Submitted:
28 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background and Objectives: Endocrowns have emerged as a minimally invasive restorative option in dentistry, aiming to preserve as much of the original tooth structure as possible. This scoping review investigates the success rates, biomechanical performance, and material efficacy of endocrowns for restoring molars, in comparison to conventional post-and-core crowns. Materials and Methods: Comprehensive literature research was conducted to identify relevant studies through PubMed and Scopus databases. The search covered publications up to March 2025. All study types focusing on molar restorations were included, except for case reports. Data extraction and screening were performed independently by two reviewers. Results: A total of 37 studies fulfilled the eligibility criteria. Eleven systematic reviews examined comparisons between endocrowns and post-and-core crowns, as well as differences in material selection, survival and success rates, and outcomes between molars and premolars. The remaining 26 studies addressed the clinical performance and longevity of endocrowns, with an emphasis on preparation design, adhesive protocols, and mechanical behavior related to material selection. Conclusions: Endocrown restorations present a conservative and predictable alternative to post-and-core crowns for molars with extensive coronal damage. However, due to variability in reported outcomes, high-quality randomized clinical trials are essential to confirm their clinical effectiveness. The development of novel, standardized treatment guidelines would provide clinicians adequate information to effectively restore endodontically treated teeth (ETT).
Keywords:
endocrowns
; endodontically-treated teeth
; biomaterials
; operative dentistry
1. Introduction
Endodontically treated teeth (ETT) are scientifically documented to be more susceptible to fracture than vital teeth. This is attributed to their significant loss of tooth structure, resulting from procedures such as caries removal, access cavity preparation, root canal preparation, irrigation, and the use of intracanal medicaments [1,2,3,4]. This process exposes the tooth to irreversible physicochemical and biomechanical changes, including dentin dehydration, collagen disruption, and reduced microhardness, conditions that compromise both structural integrity and proprioception [1,5]. Therefore, maintaining as much healthy tooth structure as possible is crucial for the long-term survival of ETT [3,6,7]. This statement is endorsed by studies demonstrating that EETs present an 80% higher risk of restoration failure compared to vital teeth [8].
Clinicians experience challenges when restoring ETT due to the increased functional and parafunctional loadings that occur on posterior teeth, which contribute to a higher risk of restoration failure [1,9]. ETT restored by post-and-core crowns exhibit higher rates of root fractures, particularly when no circumferential ferrule is obtained. Furthermore, the absence of ferrule in conjunction with the extensive removal of dentin in the core of the root canals facilitates the debonding of fiber-reinforced posts. The presence of short roots and limited restorative space is a factor associated with restoration failures [5,10]. The limitations associated with traditional restorative approaches, along with recent advancements in adhesive dentistry and dental biomaterials, have driven the development of evidence-based alternative modalities for the restoration of endodontically treated teeth (ETT) [2,3,5,9,10,11,12,13,14,15,16,17,18,19,20].
Pissis in 1995 first introduced the monobloc technique, described as a laboratory-fabricated core and crown unit designed as a single component [17]. This concept was further developed by Bindl and Mörmann in 1999, who used the term “endocrown” to describe a mono-block ceramic crown bonded to a devitalized posterior tooth [21]. The survival of these one-piece endodontic crowns is achieved through macro-mechanical retention, which serves as an anchorage for the restorative material, providing stability, and micro-mechanical retention via adhesive cementation, forming a strong bonding interface between the restoration and the tooth surface while minimizing microleakage [7,11,12,18,22]. Endocrowns have gained prominence as a minimally invasive technique compared to conventional post-and-core crowns, particularly for molars. Their anatomical design promotes minimal invasive preparation [2,12,16,23] and confines catastrophic failures commonly associated with posts [2,3,5,6,9,18,24].
Factors affecting the survival and success rates of endocrowns include, among others, the material type used and the preparation design, with emphasis on the finish line, occlusal reduction, and extension into the pulp chamber. The extent to which each factor influences the performance of endocrowns needs further investigation. While systematic reviews have focused on specific aspects such as materials or survival rates [2,7,11,12,16], the available literature on endocrown restorations remains diverse in scope, methodology, and outcomes. Given this heterogeneity and the emerging nature of adhesive and restorative techniques, a scoping review is warranted to provide a broad mapping of current evidence, clarify key concepts, and identify gaps for future research. The objective of this scoping review is to investigate and summarize the most recent data on the application of endocrowns for restoring severely damaged posterior ETT, focusing on comparing the clinical performance of endocrowns to that of post-and-core restorations, identifying the most appropriate materials and preparation techniques, and highlighting areas where additional research and standardization are needed.
2. Materials and Methods
The reporting of this review followed the recommendations of the latest PRISMA for Scoping Reviews (PRISMA-ScR) statement [25], to ensure methodological transparency and systematic reporting. The PCC (Population, Concept, Context) framework was adapted to structure the research question and facilitate the selection process (Figure 1).
2.1. Sources of Information and Search Strategy
A comprehensive search of the literature was conducted using the following electronic databases: MEDLINE through PubMed and Scopus, covering publications from inception to March 2025. The search strategy for all databases was based on the term “endocrowns” solely or combined with other keywords such as “endocrowns AND materials”, “endocrowns AND ferrule”, “endocrowns AND survival rate”, and “endocrowns AND post-and-core restorations”. Additional relevant studies were identified by manually screening the reference lists of all included articles and related reviews.
2.2. Eligibility Criteria
The search results were filtered by language, and articles published in English were eligible. The scoping review included systematic reviews, meta-analyses, umbrella reviews, literature reviews, in vitro studies, randomized controlled clinical trials, and retrospective clinical studies. Research studies on anterior teeth or premolars, as well as case reports, letters to the editor, patents, short communications, and conference abstracts were excluded to maintain the clinical relevance and quality of evidence within the defined scope.
2.3. Data Extraction, Screening, and Charting
The study selection process was conducted in two stages. First, titles and abstracts were screened by two independent reviewers (A.K.Z and K.T.) to identify potentially eligible studies. In the second stage, full-text articles were retrieved and assessed by the pre-established inclusion and exclusion criteria. In the presence of disagreements screening was conducted by a third reviewer (E.P.) until consensus was reached. Data charting was performed using a standardized extraction form created and implemented by the reviewers. To ensure consistency, all reviewers pre-tested the form on a sample of studies and refined it through discussion before proceeding with the complete data extraction. Each reviewer independently extracted data, and all charted items were cross verified to ensure accuracy. The information collected was organized into two Tables. The first table summarizes the results of systematic reviews and meta-analyses, synthesized descriptively, and categorizes thematically based on comparisons between endocrowns and post-and-core crowns, material selection, and survival and success rates. The second table reported the results of eligible literature reviews, umbrella reviews, in vitro studies, retrospective studies, and RCTs, giving an insight into clinical performance and long-term outcomes of endocrowns, preparation design, cementation processes, mechanical properties, and material selection. The table of systematic reviews and meta-analyses included author and year of publication, main objectives, search strategy and data screening information, and key findings, whereas the second Table included author and year of publication, study type, main objective, study design, and key findings. No assumptions or simplifications were made during this process.
Given the nature and purpose of scoping reviews, no formal critical appraisal of the included studies was performed. However, study type, study design, and methodological rigor of each study were considered during data synthesis and interpretation.
3. Results
A total of 1,406 articles were identified through comprehensive searches conducted in the MEDLINE database via PubMed and Scopus. After record removal due to duplicates, records not published in English language, lack of relevance (e.g., anterior teeth), ineligible study types (e.g., case reports, letters, short communications, conference abstracts), insufficient focus on posterior ETT, lack of direct evaluation of endocrowns to post-and-core restorations, or failure to meet design criteria, a total of 37 articles were included in this scoping review. The selection process is outlined in Figure 2.
The included studies were categorized into two primary groups based on study type and are reported in Table 1 and 2. All systematic reviews and meta-analyses (11 articles) [2,6,7,11,12,16,23,24,26,27,28] are included in Table 1, which were thematically subcategorized as described in the “Methods and Materials” section.
Table 2 reported 20 original research studies – including fifteen in vitro studies, three RCTs, and two retrospective clinical studies – and six reviews (umbrella narrative and literature reviews). These studies were categorized according to their main subject of interest: Ten studies evaluated the clinical performance and long-term out-comes of endocrowns [1,8,10,14,29,30,31,32,33,34], six studies focused on the preparation design and cementation procedure applied [15,18,35,36,37,38] , four studies examined the mechanical strength and load resistance influenced by material and preparation design [4,13,39,40], and six studies compared the different materials that are available for endocrown restorations [19,20,41,42,43,44].
A common area of interest among the included studies was the mechanical behavior of endocrowns – particularly fracture resistance – which was commonly evaluated under simulated masticatory conditions. Fifteen articles specifically compared endocrowns with traditional post-and-core crowns [6,8,10,13,19,23,24,26,27,29,30,31,34,37,40], while six articles compared them to other types of restorations, highlighting differences in performance outcomes [1,4,14,19,20,41] . In ten studies, the influence of restorative material on functional durability was investigated, by comparing materials such as lithium disilicate, zirconia-reinforced lithium silicate, and resin-based ceramics [2,11,16,20,28,32,33,39,42,43]. Additionally, ten studies examined the decisive role of preparation design on the final performance of endocrowns, evaluating the impact of pulp chamber depth and ferrule presence on the integrity of the final restoration [7,12,15,16,18,35,36,38,42,44]. Marginal adaptation described as a critical aspect in preventing microleakage and enhancing long-term durability was appraised in five articles [12,15,16,36,38].
4. Discussion
4.1. Key Findings of This Scoping Review
4.1.1. Clinical Indications: When and Why to Choose Endocrowns
Based on the research results, endocrowns are primarily indicated for restoring posterior ETT with substantial structural loss, particularly when post-and-core methods are not feasible [13,29,41]. Therefore, endocrowns are suitable for molars with short, obliterated, calcified or divergent roots, where conventional posts may pose clinical challenges [2,9,10,12,13,15,18,29,41]. Additionally, they are recommended for restoring teeth where an adequate ferrule effect cannot be achieved and where interocclusal space is insufficient [2,9,10,12,13,18,29,41,45]. In such cases, conventional post and core crowns may fail to provide adequate material strength, thickness, and structural support, making endocrowns a more reliable treatment modality [13]. Traditional crown preparation may require the removal of 67.5–75.6% of the tooth tissue, whereas the decay-oriented design of endocrowns facilitates the preservation of tooth viability [16,38]. Simultaneously, there is no need for post-preparation into the root canals, which has been associated with an increased chance of vertical fracture [9]. The micro- and macro-mechanical retention of endocrowns relies on the adhesive cementation and stability derived from an adequate pulp chamber for bonding [8,16]. El Ghoul et al.’s findings correlate with other studies, which indicate that endocrowns provide superior fracture resistance compared to post-and-core crowns due to their single-piece design, which minimizes internal stresses and enhances strength through improved occlusal thickness, while preserving peripheral enamel for better adhesion and load distribution [40].
Thus, endocrowns are best suited for molars with extensive coronal damage, limitations in root anatomy, or reduced interocclusal space, especially when preserving tooth structure is a clinical priority.
4.1.2. The Impact of Cuspal Reduction and Intracoronal Extension on Retention and Fracture Resistance.
To ensure the longevity of endocrown restorations, efforts have been made over the years to develop proper preparation guidelines and design protocols through numerous clinical and laboratory studies. It is essential to emphasize the potential for preparation and design modifications based on individualized clinical conditions [14]. Most recommendations focus on parameters such as cuspal reduction and occlusal thickness. While no standard line on these parameters has been established, based on the majority of eligible studies, the cuspal reduction ranges between 2-3 mm [6,15,16], with Dartora et al. suggesting a slightly broader range of 1.5 to 3 mm [41]. Otto et al. demonstrated that greater occlusal thickness in endocrowns is related to increased fracture resistance, emphasizing on the mechanical advantage of thicker restorations [14,34]. While increased occlusal thickness generally enhances fracture resistance, Taha et al., and Mostafavi et al. agreed that aggressive preparations should be avoided, as these could compromise tooth structure without providing desirable clinical benefits [16,46]. Notwithstanding, it is important to consider that other factors may influence cuspal reduction, including tooth type, interocclusal space, cavity depth, remaining axial wall thickness, and the restorative material used [16,20]. Therefore, an occlusal thickness of approximately 3 mm is generally recommended to optimize fracture resistance but ashould be carefully modified based on anatomical and material-related factors to prevent excessive tooth reduction.
In general, the occlusal thickness of endocrown restorations typically ranges between 3 mm and 7 mm [20,23,46], including the cuspal reduction and the intracoronal extension [5]. Adequate pulp chamber depth is essential for macro- and micro-mechanical retention [9,10,11,22,26,35]. It is crucial for the preparation not to extent the pulpal floor through the radicular orifices, as a more complex preparation can result in insufficient marginal and internal adaptation, ultimately compromising the long-term performance of the final restoration. [5,16,24,26]. Although there is no consensus on the exact chamber depth, Zhang et al. observed that while increasing chamber depth from 1 mm to 3 mm led to higher stress on the restoration, the stress on tooth tissue remained relatively stable, except for a noticeable increase at the root furcation with 3-mm depths, particularly under horizontal loading. It was interesting to note that the 2-mm depth exhibited the best stress distribution, which was the least concentration on the restoration and on the surrounding tooth tissues[47]. This is in agreement with Hayes et al. who found that deep extensions greater than 2 mm were factors that increased the probability for catastrophic failures under oblique forces [48]. Dartora et al., however demonstrated that the mechanical resistance of the restoration depends on the extent of the pulp chamber extension, which contributes to improved stress distribution of masticatory forces and increased resistance [10,22,35]. They also emphasized that when the pulp chamber depth is only 1mm, the restoration is prone to rotational motion [10,16,35]. Thomas et al. agrees with the fact that very shallow chambers (<2 mm) may lead to debonding, which could lead to reducing the success of the endodontic therapy due to coronal microleakage [9]. Veselinova et al. strengthened this conservative approach by using a 2-mm depth for their investigation and stating that there was no significant difference between 4-mm and 2-mm depths, but deeper extensions tended to fail more seriously[20]. Alqarni et al. found that an intracoronal depth of 2 mm provided greater fracture resistance. However, a 4 mm depth resulted in more catastrophic, non-repairable fractures, while 0 mm showed failure patterns similar to those of untreated teeth [49]. Overall, these findings suggest that while both underextension and overextension carry risks, a 2-mm pulp chamber depth may provide the best balance between retention, stress distribution, and clinical safety.
The retention of the restoration depends on the surface available for adhesion; thus, smaller pulp chambers lead to higher failure rates and debonding [7,11,13,20,21,23,26]. When endocrowns have a disadvantageous height-to-width ratio, greater leverage forces are generated, and a higher risk of restoration displacement due to adhesive rupture may occur [10,13,23,26]. In the molar region, the orientation and concentration of axial forces play a critical role in the clinical performance of endocrowns [6,23]. Another important factor is the relationship between bone height and the pulp chamber floor, which significantly influences the mechanical behavior of the restoration. Ribeiro et al. [18] demonstrated that when the pulp chamber floor is positioned above the crestal bone level, the risk of mechanical failure increases due to unfavorable stress distribution. Clinically, achieving an adequate pulp chamber depth and maintaining a favorable height-to-width ratio are essential to reduce debonding and stress concentrations—particularly in molars and in cases with limited bone support .
4.1.3. Pulp Chamber Cavity Preparation: Balancing Retention, Resistance, and Bond Strength
In addition to considerations related to the pulp chamber cavity, meticulous internal preparation is essential to ensure accurate placement and optimal adaptation of the final restoration. [10,16]. A flat surface floor with an axial wall divergence of approximately 6 degrees without undercuts but with rounded angles, increases precision in internal fit [5,16,41]. To further optimize clinical outcomes, the immediate dentin sealing (IDS) technique using flowable composite resins can be employed to cover irregularities in the pulp chamber walls [5,10]. This approach not only eliminates retentive zones that hinder the adjustment of the restoration but also improves adhesion to dentin, reduces microleakage and strengthens the bond in ETT where dentin adhesion is weaker than enamel [3,5,10,11,29]. Additionally, the cementation protocol plays a critical role in the performance of endocrowns, as optimal adhesion between the restoration and tooth structure directly influences stress distribution and fracture resistance [23]. Inadequate cementation may compromise micromechanical retention, increasing the risk of debonding [5,7]. Resin cements are the material of choice due to their excellent bonding capabilities, color adaptability, adequate mechanical properties, and resistance to dissolution [5]. However, polymerization shrinkage poses drawbacks including an increased risk of microleakage, resulting in a higher susceptibility to adhesive failure, especially when marginal gaps or insufficient retentive height occur. These conditions aggravate stress accumulation at the tooth-cement interface [7,36]. Thus, optimal internal preparation, use of immediate dentin sealing, and careful resin cementation are essential to prevent microleakage, improve retention and minimize stress at the tooth-restoration interface in endocrown restorations.
4.1.4. The Effect of Finish Line Design on Flexural Strength, Stress Distribution, and Internal Adaptation
Another major factor influencing the clinical outcome of endocrown restorations is the finish line design [7,50]. The circumferential 90-degree butt-joint margin, typically 1–2 mm in width, remains the most commonly used configuration. However, several studies have shown a growing preference for shoulder finish lines and the incorporation of a ferrule effect [5,6,15,16,24,38].
The shoulder margin design has been associated with improved flexural strength and stress distribution compared to the butt-joint margin [16,46,50,51]. Incorporating a ferrule—a short axial wall in the cervical area—acts as a bracing mechanism, enhancing both structural integrity and the surface area available for adhesion [1,13,16,23,26,28]. Einhorn et al. [15] reported that a 1 mm ferrule significantly reduced the incidence of irreparable fractures compared to a 2 mm ferrule or no ferrule. Similarly, Taha et al. [46] recommended the preconditioning of a short axial wall with a shoulder finish line to improve mechanical strength. In situations where a ferrule is absent, Mostafavi et al. and Govare et al. [16,26] suggested adding a beveled margin to enhance adhesive potential. Zeng et al. [38] evaluated stress distribution among butt-joint, 90-degree shoulder, and 135-degree shoulder designs. While the general stress patterns were similar, the 135-degree shoulder demonstrated lower stress concentration and improved biomechanical viability.
Cervical margin placement should also be carefully considered. Supragingival positioning is preferable [6,10,15,24,26,41], particularly for preserving enamel near the cementoenamel junction, which is essential for optimal bond strength [16,23,26,38]. In such scenarios, the butt-joint margin may be advantageous as a less invasive technique—preserving tooth structure, offering resistance to compressive forces, and reducing marginal leakage [16,38,46]. Taha et al. [46] demonstrated that CAD/CAM polymer-infiltrated ceramic endocrowns—whether with a butt-joint or shoulder margin—can resist forces exceeding typical axial masticatory loads in the molar region, which generally range between 600–900 N [20], with some studies reporting up to 850 N [46]. Interestingly, Einhorn et al. [15] noted that the simpler preparation associated with butt-joint designs may lead to better internal adaptation compared to configurations incorporating a ferrule.
To sum up, while the butt-joint margin remains a minimally invasive and effective option, shoulder finish lines with short ferrules may enhance fracture resistance and stress distribution Individual anatomical characteristics, enamel availability, and material choice should all be taken into consideration when choosing a margin in clinical practice.
4.1.5. Choosing the Right Material: Mechanical and Esthetic Considerations in Endocrown Performance
The advancement of biomaterials has introduced new indirect restorative materials with an elastic modulus like that of dentin, while simultaneously providing superior fracture resistance. It is well known that the elastic modulus of enamel and dentin is 84,1 GPa and 18,6 GPa, respectively [36]. As the restoration's physicomechanical characteristics get closer to that of the dentin, the risk of catastrophic fractures decreases [26]. The monoblock design of endocrowns, which minimizes material interfaces, improves stress distribution compared to conventional post-and-core restorations that combine materials with different elastic moduli [9,23]. Several studies have compared lithium disilicate-based ceramics (LD/LDS/LDSB) or lithium disilicate glass ceramics (LDGC) with different types of zirconia (monolithic zirconia, zirconia-reinforced lithium silicate/ ZLS), indirect resin-based materials (RB), or resin nanoceramics (RNC) in terms of restoration's adaptation, bond capacity, fracture resistance, optical and biomechanical properties, biocompatibility, and wear (Table 3).
Lithium disilicate based ceramics have been considered as the material of choice for endocrown restoration due to their superior adhesive properties and resistance to displacement [2,13,40]. Strong bonding is achieved through micromechanical “interlocking” between the etchable ceramic material and the resin cement, enhancing the stability of the restoration [13,26,35,40]. Additionally, its high esthetic quality and superior fracture resistance make it a promising choice for dental applications [26]. However, there are several limitations associated with LDS. The high elastic modulus of lithium disilicate ceramics, approximately 90GPa, often increases the risk of tooth fractures, which could result in irreparable fractures under excessive stress [19]. Furthermore, the material’s stiffness may induce wear on opposing natural teeth, while its brittle nature often results in restoration failure due to porcelain fracture [2,11].
Monolithic zirconia has a modulus of elasticity above 200 GPa, which is significantly higher than that of dentin and thus is prone to catastrophic failures [42]. When Veselinova et al. examined monolithic zirconia and CAD/CAM lithium disilicate endocrowns, they found that the latter exhibited higher fracture strength and less catastrophic failures compared to the former, which mainly fractured beneath the cementoenamel junction [20,52]. When Alwadai et al. examined the lithium disilicate glass ceramics versus zirconia-reinforced lithium disilicates for optimal marginal adaption, they found that both were within the range of values deemed clinically acceptable [12]. An in vitro study by Kumar et al. showed that endocrowns made from monolithic zirconia exhibited a larger internal gap compared to those made from lithium disilicate (LDS) [53]. In contrast, Falahchai et al. found that zirconia endocrowns exhibited superior marginal and internal fit compared to LDS and ZLS, with the most significant gaps consistently observed in the pulpal area and the smallest at the margins [54].
Zirconia-reinforced lithium silicate (ZLS) ceramics combine zirconia’s mechanical strength and the aesthetic properties of lithium disilicates, offering an improved alternative for endocrown restorations [43]. Jalalian et al. in their in vitro study demonstrated that ZLS has better margin adaption and higher fracture resistance than LDS, but they also ZLS have increased amounts of irreparable fractures [42]. In contrary, El Ghoul’s et al. study demonstrated that LDS exhibits the highest fracture resistance under lateral loading compared to RNC and ZLS, related to its superior adhesive properties and crystalline structure [40]. In adhesive interfaces, lateral forces are more hazardous than axial ones, because stresses are concentrated in the cervical region rather than distributed along the long axis, increasing the risk of irreparable fractures [20,40]. However, the high elastic modulus of lithium disilicate (LDS, 95 GPa) exerts greater stress on weaker surfaces, increasing the risk of irreparable fractures, whereas more flexible materials like resin nano-ceramics (RNC, 20 GPa) and zirconia-reinforced lithium silicate (ZLS, 70 GPa) distribute stress more homogeneously [40]. Manziuc et al. reported that zirconia-reinforced lithium silicate (ZLS) exhibited superior mechanical properties compared to feldspathic ceramics, lithium disilicate ceramics, and resin nano-ceramics, but demonstrates inferior esthetics due to the presence of tetragonal zirconia particles [43].
Resin-based materials, including resin nanoceramics (RNC), polymer-infiltrated ceramic networks (PICN), and millable composite resins, are emerging as reliable alternatives for endocrown restorations [2,19,37]. PICN consists of a 25% by volume polymer network and a 75% by volume ceramic network that combines the long-term aesthetic stability of ceramics with the preferred elastic modulus of resin composites [2,55]. RNC are composed of a resin-based matrix with dispersed fillers (nanoceramic particles), with the exact composition varying according to the specific product [2]. The materials exhibit high fracture resistance and an elastic modulus similar to that of dentin (18.6 GPa), thereby preventing catastrophic fractures. They tend to deform more before failing by changing the stress distribution and the contact with the surface of the restorative assembly [2,26,39,41]. Dartora et al. showed that PICN offers comparable fatigue failure load to LD restorations over the same number of loading cycles [41]. Beji Vijayakumar et al. concluded that RNCs have increased resilience to fractures compared to ZLS, although ZLS outperforms PICN in fracture resistance [2]. Keskin et al. reported survival rates of 82.7% for RNC and 86.8% for ZLS over a 3-year evaluation period, with no statistically significant difference between the two materials [32]. Resin-based materials experience fewer catastrophic failures, especially under axial loading, since they have the ability to absorb and distribute stresses homogeneously. Furthermore, these materials can be easily repaired intraorally [2]. Although their lower modulus of elasticity may reduce stress within the dentin, it can increase stress at the adhesive interface, thereby raising the risk of debonding [2,19,26,41]. The success of restorations depends on both internal and marginal fit, which is influenced by the material used. Taha et al. found that while LDGC, RNC, and resin-modified ceramics showed acceptable margin gaps, only RNC achieved a clinically acceptable fit [44].
To support clinical decision-making in the restoration of endodontically treated posterior teeth, a decision tree was developed based on the findings of this scoping review (Figure 3). This visual guide summarizes key criteria for selecting endocrown restorations, including remaining tooth structure, pulp chamber depth, presence of ferrule, available interocclusal space, material choice (LDS, ZLS, RNC), and adhesive technique. The aim is to assist clinicians in making evidence-based, case-specific restorative decisions that enhance the predictability and long-term success of treatment outcomes.
4.1.6. CAD/CAM-Fabricated Endocrowns: Precision, Efficiency, and Material Compatibility
The continuous use of CAD/CAM technology in restorative dentistry for milling endocrown restorations enables chairside treatment in a single appointment [36,56]. One of the main advantages demonstrated is the superior fracture resistance of CAD/CAM all-ceramic endocrowns, which surpasses that of non-CAD/CAM all-ceramic restorations [4,11,36]. According to Kuang et al. CAD/CAM all-ceramic endocrowns had a 5-year survival rate of 93.0% [33]. Fages et el. in their seven-year clinical trial observed a 98,66% survival rate of chairside CAD/CAM feldspathic ceramic endocrowns [30]. Similarly, Otto and Morman’s 12-year clinical study on chairside CAD/CAM feldspathic ceramic endocrowns revealed high survival rates, with 90.5% for molars and 75% for premolar [34]. Even though CAD/CAM endocrowns have extremely high survival rates and seem a successful long-term alternative, careful case selection and proper bonding techniques are essential to minimize risks and ensure successful outcomes.
4.2. Survival and Success Rates: Long-Term Outcomes and Clinical Predictability of Endocrowns
In terms of survival and success rates, endocrowns and post-and-core crowns appear to offer comparable outcomes for restoring endodontically treated molars [1,3,6,12,16,26,31]. Studies have shown that endocrowns demonstrate similar or even greater survival rates under repeated and static loads, generally due to their distinctive design and adhesive bonding mechanism, which promote better stress distribution and load transmission [4,23,27]. For instance, Fathi et al. reported a 5-year survival rate of 91.4% for endocrowns and 98.3% for post-core crowns, with no significant clinical differences [31], while Al-Dabbagh et al. demonstrated a 5-year survival rates of 89.1% for endocrowns and 98.2% for conventional crowns in molars [6]. In a 4-year retrospective study by Ayata et al. endocrowns demonstrated complete survival during follow-up period[57]. Belleflamme et al. highlighted impressive survival rates of up to 99% for endocrowns in posterior teeth, with Qamar emphasizing that this is the only long-term study providing a 10-year survival rate over in such an extended period [24,29]. Govare et al. mentioned that endocrowns had only 6% of root fractures and 71% of failures were due to loss of retention, whereas the root fracture rate for post or no post crowns was at 29% [26]. The success rate of endocrowns varies across different studies but consistently remains high, making them an excellent conservative option for restoring endodontically treated teeth.
4.3. Limitations of This Scoping Review
While this scoping review provides a broad overview of the available literature on endocrown restorations in endodontically treated molars, it is important to acknowledge several limitations associated with its methodological framework. Firstly, unlike systematic reviews, scoping reviews typically do not include an assessment of the quality of the eligible studies or an evaluation of the risk of bias using critical appraisal tools. As a result, the reliability and internal validity of the included sources were not critically appraised, which limits the ability to draw definitive conclusions or make evidence-based clinical recommendations. Additionally, although efforts were made to comprehensively search two major databases (PubMed and Scopus) and screen reference lists, relevant grey literature and unpublished data may have been missed. The variability in study designs, outcome measures, and reporting standards posed a significant challenge for data synthesis and meaningful comparison. These limitations highlight the need for future systematic reviews and meta-analyses to provide more definitive guidance based on rigorous appraisal and quantitative synthesis.
5. Conclusions
This scoping review provides a comprehensive synthesis of the current literature on the use of endocrowns for restoring extensively damaged posterior endodontically treated teeth. Based on the available evidence, endocrowns are particularly indicated in cases of significant coronal tooth structure loss, limited interocclusal space, and root canals with complex or atypical morphology. Notably, the presence of enamel along the majority of the restoration margins is a critical factor for ensuring long-term clinical success.Additionally, endocrown restorations are time-efficient, involving fewer procedural steps, reduced chairside time, and overall lower treatment costs compared to conventional post-and-core restorations. Furthermore, the use of resin-based materials and lithium disilicate ceramics has emerged as the most preferable choice, owing to their advancements in fracture resistance and aesthetic properties.
Multiple parameters influence the clinical and laboratory performance of endocrown restorations in endodontically treated teeth (ETT). Among others, the amount of the remaining tooth structure, the presence or absence of a ferrule, and the tooth’s location within the dental arch are the most critical factors for choosing a specific type of restoration. . Despite growing clinical acceptance, there is a continued need for standardization in both preparation protocols and material classification. The current literature reveals significant heterogeneity, primarily due to inconsistent descriptions of tooth preparation techniques for endocrowns.. While short-term findings are encouraging and support endocrowns as a viable alternative to conventional post-and-core restorations, the lack of robust long-term evidence limits definitive conclusions regarding their superiority in molars. Further well-designed, randomized clinical trials are necessary to resolve these discrepancies and to establish standardized treatment protocols.
References
- eAlhamdan, M.M.; Aljamaan, R.F.; Abuthnain, M.M.; Alsumikhi, S.A.; Alqahtani, G.S.; Alkharaiyef, R.A. Direct Versus Indirect Treatment Options of Endodontically Treated Posterior Teeth: A Narrative Review. Cureus 2024, 16, e67698. [Google Scholar] [CrossRef]
- Beji Vijayakumar, J.; Varadan, P.; Balaji, L.; Rajan, M.; Kalaiselvam, R.; Saeralaathan, S.; Ganesh, A. Fracture resistance of resin based and lithium disilicate endocrowns. Which is better? - A systematic review of in-vitro studies. Biomater Investig Dent 2021, 8, 104–111. [Google Scholar] [CrossRef]
- Carvalho, M.A.; Lazari, P.C.; Gresnigt, M.; Del Bel Cury, A.A.; Magne, P. Current options concerning the endodontically-treated teeth restoration with the adhesive approach. Braz Oral Res 2018, 32, e74. [Google Scholar] [CrossRef]
- Kassis, C.; Khoury, P.; Mehanna, C.Z.; Baba, N.Z.; Bou Chebel, F.; Daou, M.; Hardan, L. Effect of Inlays, Onlays and Endocrown Cavity Design Preparation on Fracture Resistance and Fracture Mode of Endodontically Treated Teeth: An In Vitro Study. J Prosthodont 2021, 30, 625–631. [Google Scholar] [CrossRef]
- AlDabeeb, D.S.; Alakeel, N.S.; Al Jfshar, R.M.; Alkhalid, T.K. Endocrowns: Indications, Preparation Techniques, and Material Selection. Cureus 2023, 15, e49947. [Google Scholar] [CrossRef]
- Al-Dabbagh, R.A. Survival and success of endocrowns: A systematic review and meta-analysis. J Prosthet Dent 2021, 125, 415.e411–415.e419. [Google Scholar] [CrossRef] [PubMed]
- Papia, E.; Habib, W.; Larsson, C. The Influence of Different Designs, Materials and Cements on the Success and Survival Rate of Endocrowns. A Systematic Review. Eur J Prosthodont Restor Dent 2020, 28, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, S.; Arakaki, Y.; Raggio, D.P.; Özcan, M. One-piece endodontic crowns in posterior teeth: An overview of systematic reviews. J Prosthet Dent 2024. [Google Scholar] [CrossRef]
- Thomas, R.M.; Kelly, A.; Tagiyeva, N.; Kanagasingam, S. Comparing endocrown restorations on permanent molars and premolars: a systematic review and meta-analysis. Br Dent J 2020. [Google Scholar] [CrossRef]
- Papalexopoulos, D.; Samartzi, T.K.; Sarafianou, A. A Thorough Analysis of the Endocrown Restoration: A Literature Review. J Contemp Dent Pract 2021, 22, 422–426. [Google Scholar] [CrossRef] [PubMed]
- AlHelal, A.A. Biomechanical behavior of all-ceramic endocrowns fabricated using CAD/CAM: A systematic review. J Prosthodont Res 2024, 68, 50–62. [Google Scholar] [CrossRef]
- Alwadai, G.S.; Al Moaleem, M.M.; Daghrery, A.A.; Albar, N.H.; Daghriri, A.A.; AlGhamdi, M.M.; Ageel, S.E.; Daghreeri, F.A.A.; Al-Amri, T.M.A.; Aridhi, W.H.; et al. A Comparative Analysis of Marginal Adaptation Values between Lithium Disilicate Glass Ceramics and Zirconia-Reinforced Lithium Silicate Endocrowns: A Systematic Review of In Vitro Studies. Med Sci Monit 2023, 29, e942649. [Google Scholar] [CrossRef] [PubMed]
- Biacchi, G.R.; Basting, R.T. Comparison of fracture strength of endocrowns and glass fiber post-retained conventional crowns. Oper Dent 2012, 37, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, P.; Manziuc, M.M.; Buduru, S.D.; Dudea, D. Endocrowns - a literature review. Med Pharm Rep 2023, 96, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, M.; DuVall, N.; Wajdowicz, M.; Brewster, J.; Roberts, H. Preparation Ferrule Design Effect on Endocrown Failure Resistance. J Prosthodont 2019, 28, e237–e242. [Google Scholar] [CrossRef]
- Mostafavi, A.S.; Allahyari, S.; Niakan, S.; Atri, F. Effect of Preparation Design on Marginal Integrity and Fracture Resistance of Endocrowns: A Systematic Review. Front Dent 2022, 19, 37. [Google Scholar] [CrossRef]
- Pissis, P. Fabrication of a metal-free ceramic restoration utilizing the monobloc technique. Pract Periodontics Aesthet Dent 1995, 7, 83–94. [Google Scholar]
- Ribeiro, V.F.; da Rosa, L.S.; Tribst, J.P.M.; Bier, C.A.S.; Morgental, R.D.; Valandro, L.F.; Baldi, A.; Scotti, N.; Pereira, G.K.R. Influence of height discrepancy between pulp chamber floor and crestal bone in the mechanical fatigue performance of endodontically-treated teeth restored with resin composite endocrowns. J Mech Behav Biomed Mater 2023, 142, 105854. [Google Scholar] [CrossRef]
- Vervack, V.; Johansson, C.; Coster, P.; Fokkinga, W.; Papia, E.; Vandeweghe, S. The fracture strength and the failure mode of lithium disilicate or resin nano ceramics as a crown, overlay, or endocrown restoration on endodontically treated teeth. J Esthet Restor Dent 2024, 36, 796–803. [Google Scholar] [CrossRef]
- Veselinova, M.; Diamantopoulou, S.; Paximada, C.; Papazoglou, E. In-Vitro Comparison of Fracture Strength of Endocrowns and Overlays in Endodontically Treated Teeth Manufactured with Monolithic Lithium Disilicate and Zirconia. J Funct Biomater 2023, 14. [Google Scholar] [CrossRef]
- Bindl, A.; Mörmann, W.H. Clinical evaluation of adhesively placed Cerec endo-crowns after 2 years--preliminary results. J Adhes Dent 1999, 1, 255–265. [Google Scholar] [PubMed]
- Ghajghouj, O.; Taşar-Faruk, S. Evaluation of Fracture Resistance and Microleakage of Endocrowns with Different Intracoronal Depths and Restorative Materials Luted with Various Resin Cements. Materials (Basel) 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Sedrez-Porto, J.A.; Rosa, W.L.; da Silva, A.F.; Münchow, E.A.; Pereira-Cenci, T. Endocrown restorations: A systematic review and meta-analysis. J Dent 2016, 52, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Qamar, Z.; Alghamdi, A.M.S.; Haydarah, N.K.B.; Balateef, A.A.; Alamoudi, A.A.; Abumismar, M.A.; Mathur, A.; Minervini, G. In Vitro Evaluation of Lithium Disilicate Endocrowns and Post and Core Crowns-A Systematic Review. J Funct Biomater 2023, 14. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Govare, N.; Contrepois, M. Endocrowns: A systematic review. J Prosthet Dent 2020, 123, 411–418.e419. [Google Scholar] [CrossRef]
- Lenz, U.; Bacchi, A.; Della Bona, A. Biomechanical performance of endocrown and core-crown restorations: A systematic review. J Esthet Restor Dent 2024, 36, 303–323. [Google Scholar] [CrossRef]
- Matos, L.M.R.; Silva, M.L.; Cordeiro, T.O.; Cardoso, S.A.M.; Campos, D.E.S.; de Muniz, I.A.F.; Barros, S.A.L.; Seraidarian, P.I. Clinical and laboratorial performance of rehabilitation of endodontically treated teeth: A systematic review. J Esthet Restor Dent 2024, 36, 1281–1300. [Google Scholar] [CrossRef]
- Belleflamme, M.M.; Geerts, S.O.; Louwette, M.M.; Grenade, C.F.; Vanheusden, A.J.; Mainjot, A.K. No post-no core approach to restore severely damaged posterior teeth: An up to 10-year retrospective study of documented endocrown cases. J Dent 2017, 63, 1–7. [Google Scholar] [CrossRef]
- Fages, M.; Raynal, J.; Tramini, P.; Cuisinier, F.J.; Durand, J.C. Chairside Computer-Aided Design/Computer-Aided Manufacture All-Ceramic Crown and Endocrown Restorations: A 7-Year Survival Rate Study. Int J Prosthodont 2017, 30, 556–560. [Google Scholar] [CrossRef]
- Fathi, A.; Ebadian, B.; Dezaki, S.N.; Mardasi, N.; Mosharraf, R.; Isler, S.; Tabatabaei, S.S. An Umbrella Review of Systematic Reviews and Meta-Analyses Evaluating the Success Rate of Prosthetic Restorations on Endodontically Treated Teeth. Int J Dent 2022, 2022, 4748291. [Google Scholar] [CrossRef]
- Keskin, S.C.; Sakar, A.; Bolay, S. A 3-year clinical evaluation of endocrown restorations with two different materials using the computer-aided design/ computer-aided manufacture system. J Dent 2024, 151, 105405. [Google Scholar] [CrossRef] [PubMed]
- Kuang, J.X.; Wu, H.Z.; Pan, Y.T.; Cheng, X.G.; Tian, Y.; Yu, Q. [A 5-year retrospective study of computer aided design and computer aided manufacturing ceramic endocrowns in endodontically treated posterior teeth]. Zhonghua Kou Qiang Yi Xue Za Zhi 2022, 57, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Otto, T.; Mörmann, W.H. Clinical performance of chairside CAD/CAM feldspathic ceramic posterior shoulder crowns and endocrowns up to 12 years. Int J Comput Dent 2015, 18, 147–161. [Google Scholar]
- Dartora, N.R.; de Conto Ferreira, M.B.; Moris, I.C.M.; Brazão, E.H.; Spazin, A.O.; Sousa-Neto, M.D.; Silva-Sousa, Y.T.; Gomes, E.A. Effect of Intracoronal Depth of Teeth Restored with Endocrowns on Fracture Resistance: In Vitro and 3-dimensional Finite Element Analysis. J Endod 2018, 44, 1179–1185. [Google Scholar] [CrossRef]
- Huang, Y.; Fokkinga, W.A.; Zhang, Q.; Creugers, N.H.J.; Jiang, Q. Biomechanical properties of different endocrown designs on endodontically treated teeth. J Mech Behav Biomed Mater 2023, 140, 105691. [Google Scholar] [CrossRef]
- Magne, P.; Carvalho, A.O.; Bruzi, G.; Anderson, R.E.; Maia, H.P.; Giannini, M. Influence of no-ferrule and no-post buildup design on the fatigue resistance of endodontically treated molars restored with resin nanoceramic CAD/CAM crowns. Oper Dent 2014, 39, 595–602. [Google Scholar] [CrossRef]
- Zeng, B.; Luo, B.; Hu, J.; Meng, D.; Zhang, J.; Cao, X.; Jiang, Q. Effect of margin designs and loading conditions on the stress distribution of endocrowns: a finite element analysis. BMC Oral Health 2024, 24, 657. [Google Scholar] [CrossRef] [PubMed]
- Anton Y Otero, C.; Bijelic-Donova, J.; Saratti, C.M.; Vallittu, P.K.; di Bella, E.; Krejci, I.; Rocca, G.T. The influence of FRC base and bonded CAD/CAM resin composite endocrowns on fatigue behavior of cracked endodontically-treated molars. J Mech Behav Biomed Mater 2021, 121, 104647. [Google Scholar] [CrossRef]
- El Ghoul, W.; Özcan, M.; Silwadi, M.; Salameh, Z. Fracture resistance and failure modes of endocrowns manufactured with different CAD/CAM materials under axial and lateral loading. J Esthet Restor Dent 2019, 31, 378–387. [Google Scholar] [CrossRef]
- Dartora, G.; Rocha Pereira, G.K.; Varella de Carvalho, R.; Zucuni, C.P.; Valandro, L.F.; Cesar, P.F.; Caldas, R.A.; Bacchi, A. Comparison of endocrowns made of lithium disilicate glass-ceramic or polymer-infiltrated ceramic networks and direct composite resin restorations: fatigue performance and stress distribution. J Mech Behav Biomed Mater 2019, 100, 103401. [Google Scholar] [CrossRef]
- Jalalian, E.; Zarbakhsh, A.; Khorshidi, S.; Golalipour, S.; Mohammadnasl, S.; Sayyari, M. Comparative analysis of endocrown fracture resistance and marginal adaptation: CAD/CAM technology using lithium disilicate vs. zirconia-reinforced lithium silicate ceramics. Saudi Dent J 2024, 36, 353–358. [Google Scholar] [CrossRef]
- Manziuc, M.; Kui, A.; Chisnoiu, A.; Labuneț, A.; Negucioiu, M.; Ispas, A.; Buduru, S. Zirconia-Reinforced Lithium Silicate Ceramic in Digital Dentistry: A Comprehensive Literature Review of Our Current Understanding. Medicina 2023, 59, 2135. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.I.; Hatata, N. Marginal and internal gaps evaluation of endocrown restoration fabricated of different CAD/CAM materials using CBCT: An In vitro study. Advanced Dental Journal 2024, 6, 208–215. [Google Scholar] [CrossRef]
- Soliman, M.; Alshamrani, L.; Yahya, B.; Alajlan, G.; Aldegheishem, A.; Eldwakhly, E. Monolithic Endocrown Vs. Hybrid Intraradicular Post/Core/Crown Restorations for Endodontically Treated Teeth; Cross-sectional Study. Saudi J Biol Sci 2021, 28, 6523–6531. [Google Scholar] [CrossRef]
- Taha, D.; Spintzyk, S.; Schille, C.; Sabet, A.; Wahsh, M.; Salah, T.; Geis-Gerstorfer, J. Fracture resistance and failure modes of polymer infiltrated ceramic endocrown restorations with variations in margin design and occlusal thickness. J Prosthodont Res 2018, 62, 293–297. [Google Scholar] [CrossRef]
- Zhang, Y.; Lai, H.; Meng, Q.; Gong, Q.; Tong, Z. The synergetic effect of pulp chamber extension depth and occlusal thickness on stress distribution of molar endocrowns: a 3-dimensional finite element analysis. J Mater Sci Mater Med 2022, 33, 56. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.; Duvall, N.; Wajdowicz, M.; Roberts, H. Effect of Endocrown Pulp Chamber Extension Depth on Molar Fracture Resistance. Oper Dent 2017, 42, 327–334. [Google Scholar] [CrossRef]
- Alqarni, H.; Qadoumi, M.; AlShehri, N.; AlNowaiser, N.; Alaqeely, R.; AlHelal, A.A.; Alrabiah, M.; Alshihri, A.; Alsayed, H. Resistance of Resin-Bonded Ceramic Endocrowns of Different Intracoronal Depths. Oral Health Prev Dent 2025, 23, 51–58. [Google Scholar] [CrossRef]
- Yılmaz, K.; Aydın, H.; Gönüldaş, F.; Kara, S.; Çiloğlu, Ö.; Özdemir, E.; Bilen, Z. Effect of Pulpal Base, Restorative Material, and Preparation Type on Marginal and Internal Fit and Fracture Strength of Endocrowns. Materials (Basel) 2025, 18. [Google Scholar] [CrossRef]
- Dong, X.; Ban, J.; Guo, H.; Zeng, Z.; Ren, N.; Bai, S.; Wang, Z. Optimization of endocrown design parameters for mandibular second molars: A 3D finite element analysis. J Mech Behav Biomed Mater 2025, 168, 107038. [Google Scholar] [CrossRef] [PubMed]
- Karn, G.; Shetty, M.; Hegde, C. Effect of different restorative design on stress concentration of lithium disilicate and monolithic zirconia endocrown on a mandibular molar - a finite element analysis. BMC Oral Health 2025, 25, 205. [Google Scholar] [CrossRef]
- Kumar, M.; Sidhu, K.; Bhushan, J. Comparative evaluation of marginal and internal fit of endocrowns with lithium disilicate, biocompatible high-performance polymer, and monolithic ceramic materials using computer-aided design and computer-aided manufacturing technology. J Conserv Dent Endod 2025, 28, 389–393. [Google Scholar] [CrossRef]
- Falahchai, M.; Ardekani, F.R.; Musapoor, N.; Hemmati, Y.B.; Asli, H.N. Effects of the Presence of Adjacent Tooth and Material Type on the Marginal and Internal Adaptation of Endocrowns Fabricated by the Digital Impression Technique. Clin Exp Dent Res 2025, 11, e70077. [Google Scholar] [CrossRef]
- Facenda, J.C.; Borba, M.; Corazza, P.H. A literature review on the new polymer-infiltrated ceramic-network material (PICN). J Esthet Restor Dent 2018, 30, 281–286. [Google Scholar] [CrossRef]
- Hiraba, H.; Nishio, K.; Takeuchi, Y.; Ito, T.; Yamamori, T.; Kamimoto, A. Application of one-piece endodontic crowns fabricated with CAD-CAM system to molars. Jpn Dent Sci Rev 2024, 60, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Ayata, M.; Küçükömeroğlu Oktay, E.; Albayrak, H.; Çakar, M.; Özcan, M. Evaluation of th clinical performance of endocrown and overlay restorations: A 4-year retrospective study. J Dent 2025, 160, 105874. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PCC Framework.
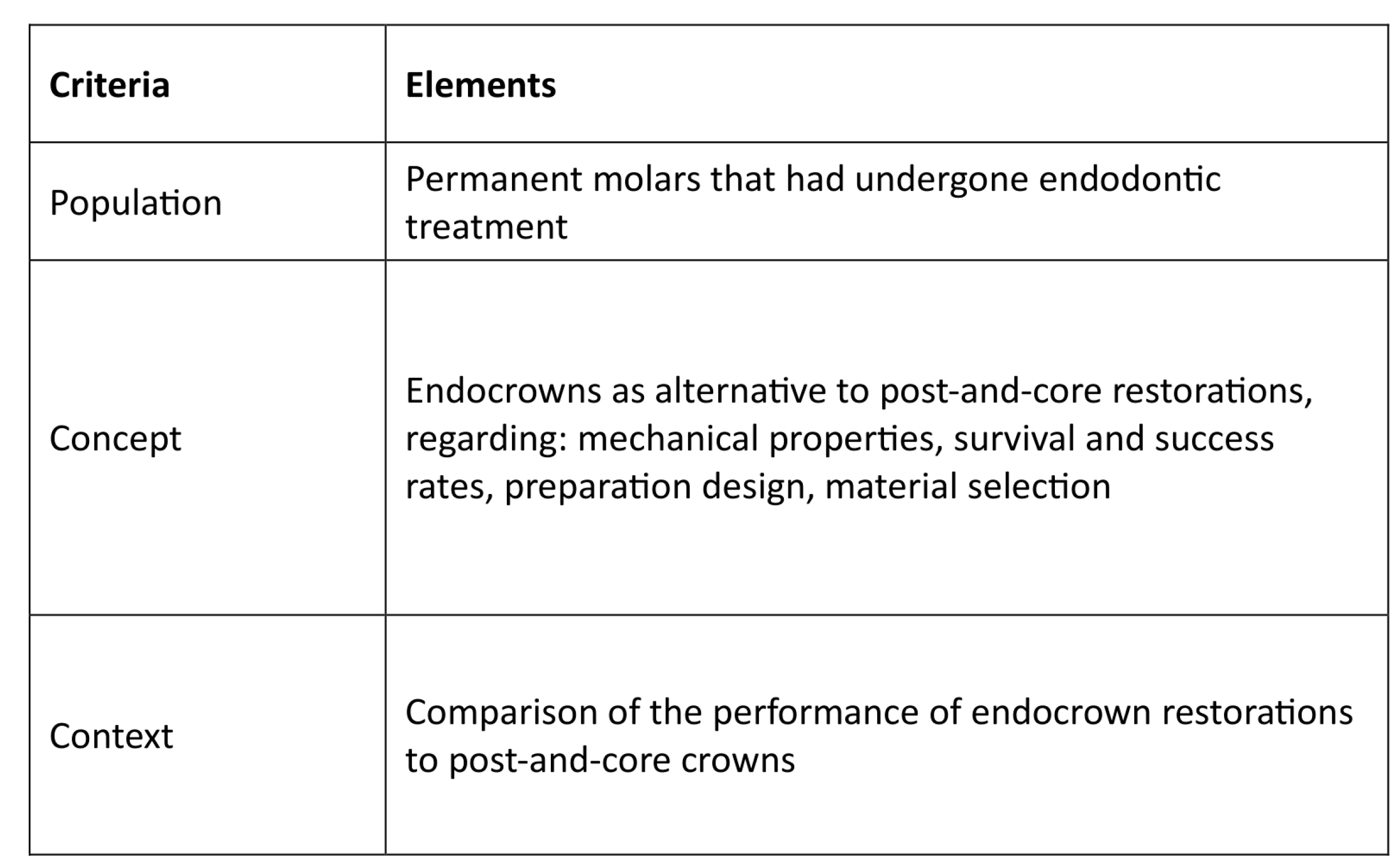
Figure 2.
PRISMA-ScR flow diagram.
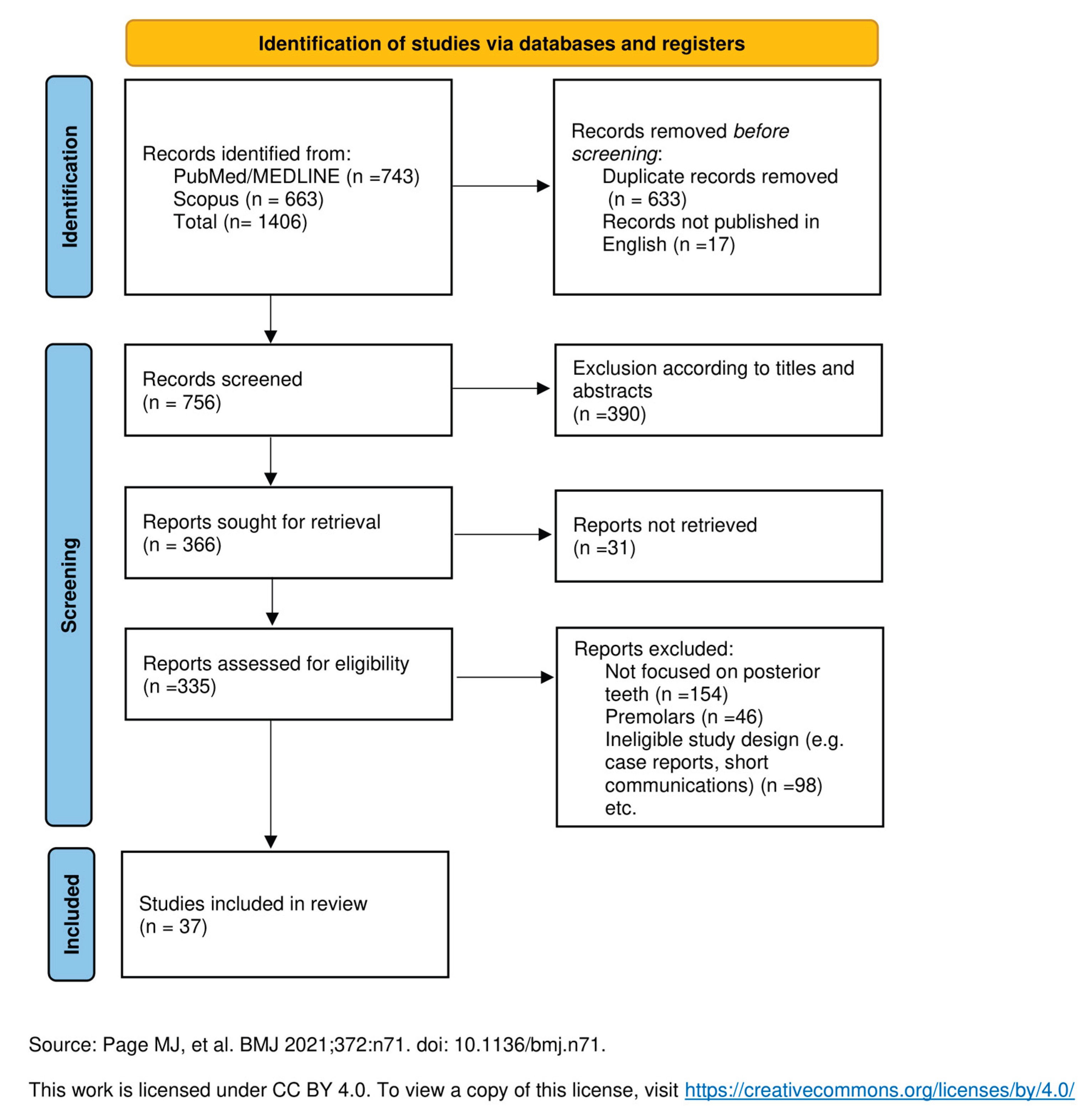
Figure 3.
Clinical Decision Tree for Endocrown Restoration Selection.
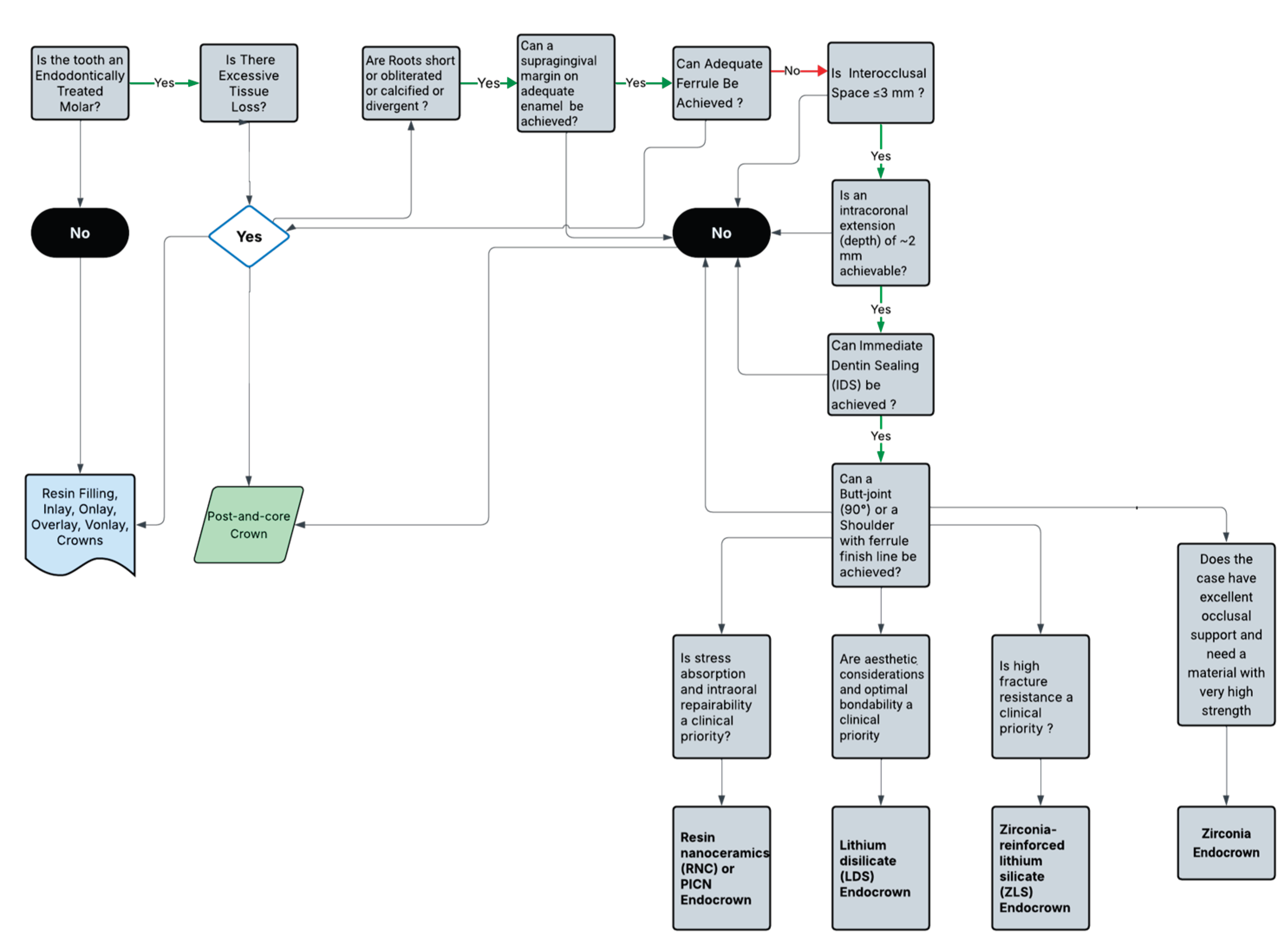

Table 1.
Systematic Reviews and Meta-analyses on Endocrown Restorations.
| Author(s)/Publication Year | Aim | Materials & Methods |
Conclusion |
|---|---|---|---|
| Comparison of Endocrown Restorations to Conventional Crowns | |||
| Sendrez- Porte et al., 2016 | Systematic review of clinical and in vitro studies comparing endocrown restorations with conventional treatments (posts-and-core crowns, composite resin, inlays/onlays), testing the hypothesis that endocrowns perform similarly. | Pubmed (MedLine), Lilacs, Ibecs, Web of Science, BBO, Scielo and Scopus Identified records: 103 Included records: 8 published between 1999 and 2014 |
Endocrowns offer comparable or superior performance to traditional methods, such as posts-and-core crowns, with demonstrated high success rates (94–100%), greater fracture strength, and favorable biomechanical performance, particularly in terms of failure patterns. Further studies are needed to validate long-term outcomes. |
| Govare et al., 2020 | Evaluation of endocrowns as a restorative option for extensively damaged teeth, assessing their predictability, success, survival rates, and fracture strength compared to post-retained restorations. | PubMed, Scopus, Embase, and the Cochrane Library Identified records: 110 Included records: 41 published between 1999 and 2018. |
Endocrowns offer a reliable alternative to post-retained restorations, especially for molars, with comparable or superior fracture strength. |
| Al-Dabbagh et al., 2021. | A review and analysis of the survival and success rates of endocrowns vs conventional crowns, offering evidence- based guidance for restoring extensively damaged teeth. | PubMed, Scopus, EMBASE, Cochrane, and Google Scholar (up to June 2019) Identified records: 2,584 Included records: 10 articles for systematic review and 3 clinical studies for meta-analysis. |
Endocrowns showed a 5-year survival rate of 91.4% and a success rate of 77.7%, compared to 98.3% and 94% for conventional crowns, with no significant differences (P > .05). |
| Qamar et al., 2023 | Comparison of the physical and mechanical properties of LDS endocrowns on posterior teeth and post-and-core restorations. | PubMed, Embase, Scopus, ISI Web of Knowledge (WoS), Google Scholar, unpublished studies, conference proceedings and cross-references up to 31 January 2023 Identified records: 291 Included records: 10 |
There is no significant difference between the fracture strength and failure rates of LDS endocrowns and conventional post-and-core crowns. |
| Lenz et al., 2024 | Comparison of the biomechanical performance of endocrowns and traditional post-and-core crown restorations (with and without intracanal posts) for rehabilitating ETT with severe coronal structure damage. | MEDLINE/PubMed, Scopus, and Web of Science based on in-vitro studies Identified records: 291 Included records: 31 published between 2015 and 2023. |
Endocrowns exhibited similar or greater biomechanical performance than post-and-core crown restorations across most evaluated studies. Demonstrated favorable survival rates under fatigue and monotonic loads, lower stress levels in restorative materials, and better failure patterns compared to post-and- core crowns. |
| Matos et al., 2024 | Assessment of clinical performance (survival rate, failure risk, fracture incidence) and laboratory outcomes (fracture mode, failure analysis) of rehabilitated ETT. | Pubmed, Scopus, Web of Science, Embase, Cochrane, Open Grey and manually Identified records: 89 articles Included records: 38 (31 in vitro and 7 RCTs) |
No significant difference in fracture resistance or failure modes between ETT with or without posts. Survival rates were similar, though failure risk was lower with posts. The need to consider tooth characteristics and remaining structure for each case. |
| Material-Based Comparison | |||
| Beji Vijayakumar et al., 2021 | Evaluation of whether RB endocrowns exhibit better fracture resistance and fewer catastrophic failures compared to LDS endocrowns in vitro studies. | PubMed, EBSCOhost, Cochrane Central Register of Clinical trials, Google Scholar and manually. Identified records: 229 Included records: 5 published between 2015 and 2020. |
RB endocrowns demonstrated similar or higher fracture resistance under axial forces and fewer catastrophic failures compared to LDS endocrowns. |
| Alwadai et al., 2023 | Analysis of in vitro studies on marginal adaptation of CAD/CAM and heat-pressed LDS and ZLS endocrowns. | Web of Science, PubMed, EMBASE, Scopus, Cochrane, Google Scholar, and ProQuest Identified records: 428 Included records: 17 published between 2016 and 2023. |
All-ceramic LDGC and zirconia endocrowns for posterior teeth, fabricated via CAD/CAM or heat-press, showed acceptable marginal adaptation. |
| AlHelal et al., 2024 | Assessment of fracture resistance of CAD/CAM vs. non-CAD/CAM endocrowns. | Embase, Web of Science, and Scopus. Identified records: 1,591 Included records: 17 |
CAD/CAM endocrowns show superior fracture resistance compared to non-CAD/CAM options. |
| Survival and Success Rates | |||
| Papia et al., 2020 | A review of literature on endocrowns, focusing on success, survival rates, and how designs, materials, and cements influence outcomes, providing guidance for restoring extensively damaged teeth. | Searches in PubMed, Cochrane and Scopus Identified records: 3,472 Included records: 6 Published between 1999 and 2017. |
Feldspathic endocrowns with a 1–4 mm pulp cavity, 1–2 mm shoulder preparation, and adhesive resin cement show promise for molars. |
| Mostafavi et al., 2022 | Evaluation of how preparation designs affect marginal integrity and fracture resistance of endocrowns, aiming to identify optimal designs for restoring severely damaged teeth. |
Searches in PubMed, Embase, Scopus, and the Cochrane Library Identified records: 200 included records: 16 published up to February 2021. |
Endocrown preparation design impacts marginal adaptation and fracture resistance, with excessive preparation reducing performance and increasing non-repairable fractures. Simpler cavity configurations are recommended. |
Abbreviations: LDGC; lithium disilicate glass-ceramic, LDS; lithium disilicate, ETT; endodontically treated teeth, CAD/CAM; computer-aided design and computer-aided manufacturing, RCT; randomized clinical trials.
Table 2.
Endocrowns: Survival and Success Rates, Indications, Preparation Design, Fracture Resistance and Material Type.
Table 2.
Endocrowns: Survival and Success Rates, Indications, Preparation Design, Fracture Resistance and Material Type.
| Author(s)/ Publication Year | Study Type | Objective | Study design | Main Findings/Conclusion |
|---|---|---|---|---|
| Clinical Performance and Long-Term Outcomes | ||||
| Otto et al., 2015 | Clinical Trial | Evaluation of long-term outcomes of chairside CAD/CAM feldspathic ceramic posterior shoulder crowns and endocrowns | 55 patients, with test group: 25 endocrowns (20 molars, five premolars) and control group: 40 shoulder crowns (8 conventional crowns and 32 “reduced prep” crowns) produced using CAD/CAM system with feldspathic ceramic and examined at baseline and up to 12 years ( mean 10 years, 8 months). | 12-year survival estimate of 95% for shoulder crowns on molars and 94.7% on premolars. In comparison, endocrowns exhibited a survival rate of 90.5% on molars and 75% on premolars. |
| Belleflamme et al., 2017 | Retrospective Study | Evaluation of ceramic and composite endocrowns with IDS, analyzing failures about tooth preparation and occlusal parameters. | Evaluation of 99 cases with mean observation period 44.7+/-34.6 months using FDI criteria, based on residual tooth tissue and preparation characteristics | Endocrowns are a reliable option, with a 10-year survival rate of 98.8% and a success rate of 54.9%. They preserve tissue and reduce failures versus post-and-core crowns. IDS increases bondingwhile LDS ceramics excel, and PICNs require further research. |
| Fages et al., 2017 | Clinical Trial | Determination of the survival rates of chairside CAD/CAM fabricated all-ceramic crowns and endocrowns for molars in clinical practice. | Three hundred twenty-threeBetween 2003 and 2008, 323 patients received 447 chairside CAD/CAM feldspathic ceramic restorations (212 crowns and 235 endocrowns) on molars by the same dentist, who then followed them up for 7 years. | The survival rate was estimated at 98.66%, and the success rate for endocrowns was almost 100%. All failures were attributed to partial ceramic fractures within the first two years of restoration. Chairside CAD/CAM all-ceramic crowns and endocrowns are an effective option in restorative dentistry, with long-term success. |
| Alhamdan et al., 2024 | Narrative Review | Assessment and comparison of treatment options to provide clinical recommendations for restoring posterior ETT. | PubMed and Google Scholar published between 1977 and2024. |
No survival rate superiority exists between direct and indirect restorations. Decisions depend on dentist experience, tooth structure, ferrule and restoration properties. |
| Ciobanu et al., 2023 | Literature Review | A comprehensive overview of endocrowns and evaluation of the impact of various materials and preparation designs on their mechanical properties, survival, success rate, and esthetics. | PubMed, Scopus, Web of Science, and Scielo Identified records: 163 Included records: 37 |
Endocrowns perform similarly or better than other restorations for extensively damaged ETT, with LDS and RNC being the most successful materials. |
| Morimoto et al., 2024 | Umbrella Review | Synthesis of evidence from systematic reviews on 1-piece endodontic crowns in posterior teeth, assessing clinical outcomes, survival, success rates, and PROMs, with a null hypothesis of no significant difference from complete crowns. |
MEDLINE/PubMed, WOS, Cochrane, OpenGrey, and manually (up to June 2024) Identified records: 468 Included records: 9 |
Indirect resin and ceramic those of complete crowns with posts. Limited data exist on zirconia and metal crowns, and PROMs remain unaddressed. The presence of low-quality studies, significant heterogeneity, and overlapping data limit conclusions. |
| Papalexopoulos et al., 2021 | Literature Review | Evaluation of endocrowns as a reliable alternative for extensively damaged ETT, focusing on their indications, contraindications, preparation, and materials. | Review of the literature with keywords “Endocrowns”, “Endodontically treated teeth’, “Literature review”, “Restorative dentistry” | Endocrowns demonstrate success rates similar to those of conventional restorations and are suitable for molars. However, further studies are needed to evaluate their success rates for premolars and anterior teeth. Retention depends on adhesive cementation, not traditional preparation. LDS or composite resin bonds outnumber resin cements. |
| Fathi et al., 2022 | Umbrella Review | Evaluation and comparison of the success rates of various prosthetic restorations on ETT. | MEDLINE/PubMed, Cochrane, and Google Scholar (up to November 2020) Identified records: 43 Included records: 14 |
Endocrowns and single crowns are equally effective for restoring ETT, with no statistically significant differences. |
| Keskin et al., 2024 | Clinical Trial | Comparison of the clinical efficacy of RNC and ZLS ceramic endocrowns in treating ETT using a chairside CAD/CAM system. | Ninety endocrown restorations fabricated in posterior teeth (52 RNC, 38 ZLS) using a CAD/CAM system with a three-year follow-up period. | The survival rates for the two groups were for RNC 82.7% and for ZLS 86.8%, highlighting their potential as materials for chairside fabrication of restoration for ETT. There were no statistically significant differences between the two materials in terms of debonding, ceramic fractures, tooth fractures, and secondary caries. |
| Kuang et al., 2022 | Retrospective Study | Evaluation of the survival rate and clinical performance of CAD/CAM ceramic endocrowns in posterior ETT. | A total of 101 CAD/CAM ceramic endocrowns on posterior teeth were performed on 74 patients from January 2016 to June 2017 and evaluated for their survival rate after 5 years. | The survival rate was 93.0% for CAD/CAM ceramic endocrowns after 5 years. with 93% on anatomic form and 95% on marginal adaptation. However, only 38% showed a good color match with adjacent teeth. No significant differences were found in survival rates based on sex, tooth position (premolars vs. molars), or materials used. |
| Design and Adhesion Considerations | ||||
| Magne et al., 2014 | In Vitro Study | Evaluation of the influence of different adhesive core buildup designs on the fatigue resistance and failure mode of endodontically treated molars restored with RNC CAD/CAM crowns using self-adhesive resin cement. | Forty-five human molars were divided into three groups (n=15) based on the restorative technique: Group I: 4-mm adhesive core buildup with complete crown restorations. Group II: 2-mm adhesive core buildup with complete crown restorations. Group III: No adhesive buildup (endocrown restoration). All groups were subjected to a failure test. | Buildup design did not significantly influence the fatigue resistance of endodontically treated molars restored with RNC CAD/CAM crowns. All designs, including those with no buildup (endocrown), survived regular masticatory forces. However, failure modes were more favorable in the 2-mm buildup and endocrown groups compared to the 4-mm buildup group. |
| Dartora et al., 2018 | In Vitro Study | Comparison of the biomechanical behavior of ETT restored with different endocrown extensions into the pulp chamber. | 30 human molars were divided into 3 groups (n=10) based on intracoronal extension depth (5 mm, 3 mm, 1 mm) and loaded to fracture. | Greater endocrown extension into the pulp chamber enhances mechanical performance, improving resistance, favoring favorable fracture modes, and optimizing stress distribution. |
| Einhorn et al., 2019 | In Vitro Study | Evaluation of the impact of ferrule inclusion on the fracture resistance of endocrowns specifically for mandibular molars. | Mandibular third molars (n = 12/group) were prepared by removing coronal tooth structure and restoring the chamber with resin core material. Ferrule heights were 1 mm, 2 mm, or none for each group. CAD/CAM LDS restorations were placed and subjected to failure testing. | Ferrule-containing endocrowns significant difference in failure stress was observed. Fewer catastrophic failures occurred with a 1 mm ferrule, although all restorations had high catastrophic failure rates at loads exceeding normal masticatory function. Further studies on adaptation and fatigue are needed. |
| Ribeiro et al., 2023 | In Vitro Study | Exploration and characterization of the influence of the height discrepancy between the pulp chamber floor and the crestal bone on the mechanical fatigue performance of ETT restored with resin composite endocrowns. | 75 human molars were divided into 5 groups (n=15) based on the pulp chamber floor position relative to crestal bone height (2 mm above, 1mm above, leveled, 1 mm below and 2 mm below). All were restored with 1.5 mm thick composite resin endocrowns and subjected to fatigue failure testing. | The insertion level of the dental element being rehabilitated with an endocrown significantly affects its mechanical fatigue performance. A higher pulp chamber floor relative to the crestal bone increases the risk of mechanical failure, while a lower pulp chamber floor height increases the risk of irreparable failures. |
| Huang et al., 2023 | In Vitro Study | Analysis of stress distribution in an endodontically treated mandibular molar with various endocrown configurations, particularly focusing on those with significant defects in the mesial wall. | Four distinct finite element models were constructed based on different endocrown configurations for a mandibular molar. Control Model: butt joint preparation with a 2 mm occlusal thickness. Experimental Models: three butt joint designs with varying distances between the bottom of the mesial wall preparation and the cemento-enamel junction set at 2 mm, 1 mm, and 0 mm, respectively. All models loaded with vertical and oblique forces. |
Increasing simulated defects in the mesial wall elevated peak Von Mises stress in the cement layer, with defects up to the cemento-enamel junction level posing the highest failure risk, particularly in cervical dentin. |
| Zeng et al., 2024 | In Vitro Study | Evaluation of the stress distribution in endocrown restorations applied to ETT, focusing on the effects of different margin designs and loading conditions, and determining how these factors influence stress concentrations and the overall mechanical performance of endocrowns. | Three-dimensional finite element models were created to simulate ETT molars restored with endocrowns. Groups: butt-joint (E0), 90°shoulder (E90) and 135° shoulder (E135) with shoulder group dimensions 1.5 mm height and 1 mm width. Static loads totaling 225 N were applied in 9 locations on the occlusal surface under both buccal and lingual loading conditions. |
The stress distribution patterns among the three margin designs were generally similar; however, the shoulder-type designs, particularly the 135° shoulder, demonstrated reduced stress concentration compared to the butt-joint design. Stress levels increased under lingual loading conditions, indicating that loading direction significantly influences stress distribution in endocrowns. |
| Mechanical Strength and Load Resistance | ||||
| Biacchi et al., 2012 | In Vitro Study | Comparison of the fracture strength of endocrowns and glass fiber post-retained conventional crowns, focusing on their mechanical performance under load to ensure the durability and functionality of ETT. | 20 human molars divided into two groups: glass fiber post-retained crowns and endocrowns anchored in the pulp chamber, subjected to controlled loading to assess fracture resistance and failure modes. | Endocrowns demonstrated superior fracture strength compared to glass fiber post-retained crowns, highlighting their reliability and durability for restoring extensively damaged ETT. |
| El Ghoul et al., 2019 | In Vitro Study | Evaluation of the fracture resistance and failure modes of endocrowns made of three CAD/CAM materials subjected to thermos-mechanical cycling loading | 80 human molars were divided into 4 groups (n = 20), (LDS crowns, CAD/CAM LDS endocrowns, CAD/CAM ZLS endocrowns and CAD/CAM RNC endocrowns) with half of them from each group being loaded axially and the other half laterally until fracture. | RNC, LDS, and ZLS endocrowns have greater fracture resistance than conventional ceramic post-and-core crowns. LDS endocrowns had the highest fracture strength under axial loading, while they also performed best under lateral loading. High rate of irreparable fractures (30-70%) across all endocrown groups highlights the need for further studies. |
| Anton Y Otero et al., 2021 | In Vitro Study | Evaluation of the fatigue resistance of cracked endodontically treated molars restored with CAD/CAM resin composite endocrowns reinforced with different fiber-reinforced composite bases. | 50 human molars were simulated with cracks and divided in 5 groups (group 1: cavity floors lined with 0.5 mm of flowable composite, group 2: cavity floors covered with one layer of FRC-net, group 3: cavity floors covered with three layers of FRC-net, group 4: cavity floors covered with 1mm of flowable FRC-resin, group 5: cavity floors covered with 2 mm of flowable FRC-resin. Groups 1,2,3 use a different flowable resin composite for preparation of chamber than groups 4 and 5 with alterations in composition. All groups submitted to loading testing for fatigue resistance. | The incorporation of fiber reinforcement did not improve the fatigue resistance of cracked endodontically treated molars with endocrown restorations, but improved the chance of repairability. |
| Kassis et al., 2021 | In Vitro Study | Evaluation of the fracture resistance and failure modes of endodontically treated mandibular molars restored with different designs of inlays, onlays, and endocrowns. | 180 human third molars divided into 6 groups (n=30): control (no preparation), inlay with EverX Posterior, inlay with G-aenial Universal Flo, onlay with EverX Posterior, onlay with G-aenial Universal Flo, and endocrown with an empty pulp chamber and subjected to compressive load. | Endocrowns exhibited the highest fracture resistance compared to inlays and onlays, with not statistically significant difference between endocrowns and onlays. Endocrowns also had a more favorable failure mode than inlays, indicating that the design of the restoration influences both fracture resistance and failure patterns. |
| Material- Based Comparisons | ||||
| Dartora et al., 2019 | Literature Review | A review of the literature about the mechanical and biological properties of ZLS in CAD/CAM systems. | Searches in PubMed, Web of Science, Cochrane and manually. 154 papers were identified; only 71 met the inclusion criteria. | ZLS restorations show better mechanical properties than feldspathic, LDS, hybrid ceramics, and RNC, but less effective than translucent or high-translucency zirconia. Marginal adaptation is almost equal to LDS. ZLS CAD/CAM restorations exhibit the least color change, compared to resin-based materials. ZLS exhibits superior mechanical properties compared to LDS. |
| Manziuc et al., 2023 | Literature Review | A review of the literature about mechanical and biological properties of ZLS in CAD/CAM systems. | PubMed, Web of Science, Cochrane and manually. Identified records: 154 Included records: 71. |
ZLS restorations show better mechanical properties than feldspathic, LDS, hybrid ceramics, and RNC, but less effective than translucent or high-translucency zirconia. Marginal adaptation is almost equal to LDS. ZLS CAD/CAM restorations exhibit the least color change, compared to resin-based materials. ZLS exhibits superior mechanical properties compared to LDS. |
| Veselinova et al., 2023 | In Vitro Study | Comparison of mechanical behavior of ETT restored with endocrowns or overlays made from either monolithic LDS or monolithic zirconia. |
48 human molars divided into 4 groups (n=12): overlays restored with monolithic LDS, overlays restored with monolithic zirconia, endocrowns restored with monolithic LDS, endocrowns restored with monolithic zirconia) and subjected to fracture strength test. | LDS endocrowns exhibit higher fracture strength and are a more reliable option compared to monolithic zirconia or overlay restorations. Endocrowns had more catastrophic failures compared to overlays. |
| Vervack et al., 2024 | In Vitro Study | Evaluation of the fracture strength and failure modes of LDS and RNC used as restorations (crown, overlay, or endocrown) on endodontically treated molars. | 60 molars were restored with two primary materials LDS and Hybrid Composite. Each material was employed in three d restoration designs: monolithic endocrown, crown with a separate composite core and overlay without core buildup or pulpal extension and subjected to fracture strength test. 10 sound served as a control group. |
There were no significant differences in fracture loads among the restoration types. The type of restoration and the material used influenced the failure modes observed. All restoration types demonstrated fracture strengths comparable to intact teeth. Endocrowns showed slightly lower fracture resistance compared to crowns and overlays but within clinically acceptable limits. LDS restorations predominantly showed catastrophic fractures while RNC restorations had more repairable fractures. |
| Jalalian et al., 2024 | In Vitro Study | Comparison of the fracture resistance and marginal adaptation of CAD/CAM LDS and ZLS endocrowns. | 24 human molars were divided in 2 groups (n=12) for ZLS and LDS endocrown fabrication using CAD/CAM. Vertical marginal gap was measured at three stages: before cementation, after cementation, and after thermomechanical cycling. Fracture resistance was tested at a 45° angle, and failure mode was assessed. | ZLS endocrowns exhibited superior marginal adaptation, higher fracture resistance and more irreparable fractures compared to LDS endocrowns, and both showed acceptable vertical marginal adaptation. |
| Taha et al., 2024 | In Vitro Study | Comparison of marginal and internal gaps in endocrowns made from three different CAD/CAM materials. | 30 human molars were divided into 3 groups (n=10): LDGC, resin-modified ceramic, and RNC and assessed for their accuracy of marginal and internal adaptation of the endocrowns with CBCT. | All tested materials exhibited clinically acceptable marginal gaps (<160 μm). The internal gaps were not clinically acceptable for all materials except for RNC. |
Abbreviations: FRC; fiber-reinforced composite, PICN; polymer-infiltrated ceramic network, LDGC; lithium disilicate glass-ceramic, LDS; lithium disilicate, ZLS; zirconia-reinforced lithium silicate glass-ceramic, RNC; resin nano-ceramic, ETT; endodontically treated teeth, CAD/CAM; computer-aided design and computer-aided manufacturing.
Table 3.
Comparison of Endocrown Materials.
| Material | Elastic Modulus | Fracture Resistance | Esthetics | Bonding | Failure Type | Best Used In |
|---|---|---|---|---|---|---|
| LDS | ~90–95 GPa | Excellent | Excellent | Strong micromechanical bond | Often catastrophic | High-esthetic zones, molars with deep chambers |
| ZLS | ~70 GPa | Very good | Moderate- High | Good | Mixed failures (some catastrophic) | Balanced cases with moderate esthetic needs |
| RNC | ~20 GPa | Moderate - High | Moderate | Weaker than LDS | Mostly restorable, flexible, debonding at adhesive interface | Bruxism, minimal prep, repairable restorations intraorally |
| PICN | ~30 GPa | Moderate | Moderate | Moderate | Deformable, restorable, debonding at adhesive interface | Patients with parafunction or low occlusal clearance |
| Monolithic Zirconia | >200 GPa | High but brittle | Low- Moderate | Weak | Catastrophic, root fracture | Rarely preferred, low-esthetic/ high-load areas only, good marginal fit |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



