Submitted:
30 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare but fatal malignancy-related complication characterized by tumor embolization in small pulmonary arteries, leading to acute respiratory failure and pulmonary hypertension. Neurotrophic tropomyosin receptor kinase (NTRK) gene fusion-positive colorectal cancer (CRC) is resistant to conventional chemotherapy but responds to tropomyosin receptor kinase (TRK) inhibitors.
We report a case of a 70-year-old male with advanced transverse colon adenocarcinoma and peritoneal metastases who developed PTTM despite a marked response to entrectinib. Postmortem findings confirmed tumor emboli, fibrocellular intimal thickening, and thrombosis within the pulmonary arteries.
Given the aggressive nature of PTTM, treatment strategies must extend beyond tumor suppression to include antiangiogenic therapy and targeted inhibition of cytokines and growth factors. This case underscores the importance of integrating TRK inhibition with approaches that mitigate mediator-induced pulmonary hypertension. Further research into predictive biomarkers and optimized therapeutic strategies combining TRK inhibitors with antiangiogenic agents is warranted to improve outcomes in NTRK fusion-positive CRC patients at risk of PTTM.
Keywords:
Pulmonary tumor thrombotic microangiopathy
; neurotrophic tropomyosin receptor kinase gene fusion
; pulmonary hypertension
; acute respiratory failure
; right heart failure
; entrectinib
; transverse colon cancer
Introduction
Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare yet aggressive pulmonary vascular complication of malignancies characterized by tumor embolization in small pulmonary arteries, leading to acute respiratory failure and pulmonary hypertension (PH). The obstruction of the pulmonary microvasculature triggers fibrocellular proliferation and secondary coagulation cascade activation, resulting in rapid clinical deterioration and high mortality rates [1,2,3]. Owing to its nonspecific imaging features and fulminant progression, PTTM is often diagnosed postmortem [2,3]. Patients commonly present with dyspnea, hypoxia, thrombocytopenia, and signs of a hypercoagulable state.
Colorectal cancer (CRC) ranks as the third most commonly diagnosed malignancy worldwide and remains the second leading cause of cancer-related mortality [4]. While conventional chemotherapy forms the backbone of treatment, rare molecular subtypes, – such as neurotrophic receptor kinase (NTRK) gene fusion-positive CRC, – require distinct therapeutic approaches [5]. NTRK gene fusion leads to constitutive activation of tropomyosin receptor kinase (TRK) signaling, driving oncogenesis via the MAPK and PI3K pathways [6,7]. Although TRK inhibitors, such as larotrectinib and entrectinib, have demonstrated efficacy in treating NTRK fusion-positive CRC, the mechanisms underlying disease progression, – including the development of PTTM, - remain poorly understood.
Case Presentation
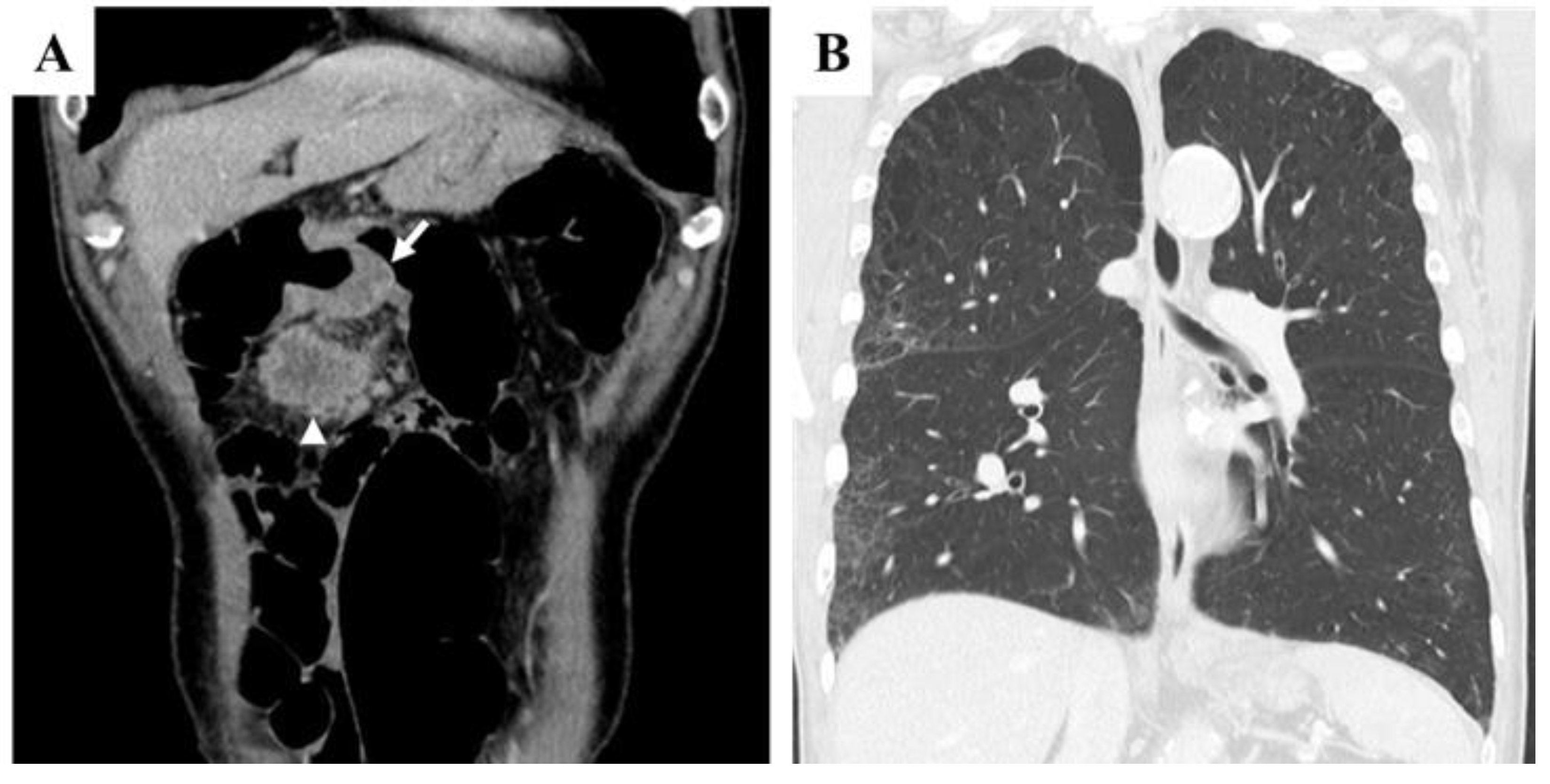
A 70-year-old Japanese male with a history of smoking and alcohol consumption underwent an annual health check-up, during which a fecal occult blood test returned positive for the first time. Subsequent investigations led to a diagnosis of transverse colon cancer with peritoneal metastases. Contrast-enhanced computed tomography (CECT) revealed an irregular mass in the transverse colon near the hepatic flexure, along with multiple peritoneal nodules primarily localized to the greater omentum [Figure 1A]. Chest CT revealed multiple blebs in both lung apices and a reticular pattern in the right lung [Figure 1B]. Despite peritoneal dissemination, no hematogenous or lymphatic metastases were evident at this stage.
Figure 1.
Pretreatment findings from abdominal contrast-enhanced CT and chest CT. A: Coronal section view showing a tumor in the transverse colon near the hepatic flexure (arrow) and a peritoneal metastatic nodule located just caudal to the primary tumor (arrowhead). Several additional peritoneal metastatic nodules were observed along the greater omentum (not shown). B: Chest CT revealed multiple blebs in both lung apices, along with a reticular pattern in the right lung lobes.
Figure 1.
Pretreatment findings from abdominal contrast-enhanced CT and chest CT. A: Coronal section view showing a tumor in the transverse colon near the hepatic flexure (arrow) and a peritoneal metastatic nodule located just caudal to the primary tumor (arrowhead). Several additional peritoneal metastatic nodules were observed along the greater omentum (not shown). B: Chest CT revealed multiple blebs in both lung apices, along with a reticular pattern in the right lung lobes.
Initial laboratory findings revealed elevated tumor markers, including carcinoembryonic antigen (CEA) at 55.0 ng/ml and carbohydrate antigen 19-9 (CA19-9) at 2527.6 U/ml. Genetic analysis confirmed that the tumor was RAS/BRAF wild-type and microsatellite instability (MSI)-negative. The patient had a history of emphysema but did not require supplemental oxygen therapy.
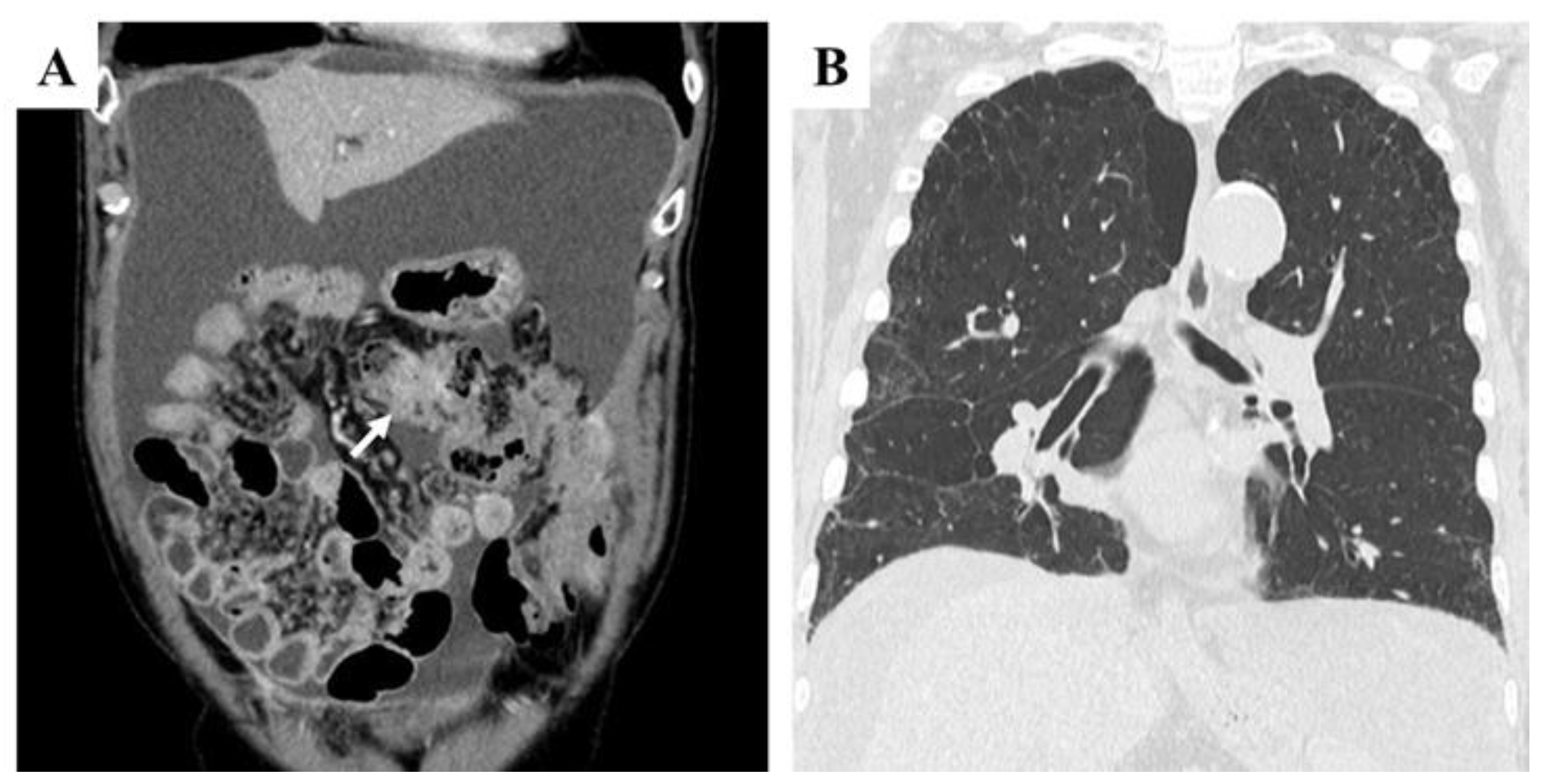
The initial treatment regimen consisted of capecitabine, oxaliplatin, and cetuximab. However, after three cycles, imaging indicated disease progression, with an increase in peritoneal disseminated nodules. Chemotherapy was subsequently modified to capecitabine plus irinotecan and bevacizumab. Despite eight cycles, significant ascites accumulation and mesenteric shortening were observed [Figure 2A]. At this stage, the tumor remained an irregular mass without evidence of hematogenous metastases, although concerns about rapid disease progression persisted. Compared with pretreatment findings, chest CT revealed no significant worsening of reticular or interstitial shadows [Figure 2B].
Figure 2.
Abdominal contrast-enhanced CT (CECT) and chest CT findings after eight cycles of chemotherapy with capecitabine, irinotecan, and bevacizumab, following resistance to capecitabine, oxaliplatin, and cetuximab. A: Coronal section view showing a large volume of ascitic fluid and mesenteric shortening. The tumor in the transverse colon appeared as an irregular mass (arrow). B: Chest CT revealed no significant progression of reticular or interstitial shadows compared with pretreatment findings.
Figure 2.
Abdominal contrast-enhanced CT (CECT) and chest CT findings after eight cycles of chemotherapy with capecitabine, irinotecan, and bevacizumab, following resistance to capecitabine, oxaliplatin, and cetuximab. A: Coronal section view showing a large volume of ascitic fluid and mesenteric shortening. The tumor in the transverse colon appeared as an irregular mass (arrow). B: Chest CT revealed no significant progression of reticular or interstitial shadows compared with pretreatment findings.
A final attempt at chemotherapy with trifluridine/tipiracil (FTD/TPI) plus bevacizumab was initiated. Despite three additional cycles, the disease continued to progress. Given the need for alternative therapeutic strategies, a genetic panel analysis was performed, revealing an NTRK1-LMNA gene fusion. Considering the established efficacy of TRK inhibitors in NTRK fusion-positive malignancies, entrectinib treatment was promptly initiated.
Within six weeks of entrectinib treatment, the patient exhibited a remarkable response. Tumor marker levels decreased significantly, with CA19-9 levels decreasing from over 24,000 U/ml to 2,470.2 U/ml. Clinically, ascites accumulation stabilized, and three rounds of cell-free and concentration ascites reinfusion therapy (CART) were performed to manage symptoms. Throughout this period, the patient remained relatively stable and continued outpatient care.
Two months after receiving entrectinib therapy, the patient developed sudden dyspnea, fever, and hypoxia, necessitating emergency hospitalization. Upon transport, his peripheral oxygen saturation was critically low at 50% on room air, improving only marginally to the low 80s with 15 liters of oxygen. Upon admission, his vital signs included a blood pressure of 102/56 mmHg, a pulse rate of 80 beats per minute, a respiratory rate of 20 breaths per minute, and a temperature of 38.5°C.
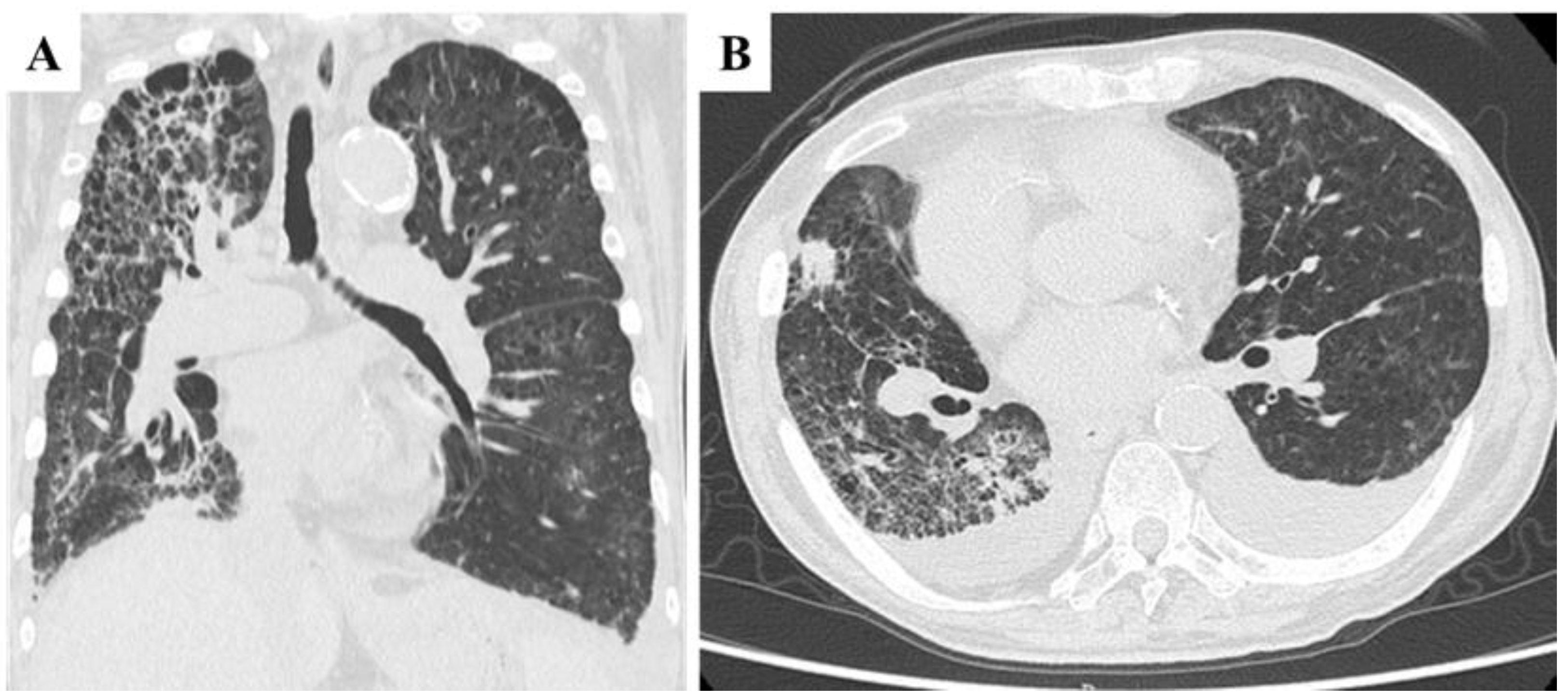
High-flow oxygen therapy was initiated; however, oxygen saturation remained precarious. The laboratory findings revealed worsening anemia, elevated liver enzymes, and significantly increased C-reactive protein (CRP) levels, suggesting a systemic inflammatory response. Chest CT imaging revealed marked progression of interstitial pneumonia in both lungs, which was most pronounced in the right lobe [Figure 3A]. Newly developed ground-glass opacities appeared in previously normal lung regions amid areas of emphysema. Additional findings included multiple infiltrative shadows, mild right lung volume reduction, and bilateral pleural effusion [Figure 3B]. These observations suggested worsening interstitial pneumonia with possible concomitant bacterial infection or drug-related lung toxicity. CT imaging of the chest and abdomen revealed no evidence of hematogenous metastasis, such as lung or liver involvement.
Figure 3.
Chest CT findings at the time of transport due to acute respiratory failure. A and B: Marked deterioration of interstitial pneumonia was observed in both lobes, with the most pronounced changes in the right lobe. Ground-glass opacities appeared against a background of emphysematous lungs, accompanied by multiple infiltrative shadows, mild right lung volume reduction (A), and bilateral pleural effusion (B).
Figure 3.
Chest CT findings at the time of transport due to acute respiratory failure. A and B: Marked deterioration of interstitial pneumonia was observed in both lobes, with the most pronounced changes in the right lobe. Ground-glass opacities appeared against a background of emphysematous lungs, accompanied by multiple infiltrative shadows, mild right lung volume reduction (A), and bilateral pleural effusion (B).
By the third day of hospitalization, signs of right-sided heart failure, including jugular vein distention and peripheral edema, had become apparent. Echocardiography revealed a peak tricuspid regurgitation velocity (TRV) of 4.5 m/s, a tricuspid regurgitation pressure gradient (TRPG) of 82.8 mmHg, and an estimated systolic pulmonary artery pressure (SPAP) of 86 mm Hg, consistent with a diagnosis of severe pulmonary hypertension. Given the suspected presence of tumor emboli within pulmonary vessels, PTTM was considered a potential underlying cause.
Despite the discontinuation of entrectinib—due to the inability to rule out drug-induced lung injury—and the initiation of empirical antibiotic therapy with meropenem and methylprednisolone, the patient’s condition continued to deteriorate. The worsening of the pleural effusion necessitated bilateral thoracentesis for symptom relief. As pulmonary function decreases, entrectinib is reintroduced on the basis of the hypothesis that tumor embolization within pulmonary arteries drives disease progression, although clinically, there was no evidence of hematogenous metastasis to other organs.
Despite these efforts, the patient’s respiratory distress worsened, and he passed away seven weeks after hospitalization. An autopsy was performed with the family’s consent.
Autopsy Findings
Macroscopic Findings:
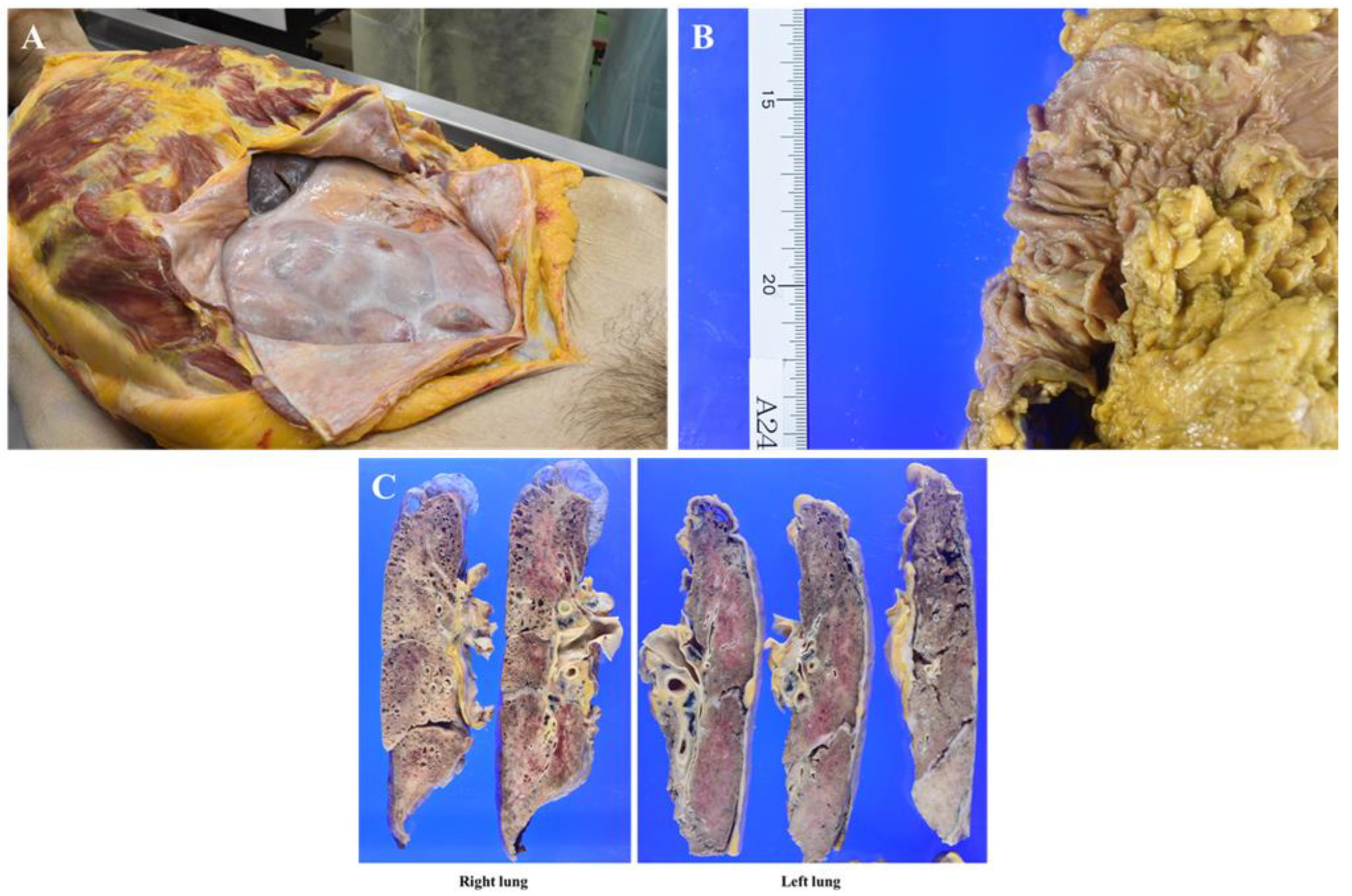
In the right thoracic cavity, minor adhesions were observed alongside 500 mL of clear yellowish pleural effusion. In contrast, the left thoracic cavity exhibited severe adhesions, making lung removal difficult, with almost no pleural effusion present. The abdominal cavity displayed extensive fibrous adhesions, with white fibrous tissue uniformly covering the serosal surfaces of the intestinal tract, leading to firm intersegmental adhesions (Figure 4A). No discernible mass lesions were present on the serosal surfaces, and ascites was minimal. The primary transverse colon lesion had significantly regressed, leaving a 3 cm square mucosal area containing several polyps, the largest measuring up to 1 cm (Figure 4B). No additional mass lesions, including disseminated foci, were detected in the abdominal cavity.
Prominent lymph node enlargement was noted in the abdominal cavity and along the periaorta. The lungs exhibited diffuse consolidation with areas of sclerosis, along with apical bullae and microcystic changes, which are likely associated with smoking (Figure 4C). No metastatic mass lesions were found within the lung parenchyma; however, multiple hilar lymphadenopathies were observed. The heart, liver, and kidneys showed no significant abnormalities.
Figure 4.
Macroscopic autopsy findings. A: The intestinal tract is uniformly covered with white fibrous tissue, leading to extensive adhesion between structures. B: The primary lesion in the transverse colon has markedly decreased in size following effective treatment, appearing as clustered polyps within a 3 cm square area, the largest measuring up to 1 cm. C: Cross-sections of both lungs revealing diffuse consolidation, apical bullae, and multiple small cysts. The left lung was adherent to the parietal pleura, with enlargement of both hilar lymph nodes.
Figure 4.
Macroscopic autopsy findings. A: The intestinal tract is uniformly covered with white fibrous tissue, leading to extensive adhesion between structures. B: The primary lesion in the transverse colon has markedly decreased in size following effective treatment, appearing as clustered polyps within a 3 cm square area, the largest measuring up to 1 cm. C: Cross-sections of both lungs revealing diffuse consolidation, apical bullae, and multiple small cysts. The left lung was adherent to the parietal pleura, with enlargement of both hilar lymph nodes.
Microscopic Findings:
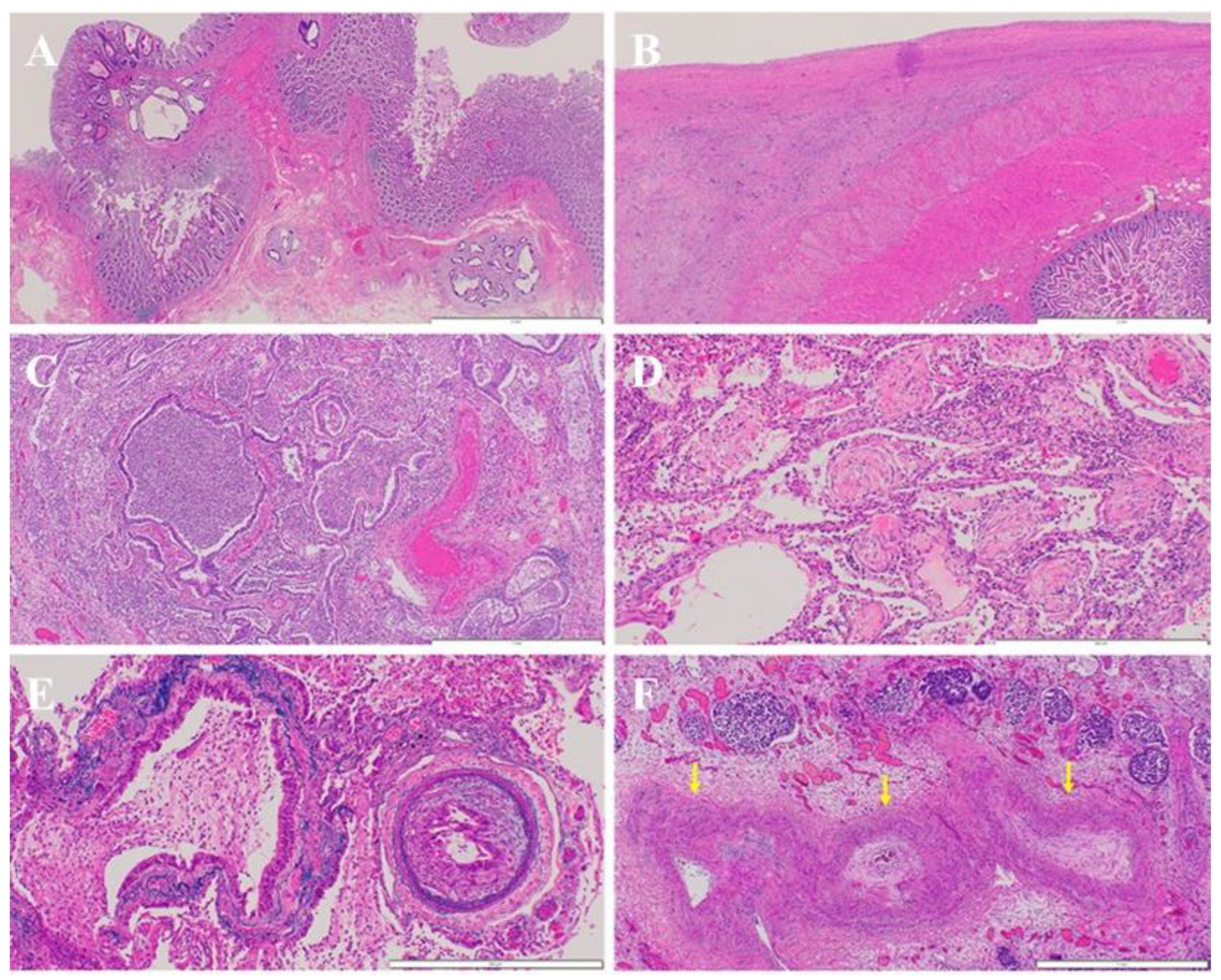
At the primary transverse colon site, chemotherapy has demonstrated significant efficacy, with well- to moderately differentiated tubular adenocarcinomas present in several polypoid areas within the mucosal layer. Scattered microscopic remnants were identified in the submucosal layer, although no evidence of lymphatic or venous invasion was observed (Figure 5A). Adenocarcinoma with extensive fibrosis was diffusely spread across the intestinal surface, leading to adherence and direct invasion of adjacent organs, including the stomach, liver, bladder, and diaphragm (Figure 5B). Additionally, widespread dissemination of adenocarcinoma was noted in the left thoracic cavity. Tumor emboli within lymphatic vessels have been identified across multiple organs, including the stomach, bladder, and pleura. With respect to lymph node metastasis, multiple metastatic lesions were present in the abdominal cavity, pulmonary hilum, and para-aortic region.
In the lungs, diffuse bronchopneumonia and organizing pneumonia were observed (Figure 5C, D), likely resulting from aspiration pneumonia, although drug-related effects contributing to organizing pneumonia could not be entirely excluded. Histopathological findings consistent with PTTM were identified in both lungs, characterized by tumor emboli, fibrous intimal thickening, and thrombus formation within numerous small pulmonary arteries (Figure 5E, F). Additionally, a small number of embolized lymphatic vessels were observed. No hematogenous metastatic lesions were found in the lung tissue, highlighting the distinct vascular involvement characteristic of PTTM.
Figure 5.
Microscopic findings at autopsy. A: At the primary site in the transverse colon, chemotherapy was highly effective, with well- to moderately differentiated adenocarcinomas observed in several polypoid regions within the mucosal layer. Microscopically, scattered remnants were detected in the submucosal layer, but no evidence of lymphatic or venous invasion was found (white bar at bottom right: 2 mm). B: Adenocarcinoma with severe fibrosis diffusely infiltrated the intestinal tract, leading to adhesion to its surface (white bar at bottom right: 2 mm). C and D: In the lungs, diffuse bronchopneumonia (C) and organizing pneumonia (D) were observed. E and F: Findings consistent with PTTM were identified. A small pulmonary artery was embolized by adenocarcinoma (E; Victoria blue and hematoxylin‒eosin staining), whereas another pulmonary artery exhibited a narrowed lumen due to intimal thickening (F; arrows) (E: white bar at bottom right: 500 µm; F: white bar at bottom right: 1 mm).
Figure 5.
Microscopic findings at autopsy. A: At the primary site in the transverse colon, chemotherapy was highly effective, with well- to moderately differentiated adenocarcinomas observed in several polypoid regions within the mucosal layer. Microscopically, scattered remnants were detected in the submucosal layer, but no evidence of lymphatic or venous invasion was found (white bar at bottom right: 2 mm). B: Adenocarcinoma with severe fibrosis diffusely infiltrated the intestinal tract, leading to adhesion to its surface (white bar at bottom right: 2 mm). C and D: In the lungs, diffuse bronchopneumonia (C) and organizing pneumonia (D) were observed. E and F: Findings consistent with PTTM were identified. A small pulmonary artery was embolized by adenocarcinoma (E; Victoria blue and hematoxylin‒eosin staining), whereas another pulmonary artery exhibited a narrowed lumen due to intimal thickening (F; arrows) (E: white bar at bottom right: 500 µm; F: white bar at bottom right: 1 mm).
The tumor mutational burden (TMB) was 1.26 mut/Mb, indicating a relatively low level of genetic alterations.
A definitive postmortem diagnosis of PTTM was established, suggesting that the condition led to severe PH and right heart failure, progressing rapidly over a short period.
Discussion
PTTM is a rare but fatal complication of malignancy characterized by tumor microemboli-induced fibrocellular intimal proliferation, vascular remodeling, and progressive PH [8]. Unlike conventional pulmonary embolism, PTTM is mediated by cytokine-driven vascular pathology, particularly platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF), which trigger endothelial activation, intimal thickening, and microvascular obstruction [2].
The diagnosis of PTTM is exceptionally difficult during life because of its rapid progression and nonspecific clinical and radiographic findings. Ground-glass opacities, interstitial lung patterns, and pleural effusion may mimic chemotherapy-induced pneumonitis or infection, delaying recognition and treatment. Therefore, in patients with malignancies who present with sudden respiratory failure and PH during therapy, a high index of suspicion for PTTM is essential.
The patient demonstrated resistance to conventional chemotherapies, including cetuximab and bevacizumab; however, entrectinib showed remarkable antitumor activity. Unfortunately, during effective entrectinib treatment, the patient developed sudden-onset acute respiratory failure and right heart dysfunction due to PH. Postmortem diagnosis revealed PTTM, which was rapidly fatal.
This case underscores the importance of recognizing PTTM in patients with malignancies presenting with acute respiratory failure during systemic therapy. This highlights the critical need for early detection and comprehensive therapeutic strategies that extend beyond tumor control to address cancer-associated vascular complications and improve patient outcomes.
Interestingly, there was no evidence of hematogenous metastasis in this case, yet prominent lymphovascular invasion suggested possible dissemination through the thoracic duct, bypassing conventional venous circulation. Given the rarity of NTRK fusion-positive CRC, its metastatic behavior remains poorly understood. Some reports suggest a proclivity for lymphatic spread, which may contribute to PTTM pathogenesis and warrants further investigation into alternative routes of tumor embolization [3].
NTRK gene fusions result in constitutive activation of TRK receptors and serve as oncogenic drivers across multiple cancer types [9]. In CRC, LNMA:NTRK1 and TPM3:NTRK1 are among the most common fusion partners [9]. These tumors are typically RAS/BRAF wild-type and resistant to anti-EGFR therapies [10]. While frequently associated with MSI-high and high TMB, a subset of NTRK fusion-positive CRCs, – such as in the present case, – may be microsatellite stable, reflecting molecular heterogeneity within this rare group [10,14].
Despite the dramatic tumor regression observed with entrectinib, PTTM progresses rapidly, ultimately leading to a fatal outcome. This dissociation between tumor control and pulmonary vascular complications emphasizes that effective antitumor therapy alone may not be sufficient for managing certain malignancies with systemic complications. Given the involvement of PDGF and VEGF in PTTM pathogenesis, antiangiogenic therapies, – such as imatinib and bevacizumab, – may offer therapeutic benefits [15]. Additionally, targeted agents previously considered ineffective in standard settings might play a crucial role when applied within a multimodal framework tailored to both tumor biology and vascular involvement.
Conclusions
This case highlights the critical role of integrating antiangiogenic strategies into treatment protocols for patients with malignancies at risk of PTTM. Future research should prioritize the identification of predictive biomarkers for PTTM development within molecularly classified CRC subtypes. Furthermore, therapeutic approaches combining TRK inhibition with antiangiogenic therapy warrant further investigation to optimize treatment efficacy and improve patient outcomes.
Author Contributions
HN contributed to the formulation of treatment policies for patients following acute changes through conference participation and was responsible for drafting the manuscript. SO oversaw the entire treatment process, including diagnostic evaluations, chemotherapy, and postacute care, and played a key role in manuscript revision. AS, JI, and TY were actively involved in treatment policy discussions, postacute care management, and manuscript refinement. MK conducted pathological examinations and autopsies, providing critical interpretations of the results. All the authors have thoroughly reviewed and approved the final manuscript.
Funding
All the authors declare that they have received no financial support from any funds or similar sources.
Institutional Revies Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Marunouchi Hospital (25-8; July 14, 2025).
Informed Consent Statement
Written informed consent was obtained from the patient’s family for the publication of this case report and accompanying images.
Data Availability Statement
The dataset supporting the conclusion of this article is included within the article.
Conflicts of Interest
All the authors declare that they have no financial or nonfinancial competing interests.
Abbreviations
The following abbreviations are used in this manuscript:
| PTTM: Pulmonary tumor thrombotic microangiopathy CRC: Colorectal cancer NTRK: Neurotrophic tropomyosin receptor kinase TRK: Tropomyosin receptor kinase MAPK: Mitogen-activated protein kinase PI3K: Phosphatidylinositol-3 kinase CECT: Contrast-enhanced computed tomography CT: Computed tomography CEA: Carcinoembryonic antigen CA19-9: Carbohydrate antigen 19-9 RAS: Rat sarcoma virus BRAF: v-raf murine sarcoma viral oncogene homolog B MSI: Microsatellite instability FTD/TPI: Trifluridine/tipiracil LMNA: Lamin A/C CART: Cell-free and concentrated ascites reinfusion therapy CRP: C-reactive protein PH: Pulmonary hypertension TRV: Tricuspid regurgitation velocity TRPG: Tricuspid regurgitation pressure gradient SPAP: Systolic pulmonary artery pressure TMB: Tumor mutational burden PDGF: Platelet-derived growth factor VEGF: Vascular endothelial growth factor ETV6: E26 transformation-specific variant transcription 6 TPM3: Tropomyosin 3 |
References
- Von Herbay, A.; Illes, A.; Waldherr, R.; Otto, H.F. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer 1990, 66, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Godbole, R.H.; Saggar, R.; Kamangar, N. Pulmonary tumor thrombotic microangiography: a systemic review. Pulm Circ 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Uruga, H.; Fujii, T.; Kurosaki, A.; Hanada, S.; Takaya, H.; Miyamoto, A.; Morokawa, N.; Homma, S.; Kishi, K. Pulmonary tumor thrombotic microangiopathy: a clinical analysis of 30 autopsy cases. Intern Med 2013, 52, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Klink, A.J.; Kavati, A.; Gassama, A.; Kozlek, T.; Gajra, A.; Antoine, R. Treatment patterns of real-world patients with TRK fusion cancer treated by US community oncologists. Target Oncol 2022, 17, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Parrish, A.G.; Szulzewsky, F. TRKing down drug resistance in NTRK fusion-positive cancers. J Pathol 2024, 264, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Lange, A.M.; Lo, H.W. Inhibiting TRK proteins in clinical cancer therapy. Cancers 2018, 10, 105. [Google Scholar] [CrossRef] [PubMed]
- Price, L.C.; Wells, A.U.; Wort, S.J. Pulmonary tumor thrombotic microangiopathy. Curr Opin Pulm Med 2016, 22, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Westphalen, C.B.; Krebs, M.G.; Le Tourneau, C.; Sokol, E.S.; Maund, S.L.; Wilson, T.R.; Jin, D.X.; Newberg, J.Y.; Fabrizio, D.; Veronese, L.; Thomas, M.; de Braud, F. Genomic context of NTRK1/2/3 fusion-positive tumors from a large real-world population. NPJ Precision Oncol 2021, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Gu, J.; Wu, K.; Zhao, X.; Lu, Y. Progress in clinical diagnosis and treatment of colorectal cancer with rare genetic variants. Cancer Biol Med 2024, 21, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Willis, C.; Au, T.; Hejazi, A.; Griswold, C.; Schabath, M.B.; Thompson, J.; Malhotra, J.; Federman, N.; Ko, G.; Appukkuttan, S.; Warnock, N.; Kong, S.X.; Hocum, B.; Brixner, D.; Stenehjem, D. Clinical characteristics and treatment patterns of patients with NTRK fusion-positive solid tumors: A multisite cohort study at US academic cancer centers. J Manag Care Spec Pharm 2024, 30, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; Mascarenhas, L.; Geoerger, B.; Dowlati, A.; Pappo, A.S.; Bielack, S.; Doz, F.; McDermott, R.; Patel, J.D.; Schilder, R.; Tahara, M.; Pfister, S.M.; Witt, O.; Ladanyi, M.; Rudzinski, E.R.; Nanda, S.; Childs, B.H.; Laetsch, T.W.; Hyman, D.M.; Drilon, A. Larotrectinib in patients with TRK fusion-positive solid tumors: A pooled analysis of three phase 1/2 clinical trials. Lancet Oncol 2020, 21, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; De Braud, F.; Drilon, A.; Siena, S.; Patel, M.R.; Cho B.C.; Liu, S.V.; Ahn, M.J.; Chiu, C.H.; Lin, J.J.; Goto, K.; Lee, J.; Bazhenova, L.; John, T.; Fakih, M.; Chawla, S.P.; Dziadziuszko, R.; Seto, T.; Heinzmann, S.; Pitcher, B.; Chen, D.; Wilson, T.R.; Rolfo, CUpdated integrated analysis of the efficacy and safety of entrectinib in patients with NTRK fusion-positive solid tumors. Clin Cancer Res 2022, 28, 1302–1312. [CrossRef]
- Arter, Z.L.; Lee, A.T.M.; Nagasaka, M.; Ou, S.H.I. Tumor mutation burden survey of AACR GENIE database revealed NTRK (NTRK+) and RET (RET+) fusions positive colorectal carcinoma (CRC) as distinct subsets. Cancer Medicine 2025, 14, e70665. [Google Scholar] [CrossRef] [PubMed]
- Gayibov, E.; Karim, A.H. A rapid review of adenocarcinoma and pulmonary tumor thrombotic microangiopathy: a deadly duo. Cureus 2025, 17, e76842. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



