Submitted:
20 August 2025
Posted:
21 August 2025
You are already at the latest version
Abstract
Fish bone ingestion is a common presentation to the emergency department, usually benign and self-limiting. But in rare instances, migration of a sharp foreign body beyond the oesophageal wall can lead to life-threatening complications such as mediastinitis, vascular injury, or pseudoaneurysm formation. We present a case of a 66-year old man who presented with recurrent complaint of chest pain that was initially diagnosed as pneumonia and low-risk chest pain. Further history revealed fish bone ingestion approximately a month earlier, coinciding with the onset of his symptoms. A computed tomography angiography (CTA) of the aorta confirmed a thoracic aortic pseudoaneurysm with an embedded fish bone. During admission, the patient developed massive haemoptysis and, despite resuscitation efforts, passed away. This case highlights the importance of maintaining a high index of suspicion for atypical aetiologies in patients with persistent or unexplained symptoms. A thorough history taking and appropriate imaging are vital in identifying rare but fatal complications.
Keywords:
foreign body
; vascular injury
; pseudoaneurysm
; aorta
; computed tomography angiography
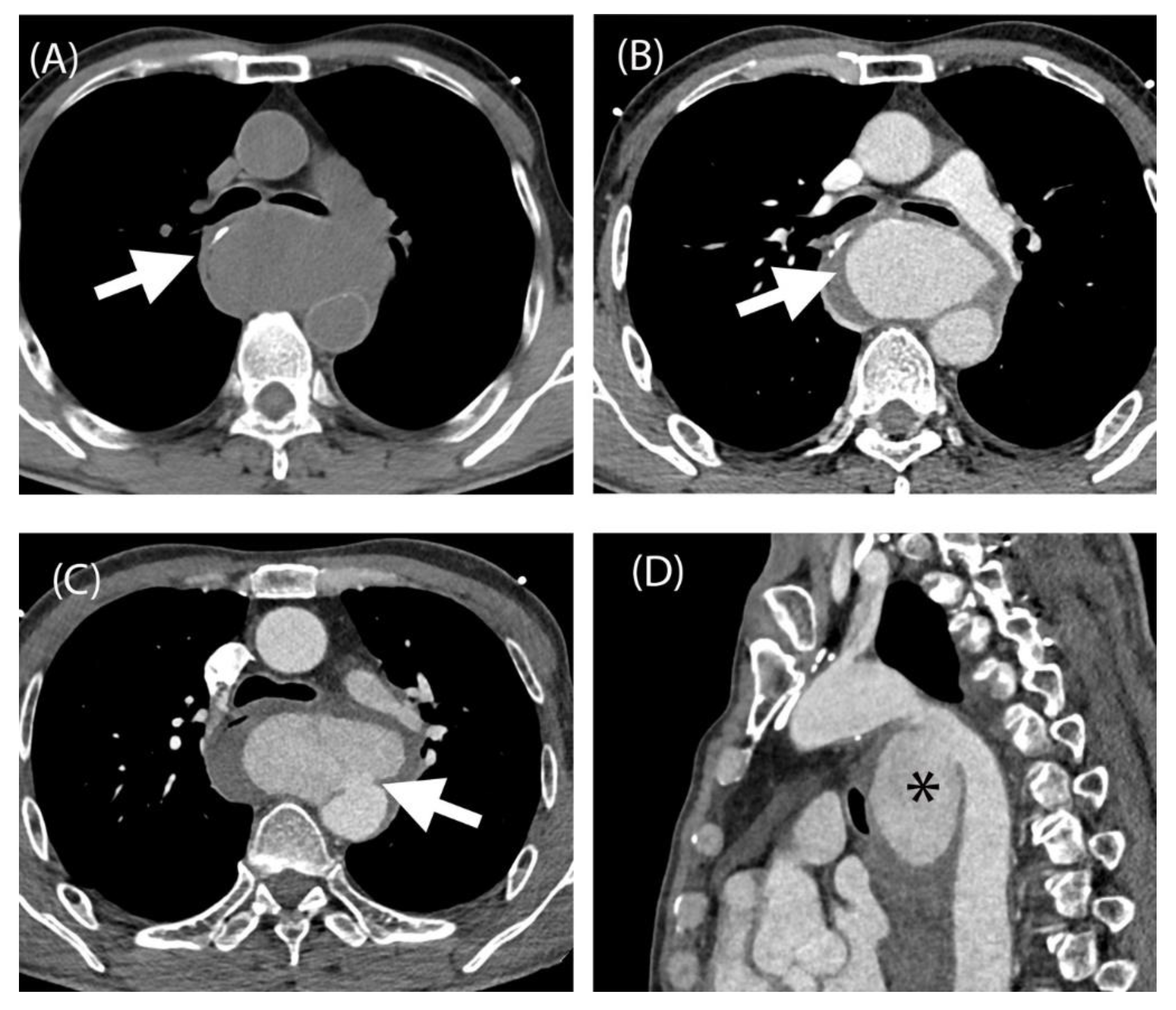
Figure 1.
Complication of ingestion fish bone complicated with aortic pseudoaneurysm. Unenhanced CTA aorta at the level of carina showing hyperdense linear structure suggestive of fish bone within the oesophageal wall (A, white arrow). Contrasted study of CTA aorta of the same level at the carina showing contrast within the pseudoaneurysm sac and surrounding haematoma (B, white arrow). CTA aorta at the level of carina showing the neck of pseudoaneurysm exerting mass effect causing displacement of carina anteriorly and oesophagus right laterally (C, white arrow). The oesophagus at this level is compressed by the pseudoaneurysm causing obstruction and failure of nasogastric tube insertion. Sagittal reformatted image of CTA aorta exhibiting the pseudoaneurysm (D, asterisk). A, unenhanced CTA aorta. B-C, arterial phase of CTA aorta. D, sagittal view of CTA aorta. Note: CTA: Computed Tomography Angiography. Common causes of thoracic pseudoaneurysm are atherosclerosis, postoperative sequela, trauma, infection and iatrogenic. Accidental fish bone ingestion is commonly encountered and is usually located to the oropharynx and can be managed by otorhinolaryngology (ORL) team via scope. However, a fish bone is able to migrate distally in the oesophagus, and thoracic oesophagus was reported to be the second most common location after cervical oesophagus [1]. Our patient had fish bone in his thoracic oesophagus which led to the injury to the adjacent aorta. Although rare, the formation of aorto-oesophageal fistula may lead to aortic pseudoaneurysm. It is usually caused by direct penetration of foreign body or infection of the oesophageal wall leading to the rupture [2]. Symptoms of penetrating fish bone injury complicated with aortic pseudoaneurysm are non-specific. Our patient presented with chronic chest pain and recurrent hospital visits. It was mistaken as pneumonia and low-risk chest pain as he was discharged a few times with planned treatment. Detailed history taking elicited neglected fish bone ingestion and presence of a mass from echocardiogram led to the CTA thoracic aorta, which localised the fish bone in the thoracic oesophagus and confirmation of its complication which was pseudoaneurysm. Treatment of thoracic pseudoaneurysm includes surgical intervention, video-assisted thoracic surgery (VATS) [3] or endovascular graft [1]. Surgical intervention is a more effective, albeit an invasive procedure, to avoid eruption of a pseudoaneurysm. However it can be debilitating to patient as it can cause traumatic injury and has a relatively high mortality rate [1]. Lung abscess is one of the complications of fish bone ingestion which can be managed by VATS. Endovascular repair is a less invasive option to treat aortic pseudoaneurysm and suitable for high-risk patients. It can effectively control the bleeding and place the patient temporarily out of danger if there are associated complications [2]. In comparison to open repair, endovascular repair has advantages in terms of quick recovery, few complications and low mortality [4]. Oesophageal repair is usually done for oesophageal perforation. Factors affecting the type of operation, whether direct repair or partial resection of the oesophagus depend on the location of perforation, the type of foreign body and the degree of mediastinitis [5]. Mediastinal infection due to foreign body may also invade to the aortic wall leading to myocytic aneurysm. Open repair is the gold standard of treatment for mycotic aneurysm but this requires high technical conditions. This includes aggressive debridement of the infection, prosthetic reconstruction as well as lifelong antibiotics treatment [2].
Figure 1.
Complication of ingestion fish bone complicated with aortic pseudoaneurysm. Unenhanced CTA aorta at the level of carina showing hyperdense linear structure suggestive of fish bone within the oesophageal wall (A, white arrow). Contrasted study of CTA aorta of the same level at the carina showing contrast within the pseudoaneurysm sac and surrounding haematoma (B, white arrow). CTA aorta at the level of carina showing the neck of pseudoaneurysm exerting mass effect causing displacement of carina anteriorly and oesophagus right laterally (C, white arrow). The oesophagus at this level is compressed by the pseudoaneurysm causing obstruction and failure of nasogastric tube insertion. Sagittal reformatted image of CTA aorta exhibiting the pseudoaneurysm (D, asterisk). A, unenhanced CTA aorta. B-C, arterial phase of CTA aorta. D, sagittal view of CTA aorta. Note: CTA: Computed Tomography Angiography. Common causes of thoracic pseudoaneurysm are atherosclerosis, postoperative sequela, trauma, infection and iatrogenic. Accidental fish bone ingestion is commonly encountered and is usually located to the oropharynx and can be managed by otorhinolaryngology (ORL) team via scope. However, a fish bone is able to migrate distally in the oesophagus, and thoracic oesophagus was reported to be the second most common location after cervical oesophagus [1]. Our patient had fish bone in his thoracic oesophagus which led to the injury to the adjacent aorta. Although rare, the formation of aorto-oesophageal fistula may lead to aortic pseudoaneurysm. It is usually caused by direct penetration of foreign body or infection of the oesophageal wall leading to the rupture [2]. Symptoms of penetrating fish bone injury complicated with aortic pseudoaneurysm are non-specific. Our patient presented with chronic chest pain and recurrent hospital visits. It was mistaken as pneumonia and low-risk chest pain as he was discharged a few times with planned treatment. Detailed history taking elicited neglected fish bone ingestion and presence of a mass from echocardiogram led to the CTA thoracic aorta, which localised the fish bone in the thoracic oesophagus and confirmation of its complication which was pseudoaneurysm. Treatment of thoracic pseudoaneurysm includes surgical intervention, video-assisted thoracic surgery (VATS) [3] or endovascular graft [1]. Surgical intervention is a more effective, albeit an invasive procedure, to avoid eruption of a pseudoaneurysm. However it can be debilitating to patient as it can cause traumatic injury and has a relatively high mortality rate [1]. Lung abscess is one of the complications of fish bone ingestion which can be managed by VATS. Endovascular repair is a less invasive option to treat aortic pseudoaneurysm and suitable for high-risk patients. It can effectively control the bleeding and place the patient temporarily out of danger if there are associated complications [2]. In comparison to open repair, endovascular repair has advantages in terms of quick recovery, few complications and low mortality [4]. Oesophageal repair is usually done for oesophageal perforation. Factors affecting the type of operation, whether direct repair or partial resection of the oesophagus depend on the location of perforation, the type of foreign body and the degree of mediastinitis [5]. Mediastinal infection due to foreign body may also invade to the aortic wall leading to myocytic aneurysm. Open repair is the gold standard of treatment for mycotic aneurysm but this requires high technical conditions. This includes aggressive debridement of the infection, prosthetic reconstruction as well as lifelong antibiotics treatment [2].
References
- Wang A, Zhou Y, Huang Q. A fish bone induced aortic arch pseudoaneurysm in a male patient: A case report. Medicine (Baltimore). 2019 July;98(29):e16486. [CrossRef]
- Zeng L, Shu W, Ma H, Hu J. Aortic injury caused by esophageal foreign body-case reports of 3 patients and literature review. Medicine (Baltimore). 2020 June 26;99(26):e20849. [CrossRef]
- Tan S, Tan S, Peng M, Yu F. Management of an Ingested Fish Bone in the Lung Using Video-Assist Thoracic Surgery: A Case Report. Medicine (Baltimore). 2015 June;94(22):e943. [CrossRef]
- Wang W, Liu X, Lu M. Case-report: endovascular treatment of aortic pseudo-aneurysm caused by Fishbone. J Cardiothorac Surg. 2015 Dec;10(1):94. [CrossRef]
- Jiang D, Lu Y, Zhang Y, Hu Z, Cheng H. Aortic penetration due to a fish bone: a case report. J Cardiothorac Surg. 2020 Dec;15(1):292. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



