Submitted:
20 July 2025
Posted:
21 July 2025
You are already at the latest version
Abstract
This article presents a case study of a 64-year-old female patient who underwent orthodontic treatment to enhance the aesthetic appearance of her smile and replace a missing tooth (46). During the preliminary visit, significant gnathological concerns were identified, including headaches, orofacial pain, and muscle fatigue. These issues had to be addressed prior to the start of the orthodontic phase of treatment. Methods: a multidisci-plinary treatment plan was implemented using a sequential approach. The initial phase involved the implementation of techniques to reduce muscle tension and manage orofacial pain, with the objective of achieving clinical stability. Following the attainment of clinical stability, the orthodontic phase commences with the aim of improving occlusion and pos-ture. Results: a significant reduction in muscle tension-related symptoms was observed, along with effective gnathological stabilization. Subsequent orthodontic treatment resulted in aesthetic and functional improvements to the smile, optimizing occlusion and overall posture. The final phase will involve implant-prosthetic rehabilitation to replace tooth 46. Conclusions: a comprehensive and accurate initial gnathological diagnosis is essential for planning effective rehabilitative therapy in patients with partial edentulism and associated conditions. A multidisciplinary approach has proven fundamental in achieving stable and predictable long-term outcomes, even after the implant-prosthetic phase.
Keywords:
case report
; TMD
; biofeedback
; splint therapy
; clear aligners
1. Introduction
This article presents a clinical case of a female patient diagnosed with temporomandibular disorder (TMD), who wants to replace the long-lost 4.6 tooth. The report outlines a comprehensive treatment pathway that includes the initial gnathological rehabilitation protocol, followed by orthodontic alignment therapy.
Temporomandibular disorders (TMDs) represent a heterogeneous set of conditions involving the temporomandibular joint, masticatory muscles and related structures. They do not constitute an unambiguous diagnosis, but include symptoms such as pain, joint noise, limitations in jaw movements and headaches. The causes are multifactorial, including trauma, occlusal disorders, systemic factors and psychological disorders such as anxiety and stress, which now play a central role in pathogenesis. The masticatory neuromuscular system has a considerable capacity for adaptation, but when this is exceeded, clinical symptoms occur. Pain can radiate to different areas of the skull and neck. Clinically, in addition to pain, intraoral signs such as tooth wear, abfraction, gingival recession and soft tissue impressions are observed. The management of TMD is complex and requires an interdisciplinary approach [1,2].
The development of TMD is multifactorial, influenced by occlusal disharmony, emotional stress, masticatory muscle fatigue, parafunctional habits, trauma, hormonal factors, and articular changes. Posteriorly edentulous patients exhibit condylar position changes due to the lack of intercuspation. TMJ noises, such as clicking and crepitus, are common in TMD patients, often associated with disc displacement or osteoarthritis, particularly in edentulous individuals [3].
The factors associated with temporomandibular joint (TMJ) dysfunction exhibit variability across different malocclusion categories, highlighting the impact of malocclusion on temporomandibular disorders (TMDs). Additionally, bruxism has been linked to various TMD symptoms, including myofascial pain, disc displacement, arthralgia, and muscular dysfunction [4]. A CBCT study indicated that greater loss of tooth-supporting zones is associated with posterior and inferior displacement of condyles [5].
Tooth loss remains a significant global issue, particularly among adults and the elderly, despite advancements in dentistry and oral disease prevention. Dental alignment is regulated by the balance between opposing muscular forces: the cheeks and lips exert inward pressure, while the tongue pushes outward. Teeth achieve a neutral position when these forces are balanced, but crowding can occur if space is insufficient. Even after eruption, changes in muscular forces can alter the tooth position. For instance, excessive tongue activity or abnormal tongue size can result in anterior open bites. Teeth tend to drift mesially due to functional forces from the alveolar bone and gingival fibers, which is particularly evident following tooth loss, leading to the tilting of adjacent teeth into the edentulous space. Moreover, occlusal contact between upper and lower teeth is essential to prevent the extrusion of opposing teeth. Partial or total edentulism disrupts the stomatognathic system, which includes teeth, masticatory muscles, the temporomandibular joint (TMJ), and related structures. Loss of occlusal contact can lead to structural remodeling and degenerative pathological changes in the TMJ when physiological limits are exceeded [6,7].
It is common that the loss of posterior teeth over a long period of time in adult patients and in the presence of other factors might have degenerative effects on the TMJ and associated structures. TMJ's osseous tissue undergoes adaptive remodeling which, if beyond physiological limits, results in pathological degeneration [8]. Several studies have examined morphological changes in the mandibular condyle in patients with partial or complete edentulism, demonstrating varying degenerative patterns, such as flattening of the posterior and superior condylar surfaces [9].Compensatory changes occur in the articular fossa, such as osseous thickening, to accommodate mechanical stress from tooth loss. The articular eminence also undergoes alterations, with pronounced flattening in edentulous patients influenced by age, gender and tooth loss. In edentulous patients, the condyle shifts posteriorly and superiorly within the articular fossa, resulting in reduced joint space and altered relationships with the articular disc [10].
The loss of one or more teeth can lead to anatomical changes, as many studies show, however all recent analyses prove that there is no association between tooth loss and the development of TMD. This demonstrates the complexity of TMD as a disorder associated with multiple risk factors related to genetics, environment, psychosocial behavior, demographics, comorbidities, without direct association with dental occlusion [11].
The absence of a posterior tooth with intact adjacent teeth is the primary cause of arch collapse due to the movement of adjacent teeth. Failure to replace missing posterior teeth leads to tipping and rotation of adjacent teeth, overeruption of opposing teeth, and reduced alveolar bone support [12]. Overeruption of unopposed teeth complicates implant-prosthetic rehabilitation. Adjacent teeth to the edentulous site may undergo non-vertical movements. Mesial tipping of teeth proximal to the extraction site is more pronounced in the maxilla, while distal tipping is more frequent in the mandible. Tooth loss alters the shape of dental arches and occlusal planes, resulting in occlusal interferences and retruded contact position (RCP) contacts. These changes are correlated with the degree of overeruption and tipping of teeth near the extraction site. Protrusive interferences are associated with distal tooth movement, while working-side interferences are linked to mesial tipping of teeth near the extraction site [13]. Studies using CBCT imaging have shown overeruption of unopposed molars within months of antagonist extraction, emphasizing the need for timely interventions [14].
Oral health extends beyond the aesthetics of the smile and encompasses the balance between teeth, muscles, and temporomandibular joints (TMJ), which are essential for functions such as chewing, swallowing, and phonation. In adult patients who wish to replace with a prosthetic bridge or implants one or more lost teeth, it is necessary to assess the presence of temporomandibular dysfunctions that could compromise the success of the treatment. These dysfunctions, often underestimated, can lead to chronic pain, occlusal alterations, and functional limitations, reducing the effectiveness and longevity of future prosthetic rehabilitations. Therefore, it is crucial to address them prior to treatment to ensure lasting results. Orthodontic treatment made it possible to normalize the position of the teeth, the shape of the dental alveolar arches, occlusal planes, improve the bite, which made it possible to prepare the patient for rational prosthetics.
A comprehensive clinical evaluation should begin with a detailed patient history and include a systematic TMD examination to assess pain intensity, functional limitations, and psychosocial distress. Utilization of validated clinical and instrumental diagnostic methods allows for the accurate identification of pain-related orofacial conditions and supports differential diagnosis. Patients experiencing active TMD symptoms are generally considered unsuitable for restorative or orthodontic interventions until adequate pain control is achieved. In cases where TMD signs develop during treatment, clinicians are advised to suspend active therapy and prioritize symptom relief. Dental or orthodontic procedures can be resumed once the patient is pain-free or once pain is effectively managed, with adjustments to the treatment plan made as clinically indicated [15].
This article describes the operative sequence in the diagnosis and treatment of a patient suffering from TMD and desiring a future replacement of the lost tooth 4.6. The importance of gnathological and orthodontic approach is emphasized, as proper management of TMJ facilitates the creation of a functional, stable, and pain-free smile, thereby improving the patient's quality of life.
2. Materials and Methods
2.1. Case Presentation
Female patient, 64 years old. She presented to the Orthognathodontic Department of the "G. d'Annunzio" University of Chieti, Italy, with a specific request to improve the aesthetics of her smile and replace tooth 4.6 which had been missing more than 5 years ago. The tooth was lost due to destructive decay, so the doctor who was treating the patient years ago decided to extract it, but it has never been replaced (Figure 1 a, b, c, d, e). During the initial visit, routine questions about general health were performed, revealing no significant findings. The patient does not have any disease or condition that requires the use of specific medications. She does not smoke or drink alcohol. She does not have insomnia or difficulty falling asleep. She never had any gnathological or orthodontic treatment previously. In addition to masticatory structures, the general function of the cranial nerves, eyes, ears, and neck have been evaluated. No abnormalities were identified upon examination. The patient asserts that she has never had any neurological examination before. No joint noises were detected upon objective inspection of the TMJ.
- Questions asked to the patient:
- Have you ever received any treatment for your temporomandibular joint problems? NO
- Do you ever wake up with tooth or jaw discomfort? YES
- Does she ever realize that she clenches her teeth hard during the day? YES
- Has anyone ever told you that you rattle your teeth during sleep? NO
- Does she experience pain when she eats? SOMETIMES
- Does she experience pain or discomfort around her eyes, ears, or other parts of her body? AROUND MATICATORY MUSCLES
- Does she have hearing problems? NO
- Does She have headaches or a sense of "tightness"? YES
- Does She have occasional headaches? YES
- Does She or she suffer from migraines? NO
- Does she feel the whole mouth burning? NO
- Does she feel burning parts of the mouth (tongue, gums, cheeks, palate)? NO
- Does she have frequent neck muscle discomfort or neck pain? YES
- Do you feel the pain move from one place to another in your face, neck, shoulders, or back? YES
- Do the jaw muscles tire easily? YES
- Do you have difficulty opening your mouth much? NO
- Does she suffer or has he suffered from arthritis? NO
- Do you have any relatives who suffer from arthritis or gout? NO
- Have you ever received a bump in the neck or jaw area? NO
- Have you ever experienced pain in the jaw joint? NO
- Have you ever had ear problems such as ringing or lowered hearing? NO
- Have you ever heard creaking-type noises coming from the jaw joint? NO
- Do you feel that you cannot open your mouth as much as you would like? NO
- Do you currently experience pain coming from the jaw joint or muscles? YES, IN MUSCLES
- Does the pain or discomfort coming from the jaw joint interfere with your work or other activities? SOMETIMES
- Are there times when you feel that the problem or pain is less or disappears altogether? SOMETIMES
- Do you feel depressed? NO
- Have you ever been seen by a psychologist? NO
- Do you have problems with insomnia? NO
- Are you currently in a particular stressful situation (work, family, study, etc.)? NO
- Does he/she drink more than one alcoholic beverage per day? NO
- Does he smoke cigarettes, pipe or cigar? NO
- Does he usually bite his nails, lips or tongue? NO
- Do you think your pain may be related to stress? MAYBE
- In your opinion, during the day, your teeth are in contact (even light contact) for: 2 min, 2 h, 10 h, 15 h, 24 h. THE PATIENT SELECT 10 H.
When multiple signs and symptoms are present, visualization tools such as VAS (Visual Analog Scale) [16] can be helpful. The graphical representation of the head (right and left sides) and the entire body allow patients, with the guidance of the doctor, to indicate all areas, describing and quantifying the pain. VAS is a fundamental tool in defining the clinical picture, as it enables the clinician to graphically construct a pain map for the patient and establish a diagnosis. When pain is present, it is assessed based on the patient’s description of the chief complaint, location, onset, characteristics, aggravating or relieving factors, past treatments, and its relationship with other issues, considering location, behavior, quality, duration, and intensity on a scale of 0 (no pain) to 10 (intense pain affecting daily activities).
The patient describes a form of recurrent headache in the frontal region with extension to the right and left temples with pain level 8. This headache often begins in the morning and persists throughout the day, preventing the patient from performing normal daily activities, forcing her to take painkillers (NSAIDs) almost every day. The patient took pain-relieving medication by herself when necessary. No neurologist prescribed the drugs; the patient has never been examined by a neurologist. Additionally, there is generalized fatigue/tension in the masseter muscles, particularly upon waking (pain level 6). The patient feels a sense of tension in the neck and shoulders area with pain level 6. The patient admits to clenching her teeth a lot during the day and, most probably, during the sleep hours as she experiences a lot of tension in the masticatory muscles and sore teeth when she wakes up.
The analysis proceeded with digital palpation of the masticatory muscles; the pain scale is identified in 4 levels from 0 (no pain) to 3 (high pain). In this case the patient scored a pain level of 3 for all intraoral masticatory muscles (TT, PES, PEI, PIS, PII, MMP, MMS).
The intraoral examination (Figure 1 a, b, c, d, e) reveals a good degree of oral hygiene; however, it is a thin gingival biotype with areas of widespread gingival recession and significant bite marks on the buccal mucosa and the edges of the tongue, with some areas also showing bite-related ulcers (Figure 1 f).
2.2. Cone Beam CT Analysis
To complete the collection of the patient's data, a CBCT was performed. Through CBCT, it is possible to perform multiple slices and obtain several images simultaneously, particularly facilitating the visualization of the TMJ areas. This allows for the identification of possible changes in the condylar fossa and/or the condylar head, thereby improving diagnostic accuracy [17].
The 3D image of the cranium was oriented in the Dolphin software according to NHP posture. The NHP orientation was carried out by the widgets present in Dolphin; hard and soft tissue views were checked for orientation in the software by visualizing the head from the front, right, and left sides. In the NHP, there are three reference planes (Figure 2 a, b, c), perpendicular to each other:
1. The transverse plane coincides with the Frankfurt plane (FH), a plane passing through two points: Orbital (Or) and Porion (Po).
2. The sagittal plane coincides with the mid-sagittal plane (MSP), a plane perpendicular to the plane FH and passing through two points: crista galli (Cg) and basion (Ba).
3. The coronal plane coincides with the anteroposterior (PO) plane, perpendicular to the FH and MSP, passing through the right and left Porion.
After defining the orientation of the head, it is possible to complete all the slices to obtain the images necessary for finalizing the diagnosis (Figure 3 a, b, c, d, e, f).
The patient's TMJ image shows the right and left condylar heads retro positioned within the condylar fossa. No other changes such as osteophytes, erosions, signs of sclerosis seem to be evident. (The lack of MRI prevents verification of the state of the articular disc).
2.3. Diagnosis and Treatment Planning
The patient request was to improve dental alignment and replace the missing tooth 4.6. During the interview, the necessary steps to be followed are explained to the patient: the primary issue is the presence of tension-type headaches induced by unconscious clenching and masticatory muscle’s tension. After the tension/pain and the clenching activity has been managed, orthodontic therapy will be performed with the use of clear aligners to meet the aesthetic needs of the patient. About the prosthetic part to replace tooth 4.6, two options are proposed: a prosthetic bridge with support on teeth 4.7 and 4.5, or the insertion of an implant. The patient chooses the latter option as she does not want teeth 4.7 and 4.5 to be modified for prosthetic purposes.
2.3.1. Gnathological Therapy
The suspicion of unconscious clenching arises during the initial visit when the patient reports issues such as tension-type headaches (characterized as headaches that must have a tension-based origin, respond to anti-inflammatory drugs, be independent of noise and light, affect both the right and left sides equally, and not be excessively debilitating), neck pain, back pain, tenderness of the masticatory muscles, fatigue while chewing hard foods, difficulty fully opening the mouth, morning muscle soreness and a feeling of muscle tension in the head and neck area. To confirm the diagnosis of sleep bruxism, a non-instrumental method was used based on the patient’s description of symptoms, questionnaires, medical history, and clinical examinations. Electromyography (EMG) and polysomnography showing muscle activity were not conducted.
During data collection, the intraoral examination typically reveals the classic signs of bruxism: a linea alba on the buccal mucosa and tooth indentations along the tongue's edges. These are hallmark signs of clenching, resulting from slow but continuous activity over time, leading to tension and soreness in the masticatory muscles, particularly the masseter and temporalis muscles, ultimately contributing to tension-type headaches [18].
The patient in this case presents all the characteristic elements of tension-type headaches induced by unconscious clenching and sleep bruxism, based on objective assessments, questionnaires and patient descriptions.
The therapy proposed to the patient is based on the use of splints combined with neural conditioning with biofeedback exercises. The therapy involves the use of the upper splint during the night, and the lower splint used during the day. In association with the lower splint, the patient must perform a sequence of exercises three times a day, which, over the course of the following months, will recondition the patient's clenching activity on a conscious level. The patient starts the protocol and is visited monthly to assess the progress of the therapy. At each visit, VAS and muscle palpation are repeated. No other forms of assessment on the degree of muscle tension and fatigue were performed. For sleep bruxism no botulinum toxin type A injection was considered.
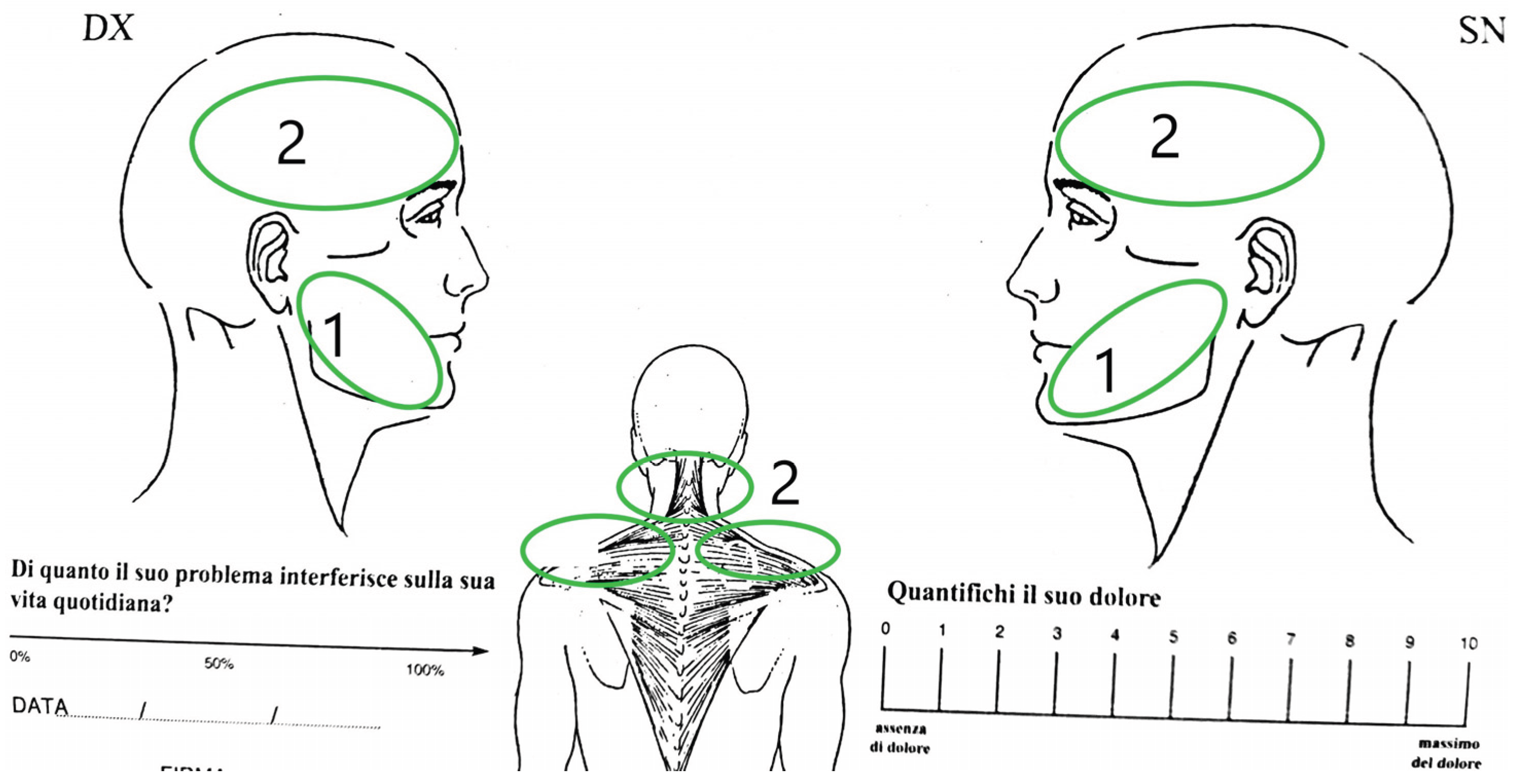
After 5 months in which the patient used the splints correctly and performed the exercise, it has been compared to the VAS performed during first visit. The patient reports significant overall improvement, with a reduction in headache levels from 8 to 5, after 3 months, and a level of 2 after 5 months. The headaches have become much more sporadic and gradually decreasing intensity: in particular, the patient reports that when the headaches occurred, they were much milder and, above all, she did not have to take NSAIDs as she had specified at the first visit. The discomfort/tension she had in her shoulders and neck had completely disappeared. No longer waking up with discomfort in the masticatory muscles and tooth soreness. The patient did not have to take any muscle relaxant medication or perform any specific massages to reduce tension (Figure 4a Vas pretreatment, 4b Vas post treatment).
Figure 4a.
Vas used at the School of Orthodontics in Chieti, pretreatment.
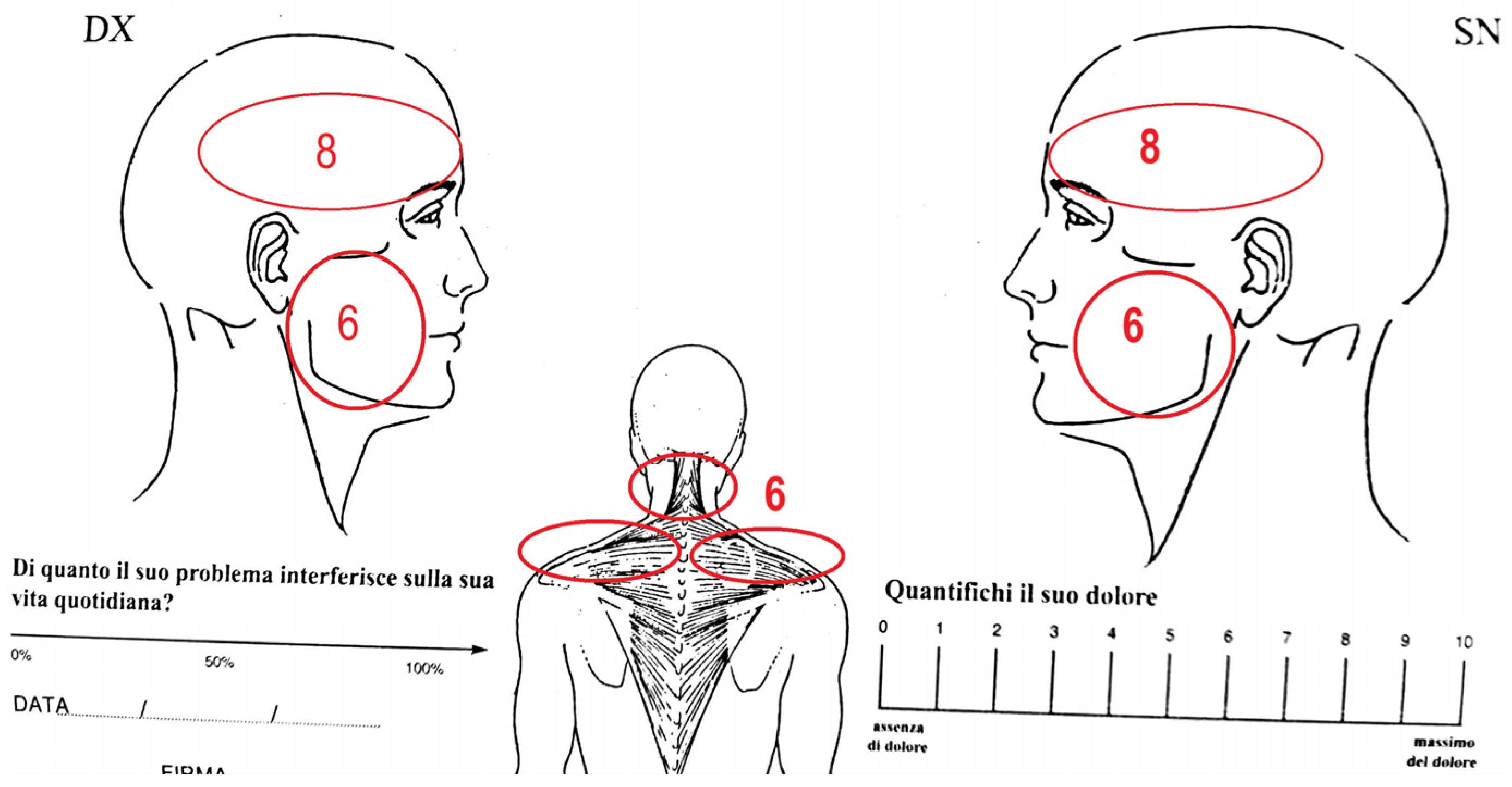
Figure 4b.
Vas post treatment.
Upon performing muscle palpation (conducted by the same clinician who performed the first analysis), the pain levels of the intraoral masticatory muscles decreased from 3 to 0-1. The improvement and muscle relaxation were highlighted by the patient, who described her face as appearing “slimmer.” This subjective evaluation was evaluated by the objective analysis of the patient's masseter muscles, as seen in the initial CBCT and a follow-up CBCT conducted a year later. The imaging showed elongation and thinning of the masseter muscles (Figure 5 a, b).
2.3.2. Orthodontic Therapy
After 6 months of splint therapy, in which the patient's condition was found to be maintained, it was decided to start orthodontic therapy with clear aligners. In this clinical case, careful consideration was given to the patient's gingival phenotype, identified as thin, with early signs of gingival recession particularly in the canine regions. Before starting orthodontic therapy, the patient was placed under monthly periodontal control to assess the gingival status. Once a good degree of stability is obtained, orthodontic therapy can be started. Teeth movements were meticulously planned to avoid exacerbating the existing recession or inducing further periodontal compromise.
The patient has a slight degree of anterior misalignment in both upper and lower arch, on the left-side she has class I molar and canine and on the right-side class I canine and molar undefined due to lack of 4.6 (Figure 1). During the initial phase of orthodontic treatment, thirty pairs of aligners were planned, with each pair worn for 15 days. Monthly follow-up visits were scheduled to assess aligner fitting, teeth movements and monitor any signs of gingival recession. After approximately 18 months, a satisfactory level of dental alignment was achieved. A refinement phase was subsequently initiated to optimize anterior and posterior occlusal contacts and to create adequate space for a future implant in region 4.6. An additional fifteen pairs of aligners were prescribed, again with each pair worn for 15 days, and monthly check-ups continued throughout this phase.
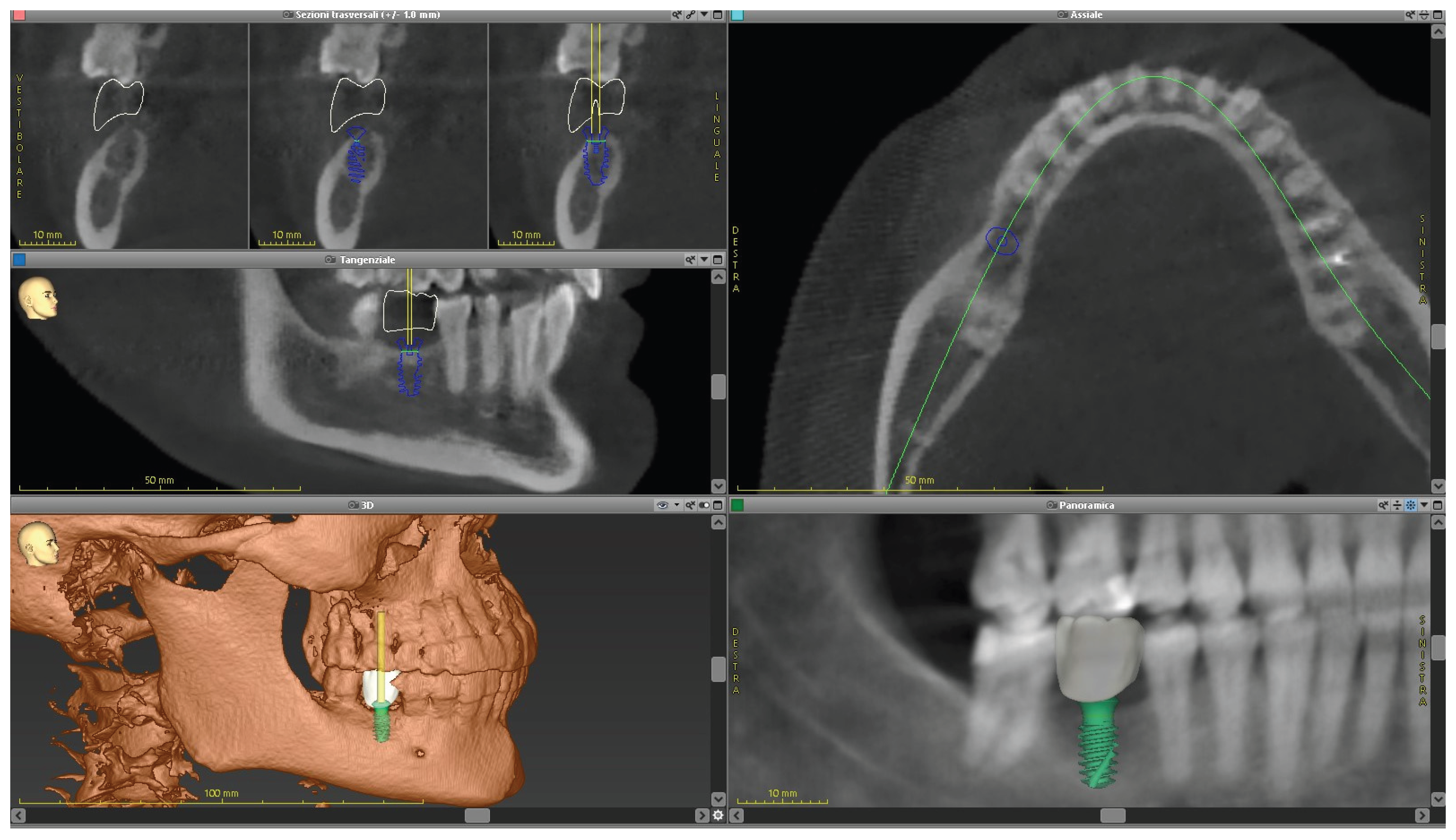
After approximately 20 months of clear aligner therapy, significant improvements were achieved, including better tooth alignment, resolution of the initial malocclusion, up righting of tooth 4.7, slight intrusion of tooth 1.6 (Figure 6 a, b, c, d, e), and occlusal contacts were modified (Figure 8 a, b). Furthermore, the patient was carefully monitored to assess any possible recurrence of pain or headaches, no such problems occurred. After the end of the treatment, the final CBCT was performed (Figure 7 a, b, c, d, e, f). From the cross-section images, it is possible to see the distance gained after orthodontic therapy and the virtual set-up for the future implant 4.6 (Figure 9 a, b, c). Entire sequence of treatment shows in Table 1.
Figure 6.
finishing terapy with clear aligners: (a) frontal view; (b) right view; (c) left view; (d) lower view; (e) upper view.
Figure 6.
finishing terapy with clear aligners: (a) frontal view; (b) right view; (c) left view; (d) lower view; (e) upper view.

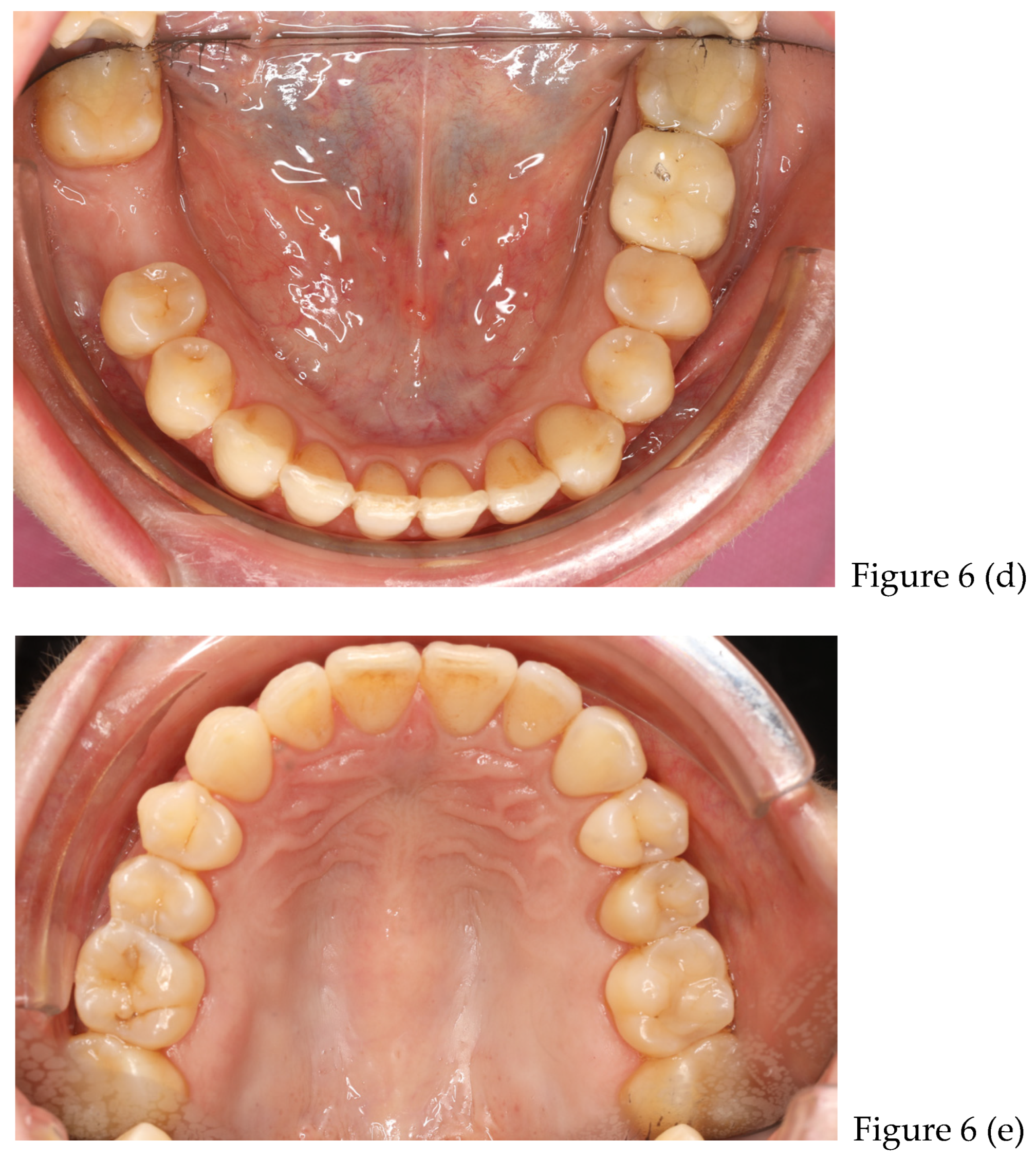
Figure 7.
(a) panoramic; (b) frontal view; (c) submento vertex lower; (d) sumento vertex upper; (e) lateral telecranium; (f) TMJ view.
Figure 7.
(a) panoramic; (b) frontal view; (c) submento vertex lower; (d) sumento vertex upper; (e) lateral telecranium; (f) TMJ view.

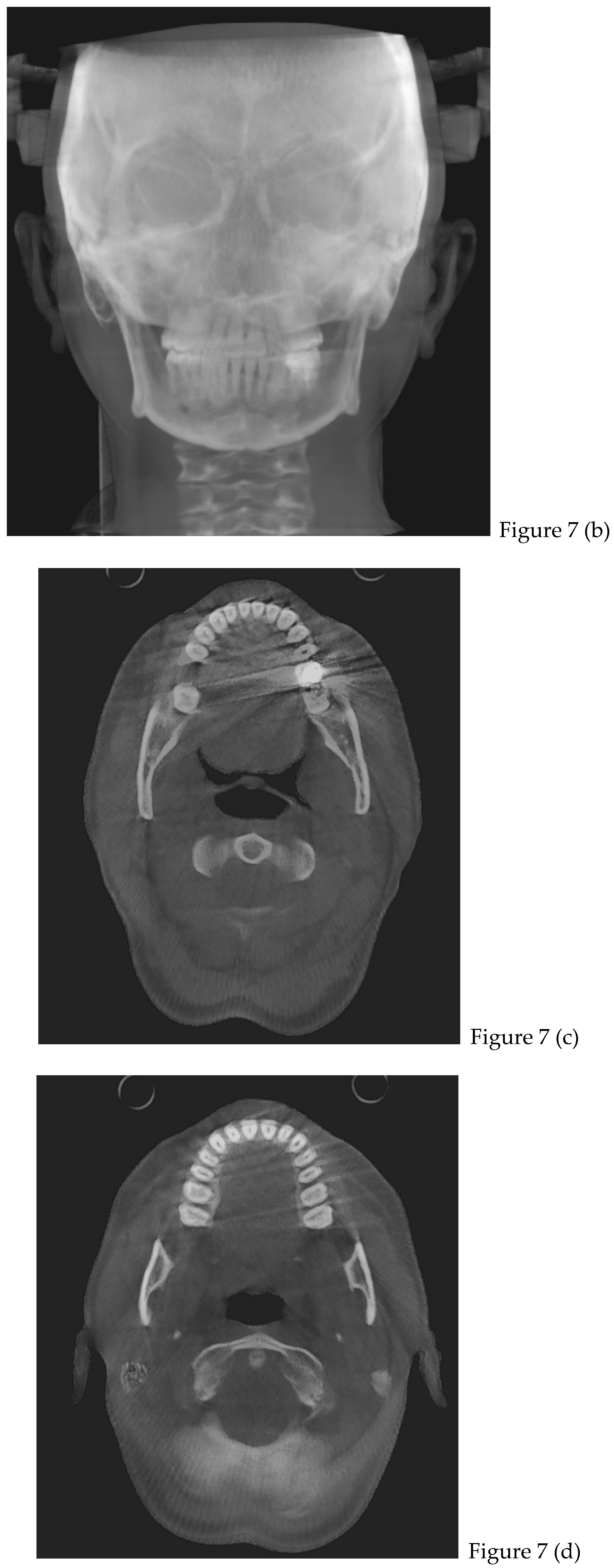
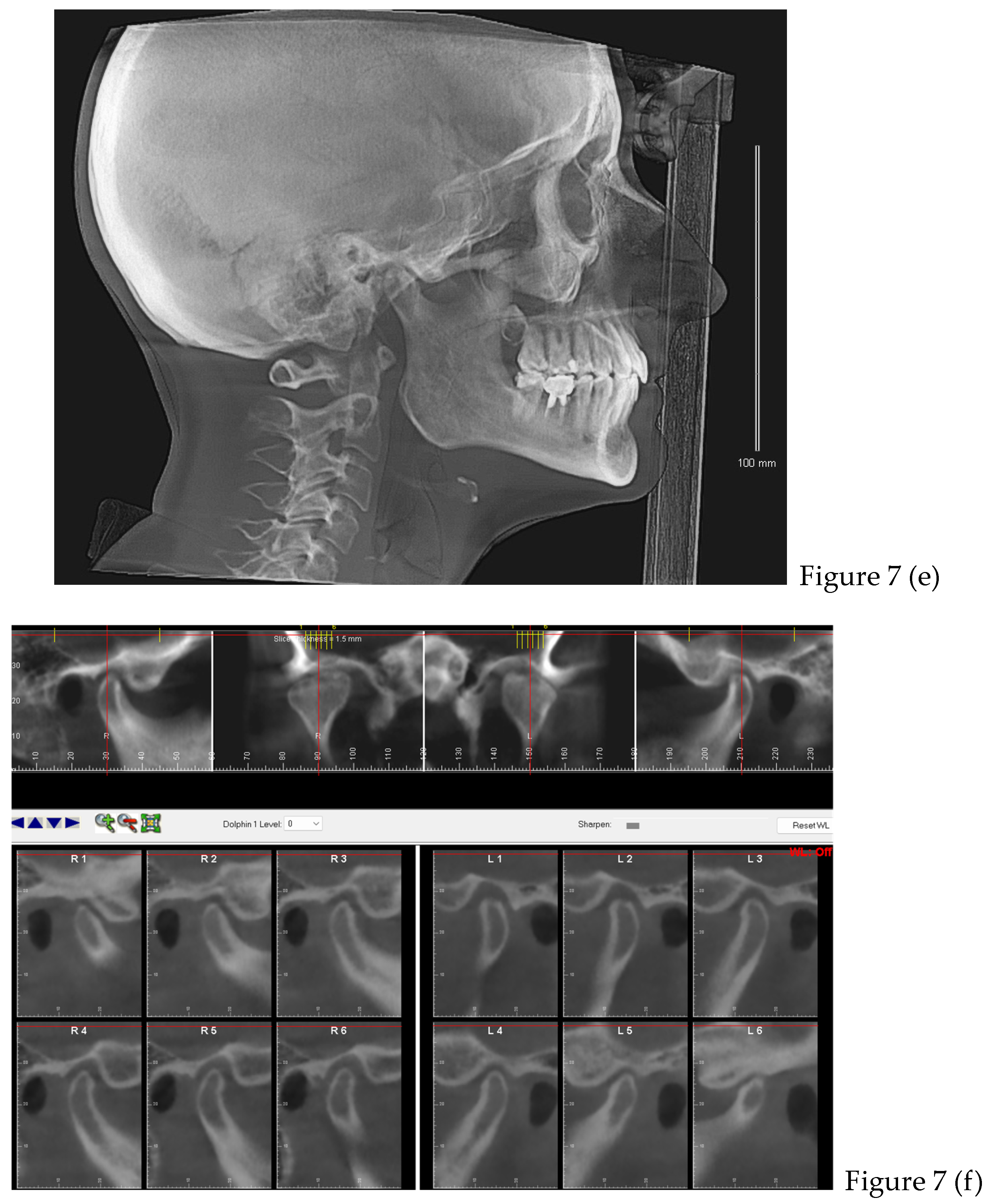
Figure 8.
(a): occlusal contacts before treatment.
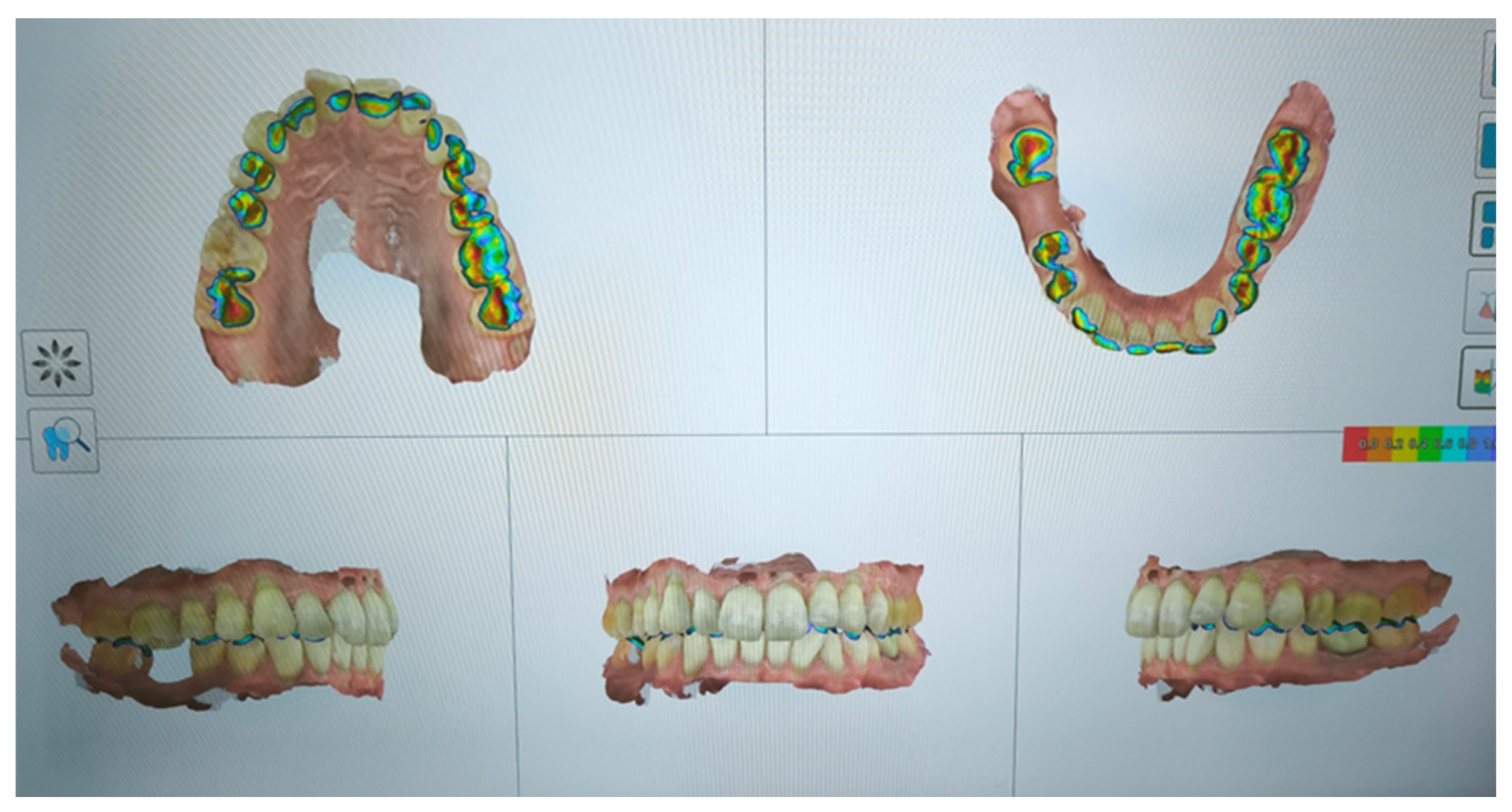
Figure 8.
(b): occlusal contacts after treatment.

Figure 9.
(a) cross section before orthodontic therapy: space 11,2mm; (b) cross section after therapy: space 12.0 mm [distance measured from the alveolar crests].
Figure 9.
(a) cross section before orthodontic therapy: space 11,2mm; (b) cross section after therapy: space 12.0 mm [distance measured from the alveolar crests].
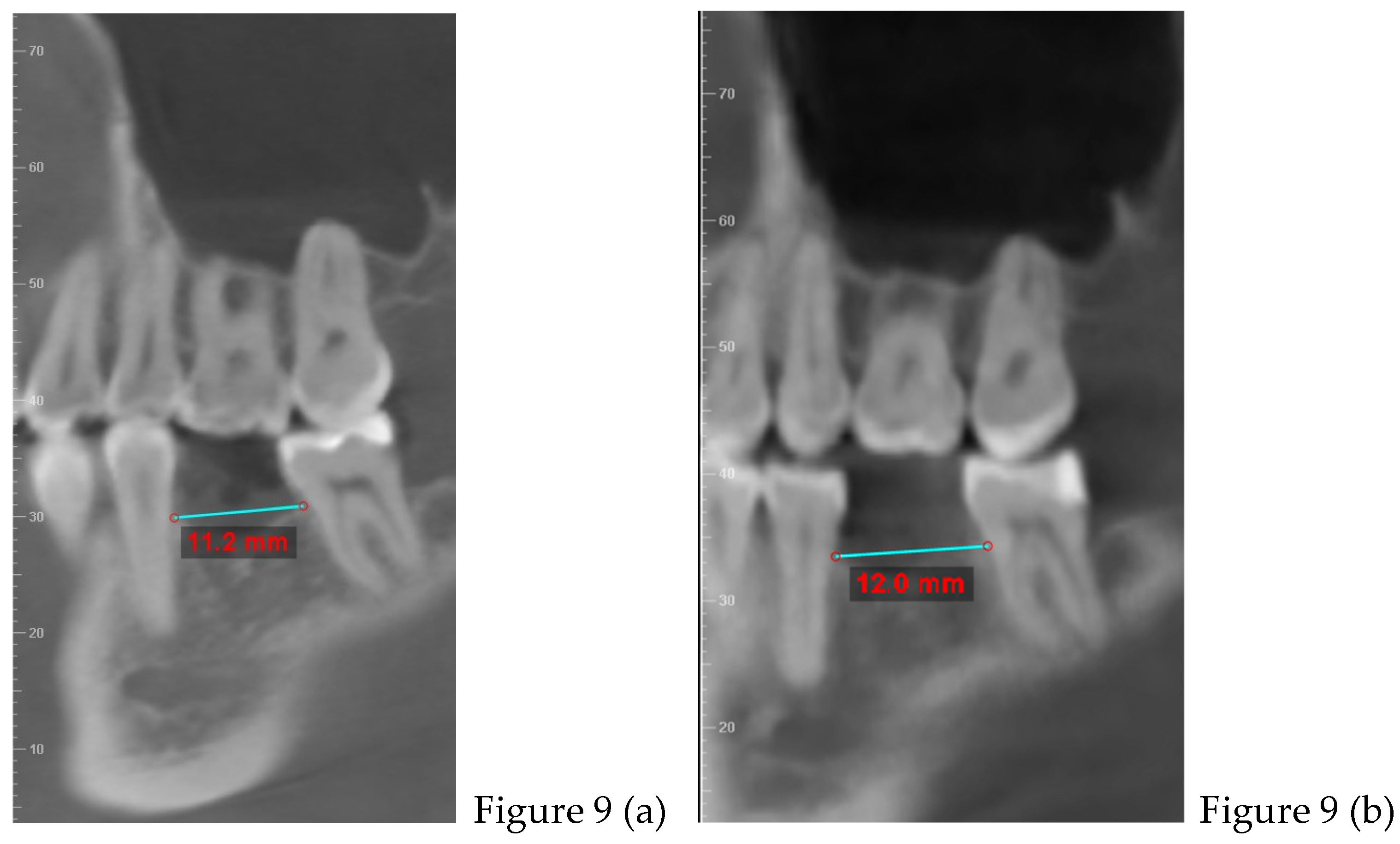
Figure 9.
(c): virtual set-up for implant placement 4.6; L: 8mm; Ø: 4.5 tissue level.
3. Discussion
Epidemiological data indicate that approximately one-third of the adult population is affected by temporomandibular disorders (TMD), with a higher prevalence observed among females. While nearly 50% of individuals with TMD experience spontaneous symptom resolution within one year without requiring clinical intervention, an estimated 75–80% of adults with persistent TMD symptoms eventually require medical treatment. In such cases, complete symptom remission may take up to three years. Common clinical manifestations include jaw clenching, joint clicking or popping, intermittent locking, and occlusal disturbances often associated with poor postural alignment. Orofacial pain refers to pain over the face, oral cavity, TMJ, and soft tissues. TMD significantly impacts the individual's physical and psychological well-being [19].
In a large part of population, the condition of pain in the orofacial area is often linked to the activity of clenching and bruxism. Factors that can compromise or damage muscles tissues include overuse or physical trauma, such as excessive stretching or a direct blow to the muscle. Often, masticatory muscles are compromised due to excessive activity; with increased muscle contractions, the physiological demands on muscle tissues also rise. However, muscle hyperactivity can reduce blood flow to the muscles, thereby decreasing the supply of nutrients necessary for normal cellular function and leading to an accumulation of metabolic waste products, which may cause muscles pain. Over time, the central nervous system can contribute to myalgia through neurogenic inflammation [20].
The co-occurrence of bruxism, temporomandibular disorders (TMDs), and headaches are common in patients. Bruxism-defined as repetitive jaw muscle activity during sleep or wakefulness is not a painful disorder but in co-occurrence with TMD worsens preexisting headache [21]. The causes are varied, including psychological factors like stress and anxiety, neurological issues such as abnormalities in the dopaminergic system, and physiological changes related to REM and NREM sleep [22].
The most important information for establishing an accurate diagnosis of TMD comes from clinical history and physical examination. In the early stages, myalgia is perceived only during muscle function. If hyperactivity persists, the pain can become chronic, presenting as a dull ache that often radiates throughout the muscle. Eventually, the pain can become severe enough to limit mandibular function. The location and degree of muscles pain and tensions are identified during a muscle examination, which can be performed through direct palpation or functional manipulation.
A healthy muscle does not cause pain or discomfort upon palpation, whereas a compromised muscle may elicit pain. The applied pressure is gentle but firm and performed using small circular movements. During palpation, the patient is asked whether the sensation is painful or merely a feeling of pressure upon touch. For comprehensive evaluation, the degree of the patient’s discomfort is recorded using the following scale: 0 (no pain), 1 (mild discomfort or tenderness), 2 (definite pain), 3 (severe pain with evident reactions, such as withdrawing from contact or tearing) [23]. To complete the analysis of the patient's condition it is necessary to use the VAS (visual analogic scale), that has been used in the context of health and healthcare for various purposes. It allows both the clinician and especially the patient to describe in more detail the areas and extent of the pain [24]. The characteristic feature of the VAS is that it makes it possible to visually describe the exact location and extent of the pain, how it occurs and how it evolves. The patient circles the affected area or indicates with a cross the precise location of the pain, and each area corresponds to a value ranging from 0 (no pain) to 10 (intense pain). It is a very useful tool, quick, clear, simple and above all it can be used by any kind of patient. Another interesting method that could be used in the preliminary diagnostic assessment of TMD is Fonseca’s questionnaire, a test consisting of 10 questions that easily helps the clinician to differentiate between types of TMD [25].
After the patient's anamnesis, performed muscle palpation and VAS it is necessary to complete the data collection through CBCT (Cone Beam Computed Tomography), performed with a low-dose radiation protocol, which involves very low exposure while providing high-quality images [26].
After the collection of the patient's objective and radiographic data, the diagnosis of head-aches tension type caused by the parafunctional activity of constant clenching can be established. The protocol, proposed by the school of orthodontics in Chieti, Italy, enables patients to become more aware of their muscular activity, particularly during times of stress in everyday activities, where the action of unconscious clenching is greatest.
The protocol is based on the use of 0.7 mm thick splints (the upper one to be used at night and the lower one during the day). During the use of the lower splint, the patient is asked to perform a biofeedback exercise to recondition the activity of the masseter and tongue muscles, so the patient becomes aware of the movements and contractions undergone by the muscles. This protocol is based on use biofeedback techniques, which have been employed for over 50 years in muscle rehabilitation to facilitate normal movement patterns after an injury. Cognitive behavioral therapy and biofeedback are noninvasive treatment options for individuals experiencing various chronic pain conditions, such as chronic low back pain, headaches, and temporomandibular disorder (TMD) [27,28].
Biofeedback is a form of treatment in which patients are trained to perceive and self-regulate their own physiological functions, such as body temperature, heart rate, muscle tension and brain activity, to improve pain control and emotional self-regulation. Biofeedback has a niche in the shape of a multidisciplinary approach because it allows the patient to become aware of, and interact with, his/her own body physiology in a conscious manner. For example, a patient may be able to reduce muscle tension, usually a reflexive response to pain, or control the breathing to remove stress, which makes the pain feel worse, through biofeedback. This therapy may be used in all types of chronic pain such as headaches, musculoskeletal pain, chronic low back pain, and in conditions related to autonomic nervous system dysfunction. There have been numerous randomized controlled trials that corroborated the fact that biofeedback, when used specifically, yields substantial pain management gain. However, whilst it has been demonstrated through records to be beneficial, biofeedback is not a magic bullet and will not be effective for all patients. It also depends on the patient's motivation and active participation as well as other psychological conditions such as anxiety or depression that will dictate the response to treatment [29].
The most critical phase of treatment protocol for TMD is patient education, which includes cognitive awareness training, relaxation therapy, and self-monitoring. These components are especially beneficial for patients with masseter hypertrophy, tension-type headaches, and bruxism. It is essential to explain to the patient the causes of their disorders, particularly the role of emotional stress, and to caution against habitual parafunctional activities (such as non-functional tooth contact or chewing on the oral mucosa). Patients must recognize their habitual behaviors involving their teeth and attempt to correct them when inappropriate.
Based on the literature that there is no single ideal form of pain therapy for TMD. Treatment of TMD should be based on a thorough diagnostic process, including the DC/TMD examination protocol, psychological evaluation, and CBCT imaging. Following the diagnostic process, once a diagnosis is established, a treatment plan can be constructed to address the patient's complaints. For severe pain, pharmacotherapy may be used (NSAID, opioids, corticosteroids, myorelaxants, anticonvulsants, benzodiazepines) while in other cases, it will be more appropriate to apply a combination of splint therapy and physiotherapy. While waiting for a custom-tailored occlusal splint, the patient can take advantage of behavioral and psychological methods, which should be continued after they have been fitted with the splint, as well as during physiotherapy treatments. The most important thing is establishing a therapeutic protocol that allows the patient to decrease the use of daily NSAIDs but above all to become more aware of her condition. After the management of tension type headache, all patient's pains have decreased.
The growing trend of adults opting for orthodontic treatment in recent years has been accompanied by an increased demand for appliances that are both more aesthetically pleasing and comfortable than conventional fixed braces. In this clinical case, the decision was taken to proceed with an aesthetic orthodontic treatment using clear aligners. Beyond the significant aesthetic benefits, the treatment plan, developed from the patient's intraoral scan, allows for virtual management of every individual tooth movement and, most importantly, enables precise measurement of the space needed for the future implant 4.6.
Successful outcomes of orthodontic treatment in adult patients depends on a detailed evaluation of periodontal health, bone quality, and systemic conditions. Cortical bone in adults tends to be denser and less vascularized due to age-related calcification, which may be accompanied by reduced remodeling capacity, hormonal imbalances, or systemic pathologies. These changes necessitate cautious force application and a customized biomechanical approach [30]. In presence of adequate spacing and sufficient bone support, all types of tooth movements (mesial, distal, buccal, lingual, extrusion, intrusion, and rotation) are feasible, adhering to the same biomechanical principles used in treating younger patients. Orthodontic forces must be light and continuous to minimize the risk of bone loss. Although structural and morphological changes in adults are like those in children, they occur more slowly, and excessive forces can prolong recovery times and increase complexity [31]. Orthodontic treatment has no negative impact on the periodontium; if minimally, controlled forces are used under non-inflammatory conditions [32].
Understanding these physiological factors in adult patients guides the choice of the simplest and most effective techniques, while maintaining a comprehensive orthodontic treatment plan.
The protocols employed in the management of active aligners are predicated on the necessity to modify the patient's arch form with a view to repositioning the roots of the teeth centrally within the cortical bone [33]. This results in dentoalveolar expansion of the arch (Figure 6 a, b, c, d), with the potential for spontaneous mandibular advancement (Figure 10 a, b). The anterior portion of the maxillary bone has experienced an increase in osteoclastic activity compared to osteoblastic activity. Consequently, there is a greater rate of bone resorption, which can lead to dehiscence and fenestrations of the teeth, particularly following orthodontic treatment. In modern humans, this condition has resulted in mandibular retro position, which has also affected cervical lordosis, causing it to straighten and thus influence the head posture [34,35].
In parafunctional patients, it is critical to diagnostic bruxism and clenching activity, as these behaviors have effects on prosthetic rehabilitation: bruxism poses mechanical risks to implants and clenching can cause muscular and joint pain, particularly when occlusion is altered. For TMD patients requiring prosthetic or implant rehabilitation, achieving complete control of clinical symptoms and a stable asymptomatic phase is essential before definitive intervention. Although bruxism is commonly regarded as a risk factor for implant failure, scientific evidence supporting this claim is limited and predominantly based on expert opinion. Caution is warranted due to the risk of mechanical overload induced by bruxism. Several studies in the literature confirm a cause-effect relationship in bruxisti patients who have undergone implant-prosthetic rehabilitation, with common complications including implant fractures, ceramic/porcelain fractures, screw loosening, screw fractures, and decementation [36].
From these considerations, it is imperative to define an optimal clinical sequence for comprehensive patient management. From the first visit, diagnosing the presence or absence of TMDs is critical, and if these conditions are identified, resolving them should be the first therapeutic step.
3. Limitations
This article reports on one clinical case and therefore does not possess a control series or comparative series of cases. The reason is the exploratory and descriptive purpose of the article, which is to describe in detail an integrated diagnostic-therapeutic treatment of a patient presenting with temporomandibular dysfunction (TMD), who later underwent orthodontic treatment in preparation for future implant rehabilitation. Although case reports do not allow statistically valid generalization, they do represent a useful clinical instrument for the dissemination of complex therapeutic pathways, particularly where these encompass the interface between a variety of dental disciplines. Nevertheless, it is accepted that, due to the absence of a comparison cohort, the opportunity for drawing causal conclusions is reduced and the findings' generalizability is compromised. Subsequent studies, with larger populations and prospective design, will be needed to confirm the reproducibility and effectiveness of the protocol described, considering the short time of analysis and follow-up.
Another limitation of the study is the absence of functional magnetic resonance images (MRI) for the examination of the joint disc. Moreover, there is no objective and instrumental evaluation from electromyographic study that would allow the different degree of activity of the masseter muscles before and after splint therapy. No assessment of the presence of sleep disorders was performed, relying solely on the patient's subjective assessment during the anamnestic questionnaire.
4. Conclusions
This case report wants to explore one of the possible methods for treating TMDs, specifically the protocol aims to describe the exclusive use of splints and biofeedback exercises and to assess how long and how far the results obtained can be maintained. In this case, almost three years have passed since the patient's first therapeutic phase, and the type of pain and fatigue that the patient described in the first visit has not recurred. The main thing that can be deduced is that the patient from the first phase of the gnathology protocol had remarkable results, allowing her to no longer use NSAIDs daily to manage her pain, greatly improving her quality of life. Biofeedback therapy has significant potential in the treatment of chronic pain due to its ability to influence the physiological response to pain and stress. Although it is not a panacea, it can be a valuable complementary tool, particularly when integrated into a comprehensive treatment plan that considers both the physical and psychological aspects of pain. The validity of biofeedback in the treatment of chronic pain is supported by a growing scientific evidence base, but its efficacy varies from individual to individual, and treatment must be customized to achieve the best results.
Through orthodontic therapy with clear aligners the clinicians met the patient's aesthetic request and, using the matching of patient's CBCT and the dental scan, it was possible to study the exact degree of movements to be made without risking increasing the degree of gum recession that the patient already had.
A key finding is the necessity of early and accurate diagnostic assessment of TMD. This step is essential to stabilize the patient’s clinical condition, reduce symptoms, and prevent complications that could compromise orthodontic or future implant-prosthetic treatments.
Author Contributions
Conceptualization, M.M. and F.F.; methodology, M.M.; validation, M.M., N.L., V. D’A.; formal analysis, M.M. and N.L., V. D’A; resources, M.M. and N.L., V. D’A; data curation, N.L., V. D’A, M.M.; writing, M.M., N.L., V. D’A; writing—review and editing, M.M. and N.L., V. D’A; supervision, M.M. and F.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval (number 23, accept date: 8 November 2018) was obtained by the Independent Ethics Committee of Chieti hospital. The study protocol was drawn following the European Union Good Practice Rules and the Helsinki Declaration. The patient provided written informed consent before the beginning of orthodontic and surgical therapies.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study. Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the
corresponding author. The data is not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
Ethical Approval and Informed Consent: This case report was conducted in accordance with the ethical standards of the institutional and national research committee and with the principles outlined in the Declaration of Helsinki. The patient provided written informed consent for the treatment and for the publication of all clinical data, including photographs and radiographs, in an anonymized form.
Abbreviations
The following abbreviations are used in this manuscript:
TMD temporomandibular disorders
| TMJ | temporomandibular joint |
| AEI | articular eminence inclination |
| VAS | visual analogic scale |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| TT | temporalis tendon |
| PES | external pterygoid muscle upper head |
| PEI | external pterygoid muscle lower head |
| PIS | internal pterygoid muscle upper head |
| PII | internal pterygoid muscle lower head |
| MMP | deep masseter muscle |
| MMS | superficial masseter muscle |
| CBCT | Cone Beam Computer Tomography |
| DICOM | Digital Imaging and Communications in Medicine |
| NHP | natural head position |
References
- Wieckiewicz M, Boening K, Wiland P, Shiau YY, Paradowska-Stolarz A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J Headache Pain. 2015;16:106.Epub 2015 Dec 7. [CrossRef] [PubMed] [PubMed Central]
- Warzocha J, Gadomska-Krasny J, Mrowiec J. Etiologic Factors of Temporomandibular Disorders: A Systematic Review of Literature Containing Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) and Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) from 2018 to 2022. Healthcare (Basel). 2024 Feb 29;12(5):575. [CrossRef] [PubMed] [PubMed Central]
- Rawat P, Saxena D, Srivastava PA, Sharma A, Swarnakar A, Sharma A. Prevalence and severity of temporomandibular joint disorder in partially versus completely edentulous patients: A systematic review. J Indian Prosthodont Soc. 2023 Jul-Sep;23(3):218-225. [CrossRef] [PubMed] [PubMed Central]
- Lekaviciute R, Kriauciunas A. Relationship Between Occlusal Factors and Temporomandibular Disorders: A Systematic Literature Review. Cureus. 2024 Feb 13;16(2):e54130. [CrossRef] [PubMed] [PubMed Central]
- Tabatabaei S, Paknahad M, Poostforoosh M. The effect of tooth loss on the temporomandibular joint space: A CBCT study. Clin Exp Dent Res. 2024 Feb;10(1):e845. [CrossRef] [PubMed] [PubMed Central]
- Okeson, Jeffrey P. (2008). Management of temporomandibular disorders an occlusion, 6 Edition. St. Louis, Missouri: Elsevier Health Sciences.
- Chen Y, Luo M, Xie Y, Xing L, Han X, Tian Y. Periodontal ligament-associated protein-1 engages in teeth overeruption and periodontal fiber disorder following occlusal hypofunction. J Periodontal Res. 2023 Feb;58(1):131-142. Epub 2022 Nov 29. [CrossRef] [PubMed]
- Ulay, G., Pekiner, F. N., & Orhan, K. (2020). Evaluation of the relationship between the degenerative changes and bone quality of mandibular condyle and articular eminence in temporomandibular disorders by cone beam computed tomography. CRANIO®, 41(3), 218–229. [CrossRef]
- Zheng H, Shi L, Lu H, Liu Z, Yu M, Wang Y, Wang H. Influence of edentulism on the structure and function of temporomandibular joint. Heliyon. 2023 Sep 23;9(10):e20307. [CrossRef] [PubMed] [PubMed Central]
- Rosado LPL, Barbosa IS, Junqueira RB, Martins APVB, Verner FS. Morphometric analysis of the mandibular fossa in dentate and edentulous patients: A cone beam computed tomography study. J Prosthet Dent. 2021 May;125(5):758.e1-758.e7. Epub 2021 Feb 17. [CrossRef] [PubMed]
- Leal MDCF, Castro MML, Sosthenes MCK. Updating The General Practitioner on The Association Between Teeth Loss and Temporomandibular Disorders: A Systematic Review. Eur J Dent. 2023 May;17(2):296-309. Epub 2022 Dec 27. [CrossRef] [PubMed] [PubMed Central]
- Konishi M, Verdonschot RG, Kakimoto N. An investigation of tooth loss factors in elderly patients using panoramic radiographs. Oral Radiol. 2021 Jul;37(3):436-442. Epub 2020 Aug 18. [CrossRef] [PubMed]
- Craddock HL. Occlusal changes following posterior tooth loss in adults. Part 3. A study of clinical parameters associated with the presence of occlusal interferences following posterior tooth loss. J Prosthodont. 2008 Jan;17(1):25-30. Epub 2007 Oct 8. [CrossRef] [PubMed]
- Wang A, Cao J, Zhang H, Zhang B, Yang G, Hu W, Chung KH. Three-dimensional position changes of unopposed molars before implant rehabilitation: a short-term retrospective cohort analysis. BMC Oral Health. 2022 Dec 3;22(1):562. [CrossRef] [PubMed] [PubMed Central]
- Aldayel AM, AlGahnem ZJ, Alrashidi IS, Nunu DY, Alzahrani AM, Alburaidi WS, Alanazi F, Alamari AS, Alotaibi RM. Orthodontics and Temporomandibular Disorders: An Overview. Cureus. 2023 Oct 15;15(10):e47049. [CrossRef] [PubMed] [PubMed Central]
- Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018 Jan 26;18(1):99-107. [CrossRef] [PubMed]
- Sánchez CAF, Laverde COD, Rodríguez SEN, Gallego GAC, Aristizábal JF, Salazar OIC. Methodology for the correction of a CBCT volume from the skull to the natural head position. MethodsX. 2024 Nov 27;13:103073. [CrossRef] [PubMed] [PubMed Central]
- McKinney R, Olmo H, McGovern B. Benign Chronic White Lesions of the Oral Mucosa. 2024 Jan 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. [PubMed]
- Wadhokar OC, Patil DS. Current Trends in the Management of Temporomandibular Joint Dysfunction: A Review. Cureus. 2022 Sep 19;14(9):e29314. [CrossRef] [PubMed] [PubMed Central]
- Okeson JP, de Leeuw R. Differential diagnosis of temporomandibular disorders and other orofacial pain disorders. Dent Clin North Am. 2011; 55(1): 105-120.
- Voß LC, Basedau H, Svensson P, May A. Bruxism, temporomandibular disorders, and headache: a narrative review of correlations and causalities. Pain. 2024 Nov 1;165(11):2409-2418. Epub 2024 Jun 18. [CrossRef] [PubMed]
- Minakuchi H, Fujisawa M, Abe Y, Iida T, Oki K, Okura K, Tanabe N, Nishiyama A. Managements of sleep bruxism in adult: A systematic review. Jpn Dent Sci Rev. 2022 Nov;58:124-136. Epub 2022 Mar 25. [CrossRef] [PubMed] [PubMed Central]
- Garstka AA, Kozowska L, Kijak K, Brzózka M, Gronwald H, Skomro P, Lietz-Kijak D. Accurate Diagnosis and Treatment of Painful Temporomandibular Disorders: A Literature Review Supplemented by Own Clinical Experience. Pain Res Manag. 2023 Jan 31;2023:1002235. [CrossRef] [PubMed] [PubMed Central]
- Åström M, Thet Lwin ZM, Teni FS, Burström K, Berg J. Use of the visual analogue scale for health state valuation: a scoping review. Qual Life Res. 2023 Oct;32(10):2719-2729. Epub 2023 Apr 7. [CrossRef] [PubMed] [PubMed Central]
- Mitro V, Caso AR, Sacchi F, Gilli M, Lombardo G, Monarchi G, Pagano S, Tullio A. Fonseca's Questionnaire Is a Useful Tool for Carrying Out the Initial Evaluation of Temporomandibular Disorders in Dental Students. Clin Pract. 2024 Aug 26;14(5):1650-1668. [CrossRef] [PubMed] [PubMed Central]
- Szcześniak M, Issa J, Öztürk I, Karahan E, Czajka-Jakubowska A, Orhan K, Dyszkiewicz-Konwińska M. The diagnostic accuracy of cone beam computed tomography in detecting temporomandibular joint bony disorders: a systematic review. Pol J Radiol. 2024 Jun 13;89:e292-e301. [CrossRef] [PubMed] [PubMed Central]
- Wie C, Dunn T, Sperry J, Strand N, Dawodu A, Freeman J, Covington S, Pew S, Misra L, Maloney J. Cognitive Behavioral Therapy and Biofeedback. Curr Pain Headache Rep. 2025 Jan 9;29(1):23. [CrossRef] [PubMed]
- Bergmann A, Edelhoff D, Schubert O, Erdelt KJ, Pho Duc JM. Effect of treatment with a full-occlusion biofeedback splint on sleep bruxism and TMD pain: a randomized controlled clinical trial. Clin Oral Investig. 2020 Nov;24(11):4005-4018. Epub 2020 May 19. [CrossRef] [PubMed] [PubMed Central]
- Alneyadi M, Drissi N, Almeqbaali M, Ouhbi S. Biofeedback-Based Connected Mental Health Interventions for Anxiety: Systematic Literature Review. JMIR Mhealth Uhealth. 2021 Apr 22;9(4):e26038. [CrossRef] [PubMed] [PubMed Central]
- Alfallaj H. Pre-prosthetic orthodontics. Saudi Dent J. 2020 Jan;32(1):7-14. Epub 2019 Aug 27. [CrossRef] [PubMed] [PubMed Central]
- Maspero C, Farronato D, Giannini L, Farronato G. Orthodontic treatment in elderly patients. Prog Orthod. 2010;11(1):62-75. Epub 2010 May 11. [CrossRef] [PubMed]
- Erbe C, Heger S, Kasaj A, Berres M, Wehrbein H. Orthodontic treatment in periodontally compromised patients: a systematic review. Clin Oral Investig. 2023 Jan;27(1):79-89. Epub 2022 Dec 11. [CrossRef] [PubMed] [PubMed Central]
- Macrì M, Medori S, Varvara G, Festa F. A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners. Applied Sciences. 2023; 13(3):1540. [CrossRef]
- Festa F, Capasso L, D'Anastasio R, Anastasi G, Festa M, Caputi S, Tecco S. Maxillary and mandibular base size in ancient skulls and of modern humans from Opi, Abruzzi, Italy: a cross-sectional study. World J Orthod. 2010 Spring;11(1):e1-4. [PubMed]
- Minervini G, Franco R, Marrapodi MM, Crimi S, Badnjević A, Cervino G, Bianchi A, Cicciù M. Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis. J Clin Med. 2023 Apr 2;12(7):2652. [CrossRef] [PubMed] [PubMed Central]
- Häggman-Henrikson B, Ali D, Aljamal M, Chrcanovic BR. Bruxism and dental implants: A systematic review and meta-analysis. J Oral Rehabil. 2024 Jan;51(1):202-217. Epub 2023 Aug 17. [CrossRef] [PubMed]
Figure 1.
(a) right view, (b) left view, (c) frontal view, (d) upper view, (e) lower view, (f) bite marks and ulcer caused by the clenching on buccal mucosa.
Figure 1.
(a) right view, (b) left view, (c) frontal view, (d) upper view, (e) lower view, (f) bite marks and ulcer caused by the clenching on buccal mucosa.

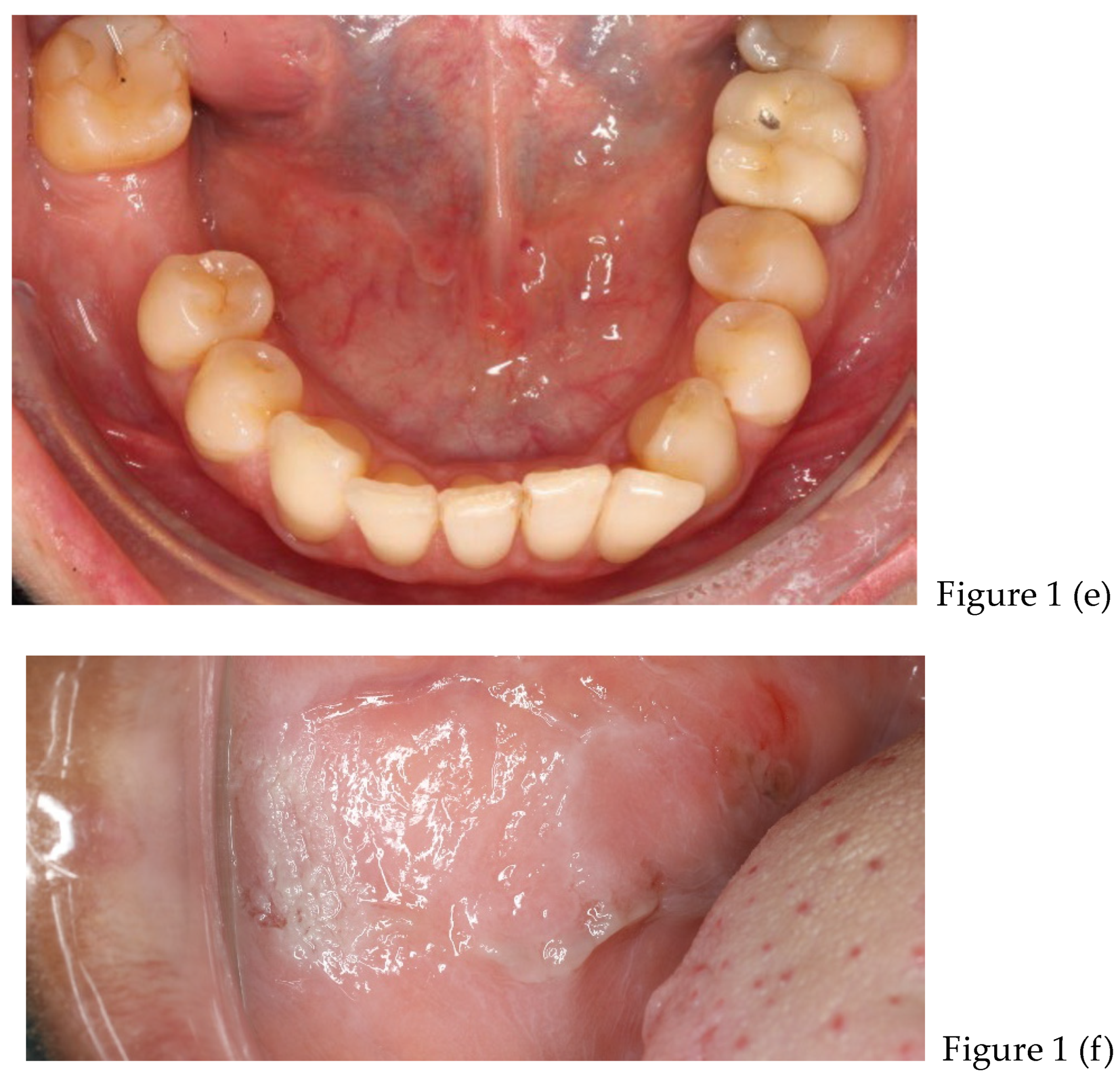
Figure 2.
(a) frontal view, (b) sagittal view, (c) bottom view.
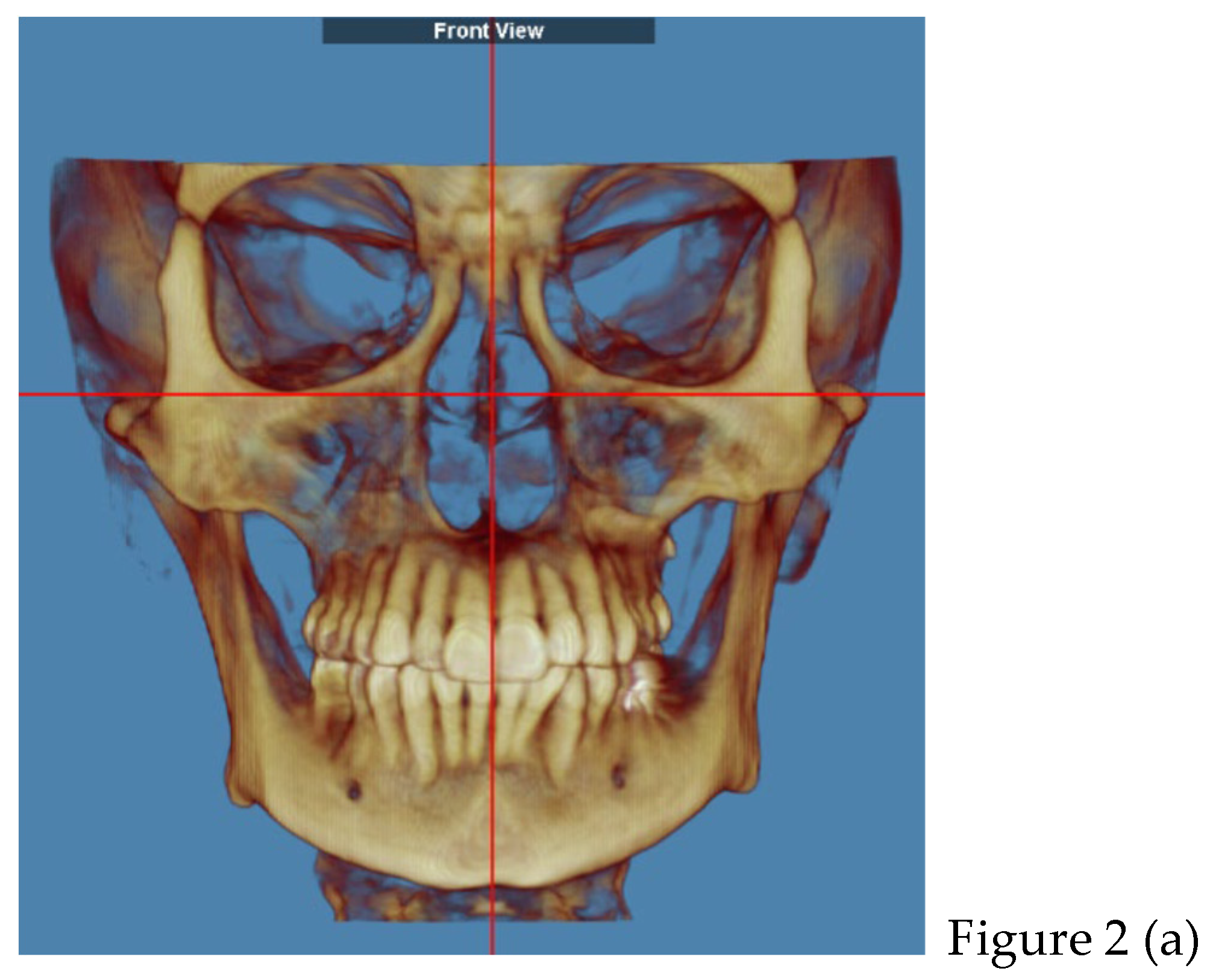
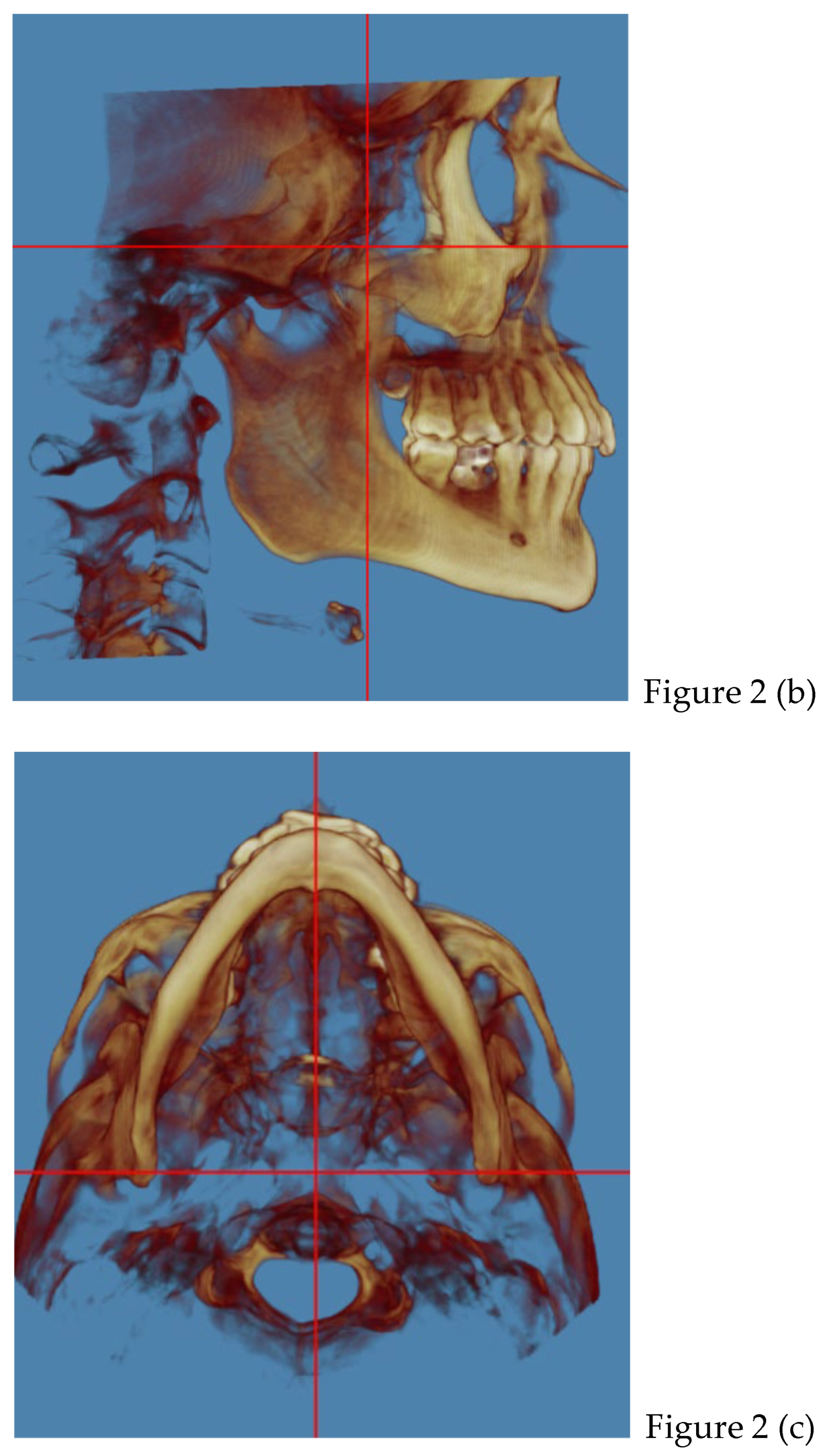
Figure 3.
(a) orthopantomography; (b) lateral teleradiograph; (c) TMJ right and left. Both condyles slightly flattened and the right one displaced posteriorly in the glenoid cavity; (d) Frontal view. (e) Submental vertex lower; (f) Submental vertex upper.
Figure 3.
(a) orthopantomography; (b) lateral teleradiograph; (c) TMJ right and left. Both condyles slightly flattened and the right one displaced posteriorly in the glenoid cavity; (d) Frontal view. (e) Submental vertex lower; (f) Submental vertex upper.
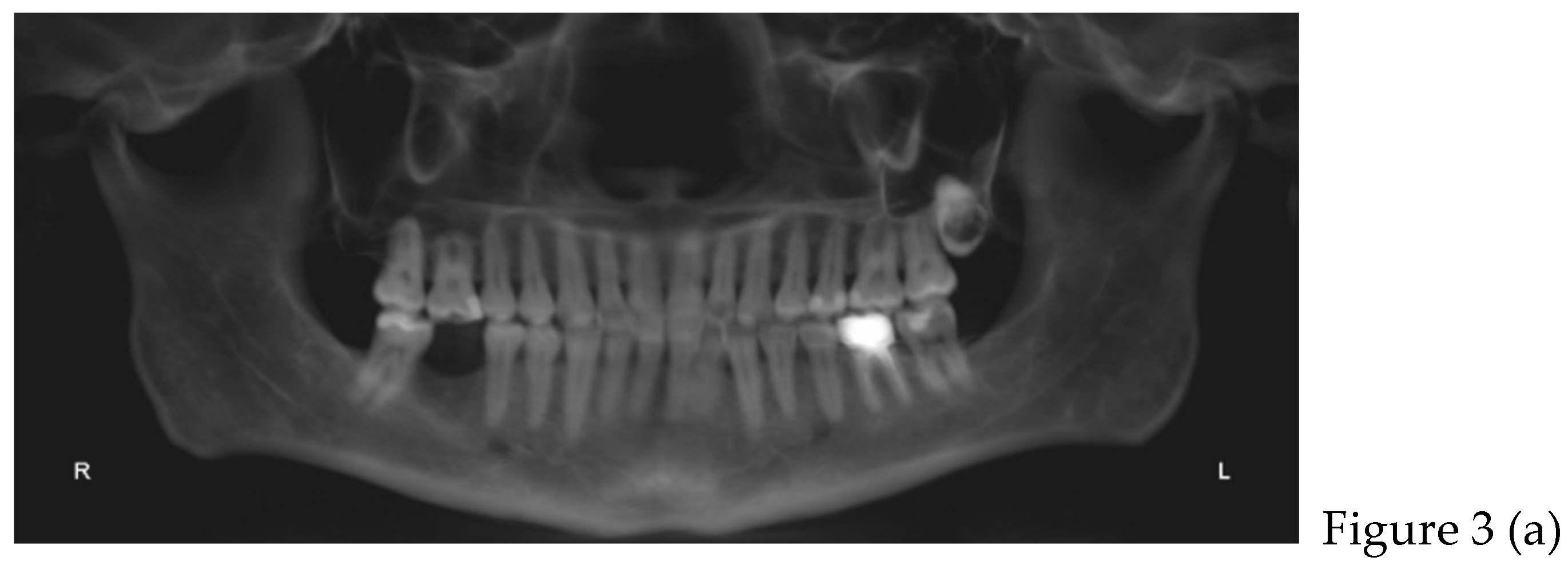
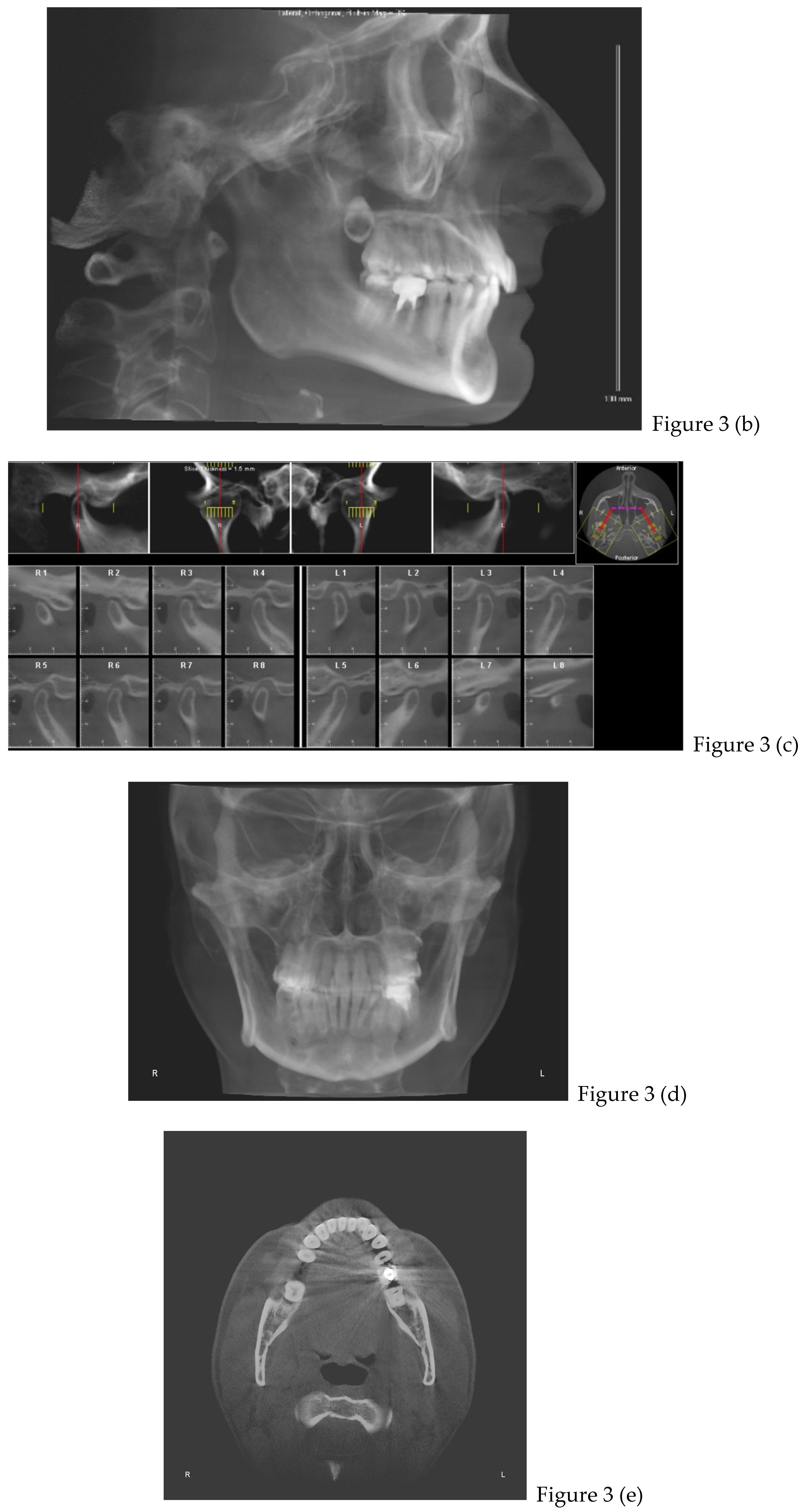
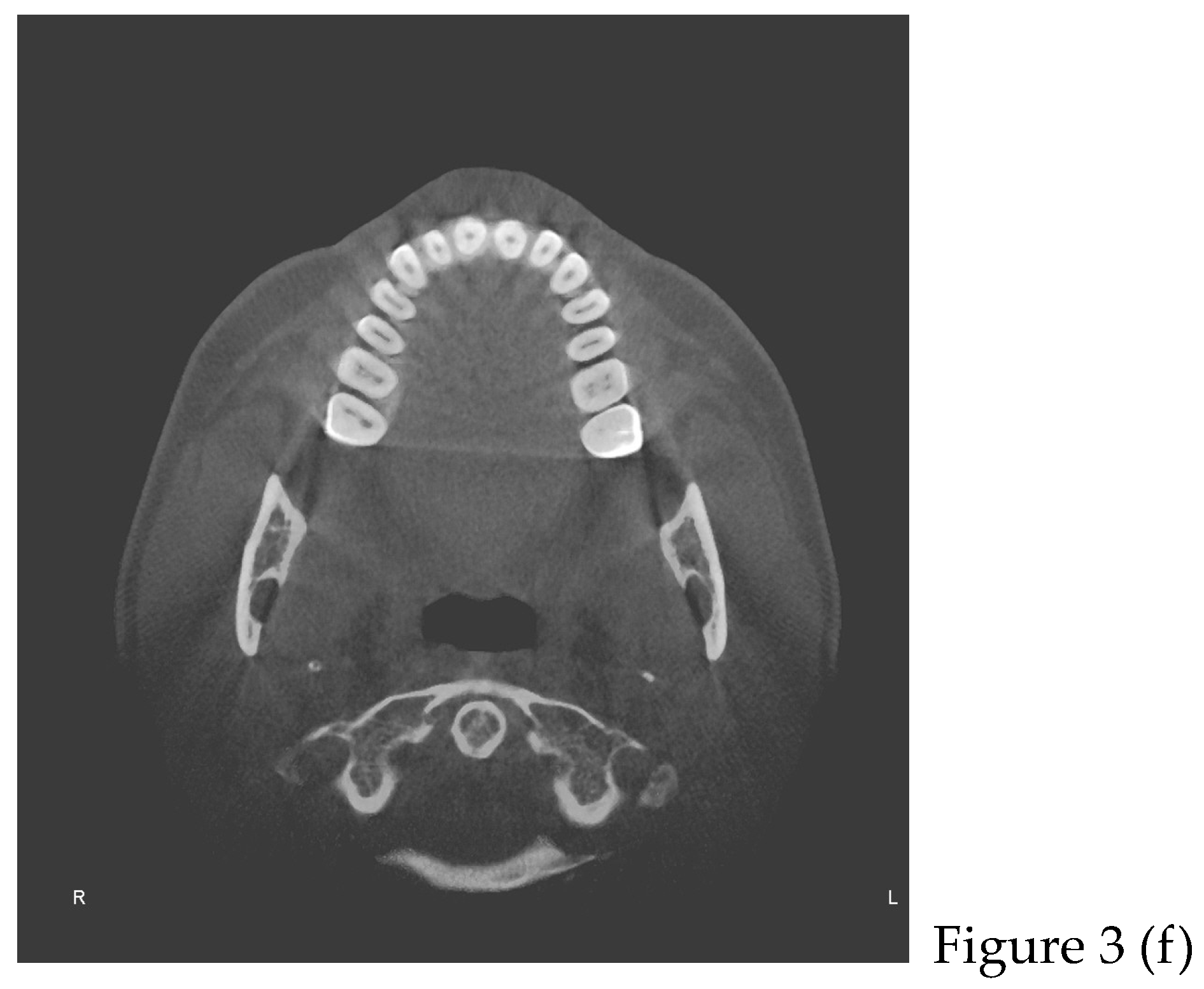
Figure 5.
difference in length of masseter muscles; (a) before therapy, (b) after therapy.
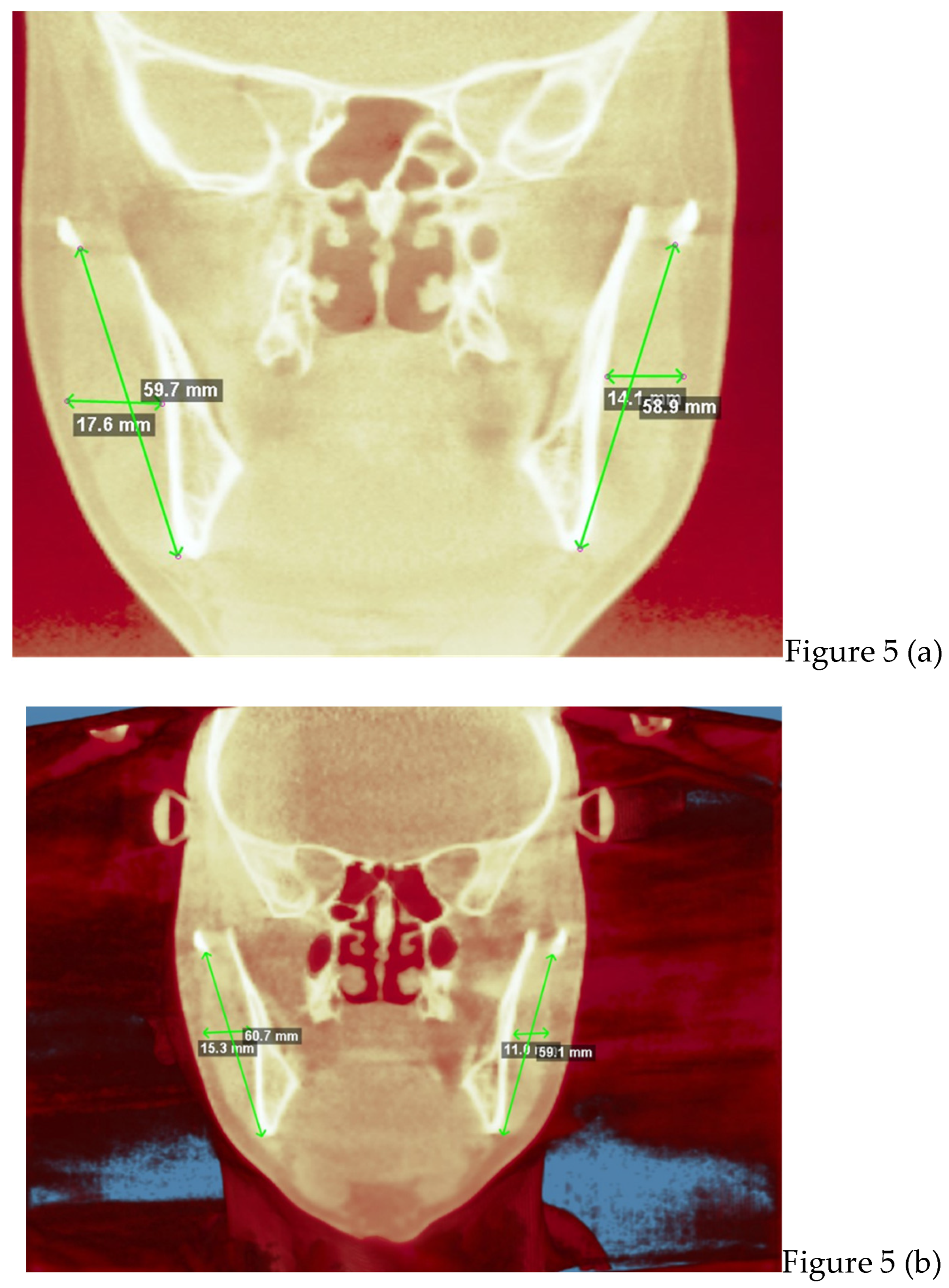
Figure 10.
(a) first CBCT, cervical straightening before therapy; (b) second CBCT, acquisition of normal cervical lordosis after orthodontic therapy.
Figure 10.
(a) first CBCT, cervical straightening before therapy; (b) second CBCT, acquisition of normal cervical lordosis after orthodontic therapy.
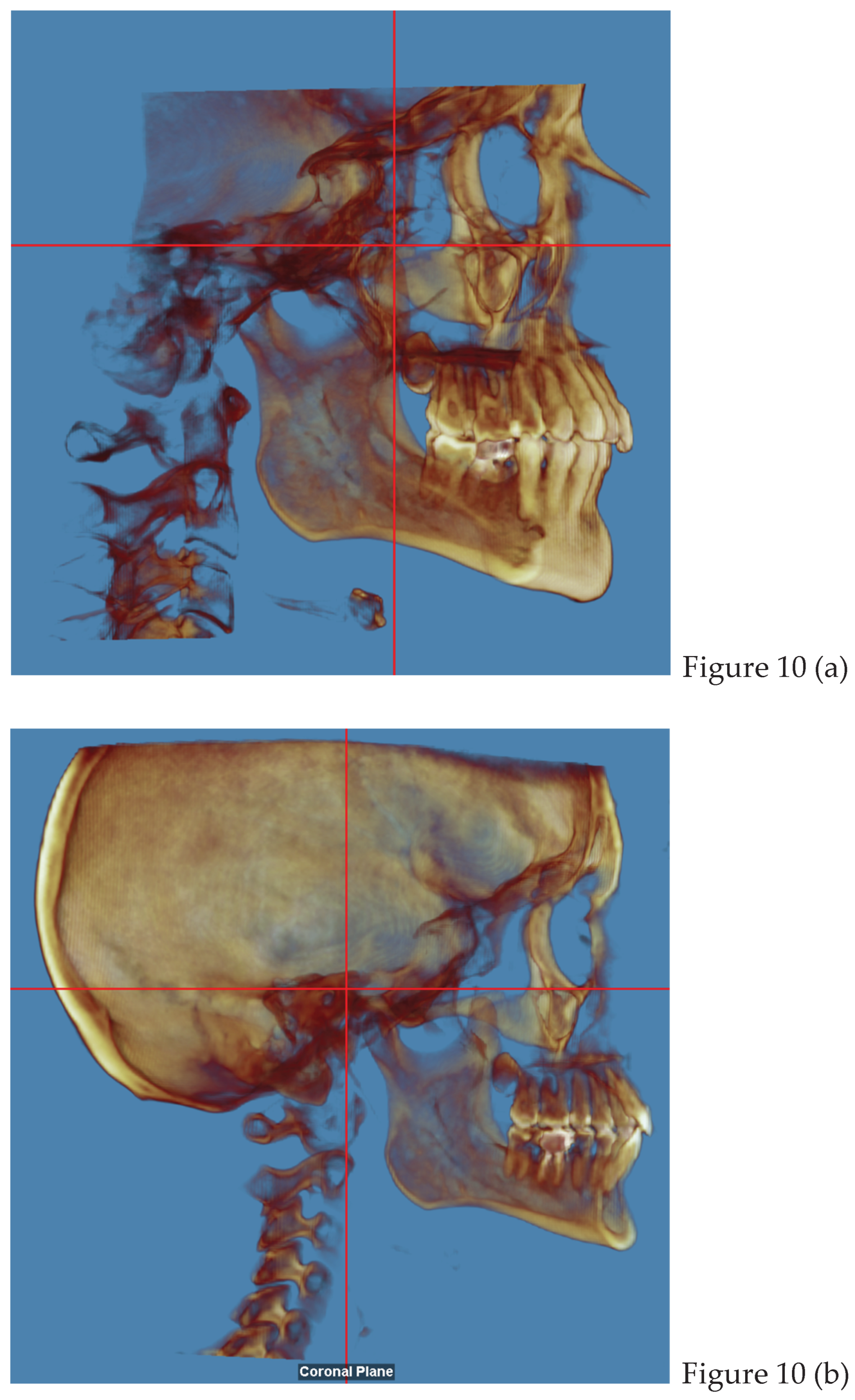

Table 1.
workflow sequence.
| FIRST VISIT | OPERATIVE WORKFLOW |
| general anamnesis | |
| dental anamnesis | |
| gnathological questionnaire | |
| muscles palpation (pain level 3) | |
| VAS (pain level 8) | |
| CBCT (t0) | |
| preliminary photos | |
| DIAGNOSIS | tension type headaches with cleanching |
| GNATOLOGICAL THERAPY | upper and lower splint + biofeedback exercise |
| monthly folow up | |
| after 2 months | VAS (pain level 5) |
| muscles palpation (pain level 2) | |
| after 5 months | VAS (pain level 2) |
| muscles palpation (pain level 1-0) | |
| 6 month | no variations/ STABILITATION |
| ORTHODONTIC THERAPY | use of 30 pairs of clear aligners (15 days each couples) |
| after 1 year | refinement with 15 pairs of clears aligners (use 15 days each couples) |
| after 8 months | Retainers + CBCT (t1) + final photos |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



