Submitted:
29 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
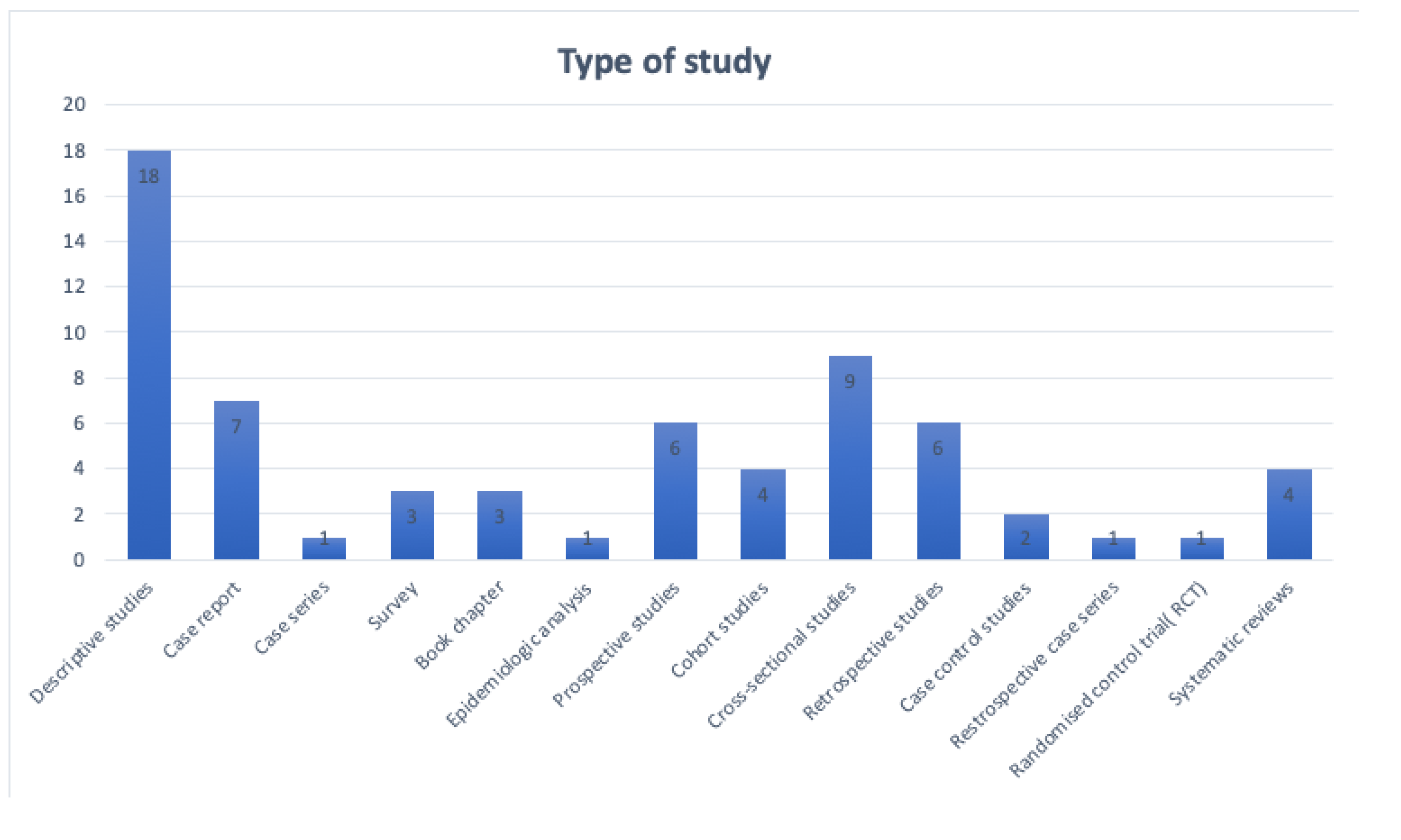
Objectives: The popularity of racket sports has been increasing globally over recent years, with tennis remaining the most played worldwide, and pickleball rising in popularity in the United States. While there are many studies addressing the injuries associated with racket sports in adults, there is minimal data available focusing on pediatric and adolescent populations. This study aims to review various injuries associated with racket sports in pediatric and adolescent populations. Methods: Using the PubMed database, we conducted a search of studies completed in the most recent 10 years that addressed injuries due to racket sports in age groups up to 18 years old, as well as adult studies that included pediatric and adolescent populations. Results: 66 studies met our inclusion criteria, with 18 of these being descriptive studies. The most common injuries reported in the studies were lower extremity injuries, specifically knee and ankle injuries. Upper extremity injuries were the next most common, specifically shoulder injuries. Most of the studies reported multiple musculoskeletal injuries as opposed to just one. Tennis was found to be the racket sport that causes the highest number of injuries, as well as the most severe injuries. Conclusions: There are not many studies on musculoskeletal injuries from racket sports in pediatric and adolescent populations. This review found tennis to be the sport with the highest number of injuries and most severe injuries. There is a significant amount of physical and mental growth occurring during childhood and adolescence, therefore more kinematic studies should be done pertaining to racket sports, which will hopefully help with injury prevention in these age groups.
Keywords:
1. Introduction
- (A)
- Tennis and variants- Tennis, Real tennis, soft tennis, Platform tennis, Paddle tennis, Padel, Squash tennis, Tennis polo, Sticke Tennis
- (B)
- Badminton and variants- Badminton, table tennis, Ball badminton, Speedminton/Crossminton,
- (C)
- Squash and variants- Squash, hardball squash, racquetball, racketball, racquets
- (D)
- Pickleball and variants- pickleball, pitton, paleta fronton, matkot/frescobol, pelota mixteca, beach tennis, speedball, qianball, racketlon, tamburello
- (E)
- Pelota and variants- Basque pelota, fives, frontenis, Jai alai [11]
2. Materials and Methods
3. Results
- Tennis:
- 1.1.
- Head and Eye injury: Patel et.al [13] studied tennis related ocular injuries in US from 2000 to 2019 and found 16000 tennis related eye injuries with males affected twice than females and young age group had highest number of injuries. One third of hospitalized patients had open globe injuries. O’Connor et al. [14] studied sport related concussion (SRC) rate in high schoolers and found overall SRC rate per 10000 exposures for boys and tennis were 0.74 and 1.94 respectively. Girls collectively had higher overall SRC rate than boys among all sports.
- 1.2.
- Upper extremity injury: There are a lot of overuse injuries to shoulder and elbows while playing tennis. Wang et al. [15] describe a case report of a youth athlete with acute anterior rotator cuff strain. Dennis et.al [16] did systematic review in young athletes and found high impact sports like tennis, badminton etc. could cause periphyseal stress injuries in shoulder, elbow, hand, wrist, foot and knee, ankle and foot. Pasulka et.al [17] did a case-control study in 1190 athletes and found that tennis at 46.7% was the sport with highest proportion of single-sport specialized athletes. Single sport specialized athletes in individual sports accounted for higher proportion of overuse injuries (44.3% vs 32.2%, p=0.037) and serious overuse injuries (28.8% vs 13.8%, p=0.011) but a lower proportion of acute injuries (28.8% vs 13.8%, p=0.001) compared to single-sport athletes involved in team sports. Kohyama et.al [18] reported a case report of stress fracture of scaphoid in an elite junior Japanese tennis player and concluded it was due to repeated practicing of attacking backhand high volley which involved too much dorsal flexion of the wrist. Young et al. [19] did a cross-sectional study of 125 professional female athletes and reported high level of infraspinatus atrophy in their dominant shoulders.
- 1.3.
- Lower extremity: Holst-Christensen et al. [20] studied mechanism of injury and return to sport rates following anterior cruciate ligament injuries in tennis among 231 patients and found that lunging, running forward to the net and movements related to smashing were the most frequent activities leading to injury. Casadei and Kiel [21] reports Little League shoulder also called proximal humeral epiphysiolysis which is common in baseball players and throwing athletes is also seen in tennis players and competitive gymnasts, and the typical age of presentation is between 11 and 16 years old with the mechanism of injury being physis remain open before the closure of growth plate. Bittner and Hartstein [22] published a case report 5th metatarsal avulsion fracture in 17-year-old male tennis. Brant et.al [23] did a descriptive epidemiology study from 2005 to 2016 using high school reporting information online (HSRIO) data and found lower extremity sports injuries were higher in girls in tennis compared to boys with rate ratios (RR) more than two to one. Girls had a higher proportion of severe lower extremity sport injuries needing imaging fall sports except volleyball. Ramponi and Baker [24] reported calcaneal apophysitis or Sever’s disease as the primary cause of heel pain in pediatric patients between 8 and 15 years from high impact sports like tennis.
- 1.4.
- Trunk and back injury: Gescheit et.al [25] performed a prospective cohort multiyear injury incidence in elite junior tennis players and found that lumbar spine was the most commonly and severely injured area in both sexes followed by shoulder injuries and knee injuries. Whale. et.al [26] data case report of 16-year-old Asian male was the elite tennis player with one month history of left shoulder pain which was later found to have first rib stress fracture.
- 2.
- Badminton:
- 3.
- Pickleball:
- 4.
- Squash:
- 5.
- Table tennis:
- 6.
- Racquet ball/paddleball:
- 7.
- Speed ball:
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SRC | Sport related concussion |
| HSRIO | High school reporting information online |
| SMASH | Shoulder Management and Assessment Serving High Performance |
| MOON | Multicentric orthopedic outcomes network |
References
- Padelathletes. Padel Statistics and Facts 2025. 2025. Available online: https://padelathletes.com/padel-statistics/ (accessed on 2 June 2025).
- Flamm, J. Pickleball Participation Surges to Nearly 20 million in 2024. 2025. Available online: https://www.thedinkpickleball.com/report-pickleball-participation-surges-to-nearly-20-million-in-2024/ (accessed on 2 June 2025).
- Vitale, K.; Liu, S. Pickleball: Review and Clinical Recommendations for This Fast-Growing Sport. Curr Sports Med Rep. 2020, 19, 406–413. [Google Scholar] [CrossRef]
- Yu, J.; Yendluri, A.; Linden, G.S.; Namiri, N.K.; Corvi, J.J.; Song, J.; Parsons, B.O.; Parisien, R.L. Increasing Incidence of Pickleball Injuries Presenting to US Emergency Departments: A 10-year Epidemiologic Analysis of Mechanisms and Trends. Orthop J Sports Med. 2025, 13, 23259671241305364. [Google Scholar] [CrossRef]
- Touhey, D.C.; Bozorgmehr, C.K.; Tartibi, D.S.; Smith, M.V.; Knapik, D.M.; Smith, M.; Knapik, D. Pickleball Injuries in the Aging Athlete: A Critical Analysis Review. Cureus. 2024, 16, e69950. [Google Scholar] [CrossRef]
- Fabricant, P.D.; Lakomkin, N.; Sugimoto, D.; Tepolt, F.A.; Stracciolini, A.; Kocher, M.S. Youth Sports Specialization and Musculoskeletal Injury: A Systematic Review of the Literature. Phys Sportsmed. 2016, 44, 257–262. [Google Scholar] [CrossRef]
- Soprano, J.V. Musculoskeletal Injuries in the Pediatric and Adolescent Athlete. Curr Sports Med Rep. 2005, 4, 329–334. [Google Scholar] [CrossRef]
- Jayanthi, N.A.; LaBella, C.R.; Fischer, D.; Pasulka, J.; Dugas, L.R. Sports-Specialized Intensive Training and The Risk of Injury in Young Athletes: A Clinical Case-Control Study. Am J Sports Med. 2015, 43, 794–801. [Google Scholar] [CrossRef]
- Theisen, D.; Frisch, A.; Malisoux, L.; Urhausen, A.; Seil, R. Monitoring of Sport Participation and Injury Risk in Young Athletes. J Sci Med Sport. 2013, 16, 200–204. [Google Scholar] [CrossRef]
- Kerr, Z.Y.; Comstock, R.D.; Dompier, T.P.; Marshall, S.W. The First Decade of Web-Based Sports Injury Surveillance (2004–2005 through 2013–2014): Methods of the National Collegiate Athletic Association Injury Surveillance Program and High School Reporting Information Online. J Athl Train. 2018, 53, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Gradasevic, H. List of 31 Racket Sports and How to Play Them. 2023. Available online: https://sportscentaur.com/list-of-31-racket-sports-and-how-to-play-them/ (accessed on 2 June 2025).
- Jayanthi, N.; Esser, S. Racket Sports. In Sports Rehabilitation and Injury Prevention; Comfort, P., Abrahamson, E., Eds.; Wiley-Blackwell, 2010; pp 265–280.
- Patel, P.S.; Uppuluri, A.; Oydanich, M.; Langer, P.D.; Zarbin, M.A.; Bhagat, N. Epidemiology of United States Tennis-Related Ocular Injuries from 2000 to 2019. Int Ophthalmol. 2023, 43, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K. L.; Baker, M. M.; Dalton, S. L.; Dompier, T. P.; Broglio, S. P.; Kerr, Z. Y. Epidemiology of Sport-Related Concussions in High School Athletes: National Athletic Treatment, Injury and Outcomes Network (NATION), 2011–2012 Through 2013–2014. J. Athl. Train. 2017, 52, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yi, N.; Ericksen, H.M.; Zhang, W. Case Report: Self-Performed Orthopedic Exams in Telehealth Treatment of a Youth Athlete with Acute Rotator Cuff Strain. Front Sports Act Living. 2023, 5, 1150850. [Google Scholar] [CrossRef]
- Caine, D.; Meyers, R.; Nguyen, J.; Schöffl, V.; Maffulli, N. Primary Periphyseal Stress Injuries in Young Athletes: A Systematic Review. Sports Med. 2022, 52, 741–772. [Google Scholar] [CrossRef]
- Pasulka, J.; Jayanthi, N.; McCann, A.; Dugas, L.R.; LaBella, C. Specialization Patterns Across Various Youth Sports and Relationship to Injury Risk. Phys Sportsmed. 2017, 45, 344–352. [Google Scholar] [CrossRef]
- Kohyama, S.; Kanamori, A.; Tanaka, T.; Hara, Y.; Yamazaki, M. Stress Fracture of the Scaphoid in an Elite Junior Tennis Player: A Case Report and Review of the Literature. J Med Case Rep. 2016, 10, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Young, S.W.; Dakic, J.; Stroia, K.; Nguyen, M.L.; Harris, A.H.; Safran, M.R. High Incidence of Infraspinatus Muscle Atrophy in Elite Professional Female Tennis Players. Am J Sports Med. 2015, 43, 1989–1993. [Google Scholar] [CrossRef]
- Holst-Christensen, T.; Hölmich, P.; Andersen, F.F.; Kaldau, N.C. Anterior Cruciate Ligament Injuries in Tennis: Injury Mechanism and Return to Sport Rates Following Injury. Scand J Med Sci Sports. 2025, 35, e70064. [Google Scholar] [CrossRef]
- asadei, K.; Kiel, C J. Proximal Humeral Epiphysiolysis. StatPearls. 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/30485006/ (accessed on 2 June 2025).
- Bittner, J.S.; Hartstein, A.J. Fifth Metatarsal Avulsion Fracture in an Adolescent Tennis Player. J Orthop Sports Phys Ther. 2019, 49, 620. [Google Scholar] [CrossRef]
- Brant, J.A.; Johnson, B.; Brou, L.; Comstock, R.D.; Vu, T. Rates and Patterns of Lower Extremity Sports Injuries in All Gender-Comparable US High School Sports. Orthop J Sports Med. 2019, 7, 2325967119873059. [Google Scholar] [CrossRef] [PubMed]
- Ramponi, D.R.; Baker, C. Sever’s Disease (Calcaneal Apophysitis). Adv Emerg Nurs J. 2019, 41, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Gescheit, D.T.; Cormack, S.J.; Duffield, R.; Kovalchik, S.; Wood, T.O.; Omizzolo, M.; Reid, M. A Multi-Year Injury Epidemiology Analysis of an Elite National Junior Tennis Program. J Sci Med Sport. 2019, 22, 11–15. [Google Scholar] [CrossRef]
- Wahle, C.F.; Hart, C.M.; Beck, J.J. First Rib Stress Fracture in an Adolescent Elite Tennis Player: A Case Report. JBJS Case Connect. 2023, 13, 1–4. [Google Scholar] [CrossRef]
- Zhou, X.; Imai, K.; Liu, X.X.; Chen, Z.; Watanabe, E.; Zeng, H. Epidemiological Characteristics of Injury in 7-22-Year-Old Badminton Players by Age and Sex. Sci Rep. 2025, 15, 2889. [Google Scholar] [CrossRef] [PubMed]
- Saragaglia, D.; Banihachemi, J.J.; Chamseddine, A.H. Acute Injuries in Badminton from 10 to 66 Years of Age: An Epidemiological Study of 140 Cases Among All Types of Practice. Eur J Orthop Surg Traumatol. 2023, 33, 1945–1951. [Google Scholar] [CrossRef]
- Zhou, X.; Imai, K.; Chen, Z.; Liu, X.; Watanabe, E.; Zeng, H. The Characteristics of Badminton-Related Pain in Pre-Adolescent and Adolescent Badminton Players. Children (Basel). 2023, 10, 1501. [Google Scholar] [CrossRef] [PubMed]
- Lau, R.; Mukherjee, S. Prevalence of Shoulder and Elbow Overuse Injuries Among Competitive Overhead Youth Athletes in Singapore. Orthop J Sports Med. 2023, 11, 23259671231156199. [Google Scholar] [CrossRef]
- Shaari, A.L.; Fano, A.N.; Ferraro, J.; Ahmed, I. Metacarpal Stress Fractures in Athletes: A Systematic Review. Hand (N Y). 2024, 15589447241266965. [CrossRef]
- Jao, K.K.; Atik, A.; Jamieson, M.P.; Sheales, M.P.; Lee, M.H.; Porter, A.; Roufas, A.; Goldberg, I.; Zamir, E.; White, A.; Skalicky, S.E. Knocked by the Shuttlecock: Twelve Sight-Threatening Blunt-Eye Injuries in Australian Badminton Players. Clin Exp Optom. 2017, 100, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Chen, Y.; Miao, J.; Zhao, M.; Keng, C.; Wang, X.; Guo, J.; Liu, Y. Doubles Trouble-85 Cases of Ocular Trauma in Badminton: Clinical Features and Prevention. Br J Sports Med. 2020, 54, 23–26. [Google Scholar] [CrossRef]
- Boroumand, S.; Park, N.; Katsnelson, B.; Qian, E.; Norman, M.; Joo, P.; Diatta, F.; Noel, O.; Moran, J.; Jimenez, A. The Perils of Pickleball: A Two Decade Analysis of Upper and Lower Extremity Injuries from America’s Fastest Growing Sport. J Sports Sci. 2025, 1–8. [Google Scholar] [CrossRef]
- Horsley, I.G. Dr.; O’Donnell, V.; Leeder, J. The Epidemiology of Injuries in English Professional Squash; A Retrospective Analysis Between 2004 and 2015. Phys Ther Sport. 2020, 46, 1–6. [Google Scholar] [CrossRef]
- Rejeb, A.; Johnson, A.; Vaeyens, R.; Horobeanu, C.; Farooq, A.; Witvrouw, E. Compelling Overuse Injury Incidence in Youth Multisport Athletes. Eur J Sport Sci. 2017, 17, 495–502. [Google Scholar] [CrossRef]
- Jendrusch, G. Augenverletzungen und Fehlsichtigkeit im Schul- und Vereinssport [Eye Injuries and Defective Vision in School and Club Sports - Arguments for DIN-approved Glasses Suitable for School Sports]. Klin Monbl Augenheilkd. 2025, 242, 521–531. [Google Scholar] [CrossRef]
- Studnicka, K.; Ampat, G.; Lumbosacral Spondylolisthesis. StatPearls. 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/32809514/ (accessed on 2 June 2025).
- Tan, Y.; Zhou, P.; Ma, C. Analysis of Sport-Injured Pattern of Anterior Cruciate Ligament in the Reconstruction Period of Chinese College Students. J Sports Med Phys Fitness. 2016, 56, 1346–1351. [Google Scholar]
- Changstrom, B.; McBride, A.; Khodaee, M. Epidemiology of Racket and Paddle Sports-Related Injuries Treated in the United States Emergency Departments, 2007-2016. Phys Sportsmed. 2022, 50, 197–204. [Google Scholar] [CrossRef]
- Cronin, K.J.; Magnuson, J.A.; Wolf, B.R.; Hawk, G.S.; Thompson, K.L.; Jacobs, C.A. MOON Shoulder Group; Hettrich, C.M.; Bishop, J.Y.; Bollier, M.J.; et al. Male Sex, Western Ontario Shoulder Instability Index Score, and Sport as Predictors of Large Labral Tears of the Shoulder: A Multicenter Orthopaedic Outcomes Network (MOON) Shoulder Instability Cohort Study. Arthroscopy. 2021, 37, 1740–1744. [Google Scholar] [CrossRef]
- Meshram, P.; Yasser, O.; Joseph, J.; Larijani, K.; Lopes Sauers, A.; Srikumaran, U.; McFarland, E.G. Descriptive Epidemiology of Injuries in Professional Speedball Athletes. J Sport Rehabil. 2022, 31, 778–784. [Google Scholar] [CrossRef]
- Johansson, F.; Cools, A.; Gabbett, T.; Fernandez-Fernandez, J.; Skillgate, E. Association Between Spikes in External Training Load and Shoulder Injuries in Competitive Adolescent Tennis Players: The SMASH Cohort Study. Sports Health. 2022, 14, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Johansson, F.; Gabbett, T.; Svedmark, P.; Skillgate, E. External Training Load and the Association with Back Pain in Competitive Adolescent Tennis Players: Results from the SMASH Cohort Study. Sports Health. 2022, 14, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Fernandez, J.; Moya-Ramon, M.; Santos-Rosa, F.J.; Gantois, P.; Nakamura, F.Y.; Sanz-Rivas, D.; Granacher, U. Within-Session Sequence of the Tennis Serve Training in Youth Elite Players. Int J Environ Res Public Health. 2020, 18, 244. [Google Scholar] [CrossRef]
- Fett, J.; Oberschelp, N.; Vuong, J.L.; Wiewelhove, T.; Ferrauti, A. Kinematic Characteristics of the Tennis Serve from the Ad and Deuce Court Service Positions in Elite Junior Players. PLoS One. 2021, 16, e0252650. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Wang, C.; Bi, Y.; Chen, L. Effect of Integrative Neuromuscular Training for Injury Prevention and Sports Performance of Female Badminton Players. Biomed Res Int. 2021, 2021, 5555853. [Google Scholar] [CrossRef]
- Stausholm, M.B.; Baun, M.; Bjordal, J.M.; Nielsen, D.; Aagaard, H.; Magnusson, S.P.; Couppé, C. Shoulder Rotational Strength Profiles of Danish National Level Badminton Players. Int J Sports Phys Ther. 2021, 16, 504–510. [Google Scholar] [CrossRef]
- Gibly, R.F.; Shomaker, T.; Bompadre, V.; Steinman, S.E. Understanding the Spectrum of Paediatric Mechanical Finger and Hand Trauma Seeking Acute Care. J Child Orthop. 2018, 12, 622–628. [Google Scholar] [CrossRef] [PubMed]
- The Dink. Experimenting with Paddle Grip Position. 2023. Available online: https://www.thedinkpickleball.com/paddle-grip-position-options/ (accessed on 6 June 2025).
- Adirim, T.A.; Cheng, T.L. Overview of Injuries in the Young Athlete. Sports Med. 2003, 33, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Berson, B.L.; Rolnick, A.M.; Ramos, C.G.; Thornton, J. An Epidemiologic Study of Squash Injuries. Am J Sports Med. 1981, 9, 103–106. [Google Scholar] [CrossRef] [PubMed]

| Location and type of injury | Number of articles describing these injuries |
|---|---|
| 1. Head 1.1. Eye injury 1.1.1. Traumatic hyphema 1.1.2. Blunt eye injury 1.1.3. Macular hole 1.2. Concussion |
13 (total) 7 2 1 1 2 |
| 2. Back 2.1. Unspecified back injury 2.2. Lumbosacral spondylolisthesis 2.3. Lumbosacral injury |
6 (total) 3 1 2 |
| 3. Upper extremity and chest 3.1. Non-specific upper extremity injury 3.2. Shoulder injury 3.2.1. Rotator cuff injury 3.2.2. Little league shoulder 3.2.3. Infraspinatus atrophy 3.3. Rib injury-1st rib stress fracture 3.4. Arm injury 3.4.1. Proximal humeral epiphysiolysis 3.4.2. Humerus diaphyseal fracture 3.5. Clavicle fracture 3.6. Elbow injury 3.7. Trunk injury 3.8. Wrist/hand injury 3.8.1. Non-specific injury 3.8.2. Metacarpal stress fracture 3.8.3. Carpal stress fracture |
29(total) 3 9 1 1 1 1 1 1 1 1 2 1 4 1 1 |
| 4. Lower extremity 4.1. Non-specific injury 4.2. Knee injury 4.2.1. ACL injury 4.2.2. Patellar tendinopathy 4.3. Ankle injury 4.4. Thigh injury 4.5. Hip injury 4.6. 5th metatarsal avulsion fracture 4.7. Sever’s disease (calcaneal apophysitis) |
39 (total) 8 10 5 1 11 1 1 1 1 |
| 5. Miscellaneous 5.1. Sprain/strains 5.2. Overuse injuries |
5(total) 2 3 |
| Location | Injury | Racket sports in which injury is reported | Comments |
|---|---|---|---|
| Head | Concussion [reference. 14,28] | Tennis (and other non-racket sports like track, lacrosse, soccer etc.) Badminton |
Girls reports more concussion per 10,000 exposures in major sports |
| Eyes | Traumatic Hyphema [ref. 13] Blunt injury to globe [ref. 13,32,33,37] Retinal detachment [ref. 32,33] |
Tennis, badminton, squash | High number of hospitalized athletes due to tennis had open globe trauma |
| Chest/ thorax | Stress fracture of the first rib [ref. 43] | Tennis | |
| Back and spine | Lumbosacral sprain [ref. 25,27,38] Lumbosacral spondylolisthesis [ref.26] |
Tennis, badminton, table tennis | |
| Shoulder | Overuse injuries, rotator cuff tendonitis, strain [ref. 16, 17,30,34,42] Proximal humeral physis stress injury (‘Little League shoulder) [ref. 21] Infraspinatus atrophy [ref. 19] Fracture [ref. 18,34,40] Labral tears [ref. 41] |
Tennis, badminton, Pickleball, speedball |
Overuse injuries common with medium to high velocity sports like tennis, badminton, squash, pickleball |
| Elbow | Tennis elbow, non-specific tennis injury [ref. 16, 29,30] | Tennis, badminton | |
| Wrist and hand | Metacarpal stress fracture [ref. 31] Carpal stress fracture [ref. 18] |
Badminton, tennis | |
| Arm | Humeral diaphyseal fracture [ref. 18, 34, 40,49] | Tennis, racquetball, pickleball, badminton | |
| Finger | Finger injury [ref. 17, 34] | Tennis, Pickleball | |
| Knee | Anterior cruciate ligament sprain or tear [ref. 22, 27, 28, 34, 39] Patellar tendinopathy [ref. 22] |
Tennis, Badminton, pickleball, table tennis | Knee is the most common site of overuse injuries |
| Foot and ankle | 5th metatarsal avulsion fracture [ref. 22] Calcaneal apophysitis [ref. 24] |
Tennis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



