
Submitted:
03 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Semaglutide, a GLP-1 (glucagon-like peptide-1) receptor agonist, is widely prescribed for weight loss in non-diabetic populations. Given the link between obesity and over-active bladder (OAB), we explored whether GLP-1 use would improve urinary out-comes beyond its weight loss benefit for non-diabetic adults undergoing BOTOX treatment for OAB. Using the TriNetX database, we conducted a retrospective cohort study of non-diabetic OAB patients treated with BOTOX alone or with concurrent GLP-1 therapy. Propensity score matching (1:1) adjusted for age, race, ethnicity, hypertension, and BMI/obesity. After matching, 992 patients were included in each group. GLP-1 use was associated with a lower incidence of urinary retention (8.6% vs. 4.9%, risk difference 3.66%, p = 0.0044) and urinary tract infection (13.3% vs. 8.8%, risk difference 4.54%, p = 0.00224), with corresponding improved one-year retention-free and UTI-free survival on Kaplan Meier (KM) analysis. Antispasmodic initiation rates were similar (11.8% vs. 10.3%, risk difference 1.55%, p = 0.6921), and KM analysis showed no significant difference. These findings suggest that GLP-1 receptor agonist use may improve select urinary outcomes in non-diabetic adults undergoing BOTOX treatment for OAB and support further investigation into its potential adjunctive role in OAB management with longer follow-up.
Keywords:
overactive bladder (OAB)
; GLP-1 receptor agonist
; onabotulinumtoxin A (BOTOX)
; diabetes
; semaglutide
; weight loss
; urinary retention
1. Introduction
Overactive bladder syndrome (OAB) is defined as urinary urgency, often accompanied by urinary frequency and nocturia, with or without incontinence. This urinary urgency can significantly interrupt a patient’s daily activities and sleep, profoundly diminishing their quality of life. The global prevalence of OAB is reported to be nearly 20%, with higher rates among female, elderly, overweight and obese populations [1]. With rates this high, several treatment strategies are offered to help patients manage their symptoms. Treatments vary in intensity, ranging from conservative measures to more advanced options. First-line often includes pelvic floor exercises to strengthen the pelvic floor muscles that suppress urgency, lifestyle therapies to mitigate the worsening effects of smoking and weight, and other less supported but more behavioral complement therapies such as hypnotherapy and acupuncture [2]. Pharmacological options, such as beta-3 adrenergic agonist drugs and anti-muscarinic agents, are common adjuncts to these first-line treatments but may be associated with undesirable side effects, like cognitive impairment. With or without these agents, improvement from more conservative treatment plans may take up to 12 weeks to manifest. Minimally invasive procedures, like percutaneous tibial nerve stimulation or sacral neuromodulation, may substitute or replace medical therapy if not effective [3]. When all else fails and symptoms persist, surgical interventions like augmentation cystoplasty and urinary diversion may provide relief to these refractory patients, albeit with variable results and significant potential for complications.
Within 15 years, onabotulinumtoxinA (BOTOX) has emerged as an option for refractory OAB. BOTOX injections into detrusor muscle are an established treatment for refractory OAB, inhibiting neurotransmitter release and leading to reduced bladder overactivity [4]. Though a promising avenue, whether to include BOTOX in a patient’s OAB treatment regimen, like all other treatment options, must depend on shared decision making between the patient and physician.
Ultimately, the management of overactive bladder, particularly in refractory cases, hinges on this nuanced and collaborative approach between patient and physician. Rather than adhering to a rigid stepwise progression, contemporary guidelines from the American Urological Association (AUA) and the European Association of Urology (EAU) now emphasize multi-dimensional, individualized care, recognizing that what works best clinically must also be acceptable and sustainable for the patient [5,6]. As such, the path to optimal symptom control is not a single trajectory but a dynamic, patient-centered dialogue that honors both medical expertise and lived experience. Factors to consider when planning treatment include a patient’s ability to perform intermittent catheterization for BOTOX, their tolerance for minor surgery and implantation, their ability to commit to frequent visits, and general preferences and goals.
Despite all the possible avenues available for treatment, there are still significant limitations. Though effective, BOTOX is associated with an increased risk of elevated post-void residual volume and urinary tract infection [7,8,9]. When compared against neuromodulation treatments like sacral nerve neuromodulation and percutaneous tibial nerve stimulation in a meta-analysis, BOTOX was still associated with more complications of urinary retention and UTI [10]. Thus, these adverse effects can necessitate intermittent catheterization for patients and may diminish the overall benefits of the treatment [11]. Especially for those populations who are at higher risk for UTIs like elderly and obese patients, BOTOX injection benefits may not outweigh the potential complications [12,13].
The association between being overweight and OAB severity is well-documented [14,15,16]. Though the pathophysiology is not yet fully understood, many proposed mechanisms have been investigated. One mechanism describes how larger waist circumference, and BMI may cause excess abdominal pressure, elevating bladder pressure and urethral mobility, further exacerbating OAB [17]. Another proposed mechanism ascribes the weakened pelvic floor brought about by obesity as the culprit [18]. Additionally, weight loss has been shown to reduce the severity of OAB symptoms, supporting obesity’s role as a modifiable risk factor in its pathogenesis [19].
GLP-1 receptor agonists (e.g, semaglutide, liraglutide) (GLP-1 RA) were first approved by the FDA in 2005 for the treatment of Type 2 Diabetes but have only recently revolutionized the market as a weight loss drug for the non-diabetic patient. Importantly, GLP-1 RA have shown to significantly reduce weight with an acceptable safety for obese or overweight patients without diabetes [19]. By mimicking the effects of endogenous GLP-1, these drugs stimulate insulin release from the pancreas, regulate appetite and satiety in the brain, and slow down gastric emptying [20].
With this in mind, we wanted to explore if the benefits of GLP-1 RA reach beyond simply weight loss. In diabetic patients, these drugs have shown to reduce albuminuria in chronic kidney disease, reduce all-cause mortality in cardiovascular disease, reduce blood pressure and dyslipidemia, and decrease metabolic complications in PCOS [21]. In non-diabetic patients, there is less direct, though intriguing support for its renoprotective, cardiovascular, and fertility effects [21,22,23,24]. Other research highlights a potential anti-inflammatory effect, reducing circulating inflammatory cytokines like TNF-a and IL-6, and highly sensitive C-reactive protein, in both mice and human models [25,26,27,28]. As inflammation, autonomic tone, and detrusor overactivity all contribute to OAB, we speculate that GLP-1 RA could additionally influence bladder function.
So far, no studies have evaluated urinary outcomes of GLP-1 RAin non-diabetic OAB patients on BOTOX. This retrospective cohort study aims to explore the potential impact of GLP-1 receptor agonist use on urinary outcomes in non-diabetic patients with refractory OAB undergoing onabotulinumtoxinA treatment, addressing a critical gap in the current literature. Using the TriNetX database, we conduct a large-scale analysis highlighting any discrepancies in outcomes between GLP-1 RA users and control cohorts.
We hypothesized that GLP-1 RA are associated with improved urinary outcomes in non-diabetic female patients with OAB receiving BOTOX beyond weight loss benefits. Primary outcomes evaluated incidence of urinary tract infection (UTI), urinary retention, and urinary antispasmodic use following BOTOX treatment.
2. Results
A total of 19,907 OAB patients who received BOTOX alone and 992 OAB patients who received both BOTOX and a GLP-1 receptor agonist (GLP-1 RA) were identified before matching. After 1:1 propensity score matching, 992 matched pairs were included for analysis.
The median follow-up duration was 365 days for the BOTOX-only cohort (IQR: 77.5 days) and 365 days for the combination cohort receiving BOTOX plus a GLP-1 receptor agonist (IQR: 163.5 days). The mean age was nearly identical (59.3 vs. 59.4 years; SMD = 0.011; p = 0.8073), and the proportion of female patients was also similar (92.0% vs. 91.1%; SMD = 0.033; p = 0.4668). The prevalence of cystitis was marginally higher in the GLP-1 group (30.1% vs. 34.2%; SMD = 0.086; p = 0.0545), though this did not reach statistical significance. (Table 1)
Medication utilization after matching revealed higher use of antimicrobials in the GLP-1 group (93.5% vs. 98.4%; SMD = 0.248; p < 0.0001), as well as increased use of antiemetics (75.1% vs. 83.9%; SMD = 0.219; p < 0.0001) and laxatives (68.5% vs. 74.6%; SMD = 0.134 ; p = 0.0028).
2.1. Urinary Retention
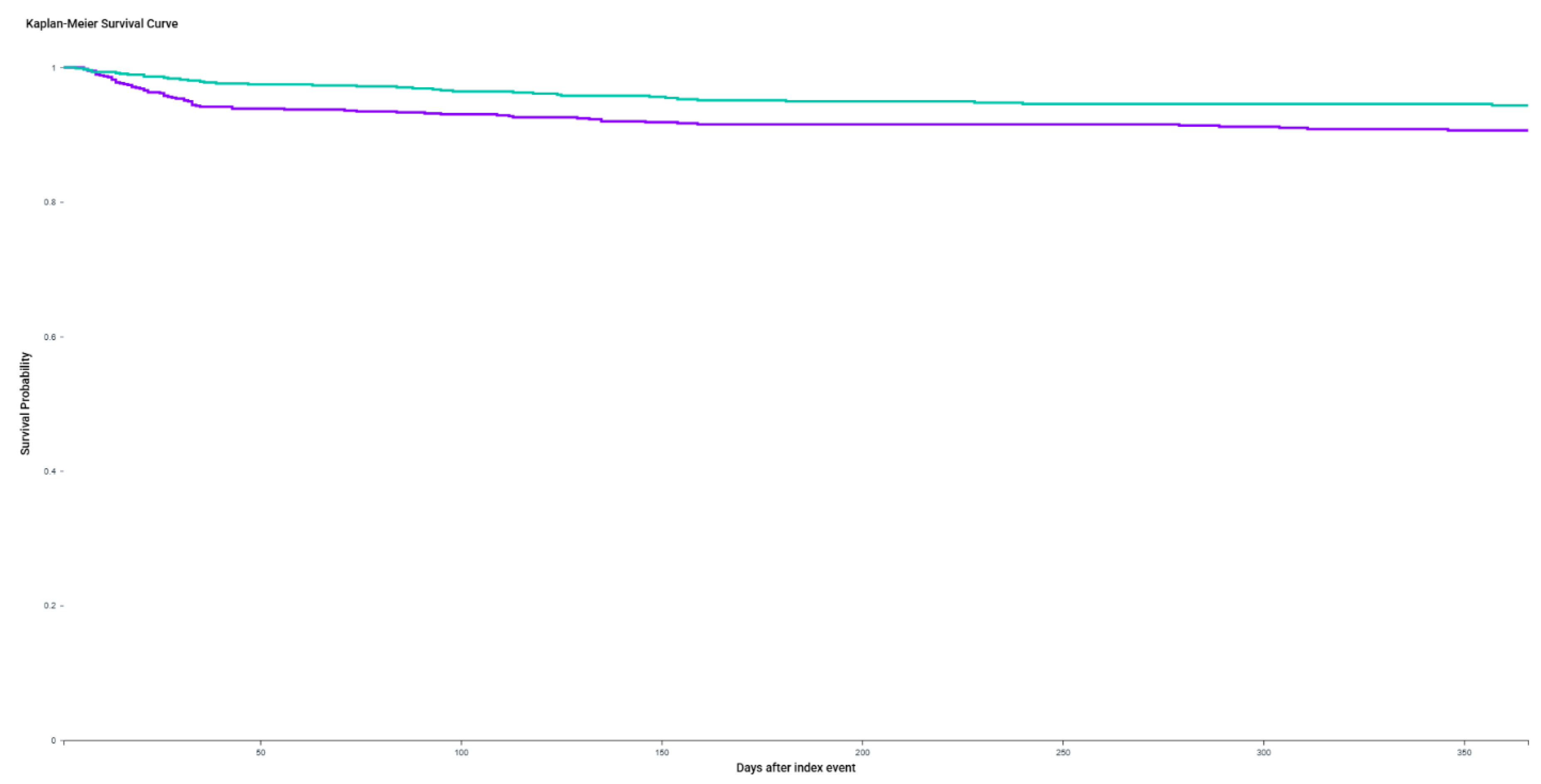
For urinary retention outcomes, 212 patients in the BOTOX-only cohort and 241 patients in the BOTOX + GLP-1 RA group were excluded due to a documented history of urinary retention prior to the index event. Among the remaining patients, retention occurred in 67 of 780 patients (8.59%) in the BOTOX-only cohort, compared to 37 of 751 patients (4.93%) in the combination cohort. This translated to an absolute risk difference of 3.66% (95% CI: 1.16%–6.17%; p = 0.0044).
Kaplan-Meier (KM) analysis, excluding patients with pre-existing retention, demonstrated significantly improved retention-free survival in the GLP-1 RA combination group (log-rank p = 0.0064). The estimated hazard ratio for retention was 1.74 (95% CI: 1.16–2.59), indicating a significantly higher risk of urinary retention in the BOTOX-only group over the one-year follow-up period.
Figure 1.
Kaplan-Meier curves for urinary retention-free survival over one year following BOTOX injection, with or without concurrent GLP-1 receptor agonist therapy. Patients treated with combination therapy (OAB + BOTOX + GLP-1 agonist) had significantly higher retention-free survival compared to those receiving BOTOX alone (log-rank p = 0.0064). At one year, the retention-free survival probability was 94.3% in the combination group versus 90.6% in the BOTOX-only group. The hazard ratio for urinary retention in the BOTOX-only group was 1.74 (95% CI: 1.16–2.59), indicating a 74% increased risk relative to combination therapy.
Figure 1.
Kaplan-Meier curves for urinary retention-free survival over one year following BOTOX injection, with or without concurrent GLP-1 receptor agonist therapy. Patients treated with combination therapy (OAB + BOTOX + GLP-1 agonist) had significantly higher retention-free survival compared to those receiving BOTOX alone (log-rank p = 0.0064). At one year, the retention-free survival probability was 94.3% in the combination group versus 90.6% in the BOTOX-only group. The hazard ratio for urinary retention in the BOTOX-only group was 1.74 (95% CI: 1.16–2.59), indicating a 74% increased risk relative to combination therapy.
2.2. Urinary Tract Infection
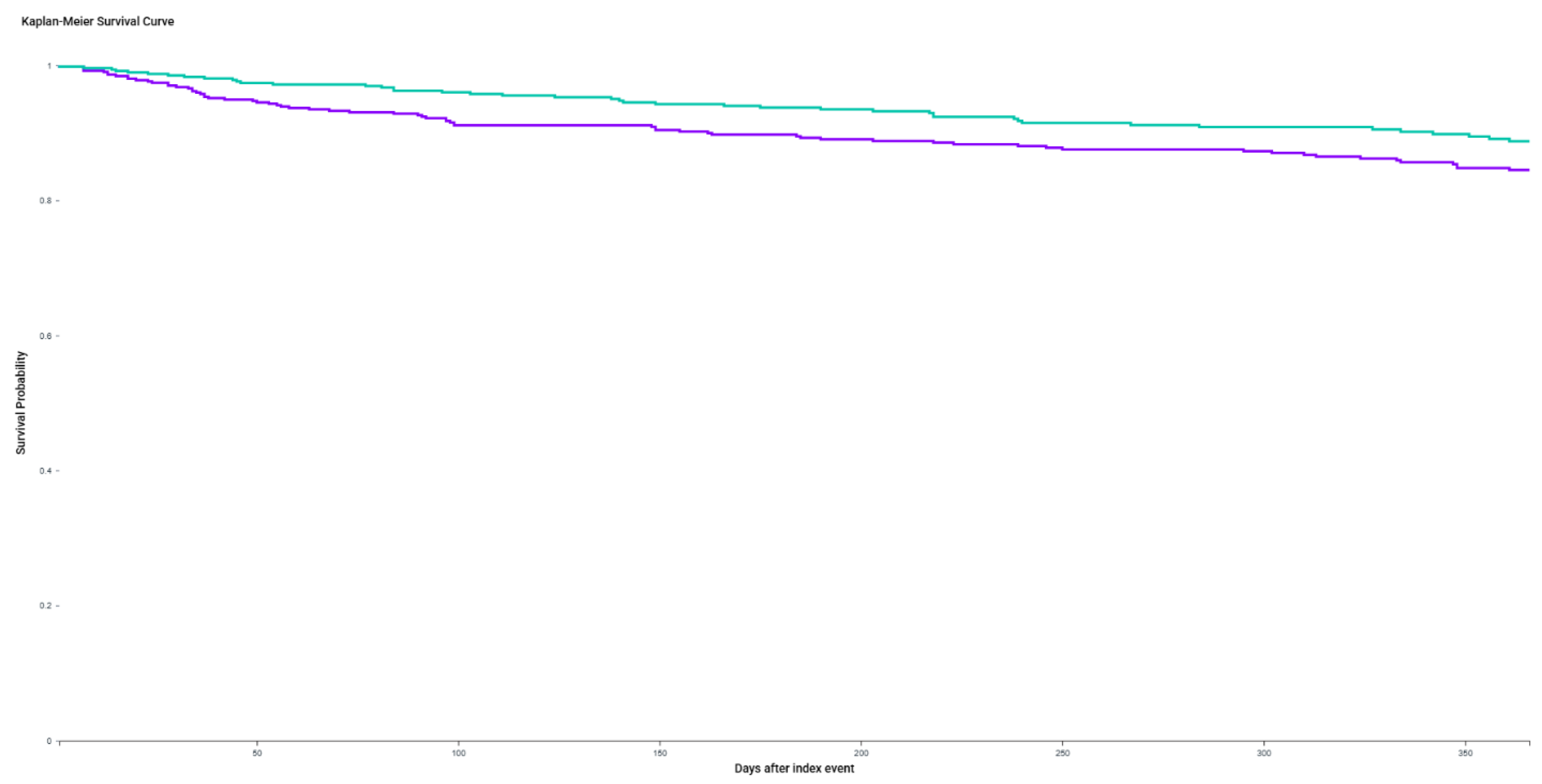
For urinary tract infection (UTI) outcomes, 475 patients in the BOTOX-only cohort and 504 in the BOTOX + GLP-1 RA cohort were excluded due to a documented history of UTI prior to the index date. Among the remaining patients, 69 of 517 (13.3%) in the BOTOX-only group developed a new UTI, compared to 43 of 488 (8.8%) in the GLP-1 combination group. This yielded a risk difference of 4.54% (95% CI: 0.67%–8.40%).
KM analysis over one year demonstrated a higher UTI-free survival probability in the GLP-1 RA combination group (88.7%) compared to the BOTOX-only group (84.5%), with a statistically significant log-rank test (χ² = 4.136, p = 0.0420).
Figure 2.
Kaplan-Meier curves for urinary tract infection (UTI)-free survival over one year following BOTOX injection, with or without concurrent GLP-1 receptor agonist therapy. Patients receiving combination therapy (OAB + BOTOX + GLP-1 RA) demonstrated significantly higher UTI-free survival compared to those receiving BOTOX alone (log-rank p = 0.042). At one year, survival probability was 88.7% in the combination group versus 84.5% in the BOTOX-only group. The hazard ratio for UTI in the BOTOX-only group was 1.48 (95% CI: 1.01–2.17), indicating a 48% increased risk relative to combination therapy.
Figure 2.
Kaplan-Meier curves for urinary tract infection (UTI)-free survival over one year following BOTOX injection, with or without concurrent GLP-1 receptor agonist therapy. Patients receiving combination therapy (OAB + BOTOX + GLP-1 RA) demonstrated significantly higher UTI-free survival compared to those receiving BOTOX alone (log-rank p = 0.042). At one year, survival probability was 88.7% in the combination group versus 84.5% in the BOTOX-only group. The hazard ratio for UTI in the BOTOX-only group was 1.48 (95% CI: 1.01–2.17), indicating a 48% increased risk relative to combination therapy.
2.3. Urinary Antispasmodic Use
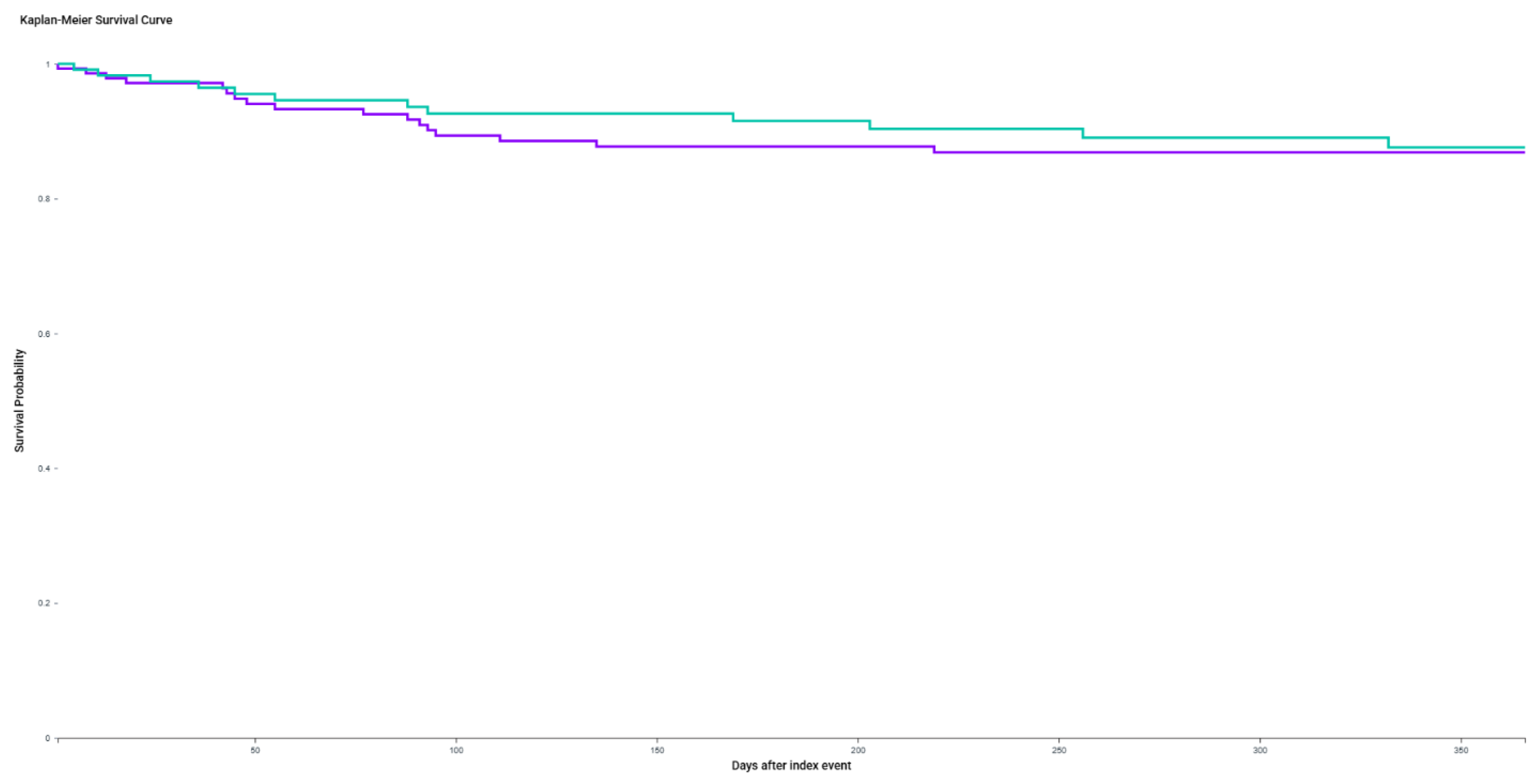
For urinary antispasmodic use, 848 patients in the BOTOX-only cohort and 875 in the GLP-1 combination cohort were excluded due to a history of prior antispasmodic use. Among the remaining patients, 17 of 144 (11.8%) in the BOTOX-only antispasmodics post-treatment, compared to 12 of 117 (10.3%) in the GLP-1 group. This yielded a risk difference of 1.55% (95% CI: -6.07% to 9.17%).
KM survival analysis demonstrated no significant difference in antispasmodic-free survival between cohorts over the three-year follow-up (log-rank p = 0.7234; HR 1.14, 95% CI: 0.55–2.39; p = 0.3984).
Figure 3.
Kaplan-Meier curve for urinary antispasmodic-free survival among patients receiving BOTOX only versus BOTOX + GLP-1 receptor agonist therapy. After excluding patients with prior antispasmodic use (n=848 in the BOTOX-only cohort and n=875 in the combination cohort), 144 BOTOX-only patients and 117 BOTOX + GLP-1 patients remained for analysis. The 1-year antispasmodic-free survival probability was 86.85% in the BOTOX-only cohort and 87.59% in the combination cohort. No significant difference was observed between groups (log-rank p = 0.7234). The hazard ratio was 1.14 (95% CI: 0.55–2.39; p = 0.3984).
Figure 3.
Kaplan-Meier curve for urinary antispasmodic-free survival among patients receiving BOTOX only versus BOTOX + GLP-1 receptor agonist therapy. After excluding patients with prior antispasmodic use (n=848 in the BOTOX-only cohort and n=875 in the combination cohort), 144 BOTOX-only patients and 117 BOTOX + GLP-1 patients remained for analysis. The 1-year antispasmodic-free survival probability was 86.85% in the BOTOX-only cohort and 87.59% in the combination cohort. No significant difference was observed between groups (log-rank p = 0.7234). The hazard ratio was 1.14 (95% CI: 0.55–2.39; p = 0.3984).
3. Discussion
Using a federated global claims database, we found that GLP-1 RA use, including semaglutide, was associated with clinical benefit in non-diabetic women receiving BOTOX for OAB. After 1:1 propensity matching and excluding patients with pre-existing diagnoses, GLP-1 RA use was linked to significantly lower incidence of urinary retention and UTIs (Table 2). Specifically, the risk of urinary retention was nearly halved in the GLP-1 RA cohort (4.9% vs. 8.6%; p = 0.0044). KM analysis also showed significantly improved retention-free survival (log-rank p = 0.0064; HR = 1.74).
Similarly, new-onset UTI rates were lower in the GLP-1 cohort (8.8% vs. 13.3%), This represented a 4.54% absolute risk reduction and better 1-year UTI-free survival (log-rank p = 0.0420). These results suggest a meaningful protective effect of GLP-1 RAs on bladder health outcomes in the OAB population, independent of diabetes status.
In contrast, rates of new antispasmodic medication use did not significantly differ between groups, either in absolute terms (11.8% vs. 10.3%; p = 0.7234) or time-to-event survival analysis (HR = 1.14; 95% CI: 0.55–2.39). This may indicate slower or less effect on symptom severity, or that GLP-1 benefit is more specific to inflammatory or infectious outcomes than to urgency symptoms.
KM survival analysis confirmed superior retention-free survival in the GLP-1 group (log-rank p = 0.0064; HR = 1.74), indicating a 74% increased risk in the BOTOX-only group over one year. These findings are consistent with prior literature suggesting that weight loss and systemic metabolic improvements can positively influence lower urinary tract function, including detrusor overactivity and bladder emptying [29,30,31].
A similar trend was observed for UTIs: 8.8% of the GLP-1 group developed incident infections compared to 13.3% in the BOTOX-only cohort, yielding a 4.54% absolute risk reduction (95% CI: 0.67–8.40%). KM analysis again demonstrated significantly improved UTI-free survival in the GLP-1 group (log-rank p = 0.042; HR = 1.48). Our data add to the ongoing debate over UTI risk linked to GLP-1 use [32,33,34].
To our knowledge, this study is the first to evaluate real-world urinary outcomes in a large non-diabetic OAB population treated with BOTOX and GLP-1 agonists. Recently, only one pilot survey had explored the impact of GLP-1 agonists on OAB symptoms [35]. Sandler et al. showed that respondents with more frequent baseline symptoms were more likely to report symptom improvement with semaglutide, even in the absence of a clear correlation with weight loss. These early insights, although anecdotal and subject to recall bias, align with our findings.
Weight loss itself clearly plays a role in OAB symptom relief. Semaglutide trials show an average 11.85% weight loss vs placebo, underscoring systemic therapeutic potential [36]. Given that obesity increases intra-abdominal pressure and weakens pelvic floor support, GLP-1-induced weight loss would alleviate the pathophysiologic contributors to OAB [37]. The American Urogynecology Society reviewed 43 publications (39 studies; 5 RCTs). They found high certainty evidence that behavioral weight loss yields modest urinary incontinence improvement at 1-2.9 years [29]. In addition to overweight populations, data from diabetic populations (versus simply overweight) show a clearly positive correlation when measuring UTI risk, particularly in women [38,39].
In addition to OAB, GLP-1 receptor agonists have gained interest across a spectrum of urologic conditions including erectile dysfunction, prostate cancer, male fertility, and urolithiasis [40,41,42,43,44,45,46,47,48]. These studies, ranging from retrospective database analyses to prospective surveys and preclinical models, suggest mostly potential benefits with mechanisms often attributed to weight loss, central neural modulation, anti-inflammatory effects, or metabolic improvements.
Beyond weight loss, several studies have linked chronic inflammation to OAB. Elevated C-reactive protein levels have been observed in affected patients correlating with worse OAB symptom scores [49,50,51]. It has been proposed that the loss of protective immunologic factors and increased cellular stress responses lead to heightened peripheral afferent nerve excitability and detrusor overactivity [52]. In support of this, preclinical studies in mouse models suggest that the antioxidant, resveratrol, can mitigate both systemic and bladder-specific oxidative stress, leading to improved bladder function [53]. UTIs, which are more prevalent in overweight individuals, may also contribute to this inflammatory cascade.
An intriguing, proposed mechanism of action for GLP-1 RAs, independent of their effects on obesity and inflammation, is neuromodulation. Studies suggest that, rather than acting primarily through GLP-1-producing neurons in the hindbrain or GLP-1 receptors in the vagus nerve, these drugs mediate weight loss via the arcuate nucleus (ARC) of the hypothalamus [54,55]. The ARC houses key regulators of appetite and metabolism, including pro-opiomelanocortin (POMC), neuropeptide Y (NPY), and agouti-related peptide (AgRP) neurons. Through its influence on the autonomic nervous system, the ARC modulates blood pressure, feeding behavior, glucose homeostasis, and innate immune responses [56]. Given this broad autonomic role, bladder control may also be affected by ARC dysfunction. Concurrently, metabolic syndrome and obesity, both known risk factors of OAB, may stem, in part, from ARC dysfunction. Notably, the extracellular perineuronal net surrounding ARC neurons undergoes remodeling in metabolic dysfunction [57]. Ultimately, if GLP-1 RAs can restore ARC neuronal function, they may offer therapeutic benefits even beyond metabolic regulation, potentially alleviating OAB symptoms.
One of the most common drawbacks to GLP-1 medication is the potential for gastrointestinal side effects [58]. This can be observed in our study with increased use of antiemetics (75.1% vs. 83.9%; SMD = 0.219; p < 0.0001) and laxatives (68.5% vs. 74.6%; SMD = 0.134; p = 0.0028). Activation of GLP1 receptors in the area postrema (AP) of the brain drives nausea/aversion while activation of the same receptors in the nucleus solitary tract plays a role in satiety [59]. Selective NTS targeting could preserve appetite suppression while minimizing nausea pathways.
Practically, these findings may help guide patient selection for BOTOX therapy. By identifying subgroups such as overweight or obese individuals using GLP-1 RAs who demonstrate more favorable risk-benefit profiles, physicians may be more inclined to recommend BOTOX treatment. This study also strengthens the viability of multimodal treatment in obese or overweight OAB patients, highlighting a tailored, more patient-centered approach to refractory disease. Ultimately, this work supports GLP-1 RA usage beyond metabolic indications in select urologic patients, such as those with treatment-resistant OAB, co-existing obesity, or heightened UTI risk.
On a larger scale, the public health implications of improving urinary symptoms are considerable. Urinary incontinence is associated with reduced mobility, impaired strength, and increased cardiovascular tone, all of which affect quality of life and independence, particularly in older women. Moreover, psychosocial burdens such as depression and social withdrawal further compound the clinical significance of OAB. Reducing incontinence-related events could therefore mitigate a spectrum of downstream complications.
This study has several notable strengths. It represents one of the largest real-world analyses to date evaluating BOTOX treatment outcomes in patients with and without GLP-1 RA use, enhancing its generalizability to routine clinical practice. The use of a large geographically diverse dataset, TriNetX, allows for robust comparisons across patient subgroups and care settings. Rigorous adjustment for baseline covariates, including comorbidities and prior medication use, strengthens the internal validity of the findings. By focusing on a non-diabetic population, the study minimizes possible confounding effects of hyperglycemia on urinary outcomes. Furthermore, the inclusion of clinically meaningful outcomes such as urinary retention, UTI incidence, and antispasmodic use provides practical relevance for urologists and other clinicians managing OAB in a rapidly growing population of GLP-1 RA users.
Despite these promising results, barriers to clinical translation remain. GLP-1 therapies are expensive, resource-intensive, and typically require specialist oversight. The growing demand and limited supply further constrain widespread adoption. Adverse effects such as gastrointestinal intolerance may limit their use in some populations.
As a retrospective study, residual confounding is possible despite adjustment. Patient-reported outcomes, such as urgency episodes and symptom severity, were not available, limiting the ability to assess subjective treatment response. Moreover, our dataset did not stratify patients by OAB subtype or symptom severity, which may affect the generalizability of our findings. Additionally, detailed clinical data on BOTOX administration such as dose, injection technique, and bladder capacity were not consistently captured, which may influence both efficacy and adverse event profiles. Finally, the GLP-1 cohort had a relatively shorter duration of follow-up, which may bias KM survival estimates and lead to a gross underestimation of long-term or delayed adverse events in this group.
Future research should pursue randomized controlled trials with extended follow-up to validate our retrospective associations and clarify the role of GLP-1 in personalized OAB management. These studies should incorporate validated symptom scores or bladder diaries to better capture user experience. Studies should also explore how GLP-1 RAs may complement non-pharmacologic therapies such as pelvic floor training or behavioral interventions.
Key questions remain about the neuromodulatory role of GLP-1 RAs. Elucidating these mechanisms may deepen our understanding of bladder neuroendocrine regulation and broaden therapeutic applications. Does ARC dysfunction contribute to OAB independently of metabolic syndrome? Could GLP-1 RAs improve bladder function through direct ARC modulation, beyond metabolic effects? Are observed benefits solely weight-related, or do these agents exert direct neurogenic or anti-inflammatory effects on bladder control? Further clinical studies are warranted.
4. Conclusions
In this large real-world study of non-diabetic patients with overactive bladder, concurrent use of GLP-1 receptor agonists was associated with a significantly lower risk of urinary retention and UTI following intravesical BOTOX treatment. These findings suggest that GLP-1 RAs may confer therapeutic benefits beyond weight loss, potentially through anti-inflammatory, metabolic, or neurogenic mechanisms. As GLP-1 usage continues to expand among overweight and obese populations, our results support its consideration as a promising adjunctive strategy for improving urinary outcomes in select OAB patients. Prospective studies are warranted to validate these associations and further define the role of GLP-1 RAs in the multimodal management of refractory OAB.
5. Materials and Methods
We conducted a retrospective cohort study using the TriNetX Research Network, a federated health research platform that aggregates de-identified electronic health record (EHR) data from participating healthcare organizations worldwide. As of 7/05/2025, the total number of non-diabetic male patients on semaglutide or other GLP-1 RAs across 115/150 healthcare organizations (HCOs) was 184,014 while the number of non-diabetic female patients on semaglutide or other GLP-1 RAs across 118/150 HCOs was 504,514. Patients with overactive bladder (OAB) who received intravesical onabotulinumtoxinA (BOTOX) injections were also identified. We then defined two cohorts for analysis: (1) OAB patients who received BOTOX alone and (2) OAB patients who received BOTOX in conjunction with a GLP-1 RA (semaglutide or equivalent).
Non-diabetic patients with OAB were initially identified using procedural and prescription data to capture BOTOX administration and GLP-1 RA exposure. Patients receiving both therapies within the same treatment period were assigned to the combination cohort. To minimize confounding, we performed 1:1 propensity score matching using a greedy nearest-neighbor algorithm with a caliper width of 0.1 pooled standard deviations. The covariates included in the propensity model were selected based on clinical relevance and potential influence on both treatment assignment and outcomes. These covariates comprised age at index (as a continuous variable), biological sex, race (White [2106-3], Black or African American [2054-5], Asian [2028-9]), and ethnicity (Hispanic or Latino [2135-2] and Not Hispanic or Latino [2186-5]). Additional variables included overweight and obesity status using ICD-10-CM codes E65–E68 and granular body mass index (BMI) categories defined by Z68.27 through Z68.42. We also adjusted for hypertensive comorbidity using ICD-10-CM codes I10–I11A. Covariate balance between treatment groups was assessed using standardized mean differences (SMD), with a threshold of <0.1 considered indicative of adequate balance.
Primary outcomes included incidence of urinary tract infection (UTI), urinary retention, and urinary antispasmodic use following BOTOX treatment. These were defined using the following codes: UTI (ICD-10-CM N39.0; urinary retention (ICD-10-CM R33); antispasmodic use (VA drug class).
For each outcome, absolute risk, risk difference, risk ratio, and odds ratio were calculated with corresponding 95% confidence intervals. Time-to-event data were evaluated using one-year Kaplan-Meier (KM) survival analysis, with survival curves compared using log-rank tests with estimated Hazard ratios (HRs). Proportionality assumptions were verified for all survival models. Median follow-up times were also reported for each matched cohort to assess observation period comparability. Patients with pre-existing diagnoses of the respective outcome prior to the BOTOX/ GLP-1 receptor agonist index date were excluded from each time-to-event analysis.
All analyses were performed within the TriNetX platform, which computes frequencies, summary statistics, covariate balance diagnostics, and outcome models using embedded statistical modules. This study was conducted in accordance with institutional and platform-level policies for research involving de-identified data and was deemed exempt from IRB review.
Funding
This research received no external funding.
Institutional Review Board Statement and Informed Consent Statement
As a federated research network utilizing de-identified data, studies using the TriNetX network do not require institutional review board approval or informed consent
Data Availability Statement
All data used is available on the TriNetX research network, www.trinetex.com
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OAB | Overactive bladder |
| UTI | Urinary Tract Infection |
| GLP-1 RA | Glucagon-Like Peptide-1 Receptor Agonist |
| BOTOX | OnabotulinumtoxinA |
| KM | Kaplan-Meier |
| BMI | Body Mass Index |
| ARC | Arcuate Nucleus |
| AP | Area Postrema |
| NTS | Nucleus Tractus Solitarius |
| POMC | Pro-Opiomelanocortin |
| NPY | Neuropeptide Y |
| AgRP | Agouti-Related Peptide |
| SMD | Standardized Mean Difference |
| HR | Hazard Ratio |
| FDA | U.S. Food and Drug Administration |
| PCOS | Polycystic Ovary Syndrome |
| AUA | American Urological Association |
| EAU | European Association of Urology |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification |
| EHR | Electronic Health Record |
| IRB | Institutional Review Board |
| VA | Veterans Affairs (used in context of drug classes |
| IQR | Interquartile Range |
| CI | Confidence Interval |
| TriNetX | A federated real world data research network/platform |
References
- Zhang L, Cai, Mo L, et al. Global prevalence of overactive bladder: a systematic review and meta-analysis. Int Urogynecol J, 2025. [CrossRef]
- UpToDate. Urgency urinary incontinence/overactive bladder (OAB) in females: Treatment. UpToDate. Updated 2025. Available online: https://www.uptodate.com/contents/urgency-urinary-incontinence-overactive-bladder-oab-in-females-treatment (accessed on 27 June 2025).
- Feloney MP, Stauss K, Leslie SW. Sacral Neuromodulation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK567751/ (accessed on 18 April 2024).
- Orasanu B, Mahajan ST. The use of botulinum toxin for the treatment of overactive bladder syndrome. Indian J Urol. 2013, 29, 2–11. [Google Scholar] [CrossRef]
- Cameron AP, Chung DE, Dielubanza EJ, et al. The AUA/SUFU guideline on the diagnosis and treatment of idiopathic overactive bladder. J Urol. 2024, 212, 11–20. [Google Scholar] [CrossRef]
- EAU Guidelines. In proceedings of the EAU Annual Congress, Madrid 2025. ISBN 978-94-92671-29-5.
- Chen YH, Kuo JH, Huang YT, Lai PC, Ou YC, Lin YC. Evaluating the Efficacy and Safety of Botulinum Toxin in Treating Overactive Bladder in the Elderly: A Meta-Analysis with Trial Sequential Analysis of Randomized Controlled Trials. Toxins 2024, 16, 484. [Google Scholar] [CrossRef]
- Palm KM, Abrams MK, Sears SB, et al. The Response of the Urinary Microbiome to Botox. Int Urogynecol J. 2024, 35, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Nitti V, Haag-Molkenteller C, Kennelly M, Chancellor M, Jenkins B, Schurch B. Treatment of neurogenic detrusor overactivity and overactive bladder with Botox (onabotulinumtoxinA): Development, insights, and impact. Medicine 2023, 102, e32377. [Google Scholar] [CrossRef] [PubMed]
- Lo CW, Wu MY, Yang SS, Jaw FS, Chang SJ. Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis. Toxins 2020, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Hsieh PF, Chiu HC, Chen KC, Chang CH, Chou ECL. Botulinum toxin A for the treatment of overactive bladder. Toxins 2016, 8, 59. [Google Scholar] [CrossRef]
- Semins MJ, Shore AD, Makary MA, Weiner J, Matlaga BR. The impact of obesity on urinary tract infection risk. Urology 2012, 79, 266–269. [Google Scholar] [CrossRef]
- Bausch K, Stangl FP, Prieto J, Bonkat G, Kranz J. Urinary infection management in frail or comorbid older individuals. Eur Urol Focus. 2024, 10, 731–733. [Google Scholar] [CrossRef]
- Hagovska M, Švihra J, Buková A, et al. The Relationship between Overweight and Overactive Bladder Symptoms. Obes Facts. 2020, 13, 297–306. [Google Scholar] [CrossRef]
- Khullar V, Sexton CC, Thompson CL, Milsom I, Bitoun CE, Coyne KS. The relationship between BMI and urinary incontinence subgroups: results from EpiLUTS. Neurourol Urodyn. 2014, 33, 392–399. [Google Scholar] [CrossRef]
- Jing W, Wei C, Huang Y, Fu T, Shen W, Xiao W. Relationship between the weight-adjusted-waist index and urinary incontinence in women: A cross-sectional study of NHANES 2007 to 2020. Medicine 2025, 104, e42996. [Google Scholar] [CrossRef] [PubMed]
- Zhang J, Chen W, Tang Z, et al. The Association between Obesity and Wet Overactive Bladder: Results from 2005 to 2020 National Health and Nutrition Examination Survey. Obes Facts, 11 May 2025. [CrossRef]
- Pomian A, Lisik W, Kosieradzki M, Barcz E. Obesity and Pelvic Floor Disorders: A Review of the Literature. Med Sci Monit. 2016, 22, 1880–1886. [Google Scholar] [CrossRef] [PubMed]
- Fazel N, Masoumi SZ, Haghani S, Rajati F. The effect of weight loss on overactive bladder symptoms in overweight and obese women: a systematic review. Nurs Midwifery Stud. 2024, 13, 77–84. [Google Scholar] [CrossRef]
- Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. Updated February 29, 2024. [Google Scholar] [PubMed]
- Xu D, Nair A, Sigston C, et al. Potential Roles of Glucagon-Like Peptide 1 Receptor Agonists (GLP-1 RAs) in Nondiabetic Populations. Cardiovasc Ther. 2022, 2022, 6820377. [Google Scholar] [CrossRef]
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al; SELECT Trial Investigators Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023, 389, 2221–2232. [Google Scholar] [CrossRef]
- Heerspink HJL, Apperloo E, Davies M, et al. Effects of Semaglutide on Albuminuria and Kidney Function in People With Overweight or Obesity With or Without Type 2 Diabetes: Exploratory Analysis From the STEP 1, 2, and 3 Trials. Diabetes Care. 2023, 46, 801–810. [Google Scholar] [CrossRef]
- Cena H, Chiovato L, Nappi RE. Obesity, Polycystic Ovary Syndrome, and Infertility: A New Avenue for GLP-1 Receptor Agonists. J Clin Endocrinol Metab. 2020, 105, e2695–e2709. [Google Scholar] [CrossRef]
- Jiang Z, Tan J, Yuan Y, Shen J, Chen Y. Semaglutide ameliorates lipopolysaccharide-induced acute lung injury through inhibiting HDAC5-mediated activation of NF-κB signaling pathway. Hum Exp Toxicol. 2022, 41, 9603271221125931. [Google Scholar] [CrossRef]
- Shnaien A, Mohammad A, Hassan E. Neuroprotective Effects of Semaglutide in Endotoxemia Mouse Model. Iran J War Public Health. 2023, 15, 199–205.
- Tan SA, Tan L. liraglutide and semaglutide attenuate inflammatory cytokines interferon-gamma, tumor necrosis factor-alpha, and interleukin-6: possible mechanism of decreasing cardiovascular risk in diabetes mellitus. Journal of the American College of Cardiology 2019, 73, 1866. [Google Scholar] [CrossRef]
- Mosenzon O, Capehorn MS, De Remigis A, Rasmussen S, Weimers P, Rosenstock J. Impact of semaglutide on high-sensitivity C-reactive protein: exploratory patient-level analyses of SUSTAIN and PIONEER randomized clinical trials. Cardiovasc Diabetol. 2022, 21, 172. [Google Scholar] [CrossRef]
- Yazdany T, Jakus-Waldman S, Jeppson PC, et al. American Urogynecologic Society Systematic Review: The Impact of Weight Loss Intervention on Lower Urinary Tract Symptoms and Urinary Incontinence in Overweight and Obese Women. Female Pelvic Med Reconstr Surg. 2020, 26, 16–29. [Google Scholar] [CrossRef]
- Subak LL, Wing R, West DS, et al. Weight loss to treat urinary incontinence in overweight and obese women. N Engl J Med. 2009, 360, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Zacche MM, Giarenis I, Thiagamoorthy G, Robinson D, Cardozo L. Is there an association between aspects of the metabolic syndrome and overactive bladder? A prospective cohort study in women with lower urinary tract symptoms. Eur J Obstet Gynecol Reprod Biol. 2017, 217, 1–5. [Google Scholar] [CrossRef]
- Ljungberg C, Bredahl Kristensen FP, Dalager-Pedersen M, Vandenbroucke-Grauls C, Sørensen HT, Nørgaard M, Thomsen RW. Risk of Urogenital Infections in People With Type 2 Diabetes Initiating SGLT2is Versus GLP-1RAs in Routine Clinical Care: A Danish Cohort Study. Diabetes Care 20 May 2025, 48, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Dave CV, Schneeweiss S, Kim D, Fralick M, Tong A, Patorno E. Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for Severe Urinary Tract Infections: A Population-Based Cohort Study. Ann Intern Med. 2019, 171, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Soogoor AR, Agrawal P, Pupo D, Kohn TP, Du Comb W, Alshak MN. MP45-11 Semaglutide Utilization In Weight Management and its Implications for Urinary Tract Infections and Urolithiasis. Jour. of Urology 2024, 211, e746. [Google Scholar] [CrossRef]
- Sandler MD, Williams AD, Wein A, et al. Effects of Glucagon like Peptide-1 agonists on patients with overactive bladder: A pilot study. Continence Reports 2025, 14, 100083. [Google Scholar] [CrossRef]
- Tan HC, Dampil OA, Marquez MM. Efficacy and Safety of Semaglutide for Weight Loss in Obesity Without Diabetes: A Systematic Review and Meta-Analysis. J ASEAN Fed Endocr Soc. 2022, 37, 65–72. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Doumouchtsis SK, Loganathan J, Pergialiotis V. The role of obesity on urinary incontinence and anal incontinence in women: a review. BJOG. 2022, 129, 162–170. [Google Scholar] [CrossRef]
- Nitzan O, Elias M, Chazan B, Saliba W. Urinary tract infections in patients with type 2 diabetes mellitus: review of prevalence, diagnosis, and management. Diabetes Metab Syndr Obes. 2015, 8, 129–136. [Google Scholar] [CrossRef]
- Ahmed AE, Abdelkarim S, Zenida M, et al. Prevalence and Associated Risk Factors of Urinary Tract Infection among Diabetic Patients: A Cross-Sectional Study. Healthcare 2023, 11, 861. [Google Scholar] [CrossRef]
- Able C, Liao B, Saffati G, et al. Prescribing semaglutide for weight loss in non-diabetic, obese patients is associated with an increased risk of erectile dysfunction: a TriNetX database study. Int J Impot Res. 2025, 37, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Varnum AA, Pozzi E, Deebel NA, et al. Impact of GLP-1 Agonists on Male Reproductive Health-A Narrative Review. Medicina 2023, 60, 50. [Google Scholar] [CrossRef]
- Alhajahjeh A, Al-Faouri R, Bahmad HF, et al. From Diabetes to Oncology: Glucagon-like Peptide-1 (GLP-1) Receptor Agonist's Dual Role in Prostate Cancer. Cancers 2024, 16, 1538. [Google Scholar] [CrossRef]
- Pourabhari Langroudi, A. , Chen, A.L., Basran, S. et al. Male sexual dysfunction associated with GLP-1 receptor agonists: a cross-sectional analysis of FAERS data. Int J Impot Res. [CrossRef]
- Fang A, Frigo DE, Hahn A, et al. GLP-1 Agonist Use Among Men With Localized Prostate Cancer: A Narrative Review and Rationale for Prospective Clinical Trials. Urology 2025, 201, 152–158. [Google Scholar] [CrossRef]
- Salvio G, Ciarloni A, Ambo N, et al. Effects of glucagon-like peptide 1 receptor agonists on testicular dysfunction: A systematic review and meta-analysis. Andrology. [CrossRef]
- Nomiyama T, Kawanami T, Irie S, et al. Exendin-4, a GLP-1 receptor agonist, attenuates prostate cancer growth. Diabetes. 2014, 63, 3891–3905. [Google Scholar] [CrossRef]
- Zhou L, Dong M, Feng G, et al. Semaglutide mitigates testicular damage in diabetes by inhibiting ferroptosis. Biochem Biophys Res Commun. 2024, 715, 149996. [Google Scholar] [CrossRef]
- Filippatos TD, Panagiotopoulou TV, Elisaf MS. Adverse Effects of GLP-1 Receptor Agonists. Rev Diabet Stud. 2014, 11, 202–230. [Google Scholar] [CrossRef]
- Chung SD, Liu HT, Lin H, Kuo HC. Elevation of serum c-reactive protein in patients with OAB and IC/BPS implies chronic inflammation in the urinary bladder. Neurourol Urodyn. 2011, 30, 417–420. [Google Scholar] [CrossRef]
- Liu HT, Jiang YH, Kuo HC. Increased serum adipokines implicate chronic inflammation in the pathogenesis of overactive bladder syndrome refractory to antimuscarinic therapy. PLoS One. 2013, 8, e76706. [Google Scholar] [CrossRef]
- Pillalamarri N, Shalom DF, Pilkinton ML, et al. Inflammatory Urinary Cytokine Expression and Quality of Life in Patients With Overactive Bladder. Female Pelvic Med Reconstr Surg. 2018, 24, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Grundy L, Caldwell A, Brierley SM. Mechanisms Underlying Overactive Bladder and Interstitial Cystitis/Painful Bladder Syndrome. Front Neurosci. 2018, 12, 931. [Google Scholar] [CrossRef]
- Meng X, Zhou J, Zhao CN, Gan RY, Li HB. Health Benefits and Molecular Mechanisms of Resveratrol: A Narrative Review. Foods. 2020, 9, 340. [Google Scholar] [CrossRef]
- Singh I, Wang L, Xia B, et al. Activation of arcuate nucleus glucagon-like peptide-1 receptor-expressing neurons suppresses food intake. Cell Biosci. 2022, 12, 178. [Google Scholar] [CrossRef]
- Secher A, Jelsing J, Baquero AF, et al. The arcuate nucleus mediates GLP-1 receptor agonist liraglutide-dependent weight loss. J Clin Invest. 2014, 124, 4473–4488. [Google Scholar] [CrossRef]
- Jais A, Brüning JC. Arcuate Nucleus-Dependent Regulation of Metabolism-Pathways to Obesity and Diabetes Mellitus. Endocr Rev. 2022, 43, 314–328. [Google Scholar] [CrossRef]
- Beddows CA, Shi F, Horton AL, et al. Pathogenic hypothalamic extracellular matrix promotes metabolic disease. Nature. 2024, 633, 914–922. [Google Scholar] [CrossRef]
- Wright EE Jr, Aroda VR. Clinical review of the efficacy and safety of oral semaglutide in patients with type 2 diabetes considered for injectable GLP-1 receptor agonist therapy or currently on insulin therapy. Postgrad Med. 2020, 132, 26–36. [Google Scholar] [CrossRef]
- Huang KP, Acosta AA, Ghidewon MY, et al. Dissociable hindbrain GLP1R circuits for satiety and aversion. Nature 2024, 632, 585–593. [Google Scholar] [CrossRef]

Table 1.
Baseline characteristics of patients receiving intravesical BOTOX injection for overactive bladder, with and without concomitant GLP-1 receptor agonist therapy (Semaglutide). Values are shown before and after 1:1 propensity score matching. Continuous variables are presented as mean ± standard deviation; categorical variables are presented as number (%). Standardized mean differences (SMD) are reported to assess covariate balance between groups.
Table 1.
Baseline characteristics of patients receiving intravesical BOTOX injection for overactive bladder, with and without concomitant GLP-1 receptor agonist therapy (Semaglutide). Values are shown before and after 1:1 propensity score matching. Continuous variables are presented as mean ± standard deviation; categorical variables are presented as number (%). Standardized mean differences (SMD) are reported to assess covariate balance between groups.
| Characteristic | OAB + BOTOX (Before Matching) | OAB + BOTOX + GLP1 RA (Before Matching) | P-Value (Before Matching) | SMD (Before Matching) | OAB + BOTOX (After Matching) | OAB + BOTOX + GLP1 RA (After Matching) | P-Value (After Matching) | SMD (After Matching) |
|---|---|---|---|---|---|---|---|---|
| Age at Index (Mean ± SD) | 62.4 ± 17.6 | 59.4 ± 13.2 | < 0.0001 | 0.1935 | 59.3 ± 13.9 | 59.4 ± 13.2 | 0.8073 | 0.011 |
| Female | 15,971 (80.2%) | 904 (91.1%) | < 0.0001 | 0.315 | 913 (92.0%) | 904 (91.1%) | 0.4668 | 0.0327 |
| Male | 3,563 (17.9%) | 63 (6.4%) | < 0.0001 | 0.3594 | 59 (5.9%) | 63 (6.4%) | 0.7085 | 0.0168 |
| Not Hispanic or Latino | 15,513 (77.9%) | 800 (80.6%) | 0.0435 | 0.0671 | 802 (80.8%) | 800 (80.6%) | 0.9093 | 0.0051 |
| White | 15,858 (79.7%) | 752 (75.8%) | 0.0034 | 0.0927 | 770 (77.6%) | 752 (75.8%) | 0.339 | 0.0429 |
| Black or African American | 1,706 (8.6%) | 127 (12.8%) | < 0.0001 | 0.1373 | 115 (11.6%) | 127 (12.8%) | 0.4104 | 0.037 |
| Hispanic or Latino | 1,333 (6.7%) | 69 (7.0%) | 0.7498 | 0.0103 | 71 (7.2%) | 69 (7.0%) | 0.8608 | 0.0079 |
| Asian | 339 (1.7%) | 10 (1.0%) | 0.0955 | 0.0601 | 10 (1.0%) | 10 (1.0%) | 1 | < 0.0001 |
| Overweight/Obesity (E65-E68) | 5,216 (26.2%) | 756 (76.2%) | < 0.0001 | 1.1554 | 755 (76.1%) | 756 (76.2%) | 0.958 | 0.0024 |
| Hypertension (I10) | 8,944 (44.9%) | 575 (58.0%) | < 0.0001 | 0.2631 | 564 (56.9%) | 575 (58.0%) | 0.6175 | 0.0224 |
| Stress Incontinence (N39.3) | 5,398 (27.1%) | 389 (39.2%) | < 0.0001 | 0.2591 | 391 (39.4%) | 389 (39.2%) | 0.9268 | 0.0041 |
| BMI 40-44.9 (Z68.41) | 880 (4.4%) | 214 (21.6%) | < 0.0001 | 0.5275 | 219 (22.1%) | 214 (21.6%) | 0.7858 | 0.0122 |
| BMI 45-49.9 (Z68.42) | 431 (2.2%) | 110 (11.1%) | < 0.0001 | 0.3647 | 104 (10.5%) | 110 (11.1%) | 0.6641 | 0.0195 |
| BMI 29-29.9 (Z68.29) | 453 (2.3%) | 53 (5.3%) | < 0.0001 | 0.1608 | 48 (4.8%) | 53 (5.3%) | 0.6096 | 0.0229 |
| BMI 28-28.9 (Z68.28) | 457 (2.3%) | 40 (4.0%) | 0.0005 | 0.0993 | 37 (3.7%) | 40 (4.0%) | 0.7273 | 0.0157 |
| BMI 27-27.9 (Z68.27) | 461 (2.3%) | 37 (3.7%) | 0.0044 | 0.0827 | 38 (3.8%) | 37 (3.7%) | 0.9063 | 0.0053 |
| Antimicrobials (AM000) | 17,619 (88.5%) | 976 (98.4%) | < 0.0001 | 0.4075 | 928 (93.5%) | 976 (98.4%) | < 0.0001 | 0.2479 |
| Antiemetics (GA605) | 12,021 (60.4%) | 832 (83.9%) | < 0.0001 | 0.5427 | 745 (75.1%) | 832 (83.9%) | < 0.0001 | 0.2185 |
| Laxatives (GA200) | 11,381 (57.2%) | 740 (74.6%) | < 0.0001 | 0.3739 | 680 (68.5%) | 740 (74.6%) | 0.0028 | 0.1344 |
| Anti-infectives, vaginal (GU300) | 7,163 (36.0%) | 585 (59.0%) | < 0.0001 | 0.4731 | 518 (52.2%) | 585 (59.0%) | 0.0025 | 0.1362 |
Table 2.
Summary of our study’s key findings.
| Outcome | Event Rate (BOTOX group) | Event Rate (BOTOX+GLP-1 group) | Risk Difference (95% CI) | KM Log-Rank p | HR (95% CI) |
|---|---|---|---|---|---|
| Urinary Retention | 8.60% | 4.90% | 3.66% (1.16-6.17%) | 0.0064 | 1.74 (1.16-2.59) |
| UTI | 13.30% | 8.80% | 4.54% (0.67-8.40%) | 0.042 | 1.48 (1.01-2.17) |
| Antispasmodic Use | 11.80% | 10.30% | 1.55% (-6.07 to 9.17%) | 0.7234 | 1.14 (0.55-2.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



