Submitted:
23 July 2025
Posted:
24 July 2025
You are already at the latest version
Abstract
Background. The dual-faced nature of some botanicals, which are used both as pharmaceuticals and dietary supplements for nutritional purposes, can lead to inconsistencies and contradictory outcomes from Food and Drug regulatory authorities in various countries.
Aims. This overview aimed to identify the sources of inconsistencies in the assessment of evidence, ensure the safety, efficacy, and quality of botanicals, and propose potential solutions to address the issues, particularly in the field of multi-component botanicals, e.g., adaptogens used in prevention and treatment of complex etiology, stress-induced, and aging-related disorders.
Overview. This review is focused on: (i) - the differences between the requirements for the quality of pharmaceuticals and dietary supplements of botanical origin, (ii) - progress, trends, pitfalls, and challenges in the adaptogens research, (iii) - Inadequate assignment of some plants to adaptogens, or insufficient scientific data in case of Eurycoma longifolia, (iv) - inconsistencies in botanical risk assessments in the case of Withania somnifera.
Proposed solutions include: (i)- establish internationally harmonized guidelines for eval-uating botanicals based on their intended use (e.g., pharmaceutical vs. dietary Supple-ment), incorporating traditional use data alongside modern scientific methods, (ii)- en-courage peer review and transparency in national assessments by mandating public dis-closure of methodologies, data sources, and expert affiliations, (iii) - create a tiered evi-dence framework that allows differentiated standards of proof for traditional botanical supplements versus pharmaceutical candidates, (iv)- promote international scientific dia-logues among regulators, researchers, and industry to develop consensus positions and avoid unilateral bans that may lack scientific rigor.
Conclusions. Harmonized standards, transparent methodologies, and a balanced, evidence-informed approach are necessary to ensure consumers receive effective and safe botanicals.
Keywords:
botanicals
; dietary supplements
; pharmaceuticals
; adaptogens
; network pharmacology
; food and drug regulation
1. Introduction
Botanical substances occupy a unique and complex position at the intersection of food and pharmaceutical regulation. Their dual-faced nature—as both traditional medicines and modern dietary supplements—creates regulatory ambiguity, particularly in the evaluation of safety, efficacy, and quality across different jurisdictions. This ambiguity can lead to inconsistencies in risk assessments and contradictory outcomes among food and drug regulatory authorities globally [1,2,3,4,5].
The dual-faced nature of some Botanicals used as pharmaceuticals and dietary supplements for
Nutrition can lead to inconsistencies and contradictory outcomes from Food and Drug regulatory authorities in various countries. As a result, they can raise conflicts of interest between the pharmaceutical and food industry and the Food and Drug regulatory authorities. This overview aims to identify the sources of inconsistencies in the assessment of evidence, ensure the safety, efficacy, and quality of botanicals, and propose potential solutions to address the issues, particularly in the field of multi-component Botanicals and Botanical Herbal Products dealing predominantly with complex etiology, e.g. stress-induced and aging related disorders and diseases.
Figure 1.
Janus' statue and his two faces: past and future. In Greek mythology, Janus (January) is a god of time and duality, depicted as having two contrasting, duplicitous faces.
Figure 1.
Janus' statue and his two faces: past and future. In Greek mythology, Janus (January) is a god of time and duality, depicted as having two contrasting, duplicitous faces.

2. Pharmaceuticals vs Nutraceuticals and Dietary Supplements
2.1. What Are the Differences Between the Requirements for the Quality of Pharmaceuticals and Dietary Supplements of Botanical Origin?
The requirements for pharmaceuticals and dietary supplements of botanical origin differ significantly in terms of regulatory oversight, quality standards, safety and efficacy requirements, and manufacturing practices (Table 1). Table 2 shows the key differences in the requirements for botanical-origin pharmaceuticals and dietary supplements under FDA (United States) vs. EMA (European Union) regulations. Table 3 includes selected true adaptogens with Pharmacopeial Recognition and some putative adaptogens, such as Eurycoma and Sideritis, which were claimed as adaptogens in publications [6,7,8,9,10,11,12,13,14,15].
The daily dose of a dietary supplement versus a herbal medicine containing the same active ingredient can differ significantly due to regulatory, intended use, and formulation factors.
2.2. Regulatory Classification, Purpose of Use, Dose and Potency, Labeling and Claims
Even if the active ingredient is identical, herbal medicines generally have higher, standardized, and therapeutically justified doses. In contrast, dietary supplements offer lower doses for general wellness and are not intended to treat diseases.
3. Progress, Trends, Pitfalls, and Challenges in the Adaptogens Research
Adaptogens are botanicals that enhance adaptability, resilience, resistance, and survival in response to stress-induced and aging-related disorders [16,17].
The term adaptogen is derived from adaptation [8], which is coined for the physiological process of adaptation of the organism to repeated action of the botanical that triggers adaptive stress response via intracellular and extracellular adaptive signaling pathways and networks in neuroendocrine-immune, cardiovascular, and gastrointestinal systems and resulting in increased adaptability, resilience, resistance, and survival in stress-induced and aging-related disorders [16,17,19].
Adaptogens play a similar role in defending the plant against environmental challenges, including viruses, harmful bacteria, insect-borne diseases, excessive UV rays, and the physiological ravages of chronic stress [19].
Figure 2.
George Canguilhem introduced the term adaptability in 1943, who defined adaptability as the ability of an organism to alter itself or its responses to the changed environment or circumstances and assumed that adaptability shows the ability to learn and improve from experience—repeated mild exposure or low doses of stress result in the increased resistance of cells and organisms to subsequent stress exposure, resulting in an adaptation that favors survival [18].
Figure 2.
George Canguilhem introduced the term adaptability in 1943, who defined adaptability as the ability of an organism to alter itself or its responses to the changed environment or circumstances and assumed that adaptability shows the ability to learn and improve from experience—repeated mild exposure or low doses of stress result in the increased resistance of cells and organisms to subsequent stress exposure, resulting in an adaptation that favors survival [18].
3.1. Adaptogens Are Stress Protectors
Adaptogens exhibit stress-protective and tonic effects after repeated dose administration, triggering adaptive stress response signaling pathways and mediating gene expression in the HPA axis and other body tissues [20,21,22,23,24,25,26,27]. The stress-protective effect achieved by multiple administrations of adaptogens is not the result of inhibiting the stress response of an organism but rather of adaptive changes in the organism in response to the repeated stress-agonistic effect of the drug. In other words, using pharmacological terminology, adaptogens are mild stress-agonists and not stress-antagonists [21].
3.2. Adaptogens Are Stimulants
A characteristic feature of adaptogens is that they act as eustressors or challengers [9]. Thus, a single administration of an adaptogen primarily produces a challenging (stimulating or stress-agonizing) effect, a fact that is utilized in sports medicine, where a single dose of adaptogen can enhance athletes' performance by making them more alert [22,23,24,25,26,27].
The stimulating effects of a single dose of adaptogens are primarily due to interactions within the central nervous system (CNS) and hypothalamic-pituitary-adrenal (HPA) axis but do not require prolonged processes such as gene and protein expression, neurogenesis, cell proliferation, and differentiation [19,20,21,22,23,24,25,26,27].
3.3. What Is Necessary and Sufficient to Be Classified as an Adaptogenic Plant?
Pharmacologic assessment of adaptogenic activity is commonly used in various animal stress tests involving exposure to cold, heat, altered atmospheric pressure and oxygen content, radiation, toxic substances, starvation, fear, and chronic diseases have shown that the most essential feature of adaptogens is an ability to increase resistance to both physical and emotional stress [22].
The most suitable pharmacological methods for assessing adaptogenic activity are chronic unpredictable stress (CUS) animal models, which induce affective behaviors in C57BL/6J mice and, once established, measure stress-related alterations in the intrinsic excitability and synaptic regulation of the medial prefrontal cortex layer 5/6 pyramidal neurons. Adult male mice received 2 weeks of 'less intense' stress or 2 or 4 weeks of 'more intense' CUS, followed by assessment of sucrose preference for anhedonia and the elevated plus maze for anxiety. They forced a swim test for evaluation of depressive-like behaviors. An intense CUS exposure results in increased anhedonia, anxiety, and depressive behaviors, while less intense stress results in no measured behavioral phenotypes. D1-and D2-PYR subpopulations differentially undergo stress-induced intrinsic and synaptic plasticity that may have functional implications for stress-related pathology, and that these adaptations may reflect unique differences in basal properties regulating output of these cells [28]
It is also necessary to trigger an adaptive stress response, activating adaptive signaling pathways, e.g., G-protein coupled (GPCR), tyrosine, toll-like receptors, and I3PK-mediated pathways that are known to promote survival in response to stress, suggesting neuroprotective activity and potential benefits of adaptogens in neurodegenerative diseases [19,29].
In addition to activating multiple cytoprotective mechanisms that increase cell survival (antioxidant, immune modulation, Hsp70 modulation [16]), adaptogens trigger the generation of hormones (e.g., corticotropin, cortisol, gonadotropin-releasing hormones, urocortin, melatonin [28]), neuropeptide N [27], and neurohormones, and neurotransmitters playing a key role in metabolic regulation and homeostasis [19], Figure 3 and Figure 4.
As a result, adaptogens are active in numerous conditions and diseases associated with stress and aging-related impairments of the neuroendocrine-immune complex, as well as energy and fatigue [30].
3.4. Progress and Trends in Adaptogens Research
Adaptogens are characterized as botanicals with polyvalent action and pleiotropic activity, often referred to as a "Ginseng-like panacea for all diseases [30]." Progress in biomedical science, particularly in network pharmacology, metabolomics, proteomics, transcriptomics, genomics, and microbiomics — collectively known as omics — and systems biology, has significantly contributed to uncovering the mechanisms of action of adaptogens and enhancing our understanding of their effects [19,29,30,31,32].
Network pharmacology is an emerging discipline that integrates systems biology, bioinformatics, and pharmacology to understand the actions of drugs on a systemic, network level. Instead of the traditional "one drug–one target" model, network pharmacology adopts the "multitarget, multi-component" paradigm, which is particularly useful for complex diseases and multi-herbal medicines [19,29,30,31,32]—Table 4.
Network pharmacology offers a robust systems-level framework for understanding drug mechanisms, especially in complex, multitarget conditions. While it introduces a more realistic model of pharmacological action, it must overcome limitations like data incompleteness, lack of dynamism, and validation gaps. For mechanistic insights, it should ideally be integrated with experimental biology and temporal models to achieve both predictive power and clinical relevance [32].
The advancement of integrative omics network pharmacology and artificial intelligence in natural products has opened new avenues for the following areas:
- elucidation of the mechanisms of action of medicinal plants,
- understanding the synergistic therapeutic actions of complex bioactive components in medicinal plants,
- providing a rationale for traditional Chinese medicine, enhancing the quality,
- of TCM drug research, and the speed and efficiency of developing new TCM products,
- discovering and developing new botanical hybrid combinations,
Unlike conventional medicines, botanical adaptogens consist of multi-component active compounds and phytochemicals, whose interactions lead to novel and unexpected pharmacological activities due to their synergistic and antagonistic effects [29,30,31,32,33]. Similarly, the pharmacological activity of a combination of several plants or herbal extracts, such as those in botanical hybrid preparations (e.g., TCM formulas), results in a new biologically active substance with unique pharmacological characteristics [31].
3.5. Pitfalls in Adaptogen Research: Inadequate Assignment of Some Plants to Adaptogens or Insufficient Scientific Data
Polyvalence of some medicinal plants often leads to unsupported claims that they are adaptogens, as is the case with Eurycoma longifolia. While it's recognized in traditional medicine across Southeast Asia and regulated in markets like the EU, the official pharmacopeial status appears to be limited to three countries: Malaysia, Indonesia, and Vietnam. Several publications claim that Eurycoma longifolia Jack is an adaptogen [34,35,36,37,38,39,40]. However, there is no scientific evidence supporting these statements. The authors refer to:
However, that is not a sufficient characteristic criterion to classify Eurycoma as an adaptogen. See the definition and characteristics of adaptogens in the Amendment below.
Furthermore, the quality of clinical trials in humans, preclinical studies in animals, and in vitro studies is not satisfactory, making it difficult to draw robust conclusions on the efficacy and safety of Eurocoma products.
E.g., Talbott et al., 2013 [37] state that:
- Active compounds of Eurycoma are 4300 dalton glycopeptides consisting of 36 amino acids.
"Eurycoma contains a group of small peptides referred to as "eurypeptides" with 4300 dalton glycopeptides 36 amino acids that are known to have effects in improving energy status and sex drive in studies of rodents. Animal studies have shown that many of the effects of the extract are mediated by its glycoprotein components. Typical dosage recommendations, based on traditional use and on the available scientific evidence in humans, including dieters and athletes, call for 50-200 mg/day of a water-extracted tongkat ali root standardized to 22% eurypeptides.”
However, the publication does not contain any information about the analytical methods used for quantification, accuracy, precision, selectivity, or purity of the analytical markers, which are essential for ensuring reproducible quality and efficacy. There is nothing in that study [27] about numerous biological active plant secondary metabolites isolated from E. longifolia various extracts e.g., quassinoids eurycomanone, 13α(21)-epoxyeurycomanone, 13,21-dihydroeurycomanone, 14,15 β -dihydroxy-klaineanone, longilactone and eurycomalacton, 9-methoxycanthin-6-one; Laurycolactone; Eurycolactone B; Eurycomalide A; Eurylactone; Longilactone; Eurycomalactone; Eurycomanone; Eurycomanol; Pasakbumin B; Hydroxyklaineanone; Biphenyl-neolignan; Quassin etc., which are known as poorly water-soluble compounds [41,42,47,48,49,50].
- According to the authors Talbott et al., 2013 [37] , the mechanism of action is related to "the bioactive complex 4300 dalton glycopeptides ("eurypeptides" with 36 amino acids) has been shown to activate the CYP17 enzyme (17 alphahydroxylase and 17,20 lyase) to enhance the metabolism of pregnenolone and progesterone to yield more DHEA (dehydroepiandrosterone) and androstenedione, respectively [40]. This glycoprotein water-soluble extract of Eurycoma longifolia has been shown to deliver anti-aging and antistress benefits subsequent to its testosterone balancing effects".
The effects of tongkat ali in restoring normal testosterone levels appears to be less due to actually "stimulating" testosterone synthesis, but rather by increasing the release rate of "free" testosterone from its binding hormone, sex-hormone-binding-globulin (SHBG).
In this way, eurycoma may be considered not so much a testosterone "booster" (such as an anabolic steroid), but rather a "maintainer" of normal testosterone levels and a "restorer" of normal testosterone levels (from "low" back "up" to normal ranges). This would make eurycoma particularly beneficial for individuals with sub-normal testosterone levels, including those who are dieting for weight loss, middle-aged individuals suffering with fatigue or depression, and intensely training athletes who may be at risk for overtraining."
That is not related to the known mechanisms of action of adaptogens on the neuroendocrine-immune complex; see Amendment below.
Furthermore, the results of a clinical study of Eurycoma longifolia (Physta®) water extract plus multivitamins show a lack of activity when Eurycoma longifolia (Physta®) was compared with placebo [36]: Results: "there were no significant between-group differences, within-group improvements were observed in the SF-12 QoL, POMS and MMSQ domains", which is associated with CNS activity of Eurycoma longifolia (Physta®) water extract plus multivitamins on quality of life, mood and stress".
This clearly shows a lack of effect Eurycoma longifolia (Physta®) on the CNS, suggesting that Eurycoma is not an adaptogen.
There are many shortcomings in conducted randomized, placebo-controlled, double-blind clinical trials, which are not in line with CONSORT recommendations [35,36,38,39,45,46,47,51], including insufficient information regarding:
- Insufficient description of the study medication (see above),
- Randomization (a method used to generate the random allocation sequence, including details of restriction)
- Implementation (who generated the allocation sequence, enrolled participants, assigned participants to their groups, etc.)
- Blinding (preparation had the same appearance, test, and odor as placebo; how care providers, those assessing outcomes, were blinded; how the success of blinding was evaluated)
- Allocation concealment (the mechanism used to implement the random allocation sequence, such as sequentially numbered containers, describing any steps taken to conceal the sequence until interventions were assigned; it is not clear whether the sequence was concealed until interventions were assigned),
- Procedure for treatment compliance (how measurements of compliance of individual patients with the treatment regimen under study were documented).
- Monitoring,
- Settings and locations where the data were collected,
- Quality assurance and quality control,
- Deviations from the protocol
- Selective reporting
- The trial was conducted per ICH guidelines for GCP.
- Voucher specimen (i.e., retention sample was retained and, if so, where it is kept or deposited).
- The role of the study sponsor/funder,
- Inappropriate statistical tools and statistical analysis (e.g., lack of between-groups comparison of changes from the baseline by two-way ANOVA, etc.).
Other limitations of the studies, e.g., Muniandy et al. 2023, [51]:
- ⇒
- a purposive sampling in a randomized, double-blinded, placebo-controlled, parallel-group study.
- ⇒
- lost to follow-up and missing data points
- ⇒
- the lack of nutritional intake information, which can be a limitation for a comprehensive analysis of the potential influence of dietary factors on the observed outcomes.
Overall, there is no convincing evidence yet to support the claim that Eurocoma is an adaptogen.
3.6. Dual-Use Dilemma and Inconsistencies in Botanical Risk Assessments in the Case of Withania Somnifera
Below is an insight into the Two Sides of the same coin and Double Standards in the assessment of Botanical safety, efficacy, and quality, with a case study of Ashwagandha [1,2,3,4,5,52,53,54,55,56,57,58,59,60,61,62].
Ashwagandha (Withania somnifera (L.) Dunal is the most popular plant in India. It has been used in the traditional medical system (Ayurveda) to treat many diseases and health conditions for thousands of years. Due to its polyvalent pharmacological activity, it is also known as Indian Ginseng [63,64,65,66].
Ashwagandha (Withania somnifera) is recognized in several national pharmacopoeias and regulatory frameworks worldwide, though its status varies by country, including:
- In India, Withania somnifera is officially included in the Indian Herbal Pharmacopeia [54]. The monograph outlines:
- o
- the plant names
- o
- geographical distribution
- o
- macroscopic and microscopic description of the roots,
- o
- chemical constituents - steroidal lactones including withanone, withaferin A, withanolides I, II, III, A, D, E, F, G, H, I, J, K, L, M, WS-L, P, and S, withasomnidienone, withanolide C, and alkaloids viz., cuscohygrine, anahygrine, tropine, pseudotropine, anaferine, isopellatierine, 3-tropyltigloate,
- o
- Assays/analytical methods including HPLC conditions fingerprints, identifying withaferin A in extracts and withanolide J in vitro culture,
- o
- quantitative standards (including total alkaloids (in total about0,2%),
- o
- adulteration,
- o
- pharmacology section,
- o
- reported activities including antistress, immunomodulatory, anticancer, antioxidant, anticonvulsive, anthelminthic, antiarthritic, chemopreventive, antibacterial, cardioprotective, antidepressant, antitoxic, hypoglycemic, diuretic, hypercholesterolemic, immunosuppressive, antiradical, and adaptogenic activities,
- o
- Therapeutic category: Adaptogen.
- In China, Ashwagandha is regulated under traditional Chinese medicine standards. Quality control measures are in place for the selection of raw materials, extraction processes, and product testing to ensure the safety and efficacy of the final product.
- In the U.S., Ashwagandha is permitted as a dietary supplement. The United States Pharmacopeia (USP) provides guidelines for its quality control, including High-Performance Liquid Chromatography (HPLC) methods to assess total withanolide content.
- Ashwagandha is allowed as a food supplement in the UK. The Medicines and Healthcare Products Regulatory Agency (MHRA) has approved clinical trials involving Ashwagandha, indicating its acceptance within certain regulatory frameworks.
- Ashwagandha is included in the Australian Register of Therapeutic Goods (ARTG), with over 320 listed medicines containing it, reflecting its acceptance in therapeutic products.
- In France, Ashwagandha root is classified under List B of medicinal plants, indicating that its potential adverse effects may outweigh its therapeutic benefits. This classification restricts its use in medicinal preparations.
- Ashwagandha is available as a dietary supplement in Germany. However, the Federal Institute for Risk Assessment (BfR) has recommended its inclusion in the EU's list of substances for which safety has not been conclusively established, suggesting caution in its use.
- Poland permits the use of Ashwagandha root but restricts the use of other parts of the plant. Additionally, the daily intake of withanolides is limited to less than 10 mg, reflecting a cautious approach to its consumption.
- In Sweden, the regulation of Ashwagandha is decentralized, allowing local authorities to make decisions regarding its use. This approach permits its availability under certain conditions.
- Within the Association of Southeast Asian Nations (ASEAN), Ashwagandha is not uniformly included in national pharmacopeias. However, efforts are underway to harmonize traditional medicine regulations across member states. The ASEAN Common Technical Document (ACTD) framework is being utilized to standardize quality, safety, and efficacy requirements for herbal products, such as Ashwagandha [2].
In summary, the incorporation of Ashwagandha into national pharmacopeias and its regulatory acceptance vary globally. While countries like India, the United States, and Australia have established standards or included it in official registers, others, such as France and Denmark, approach it with caution or restrictions. Ongoing efforts, particularly within ASEAN, aim to harmonize regulations for traditional herbal medicines, which could potentially influence Ashwagandha's status in the future.
Such a contradictory response to the regulatory requirements of the same plant products and their use in medicine is not surprising due to many objective and subjective reasons, including:
A recent case in point is the Danish Technical University (DTU) Food Institute's risk assessments of Withania somnifera (Ashwagandha) root [4,5]. These reports, which contributed to national-level restrictions and influenced regulatory positions in other countries, have been widely criticized by scientific and regulatory communities for methodological shortcomings and lack of transparency [1,52].
3.7. Key Issues Identified
- Blurring of Pharmacological and Nutritional Frameworks
Withania somnifera is traditionally consumed as a root extract in dietary supplements to support stress management, sleep, and hormonal balance. However, the DTU assessments failed to distinguish between its pharmacological and nutritional uses, applying pharmaceutical-level toxicological expectations to a botanical widely regarded as safe under traditional and evidence-based guidelines.
- 2.
- Inappropriate Aggregation of Data from Different Plant Parts
A core flaw in the DTU evaluations is the failure to differentiate between root, leaf, stem, and berry extracts, despite well-established phytochemical and pharmacological differences. This has led to the erroneous attribution of adverse effects (e.g., cytotoxicity from withaferin A, primarily found in leaves) to root-based products, undermining the validity of the conclusions.
- 3.
- Selective and Outdated Use of Scientific Literature
Although hundreds of clinical and toxicological studies on Ashwagandha have been published in the past decade, many of which demonstrate a favorable safety profile, the DTU assessments relied heavily on older and animal-based data, some of which lacked relevance to human use. Peer-reviewed safety evaluations, including those by the American Herbal Products Association (AHPA), were omitted.
- 4.
- Absence of Peer Review and Transparency
Neither of the DTU reports underwent external peer review. Key methodological details—such as criteria for evidence inclusion, levels of uncertainty, and expert qualifications—were not disclosed, raising concerns about the objectivity and reproducibility of the findings.
- 5.
- Regulatory Disparity and Industry Impact
Discrepant evaluations of the same botanical substance by different national authorities—some viewing Ashwagandha as a safe food supplement, others banning it outright—have generated regulatory friction and potential trade barriers. This inconsistency particularly disadvantages producers in countries like India, where the plant has been used safely for centuries.
3.8. Critical Assessment of Common Technical Documentation Submitted by Drug Manufacturers to Drug Authorities
On the other side, the rejections to grant 'well-established use' of some herbal medicines are often based on assessment reports of drug authorities (e.g., HMPC. EMA/HMPC/24186/2023 [67]), which identified serious problems such as:
- The published clinical trials exhibit considerable deficiencies in their quality and show methodological problems.
- o
- insufficiently characterized herbal preparations,
- o
- open (label) studies,
- o
- small sample size,
- o
- missing ITT analysis, regardless of a detailed description of dropouts and reasons for exclusion in the analysis of an outcome measure,
- o
- healthy subjects,
- o
- The efficacy score has not been validated
- o
- The results from trials on clinical pharmacology are contradictory.
- o
- There is a lack of independent replications of the single different studies.
Possible sources of inconsistency of the results of various clinical studies of Rhodiola rosea L., rhizoma et radix [68] are due to the authors' not adhering to CONSORT regarding the quality of the herbal interventions, which was not adequately characterized in respect of:
- extraction solvents and dry herb: dry native Extract Ratio (DER),
- The content of active markers, providing HPLC fingerprints to ensure consistent quality and reproducible pharmacological activity.
- The analytical methods were not validated for selectivity, accuracy, and precision.
- The authors declared that placebo capsules containing microcrystalline cellulose and silicon dioxide had the same appearance, odor, and taste as the R. rosea product, which is very unlikely due to their strong specific rose odor, test, and color, particularly when "participants were asked to self-determine their need for one additional capsule (i.e., a half dose), to be taken within four hours of the initial dose.
- The authors have not reported (or not assessed) the results of treatment compliance (counting of unused tablets), and that is a serious flaw.
- All outcome measures of the study were subjective based on self-assessment questionnaires of QOL in 48 nurses instead of the only doctor having the same unified "standard."
The imbalance between the Rhodiola treatment and placebo groups in medication use and physical and emotional health problems has had a significant impact on the results of the study [68].
3.9. Other Challenges in Adaptogens Research
It should be noted that some other challenges in adaptogens research are related to the insufficient characterization and standardization of certain active constituents, including the pyrazole alkaloid withasomnine [69,70,71], found in Withania root preparations, which is known for its sedative properties. New studies are required to demonstrate the reproducibility of well-characterized Ashwagandha-containing products.
3.10. Proposed Solutions
- Establish Internationally Harmonized Guidelines for evaluating botanicals based on their intended use (e.g., pharmaceutical vs. dietary Supplement), incorporating traditional use data alongside modern scientific methods.
- Encourage Peer Review and Transparency in national assessments by mandating public disclosure of methodologies, data sources, and expert affiliations.
- Create a Tiered Evidence Framework that allows differentiated standards of proof for traditional botanical supplements versus pharmaceutical candidates.
- Promote International Scientific Dialogues among regulators, researchers, and industry to develop consensus positions and avoid unilateral bans that may lack scientific rigor.
4. Conclusion
The inconsistencies in risk assessments of Withania somnifera underscore the broader challenge of regulating botanicals that straddle the food-pharma boundary. Without harmonized standards and transparent methodologies, regulatory decisions risk being unscientific, protectionist, or influenced by conflicts of interest. A more balanced, evidence-informed approach is urgently needed to protect consumer safety without stifling access to beneficial botanicals.
Author Contributions
Conceptualization, A.P. and T.L.; writing—preparation of original drafts, A.P.; writing—review and editing, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
The authors received no administrative and technical support or donations.
Conflicts of Interest
Alexander Panossian is self-employed at the research and development company Phytomed AB and has no shares or financial interest in any pharmaceutical company. The authors, Alexander Panossian , supported various projects without funding but received funding in previous years to develop herbal medical products from EuropharmaUSA Inc., Green Bay, Wisconsin, USA. The author AP declared that they were editorial board members of Pharmaceuticals at the time of submission. This had no impact on the peer review process and the final decision. The author Terrence Lemerond founded EuropharmaUSA Inc., a company producing herbal dietary supplements. The company had no role in the writing of the manuscript. Both authors, AP, and TL, declare that the research was conducted without any commercial or financial relationships that could potentially create a conflict of interest.
References
- Patwardhan, B.; Chaturvedi, S.; Tillu, G.; Deshpande, S.; Hegde, B. M. Danish ban on Ashwagandha: Truth, evidence, ethics, and regulations. Journal of Ayurveda and integrative medicine 2024, 15, 101028. [Google Scholar] [CrossRef] [PubMed]
- Ramadoss, M.S.K.; Koumaravelou, K. Regulatory Requirement Sufficiency for Registration of Traditional Herbal Medicine-Based Products in Association of Southeast Asian Nations Regions: A Model Study with Ashwagandha Tablets. https://www.ijpsonline.com/articles/regulatory-requirement-sufficiency-for-registration-of-traditionalherbal- medicine-based-products-in-association-of-southeast-asia-4579.html. Indian J Pharm Sci, 2022; 84, 501–512. [Google Scholar]
- Ministry of Ayush, Government of India, New Delhi. Safety of Ashwagandha. (Withania somnifera). Report of the Expert Committee constituted by Ministry of Ayush Govt. of India. Central Council for Research in Ayuredic Sciences, Ministry of Ayush, Government of India, New Delhi, 2020, 1-70. www.ccras.nic.
- Danish Technical University (DTU) Food Institute's risk assessments of Withania somnifera (Ashwagandha) root (DTU DOCX No. 19/1030299, 2020.
- Danish Technical University (DTU) Food Institute's risk assessments of Withania somnifera (Ashwagandha) root DTU DOCX 25/100205, 2025).
- EMA/HMPC/24186/2023. Final assessment report on Rhodiola rosea L., rhizoma et radix - Revision 1. Committee on Herbal Medicinal Products (HMPC). 21/05/2024; https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-rhodiola-rosea-l-rhizoma-et-radix-revision-1_en.
- EMA/HMPC/27745/2023. Final assessment report on Panax ginseng C.A.Mey., radix - Revision 1. Committee on Herbal Medicinal Products (HMPC). 12/07/2024. https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-panax-ginseng-camey-radix-revision-1_en.pdf. (accessed on 22 July 2025).
- EMA/HMPC/681519/2012. Final public statement on Withania somnifera (L.) Dunal, radix - First version. Herbal Medicinal Products (HMPC). 03/09/2013; https://www.ema.europa.eu/en/documents/public-statement/final-public-statement-withania-somnifera-l-dunal-radix-first-version_en.
- EMA/HMPC/680615/2013.Final assessment report on Eleutherococcus senticosus (Rupr. et Maxim.) Maxim., radix. Committee on Herbal Medicinal Products (HMPC). 06/10/2014 https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-eleutherococcus-senticosus-rupr-et-maxim-maxim-radix_en.
- EMA/HMPC/39455/2015. Final assessment report on Sideritis scardica Griseb.; Sideritis clandestina (Bory & Chaub.) Hayek; Sideritis raeseri Boiss. & Heldr.; Sideritis syriaca L., herba. Committee on Herbal Medicinal Products (HMPC). 28/10/2016; https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-sideritis-scardica-griseb-sideritis-clandestina-bory-chaub-hayek-sideritis-raeseri-boiss-heldr-sideritis-syriaca-l-herba_en.
- Ginseng Radix. In: WHO monographs on selected medicinal plants. World Health Organization, Geneva, Switzerland, 1999; 1:168-182.
- Radix Eleutherococci. In: WHO monographs on selected medicinal plants. World Health Organization, Geneva, Switzerland, 2002; 2: 83-96.
- Fructus Schisandrae. In: WHO monographs on selected medicinal plants. World Health Organization, Geneva, Switzerland, 2007; 3: 296-313.
- Radix Withaniae. In: WHO monographs on selected medicinal plants. World Health Organization, Geneva, Switzerland, 2009; 4: 373-391.
- National Pharmacopoeia Committee. Pharmacopoeia of the People’s Republic of China, English ed.; National Pharmacopoeia Committee: Beijing, China, 2010. [Google Scholar]
- Panossian, A. Understanding adaptogenic activity: specificity of the pharmacological action of adaptogens and other phytochemicals. Annals of the New York Academy of Sciences, 1401. [Google Scholar]
- Panossian, A. G. , Efferth, T., Shikov, A. N., Pozharitskaya, O. N., Kuchta, K., Mukherjee, P. K., Banerjee, S., Heinrich, M., Wu, W., Guo, D. A., & Wagner, H. (2021). Evolution of the adaptogenic concept from traditional use to medical systems: Pharmacology of stress- and aging-related diseases. Medicinal research reviews, 41(1), 630–703. [CrossRef]
- Canguilhem, G. Essai sur quelques problèmes concernant le normal et le pathologique. In The Normal and the Pathological; Fawcett, C.R., Cohen, R.S., Translators, *!!! REPLACE !!!*, Eds.; Zone Books: New York, NY, USA, 1991; Available online: https://www.undergroundbooks.net/pages/books/11553/georges-canguilhem-michel-foucault-intro/the-normal-and-the-pathological (accessed on 10 February 2025).
- Panossian, A.; Lemerond, T.; Efferth, T. Adaptogens in Long-Lasting Brain Fatigue: An Insight from Systems Biology and Network Pharmacology. Pharmaceuticals 2025, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- Wagner, H.; Nörr, H.; Winterhoff, H. Plant adaptogens. Phytomedicine 1994, 1, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A. , Wikman, G., & Wagner, H. (1999). Plant adaptogens. III. Earlier and more recent aspects and concepts on their mode of action. Phytomedicine : international journal of phytotherapy and phytopharmacology, 6(4), 287–300. [CrossRef]
- Panossian, A.G. Adaptogens: Tonic herbs for fatigue and stress. Altern. Compliment. Ther. 2003, 9, 327–332. [Google Scholar] [CrossRef]
- Panossian, A.; Wagner, H. Stimulating effect of adaptogens: an overview with particular reference to their efficacy following single dose administration. Phytother Res. 2005, 19, 819–838. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G. Pharmacology of Schisandra chinensis Bail.: An overview of Russian research and uses in medicine. J. Ethnopharmacol. 2008, 118, 183–212. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G.; Sarris, J. Rosenroot (Rhodiola rosea): Traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine 2010, 17, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G.; Kaur, P.; Asea, A. Adaptogens exert a stress-protective effect by modulation of expression of molecular chaperones. Phytomedicine 2009, 16, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G.; Kaur, P.; Asea, A. Adaptogens stimulate neuropeptide y and hsp72 expression and release in neuroglia cells. Front. Neurosci. 2012, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E. M. , Gomez, D., Caccamise, A., McPhail, D., & Hearing, M. (2019). Chronic unpredictable stress promotes cell-specific plasticity in prefrontal cortex D1 and D2 pyramidal neurons. Neurobiology of stress, 10, 100152. [CrossRef]
- Panossian, A. , Seo, E. J., & Efferth, T. (2018). Novel molecular mechanisms for the adaptogenic effects of herbal extracts on isolated brain cells using systems biology. Phytomedicine : international journal of phytotherapy and phytopharmacology, 50, 257–284. [CrossRef]
- Panossian, A. , & Efferth, T. (2022). Network Pharmacology of Adaptogens in the Assessment of Their Pleiotropic Therapeutic Activity. Pharmaceuticals (Basel, Switzerland), 15(9), 1051. [CrossRef]
- Panossian, A. , Lemerond, T., & Efferth, T. (2024). State-of-the-Art Review on Botanical Hybrid Preparations in Phytomedicine and Phytotherapy Research: Background and Perspectives. Pharmaceuticals (Basel, Switzerland), 17(4), 483. [CrossRef]
- Panossian, A. (2025). Trends and Pitfalls in the Progress of Network Pharmacology Research on Natural Products. Pharmaceuticals (Basel, Switzerland), 18(4), 538. [CrossRef]
- Panossian, A. (2023). Challenges in phytotherapy research. Frontiers in pharmacology, 14, 1199516. [CrossRef]
- Tambi, M. I. (2006). Eurycoma longifolia jack: a potent adaptogen in the form of water-soluble extract with the effects of maintaining men's health. Asian J Androl, 8(Suppl 1):49–50.
- George A, Liske E, Chen CK, and Ismail SB. (2013). J Sports Med Doping Stud, 2: Water Extract-Physta Does not Change Normal Ratios of Testosterone to Epitestosterone in Healthy Males, J Sports Med Doping Stud, 3:2.
- George, A. , & Henkel, R. (2014). Phytoandrogenic properties of Eurycoma longifolia as natural alternative to testosterone replacement therapy. Andrologia 46(7), 708–721. [CrossRef] [PubMed]
- Talbott, S. M. , Talbott, J. A., George, A., & Pugh, M. (2013). Effect of Tongkat Ali on stress hormones and psychological mood state in moderately stressed subjects. Journal of the International Society of Sports Nutrition 10(1), 28. [CrossRef] [PubMed]
- Thu, H. E. , Mohamed, I. N., Hussain, Z., Jayusman, P. A., & Shuid, A. N. (2017). Eurycoma Longifolia as a potential adoptogen of male sexual health: a systematic review on clinical studies. Chinese journal of natural medicines. [CrossRef]
- 2Chan, K (2021). Effects of Eurycoma longifolia supplementation: An evaluation of cell growth, exercise performance, and well-being in adult males. Doctoral thesis, Liverpool John Moores University. https://researchonline.ljmu.ac.uk/id/eprint/15104/ ; https://researchonline.ljmu.ac.uk/id/eprint/15104/1/2021kaiquinphd.
- Chinnappan, S.M. , George, A., Pandey, P., Narke, G., Choudhary, Y.K. Food & Nutrition Research, 5: aqueous root extract–Physta® on testosterone levels and quality of life in ageing male subjects: a randomised, double-blind, placebo-controlled multicentre studyFood & Nutrition Research 2021, 65, 2021. [Google Scholar] [CrossRef]
- Bhat, R. , & Karim, A. A. (2010). Tongkat Ali (Eurycoma longifolia Jack): a review on its ethnobotany and pharmacological importance. Fitoterapia, 81(7), 669–679. [CrossRef]
- Rehman, S. U. , Choe, K., & Yoo, H. H. (2016). Review on a Traditional Herbal Medicine, Eurycoma longifolia Jack (Tongkat Ali): Its Traditional Uses, Chemistry, Evidence-Based Pharmacology and Toxicology. Molecules (Basel, Switzerland). [CrossRef]
- Low, B. S. , Das, P. K., & Chan, K. L. (2013). Standardized quassinoid-rich Eurycoma longifolia extract improved spermatogenesis and fertility in male rats via the hypothalamic-pituitary-gonadal axis. Journal of ethnopharmacology, 145(3), 706–714. [CrossRef]
- Leisegang, K. , Finelli, R., Sikka, S. C., & Panner Selvam, M. K. (2022). Eurycoma longifolia (Jack) Improves Serum Total Testosterone in Men: A Systematic Review and Meta-Analysis of Clinical Trials. Medicina (Kaunas, Lithuania). [CrossRef]
- Henkel, R. R. , Wang, R., Bassett, S. H., Chen, T., Liu, N., Zhu, Y., & Tambi, M. I. (2014). Tongkat Ali as a potential herbal supplement for physically active male and female seniors--a pilot study. Phytotherapy research : PTR. [CrossRef]
- Khanijo, T. , & Jiraungkoorskul, W. (2016). Review Ergogenic Effect of Long Jack, Eurycoma Longifolia. Pharmacognosy reviews 10(20), 139–142. [CrossRef] [PubMed]
- George, A. , Udani, J., Abidin, N. Z., & Yusof, A. (2018). Efficacy and safety of Eurycoma longifolia(Physta®) water extract plus multivitamins on quality of life, mood and stress: a randomized placebo-controlled and parallel study. Food & nutrition research, 1374. [Google Scholar] [CrossRef]
- Insanu M, Pratiwi S N E, Fidrianny I. A review of the phytochemical compounds and pharmacological activities of Eurycoma longifolia. International Journal of Research in Pharmaceutical Sciences. (IJRPS), 1949.
- Mohamed, A. Farag, Abiodun O. Ajayi, Mohammed Taleb, KaiWang, and Iriny M. Ayoub. A Multifaceted Review of Eurycoma longifolia Nutraceutical Bioactives: Production, Extraction, and Analysis in Drugs and Biofluids. ACS Omega. 2023, 8, 1838−1850. [Google Scholar]
- Lee EL and Barnes, J. Tongkat Ali/Long Jack. https://www.publish.csiro.au/hc/pdf/HC22143. Journal of Primary Health Care. [CrossRef]
- Muniandy, S. , Yahya, H. M., Shahar, S., Kamisan Atan, I., Mahdy, Z. A., Rajab, N. F., George, A., & Chinnappan, S. M. (2023). Effects of Eurycoma longifolia Jack standardised water extract (Physta) on well-being of perimenopausal and postmenopausal women: protocol for a randomised, double-blinded, placebo-controlled, parallel group study. BMJ open. [CrossRef]
- Niamh Michail. 'Incorrect and misleading': Industry defends ashwagandha root extract safety amid Danish assessment. , 2023, https://www.vitafoodsinsights.com/botanicals-herbs/-incorrect-andmisleading- industry-defends-ashwagandha-root-extract-safety-amid-danish-assessment. 25 May.
- Indian Express. (2024). Denmark's ban on Ashwagandha lacks scientific rigor. Retrieved from https://indianexpress.com/article/cities/pune/denmarks-ban-on-ashwagandha-ban-based-on-2020-reportthat- lacks-scientific-rigor-says-ayush-ministry-9435664/. 2020.
- The Indian Herbal Pharmacopeia. Revised new edition 2002. Indian Drug manufacturers' association, Mumbai, pp. 467-478.
- Amritha, N. , Bhooma, V., & Parani, M. (2020). Authentication of the market samples of Ashwagandha by DNA barcoding reveals that powders are significantly more adulterated than roots. Journal of ethnopharmacology 256, 112725. [CrossRef] [PubMed]
- Balkrishna, A. , Mehta, A., & Yadav, D. (2024). Botanical risk misclassifications: Withania somnifera case review. Journal of Restorative and Alternative Medicine, Advance online publication.
- Anupama, N. , Rathi, P. Journal of Ayurveda and Integrative Medicine 14(1), 100420.
- Kalaivani, P. , Siva, R., Gayathri, V., & Langade, D. (2023). Ninety-day repeated dose toxicity of Ashwagandha (Withania somnifera) root extract in Wistar rats. Toxicology reports. [CrossRef]
- Tandon, N. , & Yadav, S. S. (2020). Safety and clinical effectiveness of Withania Somnifera (Linn.) Dunal root in human ailments. Journal of ethnopharmacology 255, 112768. [CrossRef]
- Verma, N. , Gupta, S. K., Tiwari, S., & Mishra, A. K. (2021). Safety of Ashwagandha Root Extract: A Randomized, Placebo-Controlled, study in Healthy Volunteers. Complementary therapies in medicine. [CrossRef]
- Vaidya, V. G. Gothwad, A., Ganu, G., Girme, A., Modi, S. J., & Hingorani, L. (2024). Clinical safety and tolerability evaluation of Withania somnifera (L.) Dunal (Ashwagandha) root extract in healthy human volunteers. Journal of Ayurveda and integrative medicine 15(1), 100859. [CrossRef] [PubMed]
- Mandlik Ingawale, D. S. , & Namdeo, A. G. (2021). Pharmacological evaluation of Ashwagandha highlighting its healthcare claims, safety, and toxicity aspects. Journal of dietary supplements 18(2), 183–226. [CrossRef]
- Paul, S. , Chakraborty, S., Anand, U., Dey, S., Nandy, S., Ghorai, M., Saha, S. C., Patil, M. T., Kandimalla, R., Proćków, J., & Dey, A. (2021). Withania somnifera (L.) Dunal (Ashwagandha): A comprehensive review on ethnopharmacology, pharmacotherapeutics, biomedicinal and toxicological aspects. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 143, 112175. [CrossRef]
- Mukherjee, P. K. , Banerjee, S., Biswas, S., Das, B., Kar, A., & Katiyar, C. K. (2021). Withania somnifera (L.) Dunal - Modern perspectives of an ancient Rasayana from Ayurveda. Journal of ethnopharmacology. [CrossRef]
- Mikulska, P. , Malinowska, M., Ignacyk, M., Szustowski, P., Nowak, J., Pesta, K., Szeląg, M., Szklanny, D., Judasz, E., Kaczmarek, G., Ejiohuo, O. P., Paczkowska-Walendowska, M., Gościniak, A., & Cielecka-Piontek, J. (2023). Ashwagandha (Withania somnifera)-Current Research on the Health-Promoting Activities: A Narrative Review. Pharmaceutics. [CrossRef]
- Khalid, M. U. , Sultan, M. T., Baig, I., Abbas, A., Noman, A. M., Zinedine, A., Bartkiene, E., & Rocha, J. M. (2025). A comprehensive review on the bioactivity and pharmacological attributes of Withania somnifera. Natural product research, 1–15. Advance online publication. [CrossRef]
- HMPC. EMA/HMPC/24186/2023. Assessment Report on Rhodiola rosea L., Rhizoma et Radix. Draft–Revision 1; Committee on Herbal Medicinal Products (HMPC): Amsterdam, The Netherlands, 2023; pp. 1–50. [Google Scholar]
- Punja, S. , Shamseer, L., Olson, K., & Vohra, S. (2014). Rhodiola rosea for mental and physical fatigue in nursing students: a randomized controlled trial. PloS one, 9(9), e108416. [CrossRef]
- Schröter, H.-B. , Neumann, D., Katritzky, A.R.; Swinbourne, F.J. Withasomnine. A pyrazole alkaloid from Withania somnifera Dun. Tetrahedron, 2895. [Google Scholar] [CrossRef]
- Rath, S. N. , Jena, L., Bhuyan, R., Mahanandia, N. C., & Patri, M. (2021). In silico discovery and evaluation of phytochemicals binding mechanism against human catechol-O-methyltransferase as a putative bioenhancer of L-DOPA therapy in Parkinson disease. Genomics & informatics, 19(1), e7. [CrossRef]
- Panossian A, Amaterdam J. 2017. Adaptogens in Psychiatric Practice. Chapter 8, Pp 155-181 in: Complementary and Integrative Treatments. Eds. PL. Gerbarg, PR. Muskin, RP. Brown, American Psychiatric Association Publishing. Arlington, 2018, 425 pages. https://www.appi.org/Complementary_and_Integrative_Treatments_in_Psychiatric_Practice.
- Akgul, Y. , Ferreira, D., Abourashed, E. A., & Khan, I. A. (2004). Lotaustralin from Rhodiola rosea roots. Fitoterapia, 75(6), 612–614. [CrossRef]
- Langeder, J. , Grienke, U., Döring, K., Jafari, M., Ehrhardt, C., Schmidtke, M., & Rollinger, J. M. (2021). High-performance Countercurrent Chromatography to Access Rhodiola rosea Influenza Virus Inhibiting Constituents. Planta medica, 87(10-11), 818–826. [CrossRef]
Figure 3.
Chronic stress-induced symptoms and the effect of adaptogens on key mediators and effectors of the adaptive stress response result in neuroprotection, leading to increased cognitive function and enhanced mental and physical performance. Brain cells respond adaptively by enhancing their ability to function and resist stress, as demonstrated by an update from the authors' free-access publication and their accompanying drawings. Simplified overview of the stress system (central nervous system, CNS, and peripheral tissues/organs in the periphery) and reciprocal connections of elements of the neuroendocrine-immune complex to mobilize an adaptive response against the stressor [19].
Figure 3.
Chronic stress-induced symptoms and the effect of adaptogens on key mediators and effectors of the adaptive stress response result in neuroprotection, leading to increased cognitive function and enhanced mental and physical performance. Brain cells respond adaptively by enhancing their ability to function and resist stress, as demonstrated by an update from the authors' free-access publication and their accompanying drawings. Simplified overview of the stress system (central nervous system, CNS, and peripheral tissues/organs in the periphery) and reciprocal connections of elements of the neuroendocrine-immune complex to mobilize an adaptive response against the stressor [19].
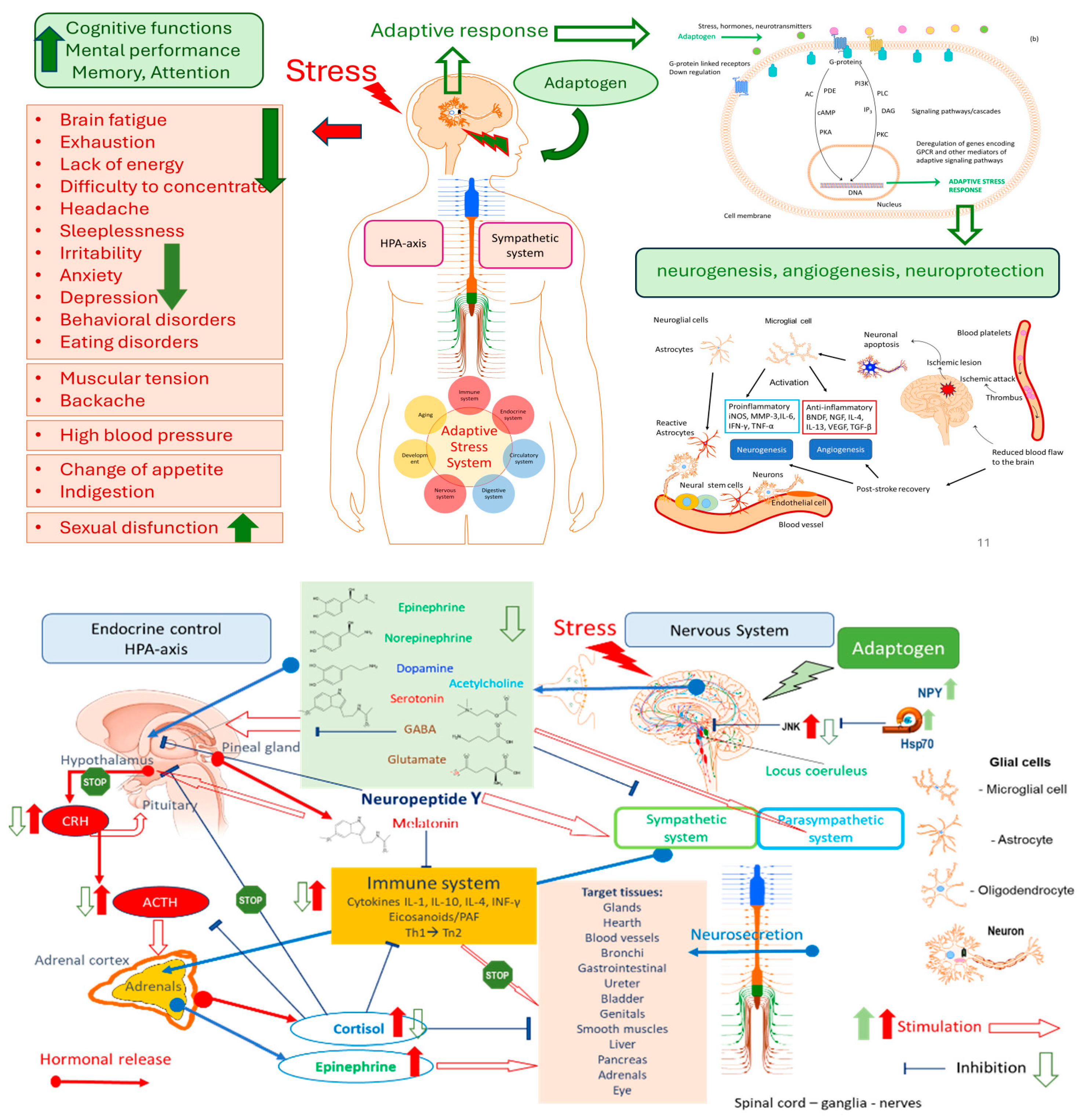
Figure 4.
The hypothetical molecular mechanisms and modes of pharmacological action of adaptogens on key mediators of the neuroendocrine-immune complex, cardiovascular, and detoxifying systems that regulate the adaptive stress response to stressors/pathogens in stress- and aging-induced diseases and disorders [19].
Figure 4.
The hypothetical molecular mechanisms and modes of pharmacological action of adaptogens on key mediators of the neuroendocrine-immune complex, cardiovascular, and detoxifying systems that regulate the adaptive stress response to stressors/pathogens in stress- and aging-induced diseases and disorders [19].
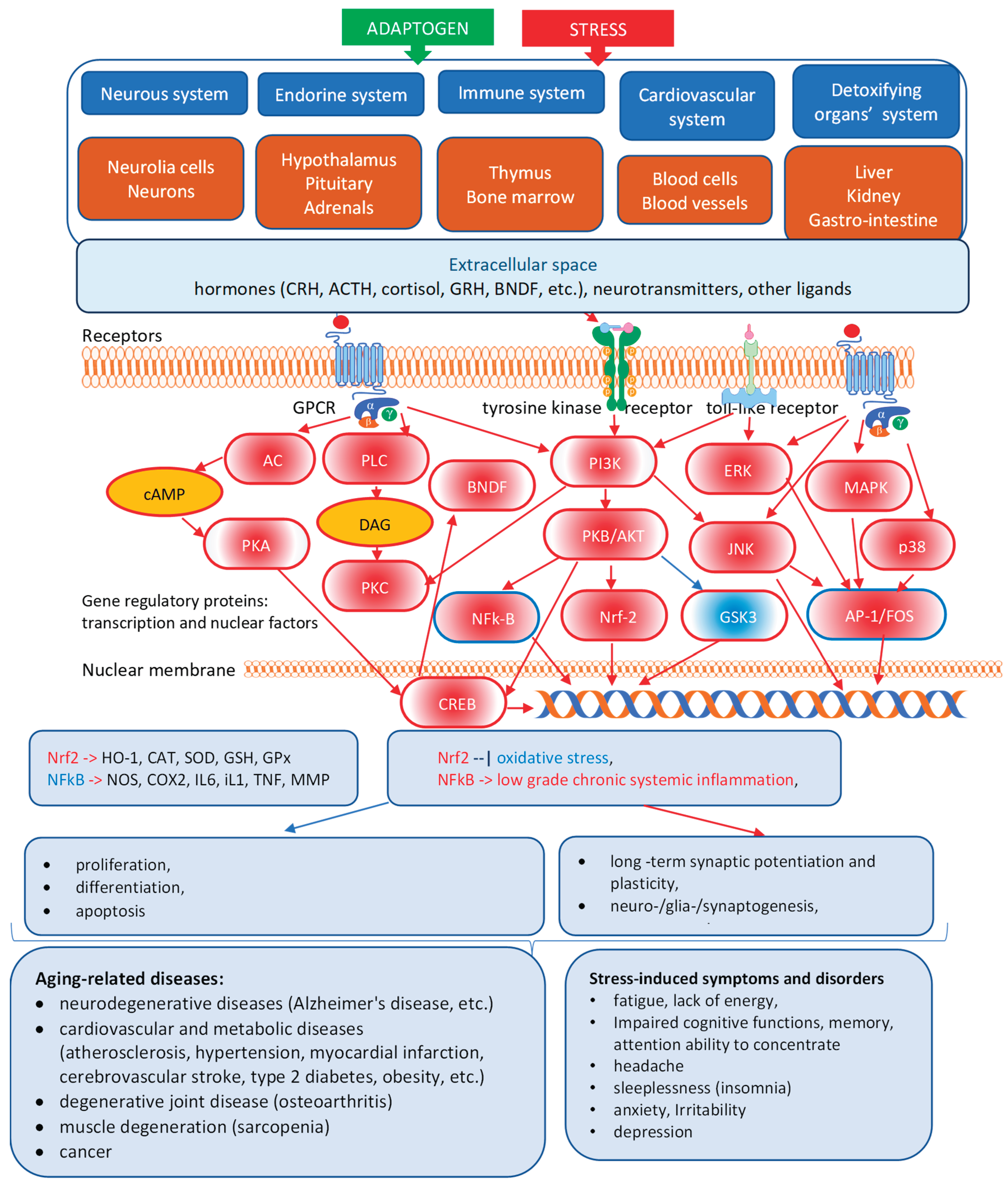

Table 1.
The comparison of differences in requirements for pharmaceuticals and dietary supplements of botanical origin.
Table 1.
The comparison of differences in requirements for pharmaceuticals and dietary supplements of botanical origin.
| Category | Pharmaceuticals | Dietary Supplements | ||
|---|---|---|---|---|
| RegulatoryOversight | Very strict | Lenient | ||
| Regulated by | Strictly regulated by drug authorities (e.g., FDA, EMA) | Loosely regulated; treated as a food category in many countries | ||
| Pre-market approval | Required (clinical trials, IND, NDA, etc.) | Not required; must follow labeling and safety guidelines. | ||
| Evidence of Safety and Efficacy | Required clinical + preclinical | Not required; General safety only | ||
| Efficacy | Must be proven through rigorous clinical trials | No requirement to prove efficacy before marketing | ||
| Safety | Extensive safety data required (nonclinical + clinical) | Only required to ensure general safety; no clinical trials mandated | ||
| Quality Standards | High | Moderate | ||
| Identity and purity | Must meet strict pharmacopoeial standards (e.g., USP, EP) | Less stringent, basic identity and purity testing is often enough | ||
| Standardization | Active ingredients must be quantified and consistent | Often contains a range of components; standardization is not always required | ||
| Contaminants (e.g., heavy metals, microbes) | Tightly controlled with established limits | Limits exist, but are less strictly enforced | ||
| Batch-to-batch consistency | Mandatory and validated | Expected but not strictly enforced | ||
| Manufacturing Requirements | Pharmaceutical grade, GMP | Food GMP | ||
| GMP Standards | Must follow pharmaceutical GMP (e.g., ICH Q7, EU GMP) | Must follow food-grade GMP (less stringent) | ||
| Process validation | Mandatory for all critical manufacturing steps | Not required for all processes | ||
| Change control & documentation. | Detailed documentation and validation are required. | Documentation is required, but it is generally simpler. | ||
| Consistencyof Botanical Source Specifics | Standardized | Variable | ||
| Botanical identity | Must be rigorously confirmed and controlled | Often confirmed, but methods may vary in rigor | ||
| Extraction process | Fully validated and standardized | May vary; often not standardized | ||
| Complex mixtures | Defined active constituents or fractions used | Often, a whole plant/extract with variable composition | ||
| Labeling Claims and Doses | Indications for use in diseases | Health supporting claims | ||
| Health claims | Medicine list "Dosage" based on age, weight, or condition.Can make therapeutic claims (e.g., "treats depression") | Supplements list "Suggested use" or "Serving size".Cannot make disease claims; only "structure/function" claims (e.g., "supports mood") | ||
| Labeling accuracy | Must match approved documentation | Must be truthful and not misleading, but with less scrutiny | ||
| Regulatory Classification |
|
|
||
| Purpose of Use | Medicines are designed for therapeutic effect and are often used for shorter-term or targeted purposes. | Supplements aim to provide nutritional support and are typically used on a long-term basis. | ||
Table 2.
FDA (United States) vs. EMA (European Union) regulations.
| Aspect | FDA (U.S.) | EMA (EU) |
|---|---|---|
| Governing Bodies | - Pharmaceuticals: Center for Drug Evaluation and Research (CDER) - Supplements: Center for Food Safety and Applied Nutrition (CFSAN) | - Pharmaceuticals: European Medicines Agency (EMA) - Supplements: Regulated at member state level (e.g., Germany: BfArM, France: ANSM) |
| Applicable Legal Frameworks | - Drugs: FD&C Act, 21 CFR- Supplements: Dietary Supplement Health and Education Act (DSHEA, 1994) | - Drugs: Directive 2001/83/EC- Supplements: Food Supplements Directive (2002/46/EC), national laws |
| Botanical Drugs | Defined as botanical drug products, subject to full NDA or IND path (e.g., Veregen®, Mytesi®) | Herbal medicinal products (HMPs), classified into: - Well-established use (WEU) - Traditional use (THMP) - Full marketing authorization |
| Supplements (Botanical) | Treated as foods, not drugs. No pre-market approval. No efficacy proof required. | Also treated as foods, but the EU is more restrictive on claims. Heavily influenced by EFSA assessments. |
| Quality Standards for Botanicals | Encourages use of USP monographs and FDA Botanical Drug Guidance (2004). Must define active constituents or marker compounds. | Uses European Pharmacopoeia (Ph. Eur.) monographs. Strict on identity, purity, and standardization. The Herbal Medicinal Products Committee (HMPC) oversees scientific guidelines. |
| Clinical Evidence (Botanical Drugs) | IND → NDA process: requires full clinical trials unless eligible for accelerated approval. | WEU: requires published literature and some clinical data. THMP: based on 30 years of traditional use (15 in the EU), with nonclinical safety evidence only |
| Labeling (Supplements) | Structure/function claims allowed: "supports immune health." Must carry a disclaimer: "This product is not intended to diagnose, treat, cure, or prevent any disease." | Health claims reviewed and authorized by EFSA; therapeutic claims prohibited on supplements. Stricter than the FDA. |
| GMP | - Drugs: 21 CFR Part 210/211- Supplements: 21 CFR Part 111 | - Drugs: EU GMP (Annexes)- Supplements: Food GMP (varies by country); less |
| Unique Points | Allows botanical drug development via standard drug approval paths. Dietary supplements are widely available with relatively light regulation, provided safety is ensured. Botanical Drug Development Guidance has been available since 2004. |
Provides a specific regulatory framework for traditional herbal medicinal products (THMPs) via simplified registration. More centralized regulation of herbal drugs via EMA's HMPC. Supplements are subject to tighter control over labeling and claims, often stricter than in the U.S. |
| Example | ||
| Echinacea supplement | Dietary Supplement, no pre-market approval | Food supplement; cannot claim therapeutic effects |
| Echinacea extract as a medicine | Must go through the full IND/NDA process | Can qualify as THMP or WEU based on evidence and monograph |
Table 3.
Countries with Pharmacopeial recognition of selected adaptogens and some putative adaptogens, such as Eurycoma and Sideritis, and their official regulatory status: ✅ - Official monograph; ⚠️ - Dietary supplement use.
Table 3.
Countries with Pharmacopeial recognition of selected adaptogens and some putative adaptogens, such as Eurycoma and Sideritis, and their official regulatory status: ✅ - Official monograph; ⚠️ - Dietary supplement use.
| Country | PharmacopoeiaMonographs | Rhodiola | Ginseng | Withania | Eleuthero-coccus | Schisandra | Eurycoma | Sideritis |
|---|---|---|---|---|---|---|---|---|
| Russia | State Pharmacopoeia | ✅ | ✅ | ✅ | ✅ | |||
| China | Pharmacopoeia of PRC | ✅ | ✅ | ✅ | ✅ | |||
| European Union | European Pharmacopoeia/EMA/HMPC Union herbal monograph | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | |
| United States | USP, USP Herbal Compendium monograph, AHP | ✅ | ✅ | ⚠️ | ⚠️ | ⚠️ | ||
| Germany | Commission E | ✅ | ✅ | ⚠️ | ✅ | ✅ | ||
| UK | ⚠️ | |||||||
| Mongolia | Mongolian Pharmacopoeia | ✅ | ✅ | ✅ | ||||
| India | Indian Herbal Pharmacopeia | ✅ | ✅ | |||||
| Pakistan | Unani/Ayurvedic Pharmacopoeia | ✅ | ||||||
| Bangladesh | Unani Pharmacopoeia | ✅ | ||||||
| Sri Lanka | Ayurvedic Pharmacopoeia | ✅ | ||||||
| South Korea | Korean Herbal Pharmacopoeia | ✅ | ✅ | ✅ | ||||
| Japan | Japanese Pharmacopoeia | ✅ | ⚠️ | ✅ | ||||
| Vietnam | Vietnamese Pharmacopoeia | ✅ | ✅ | |||||
| Lanka | ||||||||
| Australia | Australian Register of Therapeutic Goods (ARTG) | ✅ | ||||||
| Malaysia | Malaysian Pharmacopoeia | ✅ | ||||||
| Indonesia | Indonesia Pharmacopoeia | ✅ | ||||||
| South Africa | CAM regulatory framework | ⚠️ | ||||||
| WHO | WHO Monographs | ✅ | ✅ | ✅ |
✅ - Official monograph; ⚠️ - Dietary use
Table 4.
Basic Principles of Network Pharmacology: Traditional vs. Network Pharmacology.
| Feature | Traditional Pharmacology | Network Pharmacology |
|---|---|---|
| Philosophy | Reductionist – targets one gene/protein | Systems-oriented – considers multitarget interactions |
| Target Focus | Single molecule | Multiple targets, often in networks |
| Drug Design Goal | High specificity | Modulation of networks/pathways |
| View of Disease | Caused by the dysfunction of a single entity | Disease as a network perturbation |
| Data Used | Experimental pharmacokinetics/dynamics | Multi-omics, PPI networks, computational modeling |
| Mechanism Identification | Binding affinity and downstream effects | Topological influence on biological networks |
| Predictive Capacity | Limited to known targets | Broader scope; includes off-targets, repurposing, synergy predictions |
| Herbal/TCM Suitability | Not applicable | Especially suitable due to the multi-component nature |
| Validation | Strong experimental support | Requires computational and experimental integration |
| Limitations | Ignores complexity and off-target effects | Data noise, oversimplified networks, context-ignorant models |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



