Submitted:
17 July 2025
Posted:
18 July 2025
You are already at the latest version
Abstract
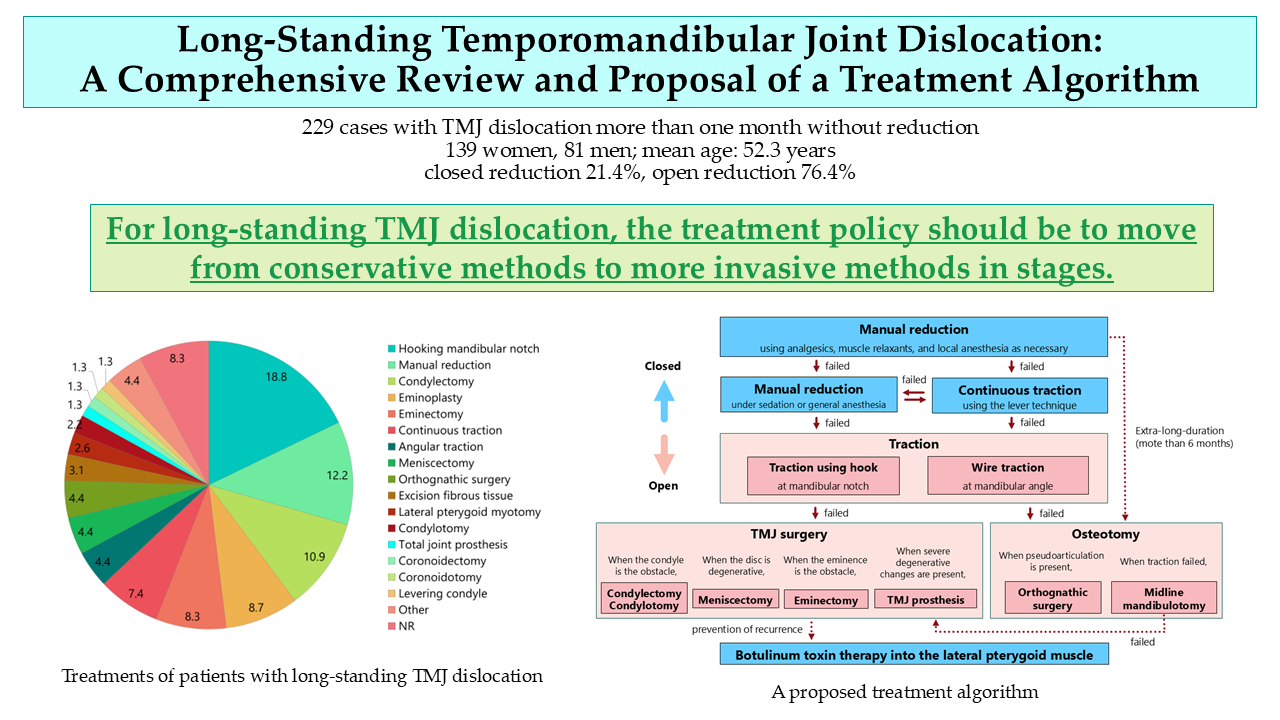
Background and Objectives: Longstanding or protracted temporomandibular joint dislocation refers to a condition that persists for more than 1 month without reduction. To elucidate the clinical characteristics and treatment results of this entity, this comprehensive review analyzed the data on this condition. Materials and Methods: Studies were assessed using electronic medical databases or manual searches from their inception until December 31, 2024. Results: Overall, 229 cases (139 women and 81 men; mean age, 52.3 years) from 113 reports were assessed. The proportion of patients with bilateral and unilateral dislocations was 72.5% and 8.7%, respectively. The mean duration after dislocation was 11.9 months. Closed and open reductions were possible in 49 (21.4%) and 175 (76.4%) patients, respectively. The mean dislocation duration was significantly (p = 0.001) shorter in patients who underwent closed reduction (4.9 months) than in those who underwent open reduction (14.8 months). Conclusions: Clinically, it is crucial to diagnose and treat the condition early and prevent it from becoming chronic. However, for cases of long-standing dislocations due to other, more serious diseases, conservative treatments such as manual reduction and continuous elastic traction should be attempted first. If the reduction fails, surgical treatment should be considered as an alternative.
Keywords:
temporomandibular joint dislocation
; long-standing
; protracted
; chronic
; reduction
; treatment
; surgery
; algorithm
1. Introduction
Dislocation of the temporomandibular joint (TMJ) refers to displacement of the mandibular condylar head from its normal position in the glenoid fossa. Dislocation is not a rare event, with an estimated incidence of 2.5–25 per 100,000 persons per year [1,2]. Dislocations can be classified as anterior, posterior, medial, lateral, and superior [3]. Anterior dislocations are most commonly observed, while dislocations in posterior, medial, and lateral directions are less frequent. A systematic review of TMJ dislocations indicated 79 acute, 35 chronic, and 311 recurrent cases [3].
The first recorded manual reduction of TMJ dislocations was described in the Edwin Smith Papyrus, dating back to the 17th century BC [4]. Edwin Smith Papyrus is a record of a surgical procedure translated into English in 1930 [4]. This reduction method is not significantly different from the current reduction method. Hippocrates also reported the method for anterior dislocations in the Hippocrates Corpus in the 5th century BC, which remains widely used today as the Hippocratic method. The Hippocratic method is the most well-known technique for the manual reduction of anterior dislocation. The physician places the thumb laterally next to the teeth and other fingers on the lower surface of the mandible and applies pressure first caudally and then dorsally [1].
Recently, consensus and evidence-based recommendations for the management of anterior condylar dislocations were published by the European Society of Temporomandibular Joint Surgeons [2]. According to these recommendations, manual reduction should be attempted initially using the Hippocratic method. If the attempt proves unsuccessful, further attempts should be made with medication (muscle relaxants and/or analgesics) and, if necessary, under sedation or general anesthesia [2]. Securing methods should be considered in patients with recurrent, long-standing, and/or habitual dislocations. Nonsurgical methods should be exhausted before attempting minimally invasive or open surgical interventions [2]. Botulinum toxin for the treatment of recurrent dislocation [5,6] should be considered as a potential therapeutic option for recurrent dislocations. Indications for open surgical treatment [7,8,9] should be established only after the failure of conservative treatments and/or minimally invasive therapy for anterior TMJ dislocation [2].
Terms such as chronic, protracted, long-standing, prolonged, and permanent have been used to describe long-term, untreated TMJ dislocations. In this review, the author employs the term "long-standing." No consensus exists regarding the duration after which an untreated dislocation should be considered long-standing. However, as most reports specify 1 month or more, this review adopts this definition.
Although consensus has been reached regarding the treatment of anterior TMJ dislocation, the incidence of long-standing dislocation is significantly lower than that of acute dislocation, and no consistent treatment method has been established. Therefore, this review comprehensively analyzes all available reports of long-standing dislocation regarding causes, symptoms, treatment, and clinical course, and proposes a treatment algorithm for long-standing TMJ dislocation.
2. Materials and Methods
2.1. Literature Review
The literature search strategy was based on comprehensive electronic medical literature databases using the keywords (“long-standing” OR “chronic” OR “protracted” OR “prolonged” OR “permanent” OR “irreducible” OR “unreduced” OR “persistent”) AND (“temporomandibular joint” OR “mandible” OR “condyle” OR “mandibular condyle”) AND (“dislocation” OR “luxation”) AND (“reduction” OR “treatment” OR “management” OR “approach”). Furthermore, a manual search was performed for articles cited in related resources. Reports identified in these databases or via a manual search without language restrictions up to December 31, 2024, were screened as described previously [10,11]. The inclusion criteria were reports of cases in which TMJ dislocations were not reduced for more than 1 month and described fundamental information such as sex, age, etiology, clinical presentation, and treatment. Duplicate reports of the same case, reports without certain diagnostic imaging findings, records with missing data, and those that were irrelevant to the purpose of the study were excluded. All reports were assessed for eligibility and reviewed by the authors.
2.2. Analysis
Fundamental clinical data, such as age, sex, affected side, etiology, chief complaint, diagnostic imaging, duration of dislocation, maximal mouth opening, open bite, treatment, complications, follow-up, and sequelae, were extracted and evaluated from the selected studies.
2.3. Statistics
Age, sex, and dislocation duration were analyzed using binomial logistic regression analysis to determine potential indicators that could be used to select treatments (closed versus open procedures). Two-tailed unpaired t-test and Mann-Whitney U tests were used to evaluate the differences between groups. The ratio of closed and open reduction was analyzed in six groups: 1 month or more but less than 2 months after dislocation, 2 months or more but more than 3 months, 3 months or more but less than 4 months, 4 months or more but less than 5 months, 5 months or more but less than 6 months, and 6 months or more after dislocation. The difference in duration after dislocation was analyzed between cases with closed reduction and those with open reduction using the Mann-Whitney U test. The etiology was classified as traumatic (e.g., trauma, fall, motor vehicle accident) or atraumatic (e.g., yawning, dental treatment), and differences were analyzed using an unpaired t-test. All analyses were conducted using the SPSS statistical software package for Windows (version 24.0; SPSS Japan Inc., Tokyo, Japan). The null hypothesis was rejected at the 5% significance level (p < 0.05).
3. Results
The number of studies retrieved from the electronic databases and registers, assessed for eligibility, and included in the systematic review are presented in a flow diagram (Figure 1). Overall, 19,604 records were retrieved from the following databases: PubMed (313), Google Scholar (19,100), Japan Medical Abstracts Society (41), and J-Stage (150). Forty-two additional records were retrieved through manual searches of relevant papers and books. The search yielded 113 reports [12-124]. Table S1 shows the demographic data of all patients. The number of evaluated reports, categorized by the original language, was as follows: English, 74; Japanese, 34; German, four; and French, one. The number of reports according to the number of cases was as fo[12–124llows: one case, 83; two cases, 13; three cases, seven; four cases, two; five cases, one; six cases, one; eight cases, two; 10 cases, one; 15 cases, one; 19 cases, one; and 20 cases, one. All the studies were case reports or case series.
3.1. Demographic Data and Diagnoses
The 113 articles included 229 patients (mean age ± standard deviation, 52.3 ± 19.5 years; range, 5–89 years) (Table S1). The demographic data and diagnostic results are summarized in Table 1. The study included 139 women (60.7%) and 81 men (35.4%). Among these cases, 171 (72.5%), 11 (4.7%), and nine (3.8%) were bilateral, left-sided, and right-sided, respectively (Table 1). The mean dislocation duration was 11.9 months (Table 1).
The first clinical diagnosis was TMJ dislocation in 100 cases (43.7%). Additionally, 39 (17%), four (1.7%), four (1.7%), and three cases were undiagnosed and presented palsy, inflammation, and neurological diseases, respectively (Table 1, Figure 2).
Previous dislocation was reported once, frequently, and sometimes in 14 (6.1%), six (2.6%), and three (1.3%) cases, respectively (Table 1). Moreover, there were 37 patients (16.2%) with no history of dislocation; however, no previous dislocation was recorded in 169 patients (73.8%).
Psychiatric diseases identified based on anamnesis included dementia or mental retardation, neurological diseases, cerebral infarction, cerebral hemorrhage, and brain injury in 19 (8.3%), 15 (6.6%), 10 (4.4%), 10 (4.4%), nine (3.9%), and four (1.7%) patients, respectively. No relevant neurological or psychiatric history was identified in 121 patients (52.8%) (Table 1
3.2. Symptoms and Etiology
Patient symptoms are summarized in Table 2. The most frequent chief complaints were preauricular pain (25.8%), inability to close the mouth (18.6%), masticatory disturbance (13.6%), and difficulty in speaking (10.2%) (Table 2).
The mean maximum mouth opening at the first visit was limited to 24.6 mm. The open bite was 14.4 mm; however, it was reported in only 11.4% of the patients (Table 2).
The percentages corresponding to each etiology in all patients are shown in Figure 3. The most prevalent etiologies were yawning (14.4%, n = 33), surgery (8.3%, n = 19), and neurological diseases (6.6%, n = 15). In 23 patients (10%), the etiologies were unknown, and 69 cases (30.1%) were not recorded (Table 2, Figure 3).
Cases with traumatic etiology (n = 41) were significantly (p = 0.001) younger than those with atraumatic etiology (n = 72) (39.2 ± 17 years vs. 51.3 ± 39.2 years).
3.3. Treatments and Sequelae
Table S2 shows the results of the treatment, complications, follow-up, and sequelae in all patients. Table 3 summarizes the treatments of these cases. Local anesthesia, sedation, and general anesthesia were administered in 18 (7.9%), 51 (22.3%), and 189 (82.5%) cases, respectively (Table S2). Continuous traction using splints or wires was attempted in 29 patients (12.7%); however, it was successful without an open procedure in 17 patients (7.4%) (Table 3). Closed manual reduction was attempted in 183 patients (79.7%) and was successful in 28 (12.2%) (Table 3). Of these, 22, five, and one were performed under general anesthesia, local anesthesia, and sedation, respectively.
Closed and open reduction were possible in 49 (21.4%) and 175 (76.4%) cases, respectively (Table 3 and Table S1). Surgical procedures included Hooking mandibular notch (18.8%), condylectomy (10.9%), eminoplasty (8.7%), eminectomy (8.3%), angular traction (4.4%), meniscectomy (4.4%), orthognathic surgery (4.4%), excision of fibrous tissue (3.1%), lateral pterygoid myotomy (2.6%), condylotomy (2.2%), total TMJ prosthesis (1.3%), coronoidectomy (1.3%), coronoidotomy (1.3%), and levering condyle (1.3%) (Table 3, Figure 5).
Regarding the approach conducted during the surgical procedure, a preauricular incision (46.7%) was the most frequent, followed by submandibular (10.5%) and zygomatic arch incisions (Table 3).
Treatment complications included facial nerve paralysis (6.9%) and redislocation (2.6%). No complications were observed in 77 patients (66.4%, Table 4). Intermaxillary fixation after reduction was performed in 122 patients (53.3%) for a mean duration of 17.5 days (Table 4). The mean follow-up period was 11.8 months, ranging from 2 weeks to 96 months [99], and was not reported in 82 patients (35.8%). At follow-up, the maximal mouth opening 36.2 mm (Table 4). Sequelae included redislocation (1.7%)%), deviation (1.3%), and condylar absorption (0.9%). No sequelae were observed in 55.9% of patients, and data were not reported for 69 patients (30.1%; Table 4).
Closed reduction was possible in more than 40% of cases within a 3-month duration; nonetheless, open reduction was required in more than 80% of cases after 4 months or more (Figure 6).
The mean age of patients who underwent closed and open reduction was 55.4 and 51.0 years, respectively, with no significant difference (p = 0.163, unpaired t-test). However, the time from dislocation to reduction was significantly shorter in patients treated with closed reduction than in those who required open reduction (4.9 ± 7.3 vs. 14.8 ± 40.4 months, respectively; p = 0.001, Mann–Whitney U test) (Figure 7).
Although age, sex, and dislocation duration were analyzed using binomial logistic regression analysis to detect potential indicators that could be used to decide treatments (closed vs. open procedures), no significant factors were identified.
4. Discussion
This represents the first comprehensive review of existing reports on long-standing TMJ dislocations. The clinical courses of 229 patients with long-standing TMJ dislocation that remained unreduced for more than one month were analyzed in this review. Although early diagnosis and treatment of TMJ dislocation remain the primary priorities, treatment is often delayed due to various factors. In cases involving dementia, mental retardation, or unconsciousness, patients themselves cannot recognize the dislocation; therefore, medical and dental professionals must detect and diagnose it as early as possible. In cases of long-standing dislocation, treatment should proceed systematically, beginning with manual reduction before considering surgical options. However, no consensus exists regarding treatment policy or algorithm, which remains a significant challenge for future research.
4.1. Etiology of Long-Standing TMJ Dislocation
Reasons for TMJ dislocations remaining untreated for more than 1 month included patients being unaware of the dislocation due to dementia, impaired consciousness, or intellectual disability; edentulous patients not wearing dentures, making occlusal changes less apparent; postponement of TMJ dislocation treatment due to more serious life-threatening conditions; or patients not seeking medical attention, remaining undiagnosed, or being misdiagnosed (Table S1). This review revealed that the most prevalent etiologies of long-standing dislocations were yawning (14.4%), surgery (8.3%), neurological diseases (6.6%), and unknown causes (10%) (Figure 2). In contrast, the common etiologies of superior condyle dislocation include motor vehicle accidents (50%), falls (20.7%), bicycle accidents (16.4%), and assault (3.4%) [11]. Compared with superior dislocations, the rate of traumatic etiology is notably lower. Long-standing TMJ dislocations can occur during routine movements such as yawning, and many cases have unknown or unspecified causes. They may result from minimal mouth opening beyond the normal range and often go unnoticed. Consequently, dislocations tend to recur during everyday movements without trauma. If the dislocation remains unrecognized due to dementia, mental retardation, psychiatric or neurological diseases, or unconsciousness, it can readily progress to a long-standing condition. In this study, patients with traumatic etiology (n = 41) were significantly younger than those with atraumatic etiology (n = 72) (39.2 years vs. 51.3 years) (Figure 4). In several cases, diagnosis or treatment of dislocations is delayed due to concurrent life-threatening injuries or conditions. Patient age, presence of neurological symptoms, and etiology may influence treatment decisions and outcomes.
When dislocation persists for extended periods, pseudoarticulation (nearthrosis) rarely develops in patients with long-standing dislocation. Although lateral excursion becomes difficult, patients can maintain a certain degree of function. To date, six cases of pseudoarticulation associated with long-standing TMJ dislocation have been reported [44,72,92,99,107,114].
Medical and dental professionals, as well as caregivers, should remain vigilant for dislocations in patients who cannot recognize abnormalities independently. Fortunately, recent advances in botulinum toxin therapy have eliminated the need for surgical treatment of habitual TMJ dislocation when botulinum therapy is administered to the lateral pterygoid muscle following manual reduction [6,125]. If TMJ dislocation can be detected and treated promptly, long-standing dislocation can be prevented, surgical treatment for TMJ dislocation will become largely unnecessary, and significant surgical intervention can be avoided [6].
4.2. Diagnosis of Long-Standing TMJ Dislocation
Generally, diagnosis is straightforward based on clinical signs. Symptoms of bilateral TMJ dislocation include anterior mandibular protrusion, facial elongation, loss of both nasolabial folds, and preauricular depression with anterolateral prominence. Difficulty closing the mouth additionally leads to drooling, impaired speech and pronunciation, and compromised chewing and swallowing. In unilateral dislocation, all these symptoms manifest on one side, with mandibular deviation to the unaffected side and crossbite. Radiography remains the primary diagnostic imaging modality. Before 1900, radiography was rarely used to diagnose TMJ dislocations; therefore, reports from before 1900 were excluded from this review. When surgical procedures for the TMJ are necessary, MRI or CT may provide valuable diagnostic information.
In most cases, early anterior TMJ dislocations can be reduced manually with relative ease [2]. However, if left untreated for more than 1 month, the likelihood of successful manual reduction decreases substantially, and the probability of requiring surgical procedures increases (Figure 5). Therefore, early detection, diagnosis, and treatment of TMJ dislocations are crucial. Nevertheless, many medical professionals remain unfamiliar with TMJ dislocations. This review reveals that numerous cases have progressed to chronicity due to missed diagnosis or misdiagnosis (Figure 2). When mouth closure or swallowing becomes difficult and mouth breathing becomes necessary, the risk of aspiration pneumonia increases. Various neurological diseases cause involuntary contractions of the masticatory muscles, particularly the lateral pterygoid muscle [6,126,127,128]. Aspiration pneumonia represents the most common cause of death in many neurological diseases, and untreated TMJ dislocation may contribute significantly to mortality in some cases. Oral surgeons and dentists with TMJ expertise should educate physicians, nurses, and other medical professionals about TMJ dislocations.
4.3. Treatment of Long-Standing TMJ Dislocation
Early diagnosis and treatment are essential for managing TMJ dislocation; however, when dislocation becomes long-standing, treatment should progress gradually from non-invasive to invasive methods. Manual reduction (utilizing analgesics, muscle relaxants, and local anesthesia as needed), manual reduction under sedation or general anesthesia, and continuous elastic traction using the lever technique should be attempted initially. Continuous traction using splints or wires was attempted in 12.7% of cases; however, it achieved success without open procedures in only 7.4% of cases (Table 3). Closed manual reduction proved successful in 12.2% of patients (Table 3). Closed reduction was achievable in more than 40% of cases within 3 months of dislocation; however, open reduction was required in more than 80% of cases after 4 months or longer (Figure 6). Furthermore, the duration since dislocation in cases where closed reduction was achievable was significantly shorter than in cases requiring open reduction (4.9 vs. 14.8 months) (Figure 6).
Reports exist of closed reduction even in cases of prolonged dislocation. Caminiti & Weinberg [72] reported successful manual reduction under general anesthesia of a unilateral TMJ dislocation that had persisted for 2 years. Ogawa et al. [97] successfully performed conservative reduction through lever action using a resin splint in a case of long-standing dislocation persisting for 3 years and 5 months. Therefore, closed reduction appears feasible even in cases of extra-long-standing dislocation persisting beyond 6 months. Nonetheless, when reduction proves impossible through conservative methods, surgical procedures must be considered. Here, surgical procedures included hook placement at the mandibular notch (18.8%), condylectomy (10.9%), eminoplasty (8.7%), eminectomy (8.3%), angular traction (4.4%), meniscectomy (4.4%), orthognathic surgery (4.4%), excision of fibrous tissue (3.1%), lateral pterygoid myotomy (2.6%), condylotomy (2.2%), total TMJ prosthesis (1.3%), coronoidectomy (1.3%), coronoidotomy (1.3%), and condylar levering (1.3%) (Table 3, Figure 4). The Fink method involves placing a hook at the mandibular notch. A strong steel hook is inserted over the mandibular notch, and force is applied in downward and backward directions to reduce the displaced condyle. McGraw introduced this method in 1899 [129].
Condylectomy, condylotomy, or craniotomy should be considered as alternatives when manual reduction proves unfeasible due to bone adhesion. Gottlieb recommended condylectomy as a surgical procedure for long-standing TMJ dislocation, as this technique is often necessary to prevent ankylosis [22]. Mazzoni first employed this method to treat long-standing TMJ dislocations in 1877 [129].
While eminectomy or eminoplasty has been applied primarily for habitual TMJ dislocation [130,131,132], both eminectomy [52,55,58,59,67,72,98,99,101,106,108,110,116,119] and eminoplasty [66,68,69,85,111,117] have also been utilized for long-standing dislocations.
Mandibulotomy enables independent movement of each condyle, thereby eliminating resistance on the contralateral side [82,90,105]. Although no such cases have been reported, if reduction remains unsuccessful using this technique due to severe fibrous or bony adhesions around the TMJ, an approach to the TMJ might become necessary. The mandibular swing procedure utilizing midline mandibulotomy has been successfully employed to access oral and oropharyngeal tumors. The advantage of midline mandibulotomy lies in preventing surgical exposure of the bilateral TMJs, facial scarring, and nerve injuries. Potential complications are lingual hematoma, damage to proximal root apices, malocclusion, and nonunion [90]. Reports remain limited, and appropriate case selection requires careful consideration.
Orthognathic surgery is considered appropriate when closed reduction proves impossible, more than 6 months have elapsed since dislocation, and oral function remains maintained to a certain degree with the condyle in a dislocated position [20,36,44,67,81,103,114,124].
TMJ prostheses are gaining increasing popularity and were applied in five cases across four reports included in this review [51,92,113,114]. A recent systematic review concluded that TMJ prostheses should be reserved for cases with severe persistent pain, bony or fibrous ankylosis, or osteomyelitis following primary closed or open management of mandibular condyle fractures [133].
Although lateral pterygoid muscle myotomy has been employed for recurrent or long-standing dislocations in several reports [12,73,107,116,134,135,136], botulinum toxin therapy may render myotomy largely unnecessary [11,126].
Following successful reduction, intermaxillary fixation is necessary to maintain occlusion and prevent recurrent dislocation. Intermaxillary fixation after reduction was performed in 71 patients (61.2%) with a mean duration of 17.5 days (Table 4). Redislocation has been reported by several researchers [36,58,74,87,108].
4.4. Limitations and Future Directions
Follow-up data were not described for 35.8% of patients. The mean follow-up period was only 11.8 months. Future research requires sufficient longitudinal follow-up to determine postoperative sequelae. Further investigation, including larger case series, is necessary to properly analyze significant factors affecting outcomes. No significant factors were identified through binary logistic analysis; apparently, no general treatment policy existed, and treatment was implemented at the discretion of the attending physician. The author proposes an algorithm for managing and treating long-standing TMJ dislocations (Figure 8) based on this review's results, previously suggested algorithms [84,90,99], and the author's personal experience. Nevertheless, neither general consensus nor sufficient evidence currently exists due to this condition's rarity. Diagnostic delays can significantly influence the choice between closed and open treatment strategies. Therefore, prompt diagnosis remains indispensable to ensure minimally invasive procedures and avoid long-term sequelae. Thus, developing and refining a management and treatment algorithm for long-standing dislocations represents an unmet need in the medical field.
5. Conclusions
Early diagnosis and treatment of TMJ dislocation remain essential to significantly reduce progression to chronic dislocation and avoid surgical intervention. TMJ specialists should educate medical professionals about TMJ dislocations and increase awareness. For long-standing TMJ dislocations, the treatment approach should advance from conservative to more invasive methods in progressive stages.
Supplementary Materials
The following information can be downloaded from www.mdpi.com/xxx/s1: Table S1. Demographic data and patient symptoms. Table S2. Treatment and follow-up data for all patients.
Funding
This work was supported by JSPS KAKENHI (Grant Number JP22K10091).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Ms. Kumiko Yasui (Library of Kyoto Medical Center) for collecting the literature.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BC | Before Christ |
| MRI | magnetic resonance imaging |
| NR | Not reported |
| SD | Standard deviation |
| TMJ | Temporomandibular joint |
References
- Neff, A.; Hell, B.; Kolk, A.; Pautke, C.; Schneider, M.; Prechel, U. S3 Leitlinie Kiefergelenkluxation; AWMF Registernummer 007-063; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V.: Berlin, Germany, 2016. [Google Scholar]
- Neff, A.; McLeod, N.; Spijkervet, F.; Riechmann, M.; Vieth, U.; Kolk, A.; Sidebottom, A.J.; Bonte, B.; Speculand, B.; Saridin, C.; et al. The ESTMJS (European Society of Temporomandibular Joint Surgeons) consensus and evidence-based recommendations on management of condylar dislocation. J. Clin. Med. 2021, 10, 5068. [Google Scholar] [CrossRef]
- Akinbami, B.O. Evaluation of the mechanism and principles of management of temporomandibular joint dislocation. Systematic review of literature and a proposed new classification of temporomandibular joint dislocation. Head Face Med. 2011, 7, 10. [Google Scholar] [CrossRef]
- Adams, F. The genuine works of Hippocrates. Translated from the Greek with a Preliminary Discourse and Annotations. Vol. 2, New York, William Wood and Company, 1886,pp107. https://www.google.co.jp/books/edition/The_Genuine_Works_of_Hippocrates/6BAWAAAAYAAJ?hl=ja &gbpv=1&dq=The+genuine+works+of+HIPPOCRATES,+Vol+2&printsec=frontcover.
- Daelen, B.; Thorwirth, V.; Koch, A. Neurogene Kiefergelenkluxation. Definition und Therapie mit Botulinumtoxin. Nervenarzt 1997, 68, 346–350. [Google Scholar] [CrossRef]
- Yoshida, K. Botulinum neurotoxin injection for the treatment of recurrent temporomandibular joint dislocation with and without neurogenic muscular hyperactivity. Toxins 2018, 10, 174. [Google Scholar] [CrossRef] [PubMed]
- Shorey, C.W.; Campbell, J.H. Dislocation of the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, T.; Hidaka, Y.; Murakami, K.-I.; Nishida, M. Chronic recurrent anterior luxation of the mandible: A review of 12 patients treated by the LeClerc procedure. Int. J. Oral Maxillofac. Surg. 1988, 17, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Undt, G.; Kermer, C.; Piehslinger, E.; Rasse, M. Treatment of recurrent mandibular dislocation, part I: Leclerc blocking procedure. Int. J. Oral Maxillofac. Surg. 1997, 26, 92–97. [Google Scholar] [CrossRef]
- Yoshida, K. Etiology of pneumoparotid: A systematic review. J. Clin. Med. 2022, 12, 144. [Google Scholar] [CrossRef]
- Yoshida, K. Superior dislocation of the mandibular condyle into the middle cranial fossa: A comprehensive review of the literature. J. Clin. Med. 2023, 12, 3781. [Google Scholar] [CrossRef]
- Kramer. Zur Behandlung der irreponiblen Unterkieferverrenkung. Centralblatt für Chirurgie. 1901, 28, 269. [Google Scholar]
- Hildebrand, O. Zur blutigen Reposition veralteter Kieferluxationen. Archiv für Klinische Chirurgie. 1902, 66, 352. [Google Scholar]
- Willcutts, M.D. Treatment of an irreducible dislocated lower jaw of 98 days’ duration. U. S. Navy Med. Bull. 1927, 25, 331–336. [Google Scholar]
- Miyakoda, T. Surgical reduction of chronic dislocation of the mandibular joint. Jpn. Surg. Soc. 1931, 1369–1370. [Google Scholar]
- Schwartz, M. Unreduced unilateral dislocation of the jaw. J. Bone Joint Surg. 1940, 22, 176–181. [Google Scholar]
- Reiß, M. Operative Reposition veralterer doppel-seitiger Unterkieferluxationen. Zahnärztl. Rundsch. 1940, 49, 1235–1240, 1282–1285, 1309–1311. [Google Scholar]
- Watanabe, I.; Hagino, T. A case of chronic bilateral mandibular anterior dislocation successfully reduced by open reduction. Med. Biol. 1942, 1, 581–583. [Google Scholar]
- Müller, G.M. Long-standing dislocation of mandible. Br. Med. J. 1946, 1, 572. [Google Scholar] [CrossRef]
- Jones, J.C.B. Treatment of unreduced bilateral forward dislocation of the temporomandibular joint. Br. Dent. J. 1949, 86, 275–278. [Google Scholar]
- Watanabe, Y.; Otake, O. Unreduced dislocation of the mandibular joint following eclampsia. Oral Surg. Oral Med. Oral Path. 1950, 3, 1010. [Google Scholar] [CrossRef]
- Gottlieb, O. Long-standing dislocation of the jaw. J. Oral Surg. 1952, 10, 25–32. [Google Scholar]
- Matsumae, G, Ito, I. A Case of nonsurgical reduction of chronic anterior dislocation of the mandible. J. Jpn. Stomatol. Soc. 1952, 1, 91–92. [Google Scholar]
- Campbell, J.; White, T.C.; Anderson, H. A case of bi-lateral dislocation of the mandible of nine months duration. Dent. Record. 1952, 72, 230–239. [Google Scholar]
- Curson, I. Long-standing bilateral dislocation of the temporomandibular joints. Br. Dent. J. 1959, 107, 351–353. [Google Scholar]
- Whinery, J.G. Bilateral condylar neck dissection for long-standing dislocation of the mandible. J. Oral Surg. Anesth. Hosp. Dent. Serv. 1961, 19, 432–435. [Google Scholar] [PubMed]
- Berg, A. Ein Fall einer veralteten, doppelseitigen Unterkieferrenkung. Zschr. Stomat. 1962, 24, 876. [Google Scholar]
- Litzow, T.J.; Royer, R.Q. Treatment of long-standing dislocation of the mandible. Staff Meet Mayo Clinic. 1962, 37, 399–403. [Google Scholar]
- Glahn, M. Malposition of the mandibular condyle. Br. J. Oral Surg. 1964, 2, 33–36. [Google Scholar] [CrossRef]
- Hogan N, Nally F. Prolonged bilateral temporomandibular joint dislocation. Irish Dent, 1964, 10: 40–42.
- Fordyce, GL. Long-standing bilateral dislocation of the jaw. Br. J. Oral Surg. 1965, 3, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Hayward, J.R. Prolonged dislocation of the mandible. J. Oral Surg. 1965, 23, 585–594. [Google Scholar]
- Topazian, R.G.; Costich, E.R. Management of protracted dislocation of the mandible. J. Trauma. 1967, 7, 257–264. [Google Scholar] [CrossRef]
- Kameyama, T.; Miura, T.; Moji, K. A case of chronic dislocation of the temporomandibular joint. Jpn. J. Oral Maxillofac. Surg. 1968, 14, 17–20. [Google Scholar] [CrossRef]
- Yoshida, Y.; Terai, H.; Nakashiro, T. Surgical reduction of chronic anterior dislocation of the temporomandibular joint. J. Jpn. Stomatol. Soc. 1970, 19, 234–240. [Google Scholar] [CrossRef]
- Rowe, P.F.; Caldwell, J.B. Correction of permanent temporomandibular joint dislocation. J. Oral Surg. 1970, 28, 222–226. [Google Scholar] [PubMed]
- Ohto, A.; Shimura, K.; Suzuki, K.; Amanai, S. A case of chronic dislocation of the temporomandibular joint. J. Kanagawa Odont. Soc. 1970, 4(3/4), 83.
- Okano, M.; Henomatsu, K.; Yoda, K.; Kawai, S. A case of open reduction of chronic temporomandibular joint dislocation. Jpn. J. Oral Maxillofac. Surg. 1971, 17, 356. [Google Scholar]
- Sujaku, C.; Kameyama, T.; Hosino, N. A case of long-standing forward dislocation of the mandible. Jpn. J. Oral Maxillofac. Surg. 1972, 18, 593–597. [Google Scholar] [CrossRef]
- Horii, M.; Murata, A.; Ikeda, S.; Kashiwagi, A.; Ishii, Y. A case of obsolute luxation of jaw joint for 6 years. Kitano Hospital J. Med. 1973, 18, 88–90. [Google Scholar]
- Rawls, H.C.; Bruni, A.; Hamilton, M.K. Surgical correction of the permanently dislocated mandible. J. Oral Surg. 1973, 31, 385–388. [Google Scholar]
- Gorman, J.M. Condylotomy for bilateral dislocation. Br. J. Oral Surg. 1974, 12, 96–98. [Google Scholar] [CrossRef]
- Hashimoto, K.; Kawachi, S.; Murase, H.; Akashi, Y.; Masuda, M.; Ohtani, T. Two cases of obsolete bilateral dislocation of the temporomandibular joints. Jpn. J. Oral Maxillofac. Surg. 1976, 22, 423–428. [Google Scholar] [CrossRef]
- Adekeye, E.O.; Shamia, R.I.; Cove, P. Inverted L-shaped ramus osteotomy for prolonged bilateral dislocation of the temporomandibular joint. Oral Surg. Oral Med. Oral Path. 1976, 41, 568–577. [Google Scholar] [CrossRef]
- Sanders, B.; Schneider, J.; Given, J. Prolonged dislocation of the mandibular condyle. J. Oral Surg. 1979, 37, 346–348. [Google Scholar]
- Littler, B.O. The role of local anaesthesia in the reduction of long-standing dislocation of the temporomandibular joint. Br. J. Oral Surg. 1980, 18, 81–85. [Google Scholar] [CrossRef]
- Kawamura, H.; Takano, N.; Abe, Y.; Kikuchi, M.; Fujita, Y.; Hayashi, S. A case of chronic bilateral dislocation of the temporomandibular joint treated by nonsurgical reduction. Jpn. J. Oral Maxillofac. Surg. 1980, 29, 341–346. [Google Scholar] [CrossRef]
- Mizuno, A.; Fujita, S.; Shimada, T.; Sekiyama, S. Long-standing luxation of the mandible, report of a case and review of the Japanese literature. Int. J. Oral Surg. 1980, 9, 225–230. [Google Scholar] [CrossRef]
- Prabhakara, B.S. Conservative treatment of bilateral persistent anterior dislocation of the mandible. J. Oral Surg. 1980, 38, 51–52. [Google Scholar]
- Stakesby Lewis, J.E. A simple technique for reduction of long-standing dislocation of the mandible. Br. J. Oral Surg. 1981, 19, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Blank DM, Stein AC, Gold BD, Berger J. Treatment of protracted bilateral mandibular dislocation with Proplast-Vitallium prostheses. Oral Surg. Oral Med. Oral Pathol. 1982, Apr;53(4):335–339. [CrossRef]
- Tipps, S.P.; Landis, C.F. Prolonged bilateral mandibular dislocation. J. Oral Maxillofac. Surg. 1982, 40, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Parekh PK, Bhatia IK. Condylectomies for prolonged bilateral temporomandibular dislocation. Arch. Orthop. Trauma Surg. (1978). 1983, 102, 123–125, 1978. [CrossRef]
- Takahashi, T.; Tamura, H.; Ioku, N. Two cases of obsolete dislocation of the temporomandibular joint. Jpn. J. Oral Maxillofac. Surg. 1984, 30, 1708–1715. [Google Scholar] [CrossRef]
- Kudo, K.; Baba, Rie. ; Chen, C-H.; Komai, T.; Fujioka, Y.; Kanamori, T. Restricting operation of anterior movement for obsolete dislocation of temporomandibular joint: a case report. Jpn. J. Oral Maxillofac. Surg. 1985, 31, 337–340. [Google Scholar] [CrossRef]
- El-Attar, A.; Ord, R.A. Longstanding mandibular dislocations: report of a case, review of the literature. Br Dent J 160:91, 1986.
- Wijmenga, J.P.; Boering, G. Blankestijn, J. Protracted dislocation of the temporomandibular joint. Int. J. Oral Maxillofac. Surg. 1986, 15, 380–388. [Google Scholar] [CrossRef]
- Hammersley, N. Chronic bilateral dislocation of the temporomandibular joint. Br. J. Oral Maxillofac. Surg. 1986, 24, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Mizuno, A.; Torii, S.; Kamiya, H.; Katayama, T.; Yokoi, C.; Shikimori, M.; Motegi, K. Eminectomy for long-standing bilateral forward dislocation of the temporomandibular joint: Report of two cases. Jpn. J. Oral Maxillofac. Surg. 1987, 33, 386–393. [Google Scholar] [CrossRef]
- Kowaka, S.; Hosoda, M.; Segami, N.; Hata, T.; Hanafusa, H.; Fujimura, K.; Fukuda, M. A case of long-standing bilateral dislocation of the mandibular condyle. Jpn. J. Oral Maxillofac. Surg. 1987, 33, 2131–2135. [Google Scholar] [CrossRef]
- Obara, S.; Oka, M.; Harada, T.; Yoshimura, Y. A case of long-standing dislocation of the temporomandibular joint with severe complications. Jpn. J. Oral Maxillofac. Surg. 1988, 34, 716–721. [Google Scholar] [CrossRef]
- Chin RS, Gropp H, Beirne OR. Long-standing mandibular dislocation: report of a case. J. Oral Maxillofac. Surg. 1988, 46, 693–696. [Google Scholar] [CrossRef]
- Tanimoto, Y.; Morizane, T.; Hadano, T.; Yoshiga, K.; Takada, K. The chronic bilateral anterior dislocation of the temporomandibular joint (TMJ): Report of a case. J. Jpn. Soc. TMJ. 1991, 3, 69–74. [Google Scholar] [CrossRef]
- Ishihara, A.; Mizuno, K.; Kamiya, Y.; Ito, A.; Imai, T.; Adachi, M.; Yamashita, T.; Fukaya, M. Reduction of obsolete dislocation of temporomandibular joint: Report of a case. Jpn. J. Oral Maxillofac. Surg. 1992, 38, 500–501. [Google Scholar] [CrossRef]
- Ishimaru, T.; Hayatsu, Y.; Ohsawa, S.; Shinozaki, F. A case of prolonged mandibular dislocation of the patient medicated with antipsychotic drugs. J. Jpn Stomatol. Soc. 1992, 41, 504–510. [Google Scholar] [CrossRef]
- Ogawa, T.; Mori, M.; Sawatari, S.; Yamamoto, Gaku. ; Yamaguchi, Y.; Yoshitake, K. A case of open reduction for long-standing anterior luxation of the temporomandibular joint. Jpn. J. Oral Maxillofac. Surg. 1992, 38, 1927–1928. [Google Scholar] [CrossRef]
- Smith WP, Johnson PA. Sagittal split mandibular osteotomy for irreducible dislocation of the temporomandibular joint. A case report. Int. J. Oral Maxillofac. Surg. 1994, 23, 16–18. [Google Scholar] [CrossRef]
- Kawakami, T.; Tsuzuki, M.; Shohara, E.; Takayama, K.; Morimoto, Y.; Sugimura,M. Surgical treatment by Dautrey procedure for long-standing anterior luxation of the temporomandibular joints. J. Jpn. Soc. TMJ. 1995, 7, 51–56. [Google Scholar] [CrossRef]
- Kato, M.; Isobe, M.; Kamiya, Y.; Ohtani, T. Two cases of obsolete dislocation of the temporomandibular joint with cerebrovascular disease. J. Jpn. Soc. Dent. Medically Compromised Patient. 1996, 5, 30–35. [Google Scholar] [CrossRef]
- Iwatsubo, R.; Hosaka, H.; Goto, K.; Murayama, T. Treatment of temporomandibular joint luxation in patients with complications. –Case report–. J. Jpn. Soc. Dent. Medically Compromised Patient. 1996, 4, 65–73. [Google Scholar] [CrossRef]
- Kurita K, Mukaida Y, Ogi N, Toyama M. Closed reduction of chronic bilateral temporomandibular joint dislocation. A case report. Int. J. Oral Maxillofac. Surg. 1996, 25, 422–423. [Google Scholar] [CrossRef] [PubMed]
- Caminiti, M.F.; Weinberg, S. Chronic mandibular dislocation: The role of non-surgical and surgical treatment. J. Can. Dent. Assoc. 1998, 64, 484–491. [Google Scholar] [PubMed]
- Hoard MA, Tadje JP, Gampper TJ, Edlich RF. Traumatic chronic TMJ dislocation: report of an unusual case and discussion of management. J. Craniomaxillofac. Trauma. 1998, 4, 44–47. [Google Scholar]
- Mizutani, H.; Hattori, H.; Senga, K.; Seko, K.; Asahina, T.; Kaneko, R.; Shinoda, M.; Ueda, M. Eight cases with chronic mandibular dislocation. J. Jpn. Soc. TMJ. 2000, 12, 52–56. [Google Scholar]
- Murakami, K.; Kondo, T.; Irisa, K.; Takahashi, K.; Kishida, T.; Itoh, T. J. J. Jpn. Soc. Dent. Medically Compromised Patient. 2002; 11, 41–46. [CrossRef]
- Takenaka, A.; Fujita, H.; Sasaki, H.; Tanabe, S.; Matsuda, S.; Yoshimura, Y. A case of old anterior temporomandibular joint dislocation treated by lysis and lavage using arthroscopic technique and manual reduction. J. Jpn. Soc. TMJ. 2003, 15, 29–32. [Google Scholar]
- Aquilina, P.; Vickers, R.; McKellar, G. Reduction of a chronic bilateral temporomandibular joint dislocation with intermaxillary fixation and botulinum toxin A. Br. J. Oral Maxillofac. Surg. 2004, 42, 272–273. [Google Scholar] [CrossRef]
- Ohno, K.; Sumitomo, S.; Mouri, K.; Kuwajima, K.; Takai, Y. Chronic dislocation of temporo-mandibular joint reset by closed reduction with intra-articular pumping technique. J. Jpn. Soc. TMJ. 2005, 17, 215–217. [Google Scholar] [CrossRef]
- Kobayakawa, M.; Kamei, K.; Sato, T.; Nakamura, M.; Ito, K.; Kobayashi, K. A case of bilateral chronic dislocation of the temporomandibular joint reduced by removal of fibrous adhesive lesions after eminectomy. Jpn. J. Oral Maxillofac. Surg. 2005, 51, 212–215. [Google Scholar] [CrossRef]
- Terakado, N.; Shintani, S.; Nakahara, Y.; Yano, J.; Hino, S.; Hamakawa, H. Conservative treatment of prolonged bilateral mandibular dislocation with the help of an intermaxillary fixation screw. Br. J. Oral Maxillofac. Surg. 2006, 44, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Debnath SC, Kotrashetti SM, Halli R, Baliga S. Bilateral vertical-oblique osteotomy of ramus (external approach) for treatment of a long-standing dislocation of the temporomandibular joint: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e79–82. [Google Scholar] [CrossRef] [PubMed]
- Lee SH, Son SI, Park JH, Park IS, Nam JH. Reduction of prolonged bilateral temporomandibular joint dislocation by midline mandibulotomy. Int. J. Oral Maxillofac. Surg. 2006, 35, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Nakayama, S.; Yoshihama, Y.; Mese, H.; Sasaki, A. Conservative reduction of obsolete dislocation of the temporomandibular joint –A case report: Innovation for a patient with severe marginal periodontitis–. J. Jpn. Soc. TMJ. 2007, 19, 171–176. [Google Scholar] [CrossRef]
- Rattan, V.; Rai, S. Management of long-standing anteromedial temporomandibular joint dislocation. Asian J. Oral Maxillofac. Surg. 2007, 19, 155–159. [Google Scholar] [CrossRef]
- Nakashima, M.; Yano, H.; Akita, S.; Tokunaga, K.; Anraku, K.; Tanaka, K.; Hirano,A. Traumatic unilateral temporomandibular joint dislocation overlooked for more than two decades. J. Craniofac Surg. 2007, 18, 14661470. [Google Scholar] [CrossRef]
- Kale, T.P.; Kotrashetti, S.M.; Janardhan, S.; Urolagin, S.B. Long standing TMJ dislocation: closed reduction –A case report and technical note. J. Int. Oral Health. 2010, 2, 59–67. [Google Scholar]
- Huang IY, Chen CM, Kao YH, Chen CM, Wu CW. Management of long-standing mandibular dislocation. Int. J. Oral Maxillofac. Surg. 2011, 40, 810–814. [CrossRef]
- Shakya, S.; Ongole, R.; Sumanth, K.N.; Denny, C.E. Chronic bilateral dislocation of temporomandibular joint. Kathmandu Univ Med J (KUMJ). 2010, 8, 251–256. [Google Scholar] [CrossRef]
- Kim, C-H. ; Kim, D-H. Chronic dislocation of temporomandibular joint persisting for 6 months: a case report. J. Korean assoc. Maxillofac. Surg. 2012, 38, 305–309. [Google Scholar] [CrossRef]
- Rattan, V.; Rai, A.; Sethi, A. Midline mandibulotomy for reduction of long-standing temporomandibular joint dislocation. Craniomaxillofac. Trauma Reconstr. 2013, 6, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Shibayama, N.; Kondo, E.; Ogami, J.; Takekawa, M.; Matsuda, M. A case of chronic mandibular dislocation treated by conservative reduction. Jpn. J. Oral Maxillofac. Surg. 2013, 59, 18–22. [Google Scholar] [CrossRef]
- Baur, D.A.; Jannuzzi, J.R.; Mercan, U.; Quereshy, F.A. Treatment of long term anterior dislocation of the TMJ. Int. J. Oral Maxillofac. Surg. 2013, 42, 1030–1033. [Google Scholar] [CrossRef]
- Elmorsy, K.A. Management of long-standing temporomandibular joint dislocation. Egypt J. Oral Maxillofac. Surg. 2014, 5, 39–44. [Google Scholar] [CrossRef]
- Hayashi, K.; Onda, T.; Ogane, S.; Yakushiji, T.; Ohata, H.; Takano, N.; Shibahara, T. A case of long standing dislocation of bilateral temporomandibular joints of the elderly. J.J. Gerodont. 2014, 28, 284–288. [Google Scholar] [CrossRef]
- Saikia, D. Long standing temporomandibular joint dislocation: a case report. IOSR-JDMS, 2014, 13, 3–8. [Google Scholar] [CrossRef]
- Pradhan, L.; Jaisani, M.R.; Sagtani, A.; Win, A. Conservative management of chronic TMJ dislocation: An old technique revived. J. Maxillofac. Oral Surg. 2015, 14 (Suppl 1), A267–S270. [Google Scholar] [CrossRef]
- Ogawa, M.; Kanbe, T.; Kubota, F.; Makiguchi, T.; Miyazaki, H.; Yokoo, S. Conservative reduction by lever action of chronic bilateral mandibular condyle dislocation. Cranio. 2015, 33, 142–147. [Google Scholar] [CrossRef]
- Arzul L, Henoux M, Marion F, Corre P. Luxation chronique bilatérale des articulations temporo-mandibulaires et syndrome de Meig. Rev. Stomatol. Chir. Maxillofac. Chir. Orale. 2015, 116, 106–110. [Google Scholar] [CrossRef]
- Marqués-Mateo, M.; Puche-Torres, M.; Iglesias-Gimilio, M.E. Temporomandibular chronic dislocation: The long-standing condition. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e776–e783. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraj, P.; Chakranarayan, A. A conservative surgical approach in the management of longstanding chronic protracted temporomandibular joint dislocation: A case report and review of literature. J. Maxillofac. Oral Surg. 2016, 15 (Suppl 2), S361–S370. [Google Scholar] [CrossRef] [PubMed]
- Güngörmüş, M.; Yavuz, M.S.; Ömezli, M.M.; Akkaş, İ. Long-term temporomandibular joint dislocation treated with bilateral eminectomy and chin-cap; Case report. Turkiye Klinikleri J. Dental Sci. Cases. 2016, 2, 75–79. [Google Scholar] [CrossRef]
- Negishi, S.; Shibasaki, M. A case of long-standing bilateral temporomandibular joint dislocation treated by intraoral condylectomy. Jpn. J. Oral Maxillofac. Surg. 2017, 63, 304–309. [Google Scholar] [CrossRef]
- Malik, K.; Debnath, S.C.; Adhyapok, A.K.; Hazarika, K. Long-standing temporomandibular joint dislocation: A rare experience. Saudi J. Oral Sci. 2017, 4, 112–116. [Google Scholar] [CrossRef]
- Shaban, S.D.; Sohal, K.S.; Moshy, J.R. A novel technique for surgical reduction of long-standing temporomandibular joint dislocation. Int. J. Head Neck Surg. 1: (3). [CrossRef]
- Dhiman, N.K.; Pandey, A.; Vishwakarma, A.K.; Verma, V.; Singh, S. Management of long standing TMJ dislocation: Report of three cases. J. Adv. Med Dent Sci. Res. 2018, 6, 55–58. [Google Scholar] [CrossRef]
- Chin, S.Y.; Berahim, N.B.; Andan, K.B.; Ramasamy, S.N. Delayed management of unrecognized bilateral temporomandibular joint dislocation: A case report. Craniomaxillofac. Trauma. Reconstr. 2018, 11, 145–149. [Google Scholar] [CrossRef]
- Gholami, M.; Shirzadeh, A.; Khalife, H. Chronic long-standing temporomandibular joint dislocation: Report of three cases and review of literature. J Maxillofac Oral Surg. 2018, 17, 502–507. [Google Scholar] [CrossRef]
- Segami, N.; Nishimura, T.; Miyaki, K.; Adachi, H. Tethering technique using bone screws and wire for chronic mandibular dislocation: a preliminary study of refractory cases. Int. J. Oral Maxillofac. Surg. 2018, 47, 1065–1069. [Google Scholar] [CrossRef]
- Balaji, S.M.; Balaji, P. Surgical management of chronic temporomandibular joint dislocations. Indian J. Dent. Res, 4: 29. [CrossRef]
- Güven, O. Nearthrosis in true long-standing temporomandibular joint dislocation; a report on pathogenesis and clinical features with review of literature. J. Craniomaxillofac. Surg. 2019, 47, 945–950. [Google Scholar] [CrossRef]
- Cuevas Queipo de Llano, A.; Monje Gil, F.; Gonzalez García, R.; Villanueva Alcojol, L.; Gonzalez Ballester, D. Long-term dislocation of the mandible: Is there an algorithm to success? intraoperative decision and review of literature. J. Maxillofac. Oral Surg. 2020, 19, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Karakida, K.; Takahashi, M.; Hamada, Y.; Aoki, J.; Hoshimoto, Y. A case of long-standing temporomandibular joint dislocation: Restoration of oral function following condylectomy. Tokai J. Exp. Clin. Med. 2020, 45, 152–155. [Google Scholar] [PubMed]
- Sarlabous, M.; Psutka, D.J. Total joint replacement after condylar destruction secondary to long-standing dislocation of the temporomandibular joint. J. Craniofac. Surg. 2020, 31, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Bavia, P.F.; Ganjawalla, K.; Keith, D.A. Long-standing unilateral temporomandibular joint (TMJ) dislocation with pseudo articulation with the base of the skull. Oral Maxillofac. Surg. Cases. 2020, 6, 1–6. [Google Scholar] [CrossRef]
- Uetsuki, R.; Ono, S.; Tada, M.; Okuda, S.; Takechi, M. Long-standing temporomandibular joint dislocation treated by intraoral condylectomy: a case report and review of the literature. J. Med. Case Rep. 2022, 16, 245. [Google Scholar] [CrossRef]
- Nikunj, A.; Khan, N.; Rajkhokar, D.; Mishra, B.; Rajurkar, S. Deg-induced oromandibular dystonia presenting as chronic temporomandibular joint dislocation: a rare case report. Cureus. 2022, 14, e23478. [Google Scholar] [CrossRef]
- Anehosur, V.; Mehra, A.; Kumar, N. Management of chronic long standing condyle dislocation. Int. Surg. J. 2023, 10, 114–120. [Google Scholar] [CrossRef]
- Ekram, S.; Tigga, C.; Prajapati, V.K.; Prakash, O. Elastic traction treatment for the management of chronic dislocation of bilateral condyle – A report of 2 case. Dent J Indira Gandhi Inst Med Sci. 2022, 1, 73–75. [Google Scholar] [CrossRef]
- Navaneetham, R.; Navaneetham, A.; Pugazhendi, S.K.; Nara, G.; Umarani, P.J. Chronic protracted dislocation of temporomandibular joint in a trauma patient – a case report. Ann. Maxillofac. Surg. 2023, 13, 130–132. [Google Scholar] [CrossRef]
- Gupta, G.; Gupta, D.K.; Gupta, N.; Chandra, N.; Sankhla, D. Conservative management of a 3 months long standing bilateral temporomandibular joint dislocation: a case report. J. Oral Med. Oral Surg. Oral Pathol. Oral Radiol. 2023, 9, 222–225. [Google Scholar] [CrossRef]
- Ogundipe, O,K. ; Ugwu, E,I.; Ajayi, O,S.; Ojo, O,O. Reduction of manually irreducible TMJ dislocation with forceps traction: Case report in a 60-year-old woman. Nigerian Dent J. 2023, 31, 1–7. [Google Scholar]
- Zou, J, Wang, L. ; Acharya, K.; Hou, X.; Li, L.; Hu, X.; Xing, X. The experience of chronic protracted mandibular dislocation treatment: manual vs. surgical reduction. BMC Oral Health. 2024, 24, 1127. [Google Scholar] [CrossRef]
- Tanaka, T.; Momozaki, N.; Honda, E.; Matsuno, A. Delayed diagnosis of temporomandibular joint dislocation in severe stroke patients. Cureus. 2024, 16, e68896. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, Y.; Nogami, S.; Iwama, R.; Otake, Y.; Sato, S.; Yamauchi, K. A case of chronic bilateral temporomandibular joint dislocation treated via a bilateral intraoral vertical ramus osteotomy. Jpn. J. Oral Maxillofac. Surg. 2024, 70, 379–384. [Google Scholar] [CrossRef]
- Yoshida, K. How doi inject botulinum toxin into the lateral and medial pterygoid muscles? Mov Disord Clin Pract 2017, 4, 285. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Botulinum toxin therapy for oromandibular dystonia and other movement disorders in the stomatognathic system. Toxins. 2022, 14, 282. [Google Scholar] [CrossRef]
- O'Connor, M. , Rooney, M.; Nienaber, C.P. Neuroleptic-induced dislocation of the jaw. Br. J. Psych 1992, 161:281–282. [CrossRef]
- Ibrahim., Z.Y.; Brooks, E.F. Ibrahim. Z.Y.; Brooks, E.F. Neuroleptic-induced bilateral temporomandibular joint dislocation. Am. J. Psychiatry. 1996, 153 (2), 2–3. [CrossRef]
- McGraw, T.A. A new method of reducing old dislocations of the lower jaw. Med. Record. 1899, 56, 511. [Google Scholar]
- Leclerc, G. ; Girard, G.Un nouveau procédé de butée dans le traitement chirurgical de la luxation récidivante de la mâchoire inférieure.Mém. Acad. Chir. 1943, 69, 457–459. [Google Scholar]
- Myrhaug, H. A new method of operation for habitual dislocation of the mandible. Review of former methods of treatment. Acta Odontol. Scand. 1951, 9, 247–260. [Google Scholar] [CrossRef]
- Dautrey, J. Reflexions sur la chirurgie de l’articulation temporo-mandibulaire. Acta. Stomatol. Belg. 1975, 72, 577–581. [Google Scholar]
- Niezen, E.T.; B van Minnen, B.; Bos, R.R.M.; Dijkstra, P.U. Temporomandibular joint prosthesis as treatment option for mandibular condyle fractures: a systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2023, 52, 88–97. [Google Scholar] [CrossRef]
- Laskin, D.M. Myotomy for the management of recurrent and protracted mandibular dislocations. 4th International Conference on Oral Surgery, Amsterdam, Copenhagen, 1973, Munskgaard 264, 1973.
- Miller, G.A.; Murphy. E.J. External pterygoid myotomy for recurrent mandibular dislocation. Oral Surg. 1976, 42, 705–714. [Google Scholar] [CrossRef]
- Sindet-Petersen, S. Intraoral myotomy of the lateral pterygoid muscle for the treatment of recurrent dislocation of the mandibular condyle. J. Oral Maxillofac. Surg. 1988, 46, 445–449. [Google Scholar] [CrossRef]
Figure 1.
Diagram of the literature search and screening strategy.
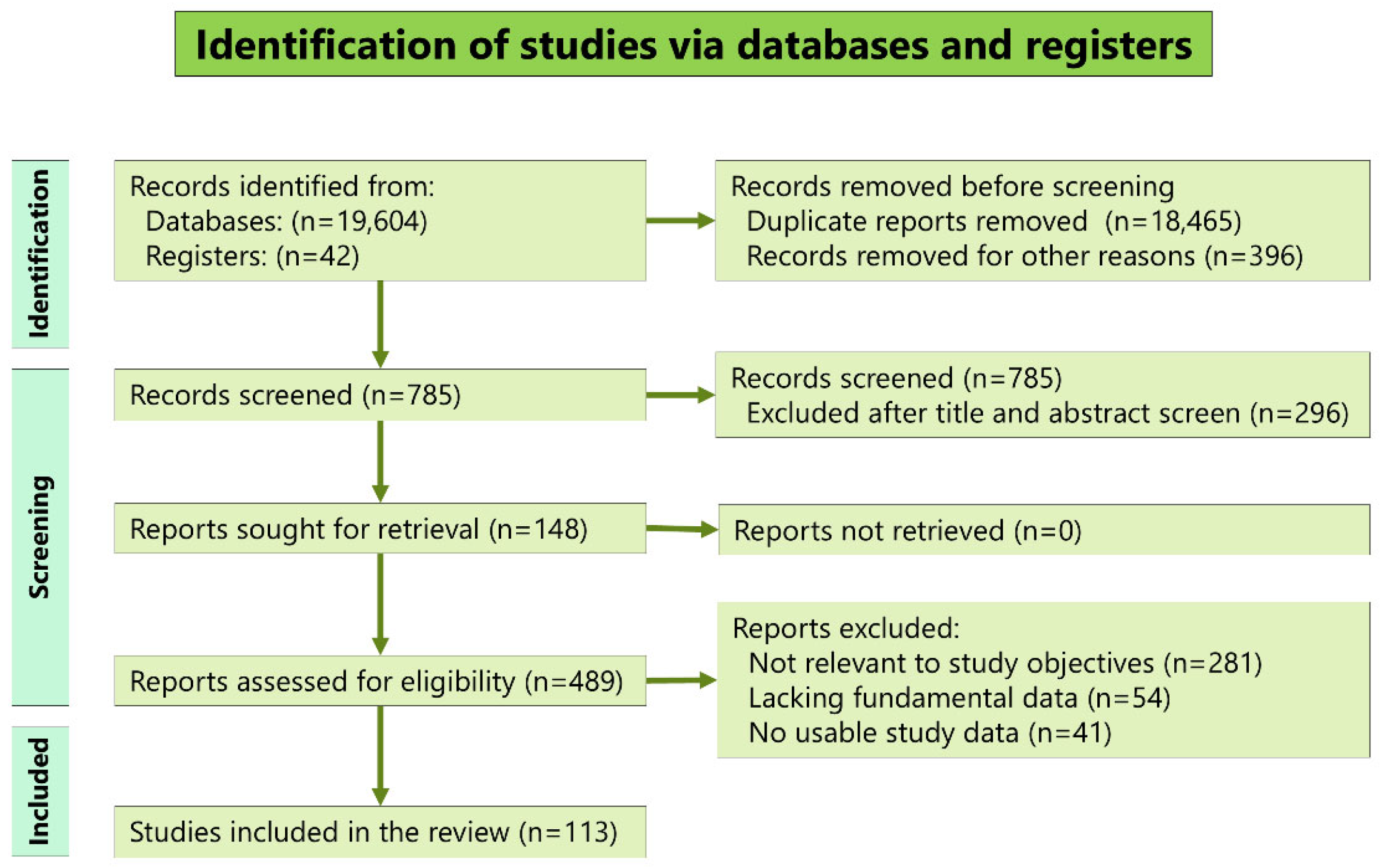
Figure 2.
First clinical diagnosis of patients with long-standing TMJ dislocation. The numbers in the pie chart represent percentages. TMJ, temporomandibular joint; NR, not reported.
Figure 2.
First clinical diagnosis of patients with long-standing TMJ dislocation. The numbers in the pie chart represent percentages. TMJ, temporomandibular joint; NR, not reported.
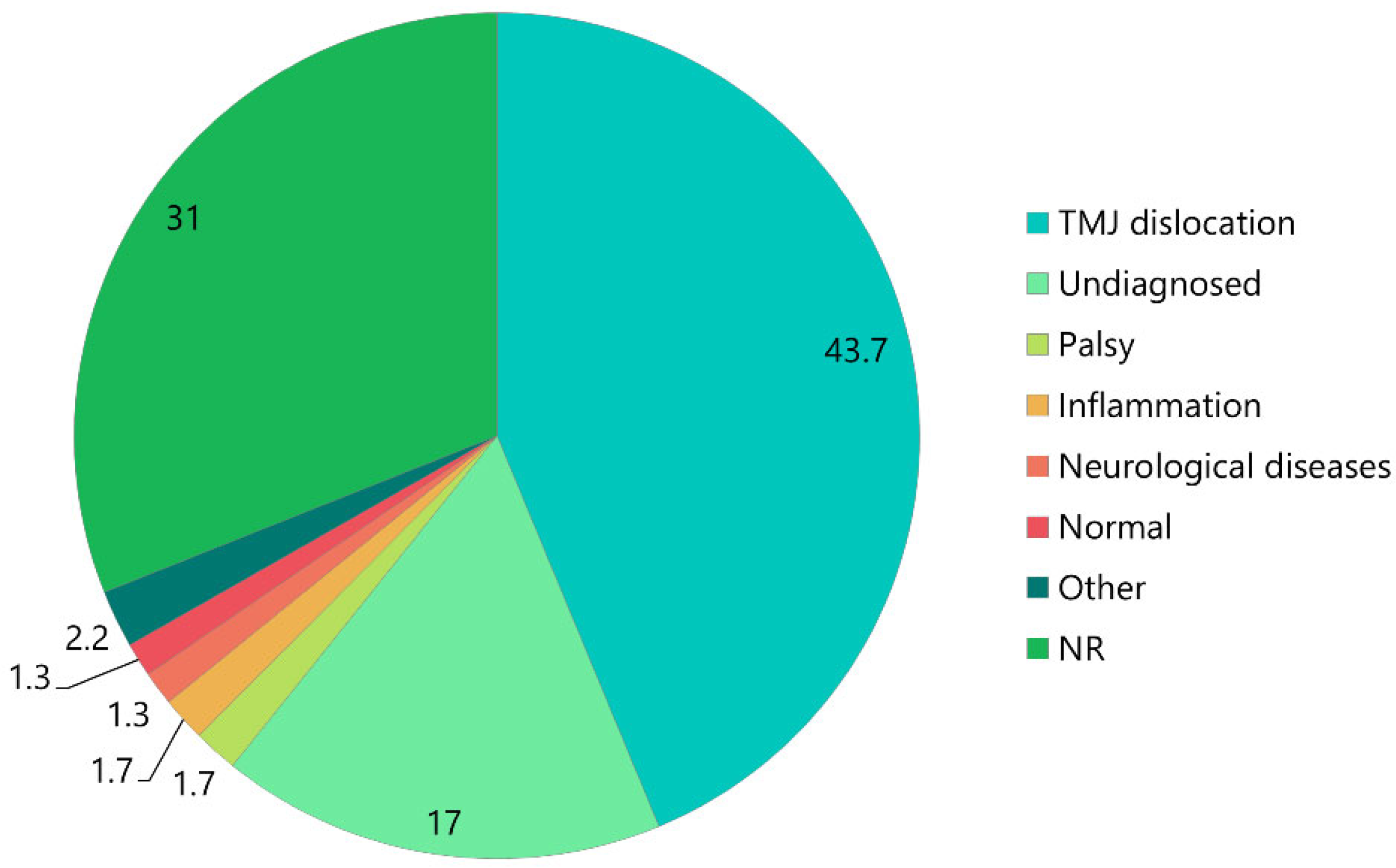
Figure 3.
Etiologies of patients with long-standing TMJ dislocation. NR, not reported.
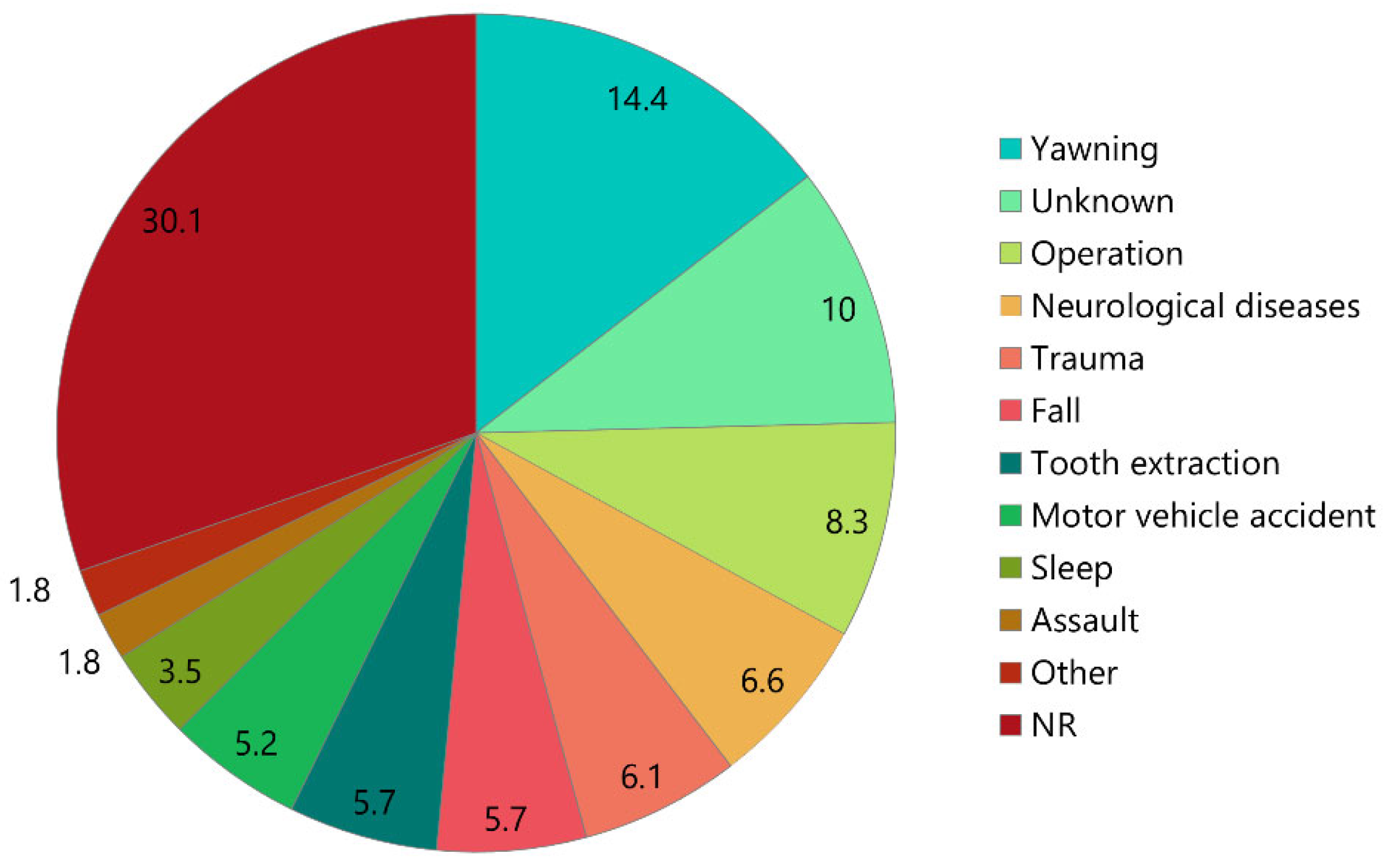
Figure 4.
Comparison of the mean age of patients with atraumatic and traumatic etiologies.
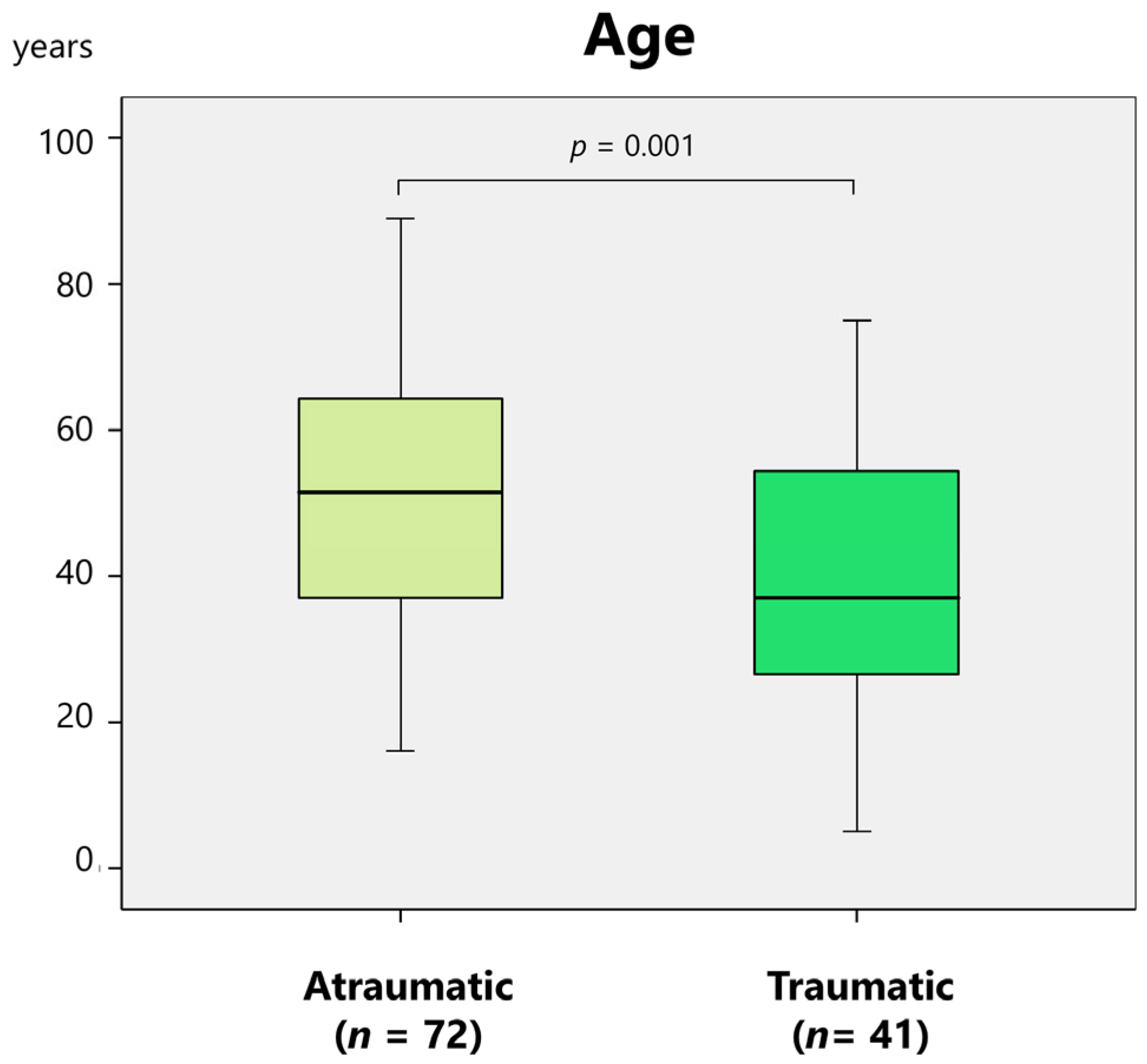
Figure 5.
Treatments of patients with long-standing TMJ dislocation. NR, not reported.
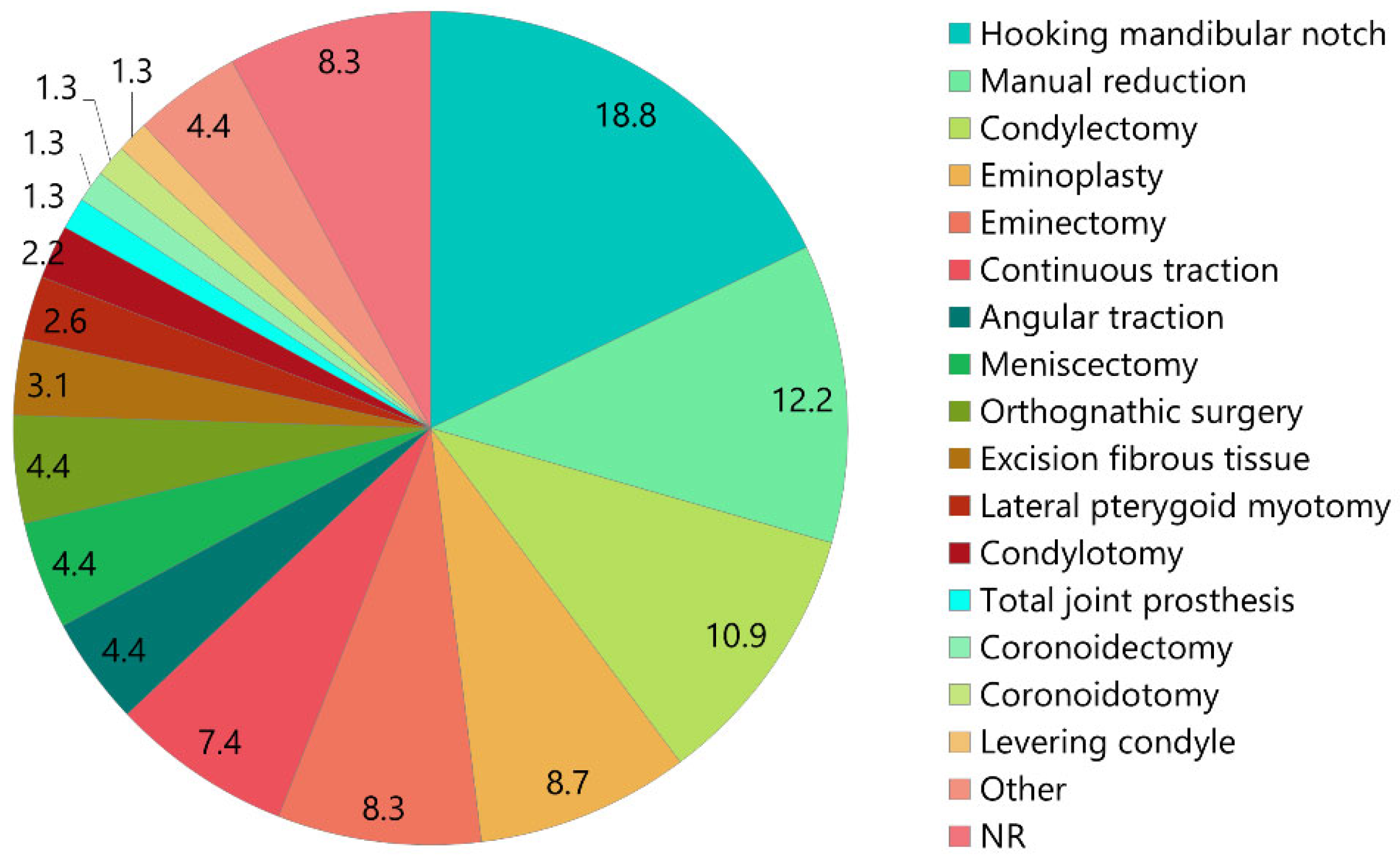
Figure 6.
Ratio of closed and open reduction according to duration after dislocation.
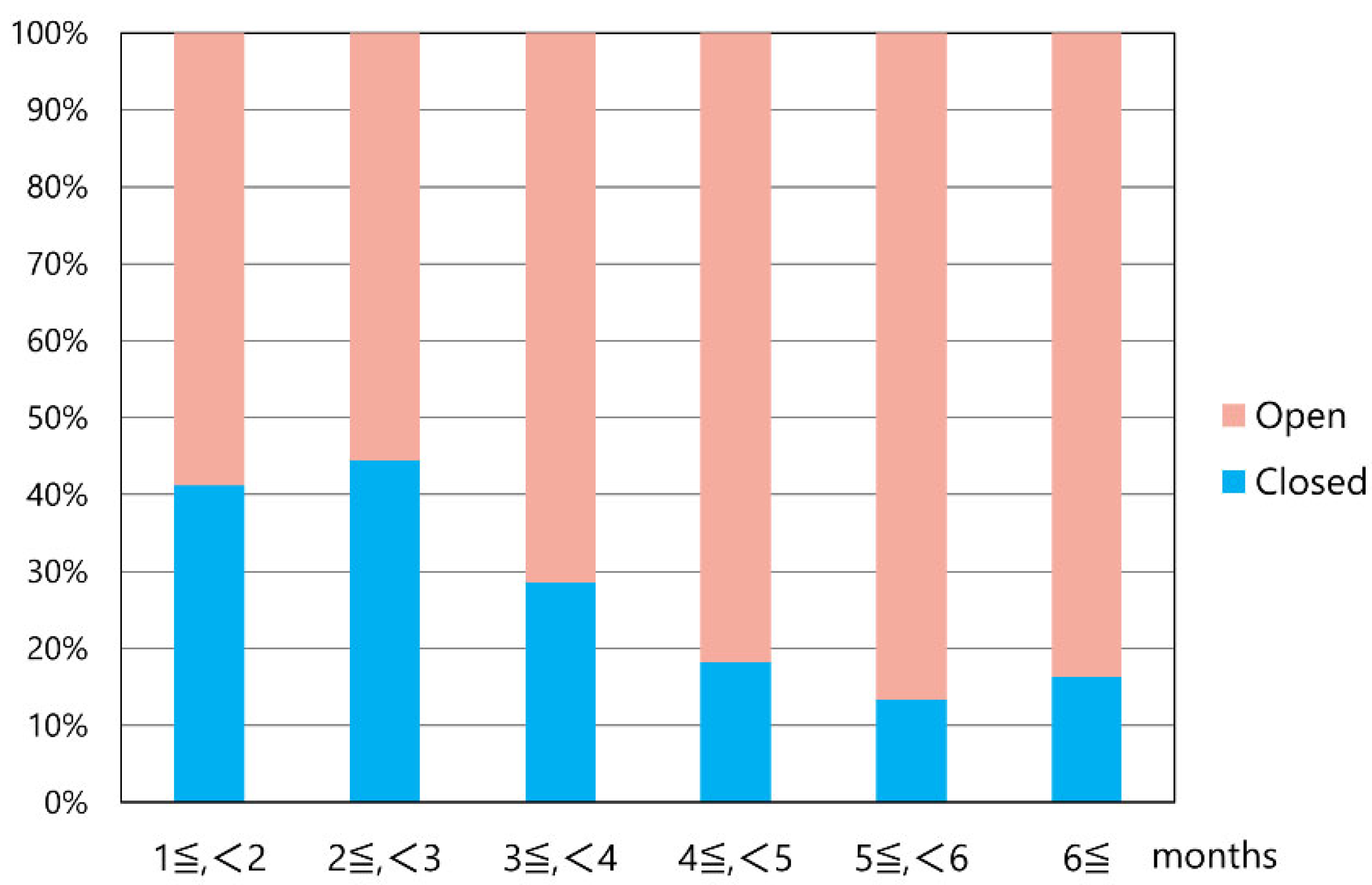
Figure 7.
Duration of closed and open reduction of patients with long-standing TMJ dislocation.
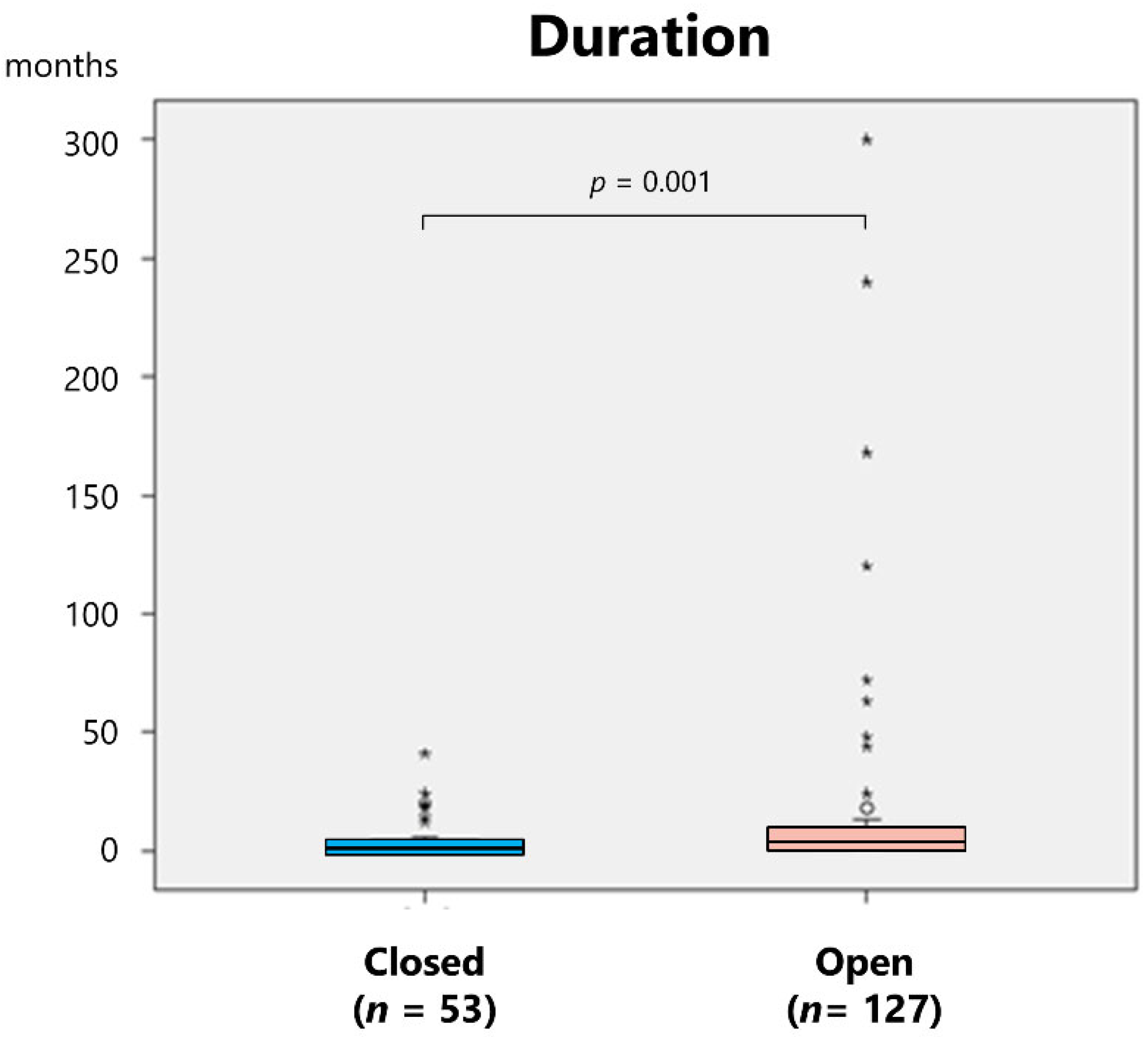
Figure 8.
A proposed treatment algorithm for long-standing TMJ dislocation.
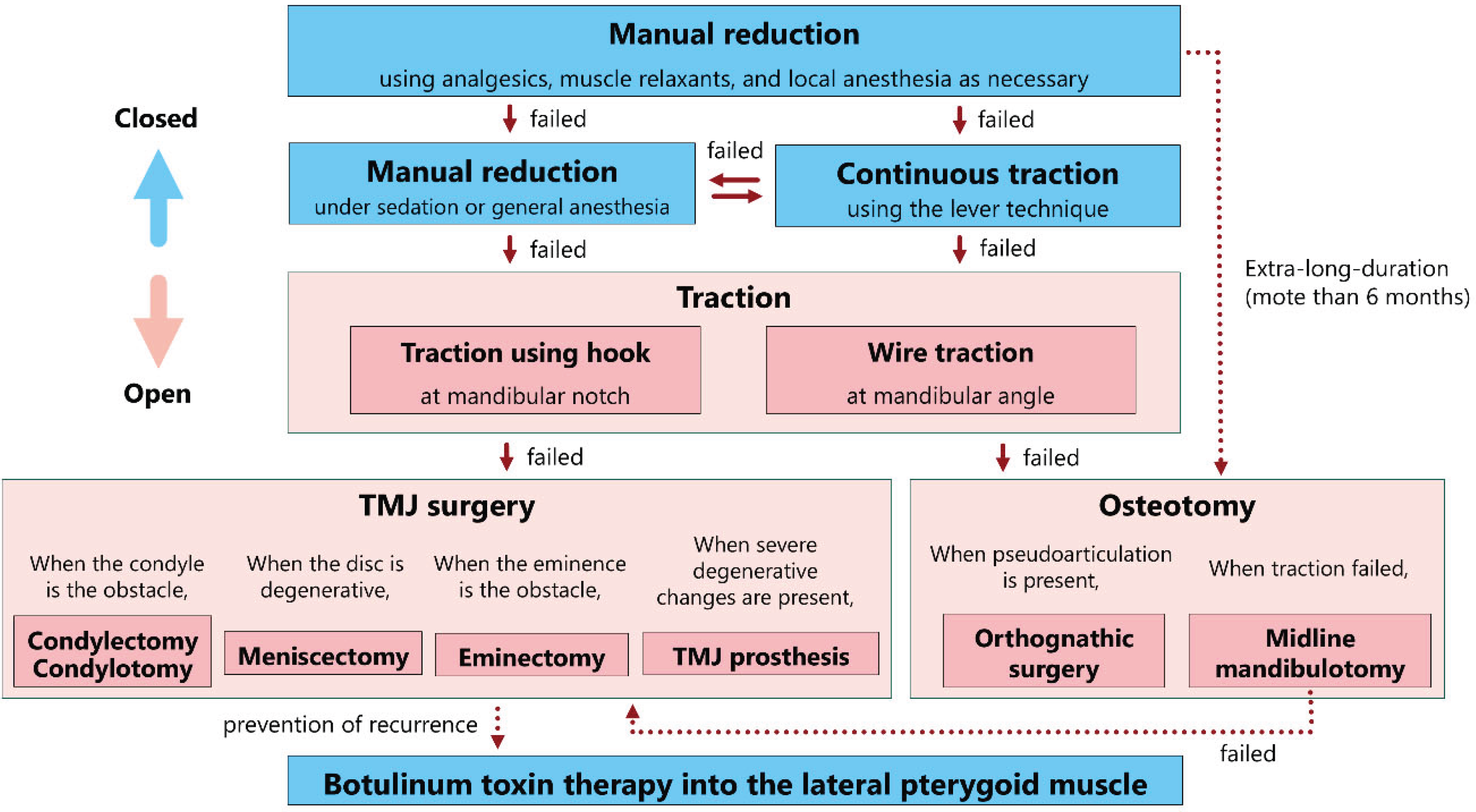

Table 1.
Summary of demographic data and diagnosis.
| Sex, (n [%)] | Women, n = 139 (60.7%); men, n = 81 (35.4%); NR, n = 9 (3.9%) |
| Age (years), [mean ± SD, range] | 52.3 ± 19.5, 5–89 |
| Affected side, (n [%)] | Bilateral, n = 171 (72.5%); left, n = 11 (4.7%); right, n = 9 (3.8%); NR, n = 31 (13.2%) |
| Duration (months), (mean ± SD, n [%], range) |
11.9 ± 34.4, n = 174 (73.7%), range 1–300 |
| First clinical diagnosis, (n [%]) | TMJ dislocation, n = 100 (43.7%); undiagnosed, n = 39 (17%); palsy, n = 4 (1.7%); inflammation, n = 4 (1.7%); neurological diseases, n = 3 (1.3%); normal, n = 3 (1.3%); other, n = 5 (2.2%); NR, n = 71 (31%) |
| Previous dislocation, (n [%]) | Once, n = 14 (6.1%); frequently, n = 6 (2.6%); sometimes, n = 3 (1.3%); N, n = 37 (16.2%); NR, n = 169 (73.8%) |
| Anamnesis, (n [%]) | Psychiatric diseases, n = 19 (8.3%); dementia or menta retardation, n = 15 (6.6%); neurological diseases, n = 10 (4.4%); cerebral infarction, n = 10 (4.4%); cerebral hemorrhage, n = 9 (3.9%); brain injury, n = 4 (1.7%); NR, n = 121 (52.8%) |
| Diagnostic image, (n [%]) | Radiography; n = 165 (69.9%); CT, n = 57 (24.2%); MRI, n = 4 (1.7%); NR, n = 45 (19.1%) |
SD, standard deviation; N, no; NR, not reported; CT, computed tomography; TMJ, temporomandibular joint; MRI, magnetic resonance imaging.
Table 2.
Summary of patient symptoms and etiology.
| Chief complaint, (n [%]) | Preauricular pain, n = 61 (25.8%); inability of mouth closing, n = 44 (18.6%); masticatory disturbance, n = 32 (13.6%); difficulty in speaking, n = 24 (10.2%); malocclusion, n = 15 (6.4%); facial deformity, n = 12 (5.1%); difficulty in swallowing, n = 12 (5.1%); other, n = 5 (2.1%); NR, n = 87 (36.9%) |
| Maximal mouth opening (mm), (mean ± SD, n [%]) |
24.6 ± 69.9, n = 62 (27.1%); NR, n = 167 (72.9%) |
| Open bite (mm), (mean ± SD, n [%]) | 14.4 ± 6.6, n = 26 (11.4%); NR, n = 203 (88.6%) |
| Edentulousness, (n [%]) | Total edentulous, n = 48 (20.3%); upper or lower, n = 8 (3.4%); N, n = 95 (40.3%); NR, n = 62 (26.3%) |
| Etiology, [n (%)] | Yawning, n = 33 (14.4%); unknown, n = 23 (10%); operation, n = 19 (8.3%); neurological diseases, n = 15 (6.6%); trauma, n = 14 (6.1%); fall, n = 13 (5.7%); tooth extraction, n = 13 (5.7%); motor vehicle accident, n = 12 (5.2%); sleep, n = 8 (3.5%); assault; n = 4 (1.8%); others, n = 4 (1.8%); NR, n = 69 (30.1%) |
SD, standard deviation; N, no; NR, not reported; TMJ, temporomandibular joint. .
Table 3.
Summary of treatments for long-standing TMJ dislocation.
| Treatment, (n [%]) |
Closed reduction, n = 49 (21.4%) Manual reduction, n = 28 (12.2%); with instruments, n = 3 (1.3%), continuous traction, n = 17 (7.4%), 3–40 days |
|
Open reduction; n = 175 (76.4%) Hooking mandibular notch, n = 43 (18.8%), condylectomy, n = 25 (10.9%), eminoplasty, n = 20 (8.7%), eminectomy, n = 19 (8.3%), angular traction, n = 10 (4.4%), meniscectomy, n = 10 (4.4%), orthognathic surgery, n = 10 (4.4%), excision of fibrous tissue, n = 7 (3.1%), lateral pterygoid myotomy, n = 6 (2.6%), condylotomy, n = 5 (2.2%), total TMJ prosthesis, n = 3 (1.3%), coronoidectomy, n = 3 (1.3%), coronoidotomy, n = 3 (1.3%), levering condyle, n = 3 (1.3%), other, n = 10 (4.4%), NR, n = 19 (8.3%) | |
|
Incision Preauricular, n = 107 (46.7%), submandibular, n = 24 (10.5%), zygomatic arch , n = 15 (6.6%), intraoral, n = 13 (5.7%), Al-Kayat Bramery, n = 4 (%), Bockenheimer-Axhausen, n = 3 (1.3%), other, n = 5 (2.2%) |
N, no; TMJ, temporomandibular joint; NR, not reported.
Table 4.
Summary of follow-up and sequelae in patients with long-standing TMJ dislocation.
| Treatment complication, (n [%]) |
Facial nerve paralysis, n = 8 (6.9%); redislocation, n = 3 (2.6%); others, n = 3 (2.6%); N, n = 77 (66.4%); NR, n = 17 (7.4%) |
| Fixation (days), (n [%], mean ± SD) |
Y, n = 122 (53.3%), 17.5 ± 15; N, n = 20 (8.7%); NR, n = 76 (33.2%) |
| Follow-up (months), (mean ± SD, n [%], range) |
11.8 ± 13, n = 147 (64.2%), 0.25–96; NR, n = 82 (35.8 |
| Maximal mouth opening at follow-up (mm), (mean ± SD, n [%], range) |
36.2 ± 6.8, n = 90 (77.6%), 22–51, 35; NR, n = 23 (19.8%) |
| Sequelae, (n [%]) | Redislocation; n = 4 (%), deviation; n = 3 (%), condylar absorption; n = 2 (%), other; n = 9 (%); N, n = 128 (55.9%); NR, n = 69 (30.1%) |
SD, standard deviation; Y, yes; N, no; TMJ, temporomandibular joint; NA, not applicable; NR, not reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



