Submitted:
05 August 2025
Posted:
06 August 2025
You are already at the latest version
Abstract
Traumatic brain injury (TBI) is a major global health concern, contributing to significant morbidity, mortality, and long-term disability. Traditional surgical interventions, such as open craniotomy, while effective, often result in substantial trauma and prolonged recovery. The current review explores the growing role of minimally invasive neurosurgical (MIN) techniques—including endoscopic evacuation, stereotactic aspiration, and robotic-assisted procedures—in the management of TBI. These approaches aim to reduce operative time, minimize disruption to healthy brain tissue, and improve neurological outcomes. Technological advancements, such as artificial intelligence (AI) and machine learning, have enhanced surgical planning and intraoperative precision, while personalized medicine is increasingly guiding treatment decisions based on patient-specific factors, including age, comorbidities, and genetic markers. The review also emphasizes the significance of neuroplasticity, rehabilitation, and ongoing monitoring in maximizing recovery. Although MIN techniques require specialized training and equipment and may be less effective in complex or diffuse injuries, evidence supports their use in appropriately selected patients. Multidisciplinary care models and integration of neurology and neurosurgery are essential for improving both short- and long-term outcomes. Furthermore, patient-centered outcomes, including quality of life and satisfaction, are increasingly recognized as critical metrics of success. Future directions include the development of disease-specific outcome measures, broader adoption of AI-driven tools, and continued refinement of surgical techniques to enhance precision and safety. Overall, MIN represents a transformative shift in TBI management, offering promising benefits in terms of recovery, functionality, and patient well-being.
Keywords:
neurotrauma
; intracerebral hemorrhage
; endoscopic neurosurgery
; craniotomy alternative
; surgical technique
; robotics
; early surgery
; postoperative recovery
; functional recovery
1. Introduction
TBI is defined as the interruption in brain function, or other evidence of brain pathology, caused by an external physical force (Figure 1)[1]. It is also defined as neurotrauma caused by a mechanical force applied to the head. In the US, there are about 1.7–2.0 million incidents of TBI annually [2]. TBI represents a major global public health concern. Recent estimates suggest that 27–69 million individuals worldwide suffer a TBI annually [3]. In the US alone, TBI contributes to approximately 2.8 million ED visits, hospitalizations, and deaths each year [4].
The burden of TBI extends beyond acute care, with many survivors experiencing long-term cognitive, emotional, and physical impairments. These outcomes impose substantial socioeconomic costs, with the US economic impact estimated at over $76 billion annually [3]. For many patients, TBI does not cease to evolve after the acute period and initial recovery. This injury is not a time related event, but a chronic health condition [5]. Patients with TBI treated in care centers mention that 1.1% of the US population have lifelong disabilities as a result of this injury [6]. Death in severe TBI was higher than 50% [7]. Results have improved over the past years, and mortality has been reduced to 30–40% [8]. In the UK, TBI is the most common cause of death and disability in people under 40 years [9]. Moderate and severe TBI are a leading cause of morbidity and mortality. So, rapid diagnosis and management allow secondary injury to be lowered. TBI is one of many causes of altered mental status [10]. This literature review examines the evolving role of MIN techniques in managing TBI, focusing on their impact on neurological outcomes, patient-centered care, and future directions for research.
Historically, the management of TBI relied heavily on traditional open craniotomy, which, while effective in relieving ICP and evacuating hematomas, often involved significant post-surgical trauma, prolonged recovery, and increased risk of complications. Over the past two decades, advances in imaging, instrumentation, and surgical navigation have catalyzed a paradigm shift toward MIN techniques [11]. Neurosurgery is a rapidly changing specialty and often pioneers new surgical techniques [12]. In 1900, for the first time, Harvey Cushing brought modern neurosurgery into the world [13]. Since then, neurosurgery has evolved substantially and is a field which relies on improving patient outcomes [14]. The operating microscope, bipolar cautery, CT scans, MRI, and image-guided surgery could all be mentioned as models that represent innovation [12]. These approaches—such as endoscopic hematoma evacuation, stereotactic aspiration, and robotic-assisted procedures—aim to minimize disruption to healthy brain tissue while achieving comparable or superior therapeutic outcomes [15].
MIN techniques offer several advantages, including reduced operative time, lower infection rates, shorter hospital stays, and improved cosmetic results [16]. Importantly, they also align with the principles of patient-centered care by enhancing postoperative quality of life and facilitating faster return to daily activities. However, these techniques are not without limitations. They often require specialized training, advanced equipment, and may be less effective in cases involving diffuse or multifocal injuries [16].
2. MIN Techniques in TBI
2.1. Overview of Techniques
Endoscopic neurosurgery involves the use of a rigid endoscope inserted through a burr hole to access intracranial pathology (Figure 2). In TBI, it is primarily used for the evacuation of acute SDH and IVH [17]. Studies have shown that endoscopic evacuation can achieve near-total hematoma removal with reduced operative time (typically 60–90 minutes), minimal cortical disruption, and lower infection rates compared to craniotomy [18]. However, its limitations include a narrow field of view, limited instrument maneuverability, and difficulty managing active bleeding in complex or multiloculated hematomas [19].
Neuroendoscopy is a specialized form of endoscopic surgery focused on ventricular and periventricular regions. It is particularly useful in TBI patients with obstructive hydrocephalus or IVH. The technique allows for direct visualization of the ventricular system and precise CSF pathway restoration. Neuroendoscopy third ventriculostomy is commonly performed to relieve hydrocephalus. While it offers reduced brain retraction and faster recovery, complications such as CSF leakage, infection, and limited access to deep-seated lesions remain concerns [20].
Stereotactic neurosurgery uses a 3D coordinate system guided by CT or MRI to target deep brain structures with high precision. In TBI, it is employed for minimally invasive hematoma aspiration, ICP monitoring, and biopsy of deep matter lesions. It is especially beneficial in patients with poor surgical tolerance or deep-seated hemorrhages. The technique minimizes collateral damage and allows for real-time monitoring. However, it requires advanced imaging infrastructure and is less effective in cases of rapidly expanding hematomas or diffuse brain injury [21].
2.2. Technological Innovations
Achieving sufficient decompression remains the cornerstone of surgical management in TBI. Traditionally, this has favored open craniotomies. However, the evolution of MIN has demonstrated that adequate decompression can be achieved while minimizing collateral damage to healthy brain tissue [22]. Techniques such as endoscopic evacuation of hematomas and stereotactic-guided aspiration have shown promising results in both decompression and neurological recovery [23]. In this context, the resurgence of neuroendoscopy was catalyzed by the development of the Hopkins rod-lens system in the 1960s, which significantly enhanced visualization [24]. Pioneers such as Griffith et al. and Auer et al. applied neuroendoscopy techniques to treat IVH and hydrocephalus, laying the foundation for its modern use in TBI [25,26].
In recent years, the convergence of robotics, AI, and minimally invasive techniques has transformed neurosurgical practice. Robotic systems now assist in tasks requiring sub-millimeter precision, such as electrode placement and hematoma evacuation, enhancing both safety and efficiency [27]. These systems are particularly beneficial in deep-seated or eloquent brain regions where manual access is limited.
ML has further enhanced preoperative planning and intraoperative navigation. ML-based image enhancement tools approved by the FDA have improved the clarity of preoperative imaging, aiding in the identification of critical structures [28]. In robot-assisted SEEG, ML algorithms optimize electrode trajectories by accounting for anatomical constraints, vascular structures, and target zones, significantly reducing planning time and improving accuracy [29].
3. Neurological Outcomes of MIN
3.1. Short-Term Outcomes
In the immediate postoperative period following TBI, particularly after MIN interventions, clinical management is directed toward the prevention of secondary brain injury. These secondary insults may arise from intracranial factors such as expanding hematomas, cerebral edema, and elevated ICP, as well as extracranial factors including hypoxia, hypotension, and systemic infections, all of which can exacerbate neuronal injury and worsen neurological outcomes [30]. The GCS remains a cornerstone in the early assessment of neurological function, providing a standardized measure of consciousness based on eye, verbal, and motor responses. Lower GCS scores are consistently associated with more severe injury and poorer prognosis [31].
Short-term neurological outcomes after MIN for TBI are influenced by both the nature of the primary injury and the occurrence of early postoperative complications. Focal neurological deficits such as hemiparesis, aphasia, and cranial nerve dysfunction are frequently observed and are largely dependent on the anatomical location and extent of the injury. Cognitive impairments are also common in the early recovery phase, with deficits in attention, processing speed, and executive function often reported. These impairments can significantly hinder a patient’s ability to engage in early rehabilitation and resume daily activities [32].
Several studies have quantified the incidence of early complications following TBI. Post-traumatic seizures occur in approximately 12–20% of patients with moderate to severe TBI, particularly within the first week post-injury [33]. Hydrocephalus, especially in cases involving intraventricular hemorrhage, has been reported in 10–45% of patients and may necessitate cerebrospinal fluid diversion procedures [34]. Infectious complications, including ventilator-associated pneumonia, are prevalent in intensive care settings, affecting up to 60% of mechanically ventilated patients [35]. Additionally, thromboembolic events such as deep vein thrombosis and pulmonary embolism are observed in 10–30% of immobilized patients, despite prophylactic measures. Although MIN techniques are associated with reduced tissue disruption, complications such as CSF leaks and surgical site infections still occur in 2–5% of cases [36].
These early complications not only prolong hospitalization but also contribute to long-term disability. A multicenter longitudinal study reported that 57% of patients with moderate to severe TBI remained moderately to severely disabled at five years post-injury, and 50% required rehospitalization during that period [37]. These findings underscore the importance of vigilant early monitoring and intervention to mitigate secondary injury and optimize neurological recovery.
3.2. Long-Term Outcomes
Long-term recovery following moderate to severe TBI is highly variable and influenced by factors such as injury severity, age, access to rehabilitation, and comorbidities. Cognitive and functional recovery can continue for months or even years post-injury. According to the TRACK-TBI study, while only 12% of patients with severe TBI showed favorable outcomes two weeks post-injury, this number increased to 52% at 12 months, indicating substantial potential for recovery over time [38].
Persistent cognitive deficits may include impairments in memory, learning, language, and executive functioning. Functional outcomes are often measured using tools like the GOSE and the DRS, which track improvements in independence and quality of life. Neurorehabilitation plays a critical role in optimizing these outcomes. Early and intensive rehabilitation has been shown to improve both cognitive and physical recovery, reduce disability, and enhance reintegration into the community [39].
3.3. Comparative Analysis
MIN techniques are increasingly favored for the management of ICH and other TBI-related pathologies. Compared to traditional open craniotomy, MIN approaches—such as endoscopic hematoma evacuation, stereotactic aspiration, and minimally invasive catheter-based techniques—are associated with reduced operative time, lower complication rates, and shorter hospital stays. Importantly, Scaggiante et al. (2018) demonstrated that MIN techniques were linked to improved neurological outcomes and faster functional recovery. In their study, outcomes were assessed using standardized neurological scales, including the mRS and the GOS, at both discharge and follow-up intervals. Functional independence, defined as an mRS score of 0–3, was significantly more common in patients treated with MIN techniques [40]. Additionally, hematoma volume reduction was quantitatively measured using serial CT imaging, and greater evacuation efficiency was correlated with better clinical outcomes [41].
Patients undergoing MIN for ICH consistently demonstrate superior cognitive and functional recovery compared to those treated with traditional craniotomy (Table 1). This advantage is supported by a growing body of evidence from clinical trials, cohort studies, and meta-analyses. Neuroendoscopic approaches have been associated with significantly higher scores on the MoCA, NIHSS, and GCS, indicating better preservation of neurological function. Furthermore, stereotactic and endoscopic techniques yield improved long-term outcomes, with higher scores on the GOSE, mRS, and Barthel Index at one-year follow-up. These metrics reflect enhanced quality of life and greater independence in daily activities. Meta-analyses further confirm that MIN techniques are linked to higher rates of favorable recovery and reduced perioperative morbidity. While conventional craniotomy remains indispensable in complex or emergent cases, accumulating evidence underscores the clinical benefits of MIN in appropriately selected patients, particularly in promoting neurological restoration and functional autonomy.
4. Factors Influencing Neurological Outcomes
A comprehensive overview of factors influencing outcomes in TBI is presented in Table 2. These factors are categorized into five domains: patient-related, injury-related, intervention-related, post-interventional care, and other contextual variables. The table highlights the multifactorial nature of TBI prognosis, emphasizing the importance of individualized assessment and treatment strategies.
4.1. Patient-Related Factors
Patients’ socio-demographic factors have been studied in multiple investigations to estimate their effect on the outcome of TBI, with gender being one of the most frequently examined variables. In a study conducted among patients with expansive ICH, being an adult aged 39 years or older was identified as a significant risk factor for developing expansive ICH following TBI [47]. Age has consistently emerged as one of the strongest predictors of outcome in the post-TBI period [48]. Rabinowitz et al. conducted a study among individuals aged 12 to 30 years and found that even within this relatively young cohort, older age was associated with a greater number and severity of post-concussive symptoms. Notably, cognitive and emotional symptoms—such as difficulty concentrating, memory problems, irritability, and anxiety—were more prevalent among the older participants in this age range [49]. Furthermore, being over 60 years old has been significantly associated with increased likelihood of hospital admission following head trauma [50]. Other studies have reported a significant increase in mortality and delays in functional recovery, including the resumption of oral intake, with advancing age [51,52].
Kanakia et al. demonstrated that in geriatric patients with traumatic SDH, pre-existing comorbidities—particularly vasculopathy conditions—were more predictive of adverse surgical outcomes than chronological age. Their multivariate analysis revealed that these comorbidities significantly contributed to the development of posttraumatic seizures and influenced discharge disposition, underscoring the importance of individualized risk stratification in neurosurgical decision-making [53]. However, multiple studies have reported contrasting findings. Kowalski et al. found that younger patients with moderate to severe TBI were more likely to present with disorders of consciousness during inpatient rehabilitation, suggesting that age alone does not confer a protective effect against early neurological complications [54]. Similarly, Laing et al. observed a higher incidence of early posttraumatic seizures among younger individuals, challenging the assumption that seizure risk increases linearly with age [55]. Yilmaz et al. also reported younger age increases the risk of acute post-TBI headaches [56]. These conflicting data can be explained by two reasons, which are not adjusting the confounders in studying the association of age or/and different outcomes having different associations with age.
Regarding gender, functional outcomes were worse in females than in males [57]. Moreover, Rabinowitz et al. reported poor symptomatic outcomes in females compared to males after a TBI such as acute post-traumatic headache [49,56]. In addition, African American patients were found to have poorer outcomes compared to white or Asian [58,59].
Lifestyles and co-morbidities were also found to contribute to the risk of poor outcomes after TBI. Two separate studies reported that tobacco use disorder was associated significantly with worse outcomes [60,61]. After controlling for age and gender, Eagle et al. demonstrated that obesity was associated with more severe post-TBI symptoms 6- and 12-months post-injury [47]. Moreover, early post-TBI seizures were found to be significantly higher in patients with a high Charlson comorbidity index (which indicates severe multiple co-morbidities such as myocardial infarction, diabetes, and dementia) [55]. Post-TBI headache and migraine were also found to yield a worse outcome [62]. In addition, Yilmaz et al. reported that headache at admission was associated with chronic post-TBI headaches [56].
Moreover, even psychological disorders such as anxiety and depression were found to be significant predictors of post-TBI headaches [56]. According to Browne et al., depression and alcohol were some of the predictors of variance in pain, depressive and PTSD severity, and physical mobility after six months from the TBI [63].
Multiple biomarkers at admission have been found to correlate with favorable outcomes in patients with TBI. In a study conducted by Trimble et al. in pediatric patients, stable hemodynamic parameters—specifically, a systolic blood pressure above 90 mmHg—and higher body temperatures on arrival (≥34.9 °C) were significantly associated with improved outcomes. Conversely, certain radiological findings have been linked to worse prognoses [64]. For example, the presence of the swirl sign on initial CT imaging, which represents areas of mixed hyperdensity and hypodensity within an acute hematoma, has been associated with active bleeding and a higher risk of hematoma expansion. Kamabu et al. demonstrated that this sign was significantly correlated with the development of expansive intracranial hematomas, necessitating more aggressive intervention [60].
Regarding cognitive outcomes, Yue et al. found that abnormalities detected on head CT imaging such as contusions, hemorrhages, or diffuse axonal injury, were strongly associated with decreased verbal memory performance. Additionally, a history of seizures was linked to impairments in short-term memory. Genetic factors also appear to influence recovery trajectories; individuals carrying the APOE-ε4 allele exhibited significantly worse performance on long-delay verbal memory tasks compared to non-carriers, suggesting a potential role for genetic screening in prognostication [65].
4.2. Injury-Related Factors
The mechanism and type of injury were also found to have effects on the outcome after TBI. Having multiple traumatic injuries was found to be significantly associated with poor outcomes in almost a dose-dependent response compared to having a single traumatic event [66]. Persisting disorders of consciousness after the trauma were associated with high-velocity injuries, intraventricular hemorrhage, subcortical contusion, and intracranial mass effect [54].
Laing et al. proposed that post-traumatic seizures were more prevalent among patients with TBI resulting from falls, and in those presenting with subdural or subarachnoid hemorrhage, as well as higher injury severity scores [55]. Moreover, patients with penetrating TBI had higher mortality rates [57]. Chang et al. identified three key predictors for the failure of non-invasive management and the need for surgical intervention in TBI patients: hematoma volume exceeding 5 cm3, a decline in GCS score between initial and follow-up CT scans, and evidence of herniation on the initial CT [67]. Interestingly, each 1 mL increase in hematoma volume was associated with a 6% increase in the likelihood of a one-point decline in the GCS, highlighting the critical role of preventing hematoma expansion in ameliorating neurological deterioration [68]. Trimble et al. reported that survival following TBI was significantly associated with less severe injuries, a higher incidence of epidural hematoma, and reduced evidence of brain ischemia on imaging [64]. Acute pain intensity and psychological distress of the patients were found to be predictors of variation in the outcome of TBI [63].
4.3. Intervention-Related Factors
Most of the studies have addressed the traditional approach of DC. In contrast, few studies addressed minimally invasive approaches such as endoscopic surgery, burr hole surgery, keyhole surgery, and minimally invasive craniectomy.
According to LaRovere et al., withdrawing life-sustaining therapies among children with TBI was the most common cause of death (70%) [69]. Generally, surgery was known to cause a reduction in poor outcomes of TBI [50], and this reduction was variable according to the severity of the injury: 80% reduction in mild injury, 56% reduction in moderate injury, and 65% reduction in severe injury [70]. The timing of the surgery has also been evaluated across multiple studies. Kim et al. mentioned that patients who underwent surgery within 4 hours after visiting the ED had significantly shorter hospital stays and less mortality [71]. Vaca et al. reported similar findings as they reported that delays after hospital arrival can substantially increase mortality for mild and moderate TBI patients [72]. This contradicts the finding of Walcott et al. as they found increasing the time to surgery causes a significant reduction in mortality [51]. Interestingly, Knettel et al. did not report any significance regarding the timing of surgery [50].
Type of surgery has also been found to affect the outcome of the trauma, but very few studies compared traditional surgeries to MIN. A study reported by Tseng et al. on endoscopically assisted surgery revealed good neurological outcomes. The mean GCS was 7.5, while the mean hemorrhage volume was 57.14 cm3, with less surgery time (mean around 60 minutes) [20]. A prospective study of surgery for TBI reported different types of surgeries. Burr hole surgery patients had a median length of hospital stay around three days, compared to other surgeries, which ranged from 4 in craniotomy to 9 in DC. These findings suggest that burr hole procedures, as a form of MIN, are associated with shorter hospital stays. Notably, the study found that length of stay was significantly correlated with mortality, whereas the type of surgical intervention—whether minimally invasive or traditional—did not independently predict mortality outcomes [73].
Other types of intervention also had an impact on the outcome of TBI. Attending the ICU resulted in around four times higher risk of poor outcomes compared to those who did not were upgraded to ICU. This can be explained by the fact that critically ill patients are the ones who attend the ICU [50]. Moreover, the usage of echocardiograms indicated a lower mortality rate, which can be explained by valuable insight given by the echo for treating the injury [74]. Walcott et al. reported that aspirin usage for patients with TBI led to a reduction in mortality [51]. The number of dysphagia interventions in TBI patients was also documented as a contributing factor to the return of oral intake after the injury, with more interventions leading to less probability of reaching total oral intake [52].
4.4. Post-Interventional Care
Multiple factors after the intervention were found to affect patient outcomes. These factors can be related to after-surgery care and non-invasive therapies. Matovu et al. reported that low temperature and convulsions resulted in a significant 1.5 and 1.6 times increase in mortality, respectively [75], in contrast to Laing et al. report, which indicated that seizures were associated with ICU admission and hospital stay but not mortality. The reason for not finding an association can be adjusting the confounders in the later study [55]. In addition, another study by Majidi et al. indicated that seizures were associated with more complications, such as pneumonia and longer hospital stays [76]. Multiple studies associated with hypotension showed that hypotension is related to poor outcomes [57,77,78]. Prehospital systolic blood pressure above 150 mm Hg is an independent predictor of increased mortality and TBI severity, supporting its use in early triage and prognostic modeling [79]. Moreover, circulatory shock development led to poor outcomes of TBI, such as longer hospital stays, disability, and disturbances of consciousness [80].
An increase in hemoglobin concentration was also reported with good outcomes [77]. Teshita et al. identified low GCS scores (<5), oxygen saturation below 90%, and hospital-acquired pneumonia as independent predictors of poor functional outcomes in TBI patients [78]. Multiple studies have shown that a GCS score below 9 is a strong predictor of poor outcomes, including increased mortality, in patients with TBI [60]. A lower average GCS score (8.1 vs. 13.5) was significantly associated with the development of post-TBI epilepsy, indicating its value as a predictive marker [81]. LaRovere et al. indicated that organ failure increases the risk of death among TBI pediatric patients [69]. Multiple factors have been independently associated with increased mortality in TBI patients, including tracheostomy, prolonged mechanical ventilation, infections, use of nasogastric or PEG tubes, spasticity, CSF leakage, wound dehiscence, and a low GCS score [60]. ICH was associated with significantly increased sleep after the injury [82].
4.5. Other Factors
Environmental (factors such as stairs at home or work) affect the well-being and quality of life among TBI patients as they already have impairment in the ability to perform physical activities [83]. Measuring the biomarkers after the injury was also found to predict the outcome of TBI. According to a review in 2012, multiple chemical substances have been reported to correlate with the outcome after TBI. MAO-A polymorphism was associated with aggression, while BDNF was associated with cognitive functions. The endothelial nitric oxide gene was related to cerebral perfusion and serotonin transporters (SLC6A4) with PTSD. Also, IL-6 was associated with survival and discharge in the ICU among severely ill patients [84]. Chiaretti et al. measured multiple biomarkers at 2 hours after admission and then after 48 hours for their effect on the GCS. High early NGF, high DCX, and low NSE levels were found to be significantly associated with better neurological outcomes. Meanwhile, BDNF and GDNF were not found to affect outcomes [85]. Lindblad et al. highlighted the prognostic value of neuroinflammatory markers in TBI, identifying complement C9 in CSF and complement factor B in serum as independent predictors of long-term outcomes [86].
5. Integration of Neurology and Neurosurgery in Patient Care
5.1. Multidisciplinary Approaches
TBI usually requires a multidisciplinary approach to reduce the risk of poor outcomes in various aspects of the injury. The fourth edition of “Brain Trauma Foundation’s Guidelines for the Management of Severe Traumatic Brain Injury” in 2016 illustrated the multidisciplinary approach used in settings of TBI. The approach was composed of multiple levels: DC, CSF drainage, prophylactic hypothermia, hyperosmolar treatment, ventilation therapies, anesthetics, analgesics, sedatives, steroids, and seizure prophylaxis for neurology. Prophylactic anti-seizure drugs were not recommended for late post-TBI seizures but rather for early seizures (within seven days of injury), according to the guidelines. However, it does not mention the importance of MIN [87].
In a meta-analysis conducted in 2022, the authors compared surgical treatment of acute SDH to conservative (non-surgical) treatment. Surgical treatment caused a reduction in mortality by 13% more than the conservative treatment percentage [88]. According to a review by Kline et al., the combination therapies were found to have positive benefits in 46% of the included studies [89]. Spears et al. found that patients receiving both surgical and pharmacological treatment experienced a 59% reduction in the risk of poor outcomes, with the benefit varying by TBI severity [70]. Multiple studies have explored the impact of combination therapy involving traditional surgical interventions, such as DC, showing enhanced outcomes when paired with pharmacological or supportive treatments, particularly in moderate to severe TBI cases. Cooper et al. compared outcomes between TBI patients receiving combination therapy (DC plus standard care) and those receiving standard care alone (including hypothermia and barbiturates). While the combination group had reduced ICP duration, fewer interventions, and shorter ICU stays, they also presented with worse GCS scores and a higher risk of unfavorable outcomes. Mortality rates were similar between groups, suggesting that although DC reduced intervention needs and length of stay, it may be associated with poorer functional outcomes [90].
Shi et al. reported a rare case of a 54-year-old woman who sustained a penetrating brain injury from a screwdriver assault. The patient underwent a combination of surgical interventions—including right cheekbone craniectomy, foreign body removal, and CSF drainage—followed by non-surgical treatments such as external ventricular drainage, antibiotics, and intravenous sodium valproate. Her GCS improved from 3 at admission to 12 by day 42, with no seizures and good neurological recovery at 6-month follow-up [91]. This case underscores the potential benefit of individualized combination therapy in complex TBI cases.
Few studies have addressed combination therapies using MIN techniques (Table 3). Noiphithak et al. conducted a RCT comparing endoscopic surgery with intraventricular fibrinolysis to EVD alone in patients with IVH. The surgical group demonstrated superior outcomes, including a higher IVH clearance rate, lower incidence of shunt dependency, and reduced disability as measured by the mRS [92].
Moreover, Arai et al. presented a case of an 88-year-old woman with mild traumatic SAH due to a fall. Lacosamide was administered for non-convulsive seizures, but consciousness deteriorated, and no progression was noticed regarding the hematoma. Fosphenytoin sodium hydrate and phenobarbital were also administered, but no improvement in consciousness was reported. After that, endoscope-assisted evacuation of the hematoma was performed. Post-operatively, the patient’s consciousness improved with no neurological defects [93]. Zhou et al. performed a clinical trial to compare minimally invasive stereotactic puncture therapy against conventional craniotomy for treating acute ICH. The MIN group reported significantly a better outcome such as improvement in the GCS, reduction in incidence of rebleeding, better functional recovery -according to the Barthel index- and less disability- according to the mRS [45].
5.2. Importance of Continuous Monitoring
Monitoring is essential not only in predicting the outcome but also in directing the treatment. According to the fourth edition of “Brain Trauma Foundation’s Guidelines for the Management of Severe Traumatic Brain Injury,” there are three types of important monitoring in TBI patients: ICP monitoring, cerebral perfusion monitoring, and advanced cerebral monitoring. Each type of monitoring is associated with a specific type of mortality: ICP with a reduction in in-hospital and 2-week post-injury mortality and cerebral perfusion with a reduction in 2-week mortality [87]. Follow-up after the surgery for a TBI can extend even to 2 years, indicating the importance of long-term follow-up. This is the case in a study conducted by Somma et al. following patients who suffered from motor accidents and underwent DC. After two years after the surgery, the patient developed a left front-orbital headache due to herniation of brain parenchyma into the left orbit. Then, minimally invasive surgery was performed to treat the herniating, and it resulted in 3-year follow-up with a good outcome [97]. Interestingly, number of follow-up sessions was significantly associated with more unfavorable outcomes, such as delayed return to work for one year. This may reflect a higher detection rate of underlying pathologies during follow-up, or conversely, that patients who did not attend follow-up required less ongoing care due to better initial recovery [98].
6. Personalized Medicine in Neurosurgery for TBI
6.1. Tailoring Surgical Approaches to Individual Patients
MIN has become an increasingly preferred approach in the management of TBI, offering advantages such as reduced operative trauma, shorter hospital stays, and improved neurological outcomes. However, the heterogeneity of TBI necessitates a personalized approach to surgical planning, where patient-specific factors significantly influence the choice of technique (Figure 3).
Age, comorbidities, and the severity of injury are among the most critical determinants. Elderly patients or those with systemic conditions such as cardiovascular disease may benefit more from MIN due to its lower physiological burden. The type, size, and location of intracranial lesions—such as SDH, contusions, or DAI—also guide the selection of endoscopic evacuation, stereotactic aspiration, or navigation-assisted decompression. Furthermore, clinical indicators like GCS scores and ICP trends are essential in determining the urgency and extent of intervention [99].
In addition to clinical and radiological parameters, genetic and molecular biomarkers are emerging as valuable tools in surgical decision-making. For instance, the presence of the APOE ε4 allele has been associated with poorer neurological recovery, potentially influencing the aggressiveness of surgical intervention. Elevated levels of NfL and inflammatory cytokines such as IL-6 and TNF-α have been linked to more severe neuronal injury, aiding in the stratification of patients for MIN versus conservative management [99].
6.2. Future Trends in Personalized Neurosurgery
The future of MIN in TBI is being shaped by the integration of AI and ML, which are poised to revolutionize surgical planning, intraoperative decision-making, and outcome prediction.
AI technologies are increasingly capable of analyzing large, complex datasets to predict clinical outcomes such as mortality, functional recovery, and complication risks. These models incorporate multimodal data—including imaging, physiological monitoring, and laboratory results—to generate individualized risk profiles and recommend optimal surgical strategies. One promising development is the use of digital twins: virtual patient models that simulate surgical outcomes under different scenarios, enabling preoperative planning tailored to individual anatomy and pathology [100].
Moreover, AI systems are being developed to integrate real-time physiological data—such as continuous ICP, cerebral oxygenation, and EEG—into adaptive models that can dynamically adjust surgical or postoperative care protocols. This real-time responsiveness enhances the precision and personalization of neurosurgical care, potentially improving both short- and long-term neurological outcomes [100].
7. Neuroplasticity and Recovery Post-Surgery
7.1. Role of Neuroplasticity in TBI Recovery
Neuroplasticity is the ability of the nervous system to adapt to external and internal stimuli and then change its constitution and function accordingly [101]. TBI leads to massive destruction of brain tissue, which demands studying the recovery of these tissues. Multiple studies have investigated the effect of MIN on functional outcomes and recovery of patients with TBI [102]. Codd et al. reported a case of 86-year-old women presented with acute SDH. The patient presented with headache, nausea, vomiting, and progressive lethargy that led to the need for airway intubation. Endoscopic burr hole evacuation of the hematoma was performed. After the surgery, the patient had significant clinical improvement and was independent for daily activities such as feeding and demonstrated full strength in her extremities [95].
Hwang et al. reported an unchanged level of consciousness when comparing the level before the endoscopic evacuation of hematoma to the level at admission. In this context, MIN has shown no significant impairment on the level of consciousness in those cases [103]. Kellner et al. demonstrated the impact of minimally invasive endoscopic intracerebral hemorrhage evacuation on functional outcomes. 100% of the patients had a 0-3 score on the premorbid mRS. After the endoscopy, around 46% had a score between 0 and 3, which suggests half of the premorbid percentage [104].
Zhou et al. compared minimally invasive stereotactic puncture therapy versus conventional craniotomy. The MIN procedure reported a significantly higher Barthel Index and lower mRS than conventional surgery. This indicates that the MIN approach may improve functional and recovery outcomes [45]. Sometimes, MIN was needed by itself to restore neuroplasticity rather than dealing with damage from the trauma. DBS was used via a minimally invasive technique to treat post-traumatic dystonia [105,106].
7.2. Rehabilitation Strategies to Enhance Neuroplasticity
Maintaining and enhancing neuroplasticity is critical for achieving optimal functional recovery in patients with TBI. Li et al. proposed a structured, three-tiered rehabilitation model tailored to the severity and complexity of patient needs. Level 1 targets individuals with physical, cognitive, and behavioral impairments, offering foundational rehabilitation support. Level 2 addresses patients with similar impairments but compounded by severe behavioral disturbances, requiring more intensive and specialized interventions. Level 3 is designed for those with ongoing rehabilitation needs, focusing on long-term support and community reintegration. This stratified approach underscores the importance of individualized rehabilitation strategies in promoting brain recovery and maximizing long-term outcomes [83].
Neurorehabilitation is the only current treatment to improve long-term outcomes in TBI patients [107]. Physical rehabilitation is crucial, as well as psychological care, which was found to be the most effective care in avoiding post-TBI symptoms [108]. According to a review by Crupi et al., multiple drugs were found to enhance brain repair and recovery by increasing cyclic 3’,5’-adenosine monophosphate, such as phosphodiesterase inhibitors (rolipram, dipyridamole, BC11-38), selective serotonin reuptake inhibitors, and serotonin-dopamine reuptake inhibitors. Moreover, neurofeedback therapy was also found to promote neuroplasticity as it uses electrical potential to enforce specific brain states [109]. Also, another technique that uses electrical potential is DBS, which was reported to treat post-traumatic dystonia [105]. Wang et al. studied the effect of this electrical stimulation by inducing short-term stimulation to the cortex. They noticed improved motor function, short-term memory, and learning ability [110]. These studies demonstrate the importance of various electrical stimulation methods in regaining neurological function. Janak et al. conducted a study on 257 patients with mild TBI. The patients complete a multidisciplinary rehabilitation program composed of cognitive rehabilitation, vestibular interventions, headache management, and psychiatric care. Patients in the intervention group had significantly fewer post-TBI symptoms and fewer post-traumatic stress disorder symptoms than the control [111]. Moreover, receiving both progesterone and vitamin D was found to promote recovery rate in patients with TBI [112].
8. Role of Neuroimaging in Assessing Surgical Outcomes
Neuroimaging plays a pivotal role in both the planning and evaluation of MIN procedures for TBI. The integration of advanced imaging modalities has significantly enhanced the precision of surgical interventions and the ability to monitor postoperative recovery.
8.1. Preoperative Neuroimaging
Preoperative neuroimaging is essential for surgical planning, particularly in the context of MIN where precision is paramount. Techniques such as high-resolution MRI, DTI, and functional MRI provide detailed anatomical and functional maps of the brain. These modalities allow surgeons to localize lesions, assess white matter tract integrity, and identify eloquent cortical areas that must be preserved during intervention. Functional brain mapping, often integrated with neuronavigational systems, enables the customization of surgical trajectories to minimize disruption of critical neural networks. For example, DTI-based tractography can delineate corticospinal tracts, guiding the placement of endoscopic or stereotactic instruments to avoid motor deficits. Moreover, magnetic resonance spectroscopy and perfusion imaging can offer metabolic and hemodynamic insights into perilesional tissue, aiding in the differentiation between viable and non-viable brain regions [113].
8.2. Postoperative Neuroimaging
Postoperative imaging is equally critical in evaluating the success of MIN procedures and monitoring the patient’s recovery trajectory. Early postoperative CT scans are typically used to confirm hematoma evacuation, assess for residual mass effect, and detect complications such as rebleeding or hydrocephalus. However, MRI offers superior soft tissue contrast and is increasingly used to assess the extent of lesion resection and to monitor for delayed ischemic or inflammatory changes [114]. Advanced imaging techniques, including serial fMRI and DTI, are being explored to track neuroplasticity and functional recovery over time. These modalities can reveal changes in brain connectivity and activation patterns that correlate with clinical improvement, providing objective markers of surgical efficacy. Intraoperative MRI is also gaining traction, allowing real-time assessment of surgical progress and immediate correction of suboptimal outcomes during the same operative session [115].
9. Complications and Risk Management in MIN
9.1. Common Complications
The fundamental goal of MIN is to lower the incidence of complications following traditional surgery; however, few complications have been documented (Figure 4). Historically, neuroendoscopy was the only procedure used in MIN. The limitations of endoscopy in ensuring surgery effectiveness, deep structure manipulation safety, and, in the sequel, appropriate hemostasis are just a few of the drawbacks compared to microsurgical methods [116].
A study conducted in Germany to evaluate the PCV in patients with severe TBI in comparison to conventional burr-hole ventriculostomy to measure ICP as a component of early clinical care, in this study, minor hemorrhage into the ipsilateral lateral ventricle in one PCV case was observed on CT scans due to an initially unsuccessful puncture (95% CI 0–6%). No infections occurred (95% CI 0–6%). One catheter infection and one failed catheter placement (each 8%, 95% CI 0–20%) occurred in the burr-hole group [117]. Moreover, several studies reported higher rates of postoperative complications which include periprocedural infection rates of and relevant bleeding complication rates of 0.5% which were indicative of surgical drilling trepanation [118]. Furthermore, an analysis of 54 patients who underwent craniotomy revealed that postoperative hemorrhage, CSF leakage, and ophthalmoplegia were among the complications reported [119].
9.2. Strategies for Risk Management
Given the associated challenges, various strategies have been developed to mitigate postoperative risks and enhance outcomes in MIN. A CT monitor within the CT suite is critical for real-time verification of control scans during ICP catheter placement. The monitor must be visible from the cranial end of the gantry, which should also be equipped with an operating light. Room design must allow at least 2 meters of clearance at the head of the CT table to accommodate surgical staff and instrument tables. As most trauma centers currently lack these specifications, future trauma room designs should incorporate them [117].
Pitskhelauri’s introduction of the MARI device into neurosurgery has enabled novel microsurgical techniques. Functioning similarly to an operating microscope, MARI allows surgeons to adjust the optical field and settings hands-free, enhancing precision and workflow efficiency [120]. Standard trephination (burr hole) approaches with a diameter of 10–14 mm can be used for microsurgery under the direction of the MARI device and Zeiss microscopes with different modifications. Thus, in the case of deep brain injuries, this approach offers a safe and small surgical corridor for extreme operations. All manipulations are feasible when combined with standard microsurgical instruments [121]. Additionally, Intraoperative Stereotactic Computed Tomography-Guided Endoscopic Surgery (ICES), a multicenter RCT, showed considerable safety and efficacy in these types of surgeries [122].
10. Patient-Centered Outcomes and QoL
10.1. Assessing QoL Post-Surgery
For TBI surgical management, adequate decompression is the key goal. Therefore, it may seem unexpected to use minimally invasive strategies to treat patients with TBI. However, MIN can provide both adequate decompressions following TBI, and enhance neurological recovery for these patients [22,123]. MIN has been used more frequently in recent years to treat patients who have experienced spontaneous ICH surgically. Because MIN helps preserve healthy brain tissue, these patients recover more quickly and have better neurological outcomes than similar patients treated with more invasive surgery [124,125]. In light of outcomes such as earlier decompression, reduced mortality, morbidity, surgical times, and blood loss in ICH patients treated with a minimally invasive procedure, we expect that MIN techniques may improve the quality of life and prove its beneficial outcomes in the surgical management of TBI patients on a long term [20].
The utilization of minimally invasive approaches is growing in the treatment of spontaneous ICH, and research indicates that MIN is linked to better neurological recovery in addition to being safe and effective. We were able to avoid craniectomy and its associated risks of increased bleeding, increased infection risk, hydrocephalus risk, and the necessity for additional treatments by opting for MIN. Simple burr-holes to remove traumatic ICH can be easily performed for isolated traumatic ICH patients, resulting in smaller incisions, less blood loss, shorter operating times, quicker recovery, and shorter hospital stays, according to a previous study. By maximizing cortical and subcortical preservation and avoiding partial lobectomy, minimally invasive approaches promote neurological recovery after surgery [20].
10.2. Patient Satisfaction and Experience
In a RCT with long-term follow-up comparing different minimally invasive surgery techniques with standard open surgery for the treatment of unruptured intracranial aneurysms, the authors focused on patient satisfaction in 5 aspects: facial hypoesthesia, facial pain or headache, masticatory discomfort, aesthetic results, and general satisfaction with the procedure. Minimally invasive surgery patients reported significantly higher satisfaction during all time points of evaluation. Moreover, all quality-of-life-domain mean scores were statistically higher in the minimally invasive surgery compared with the control group at all 3 evaluation time points [126].
11. Future Directions
Accurate assessment of medical therapies is a cornerstone of evidence-based practice [127]. A standardized global approach to outcome measurement enhances both clinical care and research by streamlining communication, improving patient handovers, and enabling cross-study and cross-population comparisons. These benefits extend to patient outcomes, neurosurgical practice, and research efforts. However, due to the distinct needs of each subspecialty, a fully uniform system is not universally applicable. Instead, tailored variations are often necessary. The future of neurosurgical quality-of-life assessment lies in increasingly specialized, disease-specific outcome measures that allow for more precise patient evaluation.
The ongoing debate in the literature underscores the need for disease-specific outcome measures to more accurately assess interventions and guide patient care strategies. TBI has the highest number of outcome measures among neurosurgical subspecialties, with nearly 100 identified tools [128]. These instruments vary in their purposes, distinguishing between acute and long-term outcomes, as well as between moderate and severe TBI. Each class of outcome measure serves a distinct role depending on the clinical context. Commonly used tools include neuropsychological assessments such as the GOS and its extended version, the GOSE [129]. Originally designed to objectively describe functional recovery after severe brain injury, the GOS classified outcomes into five categories: death, vegetative state, severe disability, moderate disability, and good recovery [130]. The GOSE, introduced in 1998, refined this by subdividing moderate and severe disability into upper and lower levels, offering a more precise assessment of functional recovery.
The GOS and GOSE remain widely used for assessing outcomes in TBI, their original intended application [131]. These tools offer a nearly comprehensive framework for evaluating functional recovery [132]. Due to their broad applicability, the GOS has also been adapted for use in other neurological conditions, including intracranial aneurysms, brain tumors, stroke, and cranioplasty [133]. A summary of the most commonly used outcome measures across neurosurgical subspecialties is presented in Table 4.
12. Conclusions
MIN techniques represent a transformative advancement in the management of TBI, offering a compelling alternative to traditional open procedures. By reducing surgical trauma, preserving healthy brain tissue, and enabling faster recovery, these approaches align with modern principles of patient-centered care. The integration of advanced technologies—such as robotics, artificial intelligence, and precision imaging—has further enhanced the safety, accuracy, and personalization of TBI interventions. While challenges remain, including the need for specialized training and equipment, the growing body of evidence supports the efficacy of MIN in improving both short- and long-term neurological outcomes. Moreover, the incorporation of multidisciplinary care, continuous monitoring, and tailored rehabilitation strategies underscores the importance of a holistic approach to TBI recovery. As research continues to evolve, future directions should focus on refining patient selection criteria, developing standardized outcome measures, and expanding access to these innovative techniques. Ultimately, MIN holds significant promise in reshaping the neurosurgical landscape and improving the quality of life for individuals affected by TBI.
Author Contributions
Conceptualization, J.P.R. and I.K.; methodology, J.P.R. and I.K.; software, J.P.R. and I.K.; validation, J.P.R., I.K., K.I., S.O.M.E., M.H.E., A.M.M., V.V.B., and A.L.F.C.; formal analysis, I.K.; investigation, I.K.; resources, J.P.R.; data curation, J.P.R.; writing—original draft preparation J.P.R., I.K., K.I., S.O.M.E., M.H.E., A.M.M., V.V.B., and A.L.F.C.; writing—review and editing, J.P.R., I.K., K.I., S.O.M.E., M.H.E., A.M.M., V.V.B., and A.L.F.C.; visualization, V.V.B.; supervision, A.L.F.C.; project administration, J.P.R. and I.K.; funding acquisition, J.P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial intelligence |
| BDNF | Brain-derived neurotrophic factor |
| CSF | Cerebrospinal fluid |
| CT | Computed tomography |
| DAI | Diffuse axonal injury |
| DBS | Deep brain stimulation |
| DC | Decompressive craniectomy |
| DCX | Doublecortin |
| DRS | Disability rating scale |
| DTI | Diffusion tensor imaging |
| ED | Emergency department |
| EEG | Electroencephalography |
| EVD | External ventricular drainage |
| FDA | U.S. Food and Drug Administration |
| GCS | Glasgow coma scale |
| GDNF | Glial cell line-derived neurotrophic factor |
| GOS | Glasgow outcome scale |
| GOSE | Glasgow outcome scale–extended |
| ICES | Intraoperative stereotactic computed tomography-guided endoscopic surgery |
| ICH | Intracranial hemorrhage |
| ICP | Intracranial pressure |
| ICU | Intensive care unit |
| IL | Interlekin |
| IVH | Intraventricular hemorrhage |
| MARI | Micro-angio-resection-interface |
| MAO | Monoamine oxidase |
| ML | Machine learning |
| MIN | Minimally invasive neurosurgery |
| MRI | Magnetic resonance imaging |
| mRS | Modified Rankin scale |
| NGF | Nerve growth factor |
| NSE | Neuron-specific enolase |
| PCV | Percutaneous computed tomography-controlled ventriculostomy |
| PEG | Percutaneous endoscopic gastrostomy |
| PTSD | Posttraumatic stress disorder |
| QoL | Quality of life |
| RCT | Randomized controlled trial |
| SAH | Subarachnoid hemorrhage |
| SDH | Subdural hemorrhage |
| SEEG | Stereo electroencephalography |
| TBI | Traumatic brain injury |
| TRACK-TBI | Transforming research and clinical knowledge in traumatic brain injury |
| UK | United Kingdom |
| US | United States |
References
- Timofeev, I.; Santarius, T.; Kolias, A.G.; Hutchinson, P.J.A. Decompressive Craniectomy - Operative Technique and Perioperative Care. Adv Tech Stand Neurosurg 2012, 38, 115–136. [Google Scholar] [CrossRef]
- Faul, M.; Coronado, V. Epidemiology of Traumatic Brain Injury. Handb Clin Neurol 2015, 127, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Global, Regional, and National Burden of Traumatic Brain Injury and Spinal Cord Injury, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019, 18, 56–87. [CrossRef]
- Invited Commentary on “Centers for Disease Control and Prevention Report to Congress: Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation”.; United States, 2015; Vol. 96;
- Masel, B.E.; DeWitt, D.S. Traumatic Brain Injury: A Disease Process, Not an Event. J Neurotrauma 2010, 27, 1529–1540. [Google Scholar] [CrossRef] [PubMed]
- Zaloshnja, E.; Miller, T.; Langlois, J.A.; Selassie, A.W. Prevalence of Long-Term Disability from Traumatic Brain Injury in the Civilian Population of the United States, 2005. J Head Trauma Rehabil 2008, 23, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment and Prognosis of Coma after Head Injury. Acta Neurochir (Wien) 1976, 34, 45–55. [Google Scholar] [CrossRef]
- Rosenfeld, J.V.; Maas, A.I.; Bragge, P.; Morganti-Kossmann, M.C.; Manley, G.T.; Gruen, R.L. Early Management of Severe Traumatic Brain Injury. Lancet 2012, 380, 1088–1098. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic Brain Injury: Integrated Approaches to Improve Prevention, Clinical Care, and Research. Lancet Neurol 2017, 16, 987–1048. [Google Scholar] [CrossRef]
- Howley, I.W.; Bennett, J.D.; Stein, D.M. Rapid Detection of Significant Traumatic Brain Injury Requiring Emergency Intervention. Am Surg 2021, 87, 1504–1510. [Google Scholar] [CrossRef]
- Buccilli, B.; Alan, A.; Aljeradat, B.G.; Shahzad, A.; Almealawy, Y.F.; Chisvo, N.S.; Ennabe, M.; Weinand, M. Neuroprotection: Surgical Approaches in Traumatic Brain Injury. Surg Neurol Int 2024, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.S.; Parker, A. The Evolution of Neurosurgery: How Has Our Practice Changed? Br J Neurosurg 2013, 27, 747–751. [Google Scholar] [CrossRef]
- Bhattacharyya, K.B. Harvey William Cushing: The Father of Modern Neurosurgery (1869-1939). Neurol India 2016, 64, 1125–1128. [Google Scholar] [CrossRef]
- Nikova, A.; Birbilis, T. The Basic Steps of Evolution of Brain Surgery. Maedica (Bucur) 2017, 12, 297–305. [Google Scholar]
- Lou, L.; Wang, H.; Chen, M.; Zhu, J.; Li, S. Robot Assisted Stereotactic Surgery Improves Hematoma Evacuation in Intracerebral Hemorrhage Compared to Frame Based Method. Sci Rep 2025, 15, 12427. [Google Scholar] [CrossRef]
- Darzi, S.A.; Munz, Y. The Impact of Minimally Invasive Surgical Techniques. Annu Rev Med 2004, 55, 223–237. [Google Scholar] [CrossRef]
- Miki, K.; Nonaka, M.; Kobayashi, H.; Horio, Y.; Abe, H.; Morishita, T.; Iwaasa, M.; Inoue, T. Optimal Surgical Indications of Endoscopic Surgery for Traumatic Acute Subdural Hematoma in Elderly Patients Based on a Single-Institution Experience. Neurosurg Rev 2021, 44, 1635–1643. [Google Scholar] [CrossRef]
- Barlas, O.; Karadereler, S.; Bahar, S.; Yesilot, N.; Krespi, Y.; Solmaz, B.; Bayindir, O. Image-Guided Keyhole Evacuation of Spontaneous Supratentorial Intracerebral Hemorrhage. Minim Invasive Neurosurg 2009, 52, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Spencer, R.J.; Manivannan, S.; Zaben, M. Endoscope-Assisted Techniques for Evacuation of Acute Subdural Haematoma in the Elderly: The Lesser of Two Evils? A Scoping Review of the Literature. Clin Neurol Neurosurg 2021, 207, 106712. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.-L.; Kuo, L.-T.; Chen, C.-M.; Yang, S.-H.; Tang, C.-T.; Lai, D.-M.; Huang, A.P.-H. Surgical Application of Endoscopic-Assisted Minimally-Invasive Neurosurgery to Traumatic Brain Injury: Case Series and Review of Literature. J Formos Med Assoc 2022, 121, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Sarigul, B.; De Macêdo Filho, L.J.; Hawryluk, G.W. Invasive Monitoring in Traumatic Brain Injury. Current Surgery Reports 2022, 10, 265–273. [Google Scholar] [CrossRef]
- Nascimento, C.N.G.; Amorim, R.L.; Mandel, M.; do Espírito Santo, M.P.; Paiva, W.S.; Andrade, A.F.; Teixeira, M.J. Endoscopic-Assisted Removal of Traumatic Brain Hemorrhage: Case Report and Technical Note. J Surg Case Rep 2015, 2015, rjv132. [Google Scholar] [CrossRef] [PubMed]
- Vadhavekar, N.H.; Sabzvari, T.; Laguardia, S.; Sheik, T.; Prakash, V.; Gupta, A.; Umesh, I.D.; Singla, A.; Koradia, I.; Ramirez Patiño, B.B.; et al. Advancements in Imaging and Neurosurgical Techniques for Brain Tumor Resection: A Comprehensive Review. Cureus 2024, 16, e72745. [Google Scholar] [CrossRef] [PubMed]
- Cockett, W.S.; Cockett, A.T. The Hopkins Rod-Lens System and the Storz Cold Light Illumination System. Urology 1998, 51, 1–2. [Google Scholar] [CrossRef]
- Auer, L.M.; Holzer, P.; Ascher, P.W.; Heppner, F. Endoscopic Neurosurgery. Acta Neurochir (Wien) 1988, 90, 1–14. [Google Scholar] [CrossRef]
- Griffith, H.B. Technique of Fontanelle and Persutural Ventriculoscopy and Endoscopic Ventricular Surgery in Infants. Childs Brain 1975, 1, 359–363. [Google Scholar] [CrossRef]
- Al-Hamadani, M.N.A.; Fadhel, M.A.; Alzubaidi, L.; Balazs, H. Reinforcement Learning Algorithms and Applications in Healthcare and Robotics: A Comprehensive and Systematic Review. Sensors (Basel) 2024, 24. [Google Scholar] [CrossRef] [PubMed]
- Gowal, S.; Dvijotham, K.; Stanforth, R.; Bunel, R.; Qin, C.; Uesato, J.; Arandjelovic, R.; Mann, T.; Kohli, P. On the Effectiveness of Interval Bound Propagation for Training Verifiably Robust Models. arXiv, 2018; arXiv:1810.12715. [Google Scholar]
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical Image Analysis Using Convolutional Neural Networks: A Review. Journal of Medical Systems 2018, 42, 226. [Google Scholar] [CrossRef] [PubMed]
- Marshall, L.F.; Marshall, S.B.; Klauber, M.R.; Van Berkum Clark, M.; Eisenberg, H.; Jane, J.A.; Luerssen, T.G.; Marmarou, A.; Foulkes, M.A. The Diagnosis of Head Injury Requires a Classification Based on Computed Axial Tomography. J Neurotrauma 1992, 9 Suppl 1, S287–292. [Google Scholar]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. A Practical Scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Lezak, M.D. Neuropsychological Assessment; Oxford University Press, USA, 2004; ISBN 0-19-511121-4.
- Green, R.E.; Colella, B.; Hebert, D.A.; Bayley, M.; Kang, H.S.; Till, C.; Monette, G. Prediction of Return to Productivity after Severe Traumatic Brain Injury: Investigations of Optimal Neuropsychological Tests and Timing of Assessment. Arch Phys Med Rehabil 2008, 89, S51–60. [Google Scholar] [CrossRef]
- Wahjoepramono, P.O.P.; Sasongko, A.B.; Halim, D.; Aviani, J.K.; Lukito, P.P.; Adam, A.; Tsai, Y.T.; Wahjoepramono, E.J.; July, J.; Achmad, T.H. Hydrocephalus Is an Independent Factor Affecting Morbidity and Mortality of ICH Patients: Systematic Review and Meta-Analysis. World Neurosurg X 2023, 19, 100194. [Google Scholar] [CrossRef]
- Stocchetti, N.; Maas, A.I.R. Traumatic Intracranial Hypertension. N Engl J Med 2014, 370, 2121–2130. [Google Scholar] [CrossRef]
- Laguardia, S.; Piccioni, A.; Alonso Vera, J.E.; Muqaddas, A.; Garcés, M.; Ambreen, S.; Sharma, S.; Sabzvari, T. A Comprehensive Review of the Role of the Latest Minimally Invasive Neurosurgery Techniques and Outcomes for Brain and Spinal Surgeries. Cureus 2025, 17, e84682. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, J.D.; Cuthbert, J.P.; Harrison-Felix, C.; Whiteneck, G.G.; Bell, J.M.; Miller, A.C.; Coronado, V.G.; Pretz, C.R. US Population Estimates of Health and Social Outcomes 5 Years after Rehabilitation for Traumatic Brain Injury. J Head Trauma Rehabil 2014, 29, E1–9. [Google Scholar] [CrossRef]
- McCrea, M.A.; Giacino, J.T.; Barber, J.; Temkin, N.R.; Nelson, L.D.; Levin, H.S.; Dikmen, S.; Stein, M.; Bodien, Y.G.; Boase, K.; et al. Functional Outcomes Over the First Year After Moderate to Severe Traumatic Brain Injury in the Prospective, Longitudinal TRACK-TBI Study. JAMA Neurol 2021, 78, 982–992. [Google Scholar] [CrossRef]
- Mostert, C.Q.B.; Singh, R.D.; Gerritsen, M.; Kompanje, E.J.O.; Ribbers, G.M.; Peul, W.C.; van Dijck, J.T.J.M. Long-Term Outcome after Severe Traumatic Brain Injury: A Systematic Literature Review. Acta Neurochir (Wien) 2022, 164, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Scaggiante, J.; Zhang, X.; Mocco, J.; Kellner, C.P. Minimally Invasive Surgery for Intracerebral Hemorrhage. Stroke 2018, 49, 2612–2620. [Google Scholar] [CrossRef] [PubMed]
- Grunert, P. From the Idea to Its Realization: The Evolution of Minimally Invasive Techniques in Neurosurgery. Minim Invasive Surg 2013, 2013, 171369. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yang, S.; Zhou, X.; Lai, R.; Tan, D. A Retrospective Cohort Study of Neuroendoscopic Surgery versus Traditional Craniotomy on Surgical Success Rate, Postoperative Complications, and Prognosis in Patients with Acute Intracerebral Hemorrhage. Comput Intell Neurosci 2022, 2022, 2650795. [Google Scholar] [CrossRef]
- Liu, Y.-B.; Kuo, L.-T.; Chen, C.-H.; Kung, W.-M.; Tsai, H.-H.; Chou, S.-C.; Yang, S.-H.; Wang, K.-C.; Lai, D.-M.; Huang, A.P.-H. Surgery for Coagulopathy-Related Intracerebral Hemorrhage: Craniotomy vs. Minimally Invasive Neurosurgery. Life (Basel) 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Wu, X.; Li, J.; Liu, Z.; Chen, F.; Zhang, L.; Zhang, H.; Wan, X.; Cheng, Q. Minimally Invasive Surgery Is Superior to Conventional Craniotomy in Patients with Spontaneous Supratentorial Intracerebral Hemorrhage: A Systematic Review and Meta-Analysis. World Neurosurg 2018, 115, 266–273. [Google Scholar] [CrossRef]
- Zhou, H.; Zhang, Y.; Liu, L.; Han, X.; Tao, Y.; Tang, Y.; Hua, W.; Xue, J.; Dong, Q. A Prospective Controlled Study: Minimally Invasive Stereotactic Puncture Therapy versus Conventional Craniotomy in the Treatment of Acute Intracerebral Hemorrhage. BMC Neurol 2011, 11, 76. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, H.; Zhang, J.; Luo, M.; Wang, Q.; Zhao, Y.; Gan, Z.; Xu, B.; Chen, X. Minimally Invasive Surgeries for Spontaneous Hypertensive Intracerebral Hemorrhage (MISICH): A Multicenter Randomized Controlled Trial. BMC Med 2024, 22, 244. [Google Scholar] [CrossRef]
- Eagle, S.R.; Puccio, A.M.; Nelson, L.D.; McCrea, M.; Giacino, J.; Diaz-Arrastia, R.; Conkright, W.; Jain, S.; Sun, X.; Manley, G.; et al. Association of Obesity with Mild Traumatic Brain Injury Symptoms, Inflammatory Profile, Quality of Life and Functional Outcomes: A TRACK-TBI Study. J Neurol Neurosurg Psychiatry 2023, 94, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Butcher, I.; Maas, A.I.R.; Lu, J.; Marmarou, A.; Murray, G.D.; Mushkudiani, N.A.; McHugh, G.S.; Steyerberg, E.W. Prognostic Value of Admission Blood Pressure in Traumatic Brain Injury: Results from the IMPACT Study. J Neurotrauma 2007, 24, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, A.R.; Li, X.; McCauley, S.R.; Wilde, E.A.; Barnes, A.; Hanten, G.; Mendez, D.; McCarthy, J.J.; Levin, H.S. Prevalence and Predictors of Poor Recovery from Mild Traumatic Brain Injury. J Neurotrauma 2015, 32, 1488–1496. [Google Scholar] [CrossRef] [PubMed]
- Knettel, B.A.; Knettel, C.T.; Sakita, F.; Myers, J.G.; Edward, T.; Minja, L.; Mmbaga, B.T.; Vissoci, J.R.N.; Staton, C. Predictors of ICU Admission and Patient Outcome for Traumatic Brain Injury in a Tanzanian Referral Hospital: Implications for Improving Treatment Guidelines. Injury 2022, 53, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Walcott, B.P.; Khanna, A.; Kwon, C.-S.; Phillips, H.W.; Nahed, B.V.; Coumans, J.-V. Time Interval to Surgery and Outcomes Following the Surgical Treatment of Acute Traumatic Subdural Hematoma. J Clin Neurosci 2014, 21, 2107–2111. [Google Scholar] [CrossRef]
- Kjaersgaard, A.; Nielsen, L.H.; Sjölund, B.H. Factors Affecting Return to Oral Intake in Inpatient Rehabilitation after Acquired Brain Injury. Brain Inj 2015, 29, 1094–1104. [Google Scholar] [CrossRef]
- Kanakia, K.P.; Wells, A.M.; Tchoulhakian, M.; Iskra, B.S.; Kaculini, C.; Tavakoli-Samour, S.; Boyd, J.T.; Hafeez, S.; Seifi, A.; Dengler, B.A. Factors Affecting Outcomes in Geriatric Traumatic Subdural Hematoma in a Neurosurgical Intensive Care Unit. World Neurosurg 2022, 158, e441–e450. [Google Scholar] [CrossRef]
- Kowalski, R.G.; Hammond, F.M.; Weintraub, A.H.; Nakase-Richardson, R.; Zafonte, R.D.; Whyte, J.; Giacino, J.T. Recovery of Consciousness and Functional Outcome in Moderate and Severe Traumatic Brain Injury. JAMA Neurol 2021, 78, 548–557. [Google Scholar] [CrossRef]
- Laing, J.; Gabbe, B.; Chen, Z.; Perucca, P.; Kwan, P.; O’Brien, T.J. Risk Factors and Prognosis of Early Posttraumatic Seizures in Moderate to Severe Traumatic Brain Injury. JAMA Neurol 2022, 79, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, T.; Roks, G.; de Koning, M.; Scheenen, M.; van der Horn, H.; Plas, G.; Hageman, G.; Schoonman, G.; Spikman, J.; van der Naalt, J. Risk Factors and Outcomes Associated with Post-Traumatic Headache after Mild Traumatic Brain Injury. Emerg Med J 2017, 34, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.R.; Lingsma, H.F.; Roozenbeek, B. Predicting Outcome after Traumatic Brain Injury. Handb Clin Neurol 2015, 128, 455–474. [Google Scholar] [CrossRef] [PubMed]
- Sorani, M.D.; Lee, M.; Kim, H.; Meeker, M.; Manley, G.T. Race\ethnicity and Outcome after Traumatic Brain Injury at a Single, Diverse Center. J Trauma 2009, 67, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Shafi, S.; Marquez de la Plata, C.; Diaz-Arrastia, R.; Shipman, K.; Carlile, M.; Frankel, H.; Parks, J.; Gentilello, L.M. Racial Disparities in Long-Term Functional Outcome after Traumatic Brain Injury. J Trauma 2007, 63, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Kamabu, L.K.; Bbosa, G.S.; Lekuya, H.M.; Cho, E.J.; Kyaruzi, V.M.; Nyalundja, A.D.; Deng, D.; Sekabunga, J.N.; Kataka, L.M.; Obiga, D.O.D.; et al. Burden, Risk Factors, Neurosurgical Evacuation Outcomes, and Predictors of Mortality among Traumatic Brain Injury Patients with Expansive Intracranial Hematomas in Uganda: A Mixed Methods Study Design. BMC Surg 2023, 23, 326. [Google Scholar] [CrossRef]
- Schneider, A.L.C.; Barber, J.; Temkin, N.; Gardner, R.C.; Manley, G.; Diaz-Arrastia, R.; Sandsmark, D. Associations of Preexisting Vascular Risk Factors With Outcomes After Traumatic Brain Injury: A TRACK-TBI Study. J Head Trauma Rehabil 2023, 38, E88–E98. [Google Scholar] [CrossRef]
- Kamins, J.; Richards, R.; Barney, B.J.; Locandro, C.; Pacchia, C.F.; Charles, A.C.; Cook, L.J.; Gioia, G.; Giza, C.C.; Blume, H.K. Evaluation of Posttraumatic Headache Phenotype and Recovery Time After Youth Concussion. JAMA Netw Open 2021, 4, e211312. [Google Scholar] [CrossRef]
- Browne, A.L.; Appleton, S.; Fong, K.; Wood, F.; Coll, F.; de Munck, S.; Newnham, E.; Schug, S.A. A Pilot Randomized Controlled Trial of an Early Multidisciplinary Model to Prevent Disability Following Traumatic Injury. Disabil Rehabil 2013, 35, 1149–1163. [Google Scholar] [CrossRef]
- Trimble, D.J.; Parker, S.L.; Zhu, L.; Cox, C.S.; Kitagawa, R.S.; Fletcher, S.A.; Sandberg, D.I.; Shah, M.N. Outcomes and Prognostic Factors of Pediatric Patients with a Glasgow Coma Score of 3 after Blunt Head Trauma. Childs Nerv Syst 2020, 36, 2657–2665. [Google Scholar] [CrossRef] [PubMed]
- Yue, J.K.; Robinson, C.K.; Burke, J.F.; Winkler, E.A.; Deng, H.; Cnossen, M.C.; Lingsma, H.F.; Ferguson, A.R.; McAllister, T.W.; Rosand, J.; et al. Apolipoprotein E Epsilon 4 (APOE-Ε4) Genotype Is Associated with Decreased 6-Month Verbal Memory Performance after Mild Traumatic Brain Injury. Brain Behav 2017, 7, e00791. [Google Scholar] [CrossRef]
- Etemad, L.L.; Yue, J.K.; Barber, J.; Nelson, L.D.; Bodien, Y.G.; Satris, G.G.; Belton, P.J.; Madhok, D.Y.; Huie, J.R.; Hamidi, S.; et al. Longitudinal Recovery Following Repetitive Traumatic Brain Injury. JAMA Netw Open 2023, 6, e2335804. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.F.; Meeker, M.; Holland, M.C. Acute Traumatic Intraparenchymal Hemorrhage: Risk Factors for Progression in the Early Post-Injury Period. Neurosurgery 2006, 58, 647–656. [Google Scholar] [CrossRef]
- Fletcher-Sandersjöö, A.; Tatter, C.; Tjerkaski, J.; Bartek, J.J.; Maegele, M.; Nelson, D.W.; Svensson, M.; Thelin, E.P.; Bellander, B.-M. Time Course and Clinical Significance of Hematoma Expansion in Moderate-to-Severe Traumatic Brain Injury: An Observational Cohort Study. Neurocrit Care 2023, 38, 60–70. [Google Scholar] [CrossRef] [PubMed]
- LaRovere, K.L.; De Souza, B.J.; Szuch, E.; Urion, D.K.; Vitali, S.H.; Zhang, B.; Graham, R.J.; Geva, A.; Tasker, R.C. Clinical Characteristics and Outcomes of Children with Acute Catastrophic Brain Injury: A 13-Year Retrospective Cohort Study. Neurocrit Care 2022, 36, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Spears, C.A.; Adil, S.M.; Kolls, B.J.; Muhumza, M.E.; Haglund, M.M.; Fuller, A.T.; Dunn, T.W. Surgical Intervention and Patient Factors Associated with Poor Outcomes in Patients with Traumatic Brain Injury at a Tertiary Care Hospital in Uganda. J Neurosurg 2021, 135, 1569–1578. [Google Scholar] [CrossRef]
- Kim, Y.J. The Impact of Time from ED Arrival to Surgery on Mortality and Hospital Length of Stay in Patients with Traumatic Brain Injury. J Emerg Nurs 2011, 37, 328–333. [Google Scholar] [CrossRef]
- Vaca, S.D.; Kuo, B.J.; Nickenig Vissoci, J.R.; Staton, C.A.; Xu, L.W.; Muhumuza, M.; Ssenyonjo, H.; Mukasa, J.; Kiryabwire, J.; Rice, H.E.; et al. Temporal Delays Along the Neurosurgical Care Continuum for Traumatic Brain Injury Patients at a Tertiary Care Hospital in Kampala, Uganda. Neurosurgery 2019, 84, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Laeke, T.; Tirsit, A.; Kassahun, A.; Sahlu, A.; Yesehak, B.; Getahun, S.; Zenebe, E.; Deyassa, N.; Moen, B.E.; Lund-Johansen, M.; et al. Prospective Study of Surgery for Traumatic Brain Injury in Addis Ababa, Ethiopia: Surgical Procedures, Complications, and Postoperative Outcomes. World Neurosurg 2021, 150, e316–e323. [Google Scholar] [CrossRef]
- Chen, F.; Komisarow, J.M.; Mills, B.; Vavilala, M.; Hernandez, A.; Laskowitz, D.T.; Mathew, J.P.; James, M.L.; Haines, K.L.; Raghunathan, K.; et al. Echocardiogram Utilization Patterns and Association With Mortality Following Severe Traumatic Brain Injury. Anesth Analg 2021, 132, 1060–1066. [Google Scholar] [CrossRef]
- Matovu, P.; Kirya, M.; Galukande, M.; Kiryabwire, J.; Mukisa, J.; Ocen, W.; Lowery Wilson, M.; Abio, A.; Lule, H. Hyperglycemia in Severe Traumatic Brain Injury Patients and Its Association with Thirty-Day Mortality: A Prospective Observational Cohort Study in Uganda. PeerJ 2021, 9, e10589. [Google Scholar] [CrossRef] [PubMed]
- Majidi, S.; Makke, Y.; Ewida, A.; Sianati, B.; Qureshi, A.I.; Koubeissi, M.Z. Prevalence and Risk Factors for Early Seizure in Patients with Traumatic Brain Injury: Analysis from National Trauma Data Bank. Neurocrit Care 2017, 27, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Scurfield, A.K.; Wilson, M.D.; Gurkoff, G.; Martin, R.; Shahlaie, K. Identification of Demographic and Clinical Prognostic Factors in Traumatic Intraventricular Hemorrhage. Neurocrit Care 2023, 38, 149–157. [Google Scholar] [CrossRef]
- Teshita, G.; Wondafrash, M.; G/Egziabher, B.; Getachew, B.; Bergene, E. Clinical Characteristics and Functional Outcome of Surgically Treated Adult Head Trauma Patients with Acute Subdural Hematoma: Ethiopian Tertiary Hospitals Experience. World Neurosurg X 2024, 21, 100264. [Google Scholar] [CrossRef] [PubMed]
- Barmparas, G.; Liou, D.Z.; Lamb, A.W.; Gangi, A.; Chin, M.; Ley, E.J.; Salim, A.; Bukur, M. Prehospital Hypertension Is Predictive of Traumatic Brain Injury and Is Associated with Higher Mortality. J Trauma Acute Care Surg 2014, 77, 592–598. [Google Scholar] [CrossRef]
- Toro, C.; Hatfield, J.; Temkin, N.; Barber, J.; Manley, G.; Ohnuma, T.; Komisarow, J.; Foreman, B.; Korley, F.K.; Vavilala, M.S.; et al. Risk Factors and Neurological Outcomes Associated With Circulatory Shock After Moderate-Severe Traumatic Brain Injury: A TRACK-TBI Study. Neurosurgery 2022, 91, 427–436. [Google Scholar] [CrossRef]
- Burke, J.; Gugger, J.; Ding, K.; Kim, J.A.; Foreman, B.; Yue, J.K.; Puccio, A.M.; Yuh, E.L.; Sun, X.; Rabinowitz, M.; et al. Association of Posttraumatic Epilepsy With 1-Year Outcomes After Traumatic Brain Injury. JAMA Netw Open 2021, 4, e2140191. [Google Scholar] [CrossRef]
- Imbach, L.L.; Valko, P.O.; Li, T.; Maric, A.; Symeonidou, E.-R.; Stover, J.F.; Bassetti, C.L.; Mica, L.; Werth, E.; Baumann, C.R. Increased Sleep Need and Daytime Sleepiness 6 Months after Traumatic Brain Injury: A Prospective Controlled Clinical Trial. Brain 2015, 138, 726–735. [Google Scholar] [CrossRef]
- Li, L.M.; Dilley, M.D.; Carson, A.; Twelftree, J.; Hutchinson, P.J.; Belli, A.; Betteridge, S.; Cooper, P.N.; Griffin, C.M.; Jenkins, P.O.; et al. Management of Traumatic Brain Injury (TBI): A Clinical Neuroscience-Led Pathway for the NHS. Clin Med (Lond) 2021, 21, e198–e205. [Google Scholar] [CrossRef] [PubMed]
- Dardiotis, E.; Grigoriadis, S.; Hadjigeorgiou, G.M. Genetic Factors Influencing Outcome from Neurotrauma. Curr Opin Psychiatry 2012, 25, 231–238. [Google Scholar] [CrossRef]
- Chiaretti, A.; Barone, G.; Riccardi, R.; Antonelli, A.; Pezzotti, P.; Genovese, O.; Tortorolo, L.; Conti, G. NGF, DCX, and NSE Upregulation Correlates with Severity and Outcome of Head Trauma in Children. Neurology 2009, 72, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, C.; Pin, E.; Just, D.; Al Nimer, F.; Nilsson, P.; Bellander, B.-M.; Svensson, M.; Piehl, F.; Thelin, E.P. Fluid Proteomics of CSF and Serum Reveal Important Neuroinflammatory Proteins in Blood-Brain Barrier Disruption and Outcome Prediction Following Severe Traumatic Brain Injury: A Prospective, Observational Study. Crit Care 2021, 25, 103. [Google Scholar] [CrossRef] [PubMed]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]
- van Essen, T.A.; Res, L.; Schoones, J.; de Ruiter, G.; Dekkers, O.; Maas, A.; Peul, W.; van der Gaag, N.A. Mortality Reduction of Acute Surgery in Traumatic Acute Subdural Hematoma since the 19th Century: Systematic Review and Meta-Analysis with Dramatic Effect: Is Surgery the Obvious Parachute? J Neurotrauma 2023, 40, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Kline, A.E.; Leary, J.B.; Radabaugh, H.L.; Cheng, J.P.; Bondi, C.O. Combination Therapies for Neurobehavioral and Cognitive Recovery after Experimental Traumatic Brain Injury: Is More Better? Prog Neurobiol 2016, 142, 45–67. [Google Scholar] [CrossRef]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; D’Urso, P.; Kossmann, T.; Ponsford, J.; Seppelt, I.; Reilly, P.; et al. Decompressive Craniectomy in Diffuse Traumatic Brain Injury. N Engl J Med 2011, 364, 1493–1502. [Google Scholar] [CrossRef]
- Shi, J.; Mao, Y.; Cao, J.; Dong, B. Management of Screwdriver-Induced Penetrating Brain Injury: A Case Report. BMC Surg 2017, 17, 3. [Google Scholar] [CrossRef]
- Noiphithak, R.; Ratanavinitkul, W.; Yindeedej, V.; Nimmannitya, P.; Yodwisithsak, P. Outcomes of Combined Endoscopic Surgery and Fibrinolytic Treatment Protocol for Intraventricular Hemorrhage: A Randomized Controlled Trial. World Neurosurg 2023, 172, e555–e564. [Google Scholar] [CrossRef]
- Arai, M.; Nakase, K.; Sasaki, R.; Nishimura, F.; Nakagawa, I. Endoscope-Assisted Evacuation of an Acute Subdural Hematoma in an Elderly Patient With Refractory Nonconvulsive Status Epilepticus: An Illustrative Case. Cureus 2024, 16, e63817. [Google Scholar] [CrossRef]
- Tanaka, T.; Goto, H.; Momozaki, N.; Honda, E. Endoscopic Hematoma Evacuation for Acute Subdural Hematoma with Improvement of the Visibility of the Subdural Space and Postoperative Management Using an Intracranial Pressure Sensor. Surg Neurol Int 2023, 14, 1. [Google Scholar] [CrossRef]
- Codd, P.J.; Venteicher, A.S.; Agarwalla, P.K.; Kahle, K.T.; Jho, D.H. Endoscopic Burr Hole Evacuation of an Acute Subdural Hematoma. J Clin Neurosci 2013, 20, 1751–1753. [Google Scholar] [CrossRef] [PubMed]
- Kuge, A.; Tsuchiya, D.; Watanabe, S.; Sato, M.; Kinjo, T. Endoscopic Hematoma Evacuation for Acute Subdural Hematoma in a Young Patient: A Case Report. Acute Med Surg 2017, 4, 451–453. [Google Scholar] [CrossRef]
- di Somma, L.; Iacoangeli, M.; Nasi, D.; Balercia, P.; Lupi, E.; Girotto, R.; Polonara, G.; Scerrati, M. Combined Supra-Transorbital Keyhole Approach for Treatment of Delayed Intraorbital Encephalocele: A Minimally Invasive Approach for an Unusual Complication of Decompressive Craniectomy. Surg Neurol Int 2016, 7, S12–16. [Google Scholar] [CrossRef]
- Vikane, E.; Hellstrøm, T.; Røe, C.; Bautz-Holter, E.; Assmus, J.; Skouen, J.S. Missing a Follow-up after Mild Traumatic Brain Injury--Does It Matter? Brain Inj 2014, 28, 1374–1380. [Google Scholar] [CrossRef]
- Honeybul, S.; Kolias, A.G. Traumatic Brain Injury: Science, Practice, Evidence and Ethics; Springer Nature, 2021; ISBN 3-030-78075-9.
- Fabrizio, C.; Termine, A. Artificial Intelligence Applications for Traumatic Brain Injury Research and Clinical Management. In Neurobiological and Psychological Aspects of Brain Recovery; Petrosini, L., Ed.; Springer International Publishing: Cham, 2023; ISBN 978-3-031-24930-3. [Google Scholar]
- Mateos-Aparicio, P.; Rodríguez-Moreno, A. The Impact of Studying Brain Plasticity. Front Cell Neurosci 2019, 13, 66. [Google Scholar] [CrossRef]
- Zeiler, F.A.; Thelin, E.P.; Helmy, A.; Czosnyka, M.; Hutchinson, P.J.A.; Menon, D.K. A Systematic Review of Cerebral Microdialysis and Outcomes in TBI: Relationships to Patient Functional Outcome, Neurophysiologic Measures, and Tissue Outcome. Acta Neurochir (Wien) 2017, 159, 2245–2273. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.-C.; Shin, D.-S. Endoscopic Treatment of Acute Subdural Hematoma with a Normal Small Craniotomy. J Neurol Surg A Cent Eur Neurosurg 2020, 81, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Kellner, C.P.; Song, R.; Pan, J.; Nistal, D.A.; Scaggiante, J.; Chartrain, A.G.; Rumsey, J.; Hom, D.; Dangayach, N.; Swarup, R.; et al. Long-Term Functional Outcome Following Minimally Invasive Endoscopic Intracerebral Hemorrhage Evacuation. J Neurointerv Surg 2020, 12, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-X.; He, L.; Zhang, C.-C.; Eisinger, R.; Pan, Y.-X.; Wang, T.; Sun, B.-M.; Wu, Y.-W.; Li, D.-Y. Deep Brain Stimulation in Post-Traumatic Dystonia: A Case Series Study. CNS Neurosci Ther 2019, 25, 1262–1269. [Google Scholar] [CrossRef]
- Rissardo, J.P.; Vora, N.M.; Tariq, I.; Mujtaba, A.; Caprara, A.L.F. Deep Brain Stimulation for the Management of Refractory Neurological Disorders: A Comprehensive Review. Medicina (Kaunas) 2023, 59, 1991. [Google Scholar] [CrossRef] [PubMed]
- Hofer, A.-S.; Schwab, M.E. Enhancing Rehabilitation and Functional Recovery after Brain and Spinal Cord Trauma with Electrical Neuromodulation. Curr Opin Neurol 2019, 32, 828–835. [Google Scholar] [CrossRef]
- Boussard, C.N.; Holm, L.W.; Cancelliere, C.; Godbolt, A.K.; Boyle, E.; Stålnacke, B.-M.; Hincapié, C.A.; Cassidy, J.D.; Borg, J. Nonsurgical Interventions After Mild Traumatic Brain Injury: A Systematic Review. Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Archives of Physical Medicine and Rehabilitation 2014, 95, S257–S264. [Google Scholar] [CrossRef]
- Crupi, R.; Cordaro, M.; Cuzzocrea, S.; Impellizzeri, D. Management of Traumatic Brain Injury: From Present to Future. Antioxidants (Basel) 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-C.; Wei, W.-Y.; Ho, P.-C. Short-Term Cortical Electrical Stimulation during the Acute Stage of Traumatic Brain Injury Improves Functional Recovery. Biomedicines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Janak, J.C.; Cooper, D.B.; Bowles, A.O.; Alamgir, A.H.; Cooper, S.P.; Gabriel, K.P.; Pérez, A.; Orman, J.A. Completion of Multidisciplinary Treatment for Persistent Postconcussive Symptoms Is Associated With Reduced Symptom Burden. J Head Trauma Rehabil 2017, 32, 1–15. [Google Scholar] [CrossRef]
- Aminmansour, B.; Nikbakht, H.; Ghorbani, A.; Rezvani, M.; Rahmani, P.; Torkashvand, M.; Nourian, M.; Moradi, M. Comparison of the Administration of Progesterone versus Progesterone and Vitamin D in Improvement of Outcomes in Patients with Traumatic Brain Injury: A Randomized Clinical Trial with Placebo Group. Adv Biomed Res 2012, 1, 58. [Google Scholar] [CrossRef]
- Talos, I.-F.; O’Donnell, L.; Westin, C.-F.; Warfield, S.K.; Wells III, W.; Yoo, S.-S.; Panych, L.P.; Golby, A.; Mamata, H.; Maier, S.S. Diffusion Tensor and Functional MRI Fusion with Anatomical MRI for Image-Guided Neurosurgery.; Springer, 2003; pp. 407–415.
- Wirtz, C.R.; Tronnier, V.M.; Bonsanto, M.M.; Haßfeld, S.; Knauth, M.; Kunze, S. NeuronavigationMethoden Und Ausblick. Der Nervenarzt 1998, 69, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.G.; Riparbelli, A.C.; Siebner, H.R.; Konge, L.; Bjerrum, F. Using Neuroimaging to Assess Brain Activity and Areas Associated with Surgical Skills: A Systematic Review. Surg Endosc 2024, 38, 3004–3026. [Google Scholar] [CrossRef] [PubMed]
- Lepsveridze, L.T.; Semenov, M.S.; Simonyan, A.S.; Pirtskhelava, S.Z.; Stepanyan, G.G.; Imerlishvili, L.K. Burr Hole Microsurgery in Treatment of Patients with Intracranial Lesions: Experience of 44 Clinical Cases. Surg Neurol Int 2020, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Krötz, M.; Linsenmaier, U.; Kanz, K.G.; Pfeifer, K.J.; Mutschler, W.; Reiser, M. Evaluation of Minimally Invasive Percutaneous CT-Controlled Ventriculostomy in Patients with Severe Head Trauma. Eur Radiol 2004, 14, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Zumofen, D.; Regli, L.; Levivier, M.; Krayenbühl, N. Chronic Subdural Hematomas Treated by Burr Hole Trepanation and a Subperiostal Drainage System. Neurosurgery 2009, 64, 1116–1121. [Google Scholar] [CrossRef]
- Feigl, G.C.; Staribacher, D.; Britz, G.; Kuzmin, D. Minimally Invasive Approaches in the Surgical Treatment of Intracranial Meningiomas: An Analysis of 54 Cases. Brain Tumor Res Treat 2024, 12, 93–99. [Google Scholar] [CrossRef]
- Pitskhelauri, D.I.; Konovalov, A.N.; Shekutev, G.A.; Rojnin, N.B.; Kachkov, I.A.; Samborskiy, D.Y.; Sanikidze, A.Z.; Kopachev, D.N. A Novel Device for Hands-Free Positioning and Adjustment of the Surgical Microscope. J Neurosurg 2014, 121, 161–164. [Google Scholar] [CrossRef]
- Pitskhelauri, D.; Konovalov, A.; Kudieva, E.; Bykanov, A.; Pronin, I.; Eliseeva, N.; Melnikova-Pitskhelauri, T.; Melikyan, A.; Sanikidze, A. Burr Hole Microsurgery for Intracranial Tumors and Mesial Temporal Lobe Epilepsy: Results of 200 Consecutive Operations. World Neurosurg 2019, 126, e1257–e1267. [Google Scholar] [CrossRef]
- Vespa, P.; Hanley, D.; Betz, J.; Hoffer, A.; Engh, J.; Carter, R.; Nakaji, P.; Ogilvy, C.; Jallo, J.; Selman, W.; et al. ICES (Intraoperative Stereotactic Computed Tomography-Guided Endoscopic Surgery) for Brain Hemorrhage: A Multicenter Randomized Controlled Trial. Stroke 2016, 47, 2749–2755. [Google Scholar] [CrossRef]
- Chen, J.W.; Paff, M.R.; Abrams-Alexandru, D.; Kaloostian, S.W. Decreasing the Cerebral Edema Associated with Traumatic Intracerebral Hemorrhages: Use of a Minimally Invasive Technique. Acta Neurochir Suppl 2016, 121, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Labib, M.A.; Shah, M.; Kassam, A.B.; Young, R.; Zucker, L.; Maioriello, A.; Britz, G.; Agbi, C.; Day, J.D.; Gallia, G.; et al. The Safety and Feasibility of Image-Guided BrainPath-Mediated Transsulcul Hematoma Evacuation: A Multicenter Study. Neurosurgery 2017, 80, 515–524. [Google Scholar] [CrossRef]
- Sujijantarat, N.; Tecle, N.E.; Pierson, M.; Urquiaga, J.F.; Quadri, N.F.; Ashour, A.M.; Khan, M.Q.; Buchanan, P.; Kumar, A.; Feen, E.; et al. Trans-Sulcal Endoport-Assisted Evacuation of Supratentorial Intracerebral Hemorrhage: Initial Single-Institution Experience Compared to Matched Medically Managed Patients and Effect on 30-Day Mortality. Oper Neurosurg 2018, 14, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Mandel, M.; Tutihashi, R.; Li, Y.; Rosi, J.J.; Ping Jeng, B.C.; Teixeira, M.J.; Figueiredo, E.G. MISIAN (Minimally Invasive Surgery for Treatment of Unruptured Intracranial Aneurysms): A Prospective Randomized Single-Center Clinical Trial With Long-Term Follow-Up Comparing Different Minimally Invasive Surgery Techniques with Standard Open Surgery. World Neurosurg 2021, 151, e533–e544. [Google Scholar] [CrossRef]
- Glick, H.A.; Polsky, D.; Willke, R.J.; Schulman, K.A. A Comparison of Preference Assessment Instruments Used in a Clinical Trial: Responses to the Visual Analog Scale from the EuroQol EQ-5D and the Health Utilities Index. Med Decis Making 1999, 19, 265–275. [Google Scholar] [CrossRef] [PubMed]
- McCauley, S.R.; Wilde, E.A.; Anderson, V.A.; Bedell, G.; Beers, S.R.; Campbell, T.F.; Chapman, S.B.; Ewing-Cobbs, L.; Gerring, J.P.; Gioia, G.A.; et al. Recommendations for the Use of Common Outcome Measures in Pediatric Traumatic Brain Injury Research. J Neurotrauma 2012, 29, 678–705. [Google Scholar] [CrossRef]
- Jennett, B. The Glasgow Coma Scale: History and Current Practice. Trauma 2002, 4, 91–103. [Google Scholar] [CrossRef]
- Wilson, E.A.; Sills, G.J.; Forrest, G.; Brodie, M.J. High Dose Gabapentin in Refractory Partial Epilepsy: Clinical Observations in 50 Patients. Epilepsy Res. 1998, 29, 161–166. [Google Scholar] [CrossRef]
- McMillan, T.; Wilson, L.; Ponsford, J.; Levin, H.; Teasdale, G.; Bond, M. The Glasgow Outcome Scale - 40 Years of Application and Refinement. Nat Rev Neurol 2016, 12, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.; Pfefferkorn, T.; Ebrahimi, C.; Ottomeyer, C.; Fesl, G.; Bender, A.; Straube, A.; Pfister, H.-W.; Heck, S.; Tonn, J.-C.; et al. Long-Term Neurological Outcome and Quality of Life after World Federation of Neurosurgical Societies Grades IV and V Aneurysmal Subarachnoid Hemorrhage in an Interdisciplinary Treatment Concept. Neurosurgery 2017, 80, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Algburi, H.A.; Ismail, M.; Mallah, S.I.; Alduraibi, L.S.; Albairmani, S.; Abdulameer, A.O.; Alayyaf, A.S.; Aljuboori, Z.; Andaluz, N.; Hoz, S.S. Outcome Measures in Neurosurgery: Is a Unified Approach Better? A Literature Review. Surg Neurol Int 2023, 14, 61. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver Agreement for the Assessment of Handicap in Stroke Patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Timmermann, C. “Just Give Me the Best Quality of Life Questionnaire”: The Karnofsky Scale and the History of Quality of Life Measurements in Cancer Trials. Chronic Illn 2013, 9, 179–190. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Minimally invasive neurosurgery (MIN) In traumatic brain injury (TBI).
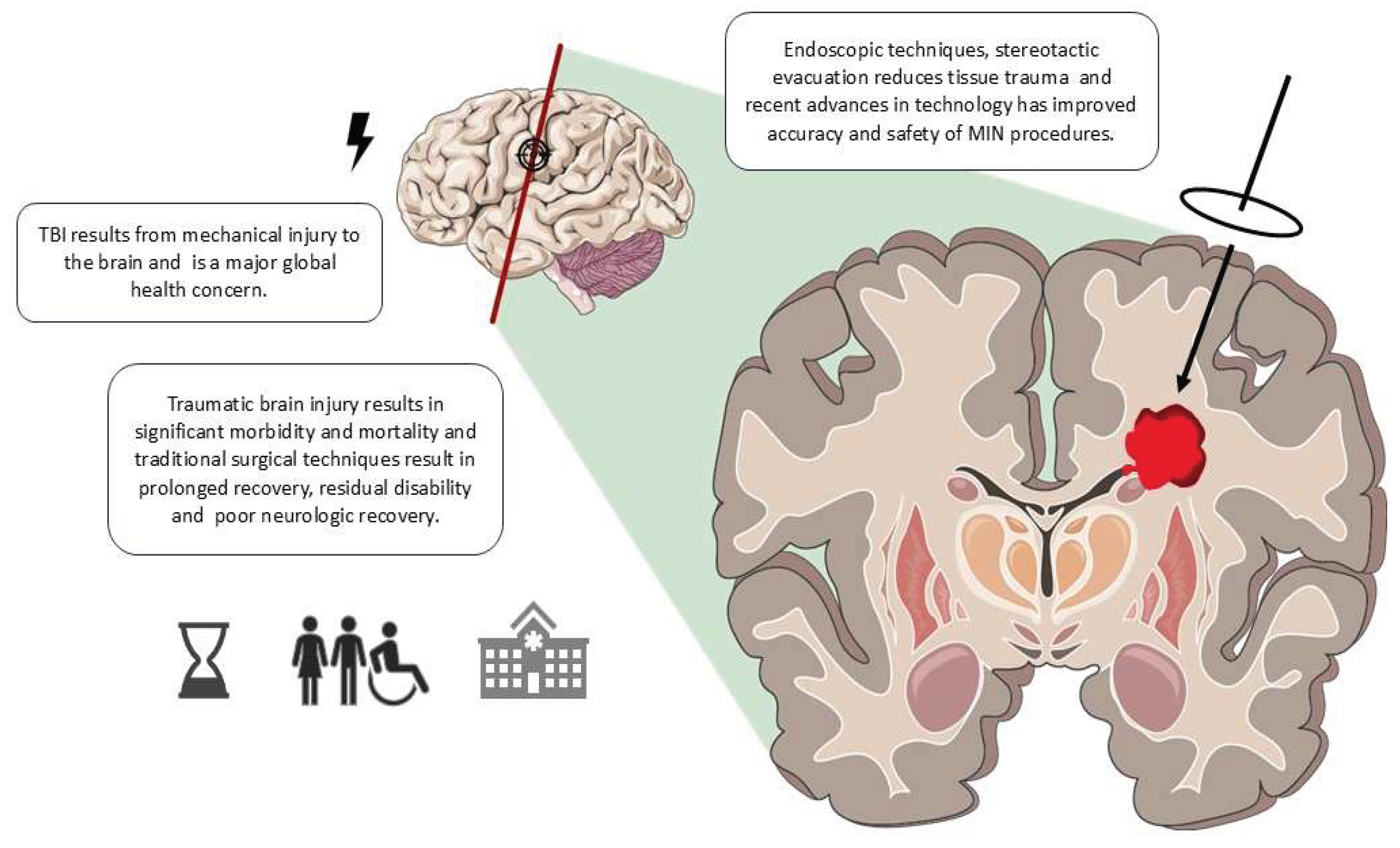
Figure 2.
Anatomical diagram of brain regions typically affected by traumatic brain injury, with labels indicating areas targeted by minimally invasive neurosurgery (MIN). Abbreviations: AI, artificial intelligence; CT, computed tomography; IVH, intraventricular hemorrhage; MRI, magnetic resonance imaging; SDH, subdural hemorrhage.
Figure 2.
Anatomical diagram of brain regions typically affected by traumatic brain injury, with labels indicating areas targeted by minimally invasive neurosurgery (MIN). Abbreviations: AI, artificial intelligence; CT, computed tomography; IVH, intraventricular hemorrhage; MRI, magnetic resonance imaging; SDH, subdural hemorrhage.
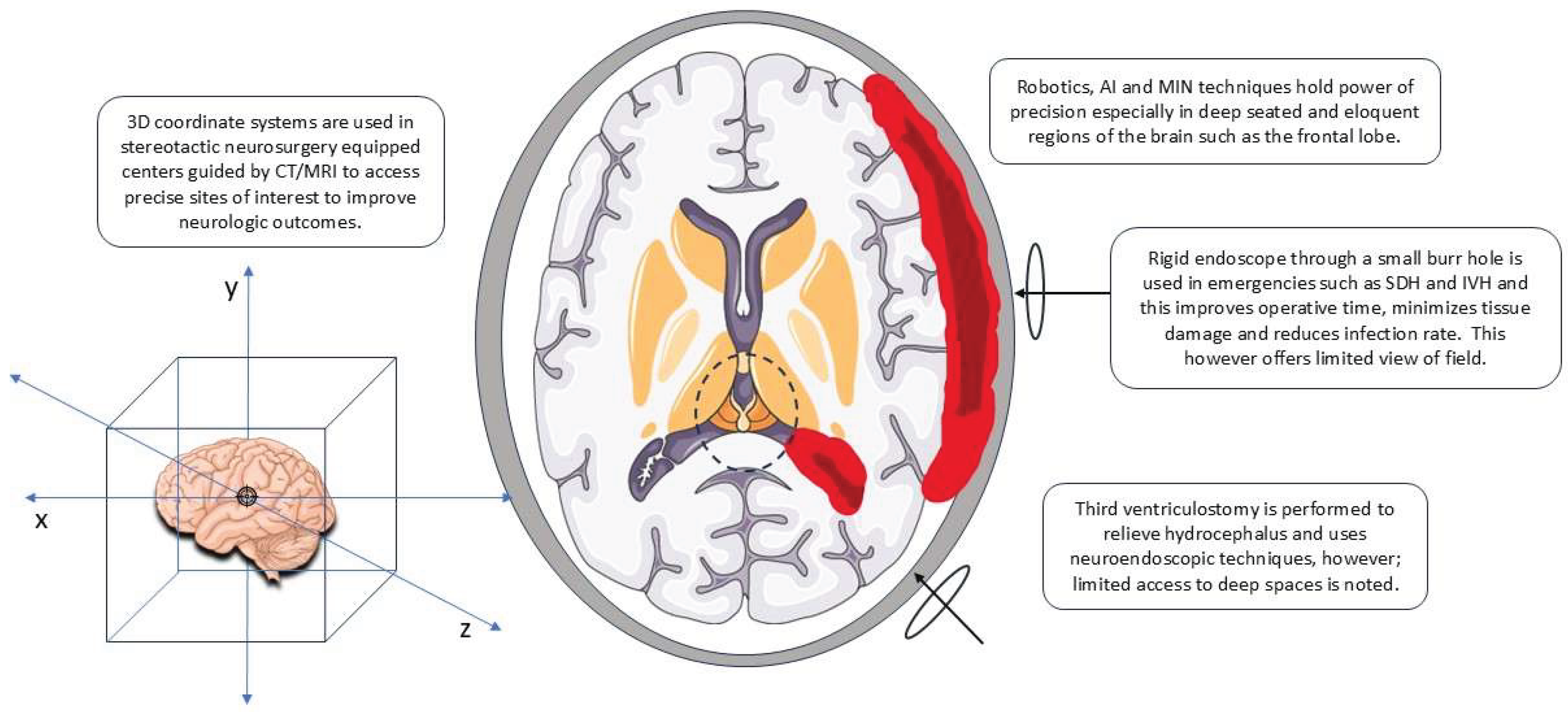
Figure 3.
Conceptual model of a personalized neurosurgical approach integrating patient data.
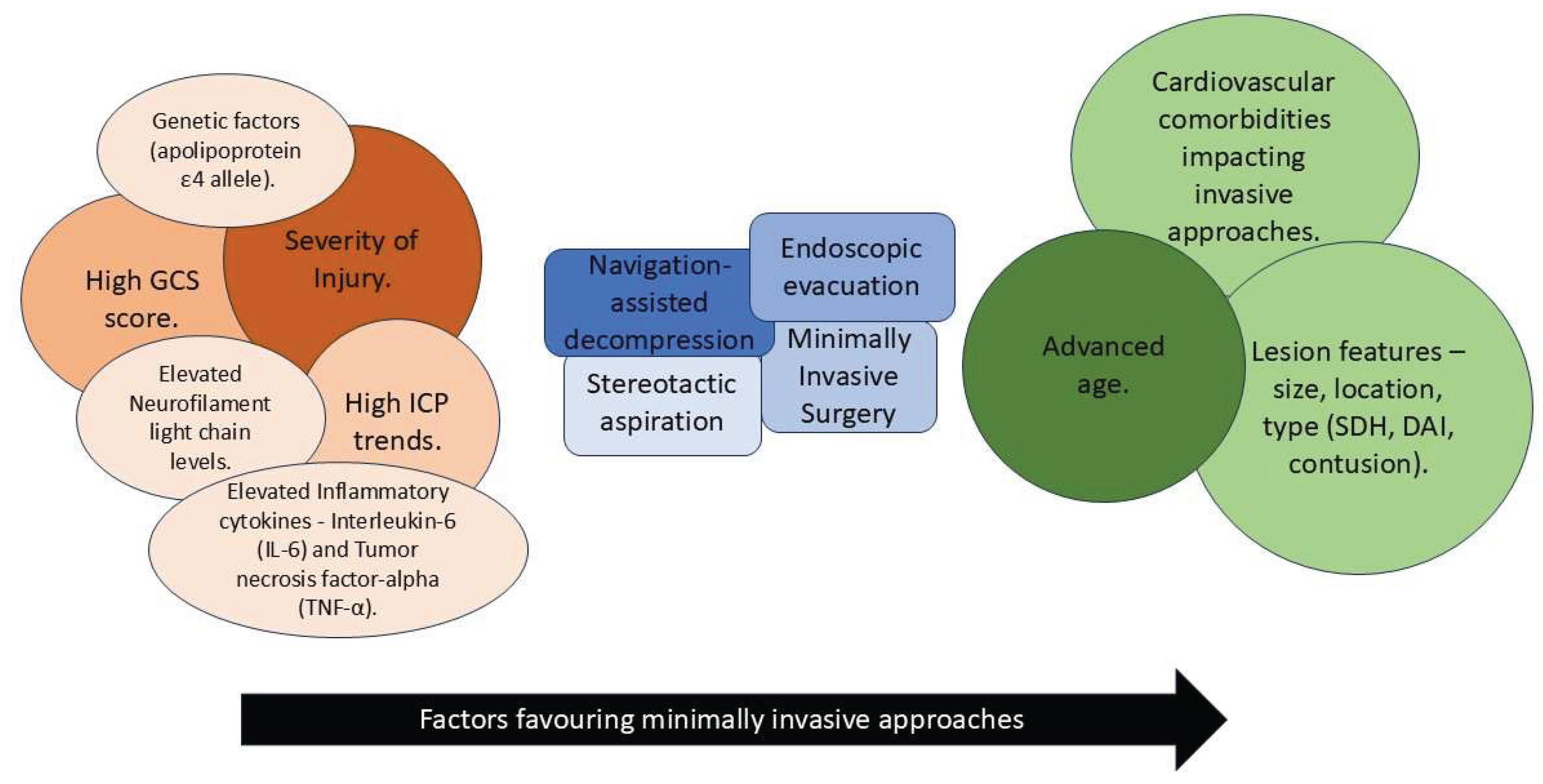
Figure 4.
Complications of minimally invasive neurosurgery in traumatic brain injury patients.
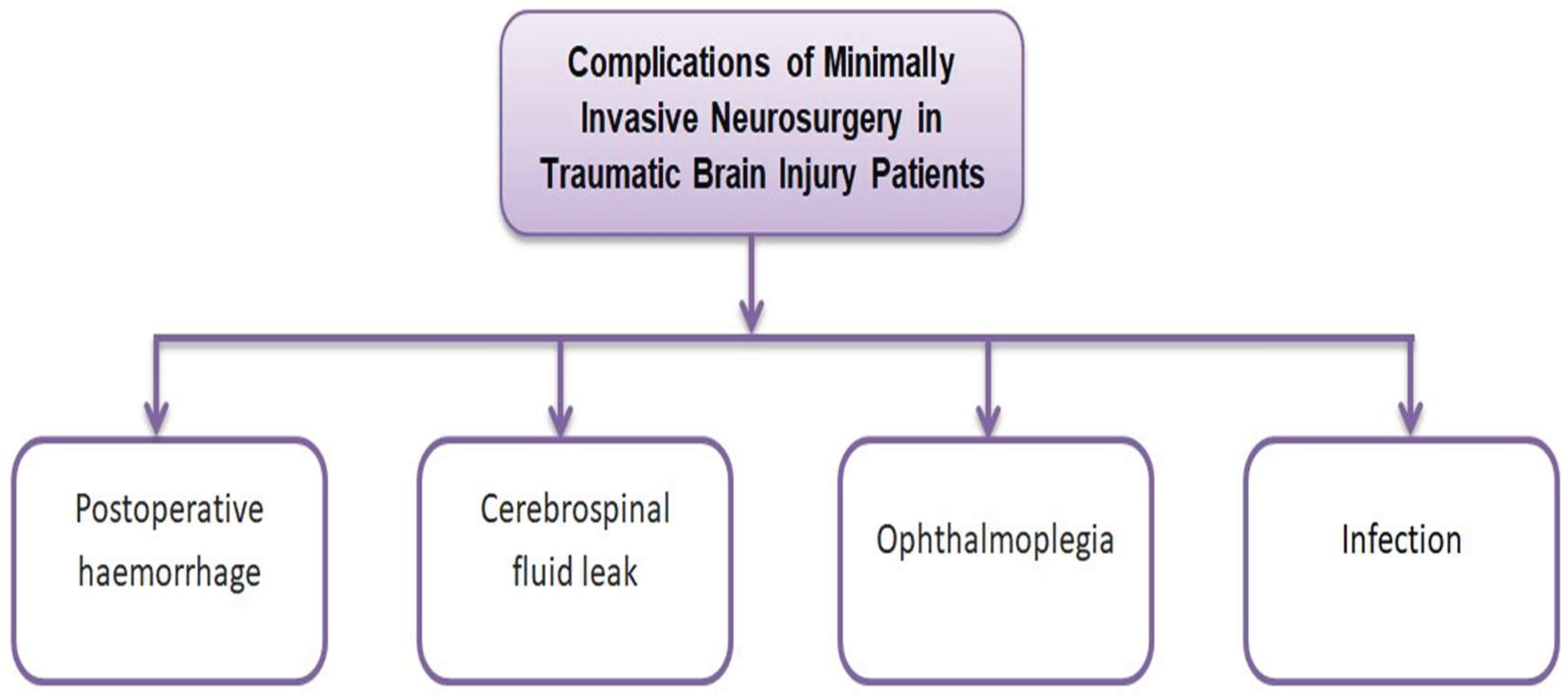

Table 1.
Statistical comparison of neurological outcomes from recent studies.
| Reference | Approach | Functional/ Cognitive outcomes | QoL/ Daily activities |
|---|---|---|---|
| Li et al. [42] | Neuroendoscopy MIN vs. traditional craniotomy | Higher MoCA cognitive scores; better limb motor and NIHSS/GCS scores in MIN group (p < 0.05) | Barthel Index and quality-of-life domains (physiological, psychological, social) significantly better in MIN group |
| Liu et al. [43] | MIN vs. craniotomy | MIN group had higher 1-year GOSE (4.0 vs. 3.1, p = 0.027) and better estimated mRS (p = 0.0427) | Lower morbidity (8.7% vs. 30.8%), and similar hospital/ICU stay |
| Xia et al. [44] | MIN vs. craniotomy | MIN associated with higher rate of “good recovery” (OR 2.27, p-value significant) | No direct QoL metrics, but functional recovery better |
| Zhou et al. [45] | Stereotactic MISPT vs. conventional craniotomy | Similar preoperative GCS, but 1-year GOS, mRS, BI significantly better in MISPT group (p < 0.001) | BI improved—indicative of better daily living ability |
| Xu et al. [46] | Endoscopic or stereotactic aspiration vs. craniotomy | For deep supratentorial hemorrhage: favorable outcome rates ~30% MIN vs. ~15% craniotomy (P = 0.001) | Improved functional outcomes imply better quality of life/daily functioning |
Abbreviations: BI, Barthel index; GCS, Glasgow Coma Scale; GOS, Glasgow Outcome Scale; GOSE, Glasgow Outcome Scale–Extended; ICU, Intensive Care Unit; MIN, Minimally Invasive Neurosurgery; MISPT, Minimally Invasive Stereotactic Puncture and Thrombolysis; MoCA, Montreal Cognitive Assessment; mRS, Modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; OR, Odds Ratio; QoL, Quality of Life.
Table 2.
Domains and factors associated with traumatic brain injury outcomes.
| Domain | Factors | Associated with outcome |
|---|---|---|
| Patient-related factors | Age, gender, race | Age: conflicting associations with poor outcomes (linked to both younger and older age, or no association); varies by outcome type. Gender: female patients are generally associated with poorer outcomes than males. Race: black patients tend to have poorer outcomes compared to white and Asian patients. |
| Life style | Smoking: associated with generally poorer outcomes. Alcohol use: linked to increased pain, depressive symptoms, PTSD severity, and reduced physical mobility. | |
| Co-morbidities | Obesity: associated with increased post-concussive symptoms. Migraine/ headache: linked to poorer outcomes. Anxiety/ depression: significant predictors of post-traumatic headache. Vasculopathy comorbidities: primary determinants of post-traumatic seizures, surgical outcomes, and discharge status. |
|
| Biomarkers | Systolic blood pressure >90 mmHg: associated with favorable outcomes. Oxygen saturation >90%: linked to favorable outcomes. Elevated arrival temperature: associated with favorable outcomes. Swirl sign: Indicative of expansive intracranial hematomas. APOE-ε4 Allele: Associated with delayed verbal memory deficits. | |
| Injury-related factors | Number of traumas | Multiple injuries: associated with worse outcomes compared to single trauma. |
| Mechanism of injury | Disorder of consciousness: associated with high-velocity injuries and intracranial hemorrhages. Early post-traumatic seizures: linked to low falls, hemorrhages, and greater injury severity. | |
| Severity of injury and inside damage | Disorder of consciousness: associated with intraventricular hemorrhages. Early post-traumatic seizures: linked to subdural/subarachnoid hemorrhages and injury severity. Surgical decision factors: based on hematoma size, cisternal compression on initial scan, and changes in GCS. | |
| Intervention-related factors | Surgery related factors | Surgery: generally associated with reduced risk of poor outcomes in TBI. Timing of surgery: evidence is conflicting regarding its impact on outcomes. Minimally invasive surgery: linked to shorter hospital stays and operative times; however, one study found no significant difference in outcomes compared to traditional surgery. |
| Other interventions | ICU admission: associated with poorer outcomes. Echocardiogram: linked to reduced mortality. Aspirin use: associated with lower mortality. Dysphagia interventions: increased interventions correlated with reduced likelihood of achieving full oral intake. | |
| Post-interventional care and complications | Hypothermia, seizures, hypotension, shock, low GCS: associated with increased mortality and complications. Elevated hemoglobin: linked to better outcomes. Mechanical ventilation: associated with higher mortality risk. Feeding tubes, spasticity, CSF leakage: predictors of increased mortality. | |
| Others | Environmental factors | Impact well-being and quality of life in TBI patients. |
| Biomarkers after injury | NGF↑, DCX↑, NSE↓: early elevated NGF and DCX, and reduced NSE levels, associated with better neurological outcomes. Complement C9 (CSF) and factor B (serum): identified as predictors of clinical outcomes. | |
Abbreviations: APOE, apolipoprotein E; DCX, doublecortin; GCS, Glasgow coma scale; ICU, intensive care unit; NGF, nerve growth factor; NSE, neuron-specific enolase; PTSD, post-traumatic stress disorder; TBI, traumatic brain injury.
Table 3.
Summary of case reports on endoscopic hematoma evacuation for acute subdural hematoma.
| References | Neurological treatment | Neurosurgery treatment | General outcome | Additional outcomes |
|---|---|---|---|---|
| Arai et al. [93] | Lacosamide, diazepam, fosphenytoin, and phenobarbital. | Endoscope-assisted acute subdural hematoma evacuation. | No effect from medication alone; full recovery followed surgery and drug therapy. | Consciousness improved; no neurological deficits; near-total hematoma cleared on CT (day 1); mRS 4 at discharge due to diffuse atrophy. |
| Tanaka et al. [94] | Antithrombotics were paused pre-operatively; restarted with antiplatelets 1 week post-operatively based on the condition. | Endoscopic hematoma evacuation. | Satisfactory outcome with no complications or rebleeding. | Op time: 61–143 min; 2 cases of elevated ICP; hospital stay: 5–250 days; mortality: 22.2%. |
| Codd et al. [95] | Prophylactic levetiracetam (seizures). | Endoscopic burr hole evacuation. | Good functional recovery; seizure-free by day 11 post-op. | Initially unresponsive; by day 4, fully oriented and mobile. Discharged day 11, neurologically intact. |
| Kuge et al. [96] | Mannitol infusion for consciousness recovery. | Endoscopic evacuation for acute subdural hematoma. | Endoscopic evacuation for acute subdural hematoma. | Post-op symptoms significantly improved. |
Table 4.
Functional outcome scales commonly used in traumatic brain injury.
| Scale | Aim | Main application | Alternative applications | References |
|---|---|---|---|---|
| Glasgow outcome scale (GOS) | Assesses functional recovery after severe brain injury | Severe brain injury following TBI | Intracranial aneurysms, tumors, strokes, and cranioplasty | Jennett et al. [129] |
| Modified Rankin scale (mRS) | Classifies functional recovery after cerebrovascular accident at discharge | Assesses cerebrovascular disease in adults (≥60) at discharge or referral | Used in aneurysms, general brain injury, hypothermia trials, sarcopenia, spinal meningiomas, and pediatric transverse myelitis | van Swieten et al. [134] |
| Karnofsky performance scale (KPS) | Assesses functional status in tumor patients | Tumors and cancers, primarily in neuro-oncology and post-treatment settings | Used measure of disability, particularly in palliative care, geriatrics, osteoarthritis, and post-revascularization surgery settings | Timmermann et al. [135] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



