Submitted:
31 July 2025
Posted:
01 August 2025
You are already at the latest version
Abstract
The purpose of this pilot study was to develop and characterize an in vivo porcine model of oxalate-induced renal injury using intravenous infusion of sodium oxalate (NaOx). 2 experimental regimens were developed to replicate acute and chronic hyperoxaluria. In the acute model, 3 different doses of 1% NaOx were administered over 15 hours, resulting in a dose-dependent increase in plasma oxalate concentration (Cmax: 42.4-122.4 µM) and transient hyperoxaluria, with a return to baseline values 6-8 hours after stopping the infusion of NaOx solution. In the chronic model, repeated infusions of NaOx for 7-11 days led to persistent hyperoxalemia (up to 302.4 µM), decreased appetite and increasing renal failure. Histological analysis revealed dose-dependent calcium oxalate (CaOx) deposits in renal tissue (1.85%-9.55% of renal surface area), consistent with moderate to severe nephrocalcinosis. The model represents the key clinical features of both acute kidney injury and the progressive nephrocalcinosis observed in primary hyperoxaluria and oxalaturia. Due to the physiological similarity between pigs and humans, the proposed porcine model is valuable for studying the pathophysiology of oxalate excess and for testing the efficacy of new therapies to counteract its toxicity.
Keywords:
hyperoxaluria
; hyperoxalemia
; nephrolithiasis
; pig model
; sodium oxalate
; calcium oxalate
1. Introduction
Hyperoxaluria is a pathological disorder characterized by the increased urinary excretion of oxalates. Under physiological conditions, oxalates are formed as the end products of the hepatic metabolism of glyoxylate, amino acids and vitamins (including glycine, hydroxyproline and vitamin C), and their renal excretion and urinary levels remain constant (less than 40 mg/24h) [1,2,3]. Primary hyperoxaluria (PH) is a rare congenital condition caused by abnormalities of glyoxylate metabolism in the liver. On the other hand, secondary hyperoxaluria is associated with environmental factors such as a high oxalate diet and diseases (including diabetes mellitus, obesity or Crohn’s disease) that can lead to excessive oxalate absorption in the intestines [4,5,6]. Regardless of the etiology, elevated endogenous or exogenous oxalate concentrations in the blood result in increased urinary oxalate excretion, leading to calcium oxalate (CaOx) crystal formation and precipitation, nephrolithiasis, nephrocalcinosis, and consequently chronic kidney disease (CKD) [7].
Preclinical studies of nephrolithiasis and hyperoxaluria require the use of appropriate animal models, which are essential for understanding the pathophysiology of the diseases and testing potential therapies. The incidence of kidney stones disease (KSD) has increased by about 50% in the past three decades, resulting in a global prevalence of 13% [8,9]. Kidney stones can be divided into four groups, of which calcium-based stones, including CaOx, are the most common, with hyperoxaluria cited as a major risk factor [10]. To date, several models of hyperoxaluria have been developed, which differ in terms of method of induction, disease course and animal species. Mice and rats are most commonly used for this purpose, mainly due to their low maintenance costs, availability and genetic engineering capabilities. However, rodent models have significant limitations - their kidneys are mono-pyramidal in structure, and they differ from humans in terms of oxalate metabolism, body size and glomerular filtration rate (GFR) dynamics, among other factors. Moreover, rodents are becoming increasingly inbred, causing their genetic diversity to decrease significantly [Shanks et al., 2009]. This has been listed as one reason for caution in extrapolating results to people, who demonstrate higher genetic variety [2,11].
For these reasons, there has been a steadily growing interest in large animal models, especially pigs, which have anatomical and physiological similarities to humans. Pigs have multi-pyramidal kidneys, with each medullary pyramid forming multiple separate papillae, allowing for a more reliable representation of human kidney processes [12]. The physiology of the kidneys, including maximum urine concentration, total renal blood flow, GFR, as well as similar body size and excretory parameters, allow diagnostic procedures to be carried out in a manner analogous to clinical conditions [2,13]. Therefore, we hypothesized that the domestic pig (Sus scrofa domestica) represents a suitable research model of acute and chronic hyperoxaluria induced by intravenous infusion of sodium oxalate (NaOx) solution. The use of these models allows not only quantitative analysis of oxalate levels in plasma and urine, but also histopathological evaluation of the kidneys. Unlike substances that require metabolism or take a long time to have an effect, including ethylene glycol (EG) and L-hydroxyproline (HYP), NaOx is a direct source of oxalate, and its intravenous administration results in an immediate increase in its plasma concentration. By assessing both the course of acute kidney injury and long-term changes in the organ’s structure, these models provide a better understanding of oxalate-dependent mechanisms of kidney injury and can be used to evaluate new therapeutic strategies.
2. Results
2.1. In Vivo Model of Mild, Moderate and Severe Hyperoxalemia
2.1.1. Serum Oxalate Concentration
The level of oxalate in the blood increased steadily and was dependent on the concentration of oxalate infused to the pigs (Figure 1A). A significant increase in plasma oxalate levels was observed following oxalate infusions, regardless of dose, with maximal concentration (Cmax) reaching 42.4±3.5, 69.6±0.2 and 122.4±4.9 μM following infusion with the low, medium and high dose, respectively. Plasma oxalate levels were generally stable 1 hour after the start of the infusion, until the end (14.5 hours). A clear significant dose-dependency was observed in the area under the curves (AUC) of the plasma oxalate levels reached and the dose of oxalate infused (Figure 1B). Plasma oxalate levels returned to baseline values ca 6-8 h after the oxalate infusion was stopped.
2.1.2. Urinary Oxalate Concentration
Urinary oxalate excretion was also monitored before, during and after oxalate infusion. As shown in Figure 2 oxalate excretion peaked during the 15-hour continuous oxalate infusion and was not dependent on the concentration of oxalate infused to the pigs. Urinary oxalate returned to baseline levels within 24 hours following the end of the oxalate infusion.
2.2. In Vivo Model of Chronic Hyperoxaluria
2.2.1. Serum Oxalate Concentration
Pigs receiving the “high dose” oxalate infusion were infused with 6 ml of 1% NaOx solution every 30 minutes. Serum oxalate concentration increased rapidly, reaching 302.4 ±11.46 μM on the 7th day (Figure 3). The deteriorating health condition of the pigs, including lack of appetite, reduced water consumption, significantly reduced activity, apathy, vomiting, and no or minimal diuresis, did not allow the study to continue. The pigs were euthanized on the 7th day.
Pigs receiving the “low dose” oxalate infusion were infused with 2 ml of 1% NaOx solution every 30 minutes. After 7 days, the serum oxalate concentration reached 176.1±181.7 mM (Figure 3). The continuous low dose oxalate infusion also induced severe hyperoxalemia and serum oxalate levels on day 11 were in the range of between 130.9 – 167.9 mM (Figure 3). The oxalate infusions were stopped on day 11 in pigs from this group as a result of the poor health condition of the pigs, which manifested as weakness and vomiting.
2.2.2. Daily Feed Intake
The amount of food consumed by the pigs was measured throughout the experimental period (Figure 4). In the pigs receiving the Low Dose infusion, there was a significant reduction in food intake by 74.6% on day 13 and by 100% on day 14, compared to the recommended feed intake (990 g). In pigs receiving the High Dose, oxalate infusion conducted at a rate of 6 ml/30 min resulted in a significant decrease in food intake, with a 49.3% reduction on day 3, 70.7% on day 4, 80.4% on day 5, and 100% on day 6 of the experimental period.
2.2.3. Oxalate Deposits in the Kidney Tissues
Each histologically evaluated sample contained renal cortex and medulla from 2 different parts of each kidney (left and right, Figure 5). Figure 6 shows the median percentage of calcium oxalate in the kidneys of pigs from the High Dose group after 7 days of oxalate infusion, which was 4 times higher than that observed in pigs from the Low Dose group after 11 days of infusion and 3 washout days. The median oxalate deposition in the kidney tissues of pigs from the High Dose Group reached 9.55%, which could be considered as severe nephrocalcinosis, while in the Low Dose Group the median percentage of oxalates was 1.85%, which could be considered as moderate nephrocalcinosis (Figure 6).
3. Discussion
The aim of Experiment 1 was to evaluate the effectiveness of a porcine model in reproducing acute hyperoxalemia and hyperoxaluria using an intravenous infusion of 1% NaOx. The intravenous administration of NaOx effectively induced acute hyperoxalemia in the pigs in a dose-dependent manner, reflected both in the Cmax and AUCs values of plasma oxalate, which were stable and reversive. Previous studies on hyperoxalemia mainly make use of animal models which require prolonged exposure to the agent and do not reflect the sharp and rapid increases in plasma oxalate concentrations (POx) observed in the present study. Ethylene glycol (EG), often used in rodent models, is metabolized in the liver, indirectly yielding oxalate, but its toxicity to other organs (especially the liver and CNS), as well as the risk of metabolic acidosis, limits its use [14]. Verhulst et al. [15] used EG in drinking water (0.75%) to induce primary hyperoxaluria (PH) in a rat model, leading to a significant increase in POx. In contrast to our study, the level did not significantly increase until week 2 of the experiment, and a plateau was not reached until week 6. Oxalate exposure can be achieved with a high oxalate diet, as in the study by Crestani et al. [16], but this method requires a longer time to induce hyperoxalemia and there is a high variability in the bioavailability of dietary oxalate. The method of intravenous infusion of NaOx used in our study, as a direct source of oxalate, allows precise control of oxalate concentration in the blood and its duration of action, and the rate of reaching a plateau within 1 hour after the start of infusion indicates high bioavailability and immediate action. Our results are in agreement with an earlier study by De Araujo et al. [3] in a rat model in which administration of NaOx (7 mg/100 g i.p.) was shown to cause features of acute kidney injury (AKI), including inflammatory infiltration and degeneration of renal tubular epithelium, within 24 hours.
Another important aspect of the presented study is the parallel analysis of urinary oxalate excretion, which confirms the physiological renal response to hyperoxalemia. Despite the differences in dosing in the acute model, peak oxalate excretion was similar between the groups and occurred mainly during the oxalate infusion, but returned to baseline levels within 24 hours after the infusion ended. This is consistent with a study by Penniston et al. [2] in a porcine model in which hyperoxaluria was induced by feeding the pigs a diet containing hydroxyproline (HYP). The authors observed a dynamic response in pigs to the administration of exogenous oxalate in the form of increased urinary oxalate excretion and a repid return to homeostasis/baseline levels. In a study by Kaplon et al. [17], the addition of HYP to the diet of pregnant sows also led to an increase in urinary oxalate excretion, with a peak on day 3 and a gradual return to baseline on day 6. Khan et al. [18,19,20] reported an increase in urinary oxalate excretion after a single injection of NaOx in mice and rats, followed by a decrease over the next 12 hours. In humans, a similar phenomenon occurs under physiological conditions, where the kidneys efficiently regulate plasma oxalate levels through glomerular filtration and tubular secretion, the latter mediated by the SLC26A anion exchanger and the Cl-/oxalate exchanger SLC26A6, unless they are damaged [21,22,23]. This result indicates a preserved compensatory capacity of the excretory system under controlled and brief exposure to NaOx.
The purpose of Experiment 2 was to evaluate the effectiveness of the porcine model in reproducing chronic hyperoxaluria using repeated intravenous infusions of 1% NaOx. In the High Dose group, maximum POx reached was 302.4 ± 11.46 µM after just 7 days of infusions, while in the Low Dose group the values were slightly lower, but still well above physiological norms. It is accepted that a decrease in GFR below 30-40 ml/min per 1.73 m2 of body surface area results in impaired renal excretion of oxalate and an increase in plasma oxalate concentration (normal limit 1-6 µM/L) [24] and can rapidly exceed the supersaturation threshold for calcium oxalate as levels >30 μmol/L are reached [25]. According to Perinpam et al. [26], in the diagnosis and monitoring of PH, enteric hyperoxaluria and urinary stone disease, in addition to parameters such as GFR or urinary oxalate excretion, POx should also be considered. In PH patients in end-stage renal disease (ESRD), plasma oxalate levels are usually higher than 80 µM/L, while in non PH hyperoxaluric patients, the POx level may range between 30-80 µM/L [1]. The increase in POx observed in our study is also consistent with clinical studies in humans [24], wherea significantly higher mean POx was observed in children with PH1 than in those without PH. Nevertheless, the POx values presented in our chronic study not only exceed the levels observed in acute clinical conditions, but are also consistent with the range noted in PH1 patients and exceed toxicity thresholds posing a high risk of developing systemic oxalosis, especially in ESRD patients [1,24]. The relationship between chronically elevated oxalate levels and the progression of CKD has been confirmed in population-based studies, where it was found that higher urinary oxalate excretion (upper quintile ≥27.8 mg/24h) significantly correlated with a more rapid decline in renal function and higher risk of ESRD [6]. Moreover, this was confirmed in the present study by clear clinical signs, especially in pigs in the High Dose groups, including apathy, vomiting and decreased appetite, with complete cessation of food intake. In studies on a rat model with induced hyperoxaluria, Verhulst et al. [15] and Crestani et al. [16] also found a significant reduction in food intake, but without such clear clinical signs as in our study. These symptoms correspond to those of the cachexia syndrome observed in the late stages of CKD and ESRD in humans. Thus, it can be concluded that this model allows modulation of the severity of changes depending on the dose and duration of infusion, which has important implications for studies on the toxic effects of oxaliplatin, as well as on the efficacy of interventional therapies.
This study shows that intravenous administration of NaOx leads to markedly different CaOx deposition in the kidneys, depending on the dose used. In the High Dose group, CaOx deposits occupied an average of 9.55% of the renal cross-sectional area, which can be classified as severe nephrocalcinosis. In the Low Dose group, the percentage was 1.85%, corresponding to moderate lesions. The significantly higher retention of CaOx crystals in the High Dose group is consistent with the higher POx levels in this group. A similar relationship between deposit accumulation and the severity of renal parenchymal damage has been observed in humans. Sayer et al. [7] showed that the presence of CaOx deposits in renal tubules correlates with epithelial damage, inflammatory infiltration and interstitial fibrosis, which can lead to permanent deterioration of renal function. This is consistent with our results, as the High Dose group not only had a higher percentage of the kidney surface occupied, but also clear clinical signs indicating deteriorating organ function. Additionally, under conditions of high POx, CaOx crystallization occurs within the renal tubules, particularly in their distal segments and in the renal medulla. A study by Khan [27] confirms that conditions in the terminal sections of the nephron (low pH, high calcium concentration, slower urine flow) promote the formation of deposits, which consequently leads to an inflammatory response and the initiation of fibrosis. Fargue et al. [23] showed that the presence of CaOx correlates with increased expression of pro-inflammatory cytokines and fibrosis mediators, leading to progressive loss of organ function. In our study, CaOx was found in both the cortex and medulla of the kidney, confirming that its distribution resembles that observed in humans [2]. A study by Mehra and Viswanathan [28] in which rats were given NaOx (2.5%) along with water for 4 weeks also found CaOx deposition in the kidneys, but the percentage of kidney surface area occupied by deposits was much lower than in our study. In contrast, in a study by Mandel et al. [29], in which pigs were fed HYP for 20 days, the formation of calcium oxalatepapillary deposits were observed, which may be precursors of kidney stones. In contrast to both studies, in our study we found kidney stones as early as day 7 (High Dose group) and day 14 (Low Dose group), greatly reducing the duration of the study and confirming the usefulness of this model for assessing the effects of oxalate toxicity on a macro- and microscopic scale.
The present study has limitations. Firstly, since our study was a pilot study, a small number of animals were used per group and an experiment on a larger group of animals and with more parameters to be evaluated, such as urine and blood creatinine levels, is certainly required. Secondly, the high dose of NaOx used in the chronic study may not be suitable for long-term studies, compared to methods such as HYP feeding or a high-oxalate diet, as high doses of NaOx have been associated with high toxicity and risk of death.
The results we presented here confirm that the porcine model allows us to reproduce both acute and chronic changes associated with hyperoxalemia and hyperoxaluria. The use of 1% NaOx not only allows us to induce nephrocalcinosis in a reproducible and dose-dependent manner, but also to study its functional and pathophysiological consequences. In addition, the pig, due to its similar anatomy and physiology to humans, provides a valuable model for translational research into new therapies for hyperoxalemia and hyperoxaluria and toxicity associated with excess oxalate.
4. Materials and Methods
4.1. Animals, Housing Conditions, Surgical Procedures
4.1.1. Bioethics
All experimental procedures were approved by the Malmö/Lund Ethics Review Committee on Animal Experiments, Lunds city court (Malmö/Lunds djurförsöksetiska nämnd, Lunds tingsrätt), Box 75, 221 00 Lund, Sweden. The research and care of animals was carried out in accordance with the principles for the care and use of experimental animals (Directive 2010/63/EU of the European Parliament and of the Council of 22 September 2010 on the protection of animals used for scientific purposes).
4.1.2. Animals and Housing
2 experiments were conducted on a total of 9 castrated male hybrid pigs ((Swedish breed × Yorkshire breed) × Hampshire breed), with an average age of 12 ± 2 weeks and an initial average weight of 12.1 ± 0.8 kg obtained from the Odarslöv research farm. Animals were maintained on a 12-hour day-night cycle, temperature 21-25°C, air exchanges 10-12/h and humidity 70 +/− 5%. The pigs were individually housed in 1.0 x 2.0 pens equipped with a dry feeding trough, a drinking nipple and a constant heating lamp (150W, 24h). They were allowed to move freely within their pens and had visual contact with each other.
4.1.3. Feed
All pigs were fed a grain-based feed for young growing pigs (53908 VÄXTILL 320 P BK, Lantmännen, Sweden). This diet is rich in calcium and magnesium, containing 61.4% carbohydrates, 17.6% crude protein, 12.4% water, 3.9% crude fiber, 3.5% crude fat and 5.1% ash, along with 0.46% calcium carbonate and 0.82 monocalcium phosphate. The daily feed intake was recalculated once a week, after the pigs were weighed, and was 4% of the animal’s current body weight, which corresponds to the amount eaten under standard pig feeding conditions. Pigs were fed twice a day at 09:00-10:00 and 17:00-18:00 (2% of bwt/meal).
4.1.4. Implantation of Central Access to the External Jugular Vein
Before surgery, the animals were premedicated intramuscularly with azaperone (2 mg/kg bwt) („Stresnil”, Janssen Pharmaceutica, Beerse, Belgium) and ketamine (20 mg/kg bwt) („Ketalar”, Parke-Davis, Morris Plains, New Jersey). The animals were anesthetized with a mixture of 1.5-3.0% isoflurane (Forene®, Abbot AB, Sweden), using a semi-open Komensaroff inhalation anesthesia system with an oxygen flow of 0.5 L/min (Medical Developments, Australia). The incision line was epidurally anesthetized with a 2% lidocaine solution (1mg/kg bwt) („Xylocaine 2%”, Aspen Pharma, Durban, RPA). The procedure was performed under aseptic conditions. Cannulas made of a 15 to 20 cm long silicone tube with a wall thickness of 0.22 mm (outer diameter 1.69 mm; inner diameter 1.47 mm) were inserted into the animals’ external jugular vein. Halfway through their length, the cannulas are equipped with 4 stops made of silicone glue, spaced approximately 1 cm apart. The incision was made along the angle of the mandible - shoulder joint. After dissecting the maxillary vein, just before its transition into the external jugular vein, a small (approximately 2 mm) incision was made. Then, a cannula was inserted into the vessel lumen to a depth of approximately 10 cm towards the heart, up to the first silicone stop. The vessel above the cannula was closed. The remaining stops were used to stabilize the long arm of the catheter in the tissues, which were inserted under the skin in the neck area approximately 7 cm from the base of the ear. Before suturing the surgical wound, ampicillin (Doctacillin®, Astra, Sweden) was administered topically at a dose of 25 mg per animal and buprenorphine (Tamgesic®, Schering-Plough, Belgium) at a dose of 15 mcg/kg bwt intramuscularly. The surgical wound was sutured with a mattress suture using size 0 non-absorbable sutures (Silk, Ethicon, Johnson and Johnson, Great Britain), which were removed 10 days after the procedure.
4.2. Experimental Design and Sample Collection
4.2.1. Experiment 1 – Animal Model of Acute Hyperoxalemia
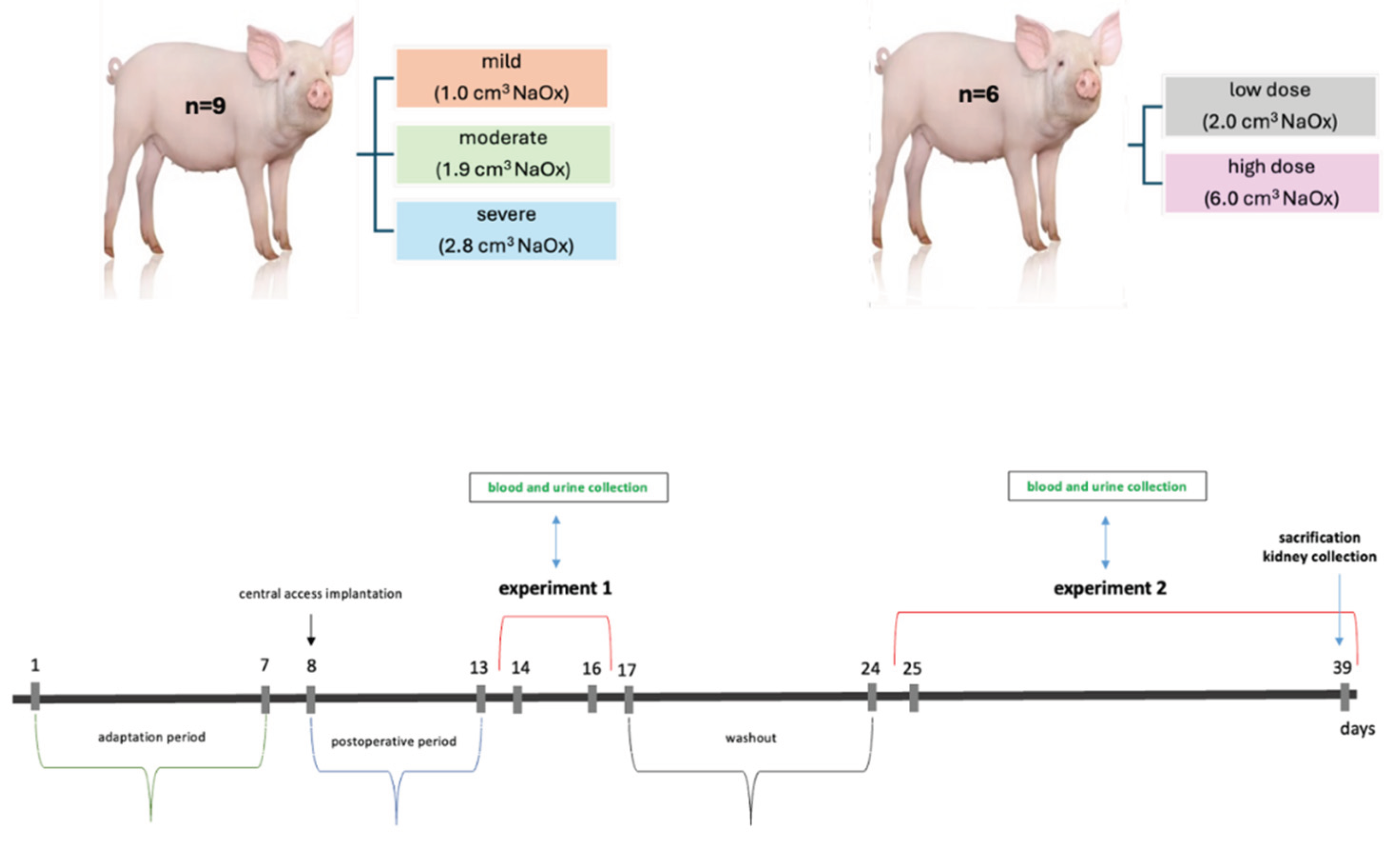
The experiment was conducted on 9 pigs, which were divided into 3 experimental groups (n=3 per group): mild, moderate and severe hyperoxalemia (Figure 7). Sodium oxalate solution (Sigma-Aldrich Chemicals, St. Louis, MO, USA) was prepared using sterile 0.9% NaCl to obtain a 1% isoosmotic solution. The solution was sterile filtered and administered intravenously by bolus injection of 1 ml (mild), 1.9 ml (moderate) or 2.8 ml (severe) via the jugular vein, every 15 minutes during a 15-hour period to obtain plasma oxalate concentrations similar to those observed in patients with hyperoxalemia and oxalosis (> 40mg/24h).
5 ml blood samples were collected from each animal one hour before the start of the experiment, one hour after the start of the infusion and every 4 hours during the infusion. Blood samples were also collected after infusion (at timepoint 20 and 24 h). Collected samples were transferred immediately into tubes with clotting activator (BD Vacutainer SST™, USA) and centrifuged (Multifuge 1, Heraeus, UK) at 3000 x g for 15 minutes at 4°C. The collected serum was stored in 1 mL aliquots at -20°C to determine the oxalate concentration per liter of blood using ion chromatography.
The animals’ daily urine was collected for 24 hours before the start of the experiment, during the infusion and then at 9 and 24 hours after the end of the infusion. Urine was acidified with 6N HCl to avoid the proliferation of bacterial flora and the formation of oxalate deposits. Urine volume was measured and then frozen (-22±2°C) to determine oxalate concentration. After 7 days from the end of experiment 1, 6 pigs were randomly chosen to be used in experiment 2.
4.2.2. Experiment 2 – Animal Model of Chronic Hyperoxaluria
The experiment was conducted on 6 pigs, which were divided into 2 experimental groups (n=3 per group) (Figure 7). Sodium oxalate (Sigma-Aldrich Chemicals, St. Louis, MO, USA) was made as a sterile 1% sodium oxalate concentration in 0.9% NaCl. The 1% sodium oxalate solution was infused into the external jugular vein by cyclically injecting a specified amount of the solution: 6 ml every 30 minutes in 3 pigs (high dose) and 2 ml/30minutes in the other 3 pigs (low dose). The infusion time of the oxalate solution was 24 hours and lasted for a maximum of 11 days.
To monitor the level of hyperoxalemia, blood samples were collected several times (0, 7, 11 and 14 days) during the 2 weeks of experimental period. Similar to experiment 1, the collected blood samples were prepared and stored at -20°C until further analysis by ion chromatography. During the experiment, the animals’ feed intake and clinical condition were monitored daily. At the end of the experiment, animals were sacrificed with sodium pentobarbital intravenous injection (140 mg/kg bwt) (Allfatal vet. Omnidea AB, Sweden) and kidneys were collected for histological analysis.
4.3. Ion Chromatography
An ICS- 900, CO-DV ion chromatograph (Thermo Scientific) was used to analyze oxalate concentrations in all samples. Serum was filtered through 3kDa centrifugal filters (VWR International, Stockholm, Sweden). Urine samples were acidified with 6N HCl to reach pH values <2. Urine samples were also filtered through 3kDa centrifugal filters (VWR International, Stockholm, Sweden). For ion chromatography the following columns were used: IonPack AG4A-SC (2x50 mm), IonPack AS4A-SC (2x250 mm), AMMS 300 supressor, mobile phase 1.8 mM Na2CO3/1.7 mM NaHCO3, flow rate 0.5 cm3/min, regenerant 75 mN H2SO4.
4.4. Histological Evaluation of Kidneys
In experiment 2, 10 3-cm kidney fragments were collected from each animal and fixed in 10% neutral buffered formalin for 24 h. Then, the tissue fragments were dehydrated in ethanol of increasing concentrations (50%, 70%, 80%, 90%, 96%, 99.8%) and embedded in paraffin according to standard histological techniques. Paraffin-embedded tissues were cut into 4-5 μm thickness sections using a rotor microtome and were evaluated using the Yasue method [30,31]. The analysis was performed using a light microscope (Axioskop 40, Zeiss, Jena, Germany) equipped with a digital camera (Coolpix B700, Nikon, Tokyo, Japan). All tissue samples were analyzed by a public domain Java image- processing program, Image J v.1.46 (National Institute of Health (NIH), Bethesda, Maryland, USA). The result is expressed as % of CaOx deposits in the tissue and presented as the sum of % CaOx positive areas from the cortex and medulla for each kidney. The severity of the nephrocalcinosis was graded using arbitrary units. Nephrocalcinosis was considered low if ≤1% of the kidney area was affected, moderate if 1-3% of the area was affected and severe if ≥3% of the area was affected.
4.5. Statistical Analysis
GraphPad Prism 10.5.0 (San Diego, CA, USA) was used for statistical analyses. Data were tested for normal (Gaussian) distribution using the Shapiro–Wilk normality test. Differences in investigated parameters were assessed using an unpaired t-test (data on plasma oxalate in High Dose Group, Chronic Experiment) or one-way ANOVA for the normally distributed datasets. For the data with non-Gaussian distribution (oxalate deposition in kidney tissue) the Mann-Whitney test was used. Normally distributed data are shown as Mean±SD (standard deviation), while data with non-Gaussian distribution are represented as Median±IQR (interquartile range). Differences were considered significant if p < 0.05.
Author Contributions
Conceptualization, D.S., T.J. and K.P.; methodology, O.F., S.K. and K.Z.; formal analysis, S.G.P., K.P., O.F., O.P., and D.S.; investigation, A.F., S.K., D.S. and K.Z.; resources, M.S. and P.W.; data curation, K.P., S.G.P., J.D., O.P., O.F., and D.S.; writing—original draft preparation, D.S. and T.J.; writing—review and editing, T.J., D.S. and J.D.; visualization, S.G.P., K.P., J.D., O.P., O.F., and D.S.; supervision, S.G.P and K.P.; project administration, T.J., P.W. and D.S.; funding acquisition, S.G.P. and K.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Anara AB.
Institutional Review Board Statement
All experimental procedures were approved by the Malmö/Lund Ethic Review Committee on Animal Experiments, Lunds city court (Malmö/Lunds djurförsöksetiska nämnd, Lunds tingsrätt), Box 75, 221 00 Lund, Sweden. The research and care of animals was carried out in accordance with the principles for the care and use of experimental animals (Directive 2010/63/EU of the European Parliament and of the Council of 22 September 2010 on the protection of animals used for scientific purposes).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors of this manuscript have the following competing interests: SGP and KP are the owners of Anara AB, Sweden. JD, MS and AF were employed by Anara AB, Sweden during the experiment. All other authors declare no competing interests.
Abbreviations
| PH | Primary hyperoxaluria |
| CaOx | Calcium oxalate |
| CKD | Chronic kidney disease |
| KSD GFR NaOx EG HYP POx AKI ESRD |
Kidney stones Glomerular filtration rate Sodium oxalate Ethylene glycol Hydroxyproline Plasma oxalate concentration Acute kidney injury End-stage renal disease |
References
- Bhasin, B.; Ürekli, H.M.; Atta, M.G. Primary and secondary hyperoxaluria: Understanding the enigma. World Journal of Nephrology 2015, 6, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Penniston, K.L.; Patel, S.R.; Schwahn, D.J.; Nakada, S.Y. Studies using a porcine model: what insights into human calcium oxalate stone formation mechanisms has this model facilitated?.Urolithiasis 45, 109–125 (2017). [CrossRef]
- De Araújo, L.; Costa-Pessoa, J. M.; de Ponte, M. C.; Oliveira-Souza, M. Sodium-oxalate induced acute kidney injury associated with glomerular and tubulointerstitial damage in rats. Frontiers in Physiology 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Meydan, N.; Barutca, S.; Caliskan, S.; Camsari, T. Urinary stone disease in diabetes mellitus. Scandinavian Journal of Urology and Nephrology 2003, 37, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Al Salhi, Y.; Tasca, A.; Palleschi, G.; Fuschi, A.; De Nunzio, C.; Mazzaferro, S.; Pastore, A.L. Obesity and kidney stone disease: a systematic review. Minerva Urology and Nephrology 2018, 70, 393–400. [Google Scholar] [CrossRef]
- Waikar, S.S.; Srivastava, A.; Palsson, R.; Shafi, T.; Hsu, C.Y.; Sharma, K.; Lash, J.P.; Chen, J.; He, J.; Lieske, J.; Xie, D.; Zhang, X.; Feldman, H.I.; Curhan, G.C. Association of urinary oxalate excretion with the risk of chronic kidney disease progression. JAMA Internal Medicine 2019, 179, 542–551. [Google Scholar] [CrossRef]
- Sayer, J. A.; Carr, G.; Simmons, N.L. Nephrocalcinosis: molecular insights into calcium precipitation within the kidney. Clinical Science 2004, 106, 549–561. [Google Scholar] [CrossRef]
- Qian, X.; Wan, J.; Xu, J.; Liu, C.; Zhong, M.; Zhang, J.; Zhang, Y.; Wang, S. Epidemiological trends of Urolithiasis at the Global, Regional, and national levels: a Population-based study. International Journal of Clinical Practice 2022, 202, 6807203. [Google Scholar] [CrossRef]
- Lang, J.; Narendrula, A.; El-Zawahry, A.; Sindhwani, P.; Ekwenna, O. Global trends in Incidence and Burden of Urolithiasis from 1990 to 2019: an analysis of global burden of Disease Study Data. European Urology Open Science 2022, 35, 37–46. [Google Scholar] [CrossRef]
- Hanstock, S.; Ferreira, D.; Adomat, H.; Eltit, F.; Wang, Q.; Othman, D.; Nelson, B.; Chew, B.; Miller, A.; Lunken, G.; Lange, D. A mouse model for the study of diet-induced changes in intestinal microbiome composition on renal calcium oxalate crystal formation. Urolithiasis 2025, 53, 4. [Google Scholar] [CrossRef]
- Shanks, N.; Greek, R.; Greek, J. Are animal models predictive for humans? Philosophy, Ethics, and Humanities in Medicine 2009, 4, 2. [Google Scholar] [CrossRef]
- Bagetti Filho, H.J.; Pereira-Sampaio, M.A.; Favorito, L.A.; Sampaio, F.J. Pig kidney: anatomical relationships between the renal venous arrangement and the kidney collecting system. The Journal of Urology 2008, 179, 1627–1630. [Google Scholar] [CrossRef]
- Giraud, S.; Favreau, F.; Chatauret, N.; Thuillier, R.; Maiga, S.; Hauet, T. Contribution of large pig for renal ischemia-reperfusion and transplantation studies: the preclinical model. BioMed Research International 2011, 2011, 532127. [Google Scholar] [CrossRef] [PubMed]
- Tzou, D.T.; Taguchi, K.; Chi, T.; Stoller, M.L. Animal models of urinary stone disease. International Journal of Surgery 2016, 36, 596–606. [Google Scholar] [CrossRef]
- Verhulst, A.; Dehmel, B.; Lindner, E.; Akerman, M.E.; D’Haese, P.C. C. Oxalobacter formigenes treatment confers protective effects in a rat model of primary hyperoxaluria by preventing renal calcium oxalate deposition. Urolithiasis 2022, 50, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Crestani, T.; Crajoinas, R.O.; Jensen, L.; Dima, L.L.; Burdeyron, P.; Hauet, T.; Giraud, S.; Steichen, C. A sodium oxalate-rich diet induces chronić kidney disease and cardiac dysfunction in rats. International Journal of Molecular Sciences 2021, 22, 9244. [Google Scholar] [CrossRef] [PubMed]
- Kaplon, D.M.; Penniston, K.L.; Darriet, C.; Crenshaw, T.D.; Nakada, S.Y. Hydroxyproline-induced hyperoxaluria using acidified and traditional diets in the porcine model. Journal of Endourology 2010, 24. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.R.; Finlayson, B.; Hackett, R.L. Histologic study of the early events in oxalate induces intranephronic calculosis. Investigative Urology 1979, 17, 199–202. [Google Scholar] [PubMed]
- Khan, S.R.; Finlayson, B.; Hackett, R.L. Experimental calcium oxalate nephrolithiasis in the rat. Role of the renal papilla. The American Journal of Pathology 1982, 107, 59–69. [Google Scholar]
- Khan, S.R.; Shevock, P.N.; Hackett, R.L. Acute hyperoxaluria, renal injury and calcium oxalate urolithiasis. The Journal of Urology 1992, 147, 226–230. [Google Scholar] [CrossRef]
- Robijn, S.; Hoppe, B.; Vervaet, B.A.; D’Haese, P.C.; Verhulst, A. Hyperoxaluria: a gut-kidney axis? Kidney International 2011, 80, 1146–1158. [Google Scholar] [CrossRef]
- Knauf, F.; Velazquez, H.; Pfann, V.; Jiang, Z.; Aronson, P.S. Characterization of renal NaCl and oxalate transport in Slc26a6. American Journal of Physiology – Renal Physiology 2019, 01, 128–133. [Google Scholar] [CrossRef]
- Fargue, S.; Wood, K.D.; Cirvelli, J.J.; Assimos, D.G.; Oster, R.A.; Knight, J. Endogenous oxalate synthesis and urinary oxalate excretion. Journal of the American Society of Nephrology 2023, 39, 1505–1507. [Google Scholar] [CrossRef]
- Hoppe, B.; Kemper, M.J.; Bökenkamp, A.; Portale, A.A.; Cohn, R.A.; Langman, C.B. Plasma calcium-oxalate supersaturation in children with primary hyperoxaluria and end stage renal disease. Kidney International 1999, 56, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, B.; Beck, B.B.; Milliner, D.S. The primary hyperoxalurias. Kidney International 2009, 75, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Perinpam, M.; Enders, F.T.; Mara, K.C.; Vaughan, L.E.; Mehta, R.A.; Voskoboev, N.; Milliner, D.S.; Lieske, J.C. Plasma oxalate in relation to eGFR in patients with primary hyperoxaluria, enteric hyperoxaluria and urinary stone disease. Clinical Biochemistry 2018, 50, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.R. Nephrocalcinosis in animal models with and without Stones. Urological Research 2010, 38, 429–438. [Google Scholar] [CrossRef]
- Mehra, Y.; Viswanathan, P. Early Evidence of Global DNA Methylation and Hydroxymethylation Changes in Rat Kidneys Consequent to Hyperoxaluria-Induced Renal Calcium Oxalate Stones. Cytology and Genetics 2022, 56, 458–465. [Google Scholar] [CrossRef]
- Mandel, N.S.; Henderson Jr, J.D.; Hung, L.Y.; Wille, D.F.; Wiessner, J.H. A porcine model of calcium oxalate kidney stone disease. The Journal of Urology 2004, 171, 1301–1303. [Google Scholar] [CrossRef]
- Evan, A.P.; Lingeman, J.E.; Coe, F.L.; Parks, J.H.; Bledsoe, S.B.; Shao, Y.; Sommer, A.J.; Paterson, R.F.; Kuo, R.L.; Grynpas, M. Randall’s plaque of patients with nephrolithiasis begins in basement membranes of thin loops of Henle. Journal of Clinical Investigation 2003, 111, 607–616. [Google Scholar] [CrossRef]
- Canela, V.H. .; Bledsoe, S.B.; Lingeman, J.E.; Gerber, G.; Worcester, E.M.; El-Achkar, T.M.; Williams Jr, J.C. Demineralization and sectioning of human kidney stones: A molecular investigation revealing the spatial heterogneity of the stone matrix. Physiological Reports 2021, 9, e14658. [Google Scholar] [CrossRef]
Figure 1.
Blood oxalate profile from pigs with mild to severe hyperoxalemia. A. Changes over infusion time and after oxalate removal; B. Area under the curve comparison. Dose 1 - 1 ml, Dose 2 - 1.9 ml, Dose 3 - 2.8 ml of 1% sodium oxalate via jugular vein every 15 min during a 15-hour period (n=3 per group). Results are presented as mean± SD. Area under the curve (AUCs) values are baseline-adjusted. Significant differences are indicated by different letters (p < 0.05).
Figure 1.
Blood oxalate profile from pigs with mild to severe hyperoxalemia. A. Changes over infusion time and after oxalate removal; B. Area under the curve comparison. Dose 1 - 1 ml, Dose 2 - 1.9 ml, Dose 3 - 2.8 ml of 1% sodium oxalate via jugular vein every 15 min during a 15-hour period (n=3 per group). Results are presented as mean± SD. Area under the curve (AUCs) values are baseline-adjusted. Significant differences are indicated by different letters (p < 0.05).
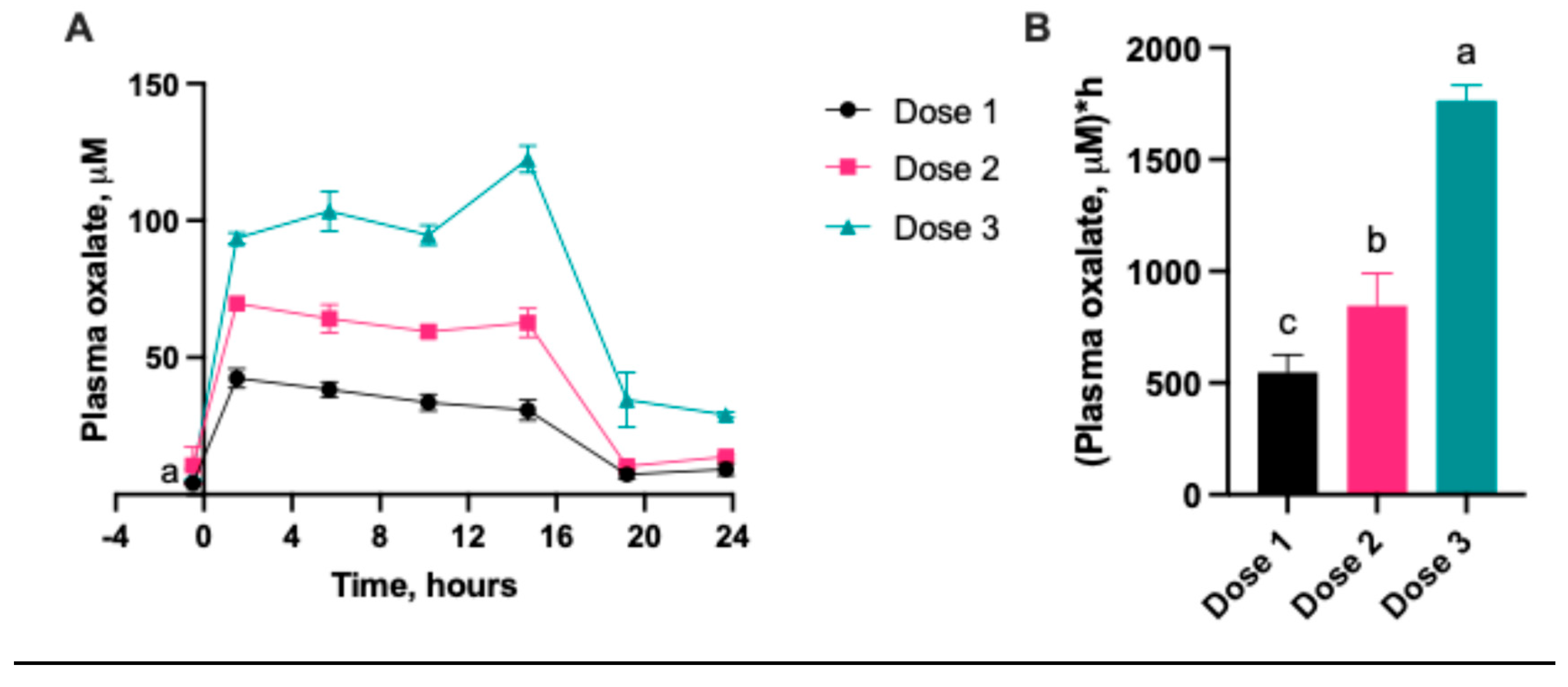
Figure 2.
Urinary oxalate concentration in pigs with mild to severe hyperoxalemia. Dose 1 - 1 ml, Dose 2 - 1.9 ml, Dose 3 - 2.8 ml of 1% sodium oxalate via jugular vein every 15 min during a 15-hour period (n=3 per group). Results are presented as mean± SD.
Figure 2.
Urinary oxalate concentration in pigs with mild to severe hyperoxalemia. Dose 1 - 1 ml, Dose 2 - 1.9 ml, Dose 3 - 2.8 ml of 1% sodium oxalate via jugular vein every 15 min during a 15-hour period (n=3 per group). Results are presented as mean± SD.
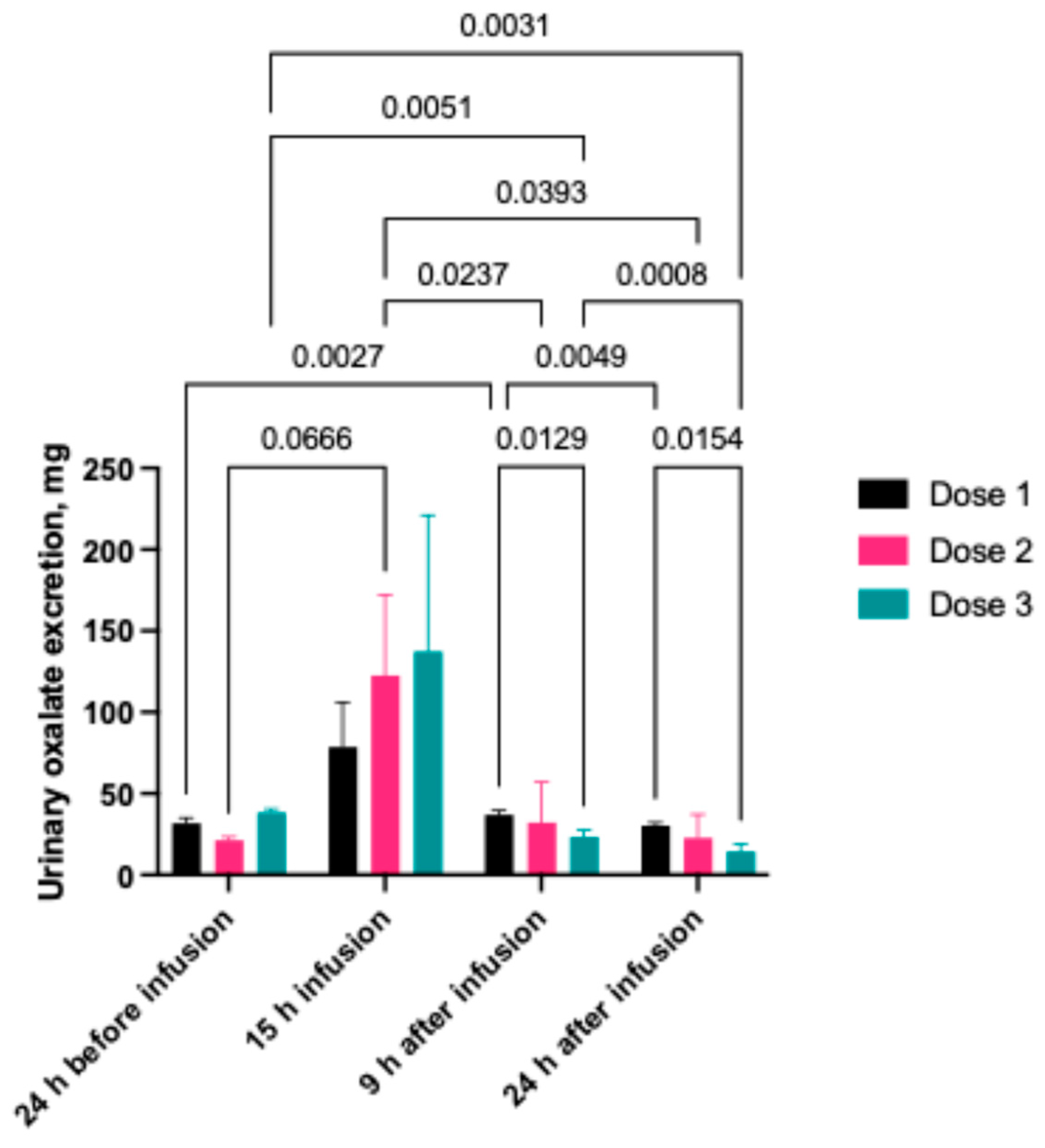
Figure 3.
Serum oxalate concentration during sodium oxalate infusion. A. High Dose (n=3) and B. Low Dose group (n=3). Blood samples were taken 24h before the start of the oxalate infusion and on 7th, 11th and 14th day of the study. Pigs were infused with 1% sodium oxalate at 2mL every 30min in the Low Dose Group, and at 6mL every 30min in the High Dose group, respectively. Oxalate infusions were stopped in the High Dose group after 7 days and in the Low Dose Group after 11 days. Plasma oxalate levels were additionally measured 3 days after oxalate infusion was stopped (day 14 results). Results are presented as mean± SD.
Figure 3.
Serum oxalate concentration during sodium oxalate infusion. A. High Dose (n=3) and B. Low Dose group (n=3). Blood samples were taken 24h before the start of the oxalate infusion and on 7th, 11th and 14th day of the study. Pigs were infused with 1% sodium oxalate at 2mL every 30min in the Low Dose Group, and at 6mL every 30min in the High Dose group, respectively. Oxalate infusions were stopped in the High Dose group after 7 days and in the Low Dose Group after 11 days. Plasma oxalate levels were additionally measured 3 days after oxalate infusion was stopped (day 14 results). Results are presented as mean± SD.
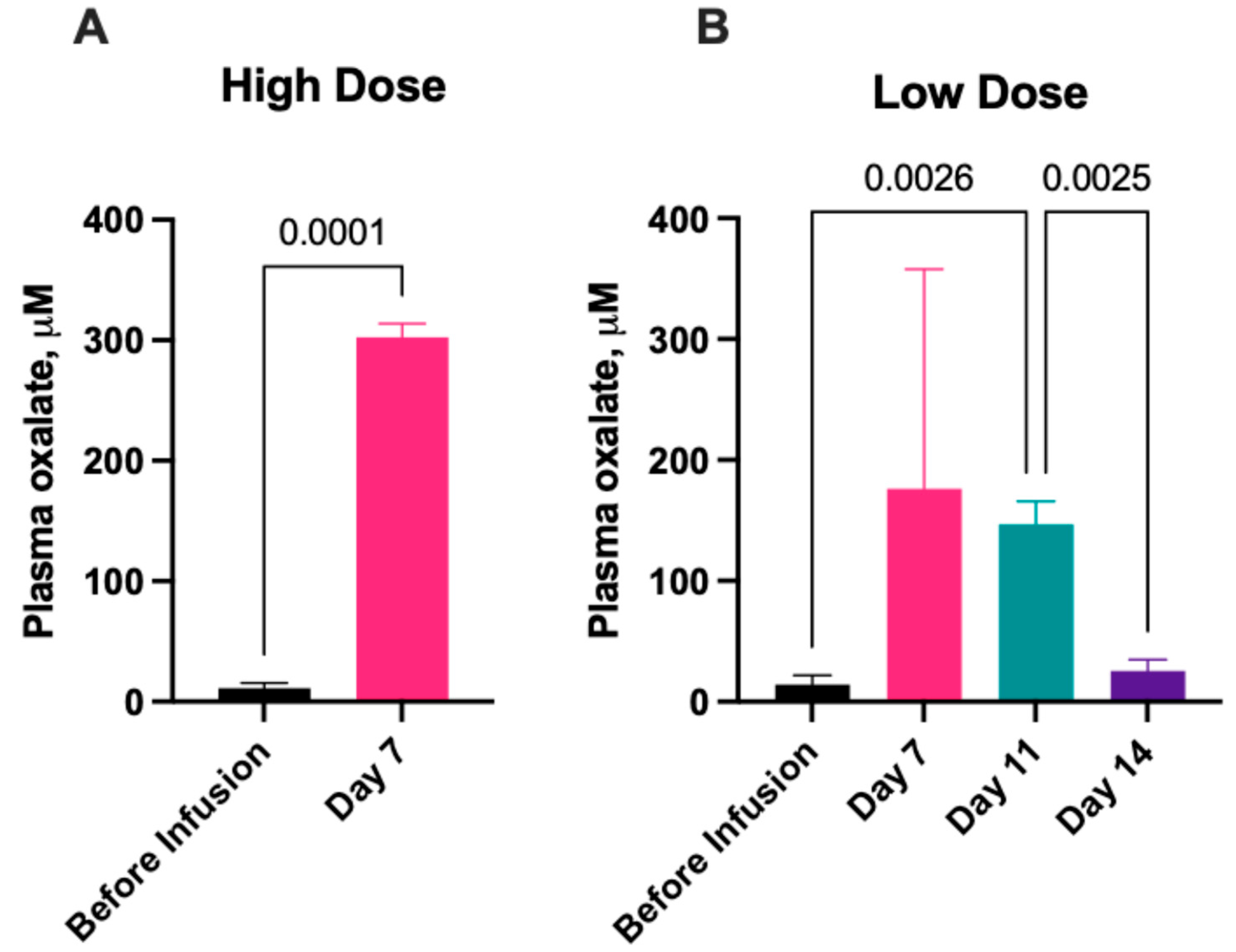
Figure 4.
Daily food intake during low and high dose oxalate infusions. Pigs in the Low Dose group were infused with 1% sodium oxalate at 2mL every 30min and pigs in the High Dose group were infused with 1% sodium oxalate at 6mL every 30min. Oxalate infusions were stopped in the High Dose group after 7 days. Results are presented as mean± SD.
Figure 4.
Daily food intake during low and high dose oxalate infusions. Pigs in the Low Dose group were infused with 1% sodium oxalate at 2mL every 30min and pigs in the High Dose group were infused with 1% sodium oxalate at 6mL every 30min. Oxalate infusions were stopped in the High Dose group after 7 days. Results are presented as mean± SD.
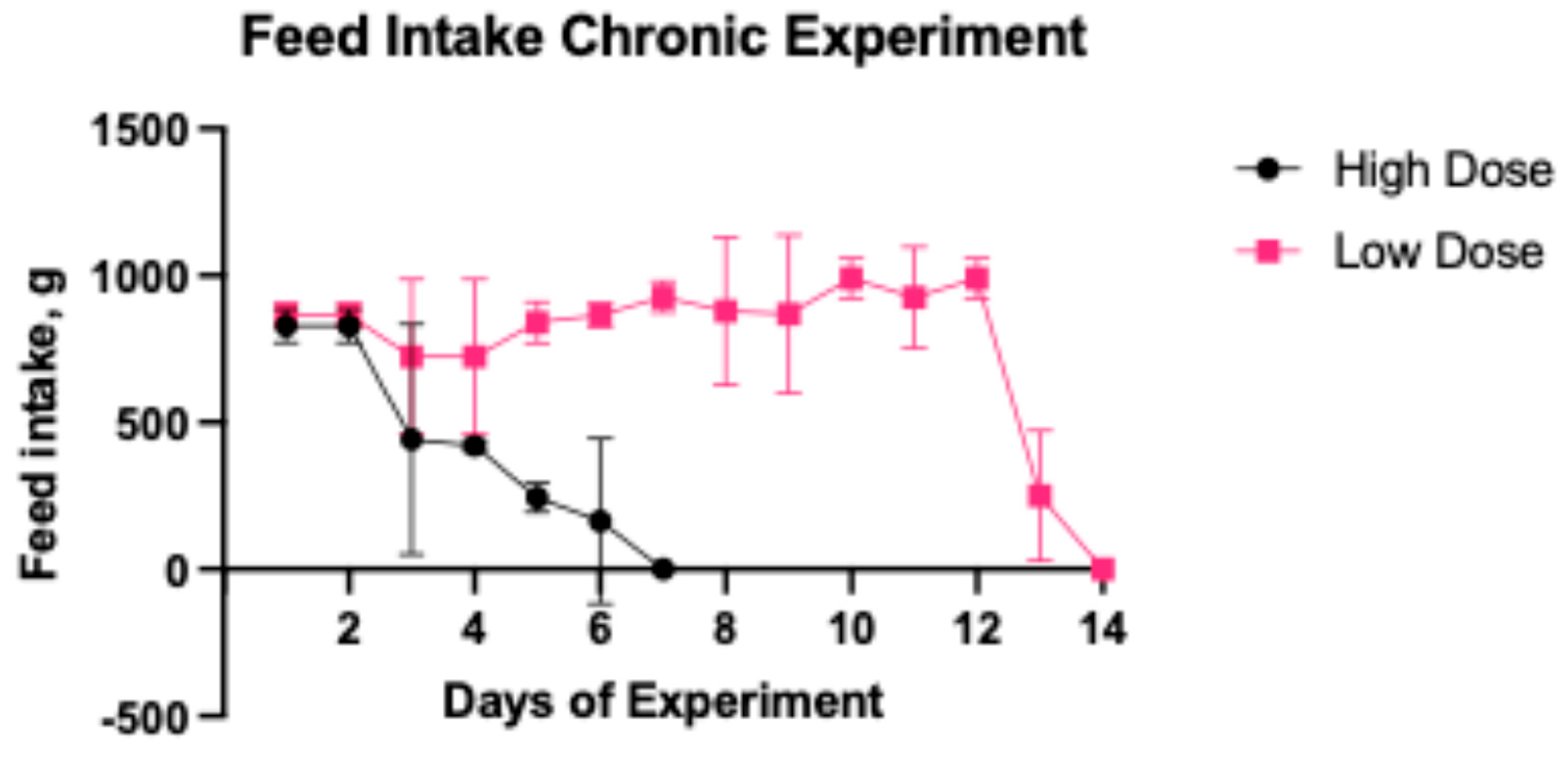
Figure 5.
Representative images of nephrocalcinosis in the renal cortex and medulla of pigs from the Low and High dose NaOX groups. The black staining represents CaOx deposits. Yasue staining, low magnification (X25).
Figure 5.
Representative images of nephrocalcinosis in the renal cortex and medulla of pigs from the Low and High dose NaOX groups. The black staining represents CaOx deposits. Yasue staining, low magnification (X25).
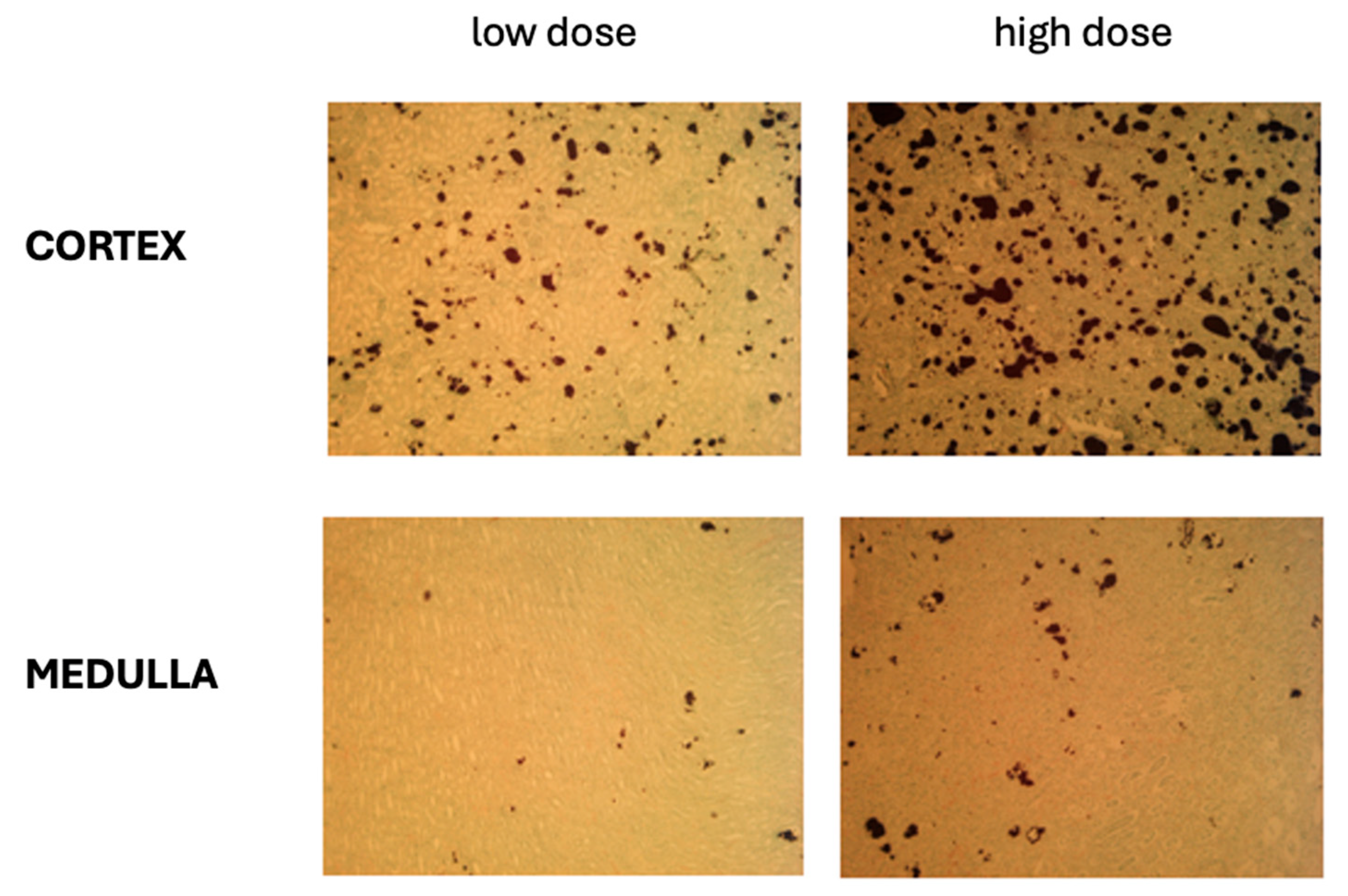
Figure 6.
Percentage nephrocalcinosis in kidney tissues of pigs from the Low and High Dose NaOX groups (Median (± IQR). Yasue staining for CaOx deposits was performed in representative samples from the right and left kidneys and affected areas were calculated as 2 independent areas from the cortex and 2 independent areas from the medulla, with a total of four images per kidney (L or R). Low magnification (X25).
Figure 6.
Percentage nephrocalcinosis in kidney tissues of pigs from the Low and High Dose NaOX groups (Median (± IQR). Yasue staining for CaOx deposits was performed in representative samples from the right and left kidneys and affected areas were calculated as 2 independent areas from the cortex and 2 independent areas from the medulla, with a total of four images per kidney (L or R). Low magnification (X25).

Figure 7.
Research groups in Experiment 1 and 2 and a simple study design.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



