Submitted:
13 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
Mpox, a zoonotic Orthopoxvirus, is a growing global health concern with clinical symptoms like smallpox, including fever, lymphadenopathy, and distinctive rashes. The increasing number of cases emphasizes how urgently antivirals and vaccinations are needed. Antiviral options like tecovirimat, cidofovir, and brincidofovir target DNA polymerase and viral assembly but show varying efficacy. Vaccines such as JYNNEOS and ACAM2000 provide cross-protection, while advancements in mRNA vaccines and recombinant viral vectors offer future promise. Mpox replicates its genome via DNA-dependent RNA polymerase, using envelope proteins for cell entry and evading immune responses through interferon signalling disruption and NF-κB activation. Challenges remain in improving animal models, addressing drug resistance, and ensuring equitable vaccine access. Bioinformatics-driven vaccine design and computational drug repurposing offer rapid solutions for Mpox. PoxApp, a mobile app for symptom tracking and AI analysis, and MPXV-CNN, a model for detecting Mpox image lesions, will accelerate diagnosis and monitoring. Strong pharmacovigilance, innovative treatments, and global collaboration are key to combating Mpox and improving public health resilience.
Keywords:
Mpox
; MPXV
; antivirals
; vaccines
; emerging therapeutics
; JYNNEOS
; ACAM2000
; LC16m8
; Cidofovir
; Brincidofovir
; Tecovirimat
; NIOCH-14
1. Introduction
Mpox is a zoonotic disease caused by infection with the Mpox virus (MPXV), a double-stranded DNA virus and a member of the Orthopoxvirus (OPXV) genus within the Poxviridae family, which also contains viruses that cause cowpox, horsepox, camelpox, and smallpox, a zoonotic viral disease [1]. Although the Mpox name implies that monkeys and other primates are the primary hosts [2], it causes a severe rash in humans, much like smallpox, caused by the OPXV genus’s variola virus. Thus, the symptoms of Mpox and smallpox are identical [3]. The first recorded case of Mpox in Africa was in 1970, that of a 9-month-old baby [4,5], and the disease subsequently spread across the continent. In 2003, an outbreak emerged after it spread to Singapore, Israel, and the UK, and, by January 2022, all six WHO regions, 127 member States had reported Mpox cases. As of 31 May 2025, WHO had reported 149,005 cases (since 2022), resulting in 359 deaths, which usually occurred among immunosuppressed hosts [6]. In US (35,002), Democratic Republic of the Congo (25,481), Brazil (14,327), Spain (8,783), Uganda (6,636), France (4,487), Mexico (4,454), Germany (4,378), Colombia (4,285), and UK (4,264) are the top 10 nations that have been impacted globally since 1 January 2022 (https://worldhealthorg.shinyapps.io/mpx_global/#sec-global). These nations account for 77.8% of global cases [7]. In the past month, Angola reported its first case [8]. More recently, the Democratic Republic of Congo reported 17,104 cases and 88 deaths between 25 November 2024 and 5 January 2025. The FDA has approved two vaccines against smallpox (ACAM2000) and smallpox/Mpox (JYNNEOS; non-replicating) [8,9,10]. Human-to-wildlife contact and expanded urbanization have increased the risks of Mpox transmission to humans [11]. Mpox comprises two genetically distinct clades: Clade II, which was formerly known as the West African clade, and Clade I, which was once known as the Central African, Congo Basin clade [12]. Clade IIa and Clade IIb are subcategories of Clade II; with a 1% fatality rate, Clade II is a milder variant of the virus, and signs include fever, chills, migraines, muscle soreness, and fatigue [13,14]. The hands, chest, face, and genital areas of individuals infected with clade IIb are covered in rashes, nodules, and vesicles. During incubation, patients are asymptomatic for 3-17 days and last for 2-14 weeks [15], and those who are immune-compromised, pregnant, nursing, or younger than one year old are more likely to suffer from severe and sometimes fatal consequences [16]. Clade I exhibits increased clinical severity, enhanced interhuman transmissibility, and elevated fatality rates. Mpox is common in Africa, and is especially prevalent in primates, non-human primates, and rodents (squirrels, Gambian signed rats, and dormice). Hunting, trapping, and handling of diseased animals or their bodily fluids is a standard mode of transmission (Figure 1). Non-human primates can be infected with the virus and exhibit symptoms similar to those of humans, while small mammals may carry the virus without showing symptoms [11]. There are no drugs specifically for Mpox [17], however, for some Mpox patients, several medications used to treat smallpox may be recommended, as they are suitable for prevention and treatment [18].
1.1. Importance of Understanding Pharmacological Approaches
Understanding the pharmacology of drugs aids in improving drug therapy and developing new and safer drugs. Pharmacological treatments against MPXV infection have mainly been studied in animal models; human trials have only recently started. Cidofovir, for example, is an antiviral medication used against cytomegalovirus, herpesvirus, poxvirus, polyomavirus, and papillomavirus [19]. It can also be used against Mpox [20]. With the advancement of biotechnology, methodologies such as microRNAs and silencing RNAs are being developed to identify suitable targets against Mpox [21]. Research into biomarker-based therapeutics advances, enabling targeted drug design for various disorders. These methods support the screening, diagnosis, and treatment of viral diseases via vaccination and adaptive therapies [22]. Combining biomarkers with in silico analysis, bioinformatics, and molecular simulations could improve drug pharmacokinetics, reduce resistance, and minimize side effects (13, 14). Another strategy involves hybridizing nanoparticles with existing drugs to enhance efficacy, targeting, and distribution (15). These approaches are currently being explored for Mpox management, which are discussed. Herein, we summarize the most recent data concerning the principal antiviral treatments for Mpox, such as brincidofovir, cidofovir, TPOXX, vaccinia immune globulin, clinical studies, case reports, randomized trials, as well as a historical perspective on pharmacology, medications, and vaccinations [23].
3. Mechanisms of Action
3.1. Viral Pathogenesis and Host Interactions
DNA viruses with genomes ranging from 150,000 to 300,000 base pairs make up the poxvirus family. Over 200 proteins involved in transcription, virion assembly, cellular entry, and genome replication are encoded by the 197 kb linear, double-stranded MPXV genome. The Mpox is a virus with an envelope 200-250 nm in size [64]. Mpox spreads via close contact between humans or animals. The respiratory or oropharyngeal mucosa is impacted by smallpox and Mpox. The virus enters through the injection site and uses ruptured tissue or mucosal membranes (those protecting the mouth, nose, eyes, urinary system, and rectum) to replicate in the surrounding tissues. It is an autonomous DNA virus that translates its viral proteins using the host’s ribosomes. However, in the cytoplasm, it can also produce its individual replicating, transcription, and mRNA-making machinery [65]. Primary viremia spreads to regional lymph nodes. Secondary viremia enters lymph nodes and organs via blood. The first symptoms of MPXV infection are usually fatigue, fever, pain, and lymphadenopathy, which can occasionally be accompanied by severe inguinal lymphadenopathy. Research into virus-host cell interactions has consistently shown striking genetic variation between Clade I and Clade II genes [66]. Viral factories are perinuclear locations where early gene transcription activities occur once the virus infects the host cells. Mpox viruses are thought to attach to parts of the extracellular matrix, glycosaminoglycans within the target cell’s surface, and proteins on the outside of the virus. The target cells’ cytoplasm receives the python’s viral envelope via low-pH enzymatic entry or plasma membrane contact at neutral pH. Poxviruses have host range factors (Hrfs) that alter the host’s virus response. As an example, the Hrf protein BR-203 inhibits the antiviral host response cell-specifically by blocking the binding of IL-1 and IL-1b receptors [67]. For mature internal and enveloped exterior virions to attach to the cell, twelve distinct kinds of viral membrane proteins must be present [68]. Once inside, the virus copies itself using a special enzyme made of multiple parts called DNA-dependent RNA polymerase. Early, intermediate, and late protein translation on the host ribosomes comes next [69]. The latent Mpox can last for two weeks. During this time, Mpox patients are usually asymptomatic and lesion-free. Chills, fever, headache, muscle soreness, and lymphadenopathy are post-latent Mpox symptoms. Men who have sex with men are experiencing a rare clinical symptom of the current Mpox outbreak: anal or vaginal rashes that spread throughout the body [70,71]. The likelihood of these severe manifestations is higher in children, older adults, HIV patients, and anyone taking immunosuppressive medications. The virus then becomes tropic to other organs and travels through the bloodstream, which is how Mpox can lead to secondary viremia [66].
The Mpox entry, replication, and release in host cells are depicted in the diagram. Upon nucleation, the virus releases itself into the host cell through endocytosis. Its DNA is released into the cytoplasm. Proteins produced by viruses are the product of transcription and DNA replication. Newly formed virions undergo exocytosis after assembly and maturation in the Golgi apparatus. To prevent Mpox from spreading, various antiviral medications target distinct steps in the viral replication cycle. These include CDV, BCV, NIOCH-14, and TPOXX (Figure 2; site of action shown in red).
3.2. Targeting Viral Replication
Targeting viral replication in MPXV requires an understanding of the virus’s life cycle, identifying essential components required for its replication, and developing strategies to interfere with these processes. As Mpox is a double-stranded DNA virus, viral enzymes are used for transcription and DNA replication, which occurs in the host cells’ cytoplasm. MPXV infection and reproduction are in three stages (Figure 2): (i) invasion of the virus; (ii) synthesis of viral proteins and replication; and (iii) viral assembly, maturation, and release [72]. Several envelope proteins that enable the virus to penetrate host cells may be attractive targets for antivirals against MPXV, as the absence of a receptor has been identified on the host cell membrane. The interference of viral genome DNA or RNA synthesis aids in the development of MPXV antivirals [73]. CDV is a powerful antiviral against OPXV. Unlike CDV, BCV has superior bioavailability and lower nephrotoxicity since its metabolism does not depend on the renal ion pathway. Both drugs work by inhibiting DNA polymerase, thereby preventing the virus from spreading. On the other hand, TPOXX works by targeting the viral envelope, a crucial component that allows the virus to infect host cells and replicate. By inhibiting the formation of this envelope, TPOXX effectively blocks the virus from maturing and spreading, thus preventing its ability to replicate within the body [74]. NIOCH-14, an antiviral currently undergoing clinical testing, acts as a nucleoside analogue that integrates into the viral genome during replication. By incorporating itself into the viral RNA or DNA, it disrupts the replication process, preventing the virus from multiplying and spreading within the host [75]. The cytoplasmic replication of DNA viruses is dependent on DNA-dependent RNA polymerase (DdRp). DdRp’s biological relevance makes it a potential Mpox therapeutic target. Using computational screening, modelling, docking, and molecular dynamics, further potential drug inhibitors can be identified [76]. In addition, RNA interference (RNAi) was shown to reduce Mpox replication in a sequence-specific and efficient way. As such, 48 siRNA constructs targeting 12 Mpox genes in 12 pools on viral replication were evaluated. The siRNAs’ effects on Mpox replication varied in strength. Intense antiviral action was demonstrated by two siRNA pools, which decreased virus replication below 10% of that observed in untreated control cells. At an IC50 of less than 10 nM, a single siRNA construct targeting the A6R gene prevented the spread of viruses almost entirely [77,78]. SiA6-a similarly suppressed all virus replication at 20 nM and CDV at 100 nM [79]. SiRNA molecules effectively target the A6R and E8L genes (involved in immune evasion and replication) of Mpox, and SiA6-a and SiE8-d, respectively, considerably reduced Mpox replication [79]. In addition, compounds from the ReFRAME and NPC libraries that inhibit other RNA virus families were also noted to inhibit vaccinia virus and Mpox, suggesting they could be effective against multiple viral infections [80,81,82,83,84]. As with most antivirals that target viral protein function, the researchers explored compounds that target host components to prevent viral escape mutations. These results also point to the use of host (ReFRAME and NPC drugs) and viral (TPOXX) combinations to treat OPXV infections [82,85].
3.3. Modulation of Host Immune Responses
The severity and outcomes of MPXV infection are greatly affected by the host immune response, with MPXV proteins manipulating the host immune pathways and responses such as complement activation, inflammatory signalling, cytokine production, NF-κB regulation, and suppressing natural killer cells. Mpox encodes several BCL-2-like proteins, including A47, B13, P1, C6, and D11, which play a key role in immune evasion and persistence within the host [86,87]. The E3 protein, which is also produced by vaccinia virus, binds to double-stranded RNA and suppresses antiviral responses by blocking the protein kinase R pathway. The homologous protein F3, which Mpox expresses, has its N-terminus truncated [88], implying that additional Mpox proteins would make up for the partial loss, but have not yet been identified. Mpox uses a variety of strategies to inhibit innate immune responses actively. For example, the MPXV B19 protein directly inhibits the transcription factor IRF3, which is essential for the production of IFN-α/β. As such, the B19R gene reduces viral infection. MPXV also encodes several ankyrin-like proteins (B17R, D9L, J1R, N4R, J3L, D1L, D7L, O1L, C1L, and B5R) that inhibit NF-κB activation which modify host immune responses [89,90]. Understanding how MPXV modulates host immune responses is essential for developing effective antivirals to overcome its immune evasion strategies, ultimately reducing the impact of MPXV infections.
3.4. Challenges in Understanding Mechanistic Pathways
As Mpox is an emerging global health threat that has spread internationally, sensitive diagnostic methods are limited to a few national reference laboratories. Understanding the molecular pathways of Mpox is challenging due to a lack of effective animal models that replicate human transmission, pathogenic mechanisms, and outcomes such as morbidity and mortality. While mice, black Prairie dogs, African rope squirrels (Funisciurus anerythrus), and Gambian pouched rats (Cricetomys gambianus) are used, the virus does not infect them the same way as they do humans. In addition, the mechanism of how monocytes, macrophages, neutrophils, and dendritic cells contribute to viral transmission requires further work. Although the smallpox vaccine provides partial cross-protection against Mpox, its effectiveness against emerging Mpox mutations is still being studied [4,91,92,93]. Further, understanding the molecular basis of Mpox, such as immune evasion, replication, and spread, as well as viral mutations, will aid in the development of effective treatments and vaccines, as well as understanding host-host transmission [94,95]. As infection with Mpox shows similar symptoms initially (fever, lymphadenopathy, headache, muscle ache) to other viruses, such as smallpox, chickenpox, or hand-foot-mouth disease, diagnosis could be challenging and requires laboratory testing. Mpox, however, does show distinct features of skin lesions and could help identify Mpox at later stages. Identification and isolation of infected people are essential, as is maintaining adequate hand hygiene and sanitation, to reduce the risk of MPXV infection and transmission. Further, it is essential to understand the mechanistic pathways of Mpox as its interaction with the host immune system is quite complex. All these factors complicate the development of antivirals against Mpox.
4. Challenges in Drug Development
4.1. Barriers to Effective Therapeutics Development
Developing treatments for MPXV infection is complicated because of its many biological components. These include a limited understanding of virus-host dynamics, medication development challenges, vaccination distribution inequities, and global health initiatives for emerging diseases. Through the development of Mpox drugs, insights into drug repurposing, small-molecule drugs, AI-driven drug target discovery, antibody treatments, and preclinical drug development have been gained, advancing strategies for more effective therapies and enhancing the overall understanding of Mpox treatment options [71,96]. Regarding treatments, CDV has potent antiviral properties; however, it is not easily absorbed by the body, and in patients on dialysis or with renal failure, the metabolites can accumulate in the proximal tubular cells, leading to kidney damage [97,98]. In this regard, BCV was developed to eliminate these side effects. The FDA allowed BCV as a treatment for smallpox in 2021 after it was shown to work better at being absorbed and converted in the body due to lipid conjugation technology. However, as noted in the earlier section above, BCV causes increased liver enzymes and is not as well tolerated compared to CDV, and many clinical studies were prematurely stopped. As such, it is essential to consider the following: (i) Drug delivery and specificity should be enhanced to target Mpox at the infection site effectively; (ii) To prevent drug-resistant strains and maintain therapeutic efficacy, several anti-MPXV drugs should be developed, with each drug targeting different phases of MPXV infections; (iii) Several variations should be developed targeting different regions of the virus; (iv) Considerations for sequential and combination medication regimens; and (v) pharmacological adjustments to decrease toxicity and adverse reactions [99,100].
4.2. Regulatory Considerations and Clinical Trial Design
Mpox classification as a public health concern and the need for effective therapies and diagnostics influence the regulatory framework surrounding the disease. International regulators, including EMA and ICMRA, published a report outlining the outcomes of the discussions on the development, testing, and availability of MPXV antivirals and vaccines. Additionally, the FDA, JPMDA, and WHO reviewed the general characteristics, regulatory status, and available evidence for various Mpox vaccines and therapeutics [101,102]. Antivirals are the first focus in the DRC, where mortality is highest, particularly among children. To prevent infection from smallpox and Mpox, the MVA-BN (modified vaccinia Ankara-Bavarian Nordic, brand name JYNNEOS, also referred to as Imvamune, Imvanex) vaccine has been used safely in the United States [103] in children since the FDA gave it emergency use clearance (EUA). Regulatory approval routes for novel vaccines should be evaluated, along with alternatives to placebo-controlled trials, such as animal models and clinical immune-bridging, where placebo studies are not feasible. According to the study, 302 participants received a placebo and 295 people received TPOXX. The median duration from randomization to lesion resolution was 7 days with tecovirimat and 8 days with placebo. The competing-risks hazard ratio for lesion resolution was 1.13 (95% CI, 0.97 to 1.31; P=0.14). Results were similar for those who started the study regimen within 7 days of symptom onset. Tecovirimat did not reduce lesion resolution days in clade I MPXV individuals with Mpox. Researchers found no safety issues. NIAID and others funded PALM007 ClinicalTrials.gov number, NCT05559099 [104]. Currently, studies are also determining the effects of TPOXX and JYNNEOS vaccine combination in a multicentre, randomized, placebo-controlled, drug-vaccine interaction phase 2 study given 4 weeks apart, and the potential supporting the combined use of these drugs for post-exposure prophylaxis [105]. BCV, along with TPOXX, is the only antiviral eligible for clinical trials, requiring careful monitoring of patient safety. The STOMP (Study of TPOXX for Human Mpox) clinical trial is still ongoing, and only interim findings have been made publicly available to evaluate the safety and effectiveness of TPOXX for treating clade II Mpox. The prevalence of TPOXX-resistant Mpox forms in clinical Mpox instances, particularly in immune-compromised individuals receiving long-term therapy, suggests that the drug’s insufficiency or resistance may cause the lack of efficacy. The new emergence of clade Ib Mpox in the DRC and Sweden, along with findings from the international clinical study STOMP (NCT05597735), noted that there is a need for new antivirals due to TPOXX not being effective against both clades [106]. Further, in an attempt to improve the JYNNEOS vaccine and allow more individuals to be vaccinated, a much lower dose, as much as 80% has been tested, via the same subcutaneous route, did not lower the effectiveness of the vaccine [107,108]. The vaccine options evaluated were ACAM2000 (second-generation vaccine against smallpox; Sanofi Pasteur) and LC16m8 (live attenuated smallpox vaccine derived from vaccinia virus; Sumitomo Dainippon Pharma Co., Ltd.). In addition, single-dose vaccines, especially in endemic areas, are an option, and given that mRNA vaccines are being evaluated against Mpox (mRNA-1769; Moderna), this could be a possibility [108]. As such, the findings support the vaccine’s potential and support clinical testing for orthopoxvirus protection, including Mpox, and for future pandemic prevention.
4.3. Need for Comprehensive Pharmacovigilance
The Mpox outbreaks show how important pharmacovigilance is for ensuring that antivirals and vaccines are safe and effective. Due to the disease’s global prevalence (Figure 3a) and ability to transmit zoonotically, robust monitoring methods are necessary to identify adverse reactions to antivirals and vaccines, assess the effectiveness of immunizations, and provide real-time data for public health measures. Additional clinical research and pharmacovigilance monitoring in high-risk groups are necessary to achieve herd immunity and effectively counter Mpox. Healthcare facilities must improve social and safety containment, monitoring, diagnostics, and infection prevention and control. Global efforts to provide vaccines, context-based risk communication, public awareness, and public engagement must prioritize the most vulnerable groups, such as the poor and wealthy living on the outbreak’s edges and those in the most affected areas. A complete immunization plan is encouraged to prevent Mpox cases from increasing exponentially, which could pose a pandemic risk. Thus far, ACAM2000 and JYNNEOS smallpox vaccines are most suitable for laboratory workers, healthcare professionals, and frontline staff who may be exposed to MPXV in their workplace [109,110]. Further clinical trials and pharmacovigilance monitoring for at-risk groups are required to assess the safety and effectiveness of currently available vaccinations to acquire herd immunity against Mpox. These include implementing social and safety containment measures, improving hospital infection prevention and control, and enhancing surveillance diagnostics. In the current Mpox outbreak, coordinated efforts should be made to contain the spread, such as equitable risk sharing, public engagement, effective vaccine distribution, and tailored risk communication strategies for disadvantaged and vulnerable groups [110].
5. Next-Generation Therapeutic Approaches
5.1. Computational and Bioinformatics Approaches
Current trends in drug discovery include the repurposing of existing therapeutic molecules and the discovery of fresh lead compounds and possible molecular targets from natural sources. By combining computational techniques with biological research, bioinformatics has quickly developed into a crucial field (Figure 3b). When computational methods for protein sequence analysis emerged in the early 1960s, bioinformatics was established. Simultaneous developments in molecular biology methods made DNA analysis easier and allowed for more effective genetic data analysis, sequencing, and interpretation. Innovations in bioinformatics were a result of advances in computer science, which also produced more advanced software and more potent computer systems that improved the capacity to evaluate and comprehend intricate biological data [111,112]. Recent research has shown that using computational methods to repurpose FDA-approved drugs is an effective strategy for identifying drug targets for several diseases, including Mpox [113,114]. Statistical biology, data analysis, machine learning, and AI work together to identify lead drug candidates with optimal drug probability, pharmacokinetic properties, and toxicity profiles for development [115]. Computational models not only reduce costs and time, they also provide information regarding how to validate the results in experiments. As a result, the development of molecular docking and molecular dynamics techniques has increased the significance of computational research in the development of antivirals [116,117]. Common docking tools include Dock, Autodock, Gold, Gide, Zdock, Rdock, FlexX, AutoDock-4, and Autodock-Vina [118]. Virtual screening tool PyRx is used in computational drug discovery to match chemical groups to therapeutic targets. GOLD-Chemscore rates macromolecule-small molecular docking program. Run simulations with Molegro Virtual Docker, another docking simulation application [119]. Several FDA-approved drugs with the most active compounds against Mpox proteins, as well as model validation for MPXV cysteine proteinase, DNA polymerase, early transcription factor and DNA topoisomerase are described in Table 1. One negative issue of using computational techniques to screen for antivirals for MPXV is that these methods do not capture the complexity of biological in vivo physiology. While computational models can predict drug interactions and efficacy, they are not able to predict potential side effects in humans. Furthermore, the quality of the data that is currently available determines how accurate the projections are, which could restrict their dependability, particularly for recently discovered illnesses like Mpox.
Identifying and combining CD4 and CD8 T cell epitopes as well as B cell epitopes through a multi-epitope approach is necessary for developing effective vaccines. Strong multi-epitope vaccines stimulate humoral and cellular responses using antigenic peptide sequences that overlap B- and T-cell epitopes [120,121]. To improve the immunogenicity of the vaccines, bioinformatics approach combined with machine learning algorithms, can be used to identify enhancers by analysing large datasets from experimental studies; such enhancers can be branched peptides, adjuvants, immune modulating agents [122]. This approach significantly reduces time, money, and risk of failure in vaccine development. In vitro and in vivo assays are expensive, labour-intensive, potentially toxic, can induce allergic reactions, and often result in high rates of clinical trial failure. Employing bioinformatics technologies to identify non-toxic and non-allergenic antigens for a disease can conserve time and resources [123]. On the contrary using bioinformatics and prediction algorithms to develop vaccines does not fully account for the complexity of the immune system, complexities of pre-existing immunity and potential adverse effects. As a result, vaccines developed primarily through bioinformatics and prediction algorithms requires extensive clinical testing to confirm their safety and efficacy.

Table 1.
FDA approved drugs repurposed to target Mpox identified using computational studies.
| Drug Name | Drug Bank ID | Protein Interaction | Mode of Action | Refs |
|---|---|---|---|---|
| Eluxadoline | DB09011 | Mu-opioid receptor | Serves as both an agonist and an antagonist of mu-opioid receptors | [125] |
| Dihydroergotamine | DB00630 | 5-HT1B and 5-HT1D serotonin receptors | Vasoconstrictor, primarily used for migraine treatment | [126] |
| Tobramycin | DB00583 | 30S ribosomal subunit | Inhibits bacterial protein synthesis | [125] |
| Nebivolol | DB01298 | Beta-adrenergic receptors | Selective beta-1 blocker with vasodilating properties | [125] |
| Pimozide | DB00501 | Dopamine D2 receptor | Antipsychotic that blocks dopamine receptors | [126,127] |
| Triptorelin | DB00112 | Gonadotropin-releasing hormone receptor | GnRH analog that inhibits gonadotropin release | [126] |
| Carfilzomib | DB08892 | Proteasome | Proteasome inhibitor used in cancer therapy | [126] |
| Tolvaptan | DB06155 | Vasopressin V2 receptor | Vasopressin receptor antagonist used for treating hyponatremia | [126,127] |
| Cobicistat | DB09019 | Cytochrome P450 3A4 | CYP3A inhibitor that increases the effectiveness of certain HIV medications | [126] |
| Conivaptan | DB04874 | Vasopressin V1A and V2 receptors | Dual vasopressin receptor antagonist used for hyponatremia treatment | [126,127] |
| Tenapanor | DB11607 | Sodium/hydrogen exchanger NHE3 | Inhibits NHE3 to reduce sodium absorption in the intestine | [126] |
| Fludarabine | DB00336 | DNA polymerase | Antimetabolite that interferes with DNA synthesis in cancer cells | [28,127,128] |
| Tigecycline | DB02280 | Bacterial ribosomal subunit | Tigecycline, a glycylcycline, binds to the 30S ribosomal subunit and prevents amino acyl tRNA molecules from entering the ribosome’s A site, therefore inhibiting protein translation in bacteria | [127] |
| Eravacycline | DB12329 | DNA-dependent RNA polymerase | Broad-spectrum antibiotic; inhibits bacterial protein synthesis. | [127] |
5.2. Pipeline Pharmaceuticals and Vaccines Against Mpox
The development of pipeline for the treatment for Mpox has advanced significantly within the last few years. Currently Mpox vaccines include, JYNNEOS, LC16m8, Imvanex, ACAM2000, Orthopox vaccine (Figure 4, Table 2), which were mainly developed against vaccinia virus but is cross-protective against Mpox pre-clinical / animal studies (Table 3), (human clinical trials) (Table 4) Testing in primates, prairie dogs, mice, the Mpox pipeline (Table 2) show safety and immunogenicity. Evaluated for antiviral efficacy, including combination therapy with antivirals, are also being evaluated [129].
Attenuated viral vaccines, like NYCBHAE3L [133], showed high survival rates and fewer lesions following the Mpox challenge in cynomolgus monkey tests as compared to non-vaccinated controls. As in cynomolgus monkeys and prairie dogs, Dryvax, when used in combination with TPOXX, induces sustained immune responses [134] and protects mice from viral challenge. Depending on when administered, these vaccines’ post-exposure efficacy varied, but they both decreased viremia and generated neutralizing antibodies [135]. The development of non-replicating Mpox vaccines like JYNNEOS and ACAM2000 has advanced. The ACAM2000 works well. However, it can have serious side effects, like heart issues. In animal experiments, JYNNEOS exhibited robust immune responses in non-human primates, significantly diminishing illness severity and viral load. ACAM2000 offered protection but exhibited potential cardiac problems, such as myocarditis. In humans, JYNNEOS was, associated with minor cardiovascular adverse events such as tachycardia, palpitation, electrocardiogram changes such as T wave inversion, and ST elevation. Nonetheless, ACAM2000, has been reported to have major cardiovascular adverse events such as myocarditis, dilated cardiomyopathy, and heart failure [136,137].
The Mpox research program includes different antiviral and vaccine studies focused on tackling Mpox. Importantly, TPOXX has been assessed for lesion recovery and viral shedding in research carried out in Brazil, Europe, and the Democratic Republic of the Congo (DRC). The PALM007 study (NCT05559099) targeted adults and children affected by Clade I Mpox in the DRC, whereas the STOMP trial (NCT05534984) included participants with Clade II Mpox in the U.S. and additional nations [138]. No safety concerns were identified in PALM007 [104]. Furthermore, Phase 4 trials for Bavarian Nordic’s smallpox vaccine have taken place in Nigeria and Uganda. Safety and immunogenicity assessments have also been conducted for NIOCH-14 and VACΔ6 in Russia, alongside LC16m8 in Colombia. Additionally, preclinical findings from the UK regarding BNT166a mRNA vaccination studies (NCT05988203) indicate robust protection. This Phase I/II study intends to assess the safety, tolerability, reactogenicity, and immunogenicity of BNT166a for active immunization against Mpox in adults between 18 and 65 years, conducted at sites in the US and UK, projected to conclude in May 2025 [139].
Table 3.
Preclinical Mpox vaccines and animal models.
| Vaccine Description | Animal Model | Key Findings | Refs |
|---|---|---|---|
| Canine distemper virus (CDV) and Vaccinia immune globulin (VIG) | EiJ mice (aged 6–12 weeks) | Immunological responses and protective effectiveness | [140] |
| Dryvax vs non-vaccinated Control | Prairie dogs | Viral pathophysiology and vaccine-induced immunity | [141] |
| Sham-vaccinated and Elstree-RIVM vaccine | Cynomolgus macaques (Macaca fascicularis) | Evaluated the safety of vaccines and protective immunity; safe and immunogenic | [142] |
| Attenuated virus NYCBH-AESL (E3L Gene Deleted) | Cynomolgus monkeys | Examined the immune system’s reaction to genetic changes | [143] |
| Modified vaccinia Ankara (MVA) | Cynomolgus monkeys | Demonstrated safety and immunogenicity of MVA-based vaccines | [144] |
| Recombinant MVA | Rhesus macaques (Macaca mulatta) | Explored enhanced immunogenicity through genetic modifications | [145] |
| MVA or Dryvax | Cynomolgus monkeys | Immune responses to conventional and modified vaccinations were compared | [146] |
| Dryvax and TPOXX | BALB/c mice | Evaluated the combined effect of vaccination and antiviral treatment which was shown to be effective | [147] |
| JYNNEOS or ACAM2000 | Cynomolgus monkeys | Compared efficacy and safety profiles of both vaccines, with safety profiles | [148] |
| LC16m8 and Lister (Elstree Strain) | Cynomolgus monkeys | Immunogenic and safe | [149] |
| Dryvax, ACAM2000, or JYNNEOS | Prairie dogs | Vaccine induced protection | [150] |
| JYNNEOS or ACAM2000 | Prairie dogs | Vaccine efficacy against orthopoxvirus infections. | [151] |
| Live smallpox vaccine | BALB/c mice | Immune responses and durability of immunity | [152] |
| ACAM2000 and TPOXX | Cynomolgus monkeys | Synergistic effects of vaccination and antiviral therapy | ([153] |
| Dryvax | Cynomolgus monkeys | Safety and long-term immunity of vaccines | [154,155] |
| Brincidofovir | Black-tailed prairie dogs | Examined the effectiveness of antiviral drug in treating poxvirus infections which showed good responses | [44] |
Table 4.
Human clinical trials against Mpox [156].
Table 4.
Human clinical trials against Mpox [156].
| InterventionTrial No. | Country | Year (Phase), Status | Number of Subjects | Primary Endpoints | Key Findings |
|---|---|---|---|---|---|
| TPOXX NCT05597735 |
Brazil | 2024 (3), recruiting | Not specified | Reduction of illness duration and contagiousness | The primary result is the duration required for the healing and re-epithelialization of all visible lesions (skin and mucosal). |
| TPOXX Oral Capsule NCT06156566 |
Belgium, France, Spain | 2024 (4), ongoing | 150 | Anal pain assessments using the health-related symptom Index, on days 7, 14, and 90 |
The health-related Symptom Index was utilized to evaluate anal pain on days 7, 14, and 90. From the 28th day of randomization until the first day, every lesion was fully healed and new skin grown |
| TPOXX Oral Capsule NCT05559099 |
The Democratic Republic of the Congo | 2022 (Randomized, placebo-controlled, double-blind study) completed | 597 | The time to lesion resolution, measured in days until all lesions are scabbed or a new layer of skin is developed |
Without posing any serious safety risks, the treatment greatly decreased viral shedding, accelerated lesion healing, and alleviated symptoms. |
| TPOXX (antiviral medication) NCT00728689 |
United States | 2008 (1), completed | 12 | A single dose of ST-246 Form I versus Form V was tested for pharmacokinetics and safety in healthy volunteers | The study found no serious adverse events with ST-246 Form I and Form V. Pharmacokinetic parameters were similar for both forms |
| MVA-BN (JYNNEOS) NCT06549530 |
The Democratic Republic of the Congo | 2024 (2), ongoing | 460 | Two weeks after the second MVA-BN injection, serum neutralizing antibodies against the vaccinia virus were measured using plaque reduction neutralization tests (PRNTs). | Test MVABN standard regimen neutralizing antibody response durability |
| JYNNEOS (vaccine for the prevention of smallpox and Mpox) NCT05512949 |
United States of America | 2022 (2), completed | 229 | The PRNT assay was used to analyse venous blood on Study Day 43 to determine if the intradermal regimen of 2x107 TCID50 MVA-BN and 1x107 TCID50 MVA-BN were non-inferior to the licensed subcutaneous regimen of 1x108 TCID50 MVA-BN | At six weeks, the dose-sparing intradermal Mpox immunization regimen induced antibody responses comparable to the conventional regimen. The vaccine was found to be safe |
| Bavarian Nordic smallpox vaccine NCT05745987 |
Nigeria, Uganda | 2024 (4), ongoing | 1560 | Degree of symptoms and RT-PCR-confirmed Mpox |
This research will ascertain whether the smallpox vaccine lessens the frequency of recurrent infections and the intensity of symptoms in those who have been exposed to Mpox. |
| MVA-BN vaccine NCT05734508 |
The Democratic Republic of the Congo | 2023 (4), completed | 500 | New drug healing time and symptom reduction |
The MVA-BN vaccine was safe, with no serious adverse events. Minor injection-site reactions were most common |
| NIOCH-14 (National Institute of Occupational Health and Safety) NCT05976100 |
Russian Federation | 2020 (1), completed | 90 | Monitoring various blood parameters (like erythrocyte, leukocyte, and platelet levels), biochemical markers (such as glucose and creatinine levels), and the occurrence of adverse events over time | NIOCH-14 was determined to be safe and well-tolerated in healthy volunteers; no significant adverse effects were noted |
| VAC∆6 vaccine NCT05846243 |
Russian Federation- Novosibirsk Region | 2021 (2 and 3), completed | 334 | The percentage of vaccinees with a titre of virus-neutralizing antibodies to vaccinia virus ≥ 1:40 | VAC∆6 vaccine was safe and well-tolerated, with no adverse and only mild reaction at the site of injection |
| LC16m8 live attenuated vaccine of vaccinia virus NCT06223919 |
Colombia | 2024 (3), active, not recruiting, Replicative live attenuated vaccinia virus vaccine: A randomized trial | 8686 | Based on each cohort’s Poisson distribution, the laboratory-confirmed Mpox incidence rate will be computed with a 95% CI. To assess efficacy, immunogenicity and, safety | The vaccine was well-tolerated, with no serious adverse events observed. |
| BNT166a (mRNA vaccines by BioNTech NCT05988203 |
United Kingdom | 2023 (2), Active, not recruiting, A Phase I/II randomized, partially observer-blind, dose-escalation trial of investigational RNA-based Mpox vaccine | 96 | The proportion of individuals who experienced at least one adverse event of special interest (AESI) between Dose 1 and day 201 after dose 1, inclusive. Overall, Safety and immunogenicity | No clinical results are published yet. Preclinical studies showed strong immune responses and full protection in animal models. |
6. Pharmacological Landscape: A Comparative Analysis
The pharmacological landscape for Mpox evaluates both existing and new vaccines and antivirals to overcome disease. While Mpox symptoms are generally less severe as those of smallpox, Mpox can still cause significant disease. As described thus far, the pharmacological landscape to Mpox includes, supportive care, antivirals and vaccines. A comparative analysis of these treatment options are summarised as follows:
Supportive care and management
- Whilst Mpox is self-limiting and usually resolve without treatment. Those with symptoms can be managed with anti-histamines for rashes, pain relief medications for headache and muscle aches, topical creams (such as antiseptics, hydrocortisone) for skin lesions, and regular hydration. In rare instances complications such as pneumonia, secondary bacterial infections, eye infections and encephalitis may occur, and medical help is advised. In such instances antivirals may be used based on the specific circumstances. Vaccines are used to prevent further spread during outbreaks.
- Individuals positive for Mpox are generally isolated to prevent spread and during outbreaks personal protective equipment such as masks, hygiene practices and social distancing are encouraged.
Antivirals
- TPOXX, approved by the FDA as a smallpox antiviral, has been shown to be effective against Mpox, reducing the mortality rate from 3.6% to 1.7% [157]; but was not effective against clade I Mpox lesions. It is currently used as a frontline treatment.
- CDV an antiviral that inhibits the synthesis of viral DNA, is used to treat MPXV, in particular those with severe diseases or who have not responded to TPOXX.
- BCV a derivative of cidofovir has been investigated to treat Mpox. Its mechanism of action is similar to cidofovir with better safety profile to cidofovir. Both CDV and BCV have been shown to considerably reduce the viral replication of Mpox clade IIa and IIb [51].
- The development of drug-resistant Mpox strains emphasizes the requirement for continuous research and surveillance to develop new antivirals or use of combination treatments [158].
- New experimental therapies are currently being developed and tested, including vaccinia immune globulin, antibodies targeting the vaccinia virus that may also cross-react with Mpox, and repurposed drugs identified through computational and biological testing for their potential effectiveness in treating Mpox.
Vaccines
- JYNNEOS vaccine against smallpox and Mpox, a modified non-replicating vaccinia Ankara virus is safe, provides strong immune responses to both smallpox virus and Mpox, and is the preferred vaccine for use during Mpox outbreaks.
- ACAM2000 vaccine against smallpox, is a live vaccinia virus vaccine and is restricted in its use against Mpox, especially in those who are immunocompromised; it has shown some protection against MPXV infections.
- JYNNEOS and ACAM2000 are regarded as safer alternatives to the older smallpox vaccines, like Dryvax, which were used during the smallpox eradication effort. While effective, the older smallpox vaccines use live, replication-competent vaccinia virus vaccine, and their use is not preferred due to the risks associated with live virus vaccines.
- LC16m8 has received emergency use authorization, LC16m8 shields animals from deadly dosages of viruses like Mpox. Little information is available on LC16m8 usage during Mpox outbreaks. The virus in LC16m8 is weakened. Itching, redness, swollen lymph nodes, fever, and exhaustion are some of the side symptoms. The vaccine virus has the potential to spread to other bodily parts. To date, LC16m8 has been donated to over 90,000 individuals. These dosages did not result in any notable safety signals, even in 50,000 youngsters. Pregnant women, those with specific skin conditions, and immunocompromised individuals should not get LC16m8 [159].
7. Future Directions in Mpox Research
7.1. Integrating Mechanistic Insights into Drug Development
Mechanistic insights into Mpox replication provide important targets for antiviral intervention. For the development of antivirals, investigating immune evasion mechanisms and virus host interactions is still essential. The focus of research is on comprehending the entire lifecycle of the Mpox, from entry to replication and assembly. One idea is that the Mpox ability to change the way host cells work, for example, by turning the endoplasmic reticulum into replication factories, may make it more resistant to immune responses and apoptosis, opens up new treatment targets. High-throughput screening techniques improve our understanding of the host factors that viruses use, while research continues to understand the pathogenetic and structural mechanisms, replication processes, and interactions of the Mpox with the innate immune system [95,160]. Despite achievements, further research is required to develop treatments for Mpox to prevent drug-resistant strains and long-term outbreaks. Improving the specificity and accessibility of antiviral, preventing resistant strains, and evaluating combination therapy to treat various infection stages are required. Reducing side effects requires lowering drug toxicity. Pharmaceutical development must be rapid and robust to combat the global Mpox outbreak and prepare for future public health emergencies [161,162].
7.2. Collaborative Efforts in Global Health Contexts
Collaboration between governments, research institutions, and health organizations has increased significantly as a result of the global response to Mpox. These collaborations concentrate on developing antivirals, re-purpose drugs, vaccines, monitoring, diagnosis, and provide equal access to care. Global health agencies like the WHO and the Centers for Disease Control and Prevention (CDC) are imperative to global efforts to combat Mpox due to their monitoring of outbreaks, support research, and advise nations on containment strategies. The Clade IIb-driven global Mpox outbreak in 2022-2023 highlighted the necessity of concerted efforts as cases extended outside of Central and West Africa’s endemic areas. Further, Clades Ia and Ib are also in circulation, with Clade Ib most recently being detected outside of Africa [163,164]. Vaccination campaigns continue to be a top priority, especially for high-risk groups. Global collaboration efforts are necessary to prevent future outbreaks, strengthening disease surveillance, increasing data sharing, and strengthening public health infrastructure. The success of prevention, control, and treatment strategies for Mpox and other emerging infectious diseases relies on a coordinated global response [165].
7.3. Potential for Personalized Medical Approaches
Personalized medicine customizes medical treatments based on unique characteristics, preferences, and genetic profiles, potentially improving the efficacy of interventions for diseases such as Mpox. Vaccines can be used in personalized medicine to direct vaccination strategies based on an individual’s specific health needs, genetic makeup and whether they are immunocompromised, in order to reduce side effects and improve outcomes [166]. In addition, artificial intelligence (AI) driven proficiency can improve patient outcomes by making it easier to develop personalized treatment plans that are specific to each patient’s needs [167,168]. AI uses patient data to recommend personalized drugs, increasing the effectiveness of treatment and reducing adverse effects [169]. Incorporating AI into healthcare processes for Mpox management is expected to improve productivity and reduce diagnostic errors [170]. AI can be used to tailor treatments by adjusting them based on patient information, such as underlying health conditions, previous vaccination history and immune status [171]. The PoxApp (https://poxapp.stanford.edu/) was developed as a mobile application to support a personalized medical approach to monitor and manage symptoms or diagnosis of Mpox cases (and other pox-related diseases). By providing real-time data on symptoms, exposures, and patient progress, it assists in personalized treatment decisions, offers diagnostic support, and monitors the effectiveness of interventions, leading to a more tailored and efficient response to outbreaks. Furthermore, a new personalized medical approach using an image-based deep convolutional neural network (MPXV-CNN) shows promise in detecting MPXV infections earlier, which could help prevent outbreaks by identifying characteristic skin lesions. MPXV-CNN has shown to have strong sensitivity and specificity across different skin tones and body regions. As such, MPXV-CNN is accessible through a web-based app for patient guidance, enhancing early detection and isolation efforts [172]. Correct diagnosis of MPXV infection necessitates laboratory validation, since clinical symptoms alone cannot be differentiated from other poxvirus infections. PCR testing of viral DNA from lesion samples (scabs, discharge, or vesicular lesions) continues to be the WHO-recommended gold standard diagnostic technique; however, specimens need to be preserved under sterile, cool, and dark conditions. Other diagnostic methods consist of immunohistochemistry, viral cultures obtained from nasopharyngeal or oropharyngeal swabs, evaluation using electron microscopy, and serological antibody analysis through ELISA. Samples obtained from vesiculopustular rashes or vesicular lesions usually provide the most precise outcomes [173]. As the recommended technique for identifying MPOX infections, PCR testing can improve infection control strategies by facilitating the early diagnosis of new cases [174]. Given its effectiveness, the Mpox vaccine ought to be made available to everybody who could be at risk of contracting the disease. To guarantee prompt diagnosis and suitable treatment, professionals need to be aware of the distinctive signs and symptoms of Mpox, a disease that is a constantly changing worldwide health concern.
8. Limitations
This review has several limitations. First, although it provides a comprehensive overview of current antiviral agents and vaccines for Mpox, much of the clinical evidence remains limited to observational studies, animal models, or early-phase trials, reducing the generalizability of findings to broader populations. Second, the effectiveness of treatments against Clade I and emerging variants of Mpox is not fully established, and data are especially lacking in vulnerable populations such as children, pregnant women, and immunocompromised individuals. Third, the computational drug repurposing strategies discussed require further experimental validation before clinical application. Finally, while global disparities in access to therapeutics and vaccines are acknowledged, this review does not address in-depth the socio-political and logistical barriers to equitable distribution, which remain critical for effective Mpox control worldwide.
9. Conclusions
A comprehensive approach to the prevention, treatment, and control of Mpox is essential as the virus poses an increasing threat to global health. Herein, we highlighted the challenges and progress in combating MPXV infections. While antiviral drugs such as TPOXX, BCV, and CDV show promise, further clinical trials are required to confirm their effectiveness and safety. TPOXX, which targets the F13L protein essential for viral envelope formation, plays a key role in modern treatment strategies. However, its limited efficacy against clade I variants highlights the need for new antivirals with broader effectiveness. Vaccination remains the most effective prevention method, with JYNNEOS and ACAM2000 leading the efforts. These vaccines, derived from the vaccinia virus, offer cross-protection against Mpox. Advancements in vaccine technologies, like mRNA and viral vectors, are transforming immunoprophylaxis, but equitable vaccine distribution, especially in endemic areas, remains a significant challenge. Research on Mpox replication and immune evasion has highlighted treatment targets, and host-directed therapies are gaining attention for improving antiviral efficacy. Despite progress, challenges such as limited animal models, viral mutations, and resource scarcity slow down treatment development. Computational biology and bioinformatics offer promising solutions for faster therapeutic identification and mutation prediction. Addressing Mpox requires global collaboration among researchers, policymakers, and agencies (CDC, WHO) to improve monitoring, diagnostics, and health measures, ensuring fair access to treatments and preparedness for future pandemics.
Author Contributions
Sh.S: Writing–original draft, Conceptualization. R.S: Writing–original draft. S.B.S: Formal Analysis, Resources, Writing–review and editing. ArM: Writing–review and editing. M.T.: Writing–review and editing. F.A.: Writing–review and editing. S.K: Writing–review and editing. G.S.N: Formal Analysis, Resources, Writing–review and editing. R.R.B: Formal Analysis, Resources, Writing–review and editing. P.S.: Writing, review, and editing, Supervision. A.M: Writing–review and editing, R.M.: Writing–review and editing. J.D.A.E.: Writing–review and editing. A.J.R.M.: Writing–review and editing. V.A.: Writing–review and editing, Supervision.
Funding
The current article processing charges (publication fees) were funded by the Facultad de Ciencias Médicas (FCM) (2-03-01-01), Universidad Nacional Autonoma de Honduras (UNAH), Tegucigalpa, MDC, Honduras, Central America (granted to Zambrano).
Acknowledgements
This article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru.
Conflicts of Interest
AJR-M is a member of the Committee on Mpox of the Colombian Association of Scientific Societies (Asociación Colombiana de Sociedades Científicas [ACSC]). AJR-M is also Chair of the Latin American Network of Research on Mpox (LAMOVI), and Member of the Expert Panel of the European Society for Clinical Microbiology and Infectious Diseases (ESCMID) for Developing the Rapid Guideline on Mpox.
Generative AI Statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Abbreviations
| MPXV | Monkeypox Virus |
| Mpox | Monkeypox |
| CDC | Centers for Disease Control and Prevention |
| WHO | World Health Organization |
| PCR | Polymerase Chain Reaction |
| DNA | Deoxyribonucleic Acid |
| RNA | Ribonucleic Acid |
| TPOXX | Tecovirimat |
| HIV | Human Immunodeficiency Virus |
| STIs | Sexually Transmitted Infections |
| FDA | Food and Drug Administration |
References
- Abdel-Rahman, S.M.; Bayici, B.Z.; Keske, Ş.; Kuşkucu, M.; Özsürekçi, Y.; Rimoin, A.W.; Rodriguez-Morales, A.J.; Ergönül, Ö. Mpox primer for clinicians: what makes the difference in 2024? Curr Opin Infect Dis 2025, 38, 143–149. [Google Scholar] [CrossRef] [PubMed]
- García-Iglesias, J.; Cabezas-Pino, A.; Membrillo de Novales, F.J.; Bautista Pérez, A.R.; Garrido Fuentes, J.; Villaamil Pérez, F.; Rodríguez-Morales, A.J.; Zamora Estay, D.; Guajardo Zuñiga, E.; Núñez Saavedra, L.J.; et al. Renaming mpox in Spanish, French, and Portuguese: using language to address stigma and racism. Lancet 2024, 404, 1301–1302. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Sridhar, S.B.; Shareef, J.; Talath, S.; Mohapatra, P.; Khatib, M.N.; Ballal, S.; Kaur, M.; Nathiya, D.; Sharma, S.; et al. The resurgence of monkeypox: Epidemiology, clinical features, and public health implications in the post-smallpox eradication era. New Microbes New Infect 2024, 62, 101487. [Google Scholar] [CrossRef] [PubMed]
- Lum, F.-M.; Torres-Ruesta, A.; Tay, M.Z.; Lin, R.T.; Lye, D.C.; Rénia, L.; Ng, L.F. Monkeypox: disease epidemiology, host immunity and clinical interventions. Nature Reviews Immunology 2022, 22, 597–613. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Chatterjee, P.; Nasipuri, M.; Basu, S.; Chakraborti, T. Computational drug repurposing for viral infectious diseases: a case study on monkeypox. Briefings in Functional Genomics 2024, 23, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Mohanty, A.; Abdelaal, A.; Reda, A.; Rodriguez-Morales, A.J.; Henao-Martinez, A.F. First Monkeypox deaths outside Africa: no room for complacency. Ther Adv Infect Dis 2022, 9, 20499361221124027. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Srivastava, S.; Mehta, R.; Kumar, S.; Sah, S.; Mohanty, A.; Feehan, J.; Al-Tawfiq, J.A.; Apostolopoulos, V. Global Mpox outbreak: Are we prepared for emerging strains? New Microbes New Infect 2024, 62, 101466. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA’s role in mpox preparedness and response, and information about mpox (formerly referred to as monkeypox). Availabe online: https://www.fda.gov/emergency-preparedness-and-response/mcm-issues/mpox (accessed on 12-01-2025).
- Wahid, M.; Mandal, R.K.; Sikander, M.; Khan, M.R.; Haque, S.; Nagda, N.; Ahmad, F.; Rodriguez-Morales, A.J. Safety and Efficacy of Repurposed Smallpox Vaccines Against Mpox: A Critical Review of ACAM2000, JYNNEOS, and LC16. J Epidemiol Glob Health 2025, 15, 88. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, A.; Reda, A.; Lashin, B.I.; Katamesh, B.E.; Brakat, A.M.; Al-Manaseer, B.M.; Kaur, S.; Asija, A.; Patel, N.K.; Basnyat, S., et al. Preventing the Next Pandemic: Is Live Vaccine Efficacious against Monkeypox, or Is There a Need for Killed Virus and mRNA Vaccines? Vaccines (Basel) 2022, 10. [CrossRef]
- Branda, F.; Romano, C.; Ciccozzi, M.; Giovanetti, M.; Scarpa, F.; Ciccozzi, A.; Maruotti, A. Mpox: An Overview of Pathogenesis, Diagnosis, and Public Health Implications. Journal of Clinical Medicine 2024, 13. [CrossRef]
- Plakkot, G.; Koka, S.; Koka, R.S.; Matus, C. Impact of the 2022 Mpox Outbreak on Future Public Health Initiatives in Ohio. Ohio Journal of Public Health 2023. [CrossRef]
- Farahat, R.A.; Sah, R.; El-Sakka, A.A.; Benmelouka, A.Y.; Kundu, M.; Labieb, F.; Shaheen, R.S.; Abdelaal, A.; Abdelazeem, B.; Bonilla-Aldana, D.K.; et al. Human monkeypox disease (MPX). Infez Med 2022, 30, 372–391. [Google Scholar] [CrossRef] [PubMed]
- Antinori, S.; Casalini, G.; Giacomelli, A.; Rodriguez-Morales, A.J. Update on Mpox: a brief narrative review. Infez Med 2023, 31, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Monkeypox (clade IIB). Monkeypox | SUNY Schenectady. Accessed March 29. Availabe online: https://sunysccc.edu/Current-Students/Monkeypox.html.
- About Mpox. Centers for Disease Control and Prevention. July 22, A.F., 2023. Availabe online: https://www.cdc.gov/poxvirus/mpox/about/index.html.
- Ortiz-Saavedra, B.; León-Figueroa, D.A.; Montes-Madariaga, E.S.; Ricardo-Martínez, A.; Alva, N.; Cabanillas-Ramirez, C.; Barboza, J.J.; Siddiq, A.; Coaguila Cusicanqui, L.A.; Bonilla-Aldana, D.K., et al. Antiviral Treatment against Monkeypox: A Scoping Review. Trop Med Infect Dis 2022, 7, doi:10.3390/tropicalmed7110369. [CrossRef]
- Patient’s Guide to mpox treatment with Tecovirimat (TPOXX). Centers for Disease Control and Prevention. Updated November 28, A.F., 2023. Availabe online: https://www.cdc.gov/poxvirus/mpox/if-sick/treatment.html#:~:text=There%20are%20no%20treatments%20specifically,used%20to%20treat% 20monkeypox%20effectively.
- De Clercq, E. Clinical potential of the acyclic nucleoside phosphonates cidofovir, adefovir, and tenofovir in treatment of DNA virus and retrovirus infections. Clinical microbiology reviews 2003, 16, 569–596. [Google Scholar] [CrossRef] [PubMed]
- Shamim, M.A.; Satapathy, P.; Padhi, B.K.; Veeramachaneni, S.D.; Akhtar, N.; Pradhan, A.; Agrawal, A.; Dwivedi, P.; Mohanty, A.; Pradhan, K.B.; et al. Pharmacological treatment and vaccines in monkeypox virus: a narrative review and bibliometric analysis. Front Pharmacol 2023, 14, 1149909. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Mu, L.; Wang, W. Monkeypox: epidemiology, pathogenesis, treatment and prevention. Signal Transduction and Targeted Therapy 2022, 7, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ophinni, Y.; Frediansyah, A.; Sirinam, S.; Megawati, D.; Stoian, A.M.; Enitan, S.S.; Akele, R.Y.; Sah, R.; Pongpirul, K.; Abdeen, Z.; et al. Monkeypox: Immune response, vaccination and preventive efforts. Narra J 2022, 2, e90. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, E.A.; Sassine, J. Antivirals with activity against mpox: a clinically oriented review. Clinical infectious diseases 2023, 76, 155–164. [Google Scholar] [CrossRef] [PubMed]
- tecovirimat., F.a.D.A.H.o.p.i.-. Availabe online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214518s000lbl.pdf.
- monkeypox., C.f.D.C.a.P.a.I.c.g.f.t.t.o. Availabe online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/treatment.html.
- Pauli, G.; Blümel, J.; Burger, R.; Drosten, C.; Gröner, A.; Gürtler, L.; Heiden, M.; Hildebrandt, M.; Jansen, B.; Montag-Lessing, T. Orthopox viruses: infections in humans. Transfusion Medicine and Hemotherapy 2010, 37, 351. [Google Scholar] [CrossRef] [PubMed]
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and treatment of monkeypox. Drugs 2022, 82, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Hudu, S.A.; Alshrari, A.S.; Al Qtaitat, A.; Imran, M. VP37 protein inhibitors for Mpox treatment: highlights on recent advances, patent literature, and future directions. Biomedicines 2023, 11, 1106. [Google Scholar] [CrossRef] [PubMed]
- Duraffour, S.; Snoeck, R.; De Vos, R.; Van Den Oord, J.J.; Crance, J.-M.; Garin, D.; Hruby, D.E.; Jordan, R.; De Clercq, E.; Andrei, G. Activity of the anti-orthopoxvirus compound ST-246 against vaccinia, cowpox and camelpox viruses in cell monolayers and organotypic raft cultures. Antiviral therapy 2007, 12, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Shabil, M.; Khatib, M.N.; Ballal, S.; Bansal, P.; Tomar, B.S.; Ashraf, A.; Kumar, M.R.; Sinha, A.; Rawat, P.; Gaidhane, A.M.; et al. Effectiveness of Tecovirimat in Mpox Cases: A Systematic Review of Current Evidence. J Med Virol 2024, 96, e70122. [Google Scholar] [CrossRef] [PubMed]
- Pourkarim, F.; Entezari-Maleki, T. Clinical considerations on monkeypox antiviral medications: An overview. Pharmacology Research & Perspectives 2024, 12, e01164. [Google Scholar] [CrossRef]
- Congo, N.I.o.H.T.a.t.i.s.b.d.n.i.c.I.m.r.i.D.R.o.t. Availabe online: https://www.niaid.nih.gov/news-events/antiviral-tecovirimat-safe-did-not-improve-clade-i-mpox-resolution-democratic-republic.
- Witwit, H.; Cubitt, B.; Khafaji, R.; Castro, E.M.; Goicoechea, M.; Lorenzo, M.M.; Blasco, R.; Martinez-Sobrido, L.; de la Torre, J.C. Repurposing Drugs for Synergistic Combination Therapies to Counteract Monkeypox Virus Tecovirimat Resistance. Viruses 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Cao, B.; Bei, Z.C.; Xu, L.; Zhang, D.; Zhao, L.; Song, Y.; Wang, H. Disulfide-incorporated lipid prodrugs of cidofovir: Synthesis, antiviral activity, and release mechanism. Eur J Med Chem 2023, 258, 115601. [Google Scholar] [CrossRef] [PubMed]
- Amaral, B.P.; Cargnelutti, J.F.; Mortari, A.P.G.; Merchioratto, I.; Feio, L.M.; Nogueira, C.W.; Weiblen, R.; Flores, E. Diphenyl diselenide and cidofovir present anti-viral activity against Bovine Alphaherpesvirus 2 in vitro and in a sheep model. Res Vet Sci 2021, 134, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Toro, J.R.; Wood, L.V.; Patel, N.K.; Turner, M.L. Topical cidofovir: a novel treatment for recalcitrant molluscum contagiosum in children infected with human immunodeficiency virus 1. Archives of Dermatology 2000, 136, 983–985. [Google Scholar] [CrossRef] [PubMed]
- Lea, A.P.; Bryson, H.M. Cidofovir. Drugs 1996, 52, 225–230, discussion 231. [Google Scholar] [CrossRef] [PubMed]
- Wolf, D.L.; Rodríguez, C.A.; Mucci, M.; Ingrosso, A.; Duncan, B.A.; Nickens, D.J. Pharmacokinetics and renal effects of cidofovir with a reduced dose of probenecid in HIV-infected patients with cytomegalovirus retinitis. The Journal of Clinical Pharmacology 2003, 43, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Cundy, K.C. Clinical pharmacokinetics of the antiviral nucleotide analogues cidofovir and adefovir. Clinical pharmacokinetics 1999, 36, 127–143. [Google Scholar] [CrossRef] [PubMed]
- Tseng, A.L.; Mortimer, C.B.; Salit, I.E. Iritis associated with intravenous cidofovir. Ann Pharmacother 1999, 33, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Pourkarim, F.; Entezari-Maleki, T. Clinical considerations on monkeypox antiviral medications: An overview. Pharmacol Res Perspect 2024, 12, e01164. [Google Scholar] [CrossRef] [PubMed]
- Andrei, G.; Snoeck, R. Cidofovir activity against poxvirus infections. Viruses 2010, 2, 2803. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, N.; Shimizu, T.; Hirano, D.; Ishikane, M.; Kataoka, Y. Lack of clinical evidence of antiviral therapy for human monkeypox: A scoping review. Journal of Infection and Chemotherapy 2023, 29, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Hutson, C.L.; Kondas, A.V.; Mauldin, M.R.; Doty, J.B.; Grossi, I.M.; Morgan, C.N.; Ostergaard, S.D.; Hughes, C.M.; Nakazawa, Y.; Kling, C. Pharmacokinetics and efficacy of a potential smallpox therapeutic, brincidofovir, in a lethal monkeypox virus animal model. MSphere 2021, 6, e00927-20. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.W. Therapeutic strategies to address monkeypox. Expert Review of Anti-infective Therapy 2022, 20, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- FDA, U.S. FDA approves drug to treat smallpox. Availabe online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-smallpox (accessed on 19).
- Marty, F.M.; Winston, D.J.; Chemaly, R.F.; Mullane, K.M.; Shore, T.B.; Papanicolaou, G.A.; Chittick, G.; Brundage, T.M.; Wilson, C.; Morrison, M.E.; et al. A Randomized, Double-Blind, Placebo-Controlled Phase 3 Trial of Oral Brincidofovir for Cytomegalovirus Prophylaxis in Allogeneic Hematopoietic Cell Transplantation. Biol Blood Marrow Transplant 2019, 25, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J. Clinical features and management of human monkeypox: a retrospective observational study in the UK. The Lancet Infectious Diseases 2022, 22, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Shamim, M.A.; Padhi, B.K.; Satapathy, P.; Veeramachaneni, S.D.; Chatterjee, C.; Tripathy, S.; Akhtar, N.; Pradhan, A.; Dwivedi, P.; Mohanty, A.; et al. The use of antivirals in the treatment of human monkeypox outbreaks: a systematic review. Int J Infect Dis 2023, 127, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Quenelle, D.C.; Lampert, B.; Collins, D.J.; Rice, T.L.; Painter, G.R.; Kern, E.R. Efficacy of CMX001 against herpes simplex virus infections in mice and correlations with drug distribution studies. The Journal of infectious diseases 2010, 202, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Prévost, J.; Sloan, A.; Deschambault, Y.; Tailor, N.; Tierney, K.; Azaransky, K.; Kammanadiminti, S.; Barker, D.; Kodihalli, S.; Safronetz, D. Treatment efficacy of cidofovir and brincidofovir against clade II Monkeypox virus isolates. Antiviral Research 2024, 231, 105995. [Google Scholar] [CrossRef] [PubMed]
- Shishkina, L.N.; Mazurkov, O.Y.; Bormotov, N.I.; Skarnovich, M.O.; Serova, O.A.; Mazurkova, N.A.; Skarnovich, M.A.; Chernonosov, A.A.; Selivanov, B.A.; Tikhonov, A.Y., et al. Safety and Pharmacokinetics of the Substance of the Anti-Smallpox Drug NIOCH-14 after Oral Administration to Laboratory Animals. Viruses 2023, 15. [CrossRef]
- Mazurkov, O.Y.; Kabanov, A.S.; Shishkina, L.N.; Sergeev, A.A.; Skarnovich, M.O.; Bormotov, N.I.; Skarnovich, M.A.; Ovchinnikova, A.S.; Titova, K.A.; Galahova, D.O. New effective chemically synthesized anti-smallpox compound NIOCH-14. Journal of General Virology 2016, 97, 1229–1239. [Google Scholar] [CrossRef] [PubMed]
- Kabanov, A.S.; Sergeev, A.A.; Shishkina, L.N.; Bulychev, L.E.; Skarnovich, M.O.; Sergeev, A.A.; Bormotov, N.I.; P’Iankov O, V.; Serova, O.A.; Bodnev, S.A.; et al. [A comparative study of the antiviral activity of chemical compounds concerning the orthopoxviruses experiments in vivo]. Vopr Virusol 2013, 58, 39–43. [Google Scholar] [PubMed]
- Шишкина, Л.; Бoгрянцева, М.; Бoрмoтoв, Н.; Усoва, С.; Скарнoвич, М.; Мазуркoв, О.; Башкина, Е.; Куцерубoва, Н.; Удальева, С.; Сергеев, А. Безoпаснoсть нoвoгo рoссийскoгo прoтивooспеннoгo препарата НИОХ-14: oткрытoе рандoмизирoваннoе клиническoе исследoвание I фазы. Безoпаснoсть и риск фармакoтерапии 2025.
- Weinstein, R.A.; Nalca, A.; Rimoin, A.W.; Bavari, S.; Whitehouse, C.A. Reemergence of monkeypox: prevalence, diagnostics, and countermeasures. Clinical infectious diseases 2005, 41, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Wittek, R. Vaccinia immune globulin: current policies, preparedness, and product safety and efficacy. International journal of infectious diseases 2006, 10, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, A.; Arunagiri, T.; Mani, S.; Kumaran, V.R.; Kannaiah, K.P.; Chanduluru, H.K. From pox to protection: understanding Monkeypox pathophysiology and immune resilience. Tropical Medicine and Health 2025, 53, 33. [Google Scholar] [CrossRef] [PubMed]
- Gilchuk, I.; Gilchuk, P.; Sapparapu, G.; Lampley, R.; Singh, V.; Kose, N.; Blum, D.L.; Hughes, L.J.; Satheshkumar, P.S.; Townsend, M.B. Cross-neutralizing and protective human antibody specificities to poxvirus infections. Cell 2016, 167, 684–694.e689. [Google Scholar] [CrossRef] [PubMed]
- Gilchuk, I.; Gilchuk, P.; Sapparapu, G.; Lampley, R.; Singh, V.; Kose, N.; Blum, D.L.; Hughes, L.J.; Satheshkumar, P.S.; Townsend, M.B.; et al. Cross-Neutralizing and Protective Human Antibody Specificities to Poxvirus Infections. Cell 2016, 167, 684–694.e689. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Wu, L.; Sun, J.; Liu, D.; Han, P.; Gao, Y.; Zhang, Y.; Xu, Y.; Qu, X.; Wang, H.; et al. Two noncompeting human neutralizing antibodies targeting MPXV B6 show protective effects against orthopoxvirus infections. Nat Commun 2024, 15, 4660. [Google Scholar] [CrossRef] [PubMed]
- Noy-Porat, T.; Tamir, H.; Alcalay, R.; Rosenfeld, R.; Epstein, E.; Cherry, L.; Achdout, H.; Erez, N.; Politi, B.; Yahalom-Ronen, Y.; et al. Generation of recombinant mAbs to vaccinia virus displaying high affinity and potent neutralization. Microbiol Spectr 2023, 11, e0159823. [Google Scholar] [CrossRef] [PubMed]
- Martinez, A.E.; Frattaroli, P.; Vu, C.A.; Paniagua, L.; Mintz, J.; Bravo-Gonzalez, A.; Zamudio, P.; Barco, A.; Rampersad, A.; Lichtenberger, P., et al. Successful Outcome after Treatment with Cidofovir, Vaccinia, and Extended Course of Tecovirimat in a Newly-Diagnosed HIV Patient with Severe Mpox: A Case Report. Vaccines (Basel) 2023, 11. [CrossRef]
- Zone., O.V. Availabe online: https://viralzone.expasy.org/149?outline=all_by_species (accessed on 07/04/2025).
- Lansiaux, E.; Jain, N.; Laivacuma, S.; Reinis, A. The virology of human monkeypox virus (hMPXV): A brief overview. Virus research 2022, 322, 198932. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Ophinni, Y.; Megawati, D.; Frediansyah, A.; Mamada, S.S.; Salampe, M.; Bin Emran, T.; Winardi, W.; Fathima, R.; Sirinam, S. Monkeypox: a comprehensive review. Viruses 2022, 14, 2155. [Google Scholar] [CrossRef] [PubMed]
- Gong, Q.; Wang, C.; Chuai, X.; Chiu, S. Monkeypox virus: a re-emergent threat to humans. Virologica Sinica 2022, 37, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Moss, B. Membrane fusion during poxvirus entry. In Proceedings of Seminars in cell & developmental biology; pp. 89-96.
- Challberg, M.D.; Englund, P.T. Purification and properties of the deoxyribonucleic acid polymerase induced by vaccinia virus. Journal of Biological Chemistry 1979, 254, 7812–7819. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Leng, P.; Zhou, H. Global transmission of monkeypox virus—a potential threat under the COVID-19 pandemic. Frontiers in Immunology 2023, 14, 1174223. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Kumar, S.; Jain, S.; Mohanty, A.; Thapa, N.; Poudel, P.; Bhusal, K.; Al-Qaim, Z.H.; Barboza, J.J.; Padhi, B.K. The Global Monkeypox (Mpox) outbreak: a comprehensive review. Vaccines 2023, 11, 1093. [Google Scholar] [CrossRef] [PubMed]
- Haller, S.L.; Peng, C.; McFadden, G.; Rothenburg, S. Poxviruses and the evolution of host range and virulence. Infection, Genetics and Evolution 2014, 21, 15–40. [Google Scholar] [CrossRef] [PubMed]
- Dsouza, L.; Pant, A.; Offei, S.; Priyamvada, L.; Pope, B.; Satheshkumar, P.S.; Wang, Z.; Yang, Z. Antiviral activities of two nucleos (t) ide analogs against vaccinia and mpox viruses in primary human fibroblasts. bioRxiv 2023. [CrossRef]
- Thakur, M.; Das, P.; Sobti, R.C.; Kaur, T. Human monkeypox: epidemiology, transmission, pathogenesis, immunology, diagnosis and therapeutics. Molecular and Cellular Biochemistry 2023, 478, 2097–2110. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. WHO advisory committee on variola virus research: report of the twenty-third meeting, virtual meeting, 3-4 November 2021; World Health Organization: 2022.
- Dutt, M.; Kumar, A.; Rout, M.; Dehury, B.; Martinez, G.; Ndishimye, P.; Kelvin, A.A.; Kelvin, D.J. Drug repurposing for Mpox: Discovery of small molecules as potential inhibitors against DNA-dependent RNA polymerase using molecular modeling approach. Journal of Cellular Biochemistry 2023, 124, 701–715. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, A.; Strand, S.; Mucker, E.; Huggins, J.W.; Jahrling, P.B.; Ibrahim, S.M. Inhibition of monkeypox virus replication by RNA interference. Virol J 2009, 6, 188. [Google Scholar] [CrossRef] [PubMed]
- Hishiki, T.; Morita, T.; Akazawa, D.; Ohashi, H.; Park, E.S.; Kataoka, M.; Mifune, J.; Shionoya, K.; Tsuchimoto, K.; Ojima, S.; et al. Identification of IMP Dehydrogenase as a Potential Target for Anti-Mpox Virus Agents. Microbiol Spectr 2023, 11, e0056623. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, A.; Strand, S.; Mucker, E.; Huggins, J.W.; Jahrling, P.B.; Ibrahim, S.M. Inhibition of Monkeypox virus replication by RNA interference. Virology journal 2009, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Pevear, D.C.; Davies, M.H.; Collett, M.S.; Bailey, T.; Rippen, S.; Barone, L.; Burns, C.; Rhodes, G.; Tohan, S. An orally bioavailable antipoxvirus compound (ST-246) inhibits extracellular virus formation and protects mice from lethal orthopoxvirus challenge. Journal of virology 2005, 79, 13139–13149. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.K.; Olson, V.A.; Karem, K.L.; Jordan, R.; Hruby, D.E.; Damon, I.K. In vitro efficacy of ST246 against smallpox and monkeypox. Antimicrobial agents and chemotherapy 2009, 53, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Chiem, K.; Nogales, A.; Lorenzo, M.; Morales Vasquez, D.; Xiang, Y.; Gupta, Y.K.; Blasco, R.; de la Torre, J.C.; Martínez-Sobrido, L. Identification of In Vitro Inhibitors of Monkeypox Replication. Microbiology Spectrum 2023, 11, e0474522. [Google Scholar] [CrossRef] [PubMed]
- Horton, A.; Berryman, H.; Surani, Y.M.; Bewley, K.; Wand, M.E.; Sutton, J.M.; Tree, J.A. The antiviral activity of licensed therapeutics against Mpox clade Ib, in vitro; alternative options for the treatment of Mpox. bioRxiv 2025, 2025.2001. 2011.632516.
- Tiwari, H.; Sharma, S.; Dixit, A.; Kumar, R.; Fatima, K.; Hazarika, Z.; Ilyas, A.; Upadhyay, S.; Borkotoky, S. Unlocking the Secret Vault of Promising Drug Targets from Mpox Proteome-A Computational Approach. 2024.
- Akazawa, D.; Ohashi, H.; Hishiki, T.; Morita, T.; Iwanami, S.; Kim, K.S.; Jeong, Y.D.; Park, E.S.; Kataoka, M.; Shionoya, K.; et al. Potential Anti-Mpox Virus Activity of Atovaquone, Mefloquine, and Molnupiravir, and Their Potential Use as Treatments. J Infect Dis 2023, 228, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Suraweera, C.D.; Hinds, M.G.; Kvansakul, M. Poxviral strategies to overcome host cell apoptosis. Pathogens 2020, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- Boys, I.N.; Johnson, A.G.; Quinlan, M.R.; Kranzusch, P.J.; Elde, N.C. Structural homology screens reveal host-derived poxvirus protein families impacting inflammasome activity. Cell reports 2023, 42. [CrossRef]
- Martínez-Fernández, D.E.; Fernández-Quezada, D.; Casillas-Muñoz, F.A.G.; Carrillo-Ballesteros, F.J.; Ortega-Prieto, A.M.; Jimenez-Guardeño, J.M.; Regla-Nava, J.A. Human Monkeypox: a comprehensive overview of epidemiology, pathogenesis, diagnosis, treatment, and prevention strategies. Pathogens 2023, 12, 947. [Google Scholar] [CrossRef] [PubMed]
- Albarnaz, J.D.; Kite, J.; Oliveira, M.; Li, H.; Di, Y.; Christensen, M.H.; Paulo, J.A.; Antrobus, R.; Gygi, S.P.; Schmidt, F.I. Quantitative proteomics defines mechanisms of antiviral defence and cell death during modified vaccinia Ankara infection. Nature Communications 2023, 14, 8134. [Google Scholar] [CrossRef] [PubMed]
- An, T.-Q.; Li, J.-N.; Su, C.-M.; Yoo, D. Molecular and cellular mechanisms for PRRSV pathogenesis and host response to infection. Virus research 2020, 286, 197980. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Liu, Y.; Dou, D.; Su, B. The unique immune evasion mechanisms of the mpox virus and their implication for developing new vaccines and immunotherapies. Virologica Sinica 2024. [CrossRef]
- Zandi, M.; Shafaati, M.; Hosseini, F. Mechanisms of immune evasion of monkeypox virus. Frontiers in microbiology 2023, 14, 1106247. [Google Scholar] [CrossRef] [PubMed]
- Hammarlund, E.; Dasgupta, A.; Pinilla, C.; Norori, P.; Früh, K.; Slifka, M.K. Monkeypox virus evades antiviral CD4+ and CD8+ T cell responses by suppressing cognate T cell activation. Proceedings of the National Academy of Sciences 2008, 105, 14567–14572. [Google Scholar] [CrossRef] [PubMed]
- Otieno, J.R.; Ruis, C.; Onoja, A.B.; Kuppalli, K.; Hoxha, A.; Nitsche, A.; Brinkmann, A.; Michel, J.; Mbala-Kingebeni, P.; Mukadi-Bamuleka, D. Global genomic surveillance of monkeypox virus. Nature Medicine 2024, 1-1. [CrossRef]
- Alakunle, E.; Kolawole, D.; Diaz-Canova, D.; Alele, F.; Adegboye, O.; Moens, U.; Okeke, M.I. A comprehensive review of monkeypox virus and mpox characteristics. Frontiers in Cellular and Infection Microbiology 2024, 14, 1360586. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Xing, H.; Wang, C.; Tang, M.; Wu, C.; Ye, F.; Yin, L.; Yang, Y.; Tan, W.; Shen, L. Mpox (formerly monkeypox): pathogenesis, prevention, and treatment. Signal Transduction and Targeted Therapy 2023, 8, 458. [Google Scholar] [CrossRef] [PubMed]
- Caetano-Pinto, P.; Nordell, P.; Nieskens, T.; Haughan, K.; Fenner, K.S.; Stahl, S.H. Amplifying the impact of kidney microphysiological systems: predicting renal clearance using mechanistic modelling based on reconstructed drug secretion. ALTEX-Alternatives to animal experimentation 2023, 40, 408–424. [Google Scholar] [CrossRef] [PubMed]
- Velioglu, A.; Erdogan, E.; Tigen, E.; Ozgen, Z.; Tuglular, S. Topical cidofovir-related acute kidney injury in a kidney transplant recipient. Clinical Transplantation 2022, 36, e14824. [Google Scholar] [CrossRef] [PubMed]
- Sankar, S.; Balakrishnan, P.; Yong, Y.K.; Raju, S.; Velu, V.; Shankar, E.M.; Larsson, M. Mpox Virus as a Global Public Health Emergency: A Scoping Review. Can J Infect Dis Med Microbiol 2025, 2025, 6683501. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Xu, A.; Guan, L.; Tang, Y.; Chai, G.; Feng, J.; Wu, Y.; Li, M.; Zhang, C.; Liu, X. A review of Mpox: Biological characteristics, epidemiology, clinical features, diagnosis, treatment, and prevention strategies. In Proceedings of Exploration; p. 20230112.
- ICMRA. Summary report of the International Coalition of Medicines Regulatory Authorities (ICMRA) workshop on mpox, October 2, 2024. Availabe online: https://www.icmra.info/drupal/news/mpox_news_announcement_25oct2024/mpox_ws_report_2oct2024.
- WHO. Clinical management of mpox (monkeypox). 2024.
- Islam, M.A.; Hemo, M.K.; Chopra, H.; Amin, M.R.; Bhattacharya, P.; Dhama, K. Old enemy with a New Face: Re-emerging Monkeypox Disease--An Update. Journal of Pure & Applied Microbiology 2022, 16. [CrossRef]
- Group, P.W. Tecovirimat for clade I MPXV infection in the Democratic Republic of Congo. New England Journal of Medicine 2025, 392, 1484–1496. [Google Scholar] [CrossRef] [PubMed]
- CTV. Study to Assess the Safety and Immunogenicity of TPOXX® When Administered Orally for 28 Days With JYNNEOS. Availabe online: https://ctv.veeva.com/study/study-to-assess-the-safety-and-pharmacokinetics-of-tpoxx-r-when-administered-orally-for-28-days.
- Witwit, H.; Cubitt, B.; Khafaji, R.; Castro, E.M.; Goicoechea, M.; Lorenzo, M.M.; Blasco, R.; Martinez-Sobrido, L.; de la Torre, J.C. Repurposing Drugs for Synergistic Combination Therapies to Counteract Monkeypox Virus Tecovirimat Resistance. Viruses 2025, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Elrewany, E.; Gebreal, A.; ElMakhzangy, R.; Fadl, N.; Elbanna, E.H.; Tolba, M.M.; Hammad, E.M.; Youssef, N.; Abosheaishaa, H. Systematic review on the efficacy, effectiveness, safety, and immunogenicity of monkeypox vaccine. Vaccines 2023, 11, 1708. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Guruparan, D.; Karuppanan, K.; Kumar, K.S. Comprehensive Insights into Monkeypox (mpox): Recent Advances in Epidemiology, Diagnostic Approaches and Therapeutic Strategies. Pathogens 2024, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I. Community transmission of monkeypox in the United Kingdom, April to May 2022. Eurosurveillance 2022, 27, 2200422. [Google Scholar] [CrossRef] [PubMed]
- Tambo, E.; Al-Nazawi, A.M. Combating the global spread of poverty-related Monkeypox outbreaks and beyond. Infectious Diseases of Poverty 2022, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, M.; Wu, P.; Wu, S.; Lee, T.-Y.; Bai, C. Application of computational biology and artificial intelligence in drug design. International journal of molecular sciences 2022, 23, 13568. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.; Singla, R.K. Bioinformatics Tools for Pharmaceutical Drug Product Development. Indo Global Journal of Pharmaceutical Sciences 2022, 12, 281–294. [Google Scholar] [CrossRef]
- Parvathaneni, V.; Kulkarni, N.S.; Muth, A.; Gupta, V. Drug repurposing: a promising tool to accelerate the drug discovery process. Drug discovery today 2019, 24, 2076–2085. [Google Scholar] [CrossRef] [PubMed]
- Odhar, H.A. Computational Repurposing of FDA Approved Drugs Against Monkeypox Virus Cysteine Proteinase: A Molecular Docking and Dynamics Simulation Study. 2022.
- Rai, M.; Singh, A.V.; Paudel, N.; Kanase, A.; Falletta, E.; Kerkar, P.; Heyda, J.; Barghash, R.F.; Singh, S.P.; Soos, M. Herbal concoction unveiled: a computational analysis of phytochemicals’ pharmacokinetic and toxicological profiles using novel approach methodologies (NAMs). Current Research in Toxicology 2023, 5, 100118. [Google Scholar] [CrossRef] [PubMed]
- Karplus, M.; McCammon, J.A. Molecular dynamics simulations of biomolecules. Nature structural biology 2002, 9, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Shoichet, B.K.; McGovern, S.L.; Wei, B.; Irwin, J.J. Lead discovery using molecular docking. Current opinion in chemical biology 2002, 6, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Flores-Holguín, N.; Frau, J.; Glossman-Mitnik, D. Computational Study of the Chemical Reactivity and Bioactivity Rates of Marine Peptides Hemiasterlin and Its A and B Derivatives Used in the Cancer Treatment through Conceptual Density Functional Theory. Computational Molecular Bioscience 2019, 9, 95–107. [Google Scholar] [CrossRef]
- Kharwar, R.; Bhatt, M.; Patel, K.; Patel, S.; Daxini, N. A computational approach to identify natural putative inhibitors to combat monkeypox. In Nanotechnology and In Silico Tools, Elsevier: 2024; pp. 285-308.
- Aiman, S.; Alhamhoom, Y.; Ali, F.; Rahman, N.; Rastrelli, L.; Khan, A.; Farooq, Q.u.A.; Ahmed, A.; Khan, A.; Li, C. Multi-epitope chimeric vaccine design against emerging Monkeypox virus via reverse vaccinology techniques-a bioinformatics and immunoinformatics approach. Frontiers in immunology 2022, 13, 985450. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L. Multi-epitope vaccines: a promising strategy against tumors and viral infections. Cellular & molecular immunology 2018, 15, 182–184. [Google Scholar] [CrossRef]
- Kleftogiannis, D.; Kalnis, P.; Bajic, V.B. Progress and challenges in bioinformatics approaches for enhancer identification. Briefings in Bioinformatics 2015, 17, 967–979. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Pritam, M.; Banerjee, M.; Singh, A.K.; Singh, S.P. Genome based screening of epitope ensemble vaccine candidates against dreadful visceral leishmaniasis using immunoinformatics approach. Microbial pathogenesis 2019, 136, 103704. [Google Scholar] [CrossRef] [PubMed]
- Nnaemeka, E.J.; Oladokun, P.; Abubakar, I.; Afolabi, S. Leveraging AI and Deep Learning in Predictive Genomics for MPOX Virus Research using MATLAB.
- Sahu, A.; Gaur, M.; Mahanandia, N.C.; Subudhi, E.; Swain, R.P.; Subudhi, B.B. Identification of core therapeutic targets for Monkeypox virus and repurposing potential of drugs against them: An in silico approach. Computers in Biology and Medicine 2023, 161, 106971. [Google Scholar] [CrossRef] [PubMed]
- Arasu, M.V.; Vijayaragavan, P.; Purushothaman, S.; Rathi, M.; Al-Dhabi, N.A.; Gopalakrishnan, V.; Choi, K.C.; Ilavenil, S. Molecular docking of monkeypox (mpox) virus proteinase with FDA approved lead molecules. Journal of Infection and Public Health 2023, 16, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Alandijany, T.A.; El-Daly, M.M.; Tolah, A.M.; Bajrai, L.H.; Khateb, A.M.; Kumar, G.S.; Dubey, A.; Dwivedi, V.D.; Azhar, E.I. A multi-targeted computational drug discovery approach for repurposing tetracyclines against monkeypox virus. Scientific Reports 2023, 13, 14570. [Google Scholar] [CrossRef] [PubMed]
- Ashley, C.N.; Broni, E.; Wood, C.M.; Okuneye, T.; Ojukwu, M.-P.T.; Dong, Q.; Gallagher, C.; Miller III, W.A. Identifying potential monkeypox virus inhibitors: an in silico study targeting the A42R protein. Frontiers in Cellular and Infection Microbiology 2024, 14, 1351737. [Google Scholar] [CrossRef] [PubMed]
- CDC. Mpox in the United States and Around the World: Current Situation. Availabe online: https://www.cdc.gov/mpox/situation-summary/index.html (accessed on 20-03-2025).
- FDA, U. Key Facts About Vaccines to Prevent Mpox Disease. Availabe online: https://www.fda.gov/vaccines-blood-biologics/vaccines/key-facts-about-vaccines-prevent-mpox-disease (accessed on 20-03-2025).
- WHO. Overview of Mpox (monkeypox) vaccines and safety surveillance. Availabe online: https://www.who.int/news-room/questions-and-answers/item/mpox-vaccines.
- WHO. Mpox: Vaccines. Availabe online: https://www.who.int/news-room/questions-and-answers/item/mpox-vaccines (accessed on 2025).
- Garcia-Atutxa, I.; Mondragon-Teran, P.; Huerta-Saquero, A.; Villanueva-Flores, F. Advancements in monkeypox vaccines development: a critical review of emerging technologies. Front Immunol 2024, 15, 1456060. [Google Scholar] [CrossRef] [PubMed]
- Berhanu, A.; King, D.S.; Mosier, S.; Jordan, R.; Jones, K.F.; Hruby, D.E.; Grosenbach, D.W. Impact of ST-246® on ACAM2000™ smallpox vaccine reactogenicity, immunogenicity, and protective efficacy in immunodeficient mice. Vaccine 2010, 29, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.; Crump, R.; Foster, S.; Hartzler, H.; Hembrador, E.; Lanier, E.R.; Painter, G.; Schriewer, J.; Trost, L.C.; Buller, R.M. Co-administration of the broad-spectrum antiviral, brincidofovir (CMX001), with smallpox vaccine does not compromise vaccine protection in mice challenged with ectromelia virus. Antiviral research 2014, 111, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Atutxa, I.; Mondragon-Teran, P.; Huerta-Saquero, A.; Villanueva-Flores, F. Advancements in monkeypox vaccines development: a critical review of emerging technologies. Frontiers in Immunology 2024, 15, 1456060. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.B.; Mehta, A.; Zahid, M.J.; Candelario, K.; Shrestha, S.; Pokharel, P. Concerns over cardiovascular manifestations associated with monkeypox immunization: a literature review. Annals of Medicine and Surgery 2023, 85, 2797–2801. [Google Scholar] [CrossRef] [PubMed]
- CDC. Tecovirimat (TPOXX) for Treatment of Mpox. 2025.
- ARENA, C.T. Mpox: Three ongoing vaccine trials to watch. September 19, 2024.
- Parker, S.; D’Angelo, J.; Buller, R.M.; Smee, D.F.; Lantto, J.; Nielsen, H.; Jensen, A.; Prichard, M.; George, S.L. A human recombinant analogue to plasma-derived vaccinia immunoglobulin prophylactically and therapeutically protects against lethal orthopoxvirus challenge. Antiviral Research 2021, 195, 105179. [Google Scholar] [CrossRef] [PubMed]
- Keckler, M.S.; Salzer, J.S.; Patel, N.; Townsend, M.B.; Nakazawa, Y.J.; Doty, J.B.; Gallardo-Romero, N.F.; Satheshkumar, P.S.; Carroll, D.S.; Karem, K.L. IMVAMUNE® and ACAM2000® provide different protection against disease when administered postexposure in an intranasal monkeypox challenge prairie dog model. Vaccines 2020, 8, 396. [Google Scholar] [CrossRef] [PubMed]
- Stittelaar, K.J.; van Amerongen, G.; Kondova, I.; Kuiken, T.; van Lavieren, R.F.; Pistoor, F.H.; Niesters, H.G.; van Doornum, G.; van der Zeijst, B.A.; Mateo, L. Modified vaccinia virus Ankara protects macaques against respiratory challenge with monkeypox virus. Journal of virology 2005, 79, 7845–7851. [Google Scholar] [CrossRef] [PubMed]
- Denzler, K.L.; Babas, T.; Rippeon, A.; Huynh, T.; Fukushima, N.; Rhodes, L.; Silvera, P.M.; Jacobs, B.L. Attenuated NYCBH vaccinia virus deleted for the E3L gene confers partial protection against lethal monkeypox virus disease in cynomolgus macaques. Vaccine 2011, 29, 9684–9690. [Google Scholar] [CrossRef] [PubMed]
- Earl, P.L.; Americo, J.L.; Wyatt, L.S.; Eller, L.A.; Whitbeck, J.C.; Cohen, G.H.; Eisenberg, R.J.; Hartmann, C.J.; Jackson, D.L.; Kulesh, D.A. Immunogenicity of a highly attenuated MVA smallpox vaccine and protection against monkeypox. Nature 2004, 428, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Earl, P.L.; Americo, J.L.; Wyatt, L.S.; Eller, L.A.; Montefiori, D.C.; Byrum, R.A.; Piatak, M.; Lifson, J.D.; Amara, R.R.; Robinson, H.L., et al. Recombinant modified vaccinia virus Ankara provides durable protection against disease caused by an immunodeficiency virus as well as long-term immunity to an orthopoxvirus in a non-human primate. Virology 2007, 366 1, 84-97. [CrossRef]
- Earl, P.L.; Americo, J.L.; Wyatt, L.S.; Espenshade, O.; Bassler, J.; Gong, K.; Lin, S.; Peters, E.; Rhodes, L.; Spano, Y.E.; et al. Rapid protection in a monkeypox model by a single injection of a replication-deficient vaccinia virus. Proceedings of the National Academy of Sciences 2008, 105, 10889–10894. [Google Scholar] [CrossRef] [PubMed]
- Grosenbach, D.W.; Jordan, R.; King, D.S.; Berhanu, A.; Warren, T.K.; Kirkwood-Watts, D.L.; Tyavanagimatt, S.R.; Tan, Y.; Wilson, R.L.; Jones, K.F.; et al. Immune responses to the smallpox vaccine given in combination with ST-246, a small-molecule inhibitor of poxvirus dissemination. Vaccine 2007, 26, 933–946. [Google Scholar] [CrossRef] [PubMed]
- Hatch, G.J.; Graham, V.A.; Bewley, K.R.; Tree, J.; Dennis, M.J.; Taylor, I.; Funnell, S.G.P.; Bate, S.R.; Steeds, K.; Tipton, T.; et al. Assessment of the Protective Effect of Imvamune and Acam2000 Vaccines against Aerosolized Monkeypox Virus in Cynomolgus Macaques. Journal of Virology 2013, 87, 7805–7815. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, I.; Ami, Y.; Suzaki, Y.; Nagata, N.; Fukushi, S.; Ogata, M.; Morikawa, S.; Hasegawa, H.; Mizuguchi, M.; Kurane, I., et al. A Single Vaccination of Nonhuman Primates with Highly Attenuated Smallpox Vaccine, LC16m8, Provides Long-term Protection against Monkeypox. Japanese journal of infectious diseases 2017, 70 4, 408-415. [CrossRef]
- Keckler, M.S.; Carroll, D.S.; Gallardo-Romero, N.F.; Lash, R.R.; Salzer, J.S.; Weiss, S.; Patel, N.R.; Clemmons, C.J.; Smith, S.K.; Hutson, C.L.; et al. Establishment of the Black-Tailed Prairie Dog (Cynomys ludovicianus) as a Novel Animal Model for Comparing Smallpox Vaccines Administered Preexposure in both High- and Low-Dose Monkeypox Virus Challenges. Journal of Virology 2011, 85, 7683–7698. [Google Scholar] [CrossRef] [PubMed]
- Keckler, M.S.; Salzer, J.S.; Patel, N.R.; Townsend, M.B.; Nakazawa, Y.J.; Doty, J.B.; Gallardo-Romero, N.F.; Satheshkumar, P.S.; Carroll, D.S.; Karem, K.L.; et al. IMVAMUNE® and ACAM2000® Provide Different Protection against Disease When Administered Postexposure in an Intranasal Monkeypox Challenge Prairie Dog Model. Vaccines 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Phelps, A.L.; Gates, A.J.; Eastaugh, L.S.; Hillier, M.; Ulaeto, D. Comparative Efficacy of Intramuscular and Scarification Routes of Administration of Live Smallpox Vaccine in a Murine Challenge Model. Vaccine 2017, 35, 3889–3896. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.T.; Berhanu, A.; Bigger, C.B.; Prigge, J.T.; Silvera, P.M.; Grosenbach, D.W.; Hruby, D.E. Co-administration of tecovirimat and ACAM2000™ in non-human primates: Effect of tecovirimat treatment on ACAM2000 immunogenicity and efficacy versus lethal monkeypox virus challenge. Vaccine 2019, 38, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Shao, L.; Huang, D.; Wei, H.; Wang, R.C.; Chen, C.Y.; Shen, L.; Zhang, W.; Jin, J.; Chen, Z.W. Expansion, Reexpansion, and Recall-Like Expansion of Vγ2Vδ2 T Cells in Smallpox Vaccination and Monkeypox Virus Infection. Journal of Virology 2009, 83, 11959–11965. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Atutxa, I.; Mondragón-Terán, P.; Huerta-Saquero, A.; Villanueva-Flores, F. Advancements in monkeypox vaccines development: a critical review of emerging technologies. Frontiers in Immunology 2024, 15. [CrossRef]
- Trials.gov, C. Mpox \(Monkeypox\), Phase: Early Phase 1, 1, 2, 3, 4, Interventional, Observational studies Availabe online: https://clinicaltrials.gov/search?cond=Mpox%20%5C(Monkeypox%5C)&aggFilters=phase:0%201%202%203%204,studyType:obs%20int (accessed on 28-01-2025).
- NIH. The antiviral tecovirimat is safe but did not improve clade I mpox resolution in Democratic Republic of the Congo. Availabe online: https://www.nih.gov/news-events/news-releases/antiviral-tecovirimat-safe-did-not-improve-clade-i-mpox-resolution-democratic-republic-congo (accessed on 20-03-2025).
- Li, P.; Al-Tawfiq, J.A.; Memish, Z.A.; Pan, Q. Preventing drug resistance: combination treatment for mpox. The Lancet 2023, 402, 1750–1751. [Google Scholar] [CrossRef] [PubMed]
- Grabenstein, J.D.; Hacker, A. Vaccines against mpox: MVA-BN and LC16m8. Expert Rev Vaccines 2024, 23, 796–811. [Google Scholar] [CrossRef] [PubMed]
- Cambaza, E.M. A Review of the Molecular Understanding of the Mpox Virus (MPXV): Genomics, Immune Evasion, and Therapeutic Targets. Zoonotic Diseases 2025, 5, 3. [Google Scholar] [CrossRef]
- Lu, J.; Xing, H.; Wang, C.; Tang, M.; Wu, C.; Ye, F.; Yin, L.; Yang, Y.; Tan, W.; Shen, L. Mpox (formerly monkeypox): Pathogenesis, prevention and treatment. Signal Transduction and Targeted Therapy 2023, 8, 458. [Google Scholar] [CrossRef] [PubMed]
- Azari, P.P.; Rukerd, M.R.Z.; Charostad, J.; Bashash, D.; Farsiu, N.; Behzadi, S.; Khoshnazar, S.M.; Heydari, S.; Nakhaie, M. Monkeypox (Mpox) vs. Innate immune responses: Insights into evasion mechanisms and potential therapeutic strategies. Cytokine 2024, 183, 156751. [Google Scholar] [CrossRef] [PubMed]
- WHO. MPOX. Availabe online: https://www.who.int/news-room/fact-sheets/detail/mpox (accessed on 25-01-2025).
- Srivastava, S.; Laxmi, *!!! REPLACE !!!*; Sharma, K.; Sridhar, S.B.; Talath, S.; Shareef, J.; Mehta, R.; Satapathy, P.; Sah, R. Clade Ib: a new emerging threat in the Mpox outbreak. Frontiers in Pharmacology 2024, 15, 1504154. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, S.; Halappa, N.R.; Fnu, K.; Reddy, S.M.; Han, G.; Yogesh, R.; Fareed, M.U.; Defne, Ş.; Danyal, B.; Palash, R. Unraveling Monkeypox: An Emerging Threat in Global Health. Cureus 2023, 15. [CrossRef]
- Kumar, D.; Malviya, R.; Srivastava, S.; Sridhar, S.B.; Talath, S.; Shareef, J.; Prajapati, B.G. Personalized Immunization against Mpox Clades I and Ib: strategies to combat the emerging epidemic. Infectious Medicine 2025, 100166. [CrossRef]
- Jeyakumar, T.; Younus, S.; Zhang, M.; Clare, M.; Charow, R.; Karsan, I.; Dhalla, A.; Al-Mouaswas, D.; Scandiffio, J.; Aling, J. Preparing for an artificial intelligence–enabled future: patient perspectives on engagement and health care professional training for adopting artificial intelligence technologies in health care settings. JMIR AI 2023, 2, e40973. [Google Scholar] [CrossRef] [PubMed]
- Najjar, R. Redefining radiology: a review of artificial intelligence integration in medical imaging. Diagnostics 2023, 13, 2760. [Google Scholar] [CrossRef] [PubMed]
- Alowais, S.A.; Alghamdi, S.S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A.I.; Almohareb, S.N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.A. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC medical education 2023, 23, 689. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision medicine, AI, and the future of personalized health care. Clinical and translational science 2021, 14, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Bohr, A.; Memarzadeh, K. Artificial intelligence in healthcare; Academic Press: 2020.
- Thieme, A.H.; Zheng, Y.; Machiraju, G.; Sadee, C.; Mittermaier, M.; Gertler, M.; Salinas, J.L.; Srinivasan, K.; Gyawali, P.; Carrillo-Perez, F. A deep-learning algorithm to classify skin lesions from mpox virus infection. Nature medicine 2023, 29, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, E.; Bayat, Z.; Farrokhi, M.; Karimian, S.; Zahedpasha, R.; Sabzehie, H.; Ramezani Poor, S.; Jafari Khouzani, P.; Aminpour, S.; Karami, M.; et al. Monkeypox: A Comprehensive Review of Virology, Epidemiology, Transmission, Diagnosis, Prevention, Treatment, and Artificial Intelligence Applications. Arch Acad Emerg Med 2024, 12, e70. [Google Scholar] [CrossRef] [PubMed]
- Nyame, J.; Punniyakotti, S.; Khera, K.; Pal, R.S.; Varadarajan, N.; Sharma, P. Challenges in the treatment and prevention of monkeypox infection; A comprehensive review. Acta Trop 2023, 245, 106960. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mpox transmission, symptoms. Mpox is a zoonotic virus that primarily infects humans through skin lesions and contact with infected rats and primates. Direct interaction with an infected individual, respiratory secretions, and vertical transfer from mother to foetus are the three modes by which the disease can pass from one individual to another (social transmission). A typical rash, headache, chills, fatigue, enlarged lymph nodes, muscle and back pain, and fever are all signs of an Mpox.
Figure 1.
Mpox transmission, symptoms. Mpox is a zoonotic virus that primarily infects humans through skin lesions and contact with infected rats and primates. Direct interaction with an infected individual, respiratory secretions, and vertical transfer from mother to foetus are the three modes by which the disease can pass from one individual to another (social transmission). A typical rash, headache, chills, fatigue, enlarged lymph nodes, muscle and back pain, and fever are all signs of an Mpox.
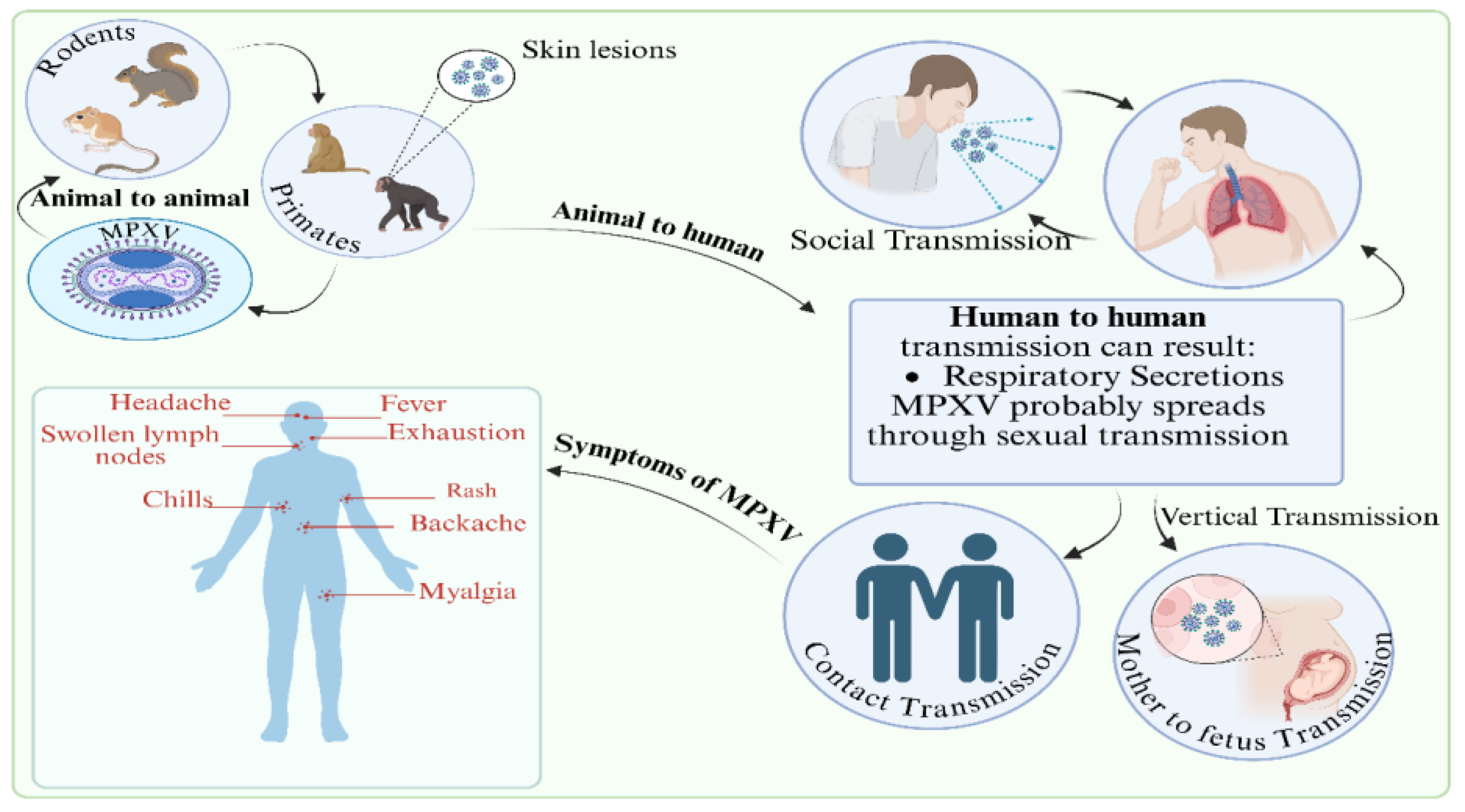
Figure 2.
MPXV infection in the human host showing (red font) action point of cidofovir, brincidofovir, NIOCH-14, and TPOXX.
Figure 2.
MPXV infection in the human host showing (red font) action point of cidofovir, brincidofovir, NIOCH-14, and TPOXX.
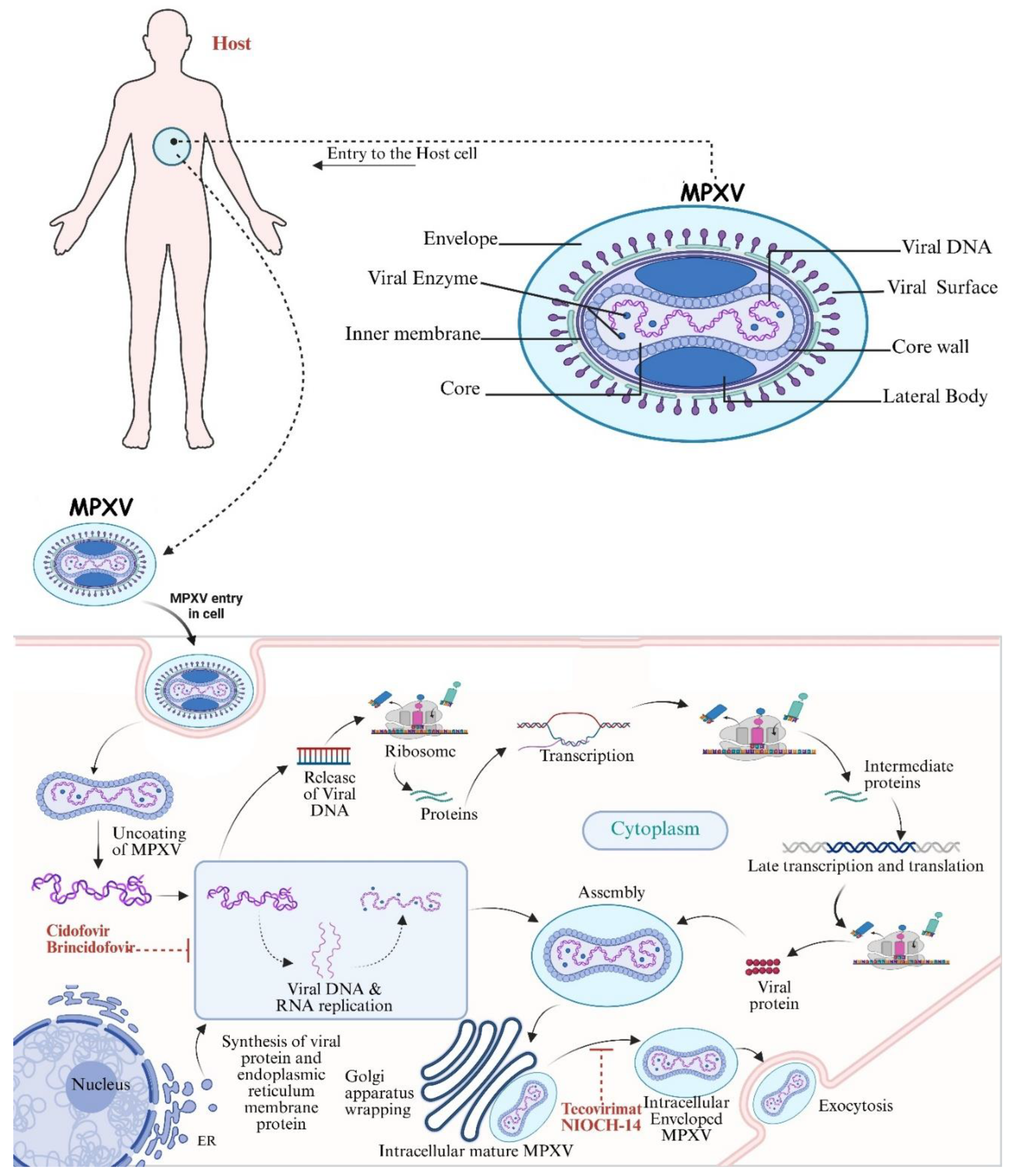
Figure 3.
(a) Global distribution of Mpox cases, highlighting affected countries and reported case numbers [7]. (b) Role of bioinformatics and computational biology in Mpox research, including diagnostic tool development, genome sequencing, drug target identification, and clinical data analysis [124].
Figure 3.
(a) Global distribution of Mpox cases, highlighting affected countries and reported case numbers [7]. (b) Role of bioinformatics and computational biology in Mpox research, including diagnostic tool development, genome sequencing, drug target identification, and clinical data analysis [124].
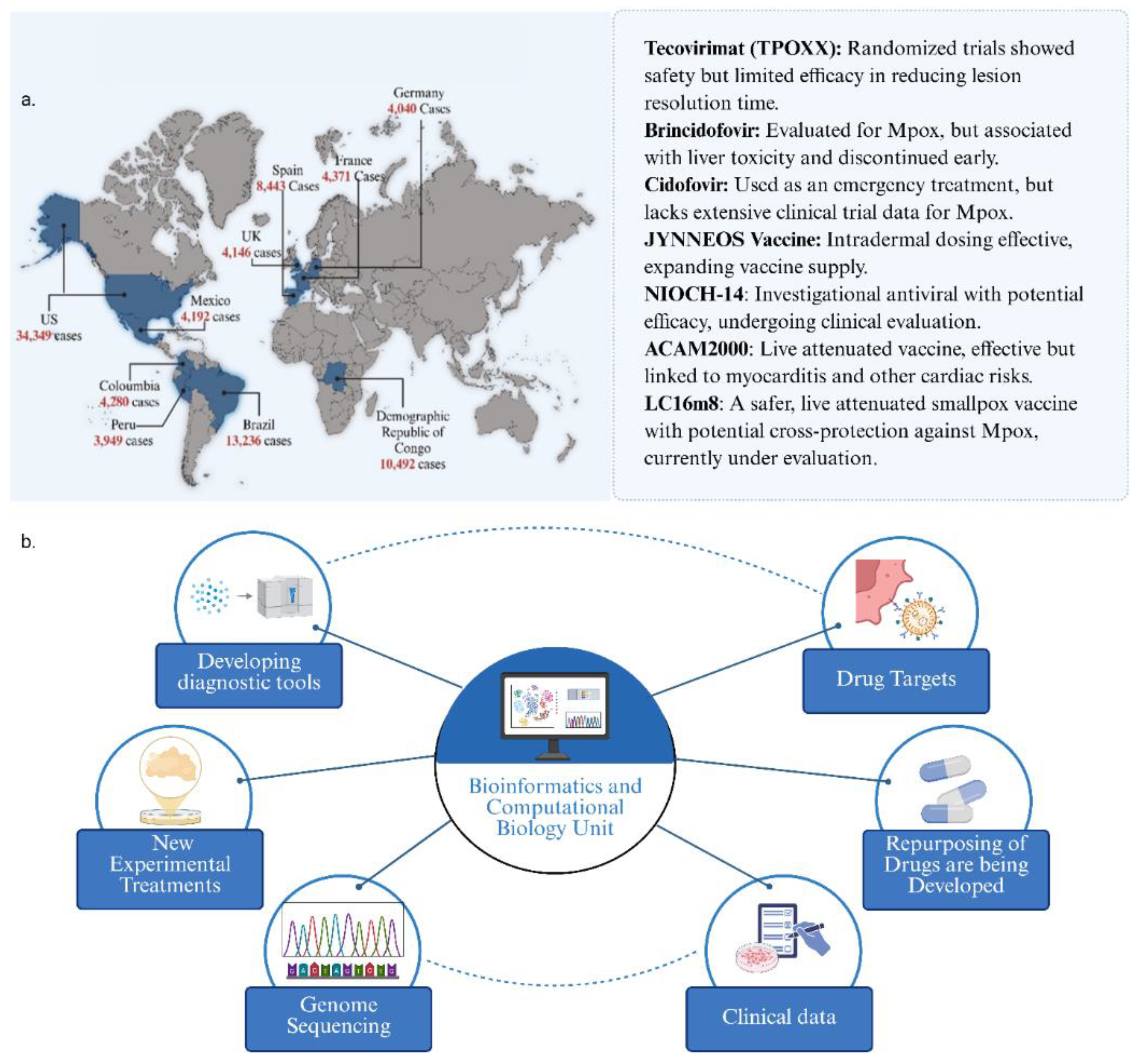
Figure 4.
Methods of Mpox vaccination. Several vaccines (JYNNEOS, LC16m8, ACAM2000, ORTHOPOX VAC), inactivated, DNA, and RNA vaccines, are being evaluated.
Figure 4.
Methods of Mpox vaccination. Several vaccines (JYNNEOS, LC16m8, ACAM2000, ORTHOPOX VAC), inactivated, DNA, and RNA vaccines, are being evaluated.
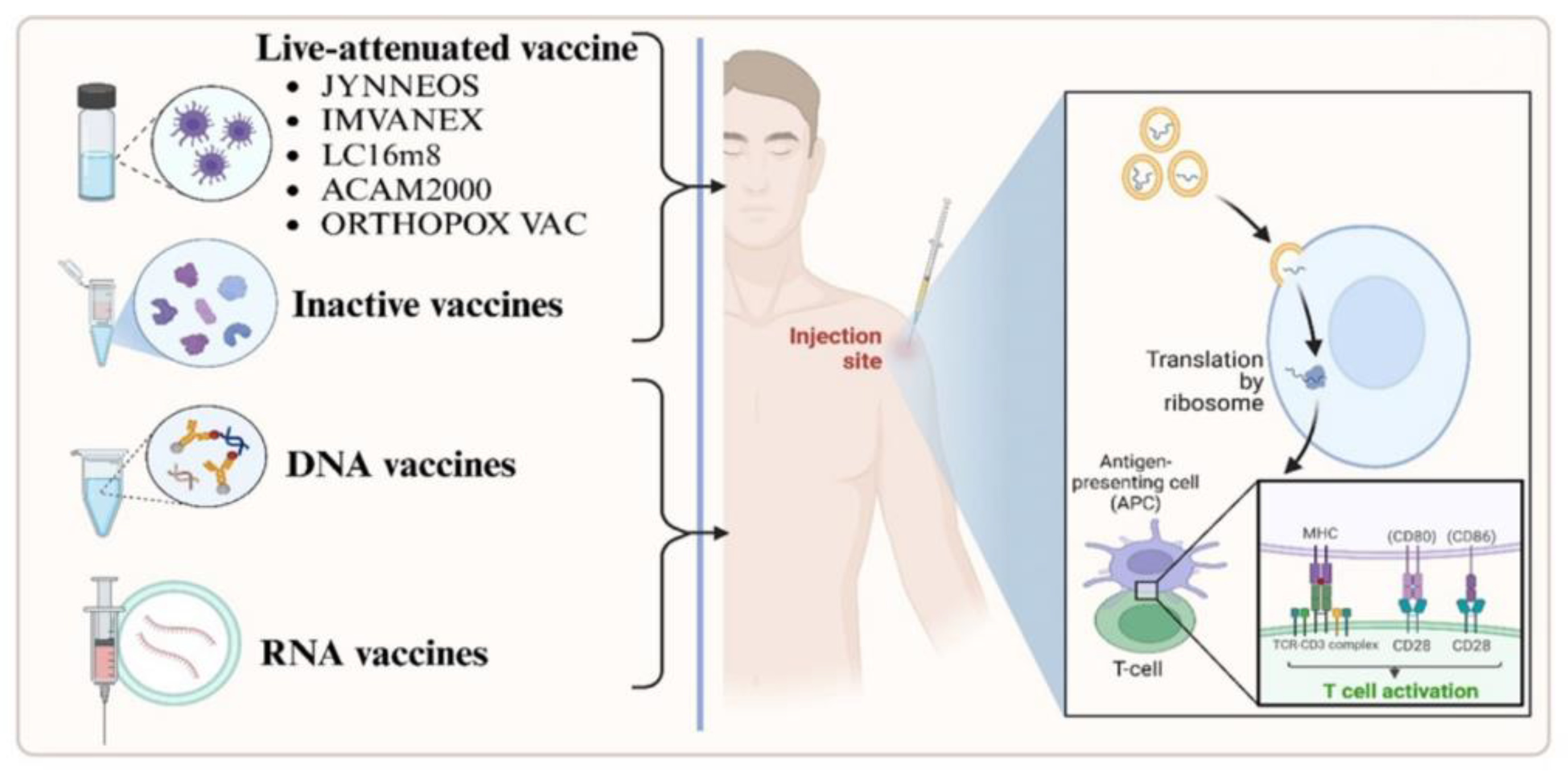
Table 2.
Vaccines against Mpox.
| Vaccine Name | Description | Dosing Regimen | Approved Countries | Reported Side Effects | Refs |
|---|---|---|---|---|---|
| ACAM2000 | Live, replicating vaccinia virus (NYCBH strain) | Single percutaneous dose (2.5 μL) | USA | Myocarditis, pericarditis, encephalitis, progressive vaccinia; contraindicated in immunocompromised individuals and those with certain skin conditions | [130,131] |
| JYNNEOS (also known as Imvanex® or Imvamune®) | Modified Vaccinia Ankara (MVA), non-replicating strain | Two subcutaneous doses (0.5 mL each), 4 weeks apart | USA, Canada, European Union | Mild to moderate local reactions (pain, redness, swelling); fewer systemic side effects; considered safe for immunocompromised individuals | [130,132] |
| LC16m8 (also known as LC16-KMB®) | Live attenuated, minimally replicating vaccinia virus | Single percutaneous dose (2 μL) | Japan | Generally well-tolerated; specific side effects not extensively reported; ongoing studies to assess safety profile | [131] |
| Orthopox Vaccine | Recombinant MVA-based vaccine (live vaccinia VACdelta6-based culture vaccine) | Dosing regimen not specified | Russian Federation (approved in November 2022) | Limited available data on side effects; further studies are required to establish safety and efficacy | [131] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



