Submitted:
14 August 2025
Posted:
15 August 2025
You are already at the latest version
Abstract
Selecting donor organs is both a science and an art. The calculus is often complex evaluating recipients’ acute needs and the quality and risks of the donor organs. Sarcoidosis is usually a disease of exclusion and considered an idiopathic inflammatory granulomatous process frequently in the lung but often with multiorgan involvement. New insights into the interplay between the environmental or occupational antigens and the susceptible genetic host in sarcoidosis have come to light. One such occupational antigen with mixed data regarding the risk of developing sarcoidosis after exposure is silica dust. Despite strict exposure limitations enforced in the United States and several other governing bodies worldwide, clusters of silicosis are on the rise due to engineered stone (quartz), which contain silica particles that when cut can create a dust that can exceed exposure limitations. Data on the quartz-sarcoidosis relationship is minimal, and thus questions exist regarding the risk of silica dust exposure and the risk of sarcoidosis. Silicosis tends to only affect the lungs, preventing them usually from being transplanted while sarcoidosis is recognized as having a high probability of multiple organ involvement. An index case discovered during organ recovery highlights the possible association between silica exposure and sarcoidosis. This case also examples the complexity of donor organ evaluation and the challenges in organ procurement from exposed individuals.
Keywords:
transplant organs
; Sarcoidosis
; occupational lung disease
; silica dust
; engineered stone
; quartz
; organ procurement
1. Introduction
Selection of donor organs for transplant requires a difficult calculus that balances the acute and chronic needs of the recipient and the presumed quality of the donor organs. Limited clinical and historical data on the donor can result in organ evaluation challenges and surprises at recovery. Known chronic progressive diseases in potential donors can result in frequent organ declines. One such chronic disease is sarcoidosis which is primarily a diagnosis of exclusion and whose pathogenesis is presumed to be due to an inciting exposure in a genetically susceptible individual [1]. Sarcoidosis can involve any organ, but pulmonary involvement is the most common. Several studies have evaluated occupational exposures initiating sarcoidosis with conflicting results regarding risks of specific exposures [2]. One exposure with conflicting data is silica dust. Challenges arise in clinically distinguishing sarcoidosis from silicosis particularly at the time of organ recovery when history and previous evaluations are not available. The challenges of determining silicosis from sarcoidosis may result in organs being declined at recovery. To add to this complexity, silicosis and silica dust exposure are again on the rise, case reports and case control studies have explored whether a new form of sarcoidosis or sarcoid-like disease exists from silica dust exposure, distinct from silicosis [3,4,5,6]. This paper presents an index case of a patient with unexpected sarcoid-like diffuse lung granulomatous process and a history of working in a quarry. It further addresses the question of appropriateness of various organs for donation in affected individuals.
2. Index Case
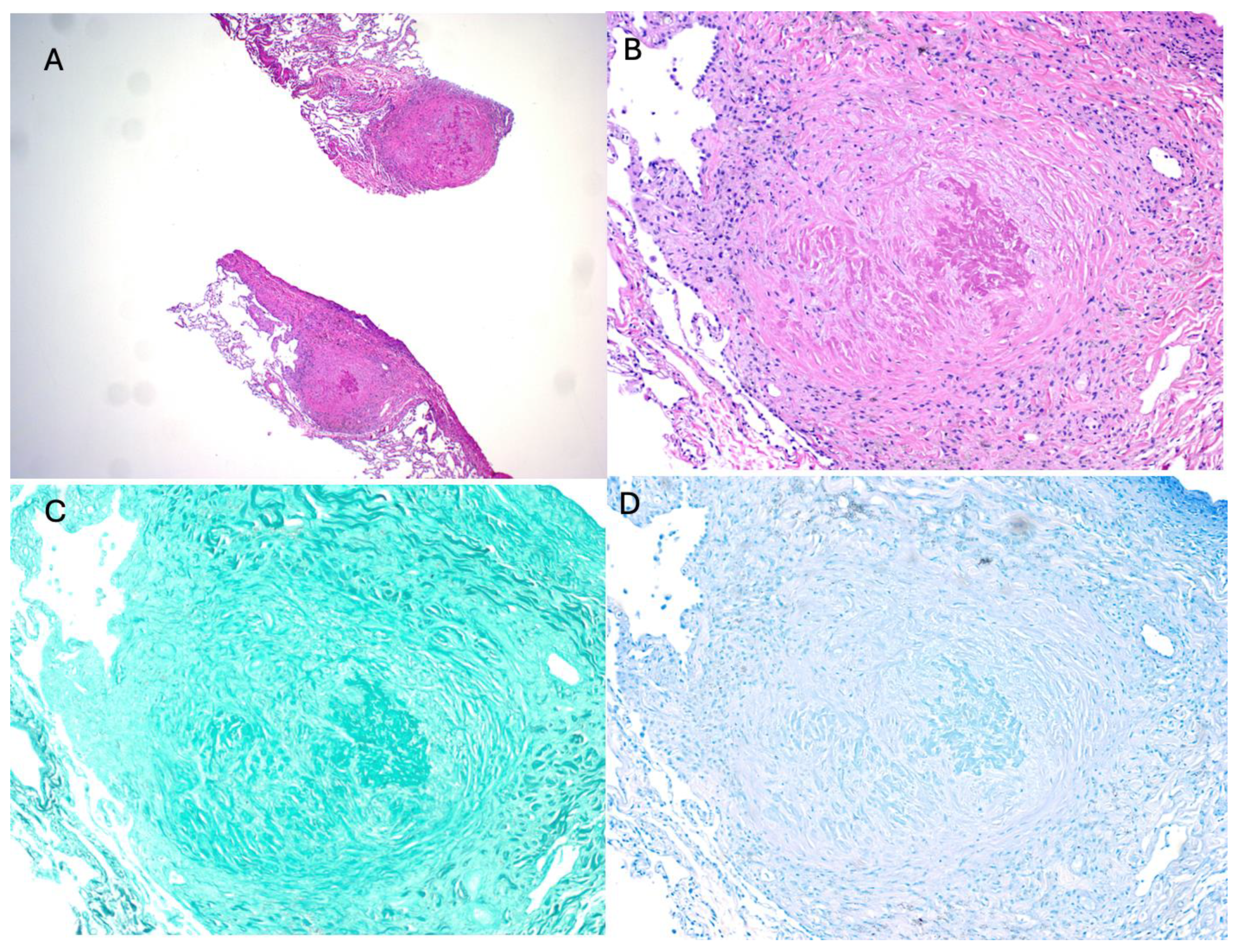
A 45-year-old man with a medical history of only alcohol-related liver cirrhosis presented to the emergency room with acute left-sided weakness. The patient had a notable occupational history of working in granite construction. Laboratory results were significant for a slightly elevated international normalized ratio (INR) consistent with his compensated liver disease. Imaging demonstrated a large right-side intracranial hemorrhage with a slight midline shift for which he received fresh frozen plasma. Despite maximal therapy, the patient herniated to brain death and the family elected for organ donation. A poor-quality computed tomography (CT) of his chest demonstrated normal lung parenchyma, no significant mediastinal lymphadenopathy and bilateral lower lobe consolidation (Figure 1A-C). Screening bronchoscopy with bronchoalveolar lavage (BAL) was likewise unremarkable. The patient’s cirrhosis was presumed due to alcohol use, and no secondary cause of cirrhosis was identified. Given his medical history and organ donor evaluation, he was deemed suitable for potential heart, lung, pancreas, kidney, and intestine donation, but prospective recipients were only identified to receive the lungs and kidneys. During organ recovery, however, the patient was noted to have innumerable small miliary surface lung nodules that appeared to outline the secondary lung lobule (Figure 2A-B). With this incidental finding, the question arose of whether the lungs and kidneys would be suitable for transplant. A surgical biopsy of the right lower lung lobe was performed, which was immediately read and demonstrated numerous caseating and non-caseating granulomas (Figure 3A – C). Routine protocol kidney biopsies were performed with no significant pathology (glomerulosclerosis, necrosis, inflammation, granulomas or arteriolar sclerosis) identified. Due to concerns and uncertainty for diagnosing a systemic inflammatory disease like sarcoidosis or a malignancy in a timely fashion, neither the lungs, kidneys, nor any other organs or tissues were ultimately used for transplant or research. Due diligence resulted in further special histologic stains performed later on the intraoperative biopsy tissue. Notably, the final surgical pathology did not demonstrate acid-fast staining or fungal organisms, ruling out miliary tuberculosis and invasive fungal infections. The kidney biopsy was also negative for granulomatous inflammation or cancer. Given the granulomatous process in the lung parenchyma, the patient was diagnosed with sarcoidosis. The question arose of what role, if any, did the patient’s occupational exposure to silica and granite play in the observed lung pathology and if the observed changes in the lung required rejection of the kidneys for transplant.
3. Sarcoidosis: Complexity in Diagnosis and Pathogenesis
Sarcoidosis is a multisystem inflammatory disease characterized usually by non-caseating granuloma formation. Organ involvement commonly includes lymph tissue, lungs, heart, brain, ocular, skin or joints [1]. Incidence and prevalence vary greatly worldwide with Scandinavian countries having an incidence of 11.5 per 100,000 with a prevalence of 160 per 100,000 [7,8]. North America has an incidence of 7 to 11 per 100,000, with a prevalence of 60 per 100,000 [9,10,11]. The incidence is much lower in East Asia with a 0.5 to 1.3 per 100,000 people and a prevalence of 2.2 per 100,000 [8,10]. Individual demographic characteristics are also strongly associated with sarcoidosis [12,13]. In the United States, the incidence and prevalence of sarcoidosis is significantly higher for black individuals (17.8 and 141.4 per 100,000, respectively) than for white individuals (8.1 and 49.8 per 100,000, respectively). The highest prevalence is in black females (178.5 per 100,000) [9,12]. The exact pathogenesis of sarcoidosis remains unknown, but it is widely hypothesized to be a disease of inciting exposure in a genetically susceptible host [1]. The granulomas of sarcoidosis can develop in virtually any organ or tissue and can cause a wide range of pathology from asymptomatic to severe manifestations of disease requiring organ transplantation [1]. The reason for the wide clinical distribution is being investigated, with inciting factors like micro-organisms, environmental/organic material exposures and genetics, being at the forefront of these important questions [1]. Racial differences in disease presentation and progression are seen with white individuals presenting with a more indolent course later in life in comparison to black individuals who present earlier often with a more aggressive form [9,13,14].
A case control etiologic study of sarcoidosis of 706 affected patients and their nearly 28,000 first and second degree relatives demonstrated a higher risk for sarcoidosis in first degree relatives with an odds ratio (OR) of 4.7 (95% confidence interval (CI) 2.3-9.7) [15]. A case control study in the Swedish National Patient Register identified 23,880 individuals with sarcoidosis and estimated familial relative risk of 3.7-fold increase with an affected first degree relative, and a 4.7-fold increase if two or more relatives had sarcoidosis [16]. Twin studies from Danish and Finnish populations demonstrated an eighty fold increase in risk in monozygotic twins for the development of sarcoidosis, which fell to 7-fold in dizygotic twins [17]. Genetic contribution to sarcoidosis has led to a multitude of genome wide analyses. The major histocompatibility complex is the most well-known genetic link, particularly the human leukocyte antigen (HLA)-DR allele, specifically DRB1*1101 allele [15,18,19,20]. The HLA-DRB1*0301 allele was associated with Lofgren’s syndrome in Scandinavian patients with sarcoidosis [21]. Genes identified as potential links to sarcoidosis susceptibility are the butyrophilin-like 2 gene and annexin A11 genes, while angiotensin-converting enzyme variants have been linked with sarcoidosis presence and severity in Black Americans and Finnish people [19,21,22,23,24,25,26,27,28]. Genes related to T-helper cells 1 (Th1) type responses, interleukin (IL)-17, macro phase metalloelastase-12 (MMP-12) and a disintegrin and metalloprotease decysin-1 protein (ADAMDEC1) were overexpressed in pulmonary sarcoidosis [29]. A gene set analysis of over 26,000 genes compared between self-limited sarcoidosis and pulmonary progressive fibrotic sarcoidosis demonstrated 334 genes that were significantly different from each other, and most related to host immune activation, proliferations and defense, with the progressive fibrotic sarcoidosis phenotype mimicking hypersensitivity pneumonitis gene profiles [30].
Diagnosis can be challenging, particularly when there is no accepted consensus on how to diagnose sarcoidosis [31]. In general, diagnosis is based on three criteria including a compatible clinical presentation, non-necrotizing granulomatous inflammation in one or more tissues, and the exclusion of alternative causes of granulomatous diseases [31]. There are several exceptions to these rules, such as classic presentations of Lofgren disease, lupus pernio, and Heerfordt’s syndrome which do not require invasive testing, and the nodular pulmonary sarcoid variant which can contain both necrotizing and non-necrotizing granulomas [31,32,33,34,35].
There was one case report of necrotizing granulomas in sarcoidosis that was initially misdiagnosed as Mycobacterium tuberculosis [36]. The patient underwent a splenectomy, which demonstrated confluent whitish nodules that replaced the spleen parenchyma [36]. Histopathology revealed extensive necrotizing granulomas, and a presumptive diagnosis of M. tuberculosis was made [36]. When traditional therapy with rifampicin, isoniazid, pyrazinamide, ethambutol daily for 6 months did not improve, the patient was started on a course of steroids for sarcoidosis treatment, with rapid improvement [36]. Invasive testing is usually pursued to rule in other granulomatous mimickers such as tuberculosis, atypical mycobacteria, histoplasmosis or other fungal infections, malignancy, types of vasculitis, drug reactions, particularly immunomodulators, hypersensitivity pneumonitis and chronic berylliosis. This degree of testing cannot be easily performed at the time of organ recovery.
Biopsies most consistent with sarcoidosis demonstrate non-necrotizing granulomas with rings of hyaline collagen surrounding cluster differentiation of cytotoxic T cells (CD)8- and CD4-positive T lymphocytes, B lymphocytes, monocytes, mast cells and fibroblasts, which surround a tightly packed central core with macrophages, epithelioid cells, multinucleated giant cells and CD4-positive T lymphocytes [37,38,39]. The degree of lymphocytic infiltration and fibrosis is patient and duration-dependent [38]. Less common, but still consistent, histopathological findings of sarcoidosis are asteroid bodies, Schaumann bodies, birefringent crystalline particles, but these are not specific for sarcoidosis [37,38]. As mentioned before, rarely, sarcoidosis can include some necrotizing granulomas. The lung parenchyma will demonstrate necrosis with perivascular masses consisting of confluent granulomas, though there will be a background of non-necrotizing granulomas in a lymphangitic distribution [40]. Alternative and more common causes of caseating granulomas must be excluded. Work-up generally includes fungal and mycobacterial stains, mycobacterial polymerase chain reaction, and serum antineutrophil cytoplasmic antibodies [40]. Notably, the presence of blood vessel wall fibrinoid necrosis peripheral to the necrotic center, which can be found by performing a Verhoeff-Martius-scarlet blue trichrome or Masson trichrome-Verhoeff stain, assesses for vascular damage caused by immune complex deposition, infection or autoimmune disease, and thus excludes necrotizing sarcoidosis [40,41].
The pathogenesis of sarcoidosis granuloma formation is complex but is hypothesized to begin with an unknown foreign antigen stimulating monocyte recruitment and differentiation, leading to macrophage aggregation and evolution into epithelioid cells, and eventually multinucleated giant cells [14,38,42]. A tight central cluster of macrophages, epithelioid cells and multinucleated giant cells forms as granulomas mature [38,42]. Antigen presenting cells, one of the many functions of alveolar macrophages, are relevant to sarcoidosis prognosis, remission or prolonged chronic inflammation [43]. A Th1 cytokine response from CD4+ T cell recognition leads to granulomatous inflammation present in sarcoidosis. CD4+ Th1 lymphocytes make up most of the lymphocytes within the granuloma, though the periphery is made of both CD4+ and CD8+ T cells.
4. Occupational Exposure to Silica: A Rising Concern and Possibly an Inducer of Sarcoidosis
Given the rise in engineered stone use, which generates high silica dust content during installation, several broader perspectives, and newer insights have been generated between silica dust and sarcoidosis [4,44]. Several studies have investigated various environmental and occupational exposures in the development of sarcoidosis. A systematic review and meta-analysis of all airborne occupational exposures associated with sarcoidosis was performed by Huntley, et al. in 2023, which included a total of 76 studies, some demonstrating silica exposure as a risk for sarcoidosis development [45]. Perhaps the best known of these studies is the ACCESS study of 706 patients with biopsy confirmed non-caseating granulomas and a clinical presentation consistent with sarcoidosis [46]. In addition to silica, an exposure history to insecticides, pesticides, mold, mildew, musty odors, and central air conditioning increased the prevalence of sarcoidosis [46]. Occupational data from 921 African Americans in 273 sibling relationships demonstrated increased prevalence of sarcoidosis with exposure to titanium, high humidity, water damage, musty odors and vegetable dust [47]. Silica was not noted to be associated with sarcoidosis in these studies. Several case reports were published of patients who developed sarcoidosis and had a history of silica or silicate exposure [48,49,50,51]. Beijer, et al. notably describes the case of a patient who was initially diagnosed with silicosis based on open lung biopsy demonstrating non-caseating granulomas with birefringent material, but no silicate nodules, with radiology studies demonstrating indistinguishable features between sarcoidosis and silicosis [48]. When the patient did not respond as expected to initial management, re-review of the pathology deemed the patient had sarcoidosis and treatment with infliximab was eventually required. In this case, the authors state the non-caseating granuloma around the birefringent crystalline or amorphous silica dust was more consistent with sarcoidosis as there was a lack of silicate nodules [48]. Mochizuka, et al. published a case where silicate nodules of dust laden hyalinized collagen were found on endobronchial ultrasound and transbronchial biopsies and sarcoid like non-caseating granulomas with clustered epithelial cells and multinucleated giant cells surrounded by lymphocytic inflammation were found on pathology from the surgical lung biopsies [52]. The authors hypothesize silica can cause a sarcoid-like granulomatous response as an antigen, similar to beryllium exposure [52]. Ronsmans and coauthors describe two patients who worked with metal-halide lamps and were diagnosed with sarcoidosis at first glance, but biopsies from lung parenchyma and mediastinal lymphadenopathy showed birefringent particles along with non-caseating granulomas of epithelioid cells and giant cells [50]. Further investigation into the workers’ exposure history revealed exposure to glass tubes that were clipped and were made of silica. Removal of the exposure led to clinical, radiographical and functional improvement without the need for additional intervention [50]. Another case report described an individual with exposure to silica dust and who developed both silicosis, as evidenced by silicate nodules in the lung parenchyma, but also had granulomas with birefringent material on biopsies obtained from the bone marrow, liver and spleen [53]. The patient underwent a unilateral lung transplant and native lung pneumonectomy. With removal of the silica dust exposure, the patient’s granulomatous process resolved, and he made an excellent recovery with pseudo normal lung function with a single lung [53]. This case highlights the presence of an overlap syndrome with silica dust acting as stimulus for silicosis in the lungs, but also as an antigen leading to a diffuse sarcoidosis-like response in the rest of the body [53].
Several retrospective and case control studies investigating the association between silica exposure and sarcoidosis have been conducted. A retrospective cohort study of men working Swedish iron foundries showed an increased risk of sarcoidosis if there was a high exposure level to silica (Incidence ratio 3.94, 95% CI 1.07 to 10.08) [54]. Interestingly, there was also an increased risk of rheumatoid arthritis in these individuals l (Incidence ratio 2.59; 95% CI 1.24 to 4.76) [54]. A Swedish case control study of nearly 11,000 men with sarcoidosis were more likely to have had an exposure history of respirable silica within the last five years, (OR 1.27, 95% CI 1.13 to 1.43), with a higher association if men were below age 35 (odds ratio (OR) 1.48, 95% CI 1.16 to 1.87) as opposed to above age 35 (OR 1.21, 95% CI 1.05 to 1.39) [55]. Jonsson, et al. performed a cohort study of 371 cases of sarcoidosis among male Swedish construction workers and found an increased risk of sarcoidosis in those exposed to medium to high levels of silica [relative risk (RR) 1.83 (95% confidence interval [56] 1.14–2.95)]. When stratified for smoking status, results demonstrated that silica exposed smokers had an increased risk of sarcoidosis (RR 2.44 (95% CI 1.37–4.33) whereas nonsmokers exposed to silica did not have an increased risk of sarcoidosis [RR 1.07 (95% CI 0.72–1.58)] [56]. A case series of 12 patients with exposure to crystalline respirable silica particles had a positive association with sarcoidosis, but the authors were particular about not assuming a causal relationship given the complexity of genetic and other exposures that undoubtedly interplay [5]. The PEDIASARC study investigated indirect exposure history in pediatric patients with sarcoidosis with the results demonstrating a higher association with sarcoidosis if the children lived with an adult who was exposed to silica, talcum, combustion or welding fumes and cleaned with scouring reagents [57]. The PEDIASARC study is one of the first to relate adult exposures to children’s risk of developing sarcoidosis [57]. Rezai et al. conducted a rapid review on occupational exposure in sarcoidosis and has discussed the above studies, risk of bias, quality of evidence, and other smaller studies of silica exposure and sarcoidosis, but ultimately concludes that the poor quality of evidence and high risk of bias precludes drawing meaningful associations between sarcoidosis and silica exposure [58].
In Israel, an influx of referrals for lung transplantation due to silicosis was first noted in 2012. These were found to be related to the use of an artificial stone (a synthetic polymer resin bound with high silica content >85%) and were found to have a particularly aggressive and fatal form of silicosis [4]. Granite contains about 25-60% of silica particles, with lighter colors containing a higher silica percentage [59]. With implementation of Occupational Safety and Health Administration (OSHA) requirements for exposure limits on silica dust, the overall prevalence of silicosis in the United States has declined [60,61,62]. However, clusters of silicosis have been on the rise, tracking back to engineered stone with high levels of silica particles, which are in high demand due to their lower cost and favorable properties of being more damage resistant than granite or marble countertops [3,59]. Engineered stone facilities were found to contain silica particle levels far above OSHA’s limits [3,59]. Fazio, et al. published a case series of 52 Latino immigrant workers with an occupational history of working with engineered stone or quartz and that presented with silicosis with 58% having a delayed diagnosis, 38% having advance disease, and an 18% mortality [3]. Silicosis was diagnosed based on history of occupational exposure to airborne silica and either imaging or pathological findings characteristic of silicosis, according to the guidelines of the Occupational Respiratory Disease Surveillance from the National Institute for Occupational Safety and Health (NIOSH) [3]. Two of the patients had an initial alternative diagnosis of sarcoidosis [3]. In China, eighteen patients had rapidly progressive silicosis after exposure to the same artificial stone described by Fazio et al. who had similar characteristics of high mortality [63]. The increasing use of engineered quartz and lack of adherence to OSHA safety limits of silica exposure will undoubtedly increase silicosis in the United States and worldwide. There may be a concomitant rise in sarcoidosis diagnoses given the previous positive associations. Silica dust exposure is able to cause silicosis and may be related to sarcoidosis. The vast diversity of genetic factors, environmental exposures, phenotypic presentations, and racial differences does raise the question of whether sarcoidosis itself is a common manifestation of other diseases that have not yet been identified. Like in the index case, separating silicosis disease from sarcoidosis at the time of organ recovery is very difficult to do.
5. Transplantation: Unexpected Challenges in Organ Donation
In the absence of an occupational history of silica exposure or a known history of silicosis or sarcoidosis, it may be very difficult to exclude these patients as donors pre-recovery of organs. The case series by Fazio and colleagues showed seven of the 52 patients exposed to silica were asymptomatic, the vast majority presented with a cough, weight loss, chest or back pain, or shortness of breath [3]. Given the relatively young demographic and the large pulmonary reserve, a significant degree of parenchymal involvement prior to symptom presentation can be expected. The patient in the index case was an immigrant and had an occupational history of working with silica particles but passed away from a spontaneous intracranial hemorrhage. He had no documented history of hypoxemia or exertional dyspnea, although it is unclear if his compensated liver disease complicated his presentation prior to his death. It was only during the organ procurement operation when surgeons identified pulmonary nodules outlining the secondary lobule did questions of organ suitability arise. To start addressing these questions, a brief review on the current organ donation recommendations for lungs, and previous literature for organ donations from individuals affected by sarcoidosis will be discussed.
The ideal lung transplant donor fits these relative criteria: 1) age less than 55 years; 2) ABO compatibility; 3) clear chest radiograph; 4) partial pressure of oxygen (PaO2) of greater than 300 mm Hg on an fraction of inspired oxygen (FiO2) of 1.0 on a positive end expiratory pressure (PEEP) of 5 cm H2O), 5) tobacco history of less than twenty years; 6) absence of significant chest trauma; 7) no evidence of aspiration or sepsis; 8) no prior cardiopulmonary surgery; 9) bronchoscopy demonstrating no evidence of gastric aspiration or purulent secretions; 10) gram stain of sputum or BAL without organisms; and 11) no history of significant chronic lung disease [64,65]. Of the potential lung donors, very few meet all of the criteria above, thus an extended donor criteria were established with the surgeon’s evaluation as the data point in the decision of whether less than ideal donor criteria are acceptable for the proposed recipient. While the specifics vary between transplant programs, published studies on extended criteria donors generally had abnormal chest radiography, PaO2 less than 300 mm Hg on PEEP of 5 cm H2O, purulent sputum on bronchoscopy and smoking history greater than 20 pack-years. Data compiled from these studies demonstrated no significant difference in the short-term outcome for transplantation success. However, Mulligan performed a long-term survival study using the Organ Procurement and Transplantation Network/Network for Organ Sharing dataset which demonstrated reduced one-year survival with extended criteria donors, and the lowest survival in recipients of extended criteria donor organs who had a lung allocation score of 70 or greater, indicating those most likely to benefit from a lung transplant had the worst outcomes after transplantation [64,66,67,68,69,70]. In these cases, significant chronic lung disease was not a flexible criterion.
In general, the presence of sarcoidosis has precluded affected individuals from organ donation. Blood donations are still possible provided the patient has made a full recovery, though after a significant amount of time (often several years) to ensure a low relapse risk [71]. A case report in 1993 described a young male donor with undiagnosed sarcoidosis led to a short-lived course of pulmonary sarcoidosis in the recipient, with eventual clearance of granulomas on biopsy eight months later [72]. No changes to the patient’s immunosuppression were described [72]. In 1994, a case report of a 32-year-old female with pulmonary arterial hypertension underwent a lung transplant from a donor with sarcoidosis, which was diagnosed by lung biopsy sixteen months prior to the donor’s death [73]. The medical staff did not know about the sarcoidosis diagnosis prior to utilization of the organs for transplantation [73]. However, the recipient did not demonstrate any signs of sarcoidosis clinically, histologically, or radiographically [73]. A case in 1990 described a 19-year-old male donor who was found to have epithelioid granulomas in the pulmonary parenchyma and hilar lymph nodes at the time of necropsy, however the donor’s heart, liver, kidneys, and corneas were already transplanted [72]. The recipient of the donor’s heart developed pulmonary interstitial granulomatous inflammation, but recipients of the other organs remained asymptomatic [72]. Padilla, et. al. [74] reviewed four publications with organs or tissue from donors with known sarcoidosis with several but not all showing donor acquired sarcoidosis. Stem cell donors with sarcoidosis resulted in the development of recipient systemic sarcoidosis in a median of 20 months after allo-stem cell transplant and 7 months after non-allo-stem cell transplant. Another case report describes a woman who underwent evaluation to be a living kidney donor for her husband and was found to have asymptomatic pulmonary sarcoidosis with bilateral hilar lymphadenopathy [75]. Work-up including biopsies of the lymph nodes demonstrated non-caseating granulomas consistent with sarcoidosis [75]. There was no renal involvement, nor respiratory limitations [75]. She and her husband proceeded with organ donation and there was no evidence of sarcoidosis in either the donor or recipient kidney in the 15-month follow-up [75]. Recipients with preexisting sarcoidosis do have a risk of developing recurrent sarcoidosis in the donated organ [76,77,78]. Patients affected by sarcoidosis with evidence of disease found at the time of organ procurement are generally not considered appropriate for organ donation.
Given the association between silica dust exposure and sarcoidosis risk, the rising cases of silicosis and silica dust exposure due to increasing use of engineered quartz, and younger individuals with asymptomatic silica dust exposure at the time of organ procurement may lead like this case to more diagnoses of “sarcoidosis”. With sarcoidosis generally not suitable for organ donation, fewer organs will be available from this group. Recent reviews and case series have now also implicated development of autoimmune conditions associated with silica exposure, including vasculitis and scleroderma [79,80,81].
This case highlights a rare phenomenon of seeing grossly abnormal pathology during organ procurement with no obvious evidence of disease during donor suitability evaluation. Silicosis is primarily a lung disease brought on by lysosomal damage that activates the NALP3 inflammasome and triggers an inflammatory cascade [62]. It forms chronically silicate nodules with concentric fibrosis surrounded by dust-laden microphages [62]. Rarely, silicosis has been seen causing constrictive pericarditis, myocardial involvement with ventricular tachycardia and increased heart disease mortality [82,83,84]. Increased prevalence of chronic kidney disease including nephropathy by some investigators [85,86,87] but not all have confirmed this finding [88]. Case reports and case series have also suggested liver function abnormalities with silicosis [89]. Transplantation of non-pulmonary organs seems reasonable on a case-by-case basis after evaluation.
A detailed exposure history may identify affected individuals who would otherwise be deemed a suitable candidate for organ donation prior to organ procurement, as was the case with this particular individual. Given the diagnostic uncertainty in this individual, and by the many small nodules, which can be seen as sarcoidosis, none of this individual’s organs were considered suitable for transplant. However, if gross pathology did not demonstrate abnormalities, presumably the kidneys may have been donated. At this time, there is no evidence to deviate from standard organ donation evaluation based solely on occupational lung exposure. There is no current ethical concern for pursuing organ suitability evaluation or transplantation in asymptomatic individuals with an exposure history of silica dust alone. Due to the time-limited nature of organ procurement, decisions must be made at the discretion of the procuring surgeon in conjunction with the transplant team. New phases of ex-vivo organ perfusion (EVLP), particularly of the lung, liver, and heart may allow for further advanced histopathological analyses to be performed in the future [90]. Preventing future complications on the recipient side from undiagnosed and asymptomatic silicosis or sarcoidosis remains an important aspect of organ transplantation. In the at-risk individual, EVLP may allow the transplant team more time to decide organ suitability as detailed histopathological analyses return, allowing more informed decisions regarding establishing silicosis and sarcoidosis and ruling in silica dust exposed donors with no evidence of disease in various organs, or ruling out subclinical disease associated with silica dust exposure.
6. Conclusions
The pathophysiology of sarcoidosis is a complex interplay between the inciting antigen and a genetically susceptible host. Both specific antigens and genes are poorly understood and incredibly diverse. Silica dust, which is currently on the rise due to the popularity of engineered stone or quartz, appears able to cause both silica dust related silicosis and likely sarcoidosis. Given the previous associations between silica exposure and sarcoidosis, transplant physician awareness is required. Advancements in ex-vivo organ perfusion have the potential to allow critical time for additional investigation of silica dust exposure that was asymptomatic and radiographically silent but were visually and histopathologically present disease in order to improve lung transplant outcomes. Though transplant medicine is evolving to meet increasing clinical indications for the treatment of end-stage organ diseases, there is not enough current evidence or advancements in the quandary of silicosis and asymptomatic sarcoidosis to recommend changing the standard of care for transplanting lungs with these findings.
Funding
This work was supported by an NHLBI funded T32 post-doctoral fellowship (HL007013) to KA.
Authorship
Participated in study design: Aribindi, Harper, and Albertson. Participated in writing paper: Aribindi, Kelly, Coley, Harper, and Albertson. Participated in literature and data analysis: Aribindi, Kelly, Coley, Harper, and Albertson. Disclosure: The authors have no potential conflicts of interest to declare.
Informed Consent Statement
Written informed consent has been obtained from the patient’s family to publish this paper.
Conflicts of Interest
Burnett Kelly is the Surgical Director of Sierra Donor Services, Treasurer of the Society of Pediatric Liver Transplantation, Chair of the Investment and Finance Committee – American Society of Transplantation.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Abbreviation Page:
mm Hg = millimeters of mercury
GMS = Grocotl-Gömöri’s methenamine silver-stain
H&E = hematoxylin and eosin
IL-17 = interlenkin-17
HLA = human leukocyte antigen
BTNZ = butyrophilin-like-z gene
ANXA11 = annexin A11 genes
Th1 = T helper 1 cell, a type of CD4 T cells
MMP-12 = macrophage metalloelastase or macrophage elastase-12
ADAMDEC1 = ADAM-like Decysine-1-a protein belonging to the disintegrin and metalloproteinase family
CD = cluster differentiation of cytotoxic T cells
ADAM = A Disintegrin and Metalloprotease protein/family of enzymes
CI = confidence interval
OR = odds ratio
RR = relative risk
OSHA = Occupational Safety and Health Administration
NIOSH = National Institute of Occupational Safety and Health
References
- Grunewald J: Grutters JC, Arkema EV, et al. Sarcoidosis. Nat Rev Dis Primers. 2019;5(1):45.
- Lin NW, Maier LA. Occupational exposures and sarcoidosis: current understanding and knowledge gaps. Curr Opin Pulm Med. 2022;28(2):144-51. [CrossRef]
- Fazio JC, Gandhi SA, Flattery J, et al. Silicosis Among Immigrant Engineered Stone (Quartz) Countertop Fabrication Workers in California. JAMA Intern Med. 2023;183(9):991-8.
- Kramer MR, Blanc PD, Fireman E, et al. Artificial stone silicosis [corrected]: disease resurgence among artificial stone workers. Chest. 2012;142(2):419-24.
- Oliver LC, Sampara P, Pearson D, et al. Sarcoidosis in Northern Ontario hard-rock miners: A case series. Am J Ind Med. 2022;65(4):268-80. [CrossRef]
- Quero A, Urrutia C, Martinez C, et al. [Silicosis and sarcoid pulmonary granulomas, silicosarcoidosis?]. Med Clin (Barc). 2002;118(2):79.
- Arkema EV, Grunewald J, Kullberg S, et al. Sarcoidosis incidence and prevalence: a nationwide register-based assessment in Sweden. Eur Respir J. 2016;48(6):1690-9.
- Arkema EV, Cozier YC. Sarcoidosis epidemiology: recent estimates of incidence, prevalence and risk factors. Curr Opin Pulm Med. 2020;26(5):527-34.
- Baughman RP, Field S, Costabel U, et al. Sarcoidosis in America. Analysis Based on Health Care Use. Ann Am Thorac Soc. 2016;13(8):1244-52.
- Brito-Zerón P, Kostov B, Superville D, et al. Geoepidemiological big data approach to sarcoidosis: geographical and ethnic determinants. Clin Exp Rheumatol. 2019;37(6):1052-64.
- Fidler LM, Balter M, Fisher JH, et al. Epidemiology and health outcomes of sarcoidosis in a universal healthcare population: a cohort study. Eur Respir J. 2019;54(4). [CrossRef]
- Hena KM. Sarcoidosis Epidemiology: Race Matters. Front Immunol. 2020;11:537382.
- Rybicki BA, Major M, Popovich J, et al. Racial differences in sarcoidosis incidence: a 5-year study in a health maintenance organization. Am J Epidemiol. 1997;145(3):234-41. [CrossRef]
- Drent M, Crouser ED, Grunewald J. Challenges of Sarcoidosis and Its Management. New England Journal of Medicine. 2021;385(11):1018-32.
- Rybicki BA, Iannuzzi MC, Frederick MM, et al. Familial aggregation of sarcoidosis. A case-control etiologic study of sarcoidosis (ACCESS). Am J Respir Crit Care Med. 2001;164(11):2085-91.
- Rossides M, Grunewald J, Eklund A, et al. Familial aggregation and heritability of sarcoidosis: a Swedish nested case-control study. Eur Respir J. 2018;52(2).
- Sverrild A, Backer V, Kyvik KO, et al. Heredity in sarcoidosis: a registry-based twin study. Thorax. 2008;63(10):894-6.
- Rivera NV, Ronninger M, Shchetynsky K, et al. High-Density Genetic Mapping Identifies New Susceptibility Variants in Sarcoidosis Phenotypes and Shows Genomic-driven Phenotypic Differences. Am J Respir Crit Care Med. 2016;193(9):1008-22.
- Rossman MD, Thompson B, Frederick M, et al. HLA-DRB1*1101: a significant risk factor for sarcoidosis in blacks and whites. Am J Hum Genet. 2003;73(4):720-35.
- Schurmann M, Reichel P, Muller-Myhsok B, et al. Results from a genome-wide search for predisposing genes in sarcoidosis. Am J Respir Crit Care Med. 2001;164(5):840-6.
- Berlin M, Fogdell-Hahn A, Olerup O, et al. HLA-DR predicts the prognosis in Scandinavian patients with pulmonary sarcoidosis. Am J Respir Crit Care Med. 1997;156(5):1601-5. [CrossRef]
- Fischer A, Nothnagel M, Schurmann M, et al. A genome-wide linkage analysis in 181 German sarcoidosis families using clustered biallelic markers. Chest. 2010;138(1):151-7. [CrossRef]
- Fischer A, Rybicki BA. Granuloma genes in sarcoidosis: what is new? Curr Opin Pulm Med. 2015;21(5):510-6.
- Fischer A, Schmid B, Ellinghaus D, et al. A novel sarcoidosis risk locus for Europeans on chromosome 11q13.1. Am J Respir Crit Care Med. 2012;186(9):877-85.
- Hofmann S, Fischer A, Nothnagel M, et al. Genome-wide association analysis reveals 12q13.3-q14.1 as new risk locus for sarcoidosis. Eur Respir J. 2013;41(4):888-900. [CrossRef]
- Hofmann S, Franke A, Fischer A, et al. Genome-wide association study identifies ANXA11 as a new susceptibility locus for sarcoidosis. Nat Genet. 2008;40(9):1103-6. [CrossRef]
- Martinetti M, Tinelli C, Kolek V, et al. "The sarcoidosis map": a joint survey of clinical and immunogenetic findings in two European countries. Am J Respir Crit Care Med. 1995;152(2):557-64.
- Valentonyte R, Hampe J, Huse K, et al. Sarcoidosis is associated with a truncating splice site mutation in BTNL2. Nat Genet. 2005;37(4):357-64.
- Crouser ED, Culver DA, Knox KS, Julian MW, Shao G, Abraham S, et al. Gene expression profiling identifies MMP-12 and ADAMDEC1 as potential pathogenic mediators of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2009;179(10):929-38. [CrossRef]
- Lockstone HE, Sanderson S, Kulakova N, et al. Gene set analysis of lung samples provides insight into pathogenesis of progressive, fibrotic pulmonary sarcoidosis. Am J Respir Crit Care Med. 2010;181(12):1367-75.
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020;201(8):e26-e51.
- Grunewald J, Eklund A. Sex-specific manifestations of Lofgren's syndrome. Am J Respir Crit Care Med. 2007;175(1):40-4. [CrossRef]
- Poate TW, Sharma R, Moutasim KA, et al. Orofacial presentations of sarcoidosis--a case series and review of the literature. Br Dent J. 2008;205(8):437-42.
- Rosen Y. Four decades of necrotizing sarcoid granulomatosis: what do we know now? Arch Pathol Lab Med. 2015;139(2):252-62. [CrossRef]
- Spiteri MA, Matthey F, Gordon T, et al. Lupus pernio: a clinico-radiological study of thirty-five cases. Br J Dermatol. 1985;112(3):315-22.
- Binesh F, Halvani H, Navabii H. Systemic sarcoidosis with caseating granuloma. BMJ Case Rep. 2012;2012.
- Ma Y, Gal A, Koss MN. The pathology of pulmonary sarcoidosis: update. Semin Diagn Pathol. 2007;24(3):150-61.
- Rossi G, Cavazza A, Colby TV. Pathology of Sarcoidosis. Clin Rev Allergy Immunol. 2015;49(1):36-44.
- Soler P, Basset F. Morphology and distribution of the cells of a sarcoid granuloma: ultrastructural study of serial sections. Ann N Y Acad Sci. 1976;278:147-60. [CrossRef]
- Mukhopadhyay S, Wilcox BE, Myers JL, et al. Pulmonary necrotizing granulomas of unknown cause: clinical and pathologic analysis of 131 patients with completely resected nodules. Chest. 2013;144(3):813-24.
- Buk SJ. Simultaneous demonstration of connective tissue elastica and fibrin by a combined Verhoeff's elastic-Martius-scarlet-blue trichrome stain. Stain Technol. 1984;59(1):1-5.
- Sakthivel P, Bruder D. Mechanism of granuloma formation in sarcoidosis. Curr Opin Hematol. 2017;24(1):59-65. [CrossRef]
- Silva E, Souchelnytskyi S, Kasuga K, et al. Quantitative intact proteomics investigations of alveolar macrophages in sarcoidosis. Eur Respir J. 2013;41(6):1331-9.
- Green BN, Johnson CD, Adams A. Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. J Chiropr Med. 2006;5(3):101-17.
- Huntley CC, Patel K, Mughal AZ, et al. Airborne occupational exposures associated with pulmonary sarcoidosis: a systematic review and meta-analysis. Occup Environ Med. 2023;80(10):580-9.
- Newman LS, Rose CS, Bresnitz EA, et al. A case control etiologic study of sarcoidosis: environmental and occupational risk factors. Am J Respir Crit Care Med. 2004;170(12):1324-30.
- Kucera GP, Rybicki BA, Kirkey KL, et al. Occupational risk factors for sarcoidosis in African-American siblings. Chest. 2003;123(5):1527-35.
- Beijer E, Meek B, Kromhout H, et al. Sarcoidosis in a patient clinically diagnosed with silicosis; is silica associated sarcoidosis a new phenotype? Respir Med Case Rep. 2019;28:100906. [CrossRef]
- Kawano-Dourado LB, Carvalho CR, Santos UP, Canzian M, Coletta et al. Tunnel excavation triggering pulmonary sarcoidosis. Am J Ind Med. 2012;55(4):390-4.
- Ronsmans S, Verbeken EK, Adams E, et al. Granulomatous lung disease in two workers making light bulbs. Am J Ind Med. 2019;62(10):908-13.
- Uzmezoglu B, Simsek C, Gulgosteren S, et al. Sarcoidosis in iron-steel industry: mini case series. Sarcoidosis Vasc Diffuse Lung Dis. 2017;34(4):365-72.
- Mochizuka Y, Kono M, Katsumata M, et al. Sarcoid-like Granulomatous Lung Disease with Subacute Progression in Silicosis. Intern Med. 2022;61(3):395-400. [CrossRef]
- Carreno Hernandez MC, Garrido Paniagua S, Colomes Iess M, et al. Accelerated silicosis with bone marrow, hepatic and splenic involvement in a patient with lung transplantation. BMJ Case Rep. 2019;12(12).
- Vihlborg P, Bryngelsson IL, Andersson L, et al. Risk of sarcoidosis and seropositive rheumatoid arthritis from occupational silica exposure in Swedish iron foundries: a retrospective cohort study. BMJ Open. 2017;7(7):e016839.
- Graff P, Larsson J, Bryngelsson IL, et al. Sarcoidosis and silica dust exposure among men in Sweden: a case-control study. BMJ Open. 2020;10(9):e038926.
- Jonsson E, Jarvholm B, Andersson M. Silica dust and sarcoidosis in Swedish construction workers. Occup Med (Lond). 2019;69(7):482-6.
- Nathan N, Montagne ME, Macchi O, et al. Exposure to inorganic particles in paediatric sarcoidosis: the PEDIASARC study. Thorax. 2022;77(4):404-7. [CrossRef]
- Rezai M, Nayebzadeh A, Catli S, et al. Occupational exposures and sarcoidosis: a rapid review of the evidence. Occup Med (Lond). 2024;74(4):266-73.
- Worker Exposure to Silica during Countertop Manufacturing, Finishing and Installation [Available from: https://www.osha.gov/sites/default/files/publications/OSHA3768.pdf.
- Silicosis, mortality, prevention and control—United States, 1968–2002. [Available from: https://www.cdc.gov/mmwr/preview/ mmwrhtml/mm5416a2.htm.
- Barnes H, Goh NSL, Leong TL, et al. Silica-associated lung disease: An old-world exposure in modern industries. Respirology. 2019;24(12):1165-75.
- Leung CC, Yu IT, Chen W. Silicosis. Lancet. 2012;379(9830):2008-18.
- Wu N, Xue C, Yu S, Y et al. Artificial stone-associated silicosis in China: A prospective comparison with natural stone-associated silicosis. Respirology. 2020;25(5):518-24.
- Chaney J, Suzuki Y, Cantu E, 3rd, et al. Lung donor selection criteria. J Thorac Dis. 2014;6(8):1032-8.
- Kotloff RM, Blosser S, Fulda GJ, et al. Management of the Potential Organ Donor in the ICU: Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations Consensus Statement. Crit Care Med. 2015;43(6):1291-325.
- Aigner C, Winkler G, Jaksch P, et al. Extended donor criteria for lung transplantation--a clinical reality. Eur J Cardiothorac Surg. 2005;27(5):757-61. [CrossRef]
- Lardinois D, Banysch M, Korom S, et al. Extended donor lungs: eleven years experience in a consecutive series. Eur J Cardiothorac Surg. 2005;27(5):762-7.
- Mulligan MJ, Sanchez PG, Evans CF, et al. The use of extended criteria donors decreases one-year survival in high-risk lung recipients: A review of the United Network of Organ Sharing Database. J Thorac Cardiovasc Surg. 2016;152(3):891-8 e2.
- Sommer W, Kuhn C, Tudorache I, et al. Extended criteria donor lungs and clinical outcome: results of an alternative allocation algorithm. J Heart Lung Transplant. 2013;32(11):1065-72.
- Whiting D, Banerji A, Ross D, et al. Liberalization of donor criteria in lung transplantation. Am Surg. 2003;69(10):909-12.
- Committee JUKUBTaTTSPA. Sarcoidosis [Available from: https://www.transfusionguidelines.org/dsg/wb/guidelines/sa004-sarcoidosis#:~:text=Must%20not%20donate.&text=Chronic%20Sarcoidosis%20can%20cause%20a,this%20condition%20should%20not%20donate.
- Burke WM, Keogh A, Maloney PJ, et al. Transmission of sarcoidosis via cardiac transplantation. Lancet. 1990;336(8730):1579.
- Heatly T, Sekela M, Berger R. Single lung transplantation involving a donor with documented pulmonary sarcoidosis. J Heart Lung Transplant. 1994;13(4):720-3.
- Padilla ML, Schilero GJ, Teirstein AS. Donor-acquired sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2002;19(1):18-24.
- Kono M, Hasegawa J, Wakai S, et al. Living Kidney Donation From a Donor With Pulmonary Sarcoidosis: A Case Report and Review of the Literature. Transplant Proc. 2017;49(5):1183-6.
- Milman N, Andersen CB, Burton CM, et al. Recurrent sarcoid granulomas in a transplanted lung derive from recipient immune cells. Eur Respir J. 2005;26(3):549-52. [CrossRef]
- Ionescu DN, Hunt JL, Lomago D, et al. Recurrent sarcoidosis in lung transplant allografts: granulomas are of recipient origin. Diagn Mol Pathol. 2005;14(3):140-5.
- Schultz HH, Andersen CB, Steinbruuchel D, et al. Recurrence of sarcoid granulomas in lung transplant recipients is common and does not affect overall survival. Sarcoidosis Vasc Diffuse Lung Dis. 2014;31(2):149-53.
- Churg A, Muller NL. Update on Silicosis. Surg Pathol Clin. 2024;17(2):193-202.
- Tomic D, Hoy RF, Sin J, et al. Autoimmune diseases, autoantibody status and silicosis in a cohort of 1238 workers from the artificial stone benchtop industry. Occup Environ Med. 2024;81(8):388-94. [CrossRef]
- Shtraichman O, Blanc PD, Ollech JE, et al. Outbreak of autoimmune disease in silicosis linked to artificial stone. Occup Med (Lond). 2015;65(6):444-50.
- Liu Y, Rong Y, Steenland K, et al. Long-term exposure to crystalline silica and risk of heart disease mortality. Epidemiology. 2014;25(5):689-96.
- Chakraborty P, Isser HS, Arava SK, et al. Ventricular Tachycardia: A Rare Case of Myocardial Silicosis. JACC Case Rep. 2020;2(14):2256-9.
- Jiang Y, Shao F. A stone miner with both silicosis and constrictive pericarditis: case report and review of the literature. BMC Pulm Med. 2013;13:71. [CrossRef]
- Ghahramani N. Silica nephropathy. Int J Occup Environ Med. 2010;1(3):108-15.
- Millerick-May ML, Schrauben S, Reilly MJ, et al. Silicosis and chronic renal disease. Am J Ind Med. 2015;58(7):730-6.
- Rosenman KD, Moore-Fuller M, Reilly MJ. Kidney disease and silicosis. Nephron. 2000;85(1):14-9.
- Steenland K, Rosenman K, Socie E, et al. Silicosis and end-stage renal disease. Scand J Work Environ Health. 2002;28(6):439-42.
- Zawilla N, Taha F, Ibrahim Y. Liver functions in silica-exposed workers in Egypt: possible role of matrix remodeling and immunological factors. Int J Occup Environ Health. 2014;20(2):146-56. [CrossRef]
- Ahmad K, Pluhacek JL, Brown AW. Ex Vivo Lung Perfusion: A Review of Current and Future Application in Lung Transplantation. Pulm Ther. 2022;8(2):149-65.
Figure 1.
CT of the chest demonstrating A) normal lung parenchyma, B) no significant mediastinal lymphadenopathy, lower lobe atelectasis, C) significant lower lobe atelectasis without lung parenchymal abnormalities in recruited lung.
Figure 1.
CT of the chest demonstrating A) normal lung parenchyma, B) no significant mediastinal lymphadenopathy, lower lobe atelectasis, C) significant lower lobe atelectasis without lung parenchymal abnormalities in recruited lung.
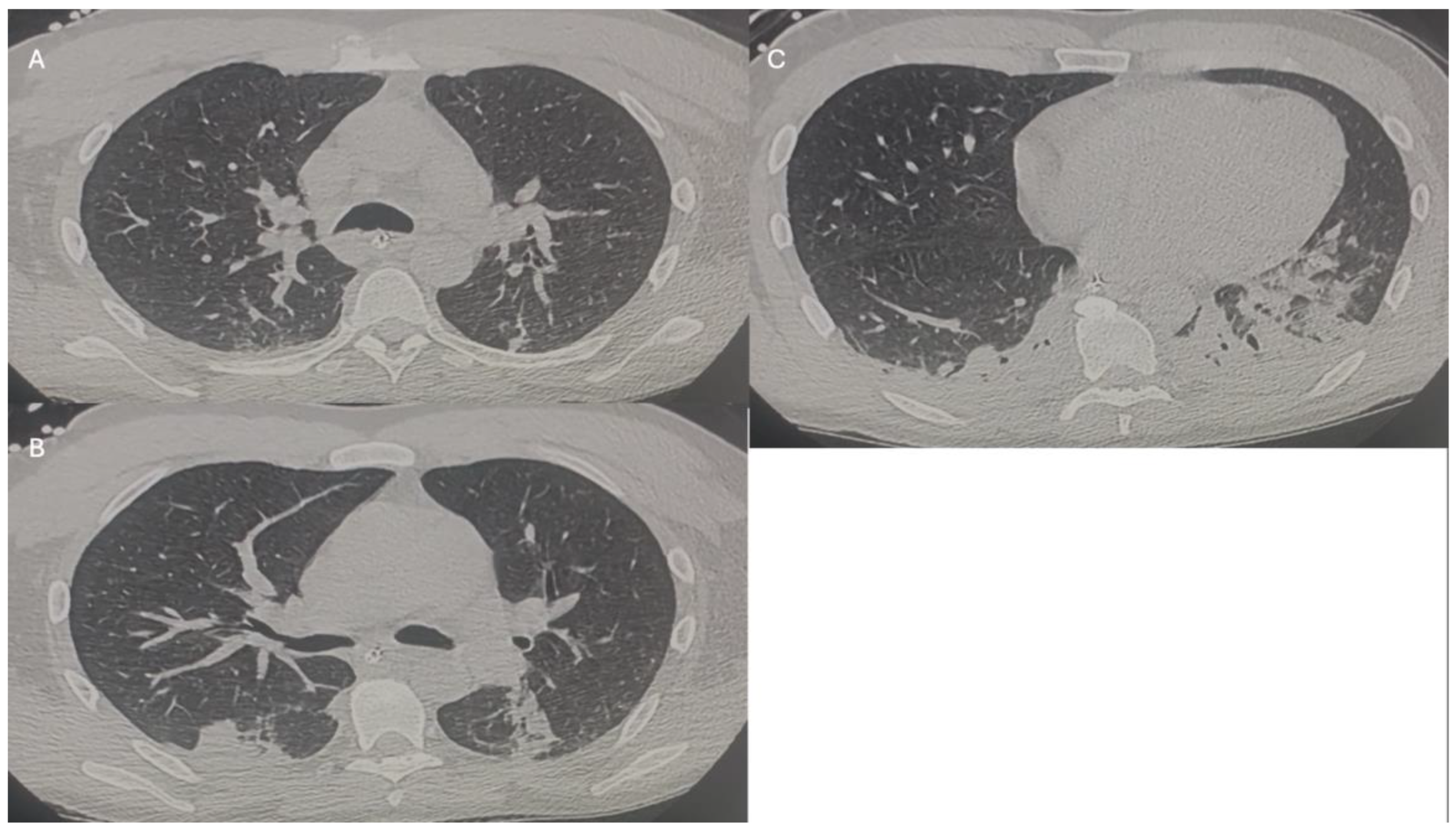
Figure 2.
These images were obtained during organ procurement surgery. A) Thick black arrow demonstrates diffuse small nodules, which were granulomas in a recruited right upper lobe. Thin white line demonstrates small nodules or granulomas in an atelectatic right lower lobe. B) Black box magnifying the granulomas outlining the secondary lobule.
Figure 2.
These images were obtained during organ procurement surgery. A) Thick black arrow demonstrates diffuse small nodules, which were granulomas in a recruited right upper lobe. Thin white line demonstrates small nodules or granulomas in an atelectatic right lower lobe. B) Black box magnifying the granulomas outlining the secondary lobule.
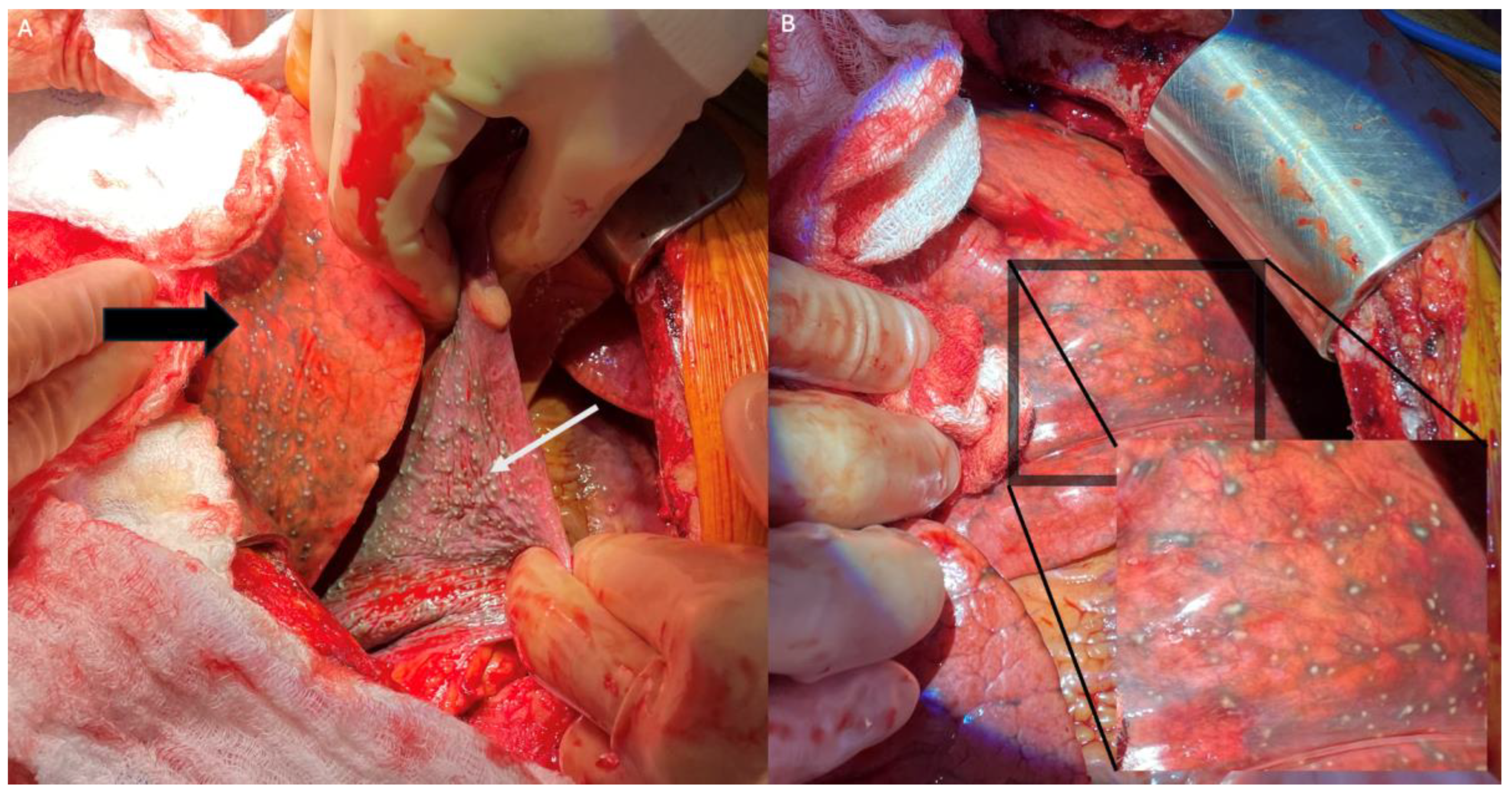
Figure 3.
A) Hematoxylin and eosin (H&E) staining at 2x magnification. B) H&E stain at 10x magnification demonstrating a caseating granuloma found in the patient. There were both caseating and non-caseating granulomas present in this patient. C) Grocott–Gömöri's methenamine silver (GMS) stain demonstrating no fungal organisms. D) Acid-fast bacteria (AFB) stain was negative for mycobacterial organisms.
Figure 3.
A) Hematoxylin and eosin (H&E) staining at 2x magnification. B) H&E stain at 10x magnification demonstrating a caseating granuloma found in the patient. There were both caseating and non-caseating granulomas present in this patient. C) Grocott–Gömöri's methenamine silver (GMS) stain demonstrating no fungal organisms. D) Acid-fast bacteria (AFB) stain was negative for mycobacterial organisms.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



