Submitted:
31 July 2025
Posted:
31 July 2025
You are already at the latest version
Abstract
Rheumatoid arthritis (RA) is a systemic autoimmune disease that, beyond joint destruc-tion, contributes to neuropsychiatric symptoms such as depression, anxiety, and cogni-tive impairment. These symptoms are often underrecognized despite their major impact on quality of life. Accumulating evidence suggests that pro-inflammatory cytokines, particularly tumor necrosis factor alpha (TNF-α) and interleukin-6 (IL-6), play a key role in this neuroimmune interface. This narrative review examined 16 clinical studies evaluating the effects of biologic therapies targeting TNF-α and IL-6 on mental health outcomes in RA. The total study population comprised 9,939 patients, including 2,467 treated with TNF-α inhibitors and 7,472 with IL-6 or IL-6 receptor inhibitors. TNF-α inhibitors were associated with improved depressive symptoms and emotional well-being. IL-6 inhibitors demonstrated similar psychiatric benefits, particularly in patients with elevated IL-6 levels. The findings highlight that biological therapies in RA may influence not only physical symptoms but also mental health, likely through modulation of neuroimmune pathways including blood–brain barrier permeability, microglial acti-vation, and HPA axis regulation. Future research is needed to clarify these Effects in populations stratified by psychiatric comorbidity and inflammatory biomarkers. Clini-cal implications: Incorporating psychiatric symptom screening and considering neuroin-flammatory profiles may help guide the selection of biologic therapy in RA, particularly in patients with comorbid depression or fatigue.
Keywords:
rheumatoid arthritis
; TNF-α inhibitors
; IL-6 inhibitors
; depression
; psychiatric symptoms
; neuropsychiatric symptoms
; biologics
; quality of life
; neuroinflammation
; neuroimmunology
; neuroimmune modulation
; blood-brain barrier
; biological therapies
1. Introduction
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disease characterized by persistent synovial inflammation, progressive joint destruction, and extra-articular manifestations. It affects approximately 0.5% to 1% of the general population worldwide, with a higher prevalence among women and individuals in middle age [1,2]. Beyond its well-established musculoskeletal symptoms, RA has a significant impact on patients’ overall health, quality of life, and psychological well-being.
In recent years, RA has been increasingly recognized not only as a joint-specific condition but as a systemic disease involving complex interactions between the immune system, neuroendocrine pathways, and the central nervous system [3,4]. Psychiatric comorbidities, especially depression and anxiety, are frequent in patients with RA. Epidemiological studies indicate that up to 40% of RA patients experience clinically significant depressive symptoms during the course of the disease [4,5]. Depression in RA is associated with worse disease outcomes, higher levels of perceived pain, increased disability, poorer treatment adherence, and even increased mortality [6,7].
The link between systemic inflammation and psychiatric symptoms (depression, fatigue, cognitive dysfunction) is increasingly supported by both experimental and clinical data. Pro-inflammatory cytokines such as TNF-α, IL-1β, IL-6, and IL-17, which play central roles in the pathogenesis of RA, are also implicated in the development of mood disorders [8,9,10]. These cytokines can cross the blood–brain barrier or signal through peripheral nerves, activating microglia and astrocytes, and disrupting neurotransmitter systems and hypothalamic–pituitary–adrenal (HPA) axis regulation [11,12]. Such interactions lead to behavioral changes often described as sickness behavior syndrome, which overlaps with the symptomatology of depression, including fatigue, anhedonia, cognitive dysfunction, and reduced motivation [13,14].
In the context of RA, the bi-directional relationship between chronic inflammation and mental health becomes particularly relevant. Effective immunomodulatory treatments targeting TNF-α and IL-6 not only reduce joint inflammation but may also exert beneficial effects on mood and quality of life [15,16]. These observations raise important questions about the underlying mechanisms connecting the immune system and psychiatric symptoms, and whether such effects could be harnessed in clinical practice to improve outcomes for RA patients.
Currently, several classes of biological therapies are available for the treatment of rheumatoid arthritis, each targeting different key components of the immune system. These include: TNF-α inhibitors (infliximab—IFX, etanercept—ETA, adalimumab—ADA, certolizumab pegol—CZP, golimumab—GLM) [2], IL-6 inhibitors (tocilizumab—TCZ, sarilumab—SAR) [17,18], B-cell depleting agents (rituximab, targeting CD20-positive B cells) [19], and T-cell co-stimulation inhibitors (abatacept, targeting CD80/CD86 via CTLA-4) [20].
Each of these drug classes acts on a distinct immunological pathway contributing to RA pathogenesis. However, among the various biological therapies approved for RA, those targeting TNF-α and IL-6 are of particular interest in the context of mental health outcomes, including neuroinflammatory and neuroendocrine alterations [21,22]. Table 1 presents the biological agents targeting TNF-α and IL-6, along with their molecular structures and immunological functions, such as cytokine neutralization or receptor blockade.
This narrative review aims to summarize current findings on the impact of TNF-α and IL-6 inhibitors on mental health outcomes, particularly depressive symptoms, in patients with RA.
2. Methods
The narrative review was conducted through a literature search using PubMed, Scopus, and Google Scholar, focusing on articles published between January 2000 and December 2024. Search terms included combinations of: “rheumatoid arthritis,” “biological therapy,” “TNF-alpha inhibitors,” “IL-6 inhibitors,” “depression,” “quality of life,” “patient-reported outcomes,” and “psychiatric symptoms.”, and/or “depression” and/or “fatigue” and/or “cognitive dysfunction”.
Randomized controlled trials (RCTs), non-interventional cohort studies, post-hoc analyses of clinical trials, and relevant preclinical studies were selected for inclusion. Articles were included if they reported outcomes related to mood disorders (e.g., depression, anxiety, anhedonia) or broader quality of life measures (e.g., PROMIS, SF-36, EQ-5D) in patients undergoing treatment with TNF-alpha or IL-6 inhibitors. Only studies published in English were considered. No systematic review methods (e.g., PRISMA guidelines) were applied, in keeping with the narrative nature of this review.
An overview of the molecular structure, pharmacological classification, and mechanisms of action of biologic agents targeting TNF-α and IL-6 used in rheumatoid arthritis is presented in Table 1. This classification includes fully human monoclonal antibodies, chimeric antibodies, humanized antibodies, receptor fusion proteins, and Fab fragments conjugated with polyethylene glycol (PEG). The table also lists commercial trade names and available biosimilars. Only biologic agents directly affecting TNF-α and IL-6 pathways are included, given their relevance to both inflammatory and neuropsychiatric outcomes discussed in this review.
3. Results
Finally, a total of 16 studies were included in the analysis. They cover both TNF-α inhibitors and IL-6/Il-6R inhibitors in relation to mental health outcomes in patients with RA (Figure 1). Across all included studies, a total of 10,499 patients were analyzed — 3,027 in studies evaluating TNF-α inhibitors and 7,472 in studies on IL-6 or IL-6R inhibitors. Among them, approximately 6,820 individuals received active treatment with biological agents: around 2,211 with TNF-α inhibitors and 4,609 with IL-6/IL-6R inhibitors.
These patients were treated either with biological monotherapy or in combination with methotrexate (MTX), and compared to placebo, MTX alone, or standard disease-modifying anti-rheumatic drugs (DMARDs). Regardless of combination, the presence of the biological agent was the key factor of interest in evaluating potential neuropsychiatric effects.
3.1. TNF-Alpha Inhibitors
A total of 10 studies evaluated TNF-α inhibitors including 5 biologic agents: infliximab (IFX) [15,23,24], etanercept (ETN) [25,26,27,28,29], adalimumab (ADL) [16], golimumab (GLM) [15], and certolizumab pegol (CZP)[30]. Table 2 provides an overview of clinical studies assessing the neuropsychiatric effects of TNF-α in RA patients. It includes details on the agents used, study populations, and administration routes, offering context for the observed associations between immune modulation and improvements in depressive symptoms.
Eight of these studies reported clear improvements in depressive symptoms or quality of life as measured by validated scales (HADS, SDS, SF-36, EQ-5D-3L, PROMIS). The two studies [24,30] found no significant improvement, particularly in subgroups with comorbid somatization or insufficient inflammatory control.
Early RCTs demonstrated the positive impact of ETN on mental health outcomes. Significant improvement in depressive symptoms and quality of life (measured by MOS SF-36) in patients receiving ETN compared to placebo was reported [25]. Similar findings were observed in subsequent studies evaluating etanercept combined with methotrexate (MTX). Machado et al. [27] and Bae et al.[26] demonstrated that ETN+MTX significantly improved depressive symptoms, as assessed by HADS, outperforming conventional DMARD combinations.
Kekow et al. [28,29] showed in double-blind trials that ETN+MTX was superior to MTX alone in improving patient-reported outcomes (PROs), including reductions in depressive symptoms, with sustained effects observed over 104 weeks of follow-up.
Similarly, Miwa et al. [23] reported that IFX, a chimeric monoclonal antibody, significantly improved depressive symptoms (measured by the SDS scale) compared to MTX in a pilot study. However, a subsequent open-label study [24] found no significant differences between IFX and MTX in depression outcomes, as measured by the HAM-D scale.
The Phase 4 AWARE study [15], a large prospective observational study, further confirmed improvements in mood and PROMIS measures in patients treated with GLM or IFX over 46–52 weeks. Additionally, Hsieh et al. reported that ADL treatment improved depressive symptoms, assessed via EQ-5D-3L, in biologic-naïve RA patients over 24 weeks.
Furthermore, Curtis et al. [30] highlighted that CZP was less effective in RA patients presenting with the somatization comorbidity phenotype (SCP), who exhibited a lower likelihood of treatment response and a higher incidence of adverse events.
3.2. IL-6/IL-6R Inhibitors
Among the six studies evaluating IL-6 pathway inhibitors, five focused on agents targeting the IL-6R — tocilizumab (TCZ) [17,31,32,33] and sarilumab (SARI) [18]. In contrast, one study investigated sirukumab (SRK), a monoclonal antibody that directly binds to IL-6 itself [34].
These studies collectively support the potential psychiatric and immunological benefits of modulating the IL-6 signaling axis, with receptor blockade showing particular promise in patients with elevated IL-6 activity (see Table 3).
All 6 studies reported improvements in depressive symptoms, fatigue, and cognitive dysfunction. RA patients with elevated baseline IL-6 levels derived greater benefits in terms of mood and quality of life improvements when were treated with SRK or SARI compared to those treated with TNF-α inhibitors [18,34]. These findings suggest that IL-6 blockade may more directly target neuroimmune pathways implicated in mood disturbances.
TCZ, a humanized IgG1 monoclonal antibody targeting the IL-6R [35], was shown to effectively reduce depressive and anxiety symptoms, with a sustained downward trend observed in more than 65% of RA patients [17]. These results were corroborated in a cohort of patients with active RA treated in routine clinical practice [31].
A pooled analysis of five RCTs comparing TCZ with conventional DMARDs reported that depression severity (based on medical records, stratified by timing and confirmed by clinical investigators) was associated with reduced rates of clinical remission (measured by CDAI and SDAI), although no such association was found with inflammatory markers such as CRP [32]. Moreover, the study highlighted that pharmacological treatment with SSRIs/SNRIs did not improve the subjective components of disease activity or pain perception among depressed individuals.
In the ARATA project, patients stratified by depressive status (BDI-II) showed a reduced treatment response. They also reported a higher prevalence of adverse symptoms compared to non-depressed individuals [33].
In a double-blind RCT evaluating SRK, a monoclonal antibody directly targeting IL-6, Sun et al. reported positive effects on depressive and anhedonic symptoms [34]. A post hoc analysis revealed that, compared to placebo, patients randomized to SRK showed significant improvements in depression and anhedonia, with outcomes positively correlated with baseline soluble IL-6 receptor levels [34].
A subsequent post hoc analysis from a RCT comparing SARI and ADL evaluated the predictive role of baseline IL-6 levels and showed that patients with high baseline IL-6 reported worse functional PRO outcomes than those with lower levels. Interestingly, SARI demonstrated greater efficacy than ADL among patients with high IL-6 levels and an inadequate response or intolerance to prior DMARD therapy [18].
Figure 2.
Immunological mechanism linking chronic elevated proinflammatory cytokines to depressive symptoms. Systemic inflammation driven by TNF -α and IL-6 contributes to neuroinflammation via blood-brain barrier disruption, microglial activation, and HPA axis dysregulation, resulting in depressive symptoms, fatigue, and cognitive dysfunction. Biological therapies mitigate these processes, improving mental health outcomes.
Figure 2.
Immunological mechanism linking chronic elevated proinflammatory cytokines to depressive symptoms. Systemic inflammation driven by TNF -α and IL-6 contributes to neuroinflammation via blood-brain barrier disruption, microglial activation, and HPA axis dysregulation, resulting in depressive symptoms, fatigue, and cognitive dysfunction. Biological therapies mitigate these processes, improving mental health outcomes.
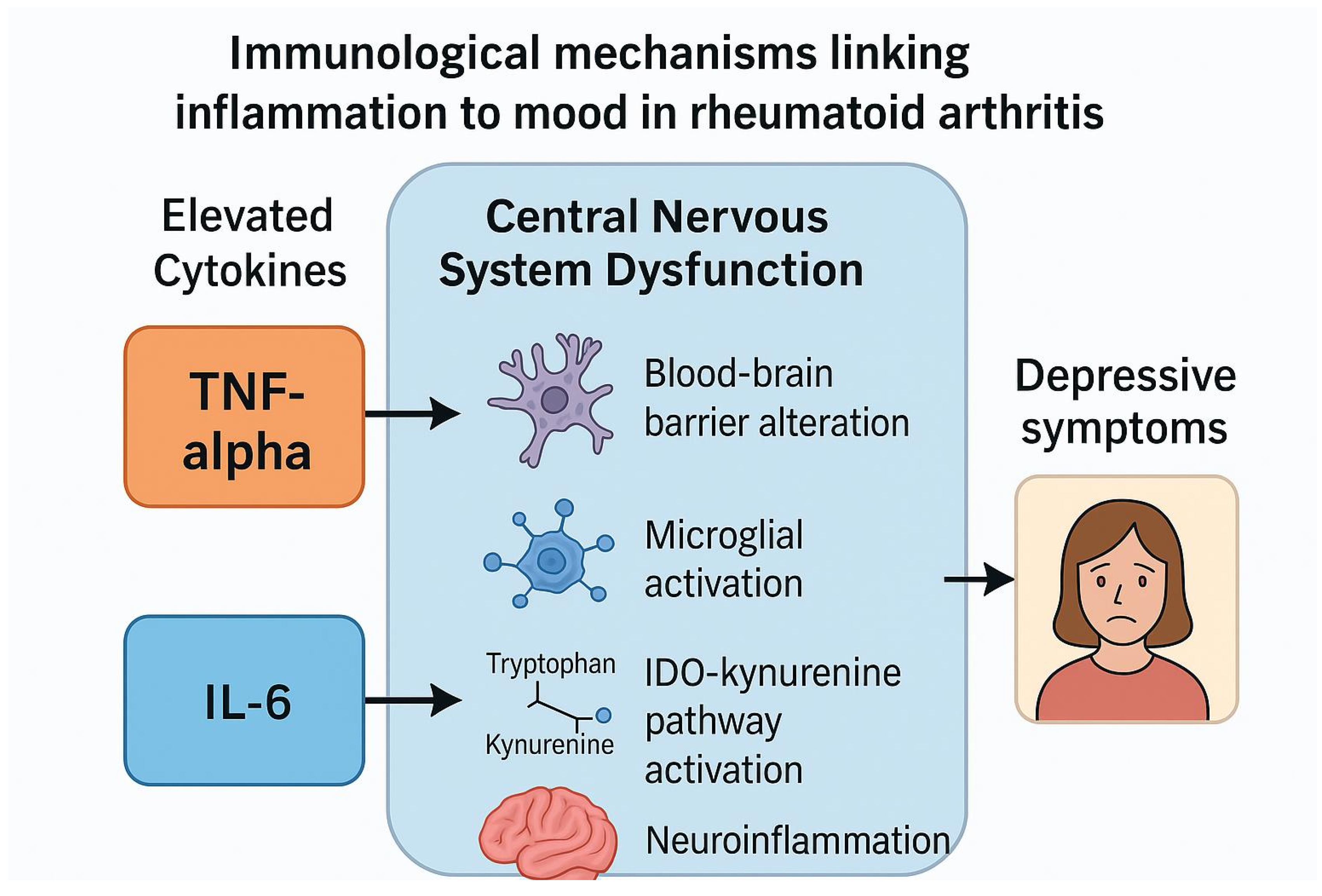
Figure 3.
Immunological mechanisms linking inflammation in rheumatoid arthritis to neuropsychiatric symptoms and the effects of biologic therapies.
Figure 3.
Immunological mechanisms linking inflammation in rheumatoid arthritis to neuropsychiatric symptoms and the effects of biologic therapies.
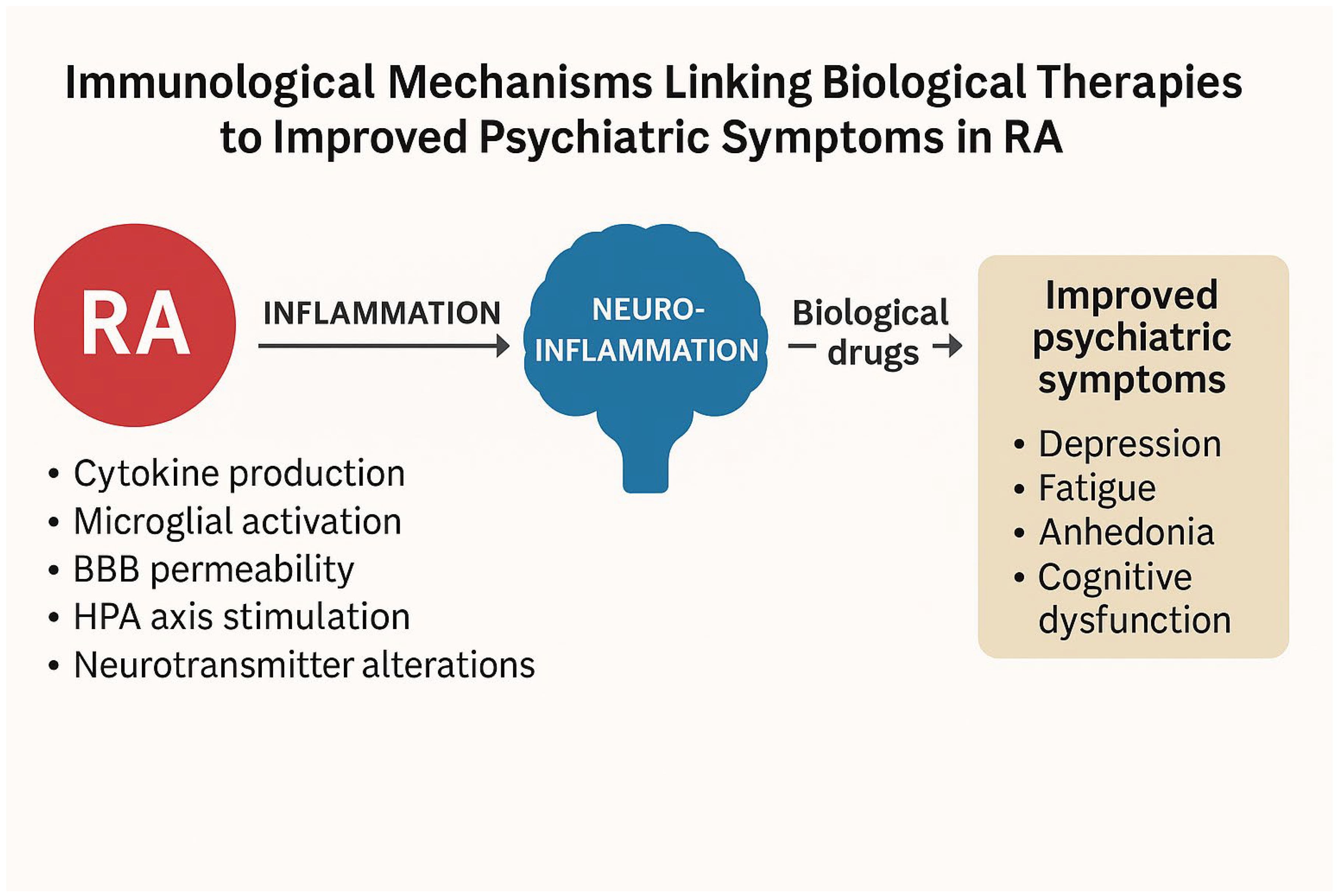
Chronic systemic inflammation in rheumatoid arthritis, mediated by cytokines such as TNF-alpha and IL-6, contributes to blood-brain barrier dysfunction, neuroinflammation, HPA axis dysregulation, and altered neurotransmission, leading to psychiatric symptoms (depression, anxiety, fatigue, and cognitive impairment). Biological therapies targeting TNF-α and IL-6/Il-6R reduce systemic inflammation, which may alleviate neuroinflammatory processes and improve mental health outcomes.
4. Discussion
This review highlights the potential psychiatric benefits of biological therapies, particularly TNF-α and IL-6 inhibitors, in patients with rheumatoid arthritis (RA). Across the 16 analyzed studies, improvements in depressive symptoms, fatigue, and cognitive dysfunction were consistently reported alongside enhanced somatic disease control and patient-reported outcomes (PROs). These findings align with the growing recognition that systemic inflammation contributes not only to joint pathology but also to psychiatric symptoms through complex neuroimmune mechanisms.
4.1. TNF-α Inhibitors and Psychiatric Outcomes
TNF-α inhibitors were among the first biologic therapies to demonstrate effects extending beyond joint inflammation. Improvements in depressive symptoms and quality of life have been consistently observed, particularly when TNF-α inhibition was combined with methotrexate [26,27]. Similar effects have been reported in other autoimmune diseases, such as psoriasis and inflammatory bowel disease, where TNF-α blockade was associated with reductions in somatic and psychiatric symptoms, including fatigue, depressive symptoms, and anxiety [36,37,38,39,40].
Further evidence comes from studies in ankylosing spondylitis (AS), which reported reductions in depressive symptoms with TNF-α inhibitors. Infliximab and etanercept, when used as part of standard treatment, were associated with reduced depression and anxiety severity and improved quality of life [41,42]. Preclinical studies provide further support: in animal models of chronic mild stress, infliximab reduced depressive-like and anxiety-like behaviors [43,44]. Moreover, TNF-α inhibitors have been explored as adjunctive treatments in bipolar disorder, where infliximab showed benefits on depressive symptoms, cognitive function, and neuroinflammatory markers [45,46,47].
These findings suggest that TNF-α plays a critical role in immune pathways that contribute not only to peripheral inflammation but also to central mechanisms implicated in mood regulation and cognition. The psychiatric benefits of TNF-α inhibition likely stem from its capacity to reduce systemic and CNS inflammation, restore blood-brain barrier (BBB) integrity, attenuate neuroinflammatory signaling, and normalize neurotransmitter systems. Preclinical models corroborate these mechanisms, showing reductions in anhedonia and anxiety-like behaviors after TNF-α blockade [11,14].
However, not all studies reported uniform benefits. Some indicated limited effects, particularly in patients with somatization comorbidity phenotypes, highlighting the complex interplay between biological and psychological factors in RA [30]. In these subgroups, inflammatory pathways may play a less dominant role compared to primary psychiatric mechanisms, potentially limiting the psychiatric impact of TNF-α inhibition.
4.2. IL-6/IL-6R Inhibitors and Psychiatric Outcomes
IL-6 inhibitors, such as tocilizumab and sarilumab, appear to offer more targeted psychiatric benefits, particularly among patients with elevated IL-6 levels. These observations support the hypothesis that IL-6 plays a direct role in neuroinflammatory processes relevant to mood disorders [18,25]. Unlike TNF-α inhibitors, IL-6 blockade demonstrated psychiatric benefits even without significant reductions in peripheral markers like CRP, suggesting that central neuroimmune effects may be more critical than systemic inflammation alone [32]. Post hoc analyses further indicated that higher baseline IL-6 or soluble IL-6 receptor levels predicted better psychiatric outcomes following IL-6 inhibition, aligning with precision medicine approaches [33].
Experimental data provide further support. IL-6 can cross the BBB, activate glial cells, and amplify neuroinflammatory responses, thereby influencing mood regulation. Moreover, IL-6 impacts the hypothalamic-pituitary-adrenal (HPA) axis and modulates neurotransmitter systems, contributing to fatigue, anhedonia, and cognitive dysfunction [12]. By mitigating these processes, IL-6 inhibitors may offer benefits for mood and cognition beyond their anti-inflammatory effects in peripheral tissues.
4.3. Proposed Mechanisms Linking Biological Therapies to Psychiatric Outcomes
The psychiatric improvements observed with TNF-α and IL-6 inhibitors are biologically plausible given the established roles of these cytokines in neuroimmune interactions. Chronic systemic inflammation affects the central nervous system (CNS) through multiple interconnected mechanisms:
- 1.
- Blood-Brain Barrier (BBB) Dysfunction
Inflammation increases BBB permeability, allowing peripheral cytokines to influence the brain microenvironment [11,22]. Both TNF-α and IL-6 contribute to this process, enabling pro-inflammatory mediators to access the CNS.
- 2.
- Microglial Activation and Neuroinflammation
Elevated TNF-α and IL-6 levels activate microglia, initiating sustained neuroinflammation and altering neurotransmission, particularly in circuits involved in mood regulation [21].
- 3.
- Hypothalamic-Pituitary-Adrenal (HPA) Axis Dysregulation
Pro-inflammatory cytokines disrupt HPA axis function, leading to hypercortisolemia and its detrimental effects on mood, cognition, and energy balance [12,22].
- 4.
- Kynurenine Pathway Activation
Inflammation increases the activity of indoleamine 2,3-dioxygenase (IDO), shifting tryptophan metabolism towards neurotoxic kynurenine metabolites linked to depressive symptoms and cognitive impairment [13,22].
- 5.
- Direct Actions of IL-6
IL-6 can cross the BBB, activate glial cells, amplify neuroinflammatory cascades, stimulate the HPA axis, and alter neurotransmission [12].
4.4. Role of Biological Therapies
Biological therapies targeting TNF-α and IL-6 may mitigate these neuroimmune mechanisms through reductions in systemic and CNS inflammation, normalization of HPA axis activity, suppression of microglial overactivation, and restoration of neurotransmitter balance. These effects likely underpin the improvements in psychiatric symptoms observed with these treatments [21].
TNF-α inhibitors, such as infliximab, etanercept, and adalimumab, reduce systemic inflammation, restore BBB integrity, decrease neurotoxic metabolite production, and downregulate neuroinflammatory signaling. These mechanisms are thought to improve monoaminergic neurotransmission (serotonin, dopamine) and support neuroplasticity, alleviating depressive symptoms. Preclinical studies support these actions, showing reductions in anhedonia and anxiety-like behaviors after TNF-α blockade [11,14].
Similarly, IL-6 inhibitors such as tocilizumab or sarilumab reduce systemic cytokine levels, CNS inflammation, and HPA axis hyperactivity. Clinical studies indicate that patients with elevated IL-6 derive greater psychiatric benefit from IL-6 receptor inhibition [18,34]. Experimental models further confirm the antidepressant-like effects of IL-6 inhibition through normalization of neuroinflammatory markers and behavior [12].
4.5. Limitations
This review is narrative in nature and does not adhere to systematic methodologies such as PRISMA guidelines. The heterogeneity of the included studies, variability in endpoints, and inconsistency of psychiatric assessment tools limit definitive conclusions. Moreover, psychiatric outcomes were often secondary or exploratory and not primary trial objectives. Despite these limitations, the consistency of findings and supporting mechanistic data emphasize the relevance of these observations.
4.6. Conclusions
Biologic therapies targeting TNF-α and IL-6 in rheumatoid arthritis may provide dual benefits, improving both joint-related disease activity and neuropsychiatric symptoms such as depression, fatigue, and cognitive dysfunction. These effects are likely mediated through modulation of systemic and central inflammatory pathways, including blood-brain barrier integrity, microglial activation, and HPA axis regulation.
While the current evidence supports these benefits, most studies assessed psychiatric outcomes as secondary endpoints. Future research should focus on well-designed prospective trials with standardized neuropsychiatric assessments and biomarker-based stratification to confirm and optimize these findings.
Recognizing psychiatric symptoms as part of the disease burden in RA opens the door to more holistic treatment approaches, where targeting immune pathways can contribute to improved mental and physical health outcomes.
4.7. Clinical Implications
Incorporating psychiatric symptom screening and considering neuroinflammatory profiles may help guide the selection of biologic therapy in RA, particularly in patients with comorbid depression or fatigue.
Author Contributions
Conceptualization, H.S. E.W.; Methodology, E.W. Investigation, H.S. E. W. Writing—original draft preparation, H.S., E. W. Writing—review and editing, E.W. Visualization, E.W. Supervision, E.W., A. M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
AA—Alopecia Areata, ADA/ADL—Adalimumab, AE—Adverse Events, AM—Amplitude Modulation, AS—Ankylosing Spondylitis, BDI—Beck Depression Inventory, BBB—Blood-Brain Barrier, CD—Crohn’s Disease, CNS—Central Nervous System, CRP—C-Reactive Protein, CT—Computed Tomography, CZP—Certolizumab Pegol, DAS28—Disease Activity Score 28, ETA—Etanercept, EQ-5D—EuroQol 5 Dimensions Questionnaire, FACIT-F—Functional Assessment of Chronic Illness Therapy-Fatigue, FDA—Food and Drug Administration, GLM—Golimumab, HAQ—Health Assessment Questionnaire, HADS—Hospital Anxiety and Depression Scale, HPA—Hypothalamic-Pituitary-Adrenal, IBD—Inflammatory Bowel Disease, IDO—Indoleamine 2,3-Dioxygenase, IgG—Immunoglobulin G, IL—Interleukin, IL-6—Interleukin-6, IL-6R—Interleukin-6 Receptor, mAb—Monoclonal Antibody, MRI—Magnetic Resonance Imaging, MTX—Methotrexate, PCS—Physical Component Summary, PHQ-9—Patient Health Questionnaire-9, PRISMA—Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PROs—Patient-Reported Outcomes, QoL—Quality of Life, RA—Rheumatoid Arthritis, SARI—Sarilumab, SF-36—Short Form Health Survey 36, SRK—Sirukumab, TCZ—Tocilizumab, TNF—Tumor Necrosis Factor, TNF-α—Tumor Necrosis Factor-alpha, UC—Ulcerative Colitis, VAS—Visual Analog Scale, WOMAC—Western Ontario and McMaster Universities Osteoarthritis Index.
References
- Alamanos, Y., Voulgari, P.V, Drosos, A.A.: Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006, 36, 182-8. [CrossRef]
- Smolen, J.S,; Aletaha, D.; McInnes, I.B:. Rheumatoid arthritis. Lancet 2016, 388, 2023-2038. [CrossRef]
- Meade, T.; Manolios, N.; Cumming, R.; Conaghan, P.G.; Katz, P. Cognitive Impairment in Rheumatoid Arthritis: A Systematic Review. Arthritis Care Res (Hoboken) 2018, 70, 39-52. PMID: 28371512. [CrossRef]
- Panjrattan, C.; Chauhan, V.S.; Nath, S.; et al.: Depression among rheumatoid arthritis patients and barriers to seeking professional help: An observational study. Ind Psychiatry J. 202332(Suppl 1):S136-S140. [CrossRef]
- Katz, P,; Pedro, S.; Michaud, K. Sleep Disorders Among Individuals With Rheumatoid Arthritis. Arthritis Care Res (Hoboken) 2023, 75, 1250-1260. Epub 2023 Jan 30. PMID: 35997482. [CrossRef]
- Maloley, P.M.; England, B.R.; Sayles, H. et al. Post-traumatic stress disorder and serum cytokine and chemokine concentrations in patients with rheumatoid arthritis. Semin Arthritis Rheum. 2019, 49, 229-235. [CrossRef]
- Albeltagy, E.S.; Elaziz, S.YA.; Abozaid, S.Y.; et.al.: Interleukin 6, interleukin 17, disease-related and contextual factor association with depression, and its severity in patients with rheumatoid arthritis. Clin Rheumatol. 2021, 40, 895-904. [CrossRef]
- Liu, Y.; Ho, R.C.; Mak, A.: The role of interleukin (IL)-17 in anxiety and depression of patients with rheumatoid arthritis. Int J Rheum Dis. 2012, 15, 183-7. [CrossRef]
- El-Tantawy, A.M.; El-Sayed, A.E.; Kora, B.A.; Amin, R.T. Psychiatric morbidity associated with some cytokines (IL-1beta, IL-12, IL-18 and TNF-alpha) among rheumatoid arthritis patients. Egypt J Immunol. 2008, 15, 1-11.
- Li, YC.; Chou, YC.; Chen.; HC, et. Al.: Interleukin-6 and interleukin-17 are related to depression in patients with rheumatoid arthritis. Int J Rheum Dis. 2019, 22,980-985. [CrossRef]
- Cheng, Y.; Desse, S.; Martinez, A.; et.al.: TNFα disrupts blood brain barrier integrity to maintain prolonged depressive-like behavior in mice. Brain Behav Immun. 2018, 69, 556-567. [CrossRef]
- Xu, D,.; Xu, Y.; Gao, X.; et.al: Potential value of Interleukin-6 as a diagnostic biomarker in human MDD and the antidepressant effect of its receptor antagonist tocilizumab in lipopolysaccharide-challenged rats. Int Immunopharmacol. 2023, 124(Part B), 110903. [CrossRef]
- Cathomas, F.; Fuertig, R.; Sigrist, H.; et. al: Hengerer, B et al. CD40-TNF activation in mice induces extended sickness behavior syndrome co-incident with but not dependent on activation of the kynurenine pathway. Brain Behav Immun.2015,50:125-140. [CrossRef]
- Brown, E.; Mc Veigh, C.J.; Santos, L.; et al.: TNFα-dependent anhedonia and upregulation of hippocampal serotonin transporter activity in a mouse model of collagen-inducedarthritis. Neuropharmacology. 2018,137:211220. [CrossRef]
- Bingham, C.O., III.; Black, S.; Shiff, N.J.; et al.: J.R. Response to Treatment with Intravenous Golimumab or Infliximab in Rheumatoid Arthritis Patients: PROMIS Results from the Real-World Observational Phase 4 AWARE Study. Rheumatol Ther. 2023, 10, 659-678. [CrossRef]
- Hsieh, S.C.; Tsai, P.H.; Kuo, C.F.; et al.: Health-related quality of life improvement by adalimumab therapy in patients with rheumatoid arthritis in Taiwan: A nationwide prospective study. J Chin Med Assoc. 2023, 86, 366-374. [CrossRef]
- Tiosano, S,; Yavne, Y.; Watad, A.; et al.: The impact of tocilizumab on anxiety and depression in patients with rheumatoid arthritis. European Journal of Clinical Investigation 2020, 50, e13268. [CrossRef]
- Strand, V.; Boklage, S.H.; Kimura, T,; et. al: High levels of interleukin-6 in patients with rheumatoid arthritis are associated with greater improvements in health-related quality of life for sarilumab compared with adalimumab. Arthritis Res Ther. 2020, 22,250. [CrossRef]
- Edwards, J.C., Leandro, M.J.: Cambridge, G. B: Lymphocyte depletion therapy with rituximab in rheumatoid arthritis. Rheum Dis Clin North Am. 2004, 30 393-403. [CrossRef]
- Genovese, M.C.; Becker, J.-C.; Schiff, M.; Luggen, M.; Sherrer, Y.; Kremer, J.; Birbara, C.; Box, J.; Natarajan, K.; Nuamah, I.; et al. Abatacept for Rheumatoid Arthritis Refractory to Tumor Necrosis Factor α Inhibition. New Engl. J. Med. 2005, 353, 1114–1123. [CrossRef]
- Yirmiya, R.; Goshen, I. Immune modulation of learning, memory, neural plasticity and neurogenesis. Brain, Behav. Immun. 2011, 25, 181–213. [CrossRef]
- Dantzer, R.; O'COnnor, J.C.; Freund, G.G.; Johnson, R.W.; Kelley, K.W. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat. Rev. Neurosci. 2008, 9, 46–56. [CrossRef]
- Miwa, Y.; Nishimi, A.; Nishimi, S.; Saito, M.; Tokunaga, T.; Yanai, R.; Takahashi, R.; Wakabayashi, K.; Kasama, T.; Hosaka, M. Combined infliximab and methotrexate treatment improves the depressive state in rheumatoid arthritis patients more effectively than methotrexate alone. Eur. J. Rheumatol. 2014, 1, 147–149. [CrossRef]
- Miwa, Y.; Isojima, S.; Saito, M.; Ikari, Y.; Kobuna, M.; Hayashi, T.; Takahashi, R.; Kasama, T.; Hosaka, M.; Sanada, K. Comparative Study of Infliximab Therapy and Methotrexate Monotherapy to Improve the Clinical Effect in Rheumatoid Arthritis Patients. Intern. Med. 2016, 55, 2581–2585. [CrossRef]
- Mathias, S.D.; Colwell, H.H.; Miller, D.P.; Moreland, L.W.; Buatti, M.; Wanke, L. Health-related quality of life and functional status of patients with rheumatoid arthritis randomly assigned to receive etanercept or placebo. Clin. Ther. 2000, 22, 128–139. [CrossRef]
- Bae, S.-C.; Gun, S.C.; Mok, C.C.; Khandker, R.; Nab, H.W.; Koenig, A.S.; Vlahos, B.; Pedersen, R.; Singh, A. Improved health outcomes with Etanercept versus usual DMARD therapy in an Asian population with established rheumatoid arthritis. BMC Musculoskelet. Disord. 2013, 14, 13–13. [CrossRef]
- Machado, D.A.; Guzman, R.M.; Xavier, R.M.; Simon, J.A.; Mele, L.; Pedersen, R.; Ferdousi, T.; Koenig, A.S.; Kotak, S.; Vlahos, B. Open-Label Observation of Addition of Etanercept Versus a Conventional Disease-Modifying Antirheumatic Drug in Subjects With Active Rheumatoid Arthritis Despite Methotrexate Therapy in the Latin American Region. Am. J. Clin. Oncol. 2014, 20, 25–33. [CrossRef]
- Kekow, J.; Moots, R.J.; Emery, P.; Durez, P.; Koenig, A.; Singh, A.; Pedersen, R.; Robertson, D.; Freundlich, B.; Sato, R. Patient-reported outcomes improve with etanercept plus methotrexate in active early rheumatoid arthritis and the improvement is strongly associated with remission: the COMET trial. Ann. Rheum. Dis. 2010, 69, 222–225. [CrossRef]
- Kekow, J.; Moots, R.; Khandker, R.; Melin, J.; Freundlich, B.; Singh, A. Improvements in patient-reported outcomes, symptoms of depression and anxiety, and their association with clinical remission among patients with moderate-to-severe active early rheumatoid arthritis. Rheumatology 2010, 50, 401–409. [CrossRef]
- Curtis, J.R.; Herrem, C.; Ndlovu, ’.N.; O’bRien, C.; Yazici, Y. A somatization comorbidity phenotype impacts response to therapy in rheumatoid arthritis: post-hoc results from the certolizumab pegol phase 4 PREDICT trial. Arthritis Res. Ther. 2017, 19, 1–11. [CrossRef]
- Harrold, L.R.; John, A.; Reed, G.W.; Haselkorn, T.; Karki, C.; Li, Y.; Best, J.; Zlotnick, S.; Kremer, J.M.; Greenberg, J.D. Impact of Tocilizumab Monotherapy on Clinical and Patient-Reported Quality-of-Life Outcomes in Patients with Rheumatoid Arthritis. Rheumatol. Ther. 2017, 4, 405–417. [CrossRef]
- Manning-Bennett, A.T.; Hopkins, A.M.; Sorich, M.J.; Proudman, S.M.; Foster, D.J.; Abuhelwa, A.Y.; Wiese, M.D. The association of depression and anxiety with treatment outcomes in patients with rheumatoid arthritis – a pooled analysis of five randomised controlled trials. Ther. Adv. Musculoskelet. Dis. 2022, 14. [CrossRef]
- Behrens, F.; Burmester, G.-R.; Hofmann, M.W.; Aringer, M.; Kellner, H.; Liebhaber, A.; Wassenberg, S.; Peters, M.A.; Zortel, M.; Amberger, C. Sustained effectiveness and safety of subcutaneous tocilizumab over two years in the ARATA observational study. Clin. Exp. Rheumatol. 2022, 41, 1463–1472. [CrossRef]
- Sun, Y.; Wang, D.; Salvadore, G.; Hsu, B.; Curran, M.; Casper, C.; Vermeulen, J.; Kent, J.M.; Singh, J.; Drevets, W.C.; et al. The effects of interleukin-6 neutralizing antibodies on symptoms of depressed mood and anhedonia in patients with rheumatoid arthritis and multicentric Castleman’s disease. Brain, Behav. Immun. 2017, 66, 156–164. [CrossRef]
- Dhillon, S. Intravenous Tocilizumab: A Review of Its Use in Adults with Rheumatoid Arthritis. BioDrugs 2013, 28, 75–106. [CrossRef]
- Persoons, P.; Vermeire, S.; Demyttenaere, K.; Fischler, B.; Vandenberghe, J.; VAN Oudenhove, L.; Pierik, M.; Hlavaty, T.; VAN Assche, G.; Noman, M.; et al. The impact of major depressive disorder on the short- and long-term outcome of Crohn's disease treatment with infliximab. Aliment. Pharmacol. Ther. 2005, 22, 101–110. [CrossRef]
- Minderhoud, I.M. Crohn’s disease, fatigue, and infliximab: Is there a role for cytokines in the pathogenesis of fatigue?. World J. Gastroenterol. 2007, 13, 2089–93. [CrossRef]
- Krishnan, R.; Cella, D.; Leonardi, C.; Papp, K.; Gottlieb, A.; Dunn, M.; Chiou, C.; Patel, V.; Jahreis, A. Effects of etanercept therapy on fatigue and symptoms of depression in subjects treated for moderate to severe plaque psoriasis for up to 96 weeks. Br. J. Dermatol. 2007, 157, 1275–1277. [CrossRef]
- Tyring, S.; Gottlieb, A.; Papp, K.; Gordon, K.; Leonardi, C.; Wang, A.; Lalla, D.; Woolley, M.; Jahreis, A.; Zitnik, R.; et al. Etanercept and clinical outcomes, fatigue, and depression in psoriasis: double-blind placebo-controlled randomised phase III trial. Lancet 2006, 367, 29–35. [CrossRef]
- Uzzan, S.; Azab, A.N. Anti-TNF-α Compounds as a Treatment for Depression. Molecules 2021, 26, 2368. [CrossRef]
- Ertenli, I.; Ozer, S.; Kiraz, S.; Apras, S.B.; Akdogan, A.; Karadag, O.; Calguneri, M.; Kalyoncu, U. Infliximab, a TNF-alpha antagonist treatment in patients with ankylosing spondylitis: the impact on depression, anxiety and quality of life level. Rheumatol. Int. 2010, 32, 323–330. [CrossRef]
- Webers, C.; Stolwijk, C.; Schiepers, O.; Schoonbrood, T.; van Tubergen, A.; Landewé, R.; van der Heijde, D.; Boonen, A. Infliximab treatment reduces depressive symptoms in patients with ankylosing spondylitis: an ancillary study to a randomized controlled trial (ASSERT). Arthritis Res. Ther. 2020, 22, 1–11. [CrossRef]
- Karson, A.; Demirtaş, T.; Bayramgürler, D.; Balcı, F.; Utkan, T. Chronic Administration of Infliximab (TNF-α Inhibitor) Decreases Depression and Anxiety-like Behaviour in Rat Model of Chronic Mild Stress. Basic Clin. Pharmacol. Toxicol. 2012, 112, 335–340. [CrossRef]
- Bayramgürler, D.; Karson, A.; Özer, C.; Utkan, T. Effects of long-term etanercept treatment on anxiety- and depression-like neurobehaviors in rats. Physiol. Behav. 2013, 119, 145–148. [CrossRef]
- Mansur, R.B.; Delgado-Peraza, F.; Subramaniapillai, M.; Lee, Y.; Iacobucci, M.; Rodrigues, N.; Rosenblat, J.D.; Brietzke, E.; Cosgrove, V.E.; Kramer, N.E.; et al. Extracellular Vesicle Biomarkers Reveal Inhibition of Neuroinflammation by Infliximab in Association with Antidepressant Response in Adults with Bipolar Depression. Cells 2020, 9, 895. [CrossRef]
- Mansur, R.B.; Subramaniapillai, M.; Lee, Y.; Pan, Z.; Carmona, N.E.; Shekotikhina, M.; Iacobucci, M.; Rodrigues, N.; Nasri, F.; Rashidian, H.; et al. Leptin mediates improvements in cognitive function following treatment with infliximab in adults with bipolar depression. Psychoneuroendocrinology 2020, 120, 104779. [CrossRef]
- Mansur, R.B.; Subramaniapillai, M.; Lee, Y.; Pan, Z.; Carmona, N.E.; Shekotikhina, M.; Iacobucci, M.; Rodrigues, N.; Nasri, F.; Rosenblat, J.D.; et al. Effects of infliximab on brain neurochemistry of adults with bipolar depression. J. Affect. Disord. 2021, 281, 61–66. [CrossRef]
Figure 1.
Flowchart of study selection. Diagram illustrating the process of identifying and selecting studies included in this review.
Figure 1.
Flowchart of study selection. Diagram illustrating the process of identifying and selecting studies included in this review.
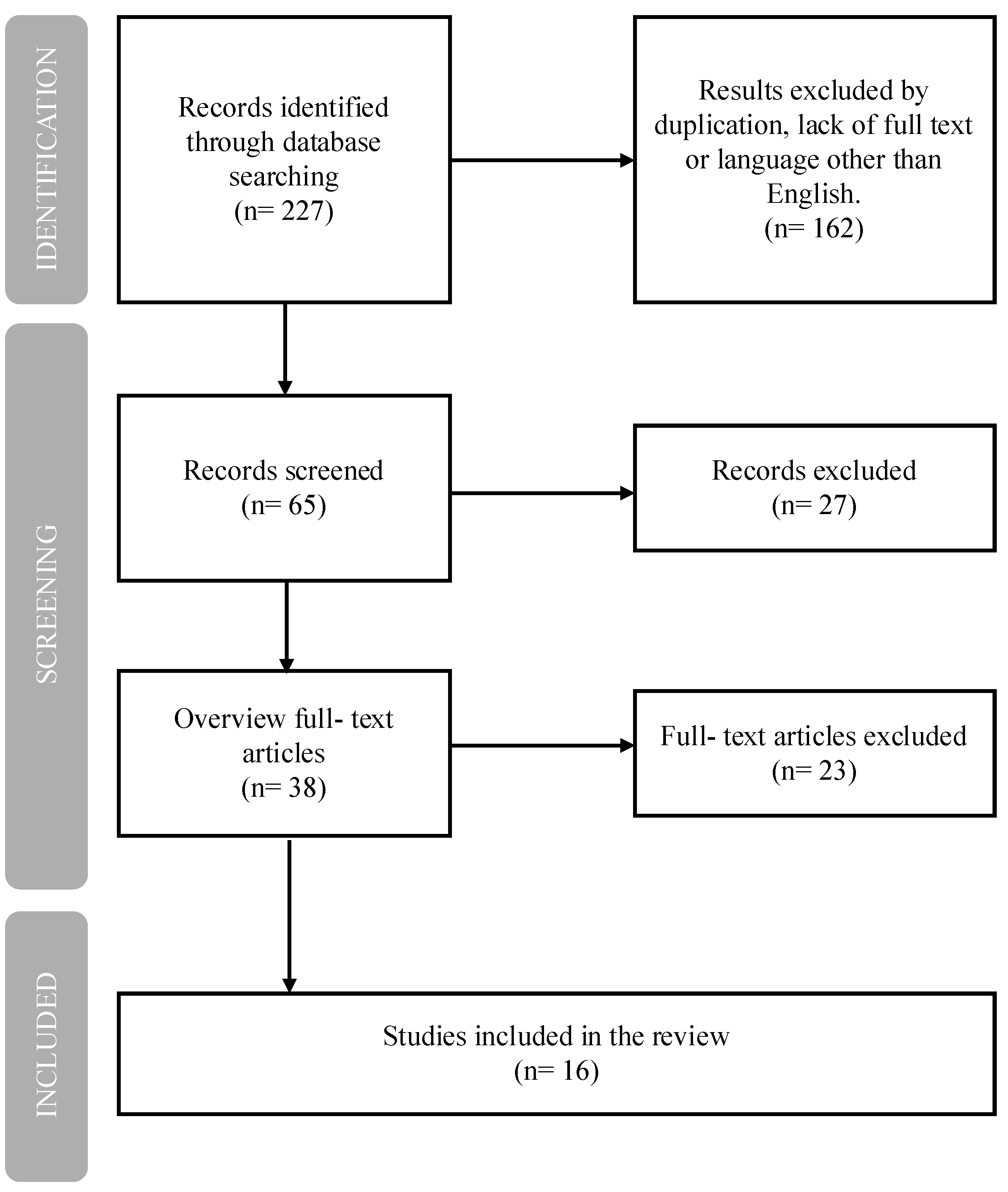

Table 1.
Summary of biologic agents targeting TNF-α and IL-6 pathways in rheumatoid arthritis, including origin, class, molecular structure, and mechanism of action *.
Table 1.
Summary of biologic agents targeting TNF-α and IL-6 pathways in rheumatoid arthritis, including origin, class, molecular structure, and mechanism of action *.
| Generic Name | Trade Name Original, Biosimilars |
Group | Molecule Type | Mechanism of Action | |
| ADL | Adalimumab | Humira, Amgevita, Hyrimoz, Idacio, Hulio, Amsparity, Imraldi | anti-TNF | Fully human monoclonal IgG1 antibody | Neutralizes TNF-α (soluble and membrane-bound forms); blocks p55/p75 receptors |
| CZP | Certolizumab Pegol | Cimzia | anti-TNF | Humanized Fab’ fragment conjugated with PEG | Neutralizes TNF-α; lacks Fc-mediated effects |
| IFX | Infliximab | Remicade, Inflectra, Remsima, Flixabi, Zessly | anti-TNF | Chimeric IgG1 monoclonal antibody (human-mouse) | Blocks TNF-α; inhibits inflammatory pathways |
| ETN | Etanercept | Enbrel, Benepali, Erelzi | anti-TNF | Fusion protein: p75 TNF receptor + Fc IgG1 | Binds TNF-α and TNF-β; acts as a decoy receptor |
| GLM | Golimumab | Simponi (s.c.), Simponi Aria (i.v.) | anti-TNF | Fully human monoclonal IgG1 antibody | Blocks TNF-α; inhibits inflammatory pathways |
| SRK | Sirukumab | None (discontinued, never approved) | anti-IL-6 | Fully human monoclonal IgG1 antibody | Neutralizes IL-6 (the cytokine, not the receptor) |
| SARI | Sarilumab | Kevzara | anti-IL-6R | Fully human monoclonal IgG1 antibody | Blocks IL-6 receptor (soluble and membrane-bound) |
| TCZ | Tocilizumab | RoActemra (EU), Actemra (USA) | anti-IL-6R | Humanized monoclonal IgG1 antibody | Blocks IL-6 receptor (soluble and membrane-bound) |
| * Only biologic drugs used in RA with documented effects on TNF-α or IL-6 pathways are included. Other biologics, such as rituximab (anti-CD20) or abatacept (T-cell costimulation inhibitor), were excluded as they are beyond the scope of this analysis focusing on neuropsychiatric outcomes. Abbreviations: ADL, adalimumab; CZP, certolizumab pegol; IFX, infliximab; ETN, etanercept; GLM, golimumab; SRK, sirukumab; SARI, sarilumab; TCZ, tocilizumab; TNF, tumor necrosis factor; IL-6, interleukin-6; IL-6R, interleukin-6 receptor; IgG1, immunoglobulin G1; Fab’, antigen-binding fragment; PEG, polyethylene glycol; Fc, crystallizable fragment of antibody; s.c., subcutaneous; i.v., intravenous. | |||||
Table 2.
Studies assessing impact of TNF-α inhibitors on depression and quality of life in RA patients.
Table 2.
Studies assessing impact of TNF-α inhibitors on depression and quality of life in RA patients.
| Study | Study Design (treatment length) | Biologic agent | Measure | Outcome |
| Miwa et al. 2014 [23] | Pilot study (30 weeks) | IFX (n=34) vs MTX (n=42) | SDS | IFX significantly improved depression vs. MTX |
| Miwa et al. 2016 [24] | Open-label cohort (6months) | IFX (n=60) vs MTX (n=53) | HAM-D | No significant difference between IFX and MTX |
| Bringham et al. 2023 [15] | Observational Phase 4 AWARE (52 weeks) | GAL (n=685) vs IFX (n= 585) | PROMIS | Improvement in all PROMIS domains incl. depression |
| Curtis et al. 2017 [ 30] | RCT Phase 4 PREDICT (52 weeks) | CZP (n=733) | Clinical data | SCP phenotype: lower treatment response, more AEs |
| Mathias et al. 2000 [25] | RCT Phase 3, double-blind (6 months) | ETN (n= 76) vs placebo (n=80) | SF-36 MOS | ETN > placebo in improving depressive symptoms |
| Bae et al. 2013[26] | Open label, multicentre (16 weeks) | ETN+MTX (n=197) vs DMARDs +MTX (n=103) | HADS | Greater improvements in ETN+MTX group (HADS) |
| Machado et al. 2014 [27] | Open label, randomized (24 weeks) | ETN+MTX (n=281) vs DMARDs+MTX (n=142) | HADS | Improvements observed in ETN+MTX depressive domains |
| Kekow et al. 2010 [28] | RCT double-blind, COMET 104 weeks | ETN+MTX (n= 274) vs MTX (n= 268) | HADS | ETN+MTX better than MTX alone in PROs |
| Kekow et al. 2011 [29] | RCT double-blind, COMET⃰ 104 weeks | ETN+MTX vs MTX | HADS | Clinical remission reduced depressive symptoms |
| Hsieh et al. 2023 [16] | Observational 24 weeks | ADL (n=100) | EQ-5D -3L | Improvements from baseline to weeks 12, 24 |
| Abbreviations: IFX, infliximab; GAL, golimumab; CZP, certolizumab pegol; ETN, etanercept; ADL, adalimumab; MTX, methotrexate; DMARDs, disease-modifying anti-rheumatic drugs; SDS, Self-Rating Depression Scale; HAM-D, Hamilton Depression Rating Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; SF-36 MOS, Medical Outcomes Study 36-Item Short Form Survey; HADS, Hospital Anxiety and Depression Scale; EQ-5D-3L, EuroQol 5 Dimensions 3 Level questionnaire; RCT, randomized controlled trial; AEs, adverse events; PROs, patient-reported outcomes. ⃰Note1: The studies by Kekow et al. (2010 and 2011) are based on the same COMET trial population Note2: The total sample includes 3,027 participants across all TNF-α inhibitor studies. Among them, approximately 2,211 patients received active treatment with a TNF-α inhibitor, either as monotherapy or in combination with methotrexate (MTX), compared to placebo, MTX alone, or standard care | ||||
Table 3.
Studies assessing impact of IL-6 inhibitors on depression and quality of life in RA patients.
Table 3.
Studies assessing impact of IL-6 inhibitors on depression and quality of life in RA patients.
| Study | Study Design/ duration | Biologic agent (n) | Measures | Outcome |
| Tiosano et al.2020 [17] | Observational 24weeks |
TCZ (n=91) | HDRS | 66% of patients achieved improvements in depressive domains. |
| Harrold et al. 2017[31] | Observational cohort study 1 year |
TCZ (n= 255) | EQ-5D | 20% to 36% of patients achieved improvements in depressive state. |
| Manning- Bennett et al. 2022[32] | 5 RCT | TCZ vs DMARDs (n=5502) | Clinical | Comorbid depression was associated with less frequent remission (CDAI and SDAI) |
| Behrens 2021 et al.[33] | Observational ARATA 52 weeks | TCZ (n= 1300) | BDI-II | Patients achieved improvements in DAS-28 and PROs; however, patients with depression presented lower response and higher adverse events rates. |
| Sun et al. 2017[34] | Post hoc analysis RCT 24 weeks |
sirukumab vs siltuximab (n=176) | PDMA includinngSF-36 | Baseline solute IL-6 receptors level predicted mental health benefit. The improvement in depressive state by sirukumab correlated positivieliy with the baseline solute IL-6R levels. |
| Strand et al. 2020 [18] | Post hoc analysis RCT MONARCH phase 3 and they were treated for 24 weeks | SARI or ADL (n=148) | SF-36 | IL-6 blockade > TNF-alpha in QoL gains no difference in the mental statate. high besline IL-6 levels better improvements in physical domains with SARI compared to ADL. |
| Abbreviations: HDRS (Hamilton Depression Rating Scale); EQ-5D (EuroQol-5 dimensions-5); DMARDs (Disease-Modifying Antirheumatic Drugs); CDAI (Clinical Disease Activity Index); SDAI (Simple Disease Activity Index); PROs (Patient- Reported Outocmes); BDI (Beck Depression Inventory), PDMA (Prevalent Depressed Mood and Anhedonia); SF-36 (Short Form Survey); n- number of participants. Note: The total sample includes 7,472 participants across all IL-6 or IL-6R inhibitor studies. Approximately 4,609 patients received active treatment with an IL-6 pathway inhibitor, either alone or in combination with MTX, and were compared to MTX, placebo, or conventional DMARDs. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



