 2021, 20. [Google Scholar] [CrossRef]
- Peng, L.-N.; Lin, M.-H.; Lee, H.-F.; Hsu, C.-C.; Chang, S.-J.; Chen, L.-K. Clinical efficacy of oligonol® supplementation on metabolism and muscle health in middle-aged and older adults: A double-blinded randomized controlled trial. Arch. Gerontol. Geriatr. 2022, 103, 104784. [Google Scholar] [CrossRef]
- Pérez-Piñero, S.; Ávila-Gandía, V.; Arias, J.A.R.; Muñoz-Carrillo, J.C.; Losada-Zafrilla, P.; López-Román, F.J. A 12-Week Randomized Double-Blind Placebo-Controlled Clinical Trial, Evaluating the Effect of Supplementation with a Spinach Extract on Skeletal Muscle Fitness in Adults Older Than 50 Years of Age. Nutrients 2021, 13, 4373. [Google Scholar] [CrossRef]
- Pratt, J.; De Vito, G.; Narici, M.; Segurado, R.; Pessanha, L.; Dolan, J.; Conroy, J.; Boreham, C.; Le Couteur, D. Plasma C-Terminal Agrin Fragment as an Early Biomarker for Sarcopenia: Results From the GenoFit Study. Journals Gerontol. Ser. A 2021, 76, 2090–2096. [Google Scholar] [CrossRef]
- Rousseau, A.-F.; Foidart-Desalle, M.; Ledoux, D.; Remy, C.; Croisier, J.-L.; Damas, P.; Cavalier, E. Effects of cholecalciferol supplementation and optimized calcium intakes on vitamin D status, muscle strength and bone health: A one-year pilot randomized controlled trial in adults with severe burns. Burns 2015, 41, 317–325. [Google Scholar] [CrossRef]
- Schneider, S.; Peipsi, A.; Stokes, M.; Knicker, A.; Abeln, V. Feasibility of monitoring muscle health in microgravity environments using Myoton technology. Med Biol. Eng. Comput. 2014, 53, 57–66. [Google Scholar] [CrossRef]
- Shin, J.; Hwang, J.H.; Han, M.; Cha, R.-H.; Kang, S.H.; An, W.S.; Kim, J.C.; Kim, S.H. Phase angle as a marker for muscle health and quality of life in patients with chronic kidney disease. Clin. Nutr. 2022, 41, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Araghi, K.; Dupont, M.M.; Shahi, P.; Bovonratwet, P.; Shinn, D.; Dalal, S.S.; Melissaridou, D.; Virk, S.S.; Iyer, S.; et al. Association between muscle health and patient-reported outcomes after lumbar microdiscectomy: early results. Spine J. 2022, 22, 1677–1686. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Elshorbagy, A.; Turner, C.; Refsum, H.; Kwok, T. The Association of Circulating Amino Acids and Dietary Inflammatory Potential with Muscle Health in Chinese Community-Dwelling Older People. Nutrients 2022, 14, 2471. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, J.P.; Zhou, A.; Hyppönen, E. Muscle Traits, Sarcopenia, and Sarcopenic Obesity: A Vitamin D Mendelian Randomization Study. Nutrients 2023, 15, 2703. [Google Scholar] [CrossRef]
- Tan, N.C.; Sankari, U.; Ng, C.E.; Koh, Y.L.E. Longitudinal study on the progression of muscle status among community-dwelling ambulatory older multiethnic Asians with type 2 diabetes mellitus. BMC Geriatr. 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Van Ancum, J.M.; Meskers, C.G.M.; Reijnierse, E.M.; Yeung, S.S.Y.; Jonkman, N.H.; Trappenburg, M.C.; Pijnappels, M.; Maier, A.B. Lack of Knowledge Contrasts the Willingness to Counteract Sarcopenia Among Community-Dwelling Adults. J. Aging Heal. 2019, 32, 787–794. [Google Scholar] [CrossRef]
- van Dongen, E.J.; Haveman-Nies, A.; Doets, E.L.; Dorhout, B.G.; de Groot, L.C. Effectiveness of a Diet and Resistance Exercise Intervention on Muscle Health in Older Adults: ProMuscle in Practice. J. Am. Med Dir. Assoc. 2020, 21, 1065–1072.e3. [Google Scholar] [CrossRef]
- Vesey, R.M.; Hofman, P.L.; Derraik, J.G.; Colle, P.; Biggs, J.B.; Munns, C.F.; Cutfield, W.S.; Gusso, S. Safety, feasibility and efficacy of side-alternating vibration therapy on bone and muscle health in children and adolescents with musculoskeletal disorders: A pilot trial. J. Paediatr. Child Heal. 2020, 56, 1257–1262. [Google Scholar] [CrossRef]
- Vingren, J.L.; Curtis, J.H.; Levitt, D.E.; Duplanty, A.A.; Lee, E.C.; McFarlin, B.K.; Hill, D.W. Adding Resistance Training to the Standard of Care for Inpatient Substance Abuse Treatment in Men With Human Immunodeficiency Virus Improves Skeletal Muscle Health Without Altering Cytokine Concentrations. J. Strength Cond. Res. 2018, 32, 76–82. [Google Scholar] [CrossRef]
- Virk, S.; Sandhu, M.; Wright-Chisem, J.; Vaishnav, A.; Albert, T.; Qureshi, S.A. The association between spondylolisthesis and decreased muscle health throughout the lumbar spine for patients with operative lumbar spinal stenosis. Eur. Spine J. 2021, 30, 2605–2612. [Google Scholar] [CrossRef]
- Virk, S.M.; Wright-Chisem, J.; Sandhu, M.B.; Vaishnav, A.; Albert, T.J.; Gang, C.H.; Qureshi, S.M. A Novel Magnetic Resonance Imaging-based Lumbar Muscle Grade to Predict Health-related Quality of Life Scores Among Patients Requiring Surgery. Spine 2020, 46, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Bonato, M.; Borghi, S.; Messina, C.; Albano, D.; Corbetta, S.; Sconfienza, L.M.; Banfi, G. Home-Based Resistance Training for Older Subjects during the COVID-19 Outbreak in Italy: Preliminary Results of a Six-Months RCT. Int. J. Environ. Res. Public Heal. 2020, 17, 9533. [Google Scholar] [CrossRef]
- Zhu, K.; Kerr, D.A.; Meng, X.; Devine, A.; Solah, V.; Binns, C.W.; Prince, R.L. Two-Year Whey Protein Supplementation Did Not Enhance Muscle Mass and Physical Function in Well-Nourished Healthy Older Postmenopausal Women. J. Nutr. 2015, 145, 2520–2526. [Google Scholar] [CrossRef]
- Andersson, P.; Linge, J.; Gurholt, T.P.; Sønderby, I.E.; Hindley, G.; Andreassen, O.A.; Leinhard, O.D. Poor muscle health and cardiometabolic risks associated with antidepressant treatment. Obesity 2024, 32, 1857–1869. [Google Scholar] [CrossRef] [PubMed]
- Andreo-López, M.C.; Zarco-Martín, M.T.; Contreras-Bolívar, V.; Fernández-Soto, M.L. Prevalence of Sarcopenia and Dynapenia and Related Clinical Outcomes in Patients with Type 1 Diabetes Mellitus. Nutrients 2023, 15, 4914. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.R.; Parker-Autry, C.; Lu, K.; Cummings, S.R.; Hepple, R.T.; Scherzer, R.; Covinsky, K.; Cawthon, P.M.; Lipsitz, L.A. Skeletal Muscle Health, Physical Performance, and Lower Urinary Tract Symptoms in Older Adults: The Study of Muscle, Mobility, and Aging. Journals Gerontol. Ser. A 2023, 79. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, C.E.; Hayes, K.; Tatucu-Babet, O.A.; Lambell, K.J.; Paul, E.; Hodgson, C.L.; Ridley, E.J. Nutrition delivery and the relationship with changes in muscle mass in adult patients receiving extracorporeal membrane oxygenation: A retrospective observational study. Aust. Crit. Care 2024, 37, 727–733. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, X.; Hong, Z.; Lin, X.; Chen, F.; Lan, J.; Zhang, Z.; Deng, H. Associations of plasma retinol and α-tocopherol levels with skeletal muscle health in Chinese children. Br. J. Nutr. 2023, 130, 2174–2181. [Google Scholar] [CrossRef]
- Olpe, T.; Wunderle, C.; Bargetzi, L.; Tribolet, P.; Laviano, A.; Stanga, Z.; Prado, C.; Mueller, B.; Schuetz, P. Muscle matters: Prognostic implications of malnutrition and muscle health parameters in patients with cancer. A secondary analysis of a randomised trial. Clin. Nutr. 2024, 43, 2255–2262. [Google Scholar] [CrossRef]
- Peng, L.; Lin, M.; Tseng, S.; Yen, K.; Lee, H.; Hsiao, F.; Chen, L. Protein-enriched soup and weekly exercise improve muscle health: A randomized trial in mid-to-old age with inadequate protein intake. J. Cachex- Sarcopenia Muscle 2024, 15, 1348–1357. [Google Scholar] [CrossRef]
- Raghupathy, R.; McLean, R.R.; Kiel, D.P.; Hannan, M.T.; Sahni, S. Higher abdominal adiposity is associated with higher lean muscle mass but lower muscle quality in middle-aged and older men and women: the Framingham Heart Study. Aging Clin. Exp. Res. 2023, 35, 1477–1485. [Google Scholar] [CrossRef]
- Sabir, Z.; Dierkes, J.; Hjartåker, A.; Rosendahl-Riise, H. The association of dietary patterns with muscle mass and strength in old age: The Hordaland Health Study. Eur. J. Nutr. 2023, 62, 2739–2750. [Google Scholar] [CrossRef]
- Seo, J.-W.; Jiang, S.; Ahn, S.; Kang, Y.S.; Sung, Y.; Li, X.; Jamrasi, P.; Sun, E.M.; Yoo, J.; Kim, B.-Y.; et al. Effect of mixed protein supplementation on golf performance and muscle function: a randomized, double-blind, placebo-controlled study. J. Int. Soc. Sports Nutr. 2024, 21, 2393368. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Shahsavarani, S.; Vatsia, S.; Katz, A.D.; Ngan, A.; Fallon, J.; Strigenz, A.; Seitz, M.; Silber, J.; Essig, D.; et al. Association between history of lumbar spine surgery and paralumbar muscle health: a propensity score-matched analysis. Spine J. 2023, 23, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Wesselink, E.O.; Pool-Goudzwaard, A.; De Leener, B.; Law, C.S.W.; Fenyo, M.B.; Ello, G.M.; Coppieters, M.W.; Elliott, J.M.; Mackey, S.; Weber, K.A. Investigating the associations between lumbar paraspinal muscle health and age, BMI, sex, physical activity, and back pain using an automated computer-vision model: a UK Biobank study. Spine J. 2024, 24, 1253–1266. [Google Scholar] [CrossRef]
- Xiong, X.; Zang, J.; Zhu, C.; Wei, W.; Wang, P.; Wang, J.; Gao, Q. Effects of Proprioceptive Neuromuscular Facilitation Technique on Balance Function and Muscle Health in Older Adults With High Fall Risk. J. Gerontol. Nurs. 2024, 50, 37–44. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Nagano, F.; Matsumoto, A.; Shimazu, S.; Shiraishi, A.; Kido, Y.; Bise, T.; Kuzuhara, A.; Hori, K.; Hamada, T.; et al. Low hemoglobin levels are associated with compromised muscle health: Insights from a post-stroke rehabilitation cohort. Geriatr. Gerontol. Int. 2024, 24, 305–311. [Google Scholar] [CrossRef]
- Yuan, W.; Chen, M.; Chen, Y.; Xu, D.; Li, Z.; Bai, H.; Xu, Q.; Jiang, Y.; Gu, J.; Li, S.; et al. Effects of soy protein-rich meals on muscle health of older adults in long-term care: A randomized clinical trial. Nutrition 2024, 126, 112507. [Google Scholar] [CrossRef]
- Zhao, X.; Yu, J.; Liu, N. Developing a predictive equation of muscular age to evaluate muscle health in Chinese community-dwelling older women. Heal. Care Women Int. 2023, 44, 1587–1600. [Google Scholar] [CrossRef]
- Bhandari, R.; Lukas, K.; Lee, K.; Shamunee, J.; Almeida, B.; Guzman, T.; Echevarria, M.; Lindenfeld, L.; Nenninger, C.; Iukuridze, A.; et al. Feasibility of telehealth exercise and nicotinamide riboside supplementation in survivors of childhood cancer at risk for diabetes: A pilot randomized controlled trial. Pediatr. Blood Cancer 2024, 72, e31369. [Google Scholar] [CrossRef]
- Distefano, G.; Harrison, S.; Lynch, J.; Link, T.M.; Kramer, P.A.; Ramos, S.V.; Mau, T.; Coen, P.M.; Sparks, L.M.; Goodpaster, B.H.; et al. Skeletal Muscle Composition, Power, and Mitochondrial Energetics in Older Men and Women With Knee Osteoarthritis. Arthritis Rheumatol. 2024, 76, 1764–1774. [Google Scholar] [CrossRef]
- Fujie, S.; Horii, N.; Kajimoto, H.; Yamazaki, H.; Inoue, K.; Iemitsu, K.; Uchida, M.; Arimitsu, T.; Shinohara, Y.; Sanada, K.; et al. Impact of resistance training and chicken intake on vascular and muscle health in elderly women. J. Cachex- Sarcopenia Muscle 2024, 16. [Google Scholar] [CrossRef]
- Kang, C.-H.; Jung, E.-S.; Jung, S.-J.; Han, Y.-H.; Chae, S.-W.; Jeong, D.Y.; Kim, B.-C.; Lee, S.-O.; Yoon, S.-J. Pasteurized Akkermansia muciniphila HB05 (HB05P) Improves Muscle Strength and Function: A 12-Week, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2024, 16, 4037. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.C.; Deutz, N.E.; Kirschner, S.K.; Engelen, M.P. Metabolic kinetics and muscle and brain health markers in older adults, and the role of age and presence of chronic morbidities: A large cross-sectional cohort study. Clin. Nutr. 2024, 43, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Kao, S.-L.; Wang, J.-H.; Lai, H.-Y.; Hsiao, F.-Y.; Chen, L.-K.; Loh, C.-H. Daily Supplementation with Protein-Enriched Lacto-Vegetarian Soups and Muscle Health in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Nutr. Heal. Aging 2025, 29, 100477. [Google Scholar] [CrossRef]
- Korzepa, M.; Marshall, R.N.; Rogers, L.M.; Belfield, A.E.; Quinlan, J.I.; Huang, Y.; Gritsas, A.; Churchward-Venne, T.A.; Glover, E.I.; van Loon, L.J.C.; et al. Postprandial plasma amino acid and appetite responses to a low protein breakfast supplemented with whey or pea protein in middle-to-older aged adults. Eur. J. Nutr. 2025, 64, 1–14. [Google Scholar] [CrossRef]
- Lee, M.-C.; Hsu, Y.-J.; Yang, H.-J.; Huang, C.-C. Enhancement of Lower Limb Muscle Strength and Reduction of Inflammation in the Elderly: A Randomized, Double-Blind Clinical Trial Comparing Lacticaseibacillus paracasei PS23 Probiotic with Heat-Treated Supplementation. Nutrients 2025, 17, 463. [Google Scholar] [CrossRef]
- Yuan, W.; Chen, M.; Chen, Y.; Xu, D.; Li, Z.; Bai, H.; Xu, Q.; Jiang, Y.; Gu, J.; Li, S.; et al. Effects of soy protein-rich meals on muscle health of older adults in long-term care: A randomized clinical trial. Nutrition 2024, 126, 112507. [Google Scholar] [CrossRef]
- Kay, J.; Upchurch, K.S. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology 2012, 51, vi5–vi9. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.A.H.R. The gold standard: not a golden standard. BMJ 2005, 330, 1121–1121. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Manini, T.; Patel, S.M.; Newman, A.; Travison, T.; Kiel, D.P.; Santanasto, A.J.; Xue, Q.; Shardell, M.; Duchowny, K.; et al. Putative Cut-Points in Sarcopenia Components and Incident Adverse Health Outcomes: An SDOC Analysis. J. Am. Geriatr. Soc. 2020, 68, 1429–1437. [Google Scholar] [CrossRef]
- Bhasin, S.; Travison, T.G.; Manini, T.M.; Patel, S.; Pencina, K.M.; Fielding, R.A.; Magaziner, J.M.; Newman, A.B.; Kiel, D.P.; Cooper, C.; et al. Sarcopenia Definition: The Position Statements of the Sarcopenia Definition and Outcomes Consortium. J. Am. Geriatr. Soc. 2020, 68, 1410–1418. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Travison, T.G.; Manini, T.M.; Patel, S.; Pencina, K.M.; Fielding, R.A.; Magaziner, J.M.; Newman, A.B.; Brown, T.; Kiel, D.P.; et al. Establishing the Link Between Lean Mass and Grip Strength Cut Points With Mobility Disability and Other Health Outcomes: Proceedings of the Sarcopenia Definition and Outcomes Consortium Conference. Journals Gerontol. Ser. A 2019, 75, 1317–1323. [Google Scholar] [CrossRef]
- Delmonico, M.J.; Kostek, M.C.; Johns, J.; Hurley, B.F.; Conway, J.M. Can dual energy X-ray absorptiometry provide a valid assessment of changes in thigh muscle mass with strength training in older adults? Eur. J. Clin. Nutr. 2007, 62, 1372–1378. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kuk, J.L. Changes in fat and skeletal muscle with exercise training in obese adolescents: Comparison of whole-body MRI and dual energy X-ray absorptiometry. Obesity 2013, 21, 2063–2071. [Google Scholar] [CrossRef]
- Nelson, M.; Fiatarone, M.; Layne, J.; Trice, I.; Economos, C.D.; Fielding, R.; Ma, R.; Pierson, R.N.; Evans, W.J. Analysis of body-composition techniques and models for detecting change in soft tissue with strength training. Am. J. Clin. Nutr. 1996, 63, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Zhu, K.; Wactawski-Wende, J.; Ochs-Balcom, H.M.; LaMonte, M.J.; Hovey, K.M.; Evans, W.; Shankaran, M.; Troen, B.R.; Banack, H.R.; Newman, A.B. The Association of Muscle Mass Measured by D3-Creatine Dilution Method With Dual-Energy X-Ray Absorptiometry and Physical Function in Postmenopausal Women. Journals Gerontol. Ser. A 2021, 76, 1591–1599. [Google Scholar] [CrossRef]
- Evans, W.J.; Hellerstein, M.; Orwoll, E.; Cummings, S.; Cawthon, P.M. D3-Creatine dilution and the importance of accuracy in the assessment of skeletal muscle mass. J. Cachex- Sarcopenia Muscle 2019, 10, 14–21. [Google Scholar] [CrossRef]
- Clark, R.V.; Walker, A.C.; Miller, R.R.; O’cOnnor-Semmes, R.L.; Ravussin, E.; Cefalu, W.T. Creatine (methyl-d3) dilution in urine for estimation of total body skeletal muscle mass: accuracy and variability vs. MRI and DXA. J. Appl. Physiol. 2018, 124, 1–9. [Google Scholar] [CrossRef]
- Broeck, J.V.D.; Buzzatti, L.; Jager-Wittenaar, H.; Perkisas, S.; Scafoglieri, A. The validity of ultrasound-derived equation models to predict whole-body muscle mass: A systematic review. Clin. Nutr. ESPEN 2021, 46, 133–141. [Google Scholar] [CrossRef]
- Harris-Love, M.O.; Avila, N.A.; Adams, B.; Zhou, J.; Seamon, B.; Ismail, C.; Zaidi, S.H.; Kassner, C.A.; Liu, F.; Blackman, M.R. The Comparative Associations of Ultrasound and Computed Tomography Estimates of Muscle Quality with Physical Performance and Metabolic Parameters in Older Men. J. Clin. Med. 2018, 7, 340. [Google Scholar] [CrossRef]
- Harris-Love, M.O.; Benson, K.; Leasure, E.; Adams, B.; McIntosh, V. The Influence of Upper and Lower Extremity Strength on Performance-Based Sarcopenia Assessment Tests. J. Funct. Morphol. Kinesiol. 2018, 3, 53. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.; Reijnierse, E.M.; Trappenburg, M.C.; Hogrel, J.-Y.; McPhee, J.S.; Piasecki, M.; Sipila, S.; Salpakoski, A.; Butler-Browne, G.; Pääsuke, M.; et al. Handgrip Strength Cannot Be Assumed a Proxy for Overall Muscle Strength. J. Am. Med Dir. Assoc. 2018, 19, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Test-Retest Reliability of Measurements of Hand-Grip Strength Obtained by Dynamometry from Older Adults: A Systematic Review of Research in the PubMed Database. . 2017, 6, 83–87. [Google Scholar]
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker For Older Adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Thomas, M.W. Walking Speed: Reference Values and Correlates for Older Adults. J. Orthop. Sports Phys. Ther. 1996, 24, 86–90. [Google Scholar] [CrossRef]
- Suetta, C.; Haddock, B.; Alcazar, J.; Noerst, T.; Hansen, O.M.; Ludvig, H.; Kamper, R.S.; Schnohr, P.; Prescott, E.; Andersen, L.L.; et al. The Copenhagen Sarcopenia Study: lean mass, strength, power, and physical function in a Danish cohort aged 20–93 years. J. Cachex- Sarcopenia Muscle 2019, 10, 1316–1329. [Google Scholar] [CrossRef]
- Agostini, D.; Gervasi, M.; Ferrini, F.; Bartolacci, A.; Stranieri, A.; Piccoli, G.; Barbieri, E.; Sestili, P.; Patti, A.; Stocchi, V.; et al. An Integrated Approach to Skeletal Muscle Health in Aging. Nutrients 2023, 15, 1802. [Google Scholar] [CrossRef]
- Buford, T.W.; Anton, S.D.; Judge, A.R.; Marzetti, E.; Wohlgemuth, S.E.; Carter, C.S.; Leeuwenburgh, C.; Pahor, M.; Manini, T.M. Models of accelerated sarcopenia: Critical pieces for solving the puzzle of age-related muscle atrophy. Ageing Res. Rev. 2010, 9, 369–383. [Google Scholar] [CrossRef]
- Rule, A.D.; Grossardt, B.R.; Weston, A.D.; Garner, H.W.; Kline, T.L.; Chamberlain, A.M.; Allen, A.M.; Erickson, B.J.; Rocca, W.A.; Sauver, J.L.S. Older Tissue Age Derived From Abdominal Computed Tomography Biomarkers of Muscle, Fat, and Bone Is Associated With Chronic Conditions and Higher Mortality. Mayo Clin. Proc. 2024, 99, 878–890. [Google Scholar] [CrossRef]
- Correa-De-Araujo, R.; Addison, O.; Miljkovic, I.; Goodpaster, B.H.; Bergman, B.C.; Clark, R.V.; Elena, J.W.; Esser, K.A.; Ferrucci, L.; Harris-Love, M.O.; et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An Interdisciplinary Workshop at the National Institute on Aging. Front. Physiol. 2020, 11, 963. [Google Scholar] [CrossRef]
- Ben Kirk, B.; Cawthon, P.M.; Arai, H.; Ávila-Funes, J.A.; Barazzoni, R.; Bhasin, S.; Binder, E.F.; Bruyere, O.; Cederholm, T.; Chen, L.-K.; et al. The Conceptual Definition of Sarcopenia: Delphi Consensus from the Global Leadership Initiative in Sarcopenia (GLIS). Age and Ageing 2024, 53. [Google Scholar] [CrossRef]
- Beaudart, C.; Alcazar, J.; Aprahamian, I.; Batsis, J.A.; Yamada, Y.; Prado, C.M.; Reginster, J.-Y.; Sanchez-Rodriguez, D.; Lim, W.S.; Sim, M.; et al. Health outcomes of sarcopenia: a consensus report by the outcome working group of the Global Leadership Initiative in Sarcopenia (GLIS). Aging Clin. Exp. Res. 2025, 37, 1–13. [Google Scholar] [CrossRef]
Figure 1.
The framework for ‘muscle health’ reflects the multidimensional aspects of general health, physical health, and physical performance. This approach is grounded in the physical dimension of health using the classification system of the International Classification of Functioning, Disability and Health (ICF) developed by the World Health Organization. This framework for muscle health includes the ICF health-related domains: (1) Body Systems/Structures and (2) Participation. The components of these domains represent categories of assessment: (1) body/muscle tissue composition, (2) muscle performance, and (3) functional performance. Each muscle health component may be quantified using various assessment tools. Guidelines concerning testing protocols and data interpretation impact the use of assessment tools to characterize muscle health. ADL: activities of daily living; IADL: instrumental activities of daily living; MRI: magnetic resonance imaging; CT: computed tomography; US: ultrasound; RFD: rate of force development; SPPB: short physical performance battery; TUG: timed up-and-go.
Figure 1.
The framework for ‘muscle health’ reflects the multidimensional aspects of general health, physical health, and physical performance. This approach is grounded in the physical dimension of health using the classification system of the International Classification of Functioning, Disability and Health (ICF) developed by the World Health Organization. This framework for muscle health includes the ICF health-related domains: (1) Body Systems/Structures and (2) Participation. The components of these domains represent categories of assessment: (1) body/muscle tissue composition, (2) muscle performance, and (3) functional performance. Each muscle health component may be quantified using various assessment tools. Guidelines concerning testing protocols and data interpretation impact the use of assessment tools to characterize muscle health. ADL: activities of daily living; IADL: instrumental activities of daily living; MRI: magnetic resonance imaging; CT: computed tomography; US: ultrasound; RFD: rate of force development; SPPB: short physical performance battery; TUG: timed up-and-go.
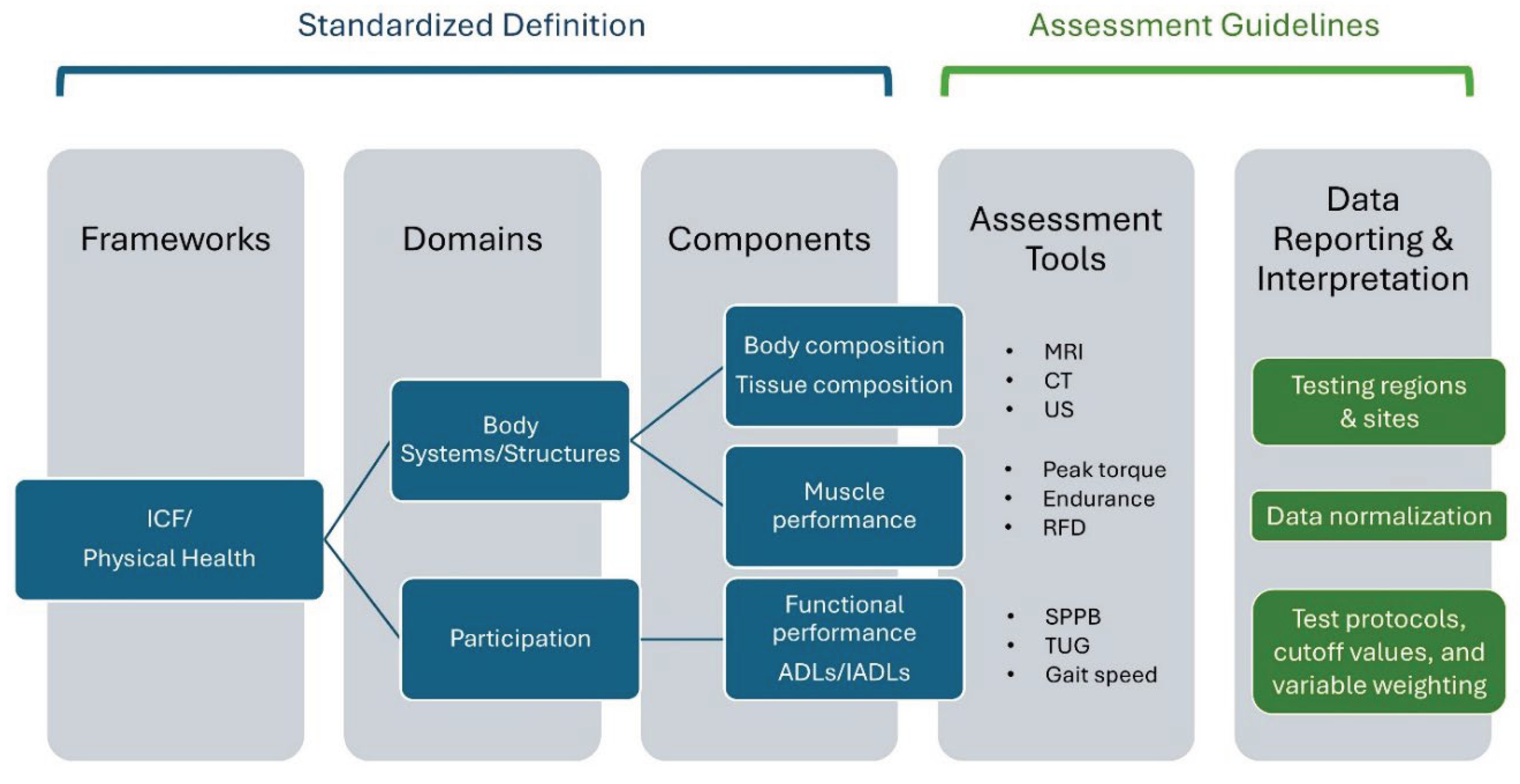
Figure 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
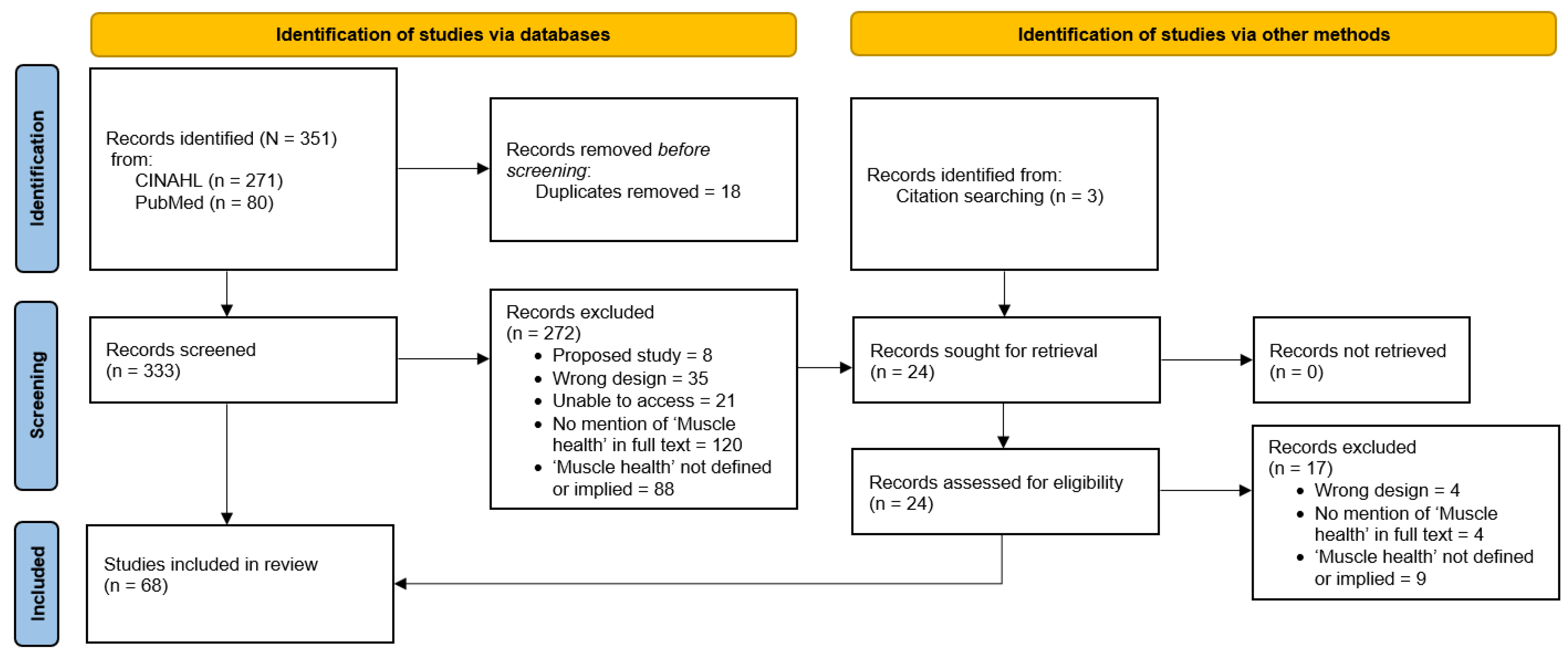

Table 1.
Summary of studies with a definition of ‘muscle health’ included.
| Study | Population | Defined | Measured | Body Composition | Tissue Composition | Performance | Functional tasks | Other |
|---|---|---|---|---|---|---|---|---|
| Anderson et al., 2022 [33] | Patients undergoing surgery for lumbar spine pathology, N=59 (32 M: 22 F), 51.5±16.9 yrs | "Muscle health and function is influenced by structural features such as size (cross-sectional area) and tissue composition (e.g., amount of fatty infiltration within the muscle compartment)", "...paraspinal muscle health (size and composition)…" | Muscle size, composition, and gene expression | CSA, mCSA, F-CSA, the proportion of fat within the muscle compartment (MRI) | Muscle, adipose, loose collagen, and dense collagen composition (tissue biopsy) | 42 genes associated with adipogenic/metabolic, atrophic, fibrogenic, inflammatory, and myogenic pathways, 40S Ribosomal Protein (RPS18) and Beta-Actin (ACTB) as controls |
||
| Andersson et al., 2024 [77] | Individuals using antipsychotic medication, N=35506 (16553 M: 18891 F), 63.3±7.5 (40-69) yrs | “…poor muscle health (i.e., low muscle mass quality/quantity)…” | Body and muscle specific size, composition, and regional fat | Abdominal subcutaneous & visceral adipose tissue volume, total thigh fat-free muscle volume (MRI) | Mean anterior thigh muscle fat infiltration (MRI) | Liver proton density fat fraction Physical activity level and Townsend deprivation index BMI |
||
| Bathgate et al., 2018 [37] | One pair of male monozygotic twins, 52 yrs | "Skeletal muscle health - Whole muscle size, strength, and power were assessed. Additionally, protein and gene expression were measured for various markers of fiber type, metabolism, growth, repair, and inflammation.” | Skeletal muscle size, composition, strength, and power, molecular markers of muscle health, cardiorespiratory and pulmonary health, and blood profiles | CSA, MT (B-mode US) Lean mass, FM, total body fat percentage, visceral adipose tissue, bone mineral content, and bone mineral density (DXA) |
Echo intensity (US) Muscle fiber composition - MHC isoforms, MyMHC expression, cellular metabolism (muscle biopsy, VL) Skeletal muscle fiber type, oxidative metabolism, citrate synthase, angiogenesis, vascular endothelial growth factor, muscular growth and repair, mechano-growth factor, insulin-like growth factor, myoblast determination protein 1, inflammatory responses (QRT-PCR) |
Knee extension (dynamometry) and grip strength | Five sprints (Monark ergometer) and WAnT (Anaerobic capacity) | Cardiorespiratory: Resting heart rate, blood pressure, VO2max, and pulmonary function Muscle biopsy, AMPK protein expression Tracked normal physical activity patterns and dietary intake |
| Bauer et al., 2024 [79] | Community-dwelling older adults ≥70 yrs with urinary tract symptoms, N=641 (264 M: 377 F), 75.5±4.4 yrs | “…age-related declines in skeletal muscle health, such as loss of muscle mass, volume, and strength/power, and related physical performance.” | Body size, muscle mass and volume, strength, power, physical function, cognition, and QoL | WBLM (D3-creatine) and thigh fat-free muscle volume (MRI) | Knee extension peak power (Keiser Air 420 exercise machine) and grip strength | 400m usual walking speed, SPPB, and four-square step test | Mobility Assessment Tool-short form, MoCA, CESD-10, EQ-5D, and CHAMPS Lower urinary tract symptoms: Lower Urinary Tract Dysfunction Research Network Symptom Index-10 Total energy expenditure, BMI |
|
| Berry et al., 2019 [38] | Adults with lower back pain, N=14 (7 M: 7 F), 52.8±14.8 yrs | "The primary outcome measures of muscle health were mCSA and FF." | mCSA, FF, strength, pain, and disability | mCSA (MRI) | FF (MRI) | Maximum lumbar extension strength (dynamometry) | Range of motion (isokinetic dynamometer), 100 mm visual analog scale, Oswestry Disability Index | |
| Bhandari et al., 2025 [93] | Cancer survivors >2 years in remission and off therapy, N=20 (10 M: 10 F), 35 (18-67) yrs | “Exercise has been shown to improve muscle health, including muscle mass, strength, and function…” | Muscle mass, composition, strength, function, metabolic variables | Whole body fat and fat-free mass, segmental muscle mass, visceral adipose tissue (BIA) | RF, GM, GL: CSA, muscle thickness, IMAT (US) | Grip strength | SPPB | Blood: HbA1c, fasting glucose, HOMA-IR, myostatin BMI, waist circumference |
| Cegielski et al., 2022 [41] | Healthy adults, N=37 (21 M: 16 F), 72±5 yrs | “…functional muscle health parameters (e.g., handgrip strength, leg strength, muscle mass by DXA imaging) …" “… established measures of muscle health (handgrip strength, 1-RM and MVC)…” |
Muscle mass, strength, function, and metabolic variables | Thigh FFM (DXA) | Muscle thickness, fascicle length, and pennation angle (US) | Unilateral leg extension 1-RM, MVC (dynamometry) and grip strength | SPPB | Blood: MPS, MPB, and ASR (COSIAM) Muscle biopsy Urine sample collected to measure D3-creatinine |
| Davis et al., 2021 [43] | Men over a 15-year span, N=522, 50.0 (IQR: 38.3-59.7) yrs | “Low muscle mass and poor muscle strength and function are key characteristics of poor muscle health.” | Muscle mass, strength, and function | SMI, whole body composition, and ALM (DXA) | TUG | Self-reported dietary data: food frequency questionnaire Self-reported physical activity: Baecke Physical Activity Questionnaire BMI |
||
| Distefano et al., 2024 [94] | Knee osteoarthritis patients, N=655 (280M: 375F), 76.1±4.9 yrs | “Muscle health, including muscle composition, power, and energetics…” | Muscle mass, fat mass, power, function, cardiovascular function, metabolic variables | Whole body muscle mass (D3-creatine), visceral adipose tissue, abdominal subcutaneous adipose tissue (MRI) | Thigh FFM volume, Thigh muscle fat infiltration (MRI) | Knee extensor peak power (pneumatic), peak power/thigh muscle volume | SPPB, gait speed (400-m) | Physical activity and fitness QoL: MAT-sf questionnaire Mitochondrial energetics: ATPmax, OXPHOS (biopsy) BMI |
| Engelen et al., 2022 [45] | Normal weight moderate and severe COPD patients, N=32 (18M: 14F), 66.8±4.4 yrs | "...and improves muscle health (mass and function as secondary outcomes)." | Muscle mass and strength, lung function, and metabolic variables | Whole body and extremity FM and FFM (DXA) | Grip strength | Blood: glucose, C-reactive protein, amino acids, fatty acids, various other health markers Respiratory muscle function: inspiratory pressure, forced expiratory volume, forced vital capacity Physical Activity Scale for the Elderly questionnaire, Saint George Respiratory Questionnaire BMI, waist circumference |
||
| Finkel et al., 2021 [47] | Males with Duchenne Muscular Dystrophy, N=31, 6.1±1.1 (4-8) yrs | "...lower leg muscle health as determined by the MRI transverse relaxation time constant (T2) from a composite of five muscles." | T2 relaxation time of lower leg muscles, muscle function, metabolic variables, and gene expression | FF (MRI) | Gait speed (10-m walk/run test), 4 stair climb, time to stand, and North Star Ambulatory Assessment | Blood: cytokine panel of multiple inflammatory markers Gene expression: NF-κB-target genes Heart rate, BMI |
||
| Furguson et al., 2024 [80] | Patients receiving extracorporeal membrane oxygenation, N=23(10 M: 13 F), 48±14 yrs |
“…muscle health (size and quality)…” | Muscle size, quality, strength, function, and nutritional data | CSA (US), mCSA (MRI) | Quadriceps thickness and RF echogenicity (US) | Knee extension MVIC (hand-held dynamometer) and muscle strength (Medical Research Council sum score with ICU mobility scale) | Highest level of mobility (ICU mobility scale) | Nutrition data: energy and protein delivery BMI |
| Jackson et al. 2022 [51] | Healthy women, N=53, 55.8±5.3 yrs | "...muscle health (muscle mass, grip strength, five-chair rise test, 4m gait speed test)": muscle mass, strength, and physical function (i.e., muscle health)." | Muscle mass, strength, function, and dietary intake | SMI (BIA) | Grip strength | Gait speed (4-m walk test) and five-time chair stand test | Intake of energy, protein, carbohydrate, and fat Risk for Sarcopenia BMI |
|
| Jacob et al., 2022 [52] | Healthy adults, N=274 (118 M: 156 F), 41.9±16.1 (18-70) yrs | "...indices of muscle health should be evaluated in samples of healthy adults to determine the optimum reference values of muscle morphology, function and functional capability." | Morphology, function, and functional capacity | VL muscle thickness, pennation angle, fascicle length, echo intensity, and contractile properties (US and tensiomyography) | Grip strength | Five-time chair stand test and 1-min chair rise test | Femur length, thigh girth Physical activity level: IPAQ, BPAQ |
|
| Locquet et al., 2019 [55] | Adults ≥65 yrs, N=232 (98 M: 134 F), 75.5±5.4 yrs (76.0±5.1 yrs M, 75.1±5.6 yrs F) | "Muscle health - SMI (kg/m2), grip strength, physical performance…" | Mass, strength, physical performance, nutritional assessment, cognitive assessment, and physical activity | SMI and areal bone mineral density (DXA) | Grip strength | SPPB | Osteoporosis diagnosis: trabecular bone score Mini-Nutritional Assessment Mini-Mental State Examination Self-reported level of physical activity, fracture risk BMI |
|
| Olpe et al., 2024 [82] | Patients with cancer, N=269 (161 M: 108 F), 68.8±13.3 yrs | “…muscle health markers (i.e., handgrip strength, computed tomography (CT)-based muscle mass and radiodensity)…” | Muscle size, composition, strength, and metabolic variables | Skeletal muscle area, SMI, muscle radiodensity, intramuscular adipose tissue (CT) | Grip strength | Blood: Plasma albumin and c-reactive protein Malnutrition risk BMI |
||
| Papaioannou et al., 2021 [57] | Physically active adults, N=191 (69 M: 122 F), 67.4±1.5 yrs M, 67.4 ± 1.6 yrs F | “…based on three indicators of muscle health: muscle mass was assessed using bioelectrical impedance and handgrip strength and 5 times sit-to-stand (5-STS)." | Muscle mass, strength, physical function, and dietary intake | SMI (BIA), SMM (Janseen Equation) | Grip strength | Five-time chair stand test | Dietary data: 90-item food-frequency questionnaire, Healthy diet score Adherence to physical activity (Actigraph GT3x) Blood: High-sensitivity c-reactive protein Risk for Sarcopenia |
|
| Parker et al., 2021 [58] | Adults during preoperative pancreatic cancer treatment, N=97 (52 M: 45 F), 66.4±7.9 yrs | "SMI and SMD were the endpoints of this study; together, they reflect skeletal muscle health." | Muscle quantity and quality | CSA, SMI - scans performed at T0 and T1 (CT) | SMD (CT) | BMI Risk for Sarcopenia |
||
| Pratt et al., 2021 [61] | Healthy older adults, N=300 (150 M: 150 F), 64.1±8.5 (50-83) yrs | “…our findings demonstrate the potential of circulating CAF as an accessible indicator of skeletal muscle health in older adults.” | Muscle mass, strength, and metabolic variables | ALM (DXA) | Grip strength | Plasma: CAF Risk of Sarcopenia |
||
| Shin et al., 2022 [64] | Adults with chronic kidney disease, N=149 (97 M: 52 F), 65±11 yrs | “PhA appears to be a reliable marker for estimating muscle health and HRQoL in patients with CKD.” “…muscle health, inflammatory and muscle-related markers…” “...BIA-derived PhA in estimating the muscle health in patients with CKD. We observed that PhA was related to SMI, handgrip strength, and gait speed; “ |
Body composition, muscle strength and function, and metabolic variables | FFM, SMM, SMI, intracellular water, extracellular water, and total body water (BIA) | Grip strength | Gait speed (6-m walk test) | Blood: Hemoglobin, albumin, high-sensitivity C-reactive protein, hemoglobin A1c, intact parathyroid hormone, total cholesterol, calcium, phosphorus, sodium, potassium, chloride, total carbon dioxide, blood urea nitrogen, creatinine, and eGFR QoL and risk of Sarcopenia BMI |
|
| Song et al., 2022 [65] | Patients who underwent 1-level lumbar microdiscectomy, N=163 (102 M: 61 F), 47.8±15.4 | "“Good” muscle health was defined as score of 2, and “poor” muscle health was defined as score of 0 to 1." “For the good muscle health group, mean PL-CSA/BMI was 169.4 mm2/kg/m2, and mean Goutallier class was 1.5.” |
Muscle size | Normalized total psoas area (MRI) | Goutallier classification (MRI) | |||
| Song et al., 2023 [87] | Healthy participants with and without a history of spine surgery, N=178 (84 M: 94 F), 65.3±12.7 yrs | Muscle health parameters – Goutallier grade, PL-CSA, PL-CSA/BMI, LIV “…novel MRI-based lumbar muscle health grading system incorporating paralumbar cross-sectional areas and Goutallier classification…” |
Body size, muscle size, and composition | Paralumbar-CSA, Paralumbar-CSA/BMI ratio, lumbar indentation value (MRI) | Goutallier classification (MRI) | BMI | ||
| Su et al., 2022 [66] | Chinese men and women (≥65 years), N=2994 (1424 M: 1570 F), 71.9±4.9 yrs | “Our data shows that serum concentrations of individual AAs can be considered biomarkers of muscle health in the older people…” | Body composition, muscle strength and function, and metabolic variables | Lean muscle mass and ALM (DXA) | Grip strength | Gait speed (6-m walk test) and five-time chair stand test | Blood: serum amino acids concentrations Dietary inflammatory index and risk of Sarcopenia BMI |
|
| Tan et al., 2022 [68] | Community-dwelling ambulatory older multi-ethnic Asian patients with Type-2 Diabetes Mellitus, N=387 (184 M: 164 F), 68.4±5.6 yrs (60-89 yrs) | "…muscle health parameters including muscle mass, strength and gait speed…" | Muscle mass, strength, and function | Muscle mass and SMI (BIA) | Grip strength | Gait speed (6-m walk test) | Physical activity: IPAQ, PASE QoL: World Health Organization Quality of Life scale Systolic and diastolic blood pressures Blood: HbA1c, total cholesterol, HDL, LDL, TG BMI |
|
| Vingren et al., 2018 [72] | Men living with Human Immunodeficiency Virus undergoing 60-day inpatient substance abuse treatment, N=16, 42±11 yrs | "...muscle health markers (mass, strength, power)." | Muscle mass, strength, power, and biochemical analysis | Muscle mass estimation (using anthropometric measurements) | Max strength and power (bench press, standing isometric squat) | Vertical jump performance | Blood: IFNγ, IL-1β, IL-2, IL-4, IL-6, IL-10, and tumor necrosis factor (TNF)-α, vascular cell adhesion molecule–1 and cortisol Skinfold thickness, body segment circumferences (upper-arm and forearm) |
|
| Virk et al., 2021 [73] | Patients with lumbar spine pathology requiring operation, N=307 (166 M: 141 F), 56.1±16.7 yrs | "…muscle health measurements including lumbar indentation value (LIV), paralumbar cross-sectional area divided by body mass index (PL-CSA/BMI), and Goutallier classification of fatty atrophy." | Muscle size, quality | LIV and PL-CSA/BMI ratio (MRI) | Goutallier classification of fatty atrophy (MRI) | HRQOLs questionnaires: visual analog pain scale back, visual analog pain scale leg, PROMIS scores, Oswestry disability index, short-form 12 mental health score, and short-form 12 physical health score BMI |
||
| Virk et al., 2021 [74] | Patients with lumbar spine pathology requiring operation, N=308 (168 M, 140 F), 57.7±18.2 yrs | "We measured muscle health by the lumbar indentation value (LIV), Goutallier classification (GC), and ratio of paralumbar muscle cross-sectional area over body mass index (PL-CSA/BMI). A muscle health grade was derived based on whether a measurement showed a statistically significant impact on visual analog scale back and leg pain." | Muscle size, health related QoL | LIV and PL-CSA/BMI ratio (MRI) | Goutallier classification of fatty atrophy (MRI) | HRQOLs questionnaires: visual analog pain scale back, visual analog pain scale leg, PROMIS scores, Oswestry disability index, short-form 12 mental health score, and short-form 12 physical health score BMI |
||
| Wesselink et al., 2024 [88] | Adults with acute or chronic back pain, N=9,564 (5,595 M: 3,969 F), 63.5±7.6 yrs | “Decline in paraspinal muscle health in BP has been characterized by increased intramuscular fat (IMF) and decreased size (i.e., muscle atrophy).” | Muscle size and composition | CSA (MRI) | IMAT (MRI) | IPAQ and back pain status BMI |
||
| Yuan et al., 2024 [91] | Older adults in long-term care facilities, N=84 (22 M: 52 F), 84.9±7.0 yrs | Muscle health-related indicator: lean mass (SLM, SMM, ASMM, and SMI), handgrip strength, five-time chair stand, and SPPB |
Muscle mass, strength, function, and QoL | SLM, SMM, ASM, and SMI (BIA) | Grip strength | Gait speed (6-m walk test), five-time chair stand test, and SPPB | Calf circumference Energy and macronutrient intake QoL |
|
| Zhao et al., 2023 [92] | Chinese community-dwelling older women >65 yrs: N=57, 70.6±4.9 yrs Normal older women: N=10, 70.4±4.4 yrs Older women with pre-Sarcopenia or sarcopenia: N=9, 70.9±3.8 yrs Older women with exercise habits: N=10, 70±3.7 yrs |
“In this study, several indicators were selected to reflect muscle health including muscle mass, grip strength, 30s chair stand, arm curl with a dumbbell, and preferred and maximal gait speed….” | Body size, muscle mass, strength, function | Upper and lower limb skeletal muscle mass and appendicular muscle mass (DXA) | Grip strength | Gait speed (preferred & maximal), chair stand test (30-s), and arm curl reps (2 kg) | BMI | |
| Zhu et al., 2015 [76] | Healthy older postmenopausal women, N=196, 74.3±2.7 yrs | “Over the 2 y, we observed a reduction in the upper arm and calf muscle areas and a decrease in hand-grip strength in women in both the protein and the placebo groups, indicating deterioration in muscle health with aging.” | Muscle mass and function | ASMM (DXA) and upper arm and calf muscle CSA (peripheral quantitative CT) | Ankle dorsiflexion, knee flexor, knee extensor, hip abductor, hip flexor, hip extensor, and hip adductor strength (strain gauge) and grip strength | TUG | Dietary intake, 24-hour urinary nitrogen, and levels of physical activity BMI |
|
| Abbreviations: AA=Amino acids, ALM=Appendicular lean mass, AMPK=5′AMP-activated protein kinase, ASMI=Appendicular skeletal muscle index, ASMM=Appendicular skeletal muscle mass, ASR=Absolute synthesis rate, BCAA=Branched-chain amino acid, B-mode=Brightness mode, BIA=Bioelectrical impedance analysis, BMI=Body mass index, BPAQ=Bone physical activity questionnaire, CAF=C-terminal agrin fragment, cESD-10=Center for epidemiologic studies depression scale, CHAMPS=Community health activities model program for seniors, CKD=Chronic kidney disease, COPD=Chronic obstructive pulmonary disease, COSIAM=Combined oral assessment of muscle, CSA= Cross sectional area, CT=Computed tomography, DXA=Dual energy x-ray absorptiometry, EAA=Essential amino acids, EQ-5D=5-level EuroQol, F=Female, F-CSA=Fat cross sectional area, FF=Fat fraction, FM=Fat mass, FFM=Fat free mass, GL=Lateral gastrocnemius. GM=Medial gastrocnemius, HbA1c=Hemoglobin A1c, HDL=High-density lipoprotein, HRQoLs=Health-related quality of life, IQR=Median with interquartile (25th, 75th percentiles) range, mCSA=Muscle cross-sectional area, ICU=Intensive care unit, IL=Interleukin, ICU=Intensive care unit, IPAQ=International physical activity questionnaire, LDL=Low-density lipoprotein, LIV=Lumbar indentation value, M=Male, mCSA=Lean muscle cross sectional area, MoCA=Montreal cognitive assessment, MPB=Muscle protein breakdown, MPS=Muscle protein synthesis, MRI=Magnetic resonance imaging, MT=Muscle thickness, MVC=Maximum voluntary contraction, MVIC=Maximum voluntary isometric contraction, mHC=Myosin heavy chain protein, MyMHC=Myosin heavy chain gene, NEAA=Sum non-essential amino acids, PASE=Physical activity scale for the elderly, PhA=Phase angle, PL-CSA/BMI= Paralumbar cross-sectional area divided by body mass index, PROMIS=Patient-reported outcomes measurement information system, RF=Rectus femoris, RM=Repetition maximum, SLM=Soft lean mass, SMD= Skeletal muscle density, SMI=Skeletal muscle index, SMM=Skeletal muscle mass, SPPB=Short physical performance battery, QoL=Quality of life, QRT-PCR= Quantitative reverse transcriptase polymerase chain reaction, Sum AA=Sum all measured amino acids, TG=Triglycerides, TNF=Tumor necrosis factor, TUG=Timed up and go test, US=Ultrasound, VO2max=Maximal aerobic capacity, VL=Vastus lateralis, WAnT=Wingate anaerobic test, Yrs=Years | ||||||||
Table 2.
Summary of studies without a definition of ‘muscle health’ included.
| Study | Population | Measured | Body Composition | Tissue Composition | Performance | Functional tasks | Other |
|---|---|---|---|---|---|---|---|
| Andreo-Lopez et al., 2023 [78] | Adults with type 1 diabetes mellitus, N=62 (21 M, 41 F), 38±14 yrs |
Body size, composition, strength, and metabolic variables | FFM, FM, total body water, extracellular water, body cellular mass index, SMI, ASMI, and FFM index (BIA) | Grip strength | Blood: Fasting blood glucose, total cholesterol, LDL and HDL cholesterol, triglycerides, albumin, prealbumin, and C reactive protein, glycated hemoglobin A1c, daily total dose insulin, daily total dose insulin per kilogram, and insulin sensitivity factor Lifestyle Parameters: 14-item PREDIMED questionnaire, IPAQ Risk for Sarcopenia BMI |
||
| Arentson-Lantz et al., 2019 [34] | Healthy older adults, N=17 (11 M: 6 F), 68±2 yrs | Muscle mass, composition, and metabolic variables | WBLM, WBFM, and LLM (DXA) | CSA and single fiber volume (biopsy with immunohistochemical analysis) | Isokinetic knee extension peak torque (dynamometry) | Dietary intake and step count Blood: blood glucose and plasma insulin (ELISA) BMI |
|
| Arentson-Lantz et al., 2019 [35] | Healthy older (60-80 years) adults, N=20 (12 M: 8 F), 68.5±1.5 yrs |
Body composition, strength, physical function, and metabolic variables | WBLM, WBFM, and LLM (DXA) | Isokinetic knee extension peak torque (dynamometry) | SPPB and peak aerobic capacity (cycle ergonomic test) | Mean Daily Energy and Macronutrient Intake Blood: blood glucose and serum insulin (ELISA) BMI |
|
| Arentson-Lantz et al., 2020 [36] | Healthy older (60-80 years) adults, N=20 (14 M: 6 F), 67.8±1.1 yrs | Body composition, strength, physical function, and dietary intake | WBLM, WBFM, and LLM (DXA) | CSA and single fiber volume (immunohistochemical analysis), protein content – signaling protein expression levels and single fiber characteristics (muscle biopsy - radioimmunoprecipitation assay buffer), | Isokinetic knee extension peak torque (dynamometry) | SPPB and peak aerobic capacity (cycle ergonomic test) | Mean Daily Energy and Macronutrient Intake BMI |
| Bislev et al., 2019 [39] | Postmenopausal women, N=104, 64.5 yrs (61-68) | Mass, function, physical performance, QoL, and metabolic variables | ALM and FM (DXA) | Maximum voluntary isometric muscle strength, maximum force production (elbow flexion and elbow extension, knee flexion [dynamometry]), and grip strength | TUG, postural stability, and chair rising test | Blood: PTH, 25(OH)D, phosphate, ionized calcium, magnesium, creatinine, and thyroid stimulating hormone Urine: Calcium, phosphate, and magnesium Self-reported physical activity, primary hyperparathyroidism-QoL, and SF36v2 BMI |
|
| Bislev et al., 2020 [40] | Healthy postmenopausal women with secondary hyperparathyroidism and vitamin D insufficiency, N=81, 65 (IQR: 61-68.4) yrs |
Muscle strength and function, cardiovascular health, and metabolic variables | ASMI and FMI (DXA) | Maximum voluntary isometric muscle strength, maximum force production (elbow flexion and elbow extension, knee flexion [dynamometry]), and grip strength | TUG | Blood: 25(OH)D, 1,25(OH)2D, PTH, Ca2+, magnesium, phosphate, eGFR, total cholesterol, HDL, LDL, and triglycerides Urine: Creatinine, plasma glucose and lipid profile: hydroxybutyrate, acetate, acetoacetate, acetone, alanine, betaine, carnitine, choline, citrate, creatine, creatinine, dimethylamine, formate, glucose, glutamate, glutamine, glycerol, glycine, isoleucine, lactate, leucine, lysine, methionine, o-phosphocholine, ornithine, phenylalanine, proline, pyruvate, succinate, threonine, trimethylamine n-oxide, tyrosine, urea, valine, τ-methylhistidine Calcium intake Cardiovascular health: blood pressure and arterial stiffness BMI |
|
| Cha et al., 2022 [42] | CKD patients, N=150 (97 M: 53 F), 65.0 ± 10.8 yrs |
Muscle mass, performance, strength, and metabolic variables | Body composition (BIA) | Grip strength | Gait speed (6-m walk test) | Blood: Indoxyl sulfate, TNF-α, IL-6, myostatin, serum creatinine, eGFR Kidney disease QoL, IPAQ |
|
| Engelen et al., 2023 [44] | Moderate to severe COPD patients and healthy controls, N=416 (190 M: 226 F), 68.1 yrs (65.5-71.0) |
Muscle mass, strength, respiratory function and metabolic variables | WBFM, extremity FM, FFM, and bone mineral density of spine and hip, ASMI and visceral adipose tissue (DXA) | Maximal leg extension force - one-leg reciprocal extensions (dynamometry), and grip strength. | Blood: Arginine, citrulline, glutamate, glutamine, glycine, histidine, hydroxyproline, isoleucine, leucine, ornithine, phenylalanine, tau-methyl-histidine, taurine, tryptophan, tyrosine, and valine Gynoid to android ratio (DXA) Habitual dietary intake and physical activity level, level of dyspnea, COPD assessment test Respiratory muscle function (hand-held mouth pressure device). BMI |
||
| English et al., 2016 [46] | Middle-aged adults, N=19 (12 M: 7 F), 51.5±1 yrs |
Muscle mass, function, and quality | WBLM, WBFM, LLM, and body fat percentage (DXA) | Muscle quality (knee extensor peak torque divided by LLM) | Unilateral knee and ankle extensor strength and knee muscle endurance (dynamometer) | Peak aerobic capacity (cycle ergometer) | Dietary intake, Cell signaling and skeletal muscle protein synthesis (muscle biopsy) BMI |
| Fujie et al., 2024 [95] | Elderly women, N=81, 67.2±5.3 yrs | Muscle mass, quality, strength, and metabolic variables | Quadriceps muscle CSA (MRI), thickness, and echogenicity (US) | 1- Repetition Maximum leg extension and biceps curl | Blood: Total cholesterol, HDL, triglycerides, angiotensin II, endothelin-1, complement component 1q, creatinine, and plasma renin activity Blood pressure, heart rate, carotid-femoral pulse wave velocity, carotid β-stiffness |
||
| Gil et al., 2022 [48] | Hospitalized COVID-19 survivors N=80 (41 M: 39 F), 59±14 yrs |
Muscle strength and size | CSA (US) | Grip strength | Self-perception of health BMI |
||
| Granic et al., 2018 [49] | Community-dwelling participants, N=722 (289 M: 433 F), 85+ yrs |
Strength, function, protein intake, and physical activity | FM and FFM (BIA) | Grip strength | TUG | Protein intake: 24-hour multiple-pass dietary recall Self-reported physical activity BMI |
|
| Groenendijk et al., 2020 [50] | Geriatric hip fracture patients, N=40 (11 M :29 F), 82±8.0 yrs |
Muscle mass and strength | ASMM (BIA), muscle thickness (US) | Grip strength | Nutritional status and dietary intake Risk for Sarcopenia |
||
| Huang et al., 2023 [81] | Healthy Chinese children 6-9 yrs, N=426 (243 M: 183 F), median 8.0 yrs (IQR=7.3-8.8 yrs) | Muscle mass, strength, and metabolic variables | ASMM (DXA) | Grip strength | Blood: plasma retinol, plasma ɑ-tocopherol Energy and nutrient intake BMI |
||
| Kang et al., 2024 [96] | Elderly adults >60 yrs, N=100 (12 M: 88 F), 65±4 yrs | Muscle strength, physical function, and muscle related hormones | Muscle mass (DXA) | Knee extension torques (isokinetic dynamometry) and grip strength | SPPB, TUG, gait speed | Blood: myostatin, follistatin, and high-sensitivity C-reactive protein | |
| Kang et al., 2024 [97] | Older adults, N=575 (274M: 301F), 50-95 yrs | Body composition, muscle and fat mass, strength, and metabolic variables | FM, lean soft tissue, appendicular skeletal muscle mass, visceral adipose tissue, android and gynoid FM ratio (DXA) | Concentric peak torque (isokinetic dynamometer) and grip strength | Blood: amino acid concentrations, C-reactive protein, aspartate, glutamate, hydroxyproline, asparagine, glutamine, citrulline, serine, glycine, arginine, threonine, alanine, taurine, proline, tau-methylhistidine, valine, methionine, isoleucine, leucine, tryptophan, phenylalanine, ornithine, histidine, lysine, tyrosine Respiratory muscle function: Maximal inspiratory pressure PASE and cognitive questionnaire Dietary intake BMI, blood pressure |
||
| Kao et al., 2025 [98] | Adults ≥65 yrs at risk of malnutrition and sarcopenia, N=97 (24 M: 73 F), 72.4±5.2 yrs | Body composition, strength, function, and metabolic variables | ASM, body fat %, skeletal muscle mass (BIA) | Grip strength | SPPB, 5-time STS, 6-m walk time | Blood: fasting glucose, HbA1c, insulin, homocysteine, creatine, other health measures for cardiometabolic risk factors, renal and liver function SARC-F, SARC- combined with calf circumference, mini nutritional assessment-short form, mini-mental state examination, geriatric depression scale-15 Waist and hip circumference, total body water, BMI |
|
| Korzepa et al., 2025 [99] | Healthy middle-to-older adults, N=22 (11 M; 11 F), 61.3±6.5 (50-70) yrs | Body composition, and metabolic variables | Body fat % (DXA) | Blood: plasma glucose, insulin, AA concentration, appetite hormones Respiratory exchange ratio, resting metabolic rate BMI |
|||
| Lee et al., 2025 [100] | Healthy older adults, N=119 (39 M: 61 F), (65-85) yrs | Body composition, strength, endurance, function, and metabolic variables | Body fat % (BIA) | 30s arm curl test and grip strength | 10-m walk test, 30s STS, TUG, and 3-min incremental step-test | Blood: HbA1c, creatinine, glucose, testosterone, cystatin C, insulin, and measures for liver function, kidney function, blood lipids, and other biomarkers | |
| Li et al., 2021 [53] | Chinese older adults with low lean mass, N=123 (61 M: 62 F), 70±4 yrs | Lean muscle mass, strength and physical performance | ASMI and lean mass (DXA) | Grip strength | SPPB | Daily dietary intake and physical activity level BMI |
|
| Locquet et al., 2018 [54] | Community-dwelling older subjects, N=288 (118 M: 170 F), 74.7±5.7 yrs | Muscle mass, strength and physical performance | SMI and areal bone mineral density (DXA) | Grip strength | SPPB | Skeletal status, fracture risk, and risk of Sarcopenia BMI |
|
| Matsumoto et al., 2023 [56] | Stroke patients with sarcopenia hospitalized, N=241 (107 M: 134 F), 79.3±10 yrs | Muscle mass, strength, and metabolic variables | SMI (BIA) | Grip strength | Blood: Albumin, c-reactive protein, and hemoglobin Functional independence measure score, ADL assessment, nutritional intake, and risk of Sarcopenia BMI |
||
| Peng et al., 2022 [59] | Middle aged and older adults, N=103 (35 M: 68 F), 64.0±8.2 yrs | Muscle size, composition, strength, performance, and metabolic variables | Total FM and FFM (BIA), and relative ASMM (MRI) | IMAT and CSA (MRI) | Grip strength | Gait speed (6-m walk test) | Blood: Serum albumin, alanine aminotransferase, uric acid, total cholesterol, HDL, LDL, triglyceride, serum creatinine, high-sensitivity C-reactive protein, and fasting glucose; Whole blood glycated hemoglobin Cognitive function, nutritional and mood status IPAQ, BMI |
| Peng et al., 2024 [83] | Adults with inadequate protein intake, N=97 (18 M: 79 F), 64.7±4.8 yrs | Muscle size, strength, physical function, metabolic variables and quality of life | Relative ASMM (BIA) | Body fat percentage (BIA) | Grip strength | Usual gait speed (6-m), 6-min walk test, and five-time chair stand test | Blood: Albumin, creatinine, alanine aminotransferase, total cholesterol, HDL, LDL, uric acid, fasting glucose, dehydroepiandrosterone sulfate, insulin-like growth factor-1, homocysteine, high-sensitive c-reactive protein, vitamin D3, glycated hemoglobin, myostatin, and leptin Cognition: MoCA, CES-D, IPAQ Nutritional status SF-36, BMI |
| Pérez-Piñero et al., 2021 [60] | Caucasian men and postmenopausal women, N=45 (8 M: 37 F), 58.9±6.1 (50-75) yrs | Muscle mass, function, strength, quality, and metabolic variables | FM, lean mass, muscle mass, and ASMM (DXA) | Muscle quality (muscle mass between the peak torques) | Knee extension torques (isokinetic and isometric dynamometry) and grip strength | Blood pressure, health-related QoL, SF-36, dietary intake BMI |
|
| Raghupathy et al., 2023 [84] | Adults and children, N=962 (428 M: 534 F), 60±9 (5-70) yrs | Body size, muscle composition, quality, strength, physical activity level, and blood markers of inflammation | ALM (DXA), subcutaneous and visceral adipose tissue (CT) | Upper extremity muscle quality (strength per kilogram of lean mass) | Knee extension (hand-held isometric dynamometry) and grip strength | Blood: IL-6, monocyte chemoattractant protein-1, resistin, and adiponectin (ELISA) Physical activity BMI |
|
| Rousseau et al., 2015 [62] | Adults with thermal burns N=15 (11 M: 4 F), 50 (25-64) yrs | Muscle strength and metabolic variables | Bone mineral density (DXA) | Knee muscle strength (isokinetic dynamometry) | Blood: 25OH–D, 1,25(OH)2–D, calcium, fibroblast growth factor 2, PTH, phosphate, creatine, collagen type 1 cross-linked C-telopeptide, serum type 1 procollagen N-terminal and serum bone alkaline phosphatase | ||
| Sabir et al., 2023 [85] | Norwegian adults, N=1317 (578 M: 739 F), 67-70 yrs | Muscle mass, body composition, strength, physical activity, and habitual dietary intake | SMM, ASMM, ASMI, total body FM and percentage (BIA) | Grip strength | Habitual dietary intake Self-reported physical activity BMI |
||
| Schneider et al., 2015 [63] | Healthy adults in microgravity environments, N=11 (9 M: 2 F), 40±7 yrs | Mechanical properties of skeletal muscles and tendons | Oscillation frequency (Hz), dynamic stiffness (N/m), elasticity, mechanical stress relaxation (ms) time, creep (Deborah number) (MyotonPRO device) BMI |
||||
| Seo et al., 2024 [86] | Healthy adults, N=60 (27 M: 30 F), ~59±9.5 (26-64) yrs | Body size, body composition, muscle strength, golf performance, physical function, and metabolic variables | SMM and FM (BIA) | Knee extension and flexion strength (dynamometry) and grip strength | Golf drive distance, club-head speed, ball speed, 2-min push-up test, and MFT balance test | Blood: lactic acid, creatine, lactate dehydrogenase, creatine kinase, blood urea nitrogen, red blood cell, white blood cell, hemoglobin, platelet, hematocrit, glucose, aspartate aminotransferase, alanine transaminase, and gamma-glutamyl transferase Dietary intake and levels of physical activity Blood pressure, heart rate, BMI |
|
| Sutherland et al., 2023 [67] | Participants from the United Kingdom Biobank with probable sarcopenia and sarcopenic obesity, N=307,281 (144,538 M: 162,743 F) 37-73 yrs | Muscle mass, strength, vitamin D levels | Combined arm skeletal muscle mass and whole-body FM (BIA) | Grip strength | Blood: serum 25(OH)D concentrations Self-reported levels of physical activity BMI |
||
| Van Ancum et al., 2020 [69] | Community-dwelling adults, N=197 (57 M: 140 F), 67.9 (57-75.1) yrs | Body composition, muscle mass, strength, and function | SMM, SMI, ALM, ALM/height2, SMM and ALM relative to body weight (BIA) | Grip strength | Gait speed (4-m walk test) | Self-reported levels of physical activity, ADL, and risk of Sarcopenia BMI |
|
| Van Dongen et al., 2020 [70] | Community-dwelling older adults, N=168, (66 M, 102 F), 75±6 yrs | Body composition and mass, muscle strength and function | Lean body mass, ALM, and FM (DXA) | Lower limb 3-Repetition Maximum test (leg press and leg extension machines) and knee extension strength (dynamometry) | Gait speed (6-min walk test and 4-m walk test), SPPB, and TUG | QoL, ADL, nutritional status, dietary intake, and risk of Sarcopenia BMI |
|
| Vesey et al., 2020 [71] | Children and adolescents with conditions that impacted musculoskeletal health, N=17, 15.7±2.9 yrs | Body composition and function | Whole body: FM, lean mass, bone mineral content, and bone mineral density Lumbar spine: bonce mineral content and bone mineral density (DXA) |
Gait speed (6 min walk test), chair stand test, balance test, and single leg jump test | BMI | ||
| Vitale et al., 2020 [75] | Healthy older adults, N=9 (3 M: 6 F), 68 ± 7 (62.9-73.1) yrs | Body composition, muscle strength and function | Lean mass, FM, ASMI (DXA) and CSA of thigh (MRI) | Maximum isometric strength of knee flexor and extensor (dynamometry) and grip strength | Chair stand test (30-s) and Mini balance evaluation systems test | BMI | |
| Xiong et al., 2024 [89] | Older adults with high fall risk, N=160, 68.5±8.9 (65-85) yrs | Muscle mass and function | Bone mineral density and lower limb muscle mass (DXA) | Berg balance scale, TUG, chair stand test (30-sec), and fall-risk assessment tool | Fall-risk questionnaire | ||
| Yoshimura et al., 2024 [90] | Stroke patients, N=955 (511 M: 443 F), 73.2±13.3 yrs | Muscle mass, strength, and metabolic variables | SMI (BIA) | Grip strength | Blood: Albumin, hemoglobin, c-reactive protein Energy and protein intake and pre-stroke ADL |
||
| Abbreviations: 25(OH)D=25-hydroxy vitamin D, 1,25(OH)2D= 1,25dihydroxy vitamin D, AA=Amino acids, ADL=Activities of daily living, ALM=Appendicular lean mass, ASMI=Appendicular skeletal muscle index, ASMM=Appendicular skeletal muscle mass, BIA=Bioelectrical impedance analysis, BMI=Body mass index, Ca2+=Ionized calcium, CESD-10=Center for epidemiologic studies depression scale, CKD=Chronic kidney disease, COPD=Chronic obstructive pulmonary disease, CSA= Cross sectional area, CT=Computed tomography, DXA=Dual energy x-ray absorptiometry, eGFR=Estimated glomerular filtration rate, ELISA=Enzyme-linked immunosorbent assay, F=Female, FM=Fat mass, FMI=Fat mass index, FFM=Fat free mass, HDL=High-density lipoprotein, IL=Interleukin, IMAT=Intramuscular adipose tissue, IPAQ=International physical activity questionnaire, LDL=Low-density lipoprotein, LLM=Leg lean tissue mass, M=Male, MoCA=Montreal cognitive assessment, MRI=Magnetic resonance imaging, PTH=Parathyroid hormone, QoL=Quality of life, SF-36=Short form-36 health survey, SMI=Skeletal muscle index, SMM=Skeletal muscle mass, SPPB=Short physical performance battery, TNF=Tumor necrosis factor, TUG=Timed up and go test, US=Ultrasound, WBFM=Whole body fat mass, WBLM=Whole body lean tissue mass, Yrs=Years | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



