
Submitted:
29 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Chronic osteoarthritis (COA) is a degenerative and progressive disease that causes inflammation and joint pain. Conventional treatment usually includes the use of drugs, which can cause significant adverse reactions, tolerance development, and limited analgesic efficacy. In recent years, the growing interest in the endocannabinoid system (ECS) has highlighted its potential as a therapeutic option for managing pain associated with COA. This study evaluated the efficacy of twice-daily (BID) oral administration of a full-spectrum Cannabis sativa oil extract for pain management over a six-week period. Three randomized study groups were formed: Cannabis, Placebo, and Control. Participants received one of the proposed treatment protocols and underwent initial evaluations, followed by pain monitoring using the Canine Brief Pain Inventory (CBPI) and the Canine Osteoarthritis Staging Tool (COAST). In the Cannabis and Placebo groups, the study was randomized and double-blind. The Cannabis extract had a concentration of 46.4 mg/ml, including cannabidiolic acid (CBDA), cannabidiol (CBD), Δ-9 tetrahidrocannabinol (THC), and tetrahydronannabinolic acid (THCA). Both groups followed a dose-escalation protocol of 0.1 mg/kg every four days during the first four weeks, concluding with two weeks at the maximum tolerated dose (DMT) of 2 mg/kg. Patients did not experience any adverse reactions. A significant pain response was obtained on day 28 of treatment, when the dose reached 2 mg/kg (DMT), the maximum dosage at which patients felt comfortable. Canine Breaf Pain Inventory (CBPI), scale results revealed a reduction in pain from time 0 to day 28 of 39.6% in the Cannabis group, 24.7% in the Placebo group, and an increase of 1.6% in the Control group. Additionally, Canine Ostheoarthritis Staging Tool (COAST), evaluation analysis indicated a reduction from level 5 to level 4 in 55.5% of cases in the Cannabis group, while no changes were observed in the Placebo and Control groups. We proposed that the total oily extract of the Cannabis sativa plant, administered by the oral route is effective in controlling the pain associated with COA in dogs, thereby improving the quality of life of the patient, our results supported it.
Keywords:
Osteoarthritis
; cannabidiolic acid
; chronic pain
; tetrahydronannabinolic acid
; Cannabidiol
; analgesia
; full spectrum extract
1. Implications
This study shows that Cannabis sativa oil extract can reduce pain in dogs with chronic osteoarthritis. Conventional treatments may cause adverse effects or lose effectiveness over time, but this research suggests that Cannabis therapy is a safe and effective adjunct.
Specifically, CBDA and THCA, along with their decarboxylated metabolites, were incorporated into a multimodal treatment approach, complementing traditional therapies. By improving mobility and comfort, this combined treatment enhances dogs’ quality of life. These findings may encourage further research into cannabis-based pain relief for other animals and even humans, offering a promising alternative for managing chronic pain conditions.
2. Introduction
Canine Chronic Osteoarthritis (COA), is a degenerative and progressive disease that affects the articular cartilage and subchondral bone of the joints over time, affecting the quality of life of dogs due to severe pain that leads to a decrease in mobility and exercise [1]. This disease can affect individuals of all ages, but there are predisposing factors such as breed, body condition, injury, joint deformities, and poorly executed exercise.
The most used drugs are non-steroidal anti-inflammatory (NSAIDS) reducing in time their doses avoiding adverse reactions. Many licensed NSAIDs provide analgesia for dogs, but no one, has been shown to be consistently superior to another, simultaneously in terms of efficacy and safety. It has been suggested that pain control in COA has been advanced by the concomitant use of carprofen with pregabalin, with quite different but complementary mechanisms of action [2].
Cannabinoids have analgesic and immunomodulatory effects in COA, an inflammatory disease. Fibroblasts present in synovial tissues of patients with rheumatoid arthritis and osteoarthritis express CB1 and CB2, GPR55 receptors more intensely in chondrocytes, articular cartilage, and subchondral bone [3,4], no statistically significant differences were observed for each evaluated joint.
The existence of the receptor for molecules such as CBD and THC, gives us the possibility to perform multimodal treatment in these patients postulates that the role of the CB2 receptor in inflammation is relevant, as its presence in inflamed tissues of humans and mice can produce an exacerbated response [5], suggests that, by blocking this receptor through treatment with cannabinoids, we might be able to reduce this hyperreactivity and reduce the response of inflammatory cells. Of the most studied endocannabinoids, Anandamide (AEA) and 2-diacylglycerol (2-AG), were found in the synovium of both affected and unaffected joints of dogs with COA. In the femoro-tibio-patellar joints with COA, the concentrations of AEA were higher, which reaffirms the role of these endocannabinoids in the control of joint inflammatory processes, [4].
The inclusion of CBD, THC, and other acids components of the plant, in multimodal pharmacological treatment, is a strategy that has been used to manage COA-related pain more effectively in dogs.
Treatment with full-spectrum Cannabis involves the comprehensive inclusion of the plant's extract, encompassing cannabinoids such as CBD and THC, acidic compounds, terpenes, flavonoids, and a wide array of other bioactive components. This approach enables the achievement of a synergistic effect, whereby the combined action of these active ingredients enhances the therapeutic potential of the plant. The best documented example of this is the so-called entourage effect, which can be seen in the THC-CBD pair, under balanced conditions [6].
Understanding the medicinal properties of cannabinoids, terpenes, and flavonoids is essential for creating optimal synergistic compositions to address specific symptoms, such as pain. CBD enhances THC's effects by improving its bioavailability and extending its half-life. Additionally, terpenes like β-myrcene provide analgesic, anti-inflammatory, antibacterial, and sedative effects, contributing to the entourage effect [7].
In addition to its antiinflammatory and antibiotic properties, α-pinene, inhibits acetylcholinesterase, which may counteract THC-induced short-term memory deficits. The β-caryophyllene is analgesic, gastric protective, and anti-inflammatory, and could directly activate the endocannabinoid system as a CB2 receptor agonist [1,7]. Although fat-soluble compounds face reduced bioavailability when administered orally, due to the active first-pass effect through the liver, studies have demonstrated that oil-based Cannabis extracts, can still achieve effective blood concentrations via oral administration.
Among the components found in Cannabis extracts, we should also mention the acid forms of these cannabinoids, THCA and CBDA, which are biosynthetic precursors of the THC and CBD molecules, respectively, and which are decarboxylated through a chemical oxidation reaction to form these active compounds. However, the acid forms of these two main cannabinoids have different effects at the systemic level and interact with each other. In terms of their effects, there is a potential use of THCA and CBD [8]. CBD/CBDA-rich hemp product would reduce acute pain scores compared to a placebo control, as an antiinflammatory agent due to its COX-2 inhibitory effects [9] in pain studies, and so anti-proliferative effects on cancer cells [10,11,12,13], with minimal adverse reactions.
Pain is an inherently subjective experience, particularly in animals. To address this challenge, several scales have been developed to assess pain in veterinary contexts. The COAST scale is designed to evaluate the progression of COA, while the Canine Brief Pain Inventory (CBPI) focuses on measuring pain intensity. The CBPI, [14], a validated questionnaire, quantifies pain through a series of 10 questions rated on a scale from 0 to 10, available for free access on the web site from the University. These questions assess the perceived intensity of pain and its impact on the daily activities of dogs, culminating in an overall evaluation of the patient. Owners are actively involved in completing the CBPI, making it a practical tool for identifying pain caused by COA.
The COAST scale complements the CBPI by staging patients based on CBPI-derived scores, as demonstrated by studies such as those by [15,16,17]. The COAST evaluation encompasses two primary steps: classification of COA based on the dog's interaction with its environment and staging through comprehensive assessments of the affected joint and radiographic findings. Staging values range from 1 to 4, reflecting the severity of the condition. Integrating both scales provides an integrated approach to assessing the impact of COA on the animal and the affected joints. The consolidated scores serve as an effective basis for determining the appropriate treatment strategy
3. Material and Methods
3.1. Study Design
The objectives of our study were to evaluate the efficacy of an oily full extract of Cannabis sativa, as an adjunctive treatment to NSAIDS in twenty-seven dogs with COA and to compare the pain intensity in dogs, with COA among the three study groups.
From a population of 70 dogs recruited by the Karü-Lawen Foundation (composed of veterinarians specialized in medical Cannabis), 27 dogs were selected to meet the following study requirements: male and female dogs, ≥7 years old; ≥8 kg, showing symptoms of COA, with progression of more than 6 months, clinically diagnosed with specialized radiological support, and either under or not under traditional pharmacological treatment.
The selection of patients was conducted through a form created using Google Workspace. Applicants provided information including email address, owner’s name and dog's name, age, sex, weight, affected joint, region of residence, and municipality. After collecting this information, those who met the study requirements were filtered, and the handlers were contacted to inform them that their dogs had been selected for the study.
A randomized controlled trial was carried out over six weeks. Three study groups were created (9 dogs each): Cannabis, Control, and Placebo.
The patients were continuously monitored by the attending veterinarian and their owner. The COAST scale was applied to stage the patients prior to treatment and during the progression of the pathology. The CPBI pain scale was also completed before treatment began and weekly by the caregiver in collaboration with the veterinarian. Before starting treatment, each dog underwent clinical, laboratory, and radiological evaluations by veterinary radiologists to confirm eligibility for inclusion in the study and to assess the clinical, laboratory, and radiological severity of their lesions. Two X-rays were taken in the standard projections of the affected limb, with a maximum effective period of 30 days.
Dogs exhibiting clinical or laboratory signs of conditions unrelated to COA, those who did not comply with the terms of informed consent, those with undisclosed pregnancies during the study, or those whose attending veterinarians did not follow the study's medical guidelines were excluded from the study.
The patients remained in their homes and continued with their regular lives throughout the study. Each dog was monitored by its attending physician with the assistance of the attending veterinarian, in addition to the attention of the tutor, who was responsible for recording noticeable changes throughout the week.
The placebo oil used was also the same oil base (extra virgin olive oil, odorless, tasteless), added to the conventional treatment. In the case of the Cannabis oil plus conventional treatment and Placebo oil plus conventional treatment group, the caregiver doesn’t know if the patient received Cannabis extract or not.
[18] recommend that in cases where a poor response to an NSAID was observed, a wash-out period ranging from 24 hours to 7 days, during which medications. We suspended treatment for one week in our patients and randomly assigned alternative drugs at doses recommended by their treating physician, as outlined by in view of these antecedents, patients were administered NSAIDs combined with pregabalin at their usual doses for all the treatment.
According to [19], currently there is no evidence to suggest that COX-2 selective NSAIDs combined with pregabalin provide superior efficacy or safety compared to other NSAIDs, veterinary specialists categorized the patients based on the state of joint deterioration, clinical symptoms, and examination results. Among the NSAIDs approved for veterinary use, systematic reviews evaluating treatments for COA, have consistently demonstrated robust evidence in the literature supporting the efficacy of meloxicam and carprofeno [2]. Considering each patient’s condition [20] and in mutual agreement with the treating physician, we determined that the use of carprofen, meloxicam, or pregabalin, randomly assigned, combined with Cannabis-derived treatments.
Therapeutic protocols:
a) Previcox®: 4mg/kg, SID, P.O., first week. Second week: 2.5 mg/kg PO SID, and from week 3 to week 6: 1.25 mg/kg PO SID and Pregabalin: 5 mg/kg, SID, PO.
b) Meloxicam: 0,1mg/kg, SID, P.O. and Pregabalin: 5 mg/kg, SID, PO.
c) Carprofen: 4 mg/kg SID, P.O., from week 2 to week 6; 2.2 mg/kg, SID, P.O. and Pregabalin: 5 mg/kg, SID, PO., 6 weeks.
3.2. Modelling
3.2.1. Randomization and Group Formation
The 27 selected patients were randomly distributed by us using Microsoft Excel, for Mac (2024), version 16.59 and 190 distributed into three study groups of 9 dogs each, to assess three treatments:
- Cannabis oil plus conventional treatment.
- Placebo oil plus conventional treatment.
- Conventional treatment
3.2.2. Validation and Quality Assurance
The validation and quality assurance of this study, are based on a series of rigorous methodological criteria that ensure the reliability and accuracy of the results obtained. From the experimental design to data analysis, processes have been implemented to minimize bias, optimize treatment safety, and reinforce the scientific solidity of the findings. Below are the key points that support the quality and validity of the study.
Randomized and double-blind design: This study was randomized and blinding minimize bias, ensuring that results are attributable to the treatment and not other factors.
Use of validated evaluation tools: The CBPI and COAST are established and reliable scales for measuring pain and disease progression.
Dose-escalation protocol: Gradual dosing helps determine the optimal dose without compromising safety.
Monitoring of adverse reactions: The absence of reported side effects supports the treatment’s safety validation.
3.3. Analysis of the oily extract of C. sativa.
Equipment (HPLC)
Waters HPLC equipment:
Degasser Serial No. M10DG2644M
Binary Pump 1525 Serial Number K1025P263A
UV-Visible Detector 2489 Serial No. M1087E218A
Column Furnace Series No. C115CH760G.
3.4. Samples
The C. sativa extract was standardized in an olive oil base and analysed by the laboratory "Terpene Analytics", providing a report of the cannabinoid content of the sample. Resin sample extracted by the Rick Simpson Oil (RSO) method, which corresponds to a dilution of the dry matter in ethanol with subsequent evaporation under controlled conditions. The result is a full spectrum resin, high in CBD-A whose cannabinoids are in the process of decarboxylation [21].
THC represents 9.45% of the total weight of the sample and THC-A 1.927%, giving a THC potential of 11.141%. CBD-A represents 24.649%, and CBD 10.376%, giving a CBD potential of 31.993%. Cannabinol (CBN) is not detected. In total, this RSO presents a total of 46,403% of cannabinoids between THC-A, THC, CBD-A, and CBD. (See Figure 1)
3.5. Drops Concentration and Treatment
A 10% (1g/10ml) oral resin drop preparation contains 2.32 mg of cannabinoids per drop, including THC-A, THC, CBD-A, and CBD (equivalent to 2 drops or 0.1 ml). Given that 2 drops contain 2.32 mg; each drop is estimated to provide approximately 1.16 mg. As administering fractional drops is not feasible, the dosage was adjusted to the nearest whole number. The treatment involved dose escalations starting at 0.1 mg/kg every four days over a period of four weeks, followed by the final two weeks at the maximum tolerated dose (DMT) [22].
3.6. Pain Assessment and Staging of Pain
The cases studied were clinically diagnosed with specialized radiological support, regardless of whether they were undergoing traditional pharmacological treatment.
The patient selection process was carried out via a Google Workspace form, in which participants provided details such as their email address, the owner's name and the dog's name, age, sex, weight, affected joint, region of residence, and municipality. Once the data was collected, eligible candidates were filtered, and their handlers were notified of their selection. The study was a randomized controlled trial conducted over six weeks, comprising three groups of 9 dogs each: A Cannabis group, a Control group, and a Placebo group.
Patients were continuously monitored by the attending veterinarian alongside their caregivers. To assess the condition of the dogs before initiating treatment and to track the progression of the pathology, the COAST scale was applied. Additionally, the CPBI pain scale was completed before treatment began and on a weekly basis by the caregiver in collaboration with the treating veterinarian.
Prior to initiating treatment, each dog underwent clinical, laboratory, and radiological evaluations by veterinary radiologists to confirm their eligibility for the study. These evaluations also determined the clinical, laboratory, and radiological severity of the lesion. Two radiographic images were taken in standard projections of the affected limb within a maximum effective period of 30 days.
Exclusion criteria included dogs exhibiting clinical or laboratory abnormalities attributable to conditions unrelated to COA, as well as those whose owners failed to comply with the informed consent terms, those with undisclosed pregnancies, or those whose veterinarians did not adhere to the study protocol. Throughout the study, patients remained in their homes, continuing their regular routines. The study was randomized and blinded.
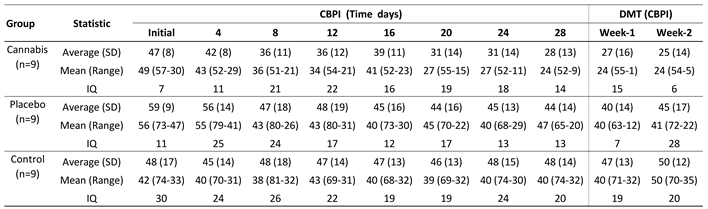
The patients underwent an initial and final COAST evaluation, as well as pain assessments using the CBPI scale every 4 days, and upon reaching the Maximum Tolerated Dose (DMT), as shown in Table 1.
3.7. Statistical Analysis of Results
For data analysis, descriptive statistics were used, including the number of cases, mean, median, and interquartile range, complemented by line graph visualizations. Statistically significant differences in pain levels, both according to treatment and across different evaluation periods, were assessed using one-way analysis of variance (ANOVA), after verifying normality with the Shapiro-Wilk test and homogeneity of variances. Comparisons of pain levels with the Maximum Tolerated Dose (DMT) were performed using a paired samples t-test. Additionally, comparisons of pain levels between groups were made using data standardized by their means, considering differences in pain levels at the start of the trial. Statistical significance was established at p < 0.05.
To better visualize the results of the study to evaluate the patients' pain levels from time 0 to day 28 we created two-line graphs (Figure 2). In the first graph (a), a decrease in pain levels can be observed in both the control and placebo groups, while the Cannabis group shows stability. However, the actual values at the beginning of the trial indicate that the groups started at 0 with different baseline pain levels. Therefore, the standardized values based on their means were presented in graph (b). This graph demonstrates that the groups started under statistically similar conditions, with no significant differences (F=2.48; p=0.10). To better visualize the results of the study by assessing the pain level of the patients from 0 to 28 days, the results were plotted in two-line graphs.
Furthermore, the results indicated that there were no statistically significant differences in pain levels one week after achieving the maximum tolerated dose. These findings are clearly depicted in Figure 3."
When evaluating the results of the Coast before and after, it was determined that only 55.5% of the patients treated with cannabis dropped to level 3, from level 4. Figure 4.
4. Discussion
Our findings are consistent with recent analyses of commercial CBD oils, which highlight the significant variability in cannabinoid concentrations across products and underscore the importance of standardized extraction and quantification methods [23]. The use of full-spectrum RSO extracts, such as the one described here, provides a broad cannabinoid profile, including both acidic and decarboxylated forms, which may enhance therapeutic potential through the entourage effect. However, the absence of CBN and the relatively high THC potential (11.141%) also emphasize the need for precise dosing and safety monitoring, particularly in veterinary applications.
To our knowledge, this is the first study conducted in Chile that evaluates the effects of Cannabis on pain in canines. We used extract rich in CBDA, CBD, THC, and THCA at a maximum dose of 2 mg/kg, administered orally during the last two weeks of treatment. Patients did not experience any adverse reactions.
A significant pain response was obtained on day 28 of treatment where the dose was 2 mg/kg (MTD), maximum dosage where patients felt comfortable [24]. The escalation dosing used has been described in previous research, where the safety of Cannabis oil was evaluated every 4 days between doses, by means of 10 escalations [22]. This dosage escalation achieves that the patient increases his tolerance to pain and decreases the interference with his daily activities, which was represented in the two scales used.
The Cannabis group showed a pain reduction of 45.67% (CBPI) notoriously surpassing the significance of the p value agreed in the hypothesis (p<0.05) and a drop in the stage of 50% of these patients (COAST), this remarkable pain reduction has been described in a previous study, but only with CBD [1,25], demonstrated that an 8-week oral administration of a whole-food nutritional supplement containing full-spectrum hemp oil (standardized to 15 mg phytocannabinoids, at 2 mg/kg BID) significantly reduced owner-reported pain in dogs. The intervention group showed notable improvements in CBPI scores (−46.2%), stair climbing (14.7%) and descending (10.6%), and overall daily activity (25.9%), while no changes were observed in the placebo group.
CBD only oil leaves a number of compounds unassessed, such as terpenes, flavonoids and other relevant cannabinoids such as THC and its biosynthetic precursors. in similar studies These compounds have been evaluated but by transdermal application and at a dose of 4 mg/kg of total cannabinoids. As a result, CBDA and THCA are consistently better absorbed than CBD or THC [26].
The advantage of using a Cannabis oil with total cannabinoids and terpenoids is to take advantage of the entourage effect, which improves the bioavailability of THC and CBD, extending their half-life, obtaining a longer analgesia and therefore a better quality of life of the patient [7]. In addition, BID administration ensures a stable and permanent effect between doses according to a study conducted in 2020, which ensures that the initial plasma depletion rate from T max is up to 12 h after dosing, thus maintaining a constant plasma concentration or steady state [27].
Three reviewed studies demonstrated a significant effect of CBD oil in reducing pain and improving the activity levels of dogs, as reported through subjective pain and activity scoring systems by both owners and veterinarians [1,2,28]. The fourth study was the first among the reviewed works to utilize objective gait analysis, which revealed no notable improvement in locomotion for canine patients receiving CBD oil treatment compared to the placebo group [29].
At present, the evidence supporting the efficacy of CBD oil in alleviating pain associated with canine osteoarthritis (OA) alongside conventional treatments, such as anti-inflammatories and other analgesics, remains weak. However, in our study, which utilized CBD, CBDA, THC, and THCA, the outcomes were highly positive in terms of improvement [20].
The results obtained, contribute and complement previous studies where the toxicology and pharmacology of the main cannabinoids, THC and CBD have been evaluated [22,27] and puts on the table the important role played in canines not only by THC and CBD, but also by their biosynthetic precursors, THCA and CBDA, whose interaction has been investigated in rats [8] and humans [9,10,11,12] and that in this study was no exception, since 24.6% and 1.9% of the total cannabinoids, corresponded to CBDA and THCA respectively, which puts in high interest the effect, bioavailability, pharmacology and toxicology of these acids, expanding the line of research and opening the possibility for other studies with greater focus on them. CBD, CBDA, and THCA are non-psychotropic and generally well-tolerated with minimal adverse effects.
Recent research highlights that CBDA and THCA exhibit superior absorption in dogs compared to CBD. Although the pharmacology of CBDA remains underexplored, evidence suggests that CBDA enhances serum CBD levels with lower doses by improving the absorption and retention of both CBD and CBDA [13]. It is worth mentioning the effect observed in the placebo group, where a 25.05% reduction in pain suggests a potential anti-inflammatory and analgesic role of the lipid matrix in canines. This effect parallels findings in humans with immune-mediated inflammatory conditions, such as rheumatoid arthritis, where phenolic compounds exert anti-inflammatory, antioxidant, and immunomodulatory actions [30]. Additionally, the use of extra-virgin sunflower oil as a cannabinoid vehicle may contribute to this response, as its fatty acid profile and antioxidant content enhance bioavailability and tolerability properties previously demonstrated in canine formulations using sunflower-based carriers [31].
5. Conclusions
The complete extract of Cannabis, based on CBD-A, CBD and THC-A, THC with CBD predominance and maximum tolerated dose (MTD) of 2 mg/kg is effective and safe as a complementary treatment for COA for 6 weeks. However, more long-term studies, using full spectrum extract of Cannabis, with higher doses and larger populations are needed to identify the effects of Cannabis over prolonged periods, as well as its effect in other species and against other pathologies that affect the quality of life of animals.
Declaration of interest: The authors declare that they have no conflicts of interest related to this study. There are no financial, personal, or professional relationships that could influence the results. Additionally, the authors do not hold any intellectual property or patents related to the findings.
Author Contributions
Conceptualization, B.E.T. and S.A.B.; methodology, A.N.S., E.S.A. y M.S.C.; validation, B.E.T and S.A.B., formal analysis, M.S.C.; investigation, B.E.T, A.N.S., M.S.C. y F.A.A.; resources, A.N.S., E.S.A. and M.S.C.; data curation, M.S.C.; writing—original draft preparation, B.T.E and S.A.B.; writing—review and editing, B.E.T. and S.A.B.; supervision, B.E.T., A.N.S, A.S.C. All authors have read and agreed to the published version of the manuscript.
Financial support statement
This research was conducted without any external funding.
Informed Consent Statement
Informed consent was obtained from all dog owners prior to the inclusion of their animals in the study.
Institutional Review Board Statement
The study was approved by the Institutional Committee for the Care and Use of Animals of the University of Mayor (Approved on April first, 2019).
Data and model availability statement:
The data collected in this study is available to other researchers without restrictions. The statistical and experimental models can be consulted whenever required. The database is under the custody of the investigators and is accessible whenever needed.
Declaration of generative AI and AI-assisted technologies in the writing process
Not applicable.
Acknowledgements
We sincerely thank the Karu Lawen Foundation for their invaluable support in the management, collection, supervision, methodology of this research and selection of patients for this study. Their dedication and contributions were crucial to its successful completion.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
References
- Brioschi, F. A. , Di Cesare, F., Gioeni, D., Rabbogliatti, V., Ferrari, F., D’urso, E. S., Amari, M., & Ravasio, G. Oral transmucosal cannabidiol oil formulation as part of a multimodal analgesic regimen: Effects on pain relief and quality of life improvement in dogs affected by spontaneous osteoarthritis. Animals 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Pye, C. , Bruniges, N., Peffers, M., & Comerford, E. Advances in the pharmaceutical treatment options for canine osteoarthritis. The Journal of small animal practice 2022, 63, 721–738. [Google Scholar] [CrossRef] [PubMed]
- Donvito, G., Nass, S.R., Wilkerson, J.L., Curry, Z.A., Schurman, L.D., Kinsey, S.G. and Lichtman, A. H. The Endogenous Cannabinoid System: A Budding Source of Targets for Treating Inflammatory and Neuropathic Pain Neuropsychopharmacol. 2018, 43, 52–79. [CrossRef]
- Zamith Cunha, R.; Salamanca, G.; Mille, F.; Delprete, C.; Franciosi, C.; Piva, G.; Gramenzi, A.; Chiocchetti, R. Endocannabinoid System Receptors at the Hip and Stifle Joints of Middle-Aged Dogs: A Novel Target for the Therapeutic Use of Cannabis sativa Extract in Canine Arthropathies. Animals 2023, 13, 2833. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, C. , Blanchet, M.R., Laviolette, M., Flamand, N. The CB2 receptor and its role as a regulator of inflammation Cell. Mol. Life Sci. 2016, 73, 4449–4470. [Google Scholar] [CrossRef]
- Anand, U. , Pacchetti, B., Anand, P., & Sodergren, M. H. Cannabis-based medicines and pain: A review of potential synergistic and entourage effects. Pain management 2021, 11, 395–403. [Google Scholar]
- Russo, E.B. , Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br, J, Pharmacol. 2011, 63, 1344–64. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rock, E. M. , Limebeer, C. L., & Parker, L. A. Effect of combined doses of Δ (9)-tetrahydrocannabinol (THC) and cannabidiolic acid (CBDA) on acute and anticipatory nausea using rat (Sprague- Dawley) models of conditioned gaping. Psychopharmacology 2015, 232, 4445–4454. [Google Scholar] [CrossRef]
- Takeda, S. , Misawa, K., Yamamoto, I., & Watanabe, K. Cannabidiolic acid as a selective cyclooxygenase-2 inhibitory component in cannabis. Drug metabolism and disposition: the biological fate of chemicals 2008, 36, 1917–1921. [Google Scholar] [CrossRef]
- De Petrocellis, L. , Ligresti, A., Moriello, A. S., Allarà, M., Bisogno, T., Petrosino, S., Stott, C. G., & Di Marzo, V. Effects of cannabinoids and cannabinoid-enriched Cannabis extracts on TRP channels and endocannabinoid metabolic enzymes. British journal of pharmacology 2011, 163, 1479–1494. [Google Scholar] [CrossRef]
- De Petrocellis, L. , Ligresti, A., Schiano Moriello, A., Lappelli, M., Verde, R., Stott, C. G., Cristino, L., Orlando, P., & Di Marzo, V. Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: pro-apoptotic effects and underlying mechanisms. British journal of pharmacology 2013, 168, 79–102. [Google Scholar] [CrossRef]
- Takeda, S. , Okazaki, H., Ikeda, E., Abe, S., Yoshioka, Y., Watanabe, K., & Aramaki, H. Down-regulation of cyclooxCygenase-2 (COX-2) by cannabidiolic acid in human breast cancer cells. The Journal of toxicological sciences 2014, 39, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Klatzkow, S. , Davis, G., Shmalberg, J., Gallastegui, A., Miscioscia, E., Tarricone, J., Elam, L., Johnson, M.D., Leonard, K.M. and Wakshlag, J. J. Evaluation of the efficacy of a cannabidiol and cannabidiolic acid rich hemp extract for pain in dogs following a tibial plateau leveling osteotomy. Front Vet. Sci. 2023, 9, 1036056. [Google Scholar] [CrossRef] [PubMed]
- University of Pennsylvania, CBPI https://www.vet.upenn.edu/research/clinical-trials-vcic/our-services/pennchart/cbpi-tool/cbpi-tool-form, from the University of Pennsylvania 2021.
- Brown, D. C. , Boston, R. C., Coyne, J. C., Farrar, J. T. The ability of the Canine Brief Pain Inventory to detect responses to treatment in dogs with osteoarthritis. Journal of the American Veterinary Medical Association 2008, 233, 1278–83. [Google Scholar] [CrossRef] [PubMed]
- Brown, D. C. The Canine Brief Pain Inventory - User Guide. https://www.vet.upenn.edu/research/clinical-trials-vcic/our.Services/pennchart/cbpi-tool, 2018.
- Cachon, T., Frykman, O., Innes, J. F., Lascelles, B., Okumura, M., Sousa, P., Staffieri, F., Steagall, P. V., Van Ryssen, B., & COAST Development Group. Face validity of a proposed tool for staging canine osteoarthritis, 2018: Canine OsteoArthritis Staging Tool (COAST). In: Veterinary journal (London, England:. 1997, 235, 1–8. [CrossRef]
- Hunt, J. , White, K. Pain management in small animal practice, 2019. In: Self I (ed). BSAVA guide to pain management in small animal practice. 1st edn. Gloucester: BSAVA: 24–41.
- Capon, H. (2019). Understanding the pharmaceutical approach to pain management in canine osteoarthritis. Companion animal | April–June 2021, Volume 26 No 6.
- Yeung, T. and Uquillas, E. Does oral cannabidiol oil in adjunct to pain medications help reduce pain and improve locomotion in dogs with osteoarthritis? Veterinary Evidence 2025, 10, 1–20. [Google Scholar] [CrossRef]
- Namdar, D. , Mazus, M., Ion., A., & Koltai, H. Variation in the compositions of cannabinoid and terpenoids in Cannabis sativa derived from inflorescence position along the stem and extraction methods. Industrial Crops & Products 2018, 113, 376–382. [Google Scholar]
- Vaughn, D. , Kulpa, J. and Paulionis, L. Preliminary Investigation of the Safety of Escalating Cannabinoid Doses in Healthy Dogs. Front. Vet. Sci. 2020, 7, 51. [Google Scholar] [CrossRef]
- Lindekamp, N., Weigel, S., Sachse, B., Schäfer, B., Rohn, S., Triesch, N. Comprehensive analysis of 19 cannabinoids in commercial CBD oils: concentrations, profiles, and safety implications. J. Consum. Prot. Food. Saf. 2024, 19, 259–267. [CrossRef]
- Gamble, L.J. , Boesch, J.M., Frye, C.W., Schwark, W.S., Mann, S., Wolfe, L., Brown, Holly., Berthelsen, E.S. & Wakshlag, J.J. Pharmacokinetics, safety, and clinical efficacy of cannabidiol treatment in osteoarthritic dogs. Frontiers in Veterinary Evidence. 2018, 5, 165. [Google Scholar] [CrossRef]
- Panda, C.; Rathinasabapathy, T.; Metzger, B.; Dodson, S.; Hanson, D.; Griffiths, J.; Komarnytsky, S. Efficacy and tolerability of full spectrum hemp oil in dogs living with pain in common household settings. Front. Vet. Sci. 2024, 11, 1384168. [Google Scholar] [CrossRef]
- Hannon, M.B. , Deabold, K.A., Talsma, B.N., et al. Serum cannabidiol, tetrahydrocannabinol (THC), and their native acid derivatives after transdermal application of a low-THC Cannabis sativa extract in beagles. J. vet. Pharmacol. Therap. 2020, 43, 508–511. [Google Scholar] [CrossRef]
- Chicoine, A. , Illing, K., Vuong, S., Pinto, K.R., Alcorn, J. and Cosford, K. Pharmacokinetic and Safety Evaluation of Various Oral Doses of a Novel 1:20 THC: CBD Cannabis Herbal Extract in Dogs. Front. Vet. Sci. 2020, 7, 583404. [Google Scholar] [CrossRef]
- Kogan, L. , Hellyer, P. & Downing, R. The Use of Cannabidiol-Rich Hemp Oil Extract to Treat Canine Osteoarthritis-Related Pain: A Pilot Study. American Holistic Veterinary Medical Association Journal 2020, 58, 35–45. [Google Scholar]
- Mejia, S. , Duerr, F.M., Griffenhagen, G. & McGrath, S. Evaluation of the Effect of Cannabidiol on Naturally Occurring Osteoarthritis-Associated Pain: A Pilot Study in Dogs. Journal of the American Animal Hospital Association 2021, 57, 81–90. [Google Scholar] [CrossRef]
- Santangelo, C. , Vari, R., Scazzocchio, B., De Sanctis, P., Giovannini, C., D'Archivio, M., & Masella, R. Anti-inflammatory activity of extra virgin olive oil polyphenols: ¿Which role in the prevention and treatment of immune-mediated inflammatory diseases? Endocrine, Metabolic & Immune Disorders - Drug Targets 2018, 18, 36–50. [Google Scholar] [CrossRef]
- Wakshlag, J. J. , Cital, S., Eaton, S. J., Prussin, R., & Hudalla, C. Pharmacokinetics of cannabidiol and cannabidiolic acid in dogs using different delivery methods. Animals 2020, 10, 1505. [Google Scholar] [CrossRef]
Figure 1.
Cannabinoid concentration in the extract analyzed by the Terpeno Analytics laboratory. Δ-9 Tetrahidrocannabinol (THC) represents 9.45% of the total weight of the resine and Δ-9 Tetrahidrocannabinol (THC-A) 1.927%, giving a THC potential of 11.141%. Cannabidiol (CBD-A) represents 24.649%, and Cannabidiol (CBD) 10.376%, giving a CBD potential of 31.993%. Cannabinol (CBN) is not detected. In total, this RSO presents a total of 46,403% of cannabinoids between THC-A, THC, CBD-A, and CBD.
Figure 1.
Cannabinoid concentration in the extract analyzed by the Terpeno Analytics laboratory. Δ-9 Tetrahidrocannabinol (THC) represents 9.45% of the total weight of the resine and Δ-9 Tetrahidrocannabinol (THC-A) 1.927%, giving a THC potential of 11.141%. Cannabidiol (CBD-A) represents 24.649%, and Cannabidiol (CBD) 10.376%, giving a CBD potential of 31.993%. Cannabinol (CBN) is not detected. In total, this RSO presents a total of 46,403% of cannabinoids between THC-A, THC, CBD-A, and CBD.
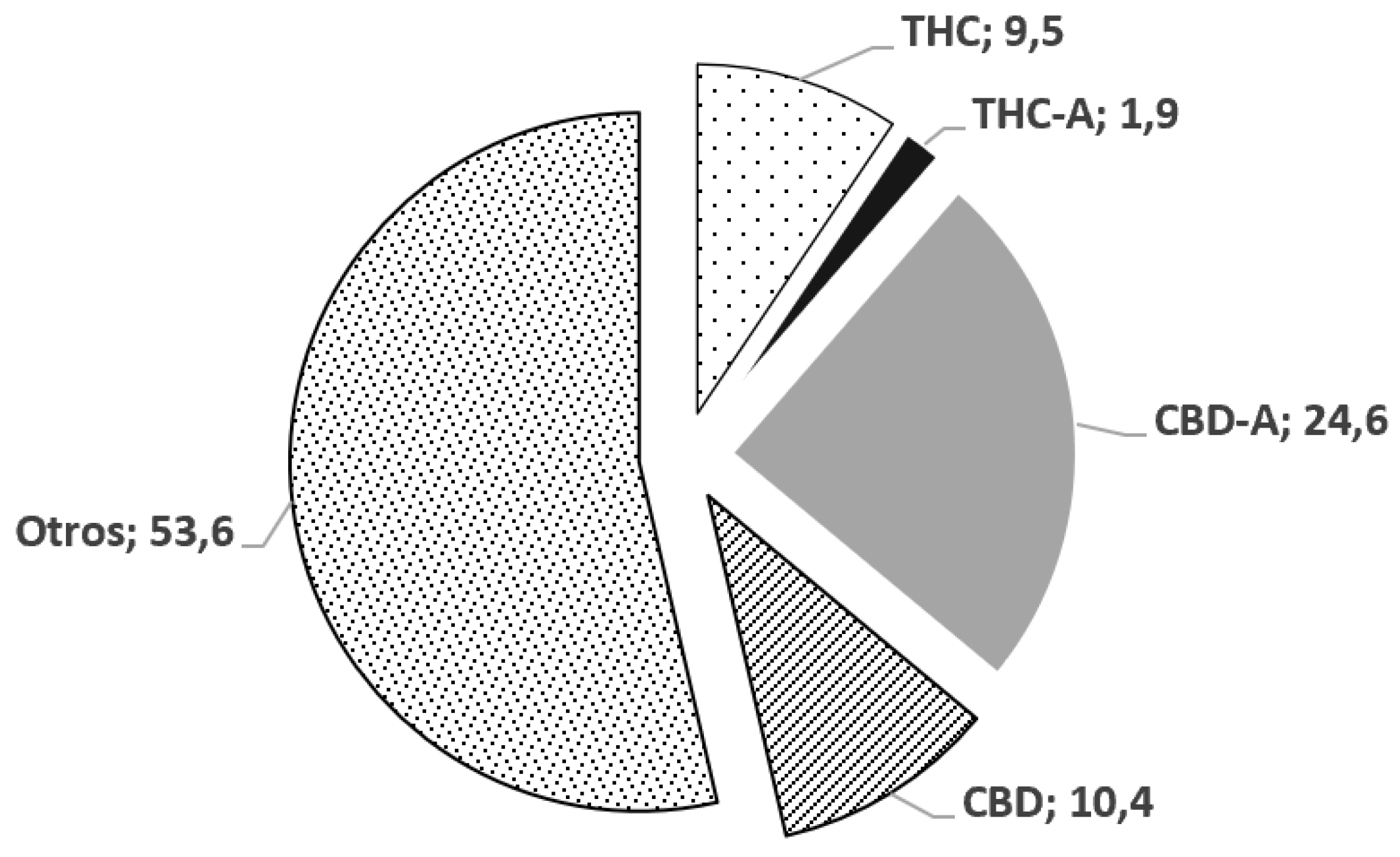
Figure 2.
Pain levels over time, based on treatment. One-way ANOVA (t0, p=0.999; t4, p=0.816; t8, p=0.265; t12, p=0.284; t16, p=0.276; t20, p=0.099; t24, p=0.053; t28, p=0.024).
Figure 2.
Pain levels over time, based on treatment. One-way ANOVA (t0, p=0.999; t4, p=0.816; t8, p=0.265; t12, p=0.284; t16, p=0.276; t20, p=0.099; t24, p=0.053; t28, p=0.024).
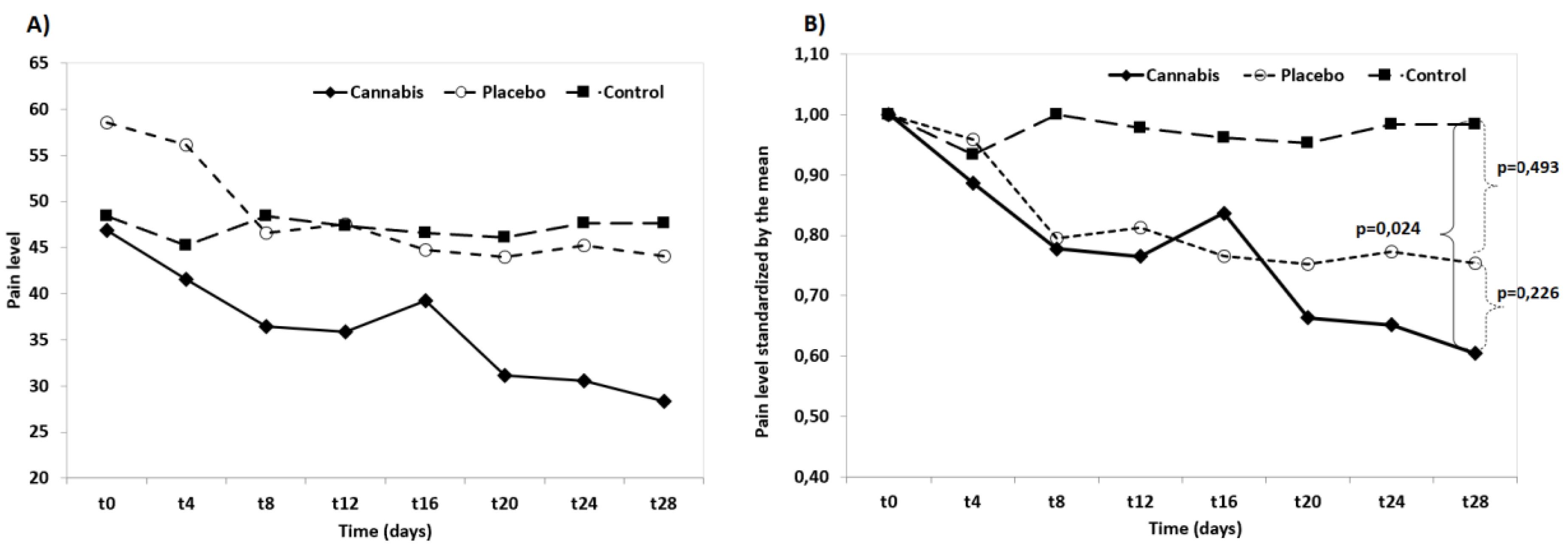
Figure 3.
Pain levels in week 1 and after 7 days. T-test (paired data). Cannabis, p=0.255, Placebo, p=0.150, Control, p=0.285).
Figure 3.
Pain levels in week 1 and after 7 days. T-test (paired data). Cannabis, p=0.255, Placebo, p=0.150, Control, p=0.285).
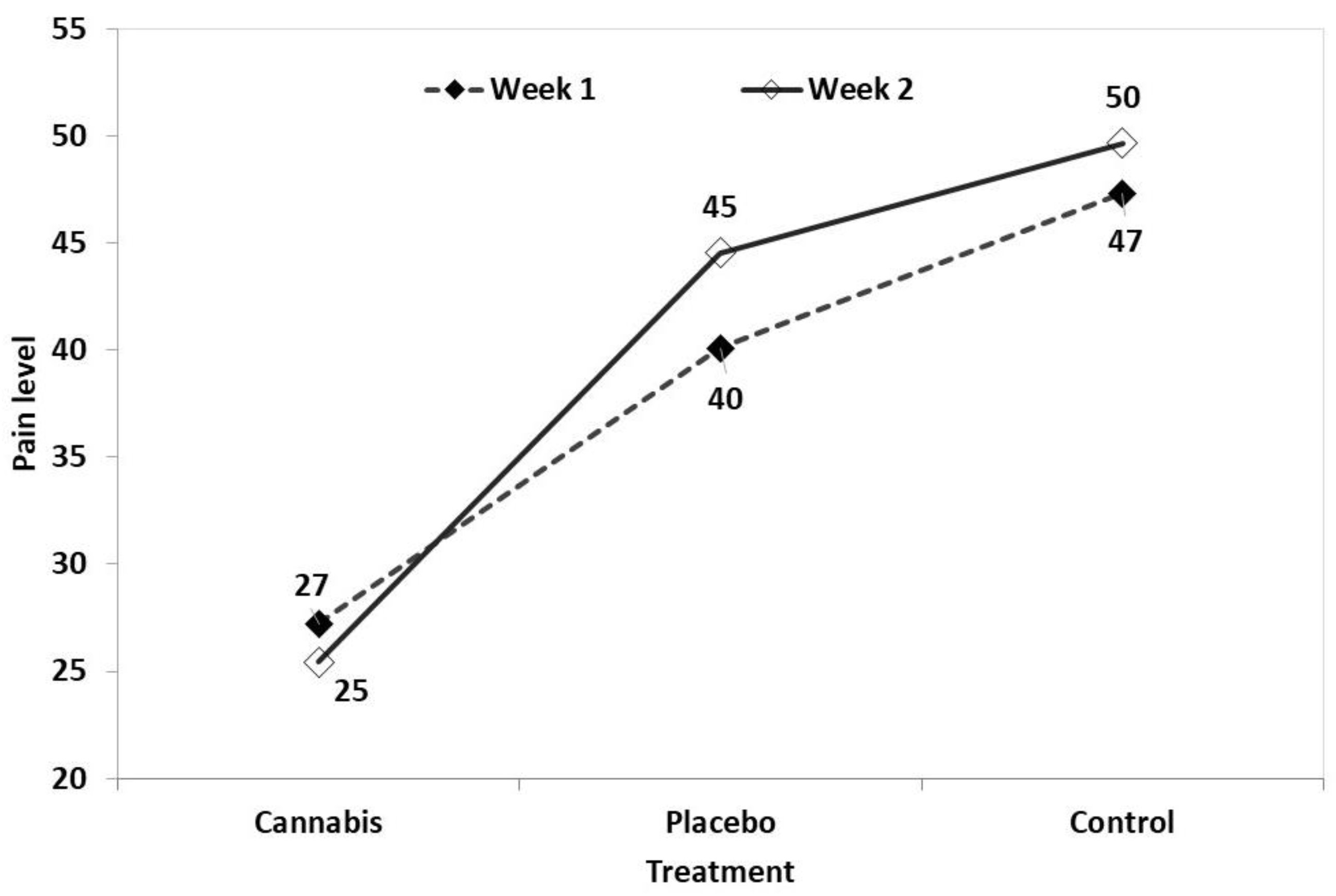
Figure 4.
Number of patients according to COAST level, before and after treatment. Cannabis group.
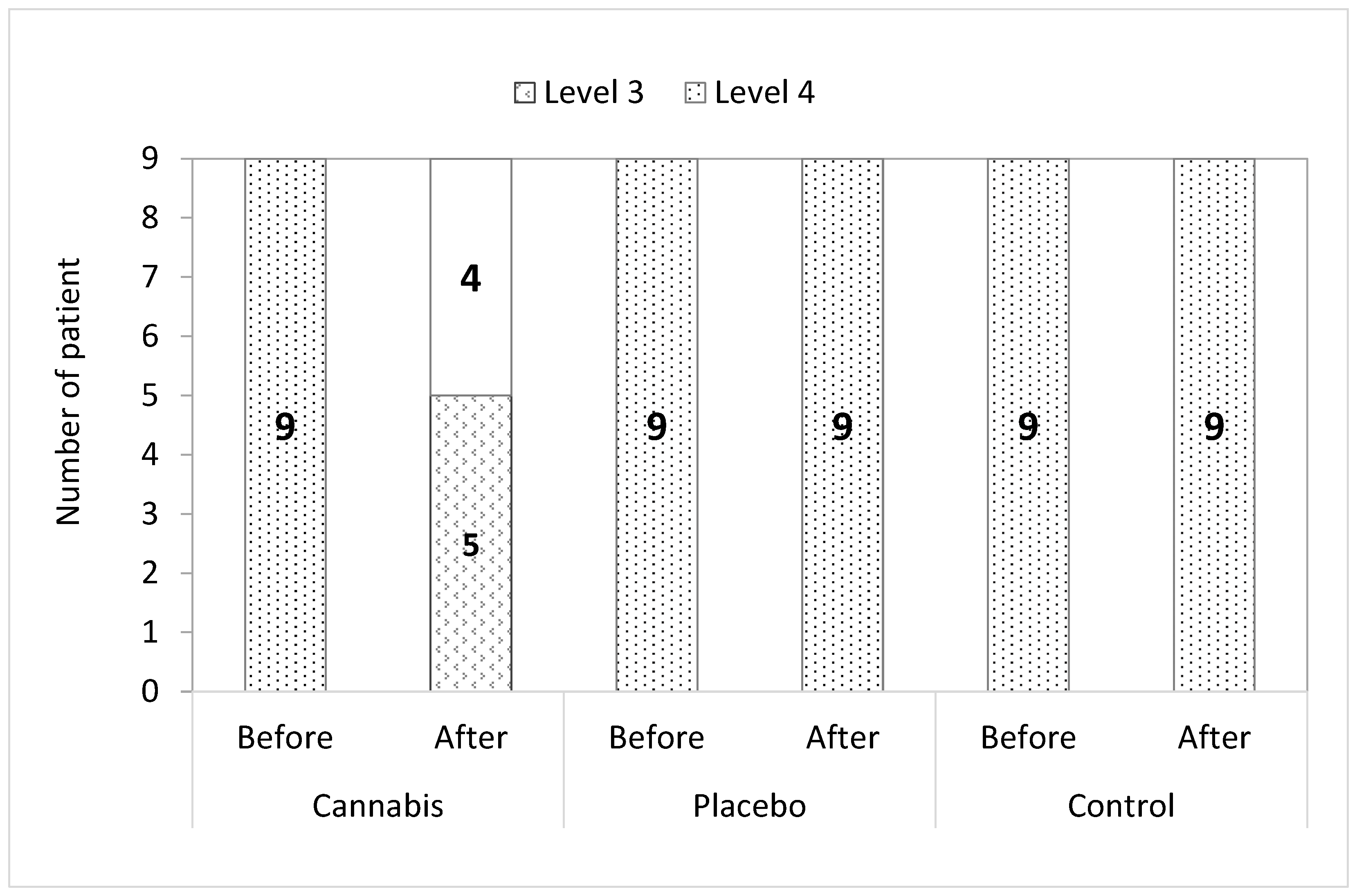

Table 1.
Results of CBPI monitoring of the sampled canines during the study periods and CBPI with Maximum Tolerated Dose (DMT) at week 1 and week 2.
Table 1.
Results of CBPI monitoring of the sampled canines during the study periods and CBPI with Maximum Tolerated Dose (DMT) at week 1 and week 2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



